november consultation #3
TRANSCRIPT

Taking into account that the patient is a well-knowntelevision personality, his age, that he has not beenproperly using the left eye throughout his life, andthat he wants to maximally improve vision in botheyes, what other evaluations and tests would you per-form? Also, what surgical approach would you use andwhat refractive goal would you target?
- In this interesting case, several factors must beweighed and evaluated. The patient has anisometro-pia, mild amblyopia, possible incipient presbyopia,and cosmetic concerns. In addition, he is not used tohaving the left eye fully corrected.
One of the most important topics to address duringthe preoperative consultation is why the patient wantsrefractive surgery. I would ask him what his goals areand then decide whether they can be achieved or, ide-ally, surpassed. I would also discuss the possibledownsides to this approach.
The patient seeks maximum improvement in visualperformance in both eyes.When a patient explicitly re-quires improvement in vision, it is crucial to determinewhether vision with daily correction is satisfactory. Ifnot and the patient desires better vision, he or she isnot likely a suitable candidate for refractive surgery.Care must be taken to establish whether the patients’dissatisfaction is realistic and can be relieved.
Regarding this television personality’s concern thatan eye deviation will occur postoperatively, it is notclear whether he has a history of strabismus. It canbe assumed that at present, there is no squint. Devia-tion would lead to poor cosmesis and perhaps affectthe visual function of the patient.
With the current spectacle and contact lens correc-tion, only the right eye is corrected. The examinationfound low myopic astigmatism in the right eye and4.50 diopters (D) of (mixed) astigmatism in the lefteye. The CDVA in the left eye is poor. Standard eye ex-aminations are reportedly normal. This implies ortho-phoria, evenwith the uncorrected vision in the left eye.Corneal topography shows no contraindications to ex-cimer laser surgery, and the left eye has a large angle k.In the past, the large angle k may have been misinter-preted as a squint or theremayhave been adisturbancein the ratio between accommodation and convergence.
First, I would further investigate the history; for ex-ample, did the patient have strabismus previously andif so, under what conditions and with what symptoms?I would then correct the left eye with a toric contact lensto simulate a postoperative situation while maintainingthe current correction in the right eye. I would ordera complete orthoptic examination to determine whetherany form of strabismus was present and to rule out fu-sion problems after full refractive correction.
If the patient is happy (cosmetically and visually) af-ter the contact lens trial phase in the left eye, I wouldperform laser in situ keratomileusis (LASIK). I wouldtake care to center the ablation on the corneal vertex.1
This is important in preventing decentration, espe-cially in eyes with a high angle k.2 Spherical overcor-rection in the left eye could achieve monovision,although monovision should also be tested preopera-tively with a trial contact lens.
If the trial phase is unsatisfactory or the orthoptic ex-amination results contraindicate correction of the lefteye, I would propose to the patient that the left eye re-main untouched and that LASIK be performed in theright eye alone.
Michiel H.A. Luger, MDUtrecht, The Netherlands
REFERENCES1. Arbelaez MC, Vidal C, Arba-Mosquera S. Clinical outcomes of
corneal vertex versus central pupil references with aberration-
free ablation strategies and LASIK. Invest Ophthalmol Vis Sci
2008; 49:5287–5294
2. Basmak H, Sahin A, Yildirim N, Papakostas TD,
Kanellopoulos AJ. Measurement of angle kappa with synopto-
phore and Orbscan II in a normal population. J Refract Surg
2007; 23:456–640
2029CONSULTATION SECTION
J CATARACT REFRACT SURG
- Thispatientmustbeapproachedcautiously. In theab-senceof ectasia,we canassume that thehighastigmatismin the left eye is congenital.Unilateralmixed astigmatismoften causes a monofixation syndrome with subtle am-blyopia.Monofixation syndrome is characterizedbysup-pression of central vision in the eye with the blurredretinal imagebutmaintenanceofperipheral binocular fu-sion. That is likely the case here, with amild reduction inCDVA to 20/25 in the left eye. The diagnosis ofmonofix-ation syndrome can be established by Worth 4-dot test-ing. Peripheral stimulation shows fusion (the patientsees 4 dots) and central stimulation shows suppression(thepatient sees2or3dots).The test shouldbeperformedwith best correction under normal room lighting.
If mild amblyopia is present, the visual benefit fromLASIK in the left eye will be limited to an improve-ment in pericentral and peripheral vision, which isless compelling to patients and less likely to producethe delight so commonly associated with LASIK. Thehigh astigmatism increases the likelihood of signifi-cant glare, so the balance of risk versus benefit is notas favorable in this patient as in others.
The patient already wears a soft contact lens;however, apparently the left eye is not properly cor-rected because the CDVA with soft lens correction is20/200. A helpful diagnostic test would be to accu-rately correct the left eye with a toric soft contact lensto see whether the patient notices significant
- VOL 35, NOVEMBER 2009
which I would determine whether the patient foundthe correction satisfactory. This method would give
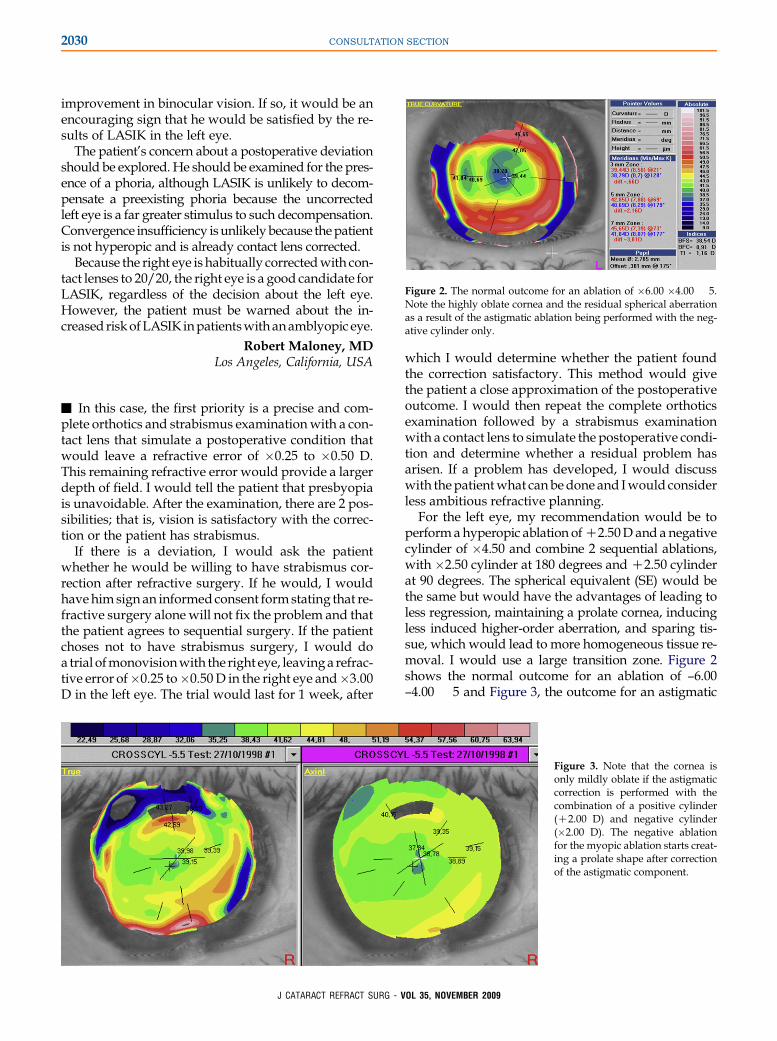
Figure 2. The normal outcome for an ablation of �6.00 �4.00 � 5.Note the highly oblate cornea and the residual spherical aberrationas a result of the astigmatic ablation being performed with the neg-ative cylinder only.
2030 CONSULTATION SECTION
improvement in binocular vision. If so, it would be anencouraging sign that he would be satisfied by the re-sults of LASIK in the left eye.
The patient’s concern about a postoperative deviationshould be explored. He should be examined for the pres-ence of a phoria, although LASIK is unlikely to decom-pensate a preexisting phoria because the uncorrectedleft eye is a far greater stimulus to such decompensation.Convergence insufficiency isunlikelybecause thepatientis not hyperopic and is already contact lens corrected.
Because the right eye is habitually correctedwith con-tact lenses to 20/20, the right eye is a good candidate forLASIK, regardless of the decision about the left eye.However, the patient must be warned about the in-creased riskofLASIK inpatientswithanamblyopic eye.
Robert Maloney, MDLos Angeles, California, USA
- In this case, the first priority is a precise and com-plete orthotics and strabismus examinationwith a con-tact lens that simulate a postoperative condition thatwould leave a refractive error of �0.25 to �0.50 D.This remaining refractive error would provide a largerdepth of field. I would tell the patient that presbyopiais unavoidable. After the examination, there are 2 pos-sibilities; that is, vision is satisfactory with the correc-tion or the patient has strabismus.
If there is a deviation, I would ask the patientwhether he would be willing to have strabismus cor-rection after refractive surgery. If he would, I wouldhave him sign an informed consent formstating that re-fractive surgery alone will not fix the problem and thatthe patient agrees to sequential surgery. If the patientchoses not to have strabismus surgery, I would doa trial ofmonovisionwith the right eye, leavinga refrac-tive error of�0.25 to�0.50D in the right eye and�3.00D in the left eye. The trial would last for 1 week, after
the patient a close approximation of the postoperativeoutcome. I would then repeat the complete orthoticsexamination followed by a strabismus examinationwith a contact lens to simulate the postoperative condi-tion and determine whether a residual problem hasarisen. If a problem has developed, I would discusswith thepatientwhat canbedone and Iwould considerless ambitious refractive planning.
For the left eye, my recommendation would be toperformahyperopic ablation ofC2.50D and a negativecylinder of �4.50 and combine 2 sequential ablations,with �2.50 cylinder at 180 degrees and C2.50 cylinderat 90 degrees. The spherical equivalent (SE) would bethe same but would have the advantages of leading toless regression, maintaining a prolate cornea, inducingless induced higher-order aberration, and sparing tis-sue, which would lead to more homogeneous tissue re-moval. I would use a large transition zone. Figure 2shows the normal outcome for an ablation of –6.00–4.00 � 5 and Figure 3, the outcome for an astigmatic
Figure 3. Note that the cornea isonly mildly oblate if the astigmaticcorrection is performed with thecombination of a positive cylinder(C2.00 D) and negative cylinder(�2.00 D). The negative ablationfor the myopic ablation starts creat-ing a prolate shape after correctionof the astigmatic component.
J CATARACT REFRACT SURG - VOL 35, NOVEMBER 2009