november 16, 2010. hydronephrosis hydroureteronephrosis pyelectasis pyelocaliectasis screening...
TRANSCRIPT
Urology Board Review
November 16, 2010
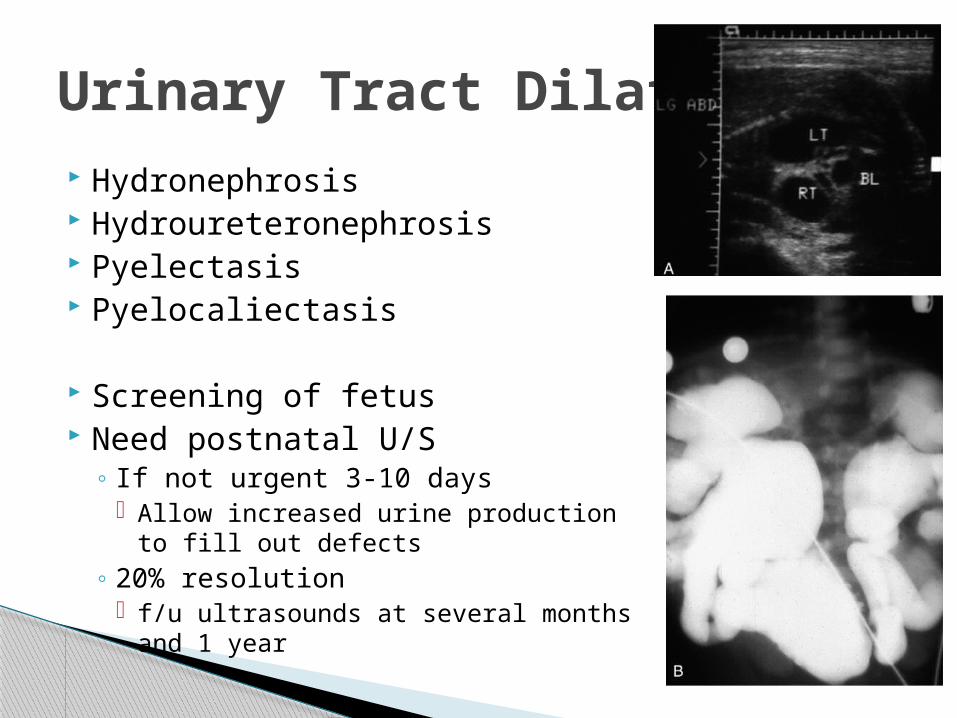
Hydronephrosis Hydroureteronephrosis Pyelectasis Pyelocaliectasis
Screening of fetus Need postnatal U/S
◦ If not urgent 3-10 days Allow increased urine production to fill
out defects◦ 20% resolution
f/u ultrasounds at several months and 1 year
Urinary Tract Dilation
On discharge examination of a female newborn infant, you notice a palpable mass in the right abdomen. An abdominal ultrasound reveals hydronephrosis. What is the next study that should be performed?
A. IVPB. CystoscopyC. VCUGD. Renal ScanE. No intervention at this time
Question 1
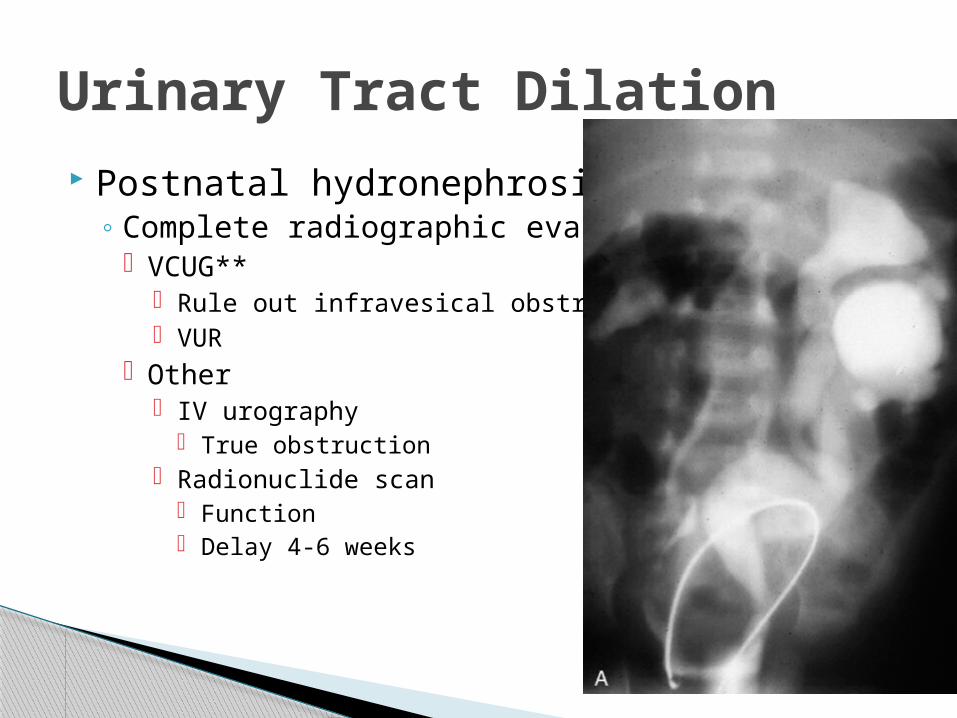
Postnatal hydronephrosis◦ Complete radiographic eval
VCUG** Rule out infravesical obstruction VUR
Other IV urography
True obstruction Radionuclide scan
Function Delay 4-6 weeks
Urinary Tract Dilation
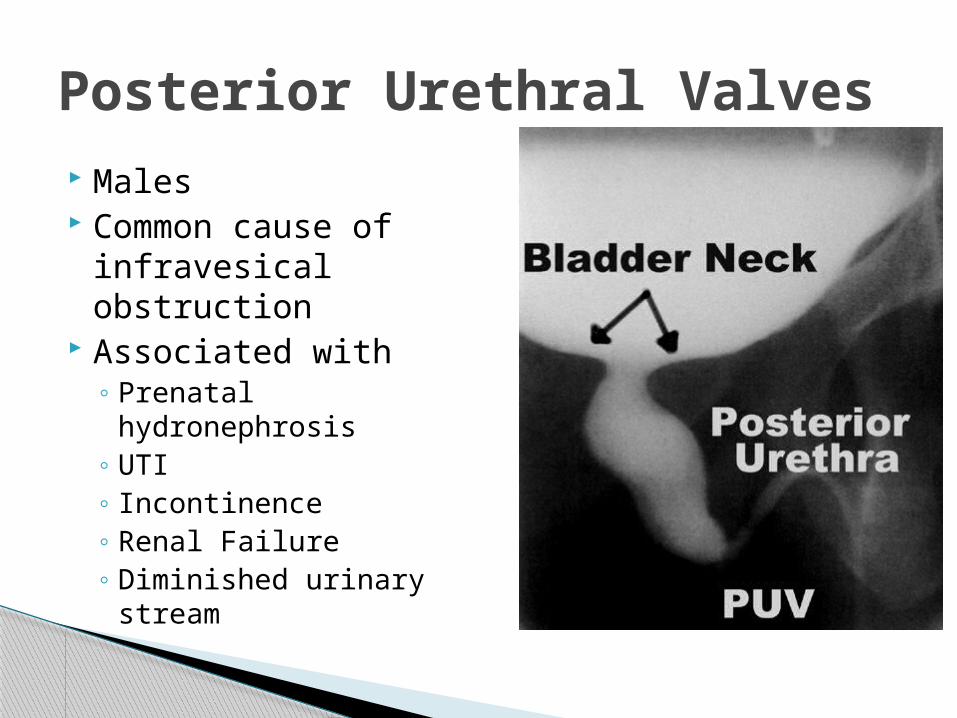
Males Common cause of
infravesical obstruction
Associated with◦ Prenatal hydronephrosis◦ UTI◦ Incontinence◦ Renal Failure◦ Diminished urinary
stream
Posterior Urethral Valves
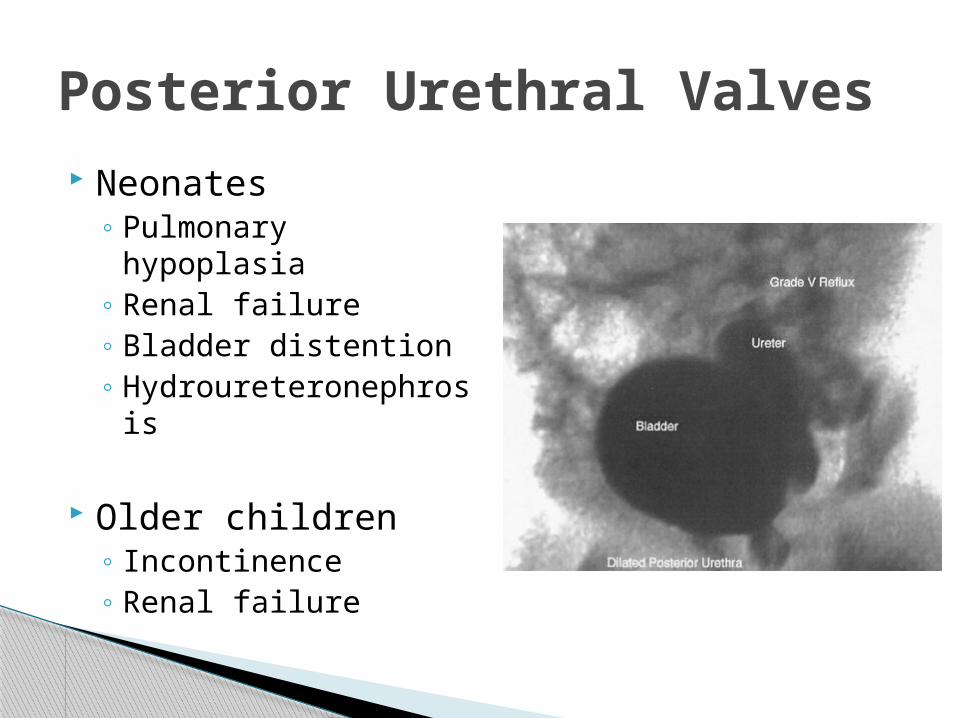
Neonates◦ Pulmonary hypoplasia◦ Renal failure◦ Bladder distention◦ Hydroureteronephrosis
Older children◦ Incontinence◦ Renal failure
Posterior Urethral Valves
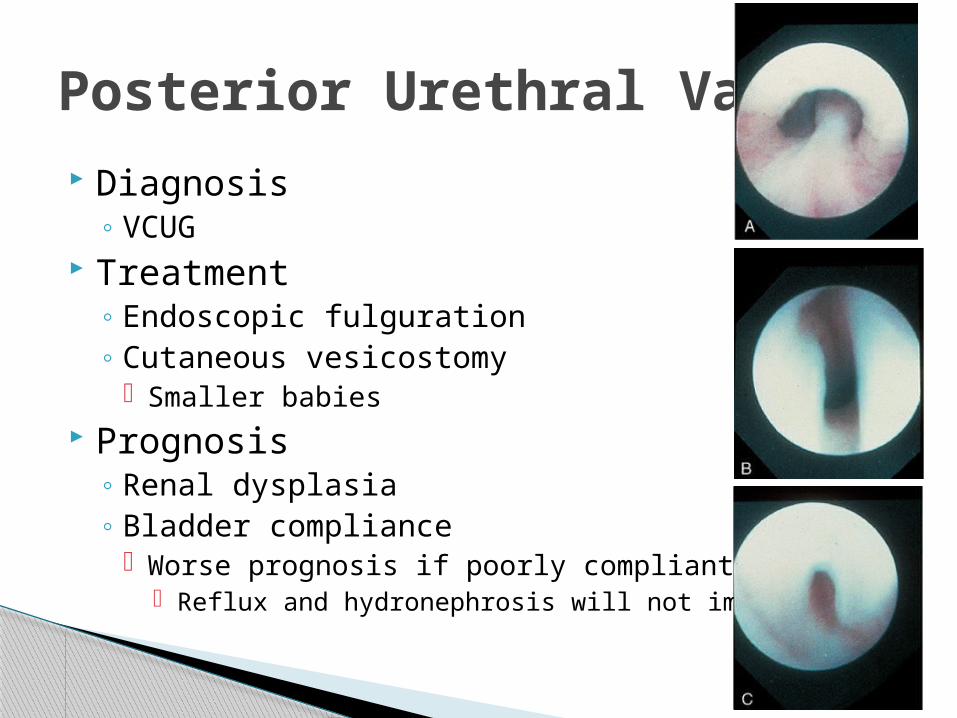
Diagnosis◦ VCUG
Treatment◦ Endoscopic fulguration◦ Cutaneous vesicostomy
Smaller babies Prognosis
◦ Renal dysplasia◦ Bladder compliance
Worse prognosis if poorly compliant Reflux and hydronephrosis will not improve
Posterior Urethral Valves
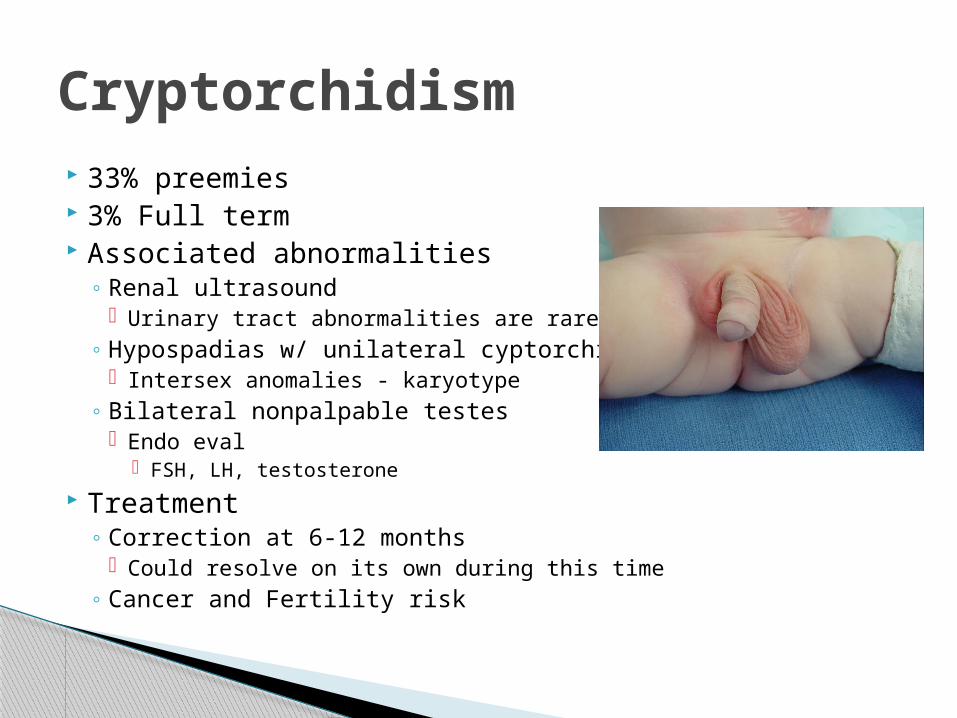
33% preemies 3% Full term Associated abnormalities
◦ Renal ultrasound Urinary tract abnormalities are rare
◦ Hypospadias w/ unilateral cyptorchidism Intersex anomalies - karyotype
◦ Bilateral nonpalpable testes Endo eval
FSH, LH, testosterone
Treatment◦ Correction at 6-12 months
Could resolve on its own during this time◦ Cancer and Fertility risk
Cryptorchidism
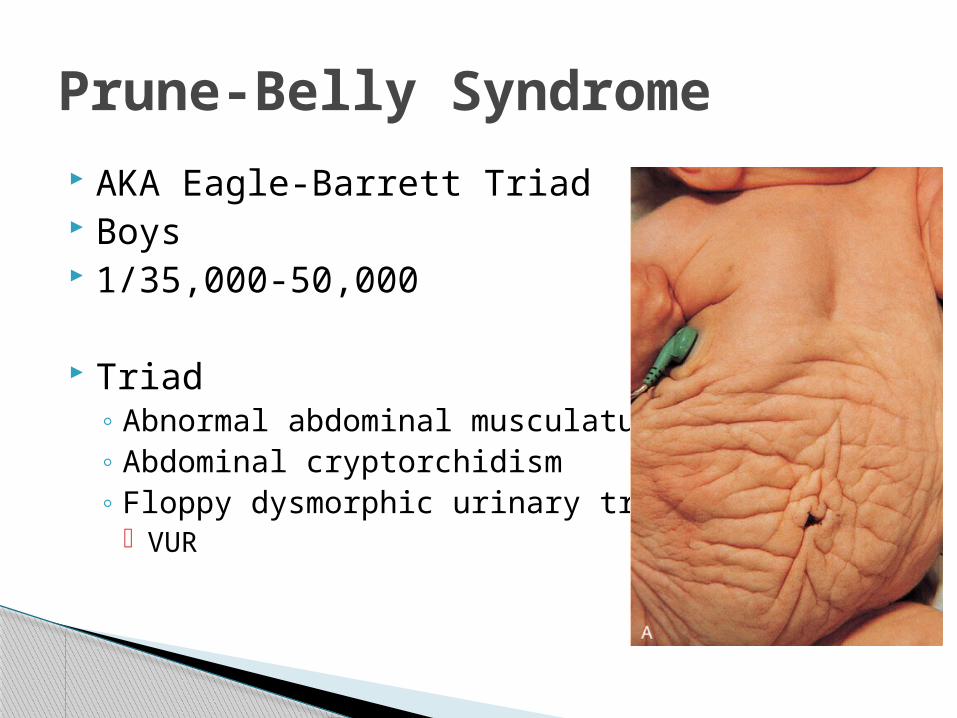
AKA Eagle-Barrett Triad Boys 1/35,000-50,000
Triad◦ Abnormal abdominal musculature◦ Abdominal cryptorchidism◦ Floppy dysmorphic urinary tracts
VUR
Prune-Belly Syndrome
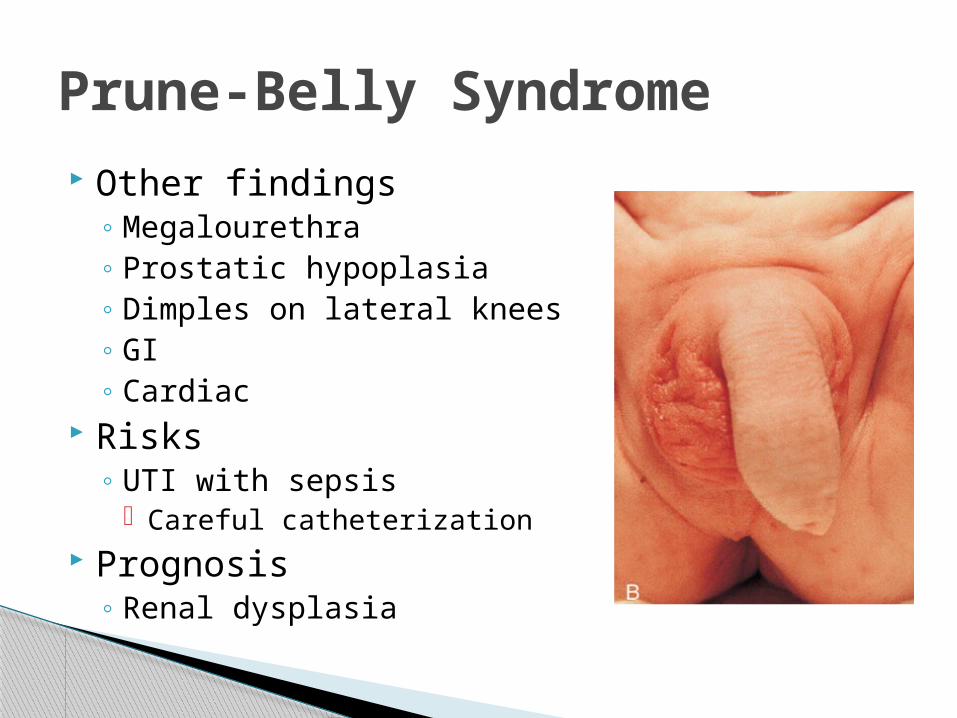
Other findings◦ Megalourethra◦ Prostatic hypoplasia◦ Dimples on lateral knees◦ GI◦ Cardiac
Risks◦ UTI with sepsis
Careful catheterization Prognosis
◦ Renal dysplasia
Prune-Belly Syndrome
A mother brings her infant into the office because she has noticed a continual drainage from her umbilicus. You suspect a patent urachus. You explain to the mother that this results from an abnormal communication between . . .
A. The bladder and umbilicusB. A ureter and the umbilicusC. The small intestine and the umbilicusD. The renal pelvis and the umbilicusE. The colon and the umbilicus
Question 2
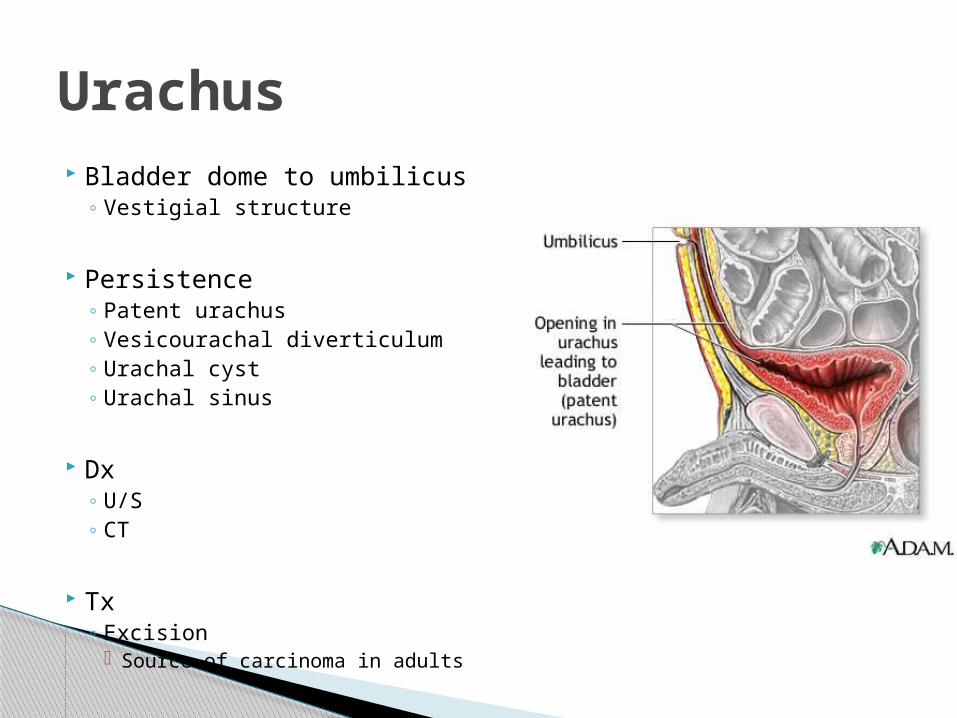
Bladder dome to umbilicus◦ Vestigial structure
Persistence◦ Patent urachus◦ Vesicourachal diverticulum◦ Urachal cyst◦ Urachal sinus
Dx◦ U/S◦ CT
Tx◦ Excision
Source of carcinoma in adults
Urachus
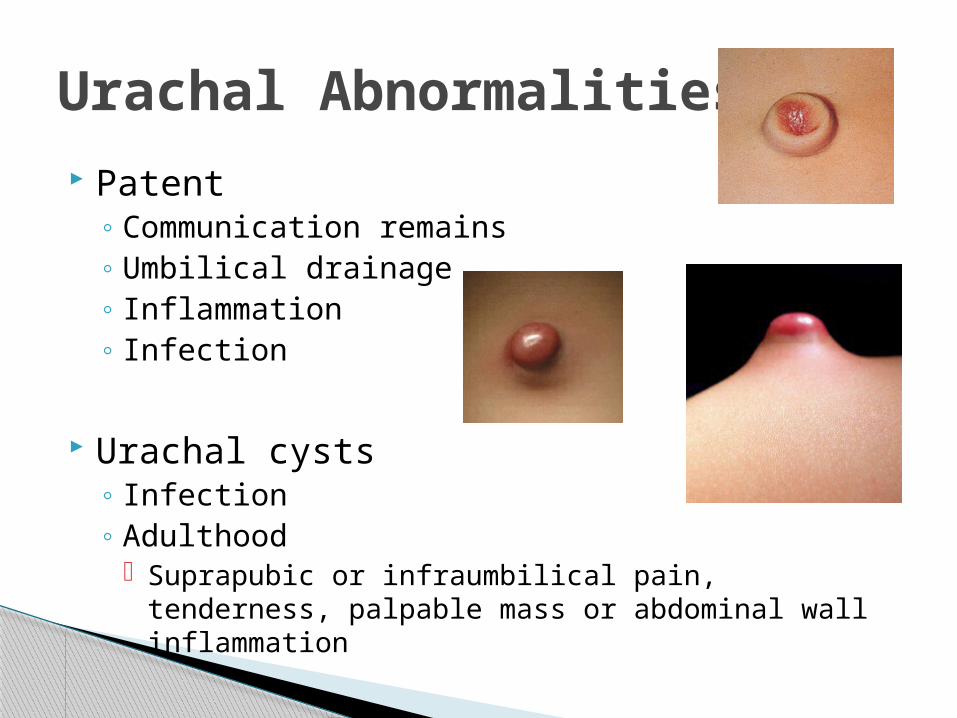
Patent◦ Communication remains◦ Umbilical drainage◦ Inflammation◦ Infection
Urachal cysts◦ Infection ◦ Adulthood
Suprapubic or infraumbilical pain, tenderness, palpable mass or abdominal wall inflammation
Urachal Abnormalities
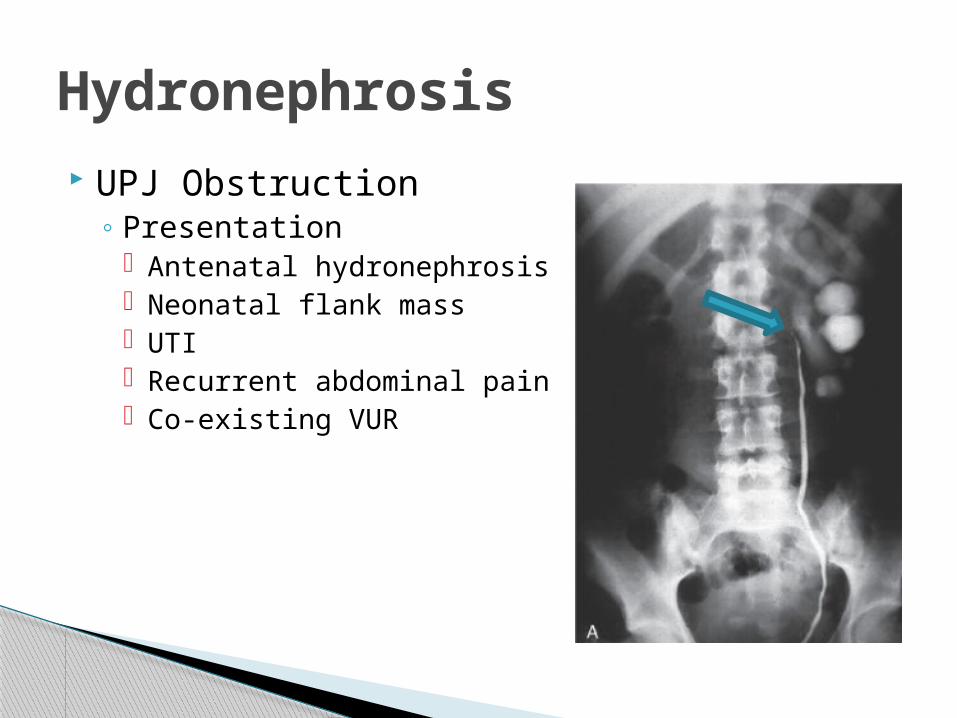
UPJ Obstruction◦ Presentation
Antenatal hydronephrosis Neonatal flank mass UTI Recurrent abdominal pain Co-existing VUR
Hydronephrosis
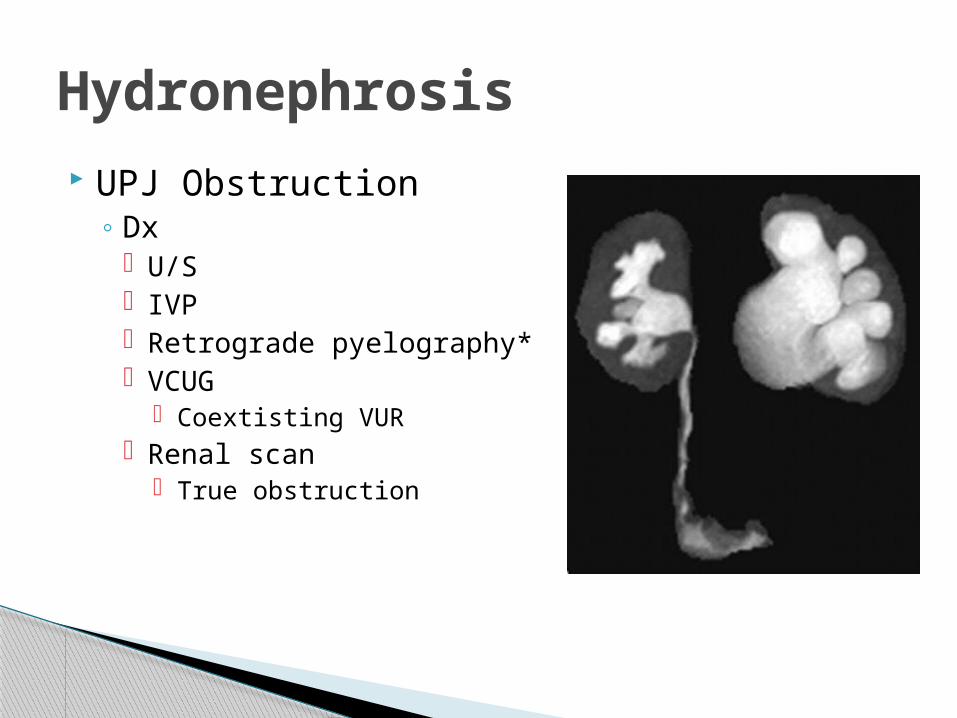
UPJ Obstruction◦ Dx
U/S IVP Retrograde pyelography* VCUG
Coextisting VUR Renal scan
True obstruction
Hydronephrosis
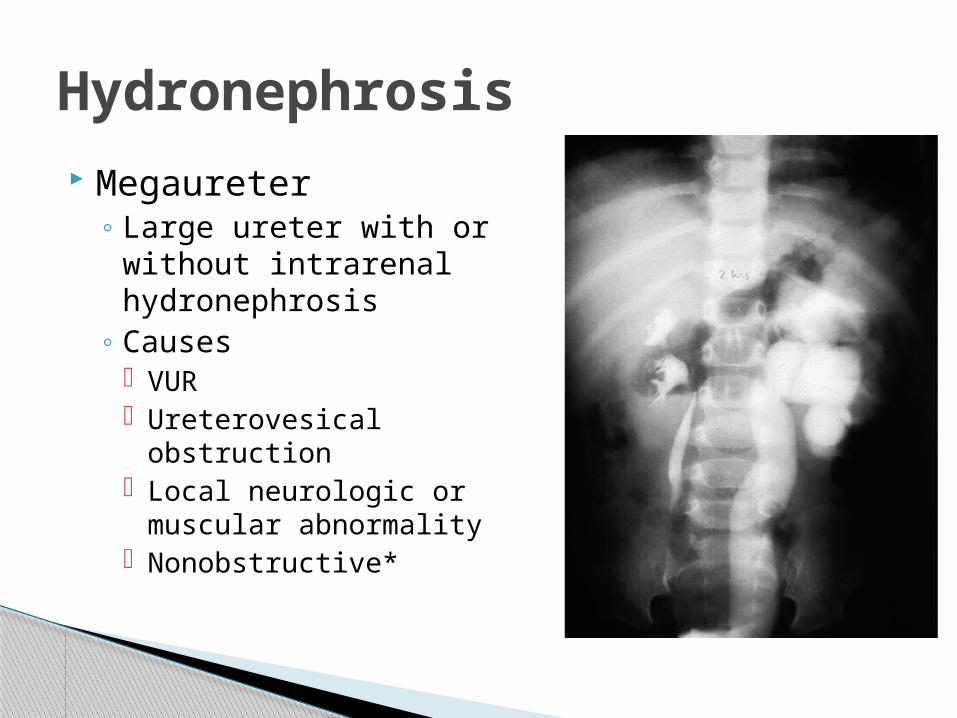
Megaureter◦ Large ureter with or
without intrarenal hydronephrosis
◦ Causes VUR Ureterovesical
obstruction Local neurologic or
muscular abnormality Nonobstructive*
Hydronephrosis
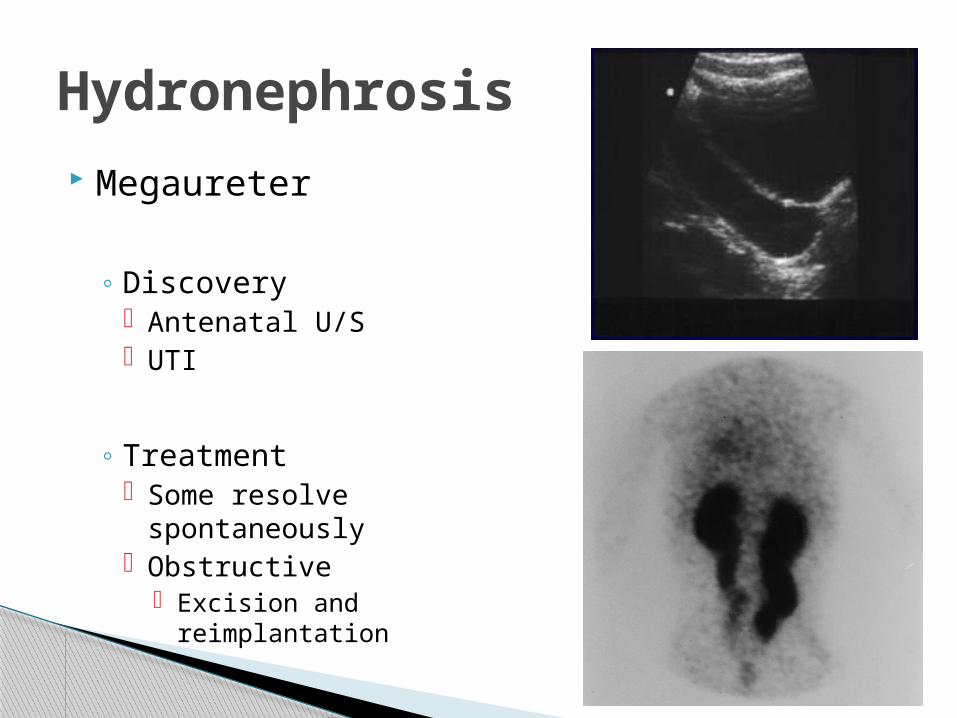
Megaureter
◦ Discovery Antenatal U/S UTI
◦ Treatment Some resolve
spontaneously Obstructive
Excision and reimplantation
Hydronephrosis
After palpating a left sided mass at a well visit in a 2 month old, a renal ultrasound shows that your patient has a multicystic dysplastic kidney. A renal scan of this dysplastic kidney is most likely to show . . .
A. Full functionB. No function C. 50% functionD. 25% functionE. 75% function
Question 3
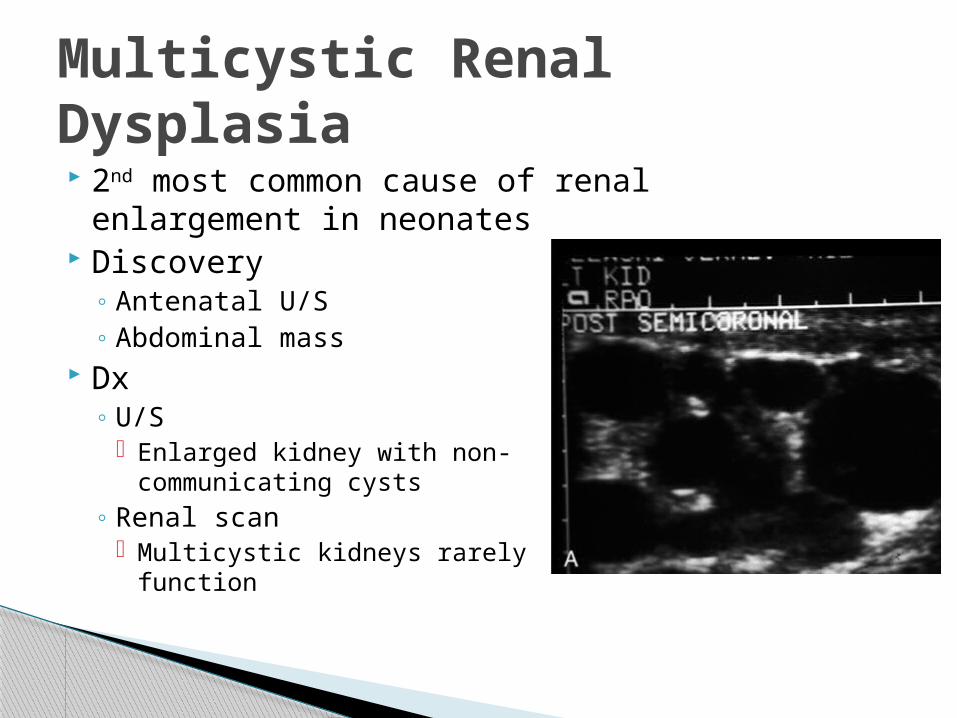
2nd most common cause of renal enlargement in neonates
Discovery◦ Antenatal U/S◦ Abdominal mass
Dx◦ U/S
Enlarged kidney with non-communicating cysts
◦ Renal scan Multicystic kidneys rarely function
Multicystic Renal Dysplasia
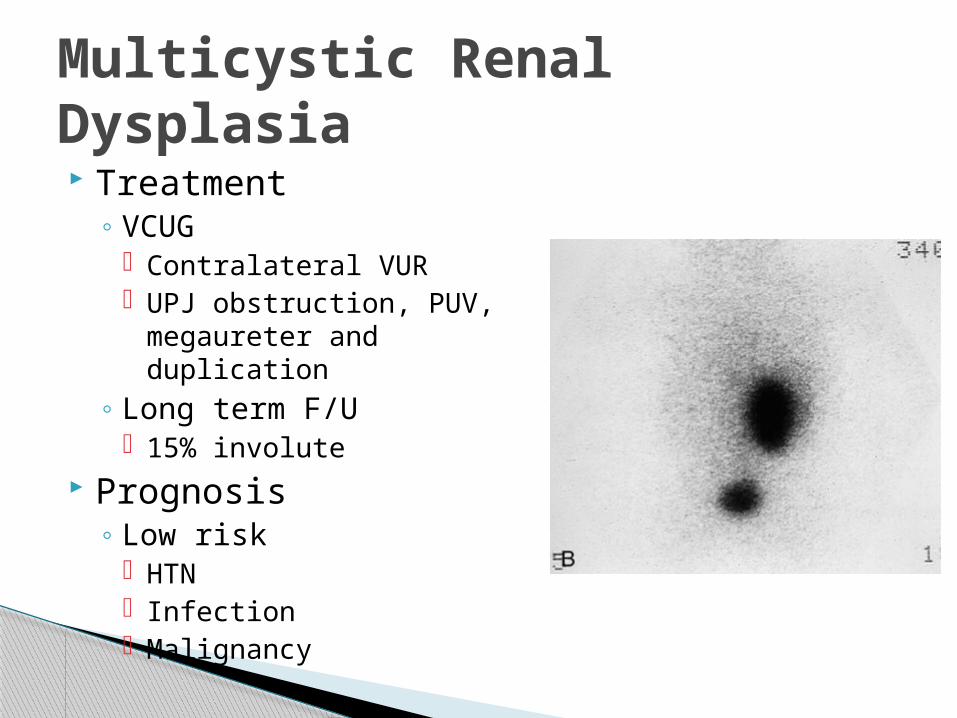
Treatment◦ VCUG
Contralateral VUR UPJ obstruction, PUV,
megaureter and duplication◦ Long term F/U
15% involute Prognosis
◦ Low risk HTN Infection Malignancy
Multicystic Renal Dysplasia
Usually benign Usually incidental finding Evaluation
◦ U/S◦ CT◦ Cyst aspiration if suspicious
DDx◦ Cystic Wilms tumor◦ Multilocular cystic dysplasia◦ Duplication anomaly with
hydronephrosis◦ Calyceal diverticulum◦ Adult polycystic disease
Simple Renal Cysts