northern care alliance nhs group salford royal nhs
TRANSCRIPT
Northern Care Alliance NHS GroupSalford Royal NHS Foundation Trust (SRFT)
Group Board (Committees in Common) The Group Board operates as a Committees in Common and conducts shared meeting of:
Group Board (Salford) – established by Salford Royal NHS Foundation Trust; andGroup Board (Oldham, Bury and Rochdale) – established by Pennine Acute Hospitals NHS Trust
Summary Minutes – Non-Confidential Mattersfrom the meeting held on: Monday, 27 April 2020
from 10.30am, via video-conferencing facility
Present:Mr Jim Potter, ChairmanMr Raj Jain, Chief Executive Officer Mrs Judith Adams, Chief Delivery Officer Mr Chris Brookes, Chief Medical Officer Ms Nicky Clarke, Chief People OfficerMr Kieran Charleson, Non-Executive DirectorMr Tim Crowley, Non-Executive DirectorMrs Carmen Drinkwater, Non-Executive DirectorMrs Nicola Firth, Director of Nursing/Chief Officer Oldham Care Organisation Mrs Elaine Inglesby-Burke CBE, Chief Nursing Officer Mrs Christine Mayer CBE, Non-Executive Director/Vice ChairmanMr Ian Moston, Chief Finance OfficerProfessor Chris Reilly, Senior Independent Director Mr Jack Sharp, Chief Strategy OfficerDr Hamish Stedman, Non-Executive Director Mr Peter Turkington, Medical Director/Chief Officer Salford Care Organisation Mr Steve Taylor, Director of Operations/Chief Officer Bury & Rochdale Care Organisation Mrs Jane Burns, Director of Corporate Services and Group SecretaryMrs Rebecca McCarthy, Deputy Group Secretary
ApologiesNone
No. Item Action1 Apologies for Absence
See above
2 Declarations of Interest The Chairman requested that officers declared any actual or potential conflict of interest relevant to their role as members of the Group Committees in Common (Group Board) and in particular to any matter being discussed at the meeting. There were no interests declared.
3 Chairman’s Opening Remarks The Chairman commended the exceptional work of all NCA staff throughout the Covid-19 pandemic. The Chairman expressed sincere condolences, on behalf of the Group Board, to those NHS staff who had lost their lives due to Covid-19, especially remembering a long-serving member of the NCA family. The Group Board held a one minute silence to pay their respect.
The Chairman acknowledged and thanked a number of companies that had shared donations and hospitality over recent weeks.
4 Minutes of the Previous Meeting (Part 2 – Held in Private) The minutes from the private meeting of the Group Board held on 30th March were approved as a true record.
1/5
NCA #
732
562
05/2
2/20
20 12:
29:0
0
1/72
No. Item Action5 Matters Arising
No matters arising.
6 Interim Governance and Board Assurance Framework 2020/21 The Chief Executive Officer presented a paper describing the interim governance arrangements in place for the period of the major incident. He confirmed that the Covid-19 operating model had been shared with the Group Board [March 2020] and described the responsibilities and accountability required during the public health emergency. He highlighted that in order to ensure effective governance arrangements were maintained throughout the period of response to the Covid-19 pandemic, a number of high-level interim principal objectives had been established for the period of the major incident response; these would be reviewed at commencement of the major incident recovery phase. He added that the high-level interim principal objectives had enabled the development of an Interim Group Board Assurance Framework (BAF) and Interim BAFs for each of the Care Organisations and the Diagnostics and Pharmacy Group Business Unit. The Interim Group BAF was presented for review by the Group Board.
The Group Board: reviewed and approved the interim governance arrangements, including the
high-level principal objectives for the period of the major incident response; and reviewed the Group Board Assurance Framework, confirming that risk was
adequately identified and effective mitigating action plans were in place.
7 Provision of Personal Protective Equipment (PPE) The Chief Medical Officer presented a paper advising that the safety of staff was front and centre in the approach of the Northern Care Alliance NHS Group (NCA) to the current global pandemic, emphasising the importance of ensuring that staff had the personal protection equipment (PPE) they needed. The Chief Medical Officer commented that a concerted collective effort, overseen by the NCA Gold Command, had coordinated a cohesive response to the provision of appropriate PPE for the NCA’s staff. The Chief Medical Officer comprehensively described action taken in relation to the provision of PPE for staff.
Group Board (Committees in Common) reviewed the information provided and confirmed the robustness of the plans in place to ensure the safety of staff.
8 COVID-19 Communication Delivery Plan The Chief Strategy Officer provided a detailed presentation on theinformation about the NCA’s Covid-19 Ccommunications Ddelivery Pplan for assuring the NCA’s Covid-19 ‘comms experience’:. The Board acknowledged the comprehensive communications approach and the importance of effective feedback mechanisms with respect to communications to evaluate how the communications were received at all levels of the organisation. The Chief Strategy Officer highlighted the initiatives in place to obtain feedback from staff across the organisation.
Group Board (Committees in Common) confirmed the Covid-19 communications delivery plan.
9 Core Services: Operational Response The Chief Delivery Officer presented a paper providing details of the NCA’s broad operational response to the Covid-19 national emergency. The Chief Delivery Officer confirmed that rapid operational action had been taken by the NCA, aligned to the national strategy and areas of learning from the new ways of working would continue to be explored as they emerged in order to ensure sustainable delivery of operational objectives and NCA recovery plans.
Group Board (Committees in Common) received and noted this update.
10 Quality Surveillance Report The Chief Nursing Officer presented a summary of key points from Incidents, Inquests, Learning From Deaths Report, Safeguarding, Learning From Experience, and the Quality Dashboard. She highlighted that many measures from the Quality Dashboard, as well as the Learning from Deaths Report, utilised data from Dr. Foster and SHMI which was typically
2/5
NCA #
732
562
05/2
2/20
20 12:
29:0
0
2/72

No. Item Actionreported several months in arrears, therefore did not yet reflect the current Covid-19 crisis.
Group Board (Committees in Common) reviewed and confirmed the Quality Surveillance Report.
11 Standards of Business Conduct: Board Level Directors (Public)The Director of Corporate Services presented a paper providing information about:
the declared interests of all members of the Board of Directors of Salford Royal NHS Foundation Trust (SRFT), the NCA Group Board and each of the Care Organisation’s Leadership Teams;
the independence of SRFT Non-Executive Directors in line with the NHS FT Code of Governance (Provision B.1.2); and
compliance with the Fit and Proper Person Requirements (FPPR), as it applies to all members of the Board of Directors of Salford Royal NHS Foundation Trust (SRFT), the NCA Group Board and each of the Care Organisation’s Leadership Teams.
The Group Board confirmed current interests for Directors as follows:Name and Position Declared InterestsMr Jim PotterChairman
None
Mrs Christine Mayer CBENon-Executive Director
Associate of Fiona MacNeill Associates, Leadership Facilitation & Coaching
Non-Executive Director, Pennine Acute Hospitals NHS Trust
Professor Chris ReillyNon-Executive Director
ASTAR TDR Expert Review Panel Scientific Advisor: Welcome Trust, Alderley
BioHub, BioVictriX Karus Therapeutics Professor of Practice KCL Board of Directors of Medicines Discovery
Catapult, NHS Transformation Unit and NW EHealth
Dr Hamish StedmanNon-Executive Director
Wife is Diabetes Specialist Nurse Manager at SRFT
Sister in law Paediatric Specialist Nurse at SRFT
Interim Chair Eccles and Irlam Health Social Care Board
Mr Kieran CharlesonNon-Executive Director
Federation of Small Businesses UK Digital Policy Chairman
NED Salford Red Devils RL Club Director Thrive Training
Mrs Carmen DrinkwaterNon-Executive Director
Non-Executive Director East Lancashire Financial Services (ELFS)
Director, Carmen Drinkwater LtdMr Tim CrowleyNon-Executive Director
Independent Audit Committee member of SCOPE
Affiliated with AQuA Member of Public Sector Internal Audit
Standards BoardMr Raj Jain Chief Executive Officer
Director North West eHealth Board Member, MIMIT
Mr Chris BrookesExecutive Chief Medical Officer Deputy Chief Executive Officer
Chief Medical Officer, England and Rugby Football League
Director, Wigan Warriors Rugby League
3/5
NCA #
732
562
05/2
2/20
20 12:
29:0
0
3/72
No. Item Action Director, Chris Brookes Sports Medicine Ltd Principal Medical Advisor to the GM HSCP
Mrs Elaine Inglesby-Burke CBEExecutive Chief Nursing Officer
Trustee of the Willowbrook Hospice: Specialist Palliative Care Unit set up as an Independent Charity, governed by a Board of Trustees and run on a day to day basis by a CEO and management team
Non-Executive Director, Advancing Quality Alliance (AQUA)
Non-Executive Director, National Institute for Health and Care Excellence (NICE)
Mr Ian MostonExecutive Chief Financial Officer
Director, RS-Chime Ltd Council Member, University of Salford Partner is Director of Workforce, Christie NHS
Foundation Trust
Mrs Judith AdamsExecutive Chief Delivery Officer
None
Mr Jack SharpChief of Strategy
None
Ms Nicola ClarkeChief of People
None
Mrs Nicola FirthChief Officer / Director of Nursing – Oldham Care Organisation
None
Mr Steven TaylorChief Officer - Bury & Rochdale Care Organisation
Governor - Hopwood Hall College
Dr Peter TurkingtonChief Officer / Medical Director, Salford Care Organisation
Private and Medico-Legal Practice at Spire Hospital Manchester
Director. Turkington Ltd
Mrs Diane MorrisonDirector of Finance, Salford Care Organisation
None
Mr Tyrone RobertsDirector of Nursing, Salford Care Organisation
None
Mrs Katie Foster – GreenwoodDirector of Operations, Salford Care Organisation
Partner works for Pennine Acute Hospitals NHS Trust
Mr Jonathan MoiseMedical Director, Oldham Care Organisation
None
Mr Dan GrimesManaging Director, Oldham Care Organisation
None
Mr David Jago None
4/5
NCA #
732
562
05/2
2/20
20 12:
29:0
0
4/72
No. Item ActionDirector of Finance, Oldham Care Organisation
Dr Shona McCallumMedical Director, Bury and Rochdale Care Organisation
Husband is the Clinical Chair for Heywood, Middleton and Rochdale (HMR) CCG
Mrs Jacqui BurrowDirector of Nursing, Bury and Rochdale Care Organisation
None
Mr Craig CarterDirector of Finance, Bury and Rochdale Care Organisation
None
Independence of Non-Executive DirectorsThe Group Board considered criteria relevant to the determination of the independence of Non-Executive Directors. The Group Board acknowledged that three Non-Executive Directors had declared a material business relationship with the NHSFT directly, or as a partner, shareholder, director or senior employee of a body that has such a relationship with the NHSFT. Additionally, the Group Board acknowledged that uniquely, Non-Executive Directors at SRFT were members only of the Board of Directors, Group Board, Strategy & Investment Committee and Board statutory committees. Non-Executive Directors were not members of any sub-Board operational management, governance or assurance committees and therefore retained significant independence from the operational management of Group.
Group Board confirmed the independence of each individual Non-Executive Director.
Chairman’s Annual Assessment of the Fit and Proper Person Requirement for all Board-level directors The Group Secretary informed the Group Board that the Chairman had conducted the annual assessment of continued compliance with the Fit and Proper Person Requirement and had concluded that all directors, including all Board-level directors, should be considered to be deemed fit and that there is nothing to suggest that any director meets any of the unfit criteria.
The Group Board endorsed the Chairman’s annual assessment of the Fit and Proper Person Requirement for all Board-level directors.
12 The Group Board received the following papers for information: Key Performance Indicator Benchmarking Report – 2019/20 Year End Learning from Experience Report Quality Improvement Dashboard Learning from Deaths Report Safeguarding Report Summary from Group Risk and Assurance (GRAC) Committee – meeting held on 20th
April 2020 Board Action Sheet
Close.
5/5
NCA #
732
562
05/2
2/20
20 12:
29:0
0
5/72
Northern Care Alliance NHS GroupSalford Royal NHS Foundation Trust (SRFT)
Meeting Group Board (Committees in Common)
Author (s) Jane Burns, Director of Corporate Services and Group Secretary
Presented by Raj Jain, Chief Executive
Date 26th May 2020
Executive Summary
The Group Board Assurance Framework (BAF) is presented to this May Group Board meeting. The high-level interim principal objectives have been identified and enabled
the development of an Interim Group BAF Principal Risks, to the delivery of the interim principal objectives, have been
identified by Group Directors. Group Directors hold responsibility for each Principal Risk and each risk is
also assigned to a relevant governance committee, where actions drive meeting agendas to ensure effective and timely management of identified risk.
All Risks have been reviewed be their relevant risk owners. Principal and operational risks, scored at 12 or above, on the Care
Organisations’ Board Assurance Frameworks/Corporate Risk Registers have been referenced within the Group Board Assurance Framework
High level Principal Risks (scored ≥ 12), to the delivery of the Interim Principal Objectives, have been identified.
8 risks score 12 and above, relating to incident plans, non-COVID19 service, staff experience, two finance risks, the transaction and 2 IT infrastructure risks.
3 of the risks score 13 one of which, risk relating to non-COVID 19, services, has been reduced to 13 from 14.
Recommendations The Group Board is asked: review the Group Board Assurance Framework, confirm that risks
are adequately identified and effective mitigating action plans are in place.
Equality Does this paper relate to a matter where equality issues may arise? N
This document does not contain confidential information and can be made available to the public.
This document contains some confidential information that would need to be redacted before the document was made available to the public.
Freedom of Information Please ‘cross’ one of the boxes
This document is entirely confidential, as the redaction of confidential information would render the document meaningless.
Title of Report Interim Board Assurance Framework 2020/21
x
1/1
NCA #
732
562
05/2
2/20
20 12:
29:0
0
6/72

Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 1 of 15
Summary
Risk Subject: Risk Score1.1 IF robust major incident plans are not in place and fully enacted 13
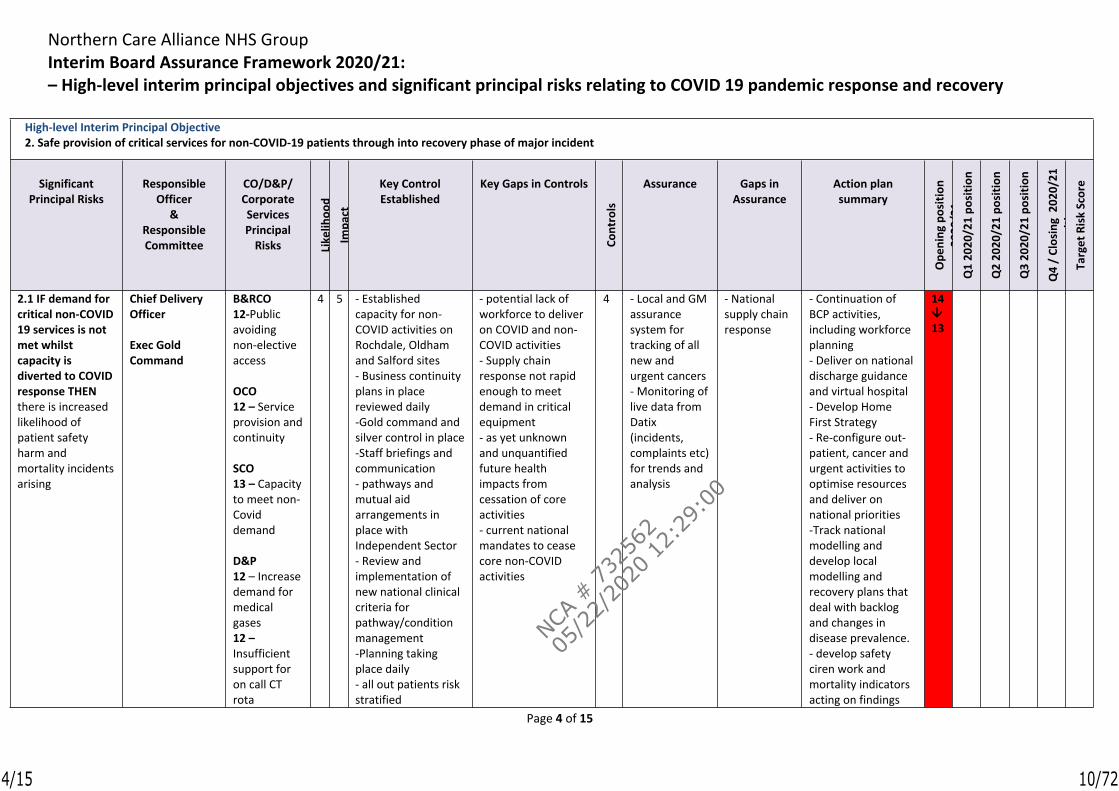
2.1 IF demand for critical non-COVID 19 services is not met whilst capacity is diverted to COVID response
Reduced to a 13 - will begin to undertake more Non-Covid work and Urgent Care presentations increase
14 13
3.1 IF we fail to have in place a process to improve experience of our staff 12
4.1 IF we do not develop an effective productivity improvement and cost reduction strategy 12
4.2 IF the planned activity and income levels and/or expenditure controls are exceeded 12
5.1 IF we fail to secure the transaction and associated investment 12
7.1 If the NCA’s IT Infrastructure, applications and end-user devices are not brought up to date and replaced or upgraded when they reach end of life
13
7.2 If plans and business case funding to develop an Single Integrated IT infrastructure are delayed by ongoing COVID Incident management and move of transaction timeline
12
1/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
7/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 2 of 15
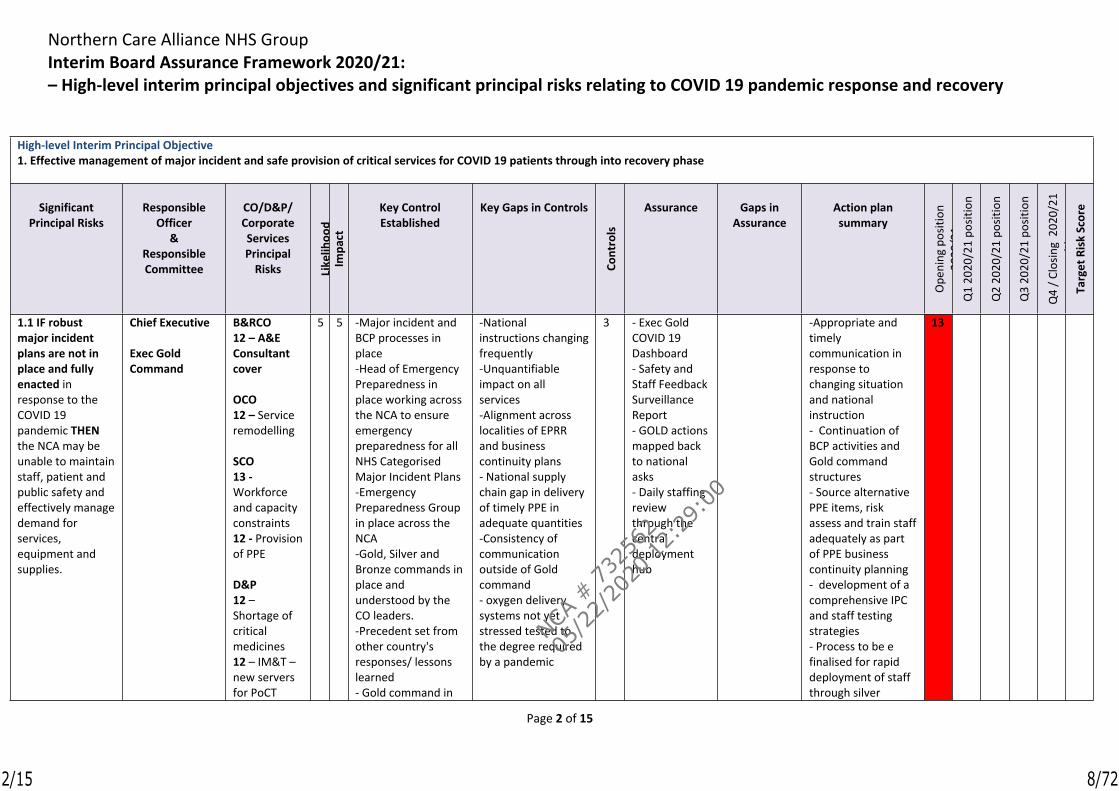
High-level Interim Principal Objective 1. Effective management of major incident and safe provision of critical services for COVID 19 patients through into recovery phase
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services Principal
Risks Like
lihoo
dIm
pact
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1Q
1 20
20/2
1 po
sitio
n
Q2
2020
/21
posit
ion
Q3
2020
/21
posit
ion
Q4
/ Clo
sing
202
0/21
po
sitio
nTa
rget
Ris
k Sc
ore
1.1 IF robust major incident plans are not in place and fully enacted in response to the COVID 19 pandemic THEN the NCA may be unable to maintain staff, patient and public safety and effectively manage demand for services, equipment and supplies.
Chief Executive
Exec Gold Command
B&RCO12 – A&E Consultant cover
OCO 12 – Service remodelling
SCO13 - Workforce and capacity constraints12 - Provision of PPE
D&P12 – Shortage of critical medicines12 – IM&T – new servers for PoCT
5 5 -Major incident and BCP processes in place-Head of Emergency Preparedness in place working across the NCA to ensure emergency preparedness for all NHS Categorised Major Incident Plans-Emergency Preparedness Group in place across the NCA-Gold, Silver and Bronze commands in place and understood by the CO leaders. -Precedent set from other country's responses/ lessons learned - Gold command in
-National instructions changing frequently-Unquantifiable impact on all services-Alignment across localities of EPRR and business continuity plans- National supply chain gap in delivery of timely PPE in adequate quantities-Consistency of communication outside of Gold command- oxygen delivery systems not yet stressed tested to the degree required by a pandemic
3 - Exec Gold COVID 19 Dashboard- Safety and Staff Feedback Surveillance Report- GOLD actions mapped back to national asks- Daily staffing review through the central deployment hub
-Appropriate and timely communication in response to changing situation and national instruction - Continuation of BCP activities and Gold command structures- Source alternative PPE items, risk assess and train staff adequately as part of PPE business continuity planning - development of a comprehensive IPC and staff testing strategies- Process to be e finalised for rapid deployment of staff through silver
13
2/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
8/72

Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 3 of 15
High-level Interim Principal Objective 1. Effective management of major incident and safe provision of critical services for COVID 19 patients through into recovery phase
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services Principal
Risks Like
lihoo
dIm
pact
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1Q
1 20
20/2
1 po
sitio
n
Q2
2020
/21
posit
ion
Q3
2020
/21
posit
ion
Q4
/ Clo
sing
202
0/21
po
sitio
nTa
rget
Ris
k Sc
ore
service not available
place for all people aspects of COVID supported by a Silver People group- local and national modelling on rate of infection and peak- recovery cell established-establishment of medical gases triggers and monitoring
command centres
3/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
9/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 4 of 15
High-level Interim Principal Objective2. Safe provision of critical services for non-COVID-19 patients through into recovery phase of major incident
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services Principal
Risks Like
lihoo
dIm
pact
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1Q
1 20
20/2
1 po
sitio
n
Q2
2020
/21
posi
tion
Q3
2020
/21
posi
tion
Q4
/ Cl
osin
g 2
020/
21
posi
tion
Targ
et R
isk
Scor
e
2.1 IF demand for critical non-COVID 19 services is not met whilst capacity is diverted to COVID response THEN there is increased likelihood of patient safety harm and mortality incidents arising
Chief Delivery Officer
Exec Gold Command
B&RCO12-Public avoiding non-elective access
OCO12 – Service provision and continuity
SCO13 – Capacity to meet non-Covid demand
D&P12 – Increase demand for medical gases 12 – Insufficient support for on call CT rota
4 5 - Established capacity for non-COVID activities on Rochdale, Oldham and Salford sites - Business continuity plans in place reviewed daily-Gold command and silver control in place-Staff briefings and communication- pathways and mutual aid arrangements in place with Independent Sector - Review and implementation of new national clinical criteria for pathway/condition management -Planning taking place daily- all out patients risk stratified
- potential lack of workforce to deliver on COVID and non-COVID activities- Supply chain response not rapid enough to meet demand in critical equipment- as yet unknown and unquantified future health impacts from cessation of core activities- current national mandates to cease core non-COVID activities
4 - Local and GM assurance system for tracking of all new and urgent cancers - Monitoring of live data from Datix (incidents, complaints etc) for trends and analysis
- National supply chain response
- Continuation of BCP activities, including workforce planning- Deliver on national discharge guidance and virtual hospital - Develop Home First Strategy- Re-configure out-patient, cancer and urgent activities to optimise resources and deliver on national priorities-Track national modelling and develop local modelling and recovery plans that deal with backlog and changes in disease prevalence.- develop safety ciren work and mortality indicators acting on findings
1413
4/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
10/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 5 of 15
- development of comprehensive IPC staff testing strategies
High-level Interim Principal Objective3. Safety and well-being of staff
5/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
11/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 6 of 15
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services Principal
Risks Like
lihoo
dIm
pact
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1Q
1 20
20/2
1 po
sitio
n
Q2
2020
/21
posi
tion
Q3
2020
/21
posi
tion
Q4
/ Cl
osin
g 2
020/
21
posi
tion
Targ
et R
isk
Scor
e
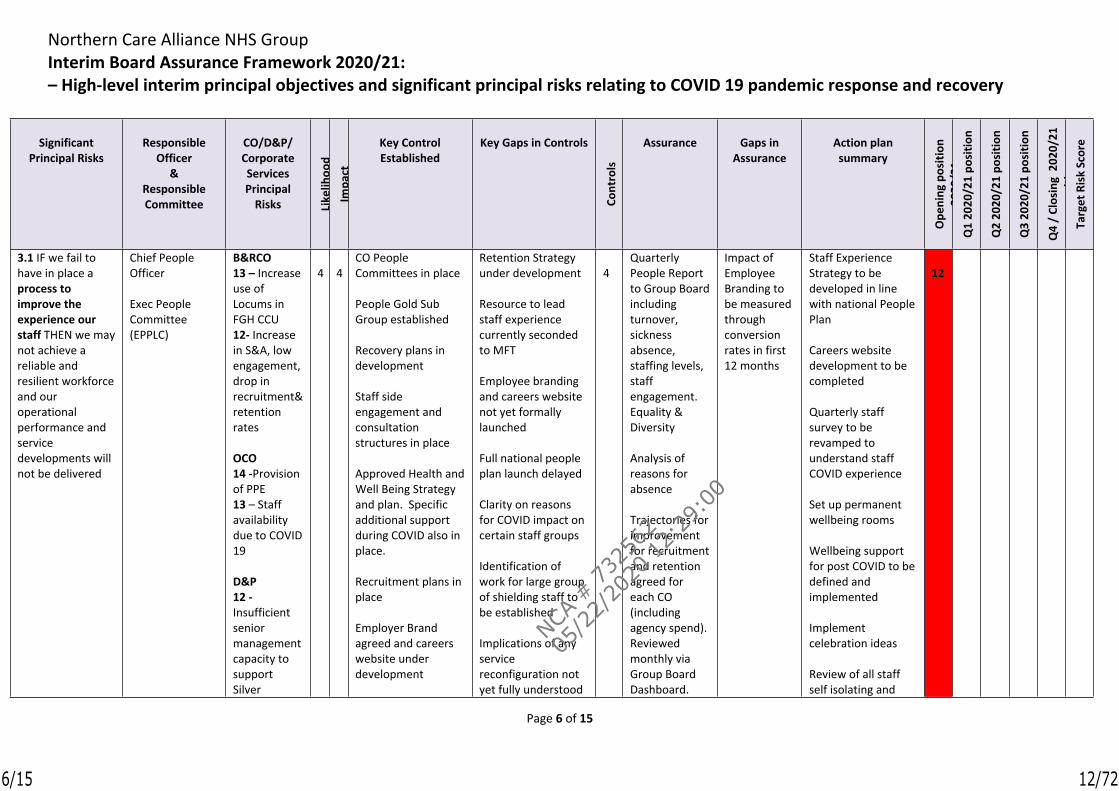
3.1 IF we fail to have in place a process to improve the experience our staff THEN we may not achieve a reliable and resilient workforce and our operational performance and service developments will not be delivered
Chief People Officer
Exec People Committee(EPPLC)
B&RCO13 – Increase use of Locums in FGH CCU12- Increase in S&A, low engagement, drop in recruitment& retention rates
OCO14 -Provision of PPE13 – Staff availability due to COVID 19
D&P12 -Insufficient senior management capacity to support Silver
4 4CO People Committees in place
People Gold Sub Group established
Recovery plans in development
Staff side engagement and consultation structures in place
Approved Health and Well Being Strategy and plan. Specific additional support during COVID also in place.
Recruitment plans in place
Employer Brand agreed and careers website under development
Retention Strategy under development
Resource to lead staff experience currently seconded to MFT
Employee branding and careers website not yet formally launched
Full national people plan launch delayed
Clarity on reasons for COVID impact on certain staff groups
Identification of work for large group of shielding staff to be established
Implications of any service reconfiguration not yet fully understood
4Quarterly People Report to Group Board including turnover, sickness absence, staffing levels, staff engagement. Equality & Diversity
Analysis of reasons for absence
Trajectories for improvement for recruitment and retention agreed for each CO (including agency spend).Reviewed monthly via Group Board Dashboard.
Impact of Employee Branding to be measured through conversion rates in first 12 months
Staff Experience Strategy to be developed in line with national People Plan
Careers website development to be completed
Quarterly staff survey to be revamped to understand staff COVID experience
Set up permanent wellbeing rooms
Wellbeing support for post COVID to be defined and implemented
Implement celebration ideas
Review of all staff self isolating and
12
6/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
12/72
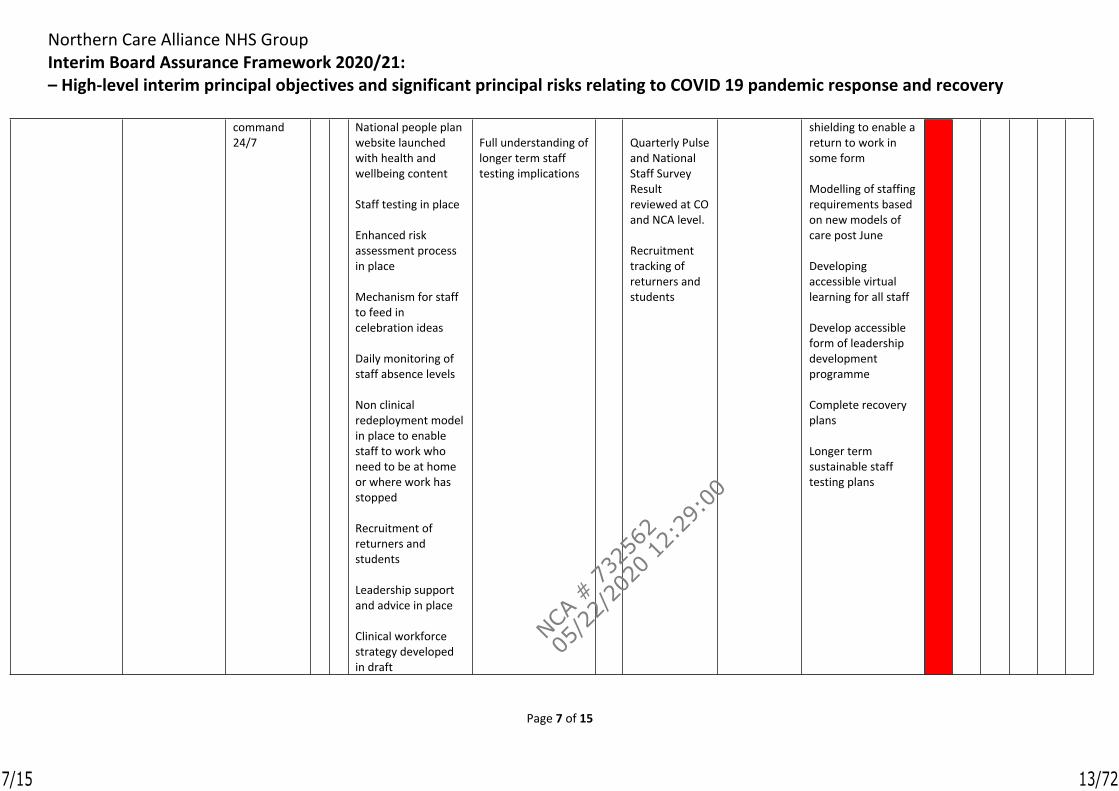
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 7 of 15
command 24/7
National people plan website launched with health and wellbeing content
Staff testing in place
Enhanced risk assessment process in place
Mechanism for staff to feed in celebration ideas
Daily monitoring of staff absence levels
Non clinical redeployment model in place to enable staff to work who need to be at home or where work has stopped
Recruitment of returners and students
Leadership support and advice in place
Clinical workforce strategy developed in draft
Full understanding of longer term staff testing implications
Quarterly Pulse and National Staff Survey Result reviewed at CO and NCA level.
Recruitment tracking of returners and students
shielding to enable a return to work in some form
Modelling of staffing requirements based on new models of care post June
Developing accessible virtual learning for all staff
Develop accessible form of leadership development programme
Complete recovery plans
Longer term sustainable staff testing plans
7/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
13/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 8 of 15
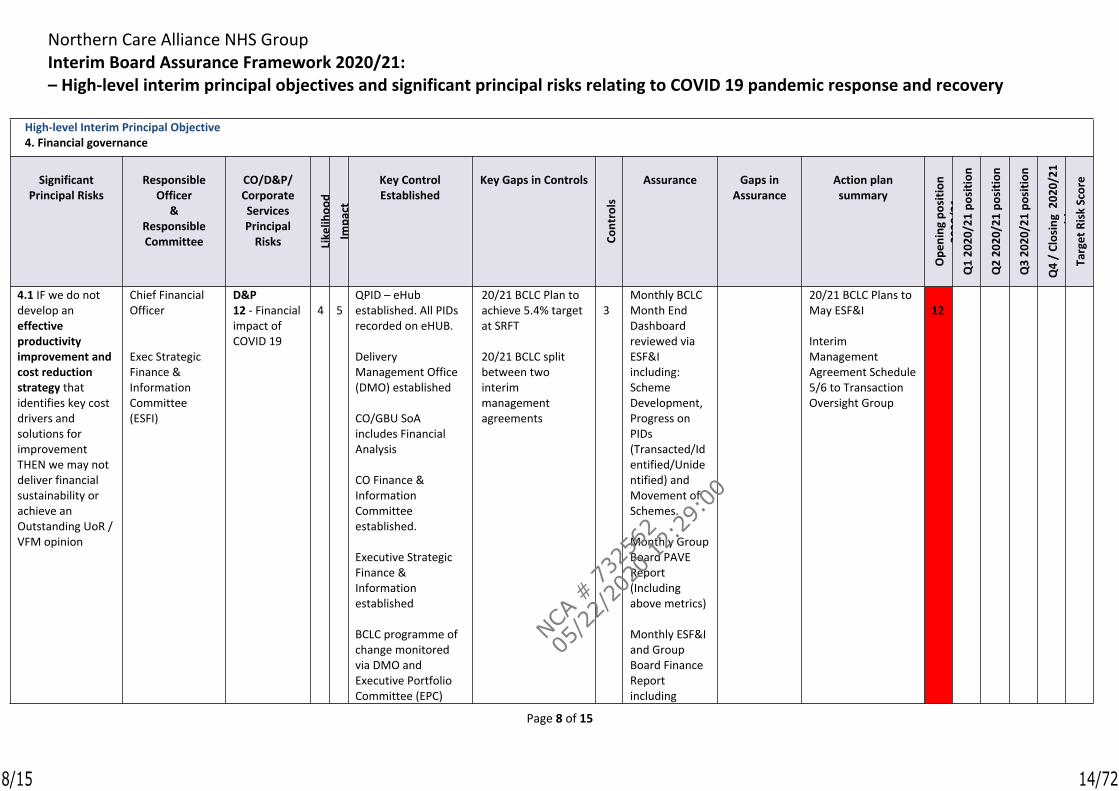
High-level Interim Principal Objective4. Financial governance
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services Principal
Risks Like
lihoo
dIm
pact
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1Q
1 20
20/2
1 po
sitio
n
Q2
2020
/21
posi
tion
Q3
2020
/21
posi
tion
Q4
/ Cl
osin
g 2
020/
21
posi
tion
Targ
et R
isk
Scor
e
4.1 IF we do not develop an effective productivity improvement and cost reduction strategy that identifies key cost drivers and solutions for improvement THEN we may not deliver financial sustainability or achieve an Outstanding UoR / VFM opinion
Chief Financial Officer
Exec Strategic Finance & Information Committee(ESFI)
D&P12 - Financial impact of COVID 19
4 5QPID – eHub established. All PIDs recorded on eHUB.
Delivery Management Office (DMO) established
CO/GBU SoA includes Financial Analysis
CO Finance & Information Committee established.
Executive Strategic Finance & Information established
BCLC programme of change monitored via DMO and Executive Portfolio Committee (EPC)
20/21 BCLC Plan to achieve 5.4% target at SRFT
20/21 BCLC split between two interim management agreements
3Monthly BCLC Month End Dashboard reviewed via ESF&I including: Scheme Development, Progress on PIDs (Transacted/Identified/Unidentified) and Movement of Schemes.
Monthly Group Board PAVE Report (Including above metrics)
Monthly ESF&I and Group Board Finance Report including
20/21 BCLC Plans to May ESF&I
Interim Management Agreement Schedule 5/6 to Transaction Oversight Group
12
8/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
14/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 9 of 15
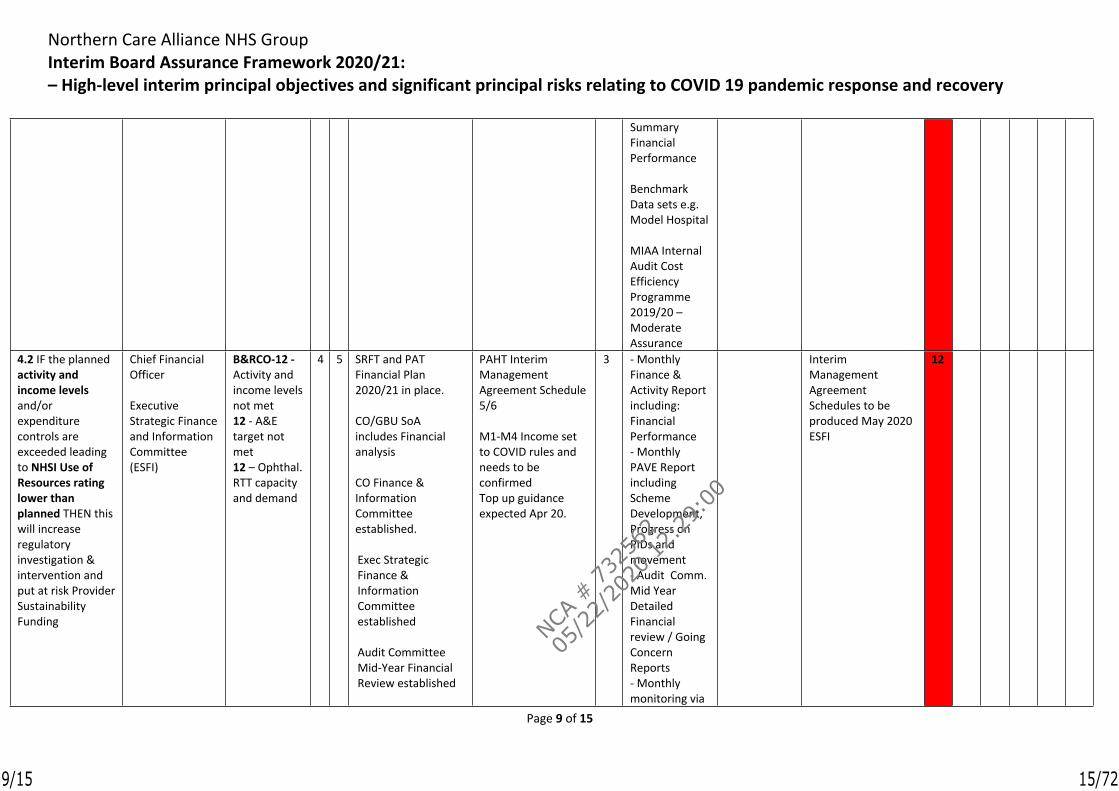
Summary Financial Performance
Benchmark Data sets e.g. Model Hospital
MIAA Internal Audit Cost Efficiency Programme 2019/20 – Moderate Assurance
4.2 IF the planned activity and income levels and/or expenditure controls are exceeded leading to NHSI Use of Resources rating lower than planned THEN this will increase regulatory investigation & intervention and put at risk Provider Sustainability Funding
Chief Financial Officer
Executive Strategic Finance and Information Committee(ESFI)
B&RCO-12 - Activity and income levels not met12 - A&E target not met12 – Ophthal. RTT capacity and demand
4 5 SRFT and PAT Financial Plan 2020/21 in place.
CO/GBU SoA includes Financial analysis
CO Finance & Information Committee established.
Exec Strategic Finance & Information Committee established
Audit Committee Mid-Year Financial Review established
PAHT Interim Management Agreement Schedule 5/6
M1-M4 Income set to COVID rules and needs to be confirmedTop up guidance expected Apr 20.
3 - Monthly Finance & Activity Report including: Financial Performance- Monthly PAVE Report including Scheme Development, Progress on PIDs and movement - Audit Comm. Mid Year Detailed Financial review / Going Concern Reports- Monthly monitoring via
Interim Management Agreement Schedules to be produced May 2020 ESFI
12
9/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
15/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 10 of 15
SRFT/PAHT Drivers of the Deficit Report
NHSI escalation meeting (CFO, CEO & Chair)
10/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
16/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 11 of 15
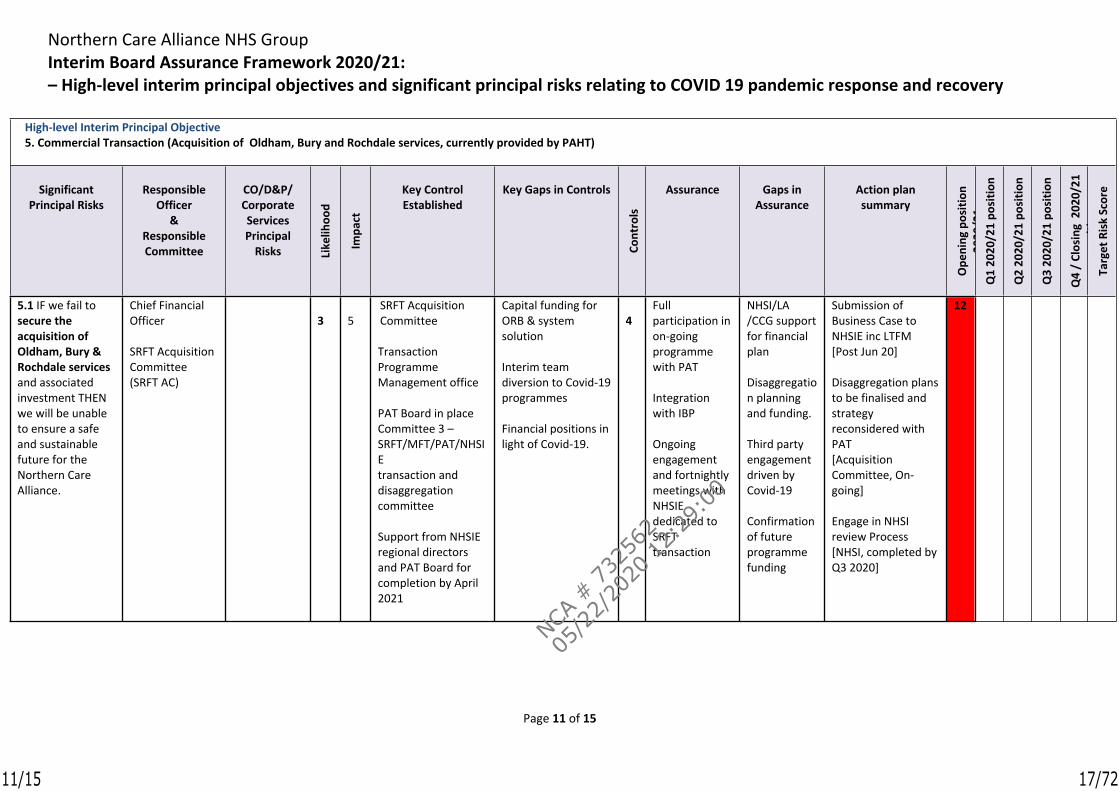
High-level Interim Principal Objective5. Commercial Transaction (Acquisition of Oldham, Bury and Rochdale services, currently provided by PAHT)
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services Principal
Risks Like
lihoo
d
Impa
ct
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1Q
1 20
20/2
1 po
sitio
n
Q2
2020
/21
posi
tion
Q3
2020
/21
posi
tion
Q4
/ Cl
osin
g 2
020/
21
posi
tion
Targ
et R
isk
Scor
e
5.1 IF we fail to secure the acquisition of Oldham, Bury & Rochdale services and associated investment THEN we will be unable to ensure a safe and sustainable future for the Northern Care Alliance.
Chief Financial Officer
SRFT Acquisition Committee(SRFT AC)
3 5SRFT Acquisition Committee
Transaction Programme Management office
PAT Board in place Committee 3 – SRFT/MFT/PAT/NHSIEtransaction and disaggregation committee
Support from NHSIE regional directors and PAT Board for completion by April 2021
Capital funding for ORB & system solution
Interim team diversion to Covid-19 programmes
Financial positions in light of Covid-19.
4Full participation in on-going programme with PAT
Integration with IBP
Ongoing engagement and fortnightly meetings with NHSIE dedicated to SRFT transaction
NHSI/LA /CCG support for financial plan
Disaggregation planning and funding.
Third party engagement driven by Covid-19
Confirmation of future programme funding
Submission of Business Case to NHSIE inc LTFM [Post Jun 20]
Disaggregation plans to be finalised and strategy reconsidered with PAT[Acquisition Committee, On-going]
Engage in NHSI review Process [NHSI, completed by Q3 2020]
12
11/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
17/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 12 of 15
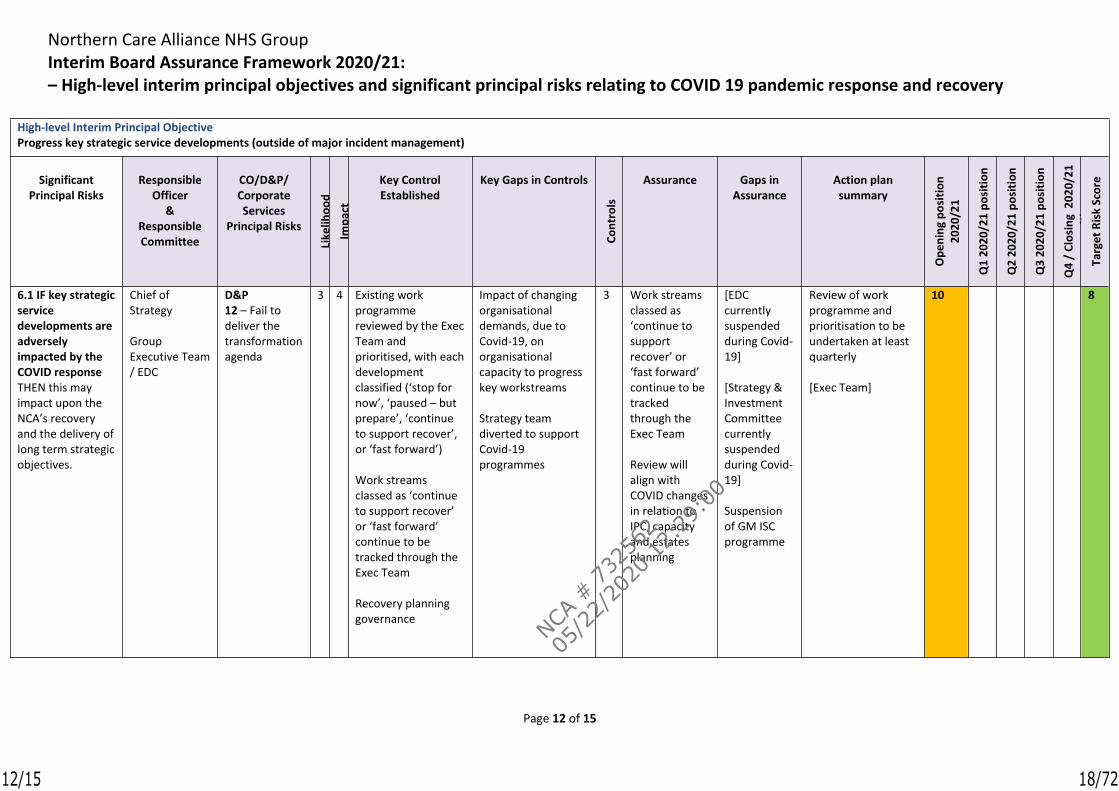
High-level Interim Principal ObjectiveProgress key strategic service developments (outside of major incident management)
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services
Principal Risks
Like
lihoo
dIm
pact
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1
Q1
2020
/21
posi
tion
Q2
2020
/21
posi
tion
Q3
2020
/21
posi
tion
Q4
/ Cl
osin
g 2
020/
21
posi
tion
Targ
et R
isk
Scor
e
6.1 IF key strategic service developments are adversely impacted by the COVID response THEN this may impact upon the NCA’s recovery and the delivery of long term strategic objectives.
Chief of Strategy
Group Executive Team / EDC
D&P12 – Fail to deliver the transformation agenda
3 4 Existing work programme reviewed by the Exec Team and prioritised, with each development classified (‘stop for now’, ‘paused – but prepare’, ‘continue to support recover’, or ‘fast forward’) Work streams classed as ‘continue to support recover’ or ‘fast forward’ continue to be tracked through the Exec Team
Recovery planning governance
Impact of changing organisational demands, due to Covid-19, on organisational capacity to progress key workstreams
Strategy team diverted to support Covid-19 programmes
3 Work streams classed as ‘continue to support recover’ or ‘fast forward’ continue to be tracked through the Exec Team
Review will align with COVID changes in relation to IPC, capacity and estates planning
[EDC currently suspended during Covid-19]
[Strategy & Investment Committee currently suspended during Covid-19]
Suspension of GM ISC programme
Review of work programme and prioritisation to be undertaken at least quarterly
[Exec Team]
10 8
12/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
18/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 13 of 15
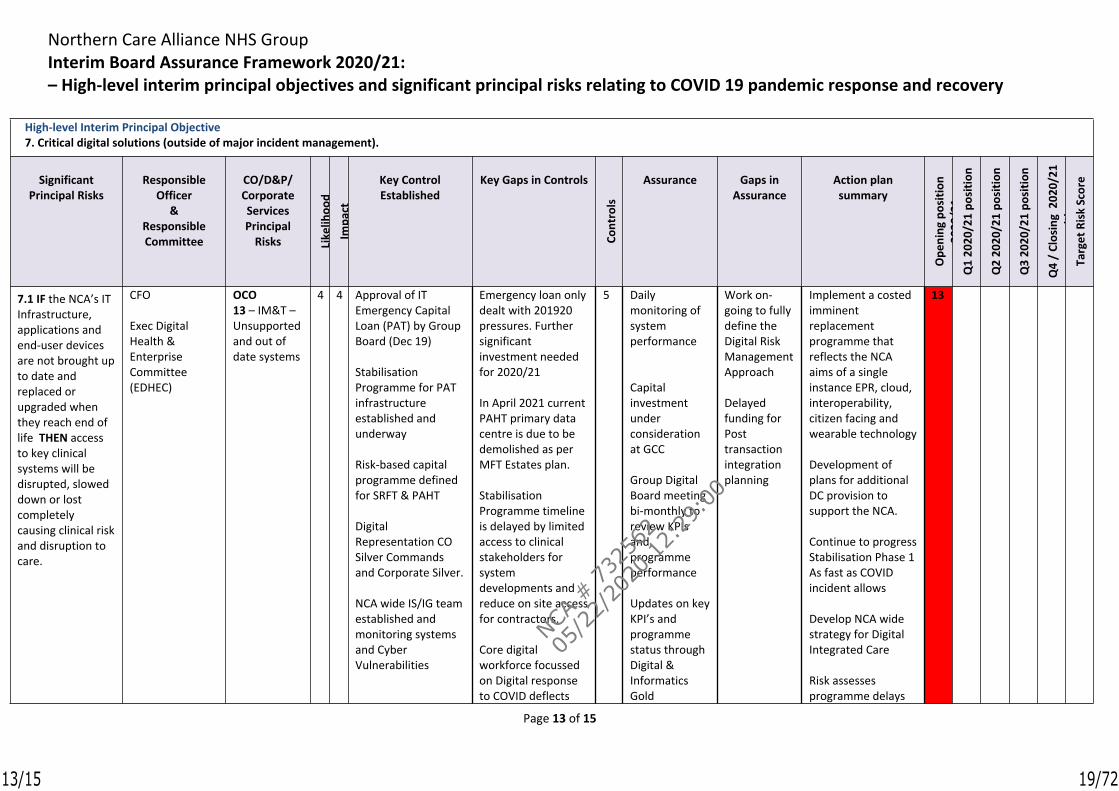
High-level Interim Principal Objective7. Critical digital solutions (outside of major incident management).
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services Principal
Risks Like
lihoo
dIm
pact
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1Q
1 20
20/2
1 po
sitio
n
Q2
2020
/21
posi
tion
Q3
2020
/21
posi
tion
Q4
/ Cl
osin
g 2
020/
21
posi
tion
Targ
et R
isk
Scor
e
7.1 IF the NCA’s IT Infrastructure, applications and end-user devices are not brought up to date and replaced or upgraded when they reach end of life THEN access to key clinical systems will be disrupted, slowed down or lost completely causing clinical risk and disruption to care.
CFO
Exec Digital Health & Enterprise Committee(EDHEC)
OCO13 – IM&T – Unsupported and out of date systems
4 4 Approval of IT Emergency Capital Loan (PAT) by Group Board (Dec 19)
Stabilisation Programme for PAT infrastructure established and underway
Risk-based capital programme defined for SRFT & PAHT
Digital Representation CO Silver Commands and Corporate Silver.
NCA wide IS/IG team established and monitoring systems and Cyber Vulnerabilities
Emergency loan only dealt with 201920 pressures. Further significant investment needed for 2020/21
In April 2021 current PAHT primary data centre is due to be demolished as per MFT Estates plan.
Stabilisation Programme timeline is delayed by limited access to clinical stakeholders for system developments and reduce on site access for contractors.
Core digital workforce focussed on Digital response to COVID deflects
5 Daily monitoring of system performance
Capital investment under consideration at GCC
Group Digital Board meeting bi-monthly to review KPIs and programme performance
Updates on key KPI’s and programme status through Digital & Informatics Gold
Work on-going to fully define the Digital Risk Management Approach
Delayed funding for Post transaction integration planning
Implement a costed imminent replacement programme that reflects the NCA aims of a single instance EPR, cloud, interoperability, citizen facing and wearable technology
Development of plans for additional DC provision to support the NCA.
Continue to progress Stabilisation Phase 1 As fast as COVID incident allows
Develop NCA wide strategy for Digital Integrated Care
Risk assesses programme delays
13
13/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
19/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 14 of 15
High-level Interim Principal Objective7. Critical digital solutions (outside of major incident management).
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services Principal
Risks Like
lihoo
dIm
pact
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1Q
1 20
20/2
1 po
sitio
n
Q2
2020
/21
posi
tion
Q3
2020
/21
posi
tion
Q4
/ Cl
osin
g 2
020/
21
posi
tion
Targ
et R
isk
Scor
e
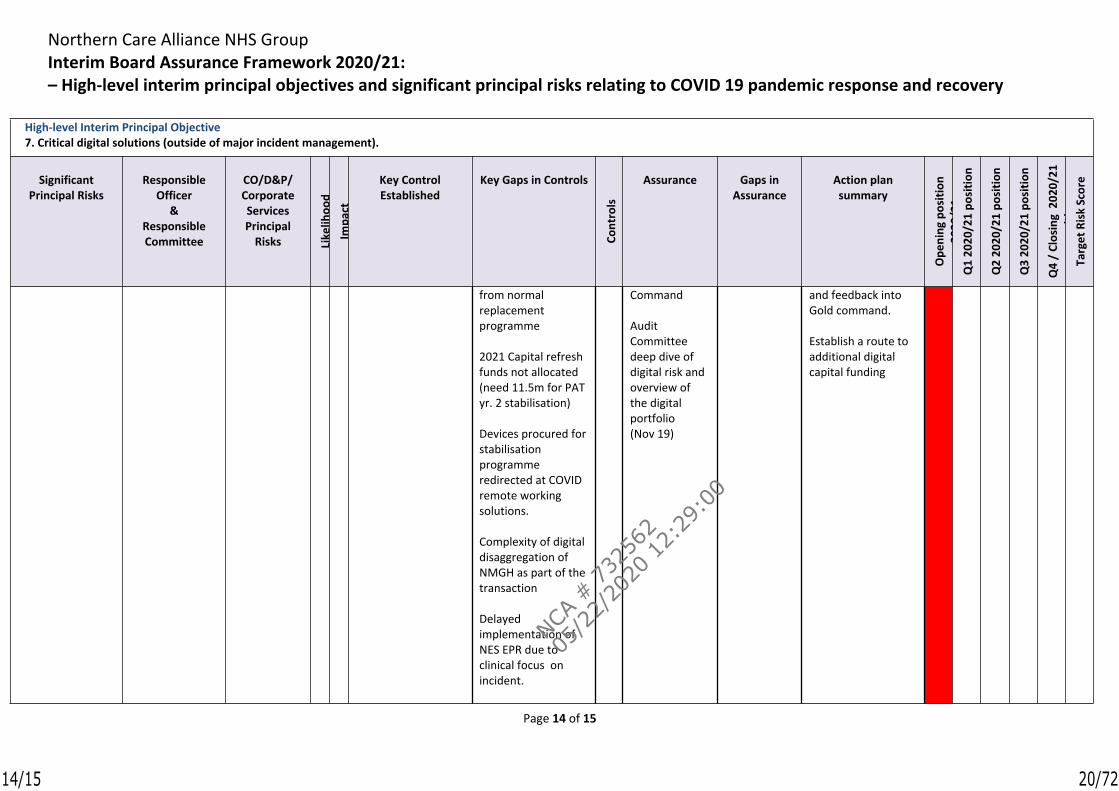
from normal replacement programme
2021 Capital refresh funds not allocated (need 11.5m for PAT yr. 2 stabilisation)
Devices procured for stabilisation programme redirected at COVID remote working solutions.
Complexity of digital disaggregation of NMGH as part of the transaction
Delayed implementation of NES EPR due to clinical focus on incident.
Command
Audit Committee deep dive of digital risk and overview of the digital portfolio (Nov 19)
and feedback into Gold command.
Establish a route to additional digital capital funding
14/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
20/72
Northern Care Alliance NHS GroupInterim Board Assurance Framework 2020/21: – High-level interim principal objectives and significant principal risks relating to COVID 19 pandemic response and recovery
Page 15 of 15
High-level Interim Principal Objective7. Critical digital solutions (outside of major incident management).
Significant Principal Risks
Responsible Officer
& Responsible Committee
CO/D&P/ Corporate Services Principal
Risks Like
lihoo
dIm
pact
Key Control Established
Key Gaps in Controls
Cont
rols
Assurance Gaps in Assurance
Action plan summary
Ope
ning
pos
ition
20
20/2
1Q
1 20
20/2
1 po
sitio
n
Q2
2020
/21
posi
tion
Q3
2020
/21
posi
tion
Q4
/ Cl
osin
g 2
020/
21
posi
tion
Targ
et R
isk
Scor
e
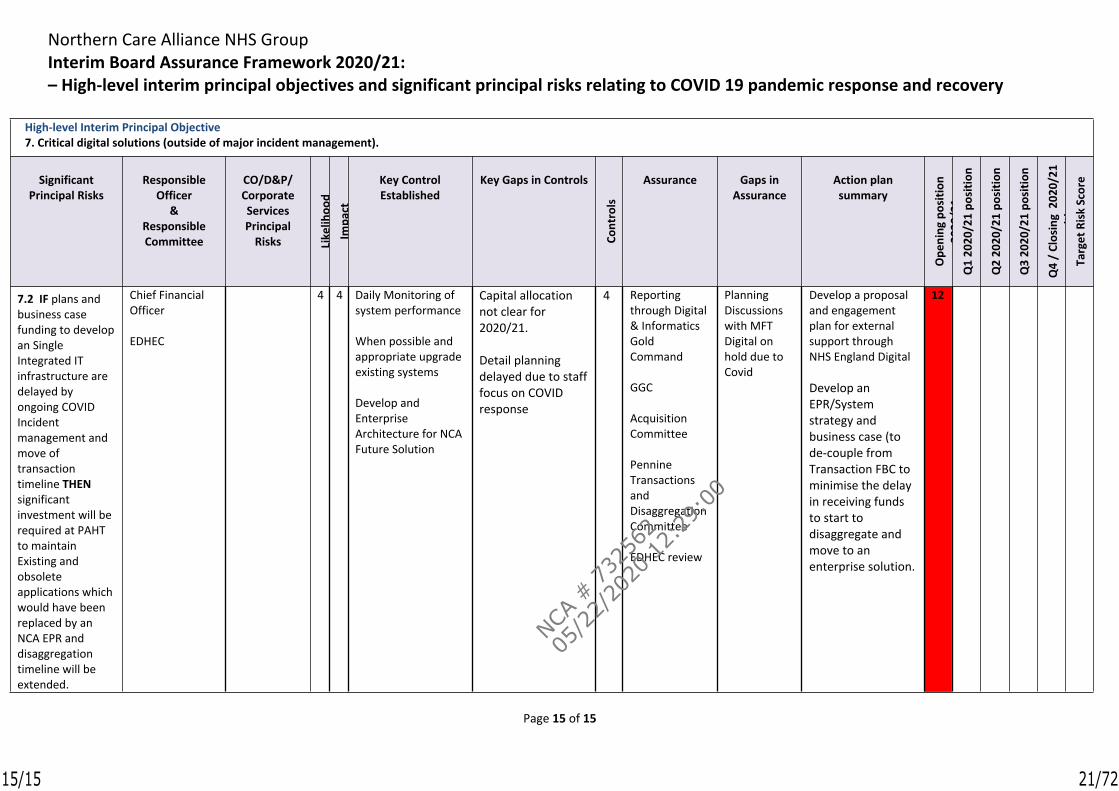
7.2 IF plans and business case funding to develop an Single Integrated IT infrastructure are delayed by ongoing COVID Incident management and move of transaction timeline THEN significant investment will be required at PAHT to maintain Existing and obsolete applications which would have been replaced by an NCA EPR and disaggregation timeline will be extended.
Chief Financial Officer
EDHEC
4 4 Daily Monitoring of system performance
When possible and appropriate upgrade existing systems
Develop and Enterprise Architecture for NCA Future Solution
Capital allocation not clear for 2020/21.
Detail planning delayed due to staff focus on COVID response
4 Reporting through Digital & Informatics Gold Command
GGC
Acquisition Committee
Pennine Transactions and Disaggregation Committee
EDHEC review
Planning Discussions with MFT Digital on hold due to Covid
Develop a proposal and engagement plan for external support through NHS England Digital
Develop an EPR/System strategy and business case (to de-couple from Transaction FBC to minimise the delay in receiving funds to start to disaggregate and move to an enterprise solution.
12
15/15
NCA #
732
562
05/2
2/20
20 12:
29:0
0
21/72
Northern Care Alliance NHS GroupSalford Royal NHS Foundation Trust (SRFT)
Meeting Group Board (Committees in Common)
Author (s)Emma Wright, Director of Information & Business IntelligenceDr Ivan Conyon, Head of Performance & Planning, Jude Adams, Chief Delivery Officer
Presented by Jude Adams, Chief Delivery Officer
Date 26th May 2020
Executive Summary
At the beginning of the new year, there is opportunity to review the scorecard presented to the Group Board. This year is no different however the context of the COVID-19 pandemic does mean that the review and subsequent proposals will be different from previous years as the organisation requires oversight of both the existing pandemic, which is likely to be a feature of how we work for some time, but also the requirement to monitor our reset and recovery.
This paper confirms our guiding principles for our organisational scorecards and also provides a refocus of how leading (signal) and lagging (retrospective) indicators are reviewed in the context of recovery and the absence of formal planning trajectories for a number of areas. The overall format of the scorecard will remain the same and will continue to provide an overview of our statutory obligations as well as our own signal and risk indicators to provide a forward view.
Recommendations The Group Board (Committees in Common) is asked to request that:
the existing Board Scorecard continues to be presented to Board alongside the newly proposed scorecard, for a transition period where amendments and changes can be made during the development process;
that the above arrangement is for an agreed finite period at which point the scorecard will be considered final and will be locked down and production of the previous version ceased; and
opportunity for further review is arranged at the Strategy & Investment Committee meeting scheduled for 23rd July 2020.
Equality Does this paper relate to a matter where equality issues may arise? N
Freedom of Information Request
This document contains some confidential information that would need to be redacted before the document was made available to the public.
Title of Report Group Board Scorecard Review
x
1/3
NCA #
732
562
05/2
2/20
20 12:
29:0
0
22/72
1. Guiding Principles
The following guiding principles will be embedded within our Group Board scorecard:
Alignment with our strategies for recovery, built around core themes as well as other major change programmes and strategies
Inclusive reporting that covers all our services, including community, maternity and social care
Inclusion of metrics particularly pertinent to the current pandemic situation and incident management
Continued focus on leading & balancing indicators rather the just retrospective performance Monitoring against nationally prescribed targets as well as local improvement trajectories Utilisation of SPC or run-charts rather than two data point comparison Triangulation of indicators to give a fuller picture of performance Alignment of risk to domain areas Accompanying commentary to give context including overall NCA performance for shadow
monitoring wherever possible
2. Format of Scorecard
The current format of the CiC Scorecard will continue, providing a retrospective view of key performance indicators alongside a set of balancing measures to enable early sight of changes which may impact on overall performance. The scorecard will continue to provide views of key domain areas however these domain areas will be clearly aligned to our key strategic programmes of change.
3. Proposed Domain Areas
The previous scorecard focused on domain areas that were particularly aligned to key performance indicators. Whilst some of these areas will remain unchanged in terms of focus (e.g. Cancer) other scorecard domains will be refocused to support our key change programmes. For example, our current “Flow” domain will be replaced with a “Home First” focus and our “Planned Care” domain will focus on the planned care recovery workstreams, continuing to monitor our statutory targets, such as Referral to Treatment but also focusing on our levels of activity and utilisation rates.
The core domains areas are proposed as follows:
Recovery – Admitted Planned Care Recovery – Non-Admitted Planned Care Recovery – Unplanned Care Recovery – Diagnostics Home First Infection Control & Prevention (COVID-19) Community & Social Care Patient Experience (including harms) Workforce
4. Next Steps
It is proposed that the existing Board Scorecard will continue to be presented to Board alongside the newly proposed scorecard for a transition period where amendments and changes can be made during the development process. This will be for an agreed finite period at which point the
2/3
NCA #
732
562
05/2
2/20
20 12:
29:0
0
23/72

scorecard will be considered final and will be locked down and production of the previous version ceased. Final sign-off of the 2020/21 scorecard will be through the S&I Committee.
3/3
NCA #
732
562
05/2
2/20
20 12:
29:0
0
24/72
May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr
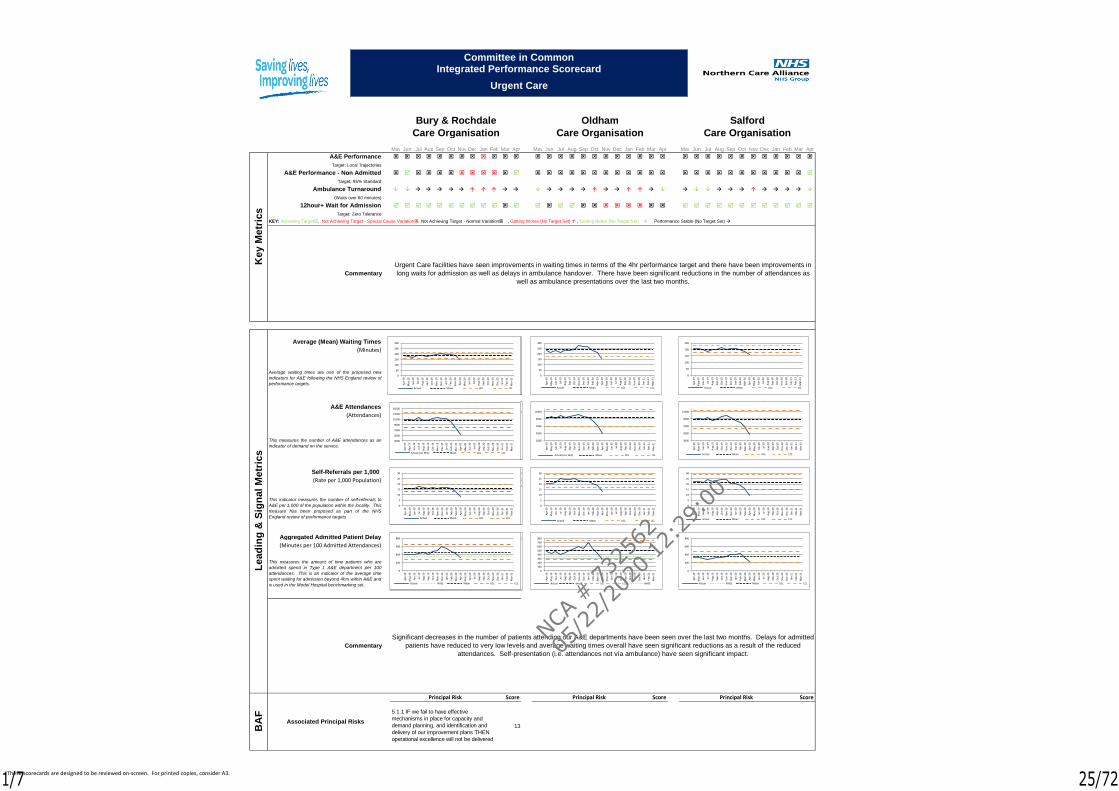
A&E Performance
Target: Local Trajectories
A&E Performance - Non Admitted
Target: 95% Standard
Ambulance Turnaround
(Waits over 60 minutes)
12hour+ Wait for Admission
Target: Zero Tolerance
KEY: Achieving Target, Not Achieving Target - Special Cause Variation, Not Achieving Target - Normal Variation, Getting Worse (No Target Set) , Getting Better (No Target Set), Performance Stable (No Target Set)
Average (Mean) Waiting Times
(Minutes)
A&E Attendances
(Attendances)
Self-Referrals per 1,000
(Rate per 1,000 Population)
Aggregated Admitted Patient Delay
(Minutes per 100 Admitted Attendances)
Score Score Score
13
Principal Risk
BA
F
Associated Principal Risks
Principal Risk Principal Risk
5.1.1 IF we fail to have effective
mechanisms in place for capacity and
demand planning, and identification and
delivery of our improvement plans THEN
operational excellence will not be delivered
Ke
y M
etr
ics
Commentary
Bury & Rochdale
Care Organisation
Urgent Care facilities have seen improvements in waiting times in terms of the 4hr performance target and there have been improvements in
long waits for admission as well as delays in ambulance handover. There have been significant reductions in the number of attendances as
well as ambulance presentations over the last two months.
Le
ad
ing
& S
ign
al
Me
tric
s
Oldham
Care Organisation
Salford
Care Organisation
Commentary
Average waiting times are one of the proposed new
indicators for A&E following the NHS England review of
performance targets.
This measures the number of A&E attendances as an
indicator of demand on the service.
This indicator measures the number of self-referrals to
A&E per 1,000 of the population within the locality. This
measure has been proposed as part of the NHS
England review of performance targets
This measures the amount of time patients who are
admitted spend in Type 1 A&E department per 100
attendances. This is an indicator of the average time
spent waiting for admission beyond 4hrs within A&E and
is used in the Model Hospital benchmarking set.
Significant decreases in the number of patients attending our A&E departments have been seen over the last two months. Delays for admitted
patients have reduced to very low levels and average waiting times overall have seen significant reductions as a result of the reduced
attendances. Self-presentation (i.e. attendances not via ambulance) have seen significant impact.
3000
5000
7000
9000
11000
13000
15000
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual (exc WiC) Mean UCL LCL
7000
9000
11000
Committee in CommonIntegrated Performance Scorecard
Urgent Care
0
5
10
15
20
25
30
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
10
20
30
0
50
100
150
200
250
300
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
200
400
0
200
400
600
800
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual NHSE Mean UCL LCL
500
1000
3000
5000
7000
9000
11000
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual (exc WiC) Mean UCL LCL
0
5
10
15
20
25
30
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
50
100
150
200
250
300
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
100
200
300
400
500
600
700
800
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL NHSE
3000
5000
7000
9000
11000
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
5
10
15
20
25
30
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
50
100
150
200
250
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
200
400
600
800
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual NHSE Mean UCL LCL
These scorecards are designed to be reviewed on-screen. For printed copies, consider A3.1/7
NCA #
732
562
05/2
2/20
20 12:
29:0
0
25/72
May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Mar
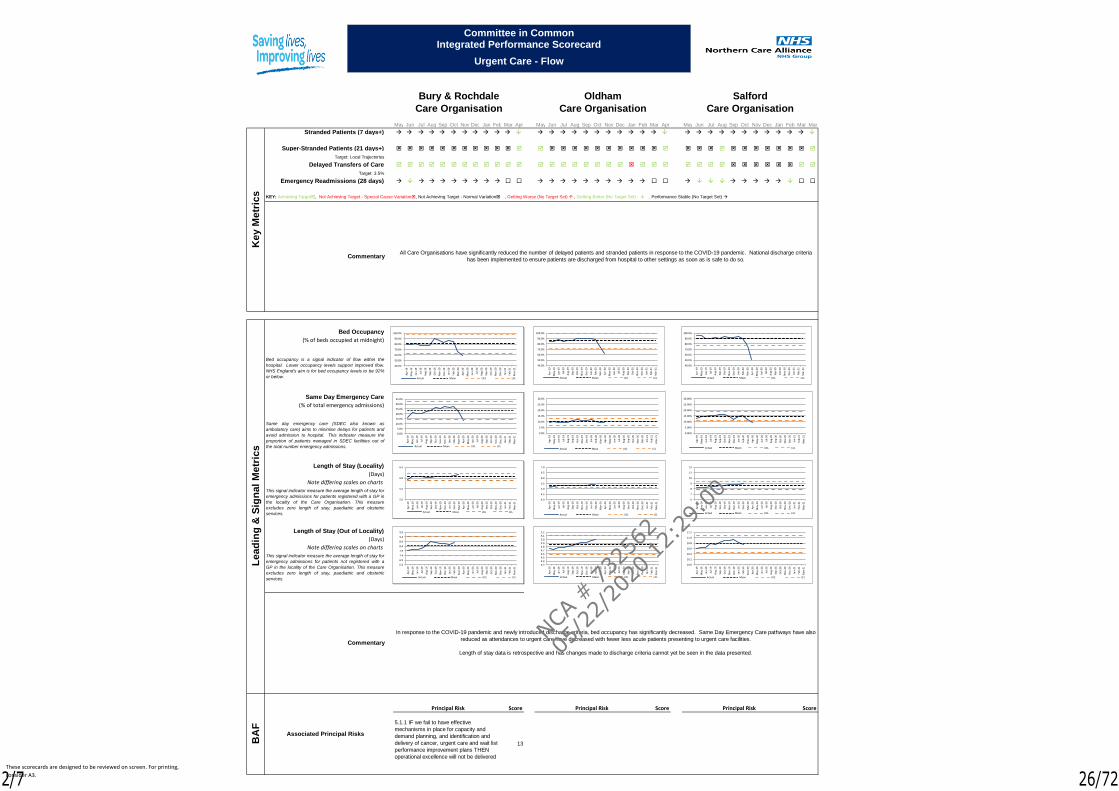
Stranded Patients (7 days+)
Super-Stranded Patients (21 days+)
Target: Local Trajectories
Delayed Transfers of Care
Target: 3.5%
Emergency Readmissions (28 days)
KEY: Achieving Target, Not Achieving Target - Special Cause Variation, Not Achieving Target - Normal Variation, Getting Worse (No Target Set) , Getting Better (No Target Set), Performance Stable (No Target Set)
Bed Occupancy
(% of beds occupied at midnight)
Same Day Emergency Care
(% of total emergency admissions)
Length of Stay (Locality)
(Days)
Note differing scales on charts
Length of Stay (Out of Locality)
(Days)
Note differing scales on charts
Score Score Score
13
Ke
y M
etr
ics
Commentary
Bury & Rochdale
Care Organisation
Le
ad
ing
& S
ign
al
Me
tric
s
Commentary
Bed occupancy is a signal indicator of flow within the
hospital. Lower occupancy levels support improved flow.
NHS England's aim is for bed occupancy levels to be 92%
or below.
Same day emergency care (SDEC also known as
ambulatory care) aims to minimise delays for patients and
avoid admission to hospital. This indicator measure the
proportion of patients managed in SDEC facilities out of
the total number emergency admissions.
This signal indicator measure the average length of stay for
emergency admissions for patients registered with a GP in
the locality of the Care Organisation. This measure
excludes zero length of stay, paediatric and obstetric
services.
This signal indicator measure the average length of stay for
emergency admissions for patients not registered with a
GP in the locality of the Care Organisation. This measure
excludes zero length of stay, paediatric and obstetric
services.
Oldham
Care Organisation
Salford
Care Organisation
All Care Organisations have significantly reduced the number of delayed patients and stranded patients in response to the COVID-19 pandemic. National discharge criteria
has been implemented to ensure patients are discharged from hospital to other settings as soon as is safe to do so.
In response to the COVID-19 pandemic and newly introduced discharge criteria, bed occupancy has significantly decreased. Same Day Emergency Care pathways have also
reduced as attendances to urgent care have decreased with fewer less acute patients presenting to urgent care facilities.
Length of stay data is retrospective and has changes made to discharge criteria cannot yet be seen in the data presented.
Principal Risk
BA
F
Associated Principal Risks
Principal Risk Principal Risk
5.1.1 IF we fail to have effective
mechanisms in place for capacity and
demand planning, and identification and
delivery of cancer, urgent care and wait list
performance improvement plans THEN
operational excellence will not be delivered
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
Committee in CommonIntegrated Performance Scorecard
Urgent Care - Flow
5.0
5.5
6.0
6.5
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
6.4
6.9
7.4
7.9
8.4
8.9
9.4
9.9
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
4.0
4.5
5.0
5.5
6.0
6.5
7.0
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
4.3
4.4
4.5
4.6
4.7
4.8
4.9
5.0
5.1
5.2
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
6
7
8
9
10
11
12
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
10.0
10.2
10.4
10.6
10.8
11.0
11.2
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
These scorecards are designed to be reviewed on screen. For printing,
consider A3.2/7
NCA #
732
562
05/2
2/20
20 12:
29:0
0
26/72
May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr
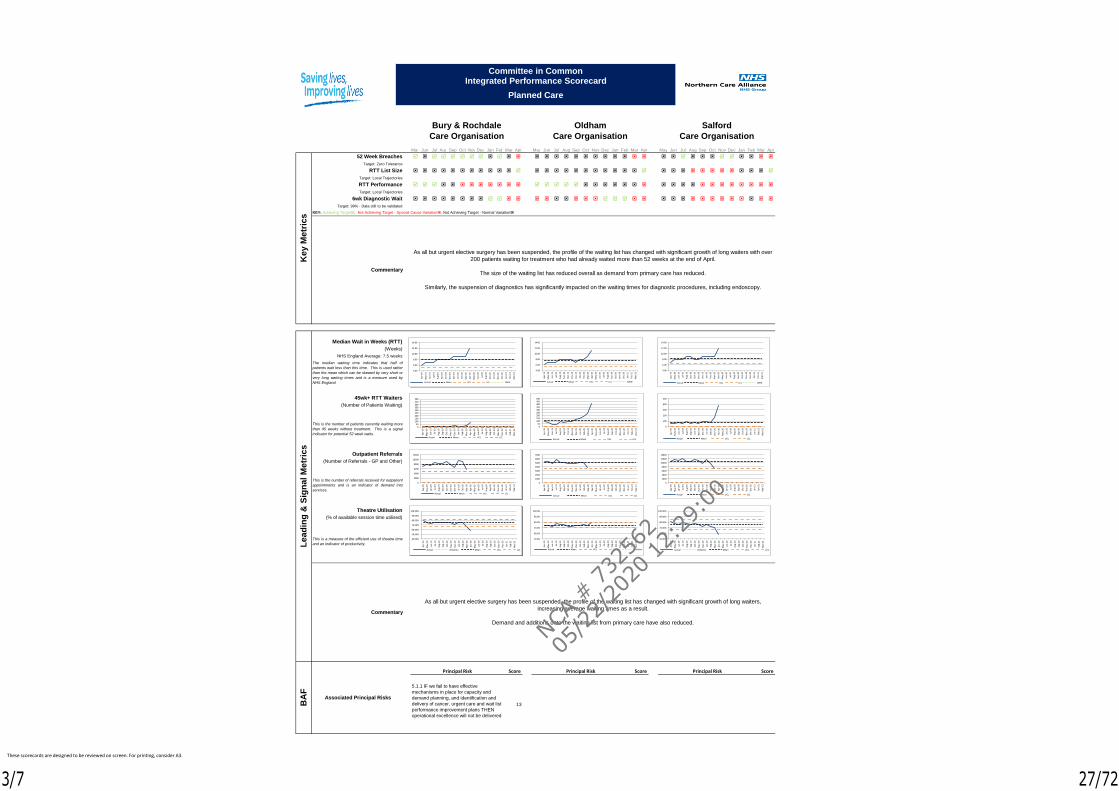
52 Week Breaches
Target: Zero Tolerance
RTT List Size
Target: Local Trajectories
RTT Performance
Target: Local Trajectories
6wk Diagnostic Wait
Target: 99% - Data still to be validated
KEY: Achieving Target, Not Achieving Target - Special Cause Variation, Not Achieving Target - Normal Variation
Median Wait in Weeks (RTT)
(Weeks)
NHS England Average: 7.5 weeks
45wk+ RTT Waiters
(Number of Patients Waiting)
Outpatient Referrals
(Number of Referrals - GP and Other)
Theatre Utilisation
(% of available session time utilised)
Score Score Score
13
Ke
y M
etr
ics
Commentary
Bury & Rochdale
Care Organisation
Oldham
Care Organisation
Salford
Care Organisation
As all but urgent elective surgery has been suspended, the profile of the waiting list has changed with significant growth of long waiters with over
200 patients waiting for treatment who had already waited more than 52 weeks at the end of April.
The size of the waiting list has reduced overall as demand from primary care has reduced.
Similarly, the suspension of diagnostics has significantly impacted on the waiting times for diagnostic procedures, including endoscopy.
Principal Risk
Le
ad
ing
& S
ign
al
Me
tric
sB
AF
Associated Principal Risks
Principal Risk Principal Risk
Commentary
The median waiting time indicates that half of
patients wait less than this time. This is used rather
than the mean which can be skewed by very short or
very long waiting times and is a measure used by
NHS England.
This is the number of patients currently waiting more
than 45 weeks without treatment. This is a signal
indicator for potential 52 week waits.
This is the number of referrals received for outpatient
appointments and is an indicator of demand into
services.
This is a measure of the efficient use of theatre time
and an indicator of productivity.
5.1.1 IF we fail to have effective
mechanisms in place for capacity and
demand planning, and identification and
delivery of cancer, urgent care and wait list
performance improvement plans THEN
operational excellence will not be delivered
As all but urgent elective surgery has been suspended, the profile of the waiting list has changed with significant growth of long waiters,
increasing average waiting times as a result.
Demand and additions onto the waiting list from primary care have also reduced.
050
100150200250300350400450500
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
Committee in CommonIntegrated Performance Scorecard
Planned Care
0
2000
4000
6000
8000
10000
12000
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
4.00
6.00
8.00
10.00
12.00
14.00
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL NHSE
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Ambition Mean UCL LCL
050
100150200250300350400450500
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
1000
2000
3000
4000
5000
6000
7000
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
4.00
6.00
8.00
10.00
12.00
14.00
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL NHSE
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL Ambition
0
100
200
300
400
500
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
2000
4000
6000
8000
10000
12000
14000
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
4.00
6.00
8.00
10.00
12.00
14.00
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL NHSE
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Ambition Mean UCL LCL
These scorecards are designed to be reviewed on screen. For printing, consider A3.
3/7
NCA #
732
562
05/2
2/20
20 12:
29:0
0
27/72
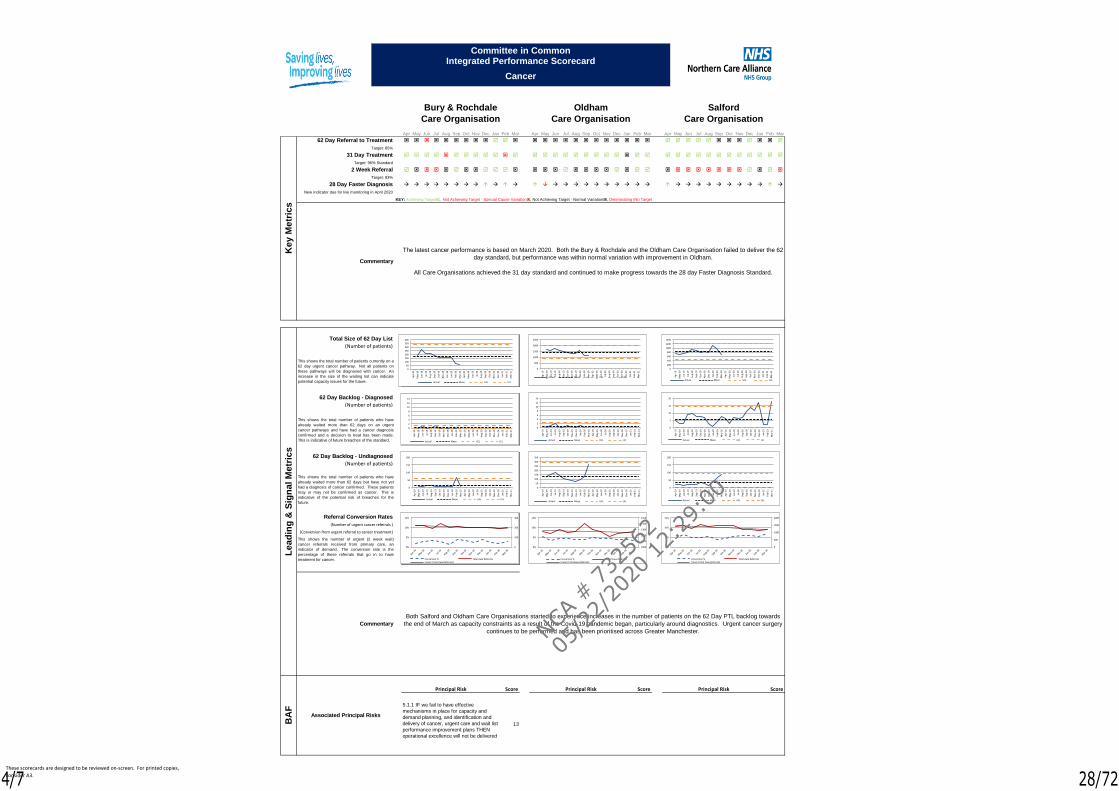
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
62 Day Referral to Treatment
Target: 85%
31 Day Treatment
Target: 96% Standard
2 Week Referral
Target: 93%
28 Day Faster Diagnosis
New indicator due for live monitoring in April 2020
Total Size of 62 Day List
(Number of patients)
62 Day Backlog - Diagnosed
(Number of patients)
62 Day Backlog - Undiagnosed
(Number of patients)
Referral Conversion Rates
(Number of urgent cancer referrals )
(Conversion from urgent referral to cancer treatment)
Score Score Score
13
Le
ad
ing
& S
ign
al
Me
tric
s
Commentary
This shows the total number of patients currently on a
62 day urgent cancer pathway. Not all patients on
these pathways will be diagnosed with cancer. An
increase in the size of the waiting list can indicate
potential capacity issues for the future.
This shows the total number of patients who have
already waited more than 62 days on an urgent
cancer pathways and have had a cancer diagnosis
confirmed and a decision to treat has been made.
This is indicative of future breaches of the standard.
This shows the total number of patients who have
already waited more than 62 days but have not yet
had a diagnosis of cancer confirmed. These patients
may or may not be confirmed as cancer. This is
indicative of the potential risk of breaches for the
future.
This shows the number of urgent (2 week wait)
cancer referrals received from primary care, an
indicator of demand. The conversion rate is the
percentage of these referrals that go in to have
treatment for cancer.
Both Salford and Oldham Care Organisations started to experience increases in the number of patients on the 62 Day PTL backlog towards
the end of March as capacity constraints as a result of the Covid-19 pandemic began, particularly around diagnostics. Urgent cancer surgery
continues to be performed and has been prioritised across Greater Manchester.
Ke
y M
etr
ics
Commentary
Bury & Rochdale
Care Organisation
KEY: Achieving Target, Not Achieving Target - Special Cause Variation, Not Achieving Target - Normal Variation, Deteriorating (No Target), Improving (No Target) , Stable (No Target)
Oldham
Care Organisation
The latest cancer performance is based on March 2020. Both the Bury & Rochdale and the Oldham Care Organisation failed to deliver the 62
day standard, but performance was within normal variation with improvement in Oldham.
All Care Organisations achieved the 31 day standard and continued to make progress towards the 28 day Faster Diagnosis Standard.
Salford
Care Organisation
Principal Risk
BA
F
Associated Principal Risks
Principal Risk Principal Risk
5.1.1 IF we fail to have effective
mechanisms in place for capacity and
demand planning, and identification and
delivery of cancer, urgent care and wait list
performance improvement plans THEN
operational excellence will not be delivered
0
2
4
6
8
10
12
14
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
Committee in CommonIntegrated Performance Scorecard
Cancer
0
50
100
150
200
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
50
100
150
200
250
300
350
400
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
100
200
300
0%
5%
10%
15%
Conversion % Total 2ww ReferralsLinear (Total 2ww Referrals)
0
2
4
6
8
10
12
14
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
50
100
150
200
250
300
350
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
500
1000
1500
2000
2500
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
1000
1100
1200
1300
1400
1500
0%
5%
10%
15%
Conversion % Total 2ww ReferralsLinear (Total 2ww Referrals)
0
5
10
15
20
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
50
100
150
200
Ap
r-1
9
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
200
400
600
800
1000
1200
1400
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
500
1000
1500
2000
0%
5%
10%
15%
Conversion % Total 2ww ReferralsLinear (Total 2ww Referrals)
These scorecards are designed to be reviewed on-screen. For printed copies,
consider A3.4/7
NCA #
732
562
05/2
2/20
20 12:
29:0
0
28/72
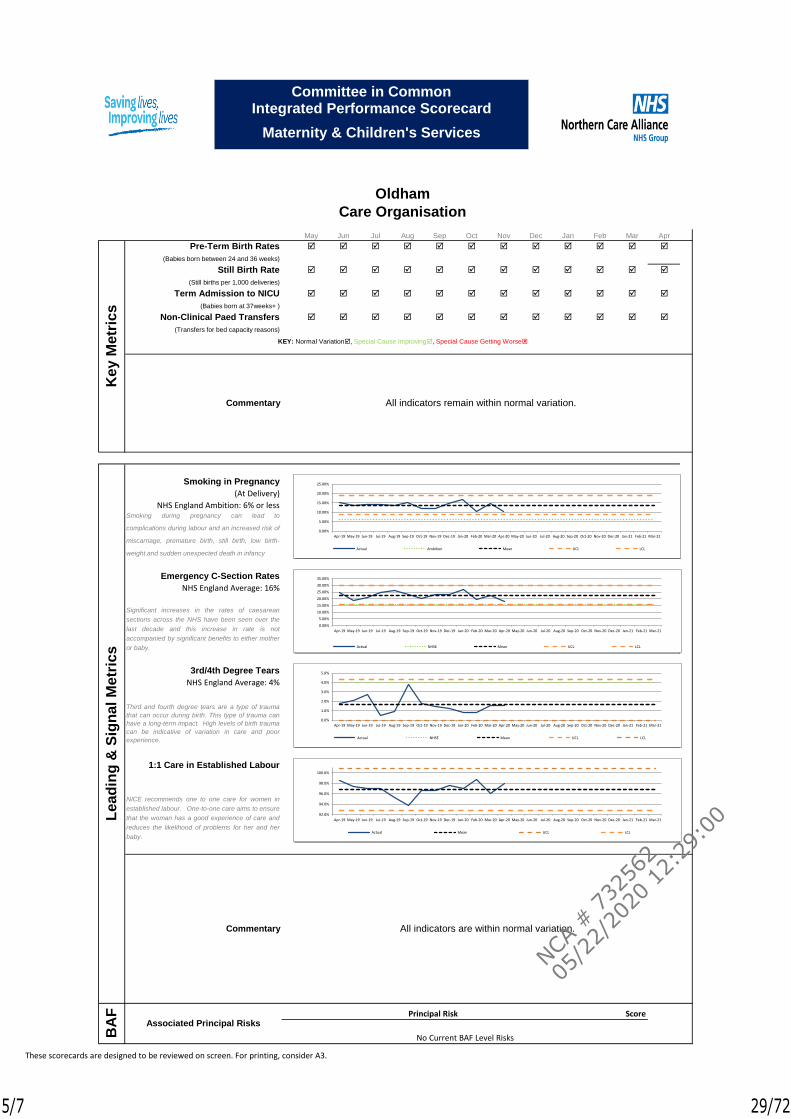
May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr
Pre-Term Birth Rates
(Babies born between 24 and 36 weeks)
Still Birth Rate
(Still births per 1,000 deliveries)
Term Admission to NICU
(Babies born at 37weeks+ )
Non-Clinical Paed Transfers
(Transfers for bed capacity reasons)
Smoking in Pregnancy
(At Delivery)
NHS England Ambition: 6% or less
Emergency C-Section Rates
NHS England Average: 16%
3rd/4th Degree Tears
NHS England Average: 4%
1:1 Care in Established Labour
Score
All indicators remain within normal variation.
Oldham
Care Organisation
BA
F
Associated Principal RisksPrincipal Risk
No Current BAF Level Risks
Lea
din
g &
Sig
na
l M
etr
ics
Ke
y M
etr
ics
Commentary
Commentary All indicators are within normal variation.
KEY: Normal Variation, Special Cause Improving, Special Cause Getting Worse
Smoking during pregnancy can lead to
complications during labour and an increased risk of
miscarriage, premature birth, still birth, low birth-
weight and sudden unexpected death in infancy
Significant increases in the rates of caesarean
sections across the NHS have been seen over the
last decade and this increase in rate is not
accompanied by significant benefits to either mother
or baby.
Third and fourth degree tears are a type of trauma
that can occur during birth. This type of trauma can
have a long-term impact. High levels of birth trauma
can be indicative of variation in care and poor
experience.
NICE recommends one to one care for women in
established labour. One-to-one care aims to ensure
that the woman has a good experience of care and
reduces the likelihood of problems for her and her
baby.
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20 Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
Actual NHSE Mean UCL LCL
Committee in CommonIntegrated Performance Scorecard
Maternity & Children's Services
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20 Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
Actual NHSE Mean UCL LCL
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20 Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
Actual Ambition Mean UCL LCL
92.0%
94.0%
96.0%
98.0%
100.0%
Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20 Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
Actual Mean UCL LCL
These scorecards are designed to be reviewed on screen. For printing, consider A3.
5/7
NCA #
732
562
05/2
2/20
20 12:
29:0
0
29/72
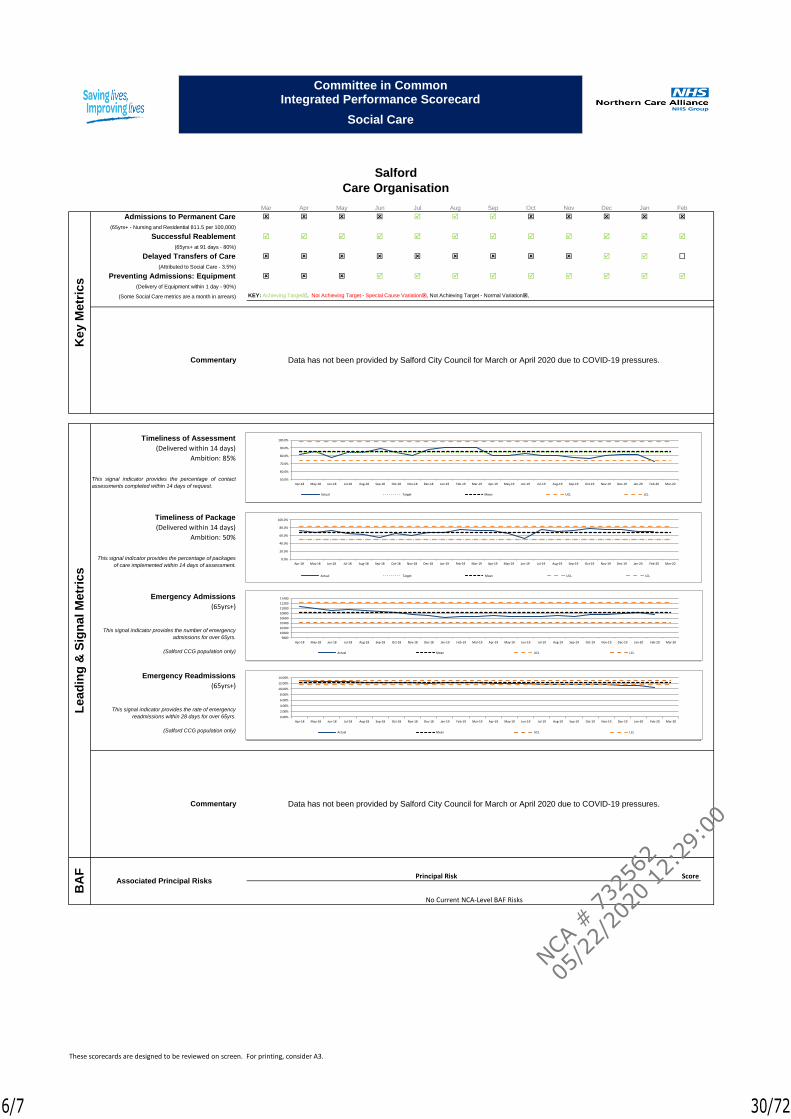
Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb
Admissions to Permanent Care
(65yrs+ - Nursing and Residential 811.5 per 100,000)
Successful Reablement
(65yrs+ at 91 days - 80%)
Delayed Transfers of Care
(Attributed to Social Care - 3.5%)
Preventing Admissions: Equipment
(Delivery of Equipment within 1 day - 90%)
(Some Social Care metrics are a month in arrears) KEY: Achieving Target, Not Achieving Target - Special Cause Variation, Not Achieving Target - Normal Variation,
Timeliness of Assessment
(Delivered within 14 days)
Ambition: 85%
Timeliness of Package
(Delivered within 14 days)
Ambition: 50%
Emergency Admissions
(65yrs+)
Emergency Readmissions
(65yrs+)
Score
Ke
y M
etr
ics
Commentary Data has not been provided by Salford City Council for March or April 2020 due to COVID-19 pressures.
BA
F
Associated Principal Risks
Le
ad
ing
& S
ign
al M
etr
ics
Principal Risk
No Current NCA-Level BAF Risks
Salford
Care Organisation
Commentary Data has not been provided by Salford City Council for March or April 2020 due to COVID-19 pressures.
This signal indicator provides the percentage of contact
assessments completed within 14 days of request.
This signal indicator provides the percentage of packages
of care implemented within 14 days of assessment.
This signal indicator provides the number of emergency
admissions for over 65yrs.
(Salford CCG population only)
This signal indicator provides the rate of emergency
readmissions within 28 days for over 65yrs.
(Salford CCG population only)
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Actual Target Mean UCL LCL
Committee in CommonIntegrated Performance Scorecard
Social Care
9800
10000
10200
10400
10600
10800
11000
11200
11400
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Actual Mean UCL LCL
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Actual Target Mean UCL LCL
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19 Apr-19 May-19 Jun-19 Jul-19 Aug-19 Sep-19 Oct-19 Nov-19 Dec-19 Jan-20 Feb-20 Mar-20
Actual Mean UCL LCL
These scorecards are designed to be reviewed on screen. For printing, consider A3.
6/7
NCA #
732
562
05/2
2/20
20 12:
29:0
0
30/72
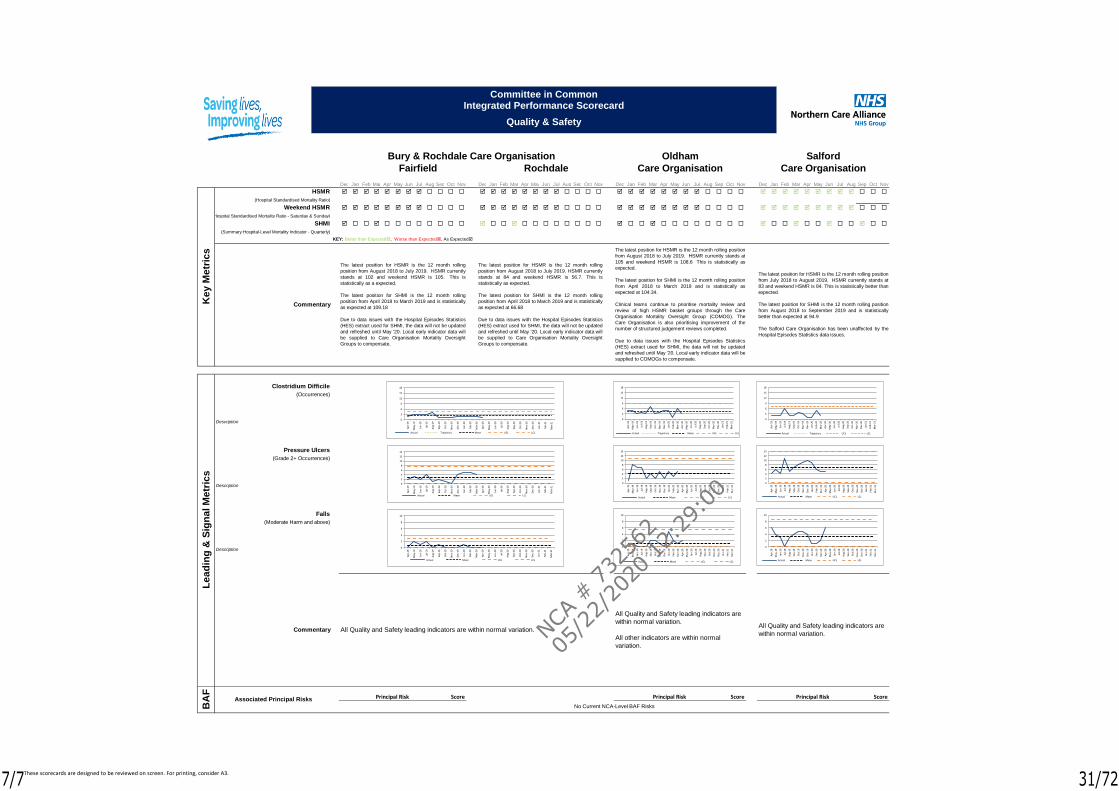
Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov
HSMR
(Hospital Standardised Mortality Ratio)
Weekend HSMR
(Hospital Standardised Mortality Ratio - Saturday & Sunday)
SHMI
(Summary Hospital-Level Mortality Indicator - Quarterly)
KEY: Better than Expected, Worse than Expected, As Expected
Clostridium Difficile
(Occurrences)
Pressure Ulcers
(Grade 2+ Occurrences)
Falls
(Moderate Harm and above)
Score Score Score
Ke
y M
etr
ics
Commentary
The latest position for HSMR is the 12 month rolling
position from August 2018 to July 2019. HSMR currently
stands at 102 and weekend HSMR is 105. This is
statistically as a expected.
The latest position for SHMI is the 12 month rolling
position from April 2018 to March 2019 and is statistically
as expected at 109.18
Due to data issues with the Hospital Episodes Statistics
(HES) extract used for SHMI, the data will not be updated
and refreshed until May '20. Local early indicator data will
be supplied to Care Organisation Mortality Oversight
Groups to compensate.
Bury & Rochdale Care Organisation
Fairfield Rochdale
The latest position for HSMR is the 12 month rolling
position from August 2018 to July 2019. HSMR currently
stands at 84 and weekend HSMR is 56.7. This is
statistically as expected.
The latest position for SHMI is the 12 month rolling
position from April 2018 to March 2019 and is statistically
as expected at 66.68
Due to data issues with the Hospital Episodes Statistics
(HES) extract used for SHMI, the data will not be updated
and refreshed until May '20. Local early indicator data will
be supplied to Care Organisation Mortality Oversight
Groups to compensate.
The latest position for HSMR is the 12 month rolling position
from August 2018 to July 2019. HSMR currently stands at
105 and weekend HSMR is 108.6 This is statistically as
expected.
The latest position for SHMI is the 12 month rolling position
from April 2018 to March 2019 and is statistically as
expected at 104.34.
Clinical teams continue to prioritise mortality review and
review of high HSMR basket groups through the Care
Organisation Mortality Oversight Group (COMOG). The
Care Organisation is also prioritising improvement of the
number of structured judgement reviews completed.
Due to data issues with the Hospital Episodes Statistics
(HES) extract used for SHMI, the data will not be updated
and refreshed until May '20. Local early indicator data will be
supplied to COMOGs to compensate.
The latest position for HSMR is the 12 month rolling position
from July 2018 to August 2019. HSMR currently stands at
83 and weekend HSMR is 84. This is statistically better than
expected.
The latest position for SHMI is the 12 month rolling position
from August 2018 to September 2019 and is statistically
better than expected at 94.9
The Salford Care Organisation has been unaffected by the
Hospital Episodes Statistics data issues.
Oldham
Care Organisation
Salford
Care Organisation
Principal Risk
Le
ad
ing
& S
ign
al M
etr
ics
BA
F
Associated Principal Risks Principal Risk Principal Risk
Commentary
Description
Description
Description
No Current NCA-Level BAF Risks
All Quality and Safety leading indicators are
within normal variation.
All other indicators are within normal
variation.
All Quality and Safety leading indicators are
within normal variation.All Quality and Safety leading indicators are within normal variation.
0
2
4
6
8
10
12
14
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
Committee in CommonIntegrated Performance Scorecard
Quality & Safety
0
2
4
6
8
10
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
3
6
9
12
15
18
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Trajectory Mean UCL LCL
0
2
4
6
8
10
12
14
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
2
4
6
8
10
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
3
6
9
12
15
18
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Trajectory Mean UCL LCL
0
2
4
6
8
10
12
14
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
2
4
6
8
10
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Mean UCL LCL
0
3
6
9
12
15
18
Ap
r-19
May
-19
Jun
-19
Jul-
19
Au
g-1
9
Sep
-19
Oct
-19
No
v-1
9
Dec
-19
Jan
-20
Feb
-20
Mar
-20
Ap
r-20
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
No
v-2
0
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Actual Trajectory UCL LCL
These scorecards are designed to be reviewed on screen. For printing, consider A3.7/7
NCA #
732
562
05/2
2/20
20 12:
29:0
0
31/72
1
Northern Care Alliance NHS GroupSalford Royal NHS Foundation Trust (SRFT)
Meeting Group Board (Committees in Common)
Author Rebecca McCarthy, Deputy Trust SecretaryJane Burns, Group Secretary
Presented by Jane Burns, Group Secretary
Date 26th May 2020
Executive Summary
NHS foundation trusts are required to self-certify whether or not they have complied with the conditions of the NHS provider licence; whether or not they have complied with governance requirements; and that they have the required resources available if providing commissioner requested services.
The following declarations are required:
Condition G6 (3): Providers must certify that they have taken all precautions necessary to comply with the licence, NHS Act and NHS Constitution (Condition G6 (3))
Condition FT4 (8): Providers must certify compliance with required governance arrangements (including Training of Governors)
Condition CoS7 (3): Providers providing commissioner requested services (CRS) must certify that they have a reasonable expectation that required resources will be available to deliver the designated service.
Although there is no submission requirement, provider Boards must confirm that they understand clearly and can confirm compliance with the above conditions. The deadline for Board sign off on self-certifications has not yet been published by NHS Improvement; however approval by the Group Board supports assurances highlighted within the Annual Governance Statement.
NHS Improvement (NHSI) may audit select providers with respect to the self-certification.
This year’s annual self-certification review has been completed to encompass compliance for the Northern Care Alliance NHS Group (NCA) including the statutory body, Salford Royal NHS Foundation Trust (SRFT) during 2019/20.
Annual Plan Objective
N/A
Principal Associated Risks
N/A
Recommendations The Group Board (Committees in Common) is asked to approve this year’s annual self-certifications as described within this paper, subject to review by the Audit Committee on the 19th June 2020.
Title of Report
Annual Self Certifications:− General Condition: G6 Systems for compliance with licence
conditions and related obligations− NHS Foundation Trust Condition FT4: Governance arrangements
including Training of Governors− Foundation Trusts only: Continuity of Services Condition CoS7:
Availability of Resources
1/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
32/72

2
Equality Does this paper relate to a matter where equality issues may arise? NIf so, has due regard been given to equality analysis of any adverse impactsThis document does not contain confidential information and can be made available to the public.
This document contains some confidential information that would need to be redacted before the document was made available to the public.
Freedom of Information
Please ‘cross’ one of the boxes
This document is entirely confidential, as the redaction of confidential information would render the document meaningless.
X
2/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
33/72

3
1. General Condition G6
1.1 General Condition 6 within the Licence requires providers to have in place effective systems and processes to ensure compliance with licence conditions and related obligations.
1.2 A management review has been undertaken confirming compliance with General Condition 6 of the NHS Provider Licence (Appendix 1). This supports the review that has also taken place of all Licence Conditions (Appendix 2).
1.3 SRFT are required to publish a G6 & CoS7 self-certification within a month following Board sign off (Appendix 3)
2. Condition FT4 including Training for Governors
2.1 Condition FT4 within the Licence sets out provisions relating to principles, systems and standards of good corporate governance. The Corporate Governance Statement includes the provisions set out in Condition FT4. A description of the principal risks to compliance with Condition FT4, and actions identified to mitigate those risks, are included within the SRFT Annual Governance Statement (which forms part of the Annual Report to be submitted on 25th June 2020).
2.2 A management review of the Corporate Governance Statement and Training of Governors has been undertaken. Please see attached Appendix 4 and 5 respectively.
3. Foundation Trusts only: Condition CoS7
3.1 Foundation Trust providers, providing commissioner requested services (CRS), must certify that they have a reasonable expectation that required resources will be available to continue to provide those services.
3.2 A management review of the availability of resources has been undertaken (Appendix 6).
3/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
34/72
Appendix 1: General Condition 6 - Management Review
4
General Condition 6 Current Arrangements/EvidenceThe Licensee shall take all reasonable precautions against the risk of failure to comply with:(a) the Conditions of this Licence,(b) any requirements imposed on it under the NHS Acts, and(c) the requirement to have regard to the NHS Constitution in providing health care services for the purposes of the NHS.
Comprehensive business planning process in place, adapted in line with Covid-19 national planning requirements.
The draft SRFT Financial Plan 2020/21, reviewed at Group Board in February/March 2020 and submitted to NHSI at the beginning of April 2020, outlines the key points of the new financial arrangements for the period between 1 April and 31 July, along with information about the draft annual plan that was submitted to NHSI on 5th March 2020.
The Group Board has established and operates an oversight framework for each of its Care Organisations, called the Group Single Oversight Framework (Group SOF). The Group SOF provides assurance on delivery of the Care Organisation Annual Plan objectives and supports quality and performance improvement. The themes of the Group SOF reflect those of the NHS Single Oversight Framework (which bases its oversight on the NHS provider licence): Quality of Care Finance and Use of Resources Operational performance Strategic Change Leadership and Improvement Capability (Well Led) Approved Group Governance Framework Manual - Sets out the control framework within which the Group’s and Care Organisations objectives are delivered. The Manual complements the Trust’s Constitution and Licence and takes full account of the NHS Foundation Trust Code of Governance. The Manual highlights processes and systems in place to oversee constitutional, regulatory and legal compliance. The Manual incorporates Reservation of Powers and Delegation of Powers, Detailed Scheme of Delegation and Standing Financial Instructions. Group Governance Framework Manual is refreshed regularly and ratified/approved by Audit Committee and the Group Board. It was last approved at the Group Board meeting on 30 September 2019 and is valid until 30 April 2021.
COVID-19 Update: During the on-going COVID-19 situation, temporary emergency modifications to the financial governance arrangements in the GGFM have been developed and approved via Gold Command and reviewed via Audit Committee in April 2020.
In March 2018, the Group Board approved an NCA Risk Management Strategy. The NCA Risk Management Strategy provides a framework for managing risks across the Group and Care Organisations, which is consistent with best practice and Department of Health guidance. The Strategy provides a clear, systematic approach to the management of risks to ensure that risk assessment is an integral part of clinical, managerial and financial processes across the organisation for the benefit of patients, staff, visitors and other stakeholders.
There is a Risk Assessment and Risk Register Policy in place describing how staff will fulfil their role in risk assessment and the production of risk registers and interaction required between directorates, divisions and the Care Organisation committees. All risks regardless of their nature or origin are managed via this process.
4/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
35/72
Appendix 1: General Condition 6 - Management Review
5
General Condition 6 Current Arrangements/Evidence
SRFT is registered with the Care Quality Commission and systems exist to ensure compliance with the registration requirements, detailed in the respective Annual Governance Statements. SRFT: CQC Inspection – ‘Outstanding’ August 2018.
2019/20 Corporate Governance Statements – Reviewed by Group Board (May 2020) and Audit Committee (June 2020). Recommendation: No material risks identified.
NHS Foundation Trust – Code of Governance Annual Review 2019/20. Although the Code is relevant to NHS Foundation Trusts, the review undertaken in March 2020 encompassed compliance for the Northern Care Alliance NHS Group (NCA). Review of compliance with each provision undertaken by the Group Board in March 2020. The SRFT Annual Report 2019/20 will confirm compliance with the provisions of the Code and an explanation of why the Trust has departed from B.1.2 and B.6.2.
Audit Committee considered and approved the NCA Internal Audit Plan for 2019/20 (April 19). The Internal Audit Plan was risk based, with an on-going programme of internal audits in finance, operations and governance. During the course of the year, Audit Committee monitored progress against the Internal Audit Plans and reviewed the work and findings of the Internal Auditor. The NCA Internal Audit Assurance Framework Review 2019/20 confirmed that ‘the organisation’s Assurance Framework is structured to meet the NHS requirements, is visibly used by the Board and clearly reflects the risks discussed by the Board.’
Audit Committee reviewed the work and findings of the External Auditor during 2019/20, including valuable insight and benchmarking information.
SRFT Annual Report and Annual Accounts 2019/20 – Prepared in accordance with NHS Foundation Trust Annual Reporting Manual for NHS Foundation Trusts.
Submission of compliance reports to NHS Improvement as required.
SRFT: Review of all Licence conditions including General, Pricing, Choice and Competition, Integrated Care, Continuity of Service and NHS Foundation Trust Conditions (Appendix 2).
Without prejudice to the generality of paragraph 1, the steps that the Licensee must take pursuant to that paragraph shall include:(a) the establishment and implementation of processes and systems to identify risks and guard against their
The NCA’s Group Assurance Framework, is based on six key elements: Clearly defined principal objectives agreed with stakeholders together with clear lines of responsibility and
accountability; Clearly defined principal risks to the achievement of these objectives together with assessment of their potential
impact and likelihood;
5/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
36/72
Appendix 1: General Condition 6 - Management Review
6
General Condition 6 Current Arrangements/Evidenceoccurrence; and(b) regular review of whether those processes and systems have been implemented and of their effectiveness.
Key controls by which these risks can be managed, this includes involvement of stakeholders in agreeing controls where risks impact on them;
Management and independent assurances that risks are being managed effectively; Board level reports identifying that risks are being reasonably managed and objectives being met together with
gaps in assurances and gaps in risk control; Board level action plans which ensure the delivery of objectives, control of risk and improvements in assurances.
The workplan of committees within the NCA’s Assurance Framework is linked so that the Group Board is assured that there is an aligned independent and executive focus on strategic risk and assurance. Routine referral of issues exists between committees ensuring a respective understanding of risk and assurance concerns.
The Group Board oversees the management of all major risks, which are actively addressed by the Group Executive Risk and Assurance Committee. The NCA Corporate Risk Register is integrated with the Board Assurance Framework thereby ensuring that risks are not only managed and communicated efficiently, but that the management of them is embedded in the NCA’s practice. The NCA Board Assurance Framework/Corporate Risk Register is reviewed on a quarterly basis, alongside the Care Organisation Board Assurance Framework/Corporate Risk Registers. Key controls and assurances, and any identified gaps are continually reviewed and action plans developed and progressed accordingly. All significant risks are detailed within the monthly Group Performance Dashboard presented to the Group Board by the Chief Executive Officer.
Audit Committee reviews the Board Assurance Framework/Corporate Risk Register and commissions additional reviews where appropriate in order to provide necessary assurance to the Group Board.
In the latter part of 2018/19, the NCA completed a Self-Assessment against the Well-Led Framework for Governance. Mersey Internal Audit (MIAA) conducted an independent review of the self-assessment, considering comprehensiveness and sources of evidence, in order to provide further assurance with respect to compliance with the Key Lines of Enquiry (KLOEs). The outcome of the independent review, in summary, concluded that the position statements were comprehensive and presented a compelling and positive picture of the NCA. It added that the thoroughness and quality of the self-assessment placed the NCA in a strong and informed position in terms of selecting an external review approach that adds most value (if and when appropriate). The Self-Assessment against the Well-Led Framework for Governance was updated in the final part of 2019/20 to reflect up-to-date practice in SRFT/PAHT.
Annual Governance Statements – To be reviewed by Audit Committee, April 2020 confirming “The Board had extensive and effective governance assurance systems in operation enabling the identification and control of risks reported through the Board Assurance Framework and Corporate Risk Register. Internal and external reviews, audits and inspections had provided sufficient evidence to state that no significant internal control issues have been identified during 2019/20, and that these control systems are fit for purpose.”
6/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
37/72
Appendix 1: General Condition 6 - Management Review
7
General Condition 6 Current Arrangements/Evidence
The SRFT financial plan is approved by the Group Board. It is subsequently submitted to NHS Improvement. The plan, including forward projections, is monitored on a monthly basis by the Care Organisation Finance Governance Committees. The Care Organisations provide a monthly Statement of Assurance to the GRAC which confirms the sufficiency of plans for the effective use of resources. Key performance indicators and financial sustainability metrics are also reviewed monthly by the Group CiC.
A process of self-assessment of CQC Fundamental Standards of Quality and Safety (previously Essential Standards) is in place and undertaken annually by each service. NCA: An internal CQC mock assessment programme is in operation whereby unannounced visits take place across each of the departments that do not take part in the NAAS/CAAS process. Assurance is provided by Audit Committee, which monitors the outcome of the mock assessment programme in-year and commissions specific reviews by the Trust’s internal auditors. (Quality Surveillance Programme in development for Covid-19)
Group Audit Committee review of:− Register of Interests for Senior Staff and Gifts and Hospitality Registers to ensure compliance with the Trust’s
Standards of Business (Annual)− The arrangements by which staff can raise issues in confidence about possible improprieties in matters of
financial reporting and control, clinical quality, patient safety or other matters to ensure arrangements are in place for the proportionate and independent investigation of such matters and appropriate follow-up action (Annual)
− Group Governance Framework Manual (Annual)− Counter Fraud Plans and Reports− Internal Audit Annual Programme, progress reports and audit outcomes − Clinical Audit Annual Programme and Developments − All risk and control related disclosure statements in particular the Annual Governance Statement, Corporate
Governance Statement, together with the accompanying Head of Internal Audit statement and External Audit Opinion.
On 30 January 2020, the Director-General of WHO declared the 2019-nCoV outbreak a public health emergency of international concern under the International Health Regulations (IHR) (2005). As the NCA is a designated Category 1 responder, under the Civil Contingences Act 2004, it has a well-established Emergency Preparedness Resilience & Response Unit (EPRRU). A clear Command and Control Structure consisting of one Gold Command Team was established, supported by specialist sub groups and Care Organisation Silver Command Teams. Gold Command and GRAC have established a purposeful risk management interaction, including effective system for the escalation of risk, to ensure the continued effectiveness of the NCA’s system of internal control for the duration of the major incident.
7/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
38/72
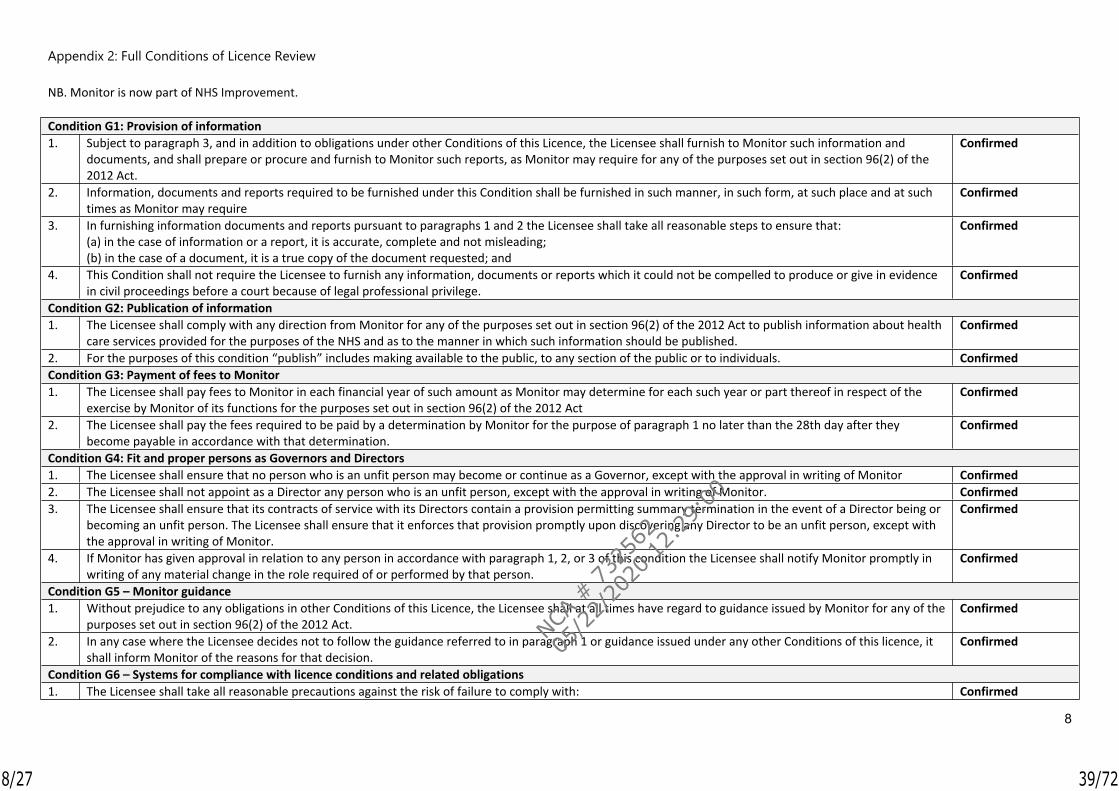
Appendix 2: Full Conditions of Licence Review
8
NB. Monitor is now part of NHS Improvement.
Condition G1: Provision of information1. Subject to paragraph 3, and in addition to obligations under other Conditions of this Licence, the Licensee shall furnish to Monitor such information and
documents, and shall prepare or procure and furnish to Monitor such reports, as Monitor may require for any of the purposes set out in section 96(2) of the 2012 Act.
Confirmed
2. Information, documents and reports required to be furnished under this Condition shall be furnished in such manner, in such form, at such place and at such times as Monitor may require
Confirmed
3. In furnishing information documents and reports pursuant to paragraphs 1 and 2 the Licensee shall take all reasonable steps to ensure that:(a) in the case of information or a report, it is accurate, complete and not misleading; (b) in the case of a document, it is a true copy of the document requested; and
Confirmed
4. This Condition shall not require the Licensee to furnish any information, documents or reports which it could not be compelled to produce or give in evidence in civil proceedings before a court because of legal professional privilege.
Confirmed
Condition G2: Publication of information1. The Licensee shall comply with any direction from Monitor for any of the purposes set out in section 96(2) of the 2012 Act to publish information about health
care services provided for the purposes of the NHS and as to the manner in which such information should be published.Confirmed
2. For the purposes of this condition “publish” includes making available to the public, to any section of the public or to individuals. ConfirmedCondition G3: Payment of fees to Monitor1. The Licensee shall pay fees to Monitor in each financial year of such amount as Monitor may determine for each such year or part thereof in respect of the
exercise by Monitor of its functions for the purposes set out in section 96(2) of the 2012 ActConfirmed
2. The Licensee shall pay the fees required to be paid by a determination by Monitor for the purpose of paragraph 1 no later than the 28th day after they become payable in accordance with that determination.
Confirmed
Condition G4: Fit and proper persons as Governors and Directors 1. The Licensee shall ensure that no person who is an unfit person may become or continue as a Governor, except with the approval in writing of Monitor Confirmed2. The Licensee shall not appoint as a Director any person who is an unfit person, except with the approval in writing of Monitor. Confirmed3. The Licensee shall ensure that its contracts of service with its Directors contain a provision permitting summary termination in the event of a Director being or
becoming an unfit person. The Licensee shall ensure that it enforces that provision promptly upon discovering any Director to be an unfit person, except with the approval in writing of Monitor.
Confirmed
4. If Monitor has given approval in relation to any person in accordance with paragraph 1, 2, or 3 of this condition the Licensee shall notify Monitor promptly in writing of any material change in the role required of or performed by that person.
Confirmed
Condition G5 – Monitor guidance1. Without prejudice to any obligations in other Conditions of this Licence, the Licensee shall at all times have regard to guidance issued by Monitor for any of the
purposes set out in section 96(2) of the 2012 Act.Confirmed
2. In any case where the Licensee decides not to follow the guidance referred to in paragraph 1 or guidance issued under any other Conditions of this licence, it shall inform Monitor of the reasons for that decision.
Confirmed
Condition G6 – Systems for compliance with licence conditions and related obligations1. The Licensee shall take all reasonable precautions against the risk of failure to comply with: Confirmed
8/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
39/72

Appendix 2: Full Conditions of Licence Review
9
(a) the Conditions of this Licence,(b) any requirements imposed on it under the NHS Acts, and(c) the requirement to have regard to the NHS Constitution in providing health care services for the purposes of the NHS.
2. Without prejudice to the generality of paragraph 1, the steps that the Licensee must take pursuant to that paragraph shall include:(a) the establishment and implementation of processes and systems to identify risks and guard against their occurrence; and(b) regular review of whether those processes and systems have been implemented and of their effectiveness.
Confirmed
3. Not later than two months from the end of each Financial Year, the Licensee shall prepare and submit to Monitor a certificate to the effect that, following a review for the purpose of paragraph 2(b) the Directors of the Licensee are or are not satisfied, as the case may be that, in the Financial Year most recently ended, the Licensee took all such precautions as were necessary in order to comply with this Condition.
Requirement to submit a certificate to NHSI for 2019/20 to be confirmed
4. The Licensee shall publish each certificate submitted for the purpose of this Condition within one month of its submission to Monitor in such manner as is likely to bring it to the attention of such persons who reasonably can be expected to have an interest in it.
Confirmed
Condition G7 – Registration with the Care Quality Commission1. The Licensee shall at all times be registered with the Care Quality Commission in so far as is necessary in order to be able lawfully to provide the services
authorised to be provided by this Licence.Confirmed
2. The Licensee shall notify Monitor promptly of:(a) any application it may make to the Care Quality Commission for the cancellation of its registration by that Commission, or(b) the cancellation by the Care Quality Commission for any reason of its registration by that Commission.
Confirmed
3. A notification given by the Licensee for the purposes of paragraph 2 shall:(a) be made within 7 days of:(i) the making of an application in the case of paragraph (a), or(ii) becoming aware of the cancellation in the case of paragraph (b), and(b) contain an explanation of the reasons (in so far as they are known to the Licensee) for:(i) the making of an application in the case of paragraph (a), or(ii) the cancellation in the case of paragraph (b).
Confirmed
Condition G8 – Patient eligibility and selection criteria1. The Licensee shall:
(a) set transparent eligibility and selection criteria,(b) apply those criteria in a transparent way to persons who, having a choice of persons from whom to receive health care services for the purposes of the NHS, choose to receive them from the Licensee, and(c) publish those criteria in such a manner as will make them readily accessible by any persons who could reasonably be regarded as likely to have an interest in them.
Confirmed
Condition G9 – Application of Section 5 (Continuity of Services)1. The Conditions in Section 5 shall apply:
(a) whenever the Licensee is subject to a contractual or other legally enforceable obligation to provide a service which is a Commissioner Requested Service, and(b) from the commencement of this Licence until the Licensee becomes subject to an obligation of the type described in sub-paragraph (a), if the Licensee is an NHS foundation trust which:
Confirmed
9/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
40/72
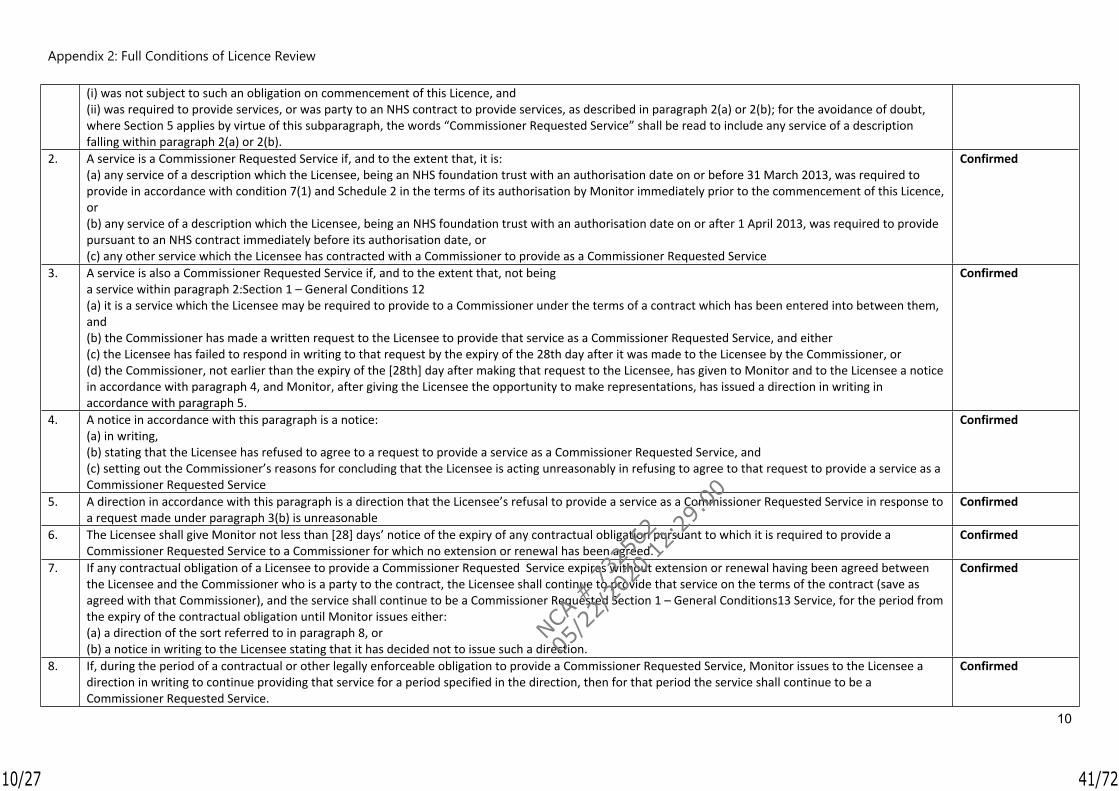
Appendix 2: Full Conditions of Licence Review
10
(i) was not subject to such an obligation on commencement of this Licence, and(ii) was required to provide services, or was party to an NHS contract to provide services, as described in paragraph 2(a) or 2(b); for the avoidance of doubt, where Section 5 applies by virtue of this subparagraph, the words “Commissioner Requested Service” shall be read to include any service of a description falling within paragraph 2(a) or 2(b).
2. A service is a Commissioner Requested Service if, and to the extent that, it is:(a) any service of a description which the Licensee, being an NHS foundation trust with an authorisation date on or before 31 March 2013, was required to provide in accordance with condition 7(1) and Schedule 2 in the terms of its authorisation by Monitor immediately prior to the commencement of this Licence, or(b) any service of a description which the Licensee, being an NHS foundation trust with an authorisation date on or after 1 April 2013, was required to provide pursuant to an NHS contract immediately before its authorisation date, or(c) any other service which the Licensee has contracted with a Commissioner to provide as a Commissioner Requested Service
Confirmed
3. A service is also a Commissioner Requested Service if, and to the extent that, not being a service within paragraph 2:Section 1 – General Conditions 12(a) it is a service which the Licensee may be required to provide to a Commissioner under the terms of a contract which has been entered into between them, and (b) the Commissioner has made a written request to the Licensee to provide that service as a Commissioner Requested Service, and either(c) the Licensee has failed to respond in writing to that request by the expiry of the 28th day after it was made to the Licensee by the Commissioner, or(d) the Commissioner, not earlier than the expiry of the [28th] day after making that request to the Licensee, has given to Monitor and to the Licensee a notice in accordance with paragraph 4, and Monitor, after giving the Licensee the opportunity to make representations, has issued a direction in writing in accordance with paragraph 5.
Confirmed
4. A notice in accordance with this paragraph is a notice:(a) in writing, (b) stating that the Licensee has refused to agree to a request to provide a service as a Commissioner Requested Service, and(c) setting out the Commissioner’s reasons for concluding that the Licensee is acting unreasonably in refusing to agree to that request to provide a service as a Commissioner Requested Service
Confirmed
5. A direction in accordance with this paragraph is a direction that the Licensee’s refusal to provide a service as a Commissioner Requested Service in response to a request made under paragraph 3(b) is unreasonable
Confirmed
6. The Licensee shall give Monitor not less than [28] days’ notice of the expiry of any contractual obligation pursuant to which it is required to provide a Commissioner Requested Service to a Commissioner for which no extension or renewal has been agreed.
Confirmed
7. If any contractual obligation of a Licensee to provide a Commissioner Requested Service expires without extension or renewal having been agreed between the Licensee and the Commissioner who is a party to the contract, the Licensee shall continue to provide that service on the terms of the contract (save as agreed with that Commissioner), and the service shall continue to be a Commissioner Requested Section 1 – General Conditions13 Service, for the period from the expiry of the contractual obligation until Monitor issues either:(a) a direction of the sort referred to in paragraph 8, or(b) a notice in writing to the Licensee stating that it has decided not to issue such a direction.
Confirmed
8. If, during the period of a contractual or other legally enforceable obligation to provide a Commissioner Requested Service, Monitor issues to the Licensee a direction in writing to continue providing that service for a period specified in the direction, then for that period the service shall continue to be a Commissioner Requested Service.
Confirmed
10/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
41/72
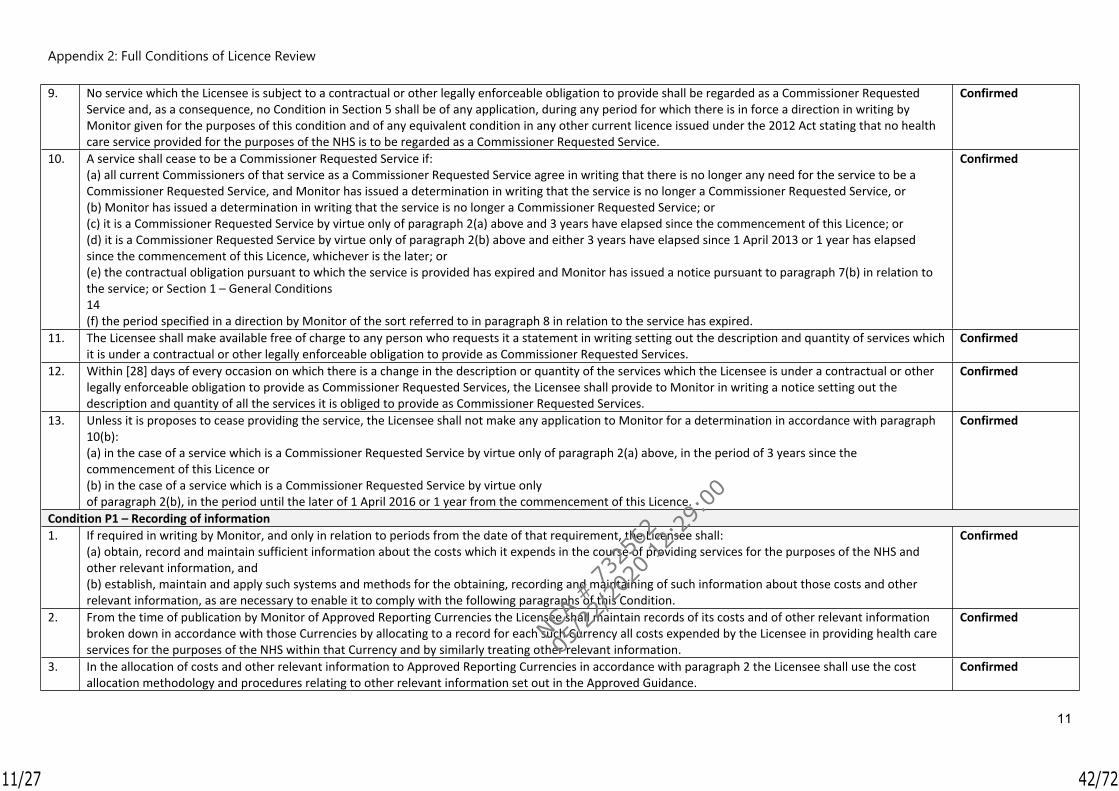
Appendix 2: Full Conditions of Licence Review
11
9. No service which the Licensee is subject to a contractual or other legally enforceable obligation to provide shall be regarded as a Commissioner Requested Service and, as a consequence, no Condition in Section 5 shall be of any application, during any period for which there is in force a direction in writing by Monitor given for the purposes of this condition and of any equivalent condition in any other current licence issued under the 2012 Act stating that no health care service provided for the purposes of the NHS is to be regarded as a Commissioner Requested Service.
Confirmed
10. A service shall cease to be a Commissioner Requested Service if:(a) all current Commissioners of that service as a Commissioner Requested Service agree in writing that there is no longer any need for the service to be a Commissioner Requested Service, and Monitor has issued a determination in writing that the service is no longer a Commissioner Requested Service, or(b) Monitor has issued a determination in writing that the service is no longer a Commissioner Requested Service; or(c) it is a Commissioner Requested Service by virtue only of paragraph 2(a) above and 3 years have elapsed since the commencement of this Licence; or(d) it is a Commissioner Requested Service by virtue only of paragraph 2(b) above and either 3 years have elapsed since 1 April 2013 or 1 year has elapsed since the commencement of this Licence, whichever is the later; or(e) the contractual obligation pursuant to which the service is provided has expired and Monitor has issued a notice pursuant to paragraph 7(b) in relation to the service; or Section 1 – General Conditions14(f) the period specified in a direction by Monitor of the sort referred to in paragraph 8 in relation to the service has expired.
Confirmed
11. The Licensee shall make available free of charge to any person who requests it a statement in writing setting out the description and quantity of services which it is under a contractual or other legally enforceable obligation to provide as Commissioner Requested Services.
Confirmed
12. Within [28] days of every occasion on which there is a change in the description or quantity of the services which the Licensee is under a contractual or other legally enforceable obligation to provide as Commissioner Requested Services, the Licensee shall provide to Monitor in writing a notice setting out the description and quantity of all the services it is obliged to provide as Commissioner Requested Services.
Confirmed
13. Unless it is proposes to cease providing the service, the Licensee shall not make any application to Monitor for a determination in accordance with paragraph 10(b): (a) in the case of a service which is a Commissioner Requested Service by virtue only of paragraph 2(a) above, in the period of 3 years since the commencement of this Licence or(b) in the case of a service which is a Commissioner Requested Service by virtue only of paragraph 2(b), in the period until the later of 1 April 2016 or 1 year from the commencement of this Licence.
Confirmed
Condition P1 – Recording of information1. If required in writing by Monitor, and only in relation to periods from the date of that requirement, the Licensee shall:
(a) obtain, record and maintain sufficient information about the costs which it expends in the course of providing services for the purposes of the NHS and other relevant information, and(b) establish, maintain and apply such systems and methods for the obtaining, recording and maintaining of such information about those costs and other relevant information, as are necessary to enable it to comply with the following paragraphs of this Condition.
Confirmed
2. From the time of publication by Monitor of Approved Reporting Currencies the Licensee shall maintain records of its costs and of other relevant information broken down in accordance with those Currencies by allocating to a record for each such Currency all costs expended by the Licensee in providing health care services for the purposes of the NHS within that Currency and by similarly treating other relevant information.
Confirmed
3. In the allocation of costs and other relevant information to Approved Reporting Currencies in accordance with paragraph 2 the Licensee shall use the cost allocation methodology and procedures relating to other relevant information set out in the Approved Guidance.
Confirmed
11/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
42/72

Appendix 2: Full Conditions of Licence Review
12
4. If the Licensee uses sub-contractors in the provision of health care services for the purposes of the NHS, to the extent that it is required to do so in writing by Monitor the Licensee shall procure that each of those sub-contractors:(a) obtains, records and maintains information about the costs which it expends in the course of providing services as sub-contractor to the Licensee, and establishes, maintains and applies systems and methods for the obtaining, recording and maintaining of that information, in a manner that complies with paragraphs 2 and 3 of this Condition, and(b) provides that information to Monitor in a timely manner.
Confirmed
5. Records required to be maintained by this Condition shall be kept for not less than six years. Confirmed
Condition P2 – Provision of information1. Subject to paragraph 3, and without prejudice to the generality of Condition G1, the Licensee shall furnish to Monitor such information and documents, and
shall prepare or procure and furnish to Monitor such reports, as Monitor may require for the purpose of performing its functions under Chapter 4 in Part 3 of the 2012 Act.
Confirmed
2. Information, documents and reports required to be furnished under this Condition shall be furnished in such manner, in such form, at such place and at such times as Monitor may require.
Confirmed
3. In furnishing information documents and reports pursuant to paragraphs 1 and 2 the Licensee shall take all reasonable steps to ensure that:(a) in the case of information or a report, it is accurate, complete and not misleading;(b) in the case of a document, it is a true copy of the document requested
Confirmed
4. This Condition shall not require the Licensee to furnish any information, documents or reports which it could not be compelled to produce or give in evidence in civil proceedings before a court because of legal professional privilege.
Confirmed
Condition P3 – Assurance report on submissions to Monitor1. If required in writing by Monitor the Licensee shall, as soon as reasonably practicable, obtain and submit to Monitor an assurance report in relation to a
submission of the sort described in para 2 and para 3 of P3.Confirmed
2. The descriptions of submissions in relation to which a report may be required under paragraph 1 are:(a) submissions of information furnished to Monitor pursuant to Condition P2, and(b) submissions of information to third parties designated by Monitor as persons from or through whom cost information may be obtained for the purposes of setting or verifying the National Tariff or of developing non-tariff pricing guidance.
Confirmed
3. An assurance report shall meet the requirements of this paragraph if all of the following conditions are met:(a) it is prepared by a person approved in writing by Monitor or qualified to act as auditor of an NHS foundation trust in accordance with paragraph 23(4) in Schedule 7 to the 2006 Act;(b) it expresses a view on whether the submission to which it relates:(i) is based on cost records which have been maintained in a manner which complies with paragraph 2 in Condition P1; (ii) is based on costs which have been analysed in a manner which complies with paragraph 3 in Condition P1, and(iii) provides a true and fair assessment of the information it contains.
Confirmed
Condition P4 – Compliance with the National Tariff1. Except as approved in writing by Monitor, the Licensee shall only provide health care services for the purpose of the NHS at prices which comply with, or are
determined in accordance with, the national tariff published by Monitor, in accordance with section 116 of the 2012 Act.Confirmed
12/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
43/72
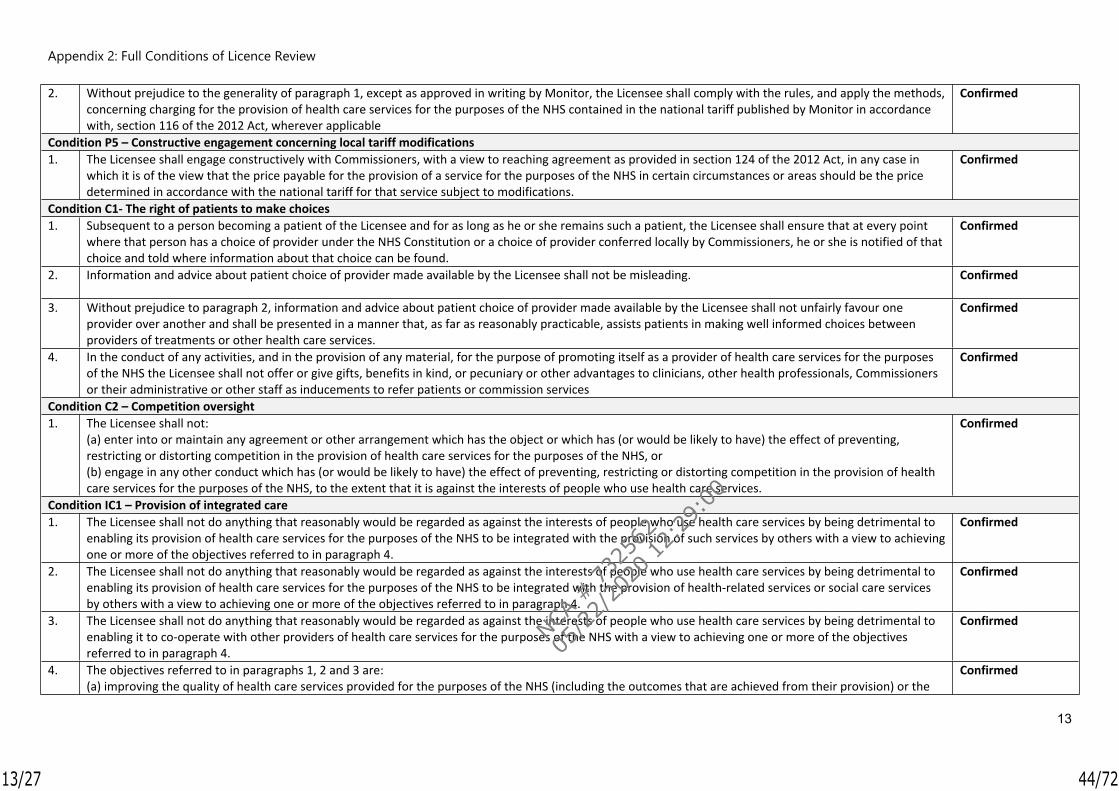
Appendix 2: Full Conditions of Licence Review
13
2. Without prejudice to the generality of paragraph 1, except as approved in writing by Monitor, the Licensee shall comply with the rules, and apply the methods, concerning charging for the provision of health care services for the purposes of the NHS contained in the national tariff published by Monitor in accordance with, section 116 of the 2012 Act, wherever applicable
Confirmed
Condition P5 – Constructive engagement concerning local tariff modifications1. The Licensee shall engage constructively with Commissioners, with a view to reaching agreement as provided in section 124 of the 2012 Act, in any case in
which it is of the view that the price payable for the provision of a service for the purposes of the NHS in certain circumstances or areas should be the price determined in accordance with the national tariff for that service subject to modifications.
Confirmed
Condition C1- The right of patients to make choices1. Subsequent to a person becoming a patient of the Licensee and for as long as he or she remains such a patient, the Licensee shall ensure that at every point
where that person has a choice of provider under the NHS Constitution or a choice of provider conferred locally by Commissioners, he or she is notified of that choice and told where information about that choice can be found.
Confirmed
2. Information and advice about patient choice of provider made available by the Licensee shall not be misleading. Confirmed
3. Without prejudice to paragraph 2, information and advice about patient choice of provider made available by the Licensee shall not unfairly favour one provider over another and shall be presented in a manner that, as far as reasonably practicable, assists patients in making well informed choices between providers of treatments or other health care services.
Confirmed
4. In the conduct of any activities, and in the provision of any material, for the purpose of promoting itself as a provider of health care services for the purposes of the NHS the Licensee shall not offer or give gifts, benefits in kind, or pecuniary or other advantages to clinicians, other health professionals, Commissioners or their administrative or other staff as inducements to refer patients or commission services
Confirmed
Condition C2 – Competition oversight1. The Licensee shall not:
(a) enter into or maintain any agreement or other arrangement which has the object or which has (or would be likely to have) the effect of preventing, restricting or distorting competition in the provision of health care services for the purposes of the NHS, or(b) engage in any other conduct which has (or would be likely to have) the effect of preventing, restricting or distorting competition in the provision of health care services for the purposes of the NHS, to the extent that it is against the interests of people who use health care services.
Confirmed
Condition IC1 – Provision of integrated care1. The Licensee shall not do anything that reasonably would be regarded as against the interests of people who use health care services by being detrimental to
enabling its provision of health care services for the purposes of the NHS to be integrated with the provision of such services by others with a view to achieving one or more of the objectives referred to in paragraph 4.
Confirmed
2. The Licensee shall not do anything that reasonably would be regarded as against the interests of people who use health care services by being detrimental to enabling its provision of health care services for the purposes of the NHS to be integrated with the provision of health-related services or social care services by others with a view to achieving one or more of the objectives referred to in paragraph 4.
Confirmed
3. The Licensee shall not do anything that reasonably would be regarded as against the interests of people who use health care services by being detrimental to enabling it to co-operate with other providers of health care services for the purposes of the NHS with a view to achieving one or more of the objectives referred to in paragraph 4.
Confirmed
4. The objectives referred to in paragraphs 1, 2 and 3 are:(a) improving the quality of health care services provided for the purposes of the NHS (including the outcomes that are achieved from their provision) or the
Confirmed
13/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
44/72
Appendix 2: Full Conditions of Licence Review
14
efficiency of their provision,(b) reducing inequalities between persons with respect to their ability to access those services, and(c) reducing inequalities between persons with respect to the outcomes achieved for them by the provision of those services.
5. The Licensee shall have regard to such guidance as may have been issued by Monitor from time to time concerning actions or behaviours that might reasonably be regarded as against the interests of people who use health care services for the purposes of paragraphs 1, 2 or 3 of this Condition.
Confirmed
Condition CoS1 – Continuing provision of Commissioner Requested Services1. The Licensee shall not cease to provide, or materially alter the specification or means of provision of, any Commissioner Requested Service otherwise than in
accordance with the following paragraphs of this Condition.Confirmed
2. If, during the period of a contractual or other legally enforceable obligation to provide a Commissioner Requested Service, or during any period when this condition applies by virtue of Condition G9(1)(b), Monitor issues to the Licensee a direction in writing to continue providing that service for a period specified in the direction, then the Licensee shall provide the service for that period in accordance with the direction.
Confirmed
3. The Licensee shall not materially alter the specification or means of provision of any Commissioner Requested Service except:(a) with the agreement in writing of all Commissioners to which the Licensee is required by a contractual or other legally enforceable obligation to provide the service as a Commissioner Requested Service; or(b) at any time when this condition applies by virtue of Condition G9(1)(b), with the agreement in writing of all Commissioners to which the Licensee provides, or may be requested to provide, the service as a Commissioner Requested Service; or(c) if required to do so by, or in accordance with the terms of its authorisation by, any body having responsibility pursuant to statute for regulating one or more aspects of the provision of health care services in England and which has been designated by Monitor for the purposes of this condition and of equivalent conditions in other licences granted under the 2012 Act.
Confirmed
4. If the specification or means of provision of a Commissioner Requested Service is altered as provided in paragraph 3 the Licensee, within [28] days of the alteration, shall give to Monitor notice in writing of the occurrence of the alteration with a summary of its nature.
Confirmed
Condition CoS2 – Restriction on the disposal of assets1. The Licensee shall establish, maintain and keep up to date, an asset register which complies with paragraphs 2 and 3 of this Condition (“the Asset Register”) Confirmed
2. The Asset Register shall list every relevant asset used by the Licensee for the provision of Commissioner Requested Services. Confirmed
3. The Asset Register shall be established, maintained and kept up to date in a manner that reasonably would be regarded as both adequate and professional. Confirmed
4. The obligations in paragraphs 5 to 8 shall apply to the Licensee if Monitor has given notice in writing to the Licensee that it is concerned about the ability of the Licensee to carry on as a going concern.
Confirmed
5. The Licensee shall not dispose of, or relinquish control over, any relevant asset except:(a) with the consent in writing of Monitor, and (b) in accordance with the paragraphs 6 to 8 of this Condition.
Confirmed
6. The Licensee shall furnish Monitor with such information as Monitor may request relating to any proposal by the Licensee to dispose of, or relinquish control over, any relevant asset.
Confirmed
7. Where consent by Monitor for the purpose of paragraph 5(a) is subject to conditions, the Licensee shall comply with those conditions. Confirmed
14/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
45/72
Appendix 2: Full Conditions of Licence Review
15
8. Paragraph 5(a) of this Condition shall not prevent the Licensee from disposing of, or relinquishing control over, any relevant asset where:(a) Monitor has issued a general consent for the purposes of this Condition (whether or not subject to conditions) in relation to:(i) transactions of a specified description; or(ii) the disposal of or relinquishment of control over relevant assets of a specified description, and the transaction or the relevant assets are of a description to which the consent applies and the disposal, or relinquishment of control, is in accordance with any conditions to which the consent is subject; or Section 5 – Continuity of Services 27(b) the Licensee is required by the Care Quality Commission to dispose of a relevant asset.
Confirmed
9. The Licensee shall have regard to such guidance as may be issued from time to time by Monitor regarding:(a) the manner in which asset registers should be established, maintained and updated, and(b) property, including buildings, interests in land, intellectual property rights and equipment, without which a licence holder’s ability to provide Commissioner Requested Services should be regarded as materially prejudiced.
Confirmed
Condition CoS3 – Standards of corporate governance and financial management1. The Licensee shall at all times adopt and apply systems and standards of corporate governance and of financial management which reasonably would be
regarded as:(a) suitable for a provider of the Commissioner Requested Services provided by the Licensee, and(b) providing reasonable safeguards against the risk of the Licensee being unable to carry on as a going concern.
Confirmed
2. In its determination of the systems and standards to adopt for the purpose of paragraph 1, and in the application of those systems and standards, the Licensee shall have regard to:(a) such guidance as Monitor may issue from time to time concerning systems and standards of corporate governance and financial management;(b) the Licensee’s rating using the risk rating methodology published by Monitor from time to time, and(c) the desirability of that rating being not less than the level regarded by Monitor as acceptable under the provisions of that methodology.
Confirmed
Condition CoS4 – Undertaking from the ultimate controller1. The Licensee shall procure from each company or other person which the Licensee knows or reasonably ought to know is at any time its ultimate controller, a
legally enforceable undertaking in favour of the Licensee, in the form specified by Monitor, that the ultimate controller (“the Covenantor”):(a) will refrain for any action, and will procure that any person which is a subsidiary of, or which is controlled by, the Covenantor (other than the Licensee and its subsidiaries) will refrain from any action, which would be likely to cause the Licensee to be in contravention of any of its obligations under the 2012 Act or this Licence, and(b) will give to the Licensee, and will procure that any person which is a subsidiary of, or which is controlled by, the Covenantor (other than the Licensee and its subsidiaries) will give to the Licensee, all such information in its possession or control as may be necessary to enable the Licensee to comply fully with its obligations under this Licence to provide information to Monitor.
Confirmed
2. The Licensee shall obtain any undertaking required to be procured for the purpose of paragraph 1 within 7 days of a company or other person becoming an ultimate controller of the Licensee and shall ensure that any such undertaking remains in force for as long as the Covenantor remains the ultimate controller of the Licensee.
Confirmed
3. The Licensee shall:(a) deliver to Monitor a copy of each such undertaking within seven days of obtaining it;(b) inform Monitor immediately in writing if any Director, secretary or other officer of the Licensee becomes aware that any such undertaking has ceased to be
Confirmed
15/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
46/72
Appendix 2: Full Conditions of Licence Review
16
legally enforceable or that its terms have been breached, and(c) comply with any request which may be made by Monitor to enforce any such undertaking.
4. For the purpose of this Condition, subject to paragraph 5, a person (whether an individual or a body corporate) is an ultimate controller of the Licensee if:(a) directly, or indirectly, the Licensee can be required to act in accordance with the instructions of that person acting alone or in concert with others, and (b) that person cannot be required to act in accordance with the instructions of another person acting alone or in concert with others.
Confirmed
5. A person is not an ultimate controller if they are:(a) a health service body, within the meaning of section 9 of the 2006 Act;(b) a Governor or Director of the Licensee and the Licensee is an NHS foundation trust;(c) any Director of the Licensee who does not, alone or in association with others, have a controlling interest in the ownership of the Licensee and the Licensee is a body corporate; or(d) a trustee of the Licensee and the Licensee is a charity.
Confirmed
Condition CoS5 – Risk pool levy1. The Licensee shall pay to Monitor any sums required to be paid in consequence of any requirement imposed on providers under section 135(2) of the 2012
Act, including sums payable by way of levy imposed under section 139(1) and any interest payable under section 143(10), by the dates by which they are required to be paid.
Confirmed
2. In the event that no date has been clearly determined by which a sum referred to in paragraph 1 is required to be paid, that sum shall be paid within 28 days of being demanded in writing by Monitor.
Confirmed
Condition CoS6 – Co-operation in the event of financial stress1. The obligations in paragraph 2 shall apply if Monitor has given notice in writing to the Licensee that it is concerned about the ability of the Licensee to carry on
as a going concern.Confirmed
2. When this paragraph applies the Licensee shall:(a) provide such information as Monitor may direct to Commissioners and to such other persons as Monitor may direct;(b) allow such persons as Monitor may appoint to enter premises owned or controlled by the Licensee and to inspect the premises and anything on them, and(c) co-operate with such persons as Monitor may appoint to assist in the management of the Licensee’s affairs, business and property.
Confirmed
Condition CoS7 – Availability of resources1. The Licensee shall at all times act in a manner calculated to secure that it has, or has access to, the Required Resources. Confirmed
2. The Licensee shall not enter into any agreement or undertake any activity which creates a material risk that the Required Resources will not be available to the Licensee.
Confirmed
3. The Licensee, not later than two months from the end of each Financial Year, shall submit to Monitor a certificate as to the availability of the Required Resources for the period of 12 months commencing on the date of the certificate, in one of the following forms:(a) “After making enquiries the Directors of the Licensee have a reasonable expectation that the Licensee will have the Required Resources available to it after taking account distributions which might reasonably be expected to be declared or paid for the period of 12 months referred to in this certificate.”(b) “After making enquiries the Directors of the Licensee have a reasonable expectation, subject to what is explained below, that the Licensee will have the Required Resources available to it after taking into account in particular (but without limitation) any distribution which might reasonably be expected to be declared or paid for the period of 12 months referred to in this certificate. However, they would like to draw attention to the following factors which may cast doubt on the ability of the Licensee to provide Commissioner Requested Services”.(c) “In the opinion of the Directors of the Licensee, the Licensee will not have the Required Resources available to it for the period of 12 months referred to in
Confirmed
(No requirement to submit a certificate to NHSI for 2019/20)
16/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
47/72
Appendix 2: Full Conditions of Licence Review
17
this certificate”.4. The Licensee shall submit to Monitor with that certificate a statement of the main factors which the Directors of the Licensee have taken into account in
issuing that certificate.Confirmed
5. The statement submitted to Monitor in accordance with paragraph 4 shall be approved by a resolution of the Board of Directors of the Licensee and signed by a Director of the Licensee pursuant to that resolution.
Confirmed
6. The Licensee shall inform Monitor immediately if the Directors of the Licensee become aware of any circumstance that causes them to no longer have the reasonable expectation referred to in the most recent certificate given under paragraph 3.
Confirmed
7. The Licensee shall publish each certificate provided for in paragraph 3 in such a manner as will enable any person having an interest in it to have ready access to it.
Confirmed
Condition FT1 – Information to update the register of NHS foundation trusts1. The obligations in the following paragraphs of this Condition apply if the Licensee is an NHS foundation trust, without prejudice to the generality of the other
conditions in this Licence.Confirmed
2. The Licensee shall ensure that Monitor has available to it written and electronic copies of the following documents:(a) the current version of Licensee’s constitution;(b) the Licensee’s most recently published annual accounts and any report of the auditor on them, and(c) the Licensee’s most recently published annual report, and for that purpose shall provide to Monitor written and electronic copies of any document establishing or amending its constitution within 28 days of being adopted and of the documents referred to in sub-paragraphs (b) and (c) within 28 days of being published.
Confirmed
3. Subject to paragraph 4, the Licensee shall provide to Monitor written and electronic copies of any document that is required by Monitor for the purpose of Section 39 of the 2006 Act within 28 days of the receipt of the original document by the Licensee.
Confirmed
4. The obligation in paragraph 3 shall not apply to:(a) any document provided pursuant to paragraph 2;(b) any document originating from Monitor; or(c) any document required by law to be provided to Monitor by another person
Confirmed
5. The Licensee shall comply with any direction issued by Monitor concerning the format in which electronic copies of documents are to be made available or provided.
Confirmed
6. When submitting a document to Monitor for the purposes of this Condition, the Licensee shall provide to Monitor a short written statement describing the document and specifying its electronic format and advising Monitor that the document is being sent for the purpose of updating the register of NHS foundation trusts maintained in accordance with section 39 of the 2006 Act.
Confirmed
Condition FT2 – Payment to Monitor in respect of registration and related costs1. The obligations in the following paragraph of this Condition apply if the Licensee is an NHS foundation trust, without prejudice to the generality of the other
conditions in this Licence.Confirmed
2. Whenever Monitor determines in accordance with section 50 of the 2006 Act that the Licensee must pay to Monitor a fee in respect of Monitor’s exercise of its functions under sections 39 and 39A of that Act the Licensee shall pay that fee to Monitor within 28 days of the fee being notified to the Licensee by Monitor in writing.
Confirmed
Condition FT3 – Provision of information to advisory panel
17/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
48/72
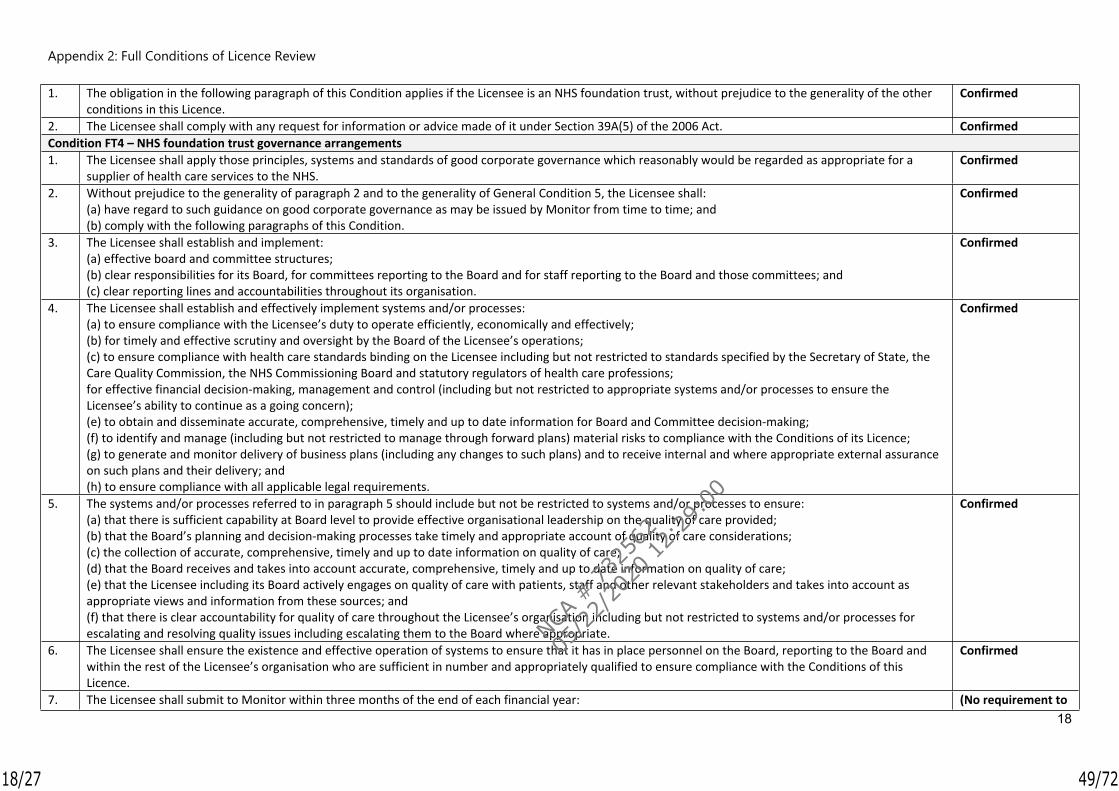
Appendix 2: Full Conditions of Licence Review
18
1. The obligation in the following paragraph of this Condition applies if the Licensee is an NHS foundation trust, without prejudice to the generality of the other conditions in this Licence.
Confirmed
2. The Licensee shall comply with any request for information or advice made of it under Section 39A(5) of the 2006 Act. ConfirmedCondition FT4 – NHS foundation trust governance arrangements1. The Licensee shall apply those principles, systems and standards of good corporate governance which reasonably would be regarded as appropriate for a
supplier of health care services to the NHS.Confirmed
2. Without prejudice to the generality of paragraph 2 and to the generality of General Condition 5, the Licensee shall:(a) have regard to such guidance on good corporate governance as may be issued by Monitor from time to time; and(b) comply with the following paragraphs of this Condition.
Confirmed
3. The Licensee shall establish and implement:(a) effective board and committee structures;(b) clear responsibilities for its Board, for committees reporting to the Board and for staff reporting to the Board and those committees; and(c) clear reporting lines and accountabilities throughout its organisation.
Confirmed
4. The Licensee shall establish and effectively implement systems and/or processes:(a) to ensure compliance with the Licensee’s duty to operate efficiently, economically and effectively;(b) for timely and effective scrutiny and oversight by the Board of the Licensee’s operations;(c) to ensure compliance with health care standards binding on the Licensee including but not restricted to standards specified by the Secretary of State, the Care Quality Commission, the NHS Commissioning Board and statutory regulators of health care professions;for effective financial decision-making, management and control (including but not restricted to appropriate systems and/or processes to ensure the Licensee’s ability to continue as a going concern);(e) to obtain and disseminate accurate, comprehensive, timely and up to date information for Board and Committee decision-making;(f) to identify and manage (including but not restricted to manage through forward plans) material risks to compliance with the Conditions of its Licence;(g) to generate and monitor delivery of business plans (including any changes to such plans) and to receive internal and where appropriate external assurance on such plans and their delivery; and(h) to ensure compliance with all applicable legal requirements.
Confirmed
5. The systems and/or processes referred to in paragraph 5 should include but not be restricted to systems and/or processes to ensure:(a) that there is sufficient capability at Board level to provide effective organisational leadership on the quality of care provided;(b) that the Board’s planning and decision-making processes take timely and appropriate account of quality of care considerations;(c) the collection of accurate, comprehensive, timely and up to date information on quality of care;(d) that the Board receives and takes into account accurate, comprehensive, timely and up to date information on quality of care;(e) that the Licensee including its Board actively engages on quality of care with patients, staff and other relevant stakeholders and takes into account as appropriate views and information from these sources; and(f) that there is clear accountability for quality of care throughout the Licensee’s organisation including but not restricted to systems and/or processes for escalating and resolving quality issues including escalating them to the Board where appropriate.
Confirmed
6. The Licensee shall ensure the existence and effective operation of systems to ensure that it has in place personnel on the Board, reporting to the Board and within the rest of the Licensee’s organisation who are sufficient in number and appropriately qualified to ensure compliance with the Conditions of this Licence.
Confirmed
7. The Licensee shall submit to Monitor within three months of the end of each financial year: (No requirement to
18/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
49/72

Appendix 2: Full Conditions of Licence Review
19
(a) a corporate governance statement by and on behalf of its Board confirming compliance with this Condition as at the date of the statement and anticipated compliance with this Condition for the next financial year, specifying any risks to compliance with this Condition in the next financial year and any actions it proposes to take to manage such risks; and(b) if required in writing by Monitor, a statement from its auditors either:(i) confirming that, in their view, after making reasonable enquiries, the Licensee has taken all the actions set out in its corporate governance statement applicable to the past financial year, or(ii) setting out the areas where, in their view, after making reasonable enquiries, the Licensee has failed to take the actions set out in its corporate governance statement applicable to the past financial year.
submit a certificate to NHSI for 2019/20)
19/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
50/72
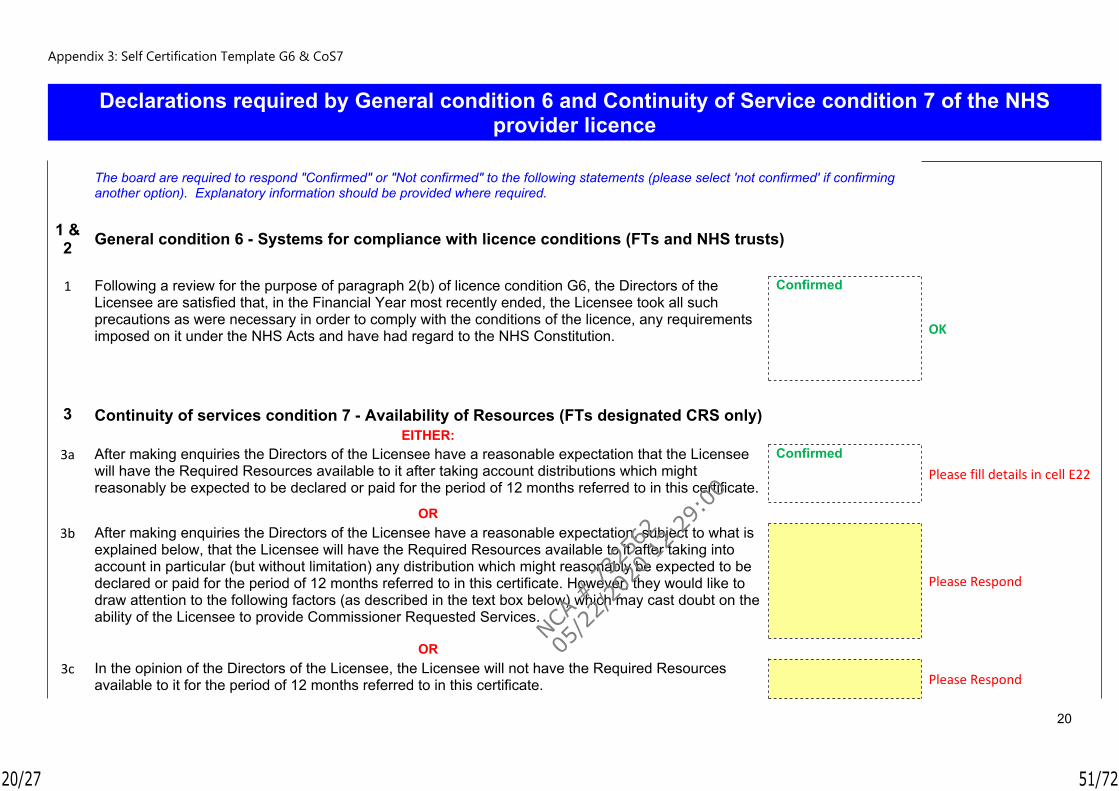
Appendix 3: Self Certification Template G6 & CoS7
20
Declarations required by General condition 6 and Continuity of Service condition 7 of the NHS provider licence
The board are required to respond "Confirmed" or "Not confirmed" to the following statements (please select 'not confirmed' if confirming another option). Explanatory information should be provided where required.
1 & 2 General condition 6 - Systems for compliance with licence conditions (FTs and NHS trusts)
1 Following a review for the purpose of paragraph 2(b) of licence condition G6, the Directors of the
Licensee are satisfied that, in the Financial Year most recently ended, the Licensee took all such precautions as were necessary in order to comply with the conditions of the licence, any requirements imposed on it under the NHS Acts and have had regard to the NHS Constitution.
Confirmed
OK
3 Continuity of services condition 7 - Availability of Resources (FTs designated CRS only) EITHER:
3a After making enquiries the Directors of the Licensee have a reasonable expectation that the Licensee will have the Required Resources available to it after taking account distributions which might reasonably be expected to be declared or paid for the period of 12 months referred to in this certificate.
ConfirmedPlease fill details in cell E22
OR 3b After making enquiries the Directors of the Licensee have a reasonable expectation, subject to what is
explained below, that the Licensee will have the Required Resources available to it after taking into account in particular (but without limitation) any distribution which might reasonably be expected to be declared or paid for the period of 12 months referred to in this certificate. However, they would like to draw attention to the following factors (as described in the text box below) which may cast doubt on the ability of the Licensee to provide Commissioner Requested Services.
Please Respond
OR 3c In the opinion of the Directors of the Licensee, the Licensee will not have the Required Resources
available to it for the period of 12 months referred to in this certificate.
Please Respond
20/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
51/72
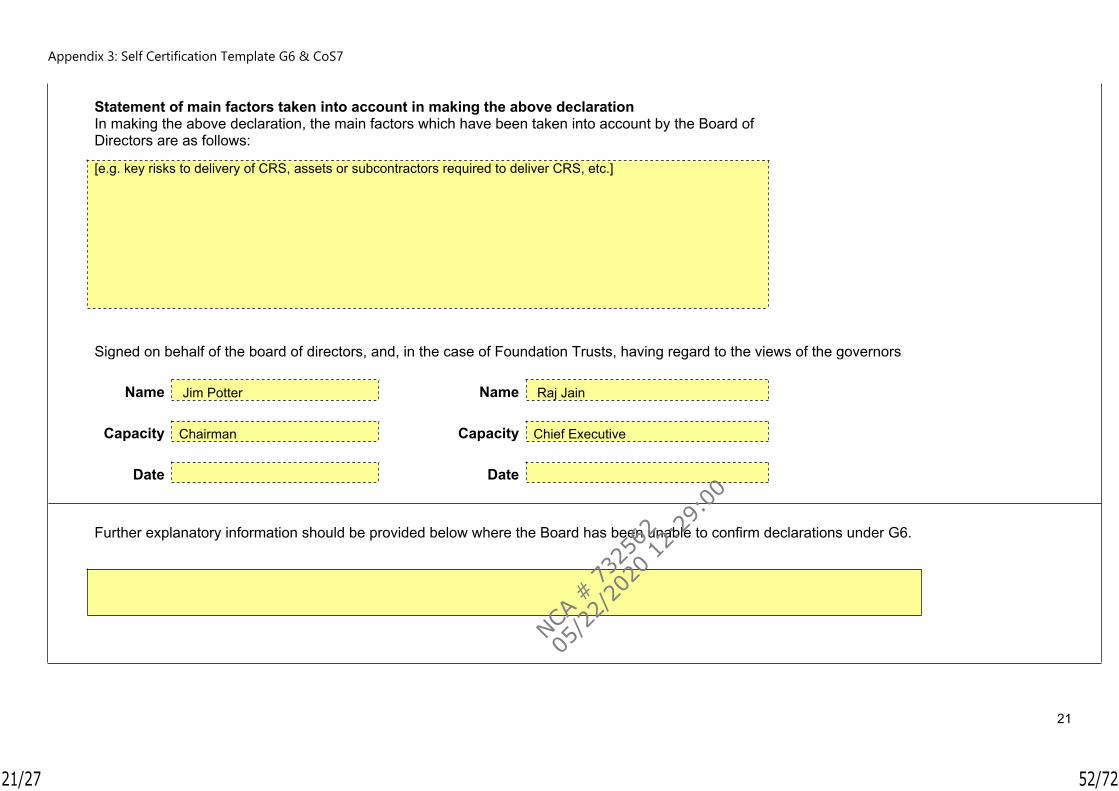
Appendix 3: Self Certification Template G6 & CoS7
21
Statement of main factors taken into account in making the above declaration
In making the above declaration, the main factors which have been taken into account by the Board of Directors are as follows:
[e.g. key risks to delivery of CRS, assets or subcontractors required to deliver CRS, etc.]
Signed on behalf of the board of directors, and, in the case of Foundation Trusts, having regard to the views of the governors Name Jim Potter Name Raj Jain Capacity Chairman Capacity Chief Executive Date Date
Further explanatory information should be provided below where the Board has been unable to confirm declarations under G6.
21/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
52/72
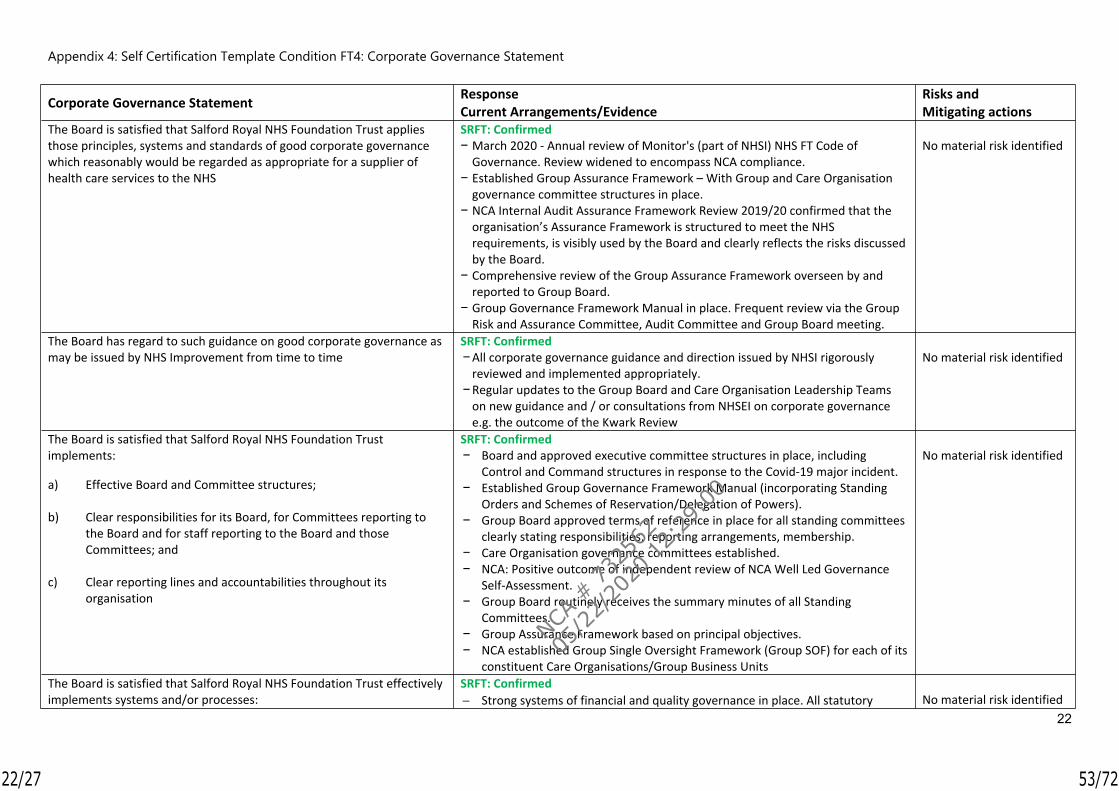
Appendix 4: Self Certification Template Condition FT4: Corporate Governance Statement
22
Corporate Governance Statement ResponseCurrent Arrangements/Evidence
Risks and Mitigating actions
The Board is satisfied that Salford Royal NHS Foundation Trust applies those principles, systems and standards of good corporate governance which reasonably would be regarded as appropriate for a supplier of health care services to the NHS
SRFT: Confirmed− March 2020 - Annual review of Monitor's (part of NHSI) NHS FT Code of
Governance. Review widened to encompass NCA compliance. − Established Group Assurance Framework – With Group and Care Organisation
governance committee structures in place. − NCA Internal Audit Assurance Framework Review 2019/20 confirmed that the
organisation’s Assurance Framework is structured to meet the NHS requirements, is visibly used by the Board and clearly reflects the risks discussed by the Board.
− Comprehensive review of the Group Assurance Framework overseen by and reported to Group Board.
− Group Governance Framework Manual in place. Frequent review via the Group Risk and Assurance Committee, Audit Committee and Group Board meeting.
No material risk identified
The Board has regard to such guidance on good corporate governance as may be issued by NHS Improvement from time to time
SRFT: Confirmed−All corporate governance guidance and direction issued by NHSI rigorously
reviewed and implemented appropriately. −Regular updates to the Group Board and Care Organisation Leadership Teams
on new guidance and / or consultations from NHSEI on corporate governance e.g. the outcome of the Kwark Review
No material risk identified
The Board is satisfied that Salford Royal NHS Foundation Trust implements:
a) Effective Board and Committee structures;
b) Clear responsibilities for its Board, for Committees reporting to the Board and for staff reporting to the Board and those Committees; and
c) Clear reporting lines and accountabilities throughout its organisation
SRFT: Confirmed− Board and approved executive committee structures in place, including
Control and Command structures in response to the Covid-19 major incident.− Established Group Governance Framework Manual (incorporating Standing
Orders and Schemes of Reservation/Delegation of Powers). − Group Board approved terms of reference in place for all standing committees
clearly stating responsibilities, reporting arrangements, membership. − Care Organisation governance committees established.− NCA: Positive outcome of independent review of NCA Well Led Governance
Self-Assessment.− Group Board routinely receives the summary minutes of all Standing
Committees. − Group Assurance Framework based on principal objectives. − NCA established Group Single Oversight Framework (Group SOF) for each of its
constituent Care Organisations/Group Business Units
No material risk identified
The Board is satisfied that Salford Royal NHS Foundation Trust effectively implements systems and/or processes:
SRFT: Confirmed Strong systems of financial and quality governance in place. All statutory No material risk identified
22/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
53/72

Appendix 4: Self Certification Template Condition FT4: Corporate Governance Statement
23
Corporate Governance Statement ResponseCurrent Arrangements/Evidence
Risks and Mitigating actions
a) To ensure compliance with the Licence holder’s duty to operate efficiently , economically and effectively
b) For timely and effective scrutiny and oversight by the Board of the Licence holder’s operations
c) To ensure compliance with health care standards binding on the Licence holder including but not restricted to standards specified by the Secretary of State, the Care Quality Commission, the NHS Commissioning Board and statutory regulators of health care professions;
d) For effective financial decision-making, management and control (including but not restricted to appropriate systems and/or processes to ensure the Licence holder’s ability to continue as a going concern)
e) To obtain and disseminate accurate, comprehensive, timely and up to date information for Board and Committee decision-making
f) To identify and manage (including but not restricted to manage through forward plans) material risks to compliance with the Conditions of its Licence;
g) To generate and monitor delivery of business plans (including any changes to such plans) and to receive internal and where appropriate external assurance on such plans and their delivery;
h) To ensure compliance with all applicable legal requirements.
audits and reporting requirements fulfilled. The Group SOF provides assurance on delivery of the Care Organisation
objectives and supports quality and performance improvement. The themes of the Group SOF reflect those of the NHS Single Oversight
Framework (which bases its oversight on the NHS provider licence: Quality of Care Finance and Use of Resources Operational performance Strategic Change Leadership and Improvement Capability (Well Led)
Performance dashboards at all levels within the NCA with divisional and corporate systems for appropriate escalation and review to ensure timely and effective scrutiny and oversight of all operations.
Effective systems and processes in place to ensure compliance with national and local healthcare standards - internal and external assurance systems in place. SRFT – CQC ‘Outstanding’.
Detailed financial plans in place and approved by the Group Board and Board of Directors. Cost Improvement programme agreed with Care Organisations and Group-wide Corporate functions.
Internal Audit Plan includes review of combined financial systems Contracts, service level agreements and leases under constant review. Biannual and rigorous review of the Trust as a Going Concern overseen by
Audit Committee and reported to Board/Group Board. Care Organisation financial performance scrutinised via respective Care Organisation Finance Governance Committee, with detailed reports to Group Board.
Group Board and committee structures fully serviced. Accurate, comprehensive, up-to-date information available for Group Board and committees.
NCA Board Assurance Framework/Corporate Risk Register in place that identifies and ensures appropriate oversight of all principal and material risks. Care Organisation/Corporate Risk Registers established.
Effective business planning arrangements in place, embedded within the corporate governance arrangements of the organisation.
Applicable legal requirements, against principal objectives and activities of the organisation reviewed and managed appropriately as part of the NCA’s
23/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
54/72

Appendix 4: Self Certification Template Condition FT4: Corporate Governance Statement
24
Corporate Governance Statement ResponseCurrent Arrangements/Evidence
Risks and Mitigating actions
corporate governance arrangements. The Board is satisfied:
a) That there is sufficient capability at Board level to provide effective organisational leadership on the quality of care provided;
b) That the Board’s planning and decision-making processes take timely and appropriate account of quality of care considerations;
c) The collection of accurate, comprehensive, timely and up to date information on quality of care;
d) That the Board receives and takes into account accurate, comprehensive, timely and up to date information on quality of care;
e) That Salford Royal NHS Foundation Trust/Pennine Acute Hospitals NHS Trust including its Board actively engages on quality of care with patients, staff and other relevant stakeholders and takes into account as appropriate views and information from these sources; and
f) That there is clear accountability for quality of care throughout Salford Royal NHS Foundation Trust/Pennine Acute Hospitals NHS Trust including but not restricted to systems and/or processes for escalating and resolving quality issues including escalating them to the Board where appropriate.
SRFT: Confirmed Group Board capability reviewed against strategic direction and business
plans. Robust appraisal and performance review arrangements in place at Board level (and throughout the organisation). Established leadership arrangements within Care Organisations. Specific focus on capability and capacity of leadership within Group Single Oversight Framework.
Quality of care fully integrated within all planning and decision-making processes. Quality Impact Assessments are required for major programmes of change at both NCA and CO level, and a process is in place to monitor and ratify these.
Integrated Performance Dashboards, QI Dashboards, patient experience, patient responsiveness reports, and quality of care initiatives provided routinely to Group Board. Outcome of clinical coding and data accuracy audits reported and reviewed via Audit Committee.
SRFT has a history of robust quality governance arrangements. These arrangements are being implemented across NCA. The first NCA–wide Quality and Productivity Improvement Strategy was developed and launched in 2019/20. A quarterly Quality Improvement Strategy Progress Report and quarterly Quality Dashboard is reviewed by the Group Board. At Care Organisation level, the Quality and Patient Experience (QPE) Governance Committees report directly to the COARCs, reviewing a suite of Quality Dashboards that track performance against key quality indicators; standardised risk assessment, and robust arrangements for staff, patients and members of the public to raise concerns with respect to the quality of care.
Nursing Assessment and Accreditation System fully established. Friends and Family Test systems in place.
Active engagement between the Group Board and the Group Council of Governors (CoG)s. Directors attend all CoG meetings and NEDs attend CoG sub-group meetings and training events. Membership and Public Engagement Strategy in place. Patient and Public Engagement Register established, although work needed to further encourage and embed its use.
Clear accountability for quality of care throughout the Trust, strong systems for appropriate escalation to Group Board.
No material risk identified
The Board of Salford Royal NHS Foundation Trust/Pennine Acute SRFT: Confirmed No material risk identified.
24/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
55/72
Appendix 4: Self Certification Template Condition FT4: Corporate Governance Statement
25
Corporate Governance Statement ResponseCurrent Arrangements/Evidence
Risks and Mitigating actions
Hospitals NHS Trust effectively implements systems to ensure that it has in place personnel on the Board, reporting to the Board and within the rest of the Licence holder’s organisation who are sufficient in number and appropriately qualified to ensure compliance with the Conditions of its provider licence.
SRFT’s Constitution sets out required numbers for Board members. Established Nominations Committees for Executive Director (ED) and Non-
Executive Director (NED) with Terms of Reference, with responsibility for review of Board composition.
ED and NED Job Descriptions and Person Specifications in place as developed via relevant Nominations Committee.
NCA People Strategy in place, including Talent Management & Leadership Development Strategies.
Code of Conduct and suitable contractual arrangements in place for Board members, incorporating requirements of the Licence condition relating to ‘fit and proper persons’.
25/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
56/72

Appendix 5: Self Certification on Training of Governors
26
Certification on Training of Governors Response
The Board is satisfied that during the financial year most recently ended the Trust has provided the necessary training to its Governors, as required in s151(5) of the Health and Social Care Act, to ensure they are equipped with the skills and knowledge they need to undertake their role.
ConfirmedA Governor Development and Training Programme is in place to include induction, annual, biennial and bespoke training. This will provide all governors with two opportunities to undertake training to equip them with the skills and knowledge to undertake their role in any 3 year term.
NHS Providers Guides for Governors and e-newsletter are disseminated to Governors throughout the year. Where a Governor has been unable to attend an internal development session, opportunities for attendance at externally facilitated training is provided.
Event Date AttendanceUnderstanding Quality Improvement (QI) 30 April 2019 10External Audit Roles and Responsibilities 27 June 2019 16North West Governor Forum 1 July 2019 8Governor Induction 12 November 2019 11Governor Listening Event 15 November 2019 6Patient Experience/QI Training 20 January 2020 5Sustainability across the NCA 11 February 2020 6
26/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
57/72
Appendix 6: CoS7 Management Review
27
3 Continuity of services condition 7 - Availability of Resources (FTs designated CRS only)
3a After making enquiries the Directors of the Licensee have a reasonable expectation that the Licensee will have the Required Resources available to it after taking account distributions which might reasonably be expected to be declared or paid for the period of 12 months referred to in this certificate.
SRFT: Confirmed
Current Arrangements
Review of all Licence conditions, including Continuity of Service (Appendix 2)
The draft SRFT Financial Plan 2020/21, reviewed at Group Board in February/March 2020 and submitted to NHSI at the beginning of April 2020, outlines the key points of the new financial arrangements for the period between 1 April and 31 July, along with information about the draft annual plan that was submitted to NHSI on 5th March 2020.
Audit Committee detailed mid-year review, in the form of an updated Going Concern Report providing financial outlook to March 2024. The review included overview of: Forecast Income and Expenditure Position
Better Care at Lower Cost (BCLC) Commissioning Intentions Working Capital, Capital Expenditure and Borrowing Cash Flow Forecast Hosted Services Risks and Uncertainties
27/27
NCA #
732
562
05/2
2/20
20 12:
29:0
0
58/72

The Northern Care Alliance NHS GroupSalford Royal NHS Foundation Trust (SRFT)
Meeting Group Board (Committees in Common)Author Rebecca McCarthy, Deputy Trust Secretary
Presented by Tim Crowley, Chairman of Audit Committee
Date 26th May 2020
Executive Summary
A summary is provided for the Group Board of the key matters and decisions from the Audit Committee meeting on 27th April 2020.
Annual Plan Objective
N/A
Principal Associated Risks
N/A
Recommendations The Group Board is asked to review the summary and the agreed actions from the meeting held on 26th April 2020.
Equality Does this paper relate to a matter where equality issues may arise? NoThis document does not contain confidential information and can be made available to the public.
This document contains some confidential information that would need to be redacted before the document was made available to the public.
Freedom of Information Please ‘cross’ one of the boxes
This document is entirely confidential, as the redaction of confidential information would render the document meaningless.
Title of Report Report from Group Audit Committee – 27th April 2020
X
1/3
NCA #
732
562
05/2
2/20
20 12:
29:0
0
59/72
Summary of Group Audit Committee meeting held on 30th April 2019 via Video Conference
Present: Mr Tim Crowley, Chairman of Audit Committee Mr Kieran Charleson, Non-Executive DirectorMrs Carmen Drinkwater, Non-Executive Director Mrs Chris Mayer CBE, Vice-ChairmanMr Jim Potter, Chairman (By invitation)Professor Chris Reilly, Senior Independent DirectorDr Hamish Stedman, Non-Executive Director
Attendance: Mrs Jane Burns, Director of Corporate Services/Group SecretaryMr Darrell Davies, Assistant Director, MIAAMr David Jago, Finance Director, Oldham Care OrganisationMr Raj Jain, Chief Executive Officer (Review of Annual Governance Statement)Mrs Diane Morrison, Finance Director, Salford Care OrganisationMr Ian Moston, Chief Financial OfficerMr Stephen Nixon, Engagement Manager, External AuditorMr Stephen Ridgway, Group Head of Financial Control Mrs Nicky Tamanis, Deputy Chief Financial Officer
Apologies: Mr Chris Brookes, Chief Medical Officer Mrs Sarah Dowbekin, Internal Audit Engagement Manager, MIAA Mr Mark Heap, Engagement Lead, External Auditor Mrs Elaine Inglesby-Burke CBE, Chief Nursing Officer
1. Audit Committee Annual Review 2019/20 and Work Plan 2020/21− Audit Committee confirmed all key duties of the committee, as delegated by the Group
Board, for 2019/20 had been fulfilled. − Reviewed the proposed reporting schedule for 2020/21 acknowledging scope for revision in
light of the major incident. Audit Committee agreed to engage further with both Internal and External Auditors, to explore governance requirements in these exceptional circumstances and redraft the workplan as required.
2. Year End Matters – Salford Royal NHS Foundation Trust
− SRFT Head of Internal Audit Opinion and Annual Report 2019/20 (including Summary of NCA and Salford Care Organisation) – Audit Committee reviewed and accepted the Head of Internal Audit Opinion – Substantial Assurance.
− Draft Annual Governance Statement 2019/20 – The Chief Executive Officer presented the draft SRFT Annual Governance Statement for inclusion within the SRFT 2019/20 Annual Report and Accounts. Audit Committee approved the Annual Governance Statement which confirmed that the Group Board had extensive and effective governance assurance systems in operation, and that no significant internal control issues had been identified during 2019/20.
− Draft Annual Report and Quality Report 2019/20 – Audit Committee reviewed the first draft of the SRFT Annual Report prepared in line with the revised Annual Report requirements and financial reporting requirements issued by NHS England/Improvement to NHS Foundation Trusts in light of pressures caused by the public sector response to Covid-19. Audit Committee provided comments and noted that final approval would take place at the Audit Committee on 19th June 2020 in line with the revised date for submission.
− Pre-Audited Annual Accounts 2019/20 including accounting policies for completion of 2019/20 Annual Accounts – Reviewed and confirmed.
− Draft Going Concern Report – Reviewed and accepted.− Response to Auditors from Those Charged with Governance – Reviewed and
confirmed.− Response to Auditors from Those Charged with Management – Reviewed and
confirmed.
2/3
NCA #
732
562
05/2
2/20
20 12:
29:0
0
60/72
3. SRFT External Audit Plan – Reviewed and confirmed.Addendum to SRFT Audit Plan relating to Covid-19 – Reviewed and confirmed.
4. Year End Matters – Pennine Acute Hospitals NHS Trust Audit Committee acknowledged that as part of the PAHT Interim Governance
Arrangements it had been agreed that the NCA Audit Committee would develop and receive all documentation relating to year-end matters relating to the Pennine Acute Hospitals NHS Trust (PAHT). The final PAHT Annual Report and Accounts and all year-end statements would be provided to PAHT Audit Committee, with a supporting Assurance Statement from NCA Audit Committee, to enable signatures as required and submission ahead of the final submission date.
− PAHT Head of Internal Audit Opinion and Annual Report 2019/20 (including Summary of NCA and Salford Care Organisation) – Audit Committee received and accepted the Head of Internal Audit Opinion – Substantial Assurance.
− Draft Annual Governance Statement 2019/20 – The Chief Executive Officer presented the draft PAHT Annual Governance Statement for inclusion within the PAHT 2019/20 Annual Report and Accounts. Audit Committee acknowledged that the Annual Governance Statement confirmed no significant internal control issues had been identified during 2019/20.
− Draft Annual Report and Quality Report 2019/20 – Audit Committee reviewed the first draft of the PAHT Annual Report prepared in line with the revised Annual Report requirements and financial reporting requirements issued by NHS England/Improvement to NHS Foundation Trusts in light of pressures caused by the public sector response to Covid-19. Audit Committee provided comments and noted that final approval would take place at the Audit Committee on 19th June 2020 in line with the revised date for submission.
− Pre-Audited Annual Accounts 2019/20 including accounting policies for completion of 2019/20 Annual Accounts – Reviewed and confirmed.
− Draft Going Concern Report – Reviewed and accepted.− Response to Auditors from Those Charged with Governance – Reviewed and
confirmed.− Response to Auditors from Those Charged with Management – Reviewed and
confirmed.
5. Addendum to PAHT Audit Plan relating to Covid-19 – Reviewed and confirmed.
6. NCA Anti-Fraud Annual Report 2019/20 – Reviewed and confirmed actions taken were appropriate.
7. Internal Audit and Anti-Fraud Plan - Proposal 2020/21 - Reviewed and confirmed the proposed Internal Audit and Anti-Fraud plan 2020/21 as presented to date, noting that this would need to be re-assessed to consider the impact of the pandemic on future activities and priorities.
8. COVID-19: Financial Governance Report - Reviewed and confirmed the financial governance arrangements in place for the period of the major incident.
9. SRFT External Auditor Contract Extension - Audit Committee reviewed and confirmed the proposed fee for the one year extension to the SRFT External Auditor contract.
3/3
NCA #
732
562
05/2
2/20
20 12:
29:0
0
61/72
1
Northern Care Alliance NHS GroupSalford Royal NHS Foundation Trust (SRFT)
Meeting Group Board (Committees in Common)
Author Rebecca McCarthy, Deputy Trust SecretaryJane Burns, Group Secretary
Presented by FOR INFORMATION ONLY
Date 26th May 2020
Executive Summary
As part of the PAHT Interim Governance Arrangements it was agreed that the NCA Audit Committee would develop and receive the PAHT Annual Report and Accounts, including Annual Governance Statement, Letter of Representation, Response to Auditors and Annual Self-Certifications.
The final PAHT Annual Report and Accounts and all year-end statements will be reviewed by NCA Audit Committee on 19th June 2020 and provided to PAHT Audit Committee and PAHT Board, with a supporting Assurance Statement from NCA Audit Committee, ahead of the final submission date.
The draft PAHT Annual Self-Certifications are provided for information to the Group Board (Committees in Common) ahead of review by NCA Audit Committee on 19th June in line with the aforementioned arrangements.
NHS foundation trusts and trusts are required to self-certify whether or not they have complied with the conditions of the NHS provider licence and whether or not they have complied with governance requirements.
Although NHS trusts are not issued with a provider licence, they are also required to self-certify whether or not they have complied with conditions equivalent to the licence that NHS Improvement has deemed appropriate, as described below.
The following declarations are required:
Condition G6 (3): Providers must certify that they have taken all precautions necessary to comply with the licence, NHS Act and NHS Constitution (Condition G6 (3))
Condition FT4 (8): Providers must certify compliance with required governance arrangements
Although there is no submission requirement; provider Boards must confirm that they understand clearly and can confirm compliance with the above conditions. The deadline for Board sign off on self-certifications has not yet been published by NHS Improvement; however approval support assurances highlighted within the Annual Governance Statement.
NHS Improvement (NHSI) may audit select providers with respect to the self-certification.
This year’s annual self-certification review has been completed to encompass
Title of ReportAnnual Self Certifications:
− General Condition: G6 Systems for compliance with licence conditions and related obligations
− NHS Foundation Trust Condition FT4:
1/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
62/72
2
compliance for the statutory body, Pennine Acute Hospitals NHS Trust (PAHT), as part of the Northern Care Alliance NHS Group (NCA) during 2019/20.
Annual Plan Objective
N/A
Principal Associated Risks
N/A
Recommendations N/A
Equality Does this paper relate to a matter where equality issues may arise? NIf so, has due regard been given to equality analysis of any adverse impactsThis document does not contain confidential information and can be made available to the public.
This document contains some confidential information that would need to be redacted before the document was made available to the public.
Freedom of Information
Please ‘cross’ one of the boxes
This document is entirely confidential, as the redaction of confidential information would render the document meaningless.
X
2/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
63/72
3
1. General Condition G6
1.1 General Condition 6 within the Licence requires providers to have in place effective systems and processes to ensure compliance with licence conditions and related obligations.
1.2 A management review has been undertaken confirming compliance with General Condition 6 of the NHS Provider Licence (Appendix 1).
1.3 PAHT are required to publish a G6 self-certification (Appendix 2) within a month following Board sign off.
2. Condition FT4
2.1 Condition FT4 within the Licence sets out provisions relating to principles, systems and standards of good corporate governance. The Corporate Governance Statement includes the provisions set out in Condition FT4. A description of the principal risks to compliance with Condition FT4, and actions identified to mitigate those risks is included within the PAHT Annual Governance Statement, which forms part of the Annual Report to be submitted on 25th June 2020.
2.2 A management review of the Corporate Governance Statement has been undertaken. Please see attached Appendix 3.
3/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
64/72
Appendix 1: General Condition 6 - Management Review
4
General Condition 6 Current Arrangements/EvidenceThe Licensee shall take all reasonable precautions against the risk of failure to comply with:(a) the Conditions of this Licence,(b) any requirements imposed on it under the NHS Acts, and(c) the requirement to have regard to the NHS Constitution in providing health care services for the purposes of the NHS.
Comprehensive business planning process in place, adapted in line with Covid-19 national planning requirements.
The draft PAHT Financial Plan 2020/21, reviewed at Group Board in February/March 2020, submitted to NHSI at the beginning of April 2020, outlines the key points of the new financial arrangements for the period between 1 April and 31 July, along with information about the draft annual plan that was submitted to NHSI on 5th March 2020.
The NCA Group Board has established and operates an oversight framework for each of its Care Organisations, called the Group Single Oversight Framework (Group SOF). The Group SOF provides assurance on delivery of the Care Organisation Annual Plan objectives and supports quality and performance improvement. The themes of the Group SOF reflect those of the NHS Single Oversight Framework (which bases its oversight on the NHS provider licence): Quality of Care Finance and Use of Resources Operational performance Strategic Change Leadership and Improvement Capability (Well Led) Approved Group Governance Framework Manual - Sets out the control framework within which the Group’s and Care Organisations objectives are delivered. The Manual highlights processes and systems in place to oversee constitutional, regulatory and legal compliance. The Manual incorporates Reservation of Powers and Delegation of Powers, Detailed Scheme of Delegation and Standing Financial Instructions. Group Governance Framework Manual is refreshed regularly and ratified/approved by Audit Committee and the Board.
COVID-19 Update: During the on-going COVID-19 situation, temporary emergency modifications to the financial governance arrangements in the GGFM have been developed and approved via Gold Command and reviewed via Audit Committee in April 2020.
In March 2018, the Group Board approved an NCA Risk Management Strategy. The NCA Risk Management Strategy provides a framework for managing risks across the Group and Care Organisations, which is consistent with best practice and Department of Health guidance. The Strategy provides a clear, systematic approach to the management of risks to ensure that risk assessment is an integral part of clinical, managerial and financial processes across the organisation for the benefit of patients, staff, visitors and other stakeholders.
There is a Risk Assessment and Risk Register Policy in place describing how staff will fulfil their role in risk assessment and the production of risk registers and interaction required between directorates, divisions and the Care Organisation committees. All risks regardless of their nature or origin are managed via this process.
PAHT are registered with the Care Quality Commission and systems exist to ensure compliance with the registration
4/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
65/72
Appendix 1: General Condition 6 - Management Review
5
General Condition 6 Current Arrangements/Evidencerequirements, detailed in the respective Annual Governance Statements. PAHT: CQC Inspection – ‘Good’ February 2020.
2019/20 Corporate Governance Statements – Reviewed by Group Board (May 2020) and Audit Committee (June 2020). Recommendation: No material risks identified.
NHS Foundation Trust – Code of Governance Annual Review 2019/20. Although the Code is relevant to NHS Foundation Trusts, the review undertaken in March 2020 encompassed compliance for the Northern Care Alliance NHS Group (NCA). Review of compliance with each provision undertaken by the Group Board in March 2020
Audit Committee considered and approved the NCA Internal Audit Plan for 2019/20 (April 19). The Internal Audit Plan was risk based, with an ongoing programme of internal audits in finance, operations and governance. During the course of the year, Audit Committee monitored progress against the Internal Audit Plan and reviewed the work and findings of the Internal Auditor.
The NCA Internal Audit Assurance Framework Review 2019/20 confirmed that ‘the organisation’s Assurance Framework is structured to meet the NHS requirements, is visibly used by the Board and clearly reflects the risks discussed by the Board.’
Audit Committee reviewed the work and findings of the External Auditor during 2019/20, including valuable insight and benchmarking information.
PAHT Annual Report and Annual Accounts 2019/20 – Prepared in accordance with the Department of Health and Social Care Group Accounting Manual 2019-20.
Submission of compliance reports to NHS Improvement as required.
Without prejudice to the generality of paragraph 1, the steps that the Licensee must take pursuant to that paragraph shall include:(a) the establishment and implementation of processes and systems to identify risks and guard against their occurrence; and(b) regular review of whether those processes and systems have been implemented and of their effectiveness.
The NCA’s Group Assurance Framework, is based on six key elements: Clearly defined principal objectives agreed with stakeholders together with clear lines of responsibility and
accountability; Clearly defined principal risks to the achievement of these objectives together with assessment of their potential
impact and likelihood; Key controls by which these risks can be managed, this includes involvement of stakeholders in agreeing controls
where risks impact on them; Management and independent assurances that risks are being managed effectively; Board level reports identifying that risks are being reasonably managed and objectives being met together with
gaps in assurances and gaps in risk control;
5/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
66/72
Appendix 1: General Condition 6 - Management Review
6
General Condition 6 Current Arrangements/Evidence Board level action plans which ensure the delivery of objectives, control of risk and improvements in assurances.
The workplan of committees within the NCA’s Assurance Framework is linked so that the Group Board is assured that there is an aligned independent and executive focus on strategic risk and assurance. Routine referral of issues exists between committees ensuring a respective understanding of risk and assurance concerns.
The Group Board oversees the management of all major risks, which are actively addressed by the Group Risk and Assurance Committee (GRAC). The NCA Corporate Risk Register is integrated with the Board Assurance Framework thereby ensuring that risks are not only managed and communicated efficiently, but that the management of them is embedded in the NCA’s practice. The NCA Board Assurance Framework/Corporate Risk Register is reviewed on a quarterly basis, alongside the Care Organisation Board Assurance Framework/Corporate Risk Registers. Key controls and assurances, and any identified gaps are continually reviewed and action plans developed and progressed accordingly. All significant risks are detailed within the monthly Group Performance Dashboard presented to the Group Board by the Chief Executive Officer.
Audit Committee reviews the Board Assurance Framework/Corporate Risk Register and commissions additional reviews where appropriate in order to provide necessary assurance to the Group Board.
The Self-Assessment against the Well-Led Framework for Governance was updated in the final part of 2019/20 to reflect up-to-date practice in NCA/PAHT.
Annual Governance Statement – Reviewed by Audit Committee, April 2020 confirming “The Board had extensive and effective governance assurance systems in operation enabling the identification and control of risks reported through the Board Assurance Framework and Corporate Risk Register. Internal and external reviews, audits and inspections had provided sufficient evidence to state that no significant internal control issues have been identified during 2019/20, and that these control systems are fit for purpose.”
The PAHT financial plan is approved by the Group Board. It is subsequently submitted to NHS Improvement. The plan is monitored on a monthly basis by the Care Organisation Finance Governance Committees. The Care Organisations provide a monthly Statement of Assurance to GRAC which confirms the sufficiency of plans for the effective use of resources. Key performance indicators and financial sustainability metrics are also reviewed monthly by the Group Board.
An internal CQC mock assessment programme is in operation whereby unannounced visits take place across each of the departments that do not take part in the NAAS/CAAS process. Assurance is provided by Audit Committee, which monitors the outcome of the mock assessment programme in-year and commissions specific reviews by the Trust’s internal auditors.
6/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
67/72
Appendix 1: General Condition 6 - Management Review
7
General Condition 6 Current Arrangements/Evidence
Audit Committee review of:− Register of Interests for Senior Staff and Gifts and Hospitality Registers to ensure compliance with the Trust’s
Standards of Business (Annual)− The arrangements by which staff can raise issues in confidence about possible improprieties in matters of
financial reporting and control, clinical quality, patient safety or other matters to ensure arrangements are in place for the proportionate and independent investigation of such matters and appropriate follow-up action (Annual)
− Group Governance Framework Manual (Annual)− Counter Fraud Plans and Reports− Internal Audit Annual Programme, progress reports and audit outcomes − Clinical Audit Annual Programme and Developments − All risk and control related disclosure statements in particular the Annual Governance Statement, Corporate
Governance Statement, together with the accompanying Head of Internal Audit statement and External Audit Opinion.
On 30 January 2020, the Director-General of WHO declared the 2019-nCoV outbreak a public health emergency of international concern under the International Health Regulations (IHR) (2005). As the NCA is a designated Category 1 responder, under the Civil Contingences Act 2004, it has a well-established Emergency Preparedness Resilience & Response Unit (EPRRU). A clear Command and Control Structure consisting of one Gold Command Team was established, supported by specialist sub groups and Care Organisation Silver Command Teams. Gold Command and GRAC have established a purposeful risk management interaction, including effective system for the escalation of risk, to ensure the continued effectiveness of the NCA’s system of internal control for the duration of the major incident.
7/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
68/72
Appendix 2: Declarations required by General condition 6 of the NHS provider licence
8
Declarations required by General condition 6 of the NHS provider licence
1 & 2 General condition 6 - Systems for compliance with license conditions
1 Following a review for the purpose of paragraph 2(b) of licence condition G6, the Directors of the Licensee are satisfied, as the case may be that, in the Financial Year most recently ended, the Licensee took all such precautions as were necessary in order to comply with the conditions of the licence, any requirements imposed on it under the NHS Acts and have had regard to the NHS Constitution.
PAHT: Confirmed
Further explanatory information should be provided below where the Board has been unable to confirm declarations under G6.
A
8/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
69/72

Appendix 3: FT4: Corporate Governance Statement Management Review
9
Corporate Governance Statement ResponseCurrent Arrangements/Evidence
Risks and Mitigating actions
The Board is satisfied that Pennine Acute Hospitals NHS Trust applies those principles, systems and standards of good corporate governance which reasonably would be regarded as appropriate for a supplier of health care services to the NHS
PAHT: Confirmed− April 2019 - Annual review of Monitor's (part of NHSI) NHS FT Code of
Governance. Review widened to encompass NCA compliance. − Established Group Assurance Framework – With Group and Care Organisation
governance committee structures in place. − NCA Internal Audit Assurance Framework Review 2019/20 confirmed that the
organisation’s Assurance Framework is structured to meet the NHS requirements, is visibly used by the Board and clearly reflects the risks discussed by the Board.
− Comprehensive review of the Group Assurance Framework overseen by and reported to Group Board.
− Group Governance Framework Manual in place. Annual review via the Group Risk and Assurance Committee, Audit Committee and Group Board meeting.
No material risk identified
The Board has regard to such guidance on good corporate governance as may be issued by NHS Improvement from time to time
PAHT: Confirmed−All corporate governance guidance and direction issued by NHSI rigorously
reviewed and implemented appropriately. − Regular updates to the Group CiC and Care Organisation Leadership
Teams on new guidance and / or consultations from NHSI on corporate governance, e.g. the outcome of the Kwark Review
No material risk identified
The Board is satisfied that Salford Royal NHS Foundation Trust/Pennine Acute Hospital NHS Trust implements:
a) Effective Board and Committee structures;
b) Clear responsibilities for its Board, for Committees reporting to the Board and for staff reporting to the Board and those Committees; and
c) Clear reporting lines and accountabilities throughout its organisation
PAHT: Confirmed− Board and approved executive committee structures in place, including
Control and Command structures in response to the Covid-19 major incident− Established Group Governance Framework Manual (incorporating Standing
Orders and Schemes of Reservation/Delegation of Powers). − Group Board approved terms of reference in place for all standing committees
clearly stating responsibilities, reporting arrangements, membership. − Care Organisation governance committees established.− NCA: Positive outcome of independent review of NCA Well Led Governance
Self-Assessment.− Group Board routinely receives the summary minutes of all Standing
Committees − NCA established Group Single Oversight Framework (Group SOF) for each of its
constituent Care Organisations.
No material risk identified
The Board is satisfied that Salford Royal NHS Foundation Trust/Pennine Acute Hospitals NHS Trust effectively implements systems and/or processes
PAHT: Confirmed Strong systems of financial and quality governance in place. All statutory
audits and reporting requirements fulfilled. No material risk identified
9/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
70/72

Appendix 3: FT4: Corporate Governance Statement Management Review
10
Corporate Governance Statement ResponseCurrent Arrangements/Evidence
Risks and Mitigating actions
a) To ensure compliance with the Licence holder’s duty to operate efficiently , economically and effectively
b) For timely and effective scrutiny and oversight by the Board of the Licence holder’s operations
c) To ensure compliance with health care standards binding on the Licence holder including but not restricted to standards specified by the Secretary of State, the Care Quality Commission, the NHS Commissioning Board and statutory regulators of health care professions;
d) For effective financial decision-making, management and control (including but not restricted to appropriate systems and/or processes to ensure the Licence holder’s ability to continue as a going concern)
e) To obtain and disseminate accurate, comprehensive, timely and up to date information for Board and Committee decision-making
f) To identify and manage (including but not restricted to manage through forward plans) material risks to compliance with the Conditions of its Licence;
g) To generate and monitor delivery of business plans (including any changes to such plans) and to receive internal and where appropriate external assurance on such plans and their delivery;
h) To ensure compliance with all applicable legal requirements.
The Group SOF provides assurance on delivery of the Care Organisation Annual Plan objectives and supports quality and performance improvement.
The themes of the Group SOF reflect those of the NHS Single Oversight Framework (which bases its oversight on the NHS provider licence): Quality of Care Finance and Use of Resources Operational performance Strategic Change Leadership and Improvement Capability (Well Led)
Performance dashboards at all levels within the NCA with divisional and corporate systems for appropriate escalation and review to ensure timely and effective scrutiny and oversight of all operations.
Effective systems and processes in place to ensure compliance with national and local healthcare standards - internal and external assurance systems in place. PAHT – CQC ‘Good, February 2020.
Financial plan in place and approved by the Group Board. Internal Audit Plan includes review of combined financial systems (PAHT)
Biannual and rigorous review of the Trust as a Going Concern overseen by Audit Committee and reported to Board
Financial performance scrutinised via respective Care Organisation Finance Governance Committee, with detailed reports to Group Board.
Group Board and committee structures fully serviced. Accurate, comprehensive, up-to-date information available for Group Board and committees.
NCA Board Assurance Framework/Corporate Risk Register in place that identifies and ensures appropriate oversight of all principal and material risks. Care Organisation/Corporate Risk Registers established.
Effective business planning arrangements in place, embedded within the corporate governance arrangements of the organisation.
Applicable legal requirements, against principal objectives and activities of the organisation reviewed and managed appropriately as part of the NCA’s corporate governance arrangements.
The Board is satisfied:
a) That there is sufficient capability at Board level to provide
PAHT: Confirmed Robust appraisal and performance review arrangements in place at Board
level (and throughout the organisation). Established leadership arrangements No material risk identified
10/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
71/72
Appendix 3: FT4: Corporate Governance Statement Management Review
11
Corporate Governance Statement ResponseCurrent Arrangements/Evidence
Risks and Mitigating actions
effective organisational leadership on the quality of care provided;
b) That the Board’s planning and decision-making processes take timely and appropriate account of quality of care considerations;
c) The collection of accurate, comprehensive, timely and up to date information on quality of care;
d) That the Board receives and takes into account accurate, comprehensive, timely and up to date information on quality of care;
e) That Salford Royal NHS Foundation Trust/Pennine Acute Hospitals NHS Trust including its Board actively engages on quality of care with patients, staff and other relevant stakeholders and takes into account as appropriate views and information from these sources; and
f) That there is clear accountability for quality of care throughout Salford Royal NHS Foundation Trust/Pennine Acute Hospitals NHS Trust including but not restricted to systems and/or processes for escalating and resolving quality issues including escalating them to the Board where appropriate.
within Care Organisations. Specific focus on capability and capacity of leadership within Group Single Oversight Framework.
Quality of care fully integrated within all planning and decision-making processes. Quality Impact Assessments are required for major programmes of change at both NCA and CO level, and a process is in place to monitor and ratify these.
Integrated Performance Dashboards, QI Dashboards, patient experience, patient responsiveness reports, and quality of care initiatives provided routinely to Group Board.
Outcome of clinical coding and data accuracy audits reported and reviewed via Audit Committee.
NCA–wide Quality and Productivity Improvement Strategy was developed and launched in 2019/20. A quarterly Quality Improvement Strategy Progress Report and quarterly Quality Dashboard is reviewed by the Group Board. At Care Organisation level, the Quality and Patient Experience (QPE) Governance Committees report directly to the COARCs, reviewing a suite of Quality Dashboards that track performance against key quality indicators; standardised risk assessment, and robust arrangements for staff, patients and members of the public to raise concerns with respect to the quality of care.
Nursing Assessment and Accreditation System fully established. Friends and Family Test systems in place.
Clear accountability for quality of care throughout the Trust, strong systems for appropriate escalation to Group Board.
The Board of Pennine Acute Hospitals NHS Trust effectively implements systems to ensure that it has in place personnel on the Board, reporting to the Board and within the rest of the Licence holder’s organisation who are sufficient in number and appropriately qualified to ensure compliance with the Conditions of its provider licence.
PAHT: ConfirmedEstablished Nominations Committees for Executive Director (ED) and Non-Executive Director (NED) with Terms of Reference, with responsibility for review of Board composition. ED and NED Job Descriptions and Person Specifications in place as developed via relevant Nominations Committee.NCA People Strategy in place, including Talent Management & Leadership Development Strategies.Code of Conduct and suitable contractual arrangements in place for Board members, incorporating requirements of the Licence condition relating to ‘fit and proper persons’.
No material risk identified.
11/11
NCA #
732
562
05/2
2/20
20 12:
29:0
0
72/72