normal posterior segment anatomy and myopic …normal posterior segment anatomy and myopic...
TRANSCRIPT

NORMAL POSTERIOR SEGMENT ANATOMY AND MYOPIC
DEGENERATION
Jessica Watson MD
*some slides/images from Elaine Binkley MD and Drew Carey MD
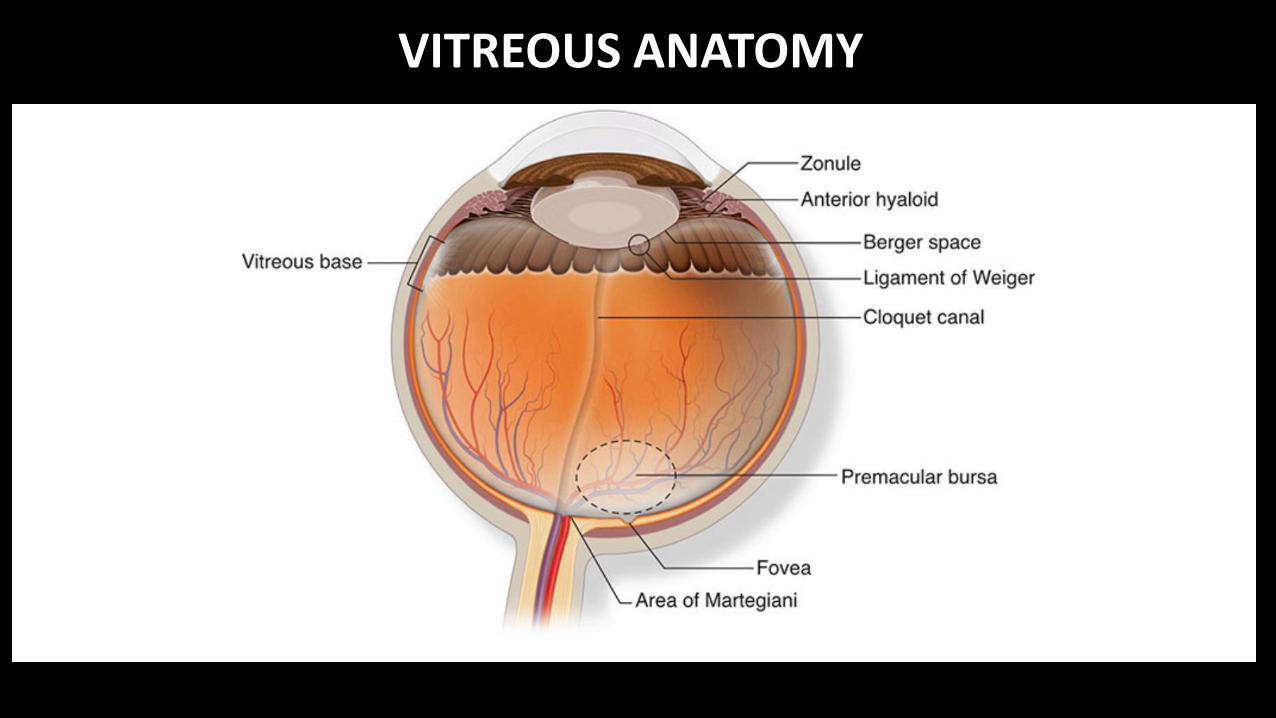
VITREOUS ANATOMY
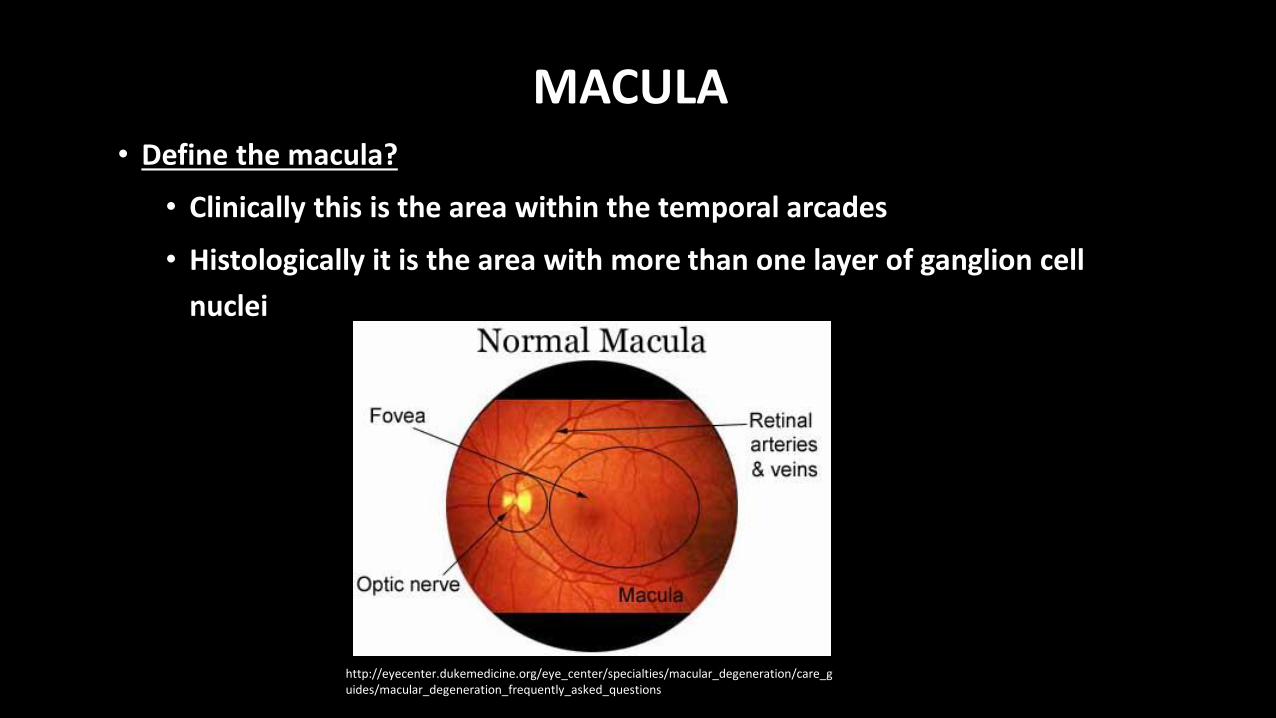
MACULA• Define the macula?
• Clinically this is the area within the temporal arcades
• Histologically it is the area with more than one layer of ganglion cell
nuclei
http://eyecenter.dukemedicine.org/eye_center/specialties/macular_degeneration/care_guides/macular_degeneration_frequently_asked_questions

MACULA
• How big is the foveal avascular zone?
• 250-600 microns
http://www.ijo.in/article.asp?issn=0301-4738;year=2011;volume=59;issue=1;spage=9;epage=11;aulast=John
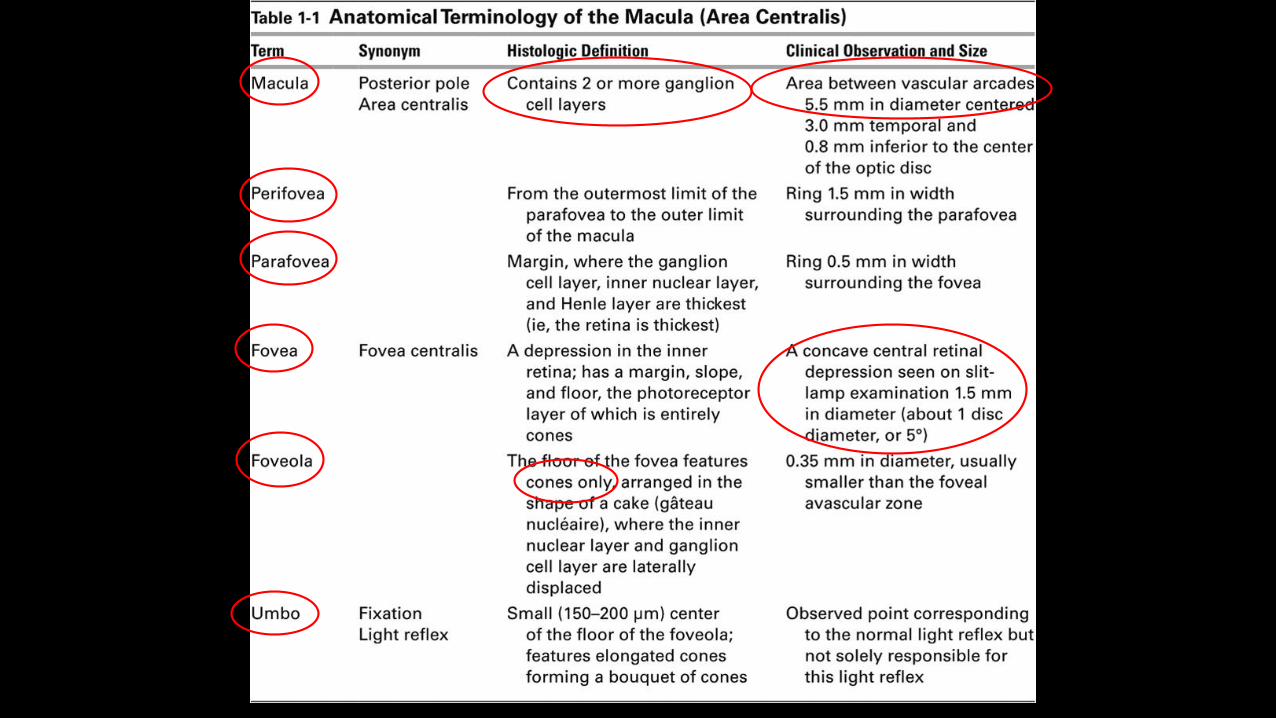

perifovea
parafovea
fovea

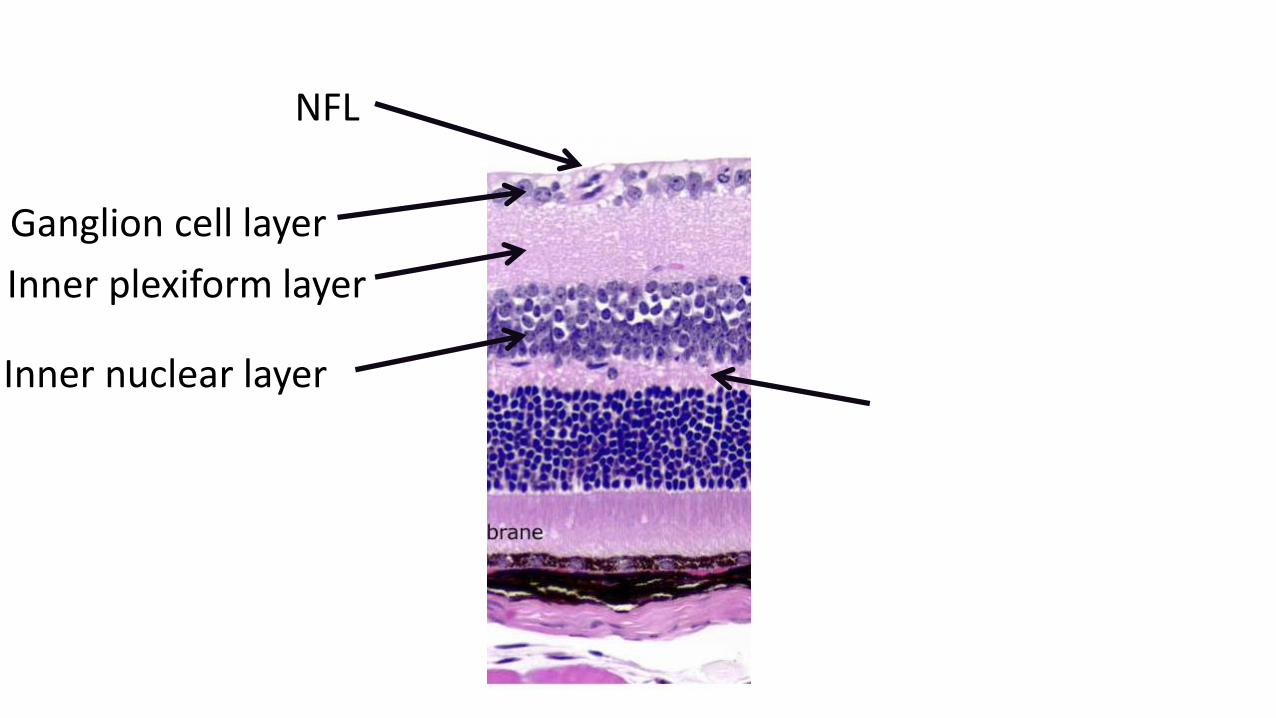
Name the structures!

NFL

Name the structures!
NFL
Ganglion cell layer

Name the structures!
NFL
Ganglion cell layer
Inner plexiform layer

NFL
Ganglion cell layer
Inner plexiform layer
Inner nuclear layer
Name the structures!
NFL
Ganglion cell layer
Inner plexiform layer
Inner nuclear layer

NFL
Ganglion cell layer
Inner plexiform layer
Inner nuclear layer Outer plexiformlayer (Henle’s layer)

NFL
Ganglion cell layer
Inner plexiformlayer
Inner nuclear layer Outer plexiformlayer (Henle’s layer)

NFL
Ganglion cell layer
Inner plexiform layer
Inner nuclear layer Outer plexiformlayer (Henle’s layer)
Outer nuclear layer

NFL
Ganglion cell layer
Inner plexiform layer
Inner nuclear layer Outer plexiform layer (Henle’s layer)
Outer nuclear layer
Photoreceptors

NFL
Ganglion cell layer
Inner plexiform layer
Inner nuclear layer Outer plexiform layer (Henle’s layer)
Outer nuclear layer
Photoreceptors
Retinal pigmented epithelium
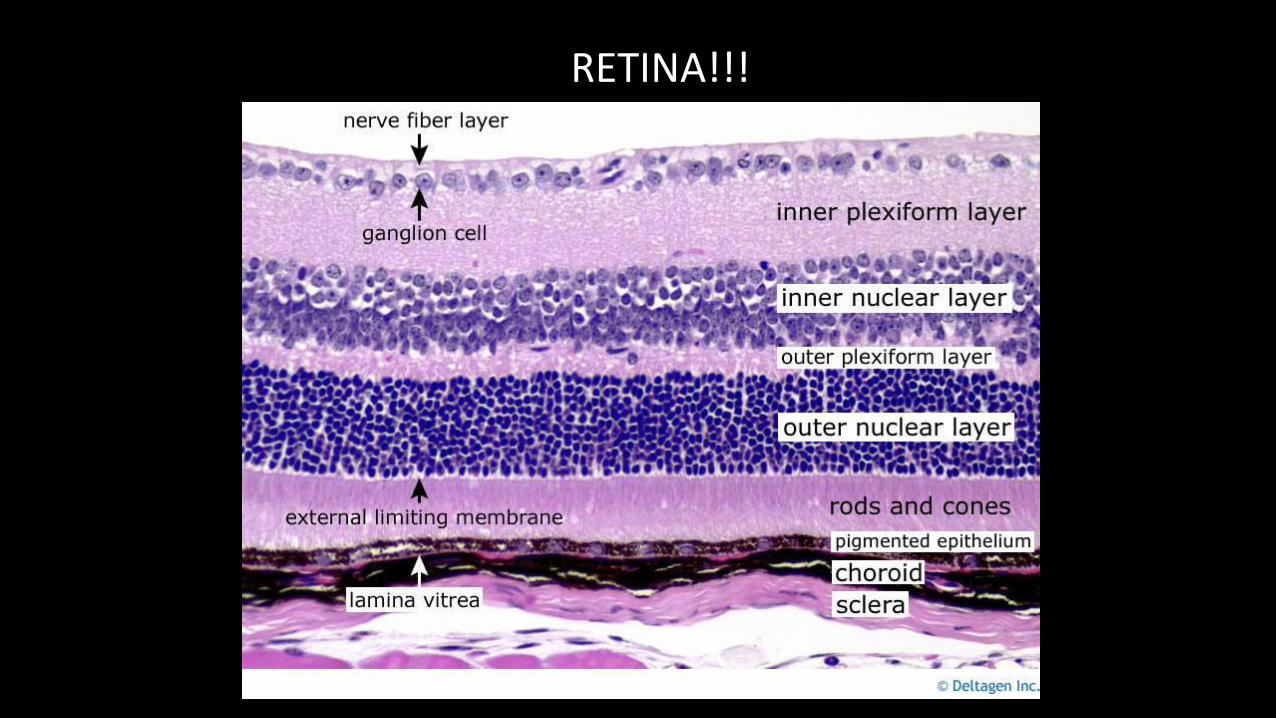
RETINA!!!

RETINA!!!
http://users.atw.hu/blp6/BLP6/HTML/common/M9780323045827-008-f002.jpg

Handbook of retinal OCT 1st ed. Duker, Waheed, and Goldman.
What disease may be shown here?

Handbook of retinal OCT 1st ed. Duker, Waheed, and Goldman.
What is wrong with this OCT?
What disease may this be?

RETINAL PIGMENTED EPITHELIUM (RPE)
• RPE
• Single layer of cuboidal epithelial cells
making up the outer layer of the retina
• Between the choriocapillaris and
outer segments of photoreceptors
• 4-6 million RPE cells per eye
• Ratio photoreceptors to RPE cells is
45:1
http://www.scienceofamd.org/learn/
https://medschool.vanderbilt.edu/ophthalmology/labs/cai

RETINAL PIGMENTED EPITHELIUM (RPE)
•RPE cells are polarized epithelial cells
•Apical side has tight junctions that make up part of the
blood-retina barrier

RETINAL PIGMENTED EPITHELIUM (RPE)
• What are the major jobs of the RPE? (5)
• 1) Visual pigment regeneration
• 2) Phagocytosis of shed photoreceptor outer segments
• 3) Transport nutrients and ions to
photoreceptors/waste removal
• 4) Absorption scattered light
• 5) Adhesion of the retina
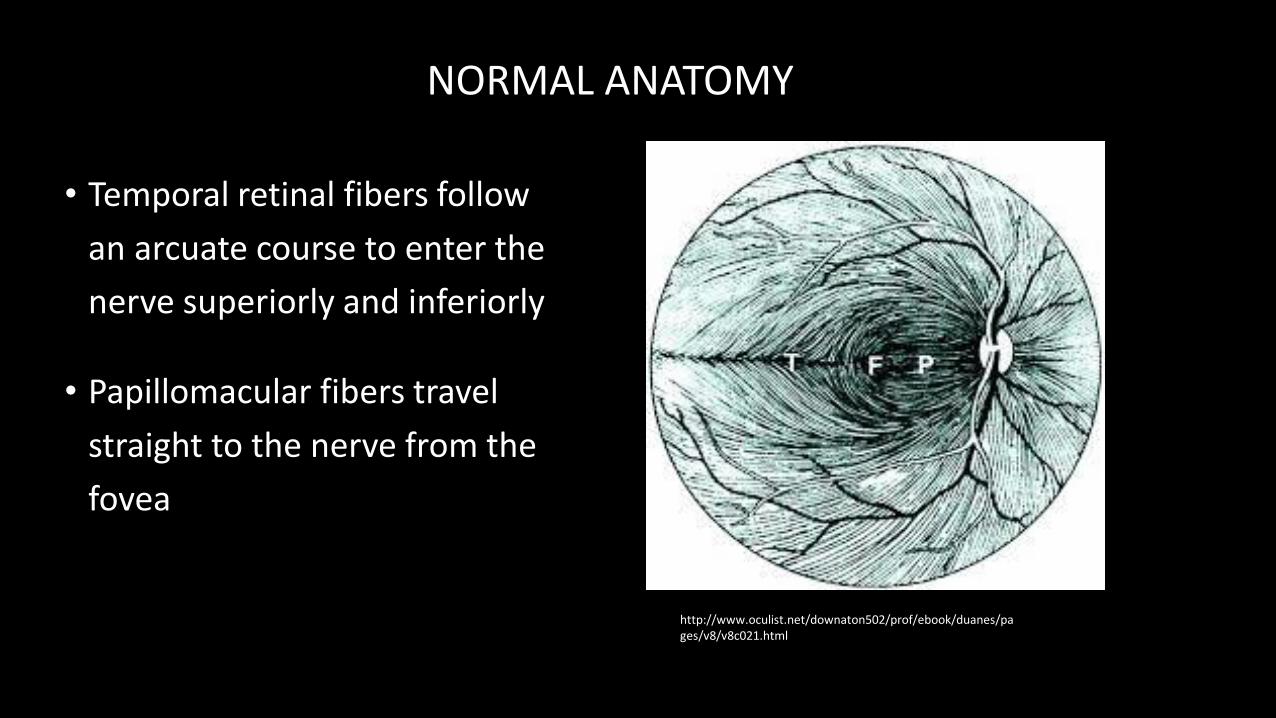
NORMAL ANATOMY
• Temporal retinal fibers follow
an arcuate course to enter the
nerve superiorly and inferiorly
• Papillomacular fibers travel
straight to the nerve from the
fovea
http://www.oculist.net/downaton502/prof/ebook/duanes/pages/v8/v8c021.html

NORMAL ANATOMY
• Müller cells are the glial cells that form the ELM and ILM (not true membranes!)
• ILM is made up of Müller footplates
• Cells are oriented perpendicular to the plane of the RPE in the middle and outer layers but parallel to the retinal surface in the inner layers
• This is why nerve fiber layer hemorrhages are linear and IRH are “dot blots”
https://www.aao.org/eyenet/article/disc-hemorrhages-in-eyes-with-glaucoma
http://www.keywordsdoctor.com/ZG90IGJsb3QgaGVtZQ/

DEGENERATIVE MYOPIA

DEGENERATIVE MYOPIA
• Myopia is a major cause of visual impairment and blindness worldwide
• Myopia most common ocular abnormality in the US (25% of the population).
• High myopia: greater than - 6 D/ 26.5 mm
• Pathologic myopia: greater than -8D/32.5 mm
• Degenerative Myopia =progressive elongation associated with secondary changes
caused by mechanical stretch
• 2% American / possibly high as 10% East Asian
DEGENERATIVE MYOPIA
• Systemic associations with high myopia
• Down syndrome
• Stickler syndrome
• Marfan syndrome
• Prematurity
• Noonan syndrome
• Ehlers–Danlos syndrome
• Pierre–Robin syndrome

PALE TESSELLATED /TIGROID FUNDUS
Due to diffuse attenuation of
the RPE with visibility of large
choroidal vessels

ANOMALOUS OPTIC NERVE HEAD
• May appear unusually
small, large or anomalous
with a “tilted”
conformation.
• Peripapillary chorioretinal
atrophy is very common
• temporal crescent of
thinned or absent RPE

LACQUER CRACKS
• Ruptures in the RPE-Bruchs
membrane-choriocapillaris
complex characterized by fine
irregular yellow lines
crisscrossing the posterior
pole
• ~ 5% of highly myopic eyes
• can be complicated by CNV

PERIPHERAL LACQUER CRACKS

• Due to break in thickened,
calcified Bruch’s
membrane
• Emanate from disc head
• Occur in diseases such as
pseudoxanthoma
elasticum, Ehlers-Danlos
syndrome, sickle cell,
Paget’s disease of bone
ANGIOD STREAK VERSUS LAQUER CRACK
https://maculacenter.com/eye-disease/pseudoxanthoma-elasticum/

SUBRETINAL “COIN” HEMORRHAGES
• May develop from lacquer
cracks in the absence of CNV
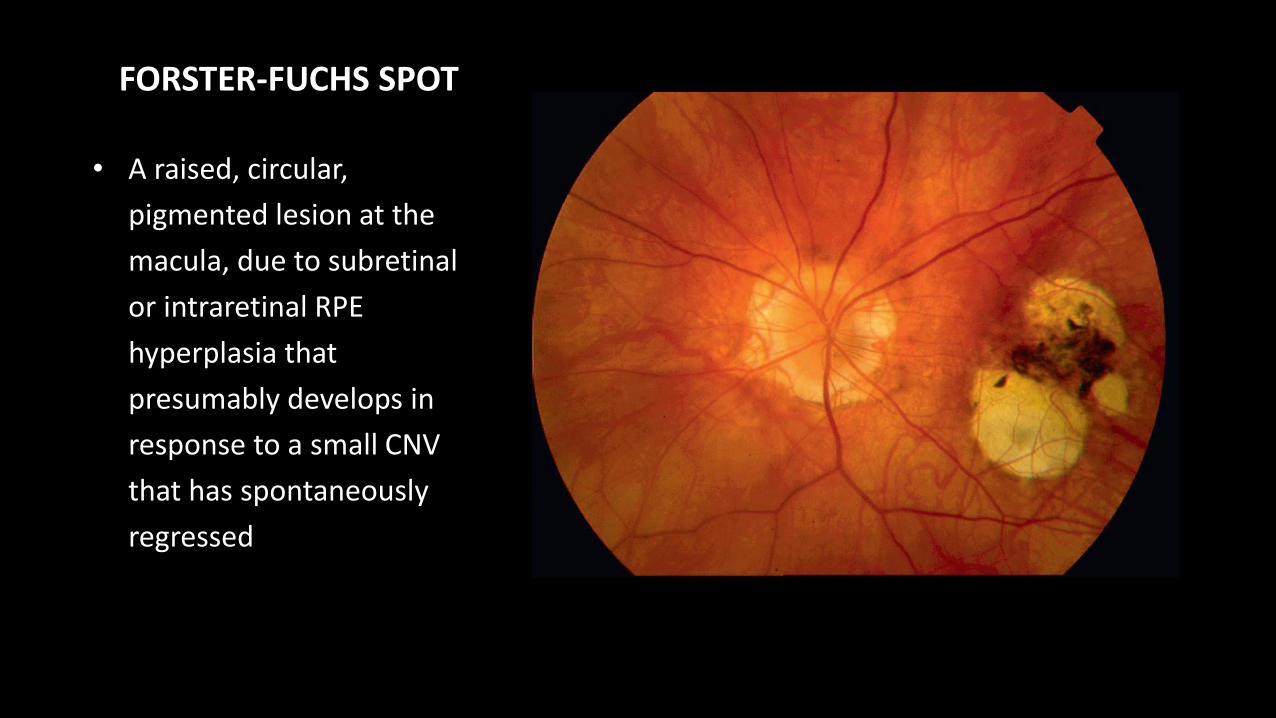
FORSTER-FUCHS SPOT
• A raised, circular,
pigmented lesion at the
macula, due to subretinal
or intraretinal RPE
hyperplasia that
presumably develops in
response to a small CNV
that has spontaneously
regressed

DIFFUSE CHORIORETINALATROPHY
• Observed as yellowish-
white, ill-defined
chorioretinal atrophy.
• Typically demonstrates a
thin choroid on OCT

PATCHY CHORIORETINALATROPHY
• Patchy, gyrate areas, of
well-defined chorioretinal
atrophy.
• Different from diffuse
chorioretinal atrophy:
• complete loss of the
choriocapillaris with
visibility of deep
choroidal vessels and
often sclera
• an absolute scotoma

STAPHYLOMA
• A peripapillary or macular
ectasia of the posterior
sclera due to focal thinning
and expansion
• ~ 1/3rd of eyes with
pathological myopia

Handbook of retinal OCT 1st ed. Duker, Waheed, and Goldman.

ANTERIOR STAPHYLOMA
• Grisk for needle injury with
retrobulbar blocks.
• May challenge retinal or
glaucoma surgeries

CNVM
• 5-10% of highly myopic
eyes
• 30% get fellow eye CNVM
• Prognosis better than AMD
• Anti-VEGF therapy
• Lower injection frequency
than AMD
• Risk of RD with injection
higher

MYOPIC CNVM
• Typically seen as a small, flat, greyish
membrane that may have a hyper-
pigmented border if chronic or
recurrent
• Majority of myopic CNV presents with
a “classic” pattern on FA with well
defined early hyperfluoresence
• On OCT, myopic CNV presents as a
highly reflective area contiguous
above the RPE with minimal
subretinal fluidHandbook of retinal OCT 1st ed. Duker, Waheed, and Goldman.

Handbook of retinal OCT 1st ed. Duker, Waheed, and Goldman.

MYOPIC CNVM
Risk factors
• Lacquer cracks
• Patchy atrophy
• Thinning of the
choriocapillaris/choroid
• Fellow eye with CNV (35% in 8
years)
• Note: Can occur without other
features of myopic degeneration
Treatment
• PDT – VIP initial stabilization, but
not improvement. Long-term
chorioretinal atrophy
• Laser – laser scar expansion, high
recurrence
• Surgical incision/translocation
• Anti-VEGF
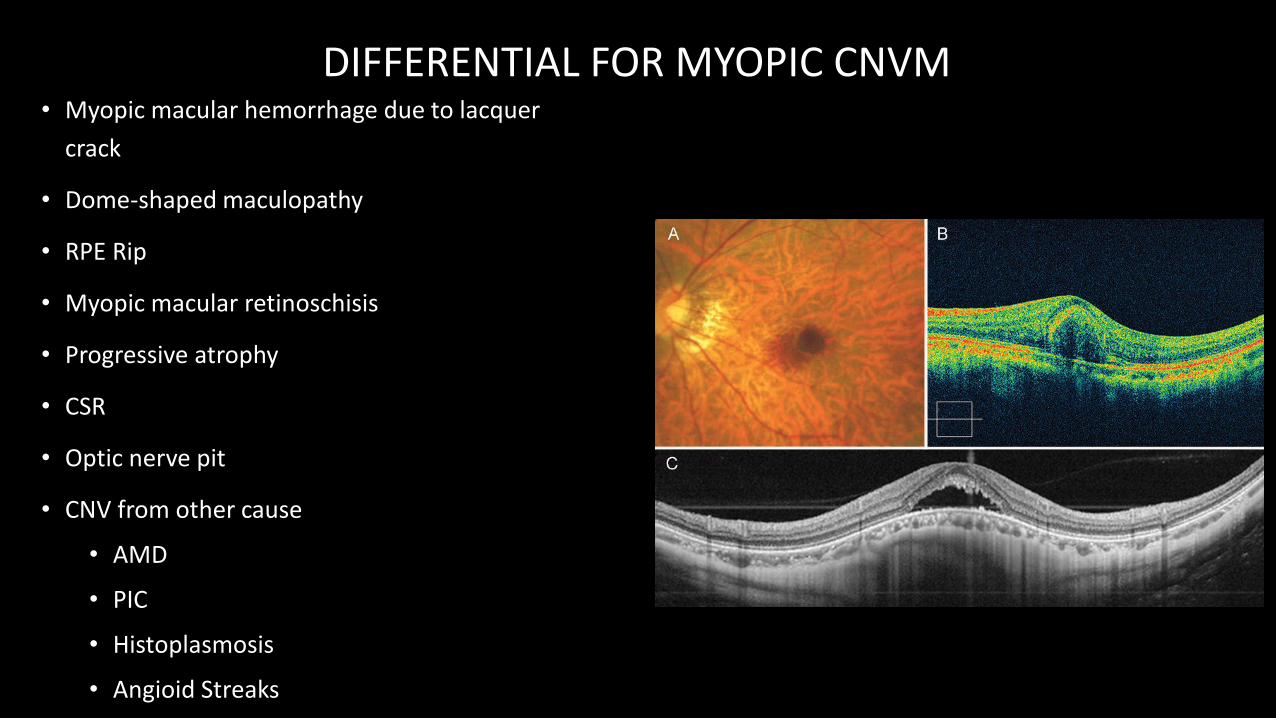
DIFFERENTIAL FOR MYOPIC CNVM• Myopic macular hemorrhage due to lacquer
crack
• Dome-shaped maculopathy
• RPE Rip
• Myopic macular retinoschisis
• Progressive atrophy
• CSR
• Optic nerve pit
• CNV from other cause
• AMD
• PIC
• Histoplasmosis
• Angioid Streaks
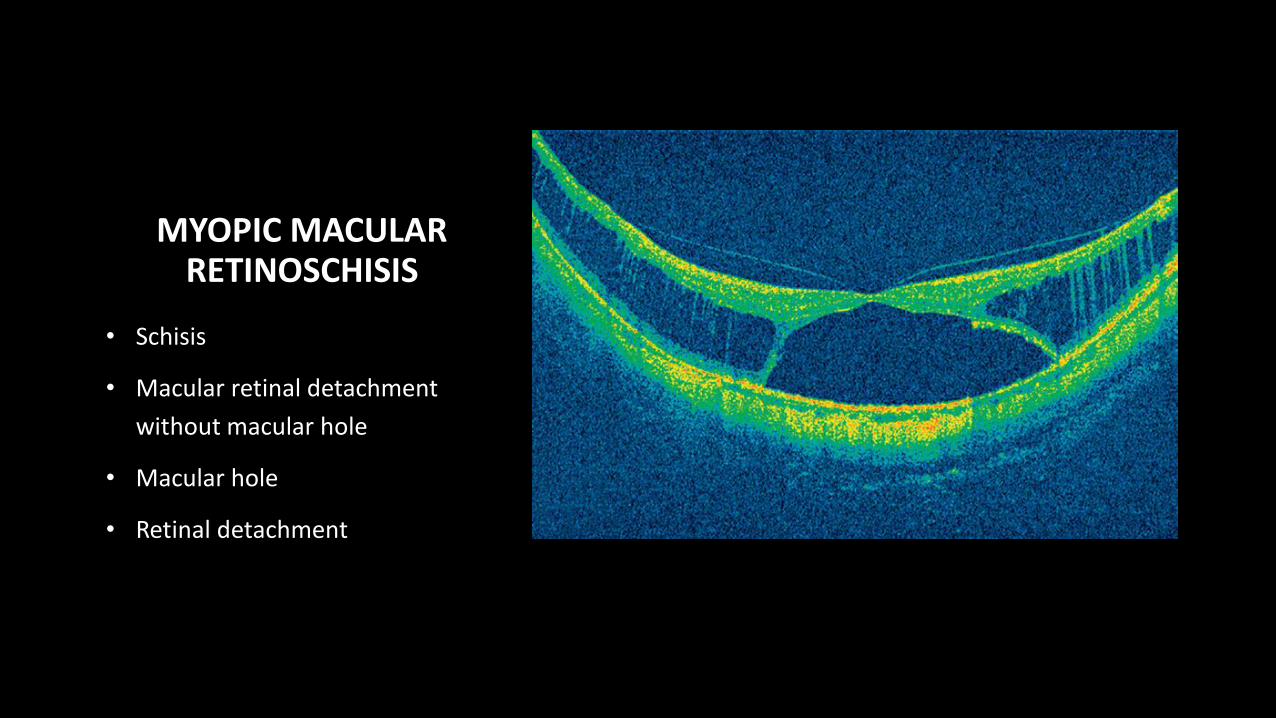
MYOPIC MACULAR RETINOSCHISIS
• Schisis
• Macular retinal detachment
without macular hole
• Macular hole
• Retinal detachment

MACULAR HOLE-ASSOCIATED DETACHMENT
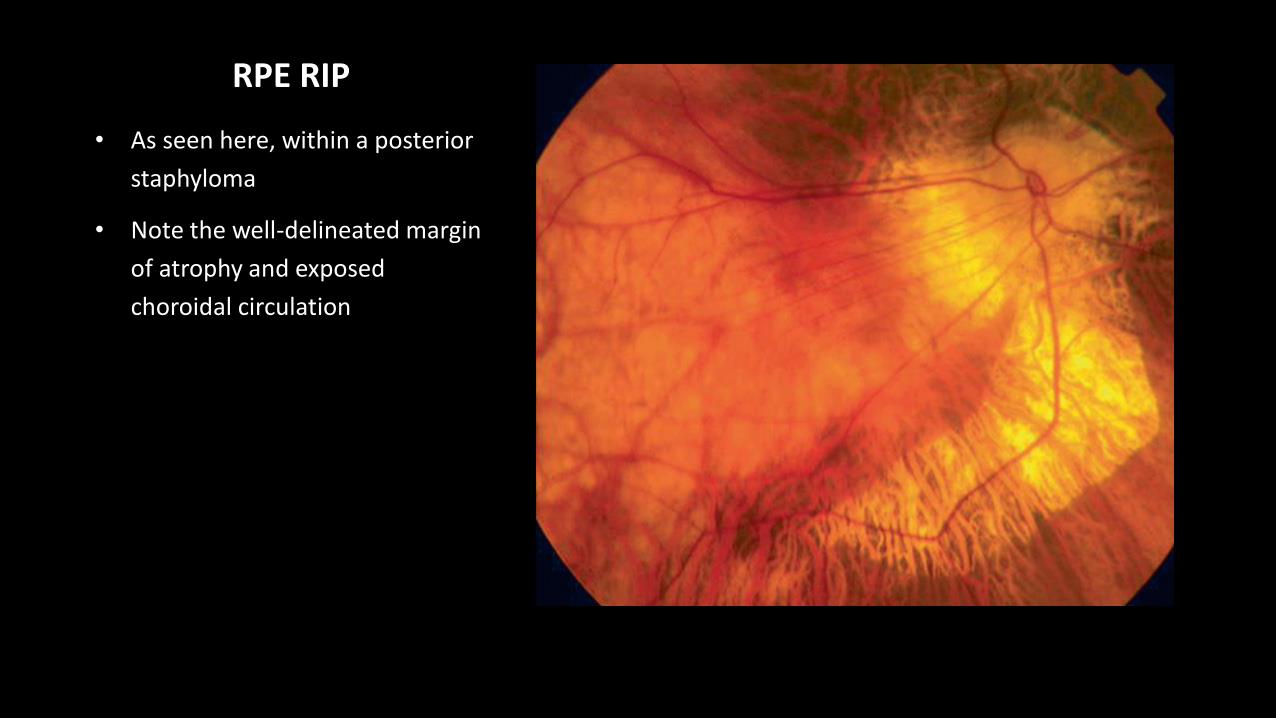
RPE RIP
• As seen here, within a posterior
staphyloma
• Note the well-delineated margin
of atrophy and exposed
choroidal circulation

• Fundus autofluorescence
demonstrates well
progressive atrophy in
pathological myopia
• The top two photographs show
the atrophy and a visual acuity
of 20/50
• Eighteen months later, there
was growth of the staphyloma
and the visual acuity dropped
to 20/100
RHEGMATOGENOUS RETINAL DETACHMENT
• Lifetime risk of RD in high myopia > 20x emmetropia
• Early PVD
• Lattice degeneration
• Asymptomatic atrophic holes
• Myopic macular holes
• Higher risk RD with cataract surgery
• 2.2% in high myopes vs 0.93% general population
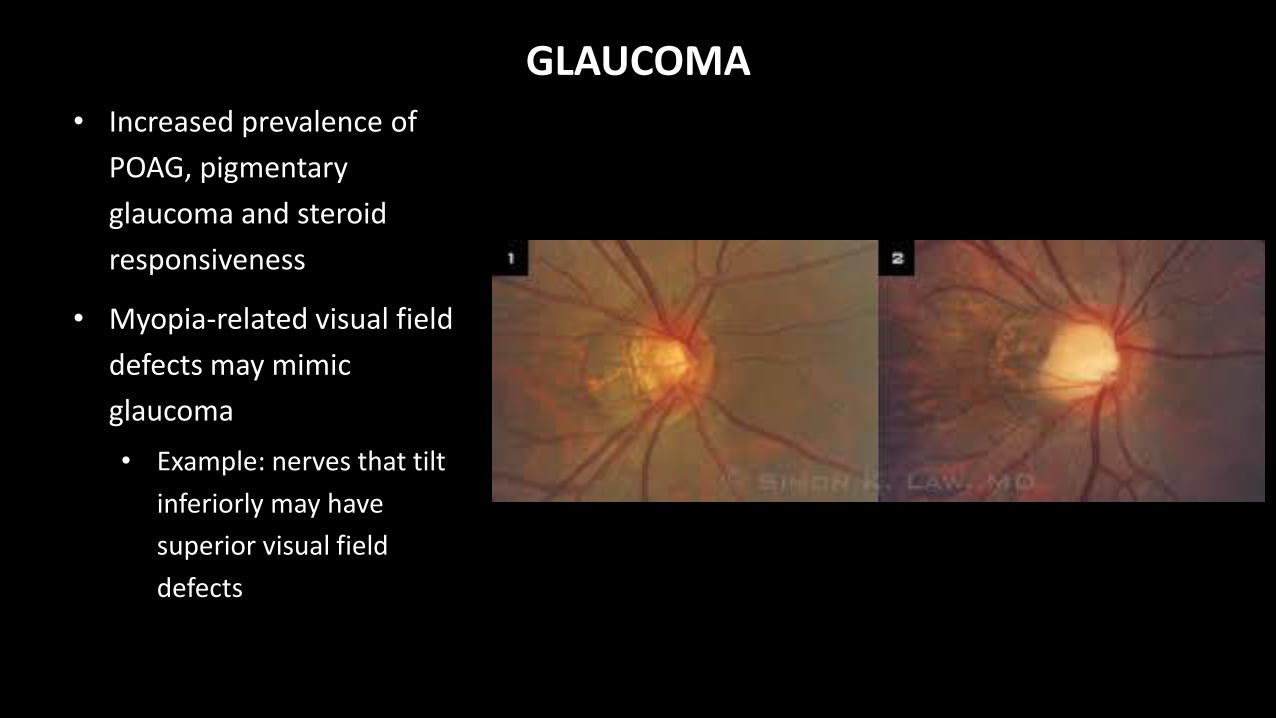
GLAUCOMA
• Increased prevalence of
POAG, pigmentary
glaucoma and steroid
responsiveness
• Myopia-related visual field
defects may mimic
glaucoma
• Example: nerves that tilt
inferiorly may have
superior visual field
defects

CASE 1
48 y/o man, asymptomatic- VA
- 20/20 OD- 20/25 OS
- MRx- -11.0 +0.50 x085 OD- -12.0 +0.50 x105 OS


→ Observe, Amsler grid

CASE 2
59 y/o woman with “missing spot” in the vision OS for past month- VA
- 20/20 OD- 20/40 OS
- MRx- -8.25 +1.25 x042 OD- -1075 +1.75 x110 OS
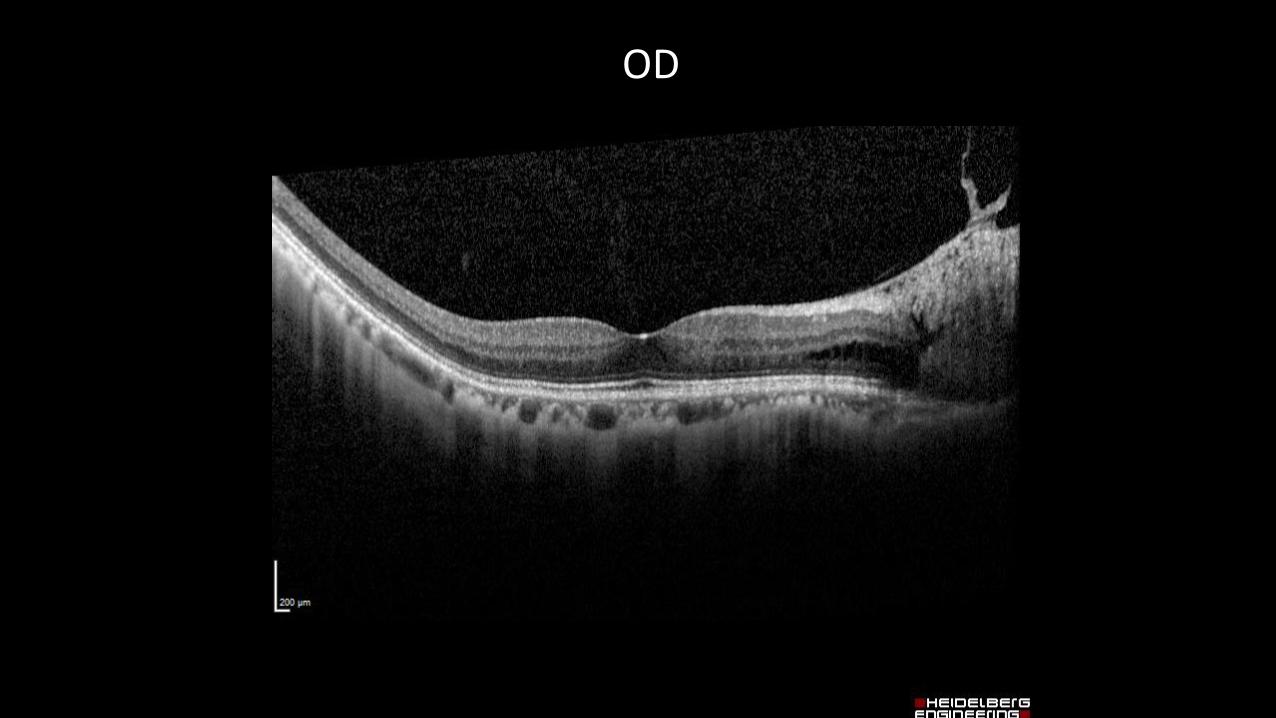
OD

OS

OS INFERIOR PARAFOVEA

OS VERTICAL LINE
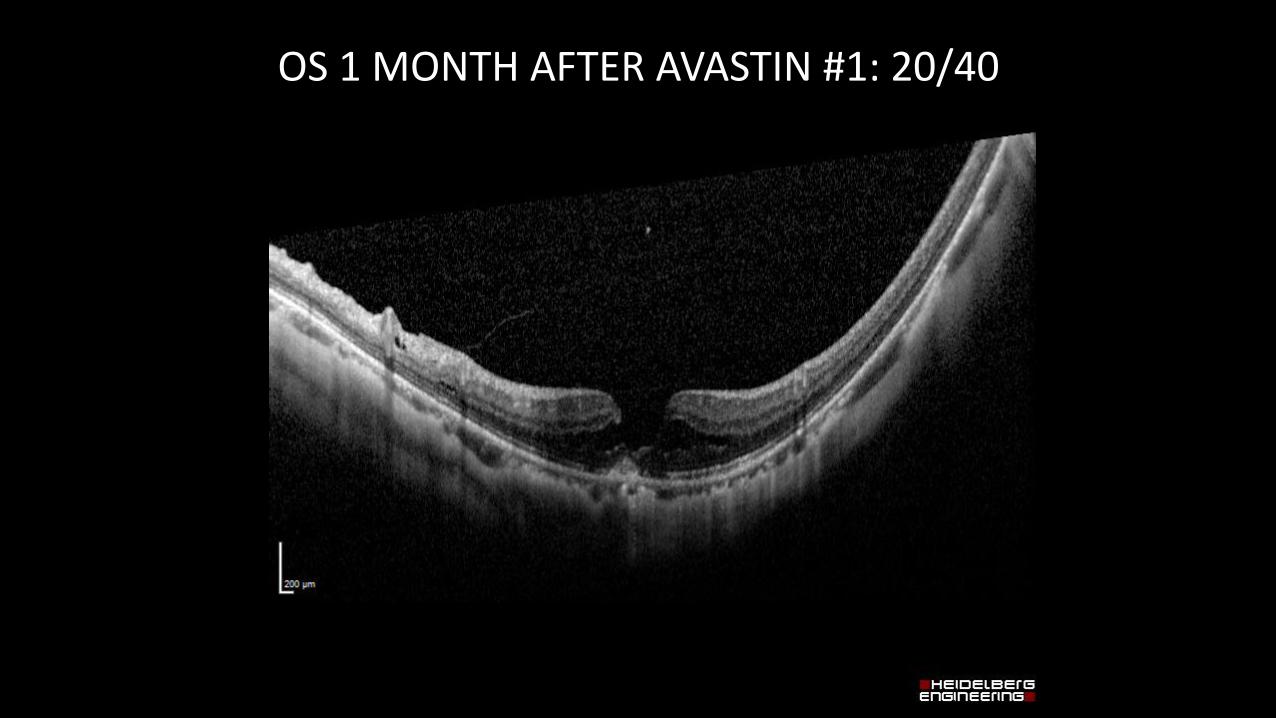
OS 1 MONTH AFTER AVASTIN #1: 20/40
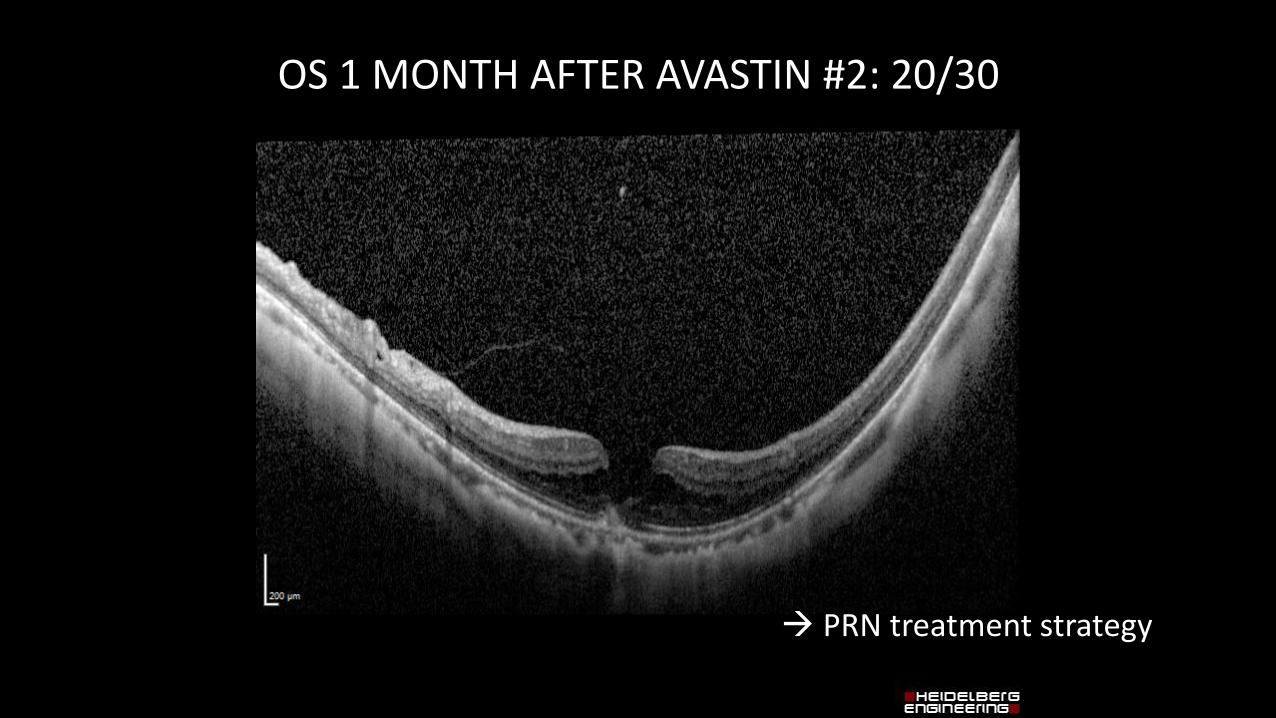
OS 1 MONTH AFTER AVASTIN #2: 20/30
→ PRN treatment strategy

THANK YOU!