normal haemostasis
TRANSCRIPT

NORMAL HEMOSTASIS
ModeratorsRespected :- Ishwar Bihana SirRespected :- Joseph SirRespected :- S.K.Bose Sir
Presented By Gaurav KumarB.sc. MLT Student Part II
Department of Haematology Post Graduate Institute of Medical Education And Research, Chandigarh

• It is a biological or physiological phenomenon which is responsible to keep the blood in fluid state in the circulation as well as to arrest bleeding followed by an injury to blood vessel.
Defination
Aims and Objective
To understand how our vascular system keep our blood in its fluid state.
To know how bleeding is arrested.
To know the role of haemostasis components.
To know the biology and mechanism of coagulation.
To know how clot is removed from vascular system.

To maintain the blood in fluid state while it remains circulating within vascular system.
To maintain the integrity of the vessels wall.
To arrest bleeding at the site of injury or blood loss by the formation of haemostatic plug.
Eventual removal of plug when healing is complete.
Importance of Hemostasis

NoPGI2
ADPase
Inhibit platelets
aggregation
TM
Thrombin
Protein CaProtein C
Destroys FVa,FVIIIa
Protein S
HSAT-III
Inhibit FXa,FIXa,thrombin
tPAplasminogen plasmin
fibrinolysis
endothelium
Overview of Hemostasis
Blood coagulation cascade
Vessel injury
NeurogenicMayogenicendothelin
vasoconstriction
Reduce blood flow
Collagen exposure+vWFTissue factor
Plt.adhen & activationserotonin
TxA2,ADP
plt.aggregation
Primary hemostatic plug
Stable 2ndry hemostatic plug
healing
fibrinolysis antiplasminogen
Cell migration & proliferation
PF
thrombin
fibrin
Blood vessels Platelets
Plasma coagulation
factorsInhibitorsFibrinolytic
system
Components of Hemostasis

Blood vesselsStructure of blood
vessels

Function of Blood Vessel Blood vessel with muscular coat help to
reduce blood loss by vasoconstriction.
Blood vessels with a pipe system transport nutrients , hormones , gases and other essential factors which are transported by blood.
Endothelial Cell Function
Normal vascular endothelium is a
thromboresistant surface.
Non-thrombogenic- don’t react with plasma or
cellular elements of the blood.
It is antithrombotic. It activates antithrombin
III.
When injured (either biologically , chemically or
mechanically) it can profoundly promote
hemostasis.

Antiplatelets Effect: Inhibition of platelet adhesion, activation and aggregation. PGI2 (Prostacyclin)-vasodilator and antiplatelet agent. NO-Nitric Oxide/PGI2 Both bind with the receptors on the platelets and inactivate them. So inhibit
platelet aggregation. ADPase: Enzymes that break down the ADP (strong proaggregating agent) released by
the platelets and thus inhibit platelet aggregation.
NoPGI2
ADPase
Inhibit platelets
aggregation
TM
Thrombin
Protein CaProtein C
Destroys FVa,FVIIIa
Protein S
HSAT-III
Inhibit Fxa,FIXa,thrombin
tPAplasminogen plasmin
fibrinolysis
Endothelial Antithrombotic Mechanism

NoPGI2
ADPase
Inhibit platelets
aggregation
TM
Thrombin
Protein CaProtein C
Destroys FVa,FVIIIa
ProteinS
HSAT-III
Inhibit Fxa,FIXa,thrombin
tPAplasminogen plasmin
fibrinolysis
Surface expressed integral membrane protein which binds thrombin & results in loss of the pro-coagulant properties of thrombin.
Thrombin/thrombomodulin complex is a potent anticoagulant complex.
Since it activates protein C to activated-Protein C.
Activated protein C down regulates coagulation by inactivating important proteins (FVa, FVIIIa)
Thrombomodulin

Heparan sulphate• Long unbranched polysaccharide expressed at the
endothelial membrane surface.• Act as a cofactor for the plasma inhibitor
antithrombin III.• Inhibits thrombin and other coagulation
factors(FIXa,FXa)
NoPGI2
ADPase
Inhibit platelets
aggregation
TM
Thrombin
Protein CaProtein C
Destroys FVa,FVIIIa
Protein S
HSAT-III
Inhibit Fxa,FIXa,thrombin
tPAplasminogen plasmin
fibrinolysis
Binding and Inhibition of Thrombin
platelet
GPIb receptor
vWF
Endothelialcell
subendothelialcollagen
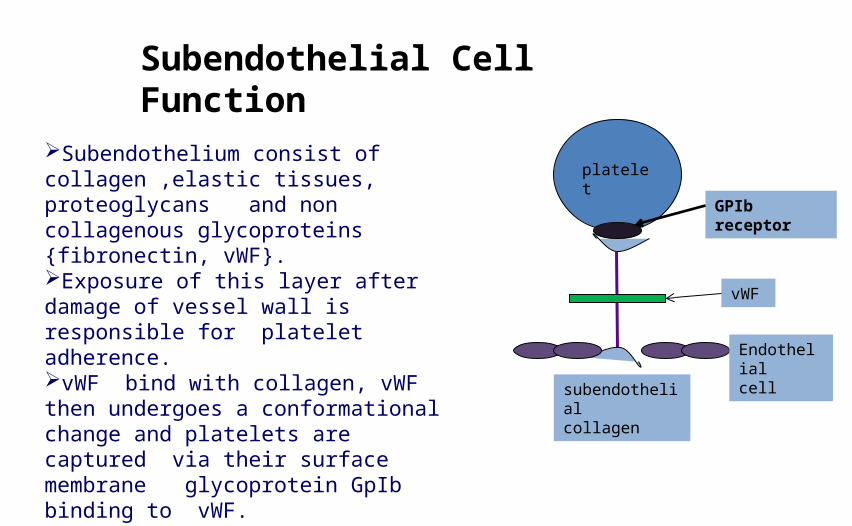
Subendothelial Cell Function
Subendothelium consist of collagen ,elastic tissues, proteoglycans and non collagenous glycoproteins {fibronectin, vWF}.Exposure of this layer after damage of vessel wall is responsible for platelet adherence.vWF bind with collagen, vWF then undergoes a conformational change and platelets are captured via their surface membrane glycoprotein GpIb binding to vWF.

The mechanism is Damage of vascular endothelium
stimulates endothelial cells
Endothelial cell Synthesize and secrete three
Substances involvedIn haemostatic plug
Formation
vWF(VIII vWF)
It help in adhesion Of platelet to
sub endothelium
PGI2
(synthesized from Arrachidonic acid
And it inhibit platelet Aggregation
PlasminogenIts release is Stimulated by
Vascular damage

April 15, 2023 15
Stages of Hemostasis
Fibrinolysis
Formation of Platelet Plug
Formation of blood clot
Vascular Constriction
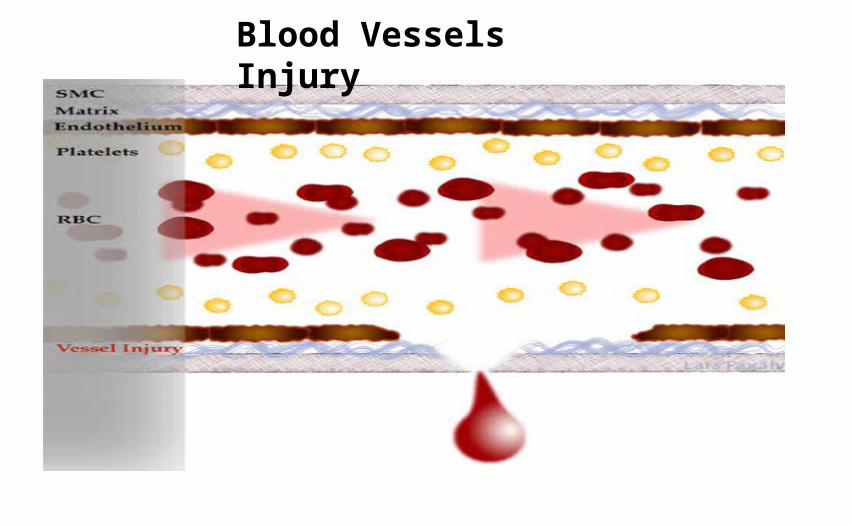
Blood Vessels Injury

Vasoconstriction Endothelial cells produce vasoconstrictors such as
angiotensin II and serotonin which help in
vasoconstriction.
Activated platelets produce thromboxane A2 (TXA2)
which is a potent vasoconstrictor.

Function of platelets
Coagulative function
Haemostatic function

Platelets membrane glycoproteins:GPIb-IX:
Constitute active receptor for vWF
Mediates vWF dependent adhesion of platelets to subendothelial
GPIIb/IIIa: On activation serve to bind
fibrinogen Mediates aggregation Also receptor for vWF, fibronectin
and thrombospondinGPIa-IIa:Constitutively active receptor for collagen.Mediates platelets adhesion independent of vWF.
Hemostatic Function

Role of Platelets in Hemostasis
With in 1-2 sec after injury to blood vessel, hemostatic process begins & proceed as out line bellow:
1. platelet adhesion2. platelets activation 3. platelets release reaction4. platelets aggregation

Platelets attach to non-platelet surfaces, such as collagen fibers in the subendothelium.
Platelets move from the blood vessels and into the tissues.
Exposure to surfaces in the tissues causes them to bind to collagen with the presence of von Willebrand factor ( vWF) and Glycoprotein IbIX, making a bridge formation.
Binding via GpI b initiates activation of platelet.
Platelets Adhesion
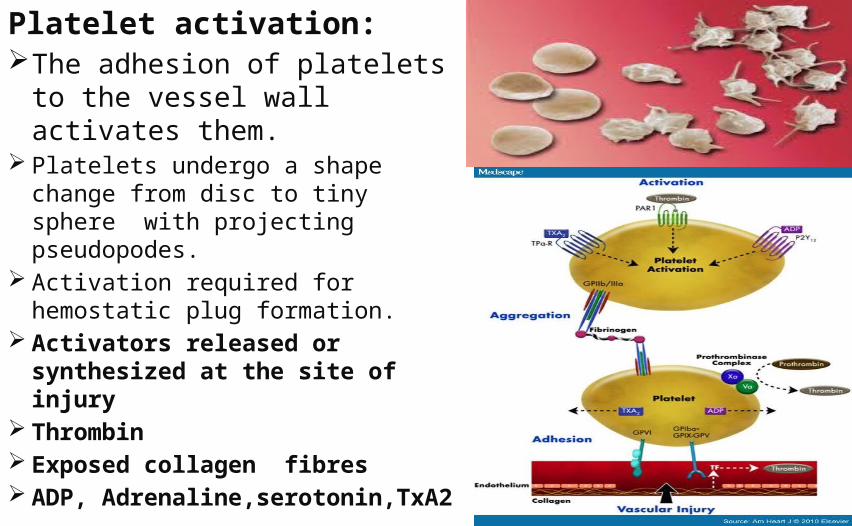
Platelet activation:The adhesion of platelets to
the vessel wall activates them.
Platelets undergo a shape change from disc to tiny sphere with projecting pseudopodes.
Activation required for hemostatic plug formation.
Activators released or synthesized at the site of injury
Thrombin Exposed collagen fibres ADP,
Adrenaline,serotonin,TxA2

Immediately after adhesion & activation process of release reaction or secretion begins.
In this process content of platelets organelles are released to the exterior.
Secretion of α granulesa) PF4b) β-Thrombomodulinc) Fibrinogend) Factor Ve) Fibronectinf) Thrombosponding) PDGFh) PAI-1
Platelets Release Reaction

Secretion of dense granules: ADP, GTP, GDP Calcium, serotonin Histamin, epinephrin
ADP released from dense granules promotes platelets aggregation.
PF-4 release from alpha granules neutralize the anticoagulant activity of heparin
PDGF – stimulate proliferation of vascular smooth muscle cell & skin fibroblast & plays a role in cut healing.
TxA2 causes shape change & stimulates release reaction from alpha & dense granules, Also induce aggregation of other platelets & local vasoconstriction

Platelet aggregation
Process by which platelets interact with one another to form a hemostatic plug.Chemical changes cause platelets to
aggregate and stick to one anotherGPIIb-IIIa complex binds vWF,
undergoes Ca++-dependent structural change, then acts as receptor for fibrinogen
Fibrinogen + activated platelets serve as a bridge between two platelets .

April 15, 2023 26
Primary haemostasis involves the binding of platelets to exposed collagen in the sub endothelium of damaged vessels.
Secondary haemostasis is the process of activation of coagulation factors leading to the production of thrombin.

Primary Hemostasis
First physiological response to vascular injury, which is mediated by platelets, in order to arrest bleedingMechanism:– Activation of platelets via stimulators such as thrombin– Adhesion of platelets to subendothelium via interaction between GPIb and von Willebrand Factor (VWF)– Release of platelet granule products in order to recruit more platelets to the injured site– Aggregation of platelets via interaction between GPIIb/IIIa (aIIb3) and fibrinogen to form the initial plug. Triggers secondary hemostasis (coagulation proteins)

• Process of blood coagulationMechanism: Coagulation proteins work in concern to generate
thrombin Thrombin converts fibrinogen to fibrin Fibrin consolidates the platelet plug made in primary
hemostasis such that a thrombus (secondary hemostatic plug) is formed
• Prevents further blood loss from the injury site
Secondary Hemostasis

April 15, 2023 29
Platelet Aggregation

INTRINSIC PATHWAY
EXTRINSIC PATHWAY
COMMON PATHWAY
Plasma Coagulation System

COAGULATION of blood take place with the help of some proteins called clotting factors present in plasma.
Clotting factor act as zymogens and under the influence of enzyme are themselves converted into active enzymes
Role of Clotting Factors

Coagulation factors in the form of zymogens precursors.• Ca++ as a co-factor and organizing surface,
Provided by platelets in vivo Provided by a phospholipids
emulsion in vitro
The coagulation process is initiated when tissue factor - bearing cells are exposed to blood at a site of injury.
Requirements for Coagulation

FX FXaCa++
PLFVIIIa
Prekallinokerin kallinokerin
FXII FXIIa
FXI FXIa
FIX FIXaCa++
FVIIa
FVIIa
Ca++
Intrinsic pathwayExpose collagen
Tissue factor
FVIIFVIIa
Extrinsic pathway
Prothrombin Thrombin
Fibrinogen Fibrin monomer
Cross linked Fibrin clotFXIII FXIIIa
Ca++
PLFVa
Ca++
FIIa
Common pathway

Fibrinolytic system keep the vascular system free of deposited fibrin clots.
Essential purpose of fibrinolysis is to digest and solublize the fibrin, thus restoring potency to occluded vessel.
Fibrinolytic system

Plasminogen activatorPlasminogen and plasmin Inhibitors of fibrinolysis:
AntiactivatorsAntiplasmins
COMPONENTS OF FIBRINOLYTIC SYSTEM

FIBRINOLYTIC PATHWAY
It involves-conversion of plasminogen to
plasmin
Plasmin break down the fibrinogen or fibrin in their degradation products

Conversion of Plasminogen To Plasmin
Plasminogen

Fibrinogen degradation product
• Plasmin initially attacks alpha chain of the fibrinogen molecule & removes small fragments designed as A,B & C from the C terminal of the Aα chains.
• Followed by degradation of Bβ chains with removal of first 42 amino acids.
• Lead to the formation of a large fragment X that still remains fibrinopeptide A.
• Next cleavage involves all the three chains in an asymmetrical manner with the release of fragment Y & D.
• Fragment Y is rapidly degraded by plasmin liberating two D&E.

Fibrin Degradation ProductDegradation of cross linked fibrin is different from fibrinogen.The fibrin degradation products are different because of the presence of covalant bonding.Thus the characteristic fragments are oligomers of X and Y D-dimer. D-E complex and Y-D complex.Fibrin degradation is slower due to the presence of crosslinkages.Normally the FDPs are cleared from the circulation by macrophages.

INHIBITORSInhibitors of Serine Proteases
Antithrombin
Inhibitor of coagulation having antithrombin activities
Types:
Antithrombin I
Show thrombin adsorbing effect of fibrin
Antithrombin II
Act jointly with heparin act as heparin cofactor
Antithrombin III(alpha 2 glycoprotein)
Antithrombin is a serin protein inhibitor that degrades the serine proteases: thrombin, FIXa, FXa, FXIa, and FXIIa. It is constantly active, but its adhesion to these factors is increased by the presence of heparan sulfate.

Other Inhibitors of Coagulation
α2 macroglobulin – It act as antithrombin, antiplasmin
and inactivate kallikrein.
α2 antitrypsin ( alpha globulin) – Inhibitor of factor
XIa and antiplasmin and is weakly antithrombin.
α2 antiplasmin – Inactivate plasmin.
Heparin – inhibit the action of thrombin.
delay the interaction of thrombin and fibrinogen.

Protein C:• It is a vitamin K dependent glycoprotein synthesized in the liver.• Protein circulate as an inert zymogen and is activated by
thrombin in the presence of thrombomodulin on the surface of vascular endothelial cell.
• Protein C proteolytic destruction of activated FV & FVIII.Protein S :• It is also vitamin k dependent protein.• Act as a cofactor in protein C reaction and enhance the action of
protein CTissue Factor Pathway Inhibitor(TFPI):• (TFPI) limits the action of tissue factor (TF). It also inhibits
excessive TF-mediated activation of FIX and FX.
INHIBITION OF COAGULATION CO FACTORS

• Endothelial cell produced Nitric oxide, PGI2 and ADPase.
• They act as a antiplatelets agents (inactivate the platelets receptor by binding with them)
• ADP produced by platelets is favour to bind with endothelial cell but ADPase inactivate or digest ADP.
• Healthy endothelium does not tolerate the presence of activated coagulation factor.
• When anti thrombin III binds with heparan sulfate. AT-III is activated & cut down the thromin molecules & some activated coagulation factors ( FIXa, Fxa)
SUMMARY
How blood is kept in fluid state in circulation ????

Normally thrombin helps in coagulation but when binds with thrombomodulin (TM) it modulate the function of thrombin which activate the protein C.
Activated protein C digest the activated FVa & FVIIIa. Endothelial cells not only prevent the platelets
aggregation but also inhibit the proteins that involve coagulation.
Endothelial cells also produce tissue plasminogen activator(tPA) which activate the plasminogen to plasmin
Plasmin cleaves fibrin strand in to the FDPs. FDPs are removed from the circulation by macrophages
and some eosinophill. By this entire process blood is kept in fluid state .

• When the blood vessels are injured mechanically, chemically & physically the first step is vasoconstriction.
• After the vasoconstriction platelets are adhere to the endothelial cell membrane. And under goes activation, release reaction and aggregation.
• Which forms the primary hemostatic plug and stop the blood leakage from injured site.
• Simultaneously activate the coagulation cascade. (extrinsic pathway, intrinsic pathway and common pathway) and
forms the fibrin mesh in the clot which establish the plug and form secondary hemostasic plug
Which is stable and irreversible. So that bleeding is arrested permanently.
How bleeding is arrested???

Essential haematology: A. V. Hoffbrand, P. A. H. Moss, J. E. Pettit - 2006 - 380 pages Hemostasis and thrombosis: basic principles and clinical practice - Page 1569 Robert W. Colman - 2006 - 1827 pagesClinical laboratory medicine: Volume 2001 - Page 987 Kenneth D. McClatchey - 2002 - 1693 pagesConsultative hemostasis and thrombosis - Page xxi Craig S. Kitchens, Barbara M. Alving, Craig M. Kessler - 2002 - 617 pageHemostasis and thrombosis protocols: Volume 489 - Page 3 David J. Perry, K. John Pasi - 1999 - 368 pagesRodak, BF, Fritsma, GA & Doig, K (2008). Hematology Clinical Principles & Applications. Saunders Elsevier. Chapters 40 & 45.McKenzie, Shirlyn B (2004). Clinical Laboratory Hematology. Pearson Prentice Hall. Chapter 35Beckman Coulter Webinars: Fundamentals of Hemostasis at URL http://www.beckmancoulter.com/LARS/personnel/webinars.asp Hemostasis Basics: Programmed Learner Part I (Provided by Siemens Healthcare Diagnostics Hemostasis Technical Services at URL http://www.dadebehring.com/education/hemostasis/tutorial.htm
References
