nhs r&d hta programme hta · 2012-10-07 · the assumptions made for the model were used to...
TRANSCRIPT
Article
A systematic review of repetitive task training with modelling of resource use, costs and effectiveness
French, Beverley, Leathley, Michael John, Sutton, Chris J, McAdam, Joanna, Thomas, Lois Helene, Forster, A, Langhorne, P, Price, C, Walker, A and Watkins, Caroline Leigh
Available at http://clok.uclan.ac.uk/4764/
French, Beverley, Leathley, Michael John, Sutton, Chris J ORCID: 0000000264061318, McAdam, Joanna ORCID: 0000000189637240, Thomas, Lois Helene ORCID: 0000000152186546, Forster, A, Langhorne, P, Price, C, Walker, A et al (2008) A systematic review of repetitive task training with modelling of resource use, costs and effectiveness. Health Technology Assessment, 12 (30). pp. 1117. ISSN 13665278
It is advisable to refer to the publisher’s version if you intend to cite from the work.http://dx.doi.org/10.3310/hta12300
For more information about UCLan’s research in this area go to http://www.uclan.ac.uk/researchgroups/ and search for <name of research Group>.
For information about Research generally at UCLan please go to http://www.uclan.ac.uk/research/
All outputs in CLoK are protected by Intellectual Property Rights law, includingCopyright law. Copyright, IPR and Moral Rights for the works on this site are retained by the individual authors and/or other copyright owners. Terms and conditions for use of this material are defined in the http://clok.uclan.ac.uk/policies/
CLoKCentral Lancashire online Knowledgewww.clok.uclan.ac.uk

A systematic review of repetitive functional task practice with modellingof resource use, costs and effectiveness
B French, M Leathley, C Sutton, J McAdam,L Thomas, A Forster, P Langhorne, C Price,A Walker and C Watkins
Health Technology Assessment 2008; Vol. 12: No. 30
HTAHealth Technology AssessmentNHS R&D HTA Programmewww.hta.ac.uk
The National Coordinating Centre for Health Technology Assessment,Alpha House, Enterprise RoadSouthampton Science ParkChilworthSouthampton SO16 7NS, UK.Fax: +44 (0) 23 8059 5639 Email: [email protected]://www.hta.ac.uk ISSN 1366-5278
FeedbackThe HTA Programme and the authors would like to know
your views about this report.
The Correspondence Page on the HTA website(http://www.hta.ac.uk) is a convenient way to publish
your comments. If you prefer, you can send your comments to the address below, telling us whether you would like
us to transfer them to the website.
We look forward to hearing from you.
August 2008
Health Technology Assessm
ent 2008;Vol. 12: No. 30
Repetitive functional task practice

How to obtain copies of this and other HTA Programme reports.An electronic version of this publication, in Adobe Acrobat format, is available for downloading free ofcharge for personal use from the HTA website (http://www.hta.ac.uk). A fully searchable CD-ROM isalso available (see below).
Printed copies of HTA monographs cost £20 each (post and packing free in the UK) to both public andprivate sector purchasers from our Despatch Agents.
Non-UK purchasers will have to pay a small fee for post and packing. For European countries the cost is£2 per monograph and for the rest of the world £3 per monograph.
You can order HTA monographs from our Despatch Agents:
– fax (with credit card or official purchase order) – post (with credit card or official purchase order or cheque)– phone during office hours (credit card only).
Additionally the HTA website allows you either to pay securely by credit card or to print out yourorder and then post or fax it.
Contact details are as follows:HTA Despatch Email: [email protected]/o Direct Mail Works Ltd Tel: 02392 492 0004 Oakwood Business Centre Fax: 02392 478 555Downley, HAVANT PO9 2NP, UK Fax from outside the UK: +44 2392 478 555
NHS libraries can subscribe free of charge. Public libraries can subscribe at a very reduced cost of £100 for each volume (normally comprising 30–40 titles). The commercial subscription rate is £300 per volume. Please see our website for details. Subscriptions can only be purchased for the current orforthcoming volume.
Payment methods
Paying by chequeIf you pay by cheque, the cheque must be in pounds sterling, made payable to Direct Mail Works Ltdand drawn on a bank with a UK address.
Paying by credit cardThe following cards are accepted by phone, fax, post or via the website ordering pages: Delta, Eurocard,Mastercard, Solo, Switch and Visa. We advise against sending credit card details in a plain email.
Paying by official purchase orderYou can post or fax these, but they must be from public bodies (i.e. NHS or universities) within the UK.We cannot at present accept purchase orders from commercial companies or from outside the UK.
How do I get a copy of HTA on CD?
Please use the form on the HTA website (www.hta.ac.uk/htacd.htm). Or contact Direct Mail Works (seecontact details above) by email, post, fax or phone. HTA on CD is currently free of charge worldwide.
The website also provides information about the HTA Programme and lists the membership of the variouscommittees.
HTA
A systematic review of repetitivefunctional task practice with modellingof resource use, costs and effectiveness
B French,1 M Leathley,1 C Sutton,1 J McAdam,1
L Thomas,1 A Forster,2 P Langhorne,3 C Price,4
A Walker3 and C Watkins1*
1 University of Central Lancashire, Preston, UK2 University of Leeds, UK3 Faculty of Medicine, University of Glasgow, UK4 Northumbria Healthcare NHS Trust, Newcastle University,
Newcastle upon Tyne, UK
* Corresponding author
Declared competing interests of authors: none
Published August 2008
This report should be referenced as follows:
French B, Leathley M, Sutton C, McAdam J, Thomas L, Forster A, et al. A systematicreview of repetitive functional task practice with modelling of resource use, costs andeffectiveness. Health Technol Assess 2008;12(30).
Health Technology Assessment is indexed and abstracted in Index Medicus/MEDLINE,Excerpta Medica/EMBASE and Science Citation Index Expanded (SciSearch®) and Current Contents®/Clinical Medicine.

NIHR Health Technology Assessment Programme
The Health Technology Assessment (HTA) Programme, part of the National Institute for HealthResearch (NIHR), was set up in 1993. It produces high-quality research information on the
effectiveness, costs and broader impact of health technologies for those who use, manage and providecare in the NHS. ‘Health technologies’ are broadly defined as all interventions used to promote health,prevent and treat disease, and improve rehabilitation and long-term care.The research findings from the HTA Programme directly influence decision-making bodies such as theNational Institute for Health and Clinical Excellence (NICE) and the National Screening Committee(NSC). HTA findings also help to improve the quality of clinical practice in the NHS indirectly in thatthey form a key component of the ‘National Knowledge Service’.The HTA Programme is needs-led in that it fills gaps in the evidence needed by the NHS. There arethree routes to the start of projects. First is the commissioned route. Suggestions for research are actively sought from people working in theNHS, the public and consumer groups and professional bodies such as royal colleges and NHS trusts.These suggestions are carefully prioritised by panels of independent experts (including NHS serviceusers). The HTA Programme then commissions the research by competitive tender. Secondly, the HTA Programme provides grants for clinical trials for researchers who identify researchquestions. These are assessed for importance to patients and the NHS, and scientific rigour.Thirdly, through its Technology Assessment Report (TAR) call-off contract, the HTA Programmecommissions bespoke reports, principally for NICE, but also for other policy-makers. TARs bring together evidence on the value of specific technologies.Some HTA research projects, including TARs, may take only months, others need several years. They cancost from as little as £40,000 to over £1 million, and may involve synthesising existing evidence,undertaking a trial, or other research collecting new data to answer a research problem.The final reports from HTA projects are peer-reviewed by a number of independent expert refereesbefore publication in the widely read journal series Health Technology Assessment.
Criteria for inclusion in the HTA journal seriesReports are published in the HTA journal series if (1) they have resulted from work for the HTAProgramme, and (2) they are of a sufficiently high scientific quality as assessed by the referees and editors.Reviews in Health Technology Assessment are termed ‘systematic’ when the account of the search,appraisal and synthesis methods (to minimise biases and random errors) would, in theory, permit thereplication of the review by others.
The research reported in this issue of the journal was commissioned by the HTA Programme as projectnumber 05/17/04. The contractual start date was in November 2005. The draft report began editorialreview in February 2007 and was accepted for publication in February 2008. As the funder, by devising acommissioning brief, the HTA Programme specified the research question and study design. The authorshave been wholly responsible for all data collection, analysis and interpretation, and for writing up theirwork. The HTA editors and publisher have tried to ensure the accuracy of the authors’ report and wouldlike to thank the referees for their constructive comments on the draft document. However, they do notaccept liability for damages or losses arising from material published in this report.The views expressed in this publication are those of the authors and not necessarily those of the HTA Programme or the Department of Health.
Editor-in-Chief: Professor Tom WalleySeries Editors: Dr Aileen Clarke, Dr Peter Davidson, Dr Chris Hyde,
Dr John Powell, Dr Rob Riemsma and Professor Ken SteinProgramme Managers: Sarah Llewellyn Lloyd, Stephen Lemon, Kate Rodger,
Stephanie Russell and Pauline Swinburne
ISSN 1366-5278
© Queen’s Printer and Controller of HMSO 2008This monograph may be freely reproduced for the purposes of private research and study and may be included in professional journals providedthat suitable acknowledgement is made and the reproduction is not associated with any form of advertising.Applications for commercial reproduction should be addressed to: NCCHTA, Alpha House, Enterprise Road, Southampton Science Park,Chilworth, Southampton SO16 7NS, UK.Published by Gray Publishing, Tunbridge Wells, Kent, on behalf of NCCHTA.Printed on acid-free paper in the UK by St Edmundsbury Press Ltd, Bury St Edmunds, Suffolk. G

Objectives: To determine whether repetitivefunctional task practice (RFTP) after stroke improveslimb-specific or global function or activities of dailyliving and whether treatment effects are dependent onthe amount of practice, or the type or timing of theintervention. Also to provide estimates of the cost-effectiveness of RFTP.Data sources: The main electronic databases weresearched from inception to week 4, September 2006.Searches were also carried out on non-English-languagedatabases and for unpublished trials up to May 2006. Review methods: Standard quantitative methodswere used to conduct the systematic review. Themeasures of efficacy of RFTP from the data synthesiswere used to inform an economic model. The modelused a pre-existing data set and tested the potentialimpact of RFTP on cost. An incremental cost perquality-adjusted life-year (QALY) gained for RFTP wasestimated from the model. Sensitivity analyses aroundthe assumptions made for the model were used to testthe robustness of the estimates.Results: Thirty-one trials with 34 intervention–controlpairs and 1078 participants were included. Overall, itwas found that some forms of RFTP resulted inimprovement in global function, and in both arm andlower limb function. Overall standardised meandifference in data suitable for pooling was 0.38 [95%confidence interval (CI) 0.09 to 0.68] for global motorfunction, 0.24 (95% CI 0.06 to 0.42) for arm functionand 0.28 (95% confidence interval 0.05 to 0.51) forfunctional ambulation. Results suggest that training maybe sufficient to have an impact on activities of dailyliving. Retention effects of training persist for up to
6 months, but whether they persist beyond this isunclear. There was little or no evidence that treatmenteffects overall were modified by time since stroke ordosage of task practice, but results for upper limbfunction were modified by type of intervention. Theeconomic modelling suggested that RFTP was cost-effective. Given a threshold for cost-effectivenessof £20,000 per QALY gained, RFTP is cost-effective so long as the net cost per patient is less than £1963.This result showed some sensitivity to the assumptionsmade for the model. The cost-effectiveness of RFTPtends to stem from the relatively modest costassociated with this intervention. Conclusions: The evidence suggests that some form of RFTP can be effective in improving lower limbfunction at any time after stroke, but that the durationof intervention effect is unclear. There is as yetinsufficient good-quality evidence to make any firmrecommendations for upper limb interventions. If task-specific training is used, adverse effects should bemonitored. While the effectiveness of RFTP is relativelymodest, this sort of intervention appears to be cost-effective. Owing to the large number of ongoing trials,this review should be updated within 2 years and anyfuture review should include a comparison againstalternative treatments. Further research shouldevaluate RFTP upper limb interventions and inparticular constraint-induced movement therapy,address practical ways of delivering RFTP interventions,be directed towards the evaluation of suitable methodsto maintain functional gain, and be powered to detectwhether RFTP interventions are cost-effective.
Health Technology Assessment 2008; Vol. 12: No. 30
iii
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Abstract
A systematic review of repetitive functional task practice withmodelling of resource use, costs and effectiveness
B French,1 M Leathley,1 C Sutton,1 J McAdam,1 L Thomas,1 A Forster,2
P Langhorne,3 C Price,4 A Walker3 and C Watkins1*
1 University of Central Lancashire, Preston, UK2 University of Leeds, UK3 Faculty of Medicine, University of Glasgow, UK4 Northumbria Healthcare NHS Trust, Newcastle University, Newcastle upon Tyne, UK* Corresponding author

Health Technology Assessment 2008; Vol. 12: No. 30
v
List of abbreviations .................................. vii
Executive summary .................................... ix
1 Introduction ............................................... 1Description of the condition ...................... 1Description of the intervention ................. 1Scope of the review .................................... 1Scope of the cost-effectiveness analysis ...... 2Objectives ................................................... 2
2 Review methods ......................................... 3Search strategy for identification of studies 3Inclusion criteria ........................................ 4Exclusion criteria ....................................... 5Types of outcome measure ......................... 5Data extraction and assessment of studyvalidity ........................................................ 6
3 Description of studies ................................ 9Description of studies ................................ 10Included studies ......................................... 10Participants ................................................. 11Interventions .............................................. 11Comparison interventions ......................... 13Primary outcomes ...................................... 14Secondary outcomes ................................... 14Excluded studies ........................................ 15Ongoing studies ......................................... 15Studies not assessed at report completion ................................................. 15Quality of included studies ........................ 15
4 Results of the review ................................. 19Primary outcomes ...................................... 19Secondary outcomes ................................... 42
5 Economic analysis ...................................... 45Background ................................................ 45Methods ...................................................... 45Results ........................................................ 47
6 Discussion ................................................... 51Summary of main results ........................... 51Overall completeness and applicability ofevidence ...................................................... 52Quality of evidence .................................... 54Potential limitations in the review process ........................................................ 55
Agreement or disagreement with previousreviews ........................................................ 55Economic analysis ...................................... 56
7 Conclusions ................................................ 59Implications for practice ............................ 59Recommendations for future research ....... 59
Acknowledgements .................................... 61
References .................................................. 63
Appendix 1 Included studies: repetitive task training ............................................... 71
Appendix 2 Included studies: constraint-induced movement therapy ....................... 87
Appendix 3 Included studies: treadmilltraining ....................................................... 99
Appendix 4 Characteristics of excluded studies ......................................................... 107
Appendix 5 Characteristics of ongoing studies ......................................................... 109
Appendix 6 Criteria for subgroup analyses ....................................................... 111
Appendix 7 Summary of baselinecharacteristics of patients from the cohort in the patient data set who survived to 3 years ........................................................ 113
Appendix 8 Numbers of patients and costs in the baseline and new groups ......... 115
Appendix 9 Cost-effectiveness at 3 years per QALY gained for RFTP on outcomemeasures that were significant in the systematic review ........................................ 117
Health Technology Assessment reportspublished to date ....................................... 119
Health Technology Assessment Programme ................................................ 137
Contents

ADL activity of daily living
ARAT Action Research Arm Test
BBT Box and Block Test
BI Barthel Index
CI confidence interval
CIMT constraint-induced movementtherapy
df degrees of freedom
EQ-5D EuroQol-5 Dimensions
FAC Functional Ambulation Classification
FIM Functional Independence Measure
FM Fugl–Meyer Assessment
FTHUE Functional Test of the HemipareticUpper Extremity
9HPT Nine Hole Peg Test
10HPT Ten Hole Peg Test
ICER incremental cost-effectiveness ratio
IQR interquartile range
MAL Motor Activity Log
MAS Motor Assessment Scale
mCIMT modified constraint-inducedmovement therapy
5MWS Five Metre Walk Speed
6MWS Six Metre Walk Speed
6MWT Six Minute Walk Test
10MWS Ten Metre Walk Speed
NHP Nottingham Health Profile
PSS Personal Social Services
QALY quality-adjusted life-year
RCT randomised controlled trial
RFTP repetitive functional task practice
RMA Rivermead Motor Assessment
RTT repetitive task training
SD standard deviation
SMD standardised mean difference
SMES Sodring Motor Evaluation Scale
TEMPA Test Evaluant des MembresSuperieurs des Personnes Agées
TM treadmill training
TUG Timed Up and Go
WMD weighted mean difference
WMFT Wolf Motor Function Test
Health Technology Assessment 2008; Vol. 12: No. 30
vii
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
List of abbreviations
All abbreviations that have been used in this report are listed here unless the abbreviation is well known (e.g. NHS), or it has been used only once, or it is a non-standard abbreviation used only in figures/tables/appendices in which case the abbreviation is defined in the figure legend or at the end of the table.


Health Technology Assessment 2008; Vol. 12: No. 30
ix
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
BackgroundThe repetitive practice of functional tasks is acomponent of current approaches to strokerehabilitation. Practice may be augmented bystrategies to enhance learning as used inmovement science approaches, by mechanicalmeans such as treadmills, or by strategies toencourage use of the affected limb in daily life byrestraining the unaffected limb.
All these approaches have a core mechanism basedon the repeated practice of functional tasks. Thishas the potential to be a resource-efficientcomponent of stroke rehabilitation, includingdelivery in a group setting, or instructed practicein the home environment. This review considersthe effectiveness and cost-effectiveness of all formsof repetitive functional task practice (RFTP).
ObjectivesThe aims of this study were:
● to determine whether RFTP after strokeimproves limb-specific or global function oractivities of daily living
● to determine whether treatment effects aredependent on the amount of practice, or thetype or timing of the intervention
● to provide cost-effectiveness estimates for RFTP.
MethodsData sourcesThe following searches were undertaken:
● electronic searches of Cochrane Stroke TrialsRegister, the Cochrane Library, MEDLINE,EMBASE, CINAHL, AMED, SportDiscus, ISIScience Citation Index, Index to Theses,ZETOC, PEDro and OT Seeker (all frominception to week 4, September 2006)
● electronic searches on non-English-languagedatabases and for unpublished trials onMetaRegister, BioMed Central, CRISP,Centerwatch, National Research Register,ReFeR, Stroke Trials Directory, REHABDATAand CIRRIE (to May 2006)
● searches of conference proceedings, referencelists of existing systematic reviews, citationsearching, publication on bulletin boards andauthor contact for all relevant trials.
Study selectionThe review included randomised and quasi-randomised trials in adults after stroke, whichincluded an intervention where an active motorsequence was performed repetitively within asingle training session, where the practice aimedtowards a clear functional goal and where theamount of task practice could be quantified.Studies using mechanical or behavioural strategiesto facilitate or encourage functional task practicewere also included. Primary outcomes includedlimb-specific or global functional measures.Secondary outcomes included measures ofactivities of daily living and adverse events.
Data extractionTwo reviewers independently screened titles andabstracts, extracted data and critically appraisedthe trials. Assessment of methodological qualitywas undertaken for allocation concealment,blinding, loss to follow-up, trial size andequivalence of treatment. Trialists were contactedfor additional information.
Data synthesisStandard Cochrane quantitative systematic review methods were used. A fixed-effect modelwas used, and results were expressed as weighted or standardised mean differences, with 95% confidence interval. Subgroup analyses were conducted for amount, timing and type of intervention, and for adequacy of allocation concealment, type of comparisongroup, equivalence of therapy time and trial size.
The measures of efficacy of RFTP from the datasynthesis were used to inform an economic model.The model used a pre-existing data set and testedthe potential impact of RFTP on cost. From themodel an incremental cost per quality-adjustedlife-year (QALY) gained for RFTP was estimated.Sensitivity analyses around the assumptions madefor the model were used to test the robustness ofthe estimates.
Executive summary

x
ResultsThirty-one trials with 34 intervention–controlpairs and 1078 participants were included.Overall, it was found that some forms of RFTPresulted in improvement in global function, andin both arm and lower limb function. Overallstandardised mean difference in data suitablefor pooling was 0.38 [95% confidence interval(CI) 0.09 to 0.68] for global motor function,0.24 (95% CI 0.06 to 0.42) for arm functionand 0.28 (95% confidence interval 0.05 to 0.51)for functional ambulation. Results suggest thattraining may be sufficient to have an impact onactivities of daily living. Retention effects oftraining persist for up to 6 months, but whetherthey persist beyond this is unclear. There waslittle or no evidence that treatment effectsoverall were modified by time since stroke ordosage of task practice, but results for upperlimb function were modified by type ofintervention. The economic modellingsuggested that RFTP was cost-effective. Given athreshold for cost-effectiveness of £20,000 perQALY gained, RFTP is cost-effective so long asthe net cost per patient is less than £1963. Thisresult showed some sensitivity to theassumptions made for the model. The cost-effectiveness of RFTP tends to stem from therelatively modest cost associated with thisintervention.
ConclusionsImplications for practiceThe evidence suggests that some form of RFTPcan be effective in improving lower limb functionat any time after stroke, but that the duration ofintervention effect is unclear. There is as yetinsufficient good-quality evidence to make anyfirm recommendations for upper limbinterventions. If task-specific training is used,adverse effects should be monitored. While theeffectiveness of RFTP is relatively modest, this sortof intervention appears to be cost-effective.
Recommendations for future researchOwing to the large number of ongoing trials, thisreview should be updated within 2 years. Anyfuture review should include a comparison against alternative treatments. Further researchshould:
● evaluate RFTP upper limb interventions and inparticular constraint-induced movementtherapy
● address practical ways of delivering RFTPinterventions
● be directed towards the evaluation of suitablemethods to maintain functional gain
● be powered to detect whether RFTPinterventions are cost-effective, include abaseline activities of daily living measure,include indirect costs and use quality of life asan outcome measure to facilitate economicanalysis.
Executive summary

Description of the conditionThe annual incidence of first ever stroke in theUK is approximately 100,000 people per year.1
Although the incidence of stroke is falling,2 strokeis still the major cause of long-term neurologicaldisability in adults.3 The prevalence of disabilityand impairment varies according to sampling ofcohorts, but approximately half of all strokesurvivors are left with severe functional problems,4
and 53% are dependent on others for help withdaily activities at 6 months after their stroke.5 Only5–20% of people with initial upper limbimpairment fully regain arm function, and30–66% regain no functional use at 6 months.6–9
At 3 weeks and 6 months after stroke, 40% and15% of people are unable to walk independentlyindoors,5 with only 18% regaining unrestrictedwalking ability.10 Initial grade of paresis is themost important predictor for motor recovery, witha longer recovery period for people with severestroke.11
Stroke is thus a leading cause of disability, and assuch contributes to 4% of NHS costs.12 Whilestroke is a costly condition in the acute stage, over40% of the 5-year cost of stroke is likely to beincurred subsequent to discharge, with 18% of the total cost being due to institutional care.13
If the disability and subsequent need forinstitutional care can be reduced, there is apotential for the long-term care costs to besubstantially lowered.
Description of the interventionSystematic reviews of treatment interventions forthe paretic upper limb suggest that patientsbenefit from exercise programmes in whichfunctional tasks are directly trained, with lessbenefit if the intervention is focused on theimpairment, such as muscle strengthening.14
Although individual studies do not agree whetherincreased therapy intensity improves overalloutcome, a recent meta-analysis15 has shown thatmore intensive therapy may at least improve therate of recovery of activities of daily living (ADLs),particularly if a direct functional approach isadopted.16
Repetitive practice of goal-directed, functionalmovement under varying conditions for procedurallearning is a feature of many forms of interventionin stroke rehabilitation. The use of intensiverepetition is grounded in neurophysiologicalhypotheses about the reasons for loss of movementafter stroke. Repeated motor practice enhancesmotor strength, speed and endurance, whilesensorimotor coupling contributes to theadaptation and recovery of neuronal pathways.17
Repetitive task training (RTT) is common as aspecific rehabilitation technique, but it is oftencombined with techniques to enhance cognitiveinvolvement in the relearning of motor skills, suchas functional relevance and knowledge ofperformance, thereby forming the underlyingprinciples in the motor relearning or movementscience physiotherapy approach.18
Intensive periods of task practice using shapingtechniques (progressively increasing the difficultyof a task in small steps and providing frequentfeedback and positive encouragement) to build upto completion of a functional task are also a majorfeature of constraint-induced movement therapy,19
where they are combined with restricted use of theunaffected limb to overcome learned non-use oradaptive strategies.
Intensive practice of functional movement can alsobe assisted by treadmills,20 gait trainers21 orrobotics.22 Mechanical assistance is used toovercome impairment which restricts the ability toparticipate, but also serves to deliver an intensityof training sufficient to develop the amount andpower of movement required for functionalperformance.
Scope of the reviewThis study will consider the impact and cost-effectiveness of all three of the major forms oftherapy that have repeated, functional taskpractice as a major component, namely repetitivetask training (RTT), constraint-induced movementtherapy (CIMT) and treadmill training (TM). Incombination, these three forms of therapy will bereferred to as repetitive functional task practice(RFTP).
Health Technology Assessment 2008; Vol. 12: No. 30
1
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Chapter 1
Introduction

Systematic reviews of TM20 and CIMT23 havealready been published. To provide an overallpicture of the relative effectiveness and cost-effectiveness of all the common forms of RFTP,the references from the systematic reviews for TMand CIMT were followed up and data wereextracted from those primary studies that also metthe inclusion criteria for this study. A systematicreview of RTT studies has already been submittedto The Cochrane Collaboration by the authors ofthis report. This review therefore presents theresults of these three interventions combined. Thecharacteristics, quality and results of the trials foreach intervention are reviewed and presentedseparately to ensure clarity, until combined insubgroup analysis to present a between-intervention overall estimate of efficacy andcomparison of effect.
Scope of the cost-effectivenessanalysisAn economic model will be developed from anexisting data set. The data set containsinformation on the natural recovery and resourceuse of a cohort of stroke patients, which allows
estimates to be made on outcomes and costs. Theefficacy of RFTP and hence its potential impact onoutcomes will be obtained from the review; thecost of RFTP will be estimated by considering staffand equipment costs. Using certain assumptions,which will be clearly outlined in the methods, themodel data and the efficacy of RFTP from thereview will be used to estimate the cost-effectiveness of RFTP. Uncertainty in the estimatewill be considered by varying the parameters ofany assumptions that are made.
ObjectivesThe objectives of this study were to carry out asystematic review and cost-effectiveness analysis todetermine:
● whether RFTP improves global or limb-specificfunctional ability and ADL function in adultsafter stroke
● the factors that could influence primaryoutcome measures for RFTP, including theeffect of amount, type and timing ofintervention
● estimates of the cost-effectiveness of RFTP.
Introduction
2
Search strategy for identificationof studiesElectronic searchesThe Cochrane Stroke Group Trials Register wassearched in October 2006, using the followingparameters: Intervention Type: “Physiotherapy” or“Occupational Therapy”, without restriction ofintervention code.
In addition, the following databases were searchedas follows: The Cochrane Library (2006 Issue 3),MEDLINE (1966 to September week 4, 2006),EMBASE (1980 to week 40, 2006), CINAHL (1982to October week 1, 2006), AMED (1985 to week40, 2006), SportDiscus (1980 to October week 1,2006), ISI Science Citation Index (1973 to 14October 2006), Index to Theses (1970 toSeptember 2006), ZETOC (to 14 October 2006),PEDro (to 3 October 2006), OT Seeker (to 21April 2006) and OT Search (to March 2006).
The main search design was reviewed by theCochrane Stroke Group Trials Search Co-ordinator. The MEDLINE search given below wasused and adapted for other databases.
MEDLINE (OVID)1 cerebrovascular disorders/ or exp basal ganglia
cerebrovascular disease/ or exp brain ischemia/or exp carotid artery diseases/ orcerebrovascular accident/ or exp braininfarction/ or exp cerebrovascular trauma/ orexp hypoxia-ischemia, brain/ or expintracranial arterial diseases/ or intracranialarteriovenous malformations/ or exp"Intracranial Embolism and Thrombosis"/ orexp intracranial hemorrhage/ or vasospasm,intracranial/ or vertebral artery dissection/
2 (stroke or poststroke or post-stroke orcerebrovasc$ or brain vasc$ or cerebral vasc$or cva$ or apoplex$ or SAH).tw.
3 ((brain$ or cerebr$ or cerebell$ or intracran$or intracerebral) adj5 (isch?emi$ or infarct$ orthrombo$ or emboli$ or occlus$)).tw.
4 ((brain$ or cerebr$ or cerebell$ orintracerebral or intracranial or subarachnoid)adj5 (haemorrhage$ or hemorrhage$ orhaematoma$ or hematoma$ or bleed$)).tw.
5 hemiplegia/ or exp paresis/
6 (hemipleg$ or hemipar$ or paresis orparetic).tw.
7 or/1-6 8 *cerebrovascular disorders/rh or exp *basal
ganglia cerebrovascular disease/rh or exp*brain ischemia/rh or exp *carotid arterydiseases/rh or *cerebrovascular accident/rh orexp *brain infarction/rh or exp *cerebrovasculartrauma/rh or exp *hypoxia-ischemia, brain/rhor exp *intracranial arterial diseases/rh or*intracranial arteriovenous malformations/rhor exp *"Intracranial Embolism andThrombosis"/rh or exp *intracranialhemorrhage/rh or *vasospasm, intracranial/rhor *vertebral artery dissection/rh
9 *hemiplegia/rh or exp *paresis/rh 10 exp *gait Disorders, neurologic/rh or *motor
skills disorders/rh11 rehabilitation/ or "activities of daily living"/ or
exercise therapy/ or occupational therapy/12 Physical Therapy Modalities/ 13 Exercise Movement Techniques/ or exercise
therapy/ or walking/14 Robotics/15 exp Psychomotor Performance/ 16 movement/ or gait/ or exp locomotion/ or exp
motor activity/ 17 "Range of Motion, Articular"/ or "Task
Performance and Analysis"/ or "Practice(Psychology)"/
18 "Recovery of Function"/ 19 ((motor or movement$ or task$ or skill$ or
performance) adj5 (repetit$ or repeat$ ortrain$ or re?train$ or learn$ or re?learn$ orpractic$ or practis$ or rehears$ or rehers$)).tw.
20 ((motor or movement$ or task$ or skill$ orperformance) adj5 (schedule$ or interventionor therap$ or program$ or regim$ orprotocol$)).tw.
21 (functional adj5 (task$ or movement)).tw. 22 or/8-2123 7 and 22
The search above was combined with theCochrane Stroke Review Group search forrandomised controlled trials.
A similar search (Search 2), given below, wasconducted without limits of study type and/orclient group, to check for trials incorrectly
Health Technology Assessment 2008; Vol. 12: No. 30
3
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Chapter 2
Review methods
indexed, and to trace trials of RFTP in other clientgroups for citation tracking.
MEDLINE OVID1 *hemiplegia/rh or exp *paresis/rh 2 exp *gait Disorders, neurologic/rh or *motor
skills disorders/rh 3 1 or 24 Physical Therapy Modalities/ 5 Exercise Movement Techniques/ or exercise
therapy/ or walking/ 6 Robotics/7 rehabilitation/ or "activities of daily living"/ or
occupational therapy/ 8 exp Psychomotor Performance/ 9 "Task Performance and Analysis"/ or "Practice
(Psychology)"/ 10 ((motor or movement$ or task$ or skill$ or
performance) adj5 (repetit$ or repeat$ ortrain$ or re?train$ or practic$ or practis$ orrehears$ or rehers$)).tw.
11 (functional adj5 (task$ or movement)).tw. 12 or/4-1113 movement/ or gait/ or exp locomotion/ or exp
motor activity/ 14 "Recovery of Function"/ 15 13 and 1416 3 and (12 or 15)
Unpublished trial data were searched for onnational and international databases to May 2006as follows: MetaRegister of Controlled Trials,BioMed Central, CRISP, Centerwatch, NationalResearch Register, ReFeR, Stroke Trials Directory,REHABDATA and CIRRIE, using simple terms forstroke and rehabilitation or physical therapy.
Physiotherapy, occupational therapy and roboticsconference proceedings were searched as follows:
● Australian Physiotherapy AssociationConference 2000, 2002, 2004
● Australian Physiotherapy Association Neurologyand Gerontology Physiotherapy Conference 2005
● American Physical Therapy Congress AnnualConference 2005
● Canadian Physiotherapy Conference 2005● UK College of Occupational Therapists
Conference 2002, 2003, 2005● National Association of Neurological
Occupational Therapists Conference 2005● World Confederation for Physical Therapy 1st
International Congress 1953, 4th InternationalCongress 1963
● World Confederation of Physiotherapy Europe:First Congress, Copenhagen 1994:Physiotherapy in Stroke Management
● Chartered Society of Physiotherapy AnnualCongress 2000, 2001, 2002, 2003, 2004, 2005
● ICORR Rehabilitation Robotics InternationalConferences 1999, 2001, 2005
Non-English-language literature was identified bysearching Chinese, Russian and Indian databasesvia Eastview, Panteleimon and Indmed, usingbroad descriptors for stroke, rehabilitation andphysical therapy. The China National Knowledgedatabase was searched in both English andChinese. Searching and translation of Chineseabstracts were undertaken by personnel from theSecond Military Medical University, Shanghai.
Other sourcesRTTThe reference lists of systematic reviews relevant tophysical or occupational therapy in strokerehabilitation were searched.11,14–16,24–45 Referencelists of publications and literature reviews relevantto RTT identified by the search were combed toidentify further relevant trials.46–48 In addition,forward citation searching was undertaken on ISIWeb of Knowledge for all included trials, and theauthors were contacted to ask for details of anyother possible relevant trials, either published orunpublished. A request for information was alsoposted to the bulletin boards of World Congress ofPhysical Therapy and PHYSIO JISCmail.
CIMT and TMStudies relevant to CIMT and TM were sourcedfrom the search identified above, and also fromexisting systematic reviews.20,23 Only those trials ofCIMT and TM that met the requirements of thisreview (i.e. RFTP intervention with suitablecomparison) were included.
Inclusion criteriaTypes of studyRandomised and quasi-randomised trials (such asthose allocating by date or alternation) wereincluded in the review. Only the first period ofcross-over trials was included.
One arm of the trial had to include RFTP,compared against usual practice (including ‘notreatment’) or an attention-control group. Fortrials of TM or CIMT, comparison groups usingalternative forms of training were included.
Examples of attention-control treatment arecomparable time spent receiving therapy on adifferent limb or participating in an activity with no
Review methods
4
potential motor benefits. Usual-practice comparisongroups were accepted when the interventionreceived by the control group was considered anormal or usual component of stroke rehabilitationpractices, including neurophysiological ororthopaedic approaches. Early after stroke it wasassumed that usual practice would mean thatpatients would receive some therapy.
Types of participantAdults (presumed 18 years and older) who hadsuffered a stroke were included. Stroke was definedaccording to the World Health Organization(WHO) definition as “a syndrome of rapidlydeveloping symptoms and signs of focal, and attimes global, loss of cerebral function lasting morethan 24 hours or leading to death, with noapparent cause other than that of vascularorigin”.49 Trials starting at any time after an acutestroke and in any setting were included.
Types of interventionTrials were required to include an interventionwhere an active motor sequence was performedrepetitively within a single training session, wherethe practice aimed towards a clear functional goal.Functional goals could involve complex wholetasks, or pretask movements for a whole limb orlimb segment such as grasp, grip or movement ina trajectory to facilitate an ADL. To be included,trials of repetitive activity were required to involvecomplex multijoint movement with functionalmeasurement of outcome, rather than the exerciseof a single joint or muscle group orientated tomotor-performance outcomes.
Any intensity and duration of task trainingschedule was included. However, trials wereincluded only if the duration or number ofrepetitions within a session of practice, and thenumber of sessions delivered, could be identified.Trials clearly using motor relearning as a wholetherapy approach were included if the amount oftask-specific training received could be identified.
Trials using person-delivered, mechanical orrobotic movement assistance were included if thepurpose of the assistance was to facilitate a task-related repetition. Trials combining repetitive taskpractice with constraint of the unaffected limbwere also included.
Exclusion criteriaTrials were excluded if they combined RFTP with other interventions such as electrical
stimulation virtual environments, biofeedback,bilateral movement, or mental rehearsal. Trials were also excluded if the intervention used mechanical means simply to increaseendurance through the intensity of practicewithout monitoring or adjustment according tothe quality of movement, such as the use of slotmachines.
Trial authors were contacted for clarification of the nature of the intervention if it was unclearwhether the trial met the definition.
Types of outcome measurePrimary outcomesThe primary outcomes chosen were global andlimb-specific functional measures. Owing to thelarge range of measures used across trials,selection of outcome measures was done by the review authors to maximise quantitativepooling. If more than one measure was available in an outcome category, measures offunctional motor ability used in the primary trialswere prioritised as follows in the differentcategories. Items marked with an asterisk aremeasures where a low score equals a positiveoutcome. In all other measures, a high scoreindicates a good outcome.
Upper limb function/reach● Arm function: Action Research Arm Test
(ARAT), Motor Assessment Scale (MAS) – upperlimb component, Frenchay Arm Test, WolfMotor Function Test (WMFT), Functional Testof the Hemiparetic Upper Extremity (FTHUE),Box and Block Test (BBT), Test Evaluant desMembres Supérieurs des Personnes Agées(TEMPA), University of Maryland ArmQuestionnaire for Stroke, Motor Activity Log(MAL).
● Hand function: MAS hand, Jebsen Test of HandFunction*, Peg Test*, Purdue Pegboard.
● Sitting balance/reach: Reaching PerformanceScale, Functional Reach.
Lower limb function/balance● Lower limb function: walking distance, walking
speed, functional ambulation, sit-to-stand*,measures of lower limb function, e.g.Rivermead Mobility Index, Sodring MotorEvaluation Scale (SMES), Step Test.
● Standing balance/reach: Berg Balance Scale.
Overall functional abilityMAS, Rivermead Motor Assessment (RMA) Scale.
Health Technology Assessment 2008; Vol. 12: No. 30
5
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

Secondary outcomesADLBarthel Index (BI), Functional IndependenceMeasure (FIM), Modified Rankin Scale, GlobalDependency Scale.
Adverse outcomePain, injury, falls.
Timing of outcome assessmentPrimary outcome timing was at the end of theintervention period. Where the end of theintervention period was not clearly defined,outcome measures at 3 months post-stroke werechosen as primary. Data are presented for follow-up less than 6 months post-stroke, and between6 months and 1 year post-stroke.
Data extraction and assessment ofstudy validitySelection of studiesOne reviewer (BF) performed the searches. Fromthe initial references, 4443 obviously irrelevantitems were excluded on title and abstract by onereviewer (BF) and checked by a second reviewer(JM). All reviewers (BF, JM, ML and LT)undertook screening on the same titles andabstracts until an acceptable level of inter-raterreliability was achieved (kappa = 0.63). From thatpoint, two reviewers (from BF, JM, ML and LT)independently screened references.
In total, 447 full papers considered potentiallyrelevant were retrieved, including 71 items inlanguages other than English. For non-English-language papers, decisions about exclusion weremade on English abstract or machine translationof the abstract via WorldLingo or TranslationBooth, if adequate. Where machine translation wasinadequate, or where inclusion was unclear fromEnglish abstracts, the methods sections of fullpapers were commercially translated by nativespeakers. Seventeen methods sections of papersand three full non-English-language papers thatwere screened as potentially relevant were alsocommercially translated. Two reviewersindependently screened all full papers andmethods section translations for non-Englishstudies. Altogether, 121 papers were progressed tomore detailed filtering by two reviewers (from ML,LT, BF and JM).
Data extraction and managementAll reviewers (BF, JM, ML and LT) undertook dataextraction and critical appraisal on eight studies.
Using unweighted multiple kappa, inter-raterreliability of judgement of seven criteria for qualityassessment was median kappa = 0.67 (range0.48–0.85). Disagreements were reviewed andinstructions for critical appraisal gradings revised.From that point, two reviewers independentlyconducted data extraction and review of themethodological quality of the eligible trials.Disagreements were resolved by discussion andreferral to a third reviewer. Data were recorded ona standardised checklist, incorporating details ofrandomisation method, study population,intervention methods and delivery, reason forlosses to follow-up, and post-therapy and follow-upoutcome measures. In addition, informationrelating to treatment monitoring, acceptability andadherence was extracted where available.
Assessment of methodological qualityItems were evaluated as adequate, inadequate orunclear, and quality assessment was undertakenusing the following criteria:
● selection bias– random allocation– allocation concealment– baseline comparability of groups
● performance bias– equal treatment of groups
● attrition bias– description of withdrawals, dropouts and
those lost to follow-up– intention-to-treat analysis– percentage loss to follow-up
● detection bias– blinding of outcome assessors.
AnalysesThe primary comparison to be undertaken was toestimate the overall effect of RFTP. Secondarycomparisons were designed to determine whethertreatment effects differed for type of intervention(RTT, CIMT or TM), or the timing or amount ofintervention.
Measures of treatment effectFor continuous outcomes using similarmeasurement scales, the weighted mean difference(WMD) with 95% confidence interval (CI) wasused. Where similar outcomes were measuredusing different outcome scales, results werecombined using standardised mean difference(SMD) with 95% confidence interval. Outcomesmeasured using both dichotomous and continuousmeasurement units were analysed using thegeneric inverse variance method. For continuousoutcomes, means of post-therapy scores and their
Review methods
6

respective standard deviations were extracted.Changes from baseline outcome data wereextracted if available across all trials.
Unit of analysis issuesStudies with multiple treatment groupsTwo RTT trials50–52 compared upper versus lowerlimb training, so are included as fourintervention–control pairs. In the subgroupanalyses, these intervention–control pairs are notincluded as separate trials, as it was consideredthat the impacts of the interventions on upper andlower limb function in the same person would notbe independent. Results for primary outcome ofthe lower limb training groups were selected, asstudies were showing that treatment effects weregreater for lower limbs. This strategy may have theeffect of inflating effect sizes, but the effect shouldnot bias the tests of subgroup effects. One RTTtrial53 compared upper and lower limb traininggroups against the same control group. To avoidthe control group being included twice, and to usea limb-specific rather than a global or an ADLmeasure, the lower limb training versus splintcontrol comparison was selected for the subgroupanalyses.
Dealing with missing dataIf data were not in a form suitable for quantitativepooling, trial authors were contacted foradditional information. Attempts were made toobtain post-therapy scores from trial authors whohad reported median and interquartile ranges(IQRs).
Assessment of heterogeneityThe degree of heterogeneity for each outcome wasassessed by the I2 statistic. If less than or equal to50%, any heterogeneity was deemed insubstantialand a fixed-effects meta-analysis was used. If the I2
statistic was greater than 50%, the individual trialcharacteristics were explored to identify potentialsources of heterogeneity. Meta-analysis was thenperformed using both fixed- and random-effectsmodelling to assess sensitivity to the choice ofmodelling approach and reported accordingly.
Clinical and methodological diversity wasaddressed by incorporation of subgroup analysesfor type of participant (time from stroke),intervention (type and amount of intervention)and study design (allocation concealment,comparison group, equivalence of treatment, lossto follow-up and trial size).
To test for subgroup effects data were stratified bysubgroup and the Q-statistic was partitioned from
the unstratified analysis into ‘within subgroups’and ‘between subgroups’. A �2 test of the resultingbetween-subgroups Q-statistic was performed,using a 10% significance level.54
Assessment of reporting biasesAssessment of the potential for reporting bias waschecked by performing a subgroup analysis basedon the trial size (number of participants) andproducing a funnel plot of the standard error (ofeffect estimate) against effect estimate.
Subgroup analysis and investigation ofheterogeneityPlanned subgroup analyses for upper and lowerlimb functional outcomes were undertaken asfollows.
● Type of intervention: trials were classified asRTT, CIMT or TM.
● Dosage of task practice: this was calculated bymultiplying the number of weeks by the numberof sessions per week by the session duration inhours. Trials were divided into those providingup to and including 20 hours’ training andthose providing more than 20 hours’ training intotal. The division at 20 hours was based on themedian value for dosage of task practice fromall included trials, and the average length ofstay in the National Sentinel Stroke Audit55
after the first 7 days of acute care, presumingthe provision of 1 hour of training per day inthe inpatient rehabilitation period.
● Time since stroke: mean time since stroke atrecruitment was used to classify trials as within0–6 months post-stroke or more than 6 monthspost-stroke. The division at 6 months was basedon the interpretation of this as the main periodof active rehabilitation. Because a number oftrials recruited very early post-stroke, a post hocanalysis grouping was included for trialsrecruiting within 14 days of stroke.
It had been intended to consider whether effectsizes were related to whether training was basedon pre-functional or functional activities or pre-intervention level of disability. In the event,most pre-functional trials were excluded becausethey contained passive or active-assistedmovement, and levels of disability proved toodifficult to classify because of mixed groups ofparticipants and unsuitable measures and data forthis purpose. Therefore, these planned subgroupanalyses are not presented.
The selection of outcome measure for subgroupanalysis was complicated by the fact that few trials
Health Technology Assessment 2008; Vol. 12: No. 30
7
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

used similar outcome measures. Subgroup analyseswere performed separately for upper and lowerlimb interventions. Outcomes for subgroupanalyses were limited to measures of walking forlower limbs and arm function for upper limbs. Ifmore than one measure was available, lower limboutcomes were prioritised in the following order:(1) walking speed, (2) walking distance and (3) functional ambulation/walking scales; andupper limb outcomes were prioritised as follows:(1) ARAT, (2) MAS – upper extremity (MAS-UE),(3) WMFT and (4) BBT. Outcome selection wasbased on evidence for correlation and similarresponsiveness to change for walking distance,speed and functional ambulation.56 For measuresof arm function, there is evidence for correlationand similar responsiveness to change for the MAS-UE and ARAT,57,58 and for correlationbetween ARAT and BBT.59 There is less evidencefor correlation between WMFT and other tests,but ARAT, BBT and WMFT all correlate well withthe Fugl–Meyer measure of arm impairment.59,60
Four trials61–64 were omitted from the subgroupanalyses because data were unsuitable for pooling.
Of the remaining 27 trials, 26 presented meansand standard deviations, so SMD could be used asthe effect measure. One trial65 was excluded fromthe subgroup analyses because it used adichotomous main outcome. This trial wasexcluded rather than using generic inversevariance, because SMD is easier for clinicians tointerpret.
Planned subgroup analyses were also carried outfor allocation concealment (adequate orinadequate/unclear). In addition, post hocsubgroup analyses were included to consider theimpact of different comparison groups (attention-control, usual care), equivalence of therapy time(equivalent time, additional time) and trial size(under 25 participants, 25 participants and over),based on the median value. Planned subgroupanalyses for intervention delivery (therapist versusself-administered, group versus individual) andintervention setting (home versus community)were not undertaken, because of insufficientnumbers of trials.
Review methods
8
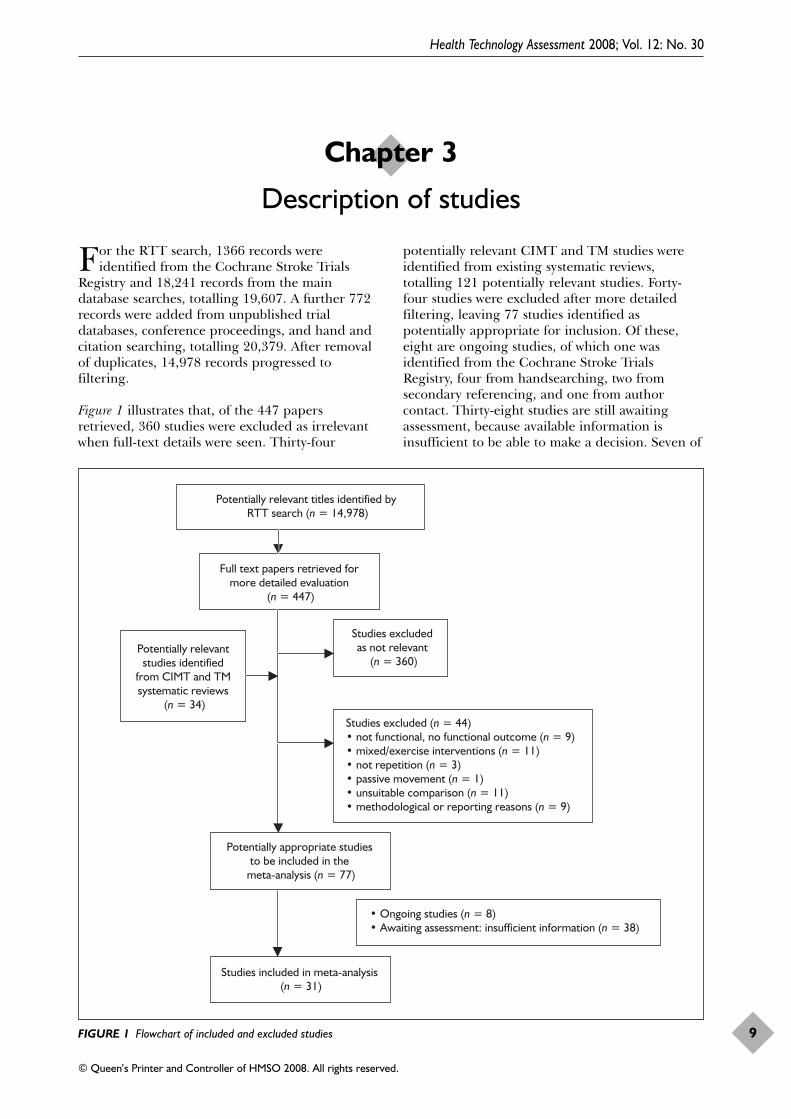
For the RTT search, 1366 records wereidentified from the Cochrane Stroke Trials
Registry and 18,241 records from the maindatabase searches, totalling 19,607. A further 772records were added from unpublished trialdatabases, conference proceedings, and hand andcitation searching, totalling 20,379. After removalof duplicates, 14,978 records progressed tofiltering.
Figure 1 illustrates that, of the 447 papersretrieved, 360 studies were excluded as irrelevantwhen full-text details were seen. Thirty-four
potentially relevant CIMT and TM studies wereidentified from existing systematic reviews,totalling 121 potentially relevant studies. Forty-four studies were excluded after more detailedfiltering, leaving 77 studies identified aspotentially appropriate for inclusion. Of these,eight are ongoing studies, of which one wasidentified from the Cochrane Stroke TrialsRegistry, four from handsearching, two fromsecondary referencing, and one from authorcontact. Thirty-eight studies are still awaitingassessment, because available information isinsufficient to be able to make a decision. Seven of
Health Technology Assessment 2008; Vol. 12: No. 30
9
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Chapter 3
Description of studies
Potentially relevant titles identified by RTT search (n = 14,978)
Full text papers retrieved for more detailed evaluation
(n = 447)
Potentially relevant studies identified
from CIMT and TM systematic reviews
(n = 34)
Studies excluded as not relevant
(n = 360)
Potentially appropriate studies to be included in the
meta-analysis (n = 77)
Studies included in meta-analysis (n = 31)
Studies excluded (n = 44)• not functional, no functional outcome (n = 9)• mixed/exercise interventions (n = 11)• not repetition (n = 3)• passive movement (n = 1)• unsuitable comparison (n = 11)• methodological or reporting reasons (n = 9)
• Ongoing studies (n = 8)• Awaiting assessment: insufficient information (n = 38)
FIGURE 1 Flowchart of included and excluded studies

these were identified from the Cochrane StrokeTrials Registry, 20 from handsearching, three fromdatabase searching, five from secondary referencesand three from author contact.
Unpublished data were sourced from the trialauthors for 11 RTT trials50,51,53,65–72 and twoCIMT trials.73,74
All of the included studies for RTT were identifiedfrom the Cochrane Stroke Trials Registry. ForCIMT and TM, all of the included studies wereidentified from existing systematic reviews, exceptfor one recent CIMT trial identified from theCochrane Stroke Trials Registry.75
Description of studiesThirty-one studies were included in total,including 34 intervention–control pairs and datafrom 1078 participants relevant to this review. Adescription of included studies is presentedseparately for each of the three forms of RFTP,namely RTT, CIMT and TM. A summary of thecharacteristics of the included studies is given inAppendices 1–3.
Included studiesRTTFourteen trials were identified, comprising 17intervention–control pairs, which met theinclusion criteria. Three trials included tworelevant intervention–control pairs: Kwakkel andcolleagues53 refer to a trial with twointervention–control pairs: a lower limb traininggroup versus splint control, and an upper limbtraining group versus splint control.Blennerhassett and Dite50 also include twointervention–control pairs: an upper limb traininggroup versus lower limb attention-control, and alower limb training group versus an upper limbtraining attention-control. Two papers report ontwo intervention–control pairs of the same trial:Salbach and colleagues51 refer to a lower limbtraining group versus upper limb trainingattention-control, and Higgins and colleagues52
refer to an upper limb training group versus lowerlimb training attention-control.
In one trial71 there were three arms, consisting ofa functional task practice group, a strengthtraining group and a usual-care group. Only thedata for the intervention–control pair of functionaltask practice versus control are included here.
DesignThe 14 trials considered comprised 13 randomisedcontrolled trials (RCTs)50,51,53,65–68,70–72,76–78 andone quasi-randomised trial.69 Four of the trialswere identified as pilot RCTs67,71,76,77 and three ofthe trials were multicentre.51,53,77 Three of thetrials were stratified for randomisation: one forbaseline level of walking deficit,51 one for genderand side of stroke,68 and one for severity ofdeficit.71
Sample sizeFour trials had 25 participants or fewer,66,67,69,76
six trials had between 25 and 49participants,50,65,71,72,77,78 and five trials had 50participants or more.51,53,68,70,71
SettingOf the 14 trials, three were carried out inCanada,51,65,67 three in Australia,50,66,78 three inthe UK,69,70,77 one in Taiwan,72 one in the USA,71
one in The Netherlands53 and one in France.76
CIMTEleven trials met the inclusion criteria. In fourtrials61,62,79,80 there were three arms consisting of amodified CIMT group, a traditional rehabilitationgroup and a no-treatment control group. In two ofthese trials the traditional rehabilitation groupalso received RTT, with the only differencebetween groups being constraint.79,80 In these trials,therefore, the no-treatment group was included asthe comparison group. In the remaining two trialsthe data for the modified CIMT and traditionalrehabilitation groups were included.61,62
DesignAll 11 trials were identified as RCTs, of which twowere identified as pilot81,82 and two aspreliminary,61,83 and one trial was labelled a‘feasibility and efficacy’ study.80 All trials weresingle centre.
Sample sizeTen trials had 25 participants or fewer.61,62,73,74,79–84
One trial had 50 participants or more.64
SettingNine trials were carried out in theUSA,61,62,73,74,80–84 one in Saudi Arabia79 and onein Thailand.64
TMSix trials were identified which met the eligibilitycriteria. One trial with three arms consisted of twoTM interventions, speed-dependent TM andlimited progressive TM, compared with
Description of studies
10

conventional gait training.85 The limitedprogressive TM group was used in this review, asspeed-dependent TM was judged to comprise twomechanisms of action.
DesignOne study was a cross-over trial,63 of which onlythe first phase was used. The remaining fivestudies were RCTs. Of these five trials, one wasidentified as a pilot controlled trial.86 All of thetrials were single centre. Three of the trials werestratified for randomisation, one for walkingspeed,87 one for deficit severity and age,88 and onefor initial time to walk 10 m without assistance.85
Sample sizeTwo trials had 25 participants or fewer,63,86 onetrial had between 26 and 49 participants,87 andthree trials had 50 participants or more.85,88,89
SettingOf the six trials, two were carried out in theUSA,86,88 three in Germany;63,85,89 and one inAustralia.87
ParticipantsRTTThe 14 trials included 680 participants, of which659 were included in the 17 intervention–controlpairs relevant to this review. All of the trialsincluded both genders, with three trials havingmore than 60% male participants.51,65,66 In twotrials, the participants had a mean age of less than6050,69 and in five trials the mean age was over70 years.51,68,70,77,78
Six trials included only participants after a firststroke53,67,68,71,72,76 and two trials includedparticipants with either first or recurrentstroke.50,51 In the remaining trials, it was unclearwhether inclusion was limited to first stroke only.
Mean time since strokeThree trials recruited within 14 days of stroke.53,68,70
A further four trials recruited within the firstmonth post-stroke,65,71,76,77 one trial recruitedwithin 3 months of stroke,50 two trials recruited within 6 months of stroke,69,78 two trials recruited within 12 months of stroke51,72
and two trials recruited participants in the chronic phase of stroke.66,67
CIMTThe 11 trials included 203 participants, and datafrom 190 participants were relevant to this review.
Thirteen participants were not included fromstudies where there was more than onecomparison group.61,62,79,80 All of the studiesincluded both genders, with six studies havingmore than 60% male participants.61,62,64,74,82,84 Infour trials, participants had a mean age of lessthan 60 years;62,64,79,80 no trials had a mean ageover 70 years.
Three trials included only subjects after a firststroke.64,74,83 In the remaining trials, it was unclearwhether inclusion was limited to first stroke only.
Mean time since strokeThree trials recruited within 19 days ofstroke,81,82,84 three trials recruited between 1 and6 months post-stroke,61,79,80 and one trial recruitedbetween 3 and 9 months post-stroke.83 Theremaining trials recruited 12 months or morepost-stroke.62,64,73,74
TMThe six studies included 254 participants, of whichdata from 229 participants were relevant to thisreview. Five of the studies included both genders,as participants in one study were all male.86 Fivestudies had more than 60% maleparticipants.63,85–87,89 Two trials had a mean ageless than 60;85,86 no trials had a mean age morethan 70 years.
Three trials included only subjects after a firststroke,63,87,89 one trial included subjects with eitherfirst or recurrent stroke,85 and in the remainingtwo trials86,88 it was unclear whether inclusion waslimited to first stroke only.
Mean time since strokeOne trial recruited within the first month ofstroke,86 one trial recruited within 3 months post-stroke,89 one trial recruited within 6months post-stroke85 and three trials recruited in the chronic phase of stroke recovery.63,87,88
InterventionsRTTTwo trials used whole therapy motorapproaches,68,70 and four trials trained singletasks, all related to balance, reach or sit-to-stand.65,66,76,77 The remaining trials consisted ofmixed functional task training. Of these, threeused a circuit-training approach.50,51,67 While all ofthe remaining trials included some functional taskpractice, this was sometimes mixed with othercomponents, including strengthening exercise and
Health Technology Assessment 2008; Vol. 12: No. 30
11
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

TM,53 upper limb exercise,69 lower limb exercise78
and shaping training.72
Of the 17 intervention–control pairs relevant tothis review, four included lower limb or mobilitytraining,50,51,53,67 one trained sit-to-standmovements,65 two trained balance in sitting andstanding,76,77 one trained functional reach insitting,66 and one trained standing balance andmobility.78 Six intervention–control pairs wereupper limb training.50,52,53,69,71,72 Twointervention–control pairs used whole therapyapproaches, training global function.68,70
SettingFour trials were carried out solely in an inpatientsetting,50,65,76,77 four trials included both inpatientand outpatient care,53,68,70,71 four trials were carriedout in outpatient or community settings51,66,67,72
and two trials were in the home environment.69,78
In three trials, the intervention was additional tousual care, of which two were during inpatientrehabilitation71,77 and one was after dischargefrom inpatient therapy, but additional tooutpatient therapy.69
Amount of task practiceThe number of hours of training variedconsiderably across the interventions. Three trialsprovided less than 10 hours’ training intotal,66,70,77 seven trials provided between 10 and21 hours’ training,50,51,65,67,68,71,76 two trialsprovided more than 40 hours’ training53,72 andtwo trials prescribed more than 40 hours’ home-exercise therapy.69,78
Duration of trainingThe length of time over which training was spreadvaried from 2 to 4 weeks for seventrials.50,66,67,71,72,76,77 For two trials, the length oftime was estimated as 3 weeks of hospital inpatienttherapy, with therapy for some patients in anoutpatient setting if required.68,70 The interventionin four trials was over 6–8 weeks51,65,69,78 and inone trial the intervention was over 20 weeks.53
Intervention deliveryAll of the interventions were delivered by trainedphysiotherapists or occupational therapists, exceptfor the self-monitored home-exerciseprogrammes,69,78 where trained staff input wasrestricted to prescription and programme review,one trial where trained physiotherapy assistantsprovided balance training77 and one trial whereregistered practical nurses delivered sit-to-standtraining.65 Three of the interventions were
delivered in a group setting of between four andseven participants per group.50,65,67
Of those programmes delivered in a circuit-classformat, trial authors reported between 70 and80% compliance.50,51,67 For the self-administeredprogrammes in a home setting, trial authorsreported 68–75% self-monitored adherence to theprescribed exercise programme.69,78
CIMTTrials were divided into those evaluatingCIMT64,73,74,83,84 and those evaluating modifiedCIMT (mCIMT).61,62,79–82 CIMT interventionsincluded wearing a padded mitten and/or sling toreduce use of the unaffected arm, together with aprogramme for improving task performance of theaffected limb using techniques such as ‘shaping’(progressively increasing the difficulty of a task insmall steps and providing frequent feedback andpositive encouragement) and repetitive taskpractice. Typically, therapy sessions lasted for6 hours with participants attending 5 days perweek. mCIMT comprised similar interventions, buttherapy time was reduced to typically 1 hour perday with participants attending 3 days per week.
SettingTwo trials were carried out solely in an inpatientsetting,81,82 and one trial included both inpatientand outpatient care.84 Seven trials were conductedin outpatient clinic settings,61,62,64,73,74,79,80 and thefinal study83 did not specify a setting, but giventhat participants were 3–9 months post-stroke it islikely to be an outpatient clinic setting.
Amount of task practiceThe number of hours of training varied acrosstrials, with those evaluating CIMT typicallyproviding a larger number of hours, with aminimum of 42 hours84 and a maximum of75 hours.74 Modified CIMT trials typically provided30 hours’ training;61,62,79,80 with the exceptions ofone trial where 15 hours’ training was provided,82
and another providing 20 hours’ training.81
Duration of trainingAll CIMT trials spread training over 2 weeks, withthe exception of one trial84 where trainingspanned 2.5 weeks. Trials evaluating mCIMTspread training over a longer period, typically10 weeks,61,62,79,80,82 with the exception of onetrial81 where training lasted for 2 weeks.
Intervention deliveryInterventions in eight trials were delivered bytrained physiotherapists and/or occupational
Description of studies
12
therapists,61,62,79–84 with one trial also includingdelivery by ‘therapy assistants’.84 In three trials itis unclear who delivered the intervention.64,73,74
In the majority of trials, it is not clear whetherinterventions were delivered on a one-to-one orgroup basis. Exceptions are one trial wheretreatment was on a one-to-one basis,83 and onetrial where participants were treated in groups ofthree to four.64
TMTwo studies evaluated unsupported TM,87,88 andfour studies evaluated bodyweight-supportedtreadmill training.63,85,86,89 One trial supportedbodyweight to a maximum of 15%,89 one trial onlyallowed bodyweight support in the first threetraining sessions,85 and one trial progressivelydecreased bodyweight support as participantsacquired greater self-support.86
Two trials practised walking training with either adefined training heart rate89 or a target heart rateof 60–70%.88 The other trials did not specify adefined heart rate.
Five trials increased the belt speed of the treadmillduring the intervention. One trial identifies theuse of a treadmill with a variable belt speed, butdoes not specify how this was used.63
SettingFour trials were carried out in an inpatientsetting63,85,86,89 and two trials in an outpatientsetting.87,88 The four trials in the inpatient settingwere in addition to usual care.
Amount of task practiceOnly one trial provided more than 20 hours’ taskpractice.88
Duration of trainingThe length of time over which training was spreadvaried from 2 to 4 weeks for four studies.63,85–87
For one study the length of time was 6 weeks89 andfor one study it was 6 months.88
Intervention deliveryAll of the interventions were delivered by trainedphysiotherapists or occupational therapists.
Comparison interventionsRTTTen intervention–control pairs compared theintervention against an attention-control: two
intervention–control pairs used a recreation orcognitive therapy control group,65,66 twointervention–control pairs from the same trialused a splint control53 and six (four from twotrials) used a comparison training programme forthe upper or lower limb.50,51,67,78
Seven intervention–control pairs compared theintervention against usual care. Of these, threewere during inpatient rehabilitation and providedequivalent hours of therapy,68,70,76 and oneprovided additional hours of therapy.71 The otherthree intervention–control pairs were afterdischarge from inpatient rehabilitation, andadditional to any outpatient treatment.69,72,78 It isunclear whether the duration of therapy for theintervention–control pair was equivalent for one ofthese trials.72
CIMTThree studies compared the intervention againstan attention-control. One trial used a bimanualneurodevelopmental therapy control group,64 onetrial used procedures designed to focus attentionon the affected limb without providing training inactive movement,73 and one trial used a controldesigned to be less intense and designed toimprove task performance with the unaffectedside.74
Three trials compared the intervention againstusual care only.81,82,84 Control groups received anequal frequency of therapy time in two trials,81,84
and in one trial control participants received halfthe amount of therapy time compared withintervention participants.82
A further three trials had two comparison groups,one receiving usual care and one receiving notreatment.61,62,80 Usual-care participants in allthree trials received an equal amount of therapy tothe intervention group; the no-treatment groupreceived no interventions during the same period.Another trial also had two comparison groups, onereceiving no treatment, the other an attention-control group that received the interventionwithout the restraint component.79
The trial by Alberts and colleagues83 comparedthe intervention to no treatment, with participantsrandomised to the latter receiving the intervention1 year later.
TMOne trial compared the intervention against an attention-control consisting of a home-exerciseprogramme to lengthen and strengthen
Health Technology Assessment 2008; Vol. 12: No. 30
13
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
muscles.87 Two trials compared against analternative intervention.88,89 One of theseinterventions was individual physiotherapyconcentrated on walking rehabilitation,89 and onewas based on common components ofconventional therapy which would not normallyhave been received as participants were late post-stroke.88 Three trials compared the interventionagainst usual care.63,85,86 These trials were duringinpatient rehabilitation and provided equivalenthours of therapy.
Primary outcomesThe 31 included trials used a wide range ofdifferent outcome measures, measurementstatistics and time intervals for follow-up. Measuresselected post-intervention are detailed below.
Upper limb functional outcomemeasuresArm● RTT: ARAT,53 WMFT,72 MAS – arm,50,68,70
BBT,52 FTHUE71 and Southern Motor GroupAssessment – upper limb activity.69
● CIMT: Action Research Arm Test61,62,64,79,80,82
and WMFT.61,73,74,79–81,83
Hand function● RTT: Nine Hole Peg Test (9HPT),52 Ten Hole
Peg Test (10HPT),69 MAS – hand.50,68,70
● CIMT: Grooved Pegboard Test,84 a key-turningtask,83 and hand grip and pinch strength.64
Sitting balance/reach● RTT: reaching distance,66 Sitting Equilibrium
Index,76 MAS – balanced sitting,68,70 and lateralreach – time to return to quiet sitting.77
Lower limb functional outcomemeasuresWalking distance ● RTT: Six Minute Walk Test (6MWT).50,51,67
● TM: 6MWT87–89 and Five Minute Walk Test.86
Measures of walking distance over 5 minuteswere converted to distance over 6 minutes, onthe assumption that participants could maintaineffort equivalently over such similar periods.
Walking speed● RTT: Ten Metre Walk Speed (10MWS) with
walking aid,53,66,67 Five Metre Walk Speed(5MWS) at comfortable speed51 and Six MetreWalk Speed (6MWS).70
● TM: 5MWS,86 10MWS85,87,89 and walking speedover 30 feet (9.1 m).88
Functional ambulation● RTT: Functional Ambulation Classification
(FAC)53,76 and MAS – walking.68,70,78
● TM: FAC.85,86
Sit-to-stand● RTT: Timed Up and Go (TUG),50,51,67
MAS – sit-to-stand,68,70 sit-to-stand time inseconds,77 and number of people able to stand safely and independently on twooccasions.65
Lower limb functional measures● RTT: SMES trunk, balance and gait subscale,68
Step Test,50,67 and Rivermead Leg and Trunk.70
Standing balance and reach● RTT: Upright Equilibrium Index,76 Functional
Reach78 and Berg Balance Scale.51
● TM: measures of standing balance using aninstrumented balance assessment system88
which was not used.
Global motor function● RTT: MAS68 and RMA score for gross
functions.70
● CIMT: none● TM: RMA score for gross functions.63,88,89
Secondary outcomesADL measures● RTT: BI51,53,68,70 and FIM.76 Two trials used the
BI scoring out of 20,53,70 while the other trialsused the scoring out of 100.
● CIMT: The BI.81
● TM: none.
Adverse events● RTT: number of falls.65
● CIMT: levels of stiffness and discomfort on theaffected side.73
● TM: no trials reported quantitative data foradverse events. Narrative reports and reasonsfor withdrawal are summarised.
Timing of outcome measurement● RTT: within the 0–6-month period post-stroke:
one trial77 measured outcome at 1 month post-intervention and three trials at 2 monthspost-intervention.67,76,78 Within the 6–12-monthpost-stroke period, one trial measured outcomeat 6 months post-intervention,50 one trial at9 months post-intervention,71 one trial at6 months post-randomisation,70 and one trial at1 year post-stroke.68
Description of studies
14

● CIMT: one trial measured outcome 3–4 monthspost-stroke84 and one trial measured outcome6 months post-intervention.74
● TM: two trials measured outcome at 3 monthspost-intervention.87,89
Excluded studiesThere is a large number of excluded studies(n = 44), described in Appendix 4. Because of thedifficulties in determining whether trialinterventions included task-specific functionalrepetition, the authors have attempted to be astransparent as possible about the basis on whichtrials were excluded. The reasons for exclusion were:
● not functional, or no functional outcome: ninestudies
● mixed interventions, or interpreted as focusingpredominantly on exercise: 11 studies
● not repetition, or unable to determine amountof practice: three studies
● passive movement: one study● comparison group also includes some form of
repetitive functional intervention: 11 studies● methodological or reporting reasons: nine studies.
The excluded studies included three trials thathad been either partially or fully translated fromChinese to English. While translation wasundertaken by native-speaking health-serviceworkers, there is the possibility that informationwas misinterpreted or misunderstood.
Ongoing studiesThere are eight ongoing studies, where theinformation available is sufficient to say that theinterventions include an element of RFTP. Theseare detailed in Appendix 5. Three trials involvetraining for standing, balance or sit-to-stand,90–92
two trials are of lower limb circuit training93,94 andone trial is of upper limb task-specific training.95
One trial uses a motor relearning approach(Langhammer B, Oslo University College, Oslo,Norway: personal communication, November2006) and one trial is of CIMT.96 All are withparticipants in the early stages of stroke recovery,except for the trial by Langhammer.
Studies not assessed at reportcompletionRTTOf the 17 studies categorised as unable to beassessed, 12 were ongoing studies identified from
trials registers, where the information availablewas insufficient to be able to exclude them at thisstage.97–108 Two studies are unpublished, and thereviewers are awaiting data.109,110 One study waspublished as a conference proceeding, and thereviewers were unable to contact the authors.111
Two studies are published, and attempts are beingmade to contact the authors to determine theexact content of the intervention.112,113
CIMTOf the seven studies awaiting assessment, three areongoing114,115 (Page S, University of CincinnatiAcademic Medical Centre, Ohio, USA: personalcommunication, February 2007). One recentlypublished study was not in the date range forsearching.75 Two related studies have recentlycompleted and been submitted for publication.116
The reviewers were unable to contact the authorsof one study to assess for eligibility.117
TMOf the 14 studies awaiting assessment, theinformation available for seven ongoing studies isinsufficient to be able to exclude them at thisstage.118–124 Three studies requiretranslation.125–127 One study is recentlycompleted128 as a follow-up to an included study,86
and three studies could not be traced.129–131
Quality of included studiesAllocationRTTAllocation concealment was adequate in eighttrials.50,51,53,67,70,71,77,78 In five trials, allocationconcealment was unclear; of these, three trialsstated that random allocation was used, butprovided no description of the procedure for itsconcealment from those recruitingparticipants;68,72,76 one trial used coin flipping torandomise participants with no further descriptionof the procedure,65 and one trial attemptedconcealment with a procedure involvingparticipants drawing cards out of a box containingten control group and ten experimental groupcards, but the procedure for ensuring that thoserecruiting participants remained unaware ofassignments is not described.66 One trial was quasi-randomised, allocating participants to interventionor control groups in alternate runs of five.69
CIMTThe procedure for allocation concealment wasunclear in all trials. Seven trials stated that randomallocation was used, but provided no description
Health Technology Assessment 2008; Vol. 12: No. 30
15
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

of the procedure.61,62,73,79,80,83,84 Four trials stateduse of tables of random numbers to allocateparticipants to intervention or control groups, withno description of the procedure.64,74,81,82
TMAllocation concealment was adequate in fourtrials.86–89 In two trials, allocation concealment wasunclear. One trial stated that participants wereassigned to groups by block randomisation on thebasis of walking speed, but provided nodescription of the procedure for concealing theallocation, or the block length.85 One trial statedrandomisation, with no description of theprocedure.63
Blinding of outcome assessorsRTTBlinding of primary outcome assessment wasstated in all but two trials.69,71 Of the studies thatstated observer blinding, three gave no details ofhow this was done.68,72,78 Four trials checkedwhether the outcome assessor had becomeunblinded,51,53,67,70 and out of these, three trialsreported that some degree of unmasking mighthave occurred.51,53,67
CIMTBlinding of outcome assessment was attempted inall trials with the exception of one trial,79 wherethere was no mention of blinding. In two trials73,84
action taken at blinding was judged likely to havebeen effective, for example employing personnelfrom outside the hospital who were blind totreatment assignment. Eight trials stated thatoutcome assessment was blinded, but did notdescribe the procedure.61,62,64,74,80–83 No trialreported checking for the possibility thatunblinding had occurred.
TMBlinding of primary outcome assessment wasstated in two trials.85,87 Neither trial describedchecks for unblinding. Two trials attemptedblinding, but report that this may not have beensuccessful,88,89 for example one trial stated that asa result of staffing limitations and institutionalsafety regulations, treadmill exercise testing wasconducted by the same staff who providedtraining,88 hence metabolic fitness tests wereunblinded. In one trial, physiotherapists notinvolved in the therapy were responsible for theassessment of the RMA Scale, but disclosure bypatients and team-mates could not be fullyexcluded.89 One trial did not mention blinding ofoutcome assessors to participants’ treatmentstatus.86
Owing to the nature of the interventions, blindingof participants, intervention providers or usualcare providers was not assessed, as it is essentiallyimpractical in this type of study.
Follow-up and exclusionsRTTAll trials provided information about numbers ofwithdrawals and reasons for withdrawal. All trialsaccounted for all participants at the end of thetrial, except for one, which included participantsin the analysis only if they completed thetreatment programme.71 Of the 14 trials in total,three trials had 10–20% loss53,68,78 and two trialshad more than 20% loss.67,70 The remaining ninetrials had less than 10% loss to follow-up.
CIMTNine trials had no withdrawals.61,62,64,73,74,79,80,82,83
One trial provided information about numbers ofwithdrawals and reasons for withdrawal;84 and onetrial81 states overall numbers of withdrawals, butnot by intervention group. All except one trial81
accounted for all participants at the end of thetrial. All trials had no loss to follow-up, except forone trial with 13% loss81 and one trial with 29%.84
TMFive trials provided information about numbers ofwithdrawals and reasons for withdrawal, andaccounted for all participants at the end of thetrial. Withdrawals and follow-up were unclear inone trial.63 Two trials had less than 10% loss tofollow-up post-treatment,87,89 two trials had11–20% loss to follow-up post-treatment85,86 andone trial had more than 20% loss to follow-uppost-treatment.88
Other potential sources of biasTo detect systematic differences in care providedto participants in comparison groups other thanthe intervention under investigation, trials wereassessed to determine whether groups were treatedequally during the intervention and during usualcare.
RTTDuring the intervention, groups were treatedequally in all trials, with the following exceptions:in one trial70 there was no significant difference inthe amount of treatment; however, the authorsstate in a supplementary paper that there mayhave been differences in elements of treatmentsuch as detailed feedback and socialconversation;132 in one trial it is not clear whethergroups were treated equally72 and in two trialsparticipants in the intervention group received
Description of studies
16

additional hours of therapy.71,77 During usual care,groups were treated equally in eighttrials.50,53,65–69,77 In four trials no information isprovided70–72,76 and in a further two trials52,78
there was no usual-care group.
CIMTDuring the intervention, comparison groupsreceiving therapy were treated equally in all excepttwo trials. In one trial,73 participants in theintervention group spent 7 hours at therehabilitation centre each weekday for 2 weeks;the comparison group received only four 10-minute periods encouraging them to focus onperforming new activities with the affected upperextremity at home and two sessions of ‘physicaltherapy’, plus a range of exercises to carry out athome. (As it was unknown how long control groupparticipants practised, equivalence of therapy timewas assumed for subgroup analyses.) In another
trial,74 participants in the intervention arm of thetrial similarly received longer periods of therapy(6 hours per day over 8 weekdays and 4 hours perday over 2 weekend days) than the comparisongroup (3 hours per day over 8 weekdays and2 weekend days of rest). Groups were treatedequally in all trials with a usual-care comparison.
TMDuring the intervention, other than theintervention provided, groups were treated equallyin all except one trial,87 where the control groupwas given a home-exercise programme to carryout for the same number of sessions as in theintervention group. However, this programme wasnot prescribed in sufficient number or intensity toprovide a training effect and instead aimed toprovide a credible sham programme. Groups weretreated equally in all trials with a usual-carecomparison.
Health Technology Assessment 2008; Vol. 12: No. 30
17
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.


Primary outcomesResults are presented separately for upper andlower limb outcomes and global function,concluding with an overall treatment effect for allforms of RFTP on functional outcome. All resultsare post-therapy, except for Langhammer andStanghelle,68 which are 3 months post-stroke, andVan Vliet and colleagues,70 which are 3 monthspost-baseline.
Upper limb function: post-therapyResults are presented for arm function, handfunction, and sitting balance and reach.
Arm functionEighteen trials recruiting 634 participantsmeasured arm function, with data suitable forpooling available for 76% (n = 485) (Figure 2).There was some heterogeneity of treatment effects
Health Technology Assessment 2008; Vol. 12: No. 30
19
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Chapter 4
Results of the review
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 02 Upper limb functionOutcome: 01 Arm function
Study Treatment Control SMD (fixed) Weight (SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 RTTBlennerhassett, 200450 15 4.90 (1.90) 15 5.10 (1.50) 6.45 –0.11 (–0.83 to 0.60) Higgins, 200652 47 29.00 (17.00) 44 28.00 (19.00) 19.58 0.06 (–0.36 to 0.47) Kwakkel, 199953 27 20.00 (22.00) 34 10.00 (19.00) 12.59 0.48 (–0.03 to 1.00) Langhammer, 200068 29 4.70 (2.00) 24 4.10 (2.30) 11.21 0.28 (–0.27 to 0.82) Turton, 199069 12 13.83 (6.00) 10 12.25 (7.20) 4.66 0.23 (–0.61 to 1.07) Van Vliet, 200570 42 3.88 (2.23) 43 3.69 (2.38) 18.30 0.08 (–0.34 to 0.51) Winstein, 200471 20 9.58 (5.70) 20 9.47 (6.30) 8.62 0.02 (–0.60 to 0.64) Yen, 200572 13 –2.57 (0.93) 17 –3.06 (1.54) 6.24 0.36 (–0.37 to 1.09)
Subtotal (95% CI) 205 207 87.66 0.17 (–0.03 to 0.36)Test for heterogeneity: �2 = 3.18, df = 7 (p = 0.87), I2 = 0%Test for overall effect: Z = 1.67 (p = 0.09)
02 CIMTAlberts, 200483 5 –28.89 (24.80) 5 –25.02 (17.96) 2.14 –0.16 (–1.40 to 1.08) Atteya, 200479 2 52.00 (6.00) 2 51.50 (10.50) 0.85 0.03 (–1.94 to 2.00) Dromerick, 200081 11 52.80 (5.90) 9 44.30 (11.10) 3.75 0.95 (0.01 to 1.89) Page, 200180 2 53.00 (6.00) 2 51.00 (10.00) 0.74 0.14 (–1.97 to 2.25) Page, 200582 5 49.80 (3.27) 5 35.80 (3.56) 0.56 3.70 (1.28 to 6.12) Taub, 199373 4 8.10 (0.42) 5 6.90 (0.70) 1.13 1.79 (0.07 to 3.50) Wittenberg, 200374 9 7.54 (2.04) 7 5.85 (2.79) 3.16 0.67 (–0.35 to 1.69)
Subtotal (95% CI) 38 35 12.34 0.77 (0.26 to 1.29)Test for heterogeneity: �2 = 10.18, df = 6 (p = 0.12), I2 = 41.0%Test for overall effect: Z = 2.93 (p = 0.003)
Total (95% CI) 243 242 100.00 0.24 (0.06 to 0.42)Test for heterogeneity: �2 = 17.99, df = 14 (p = 0.21), I2 = 22.2%Test for overall effect: Z = 2.59 (p = 0.010)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 2 Arm function

(I2 = 22.2%), although not sufficient to merit theuse of a random-effects approach.
Eight RTT trials recruited 467participants,50,52,53,68–72 with data available for 88%(n = 412) of participants. Ten CIMT trialsrecruiting 167 participants measured armfunction.61,62,64,73,74,79–83 In three of the CIMTtrials with 91 participants in total, data wereunsuitable for pooling.61,62,64 Page and colleagues(2002)61 included outcome data for nineparticipants, and provided means with nostandard deviations (ARAT: CIMT group meanchange +11.5, traditional therapy group meanchange +1.4). Page and colleagues (2004)62
included data for 13 participants, and alsoprovided means with no standard deviations(ARAT: CIMT group mean change +11.4,traditional therapy group mean change +7.1).Suputtitada and colleagues64 reported median andranges for 69 participants (ARAT: CIMT group
n = 33, median 55, range 30–57, control groupn = 36, median 47.5, range 15–54). Of theremaining seven CIMT trials with 76 participants,data were available for 96% (n = 73).
The pooled effect for the impact of RFTP on armfunction across all trials showed a small effect size,which was statistically significant: (SMD 0.24, 95% CI 0.06 to 0.42).
Hand functionSeven trials recruiting 357 participants measuredhand function, with data available for 86%(n = 307) (Figure 3). Five RTT trials recruited 324participants,50,52,68–70 with data available for 87%(n = 281) of participants. Two CIMT trials83,84
recruited 33 participants, with data available for79% (n = 26). The pooled effect for RFTP onhand function across all trials was small, andmarginally statistically non-significant (SMD 0.19,95% CI –0.03, 0.42).
Results of the review
20 FIGURE 3 Hand function
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 02 Upper limb functionOutcome: 02 Hand function
Studyor subcategory
Treatment Control SMD (fixed)(95% C)
Weight (%)
SMD (fixed)(95% CI)N Mean (SD) N Mean (SD)
01 RTT Blennerhassett, 200450
Higgins, 200652
Langhammer, 200068
Turton, 199069
Van Vliet, 200570
Subtotal (95% CI)Test for heterogeneity: �2 = 1.66, df = 4 (p = 0.80), I2 = 0%Test for overall effect: Z = 1.36 (p = 0.18)
02 CIMT Alberts, 200483
Boake, 200684
Subtotal (95% CI)Test for heterogeneity: �2 = 0.00, df = 1 (p = 0.99), I2 = 0%Test for overall effect: Z = 1.36 (p = 0.17)
Total (95% CI)Test for heterogeneity: �2 = 2.50, df = 6 (p = 0.87), I2 = 0%Test for overall effect: Z = 1.69 (p = 0.09)
9.9029.7117.10 7.19
28.04 91.93
3.11
8.07 4.96
100.00
–0.08 (–0.80 to 0.63) 0.28 (–0.13 to 0.70) 0.33 (–0.21 to 0.87)–0.11 (–0.95 to 0.73) 0.09 (–0.33 to 0.52) 0.16 (–0.07 to 0.40)
0.55 (–0.72 to 1.83) 0.55 (–0.47 to 1.56) 0.55 (–0.24 to 1.34)
0.19 (–0.03 to 0.42)
–4 –2 0 2 4
Favourscontrol
Favourstreatment
15 4.70 (2.50) 15 4.90 (2.10) 47 –9.00 (3.00) 44 –10.00 (4.00) 29 4.60 (1.90) 24 3.90 (2.30) 12 –43.50 (20.80) 10 –41.10 (20.10) 42 4.30 (2.41) 43 4.07 (2.56)145 136
5 –32.10 (49.90) 5 –65.40 (58.20) 9 0.08 (0.06) 7 0.04 (0.08) 14 12
159 148

Health Technology Assessment 2008; Vol. 12: No. 30
21
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Sitting balance/reachFive trials (all RTT) recruiting 256 participantsmeasured sitting balance or functional reach(Figure 4).66,68,70,76,77 Data were available for 82%(n = 210). There was some heterogeneity oftreatment effects (I2 = 32%), although notsufficient to merit the use of a random-effectsapproach.
The impact on sitting balance/reach showed asmall effect size that was not statistically significant(SMD 0.23, 95% CI –0.05 to 0.50).
Upper limb function: follow-upUnder 6 months post-therapyOne CIMT trial measuring hand function84 andtwo RTT trials measuring sitting balance,76,77
recruiting 78 participants in total, measured forretention effects between post-therapy and under 6 months post-therapy (Figure 5). Data were available for 86% (n = 67) and effects across trials were homogeneous
(I2 = 0%). There was a moderate effect size, which was statistically significant (SMD 0.55, 95% CI 0.06 to 1.04).
Between 6 and 12 months post-therapyFour trials50,68,70,71 (all RTT) recruiting 254participants measured arm function for retentioneffects between 6 and 12 months post-therapy(Figure 5). Data were available for 76% (n = 195).Effects across trials were homogeneous (I2 = 0%).Results showed no effect of treatment (SMD –0.02,95% CI –0.31 to 0.26).
Subgroup analysis: upper limb functionSubgroup analyses for upper limb interventionsare based on trials providing measures of armfunction. Trials that only provide measures ofhand function84 or sitting balance/reach66,76,77 aretherefore excluded. Subgroup analyses arepresented for type, amount and timing ofintervention, and to consider the impact of
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 02 Upper limb function Outcome: 03 Sitting balance/reach
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 RTTde Sèze 200176 10 3.30 (0.80) 10 3.00 (0.80) 9.61 0.36 (–0.53 to 1.24)Dean 199766 10 12.00 (0.95) 9 10.80 (0.90) 7.49 1.24 (0.23 to 2.24)Howe 200577 15 –1.90 (0.80) 18 –2.10 (0.70) 15.89 0.26 (–0.43 to 0.95)Langhammer 200068 29 5.40 (0.90) 24 5.00 (1.50) 25.38 0.33 (–0.22 to 0.87)Van Vliet 200570 42 4.54 (1.49) 43 4.63 (1.42) 41.63 –0.06 (–0.49 to 0.36)
Subtotal (95% CI) 106 104 100.00 0.23 (–0.05 to 0.50)Test for heterogeneity: �2 = 5.88, df = 4 (p = 0.21), I2 = 32.0%Test for overall effect: Z = 1.61 (p = 0.11)
Total (95% CI) 106 104 100.00 0.23 (–0.05 to 0.50)Test for heterogeneity: �2 = 5.88, df = 4 (p = 0.21), I2 = 32.0%Test for overall effect: Z = 1.61 (p = 0.11)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 4 Sitting balance/reach

specific trial features on the results. Theclassification of trials for each subgroup analysis isgiven in Appendix 6.
Type of interventionSubgroups compared the treatment effects foreight RTT trials recruiting 467 participants, andseven CIMT trials recruiting 76 participants(Figure 6). The impact of RTT on upper limb
function post-treatment just failed to reachstatistical significance (SMD 0.17, 95% CI –0.03 to0.36). The impact of CIMT on arm functionshowed some heterogeneity (I2 = 41%), but notsufficient to necessitate the use of a random-effectsapproach. There was a large and statisticallysignificant effect size (SMD 0.77, 95% CI 0.26 to1.29). The difference between effect sizes for CIMTand RTT was statistically significant (p = 0.03).
Results of the review
22
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 02 Upper limb function Outcome: 04 Follow-up
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 Under 6 months post-therapyBoake, 200684 9 0.16 (0.06) 7 0.10 (0.10) 5.65 0.71 (–0.32 to 1.74)de Sèze, 200176 10 3.60 (0.50) 10 3.40 (0.60) 7.62 0.35 (–0.54 to 1.23)Howe, 200577 15 2.50 (1.30) 16 1.90 (0.50) 11.43 0.60 (–0.12 to 1.32)
Subtotal (95% CI) 34 33 24.70 0.55 (0.06 to 1.04)Test for heterogeneity: �2 = 0.32, df = 2 (p = 0.85), I2 = 0%Test for overall effect: Z = 2.19 (p = 0.03)
02 6–12 months post-therapyBlennerhassett, 200450 10 –23.60 (12.20) 11 –31.00 (33.20) 8.04 0.28 (–0.58 to 1.14)Langhammer, 200068 27 3.90 (2.50) 27 3.50 (2.80) 20.90 0.15 (–0.39 to 0.68)Van Vliet, 200570 42 3.45 (2.40) 45 3.77 (2.37) 33.65 –0.13 (–0.55 to 0.29)Winstein, 200471 17 9.67 (5.80) 16 10.98 (6.20) 12.72 –0.21 (–0.90 to 0.47)
Subtotal (95% CI) 96 99 75.30 –0.02 (–0.31 to 0.26)Test for heterogeneity: �2 = 1.42, df = 3 (p = 0.70), I2 = 0%Test for overall effect: Z = 0.17 (p = 0.86)
–10 –5 0 5 10
Favours control Favours treatment
FIGURE 5 Arm function: follow-up at 0–6 months and more than 6 months post-therapy
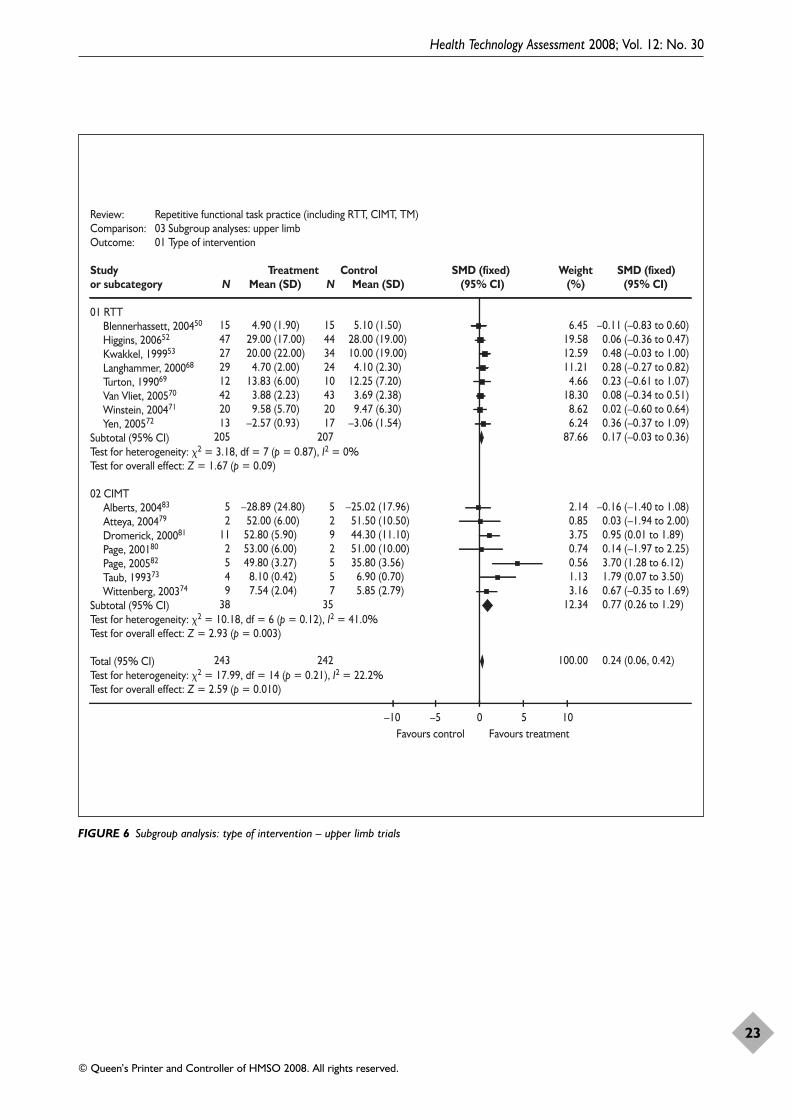
Health Technology Assessment 2008; Vol. 12: No. 30
23
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 03 Subgroup analyses: upper limb Outcome: 01 Type of intervention
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 RTTBlennerhassett, 200450 15 4.90 (1.90) 15 5.10 (1.50) 6.45 –0.11 (–0.83 to 0.60)Higgins, 200652 47 29.00 (17.00) 44 28.00 (19.00) 19.58 0.06 (–0.36 to 0.47)Kwakkel, 199953 27 20.00 (22.00) 34 10.00 (19.00) 12.59 0.48 (–0.03 to 1.00)Langhammer, 200068 29 4.70 (2.00) 24 4.10 (2.30) 11.21 0.28 (–0.27 to 0.82)Turton, 199069 12 13.83 (6.00) 10 12.25 (7.20) 4.66 0.23 (–0.61 to 1.07)Van Vliet, 200570 42 3.88 (2.23) 43 3.69 (2.38) 18.30 0.08 (–0.34 to 0.51)Winstein, 200471 20 9.58 (5.70) 20 9.47 (6.30) 8.62 0.02 (–0.60 to 0.64)Yen, 200572 13 –2.57 (0.93) 17 –3.06 (1.54) 6.24 0.36 (–0.37 to 1.09)
Subtotal (95% CI) 205 207 87.66 0.17 (–0.03 to 0.36)Test for heterogeneity: �2 = 3.18, df = 7 (p = 0.87), I2 = 0%Test for overall effect: Z = 1.67 (p = 0.09)
02 CIMTAlberts, 200483 5 –28.89 (24.80) 5 –25.02 (17.96) 2.14 –0.16 (–1.40 to 1.08)Atteya, 200479 2 52.00 (6.00) 2 51.50 (10.50) 0.85 0.03 (–1.94 to 2.00)Dromerick, 200081 11 52.80 (5.90) 9 44.30 (11.10) 3.75 0.95 (0.01 to 1.89)Page, 200180 2 53.00 (6.00) 2 51.00 (10.00) 0.74 0.14 (–1.97 to 2.25)Page, 200582 5 49.80 (3.27) 5 35.80 (3.56) 0.56 3.70 (1.28 to 6.12)Taub, 199373 4 8.10 (0.42) 5 6.90 (0.70) 1.13 1.79 (0.07 to 3.50)Wittenberg, 200374 9 7.54 (2.04) 7 5.85 (2.79) 3.16 0.67 (–0.35 to 1.69)
Subtotal (95% CI) 38 35 12.34 0.77 (0.26 to 1.29)Test for heterogeneity: �2 = 10.18, df = 6 (p = 0.12), I2 = 41.0%Test for overall effect: Z = 2.93 (p = 0.003)
Total (95% CI) 243 242 100.00 0.24 (0.06, 0.42)Test for heterogeneity: �2 = 17.99, df = 14 (p = 0.21), I2 = 22.2%Test for overall effect: Z = 2.59 (p = 0.010)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 6 Subgroup analysis: type of intervention – upper limb trials
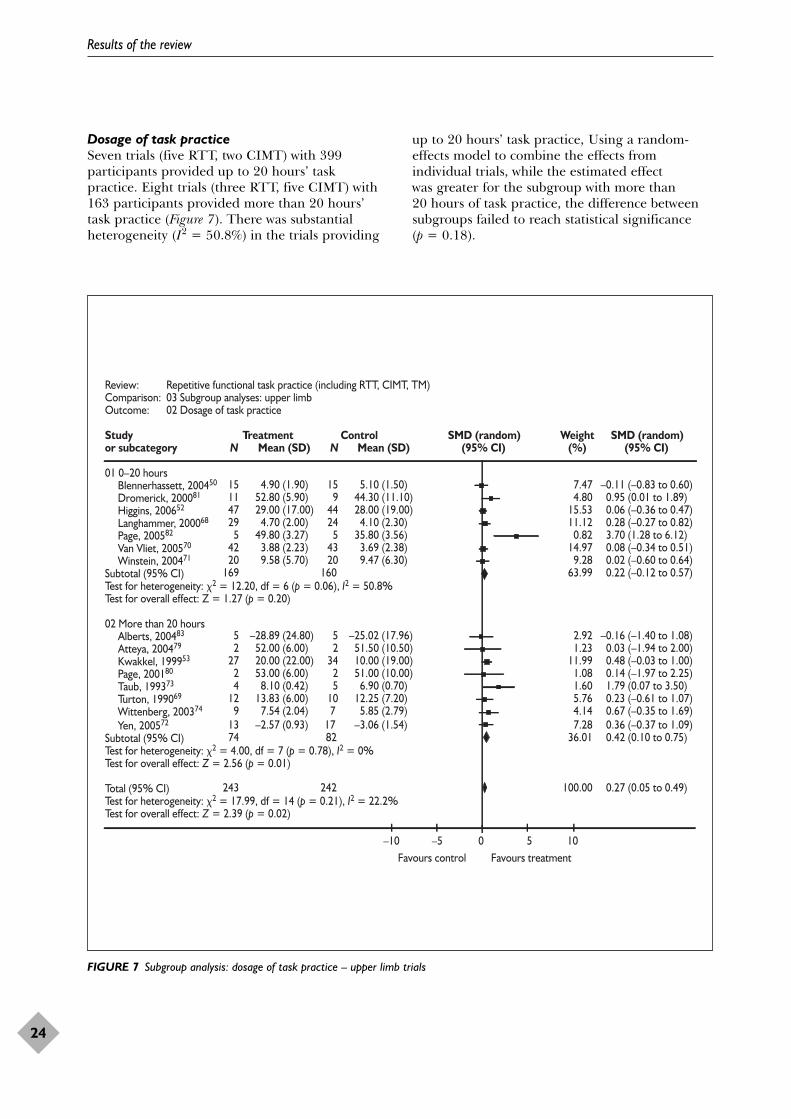
Dosage of task practiceSeven trials (five RTT, two CIMT) with 399participants provided up to 20 hours’ taskpractice. Eight trials (three RTT, five CIMT) with163 participants provided more than 20 hours’task practice (Figure 7). There was substantialheterogeneity (I2 = 50.8%) in the trials providing
up to 20 hours’ task practice, Using a random-effects model to combine the effects fromindividual trials, while the estimated effect was greater for the subgroup with more than 20 hours of task practice, the difference betweensubgroups failed to reach statistical significance(p = 0.18).
Results of the review
24
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 03 Subgroup analyses: upper limbOutcome: 02 Dosage of task practice
Study Treatment Control SMD (random) Weight SMD (random)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 0–20 hoursBlennerhassett, 200450 15 4.90 (1.90) 15 5.10 (1.50) 7.47 –0.11 (–0.83 to 0.60) Dromerick, 200081 11 52.80 (5.90) 9 44.30 (11.10) 4.80 0.95 (0.01 to 1.89) Higgins, 200652 47 29.00 (17.00) 44 28.00 (19.00) 15.53 0.06 (–0.36 to 0.47) Langhammer, 200068 29 4.70 (2.00) 24 4.10 (2.30) 11.12 0.28 (–0.27 to 0.82) Page, 200582 5 49.80 (3.27) 5 35.80 (3.56) 0.82 3.70 (1.28 to 6.12) Van Vliet, 200570 42 3.88 (2.23) 43 3.69 (2.38) 14.97 0.08 (–0.34 to 0.51) Winstein, 200471 20 9.58 (5.70) 20 9.47 (6.30) 9.28 0.02 (–0.60 to 0.64)
Subtotal (95% CI) 169 160 63.99 0.22 (–0.12 to 0.57)Test for heterogeneity: �2 = 12.20, df = 6 (p = 0.06), I2 = 50.8%Test for overall effect: Z = 1.27 (p = 0.20)
02 More than 20 hoursAlberts, 200483 5 –28.89 (24.80) 5 –25.02 (17.96) 2.92 –0.16 (–1.40 to 1.08) Atteya, 200479 2 52.00 (6.00) 2 51.50 (10.50) 1.23 0.03 (–1.94 to 2.00) Kwakkel, 199953 27 20.00 (22.00) 34 10.00 (19.00) 11.99 0.48 (–0.03 to 1.00) Page, 200180 2 53.00 (6.00) 2 51.00 (10.00) 1.08 0.14 (–1.97 to 2.25) Taub, 199373 4 8.10 (0.42) 5 6.90 (0.70) 1.60 1.79 (0.07 to 3.50) Turton, 199069 12 13.83 (6.00) 10 12.25 (7.20) 5.76 0.23 (–0.61 to 1.07) Wittenberg, 200374 9 7.54 (2.04) 7 5.85 (2.79) 4.14 0.67 (–0.35 to 1.69) Yen, 200572 13 –2.57 (0.93) 17 –3.06 (1.54) 7.28 0.36 (–0.37 to 1.09)
Subtotal (95% CI) 74 82 36.01 0.42 (0.10 to 0.75)Test for heterogeneity: �2 = 4.00, df = 7 (p = 0.78), I2 = 0%Test for overall effect: Z = 2.56 (p = 0.01)
Total (95% CI) 243 242 100.00 0.27 (0.05 to 0.49)Test for heterogeneity: �2 = 17.99, df = 14 (p = 0.21), I2 = 22.2%Test for overall effect: Z = 2.39 (p = 0.02)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 7 Subgroup analysis: dosage of task practice – upper limb trials
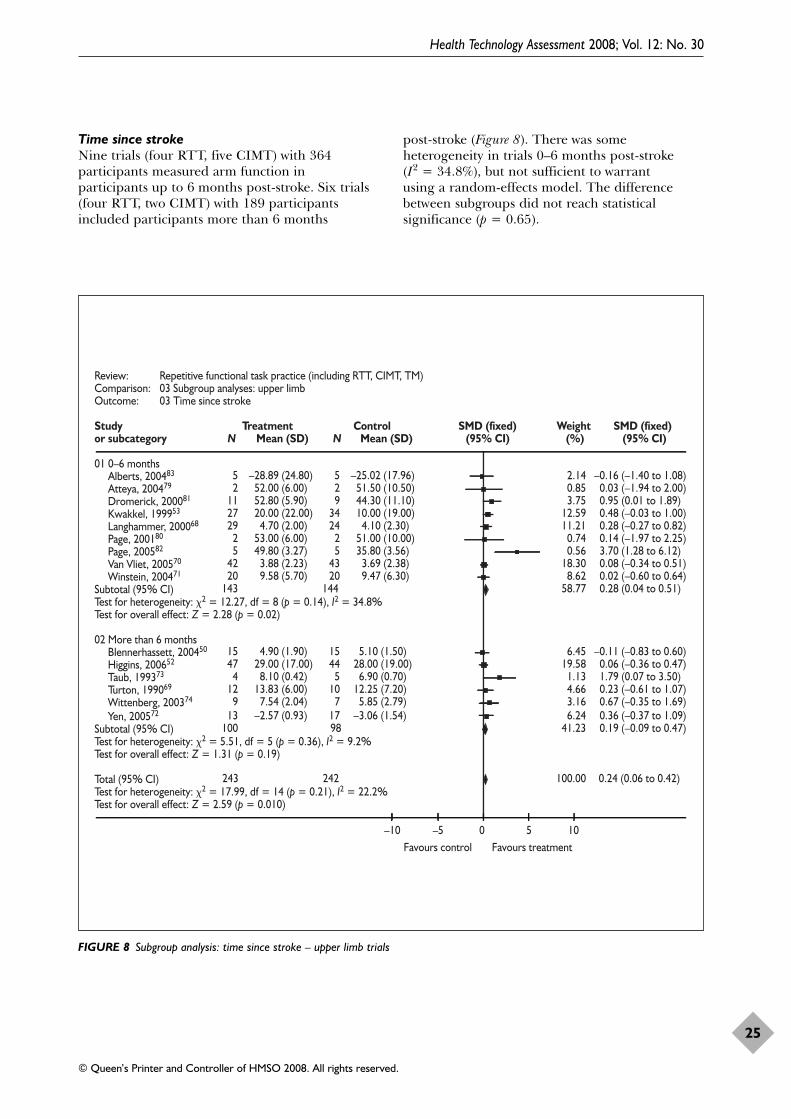
Time since strokeNine trials (four RTT, five CIMT) with 364participants measured arm function in participants up to 6 months post-stroke. Six trials(four RTT, two CIMT) with 189 participantsincluded participants more than 6 months
post-stroke (Figure 8). There was someheterogeneity in trials 0–6 months post-stroke (I2 = 34.8%), but not sufficient to warrant using a random-effects model. The differencebetween subgroups did not reach statisticalsignificance (p = 0.65).
Health Technology Assessment 2008; Vol. 12: No. 30
25
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 03 Subgroup analyses: upper limb Outcome: 03 Time since stroke
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 0–6 monthsAlberts, 200483 5 –28.89 (24.80) 5 –25.02 (17.96) 2.14 –0.16 (–1.40 to 1.08) Atteya, 200479 2 52.00 (6.00) 2 51.50 (10.50) 0.85 0.03 (–1.94 to 2.00) Dromerick, 200081 11 52.80 (5.90) 9 44.30 (11.10) 3.75 0.95 (0.01 to 1.89) Kwakkel, 199953 27 20.00 (22.00) 34 10.00 (19.00) 12.59 0.48 (–0.03 to 1.00) Langhammer, 200068 29 4.70 (2.00) 24 4.10 (2.30) 11.21 0.28 (–0.27 to 0.82) Page, 200180 2 53.00 (6.00) 2 51.00 (10.00) 0.74 0.14 (–1.97 to 2.25) Page, 200582 5 49.80 (3.27) 5 35.80 (3.56) 0.56 3.70 (1.28 to 6.12) Van Vliet, 200570 42 3.88 (2.23) 43 3.69 (2.38) 18.30 0.08 (–0.34 to 0.51) Winstein, 200471 20 9.58 (5.70) 20 9.47 (6.30) 8.62 0.02 (–0.60 to 0.64)
Subtotal (95% CI) 143 144 58.77 0.28 (0.04 to 0.51)Test for heterogeneity: �2 = 12.27, df = 8 (p = 0.14), I2 = 34.8%Test for overall effect: Z = 2.28 (p = 0.02)
02 More than 6 monthsBlennerhassett, 200450 15 4.90 (1.90) 15 5.10 (1.50) 6.45 –0.11 (–0.83 to 0.60) Higgins, 200652 47 29.00 (17.00) 44 28.00 (19.00) 19.58 0.06 (–0.36 to 0.47) Taub, 199373 4 8.10 (0.42) 5 6.90 (0.70) 1.13 1.79 (0.07 to 3.50) Turton, 199069 12 13.83 (6.00) 10 12.25 (7.20) 4.66 0.23 (–0.61 to 1.07) Wittenberg, 200374 9 7.54 (2.04) 7 5.85 (2.79) 3.16 0.67 (–0.35 to 1.69) Yen, 200572 13 –2.57 (0.93) 17 –3.06 (1.54) 6.24 0.36 (–0.37 to 1.09)
Subtotal (95% CI) 100 98 41.23 0.19 (–0.09 to 0.47)Test for heterogeneity: �2 = 5.51, df = 5 (p = 0.36), I2 = 9.2%Test for overall effect: Z = 1.31 (p = 0.19)
Total (95% CI) 243 242 100.00 0.24 (0.06 to 0.42)Test for heterogeneity: �2 = 17.99, df = 14 (p = 0.21), I2 = 22.2%Test for overall effect: Z = 2.59 (p = 0.010)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 8 Subgroup analysis: time since stroke – upper limb trials
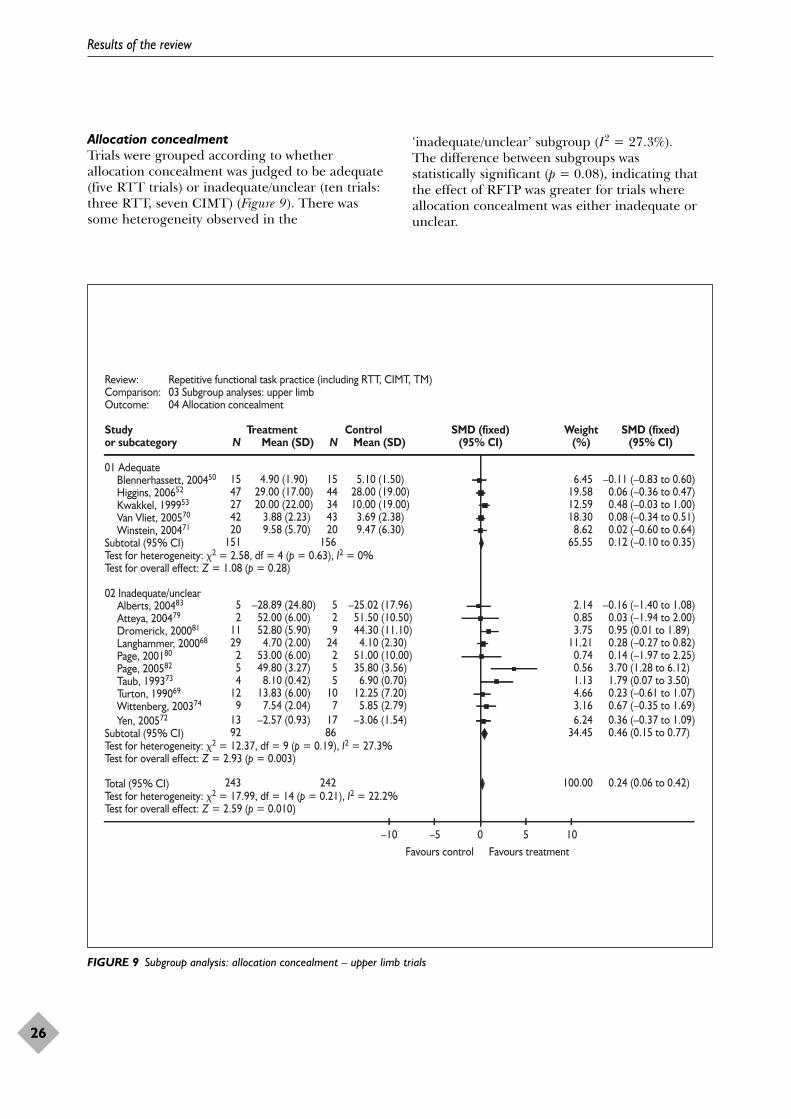
Allocation concealmentTrials were grouped according to whetherallocation concealment was judged to be adequate(five RTT trials) or inadequate/unclear (ten trials:three RTT, seven CIMT) (Figure 9). There wassome heterogeneity observed in the
‘inadequate/unclear’ subgroup (I2 = 27.3%). The difference between subgroups was statistically significant (p = 0.08), indicating thatthe effect of RFTP was greater for trials whereallocation concealment was either inadequate orunclear.
Results of the review
26
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 03 Subgroup analyses: upper limb Outcome: 04 Allocation concealment
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 AdequateBlennerhassett, 200450 15 4.90 (1.90) 15 5.10 (1.50) 6.45 –0.11 (–0.83 to 0.60) Higgins, 200652 47 29.00 (17.00) 44 28.00 (19.00) 19.58 0.06 (–0.36 to 0.47) Kwakkel, 199953 27 20.00 (22.00) 34 10.00 (19.00) 12.59 0.48 (–0.03 to 1.00) Van Vliet, 200570 42 3.88 (2.23) 43 3.69 (2.38) 18.30 0.08 (–0.34 to 0.51) Winstein, 200471 20 9.58 (5.70) 20 9.47 (6.30) 8.62 0.02 (–0.60 to 0.64)
Subtotal (95% CI) 151 156 65.55 0.12 (–0.10 to 0.35)Test for heterogeneity: �2 = 2.58, df = 4 (p = 0.63), I2 = 0%Test for overall effect: Z = 1.08 (p = 0.28)
02 Inadequate/unclearAlberts, 200483 5 –28.89 (24.80) 5 –25.02 (17.96) 2.14 –0.16 (–1.40 to 1.08) Atteya, 200479 2 52.00 (6.00) 2 51.50 (10.50) 0.85 0.03 (–1.94 to 2.00) Dromerick, 200081 11 52.80 (5.90) 9 44.30 (11.10) 3.75 0.95 (0.01 to 1.89) Langhammer, 200068 29 4.70 (2.00) 24 4.10 (2.30) 11.21 0.28 (–0.27 to 0.82) Page, 200180 2 53.00 (6.00) 2 51.00 (10.00) 0.74 0.14 (–1.97 to 2.25) Page, 200582 5 49.80 (3.27) 5 35.80 (3.56) 0.56 3.70 (1.28 to 6.12) Taub, 199373 4 8.10 (0.42) 5 6.90 (0.70) 1.13 1.79 (0.07 to 3.50) Turton, 199069 12 13.83 (6.00) 10 12.25 (7.20) 4.66 0.23 (–0.61 to 1.07) Wittenberg, 200374 9 7.54 (2.04) 7 5.85 (2.79) 3.16 0.67 (–0.35 to 1.69) Yen, 200572 13 –2.57 (0.93) 17 –3.06 (1.54) 6.24 0.36 (–0.37 to 1.09)
Subtotal (95% CI) 92 86 34.45 0.46 (0.15 to 0.77)Test for heterogeneity: �2 = 12.37, df = 9 (p = 0.19), I2 = 27.3%Test for overall effect: Z = 2.93 (p = 0.003)
Total (95% CI) 243 242 100.00 0.24 (0.06 to 0.42)Test for heterogeneity: �2 = 17.99, df = 14 (p = 0.21), I2 = 22.2%Test for overall effect: Z = 2.59 (p = 0.010)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 9 Subgroup analysis: allocation concealment – upper limb trials

Post hoc analysis: type of comparison groupSeven trials (five RTT, two CIMT) were classified as usual care or alternative treatment,and eight trials (three RTT, five CIMT) wereclassified as attention-control or no treatment
(Figure 10), with some heterogeneity observed in trials with usual care/alternative treatmentcontrols (I2 =46.1%). There was no statisticallysignificant difference between subgroups(p = 0.84).
Health Technology Assessment 2008; Vol. 12: No. 30
27
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 03 Subgroup analyses: upper limbOutcome: 05 Comparison group
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 Usual care/alternative treatmentDromerick, 200081 11 52.80 (5.90) 9 44.30 (11.10) 3.75 0.95 (0.01 to 1.89) Langhammer, 200068 29 4.70 (2.00) 24 4.10 (2.30) 11.21 0.28 (–0.27 to 0.82) Page, 200582 5 49.80 (3.27) 5 35.80 (3.56) 0.56 3.70 (1.28 to 6.12) Turton, 199069 12 13.83 (6.00) 10 12.25 (7.20) 4.66 0.23 (–0.61 to 1.07) Van Vliet, 200570 42 3.88 (2.23) 43 3.69 (2.38) 18.30 0.08 (–0.34 to 0.51) Winstein, 200471 20 9.58 (5.70) 20 9.47 (6.30) 8.62 0.02 (–0.60 to 0.64) Yen, 200572 13 –2.57 (0.93) 17 –3.06 (1.54) 6.24 0.36 (–0.37 to 1.09)
Subtotal (95% CI) 132 128 53.35 0.26 (0.01 to 0.51)Test for heterogeneity: �2 = 11.13, df = 6 (p = 0.08), I2 = 46.1%Test for overall effect: Z = 2.02 (p = 0.04)
02 Attention control/no treatmentAlberts, 200483 5 –28.89 (24.80) 5 –25.02 (17.96) 2.14 –0.16 (–1.40 to 1.08) Atteya, 200479 2 52.00 (6.00) 2 1.50 (10.50) 0.85 0.03 (–1.94 to 2.00) Blennerhassett, 200450 15 4.90 (1.90) 15 5.10 (1.50) 6.45 –0.11 (–0.83 to 0.60) Higgins, 200652 47 29.00 (17.00) 44 28.00 (19.00) 19.58 0.06 (–0.36 to 0.47) Kwakkel, 199953 27 20.00 (22.00) 34 10.00 (19.00) 12.59 0.48 (–0.03 to 1.00) Page, 200180 2 53.00 (6.00) 2 51.00 (10.00) 0.74 0.14 (–1.97 to 2.25) Taub, 199373 4 8.10 (0.42) 5 6.90 (0.70) 1.13 1.79 (0.07 to 3.50) Wittenberg, 200374 9 7.54 (2.04) 7 5.85 (2.79) 3.16 0.67 (–0.35 to 1.69)
Subtotal (95% CI) 111 114 46.65 0.22 (–0.04 to 0.49)Test for heterogeneity: �2 = 6.82, df = 7 (p = 0.45), I2 = 0%Test for overall effect: Z = 1.63 (p = 0.10)
Total (95% CI) 243 242 100.00 0.24 (0.06 to 0.42)Test for heterogeneity: �2 = 17.99, df = 14 (p = 0.21), I2 = 22.2%Test for overall effect: Z = 2.59 (p = 0.010)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 10 Subgroup analysis: type of comparison group – upper limb trials

Post hoc analysis: equivalence of therapy timeOne subgroup comprised seven trials (two RTT,five CIMT) which gave, additional therapy time tothe experimental group, and the other containedeight trials (six RTT, two CIMT) where therapytime for experimental and control groups wasequivalent (Figure 11). There was someheterogeneity of treatment effects in eachsubgroup, but not sufficient to merit the use of arandom-effects meta-analysis. There was nosignificant difference between the two subgroups (p = 0.92).
Post hoc analysis: trial size The median number of participants in the trialswas 23. A post hoc analysis was thereforeundertaken for trials with under 25 participants
versus those with 25 or more participants(Figure 12). Some heterogeneity was observed intrials with under 25 participants (I2 = 38.2%), but not enough to warrant the use of a random-effects model. The difference between effect sizesin the small trial sub-group (<25 participants) andthe larger trial sub-group (�25 participants) wasstatistically significant (p = 0.06). As the effect inthe small trial subgroup (SMD 0.62, 95% CI 0.18to 1.07) is significantly larger than in the largertrial subgroup (SMD 0.16, 95% CI –0.04 to 0.36),this may indicate some degree of reporting bias inupper limb trials. This is supported by the funnelplot in Figure 13, which has some apparentasymmetry indicating a potential lack of reporting of small negative trials with largestandard errors.
Results of the review
28
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 03 Subgroup analyses: upper limbOutcome: 06 Equivalence of therapy time
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 Additional therapy timeAlberts, 200483 5 –28.89 (24.80) 5 –25.02 (17.96) 2.14 –0.16 (–1.40 to 1.08) Atteya, 200479 2 52.00 (6.00) 2 51.50 (10.50) 0.85 0.03 (–1.94 to 2.00) Page, 200180 2 53.00 (6.00) 2 51.00 (10.00) 0.74 0.14 (–1.97 to 2.25) Page, 200582 5 49.80 (3.27) 5 35.80 (3.56) 0.56 3.70 (1.28 to 6.12) Turton, 199069 12 13.83 (6.00) 10 12.25 (7.20) 4.66 0.23 (–0.61 to 1.07) Winstein, 200471 20 9.58 (5.70) 20 9.47 (6.30) 8.62 0.02 (–0.60 to 0.64) Wittenberg, 200374 9 7.54 (2.04) 7 5.85 (2.79) 3.16 0.67 (–0.35 to 1.69)
Subtotal (95% CI) 55 51 20.76 0.25 (–0.15 to 0.65)Test for heterogeneity: �2 = 9.44, df = 6 (p = 0.15), I2 = 36.5%Test for overall effect: Z = 1.23 (p = 0.22)
02 Equivalent therapy timeBlennerhassett, 200450 15 4.90 (1.90) 15 5.10 (1.50) 6.45 –0.11 (–0.83 to 0.60) Dromerick, 200081 11 52.80 (5.90) 9 44.30 (11.10) 3.75 0.95 (0.01 to 1.89) Higgins, 200652 47 29.00 (17.00) 44 28.00 (19.00) 19.58 0.06 (–0.36 to 0.47) Kwakkel, 199953 27 20.00 (22.00) 34 10.00 (19.00) 12.59 0.48 (–0.03 to 1.00) Langhammer, 200068 29 4.70 (2.00) 24 4.10 (2.30) 11.21 0.28 (–0.27 to 0.82) Taub, 199373 4 8.10 (0.42) 5 6.90 (0.70) 1.13 1.79 (0.07 to 3.50) Van Vliet, 200570 42 3.88 (2.23) 43 3.69 (2.38) 18.30 0.08 (–0.34 to 0.51) Yen, 200572 13 –2.57 (0.93) 17 –3.06 (1.54) 6.24 0.36 (–0.37 to 1.09)
Subtotal (95% CI) 188 191 79.24 0.24 (0.03 to 0.44)Test for heterogeneity: �2 = 8.54, df = 7 (p = 0.29), I2 = 18.0%Test for overall effect: Z = 2.28 (p = 0.02)
Total (95% CI) 243 242 100.00 0.24 (0.06 to 0.42)Test for heterogeneity: �2 = 17.99, df = 14 (p = 0.21), I2 = 22.2%Test for overall effect: Z = 2.59 (p = 0.010)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 11 Subgroup analysis: equivalence of therapy time – upper limb trials
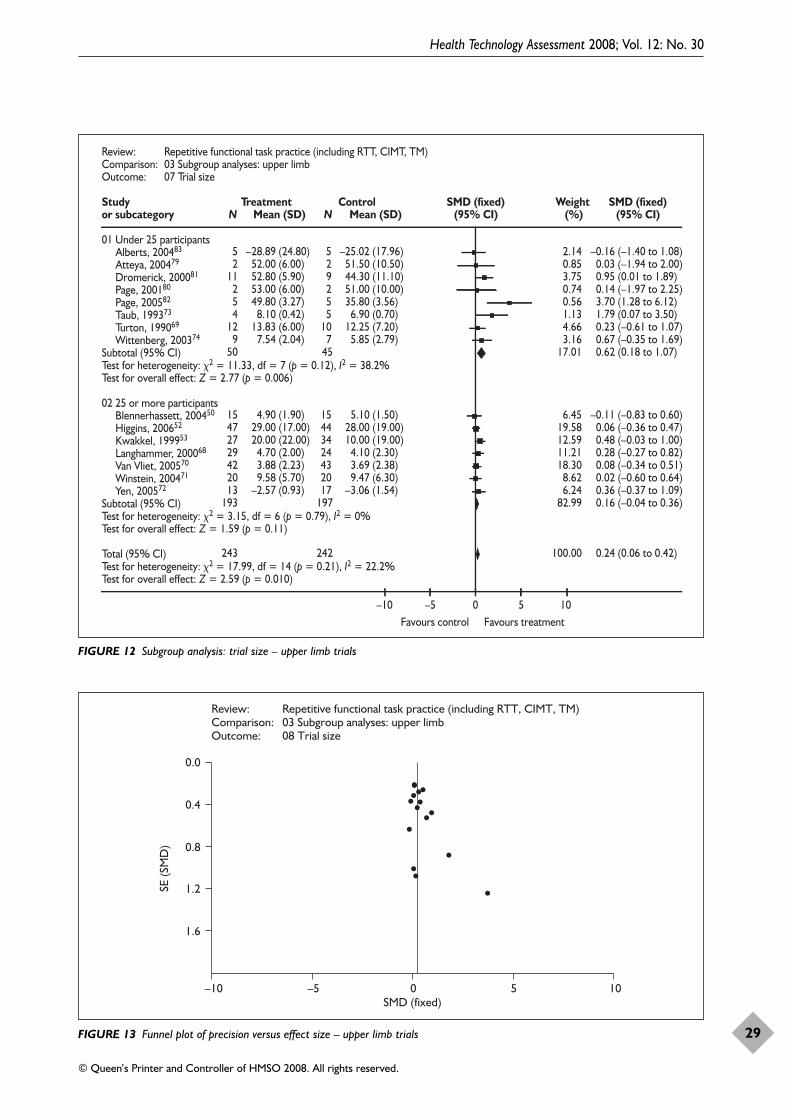
Health Technology Assessment 2008; Vol. 12: No. 30
29
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 03 Subgroup analyses: upper limbOutcome: 07 Trial size
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 Under 25 participantsAlberts, 200483 5 –28.89 (24.80) 5 –25.02 (17.96) 2.14 –0.16 (–1.40 to 1.08) Atteya, 200479 2 52.00 (6.00) 2 51.50 (10.50) 0.85 0.03 (–1.94 to 2.00) Dromerick, 200081 11 52.80 (5.90) 9 44.30 (11.10) 3.75 0.95 (0.01 to 1.89) Page, 200180 2 53.00 (6.00) 2 51.00 (10.00) 0.74 0.14 (–1.97 to 2.25) Page, 200582 5 49.80 (3.27) 5 35.80 (3.56) 0.56 3.70 (1.28 to 6.12) Taub, 199373 4 8.10 (0.42) 5 6.90 (0.70) 1.13 1.79 (0.07 to 3.50) Turton, 199069 12 13.83 (6.00) 10 12.25 (7.20) 4.66 0.23 (–0.61 to 1.07) Wittenberg, 200374 9 7.54 (2.04) 7 5.85 (2.79) 3.16 0.67 (–0.35 to 1.69)
Subtotal (95% CI) 50 45 17.01 0.62 (0.18 to 1.07)Test for heterogeneity: �2 = 11.33, df = 7 (p = 0.12), I2 = 38.2%Test for overall effect: Z = 2.77 (p = 0.006)
02 25 or more participantsBlennerhassett, 200450 15 4.90 (1.90) 15 5.10 (1.50) 6.45 –0.11 (–0.83 to 0.60) Higgins, 200652 47 29.00 (17.00) 44 28.00 (19.00) 19.58 0.06 (–0.36 to 0.47) Kwakkel, 199953 27 20.00 (22.00) 34 10.00 (19.00) 12.59 0.48 (–0.03 to 1.00) Langhammer, 200068 29 4.70 (2.00) 24 4.10 (2.30) 11.21 0.28 (–0.27 to 0.82) Van Vliet, 200570 42 3.88 (2.23) 43 3.69 (2.38) 18.30 0.08 (–0.34 to 0.51) Winstein, 200471 20 9.58 (5.70) 20 9.47 (6.30) 8.62 0.02 (–0.60 to 0.64) Yen, 200572 13 –2.57 (0.93) 17 –3.06 (1.54) 6.24 0.36 (–0.37 to 1.09)
Subtotal (95% CI) 193 197 82.99 0.16 (–0.04 to 0.36)Test for heterogeneity: �2 = 3.15, df = 6 (p = 0.79), I2 = 0%Test for overall effect: Z = 1.59 (p = 0.11)
Total (95% CI) 243 242 100.00 0.24 (0.06 to 0.42)Test for heterogeneity: �2 = 17.99, df = 14 (p = 0.21), I2 = 22.2%Test for overall effect: Z = 2.59 (p = 0.010)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 12 Subgroup analysis: trial size – upper limb trials
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 03 Subgroup analyses: upper limb Outcome: 08 Trial size
–10 –5 0 5 10
0.0
0.4
0.8
1.2
1.6
SE (S
MD
)
SMD (fixed)
FIGURE 13 Funnel plot of precision versus effect size – upper limb trials

Results of the review
30
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 04 Lower limb functionOutcome: 01 Walking distance
Study Treatment Control WMD (random) Weight WMD (random)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 RTTBlennerhassett, 200450 15 221.00 (65.40) 15 107.00 (85.60) 9.81 114.00 (59.49 to 168.52) Dean, 200067 5 42.03 (30.42) 4 4.76 (4.90) 20.79 37.27 (10.18 to 64.36) Salbach, 200451 44 40.00 (72.00) 47 5.00 (66.00) 20.04 35.00 (6.56 to 63.44)
Subtotal (95% CI) 64 66 50.65 54.59 (17.50 to 91.68)Test for heterogeneity: �2 = 6.94, df = 2 (p = 0.03), I2 = 71.2%Test for overall effect: Z = 2.88 (p = 0.004)
02 TMAda, 200387 11 99.00 (70.00) 14 13.00 (27.00) 13.09 86.00 (42.28 to 129.72) da Cunha, 200286 6 107.00 (71.52) 7 51.58 (63.00) 6.19 55.42 (–18.42 to 129.26) Eich, 200489 25 90.60 (43.50) 25 55.70 (32.60) 24.17 34.90 (13.59 to 56.21) Macko, 200588 25 281.03 (120.00) 20 264.57 (136.31) 5.90 16.46 (–59.58 to 92.50)
Subtotal (95% CI) 67 66 49.35 48.88 (19.56 to 78.20)Test for heterogeneity: �2 = 4.84, df = 3 (p = 0.18), I2 = 38.0%Test for overall effect: Z = 3.27 (p = 0.001)
Total (95% CI) 131 132 100.00 50.05 (29.65 to 70.44)Test for heterogeneity: �2 = 11.79, df = 6 (p = 0.07), I2 = 49.1%Test for overall effect: Z = 4.81 (p < 0.00001)
–1000 –500 0 500 1000 Favours control Favours treatment
FIGURE 14 Walking distance
Lower limb function: post-therapyResults are presented for walking distance, walkingspeed, functional ambulation, sit-to-stand, lowerlimb functional measures and standingbalance/reach. All results are post-therapy, exceptfor Langhammer and Stanghelle,68 which is3 months post-stroke, and Van Vliet andcolleagues,70 which is 3 months post-baseline.
Walking distanceSeven trials included a measure of walkingdistance (Figure 14). All results are change frombaseline scores except for Macko and colleagues,88
and are expressed as metres walked in 6 minutes.The degree of heterogeneity (I2 = 49.1%) in theeffect sizes of the seven trials was very close to thestudy criterion for ‘substantial’ heterogeneity, so arandom-effects model was used. Three RTTtrials50,51,67 recruiting 133 participants measuredwalking distance, with outcome data available for98% (n = 130) of participants. Four TM trials86–89
recruiting 155 participants measured walkingdistance, with outcome data available for 96%(n = 149).
For RFTP overall, pooled results showed astatistically significant difference (WMD 50.05 m,95% CI 29.65 to 70.44 m). Owing to the lack ofhomogeneity of standard deviations, resulting in asubstantial impact on the weighting of severaltrials, results were reanalysed using the SMD and arandom-effects model. The result showed a largeeffect size, which remained highly statisticallysignificant (SMD 0.98, 95% CI 0.58 to 1.39,excluding Macko and colleagues,88 which did notprovide ‘change-from-baseline’ data). To improvecomparability with effect sizes for other outcomesand for use in the economic analysis, the SMDbased on the post-treatment data from the seventrials was also computed (SMD 0.45, 95% CI 0.20to 0.70; figure not shown). As expected, the SMDbased on the post-treatment data is considerablysmaller than that based on the change-from-baseline data, primarily owing to its poorersensitivity to change.
Walking speedTen trials included a measure of walking speed(Figure 15). Results were converted into metres per
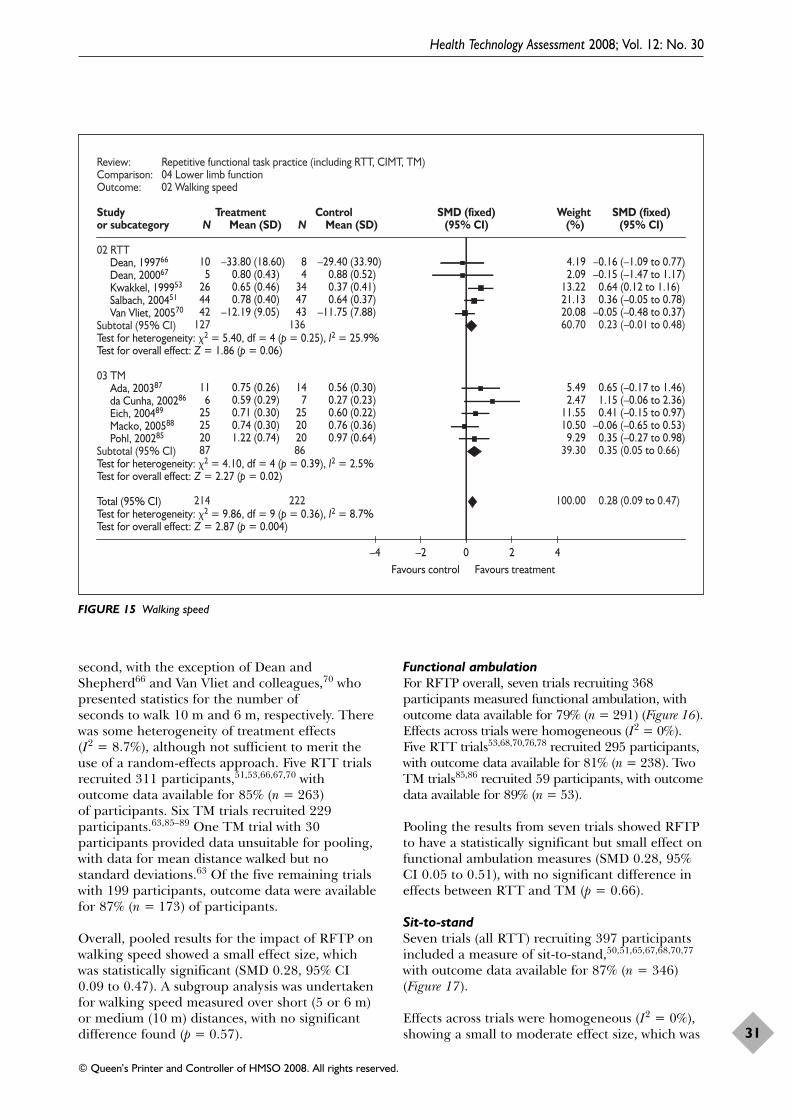
Health Technology Assessment 2008; Vol. 12: No. 30
31
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 04 Lower limb functionOutcome: 02 Walking speed
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
02 RTTDean, 199766 10 –33.80 (18.60) 8 –29.40 (33.90) 4.19 –0.16 (–1.09 to 0.77) Dean, 200067 5 0.80 (0.43) 4 0.88 (0.52) 2.09 –0.15 (–1.47 to 1.17) Kwakkel, 199953 26 0.65 (0.46) 34 0.37 (0.41) 13.22 0.64 (0.12 to 1.16) Salbach, 200451 44 0.78 (0.40) 47 0.64 (0.37) 21.13 0.36 (–0.05 to 0.78) Van Vliet, 200570 42 –12.19 (9.05) 43 –11.75 (7.88) 20.08 –0.05 (–0.48 to 0.37)
Subtotal (95% CI) 127 136 60.70 0.23 (–0.01 to 0.48)Test for heterogeneity: �2 = 5.40, df = 4 (p = 0.25), I2 = 25.9%Test for overall effect: Z = 1.86 (p = 0.06)
03 TMAda, 200387 11 0.75 (0.26) 14 0.56 (0.30) 5.49 0.65 (–0.17 to 1.46) da Cunha, 200286 6 0.59 (0.29) 7 0.27 (0.23) 2.47 1.15 (–0.06 to 2.36) Eich, 200489 25 0.71 (0.30) 25 0.60 (0.22) 11.55 0.41 (–0.15 to 0.97) Macko, 200588 25 0.74 (0.30) 20 0.76 (0.36) 10.50 –0.06 (–0.65 to 0.53) Pohl, 200285 20 1.22 (0.74) 20 0.97 (0.64) 9.29 0.35 (–0.27 to 0.98)
Subtotal (95% CI) 87 86 39.30 0.35 (0.05 to 0.66)Test for heterogeneity: �2 = 4.10, df = 4 (p = 0.39), I2 = 2.5%Test for overall effect: Z = 2.27 (p = 0.02)
Total (95% CI) 214 222 100.00 0.28 (0.09 to 0.47)Test for heterogeneity: �2 = 9.86, df = 9 (p = 0.36), I2 = 8.7%Test for overall effect: Z = 2.87 (p = 0.004)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 15 Walking speed
second, with the exception of Dean andShepherd66 and Van Vliet and colleagues,70 whopresented statistics for the number of seconds to walk 10 m and 6 m, respectively. Therewas some heterogeneity of treatment effects (I2 = 8.7%), although not sufficient to merit theuse of a random-effects approach. Five RTT trialsrecruited 311 participants,51,53,66,67,70 withoutcome data available for 85% (n = 263) of participants. Six TM trials recruited 229participants.63,85–89 One TM trial with 30participants provided data unsuitable for pooling,with data for mean distance walked but nostandard deviations.63 Of the five remaining trialswith 199 participants, outcome data were availablefor 87% (n = 173) of participants.
Overall, pooled results for the impact of RFTP onwalking speed showed a small effect size, whichwas statistically significant (SMD 0.28, 95% CI0.09 to 0.47). A subgroup analysis was undertakenfor walking speed measured over short (5 or 6 m)or medium (10 m) distances, with no significantdifference found (p = 0.57).
Functional ambulationFor RFTP overall, seven trials recruiting 368participants measured functional ambulation, withoutcome data available for 79% (n = 291) (Figure 16).Effects across trials were homogeneous (I2 = 0%).Five RTT trials53,68,70,76,78 recruited 295 participants,with outcome data available for 81% (n = 238). TwoTM trials85,86 recruited 59 participants, with outcomedata available for 89% (n = 53).
Pooling the results from seven trials showed RFTPto have a statistically significant but small effect onfunctional ambulation measures (SMD 0.28, 95%CI 0.05 to 0.51), with no significant difference ineffects between RTT and TM (p = 0.66).
Sit-to-standSeven trials (all RTT) recruiting 397 participantsincluded a measure of sit-to-stand,50,51,65,67,68,70,77
with outcome data available for 87% (n = 346)(Figure 17).
Effects across trials were homogeneous (I2 = 0%),showing a small to moderate effect size, which was

Results of the review
32 FIGURE 17 Sit-to-stand
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 04 Lower limb functionOutcome: 04 Sit-to-stand
Study TreatmentN
ControlN
(Estimate (fixed)(95% CI)
Weight(%)
Estimate (fixed)(95% CI)or subcategory Estimate (SE)
01 RTTBarreca, 200465 25 23 0.8715 (0.2812) 14.80 0.87 (0.32 to 1.42) Blennerhassett, 200450 15 15 0.7000 (0.3775) 8.21 0.70 (–0.04 to 1.44) Dean, 200067 5 4 0.5700 (0.6900) 2.46 0.57 (–0.78 to 1.92) Howe, 200577 15 15 0.2500 (0.3673) 8.67 0.25 (–0.47 to 0.97) Langhammer, 200068 29 24 0.3000 (0.2800) 14.92 0.30 (–0.25 to 0.85) Salbach, 200451 44 47 0.1600 (0.2091) 26.76 0.16 (–0.25 to 0.57) Van Vliet, 200570 42 43 0.3500 (0.2200) 24.18 0.35 (–0.08 to 0.78)
Subtotal (95% CI) 175 171 100.00 0.39 (0.18 to 0.61)Test for heterogeneity: �2 = 5.16, df = 6 (p = 0.52), I2 = 0%Test for overall effect: Z = 3.65 (p = 0.0003)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 16 Functional ambulation
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 04 Lower limb functionOutcome: 03 Functional ambulation
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 RTTde Sèze, 200176 10 2.60 (1.40) 10 1.60 (1.50) 6.62 0.66 (–0.25 to 1.57) Kwakkel, 199953 25 4.00 (1.00) 34 3.00 (2.00) 19.47 0.60 (0.07 to 1.12) Langhammer, 200068 29 4.00 (1.60) 24 3.80 (2.00) 18.54 0.11 (–0.43 to 0.65) McClellan, 200478 12 4.30 (1.20) 9 4.70 (1.00) 7.15 –0.34 (–1.21 to 0.53) Van Vliet, 200570 42 3.70 (1.62) 43 3.39 (1.93) 29.93 0.17 (–0.25 to 0.60)
Subtotal (95% CI) 118 120 81.71 0.25 (0.00 to 0.51)Test for heterogeneity: �2 = 4.60, df = 4 (p = 0.33), I2 = 13.0%Test for overall effect: Z = 1.93 (p = 0.05)
02 TMda Cunha, 200286 6 7.93 (3.65) 7 7.07 (4.50) 4.54 0.19 (–0.90 to 1.29) Pohl, 200285 20 4.60 (0.60) 20 4.30 (0.70) 13.75 0.45 (–0.18 to 1.08)
Subtotal (95% CI) 26 27 18.29 0.39 (–0.16 to 0.93)Test for heterogeneity: �2 = 0.16, df = 1 (p = 0.69), I2 = 0%Test for overall effect: Z = 1.39 (p = 0.16)
Total (95% CI) 144 147 100.00 0.28 (0.05 to 0.51)Test for heterogeneity: �2 = 4.95, df = 6 (p = 0.55), I2 = 0%Test for overall effect: Z = 2.34 (p = 0.02)
–4 –2 0 2 4 Favours control Favours treatment

statistically significant (standardised effect size0.39, 95% CI 0.18 to 0.61).
Lower limb functional measuresFour trials (all RTT) recruiting 223 participantsincluded a measure of lower limb function,50,67,68,70
with outcome data available for 79% (n = 177)(Figure 18). Effects across trials were homogeneous(I2 = 0%).
Results overall showed a small effect size, whichwas not statistically significant (SMD 0.20, 95% CI–0.10 to 0.50).
Standing balance and reachThree trials (all RTT) recruiting 137 participantsmeasured standing balance or functionalreach,51,76,78 with outcome data available for 96%(n = 132) (Figure 19).
Effects across trials were homogeneous (I2 = 0%),showing a small effect size, which was not statistically significant (SMD 0.29, 95% CI –0.06 to 0.63).
Health Technology Assessment 2008; Vol. 12: No. 30
33
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
FIGURE 18 Lower limb functional measures
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 04 Lower limb functionOutcome: 05 Lower limb functional measures
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 RTTBlennerhassett, 200450 15 11.10 (5.00) 15 8.50 (4.60) 16.59 0.53 (–0.20 to 1.26) Dean, 200067 5 9.80 (4.00) 4 5.80 (4.30) 4.40 0.86 (–0.56 to 2.28) Langhammer, 200068 29 41.00 (18.00) 24 39.00 (21.00) 30.17 0.10 (–0.44 to 0.64) Van Vliet, 200570 42 5.62 (4.02) 43 5.24 (4.30) 48.83 0.09 (–0.34 to 0.52)
Subtotal (95% CI) 91 86 100.00 0.20 (–0.10 to 0.50)Test for heterogeneity: �2 = 1.99, df = 3 (p = 0.58), I2 = 0%Test for overall effect: Z = 1.32 (p = 0.19)
Total (95% CI) 91 86 100.00 0.20 (–0.10 to 0.50)Test for heterogeneity: �2 = 1.99, df = 3 (p = 0.58), I2 = 0%Test for overall effect: Z = 1.32 (p = 0.19)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 19 Standing balance/reach
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 04 Lower limb function Outcome: 06 Standing balance and reach
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 RTTde Sèze, 200176 10 2.40 (1.60) 10 2.00 (0.80) 15.19 0.30 (–0.58 to 1.19) McClellan, 200478 12 21.90 (9.40) 9 17.80 (7.40) 15.36 0.46 (–0.42 to 1.33) Salbach, 200451 44 44.00 (11.00) 47 41.00 (13.00) 69.46 0.25 (–0.17 to 0.66)
Subtotal (95% CI) 66 66 100.00 0.29 (–0.06 to 0.63)Test for heterogeneity: �2 = 0.18, df = 2 (p = 0.91), I2 = 0%Test for overall effect: Z = 1.64 (p = 0.10)
Total (95% CI) 66 66 100.00 0.29 (–0.06 to 0.63)Test for heterogeneity: �2 = 0.18, df = 2 (p = 0.91), I2 = 0%Test for overall effect: Z = 1.64 (p = 0.10)
–4 –2 0 2 4 Favours control Favours treatment

Lower limb: follow-upUnder 6 months post-therapySix trials (four RTT67,76–78 and two TM87,89)recruiting 174 participants measured some aspectof lower limb function for retention effectsbetween post-therapy and under 6 months post-therapy (Figure 20). Outcome data wereavailable for 90% (n = 155). Effects across trials were homogeneous (I2 = 0%). Resultsshowed a small to moderate effect size which wasstatistically significant (SMD 0.37, 95% CI 0.05 to 0.69).
Between 6 and 12 months post-therapyThree RTT trials recruiting 211 participantsmeasured some aspect of lower limb function forretention effects of RTT interventions between 6and 12 months post-therapy (Figure 20).50,68,70
Outcome data were available for 80% (n = 170).
There was some degree of heterogeneity oftreatment effects (I2 = 49.1%), although notsufficient to merit the use of a random-effectsapproach (and the small effect size precludes theneed to perform a sensitivity analysis on the choiceof analytic approach). Results showed no treatmenteffect (SMD –0.01, 95% CI –0.32 to 0.29).
Subgroup analyses: lower limb functionSubgroup analyses for lower limb interventions are based on trials providing measures of walkingfunction (walking distance, walking speed orfunctional ambulation rating). Trials that onlyprovide measures of standing balance/reach76 orsit-to-stand65,77 are therefore excluded. Subgroupanalyses are presented for type, amount andtiming of intervention, and to consider the impact of adequacy of allocation concealment
Results of the review
34
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 04 Lower limb function Outcome: 07 Follow-up
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 Under 6 months post-therapyAda, 200387 13 0.83 (0.26) 13 0.64 (0.29) 7.70 0.67 (–0.13 to 1.46) de Sèze, 200176 10 3.10 (1.20) 10 2.50 (1.20) 6.09 0.48 (–0.41 to 1.37) Dean, 200067 4 84.00 (46.70) 4 81.50 (47.20) 2.52 0.05 (–1.34 to 1.43) Eich, 200489 24 0.77 (0.35) 25 0.58 (0.22) 14.64 0.64 (0.07 to 1.22) Howe, 200577 14 –4.20 (7.30) 15 –2.90 (2.50) 9.07 –0.24 (–0.97 to 0.50) McClellan, 200478 13 20.20 (9.40) 10 17.70 (8.40) 7.06 0.27 (–0.56 to 1.10)
Subtotal (95% CI) 78 77 47.08 0.37 (0.05 to 0.69)Test for heterogeneity: �2 = 4.36, df = 5 (p = 0.50), I2 = 0%Test for overall effect: Z = 2.25 (p = 0.02)
02 6–12 months post-therapyBlennerhassett, 200450 15 416.00 (171.00) 14 313.00 (154.00) 8.67 0.61 (–0.13 to 1.36) Langhammer, 200068 27 3.10 (2.30) 27 3.00 (2.30) 17.04 0.04 (–0.49 to 0.58) Van Vliet, 200570 42 3.24 (1.96) 45 3.70 (1.72) 27.21 –0.25 (–0.67 to 0.17)
Subtotal (95% CI) 84 86 52.92 –0.01 (–0.32 to 0.29)Test for heterogeneity: �2 = 3.93, df = 2 (p = 0.14), I2 = 49.1%Test for overall effect: Z = 0.08 (p = 0.93)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 20 Lower limb follow-up at 0–6 months and more than 6 months post-therapy

and type of comparison group. There wereinsufficient trials providing additional therapytime or trials of fewer than 25 participants toundertake subgroup analyses. The classification of trials for each subgroup analysis is given inAppendix 6.
Type of interventionTwelve trials (seven RTT, five TM) included ameasure of walking ability (Figure 21). There wassome heterogeneity of treatment effects withineach subgroup, but not sufficient to merit the useof random-effects analysis.
There was no statistically significant differencebetween RTT and TM interventions (p = 0.62).
Dosage of task practiceNine trials (five RTT, four TM) provided up to20 hours’ training time and three trials (two RTT,one TM) provided more than 20 hours’ trainingtime (Figure 22). There was substantialheterogeneity in the more than 20 hours’ practicesubgroup (I2 = 59.4%), so a random-effects modelwas used. There was no statistically significantdifference between subgroups (p = 0.65).
Time since strokeSix trials (three RTT, three TM) recruited0–6 months post-stroke and six trials (four RTT,two TM) recruited more than 6 months post-stroke(Figure 23). There was some heterogeneity oftreatment effects in both subgroups, but not
Health Technology Assessment 2008; Vol. 12: No. 30
35
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 05 Subgroup analyses – lower limb Outcome: 01 Type of intervention
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 RTTBlennerhassett, 200450 15 404.00 (101.00) 15 288.00 (124.00) 5.20 1.00 (0.23 to 1.76) Dean, 200067 5 80.20 (42.80) 4 88.40 (52.20) 1.75 –0.15 (–1.47 to 1.16) Kwakkel, 199953 26 0.65 (0.46) 34 0.37 (0.41) 11.09 0.64 (0.12 to 1.16) Langhammer, 200068 29 4.00 (1.60) 24 3.80 (2.00) 10.40 0.11 (–0.43 to 0.65) McClellan, 200478 12 4.30 (1.20) 9 4.70 (1.00) 4.01 –0.34 (–1.21 to 0.53) Salbach, 200451 44 0.78 (0.40) 47 0.64 (0.37) 17.72 0.36 (–0.05 to 0.78) Van Vliet, 200570 42 –12.19 (9.05) 43 –11.75 (7.88) 16.85 –0.05 (–0.48 to 0.37)
Subtotal (95% CI) 173 176 67.03 0.26 (0.05 to 0.47)Test for heterogeneity: �2 = 10.38, df = 6 (p = 0.11), I2 = 42.2%Test for overall effect: Z = 2.37 (p = 0.02)
02 TMAda, 200387 11 0.75 (0.26) 14 0.56 (0.30) 4.60 0.65 (–0.17 to 1.46) da Cunha, 200286 6 0.59 (0.29) 7 0.27 (0.23) 2.07 1.15 (–0.06 to 2.36) Eich, 200489 25 0.71 (0.30) 25 0.60 (0.22) 9.69 0.41 (–0.15 to 0.97) Macko, 200588 25 0.74 (0.30) 20 0.76 (0.36) 8.81 –0.06 (–0.65 to 0.53) Pohl, 200285 20 1.22 (0.74) 20 0.97 (0.64) 7.80 0.35 (–0.27 to 0.98)
Subtotal (95% CI) 87 86 32.97 0.35 (0.05 to 0.66)Test for heterogeneity: �2 = 4.10, df = 4 (p = 0.39), I2 = 2.5%Test for overall effect: Z = 2.27 (p = 0.02)
Total (95% CI) 260 262 100.00 0.29 (0.11, 0.46)Test for heterogeneity: �2 = 14.73, df = 11 (p = 0.20), I2 = 25.3%Test for overall effect: Z = 3.25 (p = 0.001)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 21 Subgroup analysis: type of intervention – lower limb trials

sufficient to merit a random-effects analysis. Therewas no significant difference between subgroups(p = 1.0).
Allocation concealmentTrials were grouped according to whetherallocation concealment was judged adequate (eight trials: six RTT, two TM) or inadequate/unclear (four trials: one RTT, three TM) (Figure24). There was heterogeneity within each
subgroup, but insufficient to warrant using arandom-effects meta-analysis. There was nostatistically significant difference betweensubgroups (p = 0.51).
Post hoc analysis: type of comparison groupSix trials (two RTT, four TM) were classified asusual care or alternative treatment, and six trials(five RTT, one TM) as attention-control or notreatment (Figure 25). There was some
Results of the review
36
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 05 Subgroup analyses – lower limb Outcome: 02 Dosage of task practice
Study Treatment Control SMD (random) Weight SMD (random)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 0–20 hoursAda, 200387 11 0.75 (0.26) 14 0.56 (0.30) 5.58 0.65 (–0.17 to 1.46) Blennerhassett, 200450 15 404.00 (101.00) 15 288.00 (124.00) 6.18 1.00 (0.23 to 1.76) da Cunha, 200286 6 0.59 (0.29) 7 0.27 (0.23) 2.76 1.15 (–0.06 to 2.36) Dean, 200067 5 80.20 (42.80) 4 88.40 (52.20) 2.36 –0.15 (–1.47 to 1.16) Eich, 200489 25 0.71 (0.30) 25 0.60 (0.22) 9.97 0.41 (–0.15 to 0.97) Langhammer, 200068 29 4.00 (1.60) 24 3.80 (2.00) 10.47 0.11 (–0.43 to 0.65) Pohl, 200285 20 1.22 (0.74) 20 0.97 (0.64) 8.50 0.35 (–0.27 to 0.98) Salbach, 200451 44 0.78 (0.40) 47 0.64 (0.37) 14.70 0.36 (–0.05 to 0.78) Van Vliet, 200570 42 –12.19 (9.05) 43 –11.75 (7.88) 14.27 –0.05 (–0.48 to 0.37)
Subtotal (95% CI) 197 199 74.79 0.33 (0.10 to 0.56)Test for heterogeneity: �2 = 9.59, df = 8 (p = 0.29), I2 = 16.6%Test for overall effect: Z = 2.85 (p = 0.004)
02 More than 20 hoursKwakkel, 199953 26 0.65 (0.46) 34 0.37 (0.41) 10.95 0.64 (0.12 to 1.16) Macko, 200588 25 0.74 (0.30) 20 0.76 (0.36) 9.30 –0.06 (–0.65 to 0.53) McClellan, 200478 12 4.30 (1.20) 9 4.70 (1.00) 4.96 –0.34 (–1.21 to 0.53)
Subtotal (95% CI) 63 63 25.21 0.14 (–0.44 to 0.73)Test for heterogeneity: �2 = 4.93, df = 2 (p = 0.09), I2 = 59.4%Test for overall effect: Z = 0.47 (p = 0.63)
Total (95% CI) 260 262 100.00 0.30 (0.09 to 0.51)Test for heterogeneity: �2 = 14.73, df = 11 (p = 0.20), I2 = 25.3%Test for overall effect: Z = 2.82 (p = 0.005)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 22 Subgroup analysis: dosage of task practice – lower limb trials
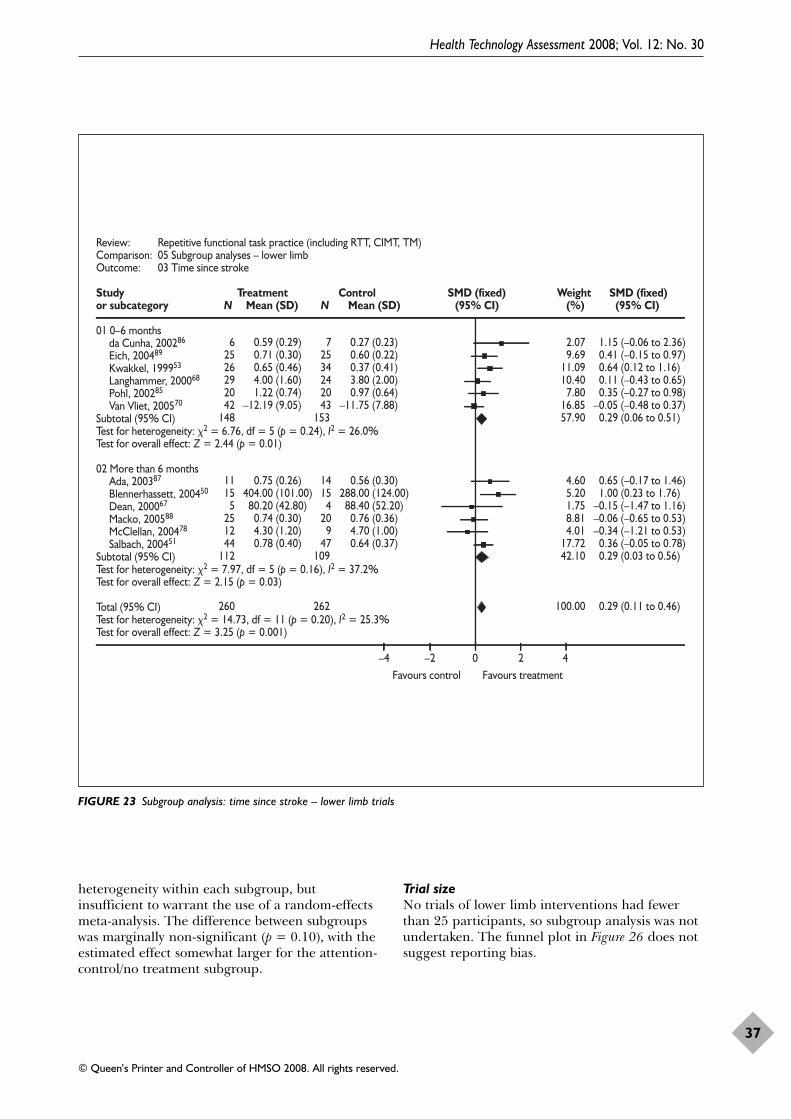
Health Technology Assessment 2008; Vol. 12: No. 30
37
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
heterogeneity within each subgroup, butinsufficient to warrant the use of a random-effectsmeta-analysis. The difference between subgroupswas marginally non-significant (p = 0.10), with theestimated effect somewhat larger for the attention-control/no treatment subgroup.
Trial sizeNo trials of lower limb interventions had fewerthan 25 participants, so subgroup analysis was notundertaken. The funnel plot in Figure 26 does notsuggest reporting bias.
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 05 Subgroup analyses – lower limbOutcome: 03 Time since stroke
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 0–6 monthsda Cunha, 200286 6 0.59 (0.29) 7 0.27 (0.23) 2.07 1.15 (–0.06 to 2.36) Eich, 200489 25 0.71 (0.30) 25 0.60 (0.22) 9.69 0.41 (–0.15 to 0.97) Kwakkel, 199953 26 0.65 (0.46) 34 0.37 (0.41) 11.09 0.64 (0.12 to 1.16) Langhammer, 200068 29 4.00 (1.60) 24 3.80 (2.00) 10.40 0.11 (–0.43 to 0.65) Pohl, 200285 20 1.22 (0.74) 20 0.97 (0.64) 7.80 0.35 (–0.27 to 0.98) Van Vliet, 200570 42 –12.19 (9.05) 43 –11.75 (7.88) 16.85 –0.05 (–0.48 to 0.37)
Subtotal (95% CI) 148 153 57.90 0.29 (0.06 to 0.51)Test for heterogeneity: �2 = 6.76, df = 5 (p = 0.24), I2 = 26.0%Test for overall effect: Z = 2.44 (p = 0.01)
02 More than 6 monthsAda, 200387 11 0.75 (0.26) 14 0.56 (0.30) 4.60 0.65 (–0.17 to 1.46) Blennerhassett, 200450 15 404.00 (101.00) 15 288.00 (124.00) 5.20 1.00 (0.23 to 1.76) Dean, 200067 5 80.20 (42.80) 4 88.40 (52.20) 1.75 –0.15 (–1.47 to 1.16) Macko, 200588 25 0.74 (0.30) 20 0.76 (0.36) 8.81 –0.06 (–0.65 to 0.53) McClellan, 200478 12 4.30 (1.20) 9 4.70 (1.00) 4.01 –0.34 (–1.21 to 0.53) Salbach, 200451 44 0.78 (0.40) 47 0.64 (0.37) 17.72 0.36 (–0.05 to 0.78)
Subtotal (95% CI) 112 109 42.10 0.29 (0.03 to 0.56)Test for heterogeneity: �2 = 7.97, df = 5 (p = 0.16), I2 = 37.2%Test for overall effect: Z = 2.15 (p = 0.03)
Total (95% CI) 260 262 100.00 0.29 (0.11 to 0.46)Test for heterogeneity: �2 = 14.73, df = 11 (p = 0.20), I2 = 25.3%Test for overall effect: Z = 3.25 (p = 0.001)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 23 Subgroup analysis: time since stroke – lower limb trials

Results of the review
38
FIGURE 24 Subgroup analysis: allocation concealment – lower limb trials
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 05 Subgroup analyses - lower limbOutcome: 04 Allocation concealment
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 AdequateAda, 200387 11 0.75 (0.26) 14 0.56 (0.30) 4.60 0.65 (–0.17 to 1.46) Blennerhassett, 200450 15 404.00 (101.00) 15 288.00 (124.00) 5.20 1.00 (0.23 to 1.76) Dean, 200067 5 80.20 (42.80) 4 88.40 (52.20) 1.75 –0.15 (–1.47 to 1.16) Eich, 200489 25 0.71 (0.30) 25 0.60 (0.22) 9.69 0.41 (–0.15 to 0.97) Kwakkel, 199953 26 0.65 (0.46) 34 0.37 (0.41) 11.09 0.64 (0.12 to 1.16) McClellan, 200478 12 4.30 (1.20) 9 4.70 (1.00) 4.01 –0.34 (–1.21 to 0.53) Salbach, 200451 44 0.78 (0.40) 47 0.64 (0.37) 17.72 0.36 (–0.05 to 0.78) Van Vliet, 200570 42 –12.19 (9.05) 43 –11.75 (7.88) 16.85 –0.05 (–0.48 to 0.37)
Subtotal (95% CI) 180 191 70.92 0.33 (0.12 to 0.53)Test for heterogeneity: �2 = 10.85, df = 7 (p = 0.15), I2 = 35.5%Test for overall effect: Z = 3.09 (p = 0.002)
02 Inadequate/unclearda Cunha, 200286 6 0.59 (0.29) 7 0.27 (0.23) 2.07 1.15 (–0.06, 2.36) Langhammer, 200068 29 4.00 (1.60) 24 3.80 (2.00) 10.40 0.11 (–0.43, 0.65) Macko, 200588 25 0.74 (0.30) 20 0.76 (0.36) 8.81 –0.06 (–0.65, 0.53) Pohl, 200285 20 1.22 (0.74) 20 0.97 (0.64) 7.80 0.35 (–0.27, 0.98)
Subtotal (95% CI) 80 71 29.08 0.20 (–0.13, 0.52)Test for heterogeneity: �2 = 3.45, df = 3 (p = 0.33), I2 = 13.0%Test for overall effect: Z = 1.20 (p = 0.23)
Total (95% CI) 260 262 100.00 0.29 (0.11 to 0.46)Test for heterogeneity: �2 = 14.73, df = 11 (p = 0.20), I2 = 25.3%Test for overall effect: Z = 3.25 (p = 0.001)
–4 –2 0 2 4 Favours control Favours treatment

Health Technology Assessment 2008; Vol. 12: No. 30
39
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 05 Subgroup analyses – lower limbOutcome: 05 Comparison group
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 Usual care/alternative treatmentda Cunha, 200286 6 0.59 (0.29) 7 0.27 (0.23) 2.07 1.15 (–0.06 to 2.36) Eich, 200489 25 0.71 (0.30) 25 0.60 (0.22) 9.69 0.41 (–0.15 to 0.97) Langhammer, 200068 29 4.00 (1.60) 24 3.80 (2.00) 10.40 0.11 (–0.43 to 0.65) Macko, 200588 25 0.74 (0.30) 20 0.76 (0.36) 8.81 –0.06 (–0.65 to 0.53) Pohl, 200285 20 1.22 (0.74) 20 0.97 (0.64) 7.80 0.35 (–0.27 to 0.98) Van Vliet, 200570 42 –12.19 (9.05) 43 –11.75 (7.88) 16.85 –0.05 (–0.48 to 0.37)
Subtotal (95% CI) 147 139 55.62 0.16 (–0.07 to 0.39)Test for heterogeneity: �2 = 5.22, df = 5 (p = 0.39), I2 = 4.3%Test for overall effect: Z = 1.34 (p = 0.18)
02 Attention control/no treatmentAda, 200387 11 0.75 (0.26) 14 0.56 (0.30) 4.60 0.65 (–0.17 to 1.46) Blennerhassett, 200450 15 404.00 (101.00) 15 288.00 (124.00) 5.20 1.00 (0.23 to 1.76) Dean, 200067 5 80.20 (42.80) 4 88.40 (52.20) 1.75 –0.15 (–1.47 to 1.16) Kwakkel, 199953 26 0.65 (0.46) 34 0.37 (0.41) 11.09 0.64 (0.12 to 1.16) McClellan, 200478 12 4.30 (1.20) 9 4.70 (1.00) 4.01 –0.34 (–1.21 to 0.53) Salbach, 200451 44 0.78 (0.40) 47 0.64 (0.37) 17.72 0.36 (–0.05 to 0.78)
Subtotal (95% CI) 113 123 44.38 0.45 (0.19 to 0.71)Test for heterogeneity: �2 = 6.86, df = 5 (p = 0.23), I2 = 27.1%Test for overall effect: Z = 3.37 (p = 0.0007)
Total (95% CI) 260 262 100.00 0.29 (0.11 to 0.46)Test for heterogeneity: �2 = 14.73, df = 11 (p = 0.20), I2 = 25.3%Test for overall effect: Z = 3.25 (p = 0.001)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 25 Subgroup analysis: type of comparison group – lower limb trials
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 05 Subgroup analyses – lower limbOutcome: 06 Trial size
–10 –5 0 5 10
0.0
0.2
0.4
0.6
0.8
SE (S
MD
)
SMD (fixed)
FIGURE 26 Funnel plot of precision versus effect size – lower limb trials
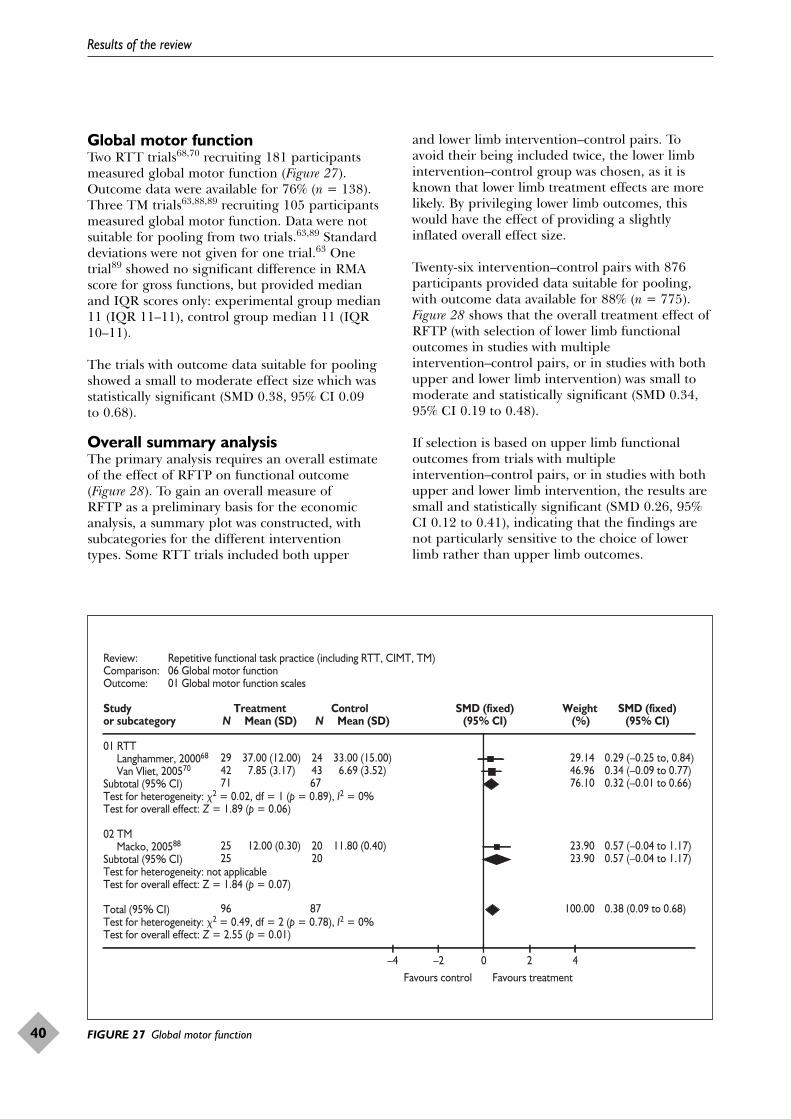
Results of the review
40
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 06 Global motor functionOutcome: 01 Global motor function scales
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 RTTLanghammer, 200068 29 37.00 (12.00) 24 33.00 (15.00) 29.14 0.29 (–0.25 to, 0.84) Van Vliet, 200570 42 7.85 (3.17) 43 6.69 (3.52) 46.96 0.34 (–0.09 to 0.77)
Subtotal (95% CI) 71 67 76.10 0.32 (–0.01 to 0.66)Test for heterogeneity: �2 = 0.02, df = 1 (p = 0.89), I2 = 0%Test for overall effect: Z = 1.89 (p = 0.06)
02 TMMacko, 200588 25 12.00 (0.30) 20 11.80 (0.40) 23.90 0.57 (–0.04 to 1.17)
Subtotal (95% CI) 25 20 23.90 0.57 (–0.04 to 1.17)Test for heterogeneity: not applicableTest for overall effect: Z = 1.84 (p = 0.07)
Total (95% CI) 96 87 100.00 0.38 (0.09 to 0.68)Test for heterogeneity: �2 = 0.49, df = 2 (p = 0.78), I2 = 0%Test for overall effect: Z = 2.55 (p = 0.01)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 27 Global motor function
Global motor functionTwo RTT trials68,70 recruiting 181 participantsmeasured global motor function (Figure 27).Outcome data were available for 76% (n = 138).Three TM trials63,88,89 recruiting 105 participantsmeasured global motor function. Data were notsuitable for pooling from two trials.63,89 Standarddeviations were not given for one trial.63 Onetrial89 showed no significant difference in RMAscore for gross functions, but provided medianand IQR scores only: experimental group median11 (IQR 11–11), control group median 11 (IQR10–11).
The trials with outcome data suitable for poolingshowed a small to moderate effect size which wasstatistically significant (SMD 0.38, 95% CI 0.09 to 0.68).
Overall summary analysisThe primary analysis requires an overall estimateof the effect of RFTP on functional outcome(Figure 28). To gain an overall measure of RFTP as a preliminary basis for the economicanalysis, a summary plot was constructed, withsubcategories for the different intervention types. Some RTT trials included both upper
and lower limb intervention–control pairs. Toavoid their being included twice, the lower limbintervention–control group was chosen, as it isknown that lower limb treatment effects are morelikely. By privileging lower limb outcomes, thiswould have the effect of providing a slightlyinflated overall effect size.
Twenty-six intervention–control pairs with 876participants provided data suitable for pooling,with outcome data available for 88% (n = 775).Figure 28 shows that the overall treatment effect ofRFTP (with selection of lower limb functionaloutcomes in studies with multipleintervention–control pairs, or in studies with bothupper and lower limb intervention) was small tomoderate and statistically significant (SMD 0.34,95% CI 0.19 to 0.48).
If selection is based on upper limb functionaloutcomes from trials with multipleintervention–control pairs, or in studies with bothupper and lower limb intervention, the results aresmall and statistically significant (SMD 0.26, 95%CI 0.12 to 0.41), indicating that the findings arenot particularly sensitive to the choice of lowerlimb rather than upper limb outcomes.

Health Technology Assessment 2008; Vol. 12: No. 30
41
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 07 Summary analysis RFTPOutcome: 01 Functional outcomes (inc. lower limb)
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) (95% CI) (%) (95% CI)
01 Upper limb RTTTurton, 199069 12 13.83 (6.00) 10 12.25 (7.20) 2.95 0.23 (–0.61 to 1.07) Winstein, 200471 20 9.58 (5.70) 20 9.47 (6.30) 5.45 0.02 (–0.60 to 0.64) Yen, 200572 13 –2.57 (0.93) 17 –3.06 (1.54) 3.94 0.36 (–0.37 to 1.09)
Subtotal (95% CI) 45 47 12.33 0.18 (–0.23 to 0.59)Test for heterogeneity: �2 = 0.52, df = 2 (p = 0.77), I2 = 0%Test for overall effect: Z = 0.85 (p = 0.39)
02 Upper limb CIMTAlberts, 200483 5 –28.89 (24.80) 5 –25.02 (17.96) 1.35 –0.16 (–1.40 to 1.08) Atteya, 200479 2 52.00 (6.00) 2 51.50 (10.50) 0.54 0.03 (–1.94 to 2.00) Boake, 200684 9 0.08 (0.06) 7 0.04 (0.08) 2.04 0.55 (–0.47 to 1.56) Dromerick, 200081 11 52.80 (5.90) 9 44.30 (11.10) 2.37 0.95 (0.01 to 1.89) Page, 200180 2 53.00 (6.00) 2 51.00 (10.00) 0.47 0.14 (–1.97 to 2.25) Page, 200582 5 49.80 (3.27) 5 35.80 (3.56) 0.36 3.70 (1.28 to 6.12) Taub, 199373 4 8.10 (0.42) 5 6.90 (0.70) 0.71 1.79 (0.07 to 3.50) Wittenberg, 200374 9 7.54 (2.04) 7 5.85 (2.79) 2.00 0.67 (–0.35 to 1.69)
Subtotal (95% CI) 47 42 9.84 0.73 (0.27 to 1.19)Test for heterogeneity: �2 = 10.33, df = 7 (p = 0.17), I2 = 32.2%Test for overall effect: Z = 3.09 (p = 0.002)
03 Lower limb RTTBlennerhassett, 200450 15 404.00 (101.00) 15 288.00 (124.00) 3.57 1.00 (0.23 to 1.76) Dean, 200067 5 80.20 (42.80) 4 88.40 (52.20) 1.20 –0.15 (–1.47 to 1.16) Kwakkel, 199953 26 0.65 (0.46) 34 0.37 (0.41) 7.62 0.64 (0.12 to 1.16) Langhammer, 200068 29 4.00 (1.60) 24 3.80 (2.00) 7.14 0.11 (–0.43 to 0.65) McClellan, 200478 12 4.30 (1.20) 9 4.70 (1.00) 2.75 –0.34 (–1.21 to 0.53) Salbach, 200451 44 0.78 (0.40) 47 0.64 (0.37) 12.17 0.36 (–0.05 to 0.78) Van Vliet, 200570 42 –12.19 (9.05) 43 –11.75 (7.88) 11.57 –0.05 (–0.48 to 0.37)
Subtotal (95% CI) 173 176 46.02 0.26 (0.05 to 0.47)Test for heterogeneity: �2 = 10.38, df = 6 (p = 0.11), I2 = 42.2%Test for overall effect: Z = 2.37 (p = 0.02)
04 Lower limb TMAda, 200387 11 0.75 (0.26) 14 0.56 (0.30) 3.16 0.65 (–0.17 to 1.46) da Cunha, 200286 6 0.59 (0.29) 7 0.27 (0.23) 1.42 1.15 (–0.06 to 2.36) Eich, 200489 25 0.71 (0.30) 25 0.60 (0.22) 6.65 0.41 (–0.15 to 0.97) Macko, 200588 25 0.74 (0.30) 20 0.76 (0.36) 6.05 –0.06 (–0.65 to 0.53) Pohl, 200285 20 1.22 (0.74) 20 0.97 (0.64) 5.35 0.35 (–0.27 to 0.98)
Subtotal (95% CI) 87 86 22.64 0.35 (0.05 to 0.66)Test for heterogeneity: �2 = 4.10, df = 4 (p = 0.39), I2 = 2.5%Test for overall effect: Z = 2.27 (p = 0.02)
05 Sitting and standing balance RTTde Sèze, 200176 10 3.30 (0.80) 10 3.00 (0.80) 2.67 0.36 (–0.53 to 1.24) Dean, 199766 10 12.00 (0.95) 9 10.80 (0.90) 2.08 1.24 (0.23 to 2.24) Howe, 200577 15 –1.90 (0.80) 18 –2.10 (0.70) 4.41 0.26 (–0.43 to 0.95)
Subtotal (95% CI) 35 37 9.16 0.51 (0.03 to 0.99)Test for heterogeneity: �2 = 2.63, df = 2 (p = 0.27), I2 = 23.9%Test for overall effect: Z = 2.10 (p = 0.04)
Total (95% CI) 387 388 100.00 0.34 (0.19 to 0.48)Test for heterogeneity: �2 = 32.31, df = 25 (p = 0.15), I2 = 22.6%Test for overall effect: Z = 4.59 (p < 0.00001)
–10 –5 0 5 10 Favours control Favours treatment
FIGURE 28 Overall impact of all forms of RFTP on functional outcome
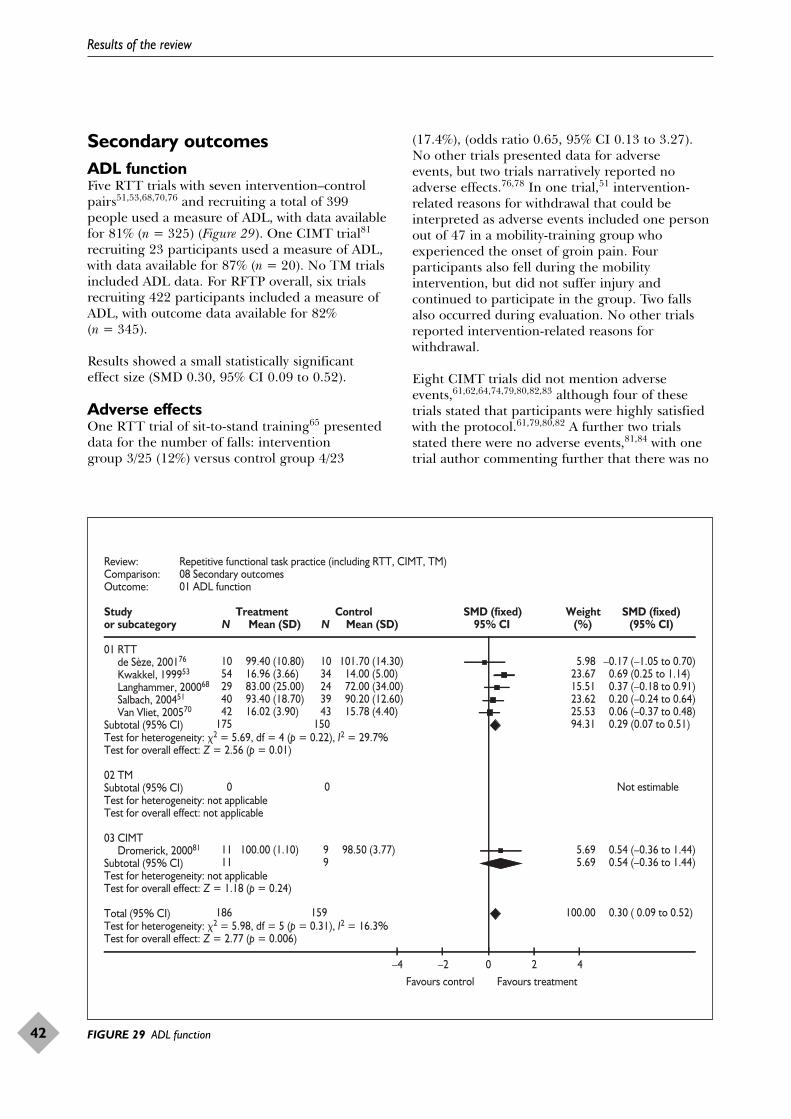
Secondary outcomesADL functionFive RTT trials with seven intervention–controlpairs51,53,68,70,76 and recruiting a total of 399people used a measure of ADL, with data availablefor 81% (n = 325) (Figure 29). One CIMT trial81
recruiting 23 participants used a measure of ADL,with data available for 87% (n = 20). No TM trialsincluded ADL data. For RFTP overall, six trialsrecruiting 422 participants included a measure ofADL, with outcome data available for 82%(n = 345).
Results showed a small statistically significanteffect size (SMD 0.30, 95% CI 0.09 to 0.52).
Adverse effectsOne RTT trial of sit-to-stand training65 presenteddata for the number of falls: intervention group 3/25 (12%) versus control group 4/23
(17.4%), (odds ratio 0.65, 95% CI 0.13 to 3.27).No other trials presented data for adverse events, but two trials narratively reported noadverse effects.76,78 In one trial,51 intervention-related reasons for withdrawal that could beinterpreted as adverse events included one personout of 47 in a mobility-training group whoexperienced the onset of groin pain. Fourparticipants also fell during the mobilityintervention, but did not suffer injury andcontinued to participate in the group. Two fallsalso occurred during evaluation. No other trialsreported intervention-related reasons forwithdrawal.
Eight CIMT trials did not mention adverseevents,61,62,64,74,79,80,82,83 although four of thesetrials stated that participants were highly satisfiedwith the protocol.61,79,80,82 A further two trialsstated there were no adverse events,81,84 with onetrial author commenting further that there was no
Results of the review
42
Review: Repetitive functional task practice (including RTT, CIMT, TM)Comparison: 08 Secondary outcomesOutcome: 01 ADL function
Study Treatment Control SMD (fixed) Weight SMD (fixed)or subcategory N Mean (SD) N Mean (SD) 95% CI (%) (95% CI)
01 RTTde Sèze, 200176 10 99.40 (10.80) 10 101.70 (14.30) 5.98 –0.17 (–1.05 to 0.70) Kwakkel, 199953 54 16.96 (3.66) 34 14.00 (5.00) 23.67 0.69 (0.25 to 1.14) Langhammer, 200068 29 83.00 (25.00) 24 72.00 (34.00) 15.51 0.37 (–0.18 to 0.91) Salbach, 200451 40 93.40 (18.70) 39 90.20 (12.60) 23.62 0.20 (–0.24 to 0.64) Van Vliet, 200570 42 16.02 (3.90) 43 15.78 (4.40) 25.53 0.06 (–0.37 to 0.48)
Subtotal (95% CI) 175 150 94.31 0.29 (0.07 to 0.51)Test for heterogeneity: �2 = 5.69, df = 4 (p = 0.22), I2 = 29.7%Test for overall effect: Z = 2.56 (p = 0.01)
02 TMSubtotal (95% CI) 0 0 Not estimableTest for heterogeneity: not applicableTest for overall effect: not applicable
03 CIMTDromerick, 200081 11 100.00 (1.10) 9 98.50 (3.77) 5.69 0.54 (–0.36 to 1.44)
Subtotal (95% CI) 11 9 5.69 0.54 (–0.36 to 1.44)Test for heterogeneity: not applicableTest for overall effect: Z = 1.18 (p = 0.24)
Total (95% CI) 186 159 100.00 0.30 ( 0.09 to 0.52)Test for heterogeneity: �2 = 5.98, df = 5 (p = 0.31), I2 = 16.3%Test for overall effect: Z = 2.77 (p = 0.006)
–4 –2 0 2 4 Favours control Favours treatment
FIGURE 29 ADL function

evidence of excess disability associated withCIMT.81 In one trial, the first three participants toreceive restraint reported stiffness and discomforton the involved side half-way through the 2-weektreatment period.73 These effects were associatedwith overuse of the affected limb and led tomodification of the intervention protocol for thefourth participant, with motor demands increasingmore slowly. The fourth participant reported nomuscle soreness. There were no intervention-related reasons for withdrawal in any CIMT ormCIMT trial. Of the six TM trials, three reportedthat there were no adverse events.85,87,89 There areno reports of adverse events in three trials.63,86,88
None of the trials reported intervention-relatedreasons for withdrawal that could be interpreted asadverse events.
Sensitivity analysisA sensitivity analysis was undertaken to evaluatethe effect on upper limb outcomes of includingcross-over and quasi-randomised trials,63,69 findingno substantive difference between including (SMD0.24, 95% CI 0.06 to 0.42) and not including(SMD 0.24, 95% CI 0.05 to 0.43) these trials. Asensitivity analysis was also undertaken on lowerlimb trials to evaluate the effect of excludingstudies with more than 20% loss to follow-up (onlyone upper limb trial had loss to follow-up ofgreater than 20%). The effect of RFTP wassignificantly greater (p = 0.02) for trials with lossto follow-up of 20% or less (SMD 0.42, 95% CI0.22 to 0.63) than for trials with more than 20% loss to follow-up (SMD –0.06, 95% CI –0.39 to 0.27).
Health Technology Assessment 2008; Vol. 12: No. 30
43
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.


BackgroundThe systematic review identified studies that willpotentially alter patient outcomes by using RTT.There were three forms of therapy that had RTTas a major component: RTT, CIMT, and TM. Thetherapies will subsequently be referred to as RFTP.The economic modelling reported below wasdesigned to determine whether RFTP is cost-effective.
Study questionFrom the perspective of the NHS, is RFTP forstroke (in addition to usual care) cost-effective over3 years as judged by the incremental cost perquality-adjusted life-year (QALY) gained?
PerspectiveThe analyses performed took the perspective ofthe NHS and Personal Social Services (PSS). Thecost of stroke tends to be higher in the acute stageowing to the inpatient cost. Once a patient isdischarged from hospital, some of the costs will beborne by the NHS through provision of therapyand aids, and some will be borne by PSS throughprovision of support services. RFTP would takeplace after the acute stage of treatment and hencewill have no effect on these costs; therefore theyare not considered in this analysis.
Current treatmentAt present, the amount of physical therapy inputto post-stroke patients varies widely. In hospital,most patients receive physiotherapy andoccupational therapy. Once their care is transferredinto the community, the provision of therapies ismuch less structured. This means that it is difficultto define a standard package of physical therapyafter stroke. For this analysis usual care was basedon observations of a cohort of patients treated inthe NHS over time with the amount of physicaltherapy varying between patients. For the costanalysis the alternative treatments compared hereare usual care and usual care plus RFTP.
MethodsForm of evaluationA cost–utility approach was adopted, assessinggains in QALYs. The authors believe this to be the
most meaningful outcome measure on which tobase the economic evaluation. The nature of RFTPmeans that it will not directly prevent death,excluding a cost-effectiveness analysis of life-yearsgained. An alternative would be to express theeffects of RFTP in terms of a change in units ofsome measure of function; however, the authorsbelieve that this would be generally lessmeaningful than identifying a cost per QALYgained. The modelling is based over a 3-yearperiod.
Choice of RFTP interventionThe economic analysis is based around the threeforms of therapy described in the systematicreview: RTT, CIMT and TM.
Measures of benefitThe health outcome summary measure is thenumber of QALYs gained. A health outcome wasneeded that could be used across the three formsof therapy described.
The patient data setThe patient data set used for the modelling is alongitudinal data set that contains follow-up datafor a cohort of 539 stroke patients, consecutivelyidentified over a 6-month period in 1996, onstroke registers in two hospitals.134 Data werecollected on admission, at discharge, and at 3 and6 months, and subsequently 1, 2, and 3 years post-stroke. The data collected in hospital includedadmission and discharge dates, basicdemographics, stroke characteristics and scanresults. At each follow-up time patient status (aliveor dead) was identified, and data were collectedregarding residence, function, social service input,therapy input and aids provided. These patientsreceived usual stroke care and their 3-year datawere used as the baseline from which to judge thepotential impact of RFTP. The baselinecharacteristics of these patients can be seen inAppendix 7. The characteristics of the data setcompare favourably with the characteristics of thepatients in the included studies.
Assumptions about health outcomesThe Barthel Activities of Daily Living Index (BI)135
at 3 years post-stroke was used to define outcomegroups, which represented a range of disability
Health Technology Assessment 2008; Vol. 12: No. 30
45
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Chapter 5
Economic analysis

levels, and such that there were similar numbers ineach group. The choice of the BI was based on itswidespread usage as a global outcome in strokeresearch and because it had been mapped ontothe EuroQol-5 Dimensions (EQ-5D).136 The BI is aten-item scale ranging from 0 (dependent onothers for ADLs) to 20 (independent of others forADLs); the items measured include mobility,transfers, grooming and feeding. The number ofpatients in each Barthel category was 28 (BI � 10); 34 (BI = 11–14); 33 (BI = 15–17), 25(BI = 18 or 19) and 30 (BI = 20).
Efficacy of RFTPA range of different outcome measures was used inthe systematic review. For each outcome theeffectiveness of RFTP was expressed as the SMDwith associated 95% CI. The exception to this wasfor walking distance, which was expressed as WMD.However, for the economic analysis, the SMD willbe used. In the economic analysis the focus was onthose outcomes that showed a significant benefit ofRFTP and where there were at least 250 patients inthe analysis of efficacy, because the estimates basedon such a sample size would be more robust.However, walking speed was not included in theeconomic analysis because it was felt that walkingdistance was the more meaningful of these twooutcomes. To determine the potential impact ofRFTP, it was necessary to estimate how a change inthe SMD would equate to a change on the BI. Itwas estimated that a change in the SMD of 0.2 wasequivalent to a change in 1 point on the BI. Thiswas based on the following assumption: SMD =(treatment mean – control mean)/SD; a ‘typical SD’for the BI in a rehabilitation stroke populationmight be 5 units; therefore, an SMD of 0.2 wouldbe 1 Barthel unit.
Patient values preferencesA study was identified that examined theassociation between the BI and the EQ-5D.136
Although this study was based in TheNetherlands, the characteristics of the patientsincluded in the study are similar to thecharacteristics of those in the present patient dataset (at 6 months). The study136 suggested that 1point on the BI was equivalent to 0.05 of a QALY.
CostThe cost estimates reflect 2005/06 prices. Directcosts have been used, valued from an NHS public-sector perspective. The majority of the costs wereobtained from national figures.137 The exception tothis was the cost for aids, which were obtained froman NHS loan store. The assumptions made aboutthe costs for the RFTP studies are detailed below.
Assumptions about costingPatient data setThe analysis focused on the costs that were likelyto be influenced by RFTP, which included the costof services, therapy and aids post-discharge. Costswere estimated from the following inputs: homecare, meals on wheels, chiropody, physiotherapy,occupational therapy, day centre, day hospital,wheelchair, walking frame, walking stick, toilet seatraiser, chair raiser, bed raiser, toilet frame, trolleyand shopping trolley. The costs that were notincluded were GP attendance, readmission tohospital, clinic attendance or medication. Alsoexcluded were hospital costs for the index strokeand subsequent hotel costs for residence ininstitutions. Although RFTP is likely to promoteindependence in everyday activities, it is unlikelythat it would prevent admission to institutions.Moreover, there was some concern that high hotelcosts of institutions, or even readmissions tohospital, would unduly influence the model andthe authors wished to adopt a conservativeapproach to the estimates of cost-effectiveness.
RFTP studiesThe RFTP studies included in the review exhibitedsome diversity in when and where they wereperformed; some were more than 10 years old andmany were not based in the UK. To estimate thecosts of such studies, an assumption was made thatthey could be performed in a similar manner inthe UK. In addition, although the studies reportedon how much therapy was provided, there were nodata on the impact of the training on subsequentresource use. Therefore, it was assumed that theRFTP training did not result in additional costsowing to readmission or clinic attendance, causedby patients’ conditions worsening.
Because of the diverse nature of studies and thedata reported therein, a somewhat pragmaticapproach to costing methodology was taken. It wasassumed that for all studies the therapy staff costwas £40 per hour and that as well as the cost ofproviding the therapy there would be anadditional 20 hours of staff training per study. Thelack of CIMT data from the UK meant that anestimate of the cost of CIMT equipment had to bemade, of £100 per patient. The TM studies used acost of £25,000 for the equipment plus anadditional £1500 for installation. Within the RTTstudies there were miscellaneous costs for whichthe following cost estimates were made: Bon SaintCôme trunk control and retraining device £1000,videotaped instructions and telephone contacts£500, and instruction booklets £600. In onestudy67 a Kinetron machine was used in one
Economic analysis
46

workstation out of ten. The original cost of thismachine was approximately £32,000. Because this device is no longer manufactured and itcontributed only a small part to the RTT input, a cost of £1000 was attributed to this device. Forall equipment the one-off cost of purchase wasused and no assumptions were made about thelifetime of the equipment or how often it wasused.
For each trial an average cost per patient wascalculated based on staff time, equipment usedand number of patients randomised into thetrial. Subsequently, an average cost per therapy(i.e. RTT, CIMT and TM) was calculated basedon the average cost for each trial and thenumber of trials that contributed to that therapymodality. From this calculation the estimatedaverage cost per patient for the individualtherapies was £651 for RTT, £1773 for CIMTand £1870 for TM. Further estimates were thenmade of the average cost per patient forcombinations of therapy. To make the calculationfor combinations of therapy, an average cost forall trials in the relevant therapy modalities wasestimated. This resulted in an average cost perpatient of £1126 for RTT and CIMT combined,and £999 for RTT and TM combined. Theoverall average cost per person of RFTP (i.e.RTT, CIMT and TM combined) for the basemodel was estimated to be £1265.
Where outcome measures reflected all forms oftherapy (overall effect), the cost of theintervention was taken from the overall averagecost of RFTP. Where outcome measures reflectedtherapy focusing on the upper limb (arm functionand ADL), the cost of the intervention was takenfrom the average cost of RTT and CIMT. Whereoutcome measures reflected therapy focusing onthe lower limb (walking distance, functionalambulation and sit-to-stand), the cost of theintervention was taken from the average cost ofRTT and TM.
The modelGroups were identified, based on the BI at 3 yearsas described above. For each group the 3-year costwas estimated: the baseline cost in this analysis. Itwas then assumed that for an SMD of 0.2, therewould be a 1-point increase per patient on the BI,that the BI scores were evenly distributed withinthe groups and that the effect would bemaintained over 3 years. Using this assumption,the number of patients in each of the Barthelgroups was re-estimated. A new (3-year) cost wasthen calculated based on the new numbers in each
of the groups. The difference between the baselinecost and the new cost was considered to representthe impact of RFTP on cost. An average cost perpatient, reflecting the potential cost saving ofRFTP, was subsequently calculated, as £47,523/150= £316.82 (Appendix 8).
Adjustment for timing of costs and benefitsFor the base model the cost–utility of RFTP over3 years was assessed, and costs and effects werediscounted at an annual rate of 3.5%.
Allowances for uncertaintySeveral sensitivity analyses were performed toexplore the impact of varying certain parameterson the base model:
● RFTP efficacy● association between the SMD and the BI● association between the BI and the EQ-5D● cost of therapy● discount rates.
The relationship between the cost of RFTP per patient and the cost per QALY was alsoexplored.
ResultsFrom the systematic review, the overall effect sizefor RFTP was SMD 0.34 (95% CI 0.19 to 0.48).The following outcomes were based on studieswhere the combined sample size was more than250 patients, and revealed a significant effect ofRFTP.
● arm function: SMD 0.24 (95% CI 0.06 to 0.42)● ADL: SMD 0.30 (95% CI 0.09 to 0.52)● walking distance: SMD 0.45 (95% CI 0.20 to
0.70)● functional ambulation: SMD 0.28 (95% CI 0.05
to 0.51)● sit-to-stand: SMD 0.39 (95% CI 0.18 to 0.61).
The effect sizes for the five outcomes are based onRTT plus one of either CIMT or TM. For armfunction there was heterogeneity of effect betweenRTT, which was non significant (SMD 0.17, 95%CI –0.03 to 0.36) and CIMT, which was significant(SMD 0.77, 95% CI 0.26 to 1.29). However, theestimates of cost-effectiveness will use thecombined effect size.
Cost-effectiveness at 3 yearsIn the base-case analysis using the overall effectsize, the incremental cost-effectiveness ratio
Health Technology Assessment 2008; Vol. 12: No. 30
47
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
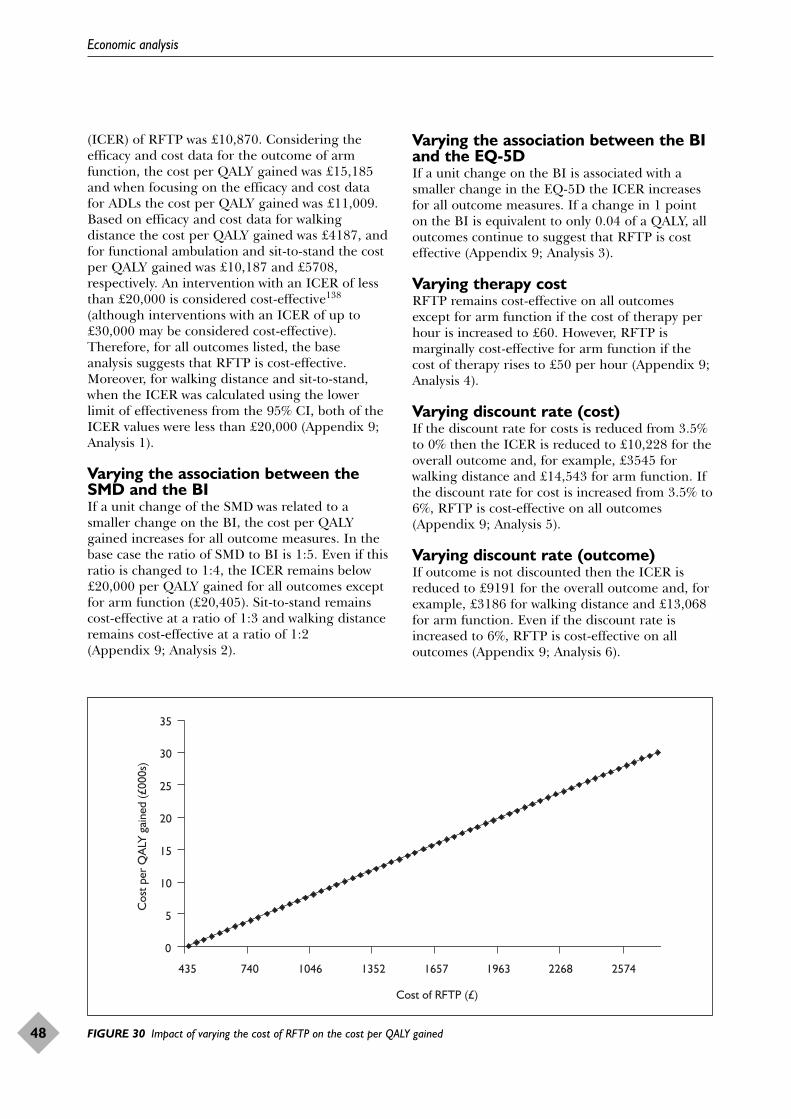
(ICER) of RFTP was £10,870. Considering theefficacy and cost data for the outcome of armfunction, the cost per QALY gained was £15,185and when focusing on the efficacy and cost datafor ADLs the cost per QALY gained was £11,009.Based on efficacy and cost data for walkingdistance the cost per QALY gained was £4187, andfor functional ambulation and sit-to-stand the costper QALY gained was £10,187 and £5708,respectively. An intervention with an ICER of lessthan £20,000 is considered cost-effective138
(although interventions with an ICER of up to£30,000 may be considered cost-effective).Therefore, for all outcomes listed, the baseanalysis suggests that RFTP is cost-effective.Moreover, for walking distance and sit-to-stand,when the ICER was calculated using the lowerlimit of effectiveness from the 95% CI, both of theICER values were less than £20,000 (Appendix 9;Analysis 1).
Varying the association between theSMD and the BIIf a unit change of the SMD was related to asmaller change on the BI, the cost per QALYgained increases for all outcome measures. In thebase case the ratio of SMD to BI is 1:5. Even if thisratio is changed to 1:4, the ICER remains below£20,000 per QALY gained for all outcomes exceptfor arm function (£20,405). Sit-to-stand remainscost-effective at a ratio of 1:3 and walking distanceremains cost-effective at a ratio of 1:2 (Appendix 9; Analysis 2).
Varying the association between the BIand the EQ-5DIf a unit change on the BI is associated with asmaller change in the EQ-5D the ICER increasesfor all outcome measures. If a change in 1 pointon the BI is equivalent to only 0.04 of a QALY, alloutcomes continue to suggest that RFTP is costeffective (Appendix 9; Analysis 3).
Varying therapy costRFTP remains cost-effective on all outcomesexcept for arm function if the cost of therapy perhour is increased to £60. However, RFTP ismarginally cost-effective for arm function if thecost of therapy rises to £50 per hour (Appendix 9;Analysis 4).
Varying discount rate (cost)If the discount rate for costs is reduced from 3.5%to 0% then the ICER is reduced to £10,228 for theoverall outcome and, for example, £3545 forwalking distance and £14,543 for arm function. Ifthe discount rate for cost is increased from 3.5% to6%, RFTP is cost-effective on all outcomes(Appendix 9; Analysis 5).
Varying discount rate (outcome)If outcome is not discounted then the ICER isreduced to £9191 for the overall outcome and, forexample, £3186 for walking distance and £13,068for arm function. Even if the discount rate isincreased to 6%, RFTP is cost-effective on alloutcomes (Appendix 9; Analysis 6).
Economic analysis
48
0
5
10
15
20
25
30
35
435 740 1046 1352 1657 1963 2268 2574
Cost of RFTP (£)
Cos
t per
QA
LY g
aine
d (£
000s
)
FIGURE 30 Impact of varying the cost of RFTP on the cost per QALY gained

Association between cost of RFTP andcost per QALY gainedThe base costs were used to calculate how achange in the cost of RFTP per patient affects theICER per QALY gained. At an ICER of £20,000
per QALY gained the average cost of RFTP perpatient is £1963, which approximates to 49 hours’contact per patient, excluding equipment costs(Figure 30).
Health Technology Assessment 2008; Vol. 12: No. 30
49
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.


Summary of main resultsUpper limb function/sitting balanceIn total, 19 RFTP trials with 634 participantsmeasured arm or hand function. Eight were RTT trials with 467 participants. Of these, twotrials were whole therapy approaches,68,70
two trials were circuit-training approaches,50,52
three trials were functional task practice mixed in with other forms of upper limb exercise,53,69,71
and one trial was the intensive practicecomponent of constraint-induced movementtherapy, without the constraint.72 All of theseinterventions were delivered by a therapist, exceptfor one trial, which consisted of self-initiatedpractice in the home environment, using a bookletof exercises, after instruction by a therapist.69 Ofthe upper limb training trials, all but two52,72 werecarried out 0–6 months post-stroke. Five trials hada total training time of 20 hours or less,50,52,68,70,71
and three trials provided more than 20 hours’total training time.53,69,72 In two of the trialstraining time was additional.69,71 All eight trials with eight intervention–control pairs relevant to this review provided data suitable for pooling.
Eleven of the 19 trials measuring arm or handfunction were CIMT trials with 190 participants.Of these, five trials were of constraint-inducedtherapy,64,73,74,83,84 and six trials were of modifiedconstraint-induced therapy.61,62,79–81,139 All of theinterventions were delivered by a therapist, in one-to-one therapy. Three trials recruited within14 days post-stroke,81,82,84 four trials recruitedbetween 15 days and 6 months post-stroke,61,79,80,83 and four trials recruited after morethan 6 months post-stroke.64,73,74,139 All but twotrials81,82 had a total training time of over20 hours, with the majority providing between 30and 60 hours’ training. In four trials, training timewas additional to the amount of training timeprovided to the comparison group,74,79,80,82 whilein one trial it was unclear whether training timebetween experimental and comparison groups wasequivalent.73 Eight CIMT trials including 151participants in eight intervention–control pairsrelevant to this review provided data suitable forpooling. Pooled results show evidence of a smalleffect (SMD 0.24, 95% CI 0.06 to 0.42).
Seven RFTP trials with 357 participants measuredhand function. There was no statisticallysignificant pooled effect (SMD 0.19, 95% CI –0.03to 0.42).
Five trials (all RTT) with 256 participantsmeasured sitting balance/reach fromsitting.66,68,70,76,77 Of these, two trials were wholetherapy approaches,68,70 while the other threetrials specifically trained sitting balance or reachfrom sitting. All of the interventions were carriedout in the 0–6-month post-stroke period and weredelivered by a therapist in a hospital setting,except for one trial where the intervention wascarried out at home, with people more than 6months post-stroke.66 All of the interventions were20 hours’ training or less. There was no evidencefor impact on sitting balance/reach (SMD 0.23,95% CI –0.05 to 0.50).
Results at follow-up for all upper limb trials to6 months post-therapy were moderate andstatistically significant (SMD 0.55, 95% CI 0.06 to1.04). Evidence for a retention effect at more than6 months post-therapy was unclear (SMD –0.02 to95% CI –0.31 to 0.26), as it was noted that thetrials with 6–12-month follow-up also showed littleor no effect post-treatment.
Treatment effects for upper limb interventionswere not modified by amount/dosage of taskpractice or time since stroke, but were modified bytype of intervention, with RTT showing a smalleffect size just failing to reach significance (SMD0.17, 95% CI –0.03 to 0.36), and CIMT showing alarge, statistically significant effect (SMD 0.77,95% CI 0.26 to 1.29). However, tests for the effectof quality of allocation concealment and trial sizewere also significant, with all of the CIMT trials inboth the inadequate/unclear allocationconcealment subgroup and the small trialssubgroup. This suggests that the results for CIMTtrials could be influenced by quality issues andreporting bias.
Lower limb function/standing balanceSeventeen RFTP trials with 747 participantsmeasured some aspect of lower limb function orstanding balance/reach. Eleven were RTT trialswith 531 participants. Of these, one trial
Health Technology Assessment 2008; Vol. 12: No. 30
51
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Chapter 6
Discussion

specifically trained sit-to-stand movements,65 threetrials trained balance,66,76,77 two trials were wholetherapy approaches,68,70 three trials were circuit-training approaches,50,51,67 and two trials werelower limb task practice mixed in with other formsof mobility exercise.53,78 All interventions weredelivered by a therapist in a hospital orcommunity setting, except for one trial, which wasa home mobility programme, where theparticipant followed videotaped exercise withtherapist telephone contact and follow-up.78 Threeof the interventions were carried out more than6 months post-stroke.51,67,78 Two trials includedmore than 20 hours’ total practice time.53,78 All 11trials had data suitable for pooling. Six of the 17trials were TM trials with 229 participants. Ofthese, two trials were of unsupported TM87,88 andfour trials were of bodyweight supportedTM.63,85,86,89 All interventions were delivered by atherapist in a hospital setting. Two interventionswere carried out more than 6 months post-stroke.87,88 Only one of the trials included morethan 20 hours’ training time.88 Five trials with 199participants provided data suitable for pooling.
Results show large statistically significant effectsfor walking distance (WMD 50.05 m, 95% CI29.65 to 70.44 m; SMD 0.98, 95% CI 0.58 to1.39). In effect, participants in the experimentalgroups could walk on average 50 m further in6 minutes than the control groups. However, therewas some heterogeneity of treatment effects forwalking distance. There were also small statisticallysignificant effects for walking speed (SMD 0.28,95% CI 0.09 to 0.47) and functional ambulation(SMD 0.28, 95% CI 0.05 to 0.51). Trials of RTTshowed a small to moderate effect on sit-to-stand(standardised effect size 0.39, 95% CI 0.18 to0.61), but no evidence of effect on lower limbfunction measures (SMD 0.20, 95% CI –0.10 to0.50) or standing balance/reach (SMD 0.29, 95%CI, –0.06 to 0.63).
Retention effects on lower limbs were small tomoderate and statistically significant up to6 months post-therapy (SMD 0.37, 95% CI 0.05 to0.69), but there was no evidence of an effect atlater than 6 months (SMD –0.01, 95% CI –0.32 to0.29). This difference in retention effects wasborderline statistically significant (p = 0.09).However, few trials had long follow-up and thosethat did tended to show little or no effect post-treatment. Findings are also quite heterogeneous,which suggests that they are inconclusive.
Treatment effects were not modified by amount oftask practice, time since stroke or type of
intervention. Tests for the effect of quality ofallocation concealment were not statisticallysignificant. However, trials with high (>20%) lossto follow-up showed a significantly lower effect ofRFTP than did trials with lower (�20%) loss. Thisis an indication that any bias due to very highdropout is not in favour of RTT, although it wouldbe important in future trials to try to characterisedropouts and attempt to determine their effect onthe effectiveness of RFTP. There was someindication that treatment effects might bemodified by type of comparison group (p = 0.10),with usual care or alternative treatmentcomparisons showing a smaller treatment effectthan attention-control or no-treatmentcomparisons. This suggests that type ofcomparison group should be taken intoconsideration in future analyses.
Global motor functionTwo RTT trials68,70 and one TM trial with datasuitable for pooling88 recruiting 242 participantsin total measured global motor function. Datawere available for 76% (n = 183). There was apooled small to moderate, statistically significanteffect (SMD 0.38, 95% CI 0.09 to 0.68).
ADL functionFive RTT trials and one CIMT trial recruiting atotal of 422 participants used an ADL measure.Outcome data were available for 83% (n = 345).Overall results indicated a small effect size thatwas statistically significant (SMD 0.30, 95% CI0.09 to 0.52).
Adverse eventsTen out of the 31 trials included some report ofadverse events. Of these, seven reported noadverse events. One RTT trial reported a numberof falls occurring during the intervention orevaluation, none of which was serious,51 and oneCIMT trial reported that three participants hadsome discomfort in the unaffected limb, attributedto overuse during the constraint period.73 Theprotocol was subsequently modified. The only trialformally to measure adverse events did not showany significant difference in fall rates between theintervention and control groups.65
Overall completeness andapplicability of evidenceThe included trials were clinically diverse in termsof timing and focus, and there are gaps in theevidence base, particularly for people more than6 months post-stroke. Of the five trials that
Discussion
52

evaluated more than 20 hours’ therapy for upperlimbs in this participant group, only three hadusable data.72–74 Only one trial evaluated 20 hoursor less of upper limb therapy in people at least6 months post-stroke.52
There were only three trials that evaluated up to20 hours of lower limb therapy in people morethan 6 months post-stroke,51,67,87 and two trialsevaluating more than 20 hours of lower limbtherapy in this group.78,88
There have been more trials undertaken withpeople in the 0–6-month post-stroke period, buthere there are also gaps in the evidence base. Ofthe seven trials evaluating upper limb therapy ofmore than 20 hours’ duration, one had dataunsuitable for pooling. Of the remaining six, onewas quasi-experimental, and three had tenparticipants or fewer. While 11 trials haveevaluated 20 hours or less of lower limb therapy,only one trial has evaluated more than 20 hours oflower limb therapy in the 0–6-month post-strokeperiod.
Although it was not possible to classify studies intomore disabled or less disabled participantsubgroups, the tables of included studies(Appendixes 1–3) illustrate the wide range ofdisability levels of the participants in the includedtrials. However, many of the trials had inclusioncriteria specifying either minimum, or minimumand maximum levels of ability, motivation toparticipate and ability to understand instruction.The general evidence provided by the reviewtherefore appears to be widely applicable, perhapswith the exception of very severely disabled peoplewith little postural control or voluntary movement,those with very mild deficits and those with severecommunication difficulties who were excluded bytrialists. The exception to the above may be inCIMT studies, which identified criteria forminimum levels of finger and wrist extension.Treatment effects for CIMT may only beapplicable to a subgroup of participants with adegree of voluntary movement in the hand orarm. There is also the possibility that exclusioncriteria for maximum residual ability reducegeneralisability. The preliminary phase of a CIMTtrial reported that less than 5% of strokeadmissions qualified for randomisation.84
Trials were excluded where repetition appeared tobe primarily for strength or endurance training(e.g. cycling and gait training), or where the typeof training appeared divorced from the functionalaim (e.g. backward walking training, slot machines
and computer games). This may haveconsequences for the applicability of the evidence.The exclusion of trials of what could be defined as‘prefunctional’ types of movement will effectivelyhave excluded a group of people who cannot yetparticipate in functional movement. The sameconsequence applies to the exclusion of trials witha large element of passive and active assistedmovement.
In terms of generalisability to the UK, only RTT-type interventions have been evaluated in thissetting. One trial is a whole therapy approach,70
one trial evaluates balance training77 and onequasi-experimental trial evaluated self-deliveredexercise in the home environment.69 RTT has nottraditionally been a significant part of therapy afterstroke in the UK, which has been dominated bythe Bobath approach. This specifically minimisesrepetitive active movement, and relies ontherapist-guided restoration of ‘normal movement’patterns, rather than the functional but unnaturalones that could occur as a result of the morepragmatic approach within RFTP. Many studies inthis review were from outside the UK, or usedtherapy approaches that have been less popular,such as motor learning. While clinical experiencesuggests that modern UK stroke units have a moreeclectic therapy approach, it may take longer forthe results to change practice within the UK thanin countries that already use RFTP routinely.
There are no published trials of either CIMT orTM in a UK setting. While all of the interventionsare likely to be transferable in principle, theireffectiveness against other forms of care usual inthe UK and their acceptability in this healthcaresetting have not been tested. In particular, thefeasibility and acceptability of CIMT and circuit-training interventions delivered in communitysettings would need to be evaluated. The intensityof CIMT and the delivery of interventions afterthe normal rehabilitation period representadditional periods of treatment to those currentlyprovided.
The acceptability and safety of the different formsof RFTP to all types of participants are alsounclear. While there were few adverse effectsreported overall, the lack of formal reporting inmany trials means that this finding is inconclusive.Of the information provided about reasons fordropouts in the trials, the most frequent cause wasphysical illness, and only a very small proportionof those participating dropped out for physicalreasons that might have been related to theintervention. However, there was also a small
Health Technology Assessment 2008; Vol. 12: No. 30
53
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

number of participants who were lost to follow-upfor reasons related to compliance or treatmentpreference. In the CIMT trials in particular,relatively long periods of constraint and intensiveperiods of practice with the affected limb have thepotential to impact on acceptability, althoughnone of the trials reported problems.
Information about recruitment was not oftenprovided, but of those that did provide information,a trial recruiting in hospital in the earlyrehabilitation period had relatively low numbers ofrefusal to participate (e.g. Kwakkel53 had four outof 101 people who did not give consent), while atrial recruiting in the community after rehabilitationhad high numbers of refusal of the intervention(e.g. Salbach51 had 73% refusal). It may be thatsome forms of intervention are less acceptable, orthat interventions only appeal to a subset of strokesurvivors, particularly if travel is involved.
No conclusions could be reached about the impactof numbers of repetitions as a measure of theintensity of practice, as this information was onlyprovided in one or two trials. The amount of taskpractice is therefore a measure of the duration (i.e.time spent).
By virtue of its focus on functional movement, thisreview does not consider the evidence forelectronic forms of delivery of repetitivemovement such as robotics or computer-mediatedpractice. The authors were also unable tocomment on the implications of different sites oftreatment, therapist-delivered versus self-deliveredinterventions or group versus individual delivery,as there were too few trials for comparison.However, the presence of two trials involving self-delivery in the home environment and four trialsinvolving group delivery of task-specific trainingsuggests that these modes of delivery are feasible,and further ongoing trials should provide moreinformation. The studies that collectedinformation showed generally high levels ofsatisfaction with the programme. Attendance levelsat community programmes were also very good,suggesting that training programmes were wellreceived by those who chose to participate.
Quality of evidenceFor lower limb trials, Salbach and colleagues51
estimate that a sample size of 60 would berequired to detect a group difference of 28 m inaverage change in the 6WMT (type I error = 0.05,type II error = 0.10, expected dropout rate of
10%) based on the results of a pilot study67 whichrecruited 91 patients. Five of the 17 trials of lowerlimb interventions had sample sizes above 60 (fourRTT, one TM). For upper limb trials, the sameresearch group estimated that a sample size of 60participants was required to detect a clinicallymeaningful difference for the BBT.52 Of the 19trials of upper limb interventions, five trials hadsample sizes greater than 60 (five RTT). No CIMTtrial had more than 25 participants.
Two-thirds of RTT trials had adequate allocationconcealment and most of the trials stated thatblinded independent assessors were used. Therapytime was non-equivalent in two trials. For TM, two out of five trials with data included in themeta-analysis described adequate allocationconcealment methods, blinding of outcomeassessors was attempted in three trials, and alltrials provided equivalent therapy time toexperimental and comparison groups. Only fourtrials (two RTT, one CIMT, one TM) had over 20%dropout. For CIMT, three trials provided dataunsuitable for pooling; and all of the CIMT trialshad unclear allocation concealment.
The overall quality of the included trials providesa degree of confidence in the pooled results forRTT and TM, although there were only five TMtrials with data suitable for pooling from 199participants. The results for CIMT have to beconsidered in the light of small size of the trials,together with the confounding effects of theselection of trials with non-equivalent therapy timein the experimental and control groups (i.e. no-treatment control groups). A number of CIMTtrials did include comparison groups who receivedtherapy with no constraint, but these wereintervention–control pairs that could not be usedfor this review as the comparison was alsorepetitive task practice. The use of no-treatmentcontrol comparison may lead to a differentconclusion from other reviews of CIMT. Three outof eight included CIMT trials compared theintervention against no therapy. This may explainthe large effect of the intervention on upper limbfunction, as the differential between these groupsmay be larger than would be expected bycomparing the intervention against usual care oranother intervention, such as bimanual training.
Non-reporting bias also has to be considered.Subgroup analysis for trial size and the funnel plotfor upper limb interventions suggested greatereffects for smaller trials, suggesting an absence ofsmall, negative trials. This might have led to smallor negative effect estimates not being included
Discussion
54
and, in particular, an ‘unbalancing’ due to the fourtrials with large effects.
Potential limitations in the reviewprocessThis review combined the results of trials of RTTwith results from trials of enhanced forms of RTT,namely TM and CIMT. Care must therefore betaken regarding attribution of pooled treatmenteffects solely to the task practice component. Forthis reason, both separate and pooled results areshown. This study also generally used fixed-effectanalyses, which some might criticise owing to thepresence of some clinical heterogeneity in thetreatments and trials combined. Many of the trialsoriginally reported data in median andinterquartile ranges. In addition, many of theoutcomes are measured on scales that are shortand bounded, where the use of means andstandard deviations can be misleading. However,the effect size for RFTP is greatest for walkingdistance, which is a truly quantitative measure. Itis also relatively consistent across other outcomes,including walking speed which is, like walkingdistance, a continuous measure with essentially nostrict upper bound. This would tend to indicatethat the use of means and standard deviations forshort, bounded, ordinal scales has notsubstantively affected the conclusions, at least forthe lower limb outcomes.
The major focus in this review was impact on task-specific function. In practice, a large number ofstudies was excluded on the basis that thereviewers did not judge the outcomes to befunctional or the intervention to be task specific.Studies were also included where the reviewers’interpretation of the intervention was thatrepetition of functional movement was a majormechanism of action, even when this was notexplicitly stated by the authors (e.g. de Sèze76).Whether balance training is truly ‘functional’ isalso a matter of interpretation, but its inclusionwas felt to be important so as not unintentionallyto exclude RFTP training for people with moresevere levels of disability, where the recovery ofbalance is a prerequisite of functional activity.
As CIMT and TM trials were sourced fromexisting reviews, trials with alternative or no-treatment comparisons were included. Two TMtrials included comparisons against alternativeforms of treatment, which is potentially likely tohave resulted in lower estimates of effect thancomparison against usual care; subgroup analysis
for type of comparison group was close tostatistical significance, with a lower effect estimatefor the usual care/alternative treatment than forthe attention-control/no-treatment comparisonsubgroup. Three CIMT trials included comparisonagainst a no-treatment group, with the potential toresult in greater estimates of effect thancomparison against usual care. However, analysisof the impact of comparison group provided noevidence of any difference between the effects inthe two subgroups.
Agreement or disagreement withprevious reviewsAll of the studies included in this review have acore component of repeated, task-specific practice,but they are also very diverse. The CIMT and TMcomponents of the review were subsets of existingreviews.20,23 While combining the results from sucha diverse group of studies has potential dangers,the summary finding of a pooled moderate impacton functional ability (SMD 0.34, 95% CI 0.19 to0.48) supports previous authors who havesuggested a focus on the efficacy of task-specifictreatments.14,34
Whether functional gain can be attributed to taskspecificity or repeated practice is unclear and anyattribution is highly speculative. This review didnot find a significant difference in treatment effectdependent on the amount of practice for lowerlimb interventions. Conversely, the greatest gainsfor lower limbs were seen in walking distance,while gains for walking speed were of a smallermagnitude, suggesting that an endurance trainingelement contained in repeated motor practicemakes some contribution to impact. In addition,this review could not take into account thepretherapy ability levels of the participants, and itmay also be that the mechanisms of repetition andtask specificity have different roles at differentstages of recovery. Repetition is the majormechanism of action of robotics, and a recentreview has shown impact at the level ofimpairment, but not for functional ability.36
For upper limb interventions, five out of eightCIMT studies with data suitable for poolingprovided more than 20 hours of therapy. Althoughthe overall difference between smaller and largeramounts of task practice was not statisticallysignificant, there was potential evidence of a trend(p = 0.18) towards larger effect sizes for more than20 hours’ practice (SMD 0.42, 95% CI 0.10 to0.75) versus 0–20 hours’ practice (SMD 0.22,
Health Technology Assessment 2008; Vol. 12: No. 30
55
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

95% CI –0.12 to 0.57) for arm function. Thisfinding is consistent with other reviews that havesuggested that upper limb recovery may requireintensive intervention.16
Overall for RFTP, there were small to moderateeffects for ADLs and global motor function, and asmall effect on functional ambulation classification.Even though the amount of change for theseoutcomes is modest, the clinical benefits are likelyto be meaningful in relation to quality of life.136
In those studies that did show a benefit andprovided later assessments, improvements at theend of training were not evident at the later stage.It is unclear from this review whether this isrelated to characteristics of the participants, theintensity of training or the degree of improvementrequired before detectable change was noted.
Evidence from RFTP interventions does notconcur with the suggestion that earlier provisionof treatment results in greater functionalimprovement, as treatment effects were notmodified by time since stroke. Improvement infunction was possible even in the later stages ofrecovery.139 A recent review concluded that it wassurprising that CIMT should work in the chronicphase of stroke, but agreed that the trial andlaboratory evidence suggested that this was thecase. However, they concluded that teachingbimanual activities rather than constraint mightcreate the same outcome.140
The authors were unable to come to anyconclusions about the previously identifieddose–response relationship between amount oftherapy and improved outcome,15 but the resultsfrom subgroup analysis suggest this as a priorityfor further research.
Economic analysisThe base-case analysis suggested that RFTP iscost-effective. This analysis is based on a numberof assumptions about therapeutic inputs that hadto be made because of the paucity of economicdata associated with the individual trials.Furthermore, in calculating cost-effectiveness theauthors had to estimate the potential impact ofRFTP on pre-existing longitudinal data. To allowfor these assumptions their magnitude was variedin sensitivity analysis. The sensitivity analysestended to find that RFTP was cost-effectiveoverall, and in particular on the outcomemeasures of walking distance and sit-to-stand.
The existing data set used to estimate the impactof RFTP was appropriate to the study’s needsbecause it reflected the normal course of recoveryafter stroke in a cohort of patients that had beensystematically identified. The disadvantage ofusing this data set was that the analysis was basedaround predetermined data, which did notspecifically lend itself to assessing the impact ofRFTP. However, the existing data did allowreasonable assumptions to be made about howRFTP may have affected outcomes and costs, andmeant that the research team did not have to waitfor 3 years to collect data on resource use andoutcomes in a UK post-stroke population.
One of the costs from the existing data set thatcould have been included was the cost incurredthrough residence in institutions. These costs tendto be high and would most likely be important inpatients with more severe disability. Not includingthe cost of residence in institutions means that thecosts of these severe states are likely to have beenunderestimated. Evidence from this reviewsuggested that RFTP reduced disability. Therefore,by excluding the high severe state costs due toinstitutionalisation, the review is likely to haveunderestimated the potential savings andconsequently the cost-effectiveness of RFTP.
Translation of the potential effect of RFTP on thepatients in the data set made an assumption aboutthe relationship between the effect size and the BI.This assumption was based around the size of thestandard deviation in rehabilitation trials. Theassumption that the standard deviation was about5 is consistent with published data.53,68,141–143
Furthermore, in this systematic review the effect ofRFTP on ADLs resulted in an SMD of 0.30. Thiswould suggest that the assumption about therelationship between the SMD and the BI was, ifanything, a conservative one, therefore, it is likelythat the cost-effectiveness of RFTP has beenunderestimated.
A further assumption was then made about therelationship between the BI and the EQ-5D. Thisassumption allowed the calculation of ICER perQALY gained. The systematic review showed thatnone of the studies used the EQ-5D and only one65
used a measure of quality of life (not includinghealth status) as an outcome. It therefore seemedunreasonable to generate an effect size for qualityof life, based on one study. Consequently, thismakes it difficult to compare directly therelationship between RFTP and quality of life, andsuggests that future RFTP studies should use aquality of life measure as an outcome.
Discussion
56

To test the assumptions that were made about therelationships between the effect size, the BI andQALYs, sensitivity analyses were performed. Theseanalyses explored what would happen if theimpact of RFTP on outcome was less than in thebase model. For the assumptions made, the costper QALY gained was more sensitive to variationsbetween the effect size and the BI than tovariations between the BI and the EQ-5D. Overall,the cost per QALY gained for walking distance didnot rise much above £20,000, except for one ofthe assumptions made in the sensitivity analysis.This means that even when the assumptions arestacked against RFTP, this intervention stilldemonstrates cost-effectiveness.
The estimation of the cost of providing RFTP inthe trials was complicated for a number of reasons.Many of the trials were not conducted in the UK,so it was difficult to cost some items of equipment.The grade of staff performing the training was notoften reported; this was further compounded bythe trials not being UK based. In addition,because the individual trials had not specificallyrecorded resource-use data, no information wasavailable about the impact of RFTP on futuretherapy, support services or provision of mobilityaids. Moreover, there were no consistent dataabout adverse events, which would have thepotential to increase costs through patientsattending clinics or being admitted to hospital. Inone study87 some patients were transported tohospital at the expense of the researcher; for allother studies post discharge, patients made theirown way to clinics. It is likely that this cost wasincurred because the intervention was being usedin the context of a research study rather thannormal clinical practice. Furthermore, if RFTP wasintroduced as a rehabilitation therapy it is unlikelythat it would incur major direct costs for patienttransport. For this reason the cost of this transportwas not included as a source of cost for RFTP.Given the lack of associated economic data, thecosting of RFTP was a fair reflection of the directcosts incurred by this intervention.
The systematic review revealed the complex natureof RFTP in terms of what is being delivered as wellas when (after stroke), where and how it isdelivered. This provided a challenge formodelling the cost-effectiveness of thisintervention. It was therefore decided that ratherthan develop a complex model, the modellingshould be kept simple and transparent. As a resultof this decision the reviewers considered howRFTP might influence 3-year costs by looking at
the potential impact on the 3-year BI. It is self-evident that to have a 3-year BI a patient must bealive; this meant that the estimate did not takeinto account the possibility that a patient who hadRFTP died within the 3-year period, which mayhave impacted on the cost. A further analysis wassubsequently performed that examined how theimpact of RFTP on the 3-month BI would affectcost at 3 years, i.e. this analysis included peoplealive at 3 months, some of whom had died by3 years. It was found that the magnitude of thepotential cost saving was similar whether the 3-month or 3-year BI scores were used.
To make the modelling feasible a number of otherassumptions had to be made. The costing of usualcare went from discharge to 3 years post-stroke,which makes the assumption that the cost over3 years would be the same whenever RFTP wasstarted. Another related assumption was that theeffect of RFTP is constant over time. It isacknowledged that these assumptions are rathergeneral. However, given the complex nature of theintervention, described in the previous paragraph,and the lack of economic data about theintervention and its likely impact on cost, theauthors believe that these assumptions provided areasonable estimate.
In summary, the systematic review was able tocombine the results from different studies andprovide an overall effect size for RFTP. The lack ofeconomic data associated with the existing studiesmeant that an economic model had to bedeveloped to estimate the potential cost-effectiveness of RFTP. The modelling had theadvantage of using effect sizes from a largesample; the disadvantage was that it relied on pre-existing data. This meant that the modelling thatwas performed relied on a number of assumptionsabout costs and effectiveness. The assumptionsthat were made were generally weighted againstRFTP. Despite these assumptions, RFTPdemonstrated that it was cost-effective.
To combat the issues around measures of costs andeffectiveness, future trials need to be sufficientlypowered to detect the effectiveness of bothfunctional and economic outcomes. Furthermore,trials need to decide a priori what resources tocost; because the effects of RFTP are likely toextend beyond its impact on direct costs futuretrials should also consider indirect and possiblyintangible costs. Economic analysis would befacilitated further by including quality of life as anoutcome measure.
Health Technology Assessment 2008; Vol. 12: No. 30
57
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.


Implications for practiceThe results of this review provide sufficientevidence to validate the general principle thatRFTP for lower limbs can result in functional gain,when compared against other forms of usual careor attention-control. While functional gain overallis modest, impact does appear to be of a clinicallymeaningful magnitude. It is, however, unclear asto whether effects are sustained over 6 monthspost-therapy.
There is insufficient evidence to make anyrecommendations for upper limb interventions.Although effects of RFTP on arm function werestatistically significant, the variable quality of theevidence and the clinical heterogeneity of theinterventions mean that further research is neededbefore specific recommendations can be made.
Some caution is needed in interpreting the lack ofevidence for adverse effects, as few trialsspecifically monitored these as an outcome. Iftask-specific training is used in clinical practice,adverse effects should be monitored.
While the overall effectiveness of RFTP isrelatively modest, this sort of intervention appearsto be cost-effective, primarily because theintervention itself has a relatively small cost.
Recommendations for futureresearchThere is a large number of ongoing trials in thisarea. The first recommendation is that this review isupdated within 2 years. The updated review shouldalso consider any potential interaction effectsbetween type of training, amount of task practiceand stroke-related impairments. This reviewfocused initially on the evidence for the efficacy ofRFTP versus usual care or attention-controlcomparisons. Any future review should includecomparison of RFTP against alternative forms oftherapy, such as strength and stamina training.
Further well-designed, adequately powered trialsevaluating the impact of upper limb interventions,and in particular CIMT, are needed. One trial waspublished shortly after the closing date for this
review, and should provide more information onefficacy. Future CIMT trials should also target andmeasure hand function.
There were insufficient trials included in thisreview to evaluate the efficacy and cost-effectiveness of different intervention deliverymethods for RFTP, such as group training, deliveryby assistants or practice in the home environment.Further research should address practical and cost-effective ways of delivering such interventions. Inparticular, the acceptability of CIMT and of circuit-training-type interventions delivered in communitysettings would need to be evaluated.
The existence of retention effects up to 6 monthspost-therapy is a promising finding, and furtherresearch should be directed towards evaluatinglong-term functional gain by routine inclusion oflonger follow-up periods of 1 or possibly 2 years.Suitable methods to maintain functional gainshould also be investigated.
Future trials need to be designed to take accountof the following:
● This study was unable to investigate the impactof training on people with different levels of pre-intervention disability, because of the widerange of baseline measures used. Analyses of thistype would be facilitated by the inclusion in trialsof baseline data using a common measure suchas the BI, which can be related to populationnorms dependent on time since stroke.
● Monitoring and reporting of adverse effectsshould be explicitly included.
● When designing future trials of any type ofRFTP it is critical that the study is powered todetect not only a clinical effect, but also whetherit is cost-effective.
● Future studies need to identify clearly whichresources are likely to be affected by RFTP andensure that they are included in any economicanalysis. In addition, studies should include aquality of life measure as one of the outcomesto facilitate economic analysis.
● The benefit of RFTP may not be clear fromdirect costs alone; therefore, future studiesshould include indirect costs and give someconsideration to the inclusion of intangible costs.
Health Technology Assessment 2008; Vol. 12: No. 30
59
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Chapter 7
Conclusions


We wish to acknowledge the help and supportof Brenda Thomas and Hazel Fraser from
the Cochrane Stroke Group, for their help in thereview process. We would also like to thank all ofthe trial authors who kindly replied to ourrequests for information, and our translators: Jie Shen, Dr Qinghai Huang, Hua Zhang,Gediminas Juaga and Luyan Fang.
Contribution of authorsBeverley French (Senior Research Fellow,University of Central Lancashire) led thesystematic review, including coordinating thereview process, managing searching and main datainput and drafting the final report. MichaelLeathley (Postdoctoral Research Fellow, Universityof Central Lancashire) led the cost-effectivenesscomponent of the review, and contributed to dataextraction and appraisal for the review.Christopher Sutton (Senior Lecturer, University ofCentral Lancashire) provided statistical expertiseto the review and cost-effectiveness analysis.Joanna McAdam (Research Coordinator,University of Central Lancashire) managed the
TM component of the review, was responsible foradministration of the review process andcontributed to data extraction and appraisal andto drafting the final report. Lois Thomas (SeniorResearch Fellow, University of Central Lancashire)managed the CIMT component of the review andcontributed to data extraction and appraisal, andto drafting the final report. Anne Forster (Reader,Elderly Care, University of Leeds), PeterLanghorne (Professor of Stroke Care, University ofGlasgow) and Christopher Price (Clinical SeniorLecturer/Consultant Physician, NorthumbriaHealthcare NHS Trust) directed the review focusand quality, and undertook critical reading ofoutputs. Andrew Walker (Senior Lecturer inHealth Economics, University of Glasgow) directedthe focus and quality of the cost-effectivenesscomponent of the review. Caroline Watkins(Professor of Stroke and Older People’s Care,University of Central Lancashire) was leadinvestigator for the project, responsible formanaging the overall review process and quality ofoutputs.
Health Technology Assessment 2008; Vol. 12: No. 30
61
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Acknowledgements

1. Department of Health. National service frameworkfor older people. London: Department of Health;2001.
2. Adamson J, Beswick A, Ebrahim S. Is stroke themost common cause of disability? J StrokeCerebrovasc Dis 2004;13:171–7.
3. Wolfe CD. The impact of stroke. Br Med Bull2000;56:275–86.
4. Lawrence ES, Coshall C, Dundas R, Stewart J,Rudd AG, Howard R. Estimates of the prevalenceof acute stroke impairments and disability in amulti-ethnic population. Stroke 2001;32:1279–84.
5. Wade DT, Langton-Hewer R. Functional abilitiesafter stroke: measurement, natural history andprognosis. J Neurol Neurosurg Psychiatry 1987;50:177–82.
6. Wade DT, Langton-Hewer R, Wood VA, Skilbeck CE, Ismail HM. The hemiplegic armafter stroke: measurement and recovery. J NeurolNeurosurg Psychiatry 1983;46:521–4.
7. Heller A, Wade DT, Wood VA, Sunderland A,Hewer RL, Ward E. Arm function after stroke:measurement and recovery over the first threemonths. J Neurol Neurosurg Psychiatry 1987;50:714–19.
8. Sunderland A, Tinson D, Bradley L, Hewer RL.Arm function after stroke. An evaluation of gripstrength as a measure of recovery and a prognosticindicator. J Neurol Neurosurg Psychiatry1989;52:1267–72.
9. Nakayama H, Jorgensen HS, Raaschou HO,Olsen TS. Recovery of upper extremity function instroke patients: the Copenhagen study. Arch PhysMed Rehabil 1994;75:852–7.
10. Lord S, McPherson K, McNaughton H, Rochester L, Weatherall M. Communityambulation after stroke: how important andobtainable is it and what measures appearpredictive? Arch Phys Med Rehabil 2004;85:234–9.
11. Hendricks HT, van Limbeek J, Geurts AC, Zwarts MJ. Motor recovery after stroke: asystematic review of the literature. Arch Phys MedRehabil 2002;83:1629–37.
12. Intercollegiate Working Party for Stroke. NationalClinical Guidelines for Stroke. London: Royal Collegeof Physicians; 2004.
13. Youman P, Wilson K, Harraf F, Kalra L. The economic burden of stroke in the United
Kingdom. Pharmacoeconomics 2003;21(Suppl 1):43–50.
14. Van Peppen RPS, Kwakkel G, Wood-Dauphinee S,Hendriks HJM, van der Wees PJ, Dekker J. Theimpact of physical therapy on functional outcomesafter stroke: what’s the evidence? Clin Rehabil2004;18:833–62.
15. Kwakkel G, van Peppen R, Wagenaar RC,Dauphinee SW, Richards C, Ashburn A. Effects ofaugmented exercise therapy time after stroke – a meta-analysis. Stroke 2004;35:2529–36.
16. Van der Lee JH, Snels IA, Beckerman H,Lankhorst GJ, Wagenaar RC, Bouter LM. Exercise therapy for arm function in strokepatients: a systematic review of randomizedcontrolled trials. Clin Rehabil 2001;15:20–31.
17. Dobkin BH. Strategies for stroke rehabilitation.Lancet Neurol 2004;3:528–36.
18. Carr J, Shepherd R. A motor relearning programmefor stroke. Oxford: Butterworth Heinemann; 1987.
19. Wolf SL, Blanton S, Baer H, Breshears J, Butler AJ. Repetitive task practice: a critical reviewof constraint-induced movement therapy in stroke.Neurologist 2002;8:325–38.
20. Moseley AM, Stark A, Cameron ID, Pollock A.Treadmill training and body weight support forwalking after stroke. Cochrane Database Syst Rev2005 (Issue 4). Art. No. CD002840. DOI10.1002/14651858.
21. Hesse S. Rehabilitation of gait after stroke –evaluation, principles of therapy, novel treatmentapproaches, and assistive devices. Top GeriatrRehabil 2003;19:109–26.
22. Volpe BT, Krebs HI, Hogan N. Is robot-aidedsensorimotor training in stroke rehabilitation arealistic option? Curr Opin Neurol 2001;14:745–52.
23. Hakkenes S, Keating JL. Constraint-inducedmovement therapy following stroke: a systematicreview of randomised controlled trials. Aust JPhysiother 2005;51:221–31.
24. Barreca S, Wolf SL, Fasoli S, Bohannon R.Treatment interventions for the paretic limb ofstroke survivors: a critical review. NeurorehabilNeural Repair 2003;17:220–6.
25. Cifu DX, Stewart DG. Factors affecting functionaloutcome after stroke: a critical review ofrehabilitation interventions. Arch Phys Med Rehabil1999;80:S35–9.
Health Technology Assessment 2008; Vol. 12: No. 30
63
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
References
26. Drukker M, de Bie RA, van Rossum E. The effectsof exercise training in institutionalised elderlypeople: a systematic review. Phys Ther Rev2001;6:273–85.
27. Duncan PW. Synthesis of intervention trials toimprove motor recovery following stroke. TopStroke Rehabil 1997;3:1–20.
28. Hiraoka K. Rehabilitation effort to improve upperextremity function in post-stroke patients: a meta-analysis. J Phys Ther Sci 2001;13:5–9.
29. Kwakkel G, Wagenaar RC, Koelman TW,Lankhorst GJ, Koetsier JC. Effects of intensity ofrehabilitation after stroke. Stroke 1997;28:1550–6.
30. Legg L, Drummond AE, Langhorne P.Occupational therapy for patients with problemsin activities of daily living after stroke. CochraneDatabase Syst Rev 2006 (Issue 4). Art. No.CD003585. DOI 10.1002/14651858.
31. Ma H, Trombly CA. A synthesis of the effects ofoccupational therapy for persons with stroke, Part II: Remediation of impairment. Am J OccupTher 2002;56:260–74.
32. Meek C, Pollock A, Potter J, Langhorne P.A systematic review of exercise trials post-stroke.Clin Rehabil 2003;17:6–13.
33. Ottenbacher KJ, Jannell S. The results of clinicaltrials in stroke rehabilitation research. Arch Neurol1993;50:37–44.
34. Pollock A, Baer G, Pomeroy V, Langhorne P.Physiotherapy treatment approaches for therecovery of postural control and lower limbfunction following stroke. Cochrane Database SystRev 2003 (Issue 2). Art. No. CD001920. DOI10.1002/14651858.
35. OST (Outpatient Service Trialists). Therapy basedrehabilitation services for stroke patients at home.Cochrane Database Syst Rev 2003 (Issue 1). Art. No.CD002925. DOI 10.1002/14651858.
36. Prange GB, Jannink MJA, Groothuis-Oudshoorn CGM, Hermens HJ,Ijzerman M. Systematic review of the effect ofrobot-aided therapy on recovery of thehemiparetic arm after stroke. J Rehabil Res Dev2006;43:171–84.
37. Saunders DH, Greig CA, Young A, Mead GE.Physical fitness training for stroke patients.Cochrane Database Syst Rev 2004 (Issue 1). Art. No.CD003316. DOI 10.1002/14651858.
38. Smidt N, de Vet HCW, Bouter LM, Dekker J.Effectiveness of exercise therapy: a best-evidencesummary of systematic reviews. Aust J Physiother2005;51:71–85.
39. Steultjens EMJ, Dekker J, Bouter LM, van de Nes JCM, Cup EHC, van den Ende CHM.Occupational therapy for stroke patients: a systematic review. Stroke 2003;34:676–87.
40. Steultjens EMJ, Dekker J, Bouter LM, Leemrijse CJ, van den Ende CHM. Evidence ofthe efficacy of occupational therapy in differentconditions: an overview of systematic reviews. Clin Rehabil 2005;19:247–54.
41. Stewart KC, Cauraugh JH, Summers JJ. Bilateralmovement training and stroke rehabilitation. J Neurol Sci 2006;244:89–95.
42. Teasell RW, Bhogal SK, Foley NC, Speechley MR.Gait retraining post stroke. Top Stroke Rehabil2003;10:34–65.
43. Trombly CA, Ma H. A synthesis of the effects ofoccupational therapy for persons with stroke, Part1: Restoration of roles, tasks, and activities. Am JOccup Ther 2002;56:250–9.
44. Van Dijk H, Hermens HJ. Distance training forthe restoration of motor function. J Telemed Telecare2004;10:63–71.
45. Walker MF, Leonardi-Bee J, Bath P, Langhorne P,Dewey M, Corr S. Individual patient data meta-analysis of randomized controlled trials ofcommunity occupational therapy for strokepatients. Stroke 2004;35:2226–32.
46. Bayona NA, Bitensky J, Salter K, Teasell R. The role of task specific training in rehabilitationtherapies. Top Stroke Rehabil 2005;12(3):58–65.
47. Carr J, Shepherd R. Neurological rehabilitation:optimizing motor performance. Edinburgh:Butterworth Heinemann; 1998.
48. Carr JH, Shepherd RB. Movement science:foundations of physical therapy in rehabilitation.Gaithersburg, MD: Aspen; 2000.
49. World Health Organisation Task Force on Strokeand Other Cerebrovascular Disorders.Recommendations on stroke prevention, diagnosis,and therapy: report of the WHO Task Force onStroke and Other Cerebrovascular Disorders. Stroke1989;20:1407–31.
50. Blennerhassett J, Dite W. Additional task-relatedpractice improves mobility and upper limbfunction early after stroke: a randomisedcontrolled trial. Aust J Physiother 2004;50:219–24.
51. Salbach NM, Mayo NE, Wood-Dauphinee S,Hanley JA, Richards CL, Côte R. A task-orientatedintervention enhances walking distance and speedin the first year post stroke: a randomizedcontrolled trial. Clin Rehabil 2004;18:509–19.
52. Higgins J, Salbach NM, Wood-Dauphinee S,Richards CL, Côté R, Mayo NE. The effect of atask oriented intervention on arm function inpeople with stroke: a randomized controlled trial.Clin Rehabil 2006;20:296–310.
53. Kwakkel G, Wagenaar RC, Twisk JWR, Langhorst GJ, Koetsier JC. Intensity of leg andarm training after primary middle-cerebral-arterystroke: a randomised trial. Lancet 1999;354:191–6.
References
64

54. Deeks JJ, Altman DG, Bradburn MJ. Statisticalmethods for examining heterogeneity andcombining results from several studies in meta-analysis. In Egger M, Davey Smith G, Altman DG,editors. Systematic review in health care: meta-analysisin context. London: BMJ Publishing; 2001.
55. Royal College of Physicians. National sentinel strokeaudit. London: Clinical Effectiveness andEvaluation Unit, Royal College of Physicians;2006.
56. Mehrholz J, Wagner K, Rutte K, Meisner D, Pohl M. Predictive validity and responsiveness ofthe functional ambulation category in hemipareticpatients after stroke. Arch Phys Med Rehabil 2007;88:1314–19.
57. Hsieh CL, Hsueh IP, Chiang FM, Lin PH. Inter-rater reliability and validity of the ActionResearch arm test in stroke patients. Age Ageing1998;27:107–13.
58. Hsueh IP, Hsieh CH. Responsiveness of two upperextremity function instruments for strokeinpatients receiving rehabilitation. Clin Rehabil2002;16:617–24.
59. Platz T, Pinowski C, van Wijck F, Kim IH,di Bella P, Johnson G. Reliability and validity ofarm function assessment with standardizedguidelines for the Fugl–Meyer Test, ActionResearch Arm Test and Box and Block Test: a multicentre study. Clin Rehabil 2005;19:404–11.
60. Wolf SL. The EXCITE Trial: attributes of the WolfMotor Function Test in patients with subacutestroke. Neurorehabil Neural Repair 2005;19:194–205.
61. Page SJ, Sisto S, Johnston MV, Levine P. Modifiedconstraint-induced therapy after subacute stroke: a preliminary study. Neurorehabil Neural Repair2002;16:290–5.
62. Page SJ, Sisto S, Levine P, McGrath RE. Efficacy ofmodified constraint-induced movement therapy inchronic stroke: a single-blinded randomizedcontrolled trial. Arch Phys Med Rehabil 2004;85:14–18.
63. Scheidtmann K, Brunner H, Muller F, Weinandy-Trapp M, Wulf D, Koenig E. Treadmilltraining in early poststroke patients – do timingand walking ability matter? [German]. Neurologieund Rehabilitation 1999;5:198–202.
64. Suputtitada A, Suwanwela NC, Tumvitee S.Effectiveness of constraint-induced movementtherapy in chronic stroke patients. J Med Assoc Thai2004;87:1482–90.
65. Barreca S, Sigouin CS, Lambert C, Ansley B.Effects of extra training on the ability of strokesurvivors to perform an independent sit-to stand:a randomized controlled trial. J Geriatr Phys Ther2004;27:59–64.
66. Dean CM, Shepherd RB. Task-related trainingimproves performance of seated reaching tasksafter stroke. Stroke 1997;28:722–8.
67. Dean CM, Richards CL, Malouin F. Task-relatedcircuit training improves performance oflocomotor tasks in chronic stroke: a randomized,controlled pilot trial. Arch Phys Med Rehabil2000;81:409–17.
68. Langhammer B, Stanghelle JK. Bobath or MotorRelearning Programme? A comparison of twodifferent approaches of physiotherapy in strokerehabilitation: a randomized controlled study. ClinRehabil 2000;14:361–9.
69. Turton A, Fraser C. The use of home therapyprogrammes for improving recovery of the upperlimb following stroke. Br J Occup Ther 1990;53:457–62.
70. Van Vliet PM, Lincoln NB, Foxall A. Comparisonof Bobath based and movement science basedtreatment for stroke: a randomised controlledtrial. J Neurol Neurosurg Psychiatry 2005;76:503–8.
71. Winstein CJ, Rose DK, Tan SM, Lewthwaite R,Chui HC, Azen SP. A randomized controlledcomparison of upper-extremity rehabilitationstrategies in acute stroke: a pilot study ofimmediate and long-term outcomes. Arch Phys MedRehabil 2004;85:620–8.
72. Yen JG, Wang RY, Chen HH, Hong CT.Effectiveness of modified constraint-inducedmovement therapy on upper limb function instroke subjects. Acta Neurol Taiwan 2005;14:16–20.
73. Taub E, Miller NE, Novack TA, Cook EW,Fleming WC, Nepomuceno CS, et al. Technique toimprove chronic motor deficit after stroke. ArchPhys Med Rehabil 1993;74:347–54.
74. Wittenberg GF, Chen R, Ishii K, Bushara KO,Eckloff S, Croarkin E, et al. Constraint-inducedtherapy in stroke: magnetic-stimulation motormaps and cerebral activation. Neurorehabil NeuralRepair 2003;17:48–57.
75. Wolf SL, Winstein CJ, Miller JP, Taub E,Uswatte G, Morris D, et al. Effect of constraint-induced movement therapy on upper extremityfunction 3 to 9 months after stroke: the EXCITErandomized clinical trial. JAMA 2006;296:2095–104.
76. de Sèze M, Wiart L, Bon-Saint-Côme A, Debelleix X, de Sèze M, Joseph P, et al.Rehabilitation of postural disturbances ofhemiplegic patients by using trunk controlretraining during exploratory exercises. Arch PhysMed Rehabil 2001;82:793–800.
77. Howe TE, Taylor I, Finn P, Jones H. Lateral weighttransference exercises following acute stroke: apreliminary study of clinical effectiveness. ClinRehabil 2005;19:45–53.
Health Technology Assessment 2008; Vol. 12: No. 30
65
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
78. McClellan R, Ada L. A six week, resource-efficientmobility program after discharge fromrehabilitation improves standing in peopleaffected by stroke: placebo-controlled, randomisedtrial. Aust J Physiother 2004;50:163–7.
79. Atteya AA. Effects of modified constraint inducedtherapy on upper limb function in subacute strokepatients. Neurosciences 2004;9:24–9.
80. Page SJ, Sisto SA, Levine P, Johnston MV, Hughes M. Modified constraint induced therapy: a randomized feasibility and efficacy study. J Rehabil Res Dev 2001;38:583–90.
81. Dromerick AW, Edwards DF, Hahn M. Does theapplication of constraint-induced movementtherapy during acute rehabilitation reduce armimpairment after ischemic stroke? Stroke2000;31:2984–8.
82. Page SJ, Levine P, Leonard AC. Modifiedconstraint-induced therapy in acute stroke: a randomized controlled pilot study. NeurorehabilNeural Repair 2005;19:27–32.
83. Alberts JL, Butler AJ, Wolf SL. The effects ofconstraint-induced therapy on precision grip: a preliminary study. Neurorehabil Neural Repair2004;18:250–8.
84. Boake C, Noser EA, Ro T, Baraniuk S, Gaber M,Johnson R, et al. Constraint-induced movementtherapy during early stroke rehabilitation.Neurorehabil Neural Repair 2006;20:1–12.
85. Pohl M, Mehrholz J, Ritschel C, Ruckriem S.Speed-dependent treadmill training in ambulatoryhemiparetic stroke patients: a randomizedcontrolled trial. Stroke 2002;33:553–8.
86. da Cunha IT, Lim PA, Qureshy H, Henson H,Monga T, Protas EJ. Gait outcomes after acutestroke rehabilitation with supported treadmillambulation training: a randomized controlledpilot study. Arch Phys Med Rehabil 2002;83:1258–65.
87. Ada L, Dean CM, Hall JM, Bampton J,Crompton S. A treadmill and overground walkingprogram improves walking in persons residing inthe community after stroke: a placebo-controlled,randomized trial. Arch Phys Med Rehabil2003;84:1486–91.
88. Macko RF, Ivey FM, Forrester LW, Hanley D,Sorkin JD, Katzel LI, et al. Treadmill exerciserehabilitation improves ambulatory function andcardiovascular fitness in patients with chronicstroke: a randomized, controlled trial. Stroke2005;36:2206–11.
89. Eich HJ, Mach H, Werner C, Hesse S. Aerobictreadmill plus Bobath walking training improveswalking in subacute stroke: a randomizedcontrolled trial. Clin Rehabil 2004;18:640–51.
90. Allison R. Pilot randomised control trial to assessthe impact of additional supported standing
practice on functional ability post-stroke. NationalResearch Register N0620164288; 2005.
91. Askim T, Indredavik B. Does intensive task specifictraining improve balance after acute stroke?Clinical Trials.gov NCT00184431; 2005.
92. Harris N. Evaluation of a repetitive practicescheme to improve sit to stand performancefollowing stroke. National Research RegisterN0234135926; 2005.
93. English C, Warden-Flood A, Stiller K, Hillier S. Is task-related training an effective means ofproviding rehabilitation to acute stroke patients?In 1st APA Neurological Physiotherapy Conference,Sydney, Australia; 2005.
94. Sherrington C, Pamphlet P, Jacka J, Olivetti L,Nugent J, Hall J. A randomised controlled trial toevaluate task-related exercise classes for olderpeople with impaired mobility. e-Aust J Physiother2005;51:S431.
95. Miller K, Galae M, Kilbreath S, Phillips B. Earlyintensive task-specific sensory and motor trainingof the upper limb following acute stroke: a pilotstudy. In Proceedings of the 3rd World Congress ofPhysical Therapy, Venice, Italy; 2002.
96. Noser E. Constraint-induced movement therapyafter subacute stroke. Stroke Trials Register. URL: www.strokecenter.org; 2004.
97. Pomeroy V. Evaluation of whether functionalstrength training can enhance recovery of mobilityafter stroke. Clinical Trials.gov NCT00322192;2006.
98. Baer G. An investigation into the efficacy of ahome-based physiotherapy rehabilitationprogramme for late-stage stroke. A pilotrandomised controlled trial. National ResearchRegister N0417121685; 2002.
99. Bhakta B. Development of an intelligent roboticsystem to aid physical therapy in stroke. NHSTrusts Clinical Trials Register ISRCTNN23388474;2003.
100. Bratava DM, Richards L, Bever CT, Haselkorn J.Robotic assisted upper-limb neurorehabilitation instroke patients. Clinical Trials.gov NCT 00372411;2006.
101. Dewald J. Selective dynamic strength training toenhance upper limb coordination following stroke.National Rehabilitation Information CenterH133G030143; 2003.
102. DeLaurentis KJ. HARI: the hand/armrehabilitation interface for training the handfollowing stroke. National RehabilitationInformation Center H133S040140; 2004.
103. Hori M, Selbert K, Scremin AME, McCarty P,Moeder S, Van der Loos HFM. Assisted movementneuro-rehabilitation: VA multi-site clinical trial.Clinical Trials.gov NCT00223808; 2005.
References
66

104. Koeneman J. Air muscle device for ankle strokerehabilitation. CRISP 5R43HD047067-02; 2004.
105. Krebs HI. The effect of proximal and distaltraining on stroke recovery. CRISP5R01HD045343-02; 2004.
106. Otfinowski J, Jassiak-Tyrkalska B, Starowicz A,Regula K. Computer-based rehabilitation ofcognitive impairments and motor arm function ofpatients with hemiparesis after stroke [Polish].Neurologia i Neurochirurgia Polska 2006;40:112–18.
107. Tang PF. Balance recovery and training on fallprevention in stroke. Clinical Trials.govNCT00166907; 2005.
108. Edinger K, Herbold J, Mohr D, Vaidya S. Value ofa fitness programme after completion ofrehabilitation therapy poststroke. Arch Phys MedRehabil 2003;84:A10.
109. McClain J. An investigation into the effect of includinga goal orientated, independently practised, exerciseprogramme in early stroke rehabilitation. MSc thesis,Southampton University; 2003.
110. Muller K, Butefisch CM, Kleiser B, Korber B,Stephan J, Netz V. Recovery of hand function afterstroke by executed and mental repetitive training.Cerebrovasc Dis 2004;15(Suppl 5):115.
111. Manova N, Venova L. Rivermead (RMA) – test andtool for motor recovery after stroke. In Proceedingsof the 14th International Congress of the WorldConfederation for Physical Therapy, Barcelona; 2003.
112. Wang RY, Chen HI, Chen CY, Yang YR. Efficacy ofBobath versus orthopaedic approach onimpairment and function at different motorrecovery stages after stroke: a randomisedcontrolled study. Clin Rehabil 2005;19:155–64.
113. Yang YR, Wang RY, Lin KH, Chu MY, Chan RC.Task-oriented progressive resistance strengthtraining improves muscle strength and functionalperformance in individuals with stroke. ClinRehabil 2006;20:860–70.
114. Dromerick AW. Very early constraint-inducedmovement therapy: stroke. CRISP5R01NS041261-03; 2004.
115. Light KE. Examining parameters of constraint-induced therapy. CRISP 5R01HD045751-02;2005.
116. Huang YY, Wu CY, Aou SH, Lin KC, Chen CL.The modified constraint-induced movementtherapy improved reach-to-grasp movement inpatients with hemiparesis after stroke. Stroke2004;35:e313.
117. Bain BJ, McKenzie K, Brownlee MG, Brodie EE,Granat M, Parker D, et al. Constraint of thehemiparetic upper limb in stroke survivorsfollowing discharge from rehabilitation. ClinRehabil 2004;18:929–32.
118. Ada L. The efficacy of treadmill training inestablishing walking after stroke. ClinicalTrials.gov NCT00167531; 2002.
119. Brown DA. Strength Training Effectiveness Post-Stroke (STEPS). Clinical Trials.gov NCT00389012;2004.
120. Duncan PW. Locomotor experience applied poststroke (LEAPS) Trial. Clinical Trials.govNCT00108030; 2006.
121. Kilbreath SL. PBWST (partial body-weightsupported treadmill training) and muscle powertraining after sub-acute stroke. Clinical Trials.govNCT00108030; 2004.
122. Hidler JM. Walking therapy in hemiparetic strokepatients using robotic-assisted treadmill training.Clinical Trials.gov NCT00075283; 2002.
123. Sivenius J. Gait trainer versus traditionalphysiotherapy in acute stroke. Clinical Trials.govNCT00307762; 2003.
124. Zielke D. The effect of partial body weightsupported treadmill training on gait rehabilitationin early acute stroke patients: preliminary data.JNPT 2003;27:177.
125. Du J-B, Song W-Q, Wang M-B. The application ofpartial body weight support treadmill training inhemiplegia rehabilitation after stroke. [Chinese].Chin J Cerebrovasc Dis 2006;3:361–4.
126. Weng C-S, Bi S, Tian Z, Yu Z-Z, Xu J, Bi S-Q, et al.Application of structured speed-dependenttreadmill training in hemiplegic patients afterstroke [Chinese]. Chin J Clin Rehabil 2004;8:7617–19.
127. Zhu H-X, Dou Z-L, Li K, Lan Y, Hu X-Q. A preliminary investigation on the correlation ofpartial body weight support training withhemiplegic gait and ambulation function afterbrain injury [Chinese]. Chin J Clin Rehabil2004;8:5205–7.
128. Wolff D. Stroke rehabilitation outcomes withsupported treadmill ambulation training. ClinicalTrials.gov NCT00037895; 2001.
129. Kim BO, Lee JJ, Cho KH, Kim SH. Gait trainingrobot (gait trainer) in rehabilitation. In Proceedingsof the 1st International Congress of International Societyof Physical and Rehabilitation Medicine (ISPRM),7–13 July. Amsterdam: ISPRM; 2001.
130. Lennihan L, Wootten ME, Wainwright M,Tenteromano L, McMahon D, Cotier J. Treadmillwith partial body-weight support versusconventional gait training after stroke. Arch PhysMed Rehabil 2003;84:E5.
131. Stephenson J, Maitland M, Beckstead J. Bodyweight support treadmill training compared withPNF training in persons with chronic stroke. JNPT2004;28:186.
Health Technology Assessment 2008; Vol. 12: No. 30
67
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

132. Van Vliet PM, Lincoln NB, Robinson E.Comparison of the content of two physiotherapyapproaches for stroke. Clin Rehabil 2001;15:398–414.
133. Salbach NM, Mayo NE, Robichaud-Ekstrand S,Hanley JA, Richards CL, Wood-Dauphinee S. Theeffect of a task-oriented walking intervention onimproving balance self-efficacy poststroke: arandomized, controlled trial. J Am Geriatr Soc2005;53:576–82.
134. Watkins CL, Leathley MJ, Jack CIA, Sharma AK.Stroke Interface Audit. Pre/post discharge audit of strokeservices and care in Liverpool and Sefton: deliverytimeliness and targeting – 36 month report. Preston:University of Central Lancashire; 2002.
135. Wade DT, Collin C. The Barthel ADL index: a standard measure of physical disability? Int Disabil Stud 1988;10:64–7.
136. Van Exel NJA, Scholte op Reimer WJM,Koopmanschap MA. Assessment of post-strokequality of life in cost-effectiveness studies: the usefulness of the Barthel Index and theEuroQol-5D. Qual Life Res 2004;13:427–33.
137. Curtis L, Netten A. Unit costs of health and socialcare. Canterbury: Personal Social Services ResearchUnit, University of Kent; 2006.
138. National Institute for Clinical Excellence. Guide tothe methods of technology appraisal. London: NICE;2004.
139. Page SJ, Gater DR, Bach YR. Reconsidering themotor recovery plateau in stroke rehabilitation.Arch Phys Med Rehabil 2004;85:1377–81.
140. Sunderland A, Tuke A. Neuroplasticity, learningand recovery after stroke: a critical evaluation ofconstraint-induced therapy. Neuropsychol Rehabil2005;15:81–96.
141. Ferrucci L, Bandinelli S, Guralnik JM, Lamponi RPT, Bertini C, Falchini M, et al.Recovery of functional status after stroke. A postrehabilitation follow-up study. Stroke1993;24:200–5.
142. Paolucci S, Antonucci G, Pratesi L, Traballesi M,Lubich S, Grasso MG. Functional outcome instroke inpatient rehabilitation: predicting no, lowand high response patients. Cerebrovasc Dis1998;8:228–34.
143. Langhammer B, Stanghelle JK. Bobath or MotorRelearning Programme? A follow-up one and fouryears post stroke. Clin Rehabil 2003;17:731–4.
144. Bobath B. Adult hemiplegia: evaluation and treatment.London: William Heinemann Medical Books;1990.
145. Bagley P, Hudson M, Forster A, Smith J, Young J.A randomized trial evaluation of the OswestryStanding Frame for patients after stroke. ClinRehabil 2005;4:354–64.
146. Brown DA, Burgar CG. Graded weight-bearingexercise for improved ambulation after stroke.URL: http://guide.stanford.edu/projects/2kprojects/stroke06.html; 2002.
147. Carey JR, Kimberley TJ, Lewis SM, Auerbach EJ,Dorsey L, Rundquist P. Analysis of fMRI andfinger tracking training in subjects with chronicstroke. Brain 2002;125:773–88.
148. Chan DYL, Chan CCH, Au DKS. Motor relearningprogramme for stroke patients: a randomizedcontrolled trial. Clin Rehabil 2006;20:191–200.
149. Chang JL, Sun B. Effect of motor relearningtraining on upper extremity function inhemiplegia patients. Modern Rehabilitation 2000;4:684–5.
150. Cirstea MC, Ptito A, Levin MF. Arm reachingimprovements with short-term practice depend onthe severity of the motor deficit in stroke. ExpBrain Res 2003;152:47–88.
151. Desrosiers J, Bourbonnais D, Corriveau H,Gosselin S, Bravo G. Effectiveness of unilateraland symmetrical bilateral task training for armduring the subacute phase after stroke: a randomized controlled trial. Clin Rehabil 2005;19:581–93.
152. Duncan P, Studenski S, Richards L, Gollub S,Lai SM, Reker D. Randomized clinical trial oftherapeutic exercise in subacute stroke. Stroke2003;34:2173–80.
153. Eng JJ, Chu KS, Kim CM, Dawson AS, Carswell A,Hepburn KE. A community-based group exerciseprogram for persons with chronic stroke. Med SciSports Exerc 2003;35:1271–8.
154. Feys HM, De Weerdt WJ, Selz BE, Cox Steck GA,Spichiger R, Vereeck LE, et al. Effect of atherapeutic intervention for the hemiplegic upperlimb in the acute phase after stroke. Stroke1998;29:785–92.
155. Gelber DA, Josefczyk PB, Herman D, Good DC,Verhulst SJ. Comparison of two therapyapproaches in the rehabilitation of the pure motorhemiparetic stroke patient. J Neurol Rehabil1995;9:191–6.
156. Hanlon RE. Motor learning following unilateralstroke. Arch Phys Med Rehabil 1996; 77:811–15.
157. Husemann B, Muller F, Krewer C, Lab A, Gille C,Heller S. Effects of locomotion training withassistance of a driven gait orthosis in hemipareticpatients after stroke [abstract]. Neurologie undRehabilitation 2004;10:187–217.
158. Inaba M, Edberg E, Montgomery J, Gillis MK.Effectiveness of functional training, active exercise,and resistive exercise for patients with hemiplegia.Phys Ther 1973;53:28–35.
159. Katz-Leurer M, Sender I, Keren O, Dvir Z. Theinfluence of early cycling training on balance in
References
68
stroke patients at the subacute stage: results of apreliminary trial. Clin Rehabil 2006;20:398–405.
160. Kayhan O, Guven Z, Erdilli S, Ozaras N,Renklitepe N. The effect of motor rehabilitation ofthe hand in stroke patients. Eur J Neurol 1996;3(Suppl 2):10.
161. Khanna PB. A randomised control study of theimmediate and long term benefits of conventionalstroke rehabilitation with task related grouptherapy in chronic stroke patients. URL:http://www.controlled-trials.com/2003; 2003.
162. Kilbreath SL, Heard R. Upper and lower limbfunction in stroke patients following task-specifictraining. In Proceedings of the Australasian Faculty ofRehabilitation Medicine 5th Annual ScientificConference, Melbourne, 1997.
163. Krutulyte G, Kimtys A, Krisciunas A. Theeffectiveness of physical therapy methods (Bobathand motor relearning program) in rehabilitationof stoke patients [Lithuanian]. Medicina (Kaunas)2003;39:889–95.
164. Li HF, Wang JH, Feng JC, Gao F. Application ofmotor relearning therapy in the earlyrehabilitation of stroke: a randomised controlledcomparison [Chinese]. Chin J Clin Rehabil2005;9(29):1–3.
165. Liao L, Luo W, Chen S. The effect of trunk controltraining on balance and lower limb function inpatients with hemiplegia [Chinese]. Chin J RehabilMed 2006;21:608–9.
166. Mudie MH, Winzeler-Mercay U, Radwan S, Lee L.Training symmetry of weight distribution afterstroke: a randomized controlled pilot studycomparing task-related reaching, Bobath andfeedback training approaches. Clin Rehabil2002;16:582–92.
167. Nelles G, Jentzen W, Jueptner M, Müller S, Diener HC. Arm training induced brain plasticityin stroke studied with serial positron emissiontomography. NeuroImage 2001;13:1146–54.
168. Pang MY, Harris JE, Eng JJ. A community-basedupper-extremity group exercise program improvesmotor function and performance of functionalactivities in chronic stroke: a randomizedcontrolled trial. Arch Phys Med Rehabil 2006;87:1–9.
169. Platz T, Winter T, Müller N, Pinkowski C,Eickhof C, Mauritz K. Arm ability training forstroke and traumatic brain injury patients withmild arm paresis: a single-blind, randomized,controlled trial. Arch Phys Med Rehabil 2001;82:961–8.
170. Pollock AS, Durard BR, Rowe PJ, Paul JP. The effect of independent practice of motor tasksby stroke patients: a pilot randomized controlledtrial. Clin Rehabil 2002;16:473–80.
171. Sunderland A, Tinson DJ, Bradley EL, Fletcher D,Langton HR, Wade DT. Enhanced physical
therapy improves recovery of arm function afterstroke. J Neurol Neurosurg Psychiatry 1992;55:530–5.
172. Theilman GT, Dean CM, Gentile AM.Rehabilitation of reaching after stroke: task-relatedtraining versus progressive resistive exercise. ArchPhys Med Rehabil 2004;85:1613–18.
173. Wellmon R, Newton RA. An examination ofchanges in gait and standing symmetry associatedwith the practice of a weight shifting task.Neurology Report 1997;21:52–3.
174. Xiao Z, Zhang L, Pang H. Application of motorrelearning programme for the recovery of upperlimb function in hemiplegic patients [Chinese].Chin J Phys Med Rehabil 2002;24:590–61.
175. Yang YR, Yen, JG, Wang RY, Yen LL, Lieu FK. Gait outcomes after additional backward walkingtraining in patients with stroke: a randomizedcontrolled trial. Clin Rehabil 2005;19:264–73.
176. Ploughman M, Corbett D. Can forced-use therapybe clinically applied after stroke? An exploratoryrandomized controlled trial. Arch Phys Med Rehabil2004;85:1417–23.
177. Ro T, Noser E, Boake C, Johnson R, Gaber M,Speroni A, et al. Functional reorganization andrecovery after constraint-induced movementtherapy in subacute stroke: case reports. Neurocase2006;12:50–60.
178. Sterr A, Elbert T, Berthold I, Kolbel S, Rockstroh B, Taub E. Longer versus shorter dailyconstraint-induced movement therapy of chronichemiparesis: an exploratory study. Arch Phys MedRehabil 2002;83:1374–7.
179. Van der Lee JH, Wagenaar RC, Lankhorst GJ,Vogelaar TW, Deville WL, Bouter LM. Forced useof the upper extremity in chronic stroke patients:results from a single-blind randomized clinicaltrial. Stroke 1999;30:2369–75.
180. Jaffe DL, Brown DA, Pierson-Carey CD,Buckley EL, Lew HL. Stepping over obstacles toimprove walking in individuals with poststrokehemiplegia. J Rehabil Res Dev 2004;41(3A):283–92.
181. Kosak MC, Reding MJ. Comparison of partialbody weight-supported treadmill gait trainingversus aggressive bracing assisted walking poststroke. Neurorehabil Neural Repair 2000;14:13–19.
182. Nilsson L, Carlsson J, Danielsson A, Fugl-Meyer A,Hellstrom K, Kristensen L, et al. Walking trainingof patients with hemiparesis at an early stage afterstroke: a comparison of walking training on atreadmill with body weight support and walkingtraining on the ground. Clin Rehabil 2001;15:515–27.
183. Laufer Y, Dickstein R, Chefez Y, Marcovitz E. The effect of treadmill training on the ambulationof stroke survivors in the early stages ofrehabilitation: a randomized study. J Rehabil ResDev 2001;38:69–78.
Health Technology Assessment 2008; Vol. 12: No. 30
69
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

184. Liston R, Mickelborough J, Harris B, Hann AW,Tallis RC. Conventional physiotherapy andtreadmill re-training for higher-level gait disordersin cerebrovascular disease. Age Ageing2000;29:311–18.
185. Richards CL, Malouin F, Wood-Dauphinee S,Williams JI, Bourchard JP, Brunet D. Task-specificphysical therapy for optimisation of gait recoveryin acute stroke patients. Arch Phys Med Rehabil1993;74:612–20.
186. Richards CL, Malouin F, Bravo G, Dumas F, Wood-Dauphinee S. The role of technology intask-oriented training in persons with subacute
stroke: a randomised controlled trial. NeurorehabilNeural Repair 2004;18:199–211.
187. Visintin M, Barbeau H, Korner-Bitensky N, Mayo NE. A new approach to retrain gait in strokepatients through body weight support andtreadmill stimulation. Stroke 1998;29:1122–8.
188. Werner C, von FS, Treig T, Konrad M, Hesse S.Treadmill training with partial body weightsupport and an electromechanical gait trainer forrestoration of gait in subacute stroke patients: a randomized crossover study. Stroke 2002;33:2895–901.
References
70
Health Technology Assessment 2008; Vol. 12: No. 30
71
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Appendix 1
Included studies: repetitive task training
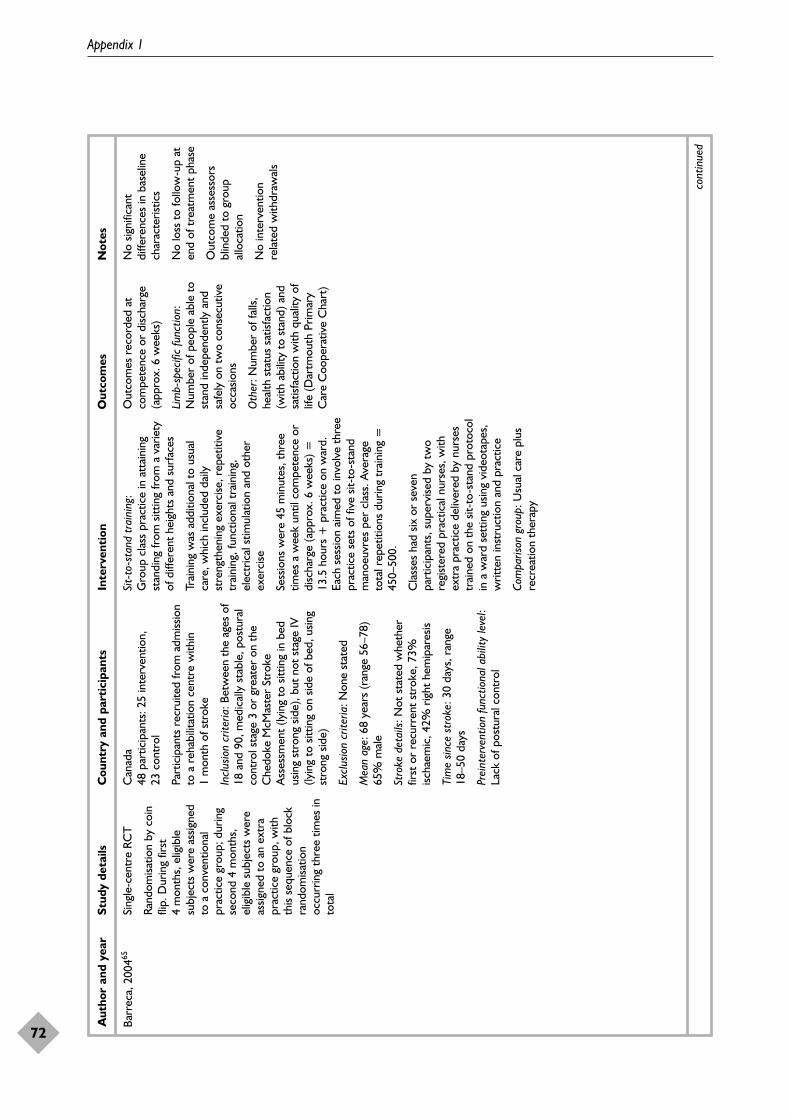
Appendix 1
72
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Barr
eca,
200
465Si
ngle
-cen
tre
RCT
Rand
omisa
tion
by c
oin
flip.
Dur
ing
first
4m
onth
s, e
ligib
lesu
bjec
ts w
ere
assig
ned
to a
con
vent
iona
lpr
actic
e gr
oup;
dur
ing
seco
nd 4
mon
ths,
elig
ible
sub
ject
s w
ere
assig
ned
to a
n ex
tra
prac
tice
grou
p, w
ithth
is se
quen
ce o
f blo
ckra
ndom
isatio
noc
curr
ing
thre
e tim
es in
tota
l
Can
ada
48 p
artic
ipan
ts: 2
5 in
terv
entio
n,
23 c
ontr
ol
Part
icip
ants
rec
ruite
d fr
om a
dmiss
ion
to a
reh
abili
tatio
n ce
ntre
with
in1
mon
th o
f str
oke
Incl
usio
n cr
iteria
: Bet
wee
n th
e ag
es o
f18
and
90,
med
ical
ly s
tabl
e, p
ostu
ral
cont
rol s
tage
3 o
r gr
eate
r on
the
Che
doke
McM
aste
r St
roke
Ass
essm
ent
(lyin
g to
sitt
ing
in b
edus
ing
stro
ng s
ide)
, but
not
sta
ge IV
(lyin
g to
sitt
ing
on s
ide
of b
ed, u
sing
stro
ng s
ide)
Excl
usio
n cr
iteria
: Non
e st
ated
Mea
n ag
e: 6
8 ye
ars
(ran
ge 5
6–78
)65
% m
ale
Stro
ke d
etai
ls: N
ot s
tate
d w
heth
erfir
st o
r re
curr
ent
stro
ke, 7
3%isc
haem
ic, 4
2% r
ight
hem
ipar
esis
Tim
e sin
ce s
trok
e: 3
0 da
ys, r
ange
18–5
0 da
ys
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l: La
ck o
f pos
tura
l con
trol
Sit-
to-s
tand
tra
inin
g:G
roup
cla
ss p
ract
ice
in a
ttai
ning
stan
ding
from
sitt
ing
from
a v
arie
tyof
diff
eren
t he
ight
s an
d su
rfac
es
Trai
ning
was
add
ition
al t
o us
ual
care
, whi
ch in
clud
ed d
aily
stre
ngth
enin
g ex
erci
se, r
epet
itive
trai
ning
, fun
ctio
nal t
rain
ing,
elec
tric
al s
timul
atio
n an
d ot
her
exer
cise
Sess
ions
wer
e 45
min
utes
, thr
eetim
es a
wee
k un
til c
ompe
tenc
e or
disc
harg
e (a
ppro
x. 6
wee
ks) =
13.5
hou
rs +
pra
ctic
e on
war
d.Ea
ch s
essio
n ai
med
to
invo
lve
thre
epr
actic
e se
ts o
f fiv
e sit
-to-
stan
dm
anoe
uvre
s pe
r cl
ass.
Ave
rage
tota
l rep
etiti
ons
durin
g tr
aini
ng =
450–
500.
Cla
sses
had
six
or
seve
npa
rtic
ipan
ts, s
uper
vise
d by
tw
ore
gist
ered
pra
ctic
al n
urse
s, w
ithex
tra
prac
tice
deliv
ered
by
nurs
estr
aine
d on
the
sit-
to-s
tand
pro
toco
lin
a w
ard
sett
ing
usin
g vi
deot
apes
,w
ritte
n in
stru
ctio
n an
d pr
actic
e
Com
paris
on g
roup
: Usu
al c
are
plus
recr
eatio
n th
erap
y
Out
com
es r
ecor
ded
atco
mpe
tenc
e or
disc
harg
e(a
ppro
x. 6
wee
ks)
Lim
b-sp
ecifi
c fu
nctio
n:N
umbe
r of
peo
ple
able
to
stan
d in
depe
nden
tly a
ndsa
fely
on
two
cons
ecut
ive
occa
sions
Oth
er: N
umbe
r of
falls
,he
alth
sta
tus
satis
fact
ion
(with
abi
lity
to s
tand
) and
satis
fact
ion
with
qua
lity
oflif
e (D
artm
outh
Prim
ary
Car
e C
oope
rativ
e C
hart
)
No
signi
fican
tdi
ffere
nces
in b
asel
ine
char
acte
ristic
s
No
loss
to
follo
w-u
p at
end
of t
reat
men
t ph
ase
Out
com
e as
sess
ors
blin
ded
to g
roup
allo
catio
n
No
inte
rven
tion
rela
ted
with
draw
als
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
73
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Blen
nerh
asse
tt,
2004
50Si
ngle
-cen
tre
RCT
Rand
omisa
tion
proc
edur
e no
tde
scrib
ed. C
once
aled
allo
catio
n to
gro
ups
usin
g in
depe
nden
tal
loca
tor
and
seal
edop
aque
env
elop
es
Aus
tral
ia30
par
ticip
ants
: 15
inte
rven
tion,
15
con
trol
Part
icip
ants
rec
ruite
d fr
om in
patie
ntad
miss
ions
to
a re
habi
litat
ion
cent
re,
2001
–200
3, w
ith a
prim
ary
diag
nosis
of s
trok
e, w
ithin
3 m
onth
s of
str
oke
Incl
usio
n cr
iteria
: Abl
e to
wal
k 10
m,
able
to
prov
ide
info
rmed
con
sent
Excl
usio
n cr
iteria
: Det
erio
ratin
gm
edic
al c
ondi
tion,
inde
pend
ent
com
mun
ity a
mbu
latio
n
Mea
n ag
e: M
obili
ty g
roup
53.
9 ye
ars
(SD
19.
8), u
pper
lim
b gr
oup
56.3
year
s (S
D10
.5)
56.6
% m
ale
Stro
ke d
etai
ls: F
irst
or r
ecur
rent
stro
ke: 7
3% is
chae
mic
, 47%
rig
hthe
mip
ares
is
Tim
e sin
ce s
trok
e: M
obili
ty g
roup
36da
ys (S
D 2
5.1)
, upp
er li
mb
grou
p50
day
s (S
D 4
9.2)
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l: A
ble
to w
alk
10 m
, 6M
WT
182
m
(SD
85)
Mob
ility
inte
rven
tion:
Low
er li
mb
circ
uit
trai
ning
: fun
ctio
nal t
asks
suc
has
sit-
to-s
tand
, ste
p-up
s, o
bsta
cle
cour
se w
alki
ng, p
lus
stre
tchi
ng a
ndst
reng
then
ing
exer
cise
, and
som
een
dura
nce
trai
ning
on
stat
iona
rybi
kes/
trea
dmill
s
Upp
er e
xtre
mity
inte
rven
tion:
Func
tiona
l tas
ks t
o im
prov
e re
ach
and
gras
p, h
and–
eye
coor
dina
tion
activ
ities
, and
str
etch
ing
and
stre
ngth
enin
g ex
erci
ses
Both
gro
ups
wer
e du
ring
inpa
tient
reha
bilit
atio
n an
d ad
ditio
nal t
o us
ual
care
of 1
hou
r of
phy
sioth
erap
y,5
days
a w
eek,
bas
ed o
n M
ovem
ent
Scie
nce
App
roac
h
Sess
ions
wer
e 60
min
utes
, fiv
etim
es a
wee
k fo
r 4
wee
ks(2
0ho
urs
tota
l tra
inin
g tim
e). E
ach
circ
uit
incl
uded
ten
5-m
inut
ew
orks
tatio
ns
Sess
ions
wer
e de
liver
ed b
y a
phys
ical
the
rapi
st in
gro
ups
of u
p to
four
sub
ject
s
Com
paris
on g
roup
: Ble
nner
hass
ett,
2004
a: lo
wer
lim
b at
tent
ion
cont
rol,
Blen
nerh
asse
tt 2
004b
:up
per
limb
atte
ntio
n co
ntro
l
Out
com
es r
ecor
ded
atba
selin
e, w
hich
was
app
rox.
6 w
eeks
pos
t-st
roke
(ran
ge54
–74
days
), an
d at
4 w
eeks
and
6 m
onth
s af
ter
trai
ning
Upp
er li
mb
func
tion:
M
AS
uppe
r ar
m, M
AS
hand
,Je
bsen
Tay
lor
Test
of H
and
Func
tion
Low
er li
mb
func
tion:
6M
WT,
TU
G, S
tep
Test
No
signi
fican
tdi
ffere
nces
rep
orte
d at
base
line
3% lo
st t
o fo
llow
-up
aten
d of
tre
atm
ent
phas
e
Out
com
e as
sess
ors
blin
ded
to g
roup
allo
catio
n
No
likel
y in
terv
entio
n-re
late
d w
ithdr
awal
s
Ave
rage
att
enda
nce
was
app
rox.
80%
, with
no s
igni
fican
t di
ffere
nce
betw
een
the
grou
ps
cont
inue
d

Appendix 1
74
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
de S
èze,
200
176Si
ngle
-cen
tre,
pilo
t RC
T
Rand
omisa
tion
tabl
eus
ed. N
o de
tails
of
allo
catio
n co
ncea
lmen
tpr
oces
s
Fran
ce20
par
ticip
ants
: ten
exp
erim
enta
l, te
n co
ntro
l
Subj
ects
rec
ruite
d fr
om a
dmiss
ions
to
a n
euro
reha
bilit
atio
n un
it in
199
8
Incl
usio
n cr
iteria
: Hem
iple
gia
caus
edby
a s
ingl
e st
roke
occ
urrin
g at
leas
t1
mon
th p
revi
ously
. Sta
tic im
bala
nce
of t
he t
runk
res
ultin
g fr
om t
he s
trok
e
Excl
usio
n cr
iteria
: Mul
tiple
cer
ebra
lle
sions
, diso
rder
s of
the
loco
mot
orsy
stem
, a s
ever
e vi
sual
or
audi
tory
defic
it, a
sev
ere
defic
it of
exe
cutiv
efu
nctio
ns, o
r de
terio
ratio
n in
gen
eral
heal
th
Mea
n ag
e: E
xper
imen
tal g
roup
63.5
year
s (S
D 1
7), c
ontr
ol g
roup
67.7
year
s (S
D 1
5)55
% m
ale
Stro
ke d
etai
ls: F
irst
stro
ke: 3
5%isc
haem
ic, 2
5% r
ight
hem
ipar
esis
Tim
e sin
ce s
trok
e: E
xper
imen
tal g
roup
36.8
days
(SD
25)
, con
trol
gro
up27
.7da
ys (S
D 1
5)
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l: La
ck o
f pos
tura
l bal
ance
Expe
rimen
tal i
nter
vent
ion:
Pos
tura
ltr
aini
ng u
sing
the
Bon
Sain
t C
ôme
devi
ce, a
cus
tom
-mou
lded
ort
hosis
that
hol
ds a
poi
ntin
g de
vice
, use
dby
the
sub
ject
to
poin
t to
tar
gets
on a
ver
tical
pan
el, w
hich
em
it lig
htan
d so
und
whe
n ac
tivat
ed. T
hesu
bjec
t pe
rfor
ms
exer
cise
s of
loca
ting
and
poin
ting
by c
ontr
ollin
gtr
unk
mov
emen
t
Inte
rven
tion
was
dur
ing
reha
bilit
atio
n an
d ad
ditio
nal t
o us
ual
care
Usu
al c
are
cons
isted
of a
Bob
ath-
insp
ired
appr
oach
and
func
tiona
lth
erap
y fo
r 1
hour
per
day
, plu
s a
sess
ion
of o
ccup
atio
nal t
hera
py5
days
a w
eek
Sess
ions
wer
e 60
min
utes
(unc
lear
whe
ther
5 o
r 7
days
per
wee
k), f
or4
wee
ks =
20–
28 h
ours
Sess
ions
wer
e de
liver
ed in
divi
dual
ly,by
a p
hysic
al t
hera
pist
Com
paris
on g
roup
: Con
vent
iona
lre
habi
litat
ion
for
2 ho
urs
per
day
Out
com
es r
ecor
ded
atba
selin
e, p
ost-
inte
rven
tion
(4 w
eeks
) and
at
2 m
onth
s
Lim
b-sp
ecifi
c fu
nctio
n: S
ittin
gEq
uilib
rium
Inde
x, U
prig
htEq
uilib
rium
Inde
x, F
AC
Mot
or p
erfo
rman
ce: T
runk
Con
trol
Tes
t, M
otric
ityIn
dex,
Ash
wor
th S
cale
ADL:
FIM
At
base
line,
pos
tura
lde
ficit
and
unila
tera
lne
glec
t te
nded
to
bem
ore
seve
re in
the
devi
ce g
roup
, alth
ough
not
signi
fican
t. Tr
unk
Con
trol
Tes
t: de
vice
grou
p 36
.6 (S
D 3
2.3)
,co
ntro
l gro
up 5
0.4
(SD
31.9
), U
prig
htEq
uilib
rium
Inde
xD
evic
e gr
oup
0.8
(SD
0.9)
, con
trol
gro
up1.
2 (S
D 1
.0).
0% lo
st t
o fo
llow
-up
aten
d of
tre
atm
ent
phas
e
Out
com
e as
sess
ors
blin
d to
tre
atm
ent
grou
p
No
inte
rven
tion
rela
ted
reas
ons
for
with
draw
al
All
subj
ects
com
plet
edtr
aini
ng
cont
inue
d
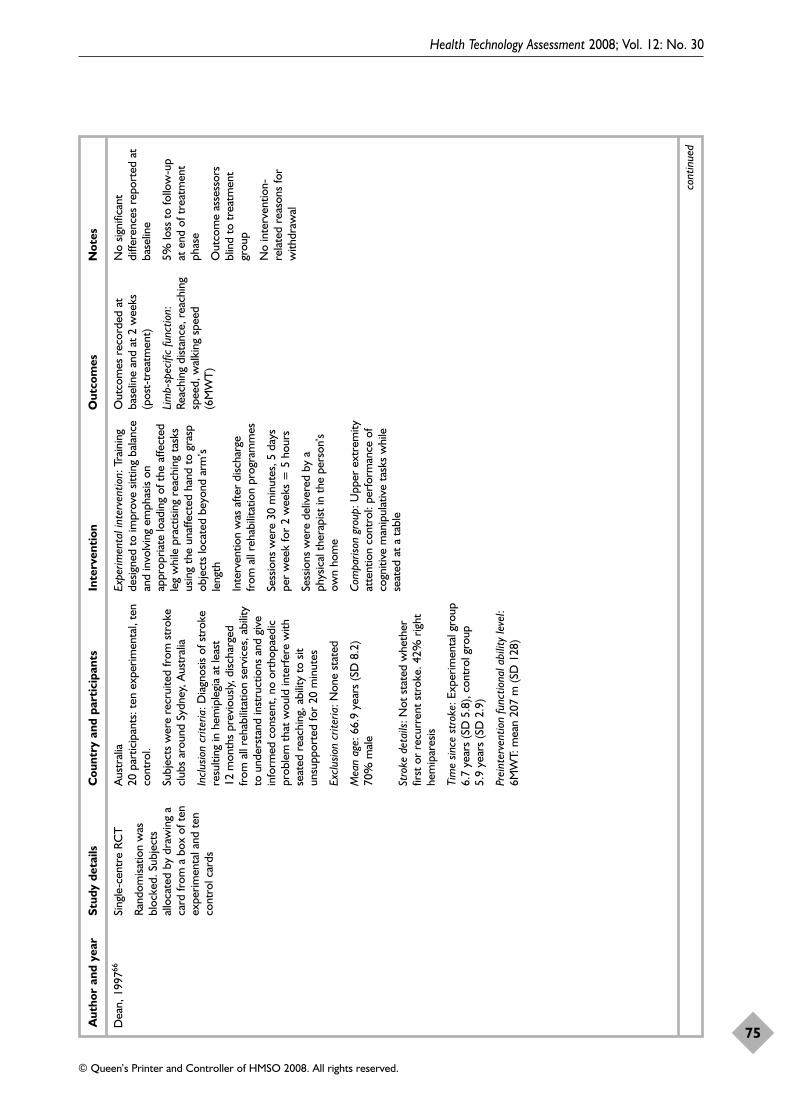
Health Technology Assessment 2008; Vol. 12: No. 30
75
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Dea
n, 1
99766
Sing
le-c
entr
e RC
T
Rand
omisa
tion
was
bloc
ked.
Sub
ject
sal
loca
ted
by d
raw
ing
aca
rd fr
om a
box
of t
enex
perim
enta
l and
ten
cont
rol c
ards
Aus
tral
ia20
par
ticip
ants
: ten
exp
erim
enta
l, te
nco
ntro
l.
Subj
ects
wer
e re
crui
ted
from
str
oke
club
s ar
ound
Syd
ney,
Aus
tral
ia
Incl
usio
n cr
iteria
: Dia
gnos
is of
str
oke
resu
lting
in h
emip
legi
a at
leas
t12
mon
ths
prev
ious
ly, d
ischa
rged
from
all
reha
bilit
atio
n se
rvic
es, a
bilit
yto
und
erst
and
inst
ruct
ions
and
giv
ein
form
ed c
onse
nt, n
o or
thop
aedi
cpr
oble
m t
hat
wou
ld in
terf
ere
with
seat
ed r
each
ing,
abi
lity
to s
itun
supp
orte
d fo
r 20
min
utes
Excl
usio
n cr
iteria
: Non
e st
ated
Mea
n ag
e: 6
6.9
year
s (S
D 8
.2)
70%
mal
e
Stro
ke d
etai
ls: N
ot s
tate
d w
heth
erfir
st o
r re
curr
ent
stro
ke. 4
2% r
ight
hem
ipar
esis
Tim
e sin
ce s
trok
e: E
xper
imen
tal g
roup
6.7
year
s (S
D5.
8), c
ontr
ol g
roup
5.
9 ye
ars
(SD
2.9)
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l:6M
WT:
mea
n 20
7 m
(SD
128
)
Expe
rimen
tal i
nter
vent
ion:
Tra
inin
gde
signe
d to
impr
ove
sittin
g ba
lanc
ean
d in
volv
ing
emph
asis
onap
prop
riate
load
ing
of t
he a
ffect
edle
g w
hile
pra
ctisi
ng r
each
ing
task
sus
ing
the
unaf
fect
ed h
and
to g
rasp
obje
cts
loca
ted
beyo
nd a
rm’s
leng
th
Inte
rven
tion
was
afte
r di
scha
rge
from
all
reha
bilit
atio
n pr
ogra
mm
es
Sess
ions
wer
e 30
min
utes
, 5 d
ays
per
wee
k fo
r 2
wee
ks =
5 h
ours
Sess
ions
wer
e de
liver
ed b
y a
phys
ical
the
rapi
st in
the
per
son’
sow
n ho
me
Com
paris
on g
roup
: Upp
er e
xtre
mity
atte
ntio
n co
ntro
l: pe
rfor
man
ce o
fco
gniti
ve m
anip
ulat
ive
task
s w
hile
seat
ed a
t a
tabl
e
Out
com
es r
ecor
ded
atba
selin
e an
d at
2 w
eeks
(pos
t-tr
eatm
ent)
Lim
b-sp
ecifi
c fu
nctio
n:
Reac
hing
dist
ance
, rea
chin
gsp
eed,
wal
king
spe
ed(6
MW
T)
No
signi
fican
tdi
ffere
nces
rep
orte
d at
base
line
5% lo
ss t
o fo
llow
-up
at e
nd o
f tre
atm
ent
phas
e
Out
com
e as
sess
ors
blin
d to
tre
atm
ent
grou
p
No
inte
rven
tion-
rela
ted
reas
ons
for
with
draw
al
cont
inue
d

Appendix 1
76
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Dea
n, 2
00067
Pilo
t RC
T
Subj
ects
gro
uped
into
mat
ched
pai
rs b
ased
on
wal
king
spe
ed, t
hen
rand
omise
d by
dra
win
gca
rds
from
a b
ox.
Car
ds d
raw
n by
ape
rson
inde
pend
ent
from
the
stu
dy
Can
ada
12 p
artic
ipan
ts: s
ix m
obili
tyin
terv
entio
n, s
ix u
pper
lim
b at
tent
ion
cont
rol g
roup
Subj
ects
rec
ruite
d fr
om a
reha
bilit
atio
n re
sear
ch g
roup
data
base
Incl
usio
n cr
iteria
: Firs
t st
roke
, at
leas
t3
mon
ths
post
-str
oke,
disc
harg
edfr
om a
ll re
habi
litat
ion
serv
ices
, abl
eto
att
end
a re
habi
litat
ion
cent
re t
hree
times
a w
eek
for
4 w
eeks
, abl
e to
wal
k 10
m
Excl
usio
n cr
iteria
: Any
med
ical
cond
ition
tha
t w
ould
pre
vent
part
icip
atio
n
Mea
n ag
e: E
xper
imen
tal g
roup
66.2
year
s (7
.7),
cont
rol g
roup
62.3
year
s (6
.6)
58%
mal
e
Stro
ke d
etai
ls: N
ot s
tate
d w
heth
erfir
st o
r re
curr
ent
stro
ke. 5
8% r
ight
hem
ipar
esis
Tim
e sin
ce s
trok
e: M
obili
ty g
roup
2.3
year
s (S
D 0
.7),
uppe
r lim
bat
tent
ion-
cont
rol g
roup
1.3
yea
rs(S
D0.
9)
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l:6M
WT
mea
n 23
5 m
(SD
139
)
Mob
ility
inte
rven
tion:
Low
er li
mb
circ
uit
trai
ning
of t
en w
orks
tatio
nsin
clud
ing
sittin
g re
ach,
sit-
to-s
tand
,st
eppi
ng, h
eel l
ifts,
sta
ndin
gba
lanc
e, le
g st
reng
then
ing,
tre
adm
illw
alki
ng, o
bsta
cle
wal
king
, slo
pe a
ndst
air
wal
king
, plu
s pa
rtic
ipat
ion
inw
alki
ng r
aces
and
rel
ays
Inte
rven
tion
was
afte
r di
scha
rge
from
all
reha
bilit
atio
n pr
ogra
mm
es
Sess
ions
wer
e 60
min
utes
, thr
eetim
es a
wee
k fo
r 4
wee
ks =
12ho
urs
Sess
ions
wer
e de
liver
ed t
o a
grou
pof
six
sub
ject
s by
tw
o ph
ysic
alth
erap
ists,
in a
reh
abili
tatio
n ce
ntre
sett
ing
Upp
er e
xtre
mity
inte
rven
tion:
Circ
uit
prog
ram
me
desig
ned
to im
prov
efu
nctio
n of
the
affe
cted
upp
er li
mb
Out
com
es r
ecor
ded
atba
selin
e, a
t 4
wee
ks(p
ost-
trea
tmen
t) a
nd2
mon
ths
afte
rco
mpl
etio
n of
tra
inin
g
Lim
b-sp
ecifi
c fu
nctio
n:6M
WT,
10M
WS
(with
and
with
out
assis
tive
devi
ce),
Step
Tes
t, T
UG
Oth
er: S
atisf
actio
n w
ithpr
ogra
mm
e
No
signi
fican
t di
ffere
nce
in w
alki
ng v
eloc
ity a
tba
selin
e fo
r to
tal g
roup
,bu
t af
ter
with
draw
als,
mea
sure
s of
wal
king
spee
d an
d di
stan
cefa
vour
ed t
he c
ontr
olgr
oup.
6M
WT:
mob
ility
grou
p 20
7.9
m (S
D 1
19),
uppe
r lim
b gr
oup
259.
6m
(SD
154
.6);
wal
king
spe
ed w
ithas
sistiv
e de
vice
: mob
ility
grou
p 70
.7cm
/s(S
D41
.8),
uppe
r lim
bgr
oup
86.1
cm/s
(SD
52.6
)
25%
loss
to
follo
w-u
p at
end
of t
reat
men
t ph
ase
Out
com
e as
sess
ors
blin
ded
to g
roup
allo
catio
n, b
ut m
ay h
ave
been
inad
vert
ently
unm
aske
d. 6
MW
Tun
dert
aken
by
one
of t
hein
vest
igat
ors
Inte
rven
tion-
rela
ted
reas
ons
for
with
draw
al:
two
subj
ects
with
drew
befo
re t
rain
ing
(one
owin
g to
tra
nspo
rt c
osts
)
Nin
e pa
rtic
ipan
tsat
tend
ed a
t le
ast
nine
out
of 1
2 se
ssio
ns
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
77
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Hig
gins
, 200
652Se
e Sa
lbac
h, 2
00451
How
e, 2
00577
Two-
cent
re, p
ilot
RCT
Gro
up a
lloca
tion
via
rand
omise
d pe
rmut
edbl
ocks
, with
the
pro
ject
man
ager
hol
ding
det
ails
of a
ssig
nmen
t un
tilal
loca
tion
by a
the
rapi
st
UK
35 p
artic
ipan
ts: 1
8 ex
perim
enta
l, 17
con
trol
Subj
ects
rec
ruite
d fr
om a
dmiss
ions
to
an
acut
e st
roke
uni
t be
twee
n 20
01 a
nd 2
002
Incl
usio
n cr
iteria
: Age
d 18
and
ove
r,ac
ute
vasc
ular
str
oke
pres
entin
g w
ithhe
mip
legi
a, m
edic
ally
sta
ble,
abl
e to
coop
erat
e, p
revi
ously
inde
pend
ently
mob
ile, a
nd in
depe
nden
t in
AD
Ls
Excl
usio
n cr
iteria
: Hist
ory
ofco
nditi
ons
or m
edic
atio
n af
fect
ing
bala
nce,
dem
entia
, im
paire
dco
nsci
ousn
ess
leve
ls, c
onco
mita
ntm
edic
al il
lnes
s or
mus
culo
skel
etal
cond
ition
, ser
ious
per
cept
ual
prob
lem
s
Mea
n ag
e: E
xper
imen
tal g
roup
:71
.5ye
ars
(SD
10.9
), co
ntro
l gro
up70
.7ye
ars
(SD
7.6
)51
% m
ale
Stro
ke d
etai
ls: U
nkno
wn
whe
ther
recu
rren
t st
roke
incl
uded
, 47%
rig
hthe
mip
ares
is
Tim
e sin
ce s
trok
e: E
xper
imen
tal g
roup
26.5
day
s (S
D 1
5.7)
, con
trol
gro
up23
.1 d
ays
(SD
17.
5)
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l:Ri
verm
ead
Mob
ility
Inde
x 24
Expe
rimen
tal g
roup
: Usu
al c
are
plus
exer
cise
s ai
med
at
impr
ovin
g la
tera
lw
eigh
t tr
ansf
eren
ce in
sitt
ing
and
stan
ding
. Thi
s in
clud
ed r
epet
ition
of
self-
initi
ated
goa
l-orie
ntat
edac
tiviti
es in
var
ious
pos
ture
s.
16 t
asks
in t
otal
, with
ten
repe
titio
ns o
f eac
h ex
erci
se
Sess
ions
wer
e 30
min
utes
, thr
eetim
es a
wee
k, fo
r 4
wee
ks =
6ho
urs
Sess
ions
wer
e de
liver
ed b
y tr
aine
dph
ysio
ther
apy
assis
tant
s
Com
paris
on g
roup
: Usu
al c
are:
no
deta
ils g
iven
Out
com
es r
ecor
ded
atba
selin
e, p
ost-
trea
tmen
t(4
wee
ks) a
nd a
t8
wee
ks p
ost-
base
line
Lim
b-sp
ecifi
c fu
nctio
n:Si
t-to
-sta
nd, s
tand
-to-
sit(t
ime
in s
econ
ds),
late
ral
reac
h te
st (t
ime
tore
turn
to
quie
t sit
ting)
No
signi
fican
t di
ffere
nces
repo
rted
at
base
line
6% lo
st t
o fo
llow
-up
aten
d of
tre
atm
ent
phas
e
Out
com
e as
sess
ors
blin
dto
tre
atm
ent
grou
p
No
inte
rven
tion-
rela
ted
reas
ons
for
with
draw
al
Subj
ects
com
plet
ed 1
0.6
sess
ions
on
aver
age cont
inue
d
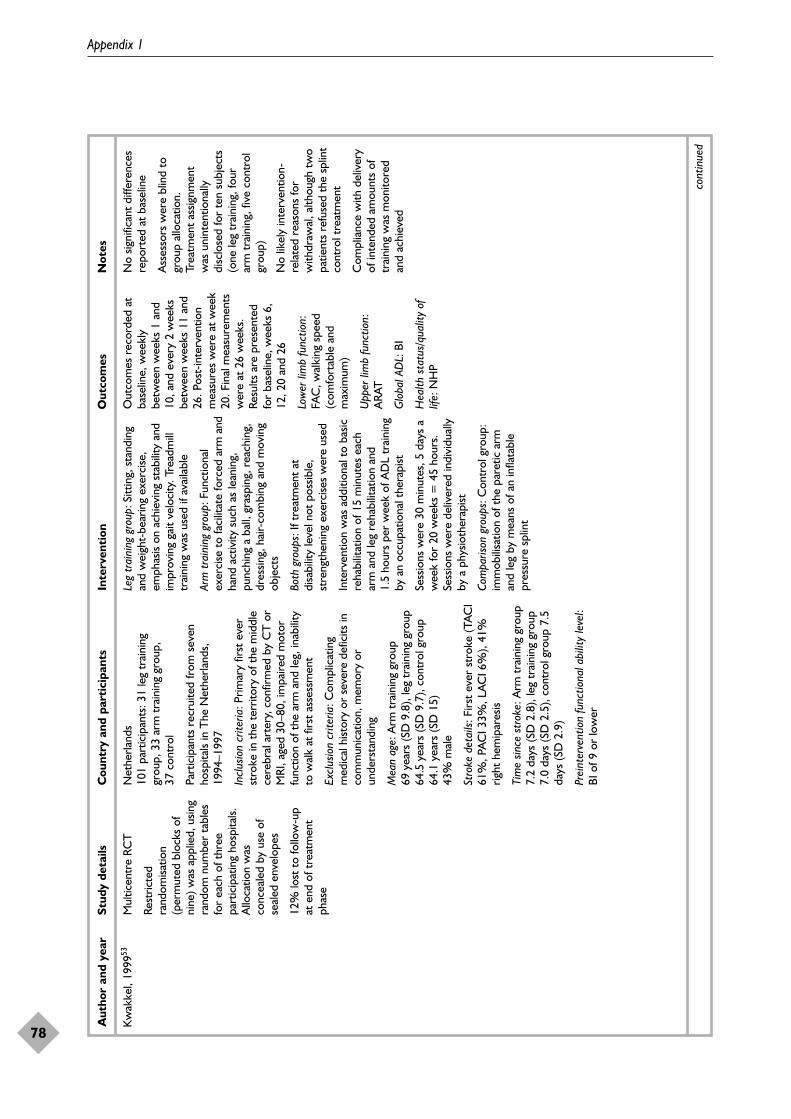
Appendix 1
78
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Kw
akke
l, 19
9953
Mul
ticen
tre
RCT
Rest
ricte
dra
ndom
isatio
n(p
erm
uted
blo
cks
ofni
ne) w
as a
pplie
d, u
sing
rand
om n
umbe
r ta
bles
for
each
of t
hree
part
icip
atin
g ho
spita
ls.A
lloca
tion
was
conc
eale
d by
use
of
seal
ed e
nvel
opes
12%
lost
to
follo
w-u
pat
end
of t
reat
men
tph
ase
Net
herla
nds
101
part
icip
ants
: 31
leg
trai
ning
grou
p, 3
3 ar
m t
rain
ing
grou
p,
37 c
ontr
ol
Part
icip
ants
rec
ruite
d fr
om s
even
hosp
itals
in T
he N
ethe
rland
s,19
94–1
997
Incl
usio
n cr
iteria
: Prim
ary
first
eve
rst
roke
in t
he t
errit
ory
of t
he m
iddl
ece
rebr
al a
rter
y, c
onfir
med
by
CT
or
MRI
, age
d 30
–80,
impa
ired
mot
orfu
nctio
n of
the
arm
and
leg,
inab
ility
to w
alk
at fi
rst
asse
ssm
ent
Excl
usio
n cr
iteria
: Com
plic
atin
gm
edic
al h
istor
y or
sev
ere
defic
its in
com
mun
icat
ion,
mem
ory
orun
ders
tand
ing
Mea
n ag
e: A
rm t
rain
ing
grou
p69
year
s (S
D 9
.8),
leg
trai
ning
gro
up64
.5ye
ars
(SD
9.7
), co
ntro
l gro
up64
.1ye
ars
(SD
15)
43%
mal
e
Stro
ke d
etai
ls: F
irst
ever
str
oke
(TA
CI
61%
, PA
CI 3
3%, L
AC
I 6%
), 41
%rig
ht h
emip
ares
is
Tim
e sin
ce s
trok
e: A
rm t
rain
ing
grou
p7.
2 da
ys (S
D 2
.8),
leg
trai
ning
gro
up7.
0 da
ys (S
D 2
.5),
cont
rol g
roup
7.5
days
(SD
2.9
)
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l:BI
of 9
or
low
er
Leg
trai
ning
gro
up: S
ittin
g, s
tand
ing
and
wei
ght-
bear
ing
exer
cise
,em
phas
is on
ach
ievi
ng s
tabi
lity
and
impr
ovin
g ga
it ve
loci
ty. T
read
mill
trai
ning
was
use
d if
avai
labl
e
Arm
tra
inin
g gr
oup:
Fun
ctio
nal
exer
cise
to
faci
litat
e fo
rced
arm
and
hand
act
ivity
suc
h as
lean
ing,
punc
hing
a b
all,
gras
ping
, rea
chin
g,dr
essin
g, h
air-
com
bing
and
mov
ing
obje
cts
Both
gro
ups:
If t
reat
men
t at
disa
bilit
y le
vel n
ot p
ossib
le,
stre
ngth
enin
g ex
erci
ses
wer
e us
ed
Inte
rven
tion
was
add
ition
al t
o ba
sicre
habi
litat
ion
of 1
5 m
inut
es e
ach
arm
and
leg
reha
bilit
atio
n an
d1.
5ho
urs
per
wee
k of
AD
L tr
aini
ngby
an
occu
patio
nal t
hera
pist
Sess
ions
wer
e 30
min
utes
, 5 d
ays
aw
eek
for
20 w
eeks
= 4
5 ho
urs.
Sess
ions
wer
e de
liver
ed in
divi
dual
lyby
a p
hysio
ther
apist
Com
paris
on g
roup
s: C
ontr
ol g
roup
:im
mob
ilisa
tion
of t
he p
aret
ic a
rman
d le
g by
mea
ns o
f an
infla
tabl
epr
essu
re s
plin
t
Out
com
es r
ecor
ded
atba
selin
e, w
eekl
ybe
twee
n w
eeks
1 a
nd10
, and
eve
ry 2
wee
ksbe
twee
n w
eeks
11
and
26. P
ost-
inte
rven
tion
mea
sure
s w
ere
at w
eek
20. F
inal
mea
sure
men
tsw
ere
at 2
6 w
eeks
.Re
sults
are
pre
sent
edfo
r ba
selin
e, w
eeks
6,
12, 2
0 an
d 26
Low
er li
mb
func
tion:
FAC
, wal
king
spe
ed(c
omfo
rtab
le a
ndm
axim
um)
Upp
er li
mb
func
tion:
ARA
T
Glo
bal A
DL:
BI
Hea
lth s
tatu
s/qu
ality
of
life:
NH
P
No
signi
fican
t di
ffere
nces
repo
rted
at
base
line
Ass
esso
rs w
ere
blin
d to
grou
p al
loca
tion.
Trea
tmen
t as
signm
ent
was
uni
nten
tiona
llydi
sclo
sed
for
ten
subj
ects
(one
leg
trai
ning
, fou
rar
m t
rain
ing,
five
con
trol
grou
p)
No
likel
y in
terv
entio
n-re
late
d re
ason
s fo
rw
ithdr
awal
, alth
ough
tw
opa
tient
s re
fuse
d th
e sp
lint
cont
rol t
reat
men
t
Com
plia
nce
with
del
iver
yof
inte
nded
am
ount
s of
trai
ning
was
mon
itore
dan
d ac
hiev
ed
cont
inue
d

Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Health Technology Assessment 2008; Vol. 12: No. 30
79
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Lang
ham
mer
, 200
068St
ratif
ied,
sin
gle-
cent
reRC
T
Subj
ects
ran
dom
ised
and
stra
tifie
d ac
cord
ing
to g
ende
r an
dhe
misp
here
site
. No
deta
ils o
f ran
dom
isatio
n
Nor
way
61 p
artic
ipan
ts: 3
3 ex
perim
enta
l, 28
con
trol
Subj
ects
rec
ruite
d fr
om p
atie
nts
atte
ndin
g ho
spita
l in
Nor
way
,19
96–1
997
Incl
usio
n cr
iteria
: Firs
t ev
er s
trok
ew
ith h
emip
ares
is ve
rifie
d cl
inic
ally
and
by C
T
Excl
usio
n cr
iteria
: Mor
e th
an o
nest
roke
inci
dent
, sub
arac
hnoi
dbl
eedi
ng, t
umou
rs o
f the
bra
in,
othe
r se
vere
med
ical
con
ditio
ns in
com
bina
tion
with
str
oke,
5 o
r m
ore
poin
ts o
n ea
ch o
f the
sco
res
on t
heM
AS
Mea
n ag
e:78
yea
rs (S
D 9
) (ra
nge
49–7
5)59
% m
ale
Stro
ke d
etai
ls: F
irst
stro
ke, 5
6% r
ight
hem
ipar
esis
Tim
e sin
ce s
trok
e: B
asel
ine
mea
sure
sta
ken
with
in 3
days
of a
dmiss
ion
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l:BI
mea
n 51
Expe
rimen
tal g
roup
: Mot
orRe
lear
ning
Pro
gram
me
as p
er C
arr
and
Shep
herd
, 198
7.18
Func
tiona
lta
sk t
rain
ing
in o
rdin
ary
sett
ings
,w
ith o
rdin
ary
task
s, u
sing
the
prin
cipl
es o
f max
imal
rep
etiti
on,
task
and
set
ting
varia
tion
Expe
rimen
tal i
nter
vent
ion
was
inst
ead
of u
sual
car
e
Sess
ions
wer
e 40
min
utes
min
imum
per
sess
ion,
5 d
ays
a w
eek
for
aslo
ng a
s ho
spita
lised
, and
con
tinui
ngin
to t
he c
omm
unity
, alth
ough
rece
ipt
of p
hysio
ther
apy
inco
mm
unity
set
tings
was
var
iabl
e
Sess
ions
wer
e de
liver
ed b
y ho
spita
lan
d ou
tpat
ient
phy
sioth
erap
ists.
Afte
r di
scha
rge,
som
e su
bjec
tsre
ceiv
ed t
hera
py in
the
ir ow
nho
mes
, at
reha
bilit
atio
n ce
ntre
s or
priv
ate
outp
atie
nt d
epar
tmen
ts,
depe
nden
t on
nee
d
Com
paris
on g
roup
: Bob
ath
prog
ram
me,
as
per
Boba
th, 1
99014
4
Out
com
es r
ecor
ded
atba
selin
e, a
nd a
t 2
wee
ks,
3 m
onth
s, 1
yea
r an
d4
year
s po
st-s
trok
e
Lim
b-sp
ecifi
c fu
nctio
n:M
AS,
SM
ES –
sub
scal
efo
r tr
unk/
bala
nce/
gait,
Berg
Bal
ance
Sca
le(1
year
onl
y)
Mot
or p
erfo
rman
ce:
SMES
– s
ubsc
ales
for
leg
func
tion
and
arm
func
tion
Glo
bal f
unct
ion:
BI,
NH
P.
Oth
er m
easu
res:
Len
gth
of s
tay,
use
of
whe
elch
air,
disc
harg
ede
stin
atio
n
Con
trol
gro
up s
light
lym
ore
depe
nden
t at
ent
ry(b
asel
ine)
, but
no
signi
fican
t di
ffere
nce
inM
AS,
SM
ES o
r BI
Dat
a av
aila
ble
for
87%
at
3 m
onth
s
Blin
ding
sta
ted,
but
no
desc
riptio
n gi
ven
No
inte
rven
tion-
rela
ted
reas
ons
for
with
draw
al
Doe
s no
t st
ate
mon
itorin
g of
tim
e sp
ent
in t
hera
py
cont
inue
d

Appendix 1
80
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
McC
lella
n, 2
00478
Dou
ble-
blin
d RC
T
Rand
omisa
tion
bynu
mbe
red,
sea
led,
opaq
ue e
nvel
opes
Aus
tral
ia26
par
ticip
ants
: 15
expe
rimen
tal,
11 c
ontr
ol
Subj
ects
rec
ruite
d on
disc
harg
e fr
omph
ysio
ther
apy
serv
ices
in s
ix h
ospi
tals
in o
ne r
egio
n
Incl
usio
n cr
iteria
: Str
oke
with
in t
hepa
st 1
8 m
onth
s, 4
5 ye
ars
and
olde
r,liv
ing
in t
he c
omm
unity
, sco
re >
0an
d <
6 on
MA
S, s
core
<6
on
item
7 o
r 8
of t
he M
AS
Excl
usio
n cr
iteria
: Una
ble
to c
onse
nt,
unco
ntro
lled
card
iac
sym
ptom
s or
othe
r m
edic
al c
ondi
tions
tha
t lim
ited
exer
cise
, or
with
a p
acem
aker
Mea
n ag
e: E
xper
imen
tal g
roup
69ye
ars
(SD
13)
, con
trol
gro
up72
year
s (S
D 9
)50
% m
ale
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or r
ecur
rent
str
oke,
50%
rig
hthe
mip
ares
is
Tim
e sin
ce s
trok
e: E
xper
imen
tal g
roup
med
ian
6.5
mon
ths
(IQR
5.5)
, con
trol
grou
p m
edia
n 4.
5 m
onth
s (IQ
R 3)
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l:A
ll su
bjec
ts c
ould
wal
k, b
ut w
ithdi
fficu
lty
Expe
rimen
tal g
roup
: Hom
e-ba
sed
exer
cise
pro
gram
me
aim
ed a
tim
prov
ing
mob
ility
in s
tand
ing
bala
nce
and
wal
king
, bas
ed o
n a
list
of 2
3 ac
tiviti
es a
rran
ged
hier
arch
ical
ly o
n th
eir
chal
leng
e to
bala
nce.
The
hom
e pr
ogra
mm
eus
ed v
ideo
sel
f-m
odel
ling
prep
ared
on a
bas
elin
e vi
sit t
o th
e cl
inic
to
pres
crib
e th
e ex
erci
se p
rogr
amm
e,te
leph
one
mon
itorin
g to
enc
oura
geco
mpl
ianc
e, a
nd t
wo
clin
ic v
isits
for
prog
ram
me
revi
ew
Sess
ions
wer
e pr
escr
ibed
60m
inut
es p
er d
ay o
ver
6 w
eeks
= 4
2 ho
urs.
Sub
ject
s w
ere
requ
ired
to k
eep
a re
cord
of
prac
tice
Com
paris
on g
roup
: Hom
e-ba
sed
exer
cise
pro
gram
me
for
impr
ovin
gup
per
limb
func
tion,
sta
rtin
g fr
omba
sic m
ovem
ent
thro
ugh
tofu
nctio
nal a
ctiv
ity, u
sing
the
sam
ese
lf-in
stru
ctio
nal v
ideo
, sel
f and
tele
phon
e m
onito
ring
and
clin
icvi
sits
as t
he e
xper
imen
tal g
roup
Out
com
es r
ecor
ded
atba
selin
e, p
ost-
trea
tmen
t(6
wee
ks) a
nd a
t14
wee
ks
Lim
b-sp
ecifi
c fu
nctio
n:Fu
nctio
nal R
each
Tes
t(c
m),
MA
S w
alki
ng
No
base
line
com
paris
ons
repo
rted
19%
lost
to
follo
w-u
p by
end
of t
reat
men
t ph
ase
Ass
esso
rs a
nd s
ubje
cts
blin
d to
gro
up a
lloca
tion
No
likel
y in
terv
entio
n-re
late
d re
ason
s fo
rw
ithdr
awal
Subj
ects
sel
f-re
port
ed75
% c
ompl
ianc
e w
ithpr
escr
ibed
exe
rcise
s
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
81
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Salb
ach,
200
4;51
Hig
gins
, 200
652St
ratif
ied,
mul
ticen
tre
RCT
Part
icip
ants
str
atifi
edin
to t
hree
gro
ups
base
don
com
fort
able
wal
king
spee
d. S
eque
nce
ofra
ndom
ass
ignm
ents
com
pute
r ge
nera
ted
inra
ndom
ly o
rder
edbl
ocks
of 2
and
4 fo
rea
ch s
trat
um. A
lloca
tion
mai
ntai
ned
in s
eale
d,op
aque
env
elop
es,
prep
ared
bef
ore
recr
uitm
ent
by p
erso
nsno
t in
volv
ed in
the
stud
y, a
nd u
nvei
led
afte
r ba
selin
eas
sess
men
t an
dst
ratif
icat
ion
Can
ada
91 p
artic
ipan
ts: 4
4 m
obili
ty, 4
7 ar
mtr
aini
ng g
roup
Subj
ects
wer
e re
crui
ted
from
nin
eho
spita
ls an
d tw
o re
habi
litat
ion
cent
res
in M
ontr
eal o
r Q
uebe
c
Incl
usio
n cr
iteria
: Firs
t or
rec
urre
ntst
roke
, und
er 1
yea
r po
st-s
trok
e at
recr
uitm
ent,
able
to
wal
k 10
m b
utw
ith r
esid
ual w
alki
ng d
efic
it fr
omm
ost
rece
nt s
trok
e, m
enta
lco
mpe
tenc
y an
d ab
ility
to
com
preh
end
inst
ruct
ions
, disc
harg
edfr
om p
hysic
al r
ehab
ilita
tion
and
resid
ent
in t
he c
omm
unity
Excl
usio
n cr
iteria
: Res
iden
t in
perm
anen
t ca
re fa
cilit
y, c
o-m
orbi
dity
prec
ludi
ng p
artic
ipat
ion
Mea
n ag
e: 7
2 ye
ars,
(ran
ge 3
8–91
)61
.5%
mal
e
Stro
ke d
etai
ls: F
irst
or r
ecur
rent
stro
ke, 8
3% is
chae
mic
, 56%
rig
hthe
mip
ares
is, 4
3% le
ft he
mip
ares
is,1%
bila
tera
l
Tim
e sin
ce s
trok
e: m
ean
228
days
(S
D 7
8)
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l:6M
WT
mea
n 20
7m
(SD
128
)
Mob
ility
inte
rven
tion:
Ten
wal
king
-re
late
d ta
sks
desig
ned
tost
reng
then
the
low
er e
xtre
miti
esan
d en
hanc
e w
alki
ng b
alan
ce,
spee
d an
d di
stan
ce in
a p
rogr
essiv
em
anne
r
Upp
er e
xtre
mity
inte
rven
tion:
Func
tiona
l tas
ks s
uch
asm
anip
ulat
ing
card
s, u
sing
ake
yboa
rd a
nd w
ritin
g w
hile
sea
ted
Inte
rven
tion
was
afte
r di
scha
rge
from
phy
sical
reh
abili
tatio
n
Sess
ions
wer
e 60
min
utes
, thr
eetim
es a
wee
k fo
r 6
wee
ks =
18ho
urs
Sess
ions
wer
e de
liver
ed in
divi
dual
lyby
a p
hysic
al o
r oc
cupa
tiona
lth
erap
ist in
a h
ospi
tal o
utpa
tient
or
reha
bilit
atio
n se
ttin
g
Com
paris
on g
roup
: Sal
bach
, 200
4:51
uppe
r ex
trem
ity t
rain
ing,
Hig
gins
,20
06:52
low
er e
xtre
mity
tra
inin
g
Out
com
es r
ecor
ded
atba
selin
e an
d at
6 w
eeks
Lim
b-sp
ecifi
c fu
nctio
n:6M
WT,
5-m
wal
k at
com
fort
able
and
max
imum
spe
ed, T
UG
,Be
rg B
alan
ce S
cale
,A
ctiv
ities
Spe
cific
Bala
nce
Con
fiden
ceSc
ale
Glo
bal A
DL:
BI
No
repo
rt o
f sig
nific
ant
diffe
renc
es a
t ba
selin
e
Inte
rven
tion-
rela
ted
reas
ons
for
with
draw
al:
one
unw
illin
g to
tra
vel,
one
expe
rienc
ed t
heon
set
of g
roin
pai
n; t
wo
wan
ted
the
othe
rin
terv
entio
n
Full
inte
ntio
n-to
-tre
atan
alys
is us
ed, w
ith
post
-inte
rven
tion
valu
esfo
r su
bjec
ts im
pute
d
Ass
esso
rs w
ere
blin
d to
grou
p al
loca
tion.
Unb
lindi
ng o
ccur
red
for
18/4
2 in
the
mob
ility
grou
p an
d 16
/43
of t
heup
per
extr
emity
tra
inin
ggr
oup,
but
did
not
bia
sth
e es
timat
ed e
ffect
as
eval
uate
d by
mul
tiple
linea
r re
gres
sion
mod
el
86%
of m
obili
ty g
roup
subj
ects
att
ende
d 17
or
mor
e se
ssio
ns o
ut o
f 18.
72%
of u
pper
ext
rem
ityat
tend
ed 1
7 or
mor
ese
ssio
ns
344
peop
le w
ere
eval
uate
d fo
r pa
rtic
ipat
ion
but
73%
ref
used
bec
ause
they
cou
ld n
ot t
oler
ate
the
trav
el r
equi
red
for
atte
ndan
ce
cont
inue
d

Appendix 1
82
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Turt
on, 1
99069
Sing
le-c
entr
e, q
uasi-
rand
omise
d tr
ial
Subj
ects
wer
e as
signe
din
alte
rnat
e ru
ns o
f fiv
e
UK
22 p
artic
ipan
ts: 1
2 ex
perim
enta
l, te
nin
the
con
trol
Subj
ects
rec
ruite
d fr
om s
trok
epa
tient
s di
scha
rged
from
inpa
tient
care
at
one
hosp
ital,
1986
–198
7
Incl
usio
n cr
iteria
: Som
e im
pairm
ent
offu
nctio
n of
the
affe
cted
upp
er li
mb
(i.e.
less
tha
n 95
% p
erfo
rman
ce o
n a
peg
tran
sfer
tas
k), a
ble
to u
nder
stan
din
stru
ctio
ns, l
ives
with
in 2
5 m
iles
(15.
5 km
) of h
ospi
tal
Excl
usio
n cr
iteria
: Non
e st
ated
Mea
n ag
e: E
xper
imen
tal g
roup
59ye
ars
(SD
11.
97),
cont
rol g
roup
58ye
ars
(SD
6.8
6)55
% m
ale
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or r
ecur
rent
str
oke,
56%
rig
hthe
mip
ares
is
Tim
e sin
ce s
trok
e: E
xper
imen
tal g
roup
24 w
eeks
(SD
25.
8), c
ontr
ol g
roup
16 w
eeks
(SD
6.1
)
Prei
nter
vent
ion
disa
bilit
y le
vel:
12.5
/20
on S
outh
ern
Mot
or A
sses
smen
t Sc
ale
Expe
rimen
tal g
roup
: Usu
alou
tpat
ient
car
e pl
us h
ome-
base
dex
erci
se p
rogr
amm
e fo
r th
e up
per
limb,
bas
ed o
n m
otor
rel
earn
ing
prin
cipl
es. E
xerc
ises
incl
uded
mov
emen
t an
d ta
sk-r
elat
ed r
each
,gr
asp
and
grip
. Sub
ject
s w
ere
visit
ed b
y an
occ
upat
iona
l the
rapi
stat
hom
e, a
nd g
iven
exe
rcise
s an
dre
petit
ions
. Exe
rcise
s w
ere
deta
iled
in a
boo
klet
. Sub
ject
s w
ere
visit
ed e
very
2–4
wee
ks fo
r re
view
.C
arer
s w
ere
invo
lved
if a
ble
and
will
ing
Subj
ects
wer
e as
signe
d tw
o to
thre
e pr
actic
e se
ssio
ns p
er d
ay(a
ppro
x. 1
hou
r), 7
day
s a
wee
k fo
r8–
11 w
eeks
= 6
3 ho
urs
appr
ox.
Sess
ions
wer
e se
lf-m
anag
ed b
y th
esu
bjec
t an
d th
eir
care
rs a
t ho
me,
with
tw
o to
thr
ee h
ome
visit
s by
an
occu
patio
nal t
hera
pist
for
prog
ram
me
revi
ew
Com
paris
on g
roup
: Usu
al o
utpa
tient
care
(som
e ha
d th
erap
y, b
ut o
ther
sdi
d no
t)
Out
com
es r
ecor
ded
atba
selin
e an
d po
st-
trea
tmen
t (8
–11
wee
ks)
Lim
b-sp
ecifi
c m
otor
perfo
rman
ce: S
ittin
g pa
rtof
the
upp
er li
mb
activ
ity a
sses
smen
t –
Sout
hern
Mot
or G
roup
Ass
essm
ent,
10H
PT
Base
line
diffe
renc
es:
Diff
eren
ce in
tim
e sin
cest
roke
: exp
erim
enta
lgr
oup
mea
n of
24
wee
ks,
and
usua
l car
e m
ean
of16
wee
ks. 1
0HPT
perf
orm
ance
:ex
perim
enta
l gro
up m
ore
disa
bled
, hom
e th
erap
ygr
oup
had
mor
e ca
rers
livin
g at
hom
e
No
loss
to
follo
w-u
p at
end
of t
reat
men
t ph
ase
Out
com
e as
sess
or n
otbl
inde
d to
tre
atm
ent
grou
p
No
inte
rven
tion-
rela
ted
reas
ons
for
with
draw
al
Self-
repo
rted
rat
es o
fco
mpl
ianc
e: m
ean
68%
(SD
25)
. Thr
ee o
ut o
f 12
sub
ject
s ra
ted
less
than
50%
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
83
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Van
Vlie
t, 20
0570
Sing
le-c
entr
e RC
T
Rand
omisa
tion
was
by
com
pute
r-ge
nera
ted
rand
om s
eque
nce
prov
ided
by
anin
depe
nden
t pe
rson
.Bl
ocke
d ra
ndom
isatio
nw
as u
sed.
Allo
catio
nsw
ere
prov
ided
inen
velo
pes
and
open
edaf
ter
initi
al a
sses
smen
t
UK
120
part
icip
ants
: 60
expe
rimen
tal,
60 c
ontr
ol
Subj
ects
wer
e re
crui
ted
from
peo
ple
adm
itted
to
a st
roke
reh
abili
tatio
nw
ard
over
a p
erio
d of
21
mon
ths
Incl
usio
n cr
iteria
: Dia
gnos
is of
str
oke,
refe
rral
to
phys
ioth
erap
y
Excl
usio
n cr
iteria
: Mor
e th
an 2
wee
kspo
st-s
trok
e, u
ncon
scio
us o
nad
miss
ion,
una
ble
to t
oile
tin
depe
nden
tly p
rior
to s
trok
e, li
ving
mor
e th
an 2
5km
from
hos
pita
l,un
able
to
tole
rate
mor
e th
an30
min
utes
of p
hysic
al t
asks
req
uire
din
initi
al a
sses
smen
t
Mea
n ag
e: E
xper
imen
tal g
roup
75ye
ars
(SD
9.1
), co
ntro
l gro
up73
.3ye
ars
(SD
10.
4)50
% m
ale
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or r
ecur
rent
str
oke.
51%
rig
hthe
mip
ares
is, 4
6% le
ft he
mip
ares
is,3%
bila
tera
l
Tim
e sin
ce s
trok
e: W
ithin
14
days
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l:Ri
verm
ead
Mot
or A
sses
smen
t gr
oss
func
tion
subs
cale
: med
ian
(IQR)
expe
rimen
tal g
roup
2 (1
–6),
cont
rol
grou
p 1
(1–4
)
Mov
emen
t sc
ienc
e th
erap
y: B
ased
on
the
prin
cipl
e th
at s
kill
inpe
rfor
man
ce is
a d
irect
func
tion
ofth
e am
ount
of p
ract
ice.
Pro
gram
me
invo
lved
use
of e
very
day
obje
cts
for
func
tiona
l tra
inin
g, a
nd p
ract
ice
outs
ide
deliv
ered
ses
sions
Inte
rven
tion
was
inst
ead
of u
sual
care
Subj
ects
rec
eive
d a
med
ian
23m
inut
es o
f tre
atm
ent
by a
phys
ioth
erap
ist p
er w
eek
day
(IQR
13–3
2m
). M
edia
n to
tal n
umbe
r of
min
utes
of t
reat
men
t w
as 3
65 (I
QR
140–
1160
), eq
uatin
g to
app
rox.
6ho
urs’
tot
al t
rain
ing
time
Trea
tmen
t w
as d
eliv
ered
by
phys
ioth
erap
ists,
occ
upat
iona
lth
erap
ists
and
phys
ioth
erap
yas
sista
nts,
in h
ospi
tal,
and
as a
nou
tpat
ient
afte
r di
scha
rge.
Trea
tmen
t w
as d
eliv
ered
for
as lo
ngas
nee
ded
Com
paris
on g
roup
: Bob
ath-
base
dth
erap
y
Out
com
es r
ecor
ded
atba
selin
e, 4
wee
ks,
3m
onth
s an
d 6
mon
ths
Lim
b-sp
ecifi
c fu
nctio
n:RM
A S
cale
, MA
S,6M
WS,
10H
PT
Glo
bal f
unct
ion:
BI,
Exte
nded
Act
iviti
es o
fD
aily
Liv
ing
At
base
line,
con
trol
gro
upha
d hi
gher
med
ian
scor
esfo
r Ri
verm
ead
gros
sfu
nctio
n, a
nd le
g an
dtr
unk
subs
cale
s, a
nd fo
rsu
pine
to
side
lyin
g,su
pine
to
sittin
g, b
alan
ced
sittin
g, a
nd s
it-to
-sta
ndse
ctio
ns o
f the
MA
S.Ex
perim
enta
l gro
up h
adhi
gher
med
ian
scor
es fo
rth
e up
per
arm
sec
tion
ofth
e M
AS
Dat
a av
aila
ble
for
71%
at
3 m
onth
s
Out
com
e as
sess
ors
blin
dto
tre
atm
ent
allo
catio
n.Bl
indi
ng a
sses
sed
assu
cces
sful
Inte
rven
tion-
rela
ted
reas
ons
for
with
draw
al:
seve
n su
bjec
ts r
efus
edou
tcom
e m
easu
rem
ent
at3
mon
ths,
5 in
the
expe
rimen
tal g
roup
and
two
in t
he c
ontr
ol g
roup
,bu
t re
ason
s ar
e no
tkn
own
cont
inue
d
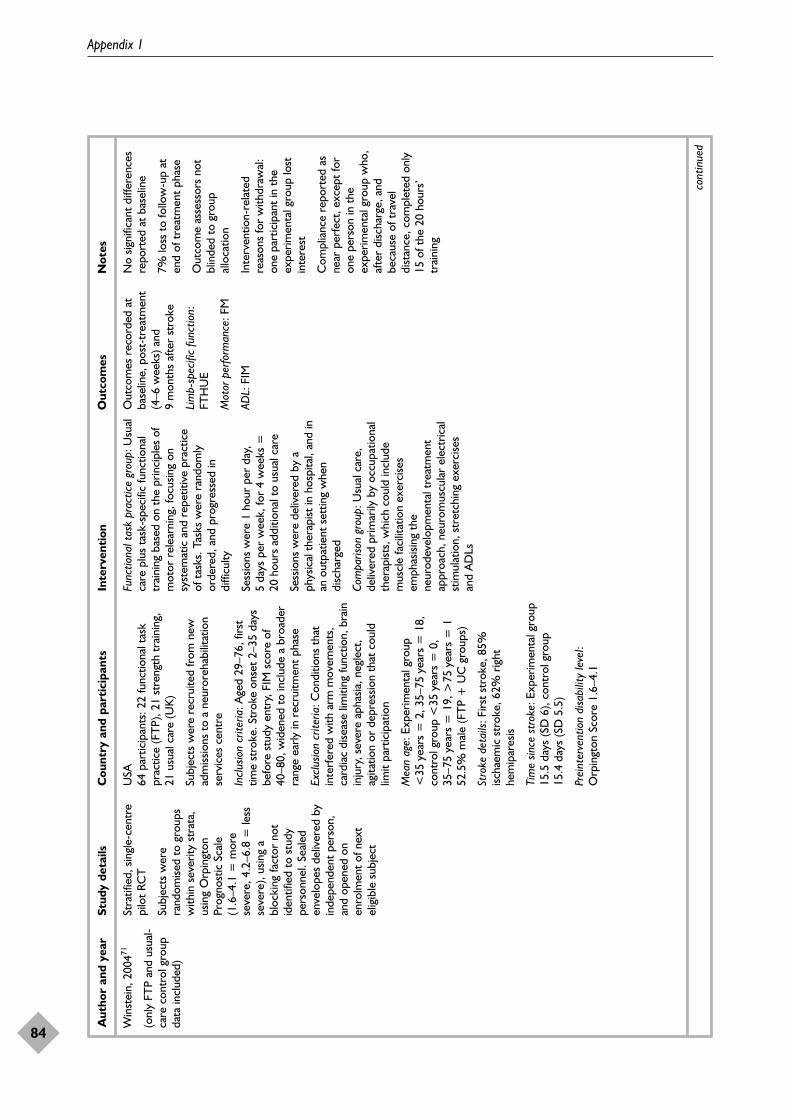
Appendix 1
84
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Win
stei
n, 2
00471
(onl
y FT
P an
d us
ual-
care
con
trol
gro
upda
ta in
clud
ed)
Stra
tifie
d, s
ingl
e-ce
ntre
pilo
t RC
T
Subj
ects
wer
era
ndom
ised
to g
roup
sw
ithin
sev
erity
str
ata,
usin
g O
rpin
gton
Prog
nost
ic S
cale
(1.6
–4.1
= m
ore
seve
re, 4
.2–6
.8 =
less
seve
re),
usin
g a
bloc
king
fact
or n
otid
entif
ied
to s
tudy
pers
onne
l. Se
aled
enve
lope
s de
liver
ed b
yin
depe
nden
t pe
rson
,an
d op
ened
on
enro
lmen
t of
nex
tel
igib
le s
ubje
ct
USA
64 p
artic
ipan
ts: 2
2 fu
nctio
nal t
ask
prac
tice
(FT
P), 2
1 st
reng
th t
rain
ing,
21 u
sual
car
e (U
K)
Subj
ects
wer
e re
crui
ted
from
new
adm
issio
ns t
o a
neur
oreh
abili
tatio
nse
rvic
es c
entr
e
Incl
usio
n cr
iteria
: Age
d 29
–76,
firs
ttim
e st
roke
. Str
oke
onse
t 2–
35 d
ays
befo
re s
tudy
ent
ry, F
IM s
core
of
40–8
0, w
iden
ed t
o in
clud
e a
broa
der
rang
e ea
rly in
rec
ruitm
ent
phas
e
Excl
usio
n cr
iteria
: Con
ditio
ns t
hat
inte
rfer
ed w
ith a
rm m
ovem
ents
,ca
rdia
c di
seas
e lim
iting
func
tion,
bra
inin
jury
, sev
ere
apha
sia, n
egle
ct,
agita
tion
or d
epre
ssio
n th
at c
ould
limit
part
icip
atio
n
Mea
n ag
e: E
xper
imen
tal g
roup
<35
year
s =
2, 3
5–75
year
s =
18,
cont
rol g
roup
<35
year
s =
0,
35–7
5ye
ars
= 1
9, >
75ye
ars
= 1
52.5
% m
ale
(FT
P +
UC
gro
ups)
Stro
ke d
etai
ls: F
irst
stro
ke, 8
5%isc
haem
ic s
trok
e, 6
2% r
ight
hem
ipar
esis
Tim
e sin
ce s
trok
e: E
xper
imen
tal g
roup
15.5
day
s (S
D 6
), co
ntro
l gro
up15
.4da
ys (S
D 5
.5)
Prei
nter
vent
ion
disa
bilit
y le
vel:
Orp
ingt
on S
core
1.6
–4.1
Func
tiona
l tas
k pr
actic
e gr
oup:
Usu
alca
re p
lus
task
-spe
cific
func
tiona
ltr
aini
ng b
ased
on
the
prin
cipl
es o
fm
otor
rel
earn
ing,
focu
sing
onsy
stem
atic
and
rep
etiti
ve p
ract
ice
of t
asks
. Tas
ks w
ere
rand
omly
orde
red,
and
pro
gres
sed
indi
fficu
lty
Sess
ions
wer
e 1
hour
per
day
,5
days
per
wee
k, fo
r 4
wee
ks =
20ho
urs
addi
tiona
l to
usua
l car
e
Sess
ions
wer
e de
liver
ed b
y a
phys
ical
the
rapi
st in
hos
pita
l, an
d in
an o
utpa
tient
set
ting
whe
ndi
scha
rged
Com
paris
on g
roup
: Usu
al c
are,
deliv
ered
prim
arily
by
occu
patio
nal
ther
apist
s, w
hich
cou
ld in
clud
em
uscl
e fa
cilit
atio
n ex
erci
ses
emph
asisi
ng t
hene
urod
evel
opm
enta
l tre
atm
ent
appr
oach
, neu
rom
uscu
lar
elec
tric
alst
imul
atio
n, s
tret
chin
g ex
erci
ses
and
AD
Ls
Out
com
es r
ecor
ded
atba
selin
e, p
ost-
trea
tmen
t(4
–6 w
eeks
) and
9m
onth
s af
ter
stro
ke
Lim
b-sp
ecifi
c fu
nctio
n:FT
HU
E
Mot
or p
erfo
rman
ce: F
M
ADL:
FIM
No
signi
fican
t di
ffere
nces
repo
rted
at
base
line
7% lo
ss t
o fo
llow
-up
aten
d of
tre
atm
ent
phas
e
Out
com
e as
sess
ors
not
blin
ded
to g
roup
allo
catio
n
Inte
rven
tion-
rela
ted
reas
ons
for
with
draw
al:
one
part
icip
ant
in t
heex
perim
enta
l gro
up lo
stin
tere
st
Com
plia
nce
repo
rted
as
near
per
fect
, exc
ept
for
one
pers
on in
the
expe
rimen
tal g
roup
who
,af
ter
disc
harg
e, a
ndbe
caus
e of
tra
vel
dist
ance
, com
plet
ed o
nly
15 o
f the
20
hour
s’tr
aini
ng
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
85
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Yen,
200
572Si
ngle
-cen
tre
RCT
No
deta
ils o
fra
ndom
isatio
n m
etho
d
Taiw
an30
par
ticip
ants
: 13
expe
rimen
tal,
17co
ntro
l
Subj
ects
rec
ruite
d fr
om a
dep
artm
ent
of n
euro
logy
Incl
usio
n cr
iteria
: Sin
gle
stro
kere
sulti
ng in
hem
ipar
esis,
min
imum
of
20 d
egre
es o
f act
ive
wris
t ex
tens
ion
and
10 d
egre
es o
f act
ive
finge
rex
tens
ion,
age
d 18
–80,
no
seve
reap
hasia
or
cogn
itive
impa
irmen
t
Excl
usio
n cr
iteria
: Oth
er d
iseas
es t
hat
wou
ld c
onfo
und
the
stud
y su
ch a
sPa
rkin
son’
s di
seas
e, s
houl
der
subl
uxat
ion,
rec
urre
nt s
trok
e du
ring
the
trai
ning
per
iod
Mea
n ag
e68
year
s (r
ange
47–
80)
46%
mal
e
Stro
ke d
etai
ls: F
irst
stro
ke, 6
0% r
ight
hem
ipar
esis
Tim
e sin
ce s
trok
e: E
xper
imen
tal g
roup
8.4
mon
ths
(SD
8),
cont
rol g
roup
6.2
mon
ths
(SD
7.9
)
Prei
nter
vent
ion
func
tiona
l abi
lity
leve
l:ba
selin
e m
ean
3.28
sec
onds
per
item
on t
he W
MFT
Expe
rimen
tal i
nter
vent
ion:
Pra
ctic
eof
15–
20 t
asks
sel
ecte
d fr
om a
batt
ery
of 5
0 ta
sks,
with
tas
ksh
apin
g, c
onsis
ting
of v
erba
lfe
edba
ck fo
r sm
all i
mpr
ovem
ents
,ta
sk s
elec
tion
base
d on
nee
ds o
fin
divi
dual
, and
per
form
ance
assis
tanc
e in
the
initi
al s
tage
s if
unab
le t
o pe
rfor
m in
depe
nden
tly
Inte
rven
tion
was
inst
ead
of u
sual
care
Sess
ions
wer
e 6
hour
s pe
r da
y. It
isun
clea
r w
heth
er t
here
wer
e fiv
e or
seve
n se
ssio
ns p
er w
eek.
Trea
tmen
t du
ratio
n w
as 2
wee
ks =
60–8
4 ho
urs
Sess
ions
wer
e de
liver
ed b
y a
phys
ical
the
rapi
st. I
t is
uncl
ear
whe
ther
ses
sions
wer
e gr
oup
base
dor
indi
vidu
al
Com
paris
on g
roup
: Reg
ular
prog
ram
me
of p
hysic
al t
hera
pyin
clud
ing
gait
trai
ning
, fac
ilita
tion,
bala
nce
trai
ning
or
occu
patio
nal
ther
apy.
It is
unc
lear
how
muc
htim
e th
e co
ntro
l gro
up s
pent
inth
erap
y
Out
com
es r
ecor
ded
atba
selin
e an
d po
st-
trea
tmen
t (2
wee
ks)
Lim
b-sp
ecifi
c fu
nctio
n:M
ean
time
take
n to
com
plet
e in
divi
dual
item
s on
the
WM
FT.
Resu
lts fo
r ite
ms
8–15
are
only
pre
sent
edfo
r su
bjec
ts a
ble
toco
mpl
ete
them
with
in2
min
utes
No
base
line
diffe
renc
esre
port
ed
No
loss
to
follo
w-u
p at
end
of t
reat
men
t ph
ase
Blin
ding
sta
ted,
but
no
desc
riptio
n gi
ven
No
inte
rven
tion-
rela
ted
reas
ons
for
with
draw
al
No
repo
rt o
f att
enda
nce
CT,
com
pute
d to
mog
raph
y; F
M, F
ugl–
Mey
er; F
TP,
func
tiona
l tas
k pr
actic
e; L
AC
I, la
cuna
r in
farc
tion;
MI,
myo
card
ial i
nfar
ctio
n; N
HP,
Not
tingh
am H
ealth
Pro
file;
PA
CI,
part
ial a
nter
ior
circ
ulat
ion
infa
rctio
n; T
AC
I, to
tal a
nter
ior
circ
ulat
ion
infa
rctio
n; U
C, u
sual
car
e.

Health Technology Assessment 2008; Vol. 12: No. 30
87
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Appendix 2
Included studies: constraint-induced movement therapy
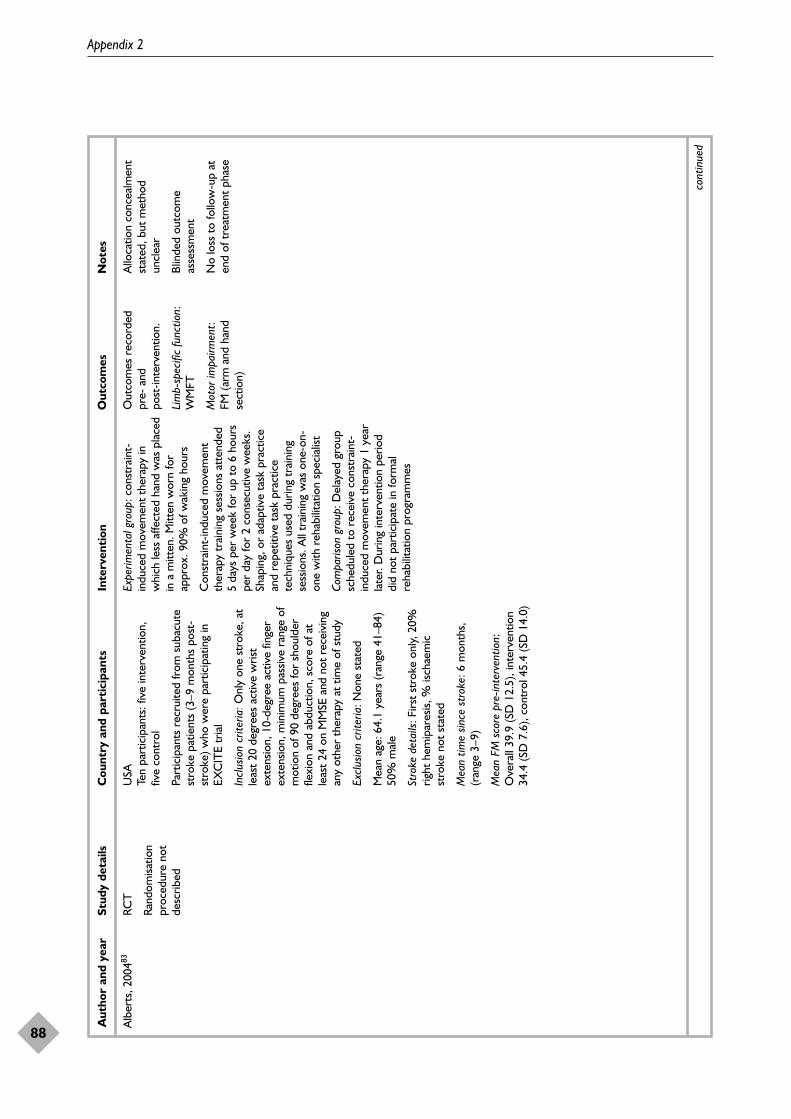
Appendix 2
88
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Alb
erts
, 200
483RC
T
Rand
omisa
tion
proc
edur
e no
tde
scrib
ed
USA
Ten
part
icip
ants
: fiv
e in
terv
entio
n,fiv
e co
ntro
l
Part
icip
ants
rec
ruite
d fr
om s
ubac
ute
stro
ke p
atie
nts
(3–9
mon
ths
post
-st
roke
) who
wer
e pa
rtic
ipat
ing
inEX
CIT
E tr
ial
Incl
usio
n cr
iteria
:Onl
y on
e st
roke
, at
leas
t 20
deg
rees
act
ive
wris
tex
tens
ion,
10-
degr
ee a
ctiv
e fin
ger
exte
nsio
n, m
inim
um p
assiv
e ra
nge
ofm
otio
n of
90
degr
ees
for
shou
lder
flexi
on a
nd a
bduc
tion,
sco
re o
f at
leas
t 24
on
MM
SE a
nd n
ot r
ecei
ving
any
othe
r th
erap
y at
tim
e of
stu
dy
Excl
usio
n cr
iteria
: Non
e st
ated
Mea
n ag
e: 6
4.1
year
s (r
ange
41–
84)
50%
mal
e
Stro
ke d
etai
ls: F
irst
stro
ke o
nly,
20%
right
hem
ipar
esis,
% is
chae
mic
stro
ke n
ot s
tate
d
Mea
n tim
e sin
ce s
trok
e: 6
mon
ths,
(ran
ge 3
–9)
Mea
n FM
sco
re p
re-in
terv
entio
n:O
vera
ll 39
.9 (S
D 1
2.5)
, int
erve
ntio
n34
.4 (S
D 7
.6),
cont
rol 4
5.4
(SD
14.
0)
Expe
rimen
tal g
roup
: con
stra
int-
indu
ced
mov
emen
t th
erap
y in
whi
ch le
ss a
ffect
ed h
and
was
pla
ced
in a
mitt
en. M
itten
wor
n fo
rap
prox
. 90%
of w
akin
g ho
urs
Con
stra
int-
indu
ced
mov
emen
tth
erap
y tr
aini
ng s
essio
ns a
tten
ded
5da
ys p
er w
eek
for
up t
o 6
hour
spe
r da
y fo
r 2
cons
ecut
ive
wee
ks.
Shap
ing,
or
adap
tive
task
pra
ctic
ean
d re
petit
ive
task
pra
ctic
ete
chni
ques
use
d du
ring
trai
ning
sess
ions
. All
trai
ning
was
one
-on-
one
with
reh
abili
tatio
n sp
ecia
list
Com
paris
on g
roup
: Del
ayed
gro
upsc
hedu
led
to r
ecei
ve c
onst
rain
t-in
duce
d m
ovem
ent
ther
apy
1 ye
arla
ter.
Dur
ing
inte
rven
tion
perio
ddi
d no
t pa
rtic
ipat
e in
form
alre
habi
litat
ion
prog
ram
mes
Out
com
es r
ecor
ded
pre-
and
po
st-in
terv
entio
n.
Lim
b-sp
ecifi
c fu
nctio
n:W
MFT
Mot
or im
pairm
ent:
FM (a
rm a
nd h
and
sect
ion)
Allo
catio
n co
ncea
lmen
tst
ated
, but
met
hod
uncl
ear
Blin
ded
outc
ome
asse
ssm
ent
No
loss
to
follo
w-u
p at
end
of t
reat
men
t ph
ase
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
89
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Att
eya,
200
479RC
T
Rand
omisa
tion
proc
edur
e no
tde
scrib
ed
Saud
i Ara
bia
Six
part
icip
ants
: tw
o in
terv
entio
n,tw
o tr
aditi
onal
the
rapy
, tw
o co
ntro
l
Incl
usio
n cr
iteria
: Str
oke
4w
eeks
to
6m
onth
s ag
o, a
ge 1
8–75
, disc
harg
edfr
om r
ehab
ilita
tion,
10-
degr
ee a
ctiv
eex
tens
ion
in fi
nger
s, m
otiv
ated
,w
illin
g to
follo
w in
terv
entio
ngu
idel
ines
Excl
usio
n cr
iteria
: Sig
nific
ant
cogn
itive
impa
irmen
t ha
emor
rhag
ic o
r bi
late
ral
lesio
ns, l
esio
ns in
the
prim
ary
sens
ory
or m
otor
cor
tical
are
as, s
igni
fican
tsp
astic
ity, s
igni
fican
t pa
in in
the
affe
cted
upp
er li
mb,
invo
lvem
ent
inan
y ot
her
expe
rimen
tal r
ehab
ilita
tion
or d
rug
stud
ies
Mea
n ag
e: 5
4.3
year
s (r
ange
45–
67)
50%
mal
e
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or s
ubse
quen
t st
roke
, 50%
rig
hthe
mip
ares
is, %
isch
aem
ic s
trok
e no
tst
ated
Mea
n tim
e sin
ce s
trok
e: 4
.7 m
onth
s(r
ange
2.3
–5.8
)
Mea
n am
ount
of u
se o
f affe
cted
arm
at
base
line
(mea
sure
d by
MAL
):co
nstr
aint
-indu
ced
mov
emen
tth
erap
y gr
oup
2, t
radi
tiona
l the
rapy
grou
p 1,
con
trol
gro
up 3
(5 is
hig
hest
ratin
g)
Expe
rimen
tal i
nter
vent
ion:
cons
trai
nt-in
duce
d m
ovem
ent
ther
apy
with
res
trai
nt o
f low
er a
rman
d ha
nd e
very
wee
kday
for
5ho
urs
usin
g a
cott
on B
obat
h sli
ng.
Patie
nts
part
icip
ated
in 3
0 m
inut
esof
phy
sical
the
rapy
and
30
min
utes
of o
ccup
atio
nal t
hera
py o
n an
outp
atie
nt b
asis
thre
e tim
es p
erw
eek
for
10 w
eeks
. Int
erve
ntio
nsin
clud
ed ‘s
hapi
ng’,
oper
ant
cond
ition
ing
met
hod
in w
hich
abe
havi
oura
l obj
ectiv
e is
appr
oach
edin
sm
all s
teps
of p
rogr
essiv
ely
incr
easin
g di
fficu
lty
Patie
nts
disc
harg
ed fr
omre
habi
litat
ion
Sett
ing:
Out
patie
nt c
linic
Com
paris
on g
roup
: tra
ditio
nal
ther
apy:
as
abov
e, b
ut w
ithou
tre
stra
int
Con
trol
gro
up r
ecei
ved
no t
hera
pydu
ring
10-w
eek
perio
d
Out
com
es r
ecor
ded
pre-
and
po
st-in
terv
entio
n
Lim
b-sp
ecifi
c fu
nctio
n:A
RAT,
WM
FT, M
AL
Mot
or im
pairm
ent:
FM
Allo
catio
n co
ncea
lmen
tun
clea
r
No
loss
to
follo
w-u
p at
end
of t
reat
men
t ph
ase
cont
inue
d

Appendix 2
90
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Boak
e, 2
00684
RCT
Met
hod
ofra
ndom
isatio
n no
tst
ated
USA
23 p
artic
ipan
ts: t
en in
terv
entio
n,
13 c
ontr
ol
Incl
usio
n cr
iteria
: Isc
haem
ic o
rha
emor
rhag
ic s
trok
e w
ithin
14
days
of e
nter
ing
tria
l, sc
ore
1–3
on it
em 5
(arm
mot
or) o
f the
NIH
SS, 1
0de
gree
s of
act
ive
mov
emen
t in
thum
b an
d tw
o fin
gers
of t
he a
ffect
edha
nd, t
otal
NIH
SS s
core
�14
if r
ight
-sid
ed a
nd �
19 if
left-
sided
str
oke,
abili
ty t
o pr
ovid
e in
form
ed c
onse
nt,
no p
revi
ous
stro
ke, n
o ne
glec
t or
spee
ch c
ompr
ehen
sion
that
wou
ldpr
even
t pa
rtic
ipat
ion
in s
tudy
Excl
usio
n cr
iteria
: NIH
SS a
rm m
otor
scor
e cr
iterio
n ex
clud
ed p
atie
nts
with
no
arm
mov
emen
t at
all,
or
node
tect
able
sho
ulde
r w
eakn
ess
Mea
n ag
e: 6
0.7
year
s, (r
ange
not
stat
ed)
65%
mal
e
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or s
ubse
quen
t st
roke
, 48%
rig
hthe
mip
ares
is, 7
8% is
chae
mic
str
oke
Mea
n tim
e sin
ce s
trok
e: w
ithin
14da
ys
Mea
n N
IHSS
tot
al s
core
at
base
line:
CIM
T g
roup
4.9
(SD
1.8
), tr
aditi
onal
grou
p 5.
3 (S
D 3
.4)
Expe
rimen
tal i
nter
vent
ion:
CIM
T fo
rup
to
3 ho
urs
per
day,
for
14–1
5da
ys a
t a
freq
uenc
y of
6 d
ays
per
wee
k, e
xclu
ding
Sun
days
.In
terv
entio
ns in
clud
ed p
erfo
rmin
gta
sks
with
the
affe
cted
upp
erex
trem
ity in
clud
ing
reac
hing
,gr
aspi
ng, l
iftin
g an
d pl
acin
g. T
ask
diffi
culty
pro
gres
sivel
y in
crea
sed
usin
g be
havi
oura
l tec
hniq
ues
ofsh
apin
g an
d su
cces
sive
appr
oxim
atio
n. P
artic
ipan
ts w
ore
mitt
en o
n un
affe
cted
han
d fo
r 90
%of
wak
ing
hour
s
Inte
rven
tion
deliv
ered
by
licen
sed
ther
apist
s an
d th
erap
y as
sista
nts
incl
udin
g oc
cupa
tiona
l and
phy
sical
ther
apist
s
Gro
up s
ize
not
stat
ed
Sett
ing:
inpa
tient
reh
abili
tatio
n un
itan
d ou
tpat
ient
reh
abili
tatio
n cl
inic
Out
com
es r
ecor
ded
post
-tre
atm
ent
and
3–4
mon
ths
afte
r st
roke
Lim
b-sp
ecifi
c fu
nctio
n:G
roov
ed P
egbo
ard
Test
,M
AL
Mot
or im
pairm
ent:
FM
Stat
es r
ando
m a
lloca
tion,
but
no d
escr
iptio
n of
proc
edur
e gi
ven
Blin
ded
outc
ome
asse
ssor
s
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
91
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Dro
mer
ick,
200
081Pi
lot
RCT
Tabl
e of
ran
dom
num
bers
USA
23 p
artic
ipan
ts: 1
1 in
terv
entio
n, n
ine
cont
rol
Patie
nts
recr
uite
d fr
om in
patie
ntfa
cilit
y
Incl
usio
n cr
iteria
: Adm
issio
n to
inpa
tient
reh
abili
tatio
n w
ithin
14
days
of is
chae
mic
str
oke,
per
siste
nthe
mip
ares
is le
adin
g to
impa
ired
uppe
r ex
trem
ity fu
nctio
n as
indi
cate
dby
sco
re o
f 1–2
on
NIH
SS, e
vide
nce
of p
rese
rved
cog
nitiv
e fu
nctio
n as
indi
cate
d by
0–1
on
the
cons
ciou
snes
s, c
omm
unic
atio
n an
dne
glec
t ite
ms
of t
he N
IHSS
, pre
senc
eof
pro
tect
ive
resp
onse
, no
uppe
rex
trem
ity in
jury
or
cond
ition
s th
atlim
ited
use
befo
re s
trok
e
Excl
usio
n cr
iterio
n: H
aem
orrh
agic
stro
ke
Mea
n ag
e: 6
6.0
year
s (r
ange
47–
83)
55%
mal
e
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or s
ubse
quen
t st
roke
, 69.
6% r
ight
hem
ipar
esis,
100
% is
chae
mic
str
oke
Mea
n tim
e sin
ce s
trok
e: N
ot s
tate
d,bu
t al
l par
ticip
ants
with
in 1
4 da
ys o
fst
roke
NIH
SS s
core
at
base
line:
Inte
rven
tion
10.2
±9.
4, c
ontr
ol 7
.5 ±
2.8
Expe
rimen
tal i
nter
vent
ion:
CIM
Tin
volv
ing
wea
ring
padd
ed m
itten
for
at le
ast
6 ho
urs
per
day
durin
g14
-day
tre
atm
ent
perio
d, w
ith20
hour
s’ t
rain
ing.
Inte
rven
tions
incl
uded
occ
upat
iona
l the
rapy
trea
tmen
t fo
cuse
d on
AD
Ls, u
pper
extr
emity
tra
inin
g an
d C
IMT
circ
uit
trai
ning
Trea
tmen
t su
perv
ised
byoc
cupa
tiona
l the
rapi
st in
bot
hgr
oups
Gro
up s
ize
not
stat
ed
Sett
ing:
Inpa
tient
Com
paris
on g
roup
: Sta
ndar
doc
cupa
tiona
l the
rapy
tre
atm
ent
incl
udin
g co
mpe
nsat
ory
tech
niqu
esfo
r A
DLs
, upp
er e
xtre
mity
stre
ngth
, ran
ge o
f mot
ion
and
posit
ioni
ng
Part
icip
ants
rec
eive
d eq
uiva
lent
time
and
inte
nsity
of t
reat
men
tdi
rect
ly s
uper
vise
d by
occ
upat
iona
lth
erap
ist
Out
com
es r
ecor
ded
pre-
and
po
st-in
terv
entio
n
Lim
b-sp
ecifi
c fu
nctio
n:A
RAT
Glo
bal A
DL:
BI,
FIM
Att
empt
at
conc
ealm
ent,
but
real
cha
nce
ofdi
sclo
sure
of a
ssig
nmen
tbe
fore
form
al e
ntry
Blin
ded
outc
ome
asse
ssm
ent
Loss
to
follo
w-u
p: 1
3%(n
=3)
cont
inue
d

Appendix 2
92
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Page
, 200
180RC
T
Rand
omisa
tion
proc
edur
e no
tde
scrib
ed
USA
Six
part
icip
ants
: tw
o in
terv
entio
n,tw
o tr
aditi
onal
reh
abili
tatio
n, t
wo
cont
rol
Incl
usio
n cr
iteria
: Str
oke
expe
rienc
edbe
twee
n 4
wee
ks a
nd 6
mon
ths
befo
re s
tudy
enr
olm
ent,
scor
e of
70
or h
ighe
r on
Mod
ified
MM
SE, n
oha
emor
rhag
ic o
r bi
late
ral l
esio
ns o
rle
sions
in t
he p
rimar
y se
nsor
y or
mot
or c
ortic
al a
reas
, age
18–
95, n
oex
cess
ive
spas
ticity
, no
exce
ssiv
e pa
inin
the
affe
cted
upp
er li
mb,
com
plet
ely
disc
harg
ed fr
om a
ll fo
rms
of p
hysic
al r
ehab
ilita
tion,
not
part
icip
atin
g in
any
exp
erim
enta
lre
habi
litat
ion
or d
rug
stud
ies
Excl
usio
n cr
iteria
: Non
e st
ated
Mea
n ag
e: 5
5.8
year
s (r
ange
44–
77)
50%
mal
e
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or s
ubse
quen
t st
roke
, 66.
7% r
ight
hem
ipar
esis,
% is
chae
mic
str
oke
not
stat
ed
Mea
n tim
e sin
ce s
trok
e: 4
.6 m
onth
s(r
ange
2–5
.5)
Mea
n FM
sco
res
pre-
inte
rven
tion:
Inte
rven
tion
40 (S
D 7
), tr
aditi
onal
reha
bilit
atio
n 56
.5 (S
D 3
.5),
cont
rol
58.5
(SD
3.5
)
Expe
rimen
tal i
nter
vent
ion:
mC
IMT
com
prisi
ng 3
0 m
inut
es o
f phy
sical
ther
apy
and
30 m
inut
es o
foc
cupa
tiona
l the
rapy
thr
ee t
imes
per
wee
k fo
r 10
wee
ks. 8
0% o
fea
ch p
hysic
al a
nd o
ccup
atio
nth
erap
y se
ssio
n fo
cuse
d on
neur
omus
cula
r fa
cilit
atio
nte
chni
ques
, with
em
phas
is on
AD
Lta
sks
whe
neve
r po
ssib
le, a
nd 2
0%fo
cuse
d on
com
pens
ator
yte
chni
ques
usin
g th
e un
affe
cted
side
(i.e.
rea
chin
g an
d pe
rfor
min
gta
sks
with
una
ffect
ed a
rm).
Low
erar
ms
and
hand
s re
stra
ined
for
5ho
urs
initi
ally
usin
g co
tton
Bob
ath
sling
Gro
up s
ize
not
stat
ed
Sett
ing:
Out
patie
nt
Com
paris
on g
roup
: Tra
ditio
nal
reha
bilit
atio
n gr
oup
rece
ived
the
abov
e w
ith n
o re
stra
int.
Con
trol
grou
p re
ceiv
ed n
o th
erap
y du
ring
the
sam
e 10
-wee
k pe
riod
Out
com
es r
ecor
ded
pre-
and
po
st-in
terv
entio
n
Lim
b-sp
ecifi
c fu
nctio
n:A
RAT,
WM
FT, M
AL
Mot
or im
pairm
ent:
FM
Stat
es r
ando
m a
lloca
tion
but
no d
escr
iptio
n of
proc
edur
e gi
ven
Blin
ded
outc
ome
asse
ssm
ent
No
loss
to
follo
w-u
p
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
93
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Page
, 200
261RC
T
Rand
omisa
tion
proc
edur
e no
tde
scrib
ed
USA
14 p
artic
ipan
ts: f
our
inte
rven
tion,
five
trad
ition
al r
ehab
ilita
tion,
five
con
trol
Incl
usio
n cr
iteria
: Str
oke
betw
een
4w
eeks
and
6 m
onth
s be
fore
stu
dyen
rolm
ent,
10-d
egre
e fin
ger
exte
nsio
n, a
nd 2
0 de
gree
s at
the
wris
t, sc
ore
of 7
0 or
hig
her
onM
odifi
ed M
MSE
, no
haem
orrh
agic
or
bila
tera
l les
ions
or
lesio
ns in
the
prim
ary
sens
ory
or m
otor
cor
tical
area
s, a
ge 1
8–95
, no
exce
ssiv
esp
astic
ity, n
o ex
cess
ive
pain
in m
ore
affe
cted
upp
er li
mb,
disc
harg
ed fr
omal
l for
ms
of r
ehab
ilita
tion,
not
part
icip
atin
g in
any
exp
erim
enta
lre
habi
litat
ion
or d
rug
stud
ies
Excl
usio
n cr
iteria
: Non
e st
ated
Mea
n ag
e: 6
4.8
year
s (r
ange
45–
83)
64%
mal
e
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or s
ubse
quen
t st
roke
, 42.
9% r
ight
hem
ipar
esis,
% is
chae
mic
str
oke
not
stat
ed
Mea
n tim
e sin
ce s
trok
e: 4
.4 m
onth
s(r
ange
4–6
)
Mea
n FM
sco
re a
t ba
selin
e: m
CIM
T31
.0, t
radi
tiona
l reh
abili
tatio
n 51
.4,
cont
rol 3
7.0
Expe
rimen
tal i
nter
vent
ion:
mC
IMT
cons
istin
g of
par
ticip
atio
n in
30
min
utes
of p
hysio
ther
apy
and
30 m
inut
es o
f occ
upat
iona
l the
rapy
thre
e tim
es p
er w
eek
for
10w
eeks
. Int
erve
ntio
n in
clud
ed P
Tco
ncen
trat
ion
on a
ffect
ed u
pper
limb
stre
tchi
ng, d
ynam
icst
and/
bala
nce
activ
ities
and
gai
ttr
aini
ng. ‘
Shap
ing’
tec
hniq
ues
appl
ied.
Les
s af
fect
ed li
mb
rest
rain
ed e
very
wee
kday
for
5-ho
ur p
erio
d
Gro
up s
ize
not
stat
ed
Sett
ing:
Sub
acut
e ou
tpat
ient
clin
ic
Com
paris
on g
roup
s:
(1) T
radi
tiona
l reh
abili
tatio
npa
rtic
ipan
ts r
ecei
ved
the
sam
eam
ount
of o
ccup
atio
nal a
ndph
ysic
al t
hera
py s
essio
ns; t
reat
edac
cord
ing
to n
euro
mus
cula
rfa
cilit
atio
n pr
inci
ples
with
som
eco
mpe
nsat
ory
tech
niqu
es t
augh
t(2
) Con
trol
par
ticip
ants
did
not
part
icip
ate
in a
ny in
terv
entio
ns fo
rth
e 10
-wee
k pe
riod
Out
com
es r
ecor
ded
pre-
and
po
st-in
terv
entio
n
Lim
b-sp
ecifi
c fu
nctio
n:A
RAT,
MA
L
Mot
or im
pairm
ent:
FM
Stat
es r
ando
m a
lloca
tion,
but
no d
escr
iptio
n of
proc
edur
e gi
ven
Blin
ded
outc
ome
asse
ssm
ent
No
loss
to
follo
w-u
p
cont
inue
d
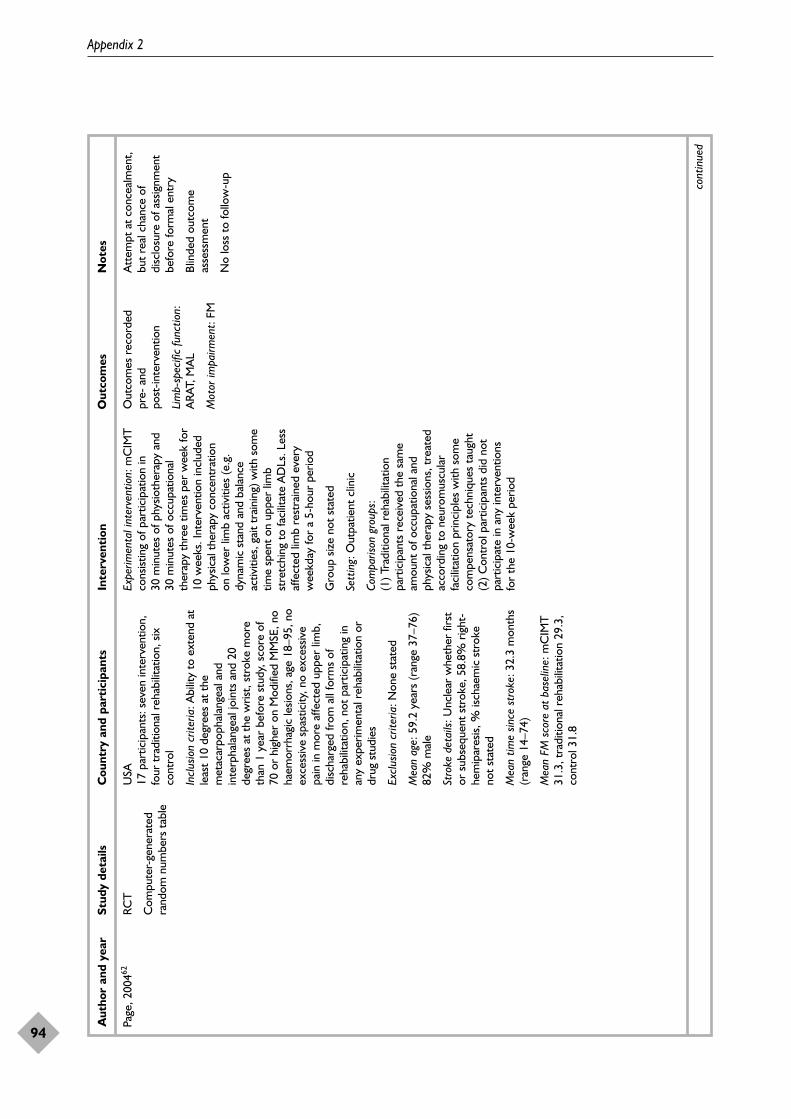
Appendix 2
94
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Page
, 200
462RC
T
Com
pute
r-ge
nera
ted
rand
om n
umbe
rs t
able
USA
17 p
artic
ipan
ts: s
even
inte
rven
tion,
four
tra
ditio
nal r
ehab
ilita
tion,
six
cont
rol
Incl
usio
n cr
iteria
: Abi
lity
to e
xten
d at
leas
t 10
deg
rees
at
the
met
acar
poph
alan
geal
and
inte
rpha
lang
eal j
oint
s an
d 20
degr
ees
at t
he w
rist,
stro
ke m
ore
than
1 y
ear
befo
re s
tudy
, sco
re o
f70
or
high
er o
n M
odifi
ed M
MSE
, no
haem
orrh
agic
lesio
ns, a
ge 1
8–95
, no
exce
ssiv
e sp
astic
ity, n
o ex
cess
ive
pain
in m
ore
affe
cted
upp
er li
mb,
disc
harg
ed fr
om a
ll fo
rms
ofre
habi
litat
ion,
not
par
ticip
atin
g in
any
expe
rimen
tal r
ehab
ilita
tion
ordr
ug s
tudi
es
Excl
usio
n cr
iteria
: Non
e st
ated
Mea
n ag
e: 5
9.2
year
s (r
ange
37–
76)
82%
mal
e
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or s
ubse
quen
t st
roke
, 58.
8% r
ight
-he
mip
ares
is, %
isch
aem
ic s
trok
eno
t st
ated
Mea
n tim
e sin
ce s
trok
e: 3
2.3
mon
ths
(ran
ge 1
4–74
)
Mea
n FM
sco
re a
t ba
selin
e: m
CIM
T31
.3, t
radi
tiona
l reh
abili
tatio
n 29
.3,
cont
rol 3
1.8
Expe
rimen
tal i
nter
vent
ion:
mC
IMT
cons
istin
g of
par
ticip
atio
n in
30
min
utes
of p
hysio
ther
apy
and
30 m
inut
es o
f occ
upat
iona
lth
erap
y th
ree
times
per
wee
k fo
r10
wee
ks. I
nter
vent
ion
incl
uded
phys
ical
the
rapy
con
cent
ratio
non
low
er li
mb
activ
ities
(e.g
.dy
nam
ic s
tand
and
bal
ance
activ
ities
, gai
t tr
aini
ng) w
ith s
ome
time
spen
t on
upp
er li
mb
stre
tchi
ng t
o fa
cilit
ate
AD
Ls. L
ess
affe
cted
lim
b re
stra
ined
eve
ryw
eekd
ay fo
r a
5-ho
ur p
erio
d
Gro
up s
ize
not
stat
ed
Sett
ing:
Out
patie
nt c
linic
Com
paris
on g
roup
s:(1
) Tra
ditio
nal r
ehab
ilita
tion
part
icip
ants
rec
eive
d th
e sa
me
amou
nt o
f occ
upat
iona
l and
phys
ical
the
rapy
ses
sions
, tre
ated
acco
rdin
g to
neu
rom
uscu
lar
faci
litat
ion
prin
cipl
es w
ith s
ome
com
pens
ator
y te
chni
ques
tau
ght
(2) C
ontr
ol p
artic
ipan
ts d
id n
otpa
rtic
ipat
e in
any
inte
rven
tions
for
the
10-w
eek
perio
d
Out
com
es r
ecor
ded
pre-
and
po
st-in
terv
entio
n
Lim
b-sp
ecifi
c fu
nctio
n:A
RAT,
MA
L
Mot
or im
pairm
ent:
FM
Att
empt
at
conc
ealm
ent,
but
real
cha
nce
ofdi
sclo
sure
of a
ssig
nmen
tbe
fore
form
al e
ntry
Blin
ded
outc
ome
asse
ssm
ent
No
loss
to
follo
w-u
p
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
95
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Page
, 200
582RC
T
Rand
om n
umbe
rs t
able
USA
Ten
part
icip
ants
: fiv
e in
terv
entio
ngr
oup,
five
tra
ditio
nal r
ehab
ilita
tion
Incl
usio
n cr
iteria
: 10-
degr
ee fi
nger
exte
nsio
n, a
nd 2
0 de
gree
s at
the
wris
t, isc
haem
ic s
trok
e fe
wer
tha
n14
day
s be
fore
stu
dy e
nrol
men
t,sc
ore
of 7
0 or
hig
her
on M
odifi
edM
MSE
, age
18–
95, n
o ex
cess
ive
spas
ticity
, no
exce
ssiv
e pa
in in
mor
eaf
fect
ed u
pper
lim
b, m
ore
affe
cted
limb
non-
use
(am
ount
of u
se s
core
of <
2.5
on M
AL)
, disc
harg
ed fr
omal
l for
ms
of r
ehab
ilita
tion,
not
part
icip
atin
g in
any
exp
erim
enta
lre
habi
litat
ion
or d
rug
stud
ies
Excl
usio
n cr
iteria
: Non
e st
ated
Mea
n ag
e: 6
0.4
year
s (r
ange
46–
72)
80%
mal
e
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or s
ubse
quen
t st
roke
, 80%
rig
hthe
mip
ares
is, 1
00%
isch
aem
ic s
trok
e
Mea
n tim
e sin
ce s
trok
e: 4
.4 d
ays
(ran
ge 2
–9)
Mea
n FM
sco
re a
t ba
selin
e: m
CIM
T33
.6, t
radi
tiona
l reh
abili
tatio
n 34
.8
Expe
rimen
tal i
nter
vent
ion:
mC
IMT
cons
istin
g of
par
ticip
atio
n in
30m
inut
es o
f phy
sioth
erap
y an
d30
min
utes
of o
ccup
atio
nal
ther
apy
thre
e tim
es p
er w
eek
for
10w
eeks
, all
adm
inist
ered
by
the
sam
e th
erap
ist. I
nter
vent
ion
incl
uded
con
cent
ratio
n on
mor
eaf
fect
ed li
mb
use
in t
hree
AD
Lsch
osen
by
part
icip
ant
and
ther
apist
(app
rox.
25
min
utes
); 5
min
utes
of t
hera
py s
pent
on
affe
cted
lim
b ra
nge
of m
otio
n.‘S
hapi
ng’ t
echn
ique
s us
ed w
ithth
ree
AD
Ls. L
ess
affe
cted
lim
bre
stra
ined
eve
ry w
eekd
ay fo
r a
5-ho
ur p
erio
d
Gro
up s
ize
not
stat
ed
Sett
ing:
Reh
abili
tatio
n ho
spita
l
Com
paris
on g
roup
: Tra
ditio
nal
reha
bilit
atio
n gr
oup
rece
ived
stan
dard
the
rapy
for
30 m
inut
es3
days
a w
eek
for
10 w
eeks
.Se
ssio
ns in
clud
ed s
tret
chin
g of
the
affe
cted
lim
b, w
eigh
t be
arin
g w
ithth
e af
fect
ed li
mb
and
man
ual
dext
erity
exe
rcise
s
Out
com
es r
ecor
ded
pre-
and
po
st-in
terv
entio
n
Lim
b-sp
ecifi
c fu
nctio
n:A
RAT,
MA
L
Mot
or im
pairm
ent:
FM
Att
empt
at
conc
ealm
ent,
but
real
cha
nce
ofdi
sclo
sure
of a
ssig
nmen
tbe
fore
form
al e
ntry
Blin
ded
outc
ome
asse
ssm
ent
No
loss
to
follo
w-u
p
cont
inue
d
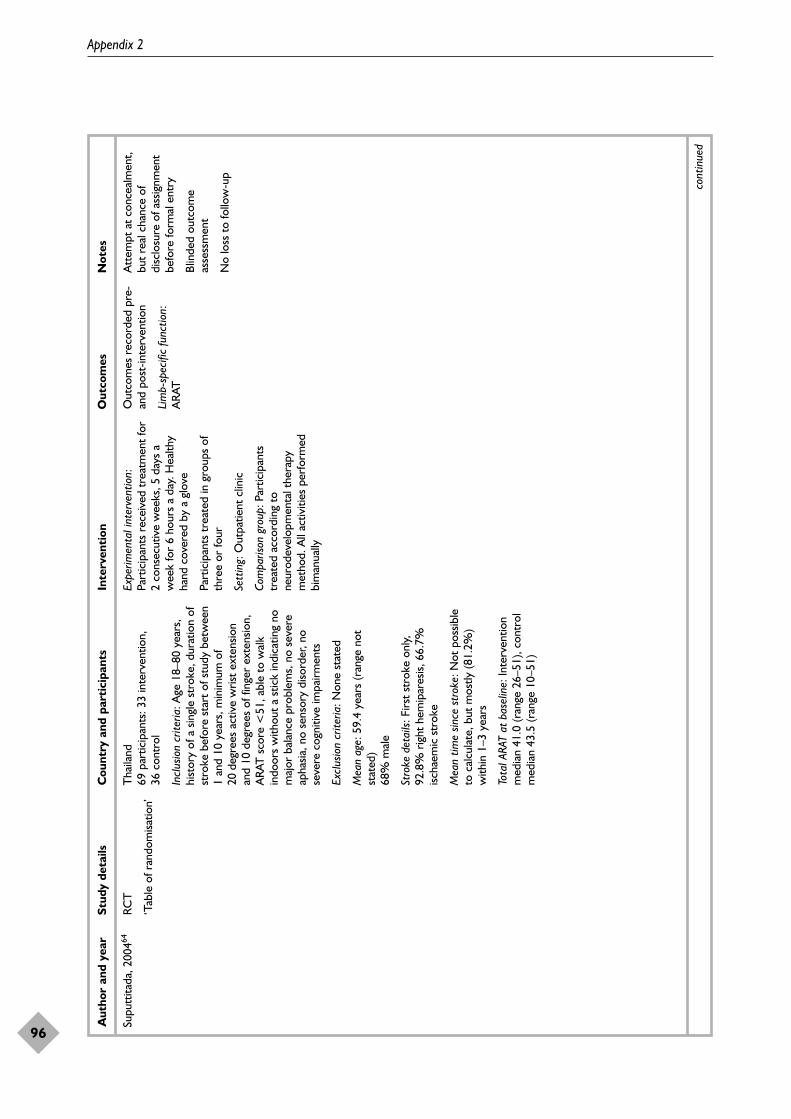
Appendix 2
96
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Supu
ttita
da, 2
00464
RCT
‘Tab
le o
f ran
dom
isatio
n’
Tha
iland
69 p
artic
ipan
ts: 3
3 in
terv
entio
n,
36 c
ontr
ol
Incl
usio
n cr
iteria
: Age
18–
80 y
ears
,hi
stor
y of
a s
ingl
e st
roke
, dur
atio
n of
stro
ke b
efor
e st
art
of s
tudy
bet
wee
n1
and
10 y
ears
, min
imum
of
20de
gree
s ac
tive
wris
t ex
tens
ion
and
10 d
egre
es o
f fin
ger
exte
nsio
n,A
RAT
sco
re <
51, a
ble
to w
alk
indo
ors
with
out
a st
ick
indi
catin
g no
maj
or b
alan
ce p
robl
ems,
no
seve
reap
hasia
, no
sens
ory
diso
rder
, no
seve
re c
ogni
tive
impa
irmen
ts
Excl
usio
n cr
iteria
: Non
e st
ated
Mea
n ag
e: 5
9.4
year
s (r
ange
not
stat
ed)
68%
mal
e
Stro
ke d
etai
ls: F
irst
stro
ke o
nly,
92.8
% r
ight
hem
ipar
esis,
66.
7%isc
haem
ic s
trok
e
Mea
n tim
e sin
ce s
trok
e: N
ot p
ossib
leto
cal
cula
te, b
ut m
ostly
(81.
2%)
with
in 1
–3 y
ears
Tota
l ARA
T at
bas
elin
e: In
terv
entio
nm
edia
n 41
.0 (r
ange
26–
51),
cont
rol
med
ian
43.5
(ran
ge 1
0–51
)
Expe
rimen
tal i
nter
vent
ion:
Part
icip
ants
rec
eive
d tr
eatm
ent
for
2 co
nsec
utiv
e w
eeks
, 5 d
ays
aw
eek
for
6 ho
urs
a da
y. H
ealth
yha
nd c
over
ed b
y a
glov
e
Part
icip
ants
tre
ated
in g
roup
s of
thre
e or
four
Sett
ing:
Out
patie
nt c
linic
Com
paris
on g
roup
: Par
ticip
ants
trea
ted
acco
rdin
g to
neur
odev
elop
men
tal t
hera
pym
etho
d. A
ll ac
tiviti
es p
erfo
rmed
bim
anua
lly
Out
com
es r
ecor
ded
pre-
and
post
-inte
rven
tion
Lim
b-sp
ecifi
c fu
nctio
n:A
RAT
Att
empt
at
conc
ealm
ent,
but
real
cha
nce
ofdi
sclo
sure
of a
ssig
nmen
tbe
fore
form
al e
ntry
Blin
ded
outc
ome
asse
ssm
ent
No
loss
to
follo
w-u
p
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
97
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Taub
, 199
373RC
T
Rand
omisa
tion
proc
edur
e no
tde
scrib
ed
USA
Nin
e pa
rtic
ipan
ts: f
our
inte
rven
tion,
five
cont
rol
Incl
usio
n cr
iteria
(ex
pres
sed
asex
clus
ion
crite
ria b
y au
thor
s): S
trok
eex
perie
nced
mor
e th
an 1
yea
r ag
o,10
-deg
ree
finge
r ex
tens
ion
and
20de
gree
s at
the
wris
t, no
bal
ance
prob
lem
s, in
abili
ty t
o m
ake
exte
nsiv
e us
e of
invo
lved
upp
erex
trem
ity s
o th
at s
igni
fican
t fu
rthe
rim
prov
emen
t co
uld
not
beex
pect
ed, n
o se
rious
cog
nitiv
ede
ficits
, no
exce
ssiv
e sp
astic
ity, n
ose
rious
unc
ontr
olle
d m
edic
alpr
oble
ms,
less
tha
n 75
yea
rs o
f age
,no
left
arm
dom
inan
ce o
r le
fthe
mip
legi
a
Age:
inte
rven
tion
med
ian
65ye
ars,
com
paris
on m
edia
n 63
year
s22
% m
ale
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or s
ubse
quen
t st
roke
, 100
% r
ight
hem
ipar
esis,
% is
chae
mic
str
oke
not
stat
ed
Mea
n tim
e sin
ce s
trok
e: N
ot s
tate
d(r
ange
1.2
–18
year
s)
Mea
n fu
nctio
nal a
bilit
y on
Em
ory
test
at b
asel
ine:
Inte
rven
tion
3.2
(est
imat
ed),
cont
rol 3
.3 (e
stim
ated
)
Expe
rimen
tal i
nter
vent
ion:
Una
ffect
ed a
rm s
ecur
ed in
res
ting
hand
spl
int
and
sling
; res
trai
ntde
vice
wor
n fo
r 14
day
s fo
r w
ell
over
90%
of w
akin
g ho
urs.
One
each
wee
kday
, pat
ient
s sp
ent
7ho
urs
at r
ehab
ilita
tion
cent
re a
ndw
ere
give
n a
varie
ty o
f tas
ks, e
.g.
thro
win
g a
ball,
pla
ying
dom
inoe
s,pu
shin
g a
broo
m
No
deta
ils g
iven
of i
nter
vent
ion
prov
ider
s
Gro
up s
ize
not
stat
ed
Sett
ing:
Reh
abili
tatio
n ce
ntre
Com
paris
on g
roup
: Att
entio
nco
ntro
l: pr
oced
ures
des
igne
d to
focu
s at
tent
ion
on t
he in
volv
edex
trem
ity, b
ut in
volv
ed li
mb
not
give
n an
y ex
perie
nce
of o
r tr
aini
ngfo
r ac
tive
mov
emen
t
Out
com
es r
ecor
ded
pre-
and
post
-inte
rven
tion
Lim
b-sp
ecifi
c fu
nctio
n:Em
ory
Mot
or F
unct
ion
Test
, Arm
Mot
or A
ctiv
ityTe
st, M
AL
Stat
es r
ando
m a
lloca
tion,
but
no d
escr
iptio
n of
proc
edur
e gi
ven
No
men
tion
of b
linde
dou
tcom
e as
sess
men
t
No
loss
to
follo
w-u
p
cont
inue
d

Appendix 2
98
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Witt
enbe
rg, 2
00374
RCT
Rand
om n
umbe
rs t
able
.Ra
ndom
isatio
npe
rfor
med
in p
airs
, if
poss
ible
, or
inin
divi
dual
s, b
ut n
ever
mor
e th
an t
wo
subj
ects
rece
ivin
g in
terv
entio
n.Bo
th m
embe
rs o
f pai
ras
signe
d to
sam
e ar
mto
avo
id s
ubje
cts
obse
rvin
g th
erap
y in
othe
r ar
m
USA
16 p
artic
ipan
ts: n
ine
inte
rven
tion,
seve
n co
ntro
l
Incl
usio
n cr
iteria
: Sin
gle,
sub
cort
ical
infa
rctio
n m
ore
than
12
mon
ths
befo
re e
ntry
to
the
stud
y, s
igni
fican
tfu
nctio
nal i
mpa
irmen
t of
the
affe
cted
side
(indi
cate
d by
a s
core
of <
2.7
onth
e M
AL)
, vol
unta
ry e
xten
sion
of a
tle
ast
10 d
egre
es o
f the
affe
cted
finge
rs a
nd 2
0 de
gree
s of
the
wris
t
Excl
usio
n cr
iteria
: Pat
ient
s w
ithou
tvo
lunt
ary
exte
nsio
n of
at
leas
t10
degr
ees
of t
he a
ffect
ed fi
nger
s or
20 d
egre
es o
f the
wris
t
Mea
n ag
e: 6
4 ye
ars
(ran
ge 4
1–81
)81
% m
ale
Stro
ke d
etai
ls: F
irst
stro
ke o
nly,
%rig
ht h
emip
ares
is no
t st
ated
, 12.
5%ha
d in
farc
ts a
ffect
ing
non-
dom
inan
tsid
e, %
isch
aem
ic s
trok
e no
t st
ated
Mea
n tim
e sin
ce s
trok
e: 3
3 m
onth
s(r
ange
12–
86)
WM
FT a
t ba
selin
e: in
terv
entio
n 6.
7(S
D 2
.0),
cont
rol 5
.5 (S
D 2
.6)
Expe
rimen
tal i
nter
vent
ion:
Res
trai
ntof
the
upp
er e
xtre
mity
dur
ing
wak
ing
hour
s an
d ta
sk-o
rient
ated
ther
apy
of t
he a
ffect
ed u
pper
extr
emity
on
10 c
ontin
uous
inpa
tient
day
s fo
r 6
hour
s a
day
(4ho
urs
a da
y on
wee
kend
s).
The
rapy
invo
lved
pro
gres
sivel
yim
prov
ing
mot
or t
ask
perf
orm
ance
by a
suc
cess
ive
appr
oxim
atio
npr
oced
ure
durin
g co
mbi
ned
phys
ical
, occ
upat
iona
l and
recr
eatio
nal t
hera
pyN
o de
tails
giv
en o
f int
erve
ntio
npr
ovid
ers
Gro
up s
ize
not
stat
ed
Sett
ing:
Clin
ical
cen
tre
Com
paris
on g
roup
: Des
igne
d to
be
less
inte
nse
(3 h
ours
a d
ay o
nw
eekd
ays
and
no t
reat
men
t on
wee
kend
s), b
ut a
lso a
imed
to
impr
ove
task
per
form
ance
with
the
unaf
fect
ed s
ide
Out
com
es r
ecor
ded
pre-
and
post
-inte
rven
tion
and
at 6
mon
ths
post
-inte
rven
tion
Lim
b-sp
ecifi
c fu
nctio
n:W
MFT
, MA
L
Mot
or im
pairm
ent:
Ass
essm
ent
of M
otor
and
Proc
ess
Skill
s
Att
empt
at
conc
ealm
ent,
but
real
cha
nce
ofdi
sclo
sure
of a
ssig
nmen
tbe
fore
form
al e
ntry
Blin
ded
outc
ome
asse
ssm
ent
No
loss
to
follo
w-u
p
MM
SE, M
ini-M
enta
l Sta
te E
xam
inat
ion;
NIH
SS, N
atio
nal I
nstit
utes
of H
ealth
Str
oke
Scal
e.

Health Technology Assessment 2008; Vol. 12: No. 30
99
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Appendix 3
Included studies: treadmill training

Appendix 3
100
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Ada
, 200
387Ra
ndom
ised,
pla
cebo
-co
ntro
lled
clin
ical
tria
l
Part
icip
ants
ran
ked
inde
scen
ding
ord
erac
cord
ing
to w
alki
ngsp
eed
and
orga
nise
din
to c
onse
cutiv
e pa
irs.
Part
icip
ants
ran
dom
lyal
loca
ted
by c
oin
toss
Aus
tral
ia29
par
ticip
ants
: 14
inte
rven
tion,
15co
ntro
l
Volu
ntee
r sa
mpl
e re
crui
ted
via
adve
rtise
men
t an
d st
roke
clu
bs
Incl
usio
n cr
iteria
: >6
mon
ths
post
-st
roke
, <5
year
s po
st-s
trok
e, fi
rst
stro
ke, p
rese
nted
with
hem
ipar
esis,
aged
50–
85, c
an w
alk
10 m
inde
pend
ently
with
a s
peed
of
<1.
2 m
/s
Excl
usio
n cr
iteria
: Car
diov
ascu
lar
prob
lem
s th
at w
ould
pre
clud
epa
rtic
ipat
ion
in t
rain
ing,
sev
ere
cogn
itive
def
icits
suc
h th
atpa
rtic
ipan
ts c
ould
not
follo
win
stru
ctio
ns
Mea
n ag
e: 6
6 ye
ars
(SD
11)
70%
mal
e
Stro
ke d
etai
ls: F
irst
stro
ke
Tim
e sin
ce s
trok
e: E
xper
imen
tal
28m
onth
s (S
D 1
7),
cont
rol 2
6m
onth
s (S
D 2
0)
Prei
nter
vent
ion
func
tiona
l abi
lity:
Mea
n w
alki
ng s
peed
(m/s
)ex
perim
enta
l 0.6
2 (S
D 0
.24)
, co
ntro
l 0.5
3 (S
D 0
.30)
Expe
rimen
tal i
nter
vent
ion:
Tre
adm
illw
alki
ng (w
ithou
t bo
dyw
eigh
tsu
ppor
t) a
nd o
verg
roun
d w
hole
-ta
sk p
ract
ice
of w
alki
ng o
f var
ious
type
s. T
he p
ropo
rtio
n of
tre
adm
illw
alki
ng d
ecre
ased
by
10%
eac
hw
eek
from
80%
in w
eek
1 to
50%
in w
eek
4
Part
icip
ants
wer
e tr
eate
d as
outp
atie
nts
in a
com
mun
ity s
ettin
gfo
r th
ree
30-m
inut
e se
ssio
ns p
erw
eek
for
4 w
eeks
= 6
hou
rs.
Two
subj
ects
tra
ined
con
curr
ently
,w
ith t
rain
ing
prov
ided
by
aph
ysio
ther
apist
Com
paris
on g
roup
: Hom
e ex
erci
sepr
ogra
mm
e co
nsist
ing
of e
xerc
ises
to le
ngth
en/s
tren
gthe
n lo
wer
lim
bm
uscl
es, t
rain
bal
ance
and
coor
dina
tion.
Par
ticip
ants
wer
eal
so e
ncou
rage
d to
wal
k ev
ery
day.
The
aim
was
to
prov
ide
a sh
ampr
ogra
mm
e to
con
trol
for
the
effe
ct o
f pla
cebo
. Par
ticip
ants
wer
e in
stru
cted
to
carr
y ou
t th
epr
ogra
mm
e th
ree
times
a w
eek
for
4w
eeks
. Pa
rtic
ipan
ts w
ere
tele
phon
ed o
nce
a w
eek
and
exer
cise
s w
ere
prog
ress
edac
cord
ingl
y
Out
com
es r
ecor
ded
pre-
and
post
-inte
rven
tion
and
at 3
mon
ths
afte
rth
e ce
ssat
ion
ofin
terv
entio
n
Lim
b-sp
ecifi
c fu
nctio
n:10
MW
S, 6
MW
T
Mot
or im
pairm
ent:
Step
leng
th o
f bot
h th
eaf
fect
ed a
nd u
naffe
cted
leg,
cad
ence
, ste
p w
idth
over
10
m
Allo
catio
n co
ncea
lmen
tad
equa
te
No
signi
fican
t di
ffere
nces
in b
asel
ine
char
acte
ristic
s
Blin
ded
outc
ome
asse
ssm
ent
Loss
to
follo
w-u
p at
end
of t
reat
men
t ph
ase:
7%
No
inte
rven
tion-
rela
ted
with
draw
als
Att
enda
nce:
Tra
nspo
rtw
as p
rovi
ded
if ne
cess
ary.
On
aver
age,
sub
ject
s in
the
expe
rimen
tal g
roup
atte
nded
11
out
of 1
2se
ssio
ns
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
101
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Da
Cuh
na, 2
00286
RCT
pilo
t st
udy
Part
icip
ants
wer
era
ndom
ised
to g
roup
sus
ing
rand
om n
umbe
rsto
pre
assig
n pa
rtic
ipan
tsba
sed
on r
ecru
itmen
tor
der
USA
15 p
artic
ipan
ts: s
even
inte
rven
tion,
eigh
t co
ntro
l
Part
icip
ants
rec
ruite
d fr
om in
patie
ntre
habi
litat
ion
Incl
usio
n cr
iteria
: With
in 6
wee
ks o
fst
roke
, gai
t sp
eed
of 0
.6m
/s o
r le
ssan
d sc
ore
0–2
on t
he F
unct
iona
lA
mbu
latio
n ca
tego
ry, s
uffic
ient
cogn
ition
to
part
icip
ate,
abl
e to
stan
d an
d to
tak
e at
leas
t on
e st
epw
ith a
ssist
ance
, sta
ble
med
ical
cond
ition
Excl
usio
n cr
iteria
: Co-
mor
bidi
ty o
rdi
sabi
lity
that
wou
ld p
recl
ude
gait
trai
ning
, car
diac
illn
ess,
unc
ontr
olle
dhe
alth
con
ditio
n fo
r w
hich
exe
rcise
is co
ntra
indi
cate
d, e
.g. d
iabe
tes,
hype
rten
sion,
low
er e
xtre
mity
join
tdi
seas
e, b
odyw
eigh
t ov
er 1
10 k
g,co
gniti
ve im
pairm
ent,
hist
ory
ofbi
late
ral c
ereb
rova
scul
ar a
ccid
ent
Mea
n ag
e: 5
7.80
yea
rs (S
D 5
.50)
inte
rven
tion,
58.
90 (S
D 1
2.90
)co
ntro
l (no
t in
clud
ing
drop
outs
)10
0% m
ale
Stro
ke d
etai
ls: 9
2% is
chae
mic
str
oke
Tim
e sin
ce s
trok
e: E
xper
imen
tal
15.7
days
(SD
7.7
), co
ntro
l 19
days
(SD
12.
7)
Prev
entio
n fu
nctio
nal a
bilit
y: M
ean
wal
king
spe
ed (m
/s):
inte
rven
tion
0.36
(SD
0.2
5), c
ontr
ol 0
.12
(SD
0.1
5) (n
ot in
clud
ing
drop
-out
s)
Expe
rimen
tal i
nter
vent
ion:
Part
icip
ants
rec
eive
d re
gula
rre
habi
litat
ion
but
with
out
the
usua
lga
it tr
aini
ng. I
n pl
ace
of u
sual
gai
ttr
aini
ng w
as t
read
mill
tra
inin
g w
ithbo
dyw
eigh
t su
ppor
t. Pa
rtic
ipan
tsw
alke
d on
a t
read
mill
with
sup
port
usin
g a
harn
ess
of u
p to
30%
body
wei
ght.
Supp
ort
was
prog
ress
ivel
y de
crea
sed
aspa
rtic
ipan
ts a
cqui
red
grea
ter
self-
supp
ort
Part
icip
ants
wer
e tr
eate
d as
inpa
tient
s fo
r fiv
e 20
-min
ute
sess
ions
per
wee
k fo
r 3
wee
ks =
5 ho
urs.
Tra
inin
g w
as d
eliv
ered
indi
vidu
ally
by
a ph
ysio
ther
apist
Com
paris
on g
roup
: Reg
ular
reha
bilit
atio
n: d
aily
ses
sions
of
phys
ioth
erap
y, k
ines
ioth
erap
y an
doc
cupa
tiona
l the
rapy
ove
r 3
hour
s.Ph
ysio
ther
apy
focu
sed
onst
reng
then
ing,
func
tion
and
mob
ility
act
iviti
es in
clud
ing
gait
trai
ning
. Occ
upat
iona
l the
rapy
rela
ted
to A
DLs
Out
com
es r
ecor
ded
pre-
and
post
-inte
rven
tion
Lim
b-sp
ecifi
c fu
nctio
n:FA
C, f
ast
wal
king
spe
edov
er 5
m, 5
MW
T
Mot
or im
pairm
ent:
Gai
ten
ergy
exp
endi
ture
, gai
ten
ergy
cos
t
Allo
catio
n co
ncea
lmen
tun
clea
r
No
signi
fican
t di
ffere
nces
in b
asel
ine
char
acte
ristic
s
Blin
ding
of o
utco
me
asse
ssor
s no
t st
ated
Inte
rven
tion-
rela
ted
with
draw
als:
one
sub
ject
drop
ped
from
the
stu
dybe
caus
e he
did
not
com
plet
e at
leas
t ni
nese
ssio
ns
Loss
to
follo
w-u
p at
end
of
trea
tmen
t ph
ase:
13%
No
deta
ils g
iven
of
atte
ndan
ce
cont
inue
d
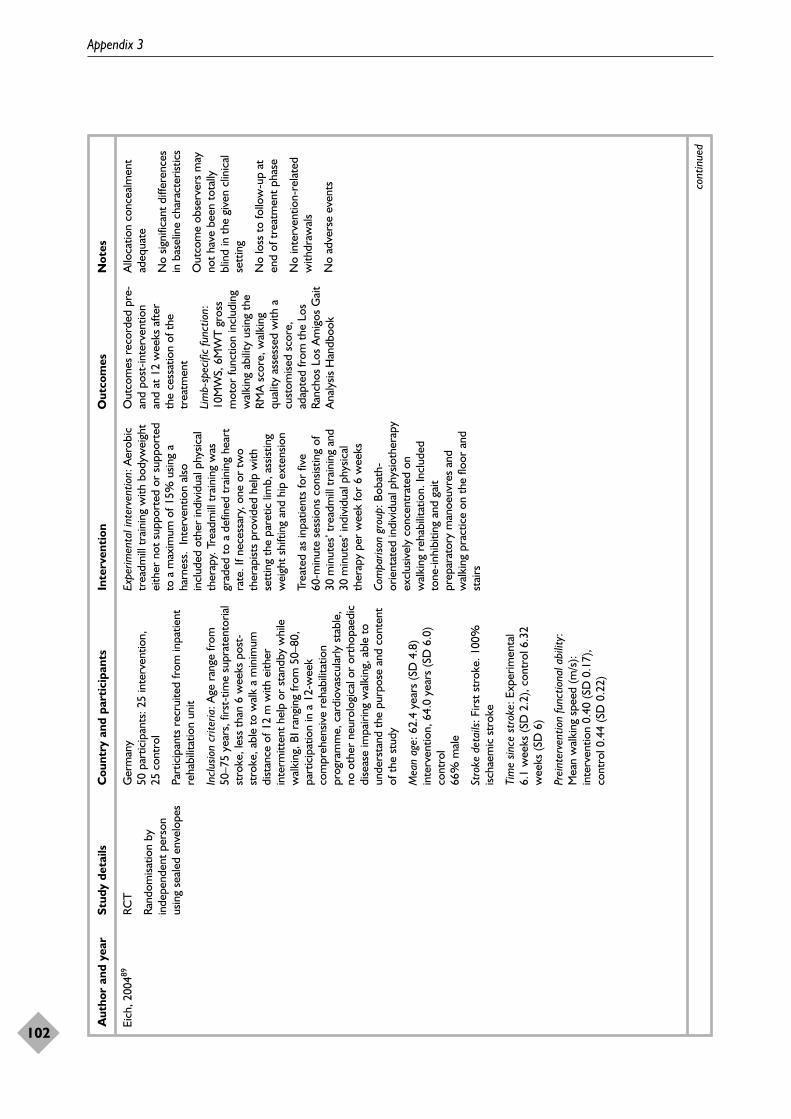
Appendix 3
102
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Eich
, 200
489RC
T
Rand
omisa
tion
byin
depe
nden
t pe
rson
usin
g se
aled
env
elop
es
Ger
man
y50
par
ticip
ants
: 25
inte
rven
tion,
25co
ntro
l
Part
icip
ants
rec
ruite
d fr
om in
patie
ntre
habi
litat
ion
unit
Incl
usio
n cr
iteria
: Age
ran
ge fr
om50
–75
year
s, fi
rst-
time
supr
aten
toria
lst
roke
, les
s th
an 6
wee
ks p
ost-
stro
ke, a
ble
to w
alk
a m
inim
umdi
stan
ce o
f 12
m w
ith e
ither
inte
rmitt
ent
help
or
stan
dby
whi
lew
alki
ng, B
I ran
ging
from
50–
80,
part
icip
atio
n in
a 1
2-w
eek
com
preh
ensiv
e re
habi
litat
ion
prog
ram
me,
car
diov
ascu
larly
sta
ble,
no o
ther
neu
rolo
gica
l or
orth
opae
dic
dise
ase
impa
iring
wal
king
, abl
e to
unde
rsta
nd t
he p
urpo
se a
nd c
onte
ntof
the
stu
dy
Mea
n ag
e: 6
2.4
year
s (S
D 4
.8)
inte
rven
tion,
64.
0 ye
ars
(SD
6.0
)co
ntro
l66
% m
ale
Stro
ke d
etai
ls: F
irst
stro
ke. 1
00%
ischa
emic
str
oke
Tim
e sin
ce s
trok
e: E
xper
imen
tal
6.1
wee
ks (S
D 2
.2),
cont
rol 6
.32
wee
ks (S
D 6
)
Prei
nter
vent
ion
func
tiona
l abi
lity:
Mea
n w
alki
ng s
peed
(m/s
):in
terv
entio
n 0.
40 (S
D 0
.17)
, co
ntro
l 0.4
4 (S
D 0
.22)
Expe
rimen
tal i
nter
vent
ion:
Aer
obic
trea
dmill
tra
inin
g w
ith b
odyw
eigh
tei
ther
not
sup
port
ed o
r su
ppor
ted
to a
max
imum
of 1
5% u
sing
aha
rnes
s. I
nter
vent
ion
also
incl
uded
oth
er in
divi
dual
phy
sical
ther
apy.
Tre
adm
ill t
rain
ing
was
grad
ed t
o a
defin
ed t
rain
ing
hear
tra
te. I
f nec
essa
ry, o
ne o
r tw
oth
erap
ists
prov
ided
hel
p w
ithse
ttin
g th
e pa
retic
lim
b, a
ssist
ing
wei
ght
shift
ing
and
hip
exte
nsio
n
Trea
ted
as in
patie
nts
for
five
60-m
inut
e se
ssio
ns c
onsis
ting
of30
min
utes
’ tre
adm
ill t
rain
ing
and
30m
inut
es’ i
ndiv
idua
l phy
sical
ther
apy
per
wee
k fo
r 6
wee
ks
Com
paris
on g
roup
: Bob
ath-
orie
ntat
ed in
divi
dual
phy
sioth
erap
yex
clus
ivel
y co
ncen
trat
ed o
nw
alki
ng r
ehab
ilita
tion.
Incl
uded
tone
-inhi
bitin
g an
d ga
itpr
epar
ator
y m
anoe
uvre
s an
dw
alki
ng p
ract
ice
on t
he fl
oor
and
stai
rs
Out
com
es r
ecor
ded
pre-
and
post
-inte
rven
tion
and
at 1
2 w
eeks
afte
rth
e ce
ssat
ion
of t
hetr
eatm
ent
Lim
b-sp
ecifi
c fu
nctio
n:10
MW
S, 6
MW
T g
ross
mot
or fu
nctio
n in
clud
ing
wal
king
abi
lity
usin
g th
eRM
A s
core
, wal
king
qual
ity a
sses
sed
with
acu
stom
ised
scor
e,ad
apte
d fr
om t
he L
osRa
ncho
s Lo
s A
mig
os G
ait
Ana
lysis
Han
dboo
k
Allo
catio
n co
ncea
lmen
tad
equa
te
No
signi
fican
t di
ffere
nces
in b
asel
ine
char
acte
ristic
s
Out
com
e ob
serv
ers
may
not
have
bee
n to
tally
blin
d in
the
giv
en c
linic
alse
ttin
g
No
loss
to
follo
w-u
p at
end
of t
reat
men
t ph
ase
No
inte
rven
tion-
rela
ted
with
draw
als
No
adve
rse
even
ts cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
103
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Mac
ko, 2
00588
RCT
Part
icip
ants
wer
era
ndom
ised
to g
roup
sus
ing
a co
mpu
ter-
base
dsy
stem
tha
t w
asst
ratif
ied
by d
efic
itse
verit
y an
d ag
e
USA
61 p
artic
ipan
ts: 3
2 in
terv
entio
n,
29 c
ontr
ol
Part
icip
ants
rec
ruite
d fr
om c
hron
icst
roke
par
ticip
ants
with
hem
ipar
etic
gait
(>6
mon
ths)
Incl
usio
n cr
iteria
: Chr
onic
hem
ipar
etic
str
oke
(mor
e th
an6
mon
ths)
, age
d 45
yea
rs o
r m
ore,
resid
ual m
ild t
o m
oder
ate
hem
iple
gic
gait
defic
its, a
chie
vem
ent
of a
dequ
ate
exer
cise
inte
nsity
with
out
signs
of m
yoca
rdia
lisc
haem
ia o
r ot
her
cont
rain
dica
tions
to t
rain
ing
Excl
usio
n cr
iteria
: Hea
rt fa
ilure
,un
stab
le a
ngin
a, p
erip
hera
l art
eria
loc
clus
ive
dise
ase,
aph
asia
, dem
entia
,un
trea
ted
maj
or d
epre
ssio
n an
dot
her
med
ical
con
ditio
ns p
recl
udin
gpa
rtic
ipat
ion
in e
xerc
ise
Mea
n ag
e: 6
3 ye
ars
(SD
10)
inte
rven
tion,
64
year
s (S
D 8
) con
trol
71%
mal
e
Stro
ke d
etai
ls: U
ncle
ar w
heth
er fi
rst
or r
ecur
rent
str
oke
Tim
e sin
ce s
trok
e: E
xper
imen
tal
grou
p 35
mon
ths
(SD
29)
, con
trol
39 m
onth
s (S
D 5
9)
Prei
nter
vent
ion
func
tiona
l abi
lity:
Mea
n w
alki
ng s
peed
(m/s
):in
terv
entio
n 0.
82 (S
D 0
.08)
, co
ntro
l 0.9
(SD
0.1
0)
Expe
rimen
tal i
nter
vent
ion:
Tre
adm
illtr
aini
ng a
t ta
rget
aer
obic
inte
nsity
of 6
0–70
% h
eart
-rat
e re
serv
e.Tr
aini
ng s
tart
ed a
t lo
w in
tens
ity(4
0–50
%) f
or 1
0–20
min
utes
and
incr
ease
d ev
ery
2 w
eeks
as
tole
rate
d. T
ask-
orie
ntat
ed t
rain
ing
adm
inist
ered
acc
ordi
ng t
o a
prog
ress
ive
aero
bic
exer
cise
form
ula.
No
body
wei
ght
supp
ort
was
pro
vide
d
Trea
ted
as o
utpa
tient
s fo
r th
ree
40-m
inut
e se
ssio
ns p
er w
eek
for
6m
onth
s
Trai
ning
was
del
iver
ed b
y ex
erci
seph
ysio
logi
sts
unde
r th
e su
perv
ision
of a
phy
sicia
n
Com
paris
on g
roup
: Mat
ched
dura
tion
expo
sure
to
staf
fim
plem
entin
g co
mm
onco
mpo
nent
s of
con
vent
iona
lth
erap
y. P
artic
ipan
ts c
ompl
eted
supe
rvise
d st
retc
hing
mov
emen
tsan
d 5
min
utes
of l
ow-in
tens
itytr
eadm
ill w
alki
ng a
t 30
–40%
hear
t-ra
te r
eser
ve w
ithou
tbo
dyw
eigh
t su
ppor
t
Out
com
es r
ecor
ded
pre-
and
post
-inte
rven
tion
Lim
b-sp
ecifi
c fu
nctio
n:W
alki
ng s
peed
ove
r30
feet
(9.1
m),
6MW
T,Ri
verm
ead
Mob
ility
Inde
x
Impa
irmen
t: W
alki
ngIm
pairm
ent
Que
stio
nnai
re. E
cono
my
of g
ait
Vo2
peak
Allo
catio
n co
ncea
lmen
tun
clea
r
No
signi
fican
t di
ffere
nces
in b
asel
ine
char
acte
ristic
s
Blin
ding
of o
utco
me
asse
ssor
s to
gro
upal
loca
tion
for
ambu
lato
rym
easu
res
and
func
tiona
lm
obili
ty. T
read
mill
exer
cise
tes
ting
not
blin
ded
Loss
to
follo
w-u
p at
end
of t
reat
men
t ph
ase:
27%
Inte
rven
tion-
rela
ted
with
draw
als:
thr
ee o
ut o
f25
sub
ject
s w
ere
lost
from
bot
h th
eex
perim
enta
l and
con
trol
grou
ps fo
r co
mpl
ianc
ere
ason
s
No
adve
rse
even
ts s
tate
d
cont
inue
d
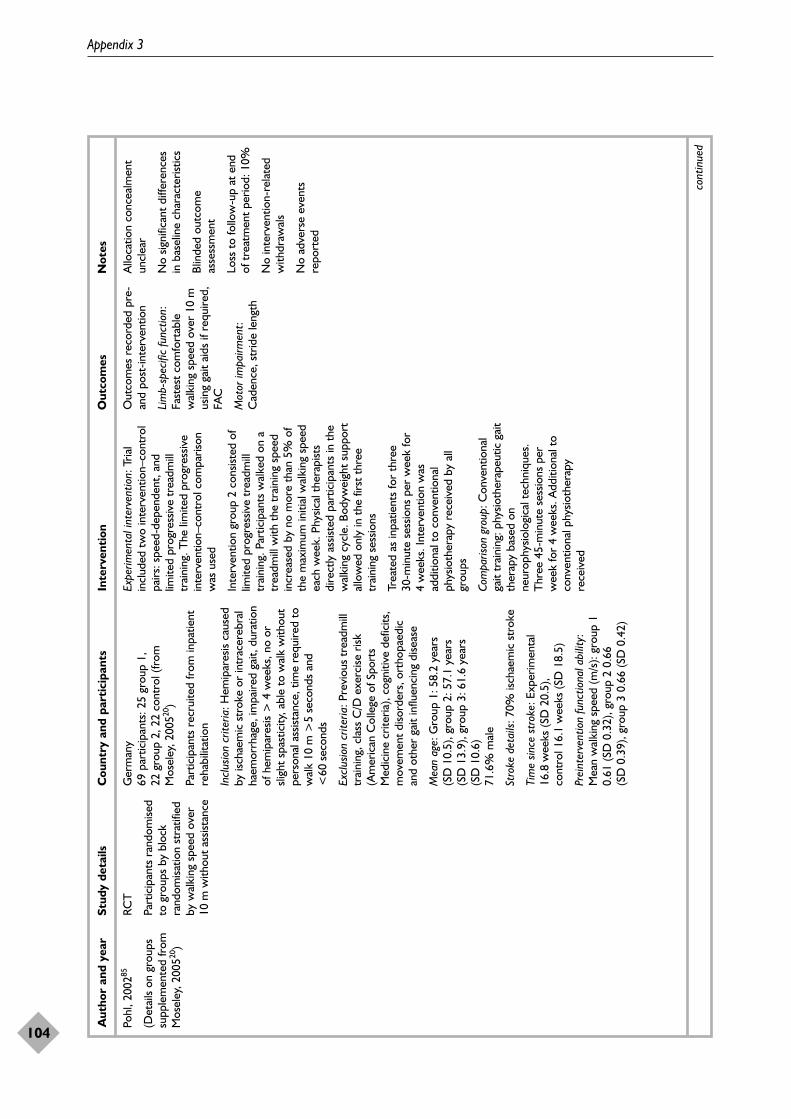
Appendix 3
104
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Pohl
, 200
285
(Det
ails
on g
roup
ssu
pple
men
ted
from
Mos
eley
, 200
520)
RCT
Part
icip
ants
ran
dom
ised
to g
roup
s by
blo
ckra
ndom
isatio
n st
ratif
ied
by w
alki
ng s
peed
ove
r10
m w
ithou
t as
sista
nce
Ger
man
y69
par
ticip
ants
: 25
grou
p 1,
22
gro
up 2
, 22
cont
rol (
from
Mos
eley
, 200
520)
Part
icip
ants
rec
ruite
d fr
om in
patie
ntre
habi
litat
ion
Incl
usio
n cr
iteria
: Hem
ipar
esis
caus
edby
isch
aem
ic s
trok
e or
intr
acer
ebra
lha
emor
rhag
e, im
paire
d ga
it, d
urat
ion
of h
emip
ares
is >
4 w
eeks
, no
orsli
ght
spas
ticity
, abl
e to
wal
k w
ithou
tpe
rson
al a
ssist
ance
, tim
e re
quire
d to
wal
k 10
m >
5 se
cond
s an
d<
60se
cond
s
Excl
usio
n cr
iteria
: Pre
viou
s tr
eadm
illtr
aini
ng, c
lass
C/D
exe
rcise
risk
(Am
eric
an C
olle
ge o
f Spo
rts
Med
icin
e cr
iteria
), co
gniti
ve d
efic
its,
mov
emen
t di
sord
ers,
ort
hopa
edic
and
othe
r ga
it in
fluen
cing
dise
ase
Mea
n ag
e: G
roup
1: 5
8.2
year
s(S
D10
.5),
grou
p 2:
57.
1 ye
ars
(SD
13.
9), g
roup
3: 6
1.6
year
s (S
D 1
0.6)
71.6
% m
ale
Stro
ke d
etai
ls: 7
0% is
chae
mic
str
oke
Tim
e sin
ce s
trok
e: E
xper
imen
tal
16.8
wee
ks (S
D 2
0.5)
, co
ntro
l 16.
1w
eeks
(SD
18.
5)
Prei
nter
vent
ion
func
tiona
l abi
lity:
Mea
n w
alki
ng s
peed
(m/s
): gr
oup
10.
61 (S
D 0
.32)
, gro
up 2
0.6
6 (S
D 0
.39)
, gro
up 3
0.6
6 (S
D 0
.42)
Expe
rimen
tal i
nter
vent
ion:
Tria
lin
clud
ed t
wo
inte
rven
tion–
cont
rol
pairs
: spe
ed-d
epen
dent
, and
limite
d pr
ogre
ssiv
e tr
eadm
illtr
aini
ng. T
he li
mite
d pr
ogre
ssiv
ein
terv
entio
n–co
ntro
l com
paris
onw
as u
sed
Inte
rven
tion
grou
p 2
cons
isted
of
limite
d pr
ogre
ssiv
e tr
eadm
illtr
aini
ng. P
artic
ipan
ts w
alke
d on
atr
eadm
ill w
ith t
he t
rain
ing
spee
din
crea
sed
by n
o m
ore
than
5%
of
the
max
imum
initi
al w
alki
ng s
peed
each
wee
k. P
hysic
al t
hera
pist
sdi
rect
ly a
ssist
ed p
artic
ipan
ts in
the
wal
king
cyc
le. B
odyw
eigh
t su
ppor
tal
low
ed o
nly
in t
he fi
rst
thre
etr
aini
ng s
essio
ns
Trea
ted
as in
patie
nts
for
thre
e 30
-min
ute
sess
ions
per
wee
k fo
r4
wee
ks. I
nter
vent
ion
was
addi
tiona
l to
conv
entio
nal
phys
ioth
erap
y re
ceiv
ed b
y al
lgr
oups
Com
paris
on g
roup
: Con
vent
iona
lga
it tr
aini
ng: p
hysio
ther
apeu
tic g
ait
ther
apy
base
d on
neur
ophy
siolo
gica
l tec
hniq
ues.
T
hree
45-
min
ute
sess
ions
per
wee
k fo
r 4
wee
ks. A
dditi
onal
to
conv
entio
nal p
hysio
ther
apy
rece
ived
Out
com
es r
ecor
ded
pre-
and
post
-inte
rven
tion
Lim
b-sp
ecifi
c fu
nctio
n:Fa
stes
t co
mfo
rtab
lew
alki
ng s
peed
ove
r 10
mus
ing
gait
aids
if r
equi
red,
FAC
Mot
or im
pairm
ent:
Cad
ence
, str
ide
leng
th
Allo
catio
n co
ncea
lmen
tun
clea
r
No
signi
fican
t di
ffere
nces
in b
asel
ine
char
acte
ristic
s
Blin
ded
outc
ome
asse
ssm
ent
Loss
to
follo
w-u
p at
end
of t
reat
men
t pe
riod:
10%
No
inte
rven
tion-
rela
ted
with
draw
als
No
adve
rse
even
tsre
port
ed
cont
inue
d

Health Technology Assessment 2008; Vol. 12: No. 30
105
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Aut
hor
and
year
Stud
y de
tails
Cou
ntry
and
par
tici
pant
sIn
terv
enti
onO
utco
mes
Not
es
Sche
idtm
ann,
199
963
(Des
crip
tion
take
nfr
om t
rans
latio
n an
dsu
pple
men
ted
byde
tails
giv
en in
Mos
eley
, 200
520)
Cro
ss-o
ver
grou
pde
sign
Part
icip
ants
ran
dom
ised
to g
roup
s (m
etho
d of
rand
omisa
tion
and
conc
ealm
ent
not
stat
ed)
Ger
man
y15
par
ticip
ants
allo
cate
d to
expe
rimen
tal t
hen
cont
rol g
roup
,an
d 15
par
ticip
ants
allo
cate
d to
cont
rol t
hen
expe
rimen
tal g
roup
Incl
usio
n cr
iteria
: Hem
ipar
esis,
str
oke
(infa
rct
or h
aem
orrh
age)
, at
leas
t4
wee
ks p
ost-
stro
ke, n
ot a
ble
tow
alk,
abl
e to
sta
nd fo
r 20
sec
onds
Excl
usio
n cr
iteria
: Car
diov
ascu
lar
prob
lem
s or
infe
ctio
ns w
ith a
decr
ease
in g
ener
al h
ealth
Age:
57.
7 (S
D 1
1)52
% m
ale
Stro
ke d
etai
ls: 6
9% is
chae
mic
str
oke
Tim
e sin
ce s
trok
e: 5
8.2
days
(S
D 2
8.6)
Prei
nter
vent
ion
abili
ty le
vel:
Abl
e to
stan
d fo
r up
to
20 s
econ
ds
Expe
rimen
tal i
nter
vent
ion:
Tre
adm
illtr
aini
ng c
ombi
ned
with
phys
ioth
erap
y w
ith b
odyw
eigh
tsu
ppor
t. Pa
rtic
ipan
ts w
alke
d on
atr
eadm
ill w
ith p
artia
l bod
ywei
ght
supp
ort
prov
ided
by
a ha
rnes
s fo
r30
min
utes
and
com
plet
ed30
min
utes
of u
sual
phy
sioth
erap
ype
r da
y
Trea
ted
as in
-par
ticip
ants
for
five
1-ho
ur s
essio
ns p
er w
eek
for
3w
eeks
Com
paris
on g
roup
: Par
ticip
ants
com
plet
ed t
wo
30-m
inut
e se
ssio
nsof
phy
sioth
erap
y pe
r da
y
Out
com
es a
sses
sed
atba
selin
e, a
t cr
oss-
over
(3w
eeks
) and
afte
rtr
eatm
ent
phas
e (a
t6
wee
ks)
Lim
b-sp
ecifi
c fu
nctio
n:RM
A S
cale
, wal
king
spee
d ov
er 1
0 m
(ite
m 6
of t
he R
MA
),co
mfo
rtab
le o
rm
axim
um
Pers
onal
ass
istan
ce,
supe
rvisi
on a
nd g
ait
aid
use
wer
e no
t re
port
ed
Mot
or im
pairm
ent:
Self-
deve
lope
d ga
it sc
ale
base
d on
clin
ical
asse
ssm
ent
Allo
catio
n co
ncea
lmen
tun
clea
r
Blin
ding
of o
utco
me
asse
ssor
s to
gro
upal
loca
tion
not
repo
rted
No
drop
outs
at
end
offir
st t
reat
men
t ph
ase
No
inte
rven
tion-
rela
ted
with
draw
als
Adv
erse
eve
nts
not
stat
ed

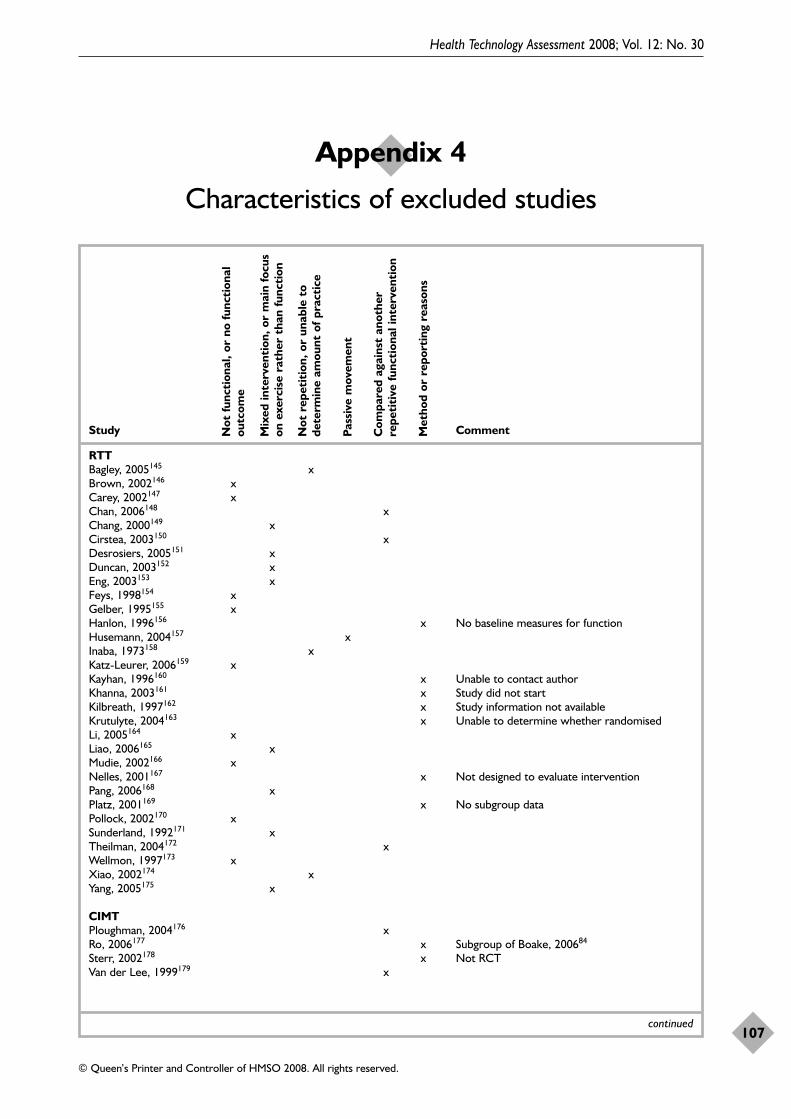
Health Technology Assessment 2008; Vol. 12: No. 30
107
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Appendix 4
Characteristics of excluded studies
Study Comment
RTTBagley, 2005145 xBrown, 2002146 xCarey, 2002147 xChan, 2006148 xChang, 2000149 xCirstea, 2003150 xDesrosiers, 2005151 xDuncan, 2003152 xEng, 2003153 xFeys, 1998154 xGelber, 1995155 xHanlon, 1996156 x No baseline measures for functionHusemann, 2004157 xInaba, 1973158 xKatz-Leurer, 2006159 xKayhan, 1996160 x Unable to contact authorKhanna, 2003161 x Study did not startKilbreath, 1997162 x Study information not availableKrutulyte, 2004163 x Unable to determine whether randomisedLi, 2005164 xLiao, 2006165 xMudie, 2002166 xNelles, 2001167 x Not designed to evaluate interventionPang, 2006168 xPlatz, 2001169 x No subgroup dataPollock, 2002170 xSunderland, 1992171 xTheilman, 2004172 xWellmon, 1997173 xXiao, 2002174 xYang, 2005175 x
CIMTPloughman, 2004176 xRo, 2006177 x Subgroup of Boake, 200684
Sterr, 2002178 x Not RCTVan der Lee, 1999179 x
continued
Not
func
tion
al, o
r no
func
tion
alou
tcom
e
Mix
ed in
terv
enti
on, o
r m
ain
focu
son
exe
rcis
e ra
ther
tha
n fu
ncti
on
Not
rep
etit
ion,
or
unab
le t
ode
term
ine
amou
nt o
f pra
ctic
e
Pass
ive
mov
emen
t
Com
pare
d ag
ains
t an
othe
rre
peti
tive
func
tion
al in
terv
enti
on
Met
hod
or r
epor
ting
rea
sons
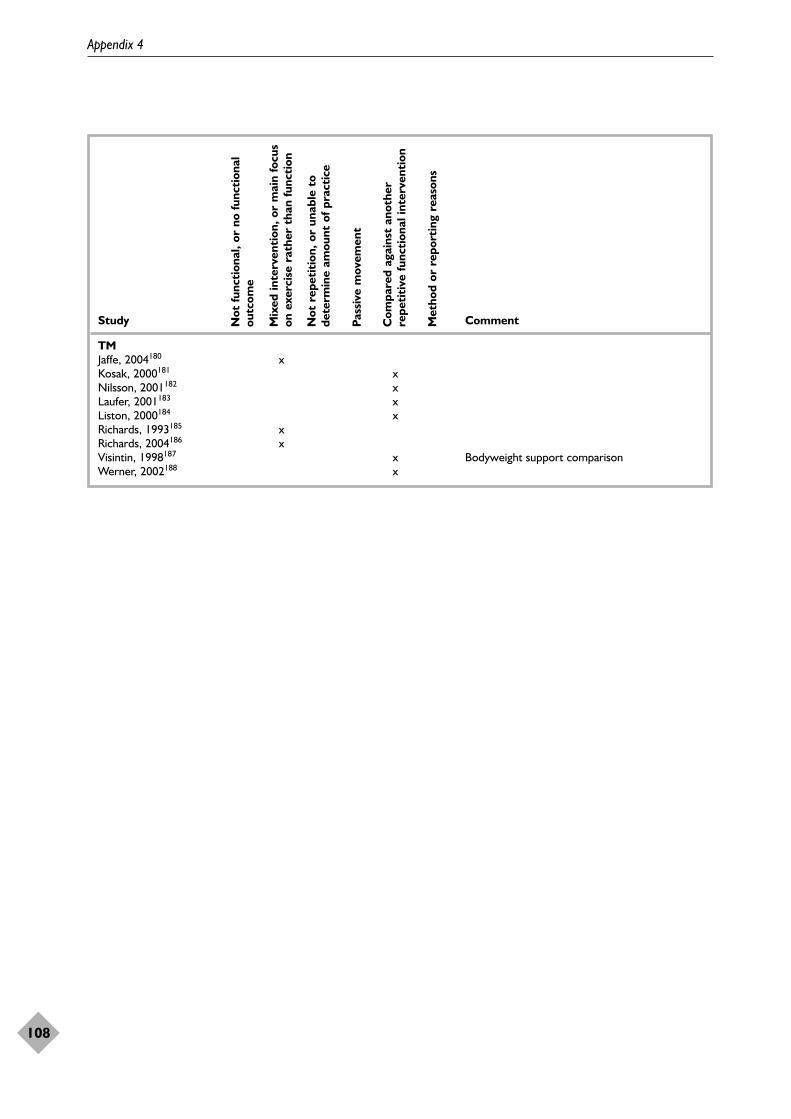
Appendix 4
108
Study Comment
TMJaffe, 2004180 xKosak, 2000181 xNilsson, 2001182 xLaufer, 2001183 xListon, 2000184 xRichards, 1993185 xRichards, 2004186 xVisintin, 1998187 x Bodyweight support comparisonWerner, 2002188 x
Not
func
tion
al, o
r no
func
tion
alou
tcom
e
Mix
ed in
terv
enti
on, o
r m
ain
focu
son
exe
rcis
e ra
ther
tha
n fu
ncti
on
Not
rep
etit
ion,
or
unab
le t
ode
term
ine
amou
nt o
f pra
ctic
e
Pass
ive
mov
emen
t
Com
pare
d ag
ains
t an
othe
rre
peti
tive
func
tion
al in
terv
enti
on
Met
hod
or r
epor
ting
rea
sons

Health Technology Assessment 2008; Vol. 12: No. 30
109
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Appendix 5
Characteristics of ongoing studies

Appendix 5
110
Stud
yTr
ial n
ame
Part
icip
ants
Inte
rven
tion
sO
utco
mes
Star
ting
dat
eN
otes
RT
TA
lliso
n, 2
00590
Pilo
t ra
ndom
ised
cont
rol t
rial t
o as
sess
0–
3 m
onth
s St
andi
ng p
ract
ice
plus
RM
A, T
runk
Con
trol
20
01Tr
ial c
ompl
ete
and
the
impa
ct o
f add
ition
al s
uppo
rted
po
st-s
trok
eus
ual c
are
Test
, Ber
g Ba
lanc
e Sc
ale
bein
g su
bmitt
ed fo
r st
andi
ng p
ract
ice
on fu
nctio
nal a
bilit
y pu
blic
atio
npo
st-s
trok
e
Ask
im, 2
00591
Doe
s in
tens
ive
task
spe
cific
tra
inin
g 0–
3 m
onth
s Ba
lanc
e tr
aini
ng p
lus
Bala
nce,
sit-
to-s
tand
, 20
05Tr
ial d
ue t
o co
mpl
ete
impr
ove
bala
nce
afte
r ac
ute
stro
ke?
post
-str
oke
usua
l car
ew
alki
ng s
peed
, AD
L, fa
lls,
2012
low
er li
mb
func
tion
Engl
ish, 2
00593
Is t
ask-
rela
ted
circ
uit
trai
ning
an
0–3
mon
ths
Task
-rel
ated
circ
uit
Bala
nce,
MA
S, g
ait
spee
d 20
03Tr
ial c
ompl
ete
and
effe
ctiv
e m
eans
of p
rovi
ding
po
st-s
trok
etr
aini
ngan
d en
dura
nce,
NH
P, be
ing
subm
itted
for
reha
bilit
atio
n to
acu
te s
trok
e pa
tient
s?pa
tient
sat
isfac
tion
publ
icat
ion
Har
ris, 2
00692
Eval
uatio
n of
a r
epet
itive
pra
ctic
e 0–
3 m
onth
s Re
petit
ive
sit-t
o-st
and
Sit-
to-s
tand
2005
Tria
l due
to
com
plet
e sc
hem
e to
impr
ove
sit-t
o-st
and
post
-str
oke
trai
ning
2006
perf
orm
ance
follo
win
g st
roke
Lang
ham
mer
, St
roke
: red
uctio
n of
phy
sical
Po
st-a
cute
M
otor
rel
earn
ing
Phys
ical
end
uran
ce,
2003
Tria
l clo
sed
inta
ke
2005
(per
sona
l pe
rfor
man
ce p
ost-
stro
ke: i
nact
ivity
or
reha
bilit
atio
nst
reng
th, b
alan
ceau
tum
n 20
05co
mm
unic
atio
n)se
cond
ary
com
plic
atio
ns?
Mill
er, 2
00295
Early
inte
nsiv
e ta
sk-s
peci
fic s
enso
ry a
nd
0–3
mon
ths
Task
-spe
cific
tra
inin
g of
M
AS,
Che
doke
McM
aste
r 20
02Ph
D d
ue t
o co
mpl
ete
mot
or t
rain
ing
of t
he u
pper
lim
b af
ter
post
-str
oke
the
uppe
r lim
b,
Impa
irmen
t In
vent
ory,
in
200
7ac
ute
stro
ke: a
pilo
t st
udy
emph
asisi
ng u
nim
anua
l Si
ckne
ss Im
pact
Pro
file,
an
d bi
man
ual f
unct
iona
l ha
nd d
exte
rity
activ
ities
Sher
ringt
on,
A r
ando
mise
d co
ntro
lled
tria
l to
173
olde
r C
ircui
t de
signe
d to
Ba
lanc
e, g
ait,
sit-t
o-st
and,
20
05Pu
blic
atio
n su
bmitt
ed.
2005
94ev
alua
te t
ask-
rela
ted
exer
cise
cla
sses
pe
ople
, 90
with
pr
ovid
e re
petit
ive,
w
alki
ng e
ndur
ance
Subg
roup
dat
a fo
r ol
der
peop
le w
ith im
paire
d m
obili
tyne
urol
ogic
al
func
tiona
l, av
aila
ble
2008
prob
lem
sta
sk-r
elat
ed e
xerc
ise
CIM
TN
oser
, 200
496C
onst
rain
t-in
duce
d m
ovem
ent
ther
apy
4–10
day
s C
IMT
Arm
and
han
d fu
nctio
n20
00Tr
ial d
ue t
o co
mpl
ete
afte
r su
bacu
te s
trok
epo
st-s
trok
eJu
ne 2
007
Health Technology Assessment 2008; Vol. 12: No. 30
111
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Appendix 6
Criteria for subgroup analyses

Appendix 6
112
Stud
yTa
sk p
ract
ice
Tim
e si
nce
Inte
rven
tion
A
lloca
tion
C
ompa
riso
n T
hera
py
Tria
l siz
eg
amou
nta
stro
keb
deliv
eryc
conc
ealm
entd
grou
peti
mef
RT
TBl
enne
rhas
sett
, 200
4501
32
AA
CEQ
2D
ean,
199
7661
31
BA
CEQ
1D
ean,
200
0671
32
AA
CEQ
1de
Sèz
e, 2
00176
12
1B
UC
EQ2
How
e, 2
00577
12
1A
UC
EQ2
Kw
akke
l, 19
9953
21
1A
AC
EQ2
Lang
ham
mer
, 200
0681
11
BU
CEQ
2M
cCle
llan,
200
4782
33
AA
CEQ
2Sa
lbac
h, 2
00451
13
2A
AC
EQ2
Turt
on, 1
99069
22
3B
UC
AD
D1
Van
Vlie
t, 20
0570
11
1A
UC
EQ2
Win
stei
n, 2
00471
11
1A
UC
AD
D2
Yen,
200
5722
31
BU
CEQ
2
TM
Ada
, 200
3871
31
AA
CEQ
2da
Cuh
na, 2
00286
12
1B
UC
EQ1
Eich
, 200
4891
21
AA
LTEQ
2M
acko
, 200
5882
31
BA
LTEQ
2Po
hl, 2
00285
12
1B
UC
EQ2
CIM
TA
lber
ts, 2
00483
22
1B
NT
AD
D1
Att
eya,
200
4792
21
BN
TA
DD
1Bo
ake,
200
6842
11
BU
CEQ
1D
rom
eric
k, 2
00081
11
1B
UC
EQ1
Page
, 200
1802
21
BN
TA
DD
1Pa
ge, 2
00582
11
1B
UC
AD
D1
Taub
, 199
3732
31
BA
CEQ
1W
itten
berg
, 200
3742
31
BA
CA
DD
1
a 1
= �
20 h
ours
, 2 =
>20
hou
rs.
b 1
= 1
–14
days
, 2 =
15
days
to
6 m
onth
s, 3
= >
6 m
onth
s.c 1
= in
divi
dual
the
rapy
, 2 =
gro
up, 3
= s
elf –
hom
e.d
A =
ade
quat
e, B
=in
adeq
uate
/unc
lear
.e
AC
= a
tten
tion
cont
rol,
UC
= u
sual
car
e, A
LT =
alte
rnat
ive
trea
tmen
t, N
T =
no
trea
tmen
t.f EQ
= e
qual
tim
e, A
DD
= a
dditi
onal
tim
e.g 1
= <
25 p
artic
ipan
ts, 2
= �
25 p
artic
ipan
ts.

Health Technology Assessment 2008; Vol. 12: No. 30
113
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Appendix 7
Summary of baseline characteristics of patients from the cohort in the patient data set who
survived to 3 years
Age (years) median (IQR) 69.5 (64 to 77)
Gender female, n (%) 58 (39)Lesion type, n (%)
IC 108 (72)Primary intracerebral haemorrhage 17 (11)Haemorrhagic transformation of IC 4 (3)No scan 21 (14)
Side, n (%)Left 52 (35)Right 64 (42)No bilateral signs 34 (23)
IC, ischaemic infarction.


Health Technology Assessment 2008; Vol. 12: No. 30
115
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Appendix 8
Numbers of patients and costs in the baseline and new groups
Baseline groups New groups
Barthel category Average cost n Total cost na Total cost Difference
�10 £4,398 28 £123,154 25.5 £111,95811–14 £6,874 34 £233,727 28.0 £192,79315–17 £4,914 33 £162,169 30.5 £149,88318 or 19 £2,153 25 £53,819 23.5 £50,58920 £1,610 30 £48,291 42.5 £68,412Total 150 £621,159 150 £573,636 £47,523Average £4,141 £3,824 £317
a Approximate.


Health Technology Assessment 2008; Vol. 12: No. 30
117
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Appendix 9
Cost-effectiveness at 3 years per QALY gained for RFTP on outcome measures that
were significant in the systematic review
Analysisa Outcome Overallb Arm ADLc Walking Functional Sit-to-functionc distanced ambulationd standd
1 SMD £10,870 £15,185 £11,009 £4,187 £10,187 £5,708SMD lower limit CI £23,947 £77,821 £49,983 £16,539 £83,239 £19,010SMD upper limit CI £6,039 £6,237 £3,942 £658 £3,025 £1,596
2 SMD: BI; 0.2:1.0 £10,870 £15,185 £11,009 £4,187 £10,187 £5,708SMD: BI; 0.2:0.8 £15,011 £20,405 £15,185 £6,658 £14,157 £8,558SMD: BI; 0.2:0.6 £21,913 £29,104 £22,144 £10,775 £20,774 £13,309SMD: BI; 0.2:0.4 £35,716 £46,503 £36,064 £19,010 £34,008 £22,810SMD: BI; 0.2:0.2 £77,126 £98,700 £77,821 £43,713 £73,711 £51,315
3 BI: EQ-5D; 1:0.05 £10,870 £15,185 £11,009 £4,187 £10,187 £5,708BI: EQ-5D; 1:0.04 £13,587 £18,981 £13,761 £5,234 £12,734 £7,135BI: EQ-5D; 1:0.03 £18,116 £25,308 £18,348 £6,979 £16,978 £9,513BI: EQ-5D; 1:0.02 £27,175 £37,962 £27,523 £10,469 £25,467 £14,269BI: EQ-5D; 1:0.01 £54,349 £75,924 £55,045 £20,937 £50,935 £28,538
4 £35 per hour £9,143 £12,712 £9,031 £3,283 £8,734 £4,664£40 per hour £10,870 £15,185 £11,009 £4,187 £10,187 £5,708£45 per hour £12,597 £17,657 £12,987 £5,092 £11,640 £6,751£50 per hour £14,323 £20,129 £14,965 £5,996 £13,093 £7,794£55 per hour £16,050 £22,602 £16,943 £6,900 £14,546 £8,837£60 per hour £17,777 £25,074 £18,921 £7,804 £15,999 £9,880
5 Discount = 0% £10,228 £14,543 £10,367 £3,545 £9,545 £5,065Discount = 3.5% £10,870 £15,185 £11,009 £4,187 £10,187 £5,708Discount = 6.0% £11,301 £15,616 £11,440 £4,619 £10,618 £6,139
6 Discount = 0% £9,191 £13,068 £9,316 £3,186 £8,577 £4,552Discount = 3.5% £10,870 £15,185 £11,009 £4,187 £10,187 £5,708Discount = 6.0% £12,227 £16,895 £12,377 £4,997 £11,488 £6,642
a 1, Base case; 2, varying the association between the SMD and the BI (shaded cells are base case); 3, varying the associationbetween the BI and the EQ-5D (shaded cells are base case); 4, varying the cost per hour of client contact with therapist(shaded cells are base case); 5, varying the discount rate on cost (shaded cells are base case); 6, varying the discount rateon outcome (shaded cells are base case).
b Cost per QALY gained, where the cost of the intervention is £1265 (based on the average cost of RTT, CIMT and TM).c Cost per QALY gained, where the cost of the intervention is £1126 (based on the average cost of RTT and CIMT).d Cost per QALY gained, where the cost of the intervention is £999 (based on the average cost of RTT and TM).


Volume 1, 1997
No. 1Home parenteral nutrition: a systematicreview.
By Richards DM, Deeks JJ, SheldonTA, Shaffer JL.
No. 2Diagnosis, management and screeningof early localised prostate cancer.
A review by Selley S, Donovan J,Faulkner A, Coast J, Gillatt D.
No. 3The diagnosis, management, treatmentand costs of prostate cancer in Englandand Wales.
A review by Chamberlain J, Melia J,Moss S, Brown J.
No. 4Screening for fragile X syndrome.
A review by Murray J, Cuckle H,Taylor G, Hewison J.
No. 5A review of near patient testing inprimary care.
By Hobbs FDR, Delaney BC,Fitzmaurice DA, Wilson S, Hyde CJ,Thorpe GH, et al.
No. 6Systematic review of outpatient servicesfor chronic pain control.
By McQuay HJ, Moore RA, EcclestonC, Morley S, de C Williams AC.
No. 7Neonatal screening for inborn errors ofmetabolism: cost, yield and outcome.
A review by Pollitt RJ, Green A,McCabe CJ, Booth A, Cooper NJ,Leonard JV, et al.
No. 8Preschool vision screening.
A review by Snowdon SK, Stewart-Brown SL.
No. 9Implications of socio-cultural contextsfor the ethics of clinical trials.
A review by Ashcroft RE, ChadwickDW, Clark SRL, Edwards RHT, Frith L,Hutton JL.
No. 10A critical review of the role of neonatalhearing screening in the detection ofcongenital hearing impairment.
By Davis A, Bamford J, Wilson I,Ramkalawan T, Forshaw M, Wright S.
No. 11Newborn screening for inborn errors ofmetabolism: a systematic review.
By Seymour CA, Thomason MJ,Chalmers RA, Addison GM, Bain MD,Cockburn F, et al.
No. 12Routine preoperative testing: a systematic review of the evidence.
By Munro J, Booth A, Nicholl J.
No. 13Systematic review of the effectiveness of laxatives in the elderly.
By Petticrew M, Watt I, Sheldon T.
No. 14When and how to assess fast-changingtechnologies: a comparative study ofmedical applications of four generictechnologies.
A review by Mowatt G, Bower DJ,Brebner JA, Cairns JA, Grant AM,McKee L.
Volume 2, 1998
No. 1Antenatal screening for Down’ssyndrome.
A review by Wald NJ, Kennard A,Hackshaw A, McGuire A.
No. 2Screening for ovarian cancer: a systematic review.
By Bell R, Petticrew M, Luengo S,Sheldon TA.
No. 3Consensus development methods, andtheir use in clinical guidelinedevelopment.
A review by Murphy MK, Black NA,Lamping DL, McKee CM, SandersonCFB, Askham J, et al.
No. 4A cost–utility analysis of interferon beta for multiple sclerosis.
By Parkin D, McNamee P, Jacoby A,Miller P, Thomas S, Bates D.
No. 5Effectiveness and efficiency of methodsof dialysis therapy for end-stage renaldisease: systematic reviews.
By MacLeod A, Grant A, Donaldson C, Khan I, Campbell M,Daly C, et al.
No. 6Effectiveness of hip prostheses inprimary total hip replacement: a criticalreview of evidence and an economicmodel.
By Faulkner A, Kennedy LG, Baxter K, Donovan J, Wilkinson M,Bevan G.
No. 7Antimicrobial prophylaxis in colorectalsurgery: a systematic review ofrandomised controlled trials.
By Song F, Glenny AM.
No. 8Bone marrow and peripheral bloodstem cell transplantation for malignancy.
A review by Johnson PWM, Simnett SJ,Sweetenham JW, Morgan GJ, Stewart LA.
No. 9Screening for speech and languagedelay: a systematic review of theliterature.
By Law J, Boyle J, Harris F, HarknessA, Nye C.
No. 10Resource allocation for chronic stableangina: a systematic review ofeffectiveness, costs and cost-effectiveness of alternativeinterventions.
By Sculpher MJ, Petticrew M, Kelland JL, Elliott RA, Holdright DR,Buxton MJ.
No. 11Detection, adherence and control ofhypertension for the prevention ofstroke: a systematic review.
By Ebrahim S.
No. 12Postoperative analgesia and vomiting,with special reference to day-casesurgery: a systematic review.
By McQuay HJ, Moore RA.
No. 13Choosing between randomised andnonrandomised studies: a systematicreview.
By Britton A, McKee M, Black N,McPherson K, Sanderson C, Bain C.
No. 14Evaluating patient-based outcomemeasures for use in clinical trials.
A review by Fitzpatrick R, Davey C,Buxton MJ, Jones DR.
Health Technology Assessment 2008; Vol. 12: No. 30
119
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
Health Technology Assessment reports published to date
No. 15Ethical issues in the design and conductof randomised controlled trials.
A review by Edwards SJL, Lilford RJ,Braunholtz DA, Jackson JC, Hewison J,Thornton J.
No. 16Qualitative research methods in healthtechnology assessment: a review of theliterature.
By Murphy E, Dingwall R, GreatbatchD, Parker S, Watson P.
No. 17The costs and benefits of paramedicskills in pre-hospital trauma care.
By Nicholl J, Hughes S, Dixon S,Turner J, Yates D.
No. 18Systematic review of endoscopicultrasound in gastro-oesophagealcancer.
By Harris KM, Kelly S, Berry E,Hutton J, Roderick P, Cullingworth J, et al.
No. 19Systematic reviews of trials and otherstudies.
By Sutton AJ, Abrams KR, Jones DR,Sheldon TA, Song F.
No. 20Primary total hip replacement surgery: a systematic review of outcomes andmodelling of cost-effectivenessassociated with different prostheses.
A review by Fitzpatrick R, Shortall E,Sculpher M, Murray D, Morris R, LodgeM, et al.
Volume 3, 1999
No. 1Informed decision making: an annotatedbibliography and systematic review.
By Bekker H, Thornton JG, Airey CM, Connelly JB, Hewison J,Robinson MB, et al.
No. 2Handling uncertainty when performingeconomic evaluation of healthcareinterventions.
A review by Briggs AH, Gray AM.
No. 3The role of expectancies in the placeboeffect and their use in the delivery ofhealth care: a systematic review.
By Crow R, Gage H, Hampson S,Hart J, Kimber A, Thomas H.
No. 4A randomised controlled trial ofdifferent approaches to universalantenatal HIV testing: uptake andacceptability. Annex: Antenatal HIVtesting – assessment of a routinevoluntary approach.
By Simpson WM, Johnstone FD, BoydFM, Goldberg DJ, Hart GJ, GormleySM, et al.
No. 5Methods for evaluating area-wide andorganisation-based interventions inhealth and health care: a systematicreview.
By Ukoumunne OC, Gulliford MC,Chinn S, Sterne JAC, Burney PGJ.
No. 6Assessing the costs of healthcaretechnologies in clinical trials.
A review by Johnston K, Buxton MJ,Jones DR, Fitzpatrick R.
No. 7Cooperatives and their primary careemergency centres: organisation andimpact.
By Hallam L, Henthorne K.
No. 8Screening for cystic fibrosis.
A review by Murray J, Cuckle H,Taylor G, Littlewood J, Hewison J.
No. 9A review of the use of health statusmeasures in economic evaluation.
By Brazier J, Deverill M, Green C,Harper R, Booth A.
No. 10Methods for the analysis of quality-of-life and survival data in healthtechnology assessment.
A review by Billingham LJ, AbramsKR, Jones DR.
No. 11Antenatal and neonatalhaemoglobinopathy screening in theUK: review and economic analysis.
By Zeuner D, Ades AE, Karnon J,Brown J, Dezateux C, Anionwu EN.
No. 12Assessing the quality of reports ofrandomised trials: implications for theconduct of meta-analyses.
A review by Moher D, Cook DJ, JadadAR, Tugwell P, Moher M, Jones A, et al.
No. 13‘Early warning systems’ for identifyingnew healthcare technologies.
By Robert G, Stevens A, Gabbay J.
No. 14A systematic review of the role of humanpapillomavirus testing within a cervicalscreening programme.
By Cuzick J, Sasieni P, Davies P,Adams J, Normand C, Frater A, et al.
No. 15Near patient testing in diabetes clinics:appraising the costs and outcomes.
By Grieve R, Beech R, Vincent J,Mazurkiewicz J.
No. 16Positron emission tomography:establishing priorities for healthtechnology assessment.
A review by Robert G, Milne R.
No. 17 (Pt 1)The debridement of chronic wounds: a systematic review.
By Bradley M, Cullum N, Sheldon T.
No. 17 (Pt 2)Systematic reviews of wound caremanagement: (2) Dressings and topicalagents used in the healing of chronicwounds.
By Bradley M, Cullum N, Nelson EA,Petticrew M, Sheldon T, Torgerson D.
No. 18A systematic literature review of spiraland electron beam computedtomography: with particular reference toclinical applications in hepatic lesions,pulmonary embolus and coronary arterydisease.
By Berry E, Kelly S, Hutton J, Harris KM, Roderick P, Boyce JC, et al.
No. 19What role for statins? A review andeconomic model.
By Ebrahim S, Davey Smith G,McCabe C, Payne N, Pickin M, SheldonTA, et al.
No. 20Factors that limit the quality, numberand progress of randomised controlledtrials.
A review by Prescott RJ, Counsell CE,Gillespie WJ, Grant AM, Russell IT,Kiauka S, et al.
No. 21Antimicrobial prophylaxis in total hipreplacement: a systematic review.
By Glenny AM, Song F.
No. 22Health promoting schools and healthpromotion in schools: two systematicreviews.
By Lister-Sharp D, Chapman S,Stewart-Brown S, Sowden A.
No. 23Economic evaluation of a primary care-based education programme for patientswith osteoarthritis of the knee.
A review by Lord J, Victor C,Littlejohns P, Ross FM, Axford JS.
Volume 4, 2000
No. 1The estimation of marginal timepreference in a UK-wide sample(TEMPUS) project.
A review by Cairns JA, van der PolMM.
No. 2Geriatric rehabilitation followingfractures in older people: a systematicreview.
By Cameron I, Crotty M, Currie C,Finnegan T, Gillespie L, Gillespie W, et al.
Health Technology Assessment reports published to date
120

No. 3Screening for sickle cell disease andthalassaemia: a systematic review withsupplementary research.
By Davies SC, Cronin E, Gill M,Greengross P, Hickman M, Normand C.
No. 4Community provision of hearing aidsand related audiology services.
A review by Reeves DJ, Alborz A,Hickson FS, Bamford JM.
No. 5False-negative results in screeningprogrammes: systematic review ofimpact and implications.
By Petticrew MP, Sowden AJ, Lister-Sharp D, Wright K.
No. 6Costs and benefits of communitypostnatal support workers: arandomised controlled trial.
By Morrell CJ, Spiby H, Stewart P,Walters S, Morgan A.
No. 7Implantable contraceptives (subdermalimplants and hormonally impregnatedintrauterine systems) versus other formsof reversible contraceptives: twosystematic reviews to assess relativeeffectiveness, acceptability, tolerabilityand cost-effectiveness.
By French RS, Cowan FM, MansourDJA, Morris S, Procter T, Hughes D, et al.
No. 8An introduction to statistical methodsfor health technology assessment.
A review by White SJ, Ashby D, Brown PJ.
No. 9Disease-modifying drugs for multiplesclerosis: a rapid and systematic review.
By Clegg A, Bryant J, Milne R.
No. 10Publication and related biases.
A review by Song F, Eastwood AJ,Gilbody S, Duley L, Sutton AJ.
No. 11Cost and outcome implications of theorganisation of vascular services.
By Michaels J, Brazier J, PalfreymanS, Shackley P, Slack R.
No. 12Monitoring blood glucose control indiabetes mellitus: a systematic review.
By Coster S, Gulliford MC, Seed PT,Powrie JK, Swaminathan R.
No. 13The effectiveness of domiciliary healthvisiting: a systematic review ofinternational studies and a selective review of the Britishliterature.
By Elkan R, Kendrick D, Hewitt M,Robinson JJA, Tolley K, Blair M, et al.
No. 14The determinants of screening uptakeand interventions for increasing uptake:a systematic review.
By Jepson R, Clegg A, Forbes C,Lewis R, Sowden A, Kleijnen J.
No. 15The effectiveness and cost-effectivenessof prophylactic removal of wisdomteeth.
A rapid review by Song F, O’Meara S,Wilson P, Golder S, Kleijnen J.
No. 16Ultrasound screening in pregnancy: asystematic review of the clinicaleffectiveness, cost-effectiveness andwomen’s views.
By Bricker L, Garcia J, Henderson J,Mugford M, Neilson J, Roberts T, et al.
No. 17A rapid and systematic review of theeffectiveness and cost-effectiveness ofthe taxanes used in the treatment ofadvanced breast and ovarian cancer.
By Lister-Sharp D, McDonagh MS,Khan KS, Kleijnen J.
No. 18Liquid-based cytology in cervicalscreening: a rapid and systematic review.
By Payne N, Chilcott J, McGoogan E.
No. 19Randomised controlled trial of non-directive counselling,cognitive–behaviour therapy and usualgeneral practitioner care in themanagement of depression as well asmixed anxiety and depression inprimary care.
By King M, Sibbald B, Ward E, BowerP, Lloyd M, Gabbay M, et al.
No. 20Routine referral for radiography ofpatients presenting with low back pain:is patients’ outcome influenced by GPs’referral for plain radiography?
By Kerry S, Hilton S, Patel S, DundasD, Rink E, Lord J.
No. 21Systematic reviews of wound caremanagement: (3) antimicrobial agentsfor chronic wounds; (4) diabetic footulceration.
By O’Meara S, Cullum N, Majid M,Sheldon T.
No. 22Using routine data to complement andenhance the results of randomisedcontrolled trials.
By Lewsey JD, Leyland AH, Murray GD, Boddy FA.
No. 23Coronary artery stents in the treatmentof ischaemic heart disease: a rapid andsystematic review.
By Meads C, Cummins C, Jolly K,Stevens A, Burls A, Hyde C.
No. 24Outcome measures for adult criticalcare: a systematic review.
By Hayes JA, Black NA, Jenkinson C, Young JD, Rowan KM,Daly K, et al.
No. 25A systematic review to evaluate theeffectiveness of interventions to promote the initiation of breastfeeding.
By Fairbank L, O’Meara S, RenfrewMJ, Woolridge M, Sowden AJ, Lister-Sharp D.
No. 26Implantable cardioverter defibrillators:arrhythmias. A rapid and systematicreview.
By Parkes J, Bryant J, Milne R.
No. 27Treatments for fatigue in multiplesclerosis: a rapid and systematic review.
By Brañas P, Jordan R, Fry-Smith A,Burls A, Hyde C.
No. 28Early asthma prophylaxis, naturalhistory, skeletal development andeconomy (EASE): a pilot randomisedcontrolled trial.
By Baxter-Jones ADG, Helms PJ,Russell G, Grant A, Ross S, Cairns JA, et al.
No. 29Screening for hypercholesterolaemiaversus case finding for familialhypercholesterolaemia: a systematicreview and cost-effectiveness analysis.
By Marks D, Wonderling D,Thorogood M, Lambert H, HumphriesSE, Neil HAW.
No. 30A rapid and systematic review of theclinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIaantagonists in the medical managementof unstable angina.
By McDonagh MS, Bachmann LM,Golder S, Kleijnen J, ter Riet G.
No. 31A randomised controlled trial ofprehospital intravenous fluidreplacement therapy in serious trauma.
By Turner J, Nicholl J, Webber L,Cox H, Dixon S, Yates D.
No. 32Intrathecal pumps for giving opioids inchronic pain: a systematic review.
By Williams JE, Louw G, Towlerton G.
No. 33Combination therapy (interferon alfaand ribavirin) in the treatment ofchronic hepatitis C: a rapid andsystematic review.
By Shepherd J, Waugh N, Hewitson P.
Health Technology Assessment 2008; Vol. 12: No. 30
121
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
No. 34A systematic review of comparisons ofeffect sizes derived from randomisedand non-randomised studies.
By MacLehose RR, Reeves BC,Harvey IM, Sheldon TA, Russell IT,Black AMS.
No. 35Intravascular ultrasound-guidedinterventions in coronary artery disease:a systematic literature review, withdecision-analytic modelling, of outcomesand cost-effectiveness.
By Berry E, Kelly S, Hutton J,Lindsay HSJ, Blaxill JM, Evans JA, et al.
No. 36A randomised controlled trial toevaluate the effectiveness and cost-effectiveness of counselling patients withchronic depression.
By Simpson S, Corney R, Fitzgerald P,Beecham J.
No. 37Systematic review of treatments foratopic eczema.
By Hoare C, Li Wan Po A, Williams H.
No. 38Bayesian methods in health technologyassessment: a review.
By Spiegelhalter DJ, Myles JP, Jones DR, Abrams KR.
No. 39The management of dyspepsia: asystematic review.
By Delaney B, Moayyedi P, Deeks J,Innes M, Soo S, Barton P, et al.
No. 40A systematic review of treatments forsevere psoriasis.
By Griffiths CEM, Clark CM, ChalmersRJG, Li Wan Po A, Williams HC.
Volume 5, 2001
No. 1Clinical and cost-effectiveness ofdonepezil, rivastigmine andgalantamine for Alzheimer’s disease: arapid and systematic review.
By Clegg A, Bryant J, Nicholson T,McIntyre L, De Broe S, Gerard K, et al.
No. 2The clinical effectiveness and cost-effectiveness of riluzole for motorneurone disease: a rapid and systematicreview.
By Stewart A, Sandercock J, Bryan S,Hyde C, Barton PM, Fry-Smith A, et al.
No. 3Equity and the economic evaluation ofhealthcare.
By Sassi F, Archard L, Le Grand J.
No. 4Quality-of-life measures in chronicdiseases of childhood.
By Eiser C, Morse R.
No. 5Eliciting public preferences forhealthcare: a systematic review oftechniques.
By Ryan M, Scott DA, Reeves C, BateA, van Teijlingen ER, Russell EM, et al.
No. 6General health status measures forpeople with cognitive impairment:learning disability and acquired braininjury.
By Riemsma RP, Forbes CA, Glanville JM, Eastwood AJ, Kleijnen J.
No. 7An assessment of screening strategies forfragile X syndrome in the UK.
By Pembrey ME, Barnicoat AJ,Carmichael B, Bobrow M, Turner G.
No. 8Issues in methodological research:perspectives from researchers andcommissioners.
By Lilford RJ, Richardson A, StevensA, Fitzpatrick R, Edwards S, Rock F, et al.
No. 9Systematic reviews of wound caremanagement: (5) beds; (6) compression;(7) laser therapy, therapeuticultrasound, electrotherapy andelectromagnetic therapy.
By Cullum N, Nelson EA, FlemmingK, Sheldon T.
No. 10Effects of educational and psychosocialinterventions for adolescents withdiabetes mellitus: a systematic review.
By Hampson SE, Skinner TC, Hart J,Storey L, Gage H, Foxcroft D, et al.
No. 11Effectiveness of autologous chondrocytetransplantation for hyaline cartilagedefects in knees: a rapid and systematicreview.
By Jobanputra P, Parry D, Fry-SmithA, Burls A.
No. 12Statistical assessment of the learningcurves of health technologies.
By Ramsay CR, Grant AM, Wallace SA, Garthwaite PH, Monk AF,Russell IT.
No. 13The effectiveness and cost-effectivenessof temozolomide for the treatment ofrecurrent malignant glioma: a rapid andsystematic review.
By Dinnes J, Cave C, Huang S, Major K, Milne R.
No. 14A rapid and systematic review of theclinical effectiveness and cost-effectiveness of debriding agents intreating surgical wounds healing bysecondary intention.
By Lewis R, Whiting P, ter Riet G,O’Meara S, Glanville J.
No. 15Home treatment for mental healthproblems: a systematic review.
By Burns T, Knapp M, Catty J, Healey A, Henderson J, Watt H, et al.
No. 16How to develop cost-consciousguidelines.
By Eccles M, Mason J.
No. 17The role of specialist nurses in multiplesclerosis: a rapid and systematic review.
By De Broe S, Christopher F, Waugh N.
No. 18A rapid and systematic review of theclinical effectiveness and cost-effectiveness of orlistat in themanagement of obesity.
By O’Meara S, Riemsma R, Shirran L, Mather L, ter Riet G.
No. 19The clinical effectiveness and cost-effectiveness of pioglitazone for type 2diabetes mellitus: a rapid and systematicreview.
By Chilcott J, Wight J, Lloyd JonesM, Tappenden P.
No. 20Extended scope of nursing practice: amulticentre randomised controlled trialof appropriately trained nurses andpreregistration house officers in pre-operative assessment in elective generalsurgery.
By Kinley H, Czoski-Murray C,George S, McCabe C, Primrose J, Reilly C, et al.
No. 21Systematic reviews of the effectiveness ofday care for people with severe mentaldisorders: (1) Acute day hospital versusadmission; (2) Vocational rehabilitation;(3) Day hospital versus outpatient care.
By Marshall M, Crowther R, Almaraz-Serrano A, Creed F, Sledge W, Kluiter H, et al.
No. 22The measurement and monitoring ofsurgical adverse events.
By Bruce J, Russell EM, Mollison J,Krukowski ZH.
No. 23Action research: a systematic review andguidance for assessment.
By Waterman H, Tillen D, Dickson R,de Koning K.
No. 24A rapid and systematic review of theclinical effectiveness and cost-effectiveness of gemcitabine for thetreatment of pancreatic cancer.
By Ward S, Morris E, Bansback N,Calvert N, Crellin A, Forman D, et al.
Health Technology Assessment reports published to date
122
No. 25A rapid and systematic review of theevidence for the clinical effectivenessand cost-effectiveness of irinotecan,oxaliplatin and raltitrexed for thetreatment of advanced colorectal cancer.
By Lloyd Jones M, Hummel S,Bansback N, Orr B, Seymour M.
No. 26Comparison of the effectiveness ofinhaler devices in asthma and chronicobstructive airways disease: a systematicreview of the literature.
By Brocklebank D, Ram F, Wright J,Barry P, Cates C, Davies L, et al.
No. 27The cost-effectiveness of magneticresonance imaging for investigation ofthe knee joint.
By Bryan S, Weatherburn G, BungayH, Hatrick C, Salas C, Parry D, et al.
No. 28A rapid and systematic review of theclinical effectiveness and cost-effectiveness of topotecan for ovariancancer.
By Forbes C, Shirran L, Bagnall A-M,Duffy S, ter Riet G.
No. 29Superseded by a report published in alater volume.
No. 30The role of radiography in primary carepatients with low back pain of at least 6weeks duration: a randomised(unblinded) controlled trial.
By Kendrick D, Fielding K, Bentley E,Miller P, Kerslake R, Pringle M.
No. 31Design and use of questionnaires: areview of best practice applicable tosurveys of health service staff andpatients.
By McColl E, Jacoby A, Thomas L,Soutter J, Bamford C, Steen N, et al.
No. 32A rapid and systematic review of theclinical effectiveness and cost-effectiveness of paclitaxel, docetaxel,gemcitabine and vinorelbine in non-small-cell lung cancer.
By Clegg A, Scott DA, Sidhu M,Hewitson P, Waugh N.
No. 33Subgroup analyses in randomisedcontrolled trials: quantifying the risks offalse-positives and false-negatives.
By Brookes ST, Whitley E, Peters TJ, Mulheran PA, Egger M,Davey Smith G.
No. 34Depot antipsychotic medication in thetreatment of patients with schizophrenia:(1) Meta-review; (2) Patient and nurseattitudes.
By David AS, Adams C.
No. 35A systematic review of controlled trialsof the effectiveness and cost-effectiveness of brief psychologicaltreatments for depression.
By Churchill R, Hunot V, Corney R,Knapp M, McGuire H, Tylee A, et al.
No. 36Cost analysis of child healthsurveillance.
By Sanderson D, Wright D, Acton C,Duree D.
Volume 6, 2002
No. 1A study of the methods used to selectreview criteria for clinical audit.
By Hearnshaw H, Harker R, CheaterF, Baker R, Grimshaw G.
No. 2Fludarabine as second-line therapy forB cell chronic lymphocytic leukaemia: a technology assessment.
By Hyde C, Wake B, Bryan S, BartonP, Fry-Smith A, Davenport C, et al.
No. 3Rituximab as third-line treatment forrefractory or recurrent Stage III or IVfollicular non-Hodgkin’s lymphoma: asystematic review and economicevaluation.
By Wake B, Hyde C, Bryan S, BartonP, Song F, Fry-Smith A, et al.
No. 4A systematic review of dischargearrangements for older people.
By Parker SG, Peet SM, McPherson A,Cannaby AM, Baker R, Wilson A, et al.
No. 5The clinical effectiveness and cost-effectiveness of inhaler devices used inthe routine management of chronicasthma in older children: a systematicreview and economic evaluation.
By Peters J, Stevenson M, Beverley C,Lim J, Smith S.
No. 6The clinical effectiveness and cost-effectiveness of sibutramine in themanagement of obesity: a technologyassessment.
By O’Meara S, Riemsma R, ShirranL, Mather L, ter Riet G.
No. 7The cost-effectiveness of magneticresonance angiography for carotidartery stenosis and peripheral vasculardisease: a systematic review.
By Berry E, Kelly S, Westwood ME,Davies LM, Gough MJ, Bamford JM,et al.
No. 8Promoting physical activity in SouthAsian Muslim women through ‘exerciseon prescription’.
By Carroll B, Ali N, Azam N.
No. 9Zanamivir for the treatment of influenzain adults: a systematic review andeconomic evaluation.
By Burls A, Clark W, Stewart T,Preston C, Bryan S, Jefferson T, et al.
No. 10A review of the natural history andepidemiology of multiple sclerosis:implications for resource allocation andhealth economic models.
By Richards RG, Sampson FC, Beard SM, Tappenden P.
No. 11Screening for gestational diabetes: asystematic review and economicevaluation.
By Scott DA, Loveman E, McIntyre L,Waugh N.
No. 12The clinical effectiveness and cost-effectiveness of surgery for people withmorbid obesity: a systematic review andeconomic evaluation.
By Clegg AJ, Colquitt J, Sidhu MK,Royle P, Loveman E, Walker A.
No. 13The clinical effectiveness of trastuzumabfor breast cancer: a systematic review.
By Lewis R, Bagnall A-M, Forbes C,Shirran E, Duffy S, Kleijnen J, et al.
No. 14The clinical effectiveness and cost-effectiveness of vinorelbine for breastcancer: a systematic review andeconomic evaluation.
By Lewis R, Bagnall A-M, King S,Woolacott N, Forbes C, Shirran L, et al.
No. 15A systematic review of the effectivenessand cost-effectiveness of metal-on-metalhip resurfacing arthroplasty fortreatment of hip disease.
By Vale L, Wyness L, McCormack K,McKenzie L, Brazzelli M, Stearns SC.
No. 16The clinical effectiveness and cost-effectiveness of bupropion and nicotinereplacement therapy for smokingcessation: a systematic review andeconomic evaluation.
By Woolacott NF, Jones L, Forbes CA,Mather LC, Sowden AJ, Song FJ, et al.
No. 17A systematic review of effectiveness andeconomic evaluation of new drugtreatments for juvenile idiopathicarthritis: etanercept.
By Cummins C, Connock M, Fry-Smith A, Burls A.
No. 18Clinical effectiveness and cost-effectiveness of growth hormone inchildren: a systematic review andeconomic evaluation.
By Bryant J, Cave C, Mihaylova B,Chase D, McIntyre L, Gerard K, et al.
Health Technology Assessment 2008; Vol. 12: No. 30
123
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
No. 19Clinical effectiveness and cost-effectiveness of growth hormone inadults in relation to impact on quality oflife: a systematic review and economicevaluation.
By Bryant J, Loveman E, Chase D,Mihaylova B, Cave C, Gerard K, et al.
No. 20Clinical medication review by apharmacist of patients on repeatprescriptions in general practice: arandomised controlled trial.
By Zermansky AG, Petty DR, RaynorDK, Lowe CJ, Freementle N, Vail A.
No. 21The effectiveness of infliximab andetanercept for the treatment ofrheumatoid arthritis: a systematic reviewand economic evaluation.
By Jobanputra P, Barton P, Bryan S,Burls A.
No. 22A systematic review and economicevaluation of computerised cognitivebehaviour therapy for depression andanxiety.
By Kaltenthaler E, Shackley P, StevensK, Beverley C, Parry G, Chilcott J.
No. 23A systematic review and economicevaluation of pegylated liposomaldoxorubicin hydrochloride for ovariancancer.
By Forbes C, Wilby J, Richardson G,Sculpher M, Mather L, Reimsma R.
No. 24A systematic review of the effectivenessof interventions based on a stages-of-change approach to promote individualbehaviour change.
By Riemsma RP, Pattenden J, Bridle C,Sowden AJ, Mather L, Watt IS, et al.
No. 25A systematic review update of theclinical effectiveness and cost-effectiveness of glycoprotein IIb/IIIaantagonists.
By Robinson M, Ginnelly L, SculpherM, Jones L, Riemsma R, Palmer S, et al.
No. 26A systematic review of the effectiveness,cost-effectiveness and barriers toimplementation of thrombolytic andneuroprotective therapy for acuteischaemic stroke in the NHS.
By Sandercock P, Berge E, Dennis M,Forbes J, Hand P, Kwan J, et al.
No. 27A randomised controlled crossover trial of nurse practitioner versus doctor-led outpatient care in abronchiectasis clinic.
By Caine N, Sharples LD,Hollingworth W, French J, Keogan M,Exley A, et al.
No. 28Clinical effectiveness and cost –consequences of selective serotoninreuptake inhibitors in the treatment ofsex offenders.
By Adi Y, Ashcroft D, Browne K,Beech A, Fry-Smith A, Hyde C.
No. 29Treatment of established osteoporosis: a systematic review and cost–utilityanalysis.
By Kanis JA, Brazier JE, Stevenson M,Calvert NW, Lloyd Jones M.
No. 30Which anaesthetic agents are cost-effective in day surgery? Literaturereview, national survey of practice andrandomised controlled trial.
By Elliott RA Payne K, Moore JK,Davies LM, Harper NJN, St Leger AS,et al.
No. 31Screening for hepatitis C amonginjecting drug users and ingenitourinary medicine clinics:systematic reviews of effectiveness,modelling study and national survey ofcurrent practice.
By Stein K, Dalziel K, Walker A,McIntyre L, Jenkins B, Horne J, et al.
No. 32The measurement of satisfaction withhealthcare: implications for practicefrom a systematic review of theliterature.
By Crow R, Gage H, Hampson S,Hart J, Kimber A, Storey L, et al.
No. 33The effectiveness and cost-effectivenessof imatinib in chronic myeloidleukaemia: a systematic review.
By Garside R, Round A, Dalziel K,Stein K, Royle R.
No. 34A comparative study of hypertonicsaline, daily and alternate-day rhDNase in children with cystic fibrosis.
By Suri R, Wallis C, Bush A,Thompson S, Normand C, Flather M, et al.
No. 35A systematic review of the costs andeffectiveness of different models ofpaediatric home care.
By Parker G, Bhakta P, Lovett CA,Paisley S, Olsen R, Turner D, et al.
Volume 7, 2003
No. 1How important are comprehensiveliterature searches and the assessment oftrial quality in systematic reviews?Empirical study.
By Egger M, Jüni P, Bartlett C,Holenstein F, Sterne J.
No. 2Systematic review of the effectivenessand cost-effectiveness, and economicevaluation, of home versus hospital orsatellite unit haemodialysis for peoplewith end-stage renal failure.
By Mowatt G, Vale L, Perez J, WynessL, Fraser C, MacLeod A, et al.
No. 3Systematic review and economicevaluation of the effectiveness ofinfliximab for the treatment of Crohn’sdisease.
By Clark W, Raftery J, Barton P, Song F, Fry-Smith A, Burls A.
No. 4A review of the clinical effectiveness andcost-effectiveness of routine anti-Dprophylaxis for pregnant women whoare rhesus negative.
By Chilcott J, Lloyd Jones M, WightJ, Forman K, Wray J, Beverley C, et al.
No. 5Systematic review and evaluation of theuse of tumour markers in paediatriconcology: Ewing’s sarcoma andneuroblastoma.
By Riley RD, Burchill SA, Abrams KR,Heney D, Lambert PC, Jones DR, et al.
No. 6The cost-effectiveness of screening forHelicobacter pylori to reduce mortalityand morbidity from gastric cancer andpeptic ulcer disease: a discrete-eventsimulation model.
By Roderick P, Davies R, Raftery J,Crabbe D, Pearce R, Bhandari P, et al.
No. 7The clinical effectiveness and cost-effectiveness of routine dental checks: asystematic review and economicevaluation.
By Davenport C, Elley K, Salas C,Taylor-Weetman CL, Fry-Smith A, Bryan S, et al.
No. 8A multicentre randomised controlledtrial assessing the costs and benefits ofusing structured information andanalysis of women’s preferences in themanagement of menorrhagia.
By Kennedy ADM, Sculpher MJ,Coulter A, Dwyer N, Rees M, Horsley S, et al.
No. 9Clinical effectiveness and cost–utility ofphotodynamic therapy for wet age-relatedmacular degeneration: a systematic reviewand economic evaluation.
By Meads C, Salas C, Roberts T,Moore D, Fry-Smith A, Hyde C.
No. 10Evaluation of molecular tests forprenatal diagnosis of chromosomeabnormalities.
By Grimshaw GM, Szczepura A,Hultén M, MacDonald F, Nevin NC,Sutton F, et al.
Health Technology Assessment reports published to date
124

No. 11First and second trimester antenatalscreening for Down’s syndrome: theresults of the Serum, Urine andUltrasound Screening Study (SURUSS).
By Wald NJ, Rodeck C, Hackshaw AK, Walters J, Chitty L,Mackinson AM.
No. 12The effectiveness and cost-effectivenessof ultrasound locating devices forcentral venous access: a systematicreview and economic evaluation.
By Calvert N, Hind D, McWilliamsRG, Thomas SM, Beverley C, Davidson A.
No. 13A systematic review of atypicalantipsychotics in schizophrenia.
By Bagnall A-M, Jones L, Lewis R,Ginnelly L, Glanville J, Torgerson D, et al.
No. 14Prostate Testing for Cancer andTreatment (ProtecT) feasibility study.
By Donovan J, Hamdy F, Neal D,Peters T, Oliver S, Brindle L, et al.
No. 15Early thrombolysis for the treatment of acute myocardial infarction: asystematic review and economicevaluation.
By Boland A, Dundar Y, Bagust A,Haycox A, Hill R, Mujica Mota R,et al.
No. 16Screening for fragile X syndrome: a literature review and modelling.
By Song FJ, Barton P, Sleightholme V,Yao GL, Fry-Smith A.
No. 17Systematic review of endoscopic sinussurgery for nasal polyps.
By Dalziel K, Stein K, Round A,Garside R, Royle P.
No. 18Towards efficient guidelines: how tomonitor guideline use in primary care.
By Hutchinson A, McIntosh A, Cox S,Gilbert C.
No. 19Effectiveness and cost-effectiveness ofacute hospital-based spinal cord injuriesservices: systematic review.
By Bagnall A-M, Jones L, Richardson G, Duffy S, Riemsma R.
No. 20Prioritisation of health technologyassessment. The PATHS model:methods and case studies.
By Townsend J, Buxton M, Harper G.
No. 21Systematic review of the clinicaleffectiveness and cost-effectiveness of tension-free vaginal tape fortreatment of urinary stress incontinence.
By Cody J, Wyness L, Wallace S,Glazener C, Kilonzo M, Stearns S,et al.
No. 22The clinical and cost-effectiveness ofpatient education models for diabetes: a systematic review and economicevaluation.
By Loveman E, Cave C, Green C,Royle P, Dunn N, Waugh N.
No. 23The role of modelling in prioritisingand planning clinical trials.
By Chilcott J, Brennan A, Booth A,Karnon J, Tappenden P.
No. 24Cost–benefit evaluation of routineinfluenza immunisation in people 65–74years of age.
By Allsup S, Gosney M, Haycox A,Regan M.
No. 25The clinical and cost-effectiveness ofpulsatile machine perfusion versus coldstorage of kidneys for transplantationretrieved from heart-beating and non-heart-beating donors.
By Wight J, Chilcott J, Holmes M,Brewer N.
No. 26Can randomised trials rely on existingelectronic data? A feasibility study toexplore the value of routine data inhealth technology assessment.
By Williams JG, Cheung WY, Cohen DR, Hutchings HA, Longo MF, Russell IT.
No. 27Evaluating non-randomised interventionstudies.
By Deeks JJ, Dinnes J, D’Amico R,Sowden AJ, Sakarovitch C, Song F, et al.
No. 28A randomised controlled trial to assessthe impact of a package comprising apatient-orientated, evidence-based self-help guidebook and patient-centredconsultations on disease managementand satisfaction in inflammatory boweldisease.
By Kennedy A, Nelson E, Reeves D,Richardson G, Roberts C, Robinson A,et al.
No. 29The effectiveness of diagnostic tests forthe assessment of shoulder pain due tosoft tissue disorders: a systematic review.
By Dinnes J, Loveman E, McIntyre L,Waugh N.
No. 30The value of digital imaging in diabeticretinopathy.
By Sharp PF, Olson J, Strachan F,Hipwell J, Ludbrook A, O’Donnell M, et al.
No. 31Lowering blood pressure to preventmyocardial infarction and stroke: a new preventive strategy.
By Law M, Wald N, Morris J.
No. 32Clinical and cost-effectiveness ofcapecitabine and tegafur with uracil forthe treatment of metastatic colorectalcancer: systematic review and economicevaluation.
By Ward S, Kaltenthaler E, Cowan J,Brewer N.
No. 33Clinical and cost-effectiveness of new and emerging technologies for earlylocalised prostate cancer: a systematicreview.
By Hummel S, Paisley S, Morgan A,Currie E, Brewer N.
No. 34Literature searching for clinical andcost-effectiveness studies used in healthtechnology assessment reports carriedout for the National Institute forClinical Excellence appraisal system.
By Royle P, Waugh N.
No. 35Systematic review and economicdecision modelling for the preventionand treatment of influenza A and B.
By Turner D, Wailoo A, Nicholson K,Cooper N, Sutton A, Abrams K.
No. 36A randomised controlled trial toevaluate the clinical and cost-effectiveness of Hickman line insertions in adult cancer patients bynurses.
By Boland A, Haycox A, Bagust A,Fitzsimmons L.
No. 37Redesigning postnatal care: arandomised controlled trial of protocol-based midwifery-led carefocused on individual women’s physical and psychological health needs.
By MacArthur C, Winter HR, Bick DE, Lilford RJ, Lancashire RJ,Knowles H, et al.
No. 38Estimating implied rates of discount inhealthcare decision-making.
By West RR, McNabb R, Thompson AGH, Sheldon TA, Grimley Evans J.
Health Technology Assessment 2008; Vol. 12: No. 30
125
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

No. 39Systematic review of isolation policies inthe hospital management of methicillin-resistant Staphylococcus aureus: a review ofthe literature with epidemiological andeconomic modelling.
By Cooper BS, Stone SP, Kibbler CC,Cookson BD, Roberts JA, Medley GF, et al.
No. 40Treatments for spasticity and pain inmultiple sclerosis: a systematic review.
By Beard S, Hunn A, Wight J.
No. 41The inclusion of reports of randomisedtrials published in languages other thanEnglish in systematic reviews.
By Moher D, Pham B, Lawson ML,Klassen TP.
No. 42The impact of screening on futurehealth-promoting behaviours and healthbeliefs: a systematic review.
By Bankhead CR, Brett J, Bukach C,Webster P, Stewart-Brown S, Munafo M,et al.
Volume 8, 2004
No. 1What is the best imaging strategy foracute stroke?
By Wardlaw JM, Keir SL, Seymour J,Lewis S, Sandercock PAG, Dennis MS, et al.
No. 2Systematic review and modelling of theinvestigation of acute and chronic chestpain presenting in primary care.
By Mant J, McManus RJ, Oakes RAL,Delaney BC, Barton PM, Deeks JJ, et al.
No. 3The effectiveness and cost-effectivenessof microwave and thermal balloonendometrial ablation for heavymenstrual bleeding: a systematic reviewand economic modelling.
By Garside R, Stein K, Wyatt K,Round A, Price A.
No. 4A systematic review of the role ofbisphosphonates in metastatic disease.
By Ross JR, Saunders Y, Edmonds PM,Patel S, Wonderling D, Normand C, et al.
No. 5Systematic review of the clinicaleffectiveness and cost-effectiveness ofcapecitabine (Xeloda®) for locallyadvanced and/or metastatic breast cancer.
By Jones L, Hawkins N, Westwood M,Wright K, Richardson G, Riemsma R.
No. 6Effectiveness and efficiency of guidelinedissemination and implementationstrategies.
By Grimshaw JM, Thomas RE,MacLennan G, Fraser C, Ramsay CR,Vale L, et al.
No. 7Clinical effectiveness and costs of theSugarbaker procedure for the treatmentof pseudomyxoma peritonei.
By Bryant J, Clegg AJ, Sidhu MK,Brodin H, Royle P, Davidson P.
No. 8Psychological treatment for insomnia inthe regulation of long-term hypnoticdrug use.
By Morgan K, Dixon S, Mathers N,Thompson J, Tomeny M.
No. 9Improving the evaluation of therapeuticinterventions in multiple sclerosis:development of a patient-based measureof outcome.
By Hobart JC, Riazi A, Lamping DL,Fitzpatrick R, Thompson AJ.
No. 10A systematic review and economicevaluation of magnetic resonancecholangiopancreatography comparedwith diagnostic endoscopic retrogradecholangiopancreatography.
By Kaltenthaler E, Bravo Vergel Y,Chilcott J, Thomas S, Blakeborough T,Walters SJ, et al.
No. 11The use of modelling to evaluate newdrugs for patients with a chroniccondition: the case of antibodies againsttumour necrosis factor in rheumatoidarthritis.
By Barton P, Jobanputra P, Wilson J,Bryan S, Burls A.
No. 12Clinical effectiveness and cost-effectiveness of neonatal screening forinborn errors of metabolism usingtandem mass spectrometry: a systematicreview.
By Pandor A, Eastham J, Beverley C,Chilcott J, Paisley S.
No. 13Clinical effectiveness and cost-effectiveness of pioglitazone androsiglitazone in the treatment of type 2 diabetes: a systematic review and economic evaluation.
By Czoski-Murray C, Warren E,Chilcott J, Beverley C, Psyllaki MA,Cowan J.
No. 14Routine examination of the newborn:the EMREN study. Evaluation of anextension of the midwife role including a randomised controlled trial of appropriately trained midwivesand paediatric senior house officers.
By Townsend J, Wolke D, Hayes J,Davé S, Rogers C, Bloomfield L, et al.
No. 15Involving consumers in research anddevelopment agenda setting for theNHS: developing an evidence-basedapproach.
By Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al.
No. 16A multi-centre randomised controlledtrial of minimally invasive directcoronary bypass grafting versuspercutaneous transluminal coronaryangioplasty with stenting for proximalstenosis of the left anterior descendingcoronary artery.
By Reeves BC, Angelini GD, BryanAJ, Taylor FC, Cripps T, Spyt TJ, et al.
No. 17Does early magnetic resonance imaginginfluence management or improveoutcome in patients referred tosecondary care with low back pain? A pragmatic randomised controlledtrial.
By Gilbert FJ, Grant AM, GillanMGC, Vale L, Scott NW, Campbell MK,et al.
No. 18The clinical and cost-effectiveness ofanakinra for the treatment ofrheumatoid arthritis in adults: asystematic review and economic analysis.
By Clark W, Jobanputra P, Barton P,Burls A.
No. 19A rapid and systematic review andeconomic evaluation of the clinical andcost-effectiveness of newer drugs fortreatment of mania associated withbipolar affective disorder.
By Bridle C, Palmer S, Bagnall A-M,Darba J, Duffy S, Sculpher M, et al.
No. 20Liquid-based cytology in cervicalscreening: an updated rapid andsystematic review and economic analysis.
By Karnon J, Peters J, Platt J, Chilcott J, McGoogan E, Brewer N.
No. 21Systematic review of the long-termeffects and economic consequences oftreatments for obesity and implicationsfor health improvement.
By Avenell A, Broom J, Brown TJ,Poobalan A, Aucott L, Stearns SC, et al.
No. 22Autoantibody testing in children withnewly diagnosed type 1 diabetesmellitus.
By Dretzke J, Cummins C,Sandercock J, Fry-Smith A, Barrett T,Burls A.
Health Technology Assessment reports published to date
126
No. 23Clinical effectiveness and cost-effectiveness of prehospital intravenousfluids in trauma patients.
By Dretzke J, Sandercock J, Bayliss S,Burls A.
No. 24Newer hypnotic drugs for the short-term management of insomnia: asystematic review and economicevaluation.
By Dündar Y, Boland A, Strobl J,Dodd S, Haycox A, Bagust A, et al.
No. 25Development and validation of methodsfor assessing the quality of diagnosticaccuracy studies.
By Whiting P, Rutjes AWS, Dinnes J,Reitsma JB, Bossuyt PMM, Kleijnen J.
No. 26EVALUATE hysterectomy trial: amulticentre randomised trial comparingabdominal, vaginal and laparoscopicmethods of hysterectomy.
By Garry R, Fountain J, Brown J,Manca A, Mason S, Sculpher M, et al.
No. 27Methods for expected value ofinformation analysis in complex healtheconomic models: developments on thehealth economics of interferon-� andglatiramer acetate for multiple sclerosis.
By Tappenden P, Chilcott JB,Eggington S, Oakley J, McCabe C.
No. 28Effectiveness and cost-effectiveness ofimatinib for first-line treatment ofchronic myeloid leukaemia in chronicphase: a systematic review and economicanalysis.
By Dalziel K, Round A, Stein K,Garside R, Price A.
No. 29VenUS I: a randomised controlled trialof two types of bandage for treatingvenous leg ulcers.
By Iglesias C, Nelson EA, Cullum NA,Torgerson DJ on behalf of the VenUSTeam.
No. 30Systematic review of the effectivenessand cost-effectiveness, and economicevaluation, of myocardial perfusionscintigraphy for the diagnosis andmanagement of angina and myocardialinfarction.
By Mowatt G, Vale L, Brazzelli M,Hernandez R, Murray A, Scott N, et al.
No. 31A pilot study on the use of decisiontheory and value of information analysisas part of the NHS Health TechnologyAssessment programme.
By Claxton Kon K, Ginnelly L, SculpherM, Philips Z, Palmer S.
No. 32The Social Support and Family HealthStudy: a randomised controlled trial andeconomic evaluation of two alternativeforms of postnatal support for mothersliving in disadvantaged inner-city areas.
By Wiggins M, Oakley A, Roberts I,Turner H, Rajan L, Austerberry H, et al.
No. 33Psychosocial aspects of genetic screeningof pregnant women and newborns: a systematic review.
By Green JM, Hewison J, Bekker HL,Bryant, Cuckle HS.
No. 34Evaluation of abnormal uterinebleeding: comparison of threeoutpatient procedures within cohortsdefined by age and menopausal status.
By Critchley HOD, Warner P, Lee AJ, Brechin S, Guise J, Graham B.
No. 35Coronary artery stents: a rapid systematicreview and economic evaluation.
By Hill R, Bagust A, Bakhai A,Dickson R, Dündar Y, Haycox A, et al.
No. 36Review of guidelines for good practicein decision-analytic modelling in healthtechnology assessment.
By Philips Z, Ginnelly L, Sculpher M,Claxton K, Golder S, Riemsma R, et al.
No. 37Rituximab (MabThera®) for aggressivenon-Hodgkin’s lymphoma: systematicreview and economic evaluation.
By Knight C, Hind D, Brewer N,Abbott V.
No. 38Clinical effectiveness and cost-effectiveness of clopidogrel andmodified-release dipyridamole in thesecondary prevention of occlusivevascular events: a systematic review andeconomic evaluation.
By Jones L, Griffin S, Palmer S, MainC, Orton V, Sculpher M, et al.
No. 39Pegylated interferon �-2a and -2b incombination with ribavirin in thetreatment of chronic hepatitis C: asystematic review and economicevaluation.
By Shepherd J, Brodin H, Cave C,Waugh N, Price A, Gabbay J.
No. 40Clopidogrel used in combination withaspirin compared with aspirin alone inthe treatment of non-ST-segment-elevation acute coronary syndromes: asystematic review and economicevaluation.
By Main C, Palmer S, Griffin S, Jones L, Orton V, Sculpher M, et al.
No. 41Provision, uptake and cost of cardiacrehabilitation programmes: improvingservices to under-represented groups.
By Beswick AD, Rees K, Griebsch I,Taylor FC, Burke M, West RR, et al.
No. 42Involving South Asian patients inclinical trials.
By Hussain-Gambles M, Leese B,Atkin K, Brown J, Mason S, Tovey P.
No. 43Clinical and cost-effectiveness ofcontinuous subcutaneous insulininfusion for diabetes.
By Colquitt JL, Green C, Sidhu MK,Hartwell D, Waugh N.
No. 44Identification and assessment ofongoing trials in health technologyassessment reviews.
By Song FJ, Fry-Smith A, DavenportC, Bayliss S, Adi Y, Wilson JS, et al.
No. 45Systematic review and economicevaluation of a long-acting insulinanalogue, insulin glargine
By Warren E, Weatherley-Jones E,Chilcott J, Beverley C.
No. 46Supplementation of a home-basedexercise programme with a class-basedprogramme for people with osteoarthritisof the knees: a randomised controlledtrial and health economic analysis.
By McCarthy CJ, Mills PM, Pullen R, Richardson G, Hawkins N,Roberts CR, et al.
No. 47Clinical and cost-effectiveness of once-daily versus more frequent use of samepotency topical corticosteroids for atopiceczema: a systematic review andeconomic evaluation.
By Green C, Colquitt JL, Kirby J,Davidson P, Payne E.
No. 48Acupuncture of chronic headachedisorders in primary care: randomisedcontrolled trial and economic analysis.
By Vickers AJ, Rees RW, Zollman CE,McCarney R, Smith CM, Ellis N, et al.
No. 49Generalisability in economic evaluationstudies in healthcare: a review and casestudies.
By Sculpher MJ, Pang FS, Manca A,Drummond MF, Golder S, Urdahl H, et al.
No. 50Virtual outreach: a randomisedcontrolled trial and economic evaluationof joint teleconferenced medicalconsultations.
By Wallace P, Barber J, Clayton W,Currell R, Fleming K, Garner P, et al.
Health Technology Assessment 2008; Vol. 12: No. 30
127
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

Volume 9, 2005
No. 1Randomised controlled multipletreatment comparison to provide a cost-effectiveness rationale for theselection of antimicrobial therapy inacne.
By Ozolins M, Eady EA, Avery A,Cunliffe WJ, O’Neill C, Simpson NB, et al.
No. 2Do the findings of case series studiesvary significantly according tomethodological characteristics?
By Dalziel K, Round A, Stein K,Garside R, Castelnuovo E, Payne L.
No. 3Improving the referral process forfamilial breast cancer geneticcounselling: findings of threerandomised controlled trials of twointerventions.
By Wilson BJ, Torrance N, Mollison J,Wordsworth S, Gray JR, Haites NE, et al.
No. 4Randomised evaluation of alternativeelectrosurgical modalities to treatbladder outflow obstruction in men withbenign prostatic hyperplasia.
By Fowler C, McAllister W, Plail R,Karim O, Yang Q.
No. 5A pragmatic randomised controlled trialof the cost-effectiveness of palliativetherapies for patients with inoperableoesophageal cancer.
By Shenfine J, McNamee P, Steen N,Bond J, Griffin SM.
No. 6Impact of computer-aided detectionprompts on the sensitivity and specificityof screening mammography.
By Taylor P, Champness J, Given-Wilson R, Johnston K, Potts H.
No. 7Issues in data monitoring and interimanalysis of trials.
By Grant AM, Altman DG, BabikerAB, Campbell MK, Clemens FJ,Darbyshire JH, et al.
No. 8Lay public’s understanding of equipoiseand randomisation in randomisedcontrolled trials.
By Robinson EJ, Kerr CEP, StevensAJ, Lilford RJ, Braunholtz DA, EdwardsSJ, et al.
No. 9Clinical and cost-effectiveness ofelectroconvulsive therapy for depressiveillness, schizophrenia, catatonia andmania: systematic reviews and economicmodelling studies.
By Greenhalgh J, Knight C, Hind D,Beverley C, Walters S.
No. 10Measurement of health-related qualityof life for people with dementia:development of a new instrument(DEMQOL) and an evaluation ofcurrent methodology.
By Smith SC, Lamping DL, Banerjee S, Harwood R, Foley B, Smith P, et al.
No. 11Clinical effectiveness and cost-effectiveness of drotrecogin alfa(activated) (Xigris®) for the treatment ofsevere sepsis in adults: a systematicreview and economic evaluation.
By Green C, Dinnes J, Takeda A,Shepherd J, Hartwell D, Cave C, et al.
No. 12A methodological review of howheterogeneity has been examined insystematic reviews of diagnostic testaccuracy.
By Dinnes J, Deeks J, Kirby J,Roderick P.
No. 13Cervical screening programmes: canautomation help? Evidence fromsystematic reviews, an economic analysisand a simulation modelling exerciseapplied to the UK.
By Willis BH, Barton P, Pearmain P,Bryan S, Hyde C.
No. 14Laparoscopic surgery for inguinalhernia repair: systematic review ofeffectiveness and economic evaluation.
By McCormack K, Wake B, Perez J,Fraser C, Cook J, McIntosh E, et al.
No. 15Clinical effectiveness, tolerability andcost-effectiveness of newer drugs forepilepsy in adults: a systematic reviewand economic evaluation.
By Wilby J, Kainth A, Hawkins N,Epstein D, McIntosh H, McDaid C, et al.
No. 16A randomised controlled trial tocompare the cost-effectiveness oftricyclic antidepressants, selectiveserotonin reuptake inhibitors andlofepramine.
By Peveler R, Kendrick T, Buxton M,Longworth L, Baldwin D, Moore M, et al.
No. 17Clinical effectiveness and cost-effectiveness of immediate angioplastyfor acute myocardial infarction:systematic review and economicevaluation.
By Hartwell D, Colquitt J, LovemanE, Clegg AJ, Brodin H, Waugh N, et al.
No. 18A randomised controlled comparison ofalternative strategies in stroke care.
By Kalra L, Evans A, Perez I, Knapp M, Swift C, Donaldson N.
No. 19The investigation and analysis of criticalincidents and adverse events inhealthcare.
By Woloshynowych M, Rogers S,Taylor-Adams S, Vincent C.
No. 20Potential use of routine databases inhealth technology assessment.
By Raftery J, Roderick P, Stevens A.
No. 21Clinical and cost-effectiveness of newerimmunosuppressive regimens in renaltransplantation: a systematic review andmodelling study.
By Woodroffe R, Yao GL, Meads C,Bayliss S, Ready A, Raftery J, et al.
No. 22A systematic review and economicevaluation of alendronate, etidronate,risedronate, raloxifene and teriparatidefor the prevention and treatment ofpostmenopausal osteoporosis.
By Stevenson M, Lloyd Jones M, De Nigris E, Brewer N, Davis S, Oakley J.
No. 23A systematic review to examine theimpact of psycho-educationalinterventions on health outcomes andcosts in adults and children with difficultasthma.
By Smith JR, Mugford M, Holland R,Candy B, Noble MJ, Harrison BDW, et al.
No. 24An evaluation of the costs, effectivenessand quality of renal replacementtherapy provision in renal satellite unitsin England and Wales.
By Roderick P, Nicholson T, ArmitageA, Mehta R, Mullee M, Gerard K, et al.
No. 25Imatinib for the treatment of patientswith unresectable and/or metastaticgastrointestinal stromal tumours:systematic review and economicevaluation.
By Wilson J, Connock M, Song F, YaoG, Fry-Smith A, Raftery J, et al.
No. 26Indirect comparisons of competinginterventions.
By Glenny AM, Altman DG, Song F,Sakarovitch C, Deeks JJ, D’Amico R, et al.
No. 27Cost-effectiveness of alternativestrategies for the initial medicalmanagement of non-ST elevation acutecoronary syndrome: systematic reviewand decision-analytical modelling.
By Robinson M, Palmer S, SculpherM, Philips Z, Ginnelly L, Bowens A, et al.
Health Technology Assessment reports published to date
128
No. 28Outcomes of electrically stimulatedgracilis neosphincter surgery.
By Tillin T, Chambers M, Feldman R.
No. 29The effectiveness and cost-effectivenessof pimecrolimus and tacrolimus foratopic eczema: a systematic review andeconomic evaluation.
By Garside R, Stein K, Castelnuovo E,Pitt M, Ashcroft D, Dimmock P, et al.
No. 30Systematic review on urine albumintesting for early detection of diabeticcomplications.
By Newman DJ, Mattock MB, DawnayABS, Kerry S, McGuire A, Yaqoob M, et al.
No. 31Randomised controlled trial of the cost-effectiveness of water-based therapy forlower limb osteoarthritis.
By Cochrane T, Davey RC, Matthes Edwards SM.
No. 32Longer term clinical and economicbenefits of offering acupuncture care topatients with chronic low back pain.
By Thomas KJ, MacPherson H,Ratcliffe J, Thorpe L, Brazier J,Campbell M, et al.
No. 33Cost-effectiveness and safety of epiduralsteroids in the management of sciatica.
By Price C, Arden N, Coglan L,Rogers P.
No. 34The British Rheumatoid Outcome StudyGroup (BROSG) randomised controlledtrial to compare the effectiveness andcost-effectiveness of aggressive versussymptomatic therapy in establishedrheumatoid arthritis.
By Symmons D, Tricker K, Roberts C,Davies L, Dawes P, Scott DL.
No. 35Conceptual framework and systematicreview of the effects of participants’ andprofessionals’ preferences in randomisedcontrolled trials.
By King M, Nazareth I, Lampe F,Bower P, Chandler M, Morou M, et al.
No. 36The clinical and cost-effectiveness ofimplantable cardioverter defibrillators: a systematic review.
By Bryant J, Brodin H, Loveman E,Payne E, Clegg A.
No. 37A trial of problem-solving by communitymental health nurses for anxiety,depression and life difficulties amonggeneral practice patients. The CPN-GPstudy.
By Kendrick T, Simons L, Mynors-Wallis L, Gray A, Lathlean J,Pickering R, et al.
No. 38The causes and effects of socio-demographic exclusions from clinicaltrials.
By Bartlett C, Doyal L, Ebrahim S,Davey P, Bachmann M, Egger M, et al.
No. 39Is hydrotherapy cost-effective? Arandomised controlled trial of combinedhydrotherapy programmes comparedwith physiotherapy land techniques inchildren with juvenile idiopathicarthritis.
By Epps H, Ginnelly L, Utley M,Southwood T, Gallivan S, Sculpher M, et al.
No. 40A randomised controlled trial and cost-effectiveness study of systematicscreening (targeted and total populationscreening) versus routine practice forthe detection of atrial fibrillation inpeople aged 65 and over. The SAFEstudy.
By Hobbs FDR, Fitzmaurice DA,Mant J, Murray E, Jowett S, Bryan S, et al.
No. 41Displaced intracapsular hip fractures in fit, older people: a randomisedcomparison of reduction and fixation,bipolar hemiarthroplasty and total hiparthroplasty.
By Keating JF, Grant A, Masson M,Scott NW, Forbes JF.
No. 42Long-term outcome of cognitivebehaviour therapy clinical trials incentral Scotland.
By Durham RC, Chambers JA, Power KG, Sharp DM, Macdonald RR,Major KA, et al.
No. 43The effectiveness and cost-effectivenessof dual-chamber pacemakers comparedwith single-chamber pacemakers forbradycardia due to atrioventricularblock or sick sinus syndrome: systematic review and economicevaluation.
By Castelnuovo E, Stein K, Pitt M,Garside R, Payne E.
No. 44Newborn screening for congenital heartdefects: a systematic review and cost-effectiveness analysis.
By Knowles R, Griebsch I, DezateuxC, Brown J, Bull C, Wren C.
No. 45The clinical and cost-effectiveness of leftventricular assist devices for end-stageheart failure: a systematic review andeconomic evaluation.
By Clegg AJ, Scott DA, Loveman E,Colquitt J, Hutchinson J, Royle P, et al.
No. 46The effectiveness of the HeidelbergRetina Tomograph and laser diagnosticglaucoma scanning system (GDx) indetecting and monitoring glaucoma.
By Kwartz AJ, Henson DB, Harper RA, Spencer AF, McLeod D.
No. 47Clinical and cost-effectiveness ofautologous chondrocyte implantationfor cartilage defects in knee joints:systematic review and economicevaluation.
By Clar C, Cummins E, McIntyre L,Thomas S, Lamb J, Bain L, et al.
No. 48Systematic review of effectiveness ofdifferent treatments for childhoodretinoblastoma.
By McDaid C, Hartley S, Bagnall A-M, Ritchie G, Light K,Riemsma R.
No. 49Towards evidence-based guidelines for the prevention of venousthromboembolism: systematic reviews of mechanical methods, oralanticoagulation, dextran and regionalanaesthesia as thromboprophylaxis.
By Roderick P, Ferris G, Wilson K,Halls H, Jackson D, Collins R,et al.
No. 50The effectiveness and cost-effectivenessof parent training/educationprogrammes for the treatment ofconduct disorder, including oppositionaldefiant disorder, in children.
By Dretzke J, Frew E, Davenport C,Barlow J, Stewart-Brown S, Sandercock J, et al.
Volume 10, 2006
No. 1The clinical and cost-effectiveness ofdonepezil, rivastigmine, galantamineand memantine for Alzheimer’s disease.
By Loveman E, Green C, Kirby J,Takeda A, Picot J, Payne E, et al.
No. 2FOOD: a multicentre randomised trialevaluating feeding policies in patientsadmitted to hospital with a recentstroke.
By Dennis M, Lewis S, Cranswick G,Forbes J.
No. 3The clinical effectiveness and cost-effectiveness of computed tomographyscreening for lung cancer: systematicreviews.
By Black C, Bagust A, Boland A,Walker S, McLeod C, De Verteuil R, et al.
Health Technology Assessment 2008; Vol. 12: No. 30
129
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
No. 4A systematic review of the effectivenessand cost-effectiveness of neuroimagingassessments used to visualise the seizure focus in people with refractoryepilepsy being considered for surgery.
By Whiting P, Gupta R, Burch J,Mujica Mota RE, Wright K, Marson A, et al.
No. 5Comparison of conference abstracts and presentations with full-text articles in the health technologyassessments of rapidly evolvingtechnologies.
By Dundar Y, Dodd S, Dickson R,Walley T, Haycox A, Williamson PR.
No. 6Systematic review and evaluation ofmethods of assessing urinaryincontinence.
By Martin JL, Williams KS, AbramsKR, Turner DA, Sutton AJ, Chapple C,et al.
No. 7The clinical effectiveness and cost-effectiveness of newer drugs for childrenwith epilepsy. A systematic review.
By Connock M, Frew E, Evans B-W, Bryan S, Cummins C, Fry-Smith A, et al.
No. 8Surveillance of Barrett’s oesophagus:exploring the uncertainty throughsystematic review, expert workshop andeconomic modelling.
By Garside R, Pitt M, Somerville M,Stein K, Price A, Gilbert N.
No. 9Topotecan, pegylated liposomaldoxorubicin hydrochloride andpaclitaxel for second-line or subsequenttreatment of advanced ovarian cancer: asystematic review and economicevaluation.
By Main C, Bojke L, Griffin S,Norman G, Barbieri M, Mather L, et al.
No. 10Evaluation of molecular techniques in prediction and diagnosis ofcytomegalovirus disease inimmunocompromised patients.
By Szczepura A, Westmoreland D,Vinogradova Y, Fox J, Clark M.
No. 11Screening for thrombophilia in high-risksituations: systematic review and cost-effectiveness analysis. The Thrombosis:Risk and Economic Assessment ofThrombophilia Screening (TREATS)study.
By Wu O, Robertson L, Twaddle S,Lowe GDO, Clark P, Greaves M, et al.
No. 12A series of systematic reviews to informa decision analysis for sampling andtreating infected diabetic foot ulcers.
By Nelson EA, O’Meara S, Craig D,Iglesias C, Golder S, Dalton J, et al.
No. 13Randomised clinical trial, observationalstudy and assessment of cost-effectiveness of the treatment of varicoseveins (REACTIV trial).
By Michaels JA, Campbell WB,Brazier JE, MacIntyre JB, PalfreymanSJ, Ratcliffe J, et al.
No. 14The cost-effectiveness of screening fororal cancer in primary care.
By Speight PM, Palmer S, Moles DR,Downer MC, Smith DH, Henriksson Met al.
No. 15Measurement of the clinical and cost-effectiveness of non-invasive diagnostictesting strategies for deep veinthrombosis.
By Goodacre S, Sampson F, StevensonM, Wailoo A, Sutton A, Thomas S, et al.
No. 16Systematic review of the effectivenessand cost-effectiveness of HealOzone®
for the treatment of occlusal pit/fissurecaries and root caries.
By Brazzelli M, McKenzie L, FieldingS, Fraser C, Clarkson J, Kilonzo M, et al.
No. 17Randomised controlled trials ofconventional antipsychotic versus newatypical drugs, and new atypical drugsversus clozapine, in people withschizophrenia responding poorly to, or intolerant of, current drugtreatment.
By Lewis SW, Davies L, Jones PB,Barnes TRE, Murray RM, Kerwin R, et al.
No. 18Diagnostic tests and algorithms used inthe investigation of haematuria:systematic reviews and economicevaluation.
By Rodgers M, Nixon J, Hempel S,Aho T, Kelly J, Neal D, et al.
No. 19Cognitive behavioural therapy inaddition to antispasmodic therapy forirritable bowel syndrome in primarycare: randomised controlled trial.
By Kennedy TM, Chalder T, McCrone P, Darnley S, Knapp M, Jones RH, et al.
No. 20A systematic review of the clinicaleffectiveness and cost-effectiveness ofenzyme replacement therapies forFabry’s disease andmucopolysaccharidosis type 1.
By Connock M, Juarez-Garcia A, FrewE, Mans A, Dretzke J, Fry-Smith A, et al.
No. 21Health benefits of antiviral therapy formild chronic hepatitis C: randomisedcontrolled trial and economicevaluation.
By Wright M, Grieve R, Roberts J,Main J, Thomas HC on behalf of theUK Mild Hepatitis C Trial Investigators.
No. 22Pressure relieving support surfaces: arandomised evaluation.
By Nixon J, Nelson EA, Cranny G,Iglesias CP, Hawkins K, Cullum NA, et al.
No. 23A systematic review and economicmodel of the effectiveness and cost-effectiveness of methylphenidate,dexamfetamine and atomoxetine for thetreatment of attention deficithyperactivity disorder in children andadolescents.
By King S, Griffin S, Hodges Z,Weatherly H, Asseburg C, Richardson G,et al.
No. 24The clinical effectiveness and cost-effectiveness of enzyme replacementtherapy for Gaucher’s disease: a systematic review.
By Connock M, Burls A, Frew E, Fry-Smith A, Juarez-Garcia A, McCabe C, et al.
No. 25Effectiveness and cost-effectiveness ofsalicylic acid and cryotherapy forcutaneous warts. An economic decisionmodel.
By Thomas KS, Keogh-Brown MR,Chalmers JR, Fordham RJ, Holland RC,Armstrong SJ, et al.
No. 26A systematic literature review of theeffectiveness of non-pharmacologicalinterventions to prevent wandering indementia and evaluation of the ethicalimplications and acceptability of theiruse.
By Robinson L, Hutchings D, CornerL, Beyer F, Dickinson H, Vanoli A, et al.
No. 27A review of the evidence on the effectsand costs of implantable cardioverterdefibrillator therapy in different patientgroups, and modelling of cost-effectiveness and cost–utility for thesegroups in a UK context.
By Buxton M, Caine N, Chase D,Connelly D, Grace A, Jackson C, et al.
Health Technology Assessment reports published to date
130

No. 28Adefovir dipivoxil and pegylatedinterferon alfa-2a for the treatment ofchronic hepatitis B: a systematic reviewand economic evaluation.
By Shepherd J, Jones J, Takeda A,Davidson P, Price A.
No. 29An evaluation of the clinical and cost-effectiveness of pulmonary arterycatheters in patient management inintensive care: a systematic review and arandomised controlled trial.
By Harvey S, Stevens K, Harrison D,Young D, Brampton W, McCabe C, et al.
No. 30Accurate, practical and cost-effectiveassessment of carotid stenosis in the UK.
By Wardlaw JM, Chappell FM,Stevenson M, De Nigris E, Thomas S,Gillard J, et al.
No. 31Etanercept and infliximab for thetreatment of psoriatic arthritis: a systematic review and economicevaluation.
By Woolacott N, Bravo Vergel Y,Hawkins N, Kainth A, Khadjesari Z,Misso K, et al.
No. 32The cost-effectiveness of testing forhepatitis C in former injecting drugusers.
By Castelnuovo E, Thompson-Coon J,Pitt M, Cramp M, Siebert U, Price A, et al.
No. 33Computerised cognitive behaviourtherapy for depression and anxietyupdate: a systematic review andeconomic evaluation.
By Kaltenthaler E, Brazier J, De Nigris E, Tumur I, Ferriter M,Beverley C, et al.
No. 34Cost-effectiveness of using prognosticinformation to select women with breast cancer for adjuvant systemic therapy.
By Williams C, Brunskill S, Altman D,Briggs A, Campbell H, Clarke M, et al.
No. 35Psychological therapies includingdialectical behaviour therapy forborderline personality disorder: a systematic review and preliminaryeconomic evaluation.
By Brazier J, Tumur I, Holmes M,Ferriter M, Parry G, Dent-Brown K, et al.
No. 36Clinical effectiveness and cost-effectiveness of tests for the diagnosisand investigation of urinary tractinfection in children: a systematic reviewand economic model.
By Whiting P, Westwood M, Bojke L,Palmer S, Richardson G, Cooper J, et al.
No. 37Cognitive behavioural therapy inchronic fatigue syndrome: a randomisedcontrolled trial of an outpatient groupprogramme.
By O’Dowd H, Gladwell P, Rogers CA,Hollinghurst S, Gregory A.
No. 38A comparison of the cost-effectiveness offive strategies for the prevention of non-steroidal anti-inflammatory drug-inducedgastrointestinal toxicity: a systematicreview with economic modelling.
By Brown TJ, Hooper L, Elliott RA,Payne K, Webb R, Roberts C, et al.
No. 39The effectiveness and cost-effectivenessof computed tomography screening forcoronary artery disease: systematicreview.
By Waugh N, Black C, Walker S,McIntyre L, Cummins E, Hillis G.
No. 40What are the clinical outcome and cost-effectiveness of endoscopy undertakenby nurses when compared with doctors?A Multi-Institution Nurse EndoscopyTrial (MINuET).
By Williams J, Russell I, Durai D,Cheung W-Y, Farrin A, Bloor K, et al.
No. 41The clinical and cost-effectiveness ofoxaliplatin and capecitabine for theadjuvant treatment of colon cancer:systematic review and economicevaluation.
By Pandor A, Eggington S, Paisley S,Tappenden P, Sutcliffe P.
No. 42A systematic review of the effectivenessof adalimumab, etanercept andinfliximab for the treatment ofrheumatoid arthritis in adults and aneconomic evaluation of their cost-effectiveness.
By Chen Y-F, Jobanputra P, Barton P,Jowett S, Bryan S, Clark W, et al.
No. 43Telemedicine in dermatology: a randomised controlled trial.
By Bowns IR, Collins K, Walters SJ,McDonagh AJG.
No. 44Cost-effectiveness of cell salvage andalternative methods of minimisingperioperative allogeneic bloodtransfusion: a systematic review andeconomic model.
By Davies L, Brown TJ, Haynes S,Payne K, Elliott RA, McCollum C.
No. 45Clinical effectiveness and cost-effectiveness of laparoscopic surgery forcolorectal cancer: systematic reviews andeconomic evaluation.
By Murray A, Lourenco T, de Verteuil R, Hernandez R, Fraser C,McKinley A, et al.
No. 46Etanercept and efalizumab for thetreatment of psoriasis: a systematicreview.
By Woolacott N, Hawkins N, Mason A, Kainth A, Khadjesari Z, Bravo Vergel Y, et al.
No. 47Systematic reviews of clinical decisiontools for acute abdominal pain.
By Liu JLY, Wyatt JC, Deeks JJ,Clamp S, Keen J, Verde P, et al.
No. 48Evaluation of the ventricular assistdevice programme in the UK.
By Sharples L, Buxton M, Caine N,Cafferty F, Demiris N, Dyer M, et al.
No. 49A systematic review and economicmodel of the clinical and cost-effectiveness of immunosuppressivetherapy for renal transplantation inchildren.
By Yao G, Albon E, Adi Y, Milford D,Bayliss S, Ready A, et al.
No. 50Amniocentesis results: investigation ofanxiety. The ARIA trial.
By Hewison J, Nixon J, Fountain J,Cocks K, Jones C, Mason G, et al.
Volume 11, 2007
No. 1Pemetrexed disodium for the treatmentof malignant pleural mesothelioma: a systematic review and economicevaluation.
By Dundar Y, Bagust A, Dickson R,Dodd S, Green J, Haycox A, et al.
No. 2A systematic review and economicmodel of the clinical effectiveness andcost-effectiveness of docetaxel incombination with prednisone orprednisolone for the treatment ofhormone-refractory metastatic prostatecancer.
By Collins R, Fenwick E, Trowman R,Perard R, Norman G, Light K, et al.
No. 3A systematic review of rapid diagnostictests for the detection of tuberculosisinfection.
By Dinnes J, Deeks J, Kunst H,Gibson A, Cummins E, Waugh N, et al.
No. 4The clinical effectiveness and cost-effectiveness of strontium ranelate forthe prevention of osteoporotic fragility fractures in postmenopausalwomen.
By Stevenson M, Davis S, Lloyd-Jones M, Beverley C.
Health Technology Assessment 2008; Vol. 12: No. 30
131
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.
No. 5A systematic review of quantitative andqualitative research on the role andeffectiveness of written informationavailable to patients about individualmedicines.
By Raynor DK, Blenkinsopp A,Knapp P, Grime J, Nicolson DJ, Pollock K, et al.
No. 6Oral naltrexone as a treatment forrelapse prevention in formerly opioid-dependent drug users: a systematic review and economicevaluation.
By Adi Y, Juarez-Garcia A, Wang D,Jowett S, Frew E, Day E, et al.
No. 7Glucocorticoid-induced osteoporosis: a systematic review and cost–utility analysis.
By Kanis JA, Stevenson M, McCloskey EV, Davis S, Lloyd-Jones M.
No. 8Epidemiological, social, diagnostic andeconomic evaluation of populationscreening for genital chlamydial infection.
By Low N, McCarthy A, Macleod J,Salisbury C, Campbell R, Roberts TE, et al.
No. 9Methadone and buprenorphine for themanagement of opioid dependence: a systematic review and economicevaluation.
By Connock M, Juarez-Garcia A,Jowett S, Frew E, Liu Z, Taylor RJ, et al.
No. 10Exercise Evaluation Randomised Trial(EXERT): a randomised trial comparingGP referral for leisure centre-basedexercise, community-based walking andadvice only.
By Isaacs AJ, Critchley JA, See Tai S, Buckingham K, Westley D,Harridge SDR, et al.
No. 11Interferon alfa (pegylated and non-pegylated) and ribavirin for thetreatment of mild chronic hepatitis C: a systematic review and economicevaluation.
By Shepherd J, Jones J, Hartwell D,Davidson P, Price A, Waugh N.
No. 12Systematic review and economicevaluation of bevacizumab andcetuximab for the treatment ofmetastatic colorectal cancer.
By Tappenden P, Jones R, Paisley S,Carroll C.
No. 13A systematic review and economicevaluation of epoetin alfa, epoetin betaand darbepoetin alfa in anaemiaassociated with cancer, especially thatattributable to cancer treatment.
By Wilson J, Yao GL, Raftery J,Bohlius J, Brunskill S, Sandercock J, et al.
No. 14A systematic review and economicevaluation of statins for the preventionof coronary events.
By Ward S, Lloyd Jones M, Pandor A,Holmes M, Ara R, Ryan A, et al.
No. 15A systematic review of the effectivenessand cost-effectiveness of differentmodels of community-based respite care for frail older people and theircarers.
By Mason A, Weatherly H, SpilsburyK, Arksey H, Golder S, Adamson J, et al.
No. 16Additional therapy for young childrenwith spastic cerebral palsy: a randomised controlled trial.
By Weindling AM, Cunningham CC,Glenn SM, Edwards RT, Reeves DJ.
No. 17Screening for type 2 diabetes: literaturereview and economic modelling.
By Waugh N, Scotland G, McNamee P, Gillett M, Brennan A,Goyder E, et al.
No. 18The effectiveness and cost-effectivenessof cinacalcet for secondaryhyperparathyroidism in end-stage renal disease patients on dialysis: asystematic review and economicevaluation.
By Garside R, Pitt M, Anderson R,Mealing S, Roome C, Snaith A, et al.
No. 19The clinical effectiveness and cost-effectiveness of gemcitabine formetastatic breast cancer: a systematicreview and economic evaluation.
By Takeda AL, Jones J, Loveman E,Tan SC, Clegg AJ.
No. 20A systematic review of duplexultrasound, magnetic resonanceangiography and computed tomographyangiography for the diagnosis and assessment of symptomatic, lowerlimb peripheral arterial disease.
By Collins R, Cranny G, Burch J,Aguiar-Ibáñez R, Craig D, Wright K, et al.
No. 21The clinical effectiveness and cost-effectiveness of treatments for childrenwith idiopathic steroid-resistantnephrotic syndrome: a systematic review.
By Colquitt JL, Kirby J, Green C,Cooper K, Trompeter RS.
No. 22A systematic review of the routinemonitoring of growth in children ofprimary school age to identify growth-related conditions.
By Fayter D, Nixon J, Hartley S,Rithalia A, Butler G, Rudolf M, et al.
No. 23Systematic review of the effectiveness ofpreventing and treating Staphylococcusaureus carriage in reducing peritonealcatheter-related infections.
By McCormack K, Rabindranath K,Kilonzo M, Vale L, Fraser C, McIntyre L,et al.
No. 24The clinical effectiveness and cost ofrepetitive transcranial magneticstimulation versus electroconvulsivetherapy in severe depression: a multicentre pragmatic randomisedcontrolled trial and economic analysis.
By McLoughlin DM, Mogg A, Eranti S, Pluck G, Purvis R, Edwards D,et al.
No. 25A randomised controlled trial andeconomic evaluation of direct versusindirect and individual versus groupmodes of speech and language therapyfor children with primary languageimpairment.
By Boyle J, McCartney E, Forbes J,O’Hare A.
No. 26Hormonal therapies for early breastcancer: systematic review and economicevaluation.
By Hind D, Ward S, De Nigris E,Simpson E, Carroll C, Wyld L.
No. 27Cardioprotection against the toxic effects of anthracyclines given tochildren with cancer: a systematic review.
By Bryant J, Picot J, Levitt G, Sullivan I, Baxter L, Clegg A.
No. 28Adalimumab, etanercept and infliximabfor the treatment of ankylosingspondylitis: a systematic review andeconomic evaluation.
By McLeod C, Bagust A, Boland A,Dagenais P, Dickson R, Dundar Y, et al.
Health Technology Assessment reports published to date
132
No. 29Prenatal screening and treatmentstrategies to prevent group Bstreptococcal and other bacterialinfections in early infancy: cost-effectiveness and expected value ofinformation analyses.
By Colbourn T, Asseburg C, Bojke L,Philips Z, Claxton K, Ades AE, et al.
No. 30Clinical effectiveness and cost-effectiveness of bone morphogeneticproteins in the non-healing of fracturesand spinal fusion: a systematic review.
By Garrison KR, Donell S, Ryder J,Shemilt I, Mugford M, Harvey I, et al.
No. 31A randomised controlled trial ofpostoperative radiotherapy followingbreast-conserving surgery in aminimum-risk older population. ThePRIME trial.
By Prescott RJ, Kunkler IH, WilliamsLJ, King CC, Jack W, van der Pol M, et al.
No. 32Current practice, accuracy, effectivenessand cost-effectiveness of the schoolentry hearing screen.
By Bamford J, Fortnum H, Bristow K,Smith J, Vamvakas G, Davies L, et al.
No. 33The clinical effectiveness and cost-effectiveness of inhaled insulin in diabetes mellitus: a systematic review and economic evaluation.
By Black C, Cummins E, Royle P,Philip S, Waugh N.
No. 34Surveillance of cirrhosis forhepatocellular carcinoma: systematicreview and economic analysis.
By Thompson Coon J, Rogers G,Hewson P, Wright D, Anderson R,Cramp M, et al.
No. 35The Birmingham Rehabilitation UptakeMaximisation Study (BRUM). Home-based compared with hospital-basedcardiac rehabilitation in a multi-ethnicpopulation: cost-effectiveness andpatient adherence.
By Jolly K, Taylor R, Lip GYH,Greenfield S, Raftery J, Mant J, et al.
No. 36A systematic review of the clinical,public health and cost-effectiveness of rapid diagnostic tests for thedetection and identification of bacterial intestinal pathogens in faeces and food.
By Abubakar I, Irvine L, Aldus CF, Wyatt GM, Fordham R, Schelenz S, et al.
No. 37A randomised controlled trialexamining the longer-term outcomes ofstandard versus new antiepileptic drugs. The SANAD trial.
By Marson AG, Appleton R, Baker GA,Chadwick DW, Doughty J, Eaton B, et al.
No. 38Clinical effectiveness and cost-effectiveness of different models of managing long-term oralanticoagulation therapy: a systematicreview and economic modelling.
By Connock M, Stevens C, Fry-Smith A,Jowett S, Fitzmaurice D, Moore D, et al.
No. 39A systematic review and economicmodel of the clinical effectiveness andcost-effectiveness of interventions forpreventing relapse in people withbipolar disorder.
By Soares-Weiser K, Bravo Vergel Y,Beynon S, Dunn G, Barbieri M, Duffy S,et al.
No. 40Taxanes for the adjuvant treatment ofearly breast cancer: systematic reviewand economic evaluation.
By Ward S, Simpson E, Davis S, Hind D, Rees A, Wilkinson A.
No. 41The clinical effectiveness and cost-effectiveness of screening for open angleglaucoma: a systematic review andeconomic evaluation.
By Burr JM, Mowatt G, Hernández R,Siddiqui MAR, Cook J, Lourenco T, et al.
No. 42Acceptability, benefit and costs of earlyscreening for hearing disability: a studyof potential screening tests and models.
By Davis A, Smith P, Ferguson M,Stephens D, Gianopoulos I.
No. 43Contamination in trials of educationalinterventions.
By Keogh-Brown MR, BachmannMO, Shepstone L, Hewitt C, Howe A,Ramsay CR, et al.
No. 44Overview of the clinical effectiveness ofpositron emission tomography imagingin selected cancers.
By Facey K, Bradbury I, Laking G,Payne E.
No. 45The effectiveness and cost-effectiveness ofcarmustine implants and temozolomidefor the treatment of newly diagnosedhigh-grade glioma: a systematic reviewand economic evaluation.
By Garside R, Pitt M, Anderson R,Rogers G, Dyer M, Mealing S, et al.
No. 46Drug-eluting stents: a systematic reviewand economic evaluation.
By Hill RA, Boland A, Dickson R, Dündar Y, Haycox A, McLeod C, et al.
No. 47The clinical effectiveness and cost-effectiveness of cardiac resynchronisation(biventricular pacing) for heart failure:systematic review and economic model.
By Fox M, Mealing S, Anderson R,Dean J, Stein K, Price A, et al.
No. 48Recruitment to randomised trials:strategies for trial enrolment andparticipation study. The STEPS study.
By Campbell MK, Snowdon C,Francis D, Elbourne D, McDonald AM,Knight R, et al.
No. 49Cost-effectiveness of functional cardiac testing in the diagnosis andmanagement of coronary artery disease: a randomised controlled trial. The CECaT trial.
By Sharples L, Hughes V, Crean A,Dyer M, Buxton M, Goldsmith K, et al.
No. 50Evaluation of diagnostic tests whenthere is no gold standard. A review ofmethods.
By Rutjes AWS, Reitsma JB,Coomarasamy A, Khan KS, Bossuyt PMM.
No. 51Systematic reviews of the clinicaleffectiveness and cost-effectiveness ofproton pump inhibitors in acute uppergastrointestinal bleeding.
By Leontiadis GI, Sreedharan A,Dorward S, Barton P, Delaney B,Howden CW, et al.
No. 52A review and critique of modelling inprioritising and designing screeningprogrammes.
By Karnon J, Goyder E, Tappenden P,McPhie S, Towers I, Brazier J, et al.
No. 53An assessment of the impact of the NHS Health Technology AssessmentProgramme.
By Hanney S, Buxton M, Green C,Coulson D, Raftery J.
Volume 12, 2008
No. 1A systematic review and economicmodel of switching from non-glycopeptide to glycopeptide antibioticprophylaxis for surgery.
By Cranny G, Elliott R, Weatherly H,Chambers D, Hawkins N, Myers L, et al.
Health Technology Assessment 2008; Vol. 12: No. 30
133
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

No. 2‘Cut down to quit’ with nicotinereplacement therapies in smokingcessation: a systematic review ofeffectiveness and economic analysis.
By Wang D, Connock M, Barton P,Fry-Smith A, Aveyard P, Moore D.
No. 3A systematic review of the effectivenessof strategies for reducing fracture risk inchildren with juvenile idiopathicarthritis with additional data on long-term risk of fracture and cost of diseasemanagement.
By Thornton J, Ashcroft D, O’Neill T, Elliott R, Adams J, Roberts C,et al.
No. 4Does befriending by trained lay workersimprove psychological well-being andquality of life for carers of people with dementia, and at what cost? A randomised controlled trial.
By Charlesworth G, Shepstone L,Wilson E, Thalanany M, Mugford M,Poland F.
No. 5A multi-centre retrospective cohort studycomparing the efficacy, safety and cost-effectiveness of hysterectomy anduterine artery embolisation for thetreatment of symptomatic uterinefibroids. The HOPEFUL study.
By Hirst A, Dutton S, Wu O, Briggs A, Edwards C, Waldenmaier L, et al.
No. 6Methods of prediction and preventionof pre-eclampsia: systematic reviews ofaccuracy and effectiveness literature witheconomic modelling.
By Meads CA, Cnossen JS, Meher S,Juarez-Garcia A, ter Riet G, Duley L, et al.
No. 7The use of economic evaluations inNHS decision-making: a review andempirical investigation.
By Williams I, McIver S, Moore D,Bryan S.
No. 8Stapled haemorrhoidectomy(haemorrhoidopexy) for the treatmentof haemorrhoids: a systematic reviewand economic evaluation.
By Burch J, Epstein D, Baba-Akbari A,Weatherly H, Fox D, Golder S, et al.
No. 9The clinical effectiveness of diabeteseducation models for Type 2 diabetes: a systematic review.
By Loveman E, Frampton GK, Clegg AJ.
No. 10Payment to healthcare professionals forpatient recruitment to trials: systematicreview and qualitative study.
By Raftery J, Bryant J, Powell J, Kerr C, Hawker S.
No. 11Cyclooxygenase-2 selective non-steroidalanti-inflammatory drugs (etodolac,meloxicam, celecoxib, rofecoxib,etoricoxib, valdecoxib and lumiracoxib)for osteoarthritis and rheumatoidarthritis: a systematic review andeconomic evaluation.
By Chen Y-F, Jobanputra P, Barton P,Bryan S, Fry-Smith A, Harris G, et al.
No. 12The clinical effectiveness and cost-effectiveness of central venous catheterstreated with anti-infective agents inpreventing bloodstream infections: a systematic review and economicevaluation.
By Hockenhull JC, Dwan K, BolandA, Smith G, Bagust A, Dündar Y, et al.
No. 13Stepped treatment of older adults onlaxatives. The STOOL trial.
By Mihaylov S, Stark C, McColl E,Steen N, Vanoli A, Rubin G, et al.
No. 14A randomised controlled trial ofcognitive behaviour therapy inadolescents with major depressiontreated by selective serotonin reuptakeinhibitors. The ADAPT trial.
By Goodyer IM, Dubicka B, Wilkinson P, Kelvin R, Roberts C, Byford S, et al.
No. 15The use of irinotecan, oxaliplatin andraltitrexed for the treatment ofadvanced colorectal cancer: systematicreview and economic evaluation.
By Hind D, Tappenden P, Tumur I,Eggington E, Sutcliffe P, Ryan A.
No. 16Ranibizumab and pegaptanib for thetreatment of age-related maculardegeneration: a systematic review andeconomic evaluation.
By Colquitt JL, Jones J, Tan SC,Takeda A, Clegg AJ, Price A.
No. 17Systematic review of the clinicaleffectiveness and cost-effectiveness of64-slice or higher computedtomography angiography as analternative to invasive coronaryangiography in the investigation ofcoronary artery disease.
By Mowatt G, Cummins E, Waugh N,Walker S, Cook J, Jia X, et al.
No. 18Structural neuroimaging in psychosis: a systematic review and economicevaluation.
By Albon E, Tsourapas A, Frew E,Davenport C, Oyebode F, Bayliss S, et al.
No. 19Systematic review and economic analysisof the comparative effectiveness ofdifferent inhaled corticosteroids andtheir usage with long-acting beta2agonists for the treatment of chronicasthma in adults and children aged 12 years and over.
By Shepherd J, Rogers G, Anderson R,Main C, Thompson-Coon J, Hartwell D,et al.
No. 20Systematic review and economic analysisof the comparative effectiveness ofdifferent inhaled corticosteroids andtheir usage with long-acting beta2agonists for the treatment of chronicasthma in children under the age of 12 years.
By Main C, Shepherd J, Anderson R,Rogers G, Thompson-Coon J, Liu Z, et al.
No. 21Ezetimibe for the treatment ofhypercholesterolaemia: a systematicreview and economic evaluation.
By Ara R, Tumur I, Pandor A, Duenas A, Williams R, Wilkinson A, et al.
No. 22Topical or oral ibuprofen for chronicknee pain in older people. The TOIBstudy.
By Underwood M, Ashby D, Carnes D,Castelnuovo E, Cross P, Harding G, et al.
No. 23A prospective randomised comparisonof minor surgery in primary andsecondary care. The MiSTIC trial.
By George S, Pockney P, Primrose J,Smith H, Little P, Kinley H, et al.
No. 24A review and critical appraisal ofmeasures of therapist–patientinteractions in mental health settings.
By Cahill J, Barkham M, Hardy G,Gilbody S, Richards D, Bower P, et al.
No. 25The clinical effectiveness and cost-effectiveness of screening programmesfor amblyopia and strabismus inchildren up to the age of 4–5 years: a systematic review and economicevaluation.
By Carlton J, Karnon J, Czoski-Murray C, Smith KJ, Marr J.
Health Technology Assessment reports published to date
134

No. 26A systematic review of the clinicaleffectiveness and cost-effectiveness andeconomic modelling of minimal incisiontotal hip replacement approaches in the management of arthritic disease ofthe hip.
By de Verteuil R, Imamura M, Zhu S,Glazener C, Fraser C, Munro N, et al.
No. 27A preliminary model-based assessmentof the cost–utility of a screeningprogramme for early age-relatedmacular degeneration.
By Karnon J, Czoski-Murray C, Smith K, Brand C, Chakravarthy U,Davis S, et al.
No. 28Intravenous magnesium sulphate andsotalol for prevention of atrialfibrillation after coronary artery bypasssurgery: a systematic review andeconomic evaluation.
By Shepherd J, Jones J, Frampton GK, Tanajewski L, Turner D,Price A.
No. 29Absorbent products for urinary/faecalincontinence: a comparative evaluationof key product categories.
By Fader M, Cottenden A, Getliffe K,Gage H, Clarke-O’Neill S, Jamieson K,et al.
No. 30A systematic review of repetitivefunctional task practice with modellingof resource use, costs and effectiveness.
By French B, Leathley M, Sutton C,McAdam J, Thomas L, Forster A, et al.
Health Technology Assessment 2008; Vol. 12: No. 30
135
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.


Health Technology Assessment 2008; Vol. 12: No. 30
137
Health Technology AssessmentProgramme
Prioritisation Strategy GroupMembers
Chair,Professor Tom Walley, Director, NHS HTA Programme,Department of Pharmacology &Therapeutics,University of Liverpool
Professor Bruce Campbell,Consultant Vascular & GeneralSurgeon, Royal Devon & ExeterHospital
Professor Robin E Ferner,Consultant Physician andDirector, West Midlands Centrefor Adverse Drug Reactions,City Hospital NHS Trust,Birmingham
Dr Edmund Jessop, MedicalAdviser, National Specialist,Commissioning Advisory Group(NSCAG), Department ofHealth, London
Professor Jon Nicholl, Director,Medical Care Research Unit,University of Sheffield, School of Health and Related Research
Dr Ron Zimmern, Director,Public Health Genetics Unit,Strangeways ResearchLaboratories, Cambridge
Director, Professor Tom Walley, Director, NHS HTA Programme,Department of Pharmacology &Therapeutics,University of Liverpool
Deputy Director, Professor Jon Nicholl,Director, Medical Care ResearchUnit, University of Sheffield,School of Health and RelatedResearch
HTA Commissioning BoardMembers
Programme Director, Professor Tom Walley, Director, NHS HTA Programme,Department of Pharmacology &Therapeutics,University of Liverpool
Chair,Professor Jon Nicholl,Director, Medical Care ResearchUnit, University of Sheffield,School of Health and RelatedResearch
Deputy Chair, Dr Andrew Farmer, University Lecturer in GeneralPractice, Department of Primary Health Care, University of Oxford
Dr Jeffrey Aronson,Reader in ClinicalPharmacology, Department ofClinical Pharmacology,Radcliffe Infirmary, Oxford
Professor Deborah Ashby,Professor of Medical Statistics,Department of Environmentaland Preventative Medicine,Queen Mary University ofLondon
Professor Ann Bowling,Professor of Health ServicesResearch, Primary Care andPopulation Studies,University College London
Professor John Cairns, Professor of Health Economics,Public Health Policy, London School of Hygiene and Tropical Medicine, London
Professor Nicky Cullum,Director of Centre for EvidenceBased Nursing, Department ofHealth Sciences, University ofYork
Professor Jon Deeks, Professor of Health Statistics,University of Birmingham
Professor Jenny Donovan,Professor of Social Medicine,Department of Social Medicine,University of Bristol
Professor Freddie Hamdy,Professor of Urology, University of Sheffield
Professor Allan House, Professor of Liaison Psychiatry,University of Leeds
Professor Sallie Lamb, Director,Warwick Clinical Trials Unit,University of Warwick
Professor Stuart Logan,Director of Health & SocialCare Research, The PeninsulaMedical School, Universities ofExeter & Plymouth
Professor Miranda Mugford,Professor of Health Economics,University of East Anglia
Dr Linda Patterson, Consultant Physician,Department of Medicine,Burnley General Hospital
Professor Ian Roberts, Professor of Epidemiology &Public Health, InterventionResearch Unit, London Schoolof Hygiene and TropicalMedicine
Professor Mark Sculpher,Professor of Health Economics,Centre for Health Economics,Institute for Research in theSocial Services, University of York
Professor Kate Thomas,Professor of Complementaryand Alternative Medicine,University of Leeds
Professor David John Torgerson,Director of York Trial Unit,Department of Health Sciences,University of York
Professor Hywel Williams,Professor of Dermato-Epidemiology,University of Nottingham
Current and past membership details of all HTA ‘committees’ are available from the HTA website (www.hta.ac.uk)
© Queen’s Printer and Controller of HMSO 2008. All rights reserved.

Health Technology Assessment Programme
138
Diagnostic Technologies & Screening PanelMembers
Chair,Dr Ron Zimmern, Director ofthe Public Health Genetics Unit,Strangeways ResearchLaboratories, Cambridge
Ms Norma Armston,Freelance Consumer Advocate,Bolton
Professor Max Bachmann,Professor of Health CareInterfaces, Department ofHealth Policy and Practice,University of East Anglia
Professor Rudy BilousProfessor of Clinical Medicine &Consultant Physician,The Academic Centre,South Tees Hospitals NHS Trust
Ms Dea Birkett, Service UserRepresentative, London
Dr Paul Cockcroft, ConsultantMedical Microbiologist andClinical Director of Pathology,Department of ClinicalMicrobiology, St Mary'sHospital, Portsmouth
Professor Adrian K Dixon,Professor of Radiology,University Department ofRadiology, University ofCambridge Clinical School
Dr David Elliman, Consultant inCommunity Child Health,Islington PCT & Great OrmondStreet Hospital, London
Professor Glyn Elwyn, Research Chair, Centre forHealth Sciences Research,Cardiff University, Departmentof General Practice, Cardiff
Professor Paul Glasziou,Director, Centre for Evidence-Based Practice,University of Oxford
Dr Jennifer J Kurinczuk,Consultant ClinicalEpidemiologist, NationalPerinatal Epidemiology Unit,Oxford
Dr Susanne M Ludgate, Clinical Director, Medicines &Healthcare Products RegulatoryAgency, London
Mr Stephen Pilling, Director,Centre for Outcomes, Research & Effectiveness, Joint Director, NationalCollaborating Centre for MentalHealth, University CollegeLondon
Mrs Una Rennard, Service User Representative,Oxford
Dr Phil Shackley, SeniorLecturer in Health Economics,Academic Vascular Unit,University of Sheffield
Dr Margaret Somerville,Director of Public HealthLearning, Peninsula MedicalSchool, University of Plymouth
Dr Graham Taylor, ScientificDirector & Senior Lecturer,Regional DNA Laboratory, TheLeeds Teaching Hospitals
Professor Lindsay WilsonTurnbull, Scientific Director,Centre for MR Investigations &YCR Professor of Radiology,University of Hull
Professor Martin J Whittle,Clinical Co-director, NationalCo-ordinating Centre forWomen’s and Childhealth
Dr Dennis Wright, Consultant Biochemist &Clinical Director, The North West LondonHospitals NHS Trust, Middlesex
Pharmaceuticals PanelMembers
Chair,Professor Robin Ferner,Consultant Physician andDirector, West Midlands Centrefor Adverse Drug Reactions, City Hospital NHS Trust,Birmingham
Ms Anne Baileff, ConsultantNurse in First Contact Care,Southampton City Primary CareTrust, University ofSouthampton
Professor Imti Choonara,Professor in Child Health,Academic Division of ChildHealth, University ofNottingham
Professor John Geddes,Professor of EpidemiologicalPsychiatry, University of Oxford
Mrs Barbara Greggains, Non-Executive Director,Greggains Management Ltd
Dr Bill Gutteridge, MedicalAdviser, National SpecialistCommissioning Advisory Group(NSCAG), London
Mrs Sharon Hart, Consultant PharmaceuticalAdviser, Reading
Dr Jonathan Karnon, SeniorResearch Fellow, HealthEconomics and DecisionScience, University of Sheffield
Dr Yoon Loke, Senior Lecturerin Clinical Pharmacology,University of East Anglia
Ms Barbara Meredith,Lay Member, Epsom
Dr Andrew Prentice, SeniorLecturer and ConsultantObstetrician & Gynaecologist,Department of Obstetrics &Gynaecology, University ofCambridge
Dr Frances Rotblat, CPMPDelegate, Medicines &Healthcare Products RegulatoryAgency, London
Dr Martin Shelly, General Practitioner, Leeds
Mrs Katrina Simister, AssistantDirector New Medicines,National Prescribing Centre,Liverpool
Dr Richard Tiner, MedicalDirector, Medical Department,Association of the BritishPharmaceutical Industry,London
Current and past membership details of all HTA ‘committees’ are available from the HTA website (www.hta.ac.uk)

Health Technology Assessment 2008; Vol. 12: No. 30
139
Therapeutic Procedures PanelMembers
Chair, Professor Bruce Campbell,Consultant Vascular andGeneral Surgeon, Departmentof Surgery, Royal Devon &Exeter Hospital
Dr Mahmood Adil, DeputyRegional Director of PublicHealth, Department of Health,Manchester
Dr Aileen Clarke,Consultant in Public Health,Public Health Resource Unit,Oxford
Professor Matthew Cooke,Professor of EmergencyMedicine, Warwick EmergencyCare and Rehabilitation,University of Warwick
Mr Mark Emberton, SeniorLecturer in OncologicalUrology, Institute of Urology,University College Hospital
Professor Paul Gregg,Professor of OrthopaedicSurgical Science, Department ofGeneral Practice and PrimaryCare, South Tees Hospital NHSTrust, Middlesbrough
Ms Maryann L Hardy, Lecturer, Division ofRadiography, University ofBradford
Dr Simon de Lusignan,Senior Lecturer, Primary CareInformatics, Department ofCommunity Health Sciences,St George’s Hospital MedicalSchool, London
Dr Peter Martin, ConsultantNeurologist, Addenbrooke’sHospital, Cambridge
Professor Neil McIntosh,Edward Clark Professor of ChildLife & Health, Department ofChild Life & Health, Universityof Edinburgh
Professor Jim Neilson,Professor of Obstetrics andGynaecology, Department ofObstetrics and Gynaecology,University of Liverpool
Dr John C Pounsford,Consultant Physician,Directorate of Medical Services,North Bristol NHS Trust
Dr Karen Roberts, NurseConsultant, Queen ElizabethHospital, Gateshead
Dr Vimal Sharma, ConsultantPsychiatrist/Hon. Senior Lecturer, Mental HealthResource Centre, Cheshire andWirral Partnership NHS Trust,Wallasey
Professor Scott Weich, Professor of Psychiatry, Division of Health in theCommunity, University ofWarwick
Disease Prevention PanelMembers
Chair, Dr Edmund Jessop, MedicalAdviser, National SpecialistCommissioning Advisory Group(NSCAG), London
Mrs Sheila Clark, ChiefExecutive, St James’s Hospital,Portsmouth
Mr Richard Copeland, Lead Pharmacist: ClinicalEconomy/Interface, Wansbeck General Hospital,Northumberland
Dr Elizabeth Fellow-Smith,Medical Director, West London Mental HealthTrust, Middlesex
Mr Ian Flack, Director PPIForum Support, Council ofEthnic Minority VoluntarySector Organisations, Stratford
Dr John Jackson, General Practitioner, Newcastle upon Tyne
Mrs Veronica James, ChiefOfficer, Horsham District AgeConcern, Horsham
Professor Mike Kelly, Director, Centre for PublicHealth Excellence, National Institute for Healthand Clinical Excellence, London
Professor Yi Mien Koh, Director of Public Health andMedical Director, London NHS (North West LondonStrategic Health Authority),London
Ms Jeanett Martin, Director of Clinical Leadership& Quality, Lewisham PCT,London
Dr Chris McCall, GeneralPractitioner, Dorset
Dr David Pencheon, Director,Eastern Region Public HealthObservatory, Cambridge
Dr Ken Stein, Senior ClinicalLecturer in Public Health,Director, Peninsula TechnologyAssessment Group, University of Exeter, Exeter
Dr Carol Tannahill, Director,Glasgow Centre for PopulationHealth, Glasgow
Professor Margaret Thorogood,Professor of Epidemiology,University of Warwick, Coventry
Dr Ewan Wilkinson, Consultant in Public Health,Royal Liverpool UniversityHospital, Liverpool
Current and past membership details of all HTA ‘committees’ are available from the HTA website (www.hta.ac.uk)
Health Technology Assessment Programme
140Current and past membership details of all HTA ‘committees’ are available from the HTA website (www.hta.ac.uk)
Expert Advisory NetworkMembers
Professor Douglas Altman,Professor of Statistics inMedicine, Centre for Statisticsin Medicine, University ofOxford
Professor John Bond,Director, Centre for HealthServices Research, University ofNewcastle upon Tyne, School ofPopulation & Health Sciences,Newcastle upon Tyne
Professor Andrew Bradbury,Professor of Vascular Surgery,Solihull Hospital, Birmingham
Mr Shaun Brogan, Chief Executive, RidgewayPrimary Care Group, Aylesbury
Mrs Stella Burnside OBE,Chief Executive, Regulation and ImprovementAuthority, Belfast
Ms Tracy Bury, Project Manager, WorldConfederation for PhysicalTherapy, London
Professor Iain T Cameron,Professor of Obstetrics andGynaecology and Head of theSchool of Medicine,University of Southampton
Dr Christine Clark,Medical Writer & ConsultantPharmacist, Rossendale
Professor Collette Clifford,Professor of Nursing & Head ofResearch, School of HealthSciences, University ofBirmingham, Edgbaston,Birmingham
Professor Barry Cookson,Director, Laboratory ofHealthcare Associated Infection,Health Protection Agency,London
Dr Carl Counsell, ClinicalSenior Lecturer in Neurology,Department of Medicine &Therapeutics, University ofAberdeen
Professor Howard Cuckle,Professor of ReproductiveEpidemiology, Department ofPaediatrics, Obstetrics &Gynaecology, University ofLeeds
Dr Katherine Darton, Information Unit, MIND – The Mental Health Charity,London
Professor Carol Dezateux, Professor of PaediatricEpidemiology, London
Dr Keith Dodd, ConsultantPaediatrician, Derby
Mr John Dunning,Consultant CardiothoracicSurgeon, CardiothoracicSurgical Unit, PapworthHospital NHS Trust, Cambridge
Mr Jonothan Earnshaw,Consultant Vascular Surgeon,Gloucestershire Royal Hospital,Gloucester
Professor Martin Eccles, Professor of ClinicalEffectiveness, Centre for HealthServices Research, University ofNewcastle upon Tyne
Professor Pam Enderby,Professor of CommunityRehabilitation, Institute ofGeneral Practice and PrimaryCare, University of Sheffield
Professor Gene Feder, Professorof Primary Care Research &Development, Centre for HealthSciences, Barts & The LondonQueen Mary’s School ofMedicine & Dentistry, London
Mr Leonard R Fenwick, Chief Executive, Newcastleupon Tyne Hospitals NHS Trust
Mrs Gillian Fletcher, Antenatal Teacher & Tutor andPresident, National ChildbirthTrust, Henfield
Professor Jayne Franklyn,Professor of Medicine,Department of Medicine,University of Birmingham,Queen Elizabeth Hospital,Edgbaston, Birmingham
Dr Neville Goodman, Consultant Anaesthetist,Southmead Hospital, Bristol
Professor Robert E Hawkins, CRC Professor and Director ofMedical Oncology, Christie CRCResearch Centre, ChristieHospital NHS Trust, Manchester
Professor Allen Hutchinson, Director of Public Health &Deputy Dean of ScHARR,Department of Public Health,University of Sheffield
Professor Peter Jones, Professorof Psychiatry, University ofCambridge, Cambridge
Professor Stan Kaye, CancerResearch UK Professor ofMedical Oncology, Section ofMedicine, Royal MarsdenHospital & Institute of CancerResearch, Surrey
Dr Duncan Keeley,General Practitioner (Dr Burch& Ptnrs), The Health Centre,Thame
Dr Donna Lamping,Research Degrees ProgrammeDirector & Reader in Psychology,Health Services Research Unit,London School of Hygiene andTropical Medicine, London
Mr George Levvy,Chief Executive, Motor Neurone Disease Association,Northampton
Professor James Lindesay,Professor of Psychiatry for theElderly, University of Leicester,Leicester General Hospital
Professor Julian Little,Professor of Human GenomeEpidemiology, Department ofEpidemiology & CommunityMedicine, University of Ottawa
Professor Rajan Madhok, Consultant in Public Health,South Manchester Primary Care Trust, Manchester
Professor Alexander Markham, Director, Molecular MedicineUnit, St James’s UniversityHospital, Leeds
Professor Alistaire McGuire,Professor of Health Economics,London School of Economics
Dr Peter Moore, Freelance Science Writer, Ashtead
Dr Andrew Mortimore, PublicHealth Director, SouthamptonCity Primary Care Trust,Southampton
Dr Sue Moss, Associate Director,Cancer Screening EvaluationUnit, Institute of CancerResearch, Sutton
Mrs Julietta Patnick, Director, NHS Cancer ScreeningProgrammes, Sheffield
Professor Robert Peveler,Professor of Liaison Psychiatry,Royal South Hants Hospital,Southampton
Professor Chris Price, Visiting Professor in ClinicalBiochemistry, University ofOxford
Professor William Rosenberg,Professor of Hepatology andConsultant Physician, Universityof Southampton, Southampton
Professor Peter Sandercock,Professor of Medical Neurology,Department of ClinicalNeurosciences, University ofEdinburgh
Dr Susan Schonfield, Consultantin Public Health, HillingdonPCT, Middlesex
Dr Eamonn Sheridan,Consultant in Clinical Genetics,Genetics Department,St James’s University Hospital,Leeds
Professor Sarah Stewart-Brown, Professor of Public Health,University of Warwick, Division of Health in theCommunity Warwick MedicalSchool, LWMS, Coventry
Professor Ala Szczepura, Professor of Health ServiceResearch, Centre for HealthServices Studies, University ofWarwick
Dr Ross Taylor, Senior Lecturer, Department ofGeneral Practice and PrimaryCare, University of Aberdeen
Mrs Joan Webster, Consumer member, HTA –Expert Advisory Network

How to obtain copies of this and other HTA Programme reports.An electronic version of this publication, in Adobe Acrobat format, is available for downloading free ofcharge for personal use from the HTA website (http://www.hta.ac.uk). A fully searchable CD-ROM isalso available (see below).
Printed copies of HTA monographs cost £20 each (post and packing free in the UK) to both public andprivate sector purchasers from our Despatch Agents.
Non-UK purchasers will have to pay a small fee for post and packing. For European countries the cost is£2 per monograph and for the rest of the world £3 per monograph.
You can order HTA monographs from our Despatch Agents:
– fax (with credit card or official purchase order) – post (with credit card or official purchase order or cheque)– phone during office hours (credit card only).
Additionally the HTA website allows you either to pay securely by credit card or to print out yourorder and then post or fax it.
Contact details are as follows:HTA Despatch Email: [email protected]/o Direct Mail Works Ltd Tel: 02392 492 0004 Oakwood Business Centre Fax: 02392 478 555Downley, HAVANT PO9 2NP, UK Fax from outside the UK: +44 2392 478 555
NHS libraries can subscribe free of charge. Public libraries can subscribe at a very reduced cost of £100 for each volume (normally comprising 30–40 titles). The commercial subscription rate is £300 per volume. Please see our website for details. Subscriptions can only be purchased for the current orforthcoming volume.
Payment methods
Paying by chequeIf you pay by cheque, the cheque must be in pounds sterling, made payable to Direct Mail Works Ltdand drawn on a bank with a UK address.
Paying by credit cardThe following cards are accepted by phone, fax, post or via the website ordering pages: Delta, Eurocard,Mastercard, Solo, Switch and Visa. We advise against sending credit card details in a plain email.
Paying by official purchase orderYou can post or fax these, but they must be from public bodies (i.e. NHS or universities) within the UK.We cannot at present accept purchase orders from commercial companies or from outside the UK.
How do I get a copy of HTA on CD?
Please use the form on the HTA website (www.hta.ac.uk/htacd.htm). Or contact Direct Mail Works (seecontact details above) by email, post, fax or phone. HTA on CD is currently free of charge worldwide.
The website also provides information about the HTA Programme and lists the membership of the variouscommittees.
HTA

A preliminary model-based assessmentof the cost–utility of a screening programme for early age-related macular degeneration
J Karnon, C Czoski-Murray, K Smith, C Brand, U Chakravarthy, S Davis, N Bansback, C Beverley, A Bird, S Harding, I Chisholm and YC Yang
Health Technology Assessment 2008; Vol. 12: No. 27
HTAHealth Technology AssessmentNHS R&D HTA Programmewww.hta.ac.uk
The National Coordinating Centre for Health Technology Assessment,Alpha House, Enterprise RoadSouthampton Science ParkChilworthSouthampton SO16 7NS, UK.Fax: +44 (0) 23 8059 5639 Email: [email protected]://www.hta.ac.uk ISSN 1366-5278
FeedbackThe HTA Programme and the authors would like to know
your views about this report.
The Correspondence Page on the HTA website(http://www.hta.ac.uk) is a convenient way to publish
your comments. If you prefer, you can send your comments to the address below, telling us whether you would like
us to transfer them to the website.
We look forward to hearing from you.
June 2008
Health Technology Assessm
ent 2008;Vol. 12: No. 27
Cost–utility of a screening program
me for early age-related m
acular degeneration