nhlbi ashma implementation
TRANSCRIPT
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 1/52
Partners Putting Guideline
Into Action
Guidelines Implementation Panel Report for: Expert Panel Report 3—Guidelines for theDiagnosis and Management of Asthma
National Asthma Education and Prevention Program

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 2/52

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 3/52

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 4/52
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 5/52
Table of Contents
Acknowledgments 1
Preface 3
Introduction 5
Background: How Can We Do Better? 5 Objectives o the GIP Report 5
Approach to Evidence Review 6A Call to Action 6
Overview of the GIP Report 7
Convening the Panel 7 Developing the GIP Implementation Plan 7
Framework or Developing GIP Recommendationsand Strategies 7 Core Temes 7 Guiding Principles o Patient-Centered Care 10 Priority Messages 10 Health Disparities: A Fundamental Issue 10 Framework or Mobilizing Asthma Partners into Action 10 Crosscutting Strategies 10 Overarching Implementation Approaches 11 Partnering or Success 11 Evaluating the GIP Implementation Plan 13
The GIP Implementation Plan: Recommendations and Strategies 15 Use Inhaled Corticosteroids 18
Communication 18 Systems Integration 19 Patient/Provider Support 19 Use a Written Asthma Action Plan 20 Communication 20 Systems Integration 22 Patient/Provider Support 22 Assess Asthma Severity 23 Communication 23
Systems Integration 24 Patient/Provider Support 25
Assess and Monitor Asthma Control 25 Communication 25 Systems Integration 27 Patient/Provider Support 27 Schedule Periodic Visits 29
Communication 29 Systems Integration 30 Patient/Provider Support 31

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 6/52
Control Environmental Exposures 32Communication 32Systems Integration 34Patient/Provider Support 35
Appendices 37
A. Levels o Evidence or EPR-3 Recommendations 38B. Patient-Centered Care Model 39C. Health Disparities 42D. Abbreviations 44
List of Figures
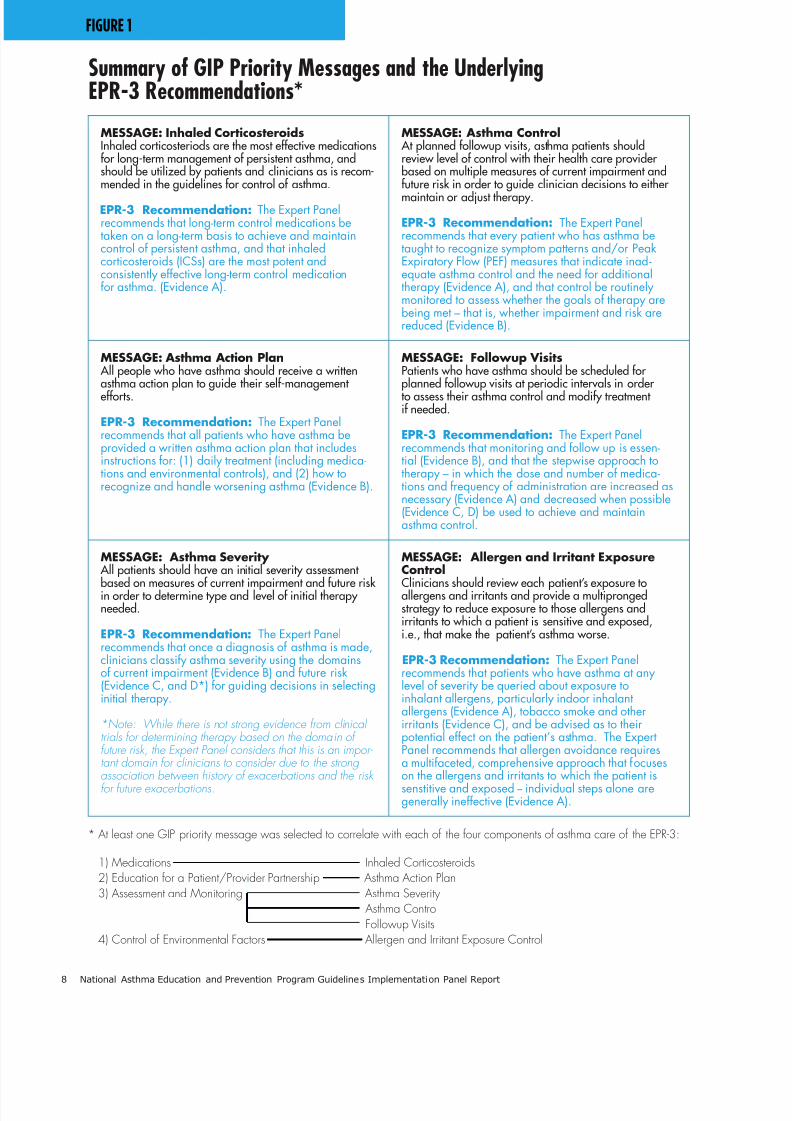
Figure 1. Summary o GIP Priority Messages and the UnderlyingEPR-3 Recommendations* 8
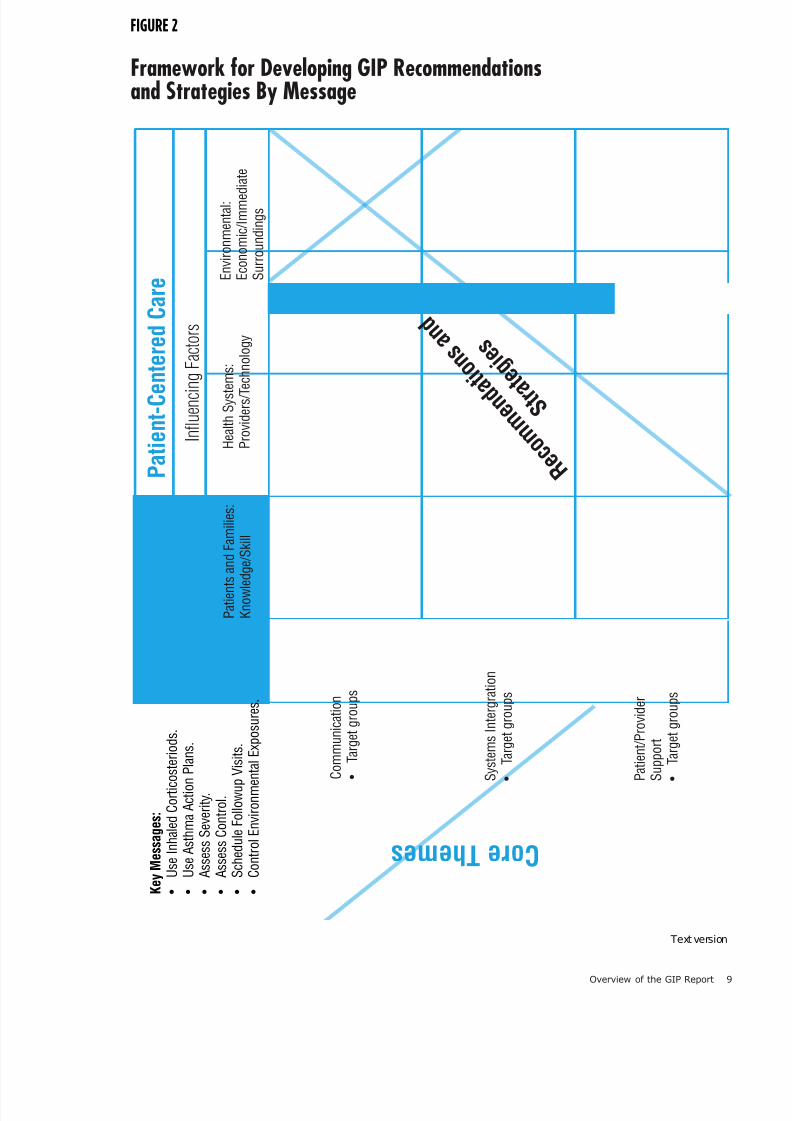
Figure 2. Framework or Developing GIP Recommendationsand Strategies By Message 9
Figure 3. Mobilizing Asthma Partners Into Action —Where Does My Organization Fit? 12
Figure 4. Overview: GIP Report Development Process 14 Figure 5. Integration o GIP Messages and Strategies or
Dynamic Engagement o Stakeholders and a ComprehensiveImplementation Approach 16
Figure 6. Menu o Implementation Activities —What Can My Organization Do? 17
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 7/52
Acknowledgments 1
Acknowledgments
NAEPP Guidelines Implementation Panel
Te NAEPP is grateul to all the Guidelines Imple-mentation Panel members or meeting the chal-lenge o developing this report with tremendousdedication and zeal, and to Dr. Kevin Weiss or hisoutstanding leadership. A special thanks to thewriting team or their extra eort to prepare thisreport.
Kevin B. Weiss, M.D., M.P.H., M.S., Chair *American Board o Medical SpecialtiesEvanston, Illinois
David B. Callahan M.D. *Centers or Disease Control and PreventionAtlanta, Georgia
Michelle M. Cloutier, M.D. *Connecticut Children’s Medical CenterHartord, Connecticut
Denise Dougherty, Ph.D.Agency or Health Care Policy and ResearchRockville, Maryland
Kurtis S. Elward, M.D., M.P.H., F.A.A.F.P. *Family Medicine o AlbemarleCharlottesville, Virginia
David GreenbergCenters or Medicare and Medicaid ServicesBaltimore, Maryland
Carol Jones, R.N., A.E.-C *Certied Asthma Educator Consultantucson, Arizona
Tomas J. Kallstrom, F.A.A.R.C., R.R.., A.E.-CAmerican Association or Respiratory CareIrving, exas
Jim Krieger, M.D., M.P.H. +
University o WashingtonHarborview Medical CenterSeattle, Washington
Marielena Lara, M.D., M.P.H. *Research and Development CorporationSanta Monica, Caliornia
Padmanbhan “Dan” Mukundan, M.D.Access Community Health Network Chicago, Illinois
Judith C. aylor-Fishwick, M.Sc., AE-CNational Respiratory raining CenterNorolk, Virginia
Gwendolyn Parker, M.D.Blue Cross Blue Shield o MichiganSoutheld, Michigan
Gary S. Rachelesky, M.D. *David Geen School o Medicine at UCLALos Angeles, Caliornia
Lawrence D. Robinson, Jr., M.D.Drew University Medical SchoolLong Beach, Caliornia
Susan K. Ross R.N., AE-C ++
Minnesota Department o HealthSt. Paul, Minnesota
James W. Stout, M.D., M.P.H., F.A.A.P.Odessa Brown Children’s ClinicUniversity o WashingtonSeattle, Washington
Te Writing eam:* Authors o Te GIP Implementation Plan:
Recommendations and Strategies + Author o appendix, Health Disparities
++ Author o appendix, Patient-Centered Care Model

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 8/52
2 National Asthma Education and Prevention Program Guidelines Implementation Panel Report

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 9/52
Preface
Te Guidelines Implementation Panel (GIP)Report was developed by a panel convened by theNational Asthma Education and Prevention Pro-gram (NAEPP), coordinated by the National Heart,Lung, and Blood Institute (NHLBI) o the NationalInstitutes o Health. Tis 17-member panel wasselected to represent a wide range o asthmaguideline end users. Members were selected tobring balance and diversity to the GIP report
development process through sharing their uniqueexperiences and varying perspectives. Teir chargewas to identiy barriers to implementing theclinical practice recommendations o the Expert Panel Report 3: Guidelines or the Diagnosis and
Management o Asthma (EPR-3), particularly among primary care providers. Te GIP wastasked to develop recommendations and strategiesor overcoming the barriers, thereby improvingacceptance and utilization o asthma guidelinesoverall.
Major emphases o the GIP Report are to closethe disparity gap or quality asthma care and topromote the principles o patient-centered carewhich includes a medical home or patients andtheir participation with healthcare providers as ullpartners in care. At the heart o the GIP Reportare six key messages derived rom a summary o priority issues that was compiled by the asthmaguidelines Expert Panel and submitted to theGIP. Tese issues were considered to be themost likely ones to result in signicant impact onasthma care processes and outcomes i the broader
asthma community were to ocus its attention andresources on them.
Preface 3
Te GIP Report was developed under theexcellent leadership o Dr. Kevin Weiss, PanelChair. Te NHLBI is grateul or the tremendousdedication o time and outstanding work o all themembers o the GIP as well as other stakeholdergroups (patient education and advocacy groups,proessional societies, voluntary health and gov-ernment organizations) during various review cycles that helped to enhance the utility o this
document.
Ultimately, the broad change in clinical practicedepends on the inuence o local primary carephysicians and other health proessionals whonot only provide state-o-the-art care to theirpatients, but also communicate to their peers theimportance o doing the same. Te NHLBI andits partners will orge new initiatives based onthis document to stimulate adoption o the GIPimplementation recommendations and strategiesat all levels, but particularly with primary care
clinicians at the community level. We ask or theassistance o every reader in reaching our ultimategoal: improving asthma care and the quality o lieor every person who has asthma.
Elizabeth G. Nabel, M.D.Director, National Heart, Lung, and Blood InstituteNational Institutes o Health

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 10/52
4 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 11/52
Introduction 5
Introduction
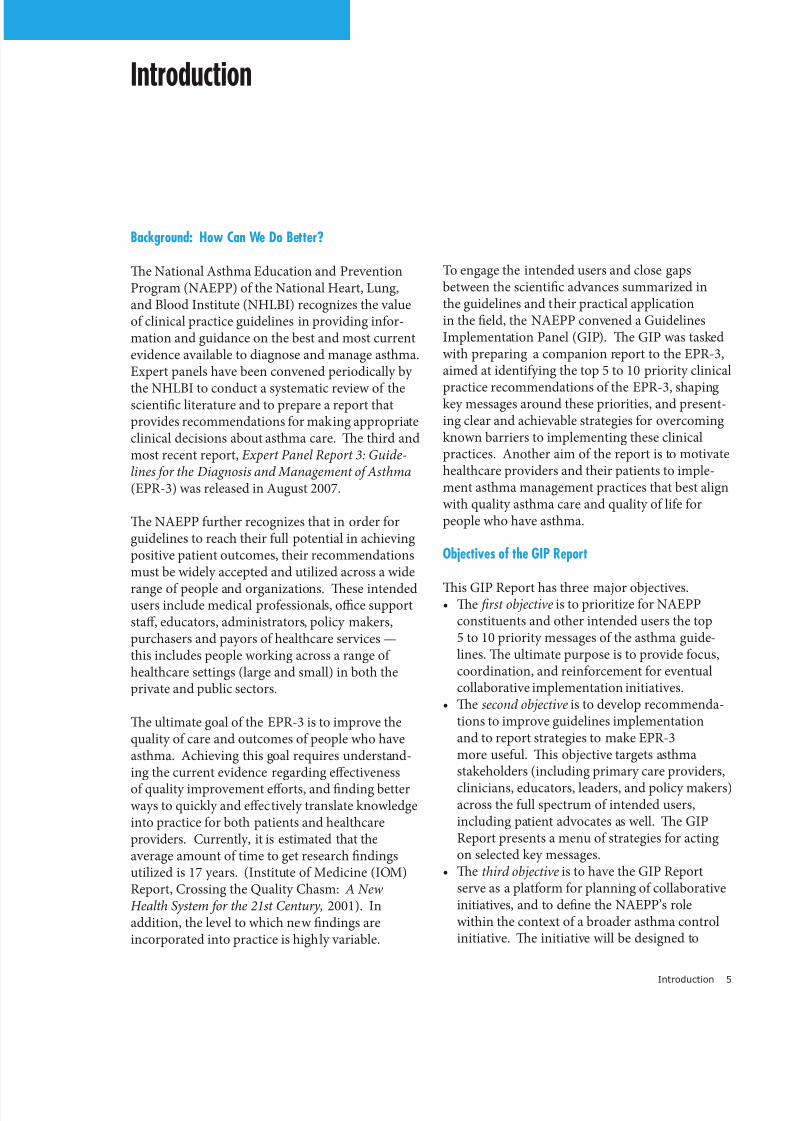
Background: How Can We Do Better?
Te National Asthma Education and PreventionProgram (NAEPP) o the National Heart, Lung,and Blood Institute (NHLBI) recognizes the valueo clinical practice guidelines in providing inor-mation and guidance on the best and most currentevidence available to diagnose and manage asthma.Expert panels have been convened periodically by
the NHLBI to conduct a systematic review o thescientic literature and to prepare a report thatprovides recommendations or making appropriateclinical decisions about asthma care. Te third andmost recent report, Expert Panel Report 3: Guide-lines or the Diagnosis and Management o Asthma(EPR-3) was released in August 2007.
Te NAEPP urther recognizes that in order orguidelines to reach their ull potential in achievingpositive patient outcomes, their recommendationsmust be widely accepted and utilized across a wide
range o people and organizations. Tese intendedusers include medical proessionals, oce supportsta, educators, administrators, policy makers,purchasers and payors o healthcare services —this includes people working across a range o healthcare settings (large and small) in both theprivate and public sectors.
Te ultimate goal o the EPR-3 is to improve thequality o care and outcomes o people who haveasthma. Achieving this goal requires understand-ing the current evidence regarding eectiveness
o quality improvement eorts, and nding betterways to quickly and eectively translate knowledgeinto practice or both patients and healthcareproviders. Currently, it is estimated that theaverage amount o time to get research ndingsutilized is 17 years. (Institute o Medicine (IOM)Report, Crossing the Quality Chasm: A NewHealth System or the 21st Century, 2001). Inaddition, the level to which new ndings areincorporated into practice is highly variable.
o engage the intended users and close gapsbetween the scientic advances summarized inthe guidelines and their practical applicationin the eld, the NAEPP convened a GuidelinesImplementation Panel (GIP). Te GIP was taskedwith preparing a companion report to the EPR-3,aimed at identiying the top 5 to 10 priority clinical
practice recommendations o the EPR-3, shapingkey messages around these priorities, and present-ing clear and achievable strategies or overcomingknown barriers to implementing these clinicalpractices. Another aim o the report is to motivatehealthcare providers and their patients to imple-ment asthma management practices that best alignwith quality asthma care and quality o lie orpeople who have asthma.
Objectives of the GIP Report
Tis GIP Report has three major objectives.• e frst objective is to prioritize or NAEPP
constituents and other intended users the top5 to 10 priority messages o the asthma guide-lines. Te ultimate purpose is to provide ocus,coordination, and reinorcement or eventualcollaborative implementation initiatives.
• esecond objective is to develop recommenda-tions to improve guidelines implementationand to report strategies to make EPR-3more useul. Tis objective targets asthmastakeholders (including primary care providers,
clinicians, educators, leaders, and policy makers)across the ull spectrum o intended users,including patient advocates as well. Te GIPReport presents a menu o strategies or actingon selected key messages.
• ethird objective is to have the GIP Reportserve as a platorm or planning o collaborativeinitiatives, and to dene the NAEPP’s rolewithin the context o a broader asthma controlinitiative. Te initiative will be designed to
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 12/52
6 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
promote partnerships and leadership amongNAEPP’s Coordinating Committee membersand other stakeholders based on the role eachindividual organization wishes to play.
Viewed in this way, the GIP Report provides the
substance and impetus to collectively ocusintended users on several important issues o theEPR-3, that, i implemented widely, could havegreat impact on improving asthma control. Tereport describes ways to apply valuable lessonslearned rom past guidelines implementationeorts. As such, the GIP Report urnishes anopportunity and invites participation within thegreater network o asthma stakeholders to: 1)direct or redirect resources toward a coordinatedapproach that ocuses eorts on activities mostlikely to succeed; 2) seek ways to pool resourcesand collaborate with partners to extend outreachand impact; and, 3) assume leadership and a moreprominent role within the asthma community orimproving guidelines implementation.
Tis report is not an ocial regulatory documento any Government agency. It will be used as theplatorm to implement a national asthma controlinitiative. Approach to Evidence Review.
Successul implementation o the asthma guide-lines can reduce morbidity and improve the quality o lie or people who have asthma as well as pro-mote eciencies and economies o scale or health-care providers. Te EPR-3 used an evidence-basedapproach to enhance acceptability by the widestrange o intended users. Moreover, the guidelinessynthesize the scientic evidence published in thelast 10 years on a comprehensive range o topicsrelated to asthma diagnosis and management.Te guidelines then present conclusions and
recommendations or clinical practice based onthis systematic review.
Several o the research protocols cited and de-scribed in the EPR-3 have tested the outcomes o specic interventions to improve adoption andimplementation o guidelines. Examples include:communicating medical treatments to patients;initiating systems changes or delivery o care; anddening and incorporating core components o
patient/provider education programs, tools, andtechniques into routine care. Rather than conductits own systematic review o asthma guidelinesimplementation research, the GIP used theevidence cited in the EPR-3 and some inorma-tion rom an Agency or Healthcare Research and
Quality analysis o patient education and quality improvement programs in asthma, Closing theQuality Gap: A Critical Analysis o Quality Improvement Strategies, 2007 (Volume 5—Asthma). Where the research was not robust,the GIP drew upon its proessional expertise.
Furthermore, in instances where a recommendedimplementation strategy has a paucity o literatureto ully inorm its use, the GIP Report may suggestthat a ocus group or brie scan o newly publishedliterature be conducted to gather additional knowl-edge prior to implementation. Te objective o theGIP Report was to apply what is already knownand widely accepted rom the published body o literature on guidelines implementation.
A Call to Action.
Te immediate challenges ahead or improvingasthma guidelines utilization are to convert whatwe know rom guidelines’ implementation,
quality improvement, and health care systemsresearch into useul tools, processes and pathways;to incorporate these resources into a system o quality care or patients; and, to build synergy orquality care delivery among asthma stakeholders.Quality asthma care must be readily and eectively delivered by healthcare practitioners and educatorsand augmented and reinorced by other stakehold-ers in the community. We invite you, as a commit-ted asthma care clinician, community practitioner,educator, or decisionmaker, to review this reportand assist in the larger eort o advancing asthma
guidelines implementation and better ensuringasthma control or people who have asthma.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 13/52
Overview of the GIP Report 7
Overview of the GIP Report
Convening the Panel.
In October 2005 the NAEPP appointed a Guide-linesImplementationPanel(GIP).Membersofthe GIP were selected to represent a balanced yetdiverse perspective o asthma stakeholders. Animportant charge to the GIP was to develop anImplementation Plan consisting o recommenda-tions and strategies designed to identiy and
overcome barriers to implementing the EPR-3clinical practice recommendations.
Developing the GIP Implementation Plan.
TheGIPcoordinatedpreparationofitsImplemen-tation Plan with the work o the Expert Panel by selecting six priority messages rom the EPR-3to provide a ocus or uture implementationefforts.Topreparethereport’srecommendationsandstrategies,thesesixtop-linemessagesare integrated with three core themes—communi-
cation,systemsintegration,andpatient-providersupport.Thesixprioritymessagesselectedweredeemed to have sufcient leveraging power topositivelyimpactpatientoutcomes.Thethreethemes were identifed by the GIP as beingassociated with successul healthcare interventions.Figure 1 lists the six priority messagesaccompanied by the specifc EPR-3 clinicalpractice recommendation underlying eachmessage.Thelevelofevidenceforeachofthe EPR -3 clinical practice recommendations isalso given. A description o the various levels
o evidence is provided in Appendix A.
TheGIPexaminedeachofthesixprioritymes-sages with respect to the three core themes in ordertodeterminetargetaudiences,recommendations,and strategies or implementing each message.TheformatforpresentingtheGIPImplementationPlan ollows this outline:• Prioritymessage• Coretheme
• Targetaudience• Recommendation• Strategy(includingpotentialkeypartners)
Framework for Developing GIP Recommenda-tions and Strategies.Theframeworkfordevelopingtherecommenda-tions and strategies o the GIP ImplementationPlanispresentedinFigure2.TheGIPconsidered
each o the six priority messages with respect toeach o the three core themes to develop appropri-ate recommendations and strategies or selectedtargetaudiences.TheGIPalsoagreedthatafun-damental element—the patient’s perspective—wasnecessarytocompletetheframework.Thus,theyidentifed several guiding principles o patient-centered care to serve as a flter or ensuring thatthe patient’s needs and wants would always remaintop priority.
Thecore themes and guiding principles o patient-
centered care o the strategy development rame-work ollow.
Core Themes .ThethreecorethemesidentiedbytheGIP include:• Communication—gettingthemessagesoutonabroadscaletoallaudiences,includingbothpatientsandproviders,inavarietyofsettings.
• SystemsIntegration—designingandcoordinat-ingmessagesforessentialplayersup,down,andacross the operational tiers o a given health
system as well as across multiple health systems;and,strengtheninglinkagesbetweenhealthandcommunity systems.
• Patient/ProviderSupport—identifyingthetools,techniques and other resources that wouldenhance guidelines implementation.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 14/52
FIGURE 1
Summary of GIP Priority Messages and the UnderlyingEPR-3 Recommendations*
Message: Inhaled Corticosteroids Inhaled corticosteriods are the most effective medicationsfor long-term management of persistent asthma, andshould be utilized by patients and clinicians as is recom-
mended in the guidelines for control of asthma.
EPR -3 Recommendation: The Expert Panelrecommends that long-term control medications betaken on a long-term basis to achieve and maintaincontrol of persistent asthma, and that inhaledcorticosteroids (ICSs) are the most potent andconsistently effective long-term control medicationfor asthma. (Evidence A).
Message: Asthma Control At planned followup visits, asthma patients shouldreview level of control with their health care provider based on multiple measures of current impairment andfuture risk in order to guide clinician decisions to either
maintain or adjust therapy.
EPR-3 Rcommtio: The Expert Panelrecommends that every patient who has asthma betaught to recognize symptom patterns and/or PeakExpiratory Flow (PEF) measures that indicate inad-
equate asthma control and the need for additionaltherapy (Evidence A), and that control be routinelymonitored to assess whether the goals of therapy arebeing met – that is, whether impairment and risk arereduced (Evidence B).
Message: Asthma Action Plan All people who have asthma should receive a writtenasthma action plan to guide their self-management efforts.
EPR -3 Rcommtio: The Expert Panelrecommends that all patients who have asthma beprovided a written asthma action plan that includesinstructions for: (1) daily treatment (including medica-
tions and environmental controls), and (2) how torecognize and handle worsening asthma (Evidence B).
Message: Followup ViitPatients who have asthma should be scheduled for planned followup visits at periodic intervals in order to assess their asthma control and modify treatment if needed.
EPR-3 Rcommtio: The Expert Panelrecommends that monitoring and follow up is essen-tial (Evidence B), and that the stepwise approach totherapy – in which the dose and number of medica-
tions and frequency of administration are increased asnecessary (Evidence A) and decreased when possible(Evidence C, D) be used to achieve and maintainasthma control.
Message: Asthma Severity All patients should have an initial severity assessment
based on measures of current impairment and future risk in order to determine type and level of initial therapy needed.
EPR-3 Rcommtio: The Expert Panel recommends that once a diagnosis of asthma is made,clinicians classify asthma severity using the domainsof current impairment (Evidence B) and future risk(Evidence C, and D*) for guiding decisions in selectinginitial therapy.
*Note: While there is not strong evidence from clinical trials for determining therapy based on the domain of future risk, the Expert Panel considers that this is an impor- tant domain for clinicians to consider due to the strongassociation between history of exacerbations and the risk for future exacerbations.
Message: Allergen and Irritant ExposureCotrol Clinicians should review each patient’s exposure toallergens and irritants and provide a multiprongedstrategy to reduce exposure to those allergens andirritants to which a patient is sensitive and exposed,i.e., that make the patient’s asthma worse.
EPR-3 Rcommtio: The Expert Panelrecommends that patients who have asthma at anylevel of severity be queried about exposure toinhalant allergens, particularly indoor inhalantallergens (Evidence A), tobacco smoke and otherirritants (Evidence C), and be advised as to theirpotential effect on the patient’s asthma. The ExpertPanel recommends that allergen avoidance requiresa multifaceted, comprehensive approach that focuseson the allergens and irritants to which the patient issenstitive and exposed -- individual steps alone aregenerally ineffective (Evidence A).
* At least one GIP priority message was selected to correlate with each o the our components o asthma care o the EPR-3:
1) Medications Inhaled Corticosteroids2) Education or a Patient/Provider Partnership Asthma Action Plan3) Assessment and Monitoring Asthma Severity
Asthma ControlFollowup Visits
4) Control o Environmental Factors Allergen and Irritant Exposure Control
8 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 15/52

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 16/52
10 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
Guiding Principles of Patient —Centered Care .Theguidingprinciplesofpatient-centeredcareidentifed by the GIP are as ollows:
• PatientKnowledgeandSkills— ensuring accessto basic health inormation presented in thepatient’s primary language and at an appro-priateliteracylevel,andaccesstoeducational
opportunities or developing appropriate sel-management skills; encouraging and supportingasenseofresponsibilityfor,condencein,andimportance o active participation in one’s ownhealth care.
• HealthcareDeliverySystems— ensuringaccesstosafe,effectivecare;promotingculturalcompetency o healthcare providers andperormance measures that are tied to positivepatient outcomes; utilizing up-to-date technol-ogy or patient/provider education and clinicalinformationsystems;and,encouragingeachpatient who has asthma to have a medical home.
• CommunitySystems—acknowledgingthe immediate environment as exerting importantinuenceoverhealth(e.g.,home,workplace,school,etc.);acknowledgingambulatoryandcommunity-based services as preerable toinstitutional care when clinically appropriate;identiying valuable community resources toaugment health care and to address the socialand fnancial needs o patients; reerringpatients to agencies and services outside o
the clinical setting.
A ull description o the Patient-Centered CareModel can be ound in Appendix B.
Priority Messages .Thesixprioritymessageswereinitiallyderivedrom a summary o overall EPR-3 priority issuesprepared by the Expert Panel to address each o the our essential components o asthma care.GIP members developed an initial list o 22potential messages rom the Expert Panel’s priority
issues summary. GIP members selected thesix priority messages rom the initial list o 22based on the criteria o: strength o evidence asprovided in EPR-3 or the guidelines recommenda-tionunderlyingeachmessage;and,feasibilityofimplementing the message. At least one priority message was selected to correlate with each o thefourcomponentsofasthmacare(seeFigure1).Thesixselectedprioritymessageswereconsideredto be most likely to produce a signifcant impact on
asthma care processes and outcomes i the asthmacommunity were to ocus attention and resourceson active implementation.
Health Disparities: A Fundamental Issue .A undamental issue to address in the contexto all six messages is the reduction o asthmadisparities.Theburdenofasthmaisnotuniform
across all populations. People o racial and ethnicminorities and those o low socioeconomicstatus are disproportionately aected. Asthmaprevalence is 25 percent higher among AmericanIndianorAlaskaNativechildren,60percenthigheramongAfricanAmericanchildren,and140percenthigher among Puerto Rican children relative toWhite children. Arican American children havea260percenthigheremergencydepartment(ED)visit rate and a 250 percent higher hospitalizationrate rom asthma compared to White children.
Access to medical care or asthma and thequality o care provided is oten lower among theminority and socioeconomically disadvantagedpopulations. Exposure to environmental actorsthatworsenasthmaisalsomorefrequent.Thesedisparities in asthma burden and care suggestthat culturally competent clinical and educationalapproaches are needed to implement the EPR-3guidelines in high-risk groups.
A summary paper highlighting important issues
affectingaccessto,andqualityof,healthcareser -vices among disparate populations was developed(seeAppendixC).ThepurposewastoinformGIPdiscussions to better ensure that these importantissues were addressed in the fnal recommenda-tions and strategies or the six priority messages.
Framework for Mobilizing AsthmaPartners into Action.
Crosscutting Strategies .Tofacilitatenavigationthroughthevolumeand
variety o implementation strategies generatedacrossallsixmessages,theGIPidentiedseveralcrosscutting activities any one o which can beintegrated across multiple messages to ormone comprehensive intervention. Listing thesecrosscutting activities is intended to provide stake-holders with a short-hand view o the nature andrangeofGIPrecommendations,therebyhelpingthem more quickly assess which strategies bestalign with the activities o their organization.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 17/52
Overview of the GIP Report 11
Thecrosscuttingactivitiesinclude:• Providingasthmaself-managementeducation topatients,theirfamilies,andtheircaregivers
• Providingclinicalpracticeandcommunicationskills-building education to clinicians andancillary healthcare proessionals
• Employingqualityimprovementstrategies• Supportingstructuresforasthmacarenancing
• Buildingnewandutilizingexistingcommunica-tion networks
Overarching Implementation Approaches .Furthermore,theGIPidentiedthreeoverarchingapproaches to eect implementation o the recom-mendationsandstrategies.Theseoverarching approaches are intended to oer the utility neededto organize and coordinate eorts in carrying outthe GIP Implementation Plan on a broad scale.Theoverarchingapproachesareto:• StimulateandcoordinateNAEPPinitiatives,partnerships,andcollaborativeactivities to acilitate implementation o the GIPImplementation Plan.
• Develop,implement,andevaluateacoordinatednationalasthmacampaigntoeducatethepublic,patients,caregivers,healthcarepractitioners,educators,employers,andadministrators about the 6 priority messages o the EPR-3 asidentifed in the GIP Implementation Plan.
• Conveneanationalasthmapolicyforumtoinclude entities such as commercial and public
healthplans,professionalassociations,expertsinperformancemeasurement,publicand privatehealthcarenancingorganizations,patientadvocacygroups,employers,workplaceadvocacygroups,stateandlocalpolicy makers,environmental,school,andother national,stateandlocalagencies.Theforumwould eature expertise in public health andhealth policy and promote the implementationo policies that advance the asthmaguideline implementation initiative.
How well these overarching approaches align withanorganization’smission,goals,andresourceswillhelp an organization determine where it best fts inthe larger scheme o the GIP Implementation Plan.
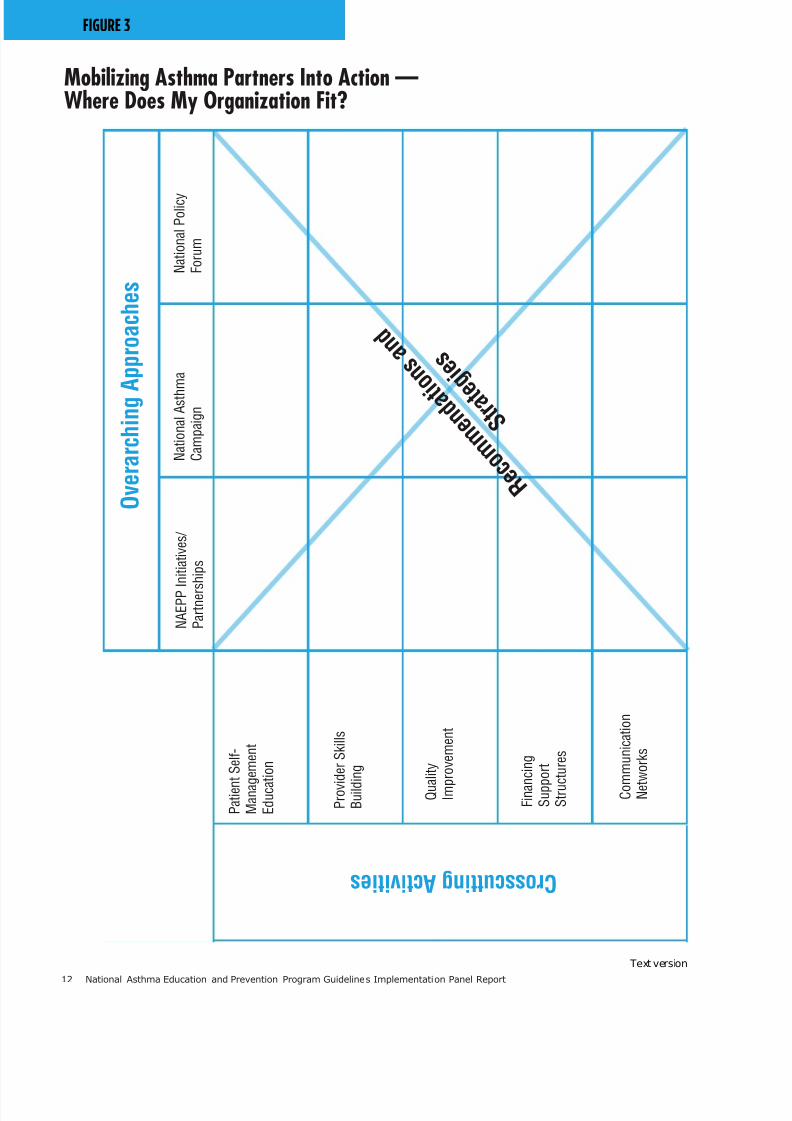
Thecrosscuttingactivitiespairedwiththeover-arching approaches orm a conceptual ramework that is useul in identiying appropriate andwilling partners to help operationalize the GIPImplementationPlan.SeeFigure3,Mobilizing
Asthma Partners Into Action—Where Does My Organization Fit?
Partnering for Success.
Theasthmacommunityhasadiverse,dedicatedand active group o stakeholders. A successulinitiative or improving asthma control will
requiretheirbroadparticipation,engagementandcollaboration. Many potential partners are identi-fed in the proposed strategies o the GIP Imple-mentationPlanthatfollows.Theyincludebutarenot limited to:• Patientsandtheirfamilies• Patienteducationandadvocacygroups• Cliniciansandeducatorsofvariousdisciplines—doctors(primarycareandspecialists),nursesandnursepractitioners,respiratorytherapists,pharmacists,physicians’assistants,asthma educators
• Professionalassociations• Providereducationgroups• Healthcareadministratorsandmanagers• Nationalaccreditingagencies• Hospitalsandemergencydepartments• Governmenthealthserviceagenciesand
programs• Managedcareorganizations• Commercialhealthplansandpayors• Expertsinperformancemeasurement• ElectronicHealthRecordcompanies
• Stateandlocalgovernmentagencies• Schools/childcarecenters,studentsandstaff • Community-basedorganizations—communitycenters,faith-basedorganizations
• Localasthmacoalitions—peereducators, communityhealthworkers,publichealth doctors,nursesandotherhealthcaredisciplines,epidemiologists and others engaged in popula-tion studies
• Academiccenters,medicalschoolsandtrainingprograms
• Mediawritersandeditors
• Worksites,employees,healthbenetsmanagers,worker advocacy groups
• Privatefoundations,localbusinesses,corpora-tions,pharmaceuticalindustry
It is important or these many partners to work together.Thus,inthespiritofcollaboration, highlights rom a drat o the GIP Report werepresented at a meeting o the NAEPP CoordinatingCommittee and other asthma stakeholders
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 18/52
12 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
FIGURE 3
Mobilizing Asthma Partners Into Action —Where Does My Organization Fit?
O v e r a r c h i n g
A p p r o a c h e s
C r o s s c u t t i n g A c t i v i t i e s
P a t i e n
t S e l f -
M a n a g e m e n t
E d u c a
t i o n
P r o v i d e r S k i l l s
B u i l d
i n g
Q u a
l i t y
I m p
r o v e m e n t
F i n a n
c i n g
S u p p
o r t
S t r u c t u r e s
C o m
m u n i c a t i o n
N e t
w o r k s
N A E P P I n i t i a t i v e s /
P a r t n e r s
h i p s
N a t i o n a l A s t h
m a
C a m p a i g n
N a t i o n a l P o l i c y
F o r u m
R e c o m m e n d a t i o
n s a n d
S t r a t e g i e s
Text version

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 19/52
Overview of the GIP Report 13
inOctober2007.Thereportisintendedto serve as a roadmap or prioritizing and initiatingfutureNAEPPactivities,andforidentifying and cementing partnerships among variousstakeholders who express interest in taking thelead on various sections o the GIP Implementa-tion Plan. Sharing highlights was an eort to getthe momentum started beore fnal release o
thereport.TheNAEPPwilltaketheleadto implement a large-scale coordinated NationalAsthma Control Initiative and engage a broadstakeholder base in collaborative implementationactivities.
Evaluating the GIP Implementation Plan.
An overall evaluation and communicationramework will be developed by the NHLBI withinput rom its partners. Partners who undertakeimplementation o the GIP strategies will beencouraged to ormulate metrics or measuringtheir outcomes based on the ramework. AnNHLBIWeb-basedPulmonaryKnowledge Network has been proposed as an active systemto monitor activities and acilitate coordinationand communication among partners regardingprogresson,andevaluationof,theirguidelinesimplementation activities.
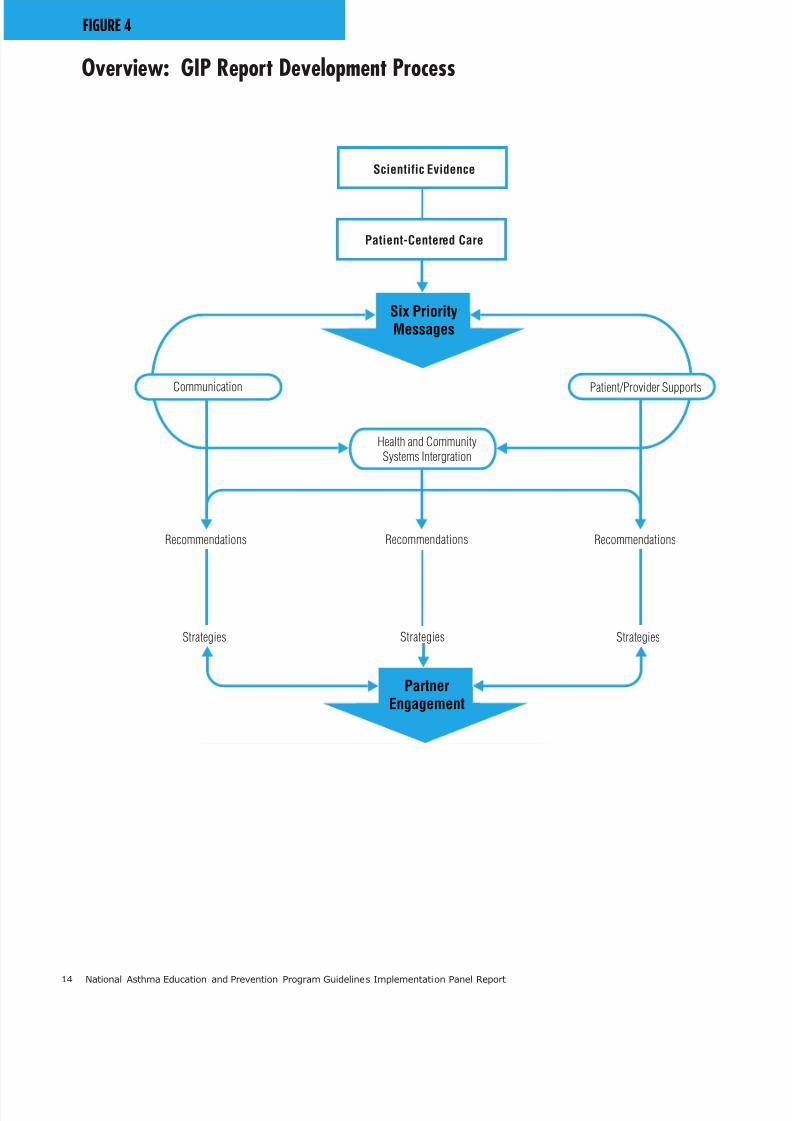
Figure 4 provides a graphic summary o theGIP Report development process and how the
implementation phase is shaped to engage partnersas active participants to help in the implementa-tion o the GIP recommendations and strategiesand thereby improve asthma control.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 20/52
14 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
FIGURE 4
Overview: GIP Report Development Process
Six PriorityMessages
Scientific Evidence
Patient-Centered Care
Communication Patient/Provider Supports
Health and CommunitySystems Intergration
RecommendationsRecommendations Recommendations
PartnerEngagement
StrategiesStrategies Strategies
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 21/52
The GIP Implementation Plan: Recommendations and Strategies 15
The GIP Implementation Plan:
Recommendations and Strategies
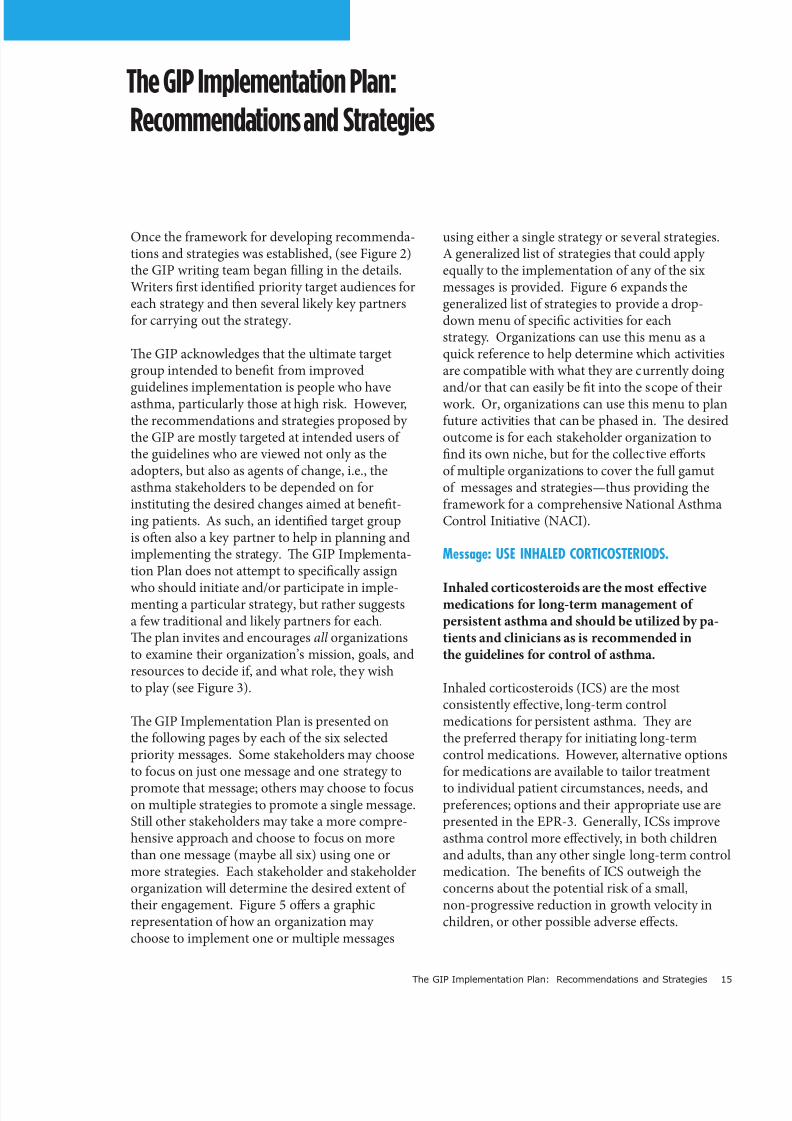
Once the ramework or developing recommenda-tions and strategies was established, (see Figure 2)the GIP writing team began lling in the details.Writers rst identied priority target audiences oreach strategy and then several likely key partnersor carrying out the strategy.
Te GIP acknowledges that the ultimate targetgroup intended to benet rom improved
guidelines implementation is people who haveasthma, particularly those at high risk. However,the recommendations and strategies proposed by the GIP are mostly targeted at intended users o the guidelines who are viewed not only as theadopters, but also as agents o change, i.e., theasthma stakeholders to be depended on orinstituting the desired changes aimed at benet-ing patients. As such, an identied target groupis ofen also a key partner to help in planning andimplementing the strategy. Te GIP Implementa-tion Plan does not attempt to specically assign
who should initiate and/or participate in imple-menting a particular strategy, but rather suggestsa ew traditional and likely partners or each.Te plan invites and encourages all organizationsto examine their organization’s mission, goals, andresources to decide i, and what role, they wishto play (see Figure 3).
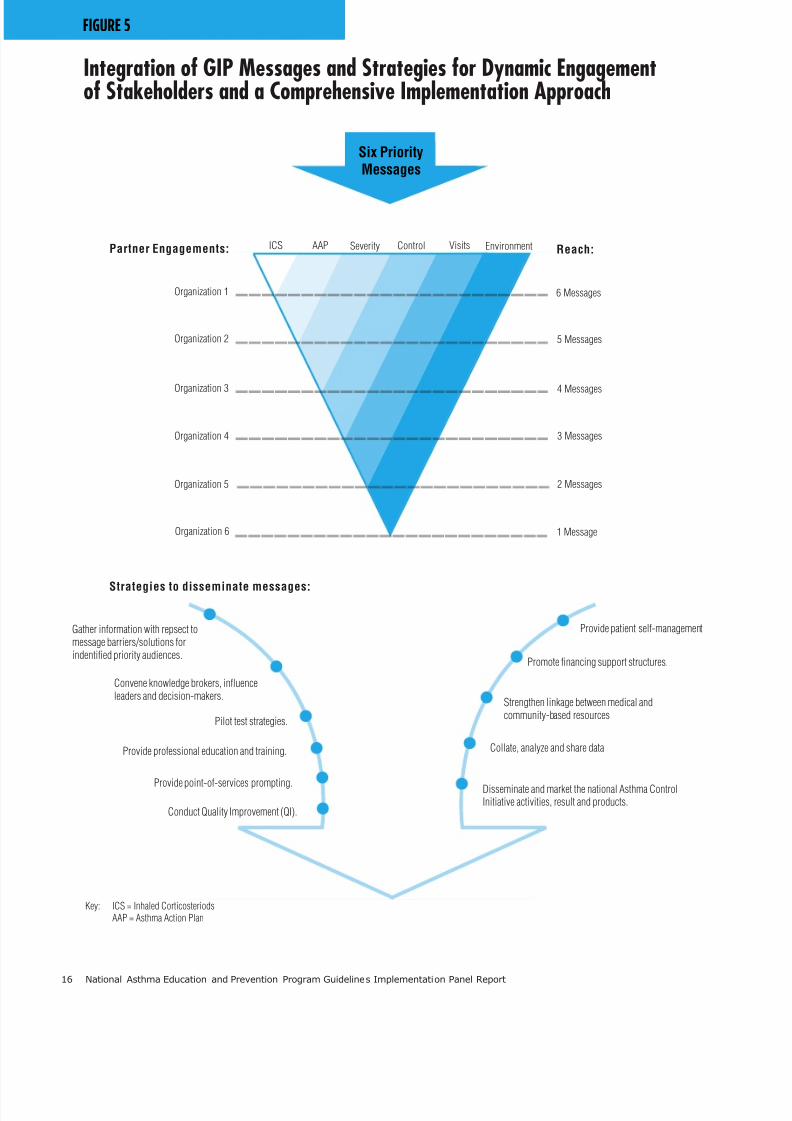
Te GIP Implementation Plan is presented onthe ollowing pages by each o the six selectedpriority messages. Some stakeholders may chooseto ocus on just one message and one strategy to
promote that message; others may choose to ocuson multiple strategies to promote a single message.Still other stakeholders may take a more compre-hensive approach and choose to ocus on morethan one message (maybe all six) using one ormore strategies. Each stakeholder and stakeholderorganization will determine the desired extent o their engagement. Figure 5 oers a graphicrepresentation o how an organization may choose to implement one or multiple messages
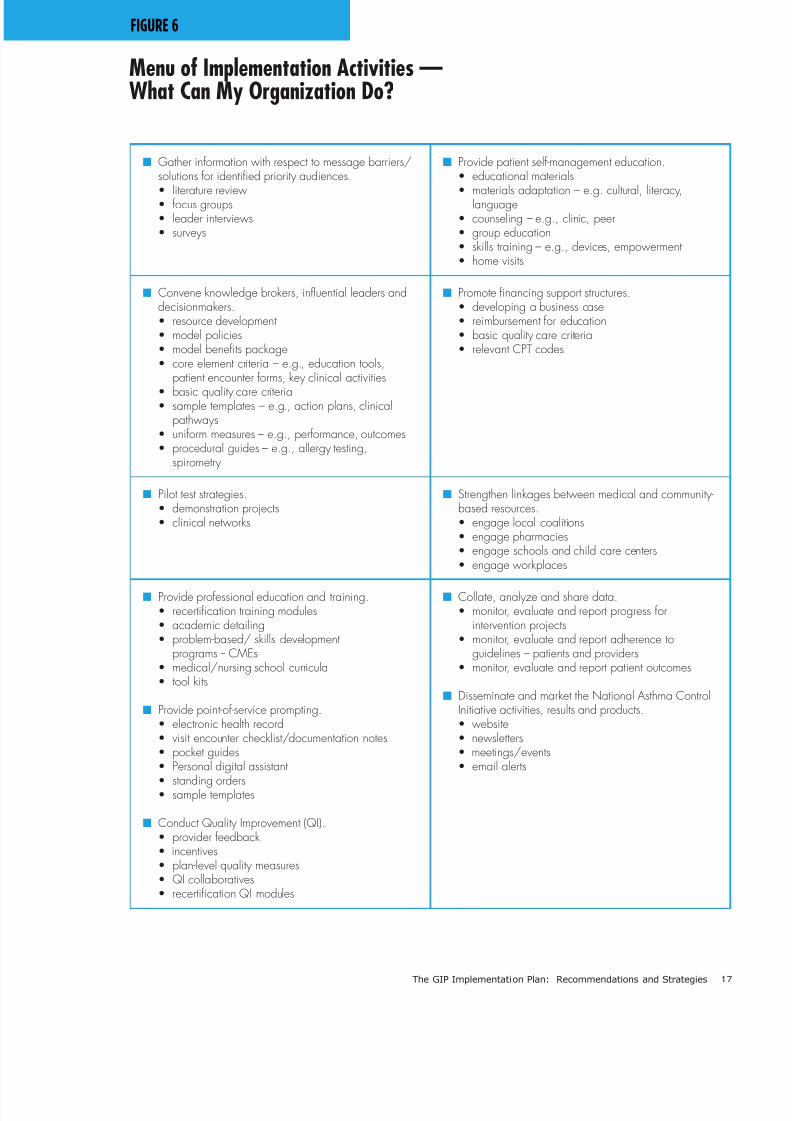
using either a single strategy or several strategies.A generalized list o strategies that could apply equally to the implementation o any o the sixmessages is provided. Figure 6 expands thegeneralized list o strategies to provide a drop-down menu o specic activities or eachstrategy. Organizations can use this menu as aquick reerence to help determine which activitiesare compatible with what they are currently doing
and/or that can easily be t into the scope o theirwork. Or, organizations can use this menu to planuture activities that can be phased in. Te desiredoutcome is or each stakeholder organization tond its own niche, but or the collective eortso multiple organizations to cover the ull gamuto messages and strategies—thus providing theramework or a comprehensive National AsthmaControl Initiative (NACI).
Message: USE INHALED CORTICOSTERIODS.
Inhaled corticosteroids are the most efectivemedications or long-term management o persistent asthma and should be utilized by pa-tients and clinicians as is recommended inthe guidelines or control o asthma.
Inhaled corticosteroids (ICS) are the mostconsistently eective, long-term controlmedications or persistent asthma. Tey arethe preerred therapy or initiating long-termcontrol medications. However, alternative optionsor medications are available to tailor treatment
to individual patient circumstances, needs, andpreerences; options and their appropriate use arepresented in the EPR-3. Generally, ICSs improveasthma control more eectively, in both childrenand adults, than any other single long-term controlmedication. Te benets o ICS outweigh theconcerns about the potential risk o a small,non-progressive reduction in growth velocity inchildren, or other possible adverse eects.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 22/52
16 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
FIGURE 5
Integration of GIP Messages and Strategies for Dynamic Engagementof Stakeholders and a Comprehensive Implementation Approach
Organization 1
Organization 2
Organization 3
Organization 4
Organization 5
Organization 6
6 Messages
5 Messages
4 Messages
3 Messages
2 Messages
1 Message
Partner Engagements: Reach:ICS AAP Severity Control Visits Environment
Six PriorityMessages
Provide patient self-management
Promote financing support structures.
Strengthen linkage between medical andcommunity-based resources
Collate, analyze and share data
Disseminate and market the national Asthma ControlInitiative activities, result and products.
Gather information with repsect tomessage barriers/solutions forindentified priority audiences.
Convene knowledge brokers, influenceleaders and decision-makers.
Pilot test strategies.
Provide professional education and training.
Provide point-of-services prompting.
Conduct Quality Improvement (QI).
Strategies to disseminate messages:
Key: ICS = Inhaled Corticosteriods
AAP = Asthma Action Plan
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 23/52
The GIP Implementation Plan: Recommendations and Strategies 17
FIGURE 6
Menu of Implementation Activities —What Can My Organization Do?
n Gather inormation with respect to message barriers/solutions or identifed priority audiences.
• literature review• focus groups• leader interviews• surveys
n Provide patient sel-management education.• educational materials
• materials adaptation – e.g. cultural, literacy,language• counseling – e.g., clinic, peer• group education• skills training – e.g., devices, empowerment• home visits
n Convene knowledge brokers, inuential leaders anddecisionmakers.• resource development• model policies• model benets package• core element criteria – e.g., education tools,
patient encounter forms, key clinical activities
• basic quality care criteria• sample templates – e.g., action plans, clinical
pathways• uniform measures – e.g., performance, outcomes• procedural guides – e.g., allergy testing,
spirometry
n Promote fnancing support structures.• developing a business case• reimbursement for education• basic quality care criteria• relevant CPT codes
n Pilot test strategies.• demonstration projects• clinical networks
n Strengthen linkages between medical and community-based resources.• engage local coalitions• engage pharmacies• engage schools and child care centers• engage workplaces
n Provide proessional education and training.• recertication training modules• academic detailing• problem-based/ skills development
programs -- CMEs• medical/nursing school curricula• tool kits
n Provide point-o-service prompting.• electronic health record• visit encounter checklist/documentation notes• pocket guides• Personal digital assistant
• standing orders• sample templates
n Conduct Quality Improvement (QI).• provider feedback • incentives• plan-level quality measures• QI collaboratives• recertication QI modules
n Collate, analyze and share data.• monitor, evaluate and report progress for
intervention projects• monitor, evaluate and report adherence to
guidelines – patients and providers• monitor, evaluate and report patient outcomes
n Disseminate and market the National Asthma ControlInitiative activities, results and products.• website• newsletters• meetings/events• email alerts
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 24/52
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 25/52
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 26/52
20 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
Proessional AssociationsRecommendation: Eliminate barriers to physiciansand other clinicians to appropriately prescribe ICSand encourage the use o ICS or persistent asthma.
Strategy 1: Convene a panel o ormally trained asthma educators in collaboration withphysicians, clinicians and midlevel providers
to collect, review and develop point-o-contactmethods and materials designed to enhance theuse o ICS. Such could include patient remind-ers, electronic health record (EHR) clinicalpathways, and tailored patient educationalmaterials.
Strategy 2: Work collaboratively with proes-sional associations and state asthma coalitionsto disseminate these products through existingmember networks using the most eectiveapproaches.
Strategy 3: In collaboration with EHR vendorsand inormatics experts develop and distributea clinical pathway template or asthma manage-ment that includes prompts to communicateand encourage appropriate use o ICS andstandardized data collection elements thatsupport evaluation o implementation activitiesand related practice-based research studies.
Patient Advocacy Groups
Recommendation: Develop messages and resourcesthat will empower patients to seek and maintaintreatment with ICS or long-term management o persistent asthma.
Strategy 1: Forge strong alliances amongpatient advocacy and education groups incollaboration with proessional associationsand other stakeholders. Trough this allianceconvene a virtual meeting o patient newslettereditors to collect and review existing materialsor wider dissemination and, where appropri-
ate, develop new content aimed at educatingand empowering patients on interactions withtheir healthcare providers. Provide this inor-mation to editors o local chapters o advocacy groups.
Strategy 2: Trough community organizations,the local medical community and proessionalassociations, identiy and/or develop presenta-tion material to support a speaker’s bureau o
clinicians, educators, patients, and amily mem-bers who are available or meetings and publicevents to convey and reinorce the message o appropriate ICS use.
Strategy 3: Utilize a targeted national asthmacampaign and social marketing initiative thatincludes the NAEPP and its partnering orga-
nizations to promote the six GIP messages,including the message on the importance o ICS or persistent or poorly controlled asthmaas well as its saety and eectiveness in ongoingasthma management.
Message: USE WRITTEN ASTHMA ACTION PLANS.
All people with asthma should receive a writtenasthma action plan to guide their sel-manage-ment eforts.
Many patients have diculty recalling instructionsor care that are given by their healthcareprovider. A written asthma action plan (AAP)provides instruction and inormation on how tosel-manage one’s asthma daily, including takingmedications appropriately, and identiying andavoiding exposure to allergens and irritants thatcan bring about asthma symptoms. In addition,the AAP provides inormation on how torecognize and handle worsening asthma, andwhen, how and who to contact in an emergency.
CommunicationRationale: o improve communication, AAPsneed to be written clearly and implemented onmany levels. First and oremost, clinicians shouldbe able to choose a ormat or patient instructionthat is consistent with their practice and their pa-tient’s needs. At the same time, however, cliniciansshould not have to create these plans anew. Forchildren, these plans should be made simple andeasy or schools, school nurses, and school-basedhealth centers to use. Schools play a signicant
role in reinorcing use o a child’s written AAP. Inaddition, AAPs should be easy or patients andtheir amilies to understand and presented in aormat that encourages sel-management. AAPsserve as the vehicle o coordination across multiplecaregivers and as a linking mechanism betweencommunity and clinical sites. Communicating thepolicies that guide use o AAPs at various points o care will reinorce their use.

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 27/52
The GIP Implementation Plan: Recommendations and Strategies 21
Prescribing CliniciansRecommendation: Provide templates or writ-ten AAPs that include the core elements o actionplans described in EPR-3, and that oer choicesby age or setting (schools, workplace, childcarecenters) and that are clear and easy to use. Tis seto sample templates will acilitate a standardizedapproach to developing an AAP or patients and
ease o use by clinicians, thereby increasing his/herwillingness to use it.
Strategy 1: Enlist the support o proessionalassociations, clinicians and patient- and provid-er-education groups to review existing AAPs;and, as necessary, develop national prototypeso written AAPs that are simple, clearly under-stood, and easily tailored to meet the needs o diverse ethnic populations and patients.
Strategy 2: Obtain buy-in rom primary care
and medical specialty associations to supportthe production and dissemination o the proto-type AAPs to clinicians.
Patients and Teir FamiliesRecommendation: Identiy patient and amily needs and preerences regarding the content andormat o written AAPs. Identiy best ways tocommunicate with patients on the importance o action plans and how to ask their healthcare pro- vider or them.
Strategy 1: Trough patient advocacy groupsand proessional associations, gather inorma-tion rom the EPR-3 and other credible sourcesto identiy and summarize messages andinstructions that patients and amilies need tobetter manage their asthma.
Strategy 2: Collect and disseminate AAPtemplates that provide inclusion o the recom-mended core elements o an action plan aspresented in EPR-3.
Strategy 3: Develop and promote the use o action plans that are culturally, educationally and linguistically meaningul to a diverse groupo patients and their amilies. Coordinate thiseort to reach patients with an outreach ap-proach to healthcare providers (see Strategy 1or Prescribing Clinicians, noted above).
Strategy 4: Work with patient advocacy andeducation organizations to encourage patientsto ask their providers or an individualizedAAP, or teach patients how to obtain a sampleplan to take to their provider to develop anindividualized AAP.
Schools, School Nurses, and School-Based Health
Centers and Childcare CentersRecommendation: Make available to schools,school nurses and/or school- based health centersor childcare centers, prototypes o the writtenAAPs that can be used or each student whohas asthma.
Strategy 1: In collaboration with the NAEPPand its School Asthma Education Subcommit-tee convene a working group with representa-tion rom primary healthcare providers (amily medicine, pediatrics and nursing), specialty
associations, state-level health and educationagencies, school boards, and school administra-tor organizations to identiy and, i appropri-ate, develop a model policy and methods orimplementing AAPs and acilitating communi-cation and the sharing o written AAPs betweenprimary care clinicians’ oces and schools orthe purpose o coordinating care. Also, identiy and encourage the acceptance and use o stan-dardized AAPs by school districts.
Strategy 2: In collaboration with proes-sional associations, asthma educators, schooleducators, and nurses, identiy existing and/or develop and implement a new educationalprogram or workshop that addresses the use o AAPs or school personnel. Tis will enhancethe education and skills o school sta, schoolnurses, and school-based health center sta inrecognizing and managing asthma based onwritten AAPs and in understanding the policy issues related to AAPs.
Strategy 3: In collaboration with the NAEPPand its School Asthma Education Subcommit-tee, develop an enhanced Web page, or “com-munity o practice” web site, that summarizesand makes accessible in one place schoolasthma inormation and resources, and thatinvites visitors to participate in a series o ea-tured venues. Market the web page widely toparticipants who share in its common purposeand who will benet rom it.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 28/52
22 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
Systems IntegrationRationale: Policies and programs that createaccountability will better ensure the use o anAAP. Furthermore, EHRs that include writtenAAP will encourage and reinorce provider use.Personal Health Records, intended or use by thepatient can support sel-management o chronicconditions such as asthma.
Government Health Services AgenciesRecommendation: Engage decisionmakers todevelop and implement policies and programsthat promote the use o written AAP as parto basic care and coordination o care.
Strategy 1: Trough collaboration o stakehold-ers working with Centers or Medicare andMeicaid Services (CMS), engage State MedicaidMedical Directors in a discussion about ways toencourage and increase the use o written AAP.
Strategy 2: Utilize a national asthma policy orum to acilitate and coordinate eorts thatencourage leadership within government healthservice agencies to develop policies, quality improvements and pay-or-perormancemeasures that include the use o writtenAAP or patients who have asthma.
Managed Care Organizations and HealthcarePayors
Recommendation: Engage decisionmakers todevelop and implement policies and programs thatpromote the creation and distribution o writtenAAPs as a basic part o eective asthma care.
Strategy 1: Trough the collaboration o (MCOs) and healthcare payors, convene ameeting o healthcare payors, benets man-agers, key MCO representatives (managers,physicians and other prescribing clinicians, andmedical group executives) to develop a modelpolicy or the use o written AAPs.
Strategy 2: Pilot test the model policy, includ-ing a method or documenting that an AAP wasprovided (e.g., using an EHR) and a method orprompting timely updates o the AAP thus bet-ter ensuring compatibility with available medi-cines and benets. Documentation will help tomonitor any associated incentive programs.
Strategy 3: Utilize a national asthma policy orum to acilitate the distribution, andencourage the adoption and implementation,o a model policy or AAPs that embeds quality measures and pay-or-perormance measuresinto the policy.
Electronic Health Record Companies
Recommendation: Facilitate the use o writtenAAPs by physicians and other clinicians by inte-grating plans into EHRs.
Strategy 1: Using an approach coordinated by EHR companies, develop and distribute a com-prehensive written AAP that is easily under-stood by patients and their amilies; and, thatis comprised o the core elements o an AAP asdescribed in the EPR-3.
Strategy 2: Ascertain and act on ways to gain
the interest and commitment o EHR com-panies to promote their module on the use o written AAPs or people who have asthma.
Patient/Provider SupportRationale: Te patient’s goals, concerns, belies,and attitudes should be addressed, as these are keysto successul use o AAPs as a sel-managementtool. Sharing in the decisionmaking process withtheir healthcare provider will encourage patients touse the AAP. In addition, engaging other members
on the patient’s healthcare team, and practitionersand educators at alternative points o care (i.e.,schools, pharmacies, etc.) will help to reinorcethe importance o patient sel management usingan AAP.
Patients, Families and their CliniciansRecommendation: Identiy and reduce the barriersto use o written AAPs by patients and their ami-lies and create an environment o shared decision-making with clinicians.
Strategy 1: Patient advocacy, education groupsand proessional associations should reer tothe EPR-3 and other credible sources to identiy and summarize known barriers or using AAPsby patients and their amilies. Tis inormationcan be used to inorm clinicians on approachesto use or overcoming these barriers. I needed,search additional recent literature or strategiesand methods that have been tested and shownto be eective in overcoming these barriers.

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 29/52
The GIP Implementation Plan: Recommendations and Strategies 23
Strategy 2: Enlist asthma educators, patientadvocacy groups, and other healthcare proes-sionals to educate patients on the skills andrationale or sel management and utilizationo their AAPs.
Strategy 3: Encourage patient education pro-grams to demonstrate techniques patients can
use to request written AAPs rom their provid-ers and motivate them to use thesetechniques.
Pharmacists and Other Health-related ProvidersRecommendation: Utilize multiple points-o-service, in particular pharmacies where patientencounters occur, to increase utilization o writtenAAPs.
Strategy 1: Convene a meeting o pharmacists,prescribing clinicians, nurse practitioners,
asthma educators, and school nurses as well aspatients and other related disciplines to discussways to improve dissemination and reinorce-ment o the use o written AAPs in a variety o settings.
Strategy 2: Work with pharmacists and health-care providers to identiy ways to better supportthe use o EHRs or reinorcing a patient’s useo his/her written AAP.
Message: ASSESS ASTHMA SEVERITY.
All patients should have an initial severity assess-ment based on measures o current impairmentand uture risk* in order to determine type andlevel o initial therapy needed.
Asthma severity is the intrinsic intensity o theasthma disease process and is measured mosteasily and directly in a patient who is not receivinglong-term control therapy. Inormation gatheredin the assessment o asthma severity is used to
characterize the patient’s asthma in order to guidedecisions or initiating therapy, afer which theocus shifs to how well the patient is able tocontrol his or her asthma by ollowing the treat-ment plan. A severity assessment ensures theappropriate use o pharmacologic agents. Bothasthma severity and asthma control are determinedby the same measures in two domains: 1) currentimpairment, and 2) uture risk. Once treatment isstarted, the results o the measures o impairment
and risk are used to monitor asthma control ratherthan severity. Monitoring the level o asthmacontrol is used to adjust medication as needed.
CommunicationRationale: Clinicians should determine sever-ity o asthma as part o their initial assessmento patients who have asthma. Asthma severity
should be documented in the patient’s record andthe signicance o this assessment explained tothe patient. Patients should know that regardlesso severity classication, all asthma is serious andrequires patients to ollow their treatment plans.Likewise, patients need to be able to communicateinormation to their healthcare providers abouttheir asthma and how it aects their lives. Tiswill help the healthcare provider to assess the levelo impairment and risk or determining a patient’sinitial asthma severity and treatment requirements.
Primary Care Providers and Other Healthcare CliniciansRecommendation: Encourage clinicians to docu-ment inormation in the patient’s record withrespect to measures o impairment and risk andalso the resulting level o asthma severity that thiscombination o measures indicates. Encourageclinicians to explain to the patient the signicanceo asthma severity at diagnosis in developing aninitial treatment plan and then how the emphasisshifs to monitoring control o asthma over the
long term using the same measures o impairmentand risk.
Strategy 1: Encourage collaboration amongproessional associations and other asthmastakeholders in setting up a clearinghouse o sample tools or assessing severity and initiat-ing therapy accordingly in clinician-riendly ormats. Develop and execute a plan orpromoting these resources to primary health-care providers and asthma specialists, and orassessing and explaining severity in dierent
populations in a variety o settings.
Strategy 2: Trough a collaboration o proes-sional associations and other stakeholders,
*Note: While there is not strong evidence rom clinical trials or determining therapy based on the domain o uture risk,the guidelines Expert Panel considers that this is animportant domain or clinicians to consider due to the strong association between history o exacerbations and the risk or uture exacerbations.

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 30/52
24 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
develop a range o innovative CME-basedprograms (webinars, teleconerences, CD-ROMs, grand rounds) to educate primary careclinicians and ED physicians and sta on how to assess asthma severity and articulate itssignicance to patients.
Patients and Teir Families
Recommendation: Educate patients who haveasthma about the role o asthma severity intheir overall asthma management.
Strategy 1: Working with patient advocacy and education groups, proessional associa-tions and the NAEPP, convene a meetingto assess gaps in the availability o exist-ing educational materials and resourcesor patients and amilies regarding asthmaseverity. Develop new educational materialsand resources as needed with a ocus on the
domains o current impairment and uturerisk and their role in assessing asthmaseverity at diagnosis and then in monitor-ing level o asthma control once treatmentis started. Disseminate resources through various channels available to educationalgroups and proessional associations or usein patient education.
Strategy 2: Use a national campaign strategy and social marketing techniques to inorm
patients, their amilies and providers whocare or them about the signicance o assessing asthma severity at the time o apatient’s initial assessment to help determinethe appropriate treatment plan.
System IntegrationRationale: All healthcare providers should beeducated about the asthma guidelines and how toassess a patient’s asthma severity at initial diagno-sis. In order to support the assessment o asthmaseverity, payors and purchasers o health benets
should understand the signicance o asthmaseverity and the importance o the guidelinesrecommendation to assess it. Every healthcareproessional who cares or people who have asthmashould understand the concept o asthma severity and how to apply it in developing a treatment plan.
Education and raining InstitutionsRecommendation: Educate clinicians-in-training(medical students, residents, nursing students,respiratory therapists, and pharmacists) on assess-ing asthma severity.
Strategy 1: Working through the American As-sociation o Medical Colleges, incorporate the
concept o assessing asthma severity into themedical school curriculum.
Strategy 2: Trough collaborative eorts o theproessional associations, boards or variousmedical disciplines, and the NAEPP, developtools to incorporate evaluation o asthmaseverity into training and MOC programs o primary care providers and clinicians (amily practice, pediatricians, physician assistants,nurses, pharmacists, and respiratory therapists).
Payors and PurchasersRecommendation: Enlist payors and purchasers o services to promote the importance o assessingasthma severity by healthcare providers.
Strategy 1: Encourage healthcare providerswho participate in Medicaid, Medicare andlarge MCOs to conduct routine assessment o asthma severity on patients during their initial visit. Implement incentives and provide eed-back reports.
Strategy 2: Explore the ability to use Interna-tional Statistical Classication o Diseases andRelated Health Problems and Current Proce-dural erminology structures to better clas-siy asthma severity. Coding should be betterdeveloped with respect to the coding o asthmaseverity.
Strategy 3: Engage proessional associations inpartnership with the NAEPP to work with EHR companies to include assessment o asthma
severity in their system.
Strategy 4: Work with ED personnel, proes-sional associations and hospital administratorsto develop a process or evaluating asthmaseverity o all patients who have untreated orpoorly controlled asthma and who are seen inthe ED. Te process that is developed shouldinclude methods or ED personnel to commu-

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 31/52
The GIP Implementation Plan: Recommendations and Strategies 25
nicate these severity level assessments to thepatient’s primary care provider.
Patient/Provider SupportRationale: When being evaluated by healthcareproviders, patients who have asthma shouldunderstand asthma severity and how it is assessed.Tey should expect that healthcare providers and
clinicians who treat them understand the concepto asthma severity and how to apply it to a patient’soverall care.
Patient Advocacy Groups and Patients with AsthmaRecommendation: All patients who arediagnosed with asthma at the time o their initialassessment should have a determination made o their asthma severity.
Strategy 1: Utilize a national asthma
campaign to serve as an outreach arm toinorm and educate patients and theiramilies about all six priority messages,including basic inormation on why it isimportant or their provider to assess asthmaseverity when initiating therapy; and, on how to ask or and obtain an asthma severity assess-ment.
Asthma Educators Recommendation: Utilize asthma educators to
teach their peers and other clinicians and educa-tors, as well as patients and amilies about theimportance o assessing asthma severity as well asthe measures o impairment and risk that are usedto determine level o severity.
Strategy 1: Trough the respective proessionalassociations, patient advocacy and educationgroups in collaboration with the NAEPP’sNational Asthma Control Initiative, developtools to be used by asthma educators to teachpatients and amilies, healthcare providers,
managed care providers, pharmacists and oth-ers about asthma severity.
Strategy 2: Develop interactive, problem-basedrain-the-rainer programs or members o asthma educator organizations that teach key guidelines recommendations related to the sixGIP messages, including asthma severity.
Strategy 3: Disseminate the educator trainingprograms and the accompanying tools througha national asthma campaign as well as throughother NAEPP partnering organizations.
Message: ASSESS AND MONITOR ASTHMA CONTROL.
At planned ollowup visits, asthma patientsshould review level o asthma control with theirhealthcare provider based on multiple measureso current impairment and uture risk in orderto guide clinician decisions to either maintainor adjust therapy.
Tere is a new emphasis on the assessment andregular monitoring o asthma control to determinei the goals o therapy are being met and whethertherapy needs to be adjusted. Te EPR-3 empha-sizes the distinction between classiying asthma
severity and monitoring asthma control, namely,to assess asthma severity to initiate therapy andto assess asthma control to determine i therapy should be adjusted. Asthma control is the de-gree to which the maniestations o asthma areminimized by therapeutic interventions—that is,the degree to which the goals o therapy are met.Asthma control (just as asthma severity) includesthe domains o current impairment and uture risk.Te concept o impairment includes requency andintensity o symptoms, current or recent unctional
limitations experienced by the patient. Te con-cept o risk includes the likelihood o either asthmaexacerbations, progressive decline in lung unction(or, or children, reduced lung growth), or risk o adverse eects rom medication. Te level o con-trol achieved in response to treatment, includingsuccess o patient adherence to a realistic andgoal-oriented treatment plan, dictates whethera treatment regimen can be maintained by thepatient, or whether medication must be adjusted(stepped up or down). Te emphasis o routinemonitoring in the updated guidelines is clearly
related to asthma control.
CommunicationRationale: In order to eectively communicate therole o assessing and monitoring asthma controlin asthma management, clinicians and educatorsshould understand patient perspectives on theconcepts o impairment and risk and on thebarriers patients ace in implementing theirtreatment plans. Clinicians need tools and
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 32/52
26 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
resources to simpliy presentation o the concepto control (impairment and risk) to patients andtheir amilies. Payors, PBMs, and Medicaid direc-tors also need to understand the concept o controland its signicance in asthma management since,through their direct access to high-risk popula-tions, they have tremendous potential to impactasthma outcomes.
Patients and Teir FamiliesRecommendation: Determine patients’understanding o asthma control and theimportance o monitoring it in long-term asthmamanagement.
Strategy 1: Engage patient advocacy groups,patient education groups, practice-basedresearch networks, and other stakeholders toreview the literature on barriers to patients as-sessing and monitoring well-controlled asthma
(drawing upon studies cited in the EPR-3 andother credible sources). Conduct ocus groups,i needed, to urther identiy barriers to patientsmonitoring asthma control; include patientswith asthma o all types, but especially thosewho have had exacerbations o their asthma inthe past 2 years. Develop a white paper to sum-marize the barriers and propose methods orovercoming them, including ways to eectively convey the control message to patients andtheir amilies.
Strategy 2: Support the use o established socialmarketing and health communications tech-niques to develop culturally appropriate mes-sages and media outreach activities by drawingupon academic and commercial entities withexpertise in this discipline.
Strategy 3: Utilize a national asthma campaignto implement a variety o social marketing andcommunication strategies that address all sixmessages, including asthma control.
CliniciansRecommendation: Develop and deliver messagesthat enhance a clinician’s willingness to assess asth-ma control using standard measures o impairmentand risk, with emphasis on high-impact strategies,e.g., MOC processes and board exams that couldbe applied across all six priority messages.
Strategy 1: Conduct surveys or ocus groupso clinicians and emergency medicine practi-tioners to evaluate the current clinical processesthey use or determining a patient’s level o asthma control and explore ways to incorporatethese amiliar practices within the new rame-work o impairment and risk.
Strategy 2: Pilot test the use o board examsand the MOC processes within primary careand emergency medicine disciplines as a vehi-cle to support incorporation o guidelines intopractice. Tis would involve dissemination o the guidelines, application o practice redesignelements to oster sustained implementation o the guidelines, and development o metrics toassess impact.
Strategy 3: Enlist the support o proessionalassociations, patient advocacy and education
groups, medical boards and other stakeholdersto develop and disseminate innovative strate-gies or CME, nursing, and other healthcaredisciplines’ education and MOC materials con- veying the use o the EPR-3 recommendationsor control in the management o asthma.
Managed Care Organizations, Payors and Pharmacy Benefts ManagersRecommendation: Identiy gaps in existing tools,develop new tools as needed, and reach consensus
on a standardized assessment tool or asthma con-trol that incorporates the core concepts in EPR-3 o impairment and risk and that can be used in casemanagement or monitoring o asthma control.
Strategy 1: Working with AHIP or BCBSA,convene a workshop o payors/PBMs aimed atdeveloping an eective approach or communi-cating the EPR-3 recommendations on assess-ing and monitoring asthma control to payorsand PBMs. Disseminate inormation on waysto implement the approach to constituents.
Strategy 2: Working through the NAEPP, co-ordinate a review o existing tools with MCOsand major purchasers o health care (e.g., largebusinesses, State governments, etc.); reach con-sensus among participants on a standardizedtool, or template, or assessing and monitoringasthma control; develop new tools, i needed.Te standardized tool would incorporate thecore concepts o control, namely, impairment
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 33/52
The GIP Implementation Plan: Recommendations and Strategies 27
and risk and could be used to monitor controlduring clinical and case management. Pilot testthe tool, and also engage the NCQA as an ally to promote the piloted standardized assessmenttool as an internal quality measure or use by MCOs. Adapt the tool to t dierent popula-tions and settings.
Strategy 3: Engage managed care entities to as-sess eective messaging techniques within theirpopulation reach in order to develop processesthat better achieve eective sel-assessment o asthma control by patients. Share this inorma-tion with the broader MCO community.
Strategy 4: Trough collaboration o theNAEPP and its partners, including possibly theIOM, develop a white paper on the eective-ness o MCOs to oster the implementationo guidelines through incentives, member
outreach and provider collaboration. Tepaper should address how well MCOs osterenhanced disease management programs andshould include an assessment o the eec-tiveness o these programs. Summarize anddisseminate this inormation widely to HealthMaintenance Organizations using a variety o ormats.
Systems IntegrationRationale: Engage and collaborate with such
entities as the NCQA and CMS to promote theasthma control message based on the domains o current impairment and uture risk since theseorganizations exert ar-reaching inuence overemployers’ health benets purchasing decisions.
National Committee or Quality AssuranceRecommendation: Develop and implementa HEDIS measure that ocially states the processo assessing control or managed care populations.
Strategy 1: Te NAEPP in collaboration with its
partners will support a NCQA working groupto identiy the oundational elements o asthmacontrol measurements, based on risk and im-pairment, which can be parlayed into a uniormcontrol measure or direct comparison romone plan to another. Tis perormance measureshould be designed to assess how well MCOstrack asthma control in their case-managedpopulation and in their membership overall.By monitoring this perormance measure, an
MCO will have demonstrated that it hasintegrated assessment o asthma control intoits programs.
Strategy 2: Convene a meeting with MCOs todevelop broad support or: 1) a HEDIS peror-mance measure on asthma control assessment,2) the use o standardized tools in clinical set-
tings, and 3) the use o case management.
Centers or Medicare and Medicaid ServicesRecommendation: Promote programs that encour-age assessment o asthma control in Medicaidrecipients.
Strategy 1: Encourage strategic alliances withlocal and regional asthma coalitions, theDepartment o Medical Assistance Services ineach state, and public health departments todisseminate inormation about disease man-
agement and other programs that incorporateasthma control messages or all recipients.
Strategy 2: Explore development o a ormalplan that species assessment and monitor-ing o asthma control is provided in Medicaiddisease management programs and providercontinuing education programs. Furthermore,provide incentives to routinely assess asthmacontrol in delivery o asthma care.
Patient/Provider SupportRationale: Although both providers and patientswill readily mention asthma control as theirprimary goal or asthma management, they ofenneither employ a systematic way o assessing andregularly monitoring asthma control nor addressthe risks associated with lack o maintainingcontrol. Physician organizations represent theclinicians, and oversee whether clinicians areperorming or supervising appropriate assessmentand monitoring o asthma patients. Patient advo-cacy groups represent those organizations
that support the patient by helping to translatecomplex disease treatment steps into clear andsimple sel-management action messages, whichinclude monitoring asthma control. Patientsshould monitor asthma control to better sel-manage their disease.
Patients and their FamiliesRecommendation: Encourage the expectationamong people who have asthma and their amilies
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 34/52
28 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
that asthma control can be attained and will beassessed during their ollowup health visits.
Strategy 1: Conduct ocus groups in diversepopulations to collect inormation on patients’understanding and belies related to asthmacontrol and inormation on messaging relatedto monitoring asthma control as part o sel
management o their disease.
Strategy 2: Work with health communicationsexperts, patient advocacy groups, and otherstakeholders to develop culturally appropriateeducational materials in a variety o ormatsand languages that address current knowledge, viewpoints, and potential misunderstandingso asthma control identied through the ocusgroups. Distribute these resources through thedissemination channels o patient and pro- vider education groups and a national asthma
campaign.
Proessional AssociationsRecommendation: Facilitate the ease with whichphysicians and other clinicians are more able toconsistently and routinely conduct assessment o impairment and risk to determine their patients’level o asthma control within varied practicesettings.
Strategy 1: Support sessions at proessional
association meetings that encourage participa-tion in the development o decision supportresources including Personal Digital Assistants,EHR clinical pathways, and patient educationalmaterials designed to enhance the assessmentand routine monitoring o asthma control.
Strategy 2: Partner with proessionalassociations to distribute useul materials andstrategies through their existingelectronic and mail member networks to helpincrease assessment and monitoring
o asthma control.
Strategy 3: In collaboration with EHR vendors,develop and test an EHR/electronic clinicalpathway template or asthma management thatincludes standard assessment tools or asthmacontrol, standard data elements to supportimplementation, and evaluation.
Strategy 4: Establish a partnership betweenthe NAEPP and proessional specialty boardsto develop materials and strategies that can beincorporated into MOC programs.
Strategy 5: Convene stakeholders who havethe expertise and resources to provide techni-cal support or a series o quality improvement
(QI) implementation studies. In collaborationwith the NAEPP and its partners, develop thesepotentially high impact QI interventions to betested by a partner organization or its practice-based research networks or eectiveness,transerability and sustainability. Facilitateassessment o QI interventions through grantsand contracts oered by various governmentagencies or member programs in order toidentiy those with the highest possible impact.
Patient Advocacy Groups
Recommendation: Develop messages that willencourage patients to sel monitor their level o asthma control and that will oster expectationsthat their asthma control shall be routinely as-sessed by their healthcare provider or the long-term management o their asthma.
Strategy 1: Convene a meeting o leaders inpublic or media communication to work withpatient advocacy groups and patient/providereducation groups to:
• Developmessagesforpatientsconcerning assessment and monitoring asthma control
• Developcontentthatcanbeprovidedto editors o State and local chapters o advocacy groups aimed at educating andempowering patients in preparation orinteractions with their healthcare providers.
Strategy 2: Trough community organizations,the local medical community and proessionalassociations, develop presentation material to
support existing or develop a new speakers’bureau o clinicians, other healthcare proes-sionals, patients and amily members who areavailable or meetings and public events toconvey and reinorce the message o monitor-ing asthma control.

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 35/52
The GIP Implementation Plan: Recommendations and Strategies 29
Message: SCHEDULE FOLLOWUP VISITS.
Patients who have asthma should be scheduledor planned ollowup visits at periodic inter-
vals in order to assess their asthma control andmodiy treatment i needed.
Asthma is highly variable. Some patients with
asthma may have severe asthma attacks withoutmany symptoms between attacks. Others, how-ever, may have requent symptoms without havinga severe asthma attack. Asthma may also vary according to the time o year. Because response toasthma therapy may vary, periodic monitoring o asthma control through clinical visits is essentialto “step up” therapy (increase the dose, number o medications and requency) as necessary; or, “stepdown” (decrease) when possible to the minimummedication necessary to maintain control. Te in-terval between ollowup visits may also vary basedon the level or duration o asthma control as wellas the level o treatment required.
Te requency o monitoring is a matter o clini-cal judgment and will vary depending on severalactors, including the level o asthma control. Ingeneral, patient visits should be scheduled at 2-to-6 week intervals while initiating therapy or step-ping up therapy to achieve control; at 1-to-6 monthintervals afer asthma control is achieved in orderto monitor i asthma control is maintained; and,
at 3-month intervals i a step-down in therapy isanticipated.
CommunicationRationale: Patients and their amilies, clinicians,healthcare administrators and policymakers may lack knowledge and appreciation about the im-portance and benet o periodic clinical ollowupo people who have asthma. Contributing actorsinclude the complexity o the message related toroutine “check ups” or asthma, even when thepatient is eeling ne, versus the tendency to visit
the doctor only during an asthma attack; and to alack o belie in the benets o preventive care. Amessage that ocuses on mutually agreed-upongoals or therapy, objective measures o control,and the benets o well-controlled asthma wouldbe a motivational cue to patients or keeping theirappointments.
Patients and FamiliesRecommendation: Implement a national asthma
campaign to educate, in particular, high-risk popu-lation segments about the importance o regularly scheduled outpatient ollowup in accordance withthe EPR-3 or people who have asthma.
Strategy 1: Conduct social marketing andhealth communications research to developaccurate and consistent, consumer-riendly
messages and identiy appropriate media chan-nels to reach people who have asthma rom di-erent cultural backgrounds and literacy levels.
Strategy 2: Conduct a pilot project or segmentso the U.S. general public to evaluate the eec-tiveness o these messages in changing asthmaknowledge, attitudes, and behaviors about pe-riodic visits and other EPR-3 priority messagesrelated to long-term management. Te pilotproject and its evaluation should examine theprojected costs and benets to expanding this
pilot project to the entire population. Presentthe results o the pilot project as a business caseor periodic visits.
CliniciansRecommendation: Develop and deliver messages toprimary care providers and ED clinicians regard-ing the importance o routine clinical ollowup orpatients who have asthma.
Strategy 1: Work with proessional associa-
tions, specialty organizations, certicationboards, and educational training programs toinclude the message o periodic visits in theirCME and MDC programs.
Strategy 2: Work with industry in developingand delivering eective educational and moti- vational strategies to promote periodic visits.
Purchasers and PayorsRecommendation: Increase awareness o the po-tential benets o consistent outpatient ollowup
among major purchasers o health benets, payors,and health actuaries as a move toward broad-scaleinsurance coverage o periodic visits in routineasthma care.
Strategy 1: Conduct a series o interviews withprivate and public payors to assess and sum-marize potential benets and barriers to theimplementation o comprehensive outpatientinsurance coverage or asthma.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 36/52
30 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
Strategy 2: Work with patient advocacy groupsto gather and disseminate existing inormationon the costs and benets o periodic outpatientasthma care as compared to sporadic asthmacare. Tis inormation will be disseminatedto purchasers and payors in presenting a caseor covered periodic asthma care. Includerecommendations promoting appropriate
reimbursement or services provided atroutinely scheduled outpatient visits.
Systems IntegrationRationale: Tere are multiple barriers within thehealthcare system and community that contributeto the lack o periodic clinical ollowup o patientswho have asthma. Several major barriers includelack o monitoring systems to track patients whohave asthma, insucient incentives or promptsor patients to encourage adherence to treatmentplans, and lack o consistent reimbursement or
ollowup visits.
Clinical Practice Gatekeepers (Administrators/ Policy Makers), Private and Public Recommendation: Implement patient monitoringand reerral policies that will promote the increaseo appropriate outpatient ollowup or persons whohave asthma, with special attention to implement-ing close ollowup afer an urgent care encounteror those whose asthma is not well controlled.
Strategy 1: Convene a group o medical direc-tors, clinicians, and clinic administrative sta rom varied healthcare settings to identiy bar-riers to ollowup care and use this inormationto develop innovative strategies to overcomethe barriers. An example o such a strategy isan automatic generation o lists o patients whoare at higher risk and greater need or ollowupbased on their lack o asthma control.
Strategy 2: Conduct a QI study in a ew o theNAEPP’s partner organizations to evaluate
the eectiveness o several monitoring andreerral strategies and their potential or broad-er dissemination and implementation. Identiy the high impact strategies to replicate withinan expanded implementation initiative.
Clinicians and Healthcare ProvidersRecommendation: Develop, implement, andevaluate QI strategies that promote outpatientollowup or asthma care.
Strategy 1: In collaboration with public andprivate healthcare providers and educatorsand their respective organizations, conveneocus groups including clinicians rom varioustypes o clinical settings and disciplines (e.g.,primary care physicians, nurse practitioners,specialists, physician’s assistants, respiratory therapists, pharmacists) to generate QI
strategies that are simple and easible.
Strategy 2: Develop and implementstrategies targeted to patients who have asthmaand are discharged rom the ED or hospital.Tese strategies could include sta educationor a reminder system or the hospital andED sta.
Strategy 3: Develop and implement strategiesthat use pharmacy databases and EHRs to es-tablish reminder systems or clinicians working
in dierent healthcare settings.
Strategy 4: Explore use o “alternative”ollowup appointments, e.g., “e-mail appoint-ments” where e-mails are exchanged to see i an oce visit or change in prescription is war-ranted.
Purchasers and PayorsRecommendation: Examine insurance coveragegaps and other barriers linked to the possible
underutilization o routine outpatient ollowup visits and develop solutions to overcoming thesebarriers.
Strategy 1: Work through a national asthmapolicy orum, in coordination with the NAEPP,to convene a consortium o private and publichealthcare purchasers and payors, as well asselected members rom the GIP to examinesystems barriers to appropriate utilization o outpatient ollowup visits. Te consortiumwould develop and evaluate strategies designed
to overcome the barriers.
Strategy 2: Conduct a study that comparescurrent costs associated with utilization o outpatient clinics by asthma patients, who areseen across a variety o healthcare settings,with the current costs associated with inpatienthospital admissions or asthma (including costo medications). Use the results to documentwhether costs o outpatient care are a barrier to
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 37/52
The GIP Implementation Plan: Recommendations and Strategies 31
reimbursement or periodic clinical care; and/or whether costs explain the reason or adiscrepancy in time intervals between actualollowup visits and the intervals recommendedin the EPR-3.
Strategy 3: Encourage consortium members todevelop perormance measures/benchmarks
or appropriate ollowup care that are based onEPR-3 and that would be easible to track or QI and perormance measure purposes.
Strategy 4: Encourage consortium membersto use the asthma outpatient care quality benchmarks to conduct a series o pilot stud-ies. Tese studies would be used to evaluatethe easibility and benet o strategies, suchas pay-or-perormance, to close the gaps thatcontribute to underutilization o outpatientollow up visits.
Patient/Provider SupportPatients and providers should ollow therecommended actions or periodic visits, such aspatient attendance at regularly scheduled clinicalappointments and provider adjustment o medica-tion (stepping up or down as needed), to acilitatemeeting the goals o therapy and better controlo asthma. I certain tools and resources, e.g.,access to appropriate medications as determinedby the physician, are made available to patients and
providers, patient’s motivation and willingness toollow through with recommended actions may beimproved.
Patients with AsthmaRecommendation: Implement educational andmotivational strategies that can be broadly dissem-inated among all patients who have asthma.
Strategy 1: Encourage healthcare providers tosend patients hard-copy and electronic remind-ers, or telephone reminders o ollowup sched-
ules, including a brie and easy-to-understandlist o what to expect rom their asthma ol-lowup appointment.
Strategy 2: Develop policies among healthcareinsurance companies to provide incentives oroutpatient ollowup clinical evaluation.
Strategy 3: Educate all persons who haveasthma and their amilies about the importance
o outpatient ollowup care as part o a nationalasthma campaign and the broader NAEPPpartnership activities.
CliniciansRecommendation: Develop and provideclinicians with “user riendly” and practical toolsto support their ollowup assessment o asthma
control, adjustment (or maintenance) o medica-tions, and review o patient sel-management skillsor patients who have asthma.
Strategy 1: Convene a working group o GIPmembers and community-based clinicians toidentiy barriers aced by clinicians that may aect their capacity and motivation in imple-menting periodic asthma check-up visits.
Strategy 2: In light o the identied barriers,determine how to clearly and simply pres-
ent inormation rom the EPR-3 on ollowupmonitoring. Summarize this inormation anddisseminate widely to a varied groupo clinical audiences so they may adapt theinormation or use in their particularsettings.
Strategy 3: Work with stakeholders, includingthe private sector and proessional associa-tions, to disseminate a targeted and simpliededucational and motivational program to all
clinicians that addresses the described barriers.Tis could include innovative CME activitiesinormed by ocus groups, as well as educa-tional and motivational programs that integratemessages about periodic visits with other key messages rom EPR-3 as well. Tis strategy could be carried out through a national asthmacampaign in collaboration with the NAEPPand other interested partners,
Schools, School Nurses, and School-based Health Centers
Recommendation: Facilitate communicationbetween primary care provider’s oces andschools about students’ AAP, the role and valueo them, including the need or periodic ollowup visits as an integral element o the treatment.
Strategy 1: Working with the NAEPP SchoolEducation Subcommittee and the Center o Disease Control (CDC) working group on

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 38/52
32 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
AAPs, conduct ocus groups consisting o school personnel and parents to identiy barriers and explore ways that schools mightacilitate students making and keepingclinic appointments or periodic asthmaollowup care.
Strategy 2: Working with the above groups,
brainstorm strategies and tools that could beused to address these barriers. Strategies couldinclude asthma clinic times afer school or arequirement that proo o an asthma clinicalevaluation be provided at the beginning o theschool year.
Strategy 3: Pilot test the strategies and tools inselected schools and disseminate the results.
Message: CONTROL ENVIRONMENTAL EXPOSURES
Clinicians should review each patient’s expo-sure to allergens and irritants and provide amultipronged strategy to reduce exposure tothose allergens and irritants to which a patient issensitive and exposed, i.e., that make a patient’sasthma worse.
Evidence demonstrates that, or an allergen- andirritant-sensitive person who has asthma, substan-tially decreasing exposure to inhalant allergensmay signicantly reduce inammation, symptoms,
and the need or medication. Furthermore, certainrespiratory irritants such as tobacco smoke and airpollution are associated with increased symptomsand increased use o healthcare services. Tere-ore, a patient’s AAP should identiy individualallergens and irritants that worsen the patient’sasthma. Tis inormation may assist in avoidingunnecessary exposures to allergens/ irritants, or atleast be an alert to exposures that might indicate aneed or increased therapy. Also, clinicians shouldconsider a patient’s success with eorts to reduceexposure to allergens and irritants as part o his/
her decision to step up or down treatment orthe long-term management o asthma. Exposurecontrol o allergens and irritants at home, schoolor work is an important measure or achievingwell-controlled asthma and is likely to improvethe allergen- and irritant-sensitive patient’s quality o lie. Community resources, including in-homesupport or allergen and irritant reduction, arehelpul in controlling environmental actors thatcan make asthma worse.
CommunicationRationale: Conducting an initial environmentalassessment or patients who have asthma at any level o severity should provide inormation thatthe clinician can use to educate patients on actionsto take toward reducing exposure to those aller-gens and irritants that worsen a patient’s asthma.Using multiple approaches to reduce exposure
to known allergens/irritants is imperative oreective exposure control since individual stepsare generally ineective.
Conducting a more detailed environmental assess-ment in the patient’s home (or other settings wherea patient spends considerable time, such as schoolor work) may also be useul or certain patients(e.g., those whose asthma is not well-controlled orwhose asthma is work related).
For patients who have persistent asthma and are
exposed to indoor allergens year round, ollowupsteps to an initial environmental assessment may include allergy testing to determine sensitivity toallergens, with results considered in the context o the patient’s overall medical history. Conductingskin or in vitro testing to conrm sensitivity helpsto narrow the ocus o a patient’s allergen/irritantexposure control strategy to those actors that willhave the greatest eect.
Clinicians
Recommendation: Provide clinicians withuser-riendly, systematic and step-wise techniquesand tools or evaluating a patient’s environmentalexposures and their possible role in the patient’sasthma. Tese techniques/tools should includeguidance to aid the clinician in determining whenan initial environmental assessment by history alone is sucient, and when a more complete in-home, school or work assessment is needed. Tetechniques/tools should also address when allergy testing and reerral to a specialist is recommendedbased on EPR-3.
Strategy 1: As part o planning a national asth-ma campaign that addresses all six GIP mes-sages, work in collaboration with the NAEPPand its partners to include a message encourag-ing clinicians to identiy environmental actorsthat worsen a patient’s asthma and to considerthe patient’s success with eorts to control ac-tors capable o making asthma worse as parto the clinician’s decision to step up or down

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 39/52
The GIP Implementation Plan: Recommendations and Strategies 33
treatment or the long-term managemento asthma.
Strategy 2: Convene a workshop o experts inenvironmental control, asthma specialists, pri-mary care providers, asthma educators, patientadvocacy groups, employers and worker advo-cates to review existing tools and, as needed,
develop new tools and protocols. Proposedtools and protocols should address a variety o clinical settings and patient cultural/ethnicsituations. Te tools should be built upon thecore elements o an environmental assessmentidentied in EPR-3. Te tools should also oerselection criteria or complementary types o assessments (interview, in-home/at school orwork), and or allergy skin or in vitro testing.Disseminate the resulting products to health-care practitioners who treat asthma.
Strategy 3: Convene a workgroup o primary care providers, allergists, representatives o health plans, and State Medicaid MedicalDirectors to explore barriers to allergy testingin primary care settings to reach consensuson, and implement policies or, supporting theuse o allergy testing in accordance with EPR-3recommendations; and, to acilitate reerrals tospecialists, as appropriate, or consultation orcomanagement o patients.
Schools, School Nurses, Childcare Centers, and Schoolbased Health Centers:Recommendation: Inorm school/childcare per-sonnel about the potential impact o their site’senvironment on students’ management o theirasthma. Provide education on allergens and irri-tants requently ound in schools/childcare centersand on what the role o school sta is in helpingstudents and sta who have asthma with theirexposure control strategies. Focus specically onthose environmental actors identied in AAPs
on le or students who have asthma. Provideaordable, practical solutions or schools/childcarecenters to use or allergen/irritant reduction.
Strategy 1: Te NAEPP School EducationSubcommittee in collaboration with interestedproessional associations, patient educationgroups, boards o education, and governmentagencies, should reerence the EPR-3 to collate a
summary o the evidence regarding the impacto allergen and irritant exposure on asthmacontrol that is tailored to a school audience.Identiy and disseminate tools and strategiesthat have been proven to reduce allergens andirritants in school and childcare environmentsand improve students’ asthma outcomes.
Strategy 2: Build upon existing (and establishnew, i needed) methods and tools or contact-ing schools and childcare centers and orientingappropriate personnel on the importance o controlling environmental actors in the man-agement o asthma.
Strategy 3: Engage asthma coalitions, proes-sional associations, government agencies,asthma educators, school administrators, schooleducators and nurses at the State or local levelto develop and implement a coordinated plan
o action to reduce exposure based on provenapproaches identied in Strategy 1 above.
Strategy 4: Establish a system o communica-tion or leverage an existing network amongdesignated school or childcare sta, asthmaeducators, the student and student’s amily,school sta who have asthma, and healthcareproviders to help exchange inormation aboutand coordinate control o the allergens andirritants in the school or childcare setting that
worsen asthma.
WorkplaceRecommendation: Inorm healthcare providers,patients, occupational specialists, health benetsmanagers, payors, employee unions/ associations,and healthcare coordinators at the workplace aboutallergens and irritants ound in the workplace thatmay cause or exacerbate asthma. Provide educa-tion on preerred approaches or controlling ex-posure to these allergens and irritants. Encourageproviders to document work exposures to allergens
and irritants in the patient’s medical record andmake work-related asthma a reportable condition.Encourage population monitoring and registries.
Strategy 1: Summarize evidence cited in EPR-3and other credible scientic literature thatdescribes the impact allergens and irritantsound in the workplace can have on asthma,and preerred approaches to controlling these
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 40/52
34 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
exposures. Disseminate the summary tostakeholders in various presentation ormatsand through their existing communicationchannels.
Strategy 2: Coordinate with the workshop strat-egy described above under Communications,Clinicians, Strategy 2 to review existing tools
that assess the association between asthmasymptoms and exposures in the work environment. Select sample(s), or developa new tool, i needed, or dissemination tohealthcare providers, patients, and worksitesthat is practical and easy to use.
Patients and FamiliesRecommendation: Develop and deliver messagesto patients that help them understand the impor-tance and ways o reducing exposure to allergensand irritants that can make asthma worse.
Address with employers the barriers to andresources or changing workplace environments,including strengthening linkages to community resources.
Strategy 1: Engage partners to use social mar-keting and health communications approaches,possibly including ocus groups with patients,or insight on messages, strategies and resourc-es to eectively overcome barriers to control-ling or eliminating allergen/irritant exposures
in their immediate environments—home,school, childcare centers and work.
Strategy 2: Obtain eedback rom ocus groupson content and ormatting o tips sheets orpresenting environmental changes that wouldovercome barriers and that are readily achiev-able within the constraints o existing resourcesand current practices in the home, school,childcare centers and workplace.
Systems Integration
Rationale: Coordinate actions to control exposureto allergens and irritants among clinicians, publichealth providers, asthma educators, school andchildcare sta, members o Boards o Education,employers, workplace sta, and health plan ad-ministrators. Encourage systems that documentinstructions given or identiying allergens/irri-tants to which a patient is sensitive in the patient’schart; and, that also document the environmentalcontrol measures a patient agrees to and is able
to take. Documentation increases patient andclinician accountability or the implementation o environmental control measures and provides dataor monitoring such activities.
Commercial Health Plans and Healthcare PayorsRecommendation: Seek coordination and agree-
ment among health plans and payors on actionstaken with respect to environmental assessment,intervention, and monitoring, and on document-ing these actions in the patient’s medical chart.Documentation includes any reerrals made tospecialists or urther testing.
Strategy 1: Convene managed care compa-nies to work with NCQA to develop a HEDISmeasure o environmental assessment andmonitoring (including monitoring successwith adherence to an allergen/irritant exposure
control strategy); prepare a dissemination andimplementation plan or the HEDIS measureand tools; garner broad support or use o themeasure and accompanying implementationtools.
Strategy 2: Working through a national asthmapolicy orum, collaborate with the NAEPP andits partners to convene a workshop o proes-sional associations, patient education groups,health plans/payors and other stakeholders to
develop policies and protocols or reerral andreimbursement o allergen/irritant-exposurecontrol education, in-home education speci-cally tailored to the individual patient, in-homeand at-work assessments, and in-home support.
Strategy 3: Convene a meeting o managed carecompanies to discuss and ormulate strategieson how to incorporate and track environmentalassessment activities in their pay-or-peror-mance systems.
Electronic Health Record CompaniesRecommendation: Embed assessment and moni-toring o environmental actors at home, schooland work and a patient-tailored exposure controlstrategy into the EHR. Build verication into thesystem that clinicians considered the patient’seorts to control actors capable o making asthmaworse beore stepping medication up/down inasthma patients who are not well controlled. Teavailability o resources or conducting environ-

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 41/52
The GIP Implementation Plan: Recommendations and Strategies 35
mental assessments and educating patients on allergen/irritant exposure control within the EHRs will encourageclinician use and accountability.
Strategy 1: Encourage the NAEPP and its partners,working in collaboration with EHR companies,to establish agreed-upon samples o environmen-tal- and occupational-assessment questions and
exposure control strategies or inclusion in EHRs.
Strategy 2: Encourage EHR companies to createa system in the EHR that prompts the use o environmental/occupational assessment questionsand exposure control strategies or clinicians touse with their asthma patients, e.g., prompts anddecision supports.
Patient/Provider SupportRationale: Provide education and resources to patients,amilies and caregivers to help reduce allergen exposure,
emphasizing that this is an important component o asthma selmanagement that should improve the patient’sasthma control and quality o lie. Patient concerns andobstacles aced in changing their environments to reduceallergen/irritant exposure must be considered in select-ing and designing eective educational materials, pro-grams and strategies. In order to enhance the implemen-tation o exposure control measures, intervention toolsand education should be provided to healthcare provid-ers and asthma educators to assess exposure and sensitiv-ity to allergens and irritants and to help them develop
tailored allergen/irritant exposure control strategies.
Patients, Teir Families and CaregiversRecommendation: Provide resources (especially or pa-tients with persistent asthma) that are deemed necessary or allergen and irritant reduction based on a patient’ssensitivities and exposures. Tis applies to patients whoare exposed to and sensitive to allergens, irritants andenvironmental tobacco smoke (ES). Resources may include, but not be limited to: in-home supplies andservices; programs on smoking cessation and ES;inormation and reerral to health, housing and social
services; and, patient education programs and materials.Tese resources should be available in culturally sensitive venues and include low literacy and multi-lingual patientmaterials, programs and other strategies.
Strategy 1: Utilize results rom the CDC Community Guide ask Force on Community Preventive Services(developed with representation rom researchers,public health ocials, health educators, certied
asthma educators, and people diagnosed withasthma) that reviews current evidence orin-home interventions and the tools used orimplementation o such programs.
Strategy 2: Identiy existing repositories or, orgather inormation on, environmental controleducation resources such as educational pro-
grams, print materials, videos, and computer-based applications. Use existing or developnew criteria to identiy samples o “model”materials and programs that are posted to a virtual repository or asthma stakeholders. Dis-seminate inormation to stakeholders about theestablished Web site and the model materialsand programs and other resources ound thereand how to access them.
Strategy 3: Encourage proessional societies,government agencies and other NAEPP part-
ners to disseminate their print materials to con-stituents on request and to post them on theirrespective Web sites or easy access by patients,providers and the public. Also, post video andcomputer-based programs on each organiza-tion’s respective Web site, and consider links toresources on each other’s sites.
Strategy 4: Encourage asthma specialists, nursecoordinators, asthma educators, and com-munity healthcare proessionals and workers
to disseminate materials to patients and thepublic in local communities and make reerralsor persons who have asthma to appropriateprograms and services.
Strategy 5: Leverage existing asthma stakehold-er networks and structures to create new chan-nels o support or an overall national asthmacampaign to promote the GIP messages. Tesenew channels would utilize media (V, maga-zines), patient advocacy groups, and State andlocal agencies to help disseminate messages
including ES and allergens and irritants thataggravate asthma.
ProvidersRecommendation: Provide the appropriatesupport education and tools or assisting health-care providers in the assessment o allergens andirritants. Encourage clinicians to include suchassessment as a key clinical activity to asthma care.

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 42/52
36 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
Strategy 1: Prompt primary care providers viaEHRs or oce system prompts to obtain expo-sure and sensitivity inormation or indoor andoutdoor environmental allergens and irritantsto record in the patient’s chart.
Strategy 2: Promote inclusion o exposure andsensitivity assessment o indoor and outdoor
environmental allergens and irritants and thereduction methods advised or persons whohave asthma as part o the curriculum o under-graduate, graduate and continuing education orphysicians, nurses, respiratory therapists, asthmaeducators, and other related health care proes-sionals. Dierent requirements should be devel-oped or dierent categories o educators, suchas proessional-level educators, nurses, masters-trained educators, and community level workers.
Strategy 3: Develop training resources and
protocols to promote allergy testing in primary care sites, including preparation to deal withpossible anaphalaxis.

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 43/52
Partners Putting GuidelinesInto Action
Guidelines Implementation Panel Report for: Expert Panel Report 3—Guidelines for the
Diagnosis and Management of Asthma
APPENDICES
Appendices 37
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 44/52
38 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
aPPendIX a
Ranking the Level of Evidence for Asthma GuidelinesRecommendations
Te system used to describe the level o evidence isas ollows (Jadad et al. 2000):
n Evidence Category A: Randomized controlledtrials (RCs), rich body o data. Evidence isrom end points o well-designed RCs thatprovide a consistent pattern o ndings inthe population or which the recommendationis made. Category A requires substantial
numbers o studies involving substantialnumbers o participants.n Evidence Category B: RCs, limited body o
data. Evidence is rom end points o interven-tion studies that include only a limited numbero patients, post hoc or subgroup analysis o RCs, or meta-analysis o RCs. In general,Category B pertains when ew randomizedtrials exist, they are small in size, they wereundertaken in a population that diers romthe target population o the recommendation,or the results are somewhat inconsistent.
n Evidence Category C: Nonrandomized trialsand observational studies. Evidence is romoutcomes o uncontrolled or nonrandomizedtrials or rom observational studies.
n Evidence Category D: Panel consensus judgment. Tis category is used only in caseswhere the provision o some guidance wasdeemed valuable, but the clinical literatureaddressing the subject was insucient to justiy
placement in one o the other categories. TePanel consensus is based on clinical experienceor knowledge that does not meet the criteria orcategories A through C.
Jadad AR, Moher M, Browman GP, Booker L, SigouinC, Fuentes M, Stevens R. Systematic reviews and meta-analtses on treatment o asthma: critical evaluation. BMJ2000;320(7234):537-40
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 45/52
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 46/52
40 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
Below is a list o the ve issues ollowed by anoverall objective and specic strategies to achievethe objective.(Adapted rom Improving Chronic Illness Care2,http://www.improvingchroniccare.org)
Patient saety —Health SystemCreate a culture, organization, and mechanisms that
promote sae, high-quality care. • Visiblysupportimprovementatalllevelsofthe
organization, beginning with the senior leader.• Promoteeectiveimprovementstrategies
aimed at comprehensive system change.• Encourageopenandsystematichandlingof
errors and quality problems to improve care.• Provideincentivesbasedonqualityofcare.• Developagreementsthatfacilitatecare
coordination within and across organizations.
Cultural competency —Delivery System Design
Sel-Management Support Empower and prepare patients to manage their health and healthcare.• Emphasizethepatient’scentralrolein
managing their health.• Useeectiveself-managementsupport
strategies that include assessment, goalsetting,action planning, problemsolving andollowup.
• Organizeinternalandcommunityresources to provide ongoing sel-management support
to patients.
Care coordination—Health System and ClinicalInormation SystemsDecision Support Promote clinical care that is consistent with scienticevidence and patient preerences.• Embedevidence-basedguidelinesintodaily
clinical practice.• Shareevidence-basedguidelinesand
inormation with patients to encourage theirparticipation.
• Useprovenprovidereducationmethods.• Integratespecialistexpertiseandprimarycare.
Organize patient and population data to acilitateecient and efective care.• Providetimelyremindersforprovidersand
patients.• Identifyrelevantsubpopulationsforproactive
care.
• Facilitateindividualpatientcareplanning.• Shareinformationwithpatientsandprovidersto
coordinate care.• Monitorperformanceofpracticeteamandcare
system.
Community policies—Community Resourcesand Policies
Mobilize community resources to meet needso patients.• Encouragepatientstoparticipateineective
community programs.• Formpartnershipswithcommunityorganiza-
tions to support and develop interventions thatll gaps in needed services.
• Advocateforpoliciestoimprovepatientcareandasthma-riendly community environments (e.g.,no smoking policies).
Case management - Delivery System Design
Assure the delivery o efective, ecient clinical careand sel-management support.• Denerolesanddistributetasksamongteam
members.• Useplannedinteractionstosupportevidence-
based care.• Provideclinicalcasemanagementservicesfor
patients whose asthma is dicult to control,who have signicant co-morbidities aectingtheir asthma, or have diculties ollowing theirasthma action plan.
• Ensureregularfollowupbythecareteam.• Givecarethatpatientsunderstandandthatts with their cultural background.
Summary o Patient Care Model/Improving Chronic IllnessWhile the GIP chose to base its recommendationsor implementation on a patient-centered model,there is no one individual model that osters changein the health care system. All models containsimilar concepts and goals and employ strategiesthat seek changes rom all entities involved in the
complicated American health system. Tis guideseeks to encourage health systems, providers, sup-porting businesses and organizations, patients, theiramilies and caregivers to seek high-quality careand to become involved in making changes in thecurrent care system. Further inormation regardingthe many concepts and models o the CCM can beound by accessing the listed resources.

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 47/52
Appendix B 41
Reerences:Excerpts rom “Crossing the Quality Chasm:
A New Health System or the 21st Century,Committee on Quality o Health Care inAmerica, Institute o Medicine, Te NationalAcademies 2001.
“Improving Chronic Illness Care” —http://www.
improvingchroniccare.org/ Bibliography: • InstituteforHealthcareImprovement
(www.IHI.org)• WagnerEH.Chronic disease management:
what will it take to improve care or chronicillness? E Clin Pract. 1998; 1:2-4
• WagnerEH,AustinBT,DavisC,HindmarshM, Schaeer J, Bonomi A. Improving chronicillness care: translating evidence into action.Health A (Millwood). 2001;20:64-78.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 48/52
42 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
APPENDIX C
Health Disparities
A crosscutting theme o this GIP report thattranscends all six messages is to reduce healthdisparities rom asthma. Te burden o asthma isnot uniorm across all populations. Low-incomepeople and racial and ethnic minorities are dis-proportionately aected. Asthma prevalence is 25percent higher among American Indian or AlaskaNative children, 60 percent higher among black children and 140 percent higher among Puerto
Rican children relative to white children. Black children have a 260 percent higher Emergency Department (ED) visit rate and a 250 percenthigher hospitalization rate rom asthma comparedto white children. Despite the higher burden o disease among these populations, access to medicalcare or asthma and the quality o care providedis ofen lower among the minority and socio-eco-nomically disadvantaged populations. Exposureto asthma triggers is also more requent. Tesedisparities in asthma burden and care suggest thatspecial eorts are needed to implement the EPR-3
guidelines in these populations.
All stakeholders involved in controlling asthmahave a role to play in reducing asthma-relatedhealth disparities. Te GIP suggests that thestakeholders consider the ollowing strategies.
Improving the quality o medical care.
Health Resources and Services Administration(HRSA) Federally Qualied Health Centers(FQHCs), public hospitals, insurers with low-income members, Medicaid agencies)
• Supportqualityimprovementeortsamong saety-net providers. Tese eorts may include registry development, electronichealth records, quality improvementcollaboratives, audit and eedback andorganizational redesign.
• Assuretheculturalappropriatenessofcare, including the cultural competence o
providers through the provision o trainingand toolkits, access to interpreters,adherence to Culturally and Linguistically Appropriate standards, and provisiono translated and culturally relevant patienteducation resources.
• Helpprovidersandpatientsdevelopmore eective communication by trainingproviders in cross-cultural, patient-centered
methods and by teaching patients to bringtheir concerns and questions to their provider visits.
Improving sel-management support.• Oerhomevisitsbycommunityhealth
workers to patients with uncontrolled asthma(e.g., disseminate Integrated ConditionAssessment System and Healthy Homes programs), (nongovernmentalorganizations (NGOs), local healthdepartments, FQHCs).
• Providecommunity-basedasthmaeducation classes (NGOs, local health departments,FQHCs).
• Reimburseforself-managementsupport (Medicaid, insurers).
Improving care coordination and casemanagement.
• Coordinateprimarycarewithspecialtycare, schools and community resources throughpatient care coordinators or health systemnavigators (FQHCs, NGOs).
• Providecasemanagementforpatientswith high risk or exacerbations (NGOs, localhealth departments, FQHCs, insurers).
• Reimburseforcarecoordinationandcase management (Medicaid, insurers).
Improving outreach and community education.
• Increaseawarenessofasthmainlow-incomeand racial/ethnic minority communities
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 49/52
Appendix C 43
through multilingual, culturally-relevantawareness campaigns (NGOs and local andstate health departments).
• Developcommonmessagesandmedia resources or local use.
• Increaseawarenessthroughdeploymentof community health workers/educators(NGOs, local health departments).
• Increaseawarenessofasthmaamong providers o social services to low incomeand racial/minority communities so thatthey can make appropriate reerrals(local health departments).
Improving surveillance o disparities.• Reportonqualityandoutcomesofasthma
care by race/ethnicity, income and insurancestatus (health providers, insurers, healthcarequality organizations).
• Reportonasthmaprevalence,exposureto
asthma triggers, urgent health servicesutilization (ED and hospital) and access tomedical homes by race/ethnicity, incomeand insurance status (local, state andnational public health agencies).
Improving control o environmental actors thatafect asthma.
• Provideresourcesforenvironmental control (e.g., bedding encasements, vacuums, cleaning supplies, High Eciency
Particulate Air lters) as part o comprehen-sive asthma education and trigger reductionprograms (Insurers, Medicaid).
• Assureaccesstoallergytestingby training saety net providers in skin testingor use o Radioallergosorbent est testing(HRSA, insurers, local public health).
Improving housing quality .
• Providehomeenvironmentalinspections or low income and racial/ethnic minority households (NGOs, local health
departments, FQHCs).• Oeradviceandassistancetolowincome
and racial/ethnic minority households,landlords and public housing agencies toremediate structural problems that contrib-ute to increased exposure to asthma triggers(NGOs, local health departments, FQHCs).
• Improvelocalhousingcodessothatthey reect current knowledge o Healthy Homesbuilding and maintenance practices
(local public health, local/state/nationalhousing code organizations, local housinginspection agencies).
• Trainlocalhousinginspectorsandother home visitors in the recognition o unhealthy indoor environmental conditionsand in the procedures to reer householdsor assistance in remediation o these
conditions (local public health).
Improving ambient air quality .• Locateschoolsandresidentialdevelopments
away rom sources o ozone, particulatematter, nitrogen oxides, reeways, industrialsources and transportation hubs (localpublic health, local asthma coalitions, localzoning and planning agencies, local transitand transportation agencies, schooldistricts).
Improving community capacity to controlasthma.
• Encouragecollaborativepartnershipsforlocal asthma coalitions to enhance theirability to contribute to community awareness,integration o services across sectors, andacilitating accountability or addressingasthma disparities.
Akinbami LJ. Te State o childhood asthma, United States,1980–2005. Advance data rom vital and health statistics; no381, Hyattsville, MD: National Center or Health Statistics.
2006.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 50/52
44 National Asthma Education and Prevention Program Guidelines Implementation Panel Report
APPENDIX D
Abbreviations
AAP Asthma Action Plan
AHIP America’s Health Insurance Plans
AMGA American Medical Group Association
BCBSA Blue Cross and Blue Shield Association
CCM Chronic Care Model
CDC Centers for Disease Control and
Prevention
CME Continuing Medical Education
CMS Centers for Medicare and Medicaid
Services
ED Emergency Department
EHR Electronic Health Records
EPR-3 Expert Panel Report 3: Guidelines for
the Diagnosis and Management of
Asthma, 2007
ETS Environmental Tobacco Smoke
FQHC FederallyQualiedHealthCenters
GIP Guidelines Implementation Panel
HEDIS Healthcare Effectiveness Data and
Information Set
HMO Health Maintenance Organization
ICS Inhaled Corticosteroids
IOM Institute of Medicine
MCO Managed Care Organization
MOC MaintenanceofCertication
NAEPP National Asthma Education and
Prevention Program
NCQA National Committee on Quality
Assurance
NGO Non-Government Organization
NHLBI National Heart, Lung, and Blood
Institute
PBM PharmacyBenetsManager
QI Quality Improvement

8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 51/52
For More Information
The National Heart, Lung, and Blood Institute (NHLBI) Health Inormation Center
(HIC) is a service o the NHLBI o the National Institutes o Health. The NHLBI HICprovides inormation to health proessionals, patients, and the public about the
HIC treatment, diagnosis, and prevention o heart, lung, and blooddiseases and sleep disorders. For more inormation, contact:
NHLBI Health Inormation Center
P.O. Box 30105Bethesda, MD 20824-0105Phone: 301-592-8573
TTY: 240-629-3255Fax: 301-592-8563Web site: http://www.nhlbi.nih.gov
DISCRIMINATION PROHIBITED: Under provisions o applicable public laws enacted
by Congress since 1964, no person in the United States shall, on the grounds o race,color, national origin, handicap, or age, be excluded rom participation in, be denied
the benefts o, or be subjected to discrimination under any program or activity (or, onthe basis o sex, with respect to any education program and activity) receiving Federalfnancial assistance. In addition, Executive Order 11141 prohibits discrimination on
the basis o age by contractors and subcontractors in the perormance o Federalcontracts, and Executive Order 11246 States that no ederally unded contractor may
discriminate against any employee or applicant or employment because o race, color,religion, sex, or national origin. Thereore, the National Heart, Lung, and Blood Insti-
tute must be operated in compliance with these laws and Executive Orders.
8/7/2019 NHLBI Ashma Implementation
http://slidepdf.com/reader/full/nhlbi-ashma-implementation 52/52