nguyen trường giang perfusion computed tomography in acute ischaemic stroke jfim hanoi 2015
TRANSCRIPT

Perfusion Computed Tomography in
Acute Ischaemic Stroke
Nguyễn Trường Giang Thai Nguyen Central General Hospital, Vietnam Central for Advanced Imaging, The University of Queensland, Australia
Hanoi, nov 2015

Outline
u Brief introduction u Stroke Imaging u Perfusion CT techniques u Use of perfusion CT in acute stroke u Future direction of perfusion CT u Conclusion
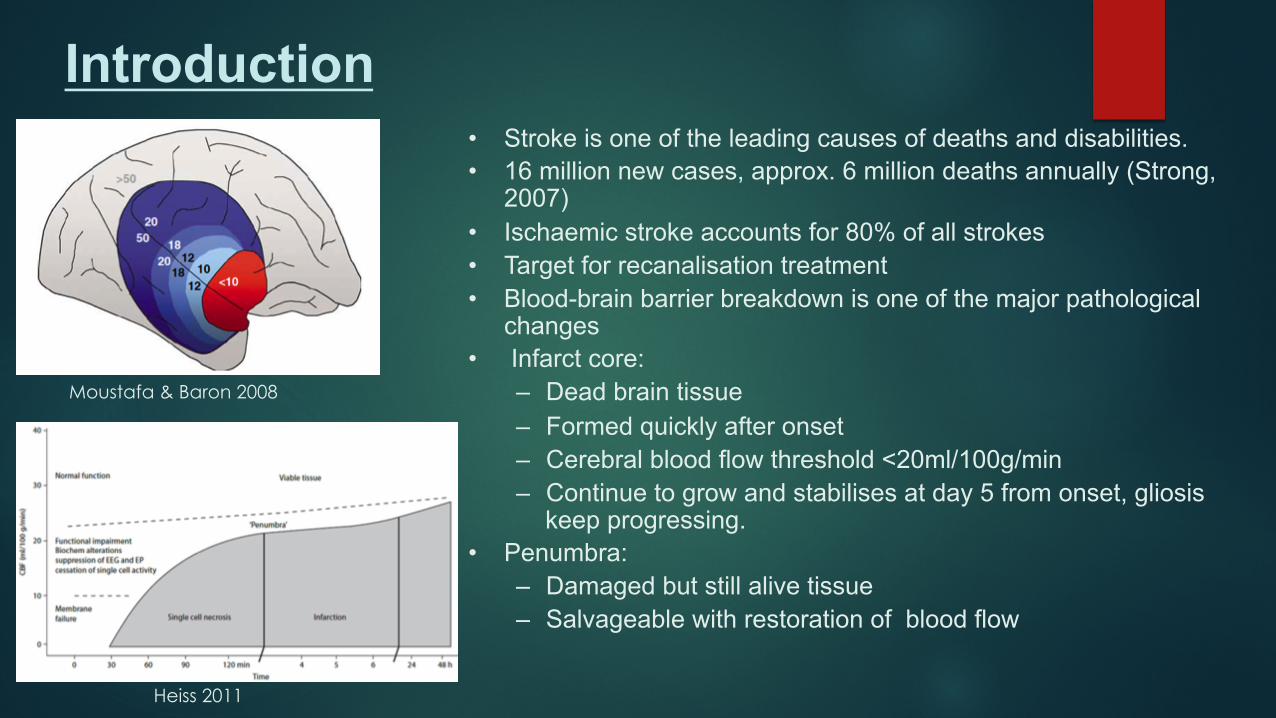
Introduction • Stroke is one of the leading causes of deaths and disabilities. • 16 million new cases, approx. 6 million deaths annually (Strong,
2007) • Ischaemic stroke accounts for 80% of all strokes • Target for recanalisation treatment • Blood-brain barrier breakdown is one of the major pathological
changes • Infarct core:
– Dead brain tissue – Formed quickly after onset – Cerebral blood flow threshold <20ml/100g/min – Continue to grow and stabilises at day 5 from onset, gliosis
keep progressing. • Penumbra:
– Damaged but still alive tissue – Salvageable with restoration of blood flow
Moustafa & Baron 2008
Heiss 2011
Four critical questions must be answered at patient admission (Shetty & Lev 2005):
a. Is this a haemorrhagic stroke? b. Is there thrombotic occlusion of a cerebral artery that can be treated
by thrombolysis or thrombectomy? c. Is an infarct core present in the ischaemic region? d. Is there potentially salvageable penumbral tissue?
Introduction

Stroke Imaging
u Target for Stroke Imaging: u Gives early diagnosis
u Differentiates subtypes of stroke
u Gives accurate amount of affected brain tissue and amount of dead brain
u Unenhanced CT, CT Angiography & Perfusion CT u Magnetic Resonance Imaging, MRA & MRP u DSA & Endovascular intervention

Stroke Imaging
4+ Ps in Stroke u Parenchyma: Indicate the early signs of acute ischaemic stroke, exclude haemorrhage
u Pipes: Gives information of vessels u Extracranial circulation (carotid and vertebral arteries of the neck)
u Intracranial circulation for evidence of intravascular thrombus
u Perfusion Assess cerebral blood volume, cerebral blood flow, and mean transit time
u Penumbra Assess tissue at risk of dying if ischemia continues without recanalization of intravascular thrombus Imaging.
u Permeability: Evaluate changes in blood-brain barrier permeability following ischaemic insult
Rowley (2001) AJNR 22(4):599-601

Stroke Imaging: Un-enhanced CT
Early signs of ischaemic stroke include:
u Dense MCA
u Obscuration of lentiform nucleus
u Narrowing of cerebral sulci

Stroke Imaging: CT angiography
• Indicate location, size of the clot • Give information of collateral vessel • Evaluate tortuosity of the carotid, access path of thrombectomy
Srinivasan (2006) Radiographics
Stroke Imaging: Perfusion CT
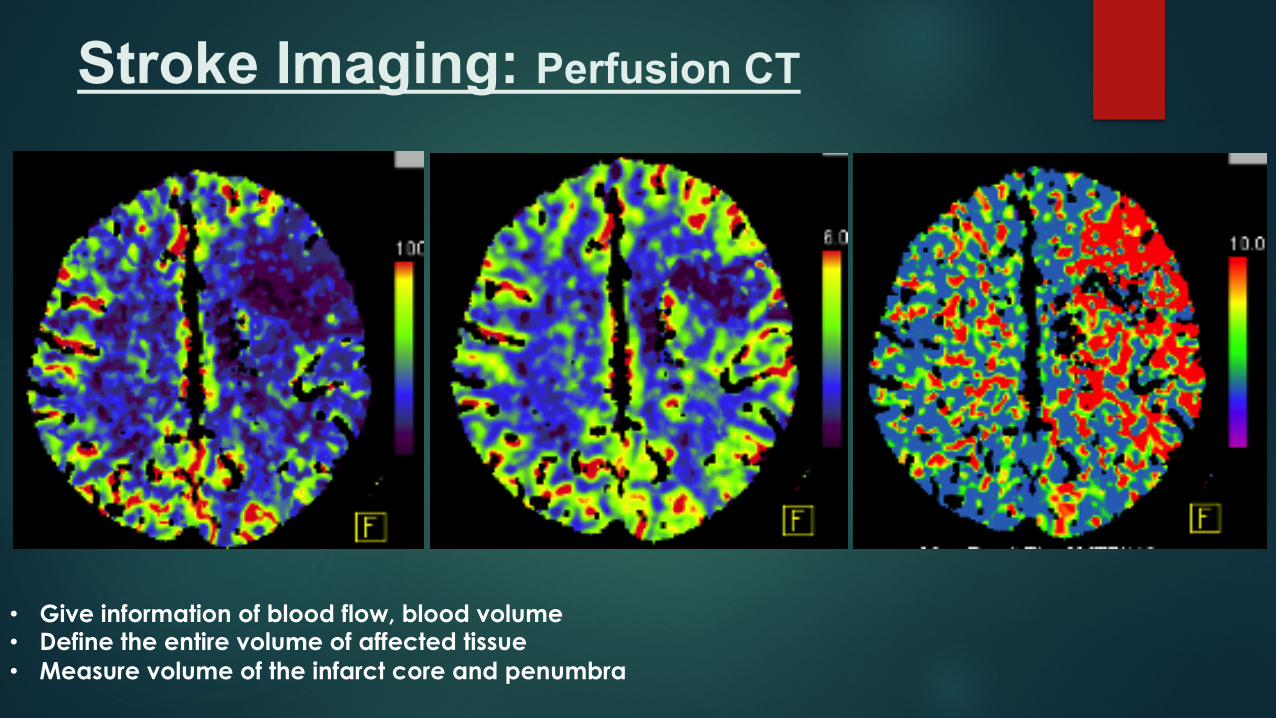
• Give information of blood flow, blood volume • Define the entire volume of affected tissue • Measure volume of the infarct core and penumbra

u Cerebral blood flow (CBF): Infarct starts when CBF<20ml/100g/min
u Cerebral blood volume (CBV): infarct threshold 2ml/100g
u Mean transit time (MTT): Abnormal threshold >145% compared to the contralateral hemisphere
u Time to peak (TPP): Abnormal cut off 4 seconds delay compared to the opposite side.
Giang Nguyen 2013, PhD Thesis, University of Queensland
Stroke Imaging: Perfusion CT
Wintermark 2006
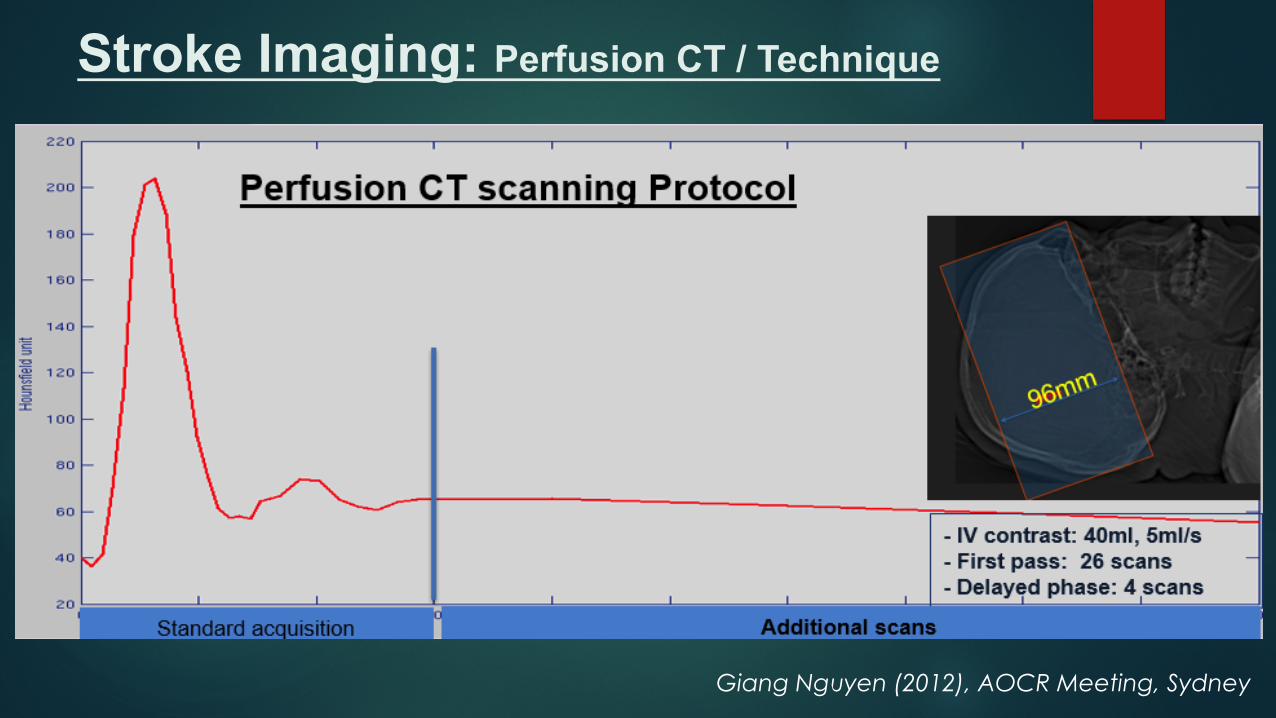
Stroke Imaging: Perfusion CT / Technique
Giang Nguyen (2012), AOCR Meeting, Sydney

Stroke Imaging: Perfusion CT / Technique
Giang Nguyen (2013) NeuroImage: Clinical
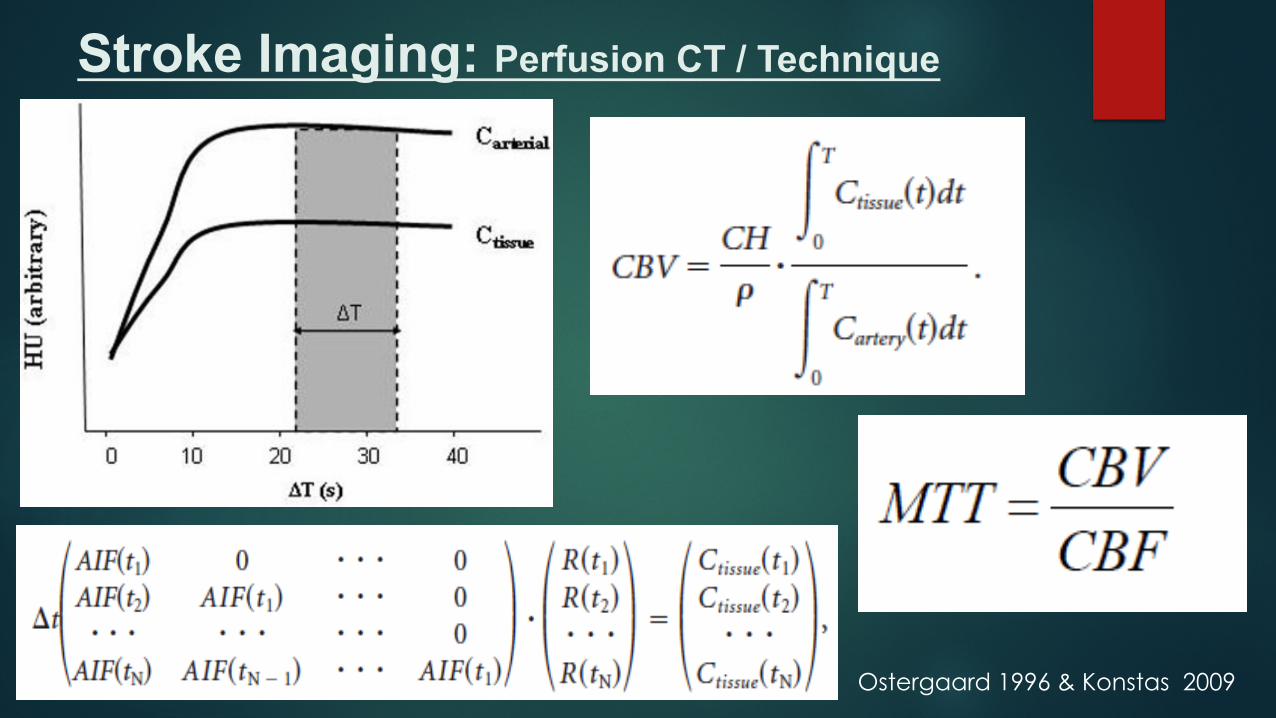
Stroke Imaging: Perfusion CT / Technique
Ostergaard 1996 & Konstas 2009

Stroke Imaging: Perfusion CT
CBF CBV MTT

Stroke Imaging: Perfusion CT / Permeability
Stroke Imaging: Perfusion CT / Permeability
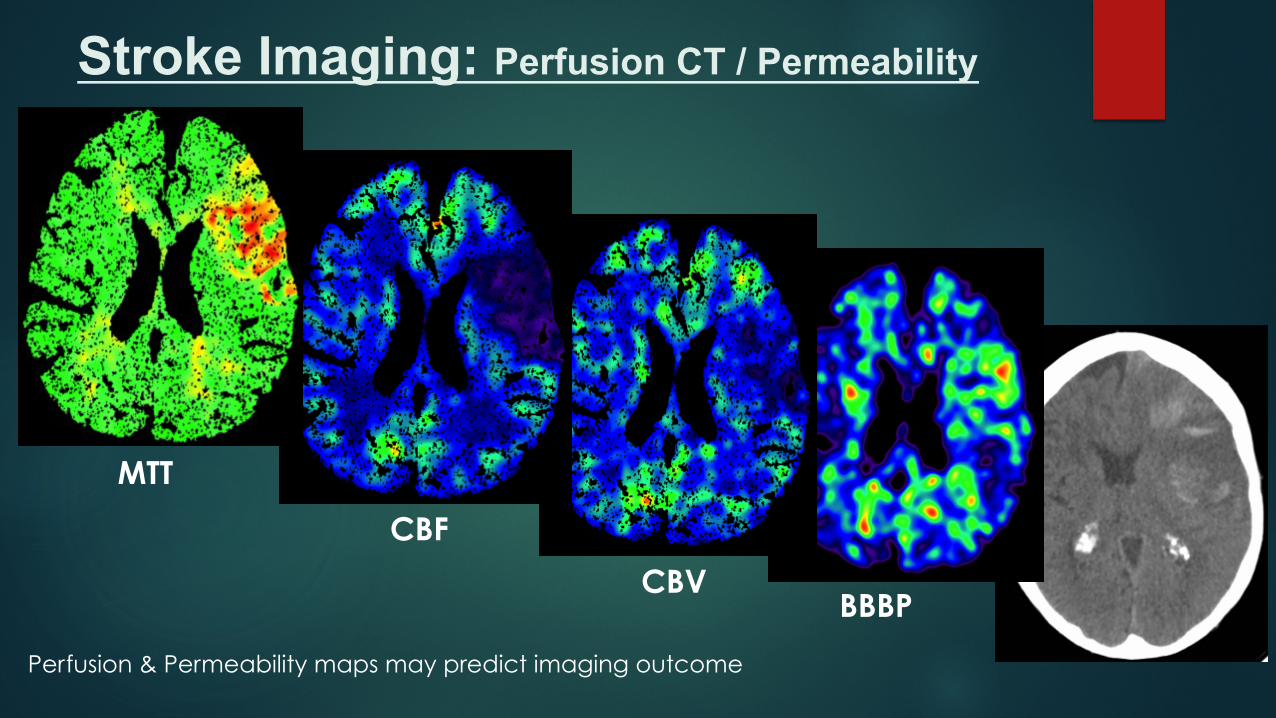
MTT
CBF
CBV BBBP
Perfusion & Permeability maps may predict imaging outcome
Stroke Imaging: Perfusion CT / Permeability
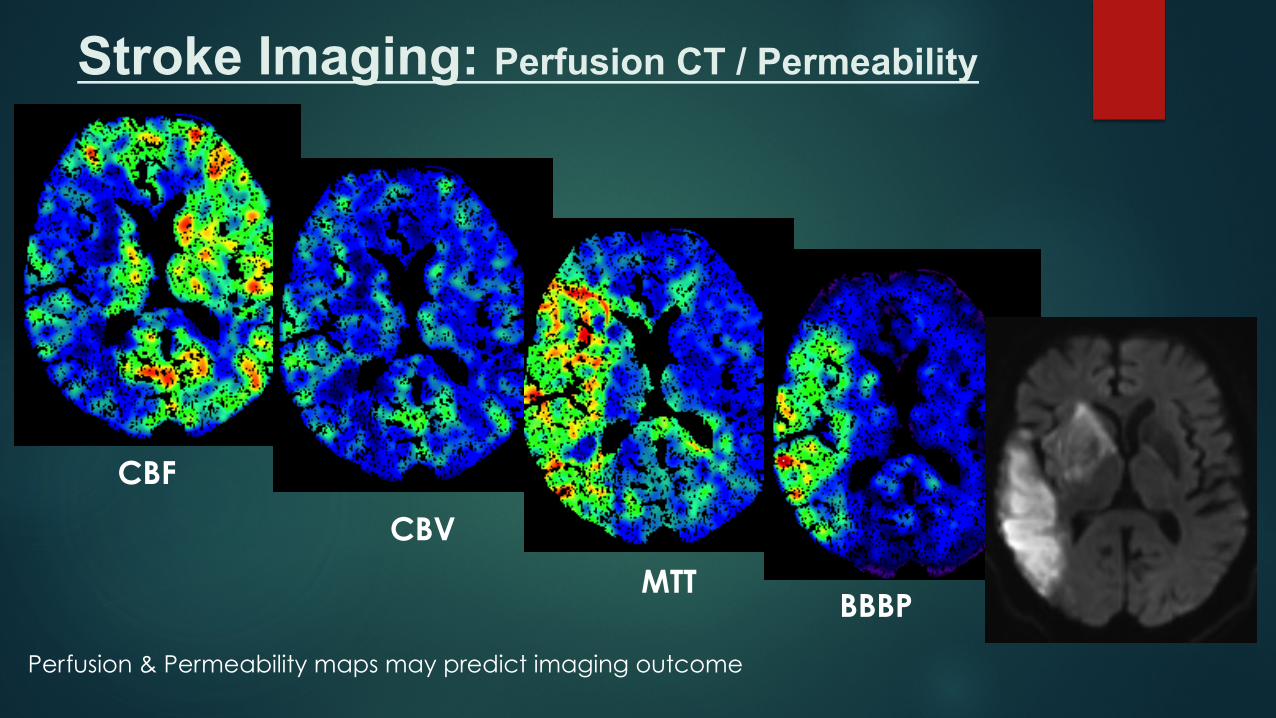
CBF
CBV
MTT BBBP
Perfusion & Permeability maps may predict imaging outcome

Stroke Imaging: Perfusion CT / Permeability
CBF
CBV
MTT BBBP
Perfusion & Permeability maps may predict imaging outcome

u Perfusion CT can be used in patient selection in some stroke centres • Help to measure brain perfusion & blood-brain barrier permeability
• High sensitive in detection ischaemic stroke in anterior circulation (Bivard 2013)
• May help predict complications (haemorrhage, massive oedema) (Nguyen 2013)
• Help considering recanalisation treatment
u However, current stroke guidelines have not included perfusion CT
§ Lacuna, posterior circulation lesions and reperfusion information need to be validated (Bivard 2013)
§ CBV based infarct volume may not replace DWI – MRI (Copen 2015)
§ Perfusion parameters are varied between software packages (Kudo 2013)
§ Benefit of Perfusion CT for selecting patients has not ben proven (Power 2015)
§ Further randomised studies are necessary (Power 2015)
Stroke Imaging: Perfusion CT / Permeability

Stroke Imaging: Perfusion CT / Technique
SVD: Single Value Decomposition IF: Inverse Filter MS: Maximum Slope bMTF: Box Modular Transfer Function
Kudo (2010) Radiology
A variety of mathematic algorithms applied to measure perfusion parameters used in different software packages may lead to inconsistency in blood flow measurement
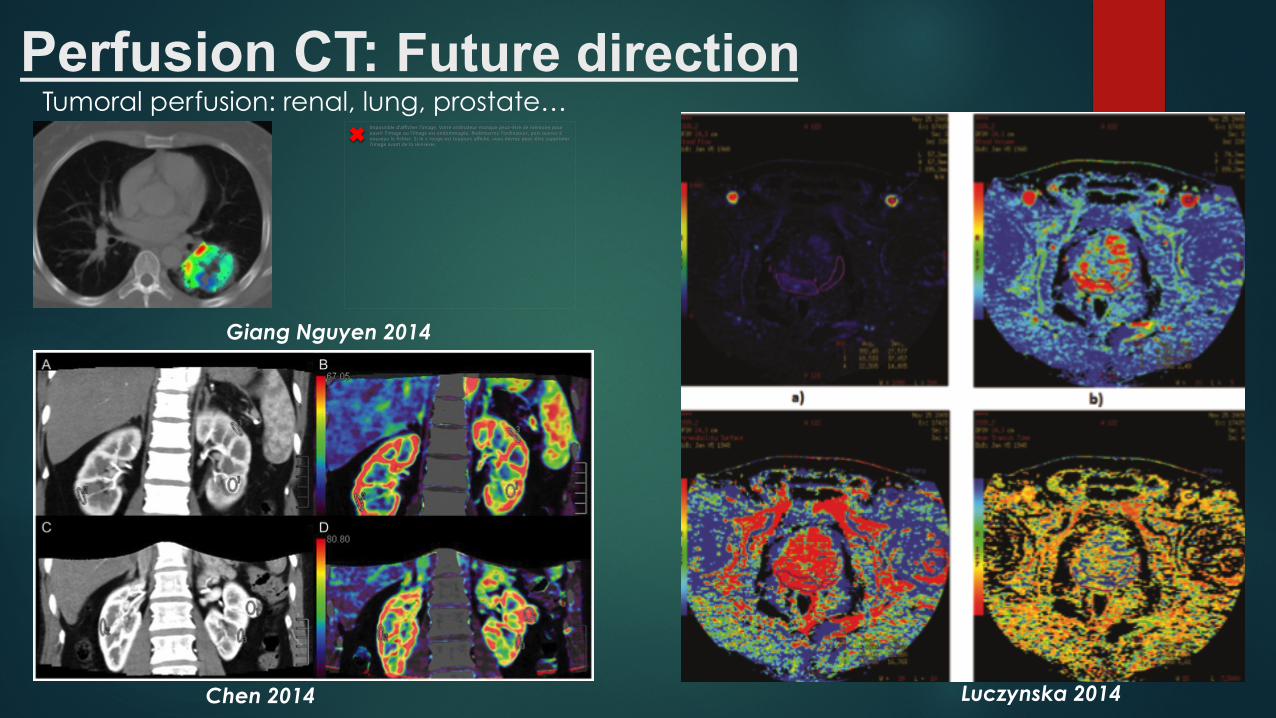
Perfusion CT: Future direction Tumoral perfusion: renal, lung, prostate…
Impossible d'afficher l'image. Votre ordinateur manque peut-être de mémoire pour ouvrir l'image ou l'image est endommagée. Redémarrez l'ordinateur, puis ouvrez à nouveau le fichier. Si le x rouge est toujours affiché, vous devrez peut-être supprimer l'image avant de la réinsérer.
Luczynska 2014 Chen 2014
Giang Nguyen 2014

Conclusion o Perfusion CT give the last 3 Ps in 4P+ in Stroke imaging: Perfusion, Penumbra
& Permeability
o Along with CT, CTA, Perfusion CT may help in patient selection for recanalisation treatment
o Perfusion CT may help to predict stroke complications and radiological outcome
o Perfusion CT may be more accessible than MRI in many stroke centres
o Software to create perfusion map needs to be consistent
o More randomised studies needed for prove benefit of perfusion CT
o Perfusion CT may be used in other body parts: lung, prostate…

Thank you!
Acknowledgement:
• Centre for Advanced Imaging, University of Queensland, Australia: David Reutens
• Royal Brisbane & Women’s Hospital, Australia:
• Alan Coulthard
• Andrew Wong
• Robert Henderson
• Dept of Radiology, Newcastle Hospital, NSW, Australia: Mark Parsons
• Thái Nguyên Central General Hospital, Vietnam