l arrive mrcp jfim hanoi 2015
TRANSCRIPT

MR cholangiography
Lionel Arrivé Hôpital Saint Antoine Paris
Hanoi nov 7th 2015

MRCP
� FSE sequences are very heavily T2-weighted
� High signal intensity from static fluid � Classical MRCP included 2D sequences � Modern MRCP should include 3D
sequences which improve both spatial resolution and contrast/noise ratio

2D versus 3D 2D 3D
S/N ratio improves with number of source images
TA 2D = TR x Nex x Ny TA 3D = TA 2D x Nz













Advantages Limitations
• Near isotropic voxel • High resolution (1x1x1mm) • Multiplanar reconstructions
• Excellent signal/noise ratio
• Time of acquisition
• Regular breathing
• Source images analysis
• Multiplanar reconstructions
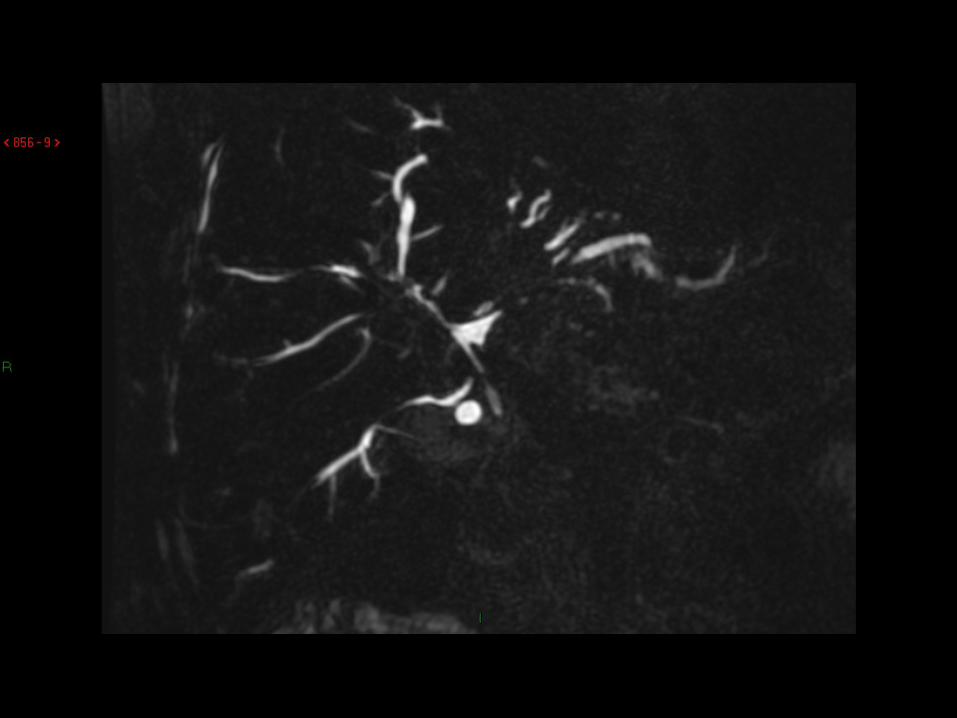
3D Sequence













2D Sequences
Still useful ?
• Poor quality of 3D sequences • When one is in a true rush ! • For dynamic analysis







Bowel signal suppression
• Paramagnetic contrast (diluted gadolinium) ou superparamagnetic contrast media
• Blueberry juice • Black tea • Pineapple juice (high concentration of
manganese)



Complementary sequences
• At least a 3D fat-supressed T1-weighted MR sequence for detection of biliary stones
• A T2-weighted MR sequence : FSE, SSFSE, or diffusion-weighted at B0
• Gadolinium injection is only optional





Systematic analysis technique
• 3D MRCP : biliary ducts analysis • T2-weighted MR sequence : liver
heterogeneity and dysmorphia • T1-weighted MR sequence : biliary stones • After gadolinium injection : heterogeneity of
contrast enhancement, biliary ducts enhancement, focal hepatic lesion

Systematic analysis technique
• Biliary ducts analysis : moderate or severe (75%) stenosis, short (2 mm) or long (10 mm), localized (25%) or diffuse
• Biliary ducts dilatation and biliary stones • Liver heterogeneity and dysmorphia • Liver and biliary duct enhancement

Systematic analysis technique
• Biliary ducts analysis : moderate or severe (75%) STENOSIS, short (2 mm) or long (10 mm), localized (25%) or diffuse
• Biliary duct DILATATION and biliary stones • Liver heterogeneity and dysmorphia • Liver and biliary duct enhancement







Biliary MR Imaging
Multiples traps ! BUT
90% of pitfalls are related to
- Overuse of the term «biliary ducts irregularities» - Overinterpretation of hepatic artery mark

Biliary MR Imaging
Multiples traps ! BUT
90% of pitfalls are related to
- Overuse of the term «biliary ducts irregularities» - Overinterpretation of hepatic artery mark













MRCP : other traps
• MR system performances (3D MRCP) • Patient information : Regular breathing • Learning curve : inter-observer variability • Numerous other traps

MRCP : other traps
• MR system performances (3D MRCP) • Patient information : Regular breathing • Learning curve : inter-observer variability • Numerous other traps: BILIARY CONTENT











Biliary MR Imaging
Multiples traps ! BUT
90% of pitfalls are related to
- Overuse of the term «biliary ducts irregularities» - Overinterpretation of hepatic artery mark

Biliary MR Imaging
Multiples traps ! BUT
90% of pitfalls are related to
- Overuse of the term «biliary ducts irregularities» - Overinterpretation of hepatic artery mark

Systematic analysis technique
• Biliary ducts analysis : moderate or severe (75%) STENOSIS, short (2 mm) or long (10 mm), localized (25%) or diffuse
• Biliary duct DILATATION and biliary stones • Liver heterogeneity and dysmorphia • Liver and biliary duct enhancement



Conclusion
• 3D MRCP with analysis of source images and multiplanar and volume reconstruction
• Don’t forget Fat-sat 3D T1-weighted MR sequence • There is a significant learning curve and analysis should
use a systematic technique • There is a lot of traps and pitfalls but 90% are related to
misuse of the term « irregularities of biliary ducts » and to misinterpretation of hepatic artery mark