newborn infant screening and assessment: emerging technologies and protocols
DESCRIPTION
NEWBORN INFANT SCREENING AND ASSESSMENT: Emerging Technologies and Protocols. James W. Hall III, Ph.D. Clinical Professor and Chair Department of Communicative Disorders College of Health Professions University of Florida Gainesville, Florida 32610-0174 [email protected]. - PowerPoint PPT PresentationTRANSCRIPT
NEWBORN INFANT SCREENING AND ASSESSMENT:
Emerging Technologies and Protocols
James W. Hall III, Ph.D.James W. Hall III, Ph.D.
Clinical Professor and ChairClinical Professor and Chair
Department of Communicative DisordersDepartment of Communicative Disorders
College of Health ProfessionsCollege of Health Professions
University of FloridaUniversity of Florida
Gainesville, Florida 32610-0174Gainesville, Florida 32610-0174
[email protected]@hp.ufl.edu


Marion Downs“Grandmother of Newborn Hearing Screening”

Year 2000 JCIH Position Statement: Principles and Guidelines for Early Hearing
Detection and Intervention Programs
JCIH = Joint Committee on Infant HearingJCIH = Joint Committee on Infant Hearing Published in:Published in:
Audiology TodayAudiology Today (Special Issue):(Special Issue): August 2000, pp. 6-27 August 2000, pp. 6-27 American Journal of Audiology 9American Journal of Audiology 9: 9-29, 2000.: 9-29, 2000. www.audiology.orgwww.audiology.org
Member organizations:Member organizations: American Academy of Audiology & ASHAAmerican Academy of Audiology & ASHA American Academy of Otolaryngology-Head & Neck SurgeryAmerican Academy of Otolaryngology-Head & Neck Surgery American Academy of PediatricsAmerican Academy of Pediatrics Council on Education of the DeafCouncil on Education of the Deaf Directors of Speech and Hearing Programs in State and Welfare Directors of Speech and Hearing Programs in State and Welfare
AgenciesAgencies

Illness or condition requiring admission of Illness or condition requiring admission of >> 48 hours to 48 hours to an NICU.an NICU.
Stigmata or other findings associated with a syndrome Stigmata or other findings associated with a syndrome known to include a sensorineural or conductive hearing known to include a sensorineural or conductive hearing loss.loss.
Family history of permanent childhood sensorineural Family history of permanent childhood sensorineural hearing losshearing loss
Craniofacial anomalies, including those with Craniofacial anomalies, including those with morphological abnormalities of pinna and ear canalmorphological abnormalities of pinna and ear canal
In-utero infection such as cytomegalovirus, herpes, In-utero infection such as cytomegalovirus, herpes, toxoplasmosis, or rubellatoxoplasmosis, or rubella
JCIH Risk Indicators for Hearing Impairment:Birth to 29 Days

Parental or caregiver concern regarding hearing, speech, Parental or caregiver concern regarding hearing, speech, language, and or developmental delaylanguage, and or developmental delay
Family history of permanent childhood hearing lossFamily history of permanent childhood hearing loss Stigmata or other findings associated with a syndrome Stigmata or other findings associated with a syndrome
known to include a sensorineural or conductive hearing known to include a sensorineural or conductive hearing loss.loss.
Postnatal infections associated with sensorineural hearing Postnatal infections associated with sensorineural hearing loss including bacterial meningitisloss including bacterial meningitis
In-utero infection such as cytomegalovirus, herpes, In-utero infection such as cytomegalovirus, herpes, toxoplasmosis, rubella, syphilistoxoplasmosis, rubella, syphilis
JCIH Risk Indicators for Hearing Impairment:29 Days to 2 Years (1)

Neonatal indicators, specifically hyperbilirubinemia at a serum level Neonatal indicators, specifically hyperbilirubinemia at a serum level requiring exchange transfusion, persistent pulmonary hypertension requiring exchange transfusion, persistent pulmonary hypertension of the newborn associated with mechanical ventilation, and of the newborn associated with mechanical ventilation, and conditions requiring extracorporeal membrane oxygenationconditions requiring extracorporeal membrane oxygenation
Syndromes associated with progressive hearing loss, such as Syndromes associated with progressive hearing loss, such as neurofibromatosis, osteopetrosis, and Usher’s syndromeneurofibromatosis, osteopetrosis, and Usher’s syndrome
Neurodegenerative disorders, such as Hunter syndrome, or sensory Neurodegenerative disorders, such as Hunter syndrome, or sensory motor neuropathies, such as Friedreich’s ataxiamotor neuropathies, such as Friedreich’s ataxia
Head traumaHead trauma Recurrent or persistent otitis media with effusion for at least 3 Recurrent or persistent otitis media with effusion for at least 3
monthsmonths
JCIH Risk Indicators for Hearing Impairment:29 Days to 2 Years (2)

Category Category Births AnnuallyBirths Annually PrevalencePrevalence Total Hearing LossTotal Hearing Loss
HealthyHealthy 3,600,0003,600,000 3/10003/1000 10,80010,800
At-riskAt-risk 400,000400,000 30/100030/1000 12,00012,000
TotalTotal 4,000,0004,000,000 5.7/10005.7/1000 22,80022,800
Northern & Hayes, 1994Northern & Hayes, 1994
UNIVERSAL NEWBORN HEARING SCREENING: Prevalence of Infant Hearing Loss in the U.S.A.

Universal Newborn Hearing Screening:Turning Point in the United States of America

UNIVERSAL NEWBORN HEARING SCREENING:Recent Events in the U.S.A.
1975-1985: 1975-1985: Hearing screening of at risk infants with ABRHearing screening of at risk infants with ABR 19931993: National Institutes of Health Consensus Conference on Early : National Institutes of Health Consensus Conference on Early
Identification of Hearing Impairment in ChildrenIdentification of Hearing Impairment in Children 19941994: Joint Committee on Infant Hearing (JCIH) Position Statement : Joint Committee on Infant Hearing (JCIH) Position Statement
(recommending ABR and OAE techniques)(recommending ABR and OAE techniques) 19981998: Yoshinaga-Itano et al. Language of early and later identified : Yoshinaga-Itano et al. Language of early and later identified
children with hearing loss. Pediatrics 102.children with hearing loss. Pediatrics 102. 19991999: American Academy of Pediatrics Task Force on Newborn and : American Academy of Pediatrics Task Force on Newborn and
Infant Hearing Screening: Diagnosis and intervention. Pediatrics 103.Infant Hearing Screening: Diagnosis and intervention. Pediatrics 103. 20002000: JCIH Position Statement. Principles and Guidelines for Early : JCIH Position Statement. Principles and Guidelines for Early
Hearing Detection & Intervention Programs. Hearing Detection & Intervention Programs.

UNIVERSAL NEWBORN HEARING SCREENING:Converging Trends in 1990s
Automated OAE and ABR devices manufactured for Automated OAE and ABR devices manufactured for newborn hearing screening newborn hearing screening
Evidence of low “refer” rates (< 4%)Evidence of low “refer” rates (< 4%) Evidence of low false-positive rates (< 2%)Evidence of low false-positive rates (< 2%) Documentation of benefits of early intervention Documentation of benefits of early intervention
(before 6 months)(before 6 months) Successful implementation of UNHS in selected statesSuccessful implementation of UNHS in selected states
EARLY IDENTIFICATION OF AND INTERVENTION FOR HEARING IMPAIRMENT IN CHILDREN
"Hearing loss of 30dB HL and greater in the frequency region "Hearing loss of 30dB HL and greater in the frequency region important for speech recognition will interfere with the normal important for speech recognition will interfere with the normal development of speech and language.development of speech and language.
"Techniques used to assess hearing of infants must be capable "Techniques used to assess hearing of infants must be capable of detecting hearing loss of this degree in infants by age three of detecting hearing loss of this degree in infants by age three months and younger.months and younger.
Of the various approaches to newborn hearing assessment Of the various approaches to newborn hearing assessment currently available, currently available, two physiologic measures...auditory two physiologic measures...auditory brainstem response (ABR) and otoacoustic emissions brainstem response (ABR) and otoacoustic emissions (OAE)...show good promise for achieving this goal(OAE)...show good promise for achieving this goal""
Joint Committee on Infant Hearing 1994 Position StatementJoint Committee on Infant Hearing 1994 Position Statement

Otoacoustic Emissions (OAEs)



NEWBORN HEARING SCREENING:OTOACOUSTIC EMISSIONS
Vohr et alVohr et al. The Rhode Island Hearing Assessment Program: . The Rhode Island Hearing Assessment Program: Experience with statewide hearing screening (1993-1996). Experience with statewide hearing screening (1993-1996). Journal of Pediatrics 133: 353-357, 1998Journal of Pediatrics 133: 353-357, 1998 53,121 babies underwent screening (NICU =5130)53,121 babies underwent screening (NICU =5130) average initial failure rate = 10%average initial failure rate = 10%failure rate for rescreens at 2 to 6 weeks = 14.7%failure rate for rescreens at 2 to 6 weeks = 14.7%over failure (refer) rate = over failure (refer) rate = 1.2%1.2%111 infants identified with permanent hearing loss111 infants identified with permanent hearing lossaverage age of intervention (amplification) = 5.7 monthsaverage age of intervention (amplification) = 5.7 months

Auditory Brainstem Response(ABR)

PEDIATRIC AUDIOLOGY: Auditory brainstem response (ABR)
stimulusclick @35 dB
electrodes Auditory EvokedResponse System
(computer)
I III V
8 ms
0.5 uV
1974 - present

UNIVERSAL NEWBORN HEARING SCREENING WITH AUTOMATED AUDITORY BRAINSTEM RESPONSE (AABR): A MULTI-SITE INVESTIGATION
J Perinatology 20 ((8): S128, December 2000.
James W. Hall III, Ph.D.James W. Hall III, Ph.D. Dan Stewart, M.D.Dan Stewart, M.D.
University of Florida University of Florida Kosair Children’s HospitalKosair Children’s Hospital
Gainesville, Florida, U.S.A.Gainesville, Florida, U.S.A. Louisville, KentuckyLouisville, Kentucky
Albert Mehl, M.D.Albert Mehl, M.D. Mark Carroll, M.S.Mark Carroll, M.S.
Boulder Community HospitalBoulder Community Hospital E.N.T. AssociatesE.N.T. Associates
Boulder, ColoradoBoulder, Colorado Huntsville, AlabamaHuntsville, Alabama
Vicki Thomson, M.A.Vicki Thomson, M.A. James Hamlett, M.D.James Hamlett, M.D.
Boulder Community Hospital Boulder Community Hospital Baptist Memorial Hospital EastBaptist Memorial Hospital East
Boulder, Colorado Boulder, Colorado Memphis, TennesseeMemphis, Tennessee

NEWBORN HEARING SCREENING WITH AABRTest Performance and Outcome
SITESITE WBNWBN ICNICN Refer Refer %% D/CD/C Refer Lost F/URefer Lost F/U False PosFalse Pos
BoulderBoulder 98%98% 2%2% 2% 2% 16% 16% 2%2%
LouisvilleLouisville >99%>99% <1%<1% 1% 1% 45% 45% .35%.35%
MemphisMemphis >99%>99% N=1N=1 3% 3% 13% 13% 2.5%2.5%
HuntsvilleHuntsville 93%93% 7%7% 1% 1% 21% 21% .05%.05%
NashvilleNashville 0%0% 100%100% 6% 6% 32% 32% 2%2%
N = 11,711N = 11,711 2% 2% 28% 28% 0.9%0.9%
AAPAAP << 4% 4% < 5% < 5% < 2%< 2%

Combination Device for Newborn Hearing Screening and Diagnosis with OAEs and ABR:
AudioScreener by Grason Stadler

Rationale for Combined OAE/ABR Screening
In ear calibration of signal intensity (OAE In ear calibration of signal intensity (OAE andand ABR) ABR) Lower refer (< 2%) and false-positive rates (< 0. 2%)Lower refer (< 2%) and false-positive rates (< 0. 2%) Minimal parental anxietyMinimal parental anxiety Fewer diagnostic follow-ups with lower costsFewer diagnostic follow-ups with lower costs Less hearing impaired infants lost to follow-upLess hearing impaired infants lost to follow-up Differentiation of conductive vs. sensory vs. neural auditory Differentiation of conductive vs. sensory vs. neural auditory
dysfunction dysfunction Quicker and more appropriate managementQuicker and more appropriate management Identification of auditory neuropathyIdentification of auditory neuropathy Earlier identification of hearing impairmentEarlier identification of hearing impairment
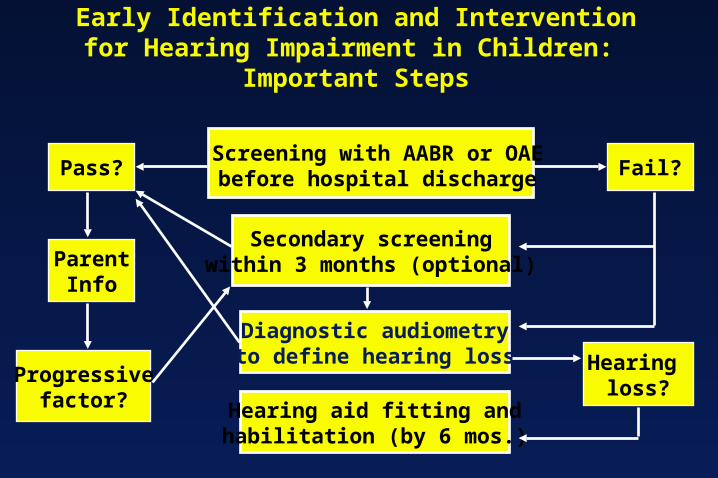
Early Identification and Intervention for Hearing Impairment in Children: Important Steps
Screening with AABR or OAEbefore hospital dischargePass?
ParentInfo
Progressivefactor?
Secondary screeningwithin 3 months (optional)
Fail?
Diagnostic audiometryto define hearing loss Hearing
loss?Hearing aid fitting andhabilitation (by 6 mos.)

Child and family historyChild and family history Otoacoustic emissionsOtoacoustic emissions ABR during initial evaluation to confirm type, degree & configuration ABR during initial evaluation to confirm type, degree & configuration
of hearing loss of hearing loss (ASSR?)(ASSR?) Acoustic immittance measures (including acoustic reflexes)Acoustic immittance measures (including acoustic reflexes) Behavioral response audiometry Behavioral response audiometry (if feasible)(if feasible)
Visual reinforcement audiometry Visual reinforcement audiometry ororConditioned play audiometryConditioned play audiometrySpeech detection and recognitionSpeech detection and recognition
Parental report of auditory & visual behaviorsParental report of auditory & visual behaviors Screening of infant’s communication milestonesScreening of infant’s communication milestones
Year 2000 JCIH Position Statement: Protocol for Confirmation of Hearing Loss
In Infants and Toddlers (0 to 6 months)


Estimation of Frequency-Specific Auditory Thresholds with Tone Burst ABRs: Initial Data Points for DSL
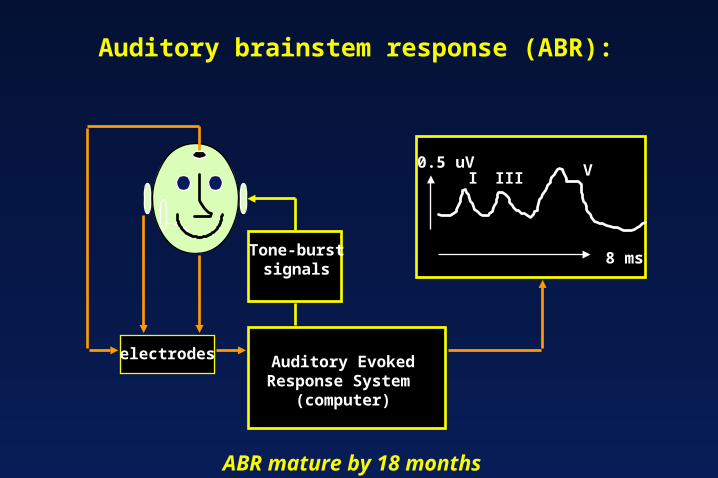
Auditory brainstem response (ABR):
Tone-burstsignals
electrodes Auditory EvokedResponse System
(computer)
I III V
8 ms
0.5 uV
ABR mature by 18 months

FREQUENCY-SPECIFIC ABRs:Tone Burst Test Protocols

Analysis TimeAnalysis Time
00StimulusStimulus 15 msec15 msec
5050
500 Hz500 Hz
1000 Hz1000 Hz
clickclick
VV
VV
VV
II
II IIIIII
IIIIII
Click versus Tone Burst ABRsClick versus Tone Burst ABRs

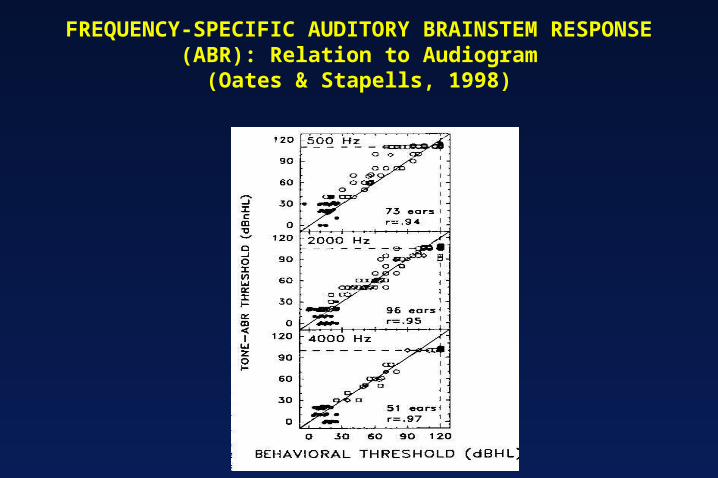
FREQUENCY-SPECIFIC AUDITORY BRAINSTEM RESPONSE (ABR): Relation to Audiogram
(Oates & Stapells, 1998)

ELECTROPHYSIOLOGIC ASSESSMENT OF AUDITORY FUNCTION IN INFANTS CASE REPORT: ABR Estimated Audiogram


An electrophysiologic response, similar to ABR.An electrophysiologic response, similar to ABR. Instrumentation includes:Instrumentation includes:
Insert earphonesInsert earphonesSurface electrodesSurface electrodesAveraging computerAveraging computer
Stimuli are pure tones (frequency specific, steady state signals) Stimuli are pure tones (frequency specific, steady state signals) activating cochlea and CNSactivating cochlea and CNS
ASSR is generated by rapid modulation of “carrier” pure tone amplitude ASSR is generated by rapid modulation of “carrier” pure tone amplitude (AM) or frequency (FM).(AM) or frequency (FM).
Signal intensity can be as high as 120 dB HLSignal intensity can be as high as 120 dB HL ASSR phase or frequency is detected automatically (vs. visual detection)ASSR phase or frequency is detected automatically (vs. visual detection)
Auditory Steady-State Response (ASSR): General Principles

Auditory Steady State Response (ASSR):Clinical Devices
GSI VIASYSGSI VIASYS AuderaAudera Descendant of Melbourne Australia system Descendant of Melbourne Australia system
Field (Rickards, Gary Rance, Barbara Cone-Wesson, Field (Rickards, Gary Rance, Barbara Cone-Wesson, et al)et al)
Bio-Logic Systems Inc.Bio-Logic Systems Inc.MASTERMASTERDescendent of Canadian system Descendent of Canadian system
(Terry Picton et al)(Terry Picton et al)

ASSR:2000 Hz tone modulated at rate of 100 Hz

ASSR:Response imbedded within EEG
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
1009080706050403020100ms

ASSR: Graphic display in vector plot of EEG samples at modulation frequency
A
B
C
c’b’
Vector length (c’) = Vector length (c’) = magnitude of activitymagnitude of activity
Vector angle (a’) = phase Vector angle (a’) = phase lag between stimulus lag between stimulus MF and EEG at MFMF and EEG at MF
a’
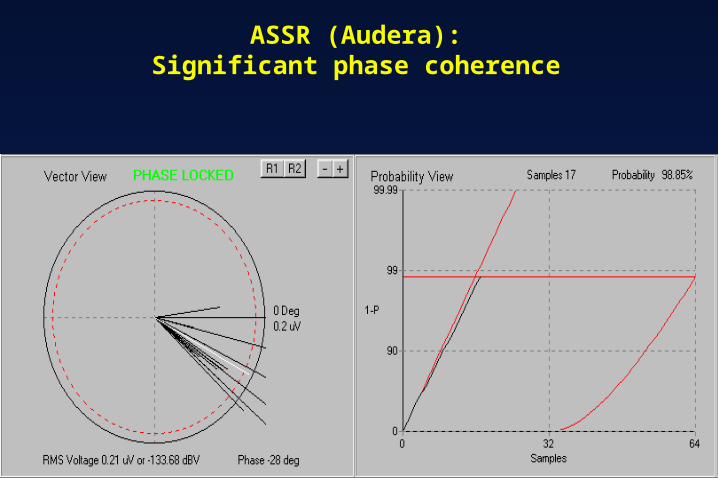
ASSR (Audera):Significant phase coherence

ASSR (Audera):Estimated Audiogram

Frequency in Hz
8K6K4K3K2K1K.50
PTABRASSR
Pure Tones vs. ASSR: Case 1 (child)
Frequency in Hz
dBHL8K
20
40
60
80
100
6K4K3K2K1K.50
Frequency in Hz
8K6K4K3K2K1K.50
PTABRASSR
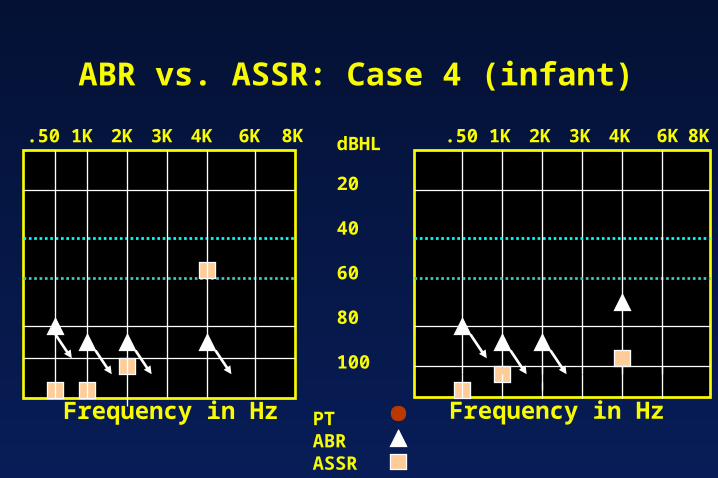
ABR vs. ASSR: Case 4 (infant)
Frequency in Hz
dBHL8K
20
40
60
80
100
6K4K3K2K1K.50

Frequency in Hz
8K6K4K3K2K1K.50
ACBC
Limitation of Tone Burst ABR in Severe-to-Profound Hearing Loss
Frequency in Hz
dB HL8K
20
40
60
80
100
6K4K3K2K1K.50
No ABR > 80 dB HL
No ASSR > 120 dB HL

Estimation of Frequency-Specific Auditory Thresholds with Auditory Electrophysiology: DSL Hearing Aid Fitting



Early Intervention for Infant Hearing Impairment: Amplification

Management of Infant Hearing Loss:Cochlear Implants

Newborn Hearing Screening and Assessment:Conclusions
Universal newborn hearing screening is feasible with Universal newborn hearing screening is feasible with automated OAE and ABR technologyautomated OAE and ABR technology
Estimation of hearing thresholds (audiogram) is possible in Estimation of hearing thresholds (audiogram) is possible in infants with electrophysiologic techniquesinfants with electrophysiologic techniquesABRs evoked by tone burst stimuliABRs evoked by tone burst stimuliAuditory steady-state response (ASSR)Auditory steady-state response (ASSR)
Intervention with hearing aids can be implemented early Intervention with hearing aids can be implemented early (before 6 months) (before 6 months)
Cochlear implant candidacy can be determined during infancyCochlear implant candidacy can be determined during infancy Early intervention leads to normal language developmentEarly intervention leads to normal language development