new technique combines electrical currents and …...63june 2011 new technique combines electrical...
TRANSCRIPT
52 Practical Pain Management | June 2011
Numerous types of electrical currents are offered in modern electromedicine. The plethora of currents is made possible by varying the frequency, amplitude
(intensity), and direction of the current in time. Within these electric current parameters are distinct and varying physi-ologic and therapeutic effects for the human biosystem.
Typically, therapeutic electric currents are classified according to their frequencies—for example, low frequency (LF; <2,000 Hz), medium frequency (MF; 2,000-100,000 Hz), or high frequency (HF; >100,000 Hz). This therapeutic classification system appears to originate from numerous physiologic investigations made in the last century.1-5 In the human biosystem, LF and MF currents are used for therapeutic stimulation of excitable cells (receptors, nerves, and muscles). Depending on the stimulating frequency delivered, physiologic and therapeutic actions may occur
that may include vasodilatation, vasoconstriction, analgesia, activation of regeneration, and facilitation of metabolism.
This article describes a new electromagnetic device and its use in combination with local anesthetic therapy to treat pain problems.
New Advanced TechnologyThe vast majority of electromedical devices available in the United States employ LF stimulation (eg, transcutaneous electrical nerve stimulation [TENS]). Balanced MF currents have been developed that produce twice the electrical current with no electrical charge. A new type of electrical current technology has been developed to enhance the stimulating lower frequencies and nonstimulating middle frequencies for increased efficacy in clinical prac-tice. The device also combines, and simultaneously delivers,
FEATURE
New Technique Combines Electrical Currents and Local Anesthetic for Pain ManagementCombined electrochemical nerve block reduced pain in 80% of patients with neuropathies and 50% of patients with intractable back pain.
Robert H. Odell, Jr., MD, PhD Interventional Pain Management Las Vegas, NV
Richard Sorgnard, PhDMorhea TechnologiesLas Vegas, NV
53
N e w T e c h n i q u e C o m b i n e s E l e c t r i c a l C u r r e n t s a n d L o c a l A n e s t h e t i c
June 2011 | Practical Pain Management
frequency-modulated (FM) and amplitude-modulated (AM) electric cell currents in the MF range. We refer to this electromedical approach as electronic signal treatment (EST).
This new technology may reach deeper into tissue structures with simultaneous modulation of ampli-tude and frequency between 2,500 Hz and 33,000 Hz. It is also capable of modulating its MF electric cell-signaling current down into the LF range at available frequency rates between 0.1 and 999 Hz.
In addition, we have combined the new EST with local anesthetic injections (bupivacaine 0.25%) with clinical success. This technique pro-vides a combined (electrical and chem-ical) nerve block that enhances treat-ment of a neuropathy or a painful condition (see Tables 1 and 2, page 63). According to the Gould Medical Dictionary, a nerve block is defined as “[t]he interruption of the passage of impulses through a nerve, as by chemical, mechanical, or electrical means.” Because nerve blocks occur at voltage-gated channels, all nerve blocks are essentially electrical. According to Szasz, “There is no such thing as a chemical block … only an electrical block.”6 We refer to this as combined electrochemical block (CEB).
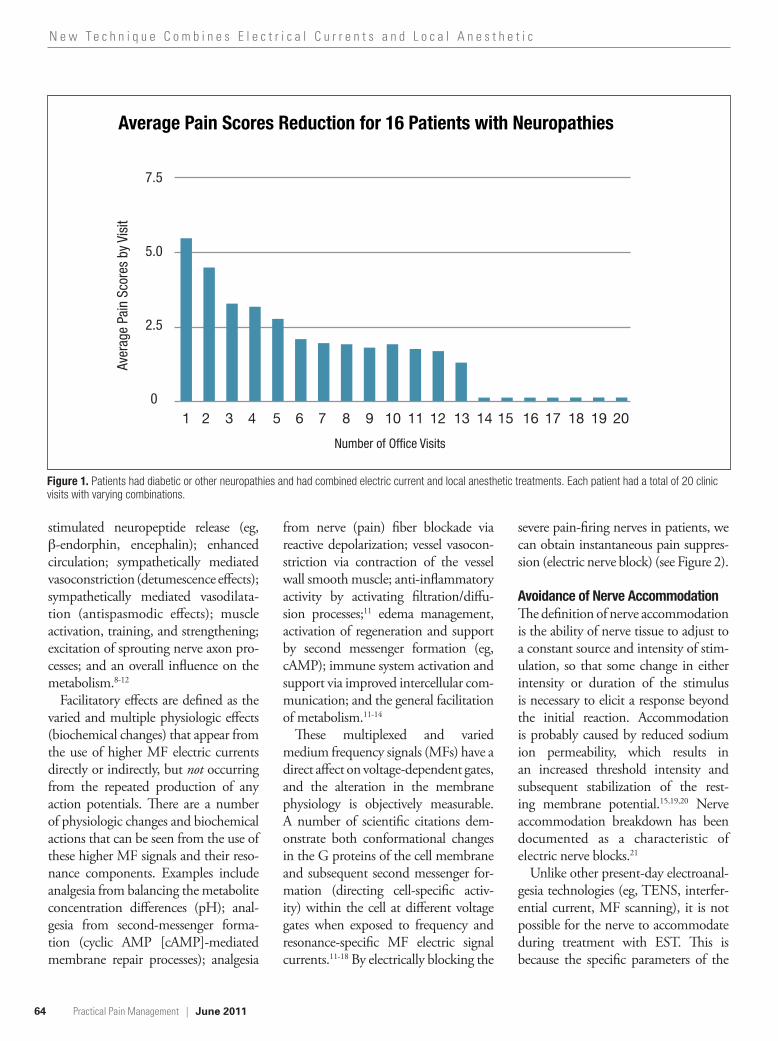
Clinical ExperiencesIt is the experience of the authors that pain is reduced by CEB in about 80% of patients who have neuropathies. As shown in Figure 1 (page 64), 16 patients with neuropathies improved over a course of 20 treatments. The CEB also has worked well in many cases of failed spine fusion syndrome and failed back surgery syndrome. In a small series of patients, more than 50% of those with hardware and intractable pain and proprioception difficulties showed improvement with bilateral transforminal epidural bupivacaine
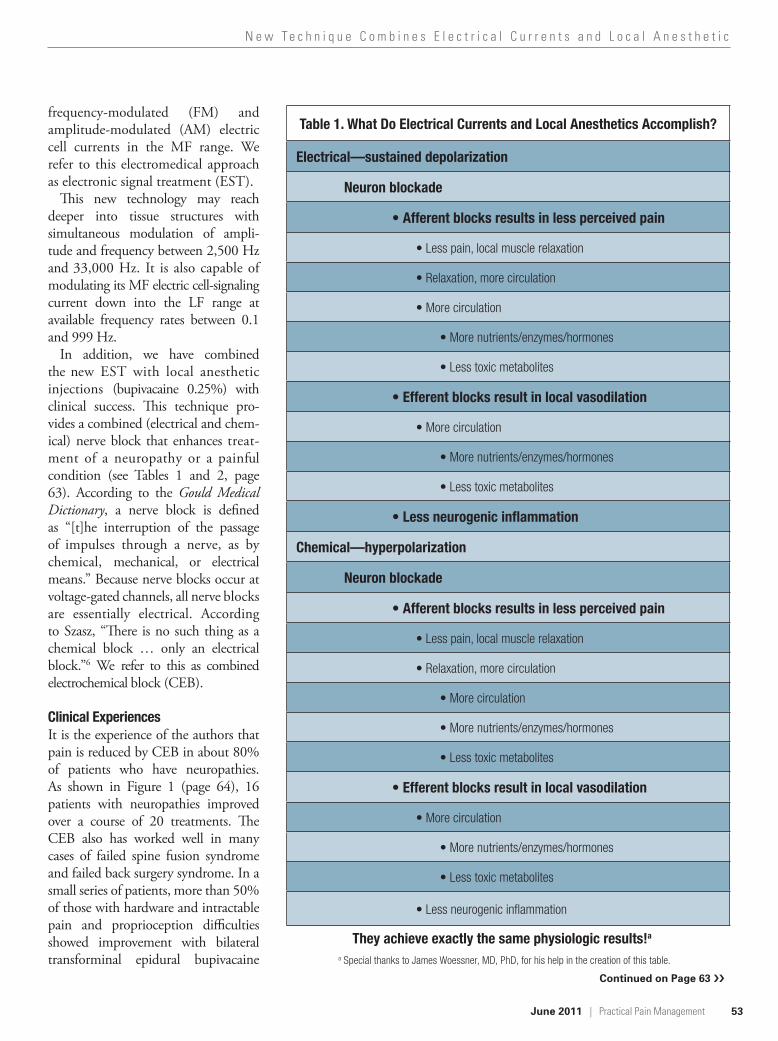
Table 1. What Do Electrical Currents and Local Anesthetics Accomplish?
Electrical—sustained depolarization
Neuron blockade
• Afferent blocks results in less perceived pain
• Less pain, local muscle relaxation
• Relaxation, more circulation
• More circulation
• More nutrients/enzymes/hormones
• Less toxic metabolites
• Efferent blocks result in local vasodilation
• More circulation
• More nutrients/enzymes/hormones
• Less toxic metabolites
• Less neurogenic inflammation
Chemical—hyperpolarization
Neuron blockade
• Afferent blocks results in less perceived pain
• Less pain, local muscle relaxation
• Relaxation, more circulation
• More circulation
• More nutrients/enzymes/hormones
• Less toxic metabolites
• Efferent blocks result in local vasodilation
• More circulation
• More nutrients/enzymes/hormones
• Less toxic metabolites
• Less neurogenic inflammation
They achieve exactly the same physiologic results!a
a Special thanks to James Woessner, MD, PhD, for his help in the creation of this table.
Continued on Page 63 ››
63
N e w T e c h n i q u e C o m b i n e s E l e c t r i c a l C u r r e n t s a n d L o c a l A n e s t h e t i c
June 2011 | Practical Pain Management
injections along with the application of EST.7 In fact, CEB may be con-sidered a less invasive alternative to spinal cord stimulator implantation.
Case ReportA 73-year-old woman had a 15-year history of low back pain with pain radiation down the legs. Diagnostic studies revealed spinal stenosis and facet arthropathy. She received three CEBs and two ESTs weekly for 3 weeks. After a pause of several days, she received two CEBs and three EST treatments over 2 weeks. At the end of this time, her visual analogue scale pain score had dropped from 10 of 10 to 2 of 10, and she was able to leave her house and walk with her husband.
Electromagnetic Physics of the Body Why does this work? One major differ-ence between the electric cell-signaling currents in EST and older devices is that EST allows greater depth of penetration through the dermal tissue by overall lowering of impedance to higher-frequency currents. This unique multiplex signaling configuration of mixed higher MF with overriding lower stimulatory frequencies (combined FM and AM signals) allows for the optimum voltage necessary to achieve proper depth of penetration while using lowered thera-peutic response frequencies to affect the voltage-gated channels and receptors within target tissue (see Table 2).
By continually varying the primary medium frequency or using the fre-quency-modulated signals in a higher
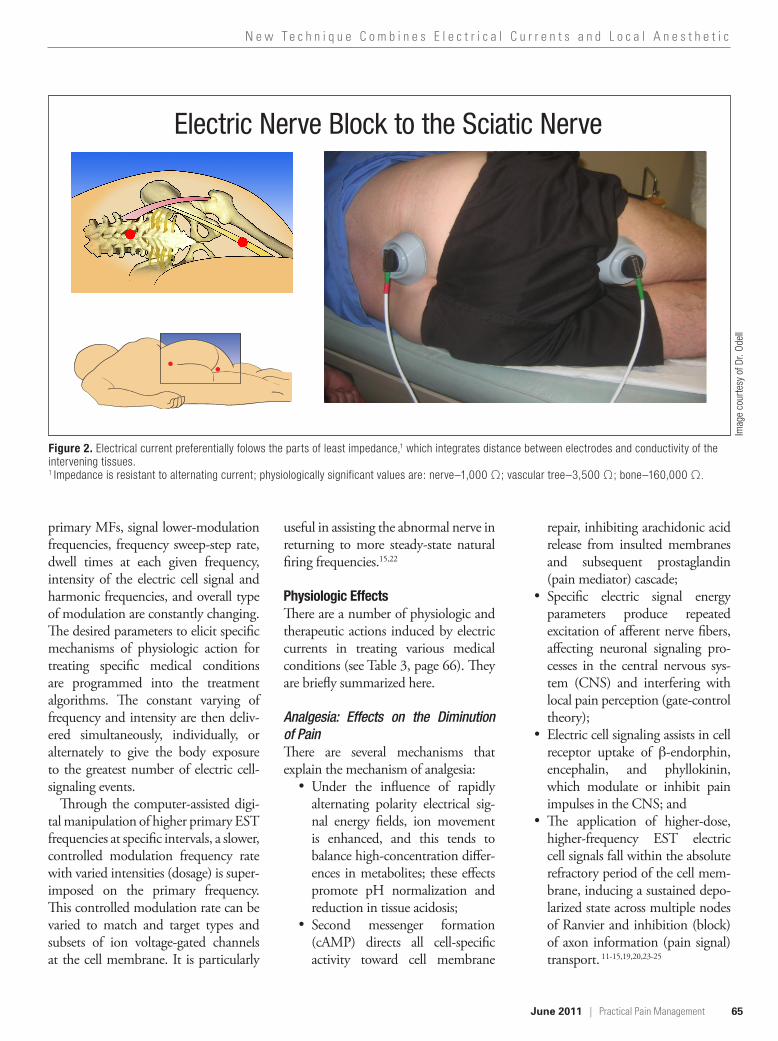
range, we can overcome the natural resistance to different tissue structures. Examples of these different resistant values are typically measured in ohms. The lowest resistance (impedance) is, in fact, neural tissue (1,000 Ω), so most (>65%) of the current (energy) will be drawn to the nerves.
Stimulatory effects are defined as the physiologic effects that appear from the use of lower electric current frequencies, which produce repeated action poten-tials (impulses) in excitable cells (LF). The induced membrane depolarization and subsequent repolarization produce a number of mechanisms of action known to be effective in treatment by varying the stimulation frequency. These include analgesia from the principle of counter-irritation; analgesia from
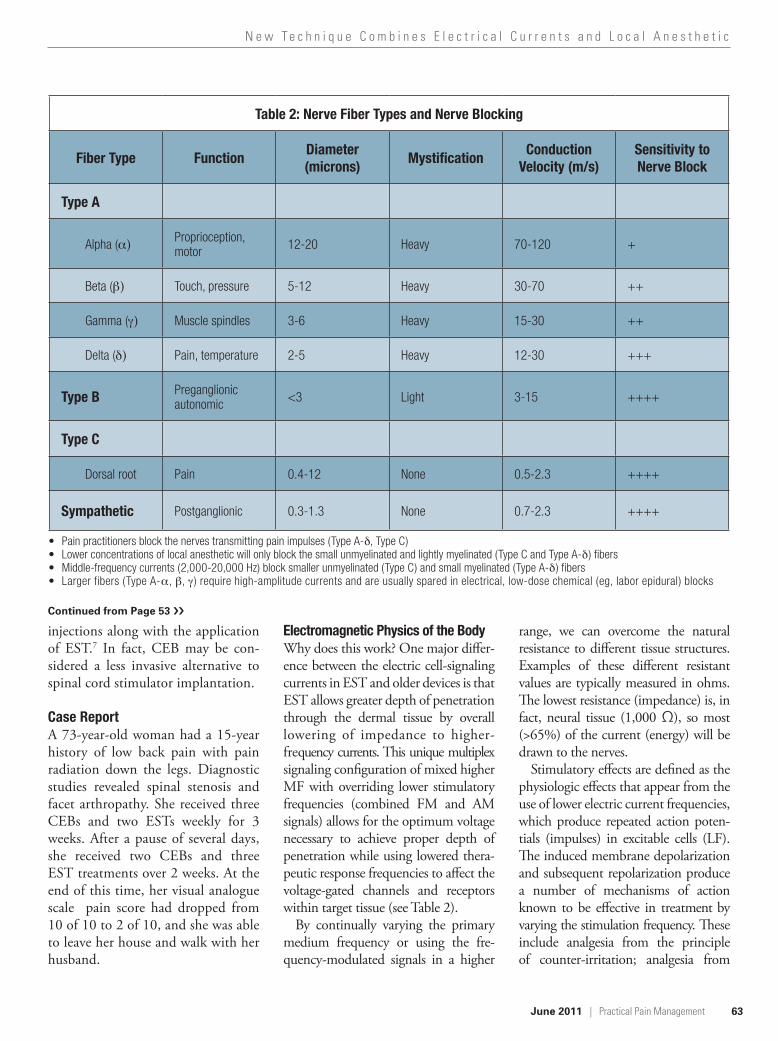
Table 2: Nerve Fiber Types and Nerve Blocking
Fiber Type Function Diameter (microns) Mystification Conduction
Velocity (m/s)Sensitivity to Nerve Block
Type A
Alpha (α) Proprioception, motor 12-20 Heavy 70-120 +
Beta (β) Touch, pressure 5-12 Heavy 30-70 ++
Gamma (γ) Muscle spindles 3-6 Heavy 15-30 ++
Delta (δ) Pain, temperature 2-5 Heavy 12-30 +++
Type B Preganglionic autonomic <3 Light 3-15 ++++
Type C
Dorsal root Pain 0.4-12 None 0.5-2.3 ++++
Sympathetic Postganglionic 0.3-1.3 None 0.7-2.3 ++++
• Pain practitioners block the nerves transmitting pain impulses (Type A-δ, Type C)• Lower concentrations of local anesthetic will only block the small unmyelinated and lightly myelinated (Type C and Type A-δ) fibers• Middle-frequency currents (2,000-20,000 Hz) block smaller unmyelinated (Type C) and small myelinated (Type A-δ) fibers• Larger fibers (Type A-α, β, γ ) require high-amplitude currents and are usually spared in electrical, low-dose chemical (eg, labor epidural) blocks
CYMBALTA® (duloxetine hydrochloride) PV 7213 AMP CYMBALTA® (duloxetine hydrochloride) PV 7213 AMP
features are consistent with either a direct toxic effect of SSRIs and SNRIs or, possibly, a drug discontinuation syndrome. It should be noted that, in some cases, the clinical picture is consistent with serotonin syndrome [see Warnings and Precautions].
When treating pregnant women with Cymbalta during the third trimester, the physician should carefully consider the potential risks and benefits of treatment. The physician may consider tapering Cymbalta in the third trimester.
Lilly maintains a pregnancy registry to monitor the pregnancy outcomes of women exposed to Cymbalta while pregnant. Healthcare providers are encouraged to register any patient who is exposed to Cymbalta during pregnancy by calling the Cymbalta Pregnancy Registry at 1-866-814-6975 or by visiting www.cymbaltapregnancyregistry.com.
Labor and Delivery—The effect of duloxetine on labor and delivery in humans is unknown. Duloxetine should be used during labor and delivery only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers—Duloxetine is excreted into the milk of lactating women. The estimated daily infant dose on a mg/kg basis is approximately 0.14% of the maternal dose. Because the safety of duloxetine in infants is not known, nursing while on Cymbalta is not recommended. However, if the physician determines that the benefit of duloxetine therapy for the mother outweighs any potential risk to the infant, no dosage adjustment is required as lactation did not influence duloxetine pharmacokinetics. (See Nursing Mothers section in full PI for additional information.)
Pediatric Use—Safety and effectiveness in the pediatric population have not been established [see Boxed Warning and Warnings and Precautions]. Anyone considering the use of Cymbalta in a child or adolescent must balance the potential risks with the clinical need.
Geriatric Use—Of the 2418 patients in premarketing clinical studies of Cymbalta for MDD, 5.9% (143) were 65 years of age or over. Of the 1041 patients in CLBP premarketing studies, 21.2% (221) were 65 years of age or over. Of the 487 patients in OA premarketing studies, 40.5% (197) were 65 years of age or over. Of the 1074 patients in the DPNP premarketing studies, 33% (357) were 65 years of age or over. Of the 1761 patients in FM premarketing studies, 7.9% (140) were 65 years of age or over. Premarketing clinical studies of GAD did not include sufficient numbers of subjects age 65 or over to determine whether they respond differently from younger subjects. In the MDD, DPNP, FM, OA, and CLBP studies, no overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. SSRIs and SNRIs, including Cymbalta, have been associated with cases of clinically significant hyponatremia in elderly patients, who may be at greater risk for this adverse event [see Warnings and Precautions]. (See Geriatric Use section in full PI for additional information.)
Gender—Duloxetine’s half-life is similar in men and women. Dosage adjustment based on gender is not necessary.
Smoking Status—Duloxetine bioavailability (AUC) appears to be reduced by about one-third in smokers. Dosage modifications are not recommended for smokers.
Race—No specific pharmacokinetic study was conducted to investigate the effects of race.
Hepatic Insufficiency—[See Warnings and Precautions-Use in Patients with Concomitant Illness.] (See Use in Patients with Concomitant Illness-Hepatic Insufficiency section in full PI for additional information.)
Severe Renal Impairment—[See Warnings and Precautions-Use in Patients with Concomitant Illness.] (See Use in Patients with Concomitant Illness-Severe Renal Impairment section in full PI for additional information.)
DRUG ABUSE AND DEPENDENCE: Abuse—In animal studies, duloxetine did not demonstrate barbiturate-like (depressant) abuse potential. While Cymbalta has not been systematically studied in humans for its potential for abuse, there was no indication of drug-seeking behavior in the clinical trials. However, it is not possible to predict on the basis of premarketing experience the extent to which a CNS active drug will be misused, diverted, and/or abused once marketed. Consequently, physicians should carefully evaluate patients for a history of drug abuse and follow such patients closely, observing them for signs of misuse or abuse of Cymbalta (e.g., development of tolerance, incrementation of dose, drug-seeking behavior).
Dependence—In drug dependence studies, duloxetine did not demonstrate dependence- producing potential in rats.
OVERDOSAGE: Signs and Symptoms—In postmarketing experience, fatal outcomes have been reported for acute overdoses, primarily with mixed overdoses, but also with duloxetine only, at doses as low as 1000 mg. Signs and symptoms of overdose (duloxetine alone or with mixed drugs) included somnolence, coma, serotonin syndrome, seizures, syncope, tachycardia, hypotension, hypertension, and vomiting.
Management of Overdose—There is no specific antidote to Cymbalta, but if serotonin syndrome ensues, specific treatment (such as with cyproheptadine and/or temperature control) may be considered. In case of acute overdose, treatment should consist of those general measures employed in the management of overdose with any drug. (See Management of Overdose section in full PI for additional information.)
NONCLINICAL TOXICOLOGY: Carcinogenesis, Mutagenesis, and Impairment of Fertility— Carcinogenesis—Duloxetine was administered in the diet to mice and rats for 2 years. In female mice receiving duloxetine at 140 mg/kg/day (11 times the maximum recommended human dose [MRHD, 60 mg/day] and 6 times the human dose of 120 mg/day on a mg/m2 basis), there was an increased incidence of hepatocellular adenomas and carcinomas. The no-effect dose was 50 mg/kg/day (4 times the MRHD and 2 times the human dose of 120 mg/day on a mg/m2 basis). Tumor incidence was not increased in male mice receiving duloxetine at doses up to 100 mg/kg/day (8 times the MRHD and 4 times the human dose of 120 mg/day on a mg/m2 basis).
In rats, dietary doses of duloxetine up to 27 mg/kg/day in females (4 times the MRHD and 2 times the human dose of 120 mg/day on a mg/m2 basis) and up to 36 mg/kg/day in males (6 times the MRHD and 3 times the human dose of 120 mg/day on a mg/m2 basis) did not increase the incidence of tumors.
Mutagenesis—Duloxetine was not mutagenic in the in vitro bacterial reverse mutation assay (Ames test) and was not clastogenic in an in vivo chromosomal aberration test in mouse bone marrow cells. Additionally, duloxetine was not genotoxic in an in vitro mammalian forward gene mutation assay in mouse lymphoma cells or in an in vitro unscheduled DNA synthesis (UDS) assay in primary rat hepatocytes, and did not induce sister chromatid exchange in Chinese hamster bone marrow in vivo.
Impairment of Fertility—Duloxetine administered orally to either male or female rats prior to and throughout mating at doses up to 45 mg/kg/day (7 times the maximum recommended human dose of 60 mg/day and 4 times the human dose of 20 mg/day on a mg/m2 basis) did not alter mating or fertility.
PATIENT COUNSELING INFORMATION: See FDA-approved Medication Guide and Patient Counseling Information section of full PI.
Additional information can be found at www.Cymbalta.com
Literature revised: November 8, 2010
Eli Lilly and CompanyIndianapolis, IN 46285, USA
Copyright © 2004, 2010, Eli Lilly and Company. All rights reserved.
PV 7213 AMP
DD HCP BS 17NOV10
49871_eldchp_DD70988B_int_sprd_fa.indd 9 4/14/11 11:01 AM
Continued from Page 53 ››
64
N e w T e c h n i q u e C o m b i n e s E l e c t r i c a l C u r r e n t s a n d L o c a l A n e s t h e t i c
Practical Pain Management | June 2011
stimulated neuropeptide release (eg, β-endorphin, encephalin); enhanced circulation; sympathetically mediated vasoconstriction (detumescence effects); sympathetically mediated vasodilata-tion (antispasmodic effects); muscle activation, training, and strengthening; excitation of sprouting nerve axon pro-cesses; and an overall influence on the metabolism.8-12
Facilitatory effects are defined as the varied and multiple physiologic effects (biochemical changes) that appear from the use of higher MF electric currents directly or indirectly, but not occurring from the repeated production of any action potentials. There are a number of physiologic changes and biochemical actions that can be seen from the use of these higher MF signals and their reso-nance components. Examples include analgesia from balancing the metabolite concentration differences (pH); anal-gesia from second-messenger forma-tion (cyclic AMP [cAMP]-mediated membrane repair processes); analgesia
from nerve (pain) fiber blockade via reactive depolarization; vessel vasocon-striction via contraction of the vessel wall smooth muscle; anti-inflammatory activity by activating filtration/diffu-sion processes;11 edema management, activation of regeneration and support by second messenger formation (eg, cAMP); immune system activation and support via improved intercellular com-munication; and the general facilitation of metabolism.11-14
These multiplexed and varied medium frequency signals (MFs) have a direct affect on voltage-dependent gates, and the alteration in the membrane physiology is objectively measurable. A number of scientific citations dem-onstrate both conformational changes in the G proteins of the cell membrane and subsequent second messenger for-mation (directing cell-specific activ-ity) within the cell at different voltage gates when exposed to frequency and resonance-specific MF electric signal currents.11-18 By electrically blocking the
severe pain-firing nerves in patients, we can obtain instantaneous pain suppres-sion (electric nerve block) (see Figure 2).
Avoidance of Nerve AccommodationThe definition of nerve accommodation is the ability of nerve tissue to adjust to a constant source and intensity of stim-ulation, so that some change in either intensity or duration of the stimulus is necessary to elicit a response beyond the initial reaction. Accommodation is probably caused by reduced sodium ion permeability, which results in an increased threshold intensity and subsequent stabilization of the rest-ing membrane potential.15,19,20 Nerve accommodation breakdown has been documented as a characteristic of electric nerve blocks.21
Unlike other present-day electroanal-gesia technologies (eg, TENS, interfer-ential current, MF scanning), it is not possible for the nerve to accommodate during treatment with EST. This is because the specific parameters of the
Average Pain Scores Reduction for 16 Patients with Neuropathies
7.5
5.0
2.5
01 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Aver
age
Pain
Sco
res
by V
isit
Number of Office Visits
Figure 1. Patients had diabetic or other neuropathies and had combined electric current and local anesthetic treatments. Each patient had a total of 20 clinic visits with varying combinations.
65
N e w T e c h n i q u e C o m b i n e s E l e c t r i c a l C u r r e n t s a n d L o c a l A n e s t h e t i c
June 2011 | Practical Pain Management
primary MFs, signal lower-modulation frequencies, frequency sweep-step rate, dwell times at each given frequency, intensity of the electric cell signal and harmonic frequencies, and overall type of modulation are constantly changing. The desired parameters to elicit specific mechanisms of physiologic action for treating specific medical conditions are programmed into the treatment algorithms. The constant varying of frequency and intensity are then deliv-ered simultaneously, individually, or alternately to give the body exposure to the greatest number of electric cell-signaling events.
Through the computer-assisted digi-tal manipulation of higher primary EST frequencies at specific intervals, a slower, controlled modulation frequency rate with varied intensities (dosage) is super-imposed on the primary frequency. This controlled modulation rate can be varied to match and target types and subsets of ion voltage-gated channels at the cell membrane. It is particularly
useful in assisting the abnormal nerve in returning to more steady-state natural firing frequencies.15,22
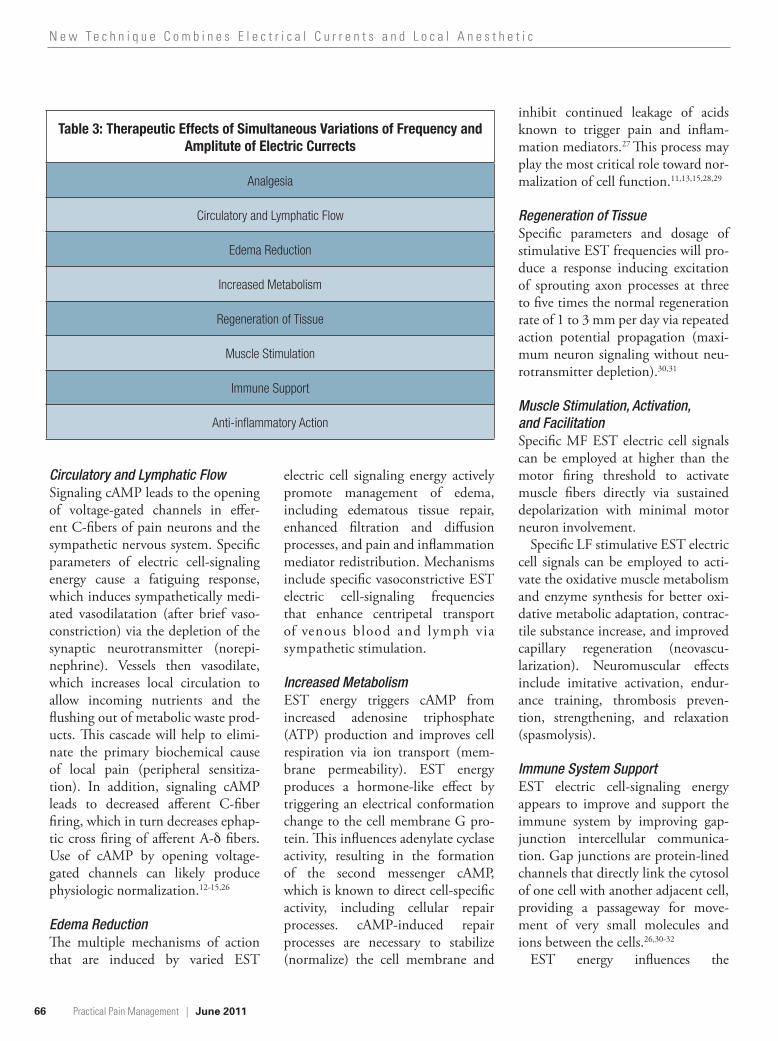
Physiologic Effects There are a number of physiologic and therapeutic actions induced by electric currents in treating various medical conditions (see Table 3, page 66). They are briefly summarized here.
Analgesia: Effects on the Diminution of PainThere are several mechanisms that explain the mechanism of analgesia: • Under the influence of rapidly
alternating polarity electrical sig-nal energy fields, ion movement is enhanced, and this tends to balance high-concentration differ-ences in metabolites; these effects promote pH normalization and reduction in tissue acidosis;
• Second messenger formation (cAMP) directs all cell-specific activity toward cell membrane
repair, inhibiting arachidonic acid release from insulted membranes and subsequent prostaglandin (pain mediator) cascade;
• Specific electric signal energy parameters produce repeated excitation of afferent nerve fibers, affecting neuronal signaling pro-cesses in the central nervous sys-tem (CNS) and interfering with local pain perception (gate-control theory);
• Electric cell signaling assists in cell receptor uptake of β-endorphin, encephalin, and phyllokinin, which modulate or inhibit pain impulses in the CNS; and
• The application of higher-dose, higher-frequency EST electric cell signals fall within the absolute refractory period of the cell mem-brane, inducing a sustained depo-larized state across multiple nodes of Ranvier and inhibition (block) of axon information (pain signal) transport. 11-15,19,20,23-25
Figure 2. Electrical current preferentially folows the parts of least impedance,1 which integrates distance between electrodes and conductivity of the intervening tissues.1 Impedance is resistant to alternating current; physiologically significant values are: nerve–1,000 Ω; vascular tree–3,500 Ω; bone–160,000 Ω.
Electric Nerve Block to the Sciatic Nerve
Imag
e co
urte
sy o
f Dr.
Ode
ll
66
N e w T e c h n i q u e C o m b i n e s E l e c t r i c a l C u r r e n t s a n d L o c a l A n e s t h e t i c
Practical Pain Management | June 2011
Circulatory and Lymphatic FlowSignaling cAMP leads to the opening of voltage-gated channels in effer-ent C-fibers of pain neurons and the sympathetic nervous system. Specific parameters of electric cell-signaling energy cause a fatiguing response, which induces sympathetically medi-ated vasodilatation (after brief vaso-constriction) via the depletion of the synaptic neurotransmitter (norepi-nephrine). Vessels then vasodilate, which increases local circulation to allow incoming nutrients and the flushing out of metabolic waste prod-ucts. This cascade will help to elimi-nate the primary biochemical cause of local pain (peripheral sensitiza-tion). In addition, signaling cAMP leads to decreased afferent C-fiber firing, which in turn decreases ephap-tic cross firing of afferent A-δ fibers. Use of cAMP by opening voltage-gated channels can likely produce physiologic normalization.12-15,26
Edema Reduction The multiple mechanisms of action that are induced by varied EST
electric cell signaling energy actively promote management of edema, including edematous tissue repair, enhanced filtration and diffusion processes, and pain and inflammation mediator redistribution. Mechanisms include specific vasoconstrictive EST electric cell-signaling frequencies that enhance centripetal transport of venous blood and lymph via sympathetic stimulation.
Increased MetabolismEST energy triggers cAMP from increased adenosine triphosphate (ATP) production and improves cell respiration via ion transport (mem-brane permeability). EST energy produces a hormone-like effect by triggering an electrical conformation change to the cell membrane G pro-tein. This influences adenylate cyclase activity, resulting in the formation of the second messenger cAMP, which is known to direct cell-specific activity, including cellular repair processes. cAMP-induced repair processes are necessary to stabilize (normalize) the cell membrane and
inhibit continued leakage of acids known to trigger pain and inflam-mation mediators.27 This process may play the most critical role toward nor-malization of cell function.11,13,15,28,29
Regeneration of TissueSpecific parameters and dosage of stimulative EST frequencies will pro-duce a response inducing excitation of sprouting axon processes at three to five times the normal regeneration rate of 1 to 3 mm per day via repeated action potential propagation (maxi-mum neuron signaling without neu-rotransmitter depletion).30,31
Muscle Stimulation, Activation, and FacilitationSpecific MF EST electric cell signals can be employed at higher than the motor firing threshold to activate muscle fibers directly via sustained depolarization with minimal motor neuron involvement.
Specific LF stimulative EST electric cell signals can be employed to acti-vate the oxidative muscle metabolism and enzyme synthesis for better oxi-dative metabolic adaptation, contrac-tile substance increase, and improved capillary regeneration (neovascu-larization). Neuromuscular effects include imitative activation, endur-ance training, thrombosis preven-tion, strengthening, and relaxation (spasmolysis).
Immune System SupportEST electric cell-signaling energy appears to improve and support the immune system by improving gap-junction intercellular communica-tion. Gap junctions are protein-lined channels that directly link the cytosol of one cell with another adjacent cell, providing a passageway for move-ment of very small molecules and ions between the cells.26,30-32
EST energy influences the
Table 3: Therapeutic Effects of Simultaneous Variations of Frequency and Amplitute of Electric Currects
Analgesia
Circulatory and Lymphatic Flow
Edema Reduction
Increased Metabolism
Regeneration of Tissue
Muscle Stimulation
Immune Support
Anti-inflammatory Action

67
N e w T e c h n i q u e C o m b i n e s E l e c t r i c a l C u r r e n t s a n d L o c a l A n e s t h e t i c
June 2011 | Practical Pain Management
electrically charged ion movements through gap junctions by increasing the transport through the cell to cell canals and by facilitating intercellular electric and chemical communication and metabolic cooperation.11,26,33 EST energy fields contribute to a func-tional improvement in tissues that are dysfunctional—for example, in the healing phase of injured tissue and in degenerative tissue changes, meta-bolic conditions, edema, and areas of regional insulted tissue.
Anti-inflammatory EffectsEST energy works through specific biosystems and their controls via mul-tiple mechanisms (listed above) by causing initial inflammation facilita-tion and then quick resolution of the inflammatory process, preventing it from leading to chronic inflammation and chronic pain.11
SafetyExtensive use over the past 15 to 20 years has established a very low risk profile of treatment with electric currents, even with these complex waveforms. The addition of local anesthetic blocks adds only an incremental risk (for infection). In the personal experience of one of the authors, the only adverse effect noted among a few hundreds patients was slightly increased pain, probably due to over-stimulation or excessive electric sig-nal energy (dosage), easily corrected in subsequent treatments. We also had one minor (first-degree) burn due to exces-sive application of electric signal energy (power density) to a poorly hydrated adhesive electrode. The burn resolved itself without additional medical inter-vention. The chances for increased expenses to the patient and third party payers treated with EST because of iat-rogenic consequences are minute.
Conclusion History has clearly shown that electric current devices have treatment merit. In most cases, electrical devices have, unfortunately, been proven to pro-duce temporary patient improve-ment. It is now evident that complex, painful conditions need more than one treatment modality or an alterna-tion of multiple and different mecha-nisms of action to sustain long-term patient treatment success.
We believe that longer-lasting out-comes can be achieved by using AM and FM currents at prescribed MF and LF parameters. When combined with a local anesthetic blocking agent, better results can be obtained. This procedure combines the positive ben-efits of intermittently generated mem-brane sustained depolarization, inter-ruption of the pain signal along the axon, normalized second messenger

68
N e w T e c h n i q u e C o m b i n e s E l e c t r i c a l C u r r e n t s a n d L o c a l A n e s t h e t i c
Practical Pain Management | June 2011
References1. Wyss OA. New principle of electric stimulation:
ambipolar stimulation by alternating cur-rent, purely sinusoidal, of middle-frequency. Experientia. 1962;18:341-342.
2. Wyss OA. Nerve stimulation with middle-frequency current pulses. Helv Physiol Pharmacol Acta. 1967;25(1):85-102.
3. May HU. Simultaneous Modulation of frequency and amplitude modulated electric signals. European Journal of Physiology. 2002;443 (suppl. 1):53-59.
4. Dalziel C. Effect of frequency on let-go currents. IEEE Trans Elect Eng. 1943;62:745-749.
5. Chatterjee I. Human body impedance and thresh-old currents for perception and pain for contact hazard analysis in the VLF-MF Band. IEEE Trans Bio Eng. 1986;33(5):486-494.
6. Szasz A. Presentation at the Clinical Electromedical Research Academy meeting; 1997; Las Vegas, NV.
7. Odell R. The Integrated Nerve Block: Electrical + Chemical; Poster Presentation to the 18th Annual International Spine Intervention Society Meeting; July 23-26, 2010; Las Vegas, NV.
8. Melzack W. Pain mechanisms: a new theory. Science. 1965;150:171-179.
9. Burton C, Maurer DD. Pain suppression by transcutaneous electrical nerve stimulation (TENS) in chronic pain. IEEE Trans Biomed Eng. 1974;21(2):81-88.
10. Bonica J, ed. The Management of Pain. 2nd ed. Philadelphia, PA: Lea and Febiger; 1990.
11. Odell R, Sorgnard R. Anti-inflammatory effects of electronic signal treatment. Pain Physician. 2008;11(6):891-907.
12. Odell R, Sorgnard R, May HU. Electroanalgesic
nerve block. Pract Pain Manag. 2006;6(3):42-54.
13. Savery F, Silver F, Edward R, et al. Assessment of electric differential treatment (EDiT) and Endosan treatment for ovarian cysts and concomitant symptoms. Adv Ther. 1991;8(5):243-249.
14. Schwartz RG. Electric sympathetic block: current theoretical concepts and clinical results. J Back Musculoskelet Rehabil. 1998;10:31-46.
15. Schwartz RG. Electric sympathetic block. Osterr Z Phys Med Rehabil. 2006;16(1):3-10.
16. Blank M. Electricity and Magnetism in Biology and Medicine. Berkeley, CA: San Francisco Press; 1992.
17. Frey A. On the Nature of Electromagnetic Field Interactions With Biological Systems. New York, NY: Springer; 1995:99-126.
18. Catarsi S, Scuri R, Brunelli M. Cyclic AMP medi-cates inhibition of the Na(+) - K(+) electrogenic pump by serotonin in tactile sensory neurons of the leech. J Physiol. 1993;462:229-242.
19. Bowman B. Electrical block of peripheral motor activity. Downey: Rancho Los Amigos Rehabilitation Engineering Center, 1981:89-102.
20. Woessner J. Electric nerve block. In: Boswell M, Cole E, eds. Weiner’s Pain Management. Boca Raton, FL: Taylor & Francis; 2006:1233-1242.
21. Kristian H, Arendt-Nielsen L, Andersen O. Breakdown of accommodation in nerve: a pos-sible role for persistent sodium current. Theor Biol Med Model. 2005;2:16.
22. Liboff A. Signal shapes in electromagnetic therapies: a primer. In: Rosche PJ, ed. Bioelectromagnetic Medicine. New York, NY: Marcel Dekker; 2004:17-38.
23. Bhadra N, Kilgore KL. High-frequency nerve
conduction block. Conf Proc IEEE Eng Med Biol Soc. 2004;7:4729-4732.
24. Bhadra N, Kilgore KL. Block of mammalian motor nerve conduction using high frequency alternating current. Presented at: 10th Annual International FES Society Conference; July 2005; Montreal, Quebec.
25. Tanner JA. Reversible blocking of nerve conduction by alternating current excitation. Nature. 1962;195:712-713.
26. Lodish H, Berk A, Zipursky SL, Matsudaira P, Baltimore D, Darnell J. Cell-cell adhesion and communication. In: Molecular Cell Biology. 4th ed. New York, NY: W. H. Freeman & Co.; 2000:974-975.
27. Alberts A, Johnson A, Lewis J, Raff M, Roberts K, Walter P. Molecular Biology of the Cell. 4th ed. New York, NY: Garland Science; 2002.
28. Farrar J. Introduction to the supplement on ion channels. J Pain. 2006;7(1):S3-S12.
29. Drevor M. Ion channels as therapeutic targets in neuropathic pain. J Pain. 2006;7(1):S3-S12.
30. Patel N, Poo MM. Orientation of neurite growth by extracellular electric fields. J Neurosci. 1982;2(4):483-496.
31. Brushart TM, Hoffman PN, Royall RM, Murinson BB, Witzel C, Gordon T. Electrical stimulation promotes motoneuron regeneration. J Neurosci. 2002;22(15):6631-6638.
32. Gibson, JR, Beierlein M, Connors BW. Functional properties of electrical synapses between inhibitory interneurons of neocortical layer. J Neurophysiol. 2005;93(1):467-480.
33. May HU. High tone power therapy. Presented at: Sixth Annual International Congress of Egyptian Society of Back Pain; April 19-20, 2006; Cairo, Egypt.
(cAMP) levels, β-adrenergic response, circulatory vasodilatation, general relaxation effects, and endogenous opiate release. The combined use of electric currents and local anesthetic should be more widely investigated in clinical practice.
Authors’ Bios and Disclosure: The device employed in this review was the NeoGen-Series available through Sanexas Corporation, Las Vegas, NV.
Robert H. Odell, Jr., MD, PhD (bio-medical engineering), practices inter-ventional pain management and anes-thesiology in Las Vegas, NV. Dr. Odell is a diplomat of the American Board of Anesthesiology, the American Board of Pain Medicine, and the American
Academy of Pain Management. He is a fellow of Interventional Pain Practice (FIPP) from the World Institute of Pain.
Over the past 6 to 7 years, Dr. Odell has been working in the clinical imple-mentation of these advanced electro-medical cell-signaling devices, which produce salutary effects for many of the most refractory pain management chal-lenges, especially neuropathy.
Richard Sorgnard, PhD (molecu-lar biology), is Executive Director for Morhea Technologies LLC, which is responsible for the design, development, and engineering of the electric cell- signaling technology used in this device. Dr. Sorgnard continues his life’s work in the signal generation and electromedi-cal field, which began with his earlier
association at the National Security Agency (NSA) in Laurel, MD.
Dr. Odell has no financial informa-tion to disclose. Dr. Sorgnard has dis-closed that he is a consultant for Sanexas International GmbH in Blaustein, Germany. Morhea Technologies LLC is involved in the ongoing research and technical development of electronic signal generation devices for the medical indus-try on a fee-for-service basis, including Sanexas International, GmbH.
Dr. Sorgnard’s wife is currently involved with the management at Sanexas and has stock ownership. Dr. Sorgnard does not own stock nor does he have any direct management involve-ment with Sanexas International GmbH or its distribution network.