‘new model of working for personalisation’ · ian anderson 13/05/10 ... high level strategy to...
TRANSCRIPT

1
Project Report
‘New Model of Working for Personalisation’

2
Document Control
Specific Audience Project Stakeholders
Purpose The purpose of this report is to outline the proposal for a ‘new model of working for personalisation’ and outline the further work that is required to implement this programme should it be agreed
Document Title Project Report
Electronic Location
PMO
Document Status Signed Off
Document Version
V2.0
Issue Date 14/05/10
Prepared By Jill Buchanan-Huck
Distribution Programme Board
Project Sponsor Authorisation Date
Ian Anderson 13/05/10
Version History
Date Name Circulation list Comment
0.1 01/04/10 Jill Buchanan-Huck First draft
0.2 01/04/10 Jill Buchanan-Huck Fiona Thompson Amended
0.3 06/04/10 Jill Buchanan-Huck PPF team Amended
1.0 12/04/10 Jill Buchanan-Huck Programme Board Signed off as discussion paper and work in progress (confidential)
1.1 20/04/10 Jill Buchanan-Huck Programme Board and Heads of Service
Amended
1.1 13/05/10 Jill Buchanan-Huck Agreed at DMT
2.0 14/05/10 Jill Buchanan-Huck DMT and identified authors of the business cases
To progress to 4 x business cases

3
Contents Page Document Control _______________________________________________________ 2
Contents Page __________________________________________________________ 3
1. Executive Summary____________________________________________________ 5
2. Background Information_________________________________________________ 9
3. Methodology ________________________________________________________ 11
4. Demographic Information ______________________________________________ 11
5. Stage 1 – Building Community (Universal Services, Early Intervention and Prevention)_____________________________________________________________________ 12
5.1 Table – Universal Services, Early Intervention and Prevention – Proposed Changes and Impacts _________________________________________________ 15
6. Stage 2 – Referral, Customer Service Centre (CSC) and web development _______ 20
6.1 Findings – Customer Service Centre: __________________________________ 20
6.2 How will this save money? ___________________________________________ 20
6.3 What can we do to generate efficiencies and improve the customer experience? 21
6.4 Fundamental Principles of New Model for CSC___________________________ 21
6.5 Specialist Team (within CSC) ________________________________________ 21
6.6 Findings - Web Development_________________________________________ 22
6.7 Table - Customer Service Centre and Web development – Proposed Changes and Impacts_____________________________________________________________ 24
7. Stage 2 – Short term Support - Crisis Response, Reablement, Intermediate Care, Telecare, Smartcare clinics _______________________________________________ 26
7.1 Crisis Response ___________________________________________________ 26
7.2 Assistive Technology/equipment ______________________________________ 27
7.3 Reablement ______________________________________________________ 29
7.4 Intermediate Care _________________________________________________ 31
7.5 Recommendation: _________________________________________________ 32
7.6 Table – Short term support / interventions – Proposed Changes and Impacts ___ 34
8. Self Directed Support__________________________________________________ 38
8.1 Assessment and care management (today) _____________________________ 38
8.2 What is needed from front line staff ____________________________________ 40
8.3 How it might look (suggested model example) ___________________________ 40

4
8.4 Recommendations: ________________________________________________ 41
8.5 Table – Self Directed Support (personal Budgets) – Proposed Changes and Impacts_____________________________________________________________ 42
Final Comments________________________________________________________ 44
APPENDIX____________________________________________________________ 46
Appendix 1 - Methodology ______________________________________________ 46
Appendix 2 – Population Projections ______________________________________ 48
Appendix 3 – Supporting People (eligible tasks) _____________________________ 51
Appendix 4 – New Model for CSC ________________________________________ 54
Appendix 5 - Staffing within specialist teams: _______________________________ 55
Appendix 6 – Call volume within Specialist Teams ___________________________ 57
Appendix 7 – Smart Care Data __________________________________________ 58
Appendix 8 – Integrated Community Service________________________________ 60
Appendix 9 – Gold Standard Reablement Pathway___________________________ 76
Appendix 10 - Detailed breakdown of staffing _______________________________ 77
Appendix 11 – Summary of Activity _______________________________________ 80
Appendix 12 – Skills Analysis ___________________________________________ 82

5
1. Executive Summary The purpose of this report is to propose a high level model of working for personalisation which ensures:
a persons journey through the different elements of Putting People First is simple, clear and results in improved outcomes for the individual
both cashable and non cashable efficiencies are delivered through implementing
the proposed model The report maintains the key principles outlined in phase 1 of New Model of Working for Personalisation, which were agreed in February 2010 by the PPF programme Board:
better outcomes for people who need support and care by providing the right
degree of support at the right time, therefore maximising a persons independence a customer journey that is simple and easy to navigate a workforce capable of meeting the changing requirements under personalisation;
the right people, at the right time individual choice as to who provides support and to what degree information, advice and guidance provided at the right time, in a variety of formats
to meet the needs of the population of Lincolnshire lean processes for the assessment of people’s needs and access to services
(proportionate to people’s needs) processes that are inclusive rather than exclusive of other professionals,
organisations, people. effective use of resources in terms of value for money and improved outcomes partnership working based on trust rather than suspicion, where benefits and risks
are shared across organisations
This report looks at the changes that are required to deliver these outcomes but recognises the good work and effective partnerships that are already happening in pockets around the county and aims to build on them as appropriate; it does not attempt in anyway to detract from the positive outcomes already being achieved. The report sets out the 4 key stages of a person’s journey 1. Universal, early intervention and preventive services; 2. CSC and Web; 3.Short term support / intervention (crisis response, assistive technology, equipment, reablement and intermediate care); 4. Maintenance – Self Directed Support (personal budgets). For each stage, the report identifies the key issues and proposed changes and recommended action for implementation by 2011 and beyond. The table below (page 5) summarises the key recommended actions for change and associated benefits and challenges. The Programme Board are asked to agree this approach in principle and to agree that an outline business case is developed for each of the four stages, outlining cost benefits, clear implementation plan and timescales for delivery.
6
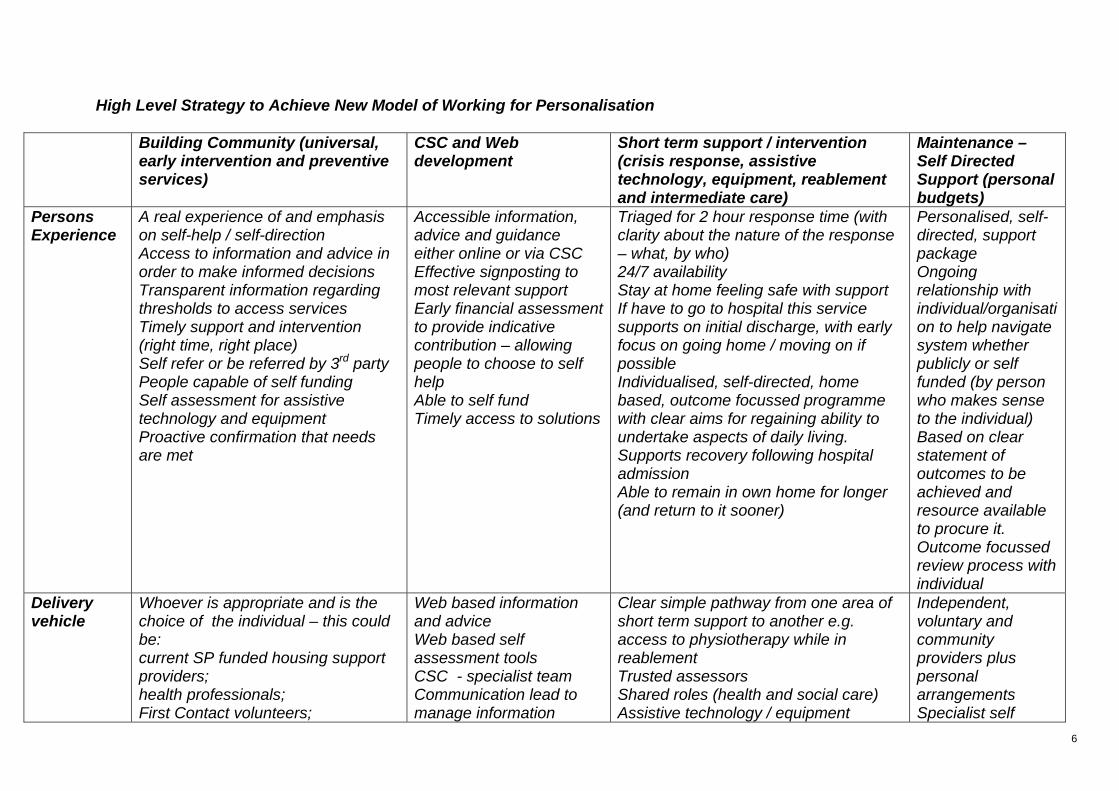
High Level Strategy to Achieve New Model of Working for Personalisation
Building Community (universal, early intervention and preventive services)
CSC and Web development
Short term support / intervention (crisis response, assistive technology, equipment, reablement and intermediate care)
Maintenance – Self Directed Support (personal budgets)
Persons Experience
A real experience of and emphasis on self-help / self-direction Access to information and advice in order to make informed decisions Transparent information regarding thresholds to access services Timely support and intervention (right time, right place) Self refer or be referred by 3rd party People capable of self funding Self assessment for assistive technology and equipment Proactive confirmation that needs are met
Accessible information, advice and guidance either online or via CSC Effective signposting to most relevant support Early financial assessment to provide indicative contribution – allowing people to choose to self help Able to self fund Timely access to solutions
Triaged for 2 hour response time (with clarity about the nature of the response – what, by who) 24/7 availability Stay at home feeling safe with support If have to go to hospital this service supports on initial discharge, with early focus on going home / moving on if possible Individualised, self-directed, home based, outcome focussed programme with clear aims for regaining ability to undertake aspects of daily living. Supports recovery following hospital admission Able to remain in own home for longer (and return to it sooner)
Personalised, self-directed, support package Ongoing relationship with individual/organisation to help navigate system whether publicly or self funded (by person who makes sense to the individual) Based on clear statement of outcomes to be achieved and resource available to procure it. Outcome focussed review process with individual
Delivery vehicle
Whoever is appropriate and is the choice of the individual – this could be: current SP funded housing support providers; health professionals; First Contact volunteers;
Web based information and advice Web based self assessment tools CSC - specialist team Communication lead to manage information
Clear simple pathway from one area of short term support to another e.g. access to physiotherapy while in reablement Trusted assessors Shared roles (health and social care) Assistive technology / equipment
Independent, voluntary and community providers plus personal arrangements Specialist self

7
Building Community (universal, early intervention and preventive services)
CSC and Web development
Short term support / intervention (crisis response, assistive technology, equipment, reablement and intermediate care)
Maintenance – Self Directed Support (personal budgets)
Third sector delivery directed support team (assessment and care management)
Shift in delivery model
Case finding predictive tools utilised to identify and refer people “at risk” Housing support providers assess for/organise assistive technology Provide call alarm/response service Assured supportive assessors for ASC and navigating to other services Provide ongoing relationship to support/disseminate information through home visits, telephone etc. Tiered service proportionate to identified risk Self assessment tools online (ties in with web and CSC development)
Self assessment tools online Use of ‘Touchstone’ for benchmarking and ongoing information Specialist team to provide information and advice, initial assessments (out of existing resources within assessment and care management) Provide call back Use of predictive tools
Supported by staff at the level of support required e.g. domiciliary care, OT, community nurse Assessment & Care Mgt (incl OT’s) within reablement Directly provided services staff involved with ongoing assessment within reablement Fully integrated delivery - clear pathways, roles and responsibilities Strong emphasis on support at home (move away from support within residential settings) Day service support as part delivery mechanism Assistive technology / equipment RAS as part of final ADL assessment
Customer choice Emphasis on self directed Specialist generic self directed team (A & CM) skilled to develop outcome focussed support plans Outcome focussed reviews (re RAS annually) e-market brokerage – online procurement of support/services third sector development of support for brokerage ASC brokerage for management of virtual budgets
Financial benefits
Delay/defer admission to more expensive public/self funded services
Decrease in number of people accessing more costly services
Reductions in emergency hospital admissions, lengths of stay and admissions to residential and nursing
Reduction in management costs Longer term

8
Building Community (universal, early intervention and preventive services)
CSC and Web development
Short term support / intervention (crisis response, assistive technology, equipment, reablement and intermediate care)
Maintenance – Self Directed Support (personal budgets)
Supporting independence (reducing dependence on a range of services)
Increased income due to early indicative financial assessment
home care Reduced staffing requirements (costs and head count) Reduced cost of maintenance packagesDecrease in numbers accessing maintenance packages
benefits of RAS
Challenges Capacity of current staffing to work in new role Developing simple processes Establishing new cross-service working protocols Overcoming potential information / privacy obstacles to a proactive and targeted prevention
Capacity of CSC staff to work in new role Capacity of ASC staff to take on new role
Resourcing to optimum level Managing interface between, crisis response, reablement, intermediate care Establishing new cross-service simple working protocols Overcoming potential information / privacy obstacles to a proactive and targeted prevention Culture change required away from services for life
Developing alternative capacity in market Reduced/re-focussed Assessment & Care Mgt capacity Reduced/re-focussed ASC directly provided services Accredited / quality assured providers

9
2. Background Information Putting People First December 20071 and Transforming Adult Social Care January 20092, set out the whole system changes that are required to create a new, high quality care system which is fair, accessible and responsive to the individual needs of those who use services and their carers by real partnership working with the local NHS, other statutory agencies, third and private sector providers, people who use services and carers and the wider community. Within the current economic climate and the need to drive out efficiencies it is important not to lose touch with the aspirations to move to truly personalised support and services, improving the outcomes for those who require our support and care. The Department of Health has, over the last year published a number of papers providing guidance for local authorities on how to ensure they deliver improved outcomes as well as efficiencies, one such papers is John Bolton’s paper ‘Use of Resources in Adult Social Care’3. John Bolton’s paper states that “good use of resources is a balancing act between user expectations and the priorities of adult social care services and wider local authority services. Only when all of these are met can a local authority deliver efficient, effective and economic adult social care in and affordable and accountable manner. This will include meeting local and central government priorities”. This report sets out to describe what we need to do in Lincolnshire to ensure we can deliver an efficient, effective and economic adult social care service that ensures the most cost-effective way of delivering the best outcomes for the people of Lincolnshire. “Health and social care need to focus on Quality, Innovation, Productivity and Prevention (QUIPP) to:
Develop lean processes for the assessment of people’s needs and access to services;
Develop preventive measures that can defer or delay people needing longer-term services (the biggest single savings can be made from reducing use of residential care and creating better community-based services delivering better outcomes);
Develop more cost-effective interventions that achieve better outcomes at lower costs; and
1 Putting People First: a shared vision and commitment to the transformation of Adult Social Care, HMGhttp://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_081118, 2 Local Authority Circular (DH) (2009) 1: Transforming Social Care, Department of Health, http://www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/LocalAuthorityCirculars/DH_095719 3 Use of Resources in Adult Social Care Use of resources in adult social care: A guide for local authorities : Department of Health - Publications

10
Assist people to construct their own packages of care through personal budgets and to help them procure these services in the most cost-effective way”
(‘Use of Resources in Adult Social Care: A local guide for local authorities’)
Within Lincolnshire the implementation of ‘Putting People First’ will ensure improved outcomes for all people who currently use adult social care and will also be of benefit both to those who are on the edge of requiring services and those who choose to fully fund and organise their own support. Most local authorities have tried to deliver Putting People First and personalisation without whole system change as have Lincolnshire. It has become evident however that to achieve the required outcomes for people and the local authority, there is a need to take a “whole system” approach to change. Further key documents to assist local authorities in implementing Putting People First have been published:
High Quality care for All,: NHS Next Stage review Final report, Darzi, 2008 Shaping the Future of Care Together, 2009;
PPF Operating Models 2009, ADASS4
Personalisation and the law: implementing PPF in the current legal framework, ADASS5 Making progress with Putting People First: self-directed support6
As set out in the Executive Summary above, key objectives the ‘new model of working for personalisation’ will deliver include:
better outcomes for people who need support and care by providing the right degree of support at the right time, therefore maximising a persons independence
a customer journey that is simple and easy to navigate a workforce capable of meeting the changing requirements under personalisation;
the right people, at the right time individual choice as to who provides support and to what degree information, advice and guidance provided at the right time, in a variety of formats
to meet the needs of the population of Lincolnshire lean processes for the assessment of people’s needs and access to services
(proportionate to people’s needs) processes that are inclusive rather than exclusive of other professionals,
organisations, people. effective use of resources in terms of value for money and improved outcomes partnership working based on trust rather than suspicion, where benefits and risks
are shared across organisations
4 PPF operating models: early learning http://www.dhcarenetworks.org.uk/Personalisation/Topics/Latest/Resource/?cid=6374 5 Personalisation and the law: implementing PPF in the current legal framework http://www.dhcarenetworks.org.uk/Personalisation/Topics/Latest/Resource/?cid=6373 6 Making progress with Putting People First: self-directed support http://www.dhcarenetworks.org.uk/Personalisation/Topics/Latest/Resource/?cid=6372

11
Delivering Putting People First and personalisation allows us to break out of the traditional boundaries and bureaucracies that have hindered how we work with individuals and partners in the past. People who use services will be integral to our new model, deciding who they want to support them at any given time. Our role therefore is to ensure the availability of high quality information, advice and guidance throughout the personalised customer journey so that whoever the individual chooses has the information they require to support and guide them. It is important to remember that the original model was diagrammatically shown as a linear model for ease of understanding, but that people’s lives are not linear and therefore an individual will access at the point that makes sense to their needs, and will dip in and out as appropriate. Each stage of the customer journey has been divided into sections 5 - 8 below. Each section sets out what each stage looks like now, what is should look like, what is required to get to where we want to be, and what is the likely impact of the change. Throughout each stage the key objectives outlined above will be assured.
3. Methodology In order to provide as much insight as possible a number of people were engaged both in the background reading, data gathering and interpretation and development of the model A comprehensive list of those involved and background reading can be found in (Appendix 1) The information obtained from all of the above sources has been used to shape the proposals within this report.
4. Demographic Information To deliver the requirements of Putting People First effectively and efficiently it is important to understand the demographic changes which will affect Lincolnshire in future years. To plan for support provision and the workforce to deliver this, we need to look beyond the Putting People First programme of 2011 and ensure the demographic changes are inherent in our long term plans for Lincolnshire. The tables (Appendix 2) show the demographic projections for Lincolnshire. The projections tell us is that no matter how we ‘cut the cake’ the number of people requiring support is increasing at the same time as we have a reduction in the growth of public funding for health and social care. Whether we look short term up to 2015 or beyond, what is clear is that doing nothing is not an option and that we need to make some fundamental changes, although we do not as yet know the timescales or impact of the ‘Personal Care at Home Bill.’

12
5. Stage 1 – Building Community (Universal Services, Early Intervention and Prevention) Much has been written over the past few years about the need for adult social care and health to move to a preventive model of service delivery. This report suggests that before we embark in developing more services in prevention we engage with local communities (whatever the make up of a community or their diversity e.g. faith, geographical) to determine with them what they see as their priorities. Key questions will be what they can do to help one another? What is already working and available? We will build on the work of First Contact Volunteers and the Bridge Project and ensure that whatever we develop is time limited with the emphasis on self help and re engaging people within their community (whatever community means to the individual). Building / developing communities will be met with differing degrees of enthusiasm and support across the county. Working with communities where we can, however, will allow for already limited resources to be spent in areas where there is no other form of support / service. Set out below are definitions of different elements of prevention all which would fit within community building/development:
Universal services – the general support available to everyone within their community including transport, leisure, education, employment, health, housing, community safety and information and advice.
Early Intervention & Preventive services - In the guidance document ‘Making a strategic shift to prevention and early intervention’; Government has identified differing levels of prevention as follows: Primary Prevention - Provision of universal access to good quality
information, supporting safer neighbourhoods, promoting health and active lifestyles, etc
Secondary Prevention - Identification of individuals at risk of specific health conditions or events (such as strokes or falls) or those who have existing low level care needs
Tertiary Prevention - Maximise people’s independence through interventions such as rehabilitation and joint case management of people with complex needs.
Social capital - Communities – fostering strong and supportive communities that value the contribution that each of their citizens can make.
The focus of the work on prevention in Lincolnshire has been on primary and secondary prevention with Health and Social Care working separately on tertiary prevention via the development of reablement services and the review of intermediate care.

13
A Prevention Strategy for Lincolnshire is in the early stages of development and has been a shared approach across the NHS, Social care, Housing and the Third Sector. The Prevention Strategy Report sets out in detail the key recommendations for developing prevention across organisations and across Lincolnshire. The Strategy focuses on two key outcomes: People are well informed about the options available to them through advice and
information when faced with potential support needs; and Through early intervention, more people are helped to avoid a crisis that could lead
to unnecessary admissions to hospitals (including psychiatric care), care homes or other long term or intensive support.
In order to deliver against these outcomes there are two clear critical strategic objectives: To demonstrate the success of investment in prevention to inform ongoing budget
setting; and To ensure that effective joint working across the whole system makes the most
efficient use of current investments in preventive services by maximising their impact
(Prevention Strategy Development Feb 2010)7 Well-being services are very popular with the public and there is growing evidence of their ability to improve people’s mental health and general well-being. It is difficult, however, to track directly whether people are being prevented from needing social care support in the future. Given that the evidence of preventive services to produce savings is not strong at present, it is important that spending on wellbeing services are not to be seen as a way of reducing pressure on budgets. Nevertheless, investment is important for other reasons, including:
To provide open access support outside Fair Access to Care Services (FASC) thresholds. The evidence suggests that authorities with limited investment of this nature face greater difficulties in maintaining thresholds for care-managed services;
To develop the social capital element expected by Putting People First and Social Care Transformation; and
As part of an overall local authority place-shaping strategy to promote health and well-being (where the contribution from social care may be relatively small compared to the overall corporate total).
(Use of Resources in Adult Social Care2009)8
7 Prevention Strategy Development Feb 2010 8 Use of Resources in Adult Social Care - Use of resources in adult social care: A guide for local authorities : Department of Health - Publications

14
There is growing evidence of the benefit of using predictive tools for case finding and early intervention. Currently these tools are mainly used in the NHS but further work is being carried out by Nuffield Trust to determine if predictive modelling tools could be used to routinely collect data from health and social care. This would enable predictions of the likelihood of hospital admission or the need for high cost adult social care. If these predictive modelling techniques are effective, this opens up the possibility of measurement of efficiencies through targeted prevention. Both efficiency and prevention are about ensuring ‘the right person accesses the system at the right time’ Health and social care need to work together to share resources, share benefits and share risks in developing joint investment strategies. We can only share resources, benefits and risks when we have a clear understanding of what organisations do. There is a great deal of duplication and while it is important not to restrict choice there is a need to streamline duplicated provision for example the tasks undertaken under the ‘Supporting People’ banner, third sector, home support. (Appendix 3 for list of eligible tasks for supporting people) In order to ensure a prevention agenda that is future proof and meeting the needs of the people of Lincolnshire and before further funding is committed to prevention we need to further understand the current spend and role/task being provided:
What is being delivered? What is the benefit? Who benefits? What is the impact if the service stops? Could any of these services be developed and delivered within natural
communities? What do communities see as their priorities? What is the exit strategy for individuals back into natural communities/out of
preventive services? Recommendations:
Take out any reference to age – while benefit may be primarily to those aged over 65 by leaving out age criteria we leave developments open to any people who would benefit from their support
Work with communities to help them determine their own priorities Review current models and provision Development of an Outline Business Case for Community Development –
incorporating Universal services, early intervention and prevention. This will sit within Health and Well-being with clear links to ASC commissioning

15
5.1 Table – Universal Services, Early Intervention and Prevention – Proposed Changes and Impacts
What it looks like now?
How should it look? How do we get there? What is the likely impact?
Information Advice and Guidance
Unclear where to go for information Varying degrees of quality Duplicated Mis information Lack of information on hospital discharge Out of date Disjointed eg website Poor information for people not requiring ASC funding
People know where to go to access information and advice Clear accessible information when it is needed One telephone number on the website Designed to ensure uniformity (this does not have to be boring) Concise/practical information and advice CSC use same website for information Shared information across organisations
Short term - redesign the ASC pages of LCC website. Medium term – ensure information is shared across organisational web sites Long term – one web site Review all of the leaflets Named person to be responsible for information/communication Development of e-market solutions i.e. shop4support- this would include information on universal and community services CSC training Strategic approach to development of Information, advice and
People Increased satisfaction Decrease in complaints Improved choice and control Accessing support at the right time Increased independence Improved outcomes
Workforce Decrease in activity to:
Area teams CSC Specialist Teams GP surgeries A&E
Increased awareness of what is available
Ease of access to information for all staff
More efficient use of staff time – not passing on to others to provide information
Performance
Improved quality of information Accessible to all Decrease in complaints Increase in satisfaction

16
What it looks like now?
How should it look? How do we get there? What is the likely impact?
Range of options as to who delivers information and advice Transparent information about access thresholds for services / support Web links to other relevant websites following search One repository for services and support
advocacy strategy involving key stakeholders including people who use services and carers County council strategy for Information, Advice and Guidance
In line with PPF milestones
Financial – assumptions Decrease in people requiring funding
following placing themselves in LTC Increase in income due to more timely
financial indicative assessment Decrease in use of ASC for brokerage Decrease in cost due to people
accessing services at the most appropriate time – not too early, not too late
Telecare/smart assist - low level equipment
Referral system Have to wait for an assessment FACS criteria
Simplified process Trusted assessors across organisations including third sector Self assessment with options for purchase
Self assessment on web for low level equipment/telecare. Accessible in GP surgeries, libraries etc Longer term - telehealth
People Increased satisfaction Decreased complaints Equipment when needed Improved choice and control Increased independence Improved outcomes
Workforce Decreased activity to:
CSC Smartcare clinics Area teams GP’s
Increase in:

17
What it looks like now?
How should it look? How do we get there? What is the likely impact?
people able to assess for low level equipment /telecare
improved job satisfaction, not having to pass onto someone else to assess for what you know is needed
Performance increased access to telecare improved waiting time for equipment Improved outcomes
Financial – assumptions Decrease in activity as above will lead
to decrease in expenditure on staffing Increase in expenditure on equipment
if we make it part of our ‘universal offer’
Decrease in expensive packages of care ie using people instead of technology
More efficient use of time – not passing from one part of the service to another
Early Intervention and Preventive services (50+ services provided by 10 providers)
Referral system Often require an assessment Duplication in some areas of the county
Developed Communities – work with communities to supply their own preventive support/services Simplified process to access
Trusted assessors – third sector, first contact volunteers, floating support, wardens, providers Further work to determine which services really need an assessment
People Increased choice and control Improved independence Supported to engage with local
community Supported out of services Improved outcomes Self help and self determination
18
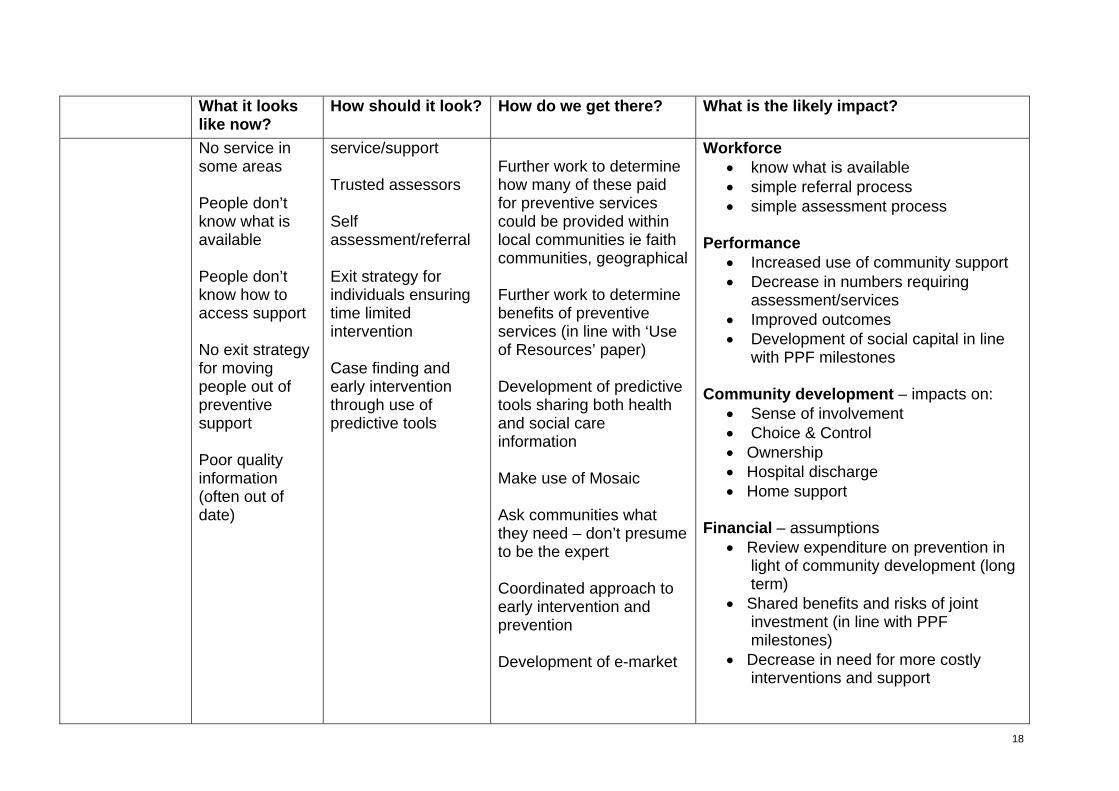
What it looks like now?
How should it look? How do we get there? What is the likely impact?
No service in some areas People don’t know what is available People don’t know how to access support No exit strategy for moving people out of preventive support Poor quality information (often out of date)
service/support Trusted assessors Self assessment/referral Exit strategy for individuals ensuring time limited intervention Case finding and early intervention through use of predictive tools
Further work to determine how many of these paid for preventive services could be provided within local communities ie faith communities, geographical Further work to determine benefits of preventive services (in line with ‘Use of Resources’ paper) Development of predictive tools sharing both health and social care information Make use of Mosaic Ask communities what they need – don’t presume to be the expert Coordinated approach to early intervention and prevention Development of e-market
Workforce know what is available simple referral process simple assessment process
Performance
Increased use of community support Decrease in numbers requiring
assessment/services Improved outcomes Development of social capital in line
with PPF milestones Community development – impacts on:
Sense of involvement Choice & Control Ownership Hospital discharge Home support
Financial – assumptions
Review expenditure on prevention in light of community development (long term)
Shared benefits and risks of joint investment (in line with PPF milestones)
Decrease in need for more costly interventions and support

19
What it looks like now?
How should it look? How do we get there? What is the likely impact?
Universal Services: Leisure Transport Employment Finance
This is more a series of questions: How accessible? How do people hear about them? What is the quality? What support is available once there? What feedback methods do they have?
Universal services will be accessible, when people want to use them, with the right degree of support
Need to work with people to ascertain what they want out of universal services Need to work with other organisations to develop services that are truly universal
People Increased choice & control Sense of belonging Inclusion in the wider community Networking Develop own circles of support
Finance - assumptions
Decrease in number of people requiring social inclusion
Decreased in overall need for services

20
6. Stage 2 – Referral, Customer Service Centre (CSC) and web development The previous stage focussed on preventing or delaying people accessing adult social care, however, even after referral it is important to ensure that people are correctly dealt with to ensure their needs are met by the most appropriate organisation in a timely manner. To support the principle of providing high quality information, advice and guidance at the first point of contact, this would involve bringing together the current work being undertaken in the CSC and the development of the web. Work carried out within CSC and on the web site will be seen as part of early intervention and prevention. In November 2009, a review was commissioned to gain a clearer understanding of the role of the CSC in working with Adult Social Care (ASC). Focusing particularly on creating efficiencies and support for adult social care.
6.1 Findings – Customer Service Centre:
Evidence suggests these tasks could be completed at CSC with additional skill levels, training and protocols:
Referrals to Telecare directly from CSC Smartcare clinics appointment system through CSC Re-route letters/faxes from area offices to CSC Introduction to Financial assessment Assistance with self assessment facilities as developed (telecare and
equipment) Minor equipment provision (Preventative agenda) Scheduled telephone reviews Scope for direct referrals into Lincolnshire Assessment and Reablement
Service (LARS)
6.2 How will this save money?
Area offices currently deal with the processing (re-routing) of 100 Telecare referrals per month. Each of these takes 45 minutes to process and make a referral
Area offices currently deal with the processing of 220 Smartcare referrals per month. Each of these takes 45 minutes to process and make a referral
Area offices around the county currently deal with the processing of 250 letters and faxes from other organisations by-passing CSC
Some people receive chargeable services free through delays in process, misinformation or misunderstandings. Making a statement through the advisors would potentially allow the directorate to make estimated charges at an earlier stage
More money could potentially be saved by the introduction of early benefits advice via helpline.
21
Providing people with a self assessment facility on line and assistance would drive forward the Preventative Agenda, whilst saving time wasted by area teams assessing those who could and would have helped themselves with appropriate information
Minor equipment provision could assist with prevention of falls and risk management to delay entry into ASC system
Scheduled telephone reviews could be done consistently by CSC and relieve the area teams from prioritising urgent work alongside duties such as this – referrals generated from reviews could be dealt with immediately rather than going through Area Office and back to CSC
6.3 What can we do to generate efficiencies and improve the customer experience?
The creation of a professional team within ASC would provide further efficiencies by generating capacity to:
Manage a central day time duty and emergency response system Select, plan and refer for reablement Encompass the Smartcare clinics Deal with routine hospital discharges Manage a professionals’ helpline Provide closer links with specialist teams such as safeguarding, brokerage,
carers team, FAB team, etc Manage unscheduled reviews until support planning becomes mainstream
6.4 Fundamental Principles of New Model for CSC
Redesigned ASC pages on LCC website to eliminate a proportion of Avoidable Contacts
Triage system (automated or manual) to either signpost callers or allocate calls to appropriate group of CSC staff
Group of less experienced Advisors to handle Simple Interventions (detailed in light blue section – diagram appendix 4)
Group of more experienced Advisors to handle Specialist Interventions (detailed in dark blue section – diagram appendix 4)
Group of ASC ‘Professionals’ to provide County-wide Duty Desk and other work currently handled at Area Offices (detailed in red section – diagram appendix 4)
6.5 Specialist Team (within CSC) There are currently 8 specialist teams working within ASC consisting of 66 staff, accommodation, equipment and travel costs. (Appendix 5) the cost of these teams (excluding Blue Badge) = £1,525,228 A short questionnaire was sent out to the specialist teams within ASC to determine their roles, processes and call volume. Further analysis will be required to ensure a full

22
understanding of the impact of moving calls and related work to the CSC. Call Volume by specialist team (6 months running up to end Feb 2010): (Appendix 6) Following on from the work to reduce avoidable contacts and ensuring suitable services are available on the web – this will make room for CSC to accommodate the work at low or no cost. The introduction of a specialist team within the CSC will allow for call volume and subsequent work to be carried out by the CSC therefore, enabling a review of the specialist teams and their function, as well as a countywide duty system, smartcare clinic appointments, professional helpline, unscheduled reviews, emergency carers service, assess and plan reablement, routine hospital discharge and short term support packages via RAS. This will impact on teams across adult social care and will bring about a more efficient way of working resulting in both cashable and non cashable savings. This team will be developed using existing resources from adult social care.
6.6 Findings - Web Development The development of the ASC pages of the web is a vital component in ensuring the provision of high quality information, advice and guidance provided to people in a timely manner. Web development will need to be in phases: Phase 1 – high quality information and advice, development of online assessments Phase 2 – connectivity with CSC – sharing data, call back, e-forms Phase 3 – connectivity with SWIFT The value of developing web based information is that it is accessible to those who may have to self fund their support, or do not want ASC involvement. It is available for friends and family outside of Lincolnshire and makes choice a real option, especially as we move to the development of online self assessment tools for assistive technology and equipment via ‘Smartassist’ and development of e-brokerage for all service and support provision. We often use the excuse that not everyone has access to the internet, but increasingly people of all ages are able to access the internet either by their own usage or that of family/friends. In a recent report by Ofcom it was reported that just 28% of people over the age of 65 have home internet access, compared to a UK average of 57% of households. However, more than two thirds of older people who are currently not connected said they would get online if they had the right support. Specifically they said they wanted courses designed for and run by older people.

23
As we continue to develop more online solutions it is vital that we also provide support to people to ensure they can access online information. This can be done via the third sector, communities, libraries and education. Web development needs to take into consideration the layout of the page, size of text, size of file (quicker loading for those not on broadband) Recommendations:
Implementation of new CSC model (Appendix 4) Develop and implement training programme for current CSC staff Remodel assessment and care management to release resources into CSC
specialist team Review specialist team function and structure in line with new CSC model Redesign ASC web pages to provide high quality information and advice Purchase online self assessment tool for assistive technology and
equipment Three phase programme: Phase 1 – high quality information and advice,
development of online assessments. Phase 2 – connectivity with CSC – sharing data, call back, e-forms. Phase 3 – connectivity with SWIFT
Incorporate ‘Touchstone’ as part of ongoing process of gathering feedback Development of Outline Business Case for CSC and Web development – this
will sit within Putting People First Team

24
6.7 Table - Customer Service Centre and Web development – Proposed Changes and Impacts What it looks like
now? How should it look? How do we get there? What is the likely impact?
Information, advice and guidance either via the web or CSC
The information on the Adult Social care (ASC) web is not fit for purpose in terms of information content The feel of the website does not reflect the transformation of ASC Not up to date Service led Repetitive Complicated Disjointed – multiple access points Lack of clarity about access routes to solutions Point of entry a
Simple Friendly Easily accessible Easy navigation Interactive Clear about what to expect Information, advice, signposting and advocacy. One contact number for ASC will be CSC Cost effective options to access information and solutions Consistent across the County 24/7 Early financial information re contribution
Radically overhaul the website Prioritise information needed on the web page Update current information Delete information that is not needed Archive old information that will still be required Create a friendly URL Place pictures and photographs to reflect the information content Change the web template Include feedback option Evaluate what works and what does not in terms of
People Increased satisfaction Improved up to date information Information easy to find, read and
understand Ease of accessing solutions Effective signposting Increased choice and control Increased independence Accessing the correct support Advocacy Self assessment on services e.g. blue
badge, assistive technology & equipment
Increase the understanding of LCC charging policy
Increase choice/options to people who self fund
Offer a medium for people to share good and bad experiences
Increase information to other professionals, carers, hard to reach groups, family, friends, neighbours, LCC staff and partner organisations.
Offer information to a wide audience about PPF, personal budgets, personalisation and the transformation of ASC

25
What it looks like now?
How should it look? How do we get there? What is the likely impact?
long way from point of solutions Reactive – preventive work not yet mainstream Lack of clarity about information sources Inconsistent messages about cost to people who use services Plethora of leaflets (repetitive, out of date)
Inclusive of all who would benefit Proactive – making use of preventive /self assessment tools Appointments arranges for smartcare clinics Simple process into reablement - short term services with long term benefit Streamlined , relevant process to the most appropriate solutions Streamlined process for written information management
Style Look and feel Content Navigation Quality
Enhance the services offered at CSC with existing staff group Enhance further the services offered at CSC through a specialist response team Radically overhaul processes Implement self assessment tools for telecare and equipment with CSC support available Ensure proactive preventative work is obligatory part of all processes
Workforce Increased satisfaction Improved up to date information Information easy to find, read and
understand Effective signposting Reflects the work currently being
undertaken Offer information about PPF, personal
budgets, personalisation and the transformation of ASC
Reduce time used searching on web Skills targeted effectively Clear priorities Clear career progression
Performance Improved quality of service Accessible to all Decrease in complaints Increase in satisfaction Use ‘Touchstone’ for benchmarking and
ongoing information Financial
Reduce the number of people accessing CSC and ASC.
Improve resource of staff time, allowing them to be more effective.
Decrease in cost due to people accessing services at the most appropriate time
Increased income potential

26
7. Stage 2 – Short term Support - Crisis Response, Reablement, Intermediate Care, Telecare, Smartcare clinics This stage of the personalised journey involves short term support or interventions aimed at supporting the individual to remain independent. These interventions will reduce the likelihood of hospital or care home admission, supporting the person as much as possible in their own home. Further research has shown that there is already an Integrated Community Services Commissioning Framework planned for Lincolnshire. This framework brings together the short term interventions (including crisis response) that will assist people in maintaining their independence, being supported at home and avoiding hospital and care home admission. The Vision for this service is: ‘To develop a wide range of integrated community based services to support more vulnerable people to maintain their independence and quality of life in a safe and appropriate way’ Refer to Appendix 7 for paper on Integrated Community Service
7.1 Crisis Response ‘Evidence shows that effective crisis response or rapid response services have a positive impact on the care pathway and outcomes for people who use services. Research by Care Service Efficiency Delivery (CSED) demonstrates that joint crisis response or rapid response services result in fewer people being unnecessarily admitted to hospital or residential care allowing them to maintain their independence at home. Crisis response services also create operating efficiencies and allow commissioner to redirect resources to community-based solutions Successful services share a number of common features:
Integrated, or jointly managed and funded A range of multi disciplinary back-up services offering domiciliary and nursing
support In most cases, community support workers and nursing support is required. Some locations have specially trained workers whilst others have domiciliary care staff working closely with district nursing teams. The frontline team is supported by a range of professionals such as occupational therapists or physiotherapists and in some cases pharmaceutical professionals supporting medicines management. There is a strong link to intermediate care (in some cases it is part of the integrated service) since admission to short term residential care may sometimes be required
A single point of access covered at all times A guaranteed response time

27
Once a referral is made, an assessment or a direct service is delivered within a locally agreed minimum time, usually two to four hours.
Time limited interventions Each site provides their support on a time-limited basis and each embraces a
reablement philosophy’ DH Care Networks CSED9 The delivery of such a service will require joint working, not only between health (PCT, LPFT and ULHT) and social care but also with early interventions and preventive services, housing related support, third sector and independent sector providers, East Midland Ambulance Service (EMAS).
This service will need to be developed to be inclusive of all individuals who may benefit from its support.
Their will need to be clear, simple processes from one stage of the pathway to another ie therapy support into reablement on an ‘as and when’ required basis without need for bureaucratic referral processes
Learning from current Intermediate care services and reablement services must be used to inform these new developments.
Involvement of people who use services and carers regarding their experiences to inform future developments
Development of clear performance criteria to measure impact of service on hospital and residential care avoidance as well as improved outcomes for individuals
Further work is required to ensure a county wide consistent service that avoids care home and hospital admission that is accessible 24/7
7.2 Assistive Technology/equipment Since the publication of DH guidance Building Telecare in England10 and the Preventative Technology Grant (2006-2008) local authorities have begun to make wider use of assistive technologies. Telecare/health offers increased choice and flexibility with equipment ranging from community alarm systems providing emergency response, sensors to support daily living and more sophisticated equipment to enable people with long term conditions to self manage their condition and remain within their own home.
o An estimated 90% of older people would choose to remain living in their own home. 500,000 older people live in care homes, in Lincolnshire approximately 6313 older people live in a care home. Recent research by the DH suggests that as many as 35% of these people could have been supported to stay at home or in extra care housing through the use of telecare.
9 DH Care Networks CSED – Crisis Response http://www.dhcarenetworks.org.uk/csed/CrisisResponse/SuccessfulServices/ 10 Building Telecare in England http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4115303

28
o Telecare has the potential to reduce unnecessary hospital admissions and improve people’s quality of life. The grant was to be used to increase the numbers of people
benefiting from telecare. Its use was to: Reduce the need for residential/nursing care; Unlock resources and redirect them to elsewhere in the
system; Increase choice and independence; Reduce the burden placed on carers and provide them with
more personal freedom; Contribute to care and support for people with long term health
conditions; Reduce acute hospital admissions; Reduce accidents and falls in the home; Support hospital discharge and intermediate care; Contribute to the development of a range of preventive
services; Help those who wish to die as home to do so with dignity. DH Care Networks CSED
We need to embed the use of assistive technology and equipment throughout the personalised journey ensuring it is inclusive of all who could benefit. The figures below show the data relating to equipment and telecare, it is clear from this that we need to look at the use of smartcare clinics and ensure they are the default for how equipment is provided.
13,825 items of equipment and 4,052 items of Telecare Assistive Technology were issued to people during the calendar year 2009.
This relates to 6628 people, all of which will have gone through the full assessment and care management process.
On average 2.7 items of equipment/telecare per person. On average 164 people a month are seen at smartcare clinics – (Appendix 8)
Across the board the number of people supported by telecare is small compared to the number of people supported by ASC. Usage of telecare is predominantly within older people’s services but even here the numbers are low.
Telecare usage in Lincolnshire
No of people in receipt of telecare
No of items of Telecare provided
Older People 1173 3696 Physical Disability 159 308 Learning disability 13 4 Mental Health 7 4 Other 10 40 Grand Total 1362 4052

29
There needs to be a shift in resources to fund equipment and a decision as to whether this is part of our universal offer and whether it is a charged for service (monitoring costs) Access to interventions such as Assistive Technology and Equipment need to be mainstreamed in order to ensure people can access them at the right time, ensuring independent living can be maintained. Referral processes need to be simple, allowing for trusted assessors and self assessment. Web development will provide online telecare and smartcare self assessment tools for use by the public, trusted assessors, CSC, reablement, intermediate care etc Expectation that all adult social care assessments consider telecare and equipment as the first solution, before moving onto more costly solutions.
7.3 Reablement The definition adopted by CSED was – ‘services for people with poor physical or mental health to help them accommodate their illness by learning or re-learning the skills necessary for daily living’ There is no blueprint for how a reablement should be developed, however most schemes tend to be developed as either: ‘Intake’ service, which commonly accepts all referrals of people assessed as needing or being eligible for homecare and then screen out only those considered unlikely to benefit from reablement. Or ‘Discharge’ or ‘discharge support’ services which primarily accept referrals of people leaving hospital, accepting only those people certain to benefit from a reablement approach. Most local authorities have developed reablement within their ‘In house – homecare service’. This service tends to focus on those needs that would ordinarily have been met via a social care homecare service, with support from therapy services usually available within intermediate care. CSED commissioned a retrospective longitudinal study with the University of York in 200711; the study looked at four schemes and found that in three out of the four schemes:
o 53% to 68% left reablement requiring no immediate homecare package
11 Retrospective Longitudinal Study (Nov 2007) http://www.dhcarenetworks.org.uk/_library/Resources/CSED/CSEDProduct/longit-study-bc.pdf

30
o 36% to 48% continued to require no homecare package two years after reablement
o In the fourth service, that operated on a selective basis, the results were significantly higher
Of those that required a homecare package within the two years after reablement:
o 34% to 54% had maintained for reduced their homecare package two years after reablement
o In the fourth service, that operated on a selective basis, the results were higher
Of those aged > 65 yrs that required a homecare package within two years after reablement:
o In three of the four schemes the number that had reduced their package was higher after 24 months than after three months
o This was even more noticeable in two of the schemes for those aged > 85 yrs As already stated there is no blueprint for the development of reablement, in Lincolnshire we have completed phase 1 of the Lincolnshire Assessment and Reablement Service (LARS). The service is defined in this brief extract from the current Service Specification developed by LCC commissioners: “LARS is available for adults (18 years and older) who have an identified community care need and meet Lincolnshire ASC Fair Access to Care eligibility criteria and who live within the administrative County of Lincolnshire. LARS is intended to be provided primarily for Older People, (including older people with mental health needs) adults with a long-term health condition and adults with a Physical Disability and/or sensory impairment. It is anticipated that the service may be required occasionally for people with a Learning Difficulty and people with Mental Health needs”. The service has been set up to operate as an intake service, to which the vast majority of referrals for older people will be directed. For other adult service user groups, a more selective approach is envisaged as noted above. LARS will be provided to:
People who are new to Adult Social Care following an initial contact assessment that identifies that they would benefit from the provision of this service;
People who are already receiving support arranged via Adult Social Care, but who experience a crisis, or rapid change in health or social care need (hospital admission for example) that cannot be met within an existing contingency plan. In such circumstances the provision of LARS may replace or complement the existing support arrangements for a time limited period.
(extract from LARS Service Specification, version 3.2, August 2009) Lincolnshire utilised the following definition of reablement as:

31
“Giving people the opportunity and confidence to regain as far as possible the skills they may have lost due to poor health or disability. Reablement can also be about helping people to gain new skills that help them to stay independent or to support them during a time of crisis in their lives”.
The LARS service has been independently evaluated Jan-Mar 201012 – the findings show that the service is achieving significantly lower results than other more established schemes. However, we must remember that Phase 1 of LARS was to establish a countywide reablement service which has been achieved. Phase 2 of LARS should see further development of the service:
Implementing phase 1 evaluation recommendations ensuring a fully trained workforce to deliver reablement, development of the assessment arm of LARS to include a generic assessment
team and occupational therapists. This will be resourced out of existing assessment and care management and directly provided services staff.
Re visit current homecare structures and boundaries in light of new service The Social Services Improvement Agency (SSIA) Wales – has published a very useful document ‘Approach to developing a Gold Standard in Reablement Service’13 The approach developed has been to work from a simple, high level pathway for reablement services; to identify standards and descriptors that are relevant to this standard; and to provide links and an evidence base that informs this standard. (The pathway is illustrated in appendix 9)
7.4 Intermediate Care Intermediate care services are jointly commissioned between Health (PCT’s) and local authorities. They usually offer a range of services to avoid hospital and care home admission. The range of services offered within intermediate care usually includes the availability a bed based as well as home based service. Intermediate Care would ordinarily have support from Physiotherapy, occupational therapy, nurses, and may have speech therapy, nutritional and health advice available. In July 2009, the DH issued new Intermediate care guidance - Intermediate Care – Halfway Home:14 This guidance provides renewed clarification of intermediate care which should change the way it works in relation to other local services and indicates the way forward for the
12 Evaluation of the Lincolnshire Assessment and Reablement Service
13 Social Services Improvement Agency – Approach to developing a Gold Standard in Reablement Service http://www.ssiacymru.org.uk/media/doc/h/3/SSIA_reablement_July_10th_workshop_material.doc 14 Intermediate Care – Halfway Home http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@pg/documents/digitalasset/dh_103154.pdf

32
next few years. It builds on the 2001 guidance on intermediate care and adds the
following.
o Inclusion of adults of all ages, such as young disabled people managing their transition to adulthood
o Renewed emphasis on those at risk of admission to residential care o Inclusion of people with dementia or mental health needs o Flexibility over the length of the time-limited period o Integration with mainstream health and social care o Timely access to specialist support as needed o Joint commissioning of a wide range of integrated services to fulfil the intermediate
care function, including social care reablement o Governance of the quality and performance of services
The policy landscape has moved on significantly and new models of care have been developed. There has been a shift to more personalised services that address inequalities, with greater focus on prevention and early intervention. Joint commissioning of a wide range of integrated services is required to fulfil the intermediate care function, including social care reablement. The original intermediate guidance has been interpreted differently in some areas, resulting in an inflexible adherence to a six-week timescale and the exclusion of some groups from services, such as older people with mental health problems and those whose discharge destination was uncertain because they were at risk of needing long-term residential care.
7.5 Recommendation: Learn from Phase 1 evaluation and implement the recommendations outlined
in the report That we use the Gold Standard assessment questions to assist us in
improving our reablement service Re design assessment and care management to ensure capacity in ongoing
assessment and review throughout reablement Re design In house homecare in light of new service e.g. virtual boundaries
for management purposes only – this may assist with lack of capacity in some areas
All staff delivering reablement are trained and competent All staff carrying out reablement assessment and planning are trained and
competent in producing outcome focussed plans and reviews That the components of the 2001 and 2009 guidance are incorporated into
the development of Lincolnshire’s Integrated Community Services. This service will need to be developed to be inclusive of all individuals who
may benefit from its support. Development of clear performance criteria to measure impact of service on
hospital and residential care avoidance as well as improved outcomes for individuals
A county wide consistent service that avoids care home and hospital admission that is accessible 24/7

33
There needs to be a shift in resources to fund equipment and a decision as to whether this is part of our universal offer and whether it is a charged for service (monitoring costs)
Expectation that all adult social care assessments consider telecare and equipment as the first solution, before moving onto more costly solutions.
Outline business case be developed to pull together all elements of short term support (this may have been done as part of the development of the Integrated Community Service)
34
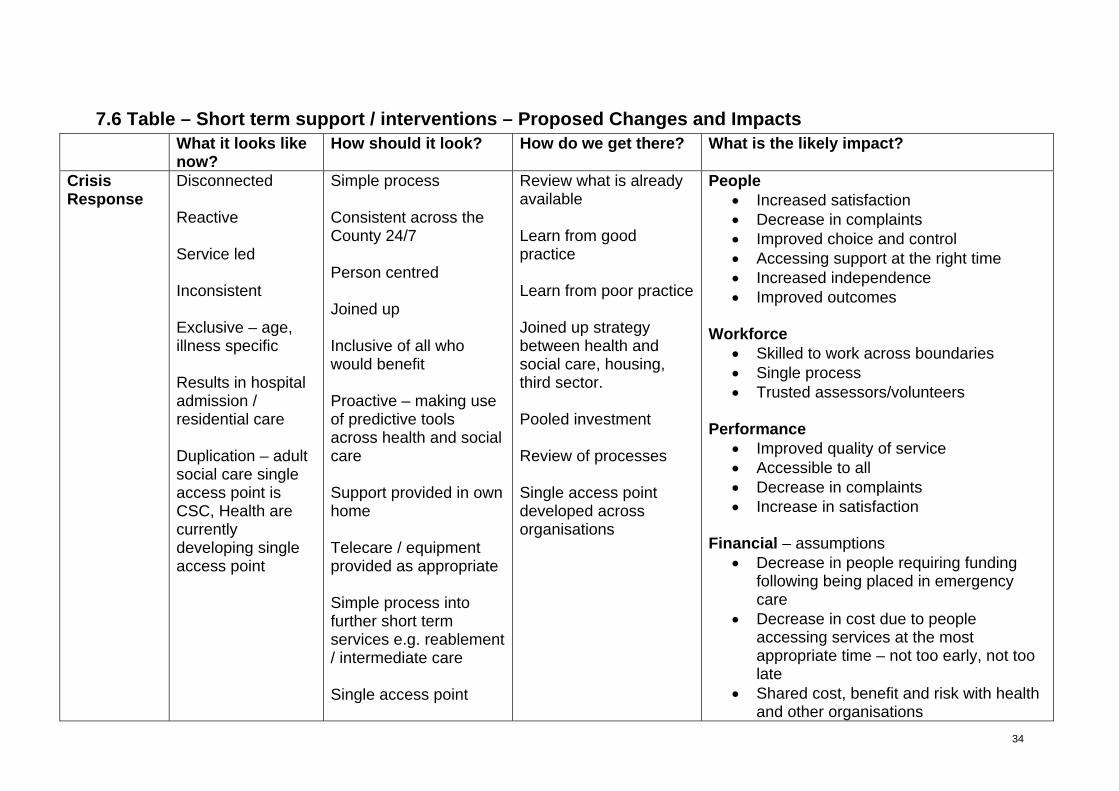
7.6 Table – Short term support / interventions – Proposed Changes and Impacts What it looks like
now? How should it look? How do we get there? What is the likely impact?
Crisis Response
Disconnected Reactive Service led Inconsistent Exclusive – age, illness specific Results in hospital admission / residential care Duplication – adult social care single access point is CSC, Health are currently developing single access point
Simple process Consistent across the County 24/7 Person centred Joined up Inclusive of all who would benefit Proactive – making use of predictive tools across health and social care Support provided in own home Telecare / equipment provided as appropriate Simple process into further short term services e.g. reablement / intermediate care Single access point
Review what is already available Learn from good practice Learn from poor practice Joined up strategy between health and social care, housing, third sector. Pooled investment Review of processes Single access point developed across organisations
People Increased satisfaction Decrease in complaints Improved choice and control Accessing support at the right time Increased independence Improved outcomes
Workforce
Skilled to work across boundaries Single process Trusted assessors/volunteers
Performance Improved quality of service Accessible to all Decrease in complaints Increase in satisfaction
Financial – assumptions Decrease in people requiring funding
following being placed in emergency care
Decrease in cost due to people accessing services at the most appropriate time – not too early, not too late
Shared cost, benefit and risk with health and other organisations

35
What it looks like now?
How should it look? How do we get there? What is the likely impact?
Assistive Technology and equipment
Telecare is predominantly used by older people Not embedded within assessment process Not part of prevention services Several monitoring systems Bureaucratic referral and assessment process Inconsistent usage of smartcare clinics Limited choice of equipment
Available for all who would benefit Available on the web for self assessment or supported via CSC Available at the right time – prevention, reablement or self directed support Trusted assessors Integral part of assessment process Simple access process Consistent usage of smartcare clinics as default - assessment at home exception Improved choice of equipment Clear guidance as to where equipment can be purchased from
Review referral and assessment process Review monitoring systems Review charging policy ie for monitoring service Awareness raising across organisations Awareness raising for the public Development of web based self assessment tool Budget identification for equipment Joint commissioning with health Review of smartcare clinic methodology Determine what data is required for performance and commissioning
People Increased satisfaction Improved choice and control Improved independence Ease of accessing solutions Accessing the correct support Self assessment Increased choice/options to people who
self fund Workforce
Increased satisfaction Improved up to date information Web based solutions Greater efficiency in use of staff time
Performance Improved quality of service Accessible to all Decrease in complaints Increase in satisfaction Increase in number of people supported
to live at home Improved quality of data
Financial Reduce the number of people accessing
CSC and ASC. Decrease in cost due to people
accessing services at the most appropriate time
Joint commissioning with health to share risks and benefits
Pooled budget with health

36
What it looks like now?
How should it look? How do we get there? What is the likely impact?
Efficient use of staff via smartcare clinics
Reablement and Intermediate care
New service – early stage of development Complex referral and assessment process Inconsistent quality across the county Below national average in performance Lack of capacity for entry into reablement Disjointed connections with Intermediate care Exclusivity of intermediate care Inconsistent quality of paperwork Unclear roles and
Simple referral and assessment process Initial assessment and ADL score by CSC or trusted assessors Assessment staff within LARS for ongoing assessment and review Occupational therapy staff situated with LARS Gold standard reablement Inclusive of all who would benefit National average in performance Staff trained to deliver reablement Implementation of Integrated Community Service
Make use of Gold standard questions Determine what Gold Standard means for Lincolnshire Re design of assessment and care management Review current In house home care boundaries (virtual boundaries for management purposes only) to improve capacity Training programme to ensure competent effective reablement is delivered Training programme re outcomes Work alongside other short term interventions to ensure simple
People Increased satisfaction Improved choice and control Improved independence Accessing the correct support as right
time Workforce
Increased satisfaction Greater efficiency in use of staff time Skilled and competent workforce Clear about role and responsibility
Performance Improved quality of service Accessible to all Decrease in complaints Increase in satisfaction Increase in number of people supported
to live at home Improved quality of data
Financial Reduce the number of people accessing
long term services Reduction in longer term support cost Decrease in cost due to people
accessing services at the most appropriate time
Efficient use of staff via smartcare clinics and telecare

37
What it looks like now?
How should it look? How do we get there? What is the likely impact?
responsibilities
Improved capacity Clear outcome based reablement plan Review process to monitor outcomes Clear roles and responsibilities 24/7 access Ongoing communication with people re post reablement (stop people expecting a service for life) Day service support as part of delivery mechanism
processes Ensure telecare and smartcare clinics are embedded as part of reablement and intermediate care service (Integrated Community Service) Agree information required for commissioning and performance RAS’d within LARS as part of final ADL review

38
8. Self Directed Support ‘Self Directed Support is a fundamental part of social care transformation; Putting People First includes a commitment to make personal budgets for norm for people who are eligible for ongoing social care. This means that:
Assessment is led by the person and focuses on the outcomes that they and their family want to achieve;
The person knows the amount of money that is likely to be available to achieve these outcomes before they decide how to use the money;
There is advice and support available to help people plan support arrangements that will achieve the agreed outcomes, and to raise concerns about those arrangements should they not work well; and
Support arrangements make the most use of natural support and mainstream services.’
Use of Resources 200915 Local Authorities are being monitored on their roll out of personal budgets with the target being set at 30% of people accessing longer term support on a personal budget by the end of March 2011. Over the last couple of years a great deal of work has been undertaken looking at processes, forms, training, and awareness raising. It is apparent that the biggest hurdle in the implementation of self directed support and personal budgets is culture in terms of staff, managers, people who use services, carers, providers, partner organisations and the general public. Implementation so far has focussed on trying to fit personal budgets into current structures and ways of working, there has been limited success. As we move to escalate personal budgets to ensure people are given real choice and control, we need to move away from traditional assessment and care management, using a blank canvas what is it we need from front line staff and how might this look
8.1 Assessment and care management (today) Assessment and care management is currently divided into three service areas, learning disability, physical disability and older people, with under 65 mental health services being provided by Lincolnshire Partnership Foundation Trust (LPFT). Table below shows high level breakdown of assessment and care management composition. Detailed breakdown (Appendix 10)
15 Use of Resources in Adult Social Care Use of resources in adult social care: A guide for local authorities : Department of Health - Publications

39
Service Area
Area Managers
Partnership/Practice Managers
Practice Supervisors / Senior Practitioner
Qualified Un qualified
LD 2 6 5 27 30 PD 1 3 6 9 (SW)
10 (OT) 17
OP 4 13 27 43 (SW) 14 (OT)
122
Total 7 22 38 103 169 With regards to process, the introduction of reablement and personal budgets should take longer if we are working in a truly personalised way. It is clear that assessment and care management do not have the capacity to take on the roles and tasks required within personalisation as well as the work they are currently involved in. With the development of the web site and the expansion of the customer service centre, the roles and responsibilities with assessment and care management need to be carefully reviewed. This is not about increasing staffing to gain capacity it is about doing things differently, supporting the principles of personalisation and ensuring that wherever possible people are given choice as to who they choose to support them throughout the process. In the current system 57.3% of people who receive an assessment go onto to receive a service/support package. Summary breakdown of cases referred, assessed, reviewed and service provided can be found in (Appendix 11) The number of people requiring an assessment by the current assessment and care management teams will decrease as:
CSC develops to undertake more stringent screening offering good quality information and advice;
CSC undertake initial assessment for reablement, smartcare clinic, unscheduled reviews, changes to packages etc;
Support planning contingency should decrease the need for people to contact area teams for short term changes to their support/service;
E-market allows for people to plan their own support and carry out their own brokerage on line
Development of trusted assessors to reduce the need for referral to ASC; People choose to produce their own support plans; Self funders having information that allows them to choose whether or not to carry
on with as assessment from ASC.

40
If people do choose ASC we need to ensure our staff are trained and able to deliver personalised assessments, support plans and reviews that are outcome focussed and meet people’s needs in ways that make sense to them.
8.2 What is needed from front line staff Local authorities are legally responsible for agreeing to all assessments, for agreeing to sign off the support plan and therefore agreeing that the actions identified will meet the outcomes and needs of the individual, and the review process. Front line staff will need to be competent that where they are chosen to support the person they have the skills and knowledge to ensure that the person has full choice and control in how their needs and outcomes are met. Where the individual lacks capacity the staff member needs to ensue that where possible the individual has choice and control and that in producing the support plan those people who care for and have knowledge of the person are involved at every step. The following skills were identified for this part of the person’s journey at a workshop with staff, people who use services and carers. It was clear in carrying out this work that there was no difference in the skills required from one service area to another. (Appendix 12)
8.3 How it might look (suggested model example) CSC Movement of
assessment and care management staff for develop specialist team to cover countywide duty, initial assessments
LARS Movement of assessment and care management into generic team to deliver ongoing outcome focussed assessment and reablement planning within LARS. RAS completed as part of final ADL score.
Self Directed Support (SDS) team
This could be a generic team to deliver support planning, brokerage and review. Or Generic support planning

41
team and Generic review team. This team could also provide ongoing social work support.
With the development of New Ways of Working and the move away from accommodation based practice there is a real opportunity to explore different ways of working that would offer a better service to the people of Lincolnshire. Patch working – move away from building based teams to patch based – this could be around GP surgeries, smartcare clinics, within x mile radius of where staff live, establishment of virtual teams. This would also build on the concept of building/developing community. Move away from service led teams, as we move towards seeing people as people and not as a disability or age. Reduce/refocus assessment and care management Reduce/refocus directly provided services Harness the specialist knowledge that is required in some areas of work but do not establish a whole service around a small % of the work. Need to decide our core business for personalisation and establish teams based on that business not on what we have always done and how we are currently structured. What are we currently doing that could be done by CSC, third sector, self, family, friends.
8.4 Recommendations:
Review roles currently being undertaken within each service area Determine core business Establish specialist team for LARS Establish specialist team for Self Directed Support Move away from service areas (lets see people as people) Reduce/refocus assessment and care management Reduce/refocus directly provided services Reduce /refocus specialist teams Develop an outline business case for the development of self directed
support (to sit within Operations)

42
8.5 Table – Self Directed Support (personal Budgets) – Proposed Changes and Impacts What it looks like
now? How should it look? How do we get there? What is the likely impact?
Assessment and care management
Disconnected Reactive Service led Task led Inconsistent practice Duplication Unclear roles and responsibilities Bureaucratic processes Inconsistent quality Lack capacity to carry out statutory duty i.e. reviews Person usually passive recipient Risk averse
Simple process Consistent practice across the County Person centred not service centred Consistent quality Outcome focussed (not service and task focussed) Person in control of self directed support process:
Who supports them
Who provides the service
Service tailored to individual needs
Clear roles and responsibilities Risk enabled
Learn from good practice Learn from poor practice Review of processes Determine core business Review current structures / accommodation etc Review roles and responsibilities Make use of data re numbers of staff, numbers of assessments, etc Development of e-market Development of market to provide flexible services / support tailored to individual
People Increased satisfaction Decrease in complaints Improved choice and control Accessing support at the right time Increased independence Improved outcomes
Workforce
Skilled Trusted assessors/volunteers Motivated Outcome focussed Capacity to carry out function Reduction/refocused assessment and
care management Reduction/refocused directly provided
services Reduction in A&CM workload
Performance Improved quality of service Decrease in complaints Increase in satisfaction Performance indicators on or beyond
target ie review
Financial – assumptions Decrease in cost due to people

43
What it looks like now?
How should it look? How do we get there? What is the likely impact?
needs accessing services at the most appropriate time – not too early, not too late
Reduced cost due to re structure of teams

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
44
Final Comments This report outlines the changes that are required to deliver the New Model of Working for Personalisation. Over the last few years we have become accustomed to saying ‘the person must be central to everything we do’, this is all about ‘choice and control’ etc. The time is now upon us when we need to make those fundamental decisions that lead to the changes that are required to move the personalisation agenda forward. The table on page 5 in the exec summary summarises the key recommended action to implement the new model and details the associated changes, benefits and challenges. Initial Model (Jan 2010) Proposed Model (April 2010) Universal Services Early Intervention and prevention
Building/Developing Communities – Universal Services Early Intervention and prevention
Crisis Response CSC and Web development
Referral CSC – (and one off responses) Short term support – Reablement Intermediate care
Short Term Support/Interventions – Crisis Response Assistive Technology & Equipment Reablement (RAS at end of reablement) Intermediate Care
Self Directed Support – RAS Support Plan Support Plan sign off Brokerage Review
Self Directed Support – Support Plan Support Plan sign off Brokerage Review

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
45
New Model of Working for Personalisation
Individual / Family &
Friends

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
46
APPENDIX
Appendix 1 - Methodology Background Reading:
Gloucestershire Village Agents In control www.in-control.org.uk - care management East Sussex Navigation Service Kent Car Navigator Manchester Gateway Service for older people CSED Care Management Processes Working to Put People First: The Strategy for the Adult Social Care Workforce in
England Skills for Care www.skillsforcare.org.uk Use of Resources in Adult Social Care – DH Operating Models: Learning from the Early Adapters – adass Report into Assessment and care management in Learning Disability Services -
Lincs First Contact Volunteers specification - Lincs Supporting People Strategic Overview – Older People 2008 - Lincs Community Support Volunteers - Lincs Key Ring - Lincs Developing Integrated Community Services – Lincs Achieving a High Quality Workforce to Put People First in Lincolnshire (Lincs)
Discussion with:
Operations Development Group Commissioners Health and wellbeing PCT LPFT PPF reference group – date had to be changed so now meeting in May – this
group would like to be actively involved in future developments and implementation Human Resources
Data Gathering on: Staffing Assessment and care management process i.e. contact, referral, assessment,
service, review Demographics Customer Service Centre Reablement First Contact and First Contact Volunteers Housing related Support Specialist teams;
o Brokerage o Carers o Safeguarding

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
47
o Blue Badge o FAB o Direct Payments o Smartcare and Telecare o Transitions
Workshops: Assessment and care management champions, LPFT champions, people who use
services and carers – identified skill requirements along the self directed support stage of the ‘personalised customer journey’
Assessment and care management champions, people who use services and carers – skill and competency requirement along the ‘personalised customer journey’ (facilitated by PCT workforce team)

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
48
Appendix 2 – Population Projections Population Projections people aged 65 and over – Lincolnshire 2009 2015 2020 2025 2030 People aged 65-69 42800 55700 51200 56400 65700
People aged 70-74 35400 43600 54300 50200 55400
People aged 75-79 28200 33200 39900 50000 46500
People aged 80-84 20500 23300 28100 34200 43100
People aged 85 and over 18700 23400 28400 36100 46300
Total 145600 179200 201990 226900 257000 Source ONS 2006 mid year population estimates projected forwards Population Projection aged 18-64 2009 2015 2020 2025 2030
People aged 18-24 60,000 60,600 57,100 57,900 63,700
People aged 25-34 69,600 83,100 88,400 86,600 83,300
People aged 35-44 97,600 86,700 88,800 100,900 106,400
People aged 45-54 98,600 111,500 108,300 98,700 101,600
People aged 55-64 100,400 100,700 114,300 125,200 121,800
Total population aged 18-64
426,200 442,600 456,900 469,300 476,800
Source PANSI – using ONS figures. Population Projections people aged 65 and over - 2009 - 2015
AGE GROUP 2009 2010 2011 2012 2013 2014 2015 People aged 65-69 42400 44500 47300 51500 54500 55700 56300 People aged 70-74 35700 36600 36900 37700 39100 41000 43200 People aged 75-79 28400 28800 29400 30100 31100 32100 32900 People aged 80-84 21300 21800 22200 22700 23100 23500 23900 People aged 85 and over 18600 19300 20000 20600 21300 22100 22900 Total 146400 151000 155800 162600 169100 174400 179200

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
49
Source: Lincolnshire Research Observatory based on ONS 2004 mid year population estimates projected forward Projections of People Living with Limiting Long-term Illness 2009 2015 2020 2025 2030 People aged 65-74 29889 37953 40323 40744 46286 People aged 75-84 24676 28628 34455 42664 45400 People aged 85 and over 9805 12270 14891 18929 24277 Total
64370 78851 89670 102336 115963
Source ONS 2001 Census calculated by applying percentages of people with a limiting long term illness in 2001 to projected population figures Projections of people predicted to have dementia 2009 2015 2020 2025 2030 People aged 65-69 533 693 638 701 816 People aged 70-74 971 1196 1489 1377 1520 People aged 75-79 1648 1935 2323 2914 2702 People aged 80-84 2464 2773 3331 4050 5096 People aged 85 and over 4360 5402 6519 8250 10557 Total
9976 12000 14300 17291 20691
Source Dementia UK report prepared by PSSRU, prevalence rates applied to population projections Falls – predicted to be admitted to hospital as a result of falls 2009 2015 2020 2025 2030 People aged 65-69 223 290 266 293 342 People aged 70-74 326 401 500 462 510 People aged 75 and over 2480 2940 3548 4427 5001 Total
3029 3631 4313 5182 5852
Source Based on 2003 study of 647721 A & E attendances and 204424 admissions to hospital for fall related injuries in people aged over 60. Number of Older People receiving community-based services provided or commissioned by CSSR 2009 2015 2020 2025 2030 People aged 65 or over 16843 20730 23356 26248 29730
Source: RAP return 07/08 figures applied to population projections

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
50
People aged under 65 predicted to have moderate or severe learning disability 2009 2015 2020 2025 2030 People age 18-24 374 379 359 368 406 People age 25-34 336 423 469 480 481 People age 35-44 600 536 550 627 665 People age 45-54 513 584 570 524 549 People age 55-64 488 494 563 612 591 Total 2310 2416 2511 2612 2693
Source PANSI People aged under 65 predicted to have a serious physical disability 2009 2015 2020 2025 2030 People age 18-24 480 485 457 463 510 People age 25-34 278 332 354 346 333 People age 35-44 1659 1474 1510 1715 1809 People age 45-54 2662 3011 2924 2665 2743 People age 55-64 5823 5841 6629 7262 7064 Total 10902 11143 11874 12451 12459
People aged under 65 predicted to have a moderate physical disability 2009 2015 2020 2025 2030 People age 18-24 2460 2485 2341 2374 2612 People age 25-34 2923 3490 3713 3637 3499 People age 35-44 5466 4855 4973 5650 5958 People age 45-54 9564 10815 10505 9574 9855 People age 55-64 14960 15004 17031 18655 18148 Total 35373 36649 38563 39890 40072

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
51
Appendix 3 – Supporting People (eligible tasks) SUPPORTING PEOPLE TASKS
Support levels may change from week to week because service users have individual and changing support needs. Please complete the following proforma and provide an estimate support provided on a weekly basis to each relevant task identified (for one service user). We only require one proforma to be completed for the service as an example of the support your services delivers Name of Service:
HOUSING RELATED SUPPORT TASKS
(funded by Supporting people)
Tick where appropriate
Time (minutes)
Setting up and maintaining the home or tenancy:
Service User risk assessments and risk management plans
Help in setting up and maintaining the home or tenancy
Help in managing finances and benefit claims
Security, health and safety in the home:
Help in establishing personal safety and security
Help maintaining the safety and security of the dwelling
Security support related to racial harassment
Home management and life skills:
Support to develop domestic/life skills
Advice and support on repair work/home improvement work
Help with shopping and running errands (ancillary, ad hoc support)
Well-being and general support:
General counselling and support
Peer support and befriending (e.g. emotional support, counselling and advice)
Supervision and monitoring of health and well being
Supervision or monitoring medication (general support and not services provided by clinicians)
Advice, advocacy and liaison:
Advice, advocacy and liaison
Support to develop social skills/behaviour management
Help in gaining and establishing access to other services

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
52
Help in establishing social contacts and activities
Help in gaining access to local community organisations
Liaison with the Probation Service and other statutory and voluntary sector agencies
Culture specific counselling/emotional support
Liaison and advocacy support from the same ethnic group
Signposting to culture specific legal services
Signposting to culture specific health/treatment services
Move-on from the service:
Help and support to find other accommodation
PERSONAL CARE TASKS (not funded by Supporting People)
Tick where appropriate
Help with medication or self medication
Assistance with dressing and undressing
Assistance regarding personal hygiene
Assistance with toileting
Assistance to eat
GENERAL SOCIAL CARE ACTIVITIES
Tick where appropriate
Carrying out domestic tasks e.g. laundry
Help with carrying out day to day tasks
Accompanying people on social and leisure activities
Taking people on holiday
Accompanying people on routine activities e.g. going to hospital
Supervision of people
FURTHER COMMENTS/DESCRIPTON OF THE SUPPORT YOU PROVIDE …………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
NAME OF SUPPORT PROVIDER..………………………………………………………….....
SIGNATURE ………………………………………………………………………………………

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
53
DATE ……………………………………………………………………………………………….

LINCOLNSHIRE COUNTY COUNCIL SUPPORTING PEOPLE IN LINCOLNSHIRE
54
Appendix 4 – New Model for CSC
EnablementApproach
ServiceUser
Relative,etc
Professional
Give
Informa
tion
Service Pledge
Pass ToArea Office
Single Episode
Simple Intervention Sp
ecialist Intervention Improved Information
Website
Progress Chasingetc
Gather initial
information
First Contact
Information/AdviceBookings
Financial
Repair/
Replace
(Berea
vement
Journe
y)
Telecare Ass
essment
Assist with Self Assess:
‐ Smart Assist
‐ Telecare
‐ Blue Badge
Expert Ad
vice
and guid
ance
(Mental He
alth Inte
rface)
Call Back
(Multiple Ep
isode)
Minor Adjustm
entsSmartCare Clinic BookingsCallback to Letter/Fax/Email Request fromArea Office
Arrange Short ‐term
Packages
Preventative Equipment
(grab rail, key safe, etc)
Financial Assessments
(Indicative RAS)
Scheduled
Phone Reviews
County‐wideDuty
SmartCareClinics
Short‐termPackages
RoutineHospital Discharge
ProfessionalHelpline
Selectand Plan
Re‐ablement
EmergencyCarer’sService
UnscheduledReviews
Improved InformationWebsite
- Improved Signposting -

Integrated Community Services Commissioning Framework 23/06/2010 55
Appendix 5 - Staffing within specialist teams:
Brokerage
Job Role Headcount FTE
Broker 10 9.11
Brokerage Team Manager 1 1
Senior Broker 2 2
13 12.11
Salary costs for whole team (without on costs) £290286
Direct Payments
Job Role Headcount FTE
Direct Payments Dev't & Coordn Officer 1 1
Direct Paymnts Devt & Coord Asst 3 2.61
4 3.61
Salary costs for whole team (without on costs) £86121
Telecare
Job Role Headcount FTE
Telecare Project Officer 1 1
Telecare Project Co-ordinator 1 1
2 2
Salary costs for whole team (without on costs) £51811
FAB Team
Job Role Headcount FTE
Financial Assessment & Benefits Coord 2 2
Financial Assessment & Benefits Officer 13 11.59 Financial Assessment & Benefits Team Man 1 1
Senr Financial Assessment & Benefits Ofr 1 1
17 15.59
Salary costs for whole team (without on costs) £338422

Integrated Community Services Commissioning Framework 23/06/2010 56
Safeguarding
Job Role Headcount FTE
Assistant Investigation Officer 3 3 Safeguarding Team Investigating Officer 9 9
Safeguarding Team Liaison Manager 2 2
Safeguarding Team Service Manager 1 1
Totals 15 15
Salary costs for whole team (without on costs) £475163 Smartcare
Job Role Headcount FTE
Business Support (JF) 1 1Business Support (JP) 1 1Business Support (MH) 1 0.49 Total 3 2.49
Salary costs for whole team (without on costs) £40214 Total cost of specialist teams (excluding Blue Badge) = £1,525,228 Blue Badge - 5 x Grade 2-Grade 6
Transitions
Job Role Headcount FTE
Community Care Officer Level 2 1 1
Occupational Therapist 1 1
Partnership Manager 1 1
Senior Practitioner 1 0.65
Service Manager 1 1
Social Worker Level 1 3 2
Transitions Personal Advisor 1 1
Totals 9 7.65
Salary costs for whole team (without on costs) £243211

Integrated Community Services Commissioning Framework 23/06/2010 57
Appendix 6 – Call volume within Specialist Teams
Brokerage
582213%
1597936%
2215051%
Incoming (internal)
Incoming (external)
Outgoing
Smartcare Clinic Bookings
45712%
159941%
188947%
Incoming (Internal)
Incoming (External)
Outgoing
Direct Payments
5078%
417363%
195629%
Incoming (Internal)
Incoming (External)
Outgoing
Telecare
2809%
180061%
89930% Incoming (Internal)
Incoming (External)
Outgoing
Blue Badge
12758%
1269776%
267216%
Incoming (Internal)
Incoming (External)
Outgoing
Specialist Teams (Call Volume)
834111%
3624849%
2956640%
Incoming (Internal)
Incoming(External)
Outgoing

Integrated Community Services Commissioning Framework 23/06/2010 58
104
128121
131
102
128
175
155
181 200
158
114
0
20
40
60
80
100
120
140
160
180
200
January February M arch April M ay June July August September October November December
2009 New Referrals
Appendix 7 – Smart Care Data
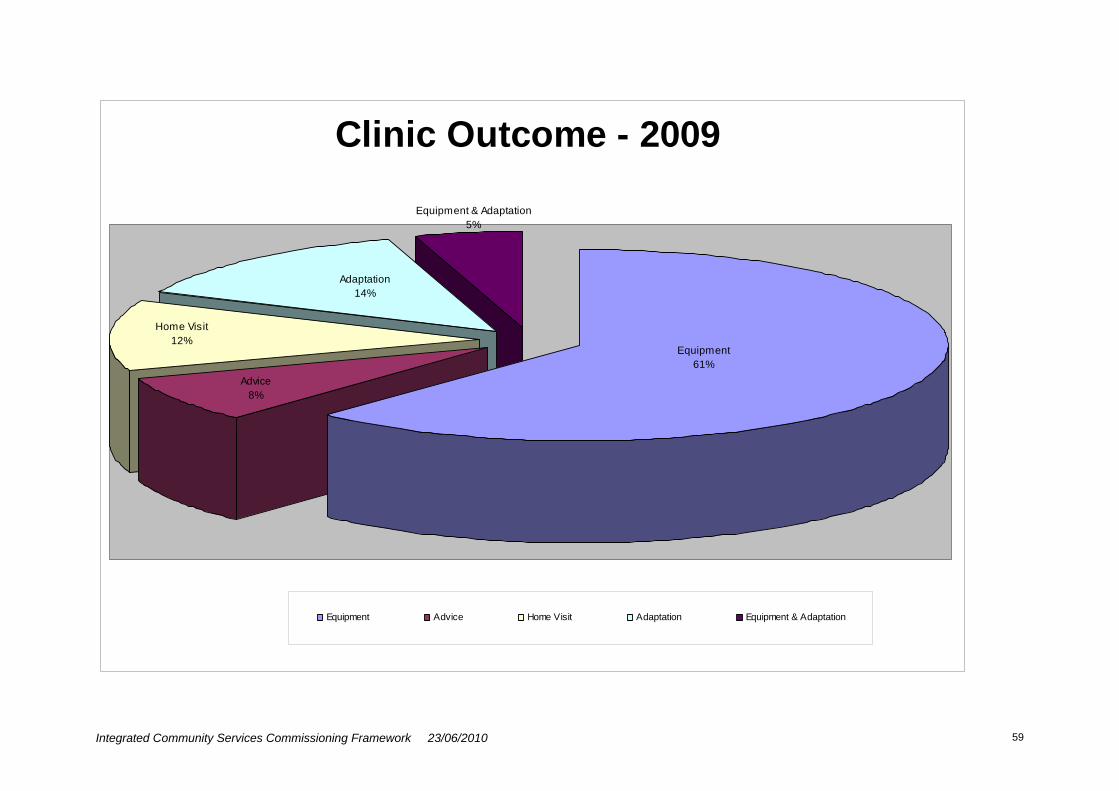
Integrated Community Services Commissioning Framework 23/06/2010 59
Clinic Outcome - 2009
Equipment & Adaptation5%
Equipment61%
Advice8%
Home Visit12%
Adaptation14%
Equipment Advice Home Visit Adaptation Equipment & Adaptation
Integrated Community Services Commissioning Framework 23/06/2010 60
Appendix 8 – Integrated Community Service
Appendix One to CC/PP LCC 2009-10 Memorandum of Agreement
DEVELOPING INTERGRATED COMMUNITY SERVICES (INTERMEDIATE CARE)
ACROSS LINCOLNSHIRE
COMMISSIONING FRAMEWORK

Integrated Community Services Commissioning Framework 23/06/2010 61
CONTENTS
1. Introduction 2. Context
3. Service Definition 4. Aims and Objectives 5. Outcomes 6. Service Components
7. Measuring Outcomes – Balance of Care

Integrated Community Services Commissioning Framework 23/06/2010 62
Vision To develop a wide range of integrated community based services to support more vulnerable people to maintain their independence and quality of life in a safe and
appropriate way Introduction
This Commissioning Specification is jointly produced between health and social care commissioners and is intended to set the strategic, commissioning framework within which services that are incorporated within intermediate care are commissioned across the county. It sets out what is meant by intermediate care, the principles that underpin such services and the key components it will be required to deliver. The over aching aim for Intermediate Care services is to ensure that wherever possible people are enabled to remain at home and independent. This document is not intended to set out ‘how’ services will be provided as it is believed for this particular range of services they will need to be developed and agreed at a locality level, in partnership with Practice Based Commissioners, to ensure the needs of the local population are addressed appropriately. Partner signatories: Ian Anderson Executive Director Lincolnshire County Council 03.06.09 Lincolnshire NHS

Integrated Community Services Commissioning Framework 23/06/2010 63

Integrated Community Services Commissioning Framework 23/06/2010 64
Our vision for the future. Diagram one illustrates our shared vision for an integrated `intermediate care system`. A system which has a recipe of services that case managers from across agencies are able to call upon to arrange timely, personalised and effective support that enables people to maximise independent living. Context Nationally and locally there is a strong emphasis on maintaining people’s ability to remain independent and at home wherever possible and avoiding unnecessary hospital admissions and admission to long term care. Over the past 5 years Lincolnshire has done a significant amount of work to ensure this aim can be achieved and the purpose of this framework is to enable localities to further develop such services and to address some of the inequities of service that have historically developed. Intermediate care services will be further developed across the County that fit with: High Quality Care for All – Next Stage Review Report Our Health, Our Care, Our Say The National Services Framework for Older People HSC 2001/01 and LAC (2001) 1 Intermediate care circular (soon to be
updated/refreshed) `Putting People First`. Shaping Health for Lincolnshire The priorities for service provision outlined in Lincolnshire County Council (LCC); Adult
Social Care, (ASC) Commissioning Plans. `It is known from the findings a bed survey undertaken by the Balance of Care Group in 2006 that at any one time approximately 35% of people who are in hospital could be discharged to a non acute setting if available. It was also noted that a number of admissions could have been avoided (Appendix 1) Definition A formal definition of Intermediate Care is contained within HSC 2001/01 and LAC (2001)1 statutory guidance from the Department of Health. Intermediate Care is a range of integrated services to promote the faster recovery from illness, prevent unnecessary acute hospital admissions and admission to long term care, support timely discharge and maximise independent living. The development of these services does not sit in isolation and will need to integrate and support initiatives such as: Long Term Conditions Programme Developing Dementia Services `Putting People First` agenda for total transformation of adult social care Improved hospital discharge arrangements. Adult Social Care’s Reablement Service development

Integrated Community Services Commissioning Framework 23/06/2010 65
Older People’s Preventative Services e.g. First Contact All of these initiatives are inextricably linked and it will be essential that they work together to deliver the overall aim of keeping people independent and safe at home. Service User Definition It is intended that this integrated service across Lincolnshire will be provided to adults with a wide range of conditions including: long term health conditions; older people with physical and mental frailty; adults with a physical disability and/or sensory impairment; adults with a learning difficulty and adults with mental health needs. Services will be provided to individuals on a basis of need, although it is anticipated that a large proportion of people supported by this service will be over the age of 65. Eligibility These services will be available to a wide range of individuals who: Reside in Lincolnshire and/or are registered with a Lincolnshire GP In respect of some elements of social care provision people will be required to meet
the County Councils` Fair Access to Care criteria. SCOPE OF THE SERVICE Aims
The over arching aim of these service developments is to:
Support people to remain independent and safe at home.
To achieve this aim services must:
Be user focused
Be prevention focused – avoidance of crisis situations
Be easily and locally accessed
Be integrated – operate together as a network of care
A range of specialist care to be rapidly accessible
Increasingly be delivered in people’s own homes
Ensure effective and timely assessment, risk management and care planning
Ensure information is shared effectively between organisations
Be provided flexibly to support individuals needs
Utilise a case management approach for those at highest risk
Be able to manage a range of different needs e.g. Mental Health, Learning Disabilities
Have continual feedback to monitor and control the systems
Anticipated Outcomes

Integrated Community Services Commissioning Framework 23/06/2010 66
Less people will be admitted to hospital unnecessarily
Fewer people will be admitted for long term care
A reduction in the utilisation of home care support
People will know what services are available and how to access them
People will feel supported and confident to remain in their own homes
Carers will have more confidence to continue to support their partners at home
There will be more rapid and timely responses to potential crisis situations
It is anticipated that there will be a range of different elements, for example:
Preventative Services
Utilising available information to identify those individuals at high risk of needing additional support e.g. GP risk stratification software – Combined PAAR and using this to pre-empt potential crisis situations arising. This is currently being rolled-out to GP practices across the County. In the future a similar predictive tool will also enable social care to identify and support people at risk of losing their independence. .
Professionals taking responsibility for taking pro-active steps to support people e.g. falls assessments, earlier referral to support services
Utilising support services such as those provided via Supporting People, First Contact Schemes and the third sector e.g. Age Concern
Increasing the use of telecare e.g. ‘Just Checking’, vital signs monitoring, falls detectors. This is currently being developed and rolled-out via the Lincolnshire Telecare Strategy, with further work being undertaken by NHS Lincolnshire to support more widespread utilisation of such technologies.
Community - Crisis Response & Rehabilitation Services
Rapid assessment and diagnosis for patients e.g. Rapid Access to Specialist teams as appropriate
Access to 24 hour assessment beds
Access to rapid response home care support
Access to Lincolnshire Assessment and Reablement Services
Access to diagnostics
A short-term programme of therapy and reablement to enable people to regain sufficient physical functioning and confidence to return or remain safely to home e.g. post surgery, post stroke, exacerbation of existing condition
Shared agenda to develop integrated `generic health and social care` rapid response services able to respond 24 hours a day, 7 days a week.

Integrated Community Services Commissioning Framework 23/06/2010 67
Early Assisted Discharge
Utilising the community services to facilitate a planned discharge from acute care by providing additional nursing and/or therapeutic support in a person’s own home or appropriate community setting.
Delivery Requirements
All providers of these services will be expected to deliver services in line with the following:
Providers of these services will be expected to work together to ensure the aims and outcomes set out on page 3 are achieved.
All people accessing these services have the right to:
o Privacy – a person’s right to be left alone, free from intrusion or public attention into their affairs
o Dignity – recognition of the intrinsic value of a person by respecting their uniqueness and personal needs
o Independence-the opportunity to act and think without referring to anyone else o Choice –the opportunity to select independently from a range of options o Rights – the maintenance of personal aspirations and abilities in all aspects of
daily life
It is expected that people wishing to access these services will be able to do through a number of routes. Each service will publish a service brochure that details access arrangements, pathways, criteria and services delivered. Access to the service will therefore be clearly signposted and where possible via single points of access (SPA). Where appropriate people will have direct access to certain services e.g. complex case managers, end of life team
Appropriate support for carers and families will be identified as part of the assessment process with appropriate referral/signposting to take place.
Access targets will be agreed with each provider e.g. response within 2 hours, 24/7 availability. This will be determined on an individual scheme basis.
Wherever possible services will be delivered within people’s own homes. Over time we will seek to reduce reliance on `bed based services` and increase availability of services that can support people in their own home.
Access to services for people with dementia will need to be assured within each locality
Increasingly the use of telehealth and telecare will be adopted by teams to support self-care and people’s independence.
Where a group of providers deliver these services within a locality steps must be taken to ensure a Multi-disciplinary Team (MDT) approach is adopted. With regular provider team meetings and increasingly electronic communication being available.

Integrated Community Services Commissioning Framework 23/06/2010 68
It is expected that providers will work together to ensure that other professionals within the network will be able to directly refer to each other without people requiring a further assessment e.g. psychological referral, request for home care, reablement assessment, etc
Trusted assessors will be identified across all organisations delivering these services and it is expected they will be empowered to access and arrange each other services across the pathway to ensure a timely and effective outcome for service users.
To support the above it is expected that providers will identify a common assessment tool e.g. Common Assessment Framework
It is expected that when a person is identified as being at high risk they will be allocated a case manager and a care plan be put in place within 24 hours of referral.
That community and hospital staff will increasingly work together to enable early assisted discharge to take place effectively.
Providers will be expected to produce a detailed workforce development plan which outlines, staffing requirements, competencies, training and development plans which identifies how providers will ensure a joint training approach across the respective teams. NHS Lincolnshire will work with providers to do this via the Workforce Development Team
Governance Arrangements
Commissioning and joint funding of services
The financial contributions for the funding of intermediate care services, performance and outcome targets will be agreed by NHS Lincolnshire and LCC Adult Social Care. For 2009/10 this agreement will be in the form of a memorandum of agreement.
Agreements will be signed by both organisations by May each financial year.
In future years, financial contributions, performance and outcome targets will also negotiated and agreed between Practice Based commissioning clusters and the Joint Commissioning Group on an annual basis. These will then form the basis of an agreement, ultimately a Section 75, between Lincolnshire NHS and Lincolnshire County Council governing arrangements for transfers of funding.
The Joint Commissioning Group will receive an annual report and a six monthly update from each intermediate care scheme within this agreement so as to monitor achievement of required performance and budgets.
Provision of services
Where intermediate services have been jointly commissioned and involve resources from both agencies arrangements must be in place to ensure that the local operational manager for the service is accountable for the performance and financial management of the service.
A quarterly activity, performance and financial report is to be shared with partner agencies (and will form the basis of 6 monthly/annual reports to JCG)

Integrated Community Services Commissioning Framework 23/06/2010 69
Any change to service provision, criteria, pathway, or funding is to be agreed between local operational managers from both agencies and a written record kept of such decisions.
Evaluation
The table at Appendix 2 sets out the proposed quality and performance measures to be utilised across the whole pathway to measure the impact services are realising.

Integrated Community Services Commissioning Framework 23/06/2010 70
GLOSSARY OF TERMS
ASSESSMENT A process whereby the needs of an individual are identified and their impact on daily living and quality of life is evaluated.
AVOIDABLE ADMISSION Admission to an acute hospital which would be
unnecessary if alternatives e.g. rapid response services were available.
CARE MANAGEMENT A process whereby an individual’s needs are assessed
and evaluated, care plans are drafted and implemented, and needs are monitored and re-assessed.
CARE MANAGER A practitioner who, as part of their role, undertakes care
management. CARE PACKAGE A combination of services designed to meet a person’s
assessed needs. CARE PLANNING Care planning is a process based on an assessment of
an individual’s assessed need that involves determining the level and type of support to meet those needs, and the objectives and potential outcomes that can be achieved.
INTERMEDIATE CARE A short period (normally no longer than six weeks) of
intensive rehabilitation and treatment to enable patients to return home following hospitalisation, or to prevent admission to long term residential care; or intensive care at home to prevent unnecessary hospital admission.
LONG-TERM CARE Refers to support services provided over a prolonged
period of time or on a permanent basis to adults who have difficulties associated with old age, long-term illness or disability. Care may be provided in residential settings such as nursing homes or in people’s own homes over a prolonged period of time or on a permanent basis.
MULTIDISCIPLINARY Multidisciplinary refers to when professionals from
different disciplines – such as social work, nursing, occupational therapy, work together.
MULTIDISCIPLINARY Multidisciplinary assessment is an

Integrated Community Services Commissioning Framework 23/06/2010 71
ASSESSMENT assessment of an individual’s needs that has actively involved professionals from different disciplines in collecting and evaluation assessment information.
RAPID RESPONSE A service designed to prevent avoidable acute
admissions by providing rapid assessment/diagnosis for older people referred from GPs. A&E, NHS Direct or social services and (if necessary) rapid access on a 24-hour basis to short-term nursing/therapy support and personal care in the patient’s own home, together with appropriate contributions from community equipment services and/or housing-based support services.
REABLEMENT The aim of reablement is to support older people to
regain or relearn living skills following an illness or change in circumstances.
REHABILITATION A programme of therapy and reablement designed to
restore independence and reduce disability.

Integrated Community Services Commissioning Framework 23/06/2010 72
Intermediate Care – Performance Outcomes and Measures Indicator Measure Baseline Target/Timescales Comment Older people with an illness are cared for at home whenever possible
A reduction in avoidable hospital admissions for ambulatory care sensitive conditions – segmented by age (To include step-up community patients)
a) Measured centrally as part of the PCT Strategic Plan (Goal 1 and Goal 4) Vital Signs local priority targets VSC21 target b) Measured locally by the Single Point of Access staff – monthly report
People spend less time within an acute hospital bed when admitted as an emergency
A reduction in emergency bed days for patients – segmented by age
Measured centrally for Vital Signs local priority targets VCS20 (& VSC 11 in 2008/09)
People will be discharged home in a planned and timely manner
A reduction in the number of occupied bed days used due to a delayed transfer of care (DTOC) caused by lack of IC
Measured centrally for Vital Signs local priority targets VSC10 + Healthcare Commission ratings exercise

Integrated Community Services Commissioning Framework 23/06/2010 73
Indicator Measure Baseline Target/Timescales Comment Patients will not need to be readmitted to hospital for the same condition within 14 days of discharge
No year on year increase in emergency re-admissions within 14 days (from daycase & inpatient discharge); for patients – segmented into age groups
Measured centrally for ULHT SLA contract monitoring
People will be provided with knowledge and equipment to prevent falls in their own environment
A reduction in emergency admissions due to falls with a LOS of more than 2 days
The Community Response and Rehabilitation service to report on progress 6 monthly
Older people feel supported to live independently at home
An increase in people 65+ being supported with care packages in their own home
Monitored centrally Local priority target: Part of VSC03 (2008/11) + Local Authority Indicator N1136
A reduction in long-term placements within residential and nursing home beds
Number of admissions of people over age of 65 per 10,000 population into care homes
2008/09; 71.6 (977 admissions)
2009/10 target: 70. (approx 950 admissions)
Local Authority indicator

Integrated Community Services Commissioning Framework 23/06/2010 74
Indicator Measure Baseline Target/Timescales Comment People will receive rehabilitation following hospital discharge whenever assessed as necessary to achieve independence
Percentage of patients who received planned rehabilitation for up to 6 weeks following hospital discharge who remain at home
2008/09 70%
2009/10 target: 74% 2010/11 target: 78%
Local Area Agreement target + Local Authority National Indicator N1125
Number of people receiving intermediate care in a residential setting (rapid response/supported discharge) to prevent hospital admission
LA SAS indicator
2008/09: 596
2009/10 target: 600
Number of people receiving intermediate care in a residential setting (rapid response/supported discharge) to facilitate timely hospital discharge and/or effective rehabilitation
LA SAS indicator
2008/09: 638
2009/10 target: 650
Number of people receiving non-residential intermediate care to prevent hospital admission
LA SAS indicator
2008/09: 2114
2009/10 target 2300
Number of people receiving non-residential intermediate care to facilitate timely hospital discharge and/or effective rehabilitation
LA SAS indicator
2008/09: 1800
2009/10 target: 1900

Integrated Community Services Commissioning Framework 23/06/2010 75
Indicator Measure Baseline Target/Timescales Comment Total number of people supported by each team per quarter: OP with mental frailty OP with Physical frailty OP with both
Referral to assessment
timescale:
RAPID RESPONSE Total % seen within 1 working day STANDARD Total % seen within 2 working days
Length of stay in service:
6 weeks for intermediate care
4 weeks for intermediate assessment
1. Bed occupancy:
% over 4 week period
Where appropriate reporting on indicators to be split into the following age ranges:
Adults – 18 – 65 years; 65-75 years of age; over 75

Integrated Community Services Commissioning Framework 23/06/2010 76
Appendix 9 – Gold Standard Reablement Pathway
Entry into
system
Reablement package
Exit point
Referral:• Comprehensive information for the service user and carer• Clearly defined eligibility criteria• Single point of access• Links to others services are clear• The role of reablement in relation to hospital discharge is clear
Screening and Assessment:• Comprehensive outcome focussed ongoing assessment• Carers are actively involved throughout
Support plan & intervention:• Roles within the service are clear and understood by all• Outcomes based and user focussed support is provided• Equipment and telecare are readily available• Support should be available 7 days a week and should be provided in a variety of settings
Dynamic reviewing:• Access is available for people whose needs are being reviewed• Reviews are a regular and ongoing feature f the service• The emphasis is on outcomes achieved• Users and carer are fully involved in the reviews
Handover/closure:• Follow‐up reviews are scheduled and undertaken• Community inclusion is enabled where there is no ongoing statutory sector support• Close links with other community providers and sectors• Evaluation is a core element of the service
Pathway element and best practice issues:
Cross‐cutting issues:• Clear strategy and vision• Understanding of investment resource required and financial benefits accrued• HR/OD strategy

Integrated Community Services Commissioning Framework 23/06/2010 77
Appendix 10 - Detailed breakdown of staffing Each service area is divided into areas/teams: Learning Disabilities North – Lincoln/Hykeham Louth/Horncastle Gainsborough/Market Rasen Fit for the Future Team
LD North Headcount FTE
Community Care Officer 2 2
Partnership Manager 3 3
Practitioner Unqualified 14 11.42
Qualified Practitioner Level 1 8 8
Qualified Practitioner Level 2 7 5.74
Senior Practitioner 3 2.49
Service Manager 1 1
Totals 38 33.65
Salary costs for whole team (without on costs) £980098 Learning Disabilities South – Grantham/Bourne Spalding/Sleaford Boston/Skegness
LD South Headcount FTE
Area Manager 1 1
Partnership Manager 3 3
Practitioner (Unqualified) 14 11.47
Qualified Practitioner Level 1 2 1.81
Qualified Practitioner Level 2 10 7.63
Senior Practitioner 2 2
Totals 32 26.91
Salary costs for whole team (without on costs) £800400 Physical Disabilities – North Louth/Horncastle Physical Disabilities – South Lincs Visual Impairment Services Physical Disabilities – South West Boston/Spalding Physical Disabilities - West
PD Headcount FTE
Area Manager 1 1
Community Care Officer Level 1 4 3.4
Community Care Officer Level 2 8 7.31 Direct Payments Dev't & Coordn Officer 1 1
Direct Payments Devt & Coord Asst 3 2.61
Occupational Therapist Level 1(OP/PD) 7 6.5
Occupational Therapist Level 2 3 2.11
Office Administrator - LVIS 1 1
Partnership Manager 3 3
Practice Supervisor 6 5.19
Service Co-ordinator 3 3
Social Worker - PD Level 1 7 6.53
Social Worker - PD Level 2 2 1.81
Support Worker 1 1
Totals 50 45.46 Salary costs for whole team (without on costs) £1256633
Older People North West – Lincoln North Hykeham West Lindsey
OP NW Headcount FTE Community Care Officer Level 1 9 8.57 Community Care Officer Level 2 25 21.99 Occupational Therapist 1 1

Integrated Community Services Commissioning Framework 23/06/2010 78
CMHT North West
Occupational Therapist Level 2 5 4 Practice Manager 5 4.61 Practice Supervisor 10 9.43 Service Manager 1 1 Social Care Co-Coordinator 3 3 Social Worker - Older People Level 1 6 5.81 Social Worker - Older People Level 2 10 9.53 Totals 75 68.94 Salary costs for whole team (without on costs) £1955705
Older People North East – Louth Louth County Hospital Horncastle Intermediate Care Team CMHT North East Skegness
OP NE Headcount FTE Area Manager 1 1 Community Care Officer Level 1 3 3 Community Care Officer Level 2 22 19.62 Occupational Therapist Level 1 2 1.5 Occupational Therapist Level 2 1 0.5 Practice Manager 2 2 Practice Supervisor 6 6 Social Care Co-ordinator 2 2 Social Worker - Older People Level 1 1 0.73 Social Worker - Older People Level 2 5 4.61 Totals 45 40.96 Salary costs for whole team (without on costs) £1156003
Older People South West – Sleaford Stamford Grantham Grantham CMHT Grantham Hospital
OP SW Headcount FTE Community Care Officer Level 1 10 10 Community Care Officer Level 2 18 16.31 Occupational Therapist Level 1(OP/PD) 2 1 Occupational Therapist Level 2 1 1 Practice Manager 3 3 Practice Supervisor 5 4.81 Service Manager 1 1 Social Care Co-ordinator 4 4 Social Worker - Older People Level 1 2 2 Social Worker - Older People Level 2 6 5.31 Totals 52 48.43 Salary costs for whole team (without on costs) £1324277
Older People East – Spalding Pilgrim Hospital Boston CMHT South East
OP SE Headcount FTE Community Care Officer Level 1 10 8.57 Community Care Officer Level 2 14 12.16 Occupational Therapist Level 2 2 2 Practice Manager 3 3 Practice Supervisor 6 5.81 Service Manager 1 1 Social Care Co-ordinator 2 2 Social Worker - Older People 8 8

Integrated Community Services Commissioning Framework 23/06/2010 79
Level 1 Social Worker - Older People Level 2 5 5 Totals 51 47.54 Salary costs for whole team (without on costs) £1349192

Integrated Community Services Commissioning Framework 23/06/2010 80
Appendix 11 – Summary of Activity Summary of Activity in Adult Social Care between the period 01.01.2009 to 31.12.2009 Events
Client Carer
Contacts Referrals
Assessments Reviews Assessments Reviews
All Assessment events
(Assessments + Reviews)
Leading to Services
Services provided
Older People 34928 12691 18437 19708 732 763 39640 18495 27874 Physical Disability 4824 2043 3283 3271 211 404 7169 2787 4355 Learning disability 841 174 284 2009 75 127 2495 616 1676 Mental Health 457 59 134 67 85 46 332 239 421 Other 1742 243 306 187 170 26 689 333 637 Substance Misuse 10 2 3 9 1 1 14 7 13 Grand Total 42802 15212 22447 25251 1274 1367 50339 22477 34976 car badges removed
Individuals Client Carer
Contacts Referrals Assessments Reviews Assessments Reviews
All Assessment events
(Assessments + Reviews)
Leading to Services
Services provided
Older People 17865 10631 11055 10582 730 759 17057 6064 16518 Physical Disability 2975 1831 2066 1990 211 404 3423 1121 2693 Learning disability 550 164 226 1606 75 127 1769 402 767 Mental Health 294 48 101 38 85 46 231 182 366 Other 1446 228 239 126 170 26 491 251 489 Substance Misuse 6 1 2 4 1 1 6 2 6 Grand Total 23136 12903 13689 14346 1272 1363 22977 8022 20839

Integrated Community Services Commissioning Framework 23/06/2010 81
Current people who use services as at 31.12.2009
Reablement (Full year estimate provided - based on 3 months data)
Client Carer
Personal Budget*
Traditional Services
Personal Budget*
Traditional Services
Est. No. of clients with a reablement
need
Reablement Successful?
*
Older People 339 9497 2120 659 Older People 3696 760
Physical Disability 354 1233 923 150
Physical Disability 308 52
Learning disability 184 1466 308 140
Learning disability 4 0
Mental Health 74 161 248 19 Mental Health 4 0
Other 24 42 300 39 Other 40 8 Substance Misuse 2 6 4 0
Substance Misuse 0 0
Grand Total 977 12405 3903 1007 Grand Total 4052 820
*includes current open direct payments, individual budgets and/or directly provided services offered via a personal budget.
*based on referral closure reason of Aim Achieved, 12 weeks after reablement assessment.
Estimated number based on 3 months of activity (October to December) and multiplied by 4.
Telecare No of people in
receipt of telecare
No of items of Telecare
provided
Older People 1173 3696 Physical Disability 159 308 Learning disability 13 4 Mental Health 7 4 Other 10 40 Substance Misuse 0 0 Grand Total 1362 4052
*based on all items of Telecare provided

Integrated Community Services Commissioning Framework 23/06/2010 82
Appendix 12 – Skills Analysis Stage of Journey Intermediate Skills Advanced Who could do this? Support Planning Problem solving
Facilitation Communication Advocacy Negotiation Conciliation Partnership working Time management Team working Professional assertiveness Observation Record keeping Enabling independence Creative thinking Financial Outcome focussed
Risk management Motivational
The person themselves Family Friends Third Sector organisation ULO Adult Social Care LPFT (whoever the person chooses)
Support Plan Sign Off
Creative thinking Communication Negotiation Financial Partnership working Risk Management
Creative thinking Communication Financial Risk Management
Adult social care/LPFT
Brokerage Facilitation Negotiation Time management Problem solving Communication Advocacy Partnership working Record keeping Enabling independence Creative thinking Financial Outcome focussed
Communication Creative thinking Financial
The person themselves Family Friends Third Sector organisation ULO Adult Social Care (whoever the person chooses)
Review Advocacy Partnership Working Time management Observation Enabling Independence Financial
Problem solving Communication Risk management Creative thinking Motivational
Adult social care/LPFT/self review