new criteria for posttraumatic stress disorder in dsm-5...
TRANSCRIPT
Paul A. Arbisi, Ph.D. ABAP, ABPP. Staff Psychologist
Minneapolis VA Medical Center Professor
Departments of Psychiatry and Psychology University of Minnesota
Private Practice
New Criteria for Posttraumatic Stress Disorder in DSM-5: Implications for Causality
What Constitutes a Traumatic Event?
How common is PTSD
Epidemiology of trauma and development of PTSD
DSM-5 Definition of PTSD
Implications for causality and compensation
Empirically Validated Treatments for PTSD
Implications for MMI and PPD ratings
Overview
Until recently, PTSD was not a compensable condition under MN Workers Compensation statutes.
Statute amended to specifically allow PTSD to be considered a “mental impairment” covered by WC without having been caused by a physical injury. Previously disallowed under Lockwood.
“mental impairment” means a diagnosis of PTSD by a licensed psychiatrist or psychologist and PTSD means the condition as described in the most recently published edition of DSM.
Significant changes in the definition of PTSD in DSM-5
Will new definition impact WC claims and PTSD claims after a personal injury?
PTSD a Consequential Injury
One of the few Psychiatric Disorders that requires the identification of a causal factor. An event at time 1 leads to the development
of emotional symptoms that cause impairment at time 2
Assumes that the traumatic event causes the development of symptoms and consequential disability.
PTSD Unique Among Psychiatric Disorders
Latitude as to What Constitutes a Traumatic Event
How common is exposure to a
traumatic event?
How frequently does PTSD ensue after exposure to a traumatic event?
Is PTSD Inevitable after Exposure to a Traumatic
Event?
Epidemiological Surveys of Trauma
National Comorbidity Survey (NCS): DSM-III-R definition, 12 specific types of trauma
61% of men and 51% of women had a history of trauma exposure
Most common: Witnessing someone being injured or killed Being involved in fire or natural disaster Being involved in life threatening accident
Detroit Area Survey DSM-IV definition, 19 types of trauma assessed
Lifetime prevalence of trauma exposure = 90% Most common was unexpected death of a loved one (60%) 77% of those exposed met Criterion A2 (so 70% had full
Criterion A stressors)
Conclusion: Trauma is not rare
Prevalence of PTSD
Estimates are surprisingly stable across studies: Men, lifetime prevalence about 5-6% Women, lifetime prevalence about 10-12% Overall, typically 7-9%
Point prevalence Typically 1-2%
Trauma exposure is common, PTSD is relatively rare.
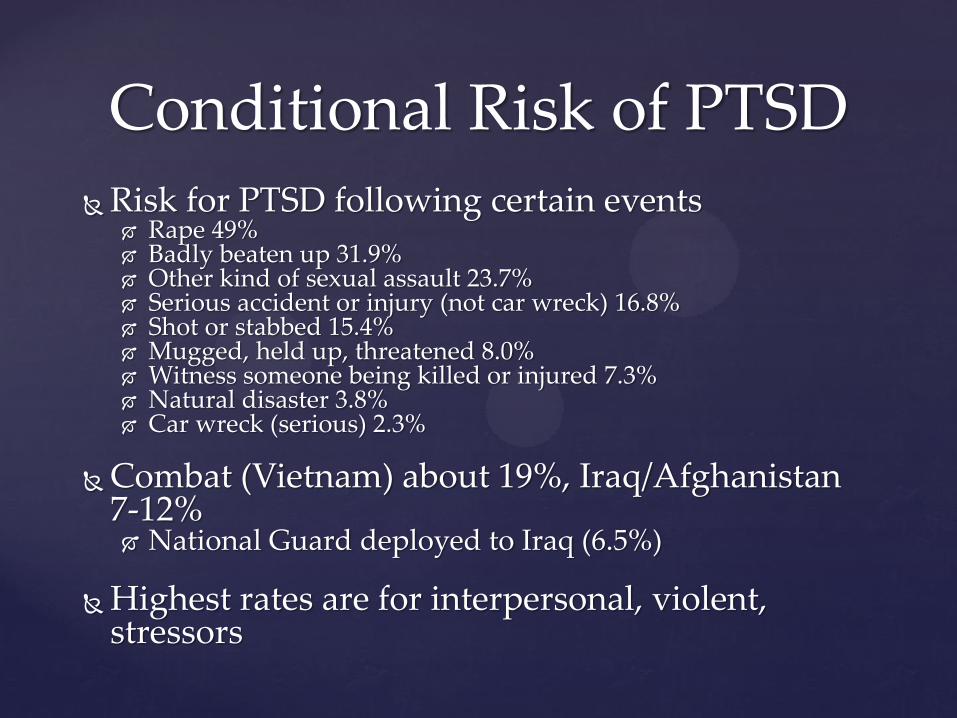
Conditional Risk of PTSD Risk for PTSD following certain events
Rape 49% Badly beaten up 31.9% Other kind of sexual assault 23.7% Serious accident or injury (not car wreck) 16.8% Shot or stabbed 15.4% Mugged, held up, threatened 8.0% Witness someone being killed or injured 7.3% Natural disaster 3.8% Car wreck (serious) 2.3%
Combat (Vietnam) about 19%, Iraq/Afghanistan
7-12% National Guard deployed to Iraq (6.5%)
Highest rates are for interpersonal, violent, stressors
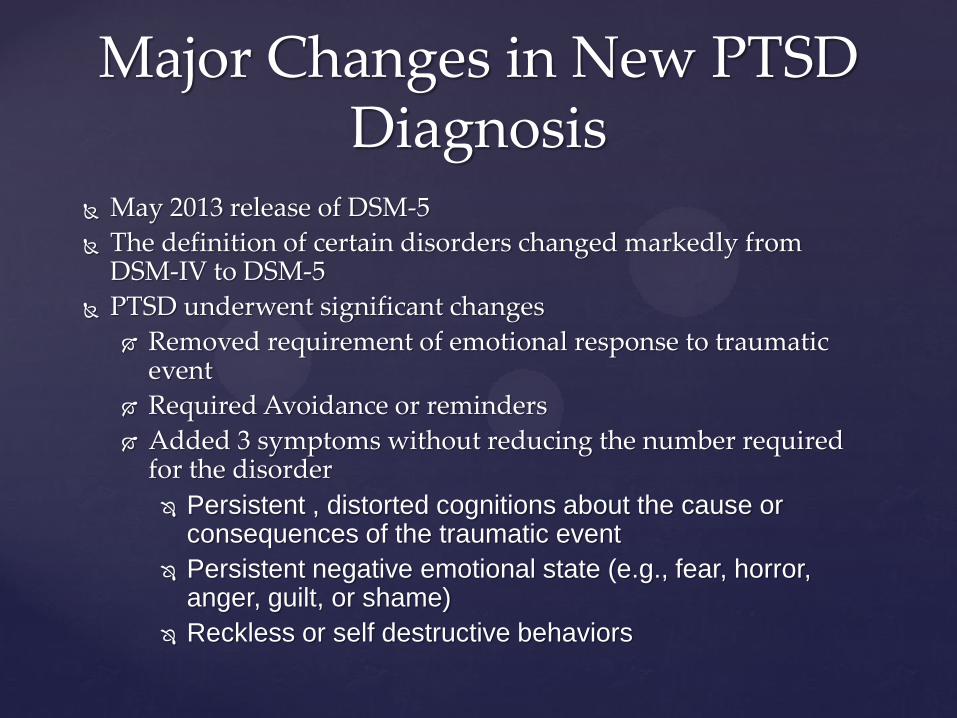
May 2013 release of DSM-5
The definition of certain disorders changed markedly from DSM-IV to DSM-5
PTSD underwent significant changes
Removed requirement of emotional response to traumatic event
Required Avoidance or reminders
Added 3 symptoms without reducing the number required for the disorder
Persistent , distorted cognitions about the cause or consequences of the traumatic event
Persistent negative emotional state (e.g., fear, horror, anger, guilt, or shame)
Reckless or self destructive behaviors
Major Changes in New PTSD Diagnosis
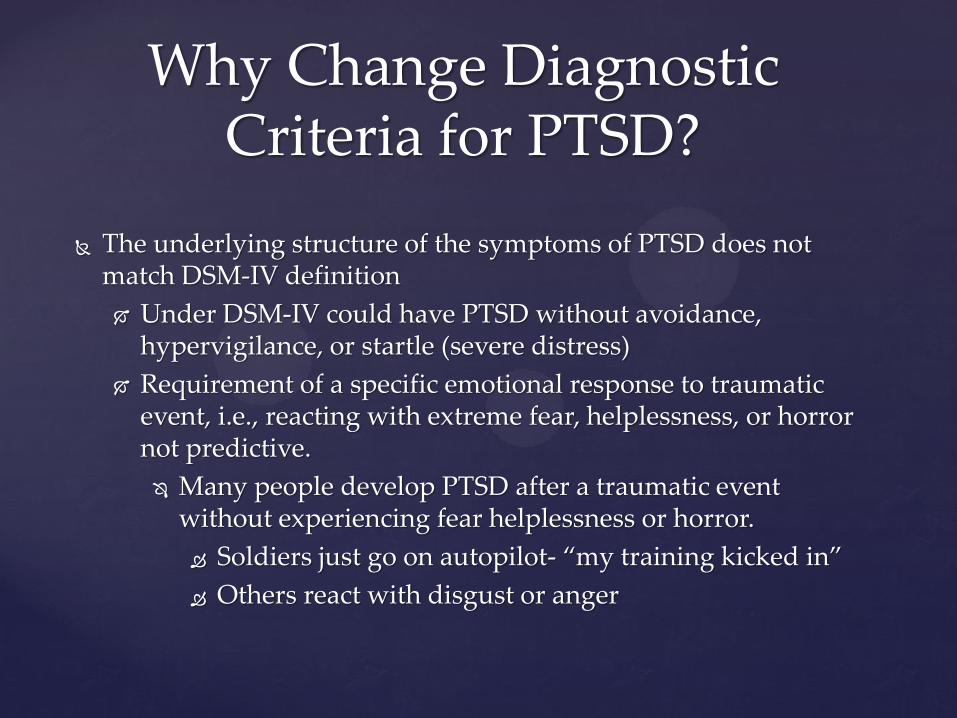
The underlying structure of the symptoms of PTSD does not match DSM-IV definition
Under DSM-IV could have PTSD without avoidance, hypervigilance, or startle (severe distress)
Requirement of a specific emotional response to traumatic event, i.e., reacting with extreme fear, helplessness, or horror not predictive.
Many people develop PTSD after a traumatic event without experiencing fear helplessness or horror.
Soldiers just go on autopilot- “my training kicked in”
Others react with disgust or anger
Why Change Diagnostic Criteria for PTSD?
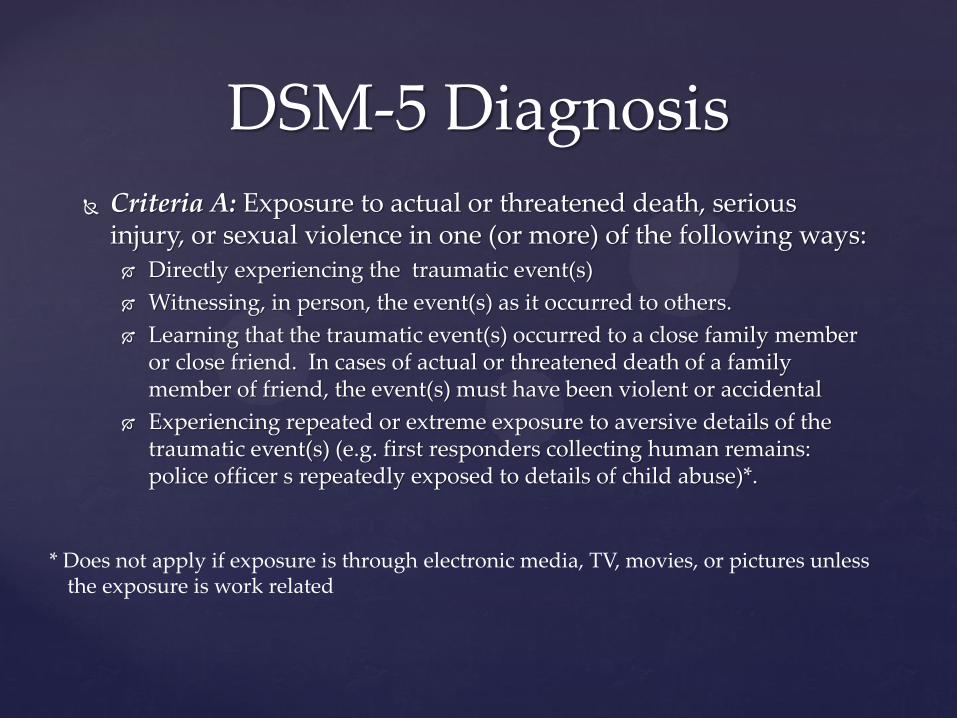
Criteria A: Exposure to actual or threatened death, serious injury, or sexual violence in one (or more) of the following ways: Directly experiencing the traumatic event(s)
Witnessing, in person, the event(s) as it occurred to others.
Learning that the traumatic event(s) occurred to a close family member or close friend. In cases of actual or threatened death of a family member of friend, the event(s) must have been violent or accidental
Experiencing repeated or extreme exposure to aversive details of the traumatic event(s) (e.g. first responders collecting human remains: police officer s repeatedly exposed to details of child abuse)*.
DSM-5 Diagnosis
* Does not apply if exposure is through electronic media, TV, movies, or pictures unless the exposure is work related
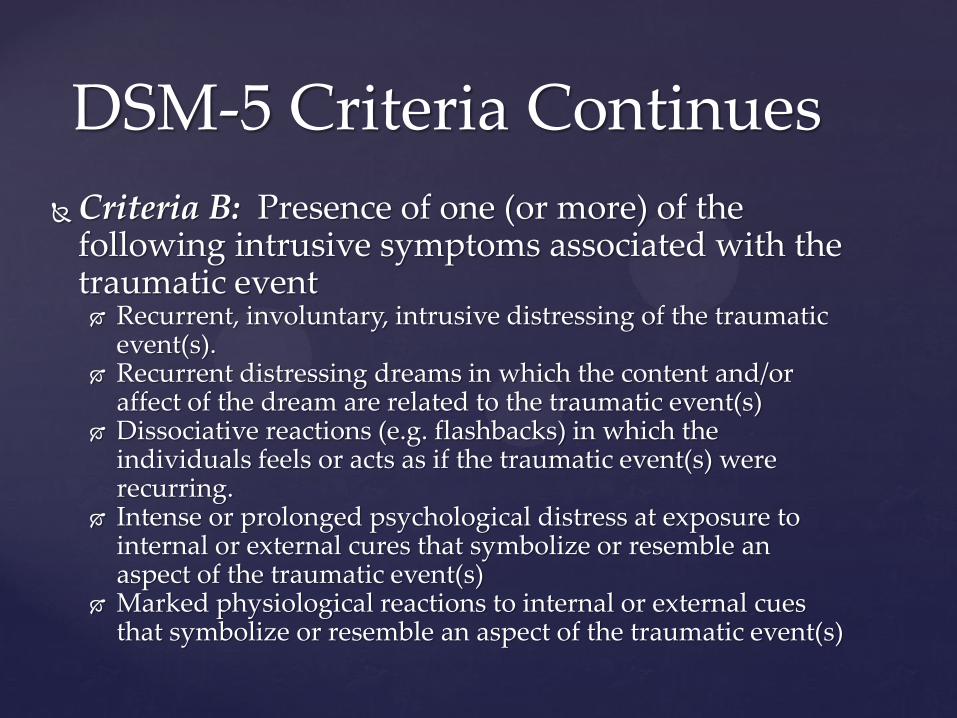
Criteria B: Presence of one (or more) of the following intrusive symptoms associated with the traumatic event Recurrent, involuntary, intrusive distressing of the traumatic
event(s). Recurrent distressing dreams in which the content and/or
affect of the dream are related to the traumatic event(s) Dissociative reactions (e.g. flashbacks) in which the
individuals feels or acts as if the traumatic event(s) were recurring.
Intense or prolonged psychological distress at exposure to internal or external cures that symbolize or resemble an aspect of the traumatic event(s)
Marked physiological reactions to internal or external cues that symbolize or resemble an aspect of the traumatic event(s)
DSM-5 Criteria Continues
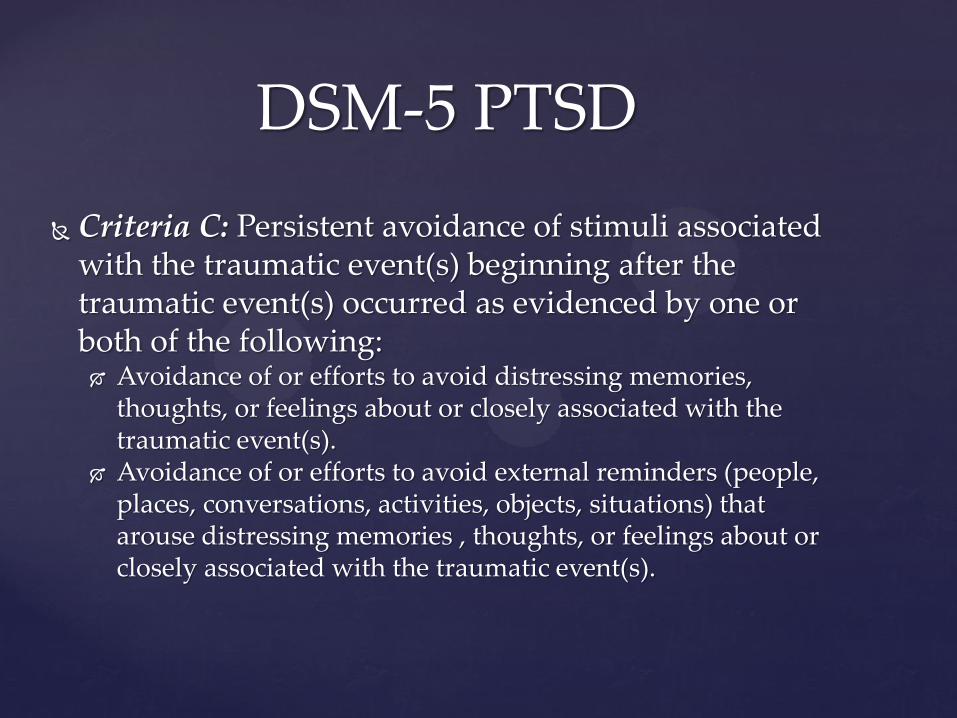
Criteria C: Persistent avoidance of stimuli associated with the traumatic event(s) beginning after the traumatic event(s) occurred as evidenced by one or both of the following: Avoidance of or efforts to avoid distressing memories,
thoughts, or feelings about or closely associated with the traumatic event(s).
Avoidance of or efforts to avoid external reminders (people, places, conversations, activities, objects, situations) that arouse distressing memories , thoughts, or feelings about or closely associated with the traumatic event(s).
DSM-5 PTSD
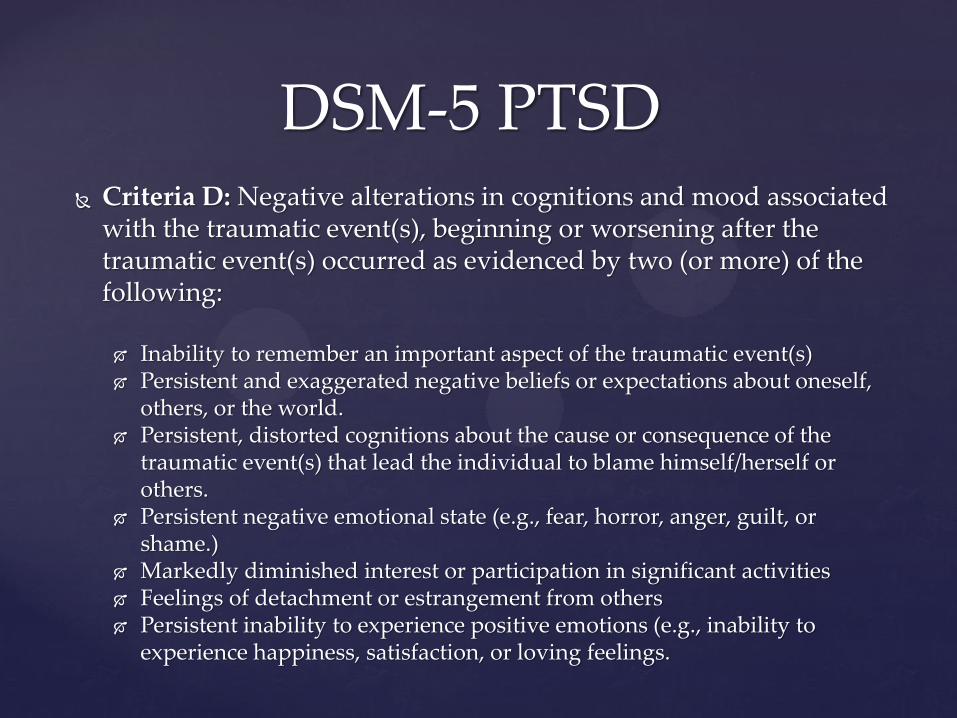
Criteria D: Negative alterations in cognitions and mood associated with the traumatic event(s), beginning or worsening after the traumatic event(s) occurred as evidenced by two (or more) of the following:
Inability to remember an important aspect of the traumatic event(s) Persistent and exaggerated negative beliefs or expectations about oneself,
others, or the world. Persistent, distorted cognitions about the cause or consequence of the
traumatic event(s) that lead the individual to blame himself/herself or others.
Persistent negative emotional state (e.g., fear, horror, anger, guilt, or shame.)
Markedly diminished interest or participation in significant activities Feelings of detachment or estrangement from others Persistent inability to experience positive emotions (e.g., inability to
experience happiness, satisfaction, or loving feelings.
DSM-5 PTSD
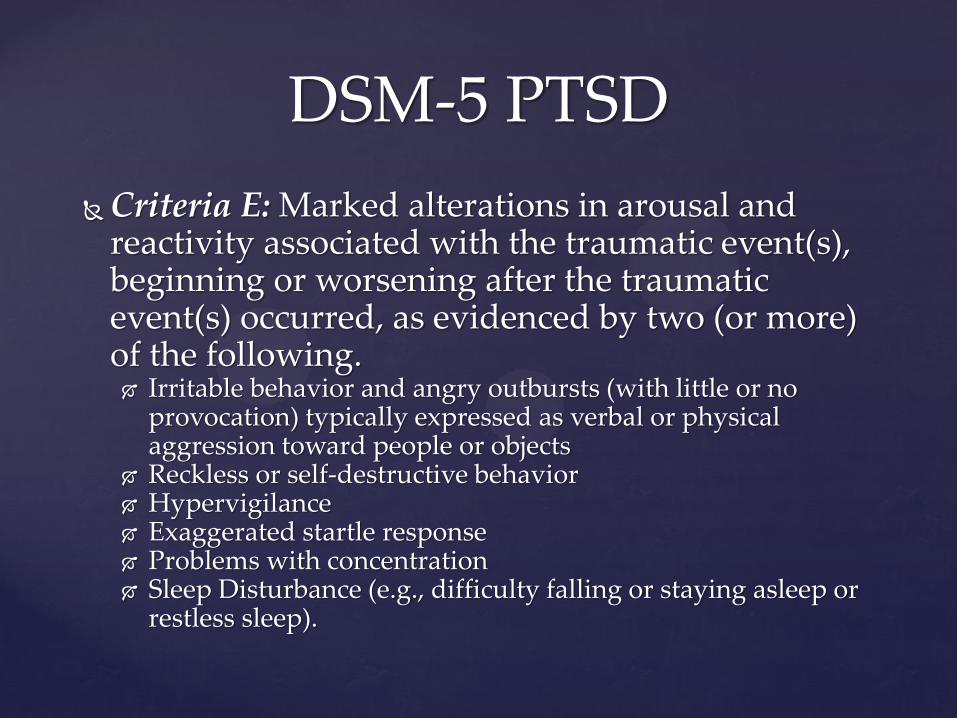
Criteria E: Marked alterations in arousal and reactivity associated with the traumatic event(s), beginning or worsening after the traumatic event(s) occurred, as evidenced by two (or more) of the following. Irritable behavior and angry outbursts (with little or no
provocation) typically expressed as verbal or physical aggression toward people or objects
Reckless or self-destructive behavior Hypervigilance Exaggerated startle response Problems with concentration Sleep Disturbance (e.g., difficulty falling or staying asleep or
restless sleep).
DSM-5 PTSD
Criteria F: Duration of the Disturbance (Criteria B, C, D, and E) is more than 1 month.
Criteria G: The disturbance cause clinically significant distress or impairment in social , occupational, or other important areas of functioning.
Criteria H: The disturbance is not attributable
to the physiological effect of substances or another medical condition.
DSM-5 PTSD
Mixed Bag
Less reliance on subjective emotional response
Greater likelihood of misattribution because of high degree of negative emotion and distress
More focus on “core” features of PTSD i.e., must have specific re-experiencing and avoidance symptoms
Includes as core symptoms aggressive and reckless behaviors that were quite likely present before the traumatic event.
More symptoms, but lower absolute percentage needed for diagnosis.
Anger counted twice.
Implications of Proposed Changes for Establishment of
Causality
May become easier for clinicians to make diagnosis of PTSD
Event occurs at Time 1, e.g., motor vehicle accident
Evaluated at Time 2
Becomes distressed when reminded of the accident, e.g. sees a vehicle of similar make and model
Avoids talking about accident
Feels angry all the time and blames others for problems
Drinks too much, gets into fights, and has problems sleeping
Does not feel able to return to work because involves driving.
Clinician Can Diagnose PTSD
Implications for Causality
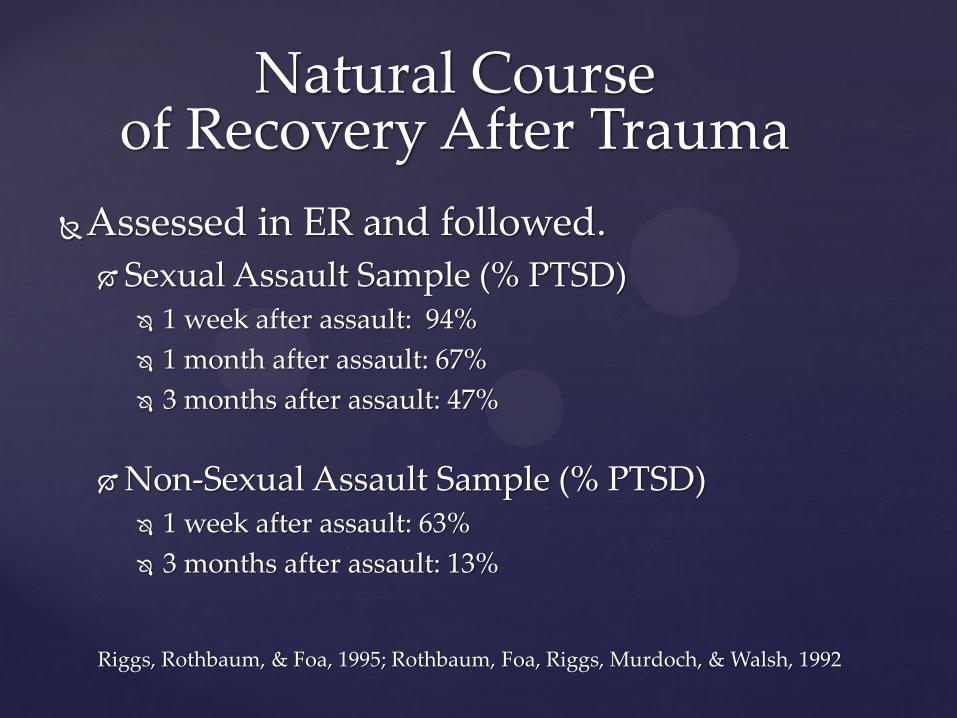
Natural Course of Recovery After Trauma
Assessed in ER and followed.
Sexual Assault Sample (% PTSD) 1 week after assault: 94%
1 month after assault: 67%
3 months after assault: 47%
Non-Sexual Assault Sample (% PTSD) 1 week after assault: 63%
3 months after assault: 13%
Riggs, Rothbaum, & Foa, 1995; Rothbaum, Foa, Riggs, Murdoch, & Walsh, 1992
Treatment is Effective Combination of psychotherapy and medication.
Prolonged Exposure Therapy (PE) (Foa, 2000). Focus on exposing patient to stressful cues or reminders
Cognitive Processing Therapy (CPT) (Resick & Schnicke, 1992) a cognitive therapy that combines a written exposure
component. Eye Movement Desensitization and Reprocessing Therapy
(EMDR) Exposure to distressing memories or thoughts while moving eyes
back and forth Exposure is the effective component, eye movement is superfluous
Cognitive Behavioral Therapy
Treatment for PTSD
Employee exposed to interpersonal violence
Employee to see therapist, but don’t force to talk about event. Most symptoms disappear within a month
If a month elapses with symptoms resulting in impairment, see therapist for empirically supported treatment for PTSD and psychiatrist for medication
CPE and PE standardized treatments lasting 10 sessions.
MMI after 14-15 sessions and adequate trail of medication
Maybe longer if co-morbid conditions e.g., Depression and Alcohol Dependence.
Maximum Medical Improvement
Unclear what rating would apply
5223.0360 CENTRAL NERVOUS SYSTEM
Subpart D. Emotional Disturbance and personality changes
10% intermittent emotional disturbance requiring intervention by a caregiver only present under stressful situation
20% mild emotional disturbance is present at all times but can live independently and relate to others
40% Moderate emotional disturbance is present at all time and can live independently but requires some supervision on a daily basis.
Weber Ratings between 10 and 20%
Permanent Partial Disability (PPD)?
Document Symptoms of PTSD
Description of symptom
For example, describe the content of Nightmares
How do the symptoms result in impairment in function.
Document presence of other psychiatric disorder
PTSD is a subjective condition and easily feigned. Must have objective measure of psychological functioning that includes validity indices
MMPI-2 Restructured Form.
Crucial Components of PTSD Evaluation

Development of PTSD Rare after exposure to traumatic event Vast majority of trauma exposed do not develop
PTSD! Events most likely to lead to PTSD involve
interpersonal violence DSM-5 Criteria for PTSD
Significant Change from DSM-IV Remains to be seen if easier to obtain the diagnosis
Effective Treatments for PTSD Must include a exposure component
With proper treatment PTSD does not result in permanent disability
Conclusions