neurovegetative regulation of the vascular system - springer · neurovegetative regulation of the...
TRANSCRIPT

Neurovegetative Regulation of the Vascular System
Blair P. Grubb* and Beverly KarabinCollege of Nursing, Health Science Campus, Syncope and Autonomic Disorders Center, The University of Toledo,Toledo, OH, USA
Abstract
The autonomic nervous system is an extensive and complex component of the human nervoussystem that governs many of the functions necessary for the maintenance of life itself. This chapterreviews various aspects of autonomic organization and regulatory functions as well as commondisturbances in the system that ultimately lead to various disease states.
Glossary of Terms
Autonomic nervoussystem (ANS)
The aspect of the human nervous system that regulates involuntaryfunctions
Hypothalamus A portion of the brain that contains a variety of nuclei that governa variety of body functions, including autonomic control
Implantable looprecorder (ILR)
Implantable device capable of recording heart rate and rhythm overprolonged periods of time
Mechanoreceptors Unmyelinated C-fibers that increase electrical activity in response tostretch
Neurocardiogenicsyncope
Also called vasovagal syncope. Caused by sudden sympatheticwithdrawal resulting in hypotension and bradycardia leading tosyncope
Neurovegetative Another term for autonomicParasympathetic Aspect of the autonomic nervous system that regulates inhibitory
functions (“rest and digest”)Reflex syncopes A group of syncopal syndromes which occur due to sympathetic
withdrawal following an abnormal response to mechanoreceptoractivation in a variety of areas
Sympathetic Aspect of the autonomic nervous system that regulates excitatoryfunctions (“flight or flight”)
Syncope The transient loss of consciousness with spontaneous recovery
Neurovegetative Control of the Vascular System
In order to survive, an animal must have the ability to constantly make moment by moment changesthat allow its internal environment to remain constant despite dramatic shifts in external conditions.Not only must the animal be able to make adjustments for the alterations in environmental
*Email: [email protected]
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 1 of 25

temperature, humidity, and barometric pressure, it must also be able to make very rapid responsesthat allow it to react when exposed to an external threat that places it in danger.
How is this moment by moment regulation achieved and how is it coordinated with the consciousperception of an emotion such as fear? The peripheral aspect of this regulation was first addressed in1878 by the French physiologist Claude Bernard who notes that the internal environment (milieuinterieur) of the body is highly regulated so as to be maintained in a stable, narrow range (Purvis1997). This consistency is a result of regulatory mechanisms that limit the variability of the bodystate. In 1929, Cannon introduced the term “homeostasis” into physiology and together with Bard,found that the key neural mechanisms for maintaining homeostasis are principally located in thehypothalamus and its two effector systems: the autonomic system and the endocrine system(Calabrese et al. 1995). This chapter will focus mainly on the autonomic aspects of vascular control,the maintenance of postural normotension, and the various clinical disorders that occur when thesesystems are disturbed.
The Autonomic Nervous System
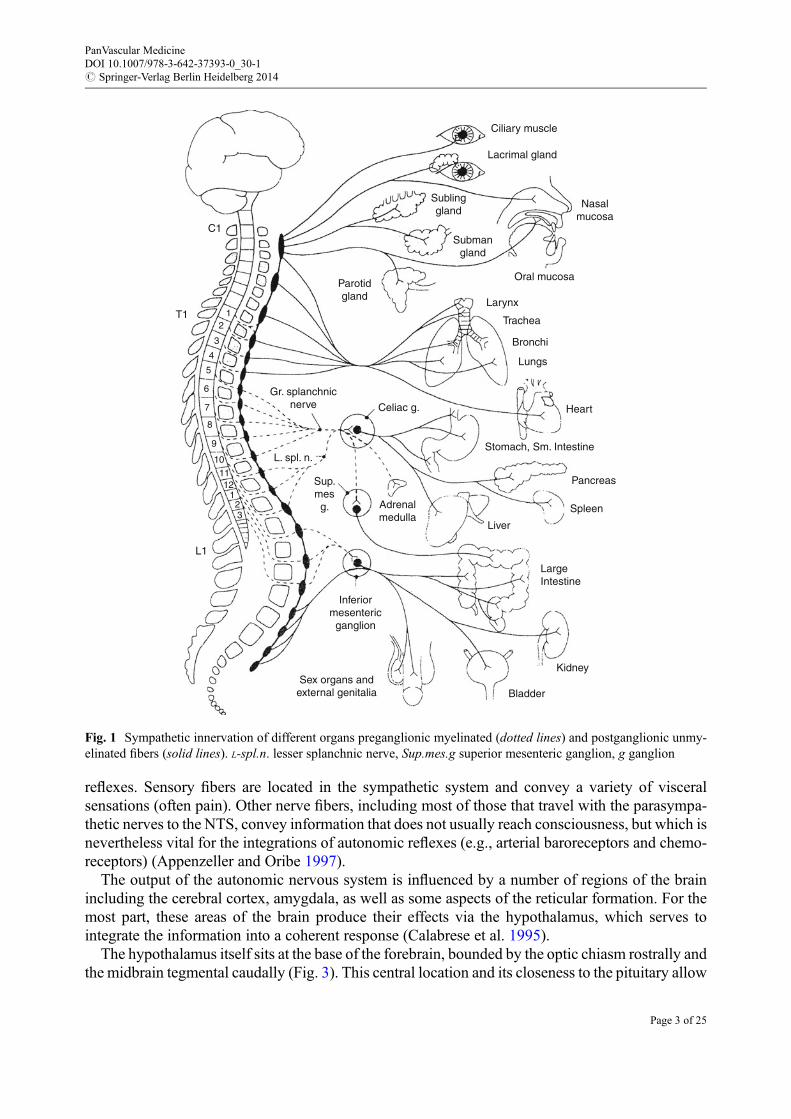
The nervous system has traditionally been divided into central and peripheral components. Thecentral nervous system is made up of the brain (comprised of the cerebrum, cerebellum, and brainstem) and the spinal cord. The peripheral nervous system includes sensory neurons (whichconnected the brain and spinal cord to sensory receptors) as well as motor neurons (which connectthe brain and spinal cord to muscles and glands). The elements of the peripheral nervous system thatare devoted to motor functions are further divided into somatic and autonomic components(Calabrese et al. 1995). The somatic component innervates the skeletal muscles, while the auto-nomic component innervates various smooth muscles, cardiac muscle, and glands. The autonomicnervous system (the very term autonomic means “self-regulating”) controls involuntary (visceral)functions and has three principal parts: sympathetic, parasympathetic, and enteric (Bennarroch1997). The sympathetic and parasympathetic divisions consist of two-neuron chains that connectthe central nervous system with the smooth muscles and glands of the viscera, blood vessels, andskin (Figs. 1 and 2). The enteric division is, for the most part, an independent system that lies withinthe walls of the gastrointestinal tract and controls many digestive functions. The sympathetic systemorganizes the involuntary responses that anticipate periods of maximum exertion (in its ultimateform, this is the so-called fight or flight response). Conversely, the parasympathetic nervous systemcontrols the involuntary responses that reflect visceral function in a state of relaxation (Cannonreferred to this as “rest and digest”). The sympathetic and parasympathetic ganglia (accumulationsof nerve cell bodies and supporting cells) are innervated by preganglionic neurons in the spinal cord.The sympathetic preganglionic axons arise from neurons in the thoracic and upper lumbar spinalcord. The preganglionic neurons that innervate the head and the organs of the thorax lie in the upperand middle thoracic segments, while those that innervate the abdominal and pelvic organs arelocated in the lower thoracic and upper lumbar segments. The parasympathetic preganglionic axonsarise from the neurons in the brain stem and sacral spinal cord.
Sensory inputs from the viscera and blood vessels modulate autonomic activity (Loewy and Spyer1990). As with other sensory neurons, the principal cell bodies sit in the dorsal root and cranial nerveganglia. The visceral sensory nerves that enter the spinal cord principally terminate in the interme-diate gray matter, close to the preganglionic neurons of the thoracolumbar and sacral cord areas. Theneurons that enter the brain stem directly via the cranial nerves VII, IX, and X terminate in the areaknown as the nucleus tractus solitarii (NTS), which integrates a number of important autonomic
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 2 of 25
reflexes. Sensory fibers are located in the sympathetic system and convey a variety of visceralsensations (often pain). Other nerve fibers, including most of those that travel with the parasympa-thetic nerves to the NTS, convey information that does not usually reach consciousness, but which isnevertheless vital for the integrations of autonomic reflexes (e.g., arterial baroreceptors and chemo-receptors) (Appenzeller and Oribe 1997).
The output of the autonomic nervous system is influenced by a number of regions of the brainincluding the cerebral cortex, amygdala, as well as some aspects of the reticular formation. For themost part, these areas of the brain produce their effects via the hypothalamus, which serves tointegrate the information into a coherent response (Calabrese et al. 1995).
The hypothalamus itself sits at the base of the forebrain, bounded by the optic chiasm rostrally andthe midbrain tegmental caudally (Fig. 3). This central location and its closeness to the pituitary allow
Ciliary muscle
Lacrimal gland
Sublinggland
Parotidgland
Gr. splanchnicnerve
Sup.mes
g. Adrenalmedulla
Inferiormesenteric
ganglion
Sex organs andexternal genitalia
L1
T1
C1
12
3
4
5
6
7
8
9
101112
123
Celiac g.
L. spl. n.
Submangland
Nasalmucosa
Oral mucosa
Bronchi
Heart
Stomach, Sm. Intestine
LargeIntestine
Kidney
Bladder
Liver
Spleen
Pancreas
Lungs
Trachea
Larynx
Fig. 1 Sympathetic innervation of different organs preganglionic myelinated (dotted lines) and postganglionic unmy-elinated fibers (solid lines). L-spl.n. lesser splanchnic nerve, Sup.mes.g superior mesenteric ganglion, g ganglion
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 3 of 25

it to integrate information from the forebrain, brain stem, spinal cord, and various endocrinesystems. The hypothalamus itself is made up of a number of discrete nuclei, each of which has itsown complex pattern of unique connections and functions (Fig. 4). These nuclei are grouped intothree distant longitudinal regions referred to as the periventricular, lateral, and medial zones. Theneurons of the periventricular nucleus project into the brain stem and spinal cord, where theyinnervate preganglionic autonomic neurons. The periventricular zone also contains an area referredto as the suprachiasmatic nucleus, which has a direct retinal input and seems to determine circadianrhythms (both visceral and behavioral) (Purvis 1997; Appenzeller and Oribe 1997).
Ciliary muscle
Lacrimal gland
Sublinggland
Pterygopal.g.
VII
III
Sex organs andexternal genitalia
S2-4
Distal colon
Abdominalvessels
Proximalcolon
Parotidgland
Otic g.
Submang.
Gallbladder, liver
1
2
3
4
5
6
7
8
9
1011
121
23
Ciliary g.
Submangland
Nasalmucosa
Oralmucosa
Bronchi
HeartStomach,Sm. Intestine
Vagus (X)
Kidney
ProstateBladder
Spleen
Pancreas
Lungs
Trachea
Larynx X
IX
Fig. 2 Parasympathetic innervation of different organs (craniosacral outflow). Dotted lines denote preganglionicmyelinated nerve fibers, and solid lines denote short unmyelinated fibers
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 4 of 25

The hypothalamus regulates autonomic nervous system activity by modulating visceral reflexinput that is principally organized at the level of the brain stem (Robertsen and Polinsky 1996). Itdoes this in two distinct manners (Loewy and Spyer 1990). Firstly, it sends projections into threevital areas of the brain stem and spinal cord. These include hypothalamic projections to the NTS,which is the major site of sensory input from the viscera. This area then acts on the nucleus of thevagus nerve as well as other parasympathetic neurons in the brain stem which control heart rate,blood pressure, and respiration. The hypothalamus also sends projections to the brain stem regionknown as the rostral ventral medulla, which controls the preganglionic output vital for sympatheticfunction. Stimulation of the lateral hypothalamus (which connects to the rostral ventral medulla)causes general sympathetic activation: sweating, blood pressure and heart rate increases,piloerection, and dilation of the pupils. The hypothalamus also sends projections directly to the
CorpusCallosum
CingulateGyrus
DorsalThalamus
Cerebellum
Nucleus TractusSolitarius
Spinal Cord
AnteriorCommissure
Hypothalamus
Pituitary
Midbrain
Pons
Medulla
BrainStem
Fig. 3 Midsagittal view of the human brain
Column of the Fornix
Anterior Commissure
Paraventricular Nucleus
Medial Preoptic Nucleus
Lateral Preoptic Nucleus
SuprachiasmaticNucleus
SupraopticNucleus
Arcuate Nucleus
Ventromedial Nucleus
Infundibulan Stalk
Anterior Pituitary
Posterior Pituitary
Anterior HypothalamicNucleus
Posterior HypothalamicArea
Mammillary Body
Ventral Tegmental Area
Lateral Hypothalamic Area
Dorsomedial HypothalamicNucleus
Mammillothalamic Tract
Fig. 4 The human hypothalamus, showing some of the nuclei in its medial (periventricular) zone
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 5 of 25

autonomic outflow areas of the spinal cord. Secondly, the hypothalamus operates directly on theendocrine system to release hormones that influence autonomic function.
A number of neurotransmitter substances have been found to participate in these regulatoryprocesses. Indeed, at least 20 neurotransmitters have been identified and include glutamate,y-aminobutyric acid (GABA), glycerin, noradrenaline, adrenaline, dopamine, serotonin,substance P, encephalin, oxytocin, vasopressin, as well as numerous other neuropeptides and purines(many of which have been colocalized) (Shepherd 1994).
Since the discovery of serotonin (5-hydroxytryptamine, or 5-HT), a tremendous amount has beenlearned about its role in cardiovascular regulation (Grubb and Karas 1998). Alterations in thedynamics of the brain serotonin biosynthesis can lead to changes in cardiovascular function.Activation of cerebral serotonin receptors produces pressor effects in some species, but producesdepressor effects in primates and humans. Several investigators have suggested that the ability of thebrain serotonin to regulate arterial blood pressure is mediated via serotonergic neural systems andtheir effect on efferent sympathetic activity. Recent animal studies have shown that the reduction insympathetic outflow that occurs as a consequence of increasing brain serotonin levels may protectthe heart against ventricular fibrillation, and its decline may contribute to the increased rates ofsudden death seen in post-myocardial infarction patients who suffer from clinical depression (Grubband Karas 1998).
Maintenance of Postural Normotension
While the assumption of upright posture represented one of the defining moments in the history ofhuman evolution, it also presented a unique challenge to a pressure control system that hadpreviously developed to meet the needs of animals that had spent their lives in a dorsal position(Greenfield 1997). Indeed, the brain, the very organ that defines our humanity, was placed in a fairlyprecarious position in respect to vascular perfusion and oxygenation. The autonomic nervous systemserves as the principal means for both long- and short-term responses to positional change. In thenormal human subject lying supine, approximately 25–30 % of the circulating blood volume residesin the thorax (Weiling and Van Lieshout 1993). Upon assuming upright posture, there is animmediate downward displacement of roughly 300–800 ml of blood to the abdomen and dependentextremities (Thompson et al. 1988). This represents a decline in volume of between 26 % and 30 %,with up to half of this fall occurring within the first few minutes of standing (Shepherd and Sheperd1992). Nearly 25 % of the body’s total blood volume may be involved in this process. This suddenredistribution in central blood volume produces a reduction in venous return to the heart. Since theheart cannot pumpwhat it does not receive, the stroke volume falls approximately 40% as a result ofthe decrease in cardiac filling pressure (Hainsworth 1996). The reference point around which thesechanges are determined is termed the venous hydrostatic indifference point (HIP) and represents thesite within the vascular system where pressure is independent of postural position (Weiling and VanLieshout 1993). In humans, the venous HIP is around the diaphragmatic level, whereas the arterialHIP is near the level of the left ventricle. This venous HIP is dynamic in nature and is influenced bythe degree of vascular compliance, as well as intravascular volume, and can be altered by factorssuch as muscular activity (Shepherd and Yanhoutte 1945). During standing, contractions of the legmuscles in conjunction with the venous valve system work to pump the blood back to the heart andthereby move the venous HIP closer to the level of the right atrium (Hainsworth 1990).
Respiratory activity may also result in an increase in venous return (Weiling and Van Lieshout1993). During deep inspiration, there is a drop in thoracic pressure that leads to an increase in inward
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 6 of 25

flow of blood. At the same time, respiration produces an increase in abdominal pressure that reducesretrograde flow due to compression of the iliac and femoral veins. Respiration may also contribute toan increase in venous return. During deep inspiration, there is a reduction in thoracic pressure whichmakes the inward flow of blood easier. Simultaneous with respiration, there is a rise in intra-abdominal pressure that decreases retrograde flow as a result of compression of both the iliac andfemoral veins.
Working at the same time as the aforementioned changes, assumption of upright posture causesa significant increase in the transmural capillary pressure in the dependent area of the body, resultingin an increase in fluid filtration into the tissue spaces (Streeten 1987). This shift in transcapillarypressure reaches a state of equilibration after approximately 30 min of upright posture. This processcan cause a net fall in plasma volume of up to 10 %.
The process of successfully maintaining upright posture requires initiation of several cardiovas-cular regulating systems in order to preserve a constant level of arterial pressure (and cerebralperfusion) against the force of gravity (Weiling and Van Lieshout 1993). Orthostatic stabilizationoccurs over about 1 min (or less). Investigations have demonstrated that the exact circulatoryresponses brought on standing (which is an active process) differ somewhat from those that occurduring head upright tilt (a passive process). Research done byWeiling and van Lieshout has definedthree phases of the orthostatic response (Weiling and Van Lieshout 1993). These include the initialresponse (which occurs during the first 30 s), the early “steady-state” alteration (at 1–2 min), andlastly the prolonged orthostatic period (after at least 5 min upright) (Hainsworth 1996).
Almost immediately after head upright tilt, cardiac stroke volume remains fairly normal despitethe fall in venous return, possibly due to the blood left in the pulmonary circulation (Weiling and VanLieshout 1993). After this, there is a slow decline in both arterial pressure and cardiac fillingpressure. This causes activation of two separate groups of pressure receptors composed of high-pressure receptors in the aortic arch and carotid sinus areas as well as low-pressure receptors in theheart and lungs (Jacobsen 1993). Inside the heart, mechanoreceptors subserved by unmyelinatedvagal afferents exist in all four cardiac chambers. These mechanoreceptors serve to produce a tonicinhibitory action on the cardiovascular areas of the medulla (most notably on the NTS) (Andresenand Kunze 1994). Baroreceptive neurons of the nucleus ambiguus and dorsal vagal nucleus, inhibitsympathoexcitatory neurons of the rostral ventrolateral medulla (Dampney 1994). The reducedvenous return and drop in filling pressure that occurs with upright posture reduces the stretch onthese receptors. Their firing rates decrease which results in a change in medullary input, producingan increase in sympathetic outflow (Appenzeller and Oribe 1997). This results in constriction of thesystemic resistance vessels as well as the splanchnic capacitance vessels. Also, there is a local axonreflex (the venoarteriolar axon reflex) that can also constrict flow to the skin, muscle, and adiposetissue that can contribute up to 50 % of the increase in limb vascular resistance seen during uprightposture (Streeten 1987).
During head upright tilt, there is also activation of the high-pressure receptor sites located in thecarotid sinus. The carotid sinus contains a group of baroreceptors and nerve endings that areprincipally situated in the enlarged area of the internal carotid artery, slightly after its origin fromthe common carotid artery (Appenzell 1997). The mechanoreceptor cells are found in the adventitiaof the arterial wall. The afferent impulses generated by local stretch on the arterial wall are thentransmitted through the sensory fibers of the carotid sinus nerve that runs with fibers of theglossopharyngeal nerve. These afferent pathways travel to the NTS of the medulla, close to thearea of the ambiguous and dorsal nuclei (Dampney 1994). The initial rise in heart rate seen during tiltis felt to be modulated by a decline in carotid artery pressure. The slow increase in diastolic pressure
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 7 of 25

that is observed following upright tilt is believed to be more closely related to a progressive increasein peripheral vascular resistance (Tseng and Tung 1995).
The initial circulatory adjustments that are seen during standing are somewhat different to thoseobserved during tilt (Hainsworth 1996). Standing is much more of an active process which isaccompanied by contractions of the muscles of the legs and abdomen, resulting in compression ofboth the capacitance and resistance vessels and a subsequent elevation of peripheral vascularresistance (Weiling and Van Lieshout 1993). This increase is enough to produce a transient increasein both right atrial pressure and cardiac output, which then causes an activation of the low-pressurereceptor of the heart. This produces an increase in neural traffic to the brain, causing a suddendecrease in peripheral vascular resistance (falling as much as 40%). This process can allow for fall inmean arterial pressure of up to 20 mmHg lasting for up to 6–8 s (Joyner and Shephard 1993). Thisfall in pressure is then compensated for by the same mechanism seen during upright tilt (Shepherdand Sheperd 1992).
The initial steady-state adjustments to upright posture involve an increase in heart rate ofapproximately 10–15 beats per minute, an increase in diastolic pressure of around 10 mmHg, andlittle or no change in systolic pressure (Talman 1993). At this point in time, compared to the supineposition, the blood volume of the thorax has declined by around 30 %, the total cardiac outputdeclines by 30 %, and the average heart rate is approximately 10–15 beats/min higher (Randall andBrown 1994).
Continued upright posture also activates a series of neurohumoral responses, the exact degree ofwhich are dependent on the subject’s volume status. The greater the degree of volume depletion, thegreater the degree of activation of renin-angiotensin-aldosterone system, as well as vasopressin(DiBona and Wilcox 1992). However, one of the most important factors in the body’s ability tocompensate for continued orthostatic stress is the influence of the arterial baroreceptors (particularlyof the carotid sinus) on peripheral vascular resistance (Joyner and Shephard 1993). The failure ofany one of these factors to operate adequately (or in a coordinated fashion) may result in an inabilityof the system to compensate for initial or prolonged orthostatic challenge (Wieling and Lieshout1993). This, in turn, could lead to a state of hypotension which, if sufficiently profound, couldproduce cerebral hypoperfusion and subsequent loss of consciousness.
Conditions Resulting from Disturbed Orthostatic Control
Avariety of different disturbances of normal orthostatic control have been elaborated. While similarin many ways, each disorder has its own unique features. Before continuing, it is valuable to recallthat when we observe nature, we see what we wish to see in accordance with what we know about itat the time. In the not too distant past, supraventricular tachycardia was felt to be a single entity andonly later was it found to be composed of multiple different subtypes. In order to make sense of theapparent chaos of nature, we attempt to classify it into some sort of coherent system that conforms toour observations and expectations. Therefore, any system of classification is in many ways arbitrary,subject to debate, and a continuing process of refinement. The following system follows that wasdeveloped by the American Autonomic Society, the basic outline of which is presented in Fig. 5(Consensus Committee of the American Autonomic Society and the American Academy of Neu-rology 1996). In some sense, all autonomic disorders may be thought of as primary of secondary innature. The primary forms are idiopathic and can be further subclassified into acute and chronicforms. Secondary autonomic disorders are those that are seen in association with another diseaseprocess or are felt to occur secondary to a known biochemical or structural abnormality. What
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 8 of 25

follows will be a brief description of each subtype, along with references for the reader seekinga more in-depth discussion.
Primary Disorders of Autonomic Insufficiency
Reflex SyncopeMost physicians have some degree of familiarity with these disorders. Initially called vasovagalsyncope by Sir Thomas Lewis, this condition is better known today as neurocardiogenic syncope(Grubb 1998a).While quite varied in presentation, it occurs more commonly in younger patients andusually consists of a distinct prodrome (often a feeling of light-headedness, nausea, and diaphoresis)of varying duration, followed by an abrupt loss of consciousness. Recovery is usually rapid andseldom has postictal state. These syncopal episodes are felt to occur as a result of a “hypersensitive”autonomic system that seems to overrespond to a variety of different stimuli (Morillo et al. 1997).The most common of these stimuli is prolonged orthostatic stress, which is thought to increase theamount of peripheral venous pooling to a point where the venous return to the right ventricle falls tosuch an extent that it virtually collapses upon itself. This hypercontractile state appears to activatemechanoreceptors that normally discharge only during stretch (Benditt et al. 1996). This suddenincrease in nerve traffic to the medulla is felt to mimic the conditions seen in hypertension, thusprovoking an apparent “paradoxic” withdrawal of sympathetic activity with resultant hypotension,bradycardia, and ultimately syncope (Kosinski et al. 1995). However, it should be kept in mind thatother types of stimuli (such as epileptic discharges or strong emotion) can provoke nearly identicalresponses, suggesting that these people have an inherent susceptibility to these events (Sutton 1996).During head upright tilt table testing, these patients will experience a sudden abrupt drop in bloodpressure that is often followed by a fall in heart rate (on occasion to the point of asystole).
Sutton and Peterson have made the astute observation stating that there is a tremendous similaritybetween the hemodynamic responses seen during neurocardiogenic syncope and carotid sinushypersensitivity potentially representing different aspects of the same disorder (Sutton and Peterson1995). Indeed, many investigators feel that in a susceptible individual, sudden activation of a large
Fig. 5 Classification of disorders of autonomic control associated with orthostatic intolerance
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 9 of 25

number of mechanoreceptor from any site, i.e., bladder, rectum, esophagus, and lungs, may provokea similar response (Kosinski 1998). The interested reader is directed to more detailed discussionselsewhere (Grubb 1998a). The fact which appears to distinguish these disorders from the remainderof those discussed in this chapter is that between the intermittent periods of decomposition that resultin syncope, these patients complain of few, if any, other symptoms. Thus, their autonomic systemsseem to function in a relatively normal fashion despite their somewhat “hypersensitive” nature, asdistinct from other conditions where the systems seem to “fail.”
Chronic SyndromesThe average practitioner is more likely to encounter the chronic forms of autonomic insufficiencythan the acute varieties. The first modern description of chronic autonomic failure was made in 1925by Bradbury and Eggleston (Bradbury and Eggleston 1925). They used the term “idiopathicorthostatic hypotension” to describe the condition and reflect an apparent lack of other features.Since that time, however, it has become increasingly recognized that, in these patients, a state ofdiffuse autonomic insufficiency exists. Thus, there is not only orthostatic hypotension and syncopebut also disturbed bladder, bowel, sudomotor, thermoregulatory, and sexual function (Freeman1995). Currently, this disorder is known as pure autonomic failure (PAF) (Consensus Committeeof the American Autonomic Society and the American Academy of Neurology 1996). Although theetiology of this remains idiopathic, some have reported evidence of peripheral postganglionicneuronal degeneration in patients with PAF (Furlan 1995). The disorder seems to occur mostoften in older adults, but younger individuals (even children) may occasionally be affected(Grubb 1998b).
A second, more severe form of autonomic failure was reported by Shy and Drager in 1960 (Shyand Drager 1960). As opposed to PAF, these patients have not only severe orthostatic hypotension,but also progressive rectal and urinary incontinence, iris atrophy, external ocular palsy, loss ofsweating, rigidity, tremor, and impotence (Low and Bannister 1997). Distal muscle wasting andfasciculations may also occur in the advanced stages of the disorder. The American AutonomicSociety has termed this condition multiple system atrophy (MSA) to emphasize the complexmultisystem effects of the disorder and has further categorized it into three different subtypes(Mathias 1995). In the first group, patients demonstrate a motor tremor that is quite similar to thatseen in Parkinson’s disease (some refer to this group as having striatonigral degeneration on the basisof autopsy observations) (Fearnley and Lees 1990; Hughes et al. 1992). The second group ofpatients demonstrate prominent cerebellar and/or pyramidal symptoms (again, on the basis ofautopsy findings, some refer to this as the olivopontocerebellar atrophy/degeneration form)(Gilman and Quinn 1996). This group displays a combination of both the aforementioned typesand is referred to as “mixed” (Mathias 1995). Some patients with MSA will have many featuressuggestive of Parkinson’s disease (Low and Bannister 1997). A resent autopsy study reported thatbetween 7 % and 22 % of patients thought to have Parkinson’s disease during life demonstratedneuropathologic findings diagnostic for MSA (Fearnley and Lees 1990; Jellinger 1991). Theaverage age of onset of MSA is usually between the fifth and seventh decade of life, althoughthere are some unfortunate individuals who begin to have signs of the disorder in their late thirties(Grubb 1998b).
More recently, a new subgroup of autonomic disorders has been identified which is commonlyreferred to as the postural orthostatic tachycardia syndrome (POTS) (Grubb et al. 1997). Thisappears to be an early, milder form of autonomic insufficiency that is characterized by excessiveheart rates occurring while in the upright position. Two principal forms of the disorder have thus farbeen identified. The more common variety is termed the peripheral dysautonomic form (Low
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 10 of 25

et al. 1995). The hallmark of the syndrome is a persistent tachycardia while upright (which mayreach rates of 160 beats/min or higher) that is associated with complaints of palpitations, severefatigue, exercise intolerance, near syncope, dizziness, and light-headedness (Low et al. 1997a).Complaints of cognitive impairment and mild disturbances in vision are also common. Manypatients will report always feeling cold while at the same time unable to tolerate extreme heat.During head upright tilt table testing, they will display a sudden increase in heart rate>30 beats/minwithin the first 5 min or will achieve a maximum heart rate of 120 beats/min associated with onlya modest decline in blood pressure (Hoeldtke and Danis 1991).
The mechanism at work in this form of POTS appears to be a failure of the peripheral vasculatureto adequately vasoconstrict under stress. This inadequate vasoconstrictive response is then com-pensated for by an excessive increase in heart rate and inotropy. Several investigators have felt thatPOTS may be the earliest sign of autonomic dysfunction, and it is currently thought that some ofthese patients (approximately 10 %) will later progress to having pure autonomic failure (Schondorfand Low 1993).
The second form of POTS, termed the “B-hypersensitivity” or “central” form, has only recentlybeen identified and is inappropriate feedback mechanism that arises from above the level of thebaroreflex, such that while the initial heart rate responses to upright posture are adequate, the braindoes not know when to stop and heart rates continue to elevate. A number of patients with this formof POTS will display “orthostatic hypertension” in addition to postural tachycardia. Although theclinical presentations of these two groups are similar, there is a tendency for the group to complainmore of tremor and migraine headaches. Serum catecholamine levels are quite high (serumnorepinephrine is often>600 ng/ml), and they demonstrate excessive heart rate responses to supineinfusion of intravenous isoproterenol infusion (30-beat/min increase in response to 1 mg/min) (Shyand Drager 1960).
Early on, investigators noted a decidedly familial tendency in these disorders, suggestinga possible genetic basis. This was recently confirmed when Robertson and colleagues isolated theexact genes responsible for this disorder in one family of severely affected patients. This defectivegene appears to code for a norepinephrine transporter substance that allows for excessive serumlevels (Shannon et al. 2000). Most investigators feel that there are probable multiple genetic forms ofthe disorder; however, these investigations are still in progress.
Recently, attention has been given to the fact that some patents with POTS may be misdiagnosedas having chronic fatigue syndrome, and there may be a considerable overlap between the twodisorders (Grubb et al. 2006). It is important to differentiate between the two because POTS patientswill often improve with therapy aimed at autonomic modulation, whereas chronic fatigue patientsoften do not (Bou-Holaigh et al. 1995).
Acute Autonomic Dysfunction
While these syndromes are thankfully uncommon, the acute autonomic neuropathies that result inhypotension and bradycardia are quite dramatic in presentation (Grubb and Kosinski 1997a). Acuteautonomic dysfunction is quite sudden in onset and is manifested by severe and widespread failureof both the sympathetic and parasympathetic systems while sparing the somatic fibers (Grubb1998b). Patients are often young and were quite healthy prior to the illness. The onset of symptomsis quite rapid, and patients can frequently report the exact day the illness began. A large percentageof these patients will relate having suffered a febrile illness (presumed to be viral) just prior to the
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 11 of 25

onset of symptoms, suggesting to some that there may be an autoimmune component to the disorder(Low and McLeod 1997).
Sympathetic nervous system function is usually so severely disrupted that there is profound ortho-static hypotension present, preventing the patient from sitting up in bedwithout passing out (AppenzellerandKornfeld 1973). Complete loss of ability to sweat is common, as are severe disruptions in bowel andbladder function (Grubb and Kosinski 1997a). Patients commonly report symptoms of bloating, nausea,abdominal pain, and vomiting. Constipation is frequent andmay alternate with periods of diarrhea (Low1983). One interesting observation has been that the heart rate in these patients may become fixed atbetween 45 and 55 beats/min and be associated with complete chronotropic incompetence. The patient’spupils may become quite dilated and be poorly responsive to light. As was alluded to previously,orthostatic hypotension is severe and patients may experience several syncopal episodes daily (Yahr andFrontera 1975). The clinical picture is quite similar to Guillain-Barre syndrome, except that respiration isnot affected. The long-term prognosis of these patients varies widely, with many experiencing near-complete recoveries and others suffering a chronic debilitating course. Some patients may be left withsignificant residual defects (Low and McLeod 1997).
Secondary Causes of Autonomic Insufficiency
There are a significant number of different disorders which may disturb normal autonomic function.A partial list of these disorders is offered in Table 1. It is of paramount importance that the physicianrecognize when a disturbance in normal autonomic function is part of a more general disease process.In some patients, more than one problem may combine to produce a synergistic disruption inautonomic balance. Several uncommon, yet nonetheless important enzymatic abnormalities havebeen discovered which can produce states of autonomic insufficiency (Robertson 1995). The mostimportant of these has been isolated dopamine b-hydroxylase deficiency syndrome, a disease whichcan now be easily treated with replacement therapy. Other deficiency syndromes affecting autonomicfunction include those associated with nerve growth factor, aromatic L-amino acid decarboxylase,monoamine oxidase, and other sensory neuropeptides (Robertsen and Polinsky 1996).
Systemic illnesses with multiple organ involvement such as cancer, renal failure, diabetesmellitus, autoimmune disorders, amyloidosis, and acquired immune deficiency syndrome may alldisturb autonomic function sufficiently to allow severe hypotension and syncope to occur (Grubb1998b). Recently, a link has been made between neurodegenerative disorders (such as Alzheimer’sdisease) and orthostatic hypotension (Passant et al. 1996).
One of the most important things to keep in mind when seeing a patient with any form ofautonomic insufficiency is the large number of pharmacologic agents that may either cause orexacerbate orthostatic hypotension (Table 2). All of these are peripherally acting vasodilatory agentssuch as the angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, hydralazine,guanethidine, and prazosin. Although therapeutic in some patients, beta-blockers may worsensyncope in others. Recently, we have become increasingly aware of growing numbers of patientswith congestive heart failure experiencing dysautonomic syncope (Ferguson and Mark 1994). It iswell recognized that heart failure is accompanied by significant alterations in autonomic function. Itseems that, in these patients, the combination of low cardiac output, volume depletion due todiuretics, vasodilator therapy, and beta-blockage all serve to impede the previously discussedmechanisms the body uses to adapt to upright posture, which then predisposes them to periods oforthostatic intolerance.
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 12 of 25

Clinical Characteristics
The principal characteristic shared by all these disorders is a disturbance in cardiovascular regulationto such a degree that postural hypotension and/or tachycardia can occur. In the past, orthostatichypotension was defined as a >20 mmHg fall in blood pressure over a 3-min period after standing.However, a less profound fall in blood pressure associated with symptoms can be just as important.Many patients will demonstrate a gradual progressive fall in blood pressure over a somewhat longer
Table 1 Autonomic disorders associated with orthostatic intolerance
I. Primary autonomic disorders
(1) Acute pandysautonomia
(2) Pure autonomic failure
(3) Multiple system atrophy
(a) Parkinsonian
(b) Pyramidal/cerebellar
(c) Mixed
(4) Reflex syncope
(a) Neurocardiogenic syncope
(b) Carotid sinus hypersensitivity
II. Secondary autonomic failure
(1) Central origin
(a) Cerebral cancer
(b) Multiple sclerosis
(c) Age related
(d) Syringobulbia
(2) Peripheral forms
(a) Afferent
– Guillain-Barre syndrome
– Tabes dorsalis
– Holmes-Adie syndrome
(b) Efferent
– Diabetes mellitus
– Nerve growth factor deficiency
– Dopamine beta-hydroxylase deficiency
(c) Afferent/efferent
– Familial dysautonomia
(d) Spinal origin
– Transverse myelitis
– Syringomyelia
– Spinal tumors
(e) Other causes
– Renal failure
– Paraneoplastic syndromes
– Autoimmune/collagen vascular disease
– Human immunodeficiency virus infection
– Amyloidosis
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 13 of 25

period of time (approximately 10–15 min) that will elicit symptoms (Low and Bannister 1997). Thepresence and severity of symptoms is dependent on the rate of fall in blood pressure and on theabsolute amount of change. The loss of consciousness in orthostatic or “dysautonomic” syncope isusually slow and gradual and typically occurs when the patient is standing or walking. Interestingly,a number of older patients do not appear to perceive this fall in blood pressure and will report theseepisodes as “drop attacks” (Sutton 1996). These individuals who do perceive symptoms reportfeelings of blurred vision, dizziness, tunnel vision, and “seeing stars.” One difference betweenneurocardiogenic and dysautonomic syncope is that the latter is usually associated with diaphoresisand bradycardia. Dysautonomic syncope tends to be more frequent during the early morning hours.Any situation that tends to favor peripheral venous pooling (fatigue, extreme heat, alcohol) mayexacerbate hypotension. Over time, some patients will demonstrate a fairly fixed heart rate(approximately 50–70 beats/min) associated with significant orthostatic intolerance. A commonproblem that is seen in diabetics and a number of older patients is a combination of supinehypertension and upright hypotension. This presumably occurs due to a failure of the autonomicsystem to compensate for any change in position (i.e., failure to vasoconstrict when upright and tovasodilate when prone) (Low and Bannister 1997). Patients suffering from this hyper- and hypo-tension can be challenging to treat. On occasion, it can be difficult to distinguish between the variousautonomic disorders as there can be a significant amount of overlap between them (similar to theproblems encountered with the subtypes of chronic obstructive pulmonary disease) (Fig. 6).
Diagnostic Evaluations
The single most important aspect of evaluation is a detailed history and comprehensive physicalexamination. When did symptoms begin? Is syncope the main problem or near syncope? When doepisodes occur and what makes themworse? Is there any pattern to the episodes? How do bystandersdescribe the patient during episodes? What other organ systems appear disturbed? A careful andthorough history and physical examination will have a much higher diagnostic yield than theindiscriminate ordering of multiple laboratory tests. Rather, diagnostic laboratory examination
Table 2 Pharmacologic agents that may cause or worsen orthostatic intolerance
Angiotensin-converting enzyme inhibitors
Alpha-receptor blockers
Calcium channel blockers
Beta-blockers
Phenothiazines
Tricyclic antidepressants
Bromocriptine
Ethanol
Opiates
Diuretics
Hydralazine
Ganglionic blocking agents
Nitrates
Sildenafil citrate
Monoamine oxidase inhibitors
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 14 of 25

should be selected in a careful and directed manner to confirm the diagnosis suggested by history andphysical examination.
It is beyond the scope of this chapter to discuss every autonomic disorder and the variouslaboratory test used in their evaluation. The reader desiring more information is directed to severalexcellent texts on the subject (Appenzeller and Oribe 1997; Robertsen and Polinsky 1996; Mathiasand Bannister 1999; Low 1997; Grubb and Olshansky 1998; Robertson and Biaggioni 1995).During evaluation of a patient, it is extremely important to identify any drugs that could potentiallycause hypotension (see Table 2). This includes not only prescription and over-the-counter pharma-ceuticals but also herbal remedies. One must also consider the possibility of illicit drug use oralcohol abuse that the patient may not admit to unless directly asked. Many women will report thatsymptoms worsen around the time of their menstrual cycles and may also worsen around the time ofmenopause.
As the autonomic areas of the brain are not easily accessible to direct measurement, the autonomicfunction is measured by noting the responses of different organ systems to a number of differentpharmacologic or physiologic challenges. More recently, it has become possible to determine urine,serum, and cerebrospinal fluid levels of a variety of neurotransmitter substances. However, thesimplest and most important determination is that of heart rate and blood pressure in the supine,sitting, and standing positions. Measurement should also be made after 3 and then 5 min upright.Blood pressure determinations should be performed with the arm extended horizontally (to avoidany possible hydrostatic effect of the fluid column of the arm). Since the body’s response to activestanding differs from that of passive tilt, we often perform tilt table testing of patients. There is anextensive literature available on the methodology and of tilt table testing, and the interested reader isdirected to these sources (Grubb and Kosinski 1997b). Other autonomic function tests are availableand can provide useful information in selected patients; the details are available elsewhere (Mathiasand Bannister 1999; Low 1997; Grubb and Olshansky 1998; Robertson and Biaggioni 1995).
Briefly, however, some concepts of tilt table testing will be reviewed. Tilt table testing is based onthe idea that a potent orthostatic stimulus, such as prolonged upright posture, could be employed tocause a significant amount of venous polling to occur, thereby provoking the aforementionedresponses in susceptible individuals. As opposed to standing, being strapped to a table capable ofinclining to between 60� and 80� for the most part inhibits the skeletal muscle pump which makesthe autonomic system function on its own. Thus, deprived of part of the compensatory system that anaffected individual has come to depend on, abnormal responses are more likely to be seen. Several
ReflexSyncope
PureAutonomic
Failure
MultipleSystemAtrophy
PosturalOrthostaticTachycardiaSyndrome
Fig. 6 The overlap between various autonomic disorders associated with orthostatic intolerance
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 15 of 25

observations have supported the concept that an abnormal tilt table test is for the most part equivalentto spontaneous events (Sutton and Peterson 1995). First among these observations is that bothspontaneous and tilt-induced episodes of syncope resulted in a prodrome of nausea, light-headedness, pallor, diaphoresis, and the loss of postural tone. Secondly, the temporal sequence ofheart rate and blood pressure changes are for the most part the same as those found duringspontaneous episodes. The serum catecholamine changes that were discussed previously areidentical to those in spontaneous and tilt-induced syncope, with both demonstrating rapid surgesin plasma epinephrine preceding loss of consciousness. Lastly, tilt table testing has been able toreproduce spontaneously observed periods of asystole in patients with negative electrophysiologicstudy.
Two basic methods of tilt table testing have evolved, both of which are simple, safe, andinexpensive (Grubb 1998a). The first uses a passive tilt for a period of 45 min at an angle of between60� and 80� (most centers now use 70�). No productive pharmacologic agents are used. The secondmethod often uses a shorter tilt duration time in association with a variety of different provocativeagents such as isoproterenol, nitroglycerin, and adenosine. Detailed discussions of these agents arebeyond the scope of this chapter and the interested reader is directed elsewhere (Grubb and Kosinski1997b).
At our institution, we use a two-stage tilt table protocol. Studies are usually done in the morningfollowing an overnight fast, and an intravenous line is then established. After a rest period of10–15 min, the patient is positioned on a tilt table with footboard support and inclines to an angle of70� for 30 min (Fig. 7). Heart rate and rhythm are monitored continuously via a defibrillator monitorand blood pressures are taken by sphygmomanometer every 3 min. Cardiopulmonary resuscitationequipment is present, as are a registered nurse and a physician. If symptomatic hypotension andbradycardia (or tachycardia) occur, reproducing the patient’s symptoms, the patients is then loweredto the supine position and the test concluded. If this initial phase of the test is unremarkable, then thepatient is lowered to the supine position and an intravenous infusion of isoproterenol is started. Thedose is then titrated to increase the heart rate to 20–25% above the initial supine value. Upright tilt is
Fig. 7 Head upright tilt table testing
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 16 of 25

then performed as previously described for 15min. Isoproterenol is not given to patients with knownsevere coronary artery disease or hypertrophic cardiomyopathy.
Abnormal response patterns can be grouped into five broad types (see Fig. 8). The first of thesepatterns is the classic neurocardiogenic (vasovagal) response, characterized by a fairly abrupt fall inblood pressure (with or without concomitant bradycardia) (Fig. 9). The second pattern, which wehave chosen to call “dysautonomic,” is characterized by a gradual decline in both systolic anddiastolic blood pressure that ultimately culminate in a loss of consciousness. The latter is morecommonly seen in the autonomic failure syndromes. The third pattern, a postural orthostatictachycardia response, is characterized by a greater than 30-beat/min increase in the first 5–10 minof upright tilt or by achieving a heart rate of�120 beats/min during the same time period. The fourthpattern has been called “cerebral syncope.” The response of the cerebrovasculature during neurocar-diogenic syncope has been extensively investigated using transcranial Doppler ultrasonography.These studies have shown that during tilt-induced neurocardiogenic syncope, cerebral arteriolarvasoconstriction occurs concomitant with (or occasionally is preceded by) the onset of hypotensionand loss of consciousness. Recently, several investigators have reported cases of tilt-inducedsyncope due to cerebral vasoconstriction alone (as observed by transcranial Doppler) in the absenceof systemic hypotension. The last response pattern is called a psychogenic or psychosomaticresponse. In these patients, syncope occurs during tilt in the absence of any identifiable change inheart rate, blood pressure, transcranial blood flow, or encephalographic pattern. These individualsare frequently found to suffer from severe psychiatric disorders that can range from conversionreactions to anxiety disorders to major depression. It is important to remember that patients sufferingfrom conversion reactions are not consciously aware of their actions. A large number of youngpeople (especially young women) with psychogenic syncope were found to be the victims of sexualabuse. Syncope in an abused child or adolescent may be a “cry for help.” Their cries should not fallupon deaf ears.
Therapeutic Modalities
A detailed description of all potential therapies for autonomic disorders is beyond the scope of thischapter; however, a brief review can be presented (more extensive discussions can be foundelsewhere) (Grubb 1998a; Furlan 1995). The first task is to determine whether the condition isprimary or secondary in nature and to identify any possible reversible causes (such as anemia, drugs,or volume depletion).
Abnormal Responses SeenDuring Tilt Table Testing
neurocardiogenic POTS dysautonomic psychogenicsyncope
cerebralsyncope
Fig. 8 Abnormal responses seen during table testing
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 17 of 25

It is equally important to educate the patient and family as to the nature of the disorder. Patientsshould be advised to avoid conditions that could exacerbate the condition, such as alcohol,dehydration, and extreme heat. Patients are encouraged to increase their fluid (and in some casessalt) intake and recognize any potential warning signs of impending episode and assume a supineposition.
Nonpharmacologic therapies should be encouraged. Moderate aerobic and isometric exercise ishelpful in maximizing venous return from the skeletal muscle pump. Some groups have found tilttraining helpful in neurocardiogenic syncope. Sleeping with the head of the bed upright (6–12 in. isuseful in the autonomic failure syndromes, as are elastic support hose that provide at least 30 mmHgankle counterpressure. Biofeedback therapy is useful in neurocardiogenic syncope, especially whenpsychological stimuli trigger episodes (McGrady et al. 1997).
Fig. 9 Blood pressure (BP) and heart rate (HR) patterns observed in abnormal responses to tilt table testing
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 18 of 25

Any pharmacotherapy should be used carefully and should be selected to fit the needs of eachpatient with respect to the type of disorder being treated, as well as any concomitant conditions orother medications the patient may be using. Keep in mind that any drug used to treat autonomicdisorders may, on occasion, worsen symptoms (a “pro-syncopal” effect).
One of the most commonly used agents for neurocardiogenic syncope is beta-blockers (Grubb1998a). These are presumed to work due to their negative inotropic actions on the heart, which isthought to lessen the degree of mechanoreceptor activation during periods of decreased venousreturn. Beta-blockers also increase peripheral vascular resistance by allowing unopposed alpha-receptor stimulations. A very useful agent in treating patients is fludrocortisone (Low and Bannister1997). This mineral corticoid agent expands fluid volume and also increases peripheral alpha-receptor sensitivity (thus promoting vasoconstriction). Care must be taken since the drug maycause hypokalemia and hypomagnesemia. Desmopressin may also be useful in selected patients.
Avariety of different vasoconstrictive substances can be used. Methylphenidate has been reportedto be effective due to its peripheral alpha-receptor-stimulating effects (Grubb et al. 1996). However,central nervous system stimulation and the potential for abuse limit its use. The related agentmidodrine offers the same degree of vasoconstriction without any central nervous system stimula-tion and has been demonstrated to be effective in both neurocardiogenic syncope and orthostatichypotension (Low et al. 1997b; Sra et al. 1997; Robertson and Davis 1995; Ward et al. 1998; Grubbet al. 1999). Yohimbine, ephedrine, and theophylline have also been employed (Grubb 1998a).
The alpha-receptor-altering agent clonidine has been shown to cause a paradoxic elevation inblood pressure in dysautonomic patients who have several postganglionic sympathetic lesions. Inthese patients, the vascular postjunctional alpha-2 receptor density (distributed widely in thevascular system) increases markedly and becomes hypersensitive (Robertsen and Polinsky 1996).While in normal subjects clonidine causes the sympathetic system to lower its output and therebylower blood pressure, in some patients with autonomic failure, they have little or no peripheralsympathetic stimulation, thus allowing its peripheral vasoconstrictive actions to be expressed. Thedrug must be used carefully as it may worsen hypotension.
For some time, it was noted that many patients with autonomic failure may also beanemic. Hoedtke and Streeten were the first to report that erythropoietin administered by subcuta-neous injection produced dramatic elevations in blood pressure while at the same time raising bloodcounts (Hoeldtke and Streeton 1993). Later studies have shown that these effects are independentand that erythropoietin has direct vasoconstrictive effects (Grubb and Kosinski 1994). As mentionedpreviously, there is a body of evidence demonstrating that serotonin plays an important role in thecentral nervous system regulation of heart rate and blood pressure (Grubb and Kosinski 1996). Insome autonomic disturbances, especially neurocardiogenic syncope, there appears to bea disturbance in serotonin production and receptor density. Serotonin reuptake inhibitors (such asfluoxetine and paroxetine) have been demonstrated to be remarkably effective in treating neurocar-diogenic syncope and may also be effective in treating other autonomic disturbances (Grubbet al. 1993; DiGirolamo et al. 1999).
The mesenteric vasoconstrictor octreotide has also proven useful in the treatment of refractoryorthostatic hypotension and POTS.
Permanent pacemaker placement may be a useful therapy in patients suffering from recurrentdrug-resistant neurocardiogenic syncope (NCS) who have a prominent bradycardic or asystoliccomponent (Benditt et al. 1995). The recent ISSUE 3 trial demonstrated a marked reduction insyncopal frequency with permanent pacing in patients whose syncope was associated with asystoleas documented by an implantable loop recorder (ILR) (Brignole et al. 2012). We often use ILRs toidentify this subgroup of patients who are most likely to benefit from pacing. Pacing systems that can
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 19 of 25

sense blood pressure changes and respond to the initial drop in blood pressure often seen in NCSappear to be superior to standard pacing systems.
The physician should remember that in the autonomic failure syndromes (as opposed to the reflexsyncopes), hypotension is but one aspect of a much broader group of symptoms relating toautonomic dysfunction. The physician should keep in mind that some symptoms are easier totreat than others and avoid giving the patient unrealistic expectations. Both physician and patientshould also keep in mind that these disorders are chronic in nature and, in some cases, mayprogressively worsen over time. Thus, therapies may have to be periodically altered to meet thepatient’s changing needs. It is also important to realize that patients suffering from severe forms ofautonomic disturbance have a wide variety of secondary social and personal difficulties, includingoccupational, psychological, marital, legal, and often financial problems. Many physicians feel ill atease addressing these matters, yet it is often these issues that have the greatest impact on the patients’lives. The physician should assist in helping the patient gain access to social workers, psychologists,rehabilitation specialists, and legal council when necessary.
The attitude of the physician toward the patient with a severe autonomic disorder is of paramountimportance. A positive (yet realistic) approach by a well-versed and sympathetic caregiver hasa tremendous impact on the patient. Hope is a potent medicine that should be fostered.
Summary
The autonomic nervous system is both complex and diffuse and involved in virtually every organsystem and most disease processes. Disturbances in this system are diverse in presentation, yetfrequently present with complaints of syncope and near syncope. A basic understanding of thesedisorders is necessary for their recognition and management. Ongoing investigations will continueto help better define the broad spectrum of this group of disorders while at the same time identifybetter diagnostic and therapeutic modalities.
References
Andresen MC, Kunze DL (1994) Nucleus tractus solitarius: gateway to neural circulatory control.Annu Rev Physiol 56:93–116
Appenzell O (1997) Neurogenic control of the circulation. In: Appenzeller O, Oribe E (eds) Theautonomic nervous system: an introduction to basic and clinical concepts. Elsevier, Amsterdam,pp 65–90
Appenzeller O, Kornfeld M (1973) Acute pandysautonomia: clinical and morphologic study. ArchNeurol 29:334–339
Appenzeller O, Oribe E (eds) (1997) The autonomic nervous system: an introduction to basic andclinical concepts. Elsevier, Amsterdam
Benditt DG, Petersen ME, Luriek KG et al (1995) Cardiac pacing for prevention of recurrentvasovagal syncope. Ann Intern Med 122:204–209
Benditt DG, Lurie K, Adler S, Sakagucki S, Shulti P (1996) Pathophysiology of vasovagal syncope.In: Blancc JJ, Benditt DG, Sutton R (eds) Neurally mediated syncope: pathophysiology, inves-tigations and treatment. Futura, Armonk, pp 1–24
Bennarroch E (1997) Central autonomic network: functional organization and clinical correlations.Futura, Armonk
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 20 of 25

Bou-Holaigh I, Rowe P, Kan J, Calkins H (1995) The relationship between neutrally medicatedhypotension and chronic fatigue syndrome. JAMA 274:961–967
Bradbury S, Eggleston C (1925) Postural hypotension: a report of three cases. Am Heart J 1:73–86Brignole M, Menozzi C, Moya A et al (2012) Pacemaker therapy in patients with neurally mediated
syncope and documented asystole. Circulation 125:2566–2571Calabrese R, Gordon T, Hawkins R, Qian N (1995) Essentials of neural science and behavior.
Appleton and Lange, NorwalkConsensus Committee of the American Autonomic Society and the American Academy of Neurol-
ogy (1996) Consensus statement on the definition of the orthostatic hypotension, pure autonomicfailure and multiple system atrophy. Neurology 46:1470–1471
Dampney RA (1994) Functional organization of central pathways regulating the cardiovascularsystem. Physiol Rev 74:323–364
DiBona GF, Wilcox CS (1992) The kidney and the sympathetic nervous system. In: Bannister R,Mathias C (eds) Autonomic failure. Oxford Medical Publications, Oxford, pp 178–196
DiGirolamo E, Iorio CD, Sabatini P, Lenzio L, Barbone C, Barsotti A (1999) Effects on paroxetinehydrochloride, a selective serotonin, on refractory vasovagal syncope: a randomized, double-blind, placebo-controlled study. J Am Coll Cardiol 33:1227–1230
Fearnley TM, Lees AJ (1990) Striatonigral degeneration: a clinicopathologic study. Brain113:1823–1842
Ferguson D, Mark A (1994) Clinical neurocardiology: role of the autonomic nervous system inclinical heart failure. In: Armour J, Ardell T (eds) Neurocardiology. Oxford University Press,Oxford, pp 397–424
Freeman R (1995) Pure autonomic failure. In: Robertson D, Biaggioni I (eds) Disorders of theautonomic nervous system. Harwood Academic, Luxembourg, pp 83–106
Furlan R (1995) Pure autonomic failure: complex abnormalities in the neural mechanisms regulatingthe cardiovascular system. J Auton Nerv Syst 51:223–235
Gilman S, Quinn NP (1996) The relationship of multiple system atrophy to sporadic olivoponto-cerebellar atrophy and other forms of idiopathic late onset cerebellar atrophy. Neurology46:1197–1199
Greenfield S (1997) The human brain. Phoenix-Orion Books, London, pp 135–138Grubb BP (1998a) Neurocardiogenic syncope. In: Grubb BP, Olshansky B (eds) Syncope: mech-
anisms and management. Futura, Armonk, pp 73–106Grubb BP (1998b) Dysautonomic syncope. In: Grubb BP, Olshansky B (eds) Syncope: mechanisms
and management. Futura, Armonk, pp 107–126Grubb BP, Karas B (1998) The potential role of serotonin in the pathogenesis of neurocardiogenic
syncope and related autonomic disorders. J Interv Card Electrophysiol 2:325–332Grubb BP, Kosinski D (1994) Erythropoietin as a therapy for severe refractory orthostatic hypoten-
sion. Clin Auton Res 4:212Grubb BP, Kosinski D (1996) Serotonin and syncope: an emerging connection? Eur J Card Pacing
Electrophysiol 5:3063–3314Grubb BP, Kosinski D (1997a) Acute pandysautonomic syncope. Eur J Card Pacing Electrophysiol
7:10–14Grubb BP, Kosinski D (1997b) Tilt table testing: concepts and limitations. PACE 20(part
II):781–787Grubb BP, Olshansky B (eds) (1998) Syncope: mechanisms and management. Futura, ArmonkGrubb BP, Samoil D, Kosinski D et al (1993) Fluoxetine hydrochloride for the treatment of severe
refractory orthostatic hypotension. PACE 16:801–805
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 21 of 25

Grubb BP, Kosinski D, Mouhaffel A, Pothoulakis A (1996) The use of methylphenidate in thetreatment of refractory neurocardiogenic syncope. PACE 19:836–840
Grubb BP, Kosinski D, Boehm K, Kip K (1997) The postural orthostatic tachycardia syndrome:a neurocardiogenic variant identified during head up tilt table testing. PACE 20:2205–2212
Grubb BP, Karas B, Kosinski D, Boehm K (1999) Preliminary observations on the use of midodrinehydrochloride in the treatment of refractory neurocardiogenic syncope. J Interv CardElectrophysiol 3:139–143
Grubb BP, Kanjwal Y, Kosinski D (2006) The postural tachycardia syndrome: a concise guide todiagnosis and management. J Cardiovasc Electrophysiol 17:108–112
Hainsworth R (1990) The importance of vascular capacitance in cardiovascular control. Newsphysiol Sci 5:250–254
Hainsworth R (1996) Physiology and pathophysiology of syncope. In: Kenny R (ed) Syncope in theolder patient. Chapman and Hall Medical Publishers, London, pp 15–31
Hoeldtke RD, Danis KM (1991) The orthostatic tachycardia syndrome: evaluation of autonomicfunction. J Clin Endocrinol Metab 73:132–139
Hoeldtke RD, Streeton DH (1993) Treatment of orthostatic hypotension with erythropoietin. N EnglJ Med 329:611–615
Hughes AJ, Daniel DE, Kilford L, Lees AJ (1992) Accuracy of clinical diagnosis of idiopathicParkinson’s disease: a clinic ¼ pathological study of 100 cases. J Neurol Neurosurg Psychiatry55:181–184
Jacobsen TN (1993) Relative contributions of cardiopulmonary and sinoaortic baroreflexes incausing sympathetic activation in human skeletal muscle circulation during orthostatic stress.Circ Res 73:367–378
Jellinger K (1991) Pathology of Parkinson’s disease: changes other than the nigrostriatal pathway.Mol Chem Neuropathol 14:153–197
Joyner MJ, Shephard JT (1993) Autonomic control of the circulation. In: Low P (ed) Clinicalautonomic disorders, 1st edn. Little Brown, Boston, pp 55–67
Kosinski D (1998) Miscellaneous causes of syncope. In: Grubb BP, Olshansky B (eds) Syncope:mechanisms and management. Futura, Armonk, pp 297–304
Kosinski D, Grubb BP, Temesy-Armos P (1995) Pathophysiological aspects of neurocardiogenicsyncope. PACE 18:716–721
Loewy A, Spyer K (eds) (1990) Central regulation of autonomic functions. Oxford University Press,Oxford
Low PA (1983) Acute panautonomic neuropathy. Ann Neurol 13:412–417Low P (ed) (1997) Clinical autonomic disorders. Lippincott-Raven, BostonLow PA, Bannister R (1997) Multiple system atrophy and pure autonomic failure. In: Low
P (ed) Clinical autonomic disorders, 2nd edn. Lippincott-Raven, Philadelphia, pp 555–573Low P, McLeod J (1997) Autonomic neuropathies. In: Low P (ed) Clinical autonomic disorders.
Lippincott-Raven, Philadelphia, pp 463–486Low P, Opfer-Gehrking T, Textor S et al (1995) Postural tachycardia syndrome (POTS). Neurology
45:519–525Low PA, Novak V, Novak P, Sandroni P et al (1997a) Postural tachycardia syndrome. In: Low
P (ed) Clinical autonomic disorders. Lippincott-Raven, Philadelphia, pp 681–698Low P, Gilden J, Freeman R et al (1997b) Efficacy of midodrine vs placebo in neurocardiogenic
orthostatic hypotension. JAMA 277:1046–1051Mathias CJ (1995) The classification and nomenclature of autonomic disorders: ending chaos,
restoring conflict, and hopefully achieving clarity. Clin Auton Res 5:307–310
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 22 of 25

Mathias C, Bannister R (eds) (1999) Autonomic failure: a textbook of clinical disorders of theautonomic nervous system. Oxford Medical Publications, Oxford
McGrady A, Bush E, Grubb BP (1997) Outcome of biofeedback-assisted relaxation for neurocar-diogenic syncope and headache: a clinical replication series. Appl Psychophysiol Biofeedback22:63–72
Morillo CA, Ellenbagen KA, Pava F (1997) Pathophysiologic basis for vasodepressor syncope. In:Klein G (ed) Syncope: cardiology clinics of North America. Saunders, Philadelphia, pp 233–250
Passant U, Warkentin S, Karlson S et al (1996) Orthostatic hypotension in organic dementia:relationship between blood pressure, cortical blood flow, and symptoms. Clin Auton Res 6:29–36
Purvis D (ed) (1997) Neuroscience. Sinauer Associates, SunderlandRandall DC, Brown DR (1994) Autonomic nervous system control of cardiovascular function in the
awake animal. In: Armour JA, Ardell JL (eds) Neurocardiology. Oxford University Press, Oxford,pp 343–364
Robertsen D, Polinsky R (eds) (1996) A primer on the autonomic nervous system. Academic, SanDiego
Robertson D (1995) Genetic disorders of the autonomic nervous system. In: Robertson D, BiaggioniI (eds) Disorders of the autonomic nervous system. Harwood Academic, Luxembourg,pp 197–216
Robertson D, Biaggioni I (eds) (1995) Disorders of the autonomic nervous system. HarwoodAcademic, Luxembourg
Robertson D, Davis TL (1995) Recent advances in the treatment of orthostatic hypotension.Neurology 5:526–532
Schondorf R, Low P (1993) Idiopathic postural orthostatic tachycardia syndrome: an attenuatedform of pandysautonomia? Neurology 43:132–137
Shannon J, Flattem B, Jordan T, Jacob G, Black B, Biaggioni I, Blakely R, Robertson D (2000)Orthostatic intolerance and tachycardia associated with norepinephrine-transporter deficiency.N Engl J Med 342:541–549
Shepherd G (1994) Neurobiology. Oxford University Press, OxfordShepherd JT, Sheperd RFJ (1992) Control of the blood pressure and circulation in man. In:
Bannister R, Mathias C (eds) Autonomic failure: a textbook of clinical disorders of the autonomicnervous system. Oxford Medical Publishers, Oxford, pp 78–93
Shepherd JT, Yanhoutte PM (1945) Veins and their control. Saunders, Philadelphia, pp 171–180Shy GM, Drager GA (1960) A neurologic syndrome associated with orthostatic hypotension. Arch
Neurol 3:511–527Sra J, Maglio C, Biehl M et al (1997) Efficacy of midodrine hydrochloride in neurocardiogenic
syncope refractory to standard therapy. J Cardiovasc Electrophysiol 8:42–46Streeten D (1987) Physiology of the microcirculation. In: Streeten D (ed) Orthostatic disorders of the
circulation. Plenum Medical, New York, pp 1–12Sutton R (1996) Vasovagal syncope: clinical features, epidemiology and natural history. In: Blanc
JJ, Denditt D, Sutton R (eds) Neurally mediated syncope: pathophysiology, investigations andtreatment. Futura, Armonk, pp 71–76
Sutton R, Peterson M (1995) The clinical spectrum of neurocardiogenic syncope. J CardiovascElectrophysiol 6:569–576
Talman W (1993) The central nervous system and cardiovascular control in health and disease. In:Low P (ed) Clinical autonomic disorders, 1st edn. Little Brown, Boston, pp 39–51
Thompson WO, Thompson PK, Daiey ME (1988) The effect of upright posture on the compositionand volume of the blood in man. J Clin Invest 5:573–609
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 23 of 25

Tseng CJ, Tung CS (1995) Brain stem and cardiovascular regulation. In: Robertson D, BiaggioniI (eds) Disorders of the autonomic nervous system. Harwood Academic, Luxembourg, pp 9–24
Ward CR, Gray JC, Gilroy JT, Kenny RM (1998) Midodrine: a role in the management ofneurocardiogenic syncope. Heart 79:45–49
Weiling W, Van Lieshout JJ (1993) Maintenance of postural normotension in humans. In: LowP (ed) Clinical autonomic disorders, 1st edn. Little Brown, Boston, pp 69–75
Wieling W, Lieshout J (1993) Maintenance of postural normotension in humans. In: LowP (ed) Clinical autonomic disorders. Little Brown, Boston, pp 69–73
Yahr MD, Frontera AT (1975) Acute autonomic neuropathy. Arch Neurol 32:132–133
Further ReadingKanjwal K, Karabin B, Kanjwal Y, Grubb BP (2010) Preliminary observations on the use of closed-
loop cardiac pacing in patients with refractory neurocardiogenic syncope. J Interv CardElectrophysiol 27:69–73
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 24 of 25

Index Terms:
Acute autonomic neuropathy 11Autonomic nervous system (ANS) 2Biofeedback 18Carotid sinus hypersensitivity 9Cerebral syncope 17Drop attacks 14Homeostasis 2Hypothalamus 5Mechanoreceptors 7, 9Multiple system atrophy (MSA) 10Neurocardiogenic syncope (NCS) 9, 19Orthostatic hypotension 10Postural orthostatic tachycardia syndrome (POTS) 11Serotonin 6, 19Vasovagal syncope 9
See Neurocardiogenic syncope (NCS)
PanVascular MedicineDOI 10.1007/978-3-642-37393-0_30-1# Springer-Verlag Berlin Heidelberg 2014
Page 25 of 25