nephrology grand rounds - nyu langone health · pdf file · 2014-08-13increased...
TRANSCRIPT

Nephrology Grand Rounds
Vasishta Tatapudi, MD March 26th, 2013.

History
• C/C: A 60 year old Chinese female patient with edema and 6.9g proteinuria in a 24 hour urine collection.
• HPI: Patient was seen in clinic 1 month prior to admission with c/o generalized fatigue, shortness of breath, occasional palpitations and lower extremity swelling for 3-4 months. Initial labs showed Microalb/Cr ratio of 6.7g/g, hypoabuminemia and elevated cholesterol levels. She returned to clinic 3 weeks later, 24 hour urine collection for protein was ordered. She was followed up one week later. EKG showing premature atrial complexes prompted transfer to ER.

Medical history: None. Surgical history: None. Medications: Lasix 40mg bid, crestor 10mg daily. Allergies: None.

• Health maintenance: Mammogram and pap smear in May 2012, both normal. Never had a colonoscopy.
• Family History: Father had heart disease. Sister had breast cancer at age of 60.
• Social History: Works as a receptionist and lives with her husband. No history of smoking, alcohol or drug use.

Review of Systems • Denied history of chest pain. • No history of cough, expectoration, wheezing, fever. • Never observed blood in urine or frothy urine. • Did not notice decreased urine output or a change in urinary habits. • No skin rash, oral ulcers, joint pain. • No changes in bowel habits, dark or bloody stool. • No decrease in appetite, night sweats or weight loss.

Physical Exam
General: Elderly female patient, lying in bed, 1 pillow, no distress. Vital signs: 98 F, HR 98, RR 16, BP 110/55. HEENT/Neck: No JVD, no lymphadenopathy. RS: CTA. CVS: S1, S2 normal, no added sounds. Abdomen: No distention, no organomegaly. CNS: No focal deficits. Normal reflexes. Extremities: Pitting edema upto b/l knees. Skin: No rash, purpura.

Laboratory Data
Hemoglobin 13.4 Sodium 134 Protein 5.6
Hematocrit 39.8 Potassium 2.9 Albumin 2.7
MCV 93.7 Chloride 90 ALT 25
White count 6.7 Bicarbonate 37 AST 61
Platelets 464 Blood urea 19 ALP 132
Eosinophils 0.4% Creatinine 0.9 Total Bili. 0.4
Glucose 87 Direct Bili. 0.1
Calcium 8.5
AG 7

Lipid Panel Urinalysis Tot. Chol. 586
LDL 493
HDL 25
Trig. 340
BNP 1220
Troponin 0.4980
Color Yellow Specific Gravity 1.010 pH 6.5 Glucose Negative Bilirubin Negative Ketones Negative Blood Negative Protein 3+ Leuk. Est. Negative Nitrite Negative RBC 2-3 WBC 0-2 Casts Negative Bacteria Negative
U. Prt. 150.5
U. Cr. 31.2
P/Cr 4.8g/g
Urine Protein/Creatinine

• EKG: normal sinus rhythm.
• Chest x-ray: clear lung fields, cardiomegaly, no mass.
• Echo: LA is severely dilated, myocardium of the LV is severely thickened, hyperdynamic LV wall motion and EF(75%). Myocardium of RV is thickened. No evidence of pulmonary hypertension.
• Renal U/S: Increased parenchymal echogenicity bilaterally. Upper normal sized kidneys, right-13, left 13.1. No hydronephrosis, calculi. Patent renal artery and veins.

Work-up
HbA1c 5.5 HIV rapid test
Negative
HBsAg Negative ANA Negative
HBsAb Negative C3 157(75-140)
HBcAb Negative C4 35(10-34)
HCV Ab Negative

Work-up
• SPEP: Marked hypoproteinemia, marked hypoalbuminemia, increased alpha 2 globulins and decreased gamma globulins.
• UPEP: Albumin and other proteins observed, compatible with non selective proteinuria.
• Serum IF: Faint band in Lambda is present against a dense polyclonal background.
• Urine IF: Free Kappa band present. Ig Levels Serum Free Light Chains IgG 484(694-1618)
IgA 246(81-463)
IgM 172(48-271)
Kappa 675(3.3-19.4)
Lambda 19(5.7-26.3)
K/L Ratio 34.1(0.3-1.65)

Work-up
• Skeletal Survey: No definite lytic or sclerotic osseous lesions or areas of erosion or aggressive appearing bone destruction are identified.

Differential Diagnosis
• Primary amyoidosis • Monoclonal immunoglobulin deposition disease Membranous nephropathy-primary/secondary FSGS-primary/secondary Minimal change disease Lupus Nephritis-Class V

Kidney Biopsy
Courtesy Dr. Ming Wu.

Primary Amyloidosis

Amyloid
• Rudolph Virchow used the term amyloid to describe ‘waxy eosinophilic’ tissue deposits, believed to be polysaccharide derivatives.
• Amylum is Latin for Starch. • In 1959, electron microscopic examination of ultrathin sections of
amyloidotic tissues revealed the presence of fibrils.
Glenner GG. N Engl J Med. 1980;302:1283-1292. Jean D. Sipe, Alan S. CohenVolume 130, Issues 2–3, June 2000,

Ultrastructure
Glenner GG. N Engl J Med. 1980;302:1283-1292.
Merlini, Bellotti, N Engl J Med 2003;349:583-96.

Cross β Pleated Sheet Structure of Filaments
Pauling, Proc Natl Acad Sci U S A. 1951 November; 37(11): 729–740.

Amyloidosis
• Amyloidosis is a generic term for a family of diseases defined by morphologic criteria.
• The diseases are characterized by the deposition in extracellular spaces of a proteinaceous material.
• Amyloidoses may be classified based on precursor proteins.
Ronco et al, Renal Amyloidosis, Comprehensive clinical nephrology.

Merlini, Bellotti, N Engl J Med 2003;349:583-96.

Apolipoprotein A1-Cardiac Amyloid
Merlini, Bellotti, N Engl J Med 2003;349:583-96.

Amyloidogenesis
Merlini, Bellotti, N Engl J Med 2003;349:583-96.

SAP Scintigraphy
Hazenberg et al, The American Journal of Medicine, Vol 119, No 4, April 2006

Monoclonal Ig Related Disease
• The glomerular capillaries are a favorite site for the deposition of abnormal proteins.
• Categorization based on electron microscopy. • Amyloidosis, cryoglobulinemic and immunotactoid
glomerulonephritis GN. • Monoclonal immunoglobulin deposition disease (MIDD).
Ronco et al, Renal Amyloidosis, Comprehensive clinical nephrology. Sanjeev, Sethi, N Engl J Med 2012;366:1119-31.
AL Amyloidosis
• Free immunoglobulin subunits, mostly light chains, secreted by a single clone of B cells, are the cause of the most frequent and severe amyloidosis affecting the kidney.
• In AL amyloidosis, there is a striking overrepresentation of the λ isotype, which is twofold to fourfold more frequent than the κ isotype.
• The incidence of AL amyloidosis is nine per million per year. • Fewer than one of four patients with AL amyloidosis is considered
to have an overt immunoproliferative disease.

Pathology-AL Amyloidosis
Diagnostic Atlas of Renal Pathology: A Companion to Brenner & Rector's The Kidney, 9th edition , Agnes B. Fogo. Ronco et al, Renal Amyloidosis, Comprehensive clinical nephrology.

Clinical Features
Merlini, Bellotti, N Engl J Med 2003;349:583-96.

Diagnosis
• Particular vigilance should be maintained in patients with multiple myeloma or monoclonal gammopathy of undetermined significance (MGUS), especially of the λ isotype.
• Biopsy of an affected organ is usually diagnostic, but less invasive alternatives should be preferred first.
• Indications to look for hereditary causes of Amyloidosis. • MGUS and Hereditary Amyloid may co-exist.

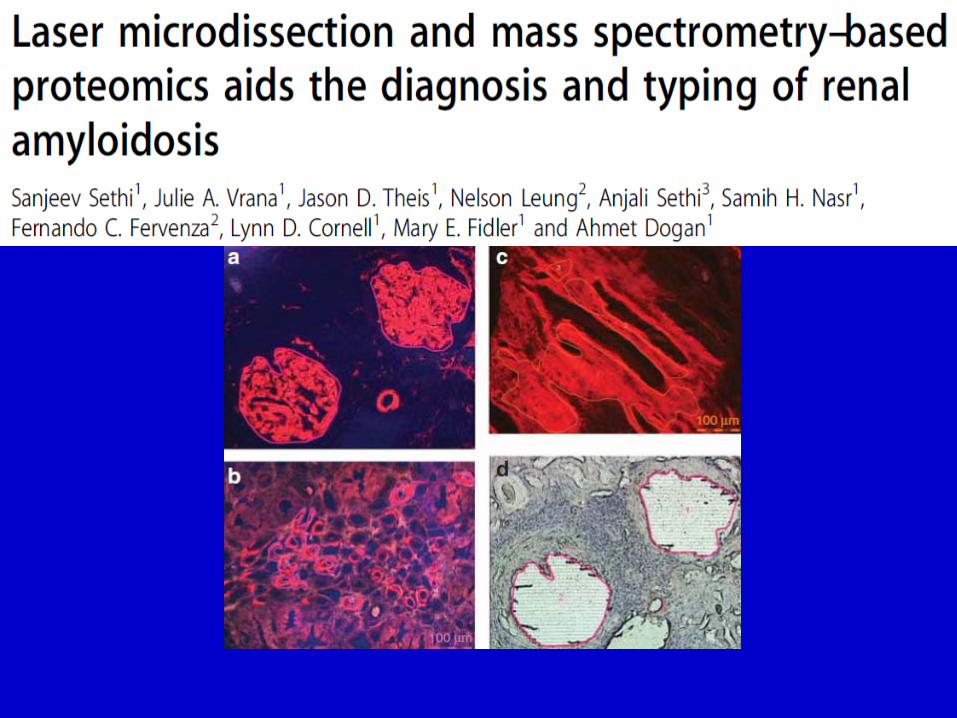
Proteomic Analysis
• Although renal biopsy can type AL and AA amyloidosis, some cases pose problems in accurate typing of amyloid, and ancillary tests including genetic analysis are often required.
• Accurate typing of amyloidosis has implications for prognosis, genetic counseling, and treatment.
• Laser microdissection (LMD) and tandem mass spectrometry (MS)–based proteomic analysis is a sensitive and specific tool for the diagnosis of amyloidosis.
Sanjeev Sethi et al, Kidney International (2012) 82, 226–234.

Treatment

• Goal: To demonstrate that high-dose melphalan would improve the survival rate compared to standard therapy. • Study Design: Multicenter, randomized, controlled trial. • Included 100 patients. • Treatment: Melphalan+Dexamethasone vs HDM+ASCT. • M/Dex: 10mg/m2+40mg/d x 4 days for 12 to 18 months. • HDM+ASCT: 200mg/m - day zero+ 2x106 CD34+ cells – day two. • Primary outcome: Overall survival.
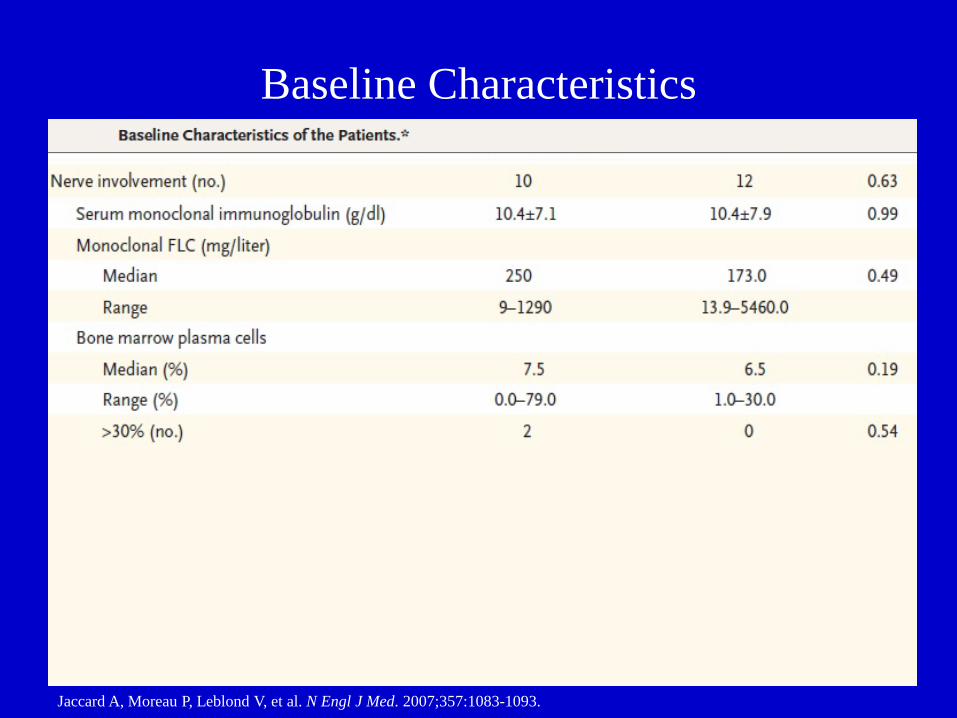
Baseline Characteristics
Jaccard A, Moreau P, Leblond V, et al. N Engl J Med. 2007;357:1083-1093.

Results
Jaccard A, Moreau P, Leblond V, et al. N Engl J Med. 2007;357:1083-1093.

Hematologic Response
Jaccard A, Moreau P, Leblond V, et al. N Engl J Med. 2007;357:1083-1093.
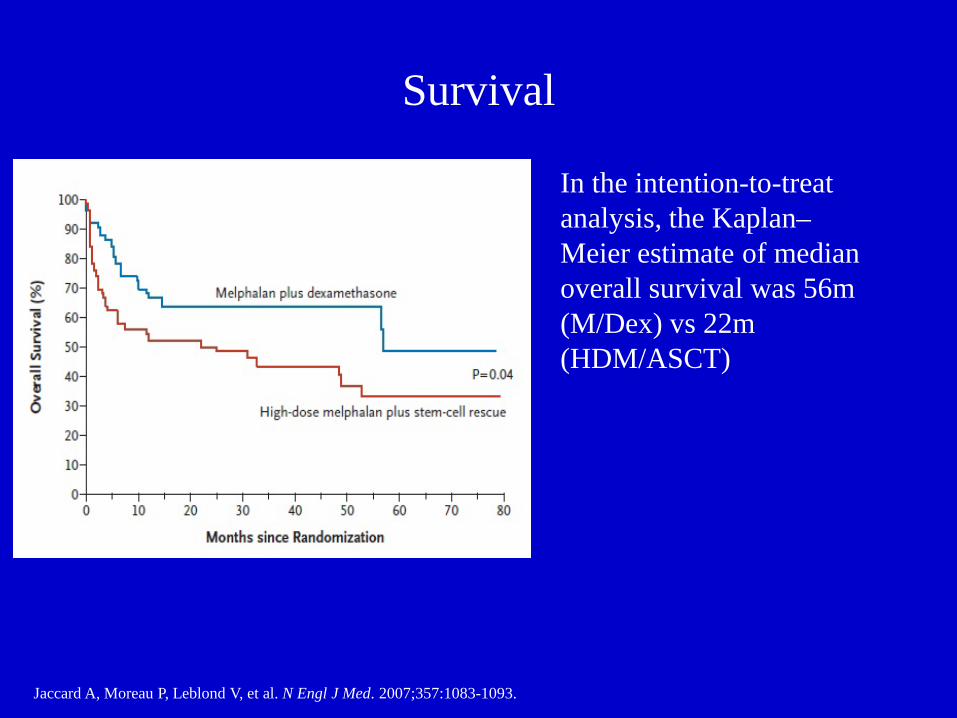
Survival
Jaccard A, Moreau P, Leblond V, et al. N Engl J Med. 2007;357:1083-1093.
In the intention-to-treat analysis, the Kaplan– Meier estimate of median overall survival was 56m (M/Dex) vs 22m (HDM/ASCT)

Conclusions of Study
• High-dose melphalan plus autologous stem-cell rescue was not superior to the outcome with standard-dose melphalan plus dexamethasone.
• Treatment-related mortality in the HDM group (24%) was higher than that reported in single-center studies from amyloidosis referral centers (4% to 14%).
• The high mortality was likely due to enrollment of patients who had severe organ dysfunction and would not be eligible for HDM/ASCT at many referral centers.
Jaccard A, Moreau P, Leblond V, et al. N Engl J Med. 2007;357:1083-1093.

Thank you.