neonatal physical therapy. part ii: practice frameworks ... physical therapy. part ii: practice...
TRANSCRIPT

S P E C I A L C O M M U N I C A T I O N
Neonatal Physical Therapy. Part II:Practice Frameworks andEvidence-Based Practice GuidelinesJane K. Sweeney, PT, PhD, PCS, FAPTA, Carolyn B. Heriza, PT, EdD, FAPTA, Yvette Blanchard, PT, ScD,and Stacey C. Dusing, PT, PhD
Doctoral Programs in Pediatric Science (J.K.S., C.B.H.), Rocky Mountain University of Health Professions, Provo, Utah;Pediatric Rehab Northwest, LLC (J.K.S.), Gig Harbor, Washington; Physical Therapy Program (Y.B.), University ofHartford, Hartford, Connecticut; and Department of Physical Therapy, Virginia Commonwealth University (S.C.D.),Richmond, Virginia
Purpose: (1) To outline frameworks for neonatal physical therapy based on 3 theoretical models, (2) todescribe emerging literature supporting neonatal physical therapy practice, and (3) to identify evidence-basedpractice recommendations. Key Points: Three models are presented as a framework for neonatal practice: (1)dynamic systems theory including synactive theory and the theory of neuronal group selection, (2) the Inter-national Classification of Functioning, Disability and Health, and (3) family-centered care. Literature is sum-marized to support neonatal physical therapists in the areas of examination, developmental care, interven-tion, and parent education. Practice recommendations are offered with levels of evidence identified.Conclusions: Neonatal physical therapy practice has a theoretical and evidence-based structure, and evidenceis emerging for selected clinical procedures. Continued research to expand the science of neonatal physicaltherapy is critical to elevate the evidence and support practice recommendations. (Pediatr Phys Ther 2010;22:2–16) Key words: clinical practice guidelines, evidence-based practice, high-risk infant, neonatal intensivecare units, neonatology, physical therapy, infant born preterm, reference standards/clinical
INTRODUCTION
Evidence-based practice guidelines are presented tosupport pediatric physical therapists (PTs) preparing forand practicing in the advanced subspecialty of neonatol-ogy. Theoretical frameworks, the emerging literature base,and evidence-based practice recommendations highlightthis second article of a 2-part series on neonatal physicaltherapy practice. In part I, neonatal physical therapy clin-ical competencies, neonatal intensive care unit (NICU)clinical training models, and a clinical decision-makingalgorithm were described.1 The series was developed by a
NICU Task Force of pediatric PTs with neonatal expertiseappointed by the Section on Pediatrics, American PhysicalTherapy Association, and reviewed by an expert panel ofneonatal practitioners representing diverse geographic re-gions of the United States.
PRACTICE FRAMEWORK
The NICU Practice Guidelines are based on 3 theoret-ical concepts: (1) dynamic systems theory (DST) of devel-opment; (2) the International Classification of Function-ing, Disability and Health (ICF); and (3) family-centeredcare. These concepts offer a theoretical structure for under-standing and organizing neonatal physical therapy andprovide a framework for optimizing functional movementand posture of infants to promote functional activities anddevelopment of the infant-family system.
Dynamic Systems
In the dynamic systems model, all system componentsinteract to produce meaningful, functional behavior.2 Mul-tiple interacting systems and environments influence neo-natal functional performance (Fig 1). In the NICU, dy-namic system components include the following:
0898-5669/110/2201-0002Pediatric Physical TherapyCopyright © 2010 Section on Pediatrics of the American PhysicalTherapy Association.
Address Correspondence to: Jane Sweeney, PT, PhD, PCS, FAPTA, 881430th Street, Ct NW, Gig Harbor, WA 98335. E-mail: [email protected] Support: Supported in part by the Section on Pediatrics, APTA, forwhich the authors served as members of the NICU Task Force.
DOI: 10.1097/PEP.0b013e3181cdba43
2 Sweeney et al Pediatric Physical Therapy

• The infant’s biological makeup (ie, physiologic,behavioral, physical, social, and psychologicalelements);
• The sociocultural (ie, professionals and family) andphysical environments in which neonatal move-ments and postural control develop; and
• The task or goal of the neonate, such as self-regulation of physiologic processes, behavioralstate, posture and movement, and attention to andinteraction with caregivers.3
Biological components of the infant do not act inde-pendently of each other or the physical and socioculturalenvironment in which a behavioral task is accomplished.For example, to conserve energy, the neonate needs toorganize sleep-wake periods. If the nursery environmenthas continuous 24-hour bright lighting or if the neonatesare awakened frequently during deep sleep, they may ex-perience difficulty organizing biological systems to pro-mote either sleep or alertness.
In a dynamic systems context, the need for functionrecruits and assembles the necessary and most availableelements to complete the movement for a task performedwithin the immediate environment.3,4 For example, an in-fant may bring a hand to the mouth to suck on the fingersto console and decrease stress. If the infant is in the supineposition and lacks strength to move against gravity, efforts tobring the hand to the mouth will not be successful. Repeatedattempts to accomplish the movement by pressing the headand trunk against a firm surface (ie, the mattress) may con-tribute to disruption of physiologic systems leading to apneaor bradycardia. If attempts are continued, with time, this mayresult in an excessively extended posture.
As illustrated in Figure 1, any system component the-oretically can facilitate or constrain an infant’s functional
movement and postural control. In the previous example,the supine position constrains the infant’s ability to be suc-cessful in the hand-to-mouth task. The interaction be-tween the environmental component and the infant’s neu-romuscular system prevents the functional activity ofengaging the hand in the mouth. A small change in onecomponent may produce a large change in movement andpostural control. By changing the infant’s position fromsupine position to a supported side-lying position, the in-fant may then explore and practice strategies for bringingthe hand to the mouth without the effects of gravity.
The infant’s attempts to initiate, practice, and learn amotor task (associative learning and memory) such as thehand-to-mouth maneuver, signal an optimal time for the neo-natal PT, and other caregivers to facilitate this movement.According to DST, periods of learning are periods of transi-tion. It is during these periods that the system(s) is mostresponsive to change, and motor learning can be optimized.4
Both the synactive theory of development5 and thetheory of neuronal group selection (TNGS)6 are examplesof dynamic systems models. These theories, described sep-arately below, combine to provide a behavioral organiza-tion and a neuronal framework applicable to neonatalphysical therapy practice.
Synactive Theory of Development. Als5,7 described abehavioral organization process of subsystem interactionand interdependence (synaction) as the neonate respondsto the challenges of the extrauterine environment. In thisdynamic systems model, physiologic stability is consideredas the foundation system for organizing movement, behav-ioral state, attention/interaction, and self-regulation.
Als8 highlighted the infant’s behavior as a continuousexpression of brain function available for observation by care-givers. Ongoing observations of infant behaviors at rest, dur-ing and after care procedures allow caregivers to interpret theinfant’s adaptation to the new extrauterine environment.These systematic observations are the base for the NewbornIndividualized Care and Development Program (NIDCAP)developed by Als9,10 and for her program of NIDCAP out-comes research on NICU developmental care.11–14
As shown in Figure 1, the neonatal PT can apply thismodel by observing infant communication through the (1)autonomic system (respiratory and heart rates, oxygen sat-uration, color, hiccoughs, sneezes, tremors, and startles),(2) musculoskeletal and neurologic systems (joint align-ment, body posture, tone, and movement), (3) state system(range, robustness, attention, transitions, and capacity toorient to animate and inanimate objects), and (4) self-regulation of state, motor, and autonomic systems.15,16 Bysupporting organization of the motor system, the neonataltherapist also supports organization of the autonomic,state, and self-regulation systems, freeing the infant to at-tend and interact with parents and with the environment.
It is imperative that neonatal PTs focus not only on thephysiologic and sensorimotor components of infant functionbut also on the maturation and organization of behavior inneonates. Three primary concepts guiding the clinical appli-cation of infant behavioral observation and providing a matrix
Fig. 1. Dynamic systems and interacting environments influenc-ing neonatal functional performance and interaction of theinfant-family system.
Pediatric Physical Therapy Neonatal PT Practice Guidelines: Part II 3

for understanding behavioral organization in a developmen-tal context16,17 are described in Table 1.
Behavioral observation must guide examination, in-tervention, and parent teaching in neonatal physical ther-apy. Infant behavioral organization concepts are the cor-nerstone for understanding infant readiness toparticipate and maintain stability in all neonatal therapycontacts. Facilitating and supporting infant behavioralorganization, reinforcing movement and postural com-ponents of infant self-regulation, and facilitating andsupporting mutual affective regulation between parentsand infants are priorities in neonatal therapy.16,17
Theory of Neuronal Group Selection. Edelman’s the-ory on how the nervous system becomes organized, storesinformation, and creates new behavioral patterns is identi-
fied as the TNGS.2,6,18–20 The theory is based on biologicalresearch and behavioral observations.21–23 A key concept ofthe theory is that the brain operates as a selective system. Inaddition, the brain is strongly affected by signals from thebody and the environment either during fetal developmentor development after birth.18 As a result, no 2 brains arealike, and each person’s brain is continually changing.
This theory has 3 main tenets2,19,20 for the develop-ment of the brain that are described in Table 2. Extensiveevidence in adult animal models and humans is now avail-able that the brain is a highly dynamic organ capable ofstructural and functional organization and reorganizationin response to a variety of internal and external pressures.This neural plasticity is the mechanism by which the brainencodes experience and learns new behaviors.24–27
TABLE 1Guiding Concepts for Clinical Use of Infant Behavioral Observation to Support Development in Infants at High Risk16,17
Concepts Description Developmental Context for Infant at High Risk
Infant competency ● Skills, abilities, predispositions uniquelysuited to meet survival and emotional needsof newborn infant in neonatal period
● Potential for similar competencies under specific conditions of on-goingand carefully matched support from caregivers
● Limited capacities for prolonged interactionsResponses often subtle and difficult to interpret
● Example: healthy newborn ● Example: infant at high riskHears and locates sounds Responds to sound but does not always locate its sourcePrefers mother’s voice Signs of distress subtle and include the following:Sends clear signals of distress when needssupport
PalenessLoss of muscle tone
Maintains prolonged periods ofinteractions with caregivers and parents
DrowsinessAlert for brief periodsDoes best when caregivers limit sensory input to one modality (eg,visual only, no auditory)
Behavioral states ● Predictable and unique behavioral patternscreating matrix against which infantresponses are understood
● Healthy newborn
● Behavioral states present but may not be fully developed based ongestational age
● Behavioral states less clear and difficult to identify with rapid transitionsand difficulty consoling
Behavioral states clear, robust, easy toidentify
● Require environmental and social adaptations and protection to supportemergence of behavioral states
Transitions from one behavioral state toanother smooth and gradual
● Example: healthy newborn ● Example: infant at high riskDrowsy infant not as socially responsive asquietly alert infant
May not reach alertness allowing social responsivenessMay appear to be sleeping when feedingMay best reach quiet alert state in quiet, dark room when swaddledand held
Crying infant tremor more than sleepinginfantBecome drowsy as transition from alert tosleep state
Self-regulation ● Infant’s ability to organize, regulate andmodulate autonomic, motor, and statesystems influencing caregivers’ choices tobest support development
● Ability to self-regulate limited and influenced by environmental andsocial demands
● Return to self-regulation costly in terms of energy expenditure anddevelopmental experiences
● Tasks of caregiversMinimize periods of loss of self-regulationFacilitate prolonged periods of self-regulation through well-timed,individualized, support to infant
● Example: healthy newborn ● Example: infant at high riskEasily accomplish tasks of Able to maintain regulated breathing
Pink color and tucked posture when swaddledLoss of stability when unwrapped or turned prone to supine positionwithout support
Stabilizing breathingReducing number of startles and tremorsMaintaining temperature controlFeeding successfully
4 Sweeney et al Pediatric Physical Therapy

Motor skill acquisition is associated with changes ingene expression, dendritic growth, synapse addition, andneuronal activity in the motor cortex and cerebellum(Fig 2).25–27 Practice of a newly learned behavior may berequired to induce lasting neural changes. Some forms ofplasticity therefore require not only the acquisition of askill but also the continued performance of that skillover time.26 It is hypothesized that plasticity broughtabout through practice represents the instantiation ofskill with neuronal circuitry making the acquired behav-ior resistant to decay in the absence of training.26,27
Infants born preterm enter the world with a centralnervous system that has had less time to mature within aprotected uterine environment. The external NICU envi-ronment involves respiratory support, physiologic moni-toring equipment, isolettes, absent postural containmentprovided by the uterus and amniotic fluid, aversive andpainful stimuli, separation from parents, irregular patternsof handling from multiple caregivers, and unfiltered noiseand light. Edelman6 hypothesized that when the brain is inunusual sensory circumstances, events of brain develop-ment are modified such as (1) preservation of cells that
TABLE 2Three Main Tenets of the Theory of Neuronal Group Selection2,6,18–23
Type of Selection Timing Processes of Development Outcomes
Developmental selection(yields primaryrepertoires)
Occurs during fetal life ● Constrained by genes and epigenetic events ofcell division, motion, and death anddependent on context and history
● Primary movement repertories containingpreexistent or innate movement patternshaving value for survival of the species
● Neurons branch in different directionscreating immense, variable and diverse neuralcircuits
● Neurons compete to make synapses● Synaptic connections weakened or
strengthened by experience, repetition andexploration in womb
● Examples:Kicking and steppingHand to mouthSucking (grasping breast or nipple withmouth for feeding)Grasping objects with handsKeeping interesting objects in sight
● Strengthened connections lead to selection ofprimary movement repertories having valuefor survival of the species
● Primary movement patterns not constraintsbut “prods” that start movement activity andself- organization process
Experiential selection(yields secondaryrepertories)
Overlaps early period ofprimary repertoiresand extendsthroughout life
● Postbirth, infant interacts with newenvironment
● Secondary movement repertories selectedthrough
● Experience drives change and synapticconnections weakened or strengthened
ExperienceExploration
● Synaptic connections strengthened byexperience, repetition, and exploration lead toselection of secondary repertories that satisfyenvironmental constraints and evolvedinternal value system and support successfuladaptive (goal directed) movements withintask constraints
Repetition● Selected secondary movement repertories
demonstrateFunctional variabilityAdaptive valueSuccessful in environmentLikely to be used in future
● Preferred adaptive movement patternsintegrate with subsequent motor learning andadaptation
● Process maintains plasticity continuingthroughout life
● Example:Experience of hand to mouth behaviorand sucking in utero continues to providebasic perception-action pattern for adaptingsucking to breast and bottle feeding
Reentrant mapping Occurs postnatally ● MapsLink secondary repertoires forming higherEither strengthened or weakened dependenton current and past experiencesorder globalmappingsEnsures linkage and integration of complexLink in different regions to form higher order,global mappings involving motor and sensorysystemsfunctions and behaviorsCoordinated in space and time throughongoing signaling across reciprocalconnectionsContinually modified during lifetime
● Neural maps in cortex selected throughcurrent and past experience
● Example: during early breast feeding, infant:Practices number of ways to suck andswallowPerceives movement of lips, jaw, tongue,and throat and tastes milkPerceives warmth of mother’s skin andhears her voiceEach somatosensory connection has itsown mapThrough repetition of sucking andswallowing, infant selects movementpattern most successful and perception-action system related to sucking andswallowing determined
Pediatric Physical Therapy Neonatal PT Practice Guidelines: Part II 5

otherwise would be eliminated, (2) elimination of cells thatotherwise would be preserved, (3) modification of den-dritic and axonal pruning events, and (4) changes in con-nectivity (synapses). Neuronal changes, such as these,were reported by Bourjeois et al29 in monkeys deliveredprematurely. The number of visual cortical cells was un-changed, but the synapses were significantly different insize, type, and laminar distribution, with the extent ofthese differences related to varying levels of prematurity.Neuronal changes were also reported by Als et al30 ininfants born preterm (28 –33 weeks) who received theNIDCAP program from 72 hours of NICU admission toage 2 weeks corrected for prematurity compared with acontrol group receiving standard care. Both groups wereassessed at corrected ages of 2 weeks and 9 months onhealth status, growth, and neurobehavior; brain neuro-structure (MRI) and neuroelectrophysiology (EEG) werecompared at the corrected age of 2 weeks. Results indicatedconsistently better neurobehavioral function at 2 weeks and 9months corrected age and more mature fiber structure in thecortex at 2 weeks corrected age for of infants receiving theNIDCAP program.
Neonatal PTs are responsible for nurturing braingrowth. Brain development depends on a complex inter-play between genes and environmental experiences.Early sensory information and motor experiences mayhave an effect on the architecture of the brain. Earlyinteractions not only create a context but also directlyaffect the way the brain is “wired.”31 Because each infanthas unique brain maturational levels at the time of birth,the same extrauterine environment and caregiving expe-riences may have different effects on brain structure.
Neonatal therapy examination and intervention strategiesshould therefore be carefully modulated and paced to protectthe architecture and maturation of the infant’s brain.
International Classification of Functioning,Disability and Health
The ICF is compatible with the dynamic systems modelof development and learning. The ICF model represents in-teractive, complex relationships between an individual’shealth and the contextual factors of the environment and theperson.32 This framework, adopted by the House of Delegates,American Physical Therapy Association, 200833 typifies PTpractice and provides a structure for understanding and orga-nizing practice. Within this framework, the neonatal therapistaddresses the (1) functional and structural integrity of thebody parts and systems, (2) promotion of age-appropriatepostural and movement activities, and (3) appropriate inter-action among the neonate, family, and professionals in theNICU. The neonatal therapist also considers impairments,activity limitations, and participation restrictions or changesin physical function or health resulting from injury, disease,or other causes.
Three components of function are (1) body and bodyparts, such as the ability of the neonate to control the physi-ologic function of breathing; (2) infant as a whole using themotor system to accomplish a task, such as bringing hands tothe mouth or grasping a caregiver’s finger; and (3) infant inthe NICU, home, and community environments performingsocial functions such as interacting with caregivers duringfeeding in the NICU, home, or daycare center (Fig 3).32 These3 components of function are essential to support the neo-nate’s physiologic, behavioral, physical, social, and psycho-logical well-being and to promote a meaningful life for theinfants and their families.
Three components of disease or active pathology, im-pairment, activity limitation, and participation restrictionresulting from injury, disease, or other causes are also de-picted in Figure 3. Impairment is a loss or abnormality of
Fig. 2. Neural events underlying motor map organization andreorganization and motor learning. Motor experience such ashand-to-mouth behavior induces a set of neural signaling path-ways that activates gene expression within the motor cortex,which precedes synapse formation which in turn precedes motormap reorganization leading to learned sucking behavior.24–27
Adapted with permission from Kleim.25 The picture of infant de-picting hand-to-mouth behavior is reprinted with permissionfrom VandenBerg et al.28
Fig. 3. International Classification of Functioning, Disability andHealth (ICF). Adapted with permission from the InternationalClassification of Functioning, Disability and Health.32
6 Sweeney et al Pediatric Physical Therapy

body structure or of a physiologic or psychological func-tion. Examples in the neonate include the inability to con-trol the physiologic systems resulting in apnea or restrictedjoint mobility contributing to decreased movement. Activ-ity limitation is a restriction of the ability to perform aphysical action, activity, or task in an efficient, typicallyexpected, or competent manner. In the neonate, activitylimitation may occur when the infant is unable to producethe antigravity, midline movement to bring hands to themouth for sucking, a strategy often used for self-regulation.Participation restriction is the inability to participate inage-specific or gender-related roles in a particular social orphysical environment. In the NICU, examples are feedingand attention/interaction activities such as auditory atten-tion and visual interaction with caregivers during feeding.
The 2 contextual factors in Figure 3 are environmen-tal (external influence on function) and personal (internalinfluence on function). Personal factors are the character-istics of the individual that are not part of a health condi-tion or health state.32,34,35 These factors influence the rela-tionships among body functions and structures, activities,and participation34 and can either constrain or promotefunction.
Examples of environmental factors in the NICU arelight and noise. Excessively high noise and light levels inthe NICU may impede the infant’s physiologic, motor, orbehavioral self-regulation; dimming the lights and decreas-ing the noise may promote physiologic, motor, or behav-ioral stability.
Examples of personal factors of infants born preterm aresensitivity or irritability to internal and external stressors (eg,pain, hunger, and handling) leading rapidly to overstimula-tion, agitation, or exhaustion, which may impede the infant’sability to self-calm or self-regulate the physiologic, motor, orstate systems. Swaddling or the flexed, tucked side-lying po-sition with the hands or fingers near the face and mouth maydecrease physiologic distress, improve motor organization,and increase self-regulatory behavior.
The scope of the ICF framework and emphases on con-text and function can guide neonatal therapists in visualizingthe complexity of the infant’s internal and external environ-ment and in anticipating how neonatal therapy procedureswill support or overload infant and family functioning.
Family-Centered Care
Collaborative partnerships with families and neonatalpractitioners are the cornerstone for caregiving success inneonatal physical therapy. Building parent and profes-sional partnerships and adapting the care and teaching tofamily priorities, learning styles, emotional stresses, andcultural variables are essential considerations for makinginterventions effective.36 Centering neonatal physical ther-apy care on family needs requires understanding andempathy for the complex stresses and losses parents areexperiencing as they cope with new roles as parents ofmedically fragile infants in the NICU environment. Al-though the NICU experience for parents may vary depend-
ing on the nature of the delivery, level of prematurity, andseverity of illness, their consistent focus is on the baby’ssurvival and developmental outcome. In addition, they aremourning the loss of the “imagined” or “wished for” babyas they struggle to develop a bond with their “real” ba-by.37,38 Emotional trauma relating to a preterm birth, un-expected financial stress on the family, and ongoing psy-chological stresses during parenting attempts in the NICUcontribute to the posttraumatic stress disorder reported inparents with infants requiring intensive care.39–41
Neonatal PTs can play an important role in alleviatingparent stress and anxiety and in helping parents interactwith their infant who may be medically fragile by learningto respond to the baby’s behavioral cues for signaling readi-ness to feed or engage in social interaction and to disengagefor a break. Helping parents understand and respond toinfant cues is considered critical to helping them maintaintheir roles as parents and mitigate levels of stress and de-pression.16,42–46 Developmentally appropriate interven-tions that focus on helping parents read infant cues,enhance parent-child interactions, and support the parent-child relationship are reported to improve developmentaloutcome and enhance the child’s cognitive and socioemo-tional development.47–51 Neonatal PTs have a responsibilityto individualize their approach and intervention strategiesto meet the unique needs of the infant and family withrespect to ensuring that family members acquire confi-dence and skill in movement and postural managementwith their infant related to holding, carrying, feeding, anddressing. The family is therefore a primary focus for collab-oration and support by the neonatal PT and for early inclu-sion in NICU developmental intervention and dischargeplans.
PHYSICAL THERAPY IN THE NICU: EVIDENCE FORPRACTICE
A key competency in providing care in any physicaltherapy setting is critical appraisal of relevant research andthe application of evidence to practice. In this section, anoverview of recent evidence is provided for the develop-mental and therapeutic interventions in the NICU settingwhere neonatal therapists may participate in a variety ofservice delivery approaches involving program develop-ment, consultation, and direct therapy services. Programdevelopment services may focus on recommendations foradvancing developmental care for all infants in the NICUwith policy and training implications. Consultative ser-vices may include making infant-specific recommenda-tions, which are updated at regular intervals, but the inter-vention is provided by the infant’s primary caregivers.Direct neonatal physical therapy services are provided toaddress an infant’s specific musculoskeletal, neuromuscu-lar, or neurobehavioral needs. Family education is an im-portant component of both consultative and direct therapyservices and includes discharge teaching for coordinationof follow-up through interdisciplinary clinics and localearly intervention programs. This literature overview and
Pediatric Physical Therapy Neonatal PT Practice Guidelines: Part II 7

evidence-based recommendations are intended for all ser-vice delivery models used by the PTs in NICU settings.
Examination
A range of tests and measures are available for exam-ination of neonates. Many instruments, potentially usefulin neonatal physical therapy practice for selected infants,are identified in the examination and evaluation compe-tency in Part I of the NICU Practice Guidelines.1 Criticalcomponents in the examination competency for neonatalPTs are (1) determining infant readiness to begin neuro-logic and neuromotor examination and (2) monitoring andmodifying changes in physiologic and behavioral stabilityduring and after examination procedures. Significantlygreater physiologic cost (increased heart rate and meanarterial pressure) and behavioral stress (increased fingersplay, arm salute, hiccoughs, yawns, and mottled skincolor) were demonstrated by neonates at 30 to 35 weekspost-conception compared with infants born at term dur-ing neurologic examination procedures administered by aneonatal PT. Greater physiologic and behavioral stress wasdemonstrated by both groups of neonates during the neu-romotor items compared with neurobehavioral items.52,53
Risk management considerations for presumed be-nign neurologic examination procedures are raised fromthis preliminary research. For infants born at less than 35weeks of gestation, the reliability, diagnostic benefit, andphysiologic cost of neurologic examination, especiallyneuromotor items, must be scrutinized, and infants withborderline stability should be excluded from evaluativehandling. At any gestational age or acuity level, nonhan-dling observation of an infant’s movement, posture, behav-ioral organization, and physiologic stability (particularlyduring routine nursing care) are advised for determiningbaseline function and for collaboration with neonatalnurses and neonatologists on optimal timing for evaluativehandling.
Intervention
Developmental Care. This caregiving approach is de-signed to promote the neurobehavioral and physiologic orga-nization of an infant’s autonomic, motor, state/attention, andself-regulation systems as the infant matures.51 A variety ofgeneral environmental, behavioral, and care strategies can beused to modulate neonatal physiologic and behavioralchanges during each episode of care and accommodate thevarying maturation and acuity levels of infants.
Individualized developmental care is developmentalcare designed and updated for each infant in addition to ageneralized developmental care plan for all infants. Forexample, in a NICU where general developmental careprinciples are applied, overhead lights may be dimmed,isolettes covered, and caregiving procedures clustered. In anursery providing individualized developmental care us-ing a NIDCAP approach, each infant’s needs are evaluatedand a specific developmental plan developed and evaluatedon an ongoing basis.
In a Cochrane review of developmental care54 including36 randomized clinical trials (RCTs) of both general and in-dividualized developmental care, some benefits and no harm-ful effects were reported from neonatal developmental carefor infants born prematurely. The benefits of individualizeddevelopmental care documented in small RCTs included re-duced incidence of necrotizing enterocolitis and chronic lungdisease following NIDCAP interventions,54 improved behav-ior in preschool-age children who received NIDCAP-basedcare in the NICU,55 and faster transition to all nipple feedingsfollowing a daily combination of vestibular, tactile, auditory,and visual stimulation.56 The results of these small RCTs areencouraging and suggest a positive, short-term effect of devel-opmental care on the behavior of infants born preterm.54
Larger scale RCTs are needed to confirm these preliminary,positive findings.
Two large RCTs conducted in The Netherlands withinfants born at less than 32 weeks of gestation havecalled into question the benefit of basic developmentalcare (isolette covers to filter light and sound and flexed,midline, nested body positioning procedures).57,58 In thefirst study, no group differences in respiratory support,neurologic status, or growth were documented at termequivalent age between infants receiving standard new-born care compared with infants receiving basic devel-opmental care in the NICU.57 In the second study, basicdevelopmental care was compared with the NIDCAP ap-proach (weekly, individualized behavioral observation,and developmental care plan updates) to determineshort- and long-term effects. No group differences be-tween individualized (NIDCAP) and basic developmen-tal care were found in respiratory support, intensive careduration, growth and development at term equivalentage, and growth, cognitive, or motor development at 1 or2 years of age. Although these studies question the effectof individualized versus basic developmental care onneurodevelopmental and growth outcomes, neither ofthe RCTs included measures of behavior, self-regula-tion, feeding, or family coping which may have differedbetween groups.57,58
In contrast, Peters et al13 recently reported reducedlength of intensive care stay and incidence of chroniclung disease in a well-designed and controlled interven-tion study of NIDCAP effects. Preliminary data fromindividualized developmental care (NIDCAP) proce-dures indicated reduction in the rate and severity ofmental disability.11,13 In combination, these studies sug-gest that individualized developmental care may de-crease potential medical complications and varied short-term outcomes such as length of stay, level of alertness,and feeding progression. Further research prioritizinglong-term motor and cognitive outcomes will offer ex-panded analyses on the efficacy of basic and individual-ized developmental care. Larger longitudinal RCTs areneeded to determine how individualized developmentalcare affects behavior, emotional stability, and parent-child interactions (Table 3).
8 Sweeney et al Pediatric Physical Therapy

Direct Intervention. Direct therapy service refers toservice provided by a neonatal therapist at regular intervalsto address a specific impairment or activity limitation. Di-rect therapy includes, but is not limited to, handling topromote movement or postural control, joint alignmentand range of motion, cranial shaping, feeding performance,environmental modulation, and behavioral stability duringcaregiving. Research on direct therapy services is limited topreliminary results with a strong need for replication usinglarger samples and randomization.
Body positioning. Infants born preterm have immaturemusculoskeletal systems that are influenced by position-ing.59 During fetal development, the uterine walls providecontainment, facilitate trunk and extremity flexion, and pro-vide reactionary forces in response to fetal movements.55 In-fants born preterm must cope with gravity, a lack of fluid tosupport movement, and no reactionary forces to support boneand joint formation.60 Exposure to prolonged atypical posi-tioning in the NICU has been associated with torticollis, po-sitional plagiocephaly, reduced movement quality, and lowerextremity malalignment.59,61–63 Developmentally supportivepositioning may enhance the development of normal skeletalalignment and provide opportunities for normal movementpatterns. Therapists can play a vital role in program develop-ment and consultation relating to positioning. As experts inthe musculoskeletal system, PTs with neonatal training havethe expertise to establish positioning guidelines for NICUs,aid in staff development, and consult on individualized posi-tioning for infants. Because neonatal PTs do not position in-fants each time they need to be moved, a primary role of the
therapist is to collaborate with and support caregivers in po-sitioning infants to prevent secondary complications.
Infants born preterm are frequently cared for in mul-tiple positions for respiratory support and skin care. Al-though these varied positions are counter to the AmericanAcademy of Pediatrics recommendations61 for a preferredsupine sleeping position to reduce the risk of sudden infantdeath syndrome, the infants remain continuously moni-tored in the NICU setting. In an updated statement, theAmerican Academy of Pediatrics advised that all infantstransition to the supine sleeping position by hospital dis-charge and encouraged detailed discharge instruction onsudden infant death syndrome prevention including su-pine sleeping without soft bedding.64 The evidence in thesepractice guidelines relating to prone sleeping position anduse of nests or blanket rolls may not be appropriate forinfants approaching discharge.62,65–68
Although physiologic benefits contribute to the frequentuse of the prone position in the NICU, neonates may develop“flat” trunks, hyperextended and excessively rotated cervicalspines, and abducted hips when lying in the prone position,which may contribute to prolonged atypical postures ininfancy.69 Clinicians frequently modify the prone positionto improve posture while retaining physiologic benefits.The use of a horizontal positioning roll under the pelvis toelevate the hips and support hip flexion may lead to pla-giocephaly, and to increased cervical and thoracic exten-sion.65 In contrast, the use of a vertical positioning roll onthe torso parallel to the spine (alone or in combination
TABLE 3Developmental Outcomes with Developmental Care
Study Sample Intervention Results
Westrup et al55 11 experimental and 15 control; �32weeks of gestation; randomized
NIDCAP or standard of care At 63 mo, the NIDCAP group had fewerchildren with behavioral impairmentsthan the control group.
No differences in coordination or cognition
Maguire et al57 98 basic developmental care, 94 controlall born �32 weeks of gestation;randomized
Basic developmental care � isolette coverand positioning nest
No differences in NICU variables includinglength of stay or weight gain.
No difference in neurologic examination atterm
Maguire etal57,58
84 interventions; 84 controls (isolettecovers and nesting); �32 weeks ofgestation
Intervention � NIDCAP assessment weeklyand individual care plan
No difference in respiratory support, lengthof stay, growth, or neurodevelopment atterm
No difference in motor or cognitiveabilities on the Bayley Scales or growthat 1 or 2 y
Peters et al13 56–NIDCAP; 55–basic developmentalcare; born �32 weeks of gestation
NIDCAP: trained nursing care �80% timeand biweekly NIDCAP assessments
Standard of care: covers, positioningdevices, and kangaroo care available atnurse’s discretion, non-NIDCAP trainednurses providing care
Length of stay significantly less in NIDCAPgroup (74.9 vs. 84.0 days)
Decreased rate of severe disability inNIDCAP group. No group difference inscores on Bayley scales of infantdevelopment for motor or cognitiveoutcomes
Fewer infants in NIDCAP group hadchronic lung disease
Pediatric Physical Therapy Neonatal PT Practice Guidelines: Part II 9

with a horizontal roll under the pelvis) has been associatedwith improved scapular position and hip flexion.67
In the supine position, infants born preterm may haveincreased hip and shoulder abduction and external rota-tion. Two small studies advocated use of body positioning“nests” to encourage flexion of the extremities and midlinehead position.62,66 In a pilot study of 10 infants, smooth,midline movements of the extremities were observed wheninfants were in a supine nest with extremity flexion sup-port compared with the supine position without the nest.62
Although this study provided preliminary evidence thatflexed, supine positioning provided opportunities for prac-ticing flexed, midline motor patterns commonly seen ininfants born at term gestation, no follow-up observationsof the neonates were reported regarding effects on move-ment after the nest was discontinued.62 Varied positioningincluding supine, prone, and side-lying positions has beenfound to reduce the negative consequences that may arisefrom infants remaining in a single position.65,68
Swaddling with hands to mouth and lower extremityflexion while the infant is positioned in prone, supine, orside lying has been reported to improve neuromusculardevelopment at 34 weeks post-conception.70
Although these studies provide preliminary evidence forthe use of positioning strategies to encourage extremity flex-ion, no recent studies have addressed the effects of position-ing devices on movement quality, muscle imbalances, pos-tural control, or long-term musculoskeletal changes.
Joint range of motion. Passive range of motion in theextremities has been advocated as an intervention to in-crease bone mineral density; however, a recent Cochranereview of 6 RCTs found only a small, transient increase inweight gain and bone mineral density immediately after aprotocol of passive range of motion to multiple joints in allextremities 5 times per week for 3 to 4 weeks with nodifference reported at 12 months of age.71 The Cochranereview panel concluded that this evidence was insufficientfor implementing range of motion in infant born preterm toimprove bone density and weight gain.71
Therapeutic neuromotor handling. The use of thera-peutic handling or therapist-provided, hands-on interven-tion to advance motor development of infants born pre-term while in the NICU was investigated in 2 small studieswith similar approaches to intervention.72,73 Girolami etal73 included infants born preterm with atypical or asym-metrical movement responses on the Neonatal BehavioralAssessment Scale (NBAS). Cameron et al72 selected infantsat high risk of disabilities based on birth weight (�1500 g)and gestational age (�32 weeks) but with no evidence of amovement abnormality. In both studies, intervention wasprovided 5 days per week focused on midline hand skills,trunk and extremity flexion, and postural (neck/trunk)control. Girolami et al73 reported improved SupplementalMotor Test scores including enhanced antigravity and mid-line movements before NICU discharge. Cameron et al72
found no group differences on the Alberta Infant MotorScales at 4 months of corrected age; however, no post-
intervention comparison was conducted before NICU dis-charge. The findings from these 2 studies suggest thatinfants with a high risk birth history, but no atypical ordisorganized movement, are not likely to need direct phys-ical therapy services, but infants at 35 weeks post-concep-tion with asymmetrical or atypical development may ben-efit from therapeutic neuromotor handling.73 AdditionalRCTs with rigorous subject selection, discriminative andevaluative measures to determine eligibility and outcomes,and detailed intervention methods are needed to expandthe evidence regarding therapeutic handling in the NICUfor infants with atypical movement.
Multimodal sensory stimulation. Because infants bornpreterm are exposed to excessive overhead light, loudnoises, and noxious procedures in intensive care environ-ments, techniques to limit the consequences of negative stim-uli are often included in developmental care plans,51 and pro-vision of positive sensory experiences (tactile, vestibular,auditory, and visual) has been encouraged in some settings. A2006 Cochrane review, which summarized evidence for sen-sory intervention, indicated that a program including a com-bination of sensory stimuli may enhance state regulation,speed transition to full nipple feedings, and shorten length ofhospital stay, whereas tactile stimulation alone may improveshort-term growth and reduce length of stay.54 All studiesincluded in the review had small samples, and many hadmethodologic limitations including wide variations in sen-sory conditions. Two recent, small RCTs extended the Co-chrane review findings. A study comparing massage (tactile),massage plus kinesthetic stimulation (passive joint motion),and no intervention found no group differences inweight gain or length of stay for infants born weighingless than 1500 g.74 In an RCT including massage as onecomponent of a multimodal stimulation intervention forinfants between 31 and 34 weeks post- conception, in-fants exhibited reduced heart rate, increased visual-au-ditory orientation, and increased sensorimotor skills af-ter the intervention. In addition, after the multimodalinterventions, infants had increased body length and de-creased length of stay compared with infants withoutintervention.75
In combination, the 2006 Cochrane review54 andthese recent RCTs74,75 suggest that a multimodal approachto intervention may improve sensorimotor development,increase weight gain, and reduce length of stay in selectedinfants born preterm. Neonatal PTs must scrutinize thesedata and continue to explore appropriate thresholds andtypes of sensory stimuli for neonates. White-Traut et al76
cautioned that multimodal sensory stimulation may becontraindicated for infants with periventricular leukoma-lacia. Additional research is needed to determine the phys-iologic and behavioral readiness of infants born preterm formultimodal intervention in the NICU and developmentaloutcomes after NICU discharge (Table 4).
Support of infant feeding. Feeding is a functional ac-tivity of the highest priority for infants and caregivers andas such is an integral part of neonatal PT practice. Minimal
10 Sweeney et al Pediatric Physical Therapy
evidence is currently available to support oral-facial stim-ulation to hasten feeding progression in neonates. In asmall RCT reported by Fucile et al,77 a decrease in transi-tion time (days) to all oral (nipple) feedings was docu-
mented in infants receiving an oral stimulation programcompared with controls. No differences occurred, how-ever, in hospital stay or in postconceptual age when all oralfeedings were achieved.77 Researchers affirmed in 2 recent
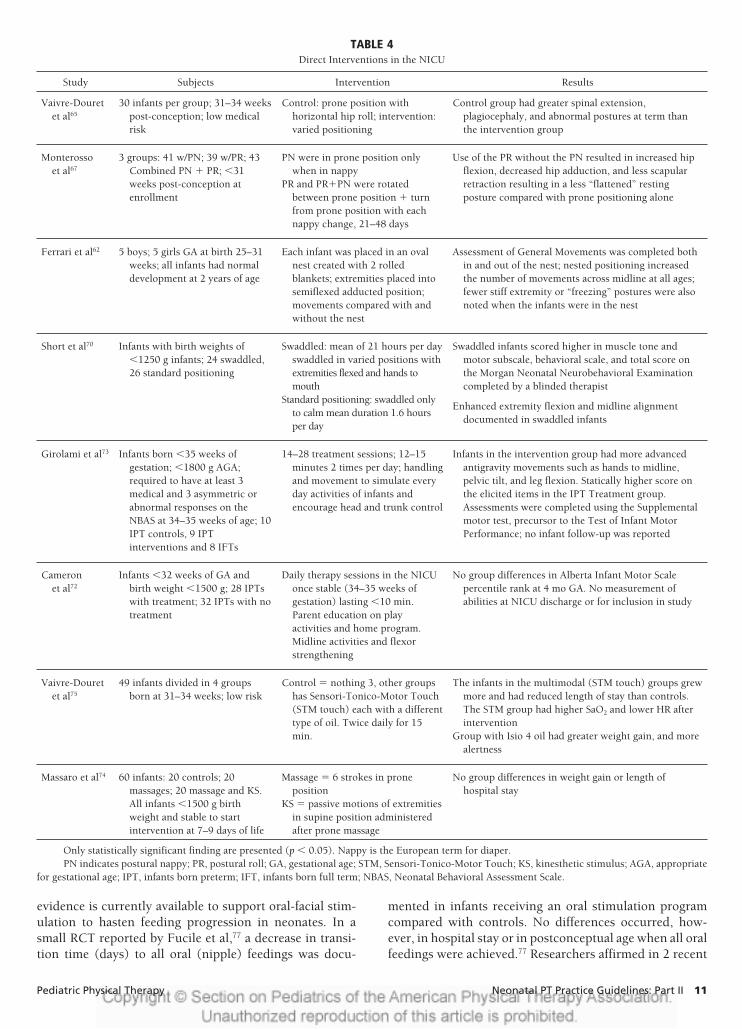
TABLE 4Direct Interventions in the NICU
Study Subjects Intervention Results
Vaivre-Douretet al65
30 infants per group; 31–34 weekspost-conception; low medicalrisk
Control: prone position withhorizontal hip roll; intervention:varied positioning
Control group had greater spinal extension,plagiocephaly, and abnormal postures at term thanthe intervention group
Monterossoet al67
3 groups: 41 w/PN; 39 w/PR; 43Combined PN � PR; �31weeks post-conception atenrollment
PN were in prone position onlywhen in nappy
Use of the PR without the PN resulted in increased hipflexion, decreased hip adduction, and less scapularretraction resulting in a less “flattened” restingposture compared with prone positioning alone
PR and PR�PN were rotatedbetween prone position � turnfrom prone position with eachnappy change, 21–48 days
Ferrari et al62 5 boys; 5 girls GA at birth 25–31weeks; all infants had normaldevelopment at 2 years of age
Each infant was placed in an ovalnest created with 2 rolledblankets; extremities placed intosemiflexed adducted position;movements compared with andwithout the nest
Assessment of General Movements was completed bothin and out of the nest; nested positioning increasedthe number of movements across midline at all ages;fewer stiff extremity or “freezing” postures were alsonoted when the infants were in the nest
Short et al70 Infants with birth weights of�1250 g infants; 24 swaddled,26 standard positioning
Swaddled: mean of 21 hours per dayswaddled in varied positions withextremities flexed and hands tomouth
Standard positioning: swaddled onlyto calm mean duration 1.6 hoursper day
Swaddled infants scored higher in muscle tone andmotor subscale, behavioral scale, and total score onthe Morgan Neonatal Neurobehavioral Examinationcompleted by a blinded therapist
Enhanced extremity flexion and midline alignmentdocumented in swaddled infants
Girolami et al73 Infants born �35 weeks ofgestation; �1800 g AGA;required to have at least 3medical and 3 asymmetric orabnormal responses on theNBAS at 34–35 weeks of age; 10IPT controls, 9 IPTinterventions and 8 IFTs
14–28 treatment sessions; 12–15minutes 2 times per day; handlingand movement to simulate everyday activities of infants andencourage head and trunk control
Infants in the intervention group had more advancedantigravity movements such as hands to midline,pelvic tilt, and leg flexion. Statically higher score onthe elicited items in the IPT Treatment group.Assessments were completed using the Supplementalmotor test, precursor to the Test of Infant MotorPerformance; no infant follow-up was reported
Cameronet al72
Infants �32 weeks of GA andbirth weight �1500 g; 28 IPTswith treatment; 32 IPTs with notreatment
Daily therapy sessions in the NICUonce stable (34–35 weeks ofgestation) lasting �10 min.Parent education on playactivities and home program.Midline activities and flexorstrengthening
No group differences in Alberta Infant Motor Scalepercentile rank at 4 mo GA. No measurement ofabilities at NICU discharge or for inclusion in study
Vaivre-Douretet al75
49 infants divided in 4 groupsborn at 31–34 weeks; low risk
Control � nothing 3, other groupshas Sensori-Tonico-Motor Touch(STM touch) each with a differenttype of oil. Twice daily for 15min.
The infants in the multimodal (STM touch) groups grewmore and had reduced length of stay than controls.The STM group had higher SaO2 and lower HR afterintervention
Group with Isio 4 oil had greater weight gain, and morealertness
Massaro et al74 60 infants: 20 controls; 20massages; 20 massage and KS.All infants �1500 g birthweight and stable to startintervention at 7–9 days of life
Massage � 6 strokes in proneposition
No group differences in weight gain or length ofhospital stay
KS � passive motions of extremitiesin supine position administeredafter prone massage
Only statistically significant finding are presented (p � 0.05). Nappy is the European term for diaper.PN indicates postural nappy; PR, postural roll; GA, gestational age; STM, Sensori-Tonico-Motor Touch; KS, kinesthetic stimulus; AGA, appropriate
for gestational age; IPT, infants born preterm; IFT, infants born full term; NBAS, Neonatal Behavioral Assessment Scale.
Pediatric Physical Therapy Neonatal PT Practice Guidelines: Part II 11

RCTs that oral-facial stimulation did not decrease thepostconceptual age at which infants attained a daily sched-ule of all oral feedings.78,79 In contrast, a 2005 Cochranereview panel80 analyzed evidence from 21 studies, includ-ing 15 RCTs, and found nonnutritive sucking with a paci-fier before, during, or after gavage or bottle feedings tosignificantly decrease length of hospital stay and toimprove feeding behavior (decreased defensive or fussybehavior during and after feeding). Long-term benefits ofnonnutritive sucking have not been established.80
Evidence is emerging for pacing and flow rate inter-ventions to support feeding in infants born preterm. Pacedfeeding, allowing 3 to 5 sucks on the bottle followed by 3-to 5-second breathing pauses, seems beneficial. In a small,nonrandomized trial Law-Morstatt et al81 found fewer bra-dycardia episodes and improved sucking skill maturity atdischarge in infants (n � 18) receiving pacing techniquesduring feeding compared with controls receiving caregivereducation intervention after discharge.81
Slowing the fluid flow rate has been shown to im-prove efficiency and physiologic stability during feed-ing. In a crossover design, 20 infants were randomlygiven a fast-flowing (cross-cut) nipple or a standard-flowing, single-hole nipple.82 When fed with the fasterflowing nipple, infants were less efficient, took longer tofeed, consumed less volume, and had higher respiratoryrates than when fed with a single-hole nipple. Futureresearch is needed to expand the level of evidence onpacing effects and flow rate adaptations and to explorethe effects of feeding positions.
Infant behavioral readiness is beginning to guide feedingdecisions rather than volume requirements only.83–85 Kirk etal83 reported decreased postconceptual age (6 days) when alloral (nipple) feedings were reached by 51 infants in a histor-ical control design with feedings initiated and advanced ac-cording to behavioral cues. McCain84 demonstrated a similardecrease (5 days) to all oral feedings when infant arousal cuesand nonnutritive sucking behaviors were used as indicators ofreadiness to feed in an RCT of 81 infants in 2 NICUs.
Neonatal PTs can support behavioral readiness andfeeding progression by teaching parents to interpret andvalue infant behavioral cues and by supporting infant phys-iologic and motor organization. Consistent with DST, in-fants who are organized and practice feeding while main-taining behavioral and physiologic stability are more likelyto be successful feeders.
Adjunct interventions. Neonatal massage as a singlemodality has been advocated to reduce stress levels andimprove infant-parent attachment in the NICU environ-ment86; however, a 2004 Cochrane review of massage inneonates stressed the need for additional research beforeintegration of massage into routine care.87 Supporting aninfant’s body with hand swaddling (facilitated body tuck)without massage88 and skin-to-skin holding by parents89
provide human touch and are less likely to contribute topotential overstimulation in neonates who are vulnera-ble.90 Similarly, the Cochrane review on the efficacy ofchest physical therapy with neonates indicated that addi-
tional research was required before inclusion into routineneonatal care related to reported adverse effects of bruis-ing, rib fractures, and intracranial lesions.91
Neonatal hydrotherapy for neonates who are medicallystable with movement impairment was introduced in a mul-tiple case series92 in which adequate physiologic tolerance(7% increase in mean arterial pressure and 7% increase inheart rate) was documented and a hydrotherapy protocol wasdetailed. In a later study, effects of hydrotherapy (immersionin swaddled and semiflexed position) before feeding indi-cated improved feeding efficiency and short-term mean dailyweight gain in 31 infants born preterm (32–36 weeks post-conception) with no difference found between high- and low-risk groups.93 Further investigation of neonatal hydrotherapyeffects on breast-feeding proficiency, bone density, gastroin-testinal reflux patterns, and behavioral organization may ex-pand future clinical use of this aquatic intervention in theNICU setting for stable neonates.
Parent Education in the NICU
Parent and caregiver teaching is a primary role of ther-apists in the NICU. Research on educating parents to in-terpret the meaning of their infant’s behavioral cues anddevelopmental status has been shown to reduce parentalstress94 and improve parental mental health.95 Derived pri-marily from the NBAS or NIDCAP models, the followinginstruments have been developed to attune parents to theirinfant’s capabilities: (1) Mother’s Assessment of the Behav-ior of the Infant,96 (2) Family Administered Neonatal Ac-tivities,97 (3) Creating Opportunities for Parent Empower-ment,95 and (4) Newborn Behavioral Observation System.16
A meta-analysis by Das Eiden et al98 indicated that NBAS-based interventions during the neonatal period have asmall to moderate beneficial effect on the quality of laterparenting.
Emerging research on parents’ preferred instruc-tional method in the NICU indicates support for multi-modal (discussion, demonstration, video, and written)instruction.99 –102 Effects of NICU parent education pro-grams specifically designed to promote infant motor or-ganization and development have not been reported butparent-delivered motor programs after NICU dischargeare supported.103,104 Additional research with both par-ent and infant outcome measures is needed to furtherinvestigate the efficacy of parent education and parent-delivered intervention in the NICU.
EVIDENCE-BASED PRACTICE RECOMMENDATIONS
Implementation of clinical procedures with researchevidence and participation by practitioners in clinical stud-ies in the NICU are critical to the advancement of neonatalphysical therapy. As the state of our science expands, theevidence base to support neonatal physical therapy prac-tice will continue to emerge. Practice recommendations,rated according to a 5-level hierarchy of evidence (Table5), are outlined in Table 6 to guide neonatal PTs in design-ing plans of care. The evidence levels range between I and
12 Sweeney et al Pediatric Physical Therapy
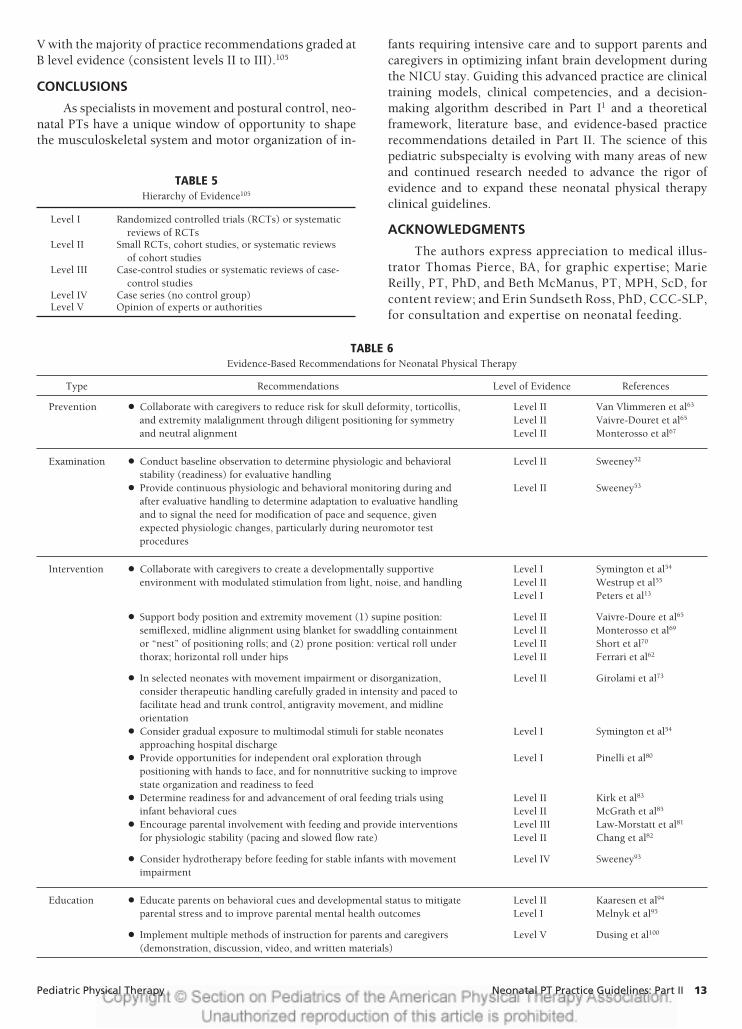
V with the majority of practice recommendations graded atB level evidence (consistent levels II to III).105
CONCLUSIONS
As specialists in movement and postural control, neo-natal PTs have a unique window of opportunity to shapethe musculoskeletal system and motor organization of in-
fants requiring intensive care and to support parents andcaregivers in optimizing infant brain development duringthe NICU stay. Guiding this advanced practice are clinicaltraining models, clinical competencies, and a decision-making algorithm described in Part I1 and a theoreticalframework, literature base, and evidence-based practicerecommendations detailed in Part II. The science of thispediatric subspecialty is evolving with many areas of newand continued research needed to advance the rigor ofevidence and to expand these neonatal physical therapyclinical guidelines.
ACKNOWLEDGMENTS
The authors express appreciation to medical illus-trator Thomas Pierce, BA, for graphic expertise; MarieReilly, PT, PhD, and Beth McManus, PT, MPH, ScD, forcontent review; and Erin Sundseth Ross, PhD, CCC-SLP,for consultation and expertise on neonatal feeding.
TABLE 5Hierarchy of Evidence105
Level I Randomized controlled trials (RCTs) or systematicreviews of RCTs
Level II Small RCTs, cohort studies, or systematic reviewsof cohort studies
Level III Case-control studies or systematic reviews of case-control studies
Level IV Case series (no control group)Level V Opinion of experts or authorities
TABLE 6Evidence-Based Recommendations for Neonatal Physical Therapy
Type Recommendations Level of Evidence References
Prevention ● Collaborate with caregivers to reduce risk for skull deformity, torticollis,and extremity malalignment through diligent positioning for symmetryand neutral alignment
Level II Van Vlimmeren et al63
Level II Vaivre-Douret et al65
Level II Monterosso et al67
Examination ● Conduct baseline observation to determine physiologic and behavioralstability (readiness) for evaluative handling
Level II Sweeney52
● Provide continuous physiologic and behavioral monitoring during andafter evaluative handling to determine adaptation to evaluative handlingand to signal the need for modification of pace and sequence, givenexpected physiologic changes, particularly during neuromotor testprocedures
Level II Sweeney53
Intervention ● Collaborate with caregivers to create a developmentally supportiveenvironment with modulated stimulation from light, noise, and handling
Level I Symington et al54
Level II Westrup et al55
Level I Peters et al13
● Support body position and extremity movement (1) supine position:semiflexed, midline alignment using blanket for swaddling containmentor “nest” of positioning rolls; and (2) prone position: vertical roll underthorax; horizontal roll under hips
Level II Vaivre-Doure et al65
Level II Monterosso et al69
Level II Short et al70
Level II Ferrari et al62
● In selected neonates with movement impairment or disorganization,consider therapeutic handling carefully graded in intensity and paced tofacilitate head and trunk control, antigravity movement, and midlineorientation
Level II Girolami et al73
● Consider gradual exposure to multimodal stimuli for stable neonatesapproaching hospital discharge
Level I Symington et al54
● Provide opportunities for independent oral exploration throughpositioning with hands to face, and for nonnutritive sucking to improvestate organization and readiness to feed
Level I Pinelli et al80
● Determine readiness for and advancement of oral feeding trials usinginfant behavioral cues
Level II Kirk et al83
Level II McGrath et al85
● Encourage parental involvement with feeding and provide interventionsfor physiologic stability (pacing and slowed flow rate)
Level III Law-Morstatt et al81
Level II Chang et al82
● Consider hydrotherapy before feeding for stable infants with movementimpairment
Level IV Sweeney93
Education ● Educate parents on behavioral cues and developmental status to mitigateparental stress and to improve parental mental health outcomes
Level II Kaaresen et al94
Level I Melnyk et al95
● Implement multiple methods of instruction for parents and caregivers(demonstration, discussion, video, and written materials)
Level V Dusing et al100
Pediatric Physical Therapy Neonatal PT Practice Guidelines: Part II 13

REFERENCES
1. Sweeney JK, Heriza CB, Blanchard Y. Neonatal physical therapy.Part 1: Clinical competencies and NICU clinical training models.Pediatr Phys Ther. 2009;21:296–307.
2. Thelen E, Smith LB. A Dynamic Approach to the Development of Cog-nition and Action. Cambridge, MA: Massachusetts Institute of Tech-nology Press/Bradford Books Series in Cognitive Psychology; 1994.
3. Heriza CB, Sweeney J. Pediatric physical therapy. Part 1: Practicescope, scientific foundations, and theory. Infants Young Child. 1994;7:20–32.
4. Heriza CB. Motor development: traditional and contemporary the-ories. In: Lister M, ed. Contemporary Management of Motor ControlProblems. Proceedings of the II Step Conference. Alexandria, VA: TheFoundation for Physical Therapy; 1991:99–126.
5. Als H. Toward a synactive theory of development: promise for theassessment and support of infant individuality. Infant Mental HealthJ. 1982;3:229–243.
6. Edelman GM. Neural Darwinism. The Theory of Neuronal Group Se-lection. New York, NY: Basic Books, Inc; 1987.
7. Als H. A synactive model of neonatal behavioral organization:framework for the assessment of neurobehavioral development inthe premature infant and for support of infants and parents in theneonatal intensive care environment. Phys Occup Ther Pediatr. 1986;6:3–53.
8. Als H. Neurobehavioral development of the preterm infant. In: MartinRJ, Fanaroff AA, Walsh M, eds. Fanaroff and Martin’s Neonatal-PerinatalMedicine: Diseases of the Fetus and Infant. 8th ed. St Louis, MO: Mosby;2006;1051–1068.
9. Als H, Lawhon G, Brown E, et al. Individualized behavioral andenvironmental care for the very low birth weight preterm infant athigh risk for bronchopulmonary dysplasia: neonatal intensive careunit and developmental outcome. Pediatrics. 1986;78:1123–1132.
10. Als H. Newborn Individualized Developmental Care and Assess-ment Program (NIDCAP): new frontier for neonatal and perinatalmedicine. J Neonatal Perinatal Med. 2009:138–147.
11. McAnulty GB, Duffy FH, Butler SC, et al. Effects of the Newborn Indi-vidualized Developmental Care and Assessment Program (NIDCAP) atage 8 years: prelimary data. Clin Pediatr (Philadelphia). 2009; [Epubahead of print].
12. McAnulty G, Duffy F, Butler S, et al. Individualized developmentalcare for a large sample of very preterm infants: health, neurobehav-iour and neurophysiology. Acta Paediatr. 2009;12:1920–1926.
13. Peters KL, Rosychuk RJ, Hendson L, et al. Improvement of short-and long-term outcomes for very low birth weight infants: the Ed-monton NIDCAP trial. Pediatrics. 2009;124:1009–1020.
14. Maguire CM, Walther FJ, Sprij AJ, et al. Effects of individualizeddevelopmental care in a randomized, controlled trial on preterminfants �32 weeks. Pediatrics. 2009;124:1021–1030.
15. Als H. Reading the premature infant. In Goldson E, ed. Nurturing thePremature Infant: Developmental Interventions in the Neonatal Inten-sive Care Nursery. New York: Oxford University Press; 1999:18–85.
16. Nugent JK, Keefer CH, Minear S, et al. Understanding Newborn Be-havior and Early Relationships. The Newborn Behavioral Observations(NBO) System Handbook. Baltimore, MD: Brookes; 2007.
17. Blanchard Y, Mouradian LM. Integrating neurobehavioral conceptsinto early intervention eligibility evaluation. Infants Young Child.2000;13:41–50.
18. Edelman GM. Second Nature: Brain Science and Human Knowledge.New Haven, CT: Yale University Press; 2006:23–34.
19. Edelman GM, Tononi G. A Universe of Consciousness. How MatterBecomes Imagination. New York, NY: Basic Books; 2000:79–92.
20. Sporns O, Edelman GM. Solving Bernstein’s problem: a proposal forthe development of coordinated movement by selection. Child Dev.1993;64:960–981.
21. Campbell SK. The child’s development of functional movement. In:Campbell SK, Vander Linden DW, Palisano RJ, eds. Physical Ther-apy for Children. 3rd ed. Philadelphia, PA: Saunders; 2006:33–76.
22. Thelen E. Coupling perception and action in the development ofskill: a dynamic approach. In: Bloch H, Bertenthal BI, eds. Sensory-Motor Organization and Development in Infancy and Early Childhood.Dordrecht, The Netherlands: Kluwer Academic; 1990:39–56.
23. Campbell SK. Revolution in progress: a conceptual framework ofexamination and intervention. Part II. Neurol Rep. 2000;24:42–46.
24. Adkins DL, Boychuk J, Remple MS, et al. Motor training inducesexperience-specific patterns of plasticity across motor cortex andspinal cord. J Appl Physiol. 2006;101:1776–1782.
25. Kleim JA. Experience dependent brain plasticity: Translating basicscience into clinical practice. Paper presented at the: III Step Con-ference, Linking Movement Science and Intervention, Pediatric andNeurology Sections, American Physical Therapy Association. July17, 2005, Salt Lake City, UT.
26. Kleim JA, Jones TA. Principles of experience-dependent neural plas-ticity: implications for rehabilitation after brain damage. J SpeechLang Hear Res. 2008;51:S225–S239.
27. Monfils MH, Plautz EJ, Kleim JA. In search of the motor engram:motor map plasticity as a mechanism for encoding motor experi-ence. Neuroscientist. 2005;11:471–483.
28. VandenBerg K, Browne JV, Perez, et al. Getting to Know Your Baby.Oakland, CA. Special Start Training Program. Mills College, Depart-ment of Education; 2003.
29. Bourjeois JP, Jastreboff PJ, Rakic P. Synaptogenesis in visual cortexof normal and preterm monkeys: evidence for intrinsic regulation ofsynaptic overproduction. Proc Nat Acad Sci U S A. 1989;86:4297–4301.
30. Als H, Duffy FH, McAnulty GB, et al. Early experience alters brainfunction and structure. Pediatrics. 2004;113:846–857.
31. Shore R. Rethinking the Brain: New Insights into Early Development.New York, NY: Families and Work Institute; 1997.
32. International Classification of Functioning, Disability and Health. Ge-neva, Switzerland: World Health Organization; 2001.
33. APTA endorses ICF Model. PT Bulletin Online. 2008;9:4.34. Palisano RJ. A collaborative model of service delivery for children
with movement disorders: a framework for evidence-based decisionmaking. Phys Ther. 2006;86:1295–1305.
35. Jette AM. Toward a common language for function, disability, andhealth. Phys Ther. 2006;86:726,734.
36. Dunn MS, Reilly MC, Johnston AM, et al. Development and dissem-ination of potentially better practices for the provision of family-centered care in neonatology: the Family-Centered Care Map. Pedi-atrics. 2006;118:S95–S107.
37. Bruschweiler-Stern N. Mere a terme et mere premature. In: Dugnat M,ed. Le monde relationnel du bebe. Ramonville Saint-Agne: ERES; 1997.
38. Klaus MH, Kennell JH, Klaus PH. Bonding. Reading, MA: Addison-Wesley; 1995.
39. DeMier RL, Hynan MT, Harris HB, et al. Perinatal stressors as pre-dictors of symptoms of posttraumatic stress in mothers of infants athigh-risk. J Perinatol. 1996;16:276–280.
40. Callahan JL, Borja SE, Hynan MT. Modification of the PerinatalPTSD Questionnaire to enhance clinical utility. J Perinatol. 2006;26:533–539.
41. Shaw RJ, Bernard RS, Deblois T, et al. (2009). The relationshipbetween acute stress disorder and posttraumatic stress disorder inthe neonatal intensive care unit. Psychosomatics. 2009;50:131–137.
42. Browne JV, Talmi A. Family-based intervention to enhance infant-parent relationships in the neonatal intensive care unit. J PediatrPsychol. 2005;30:667–677.
43. Lawhon G. Facilitation of parenting the premature infant within thenewborn intensive care unit. J Perinat Neonatal Nurs. 2002;16:71–83.
44. Loo KK, Espinosa M, Tyler R, et al. Using knowledge to cope withstress in the NICU: how parents integrate learning to read the phys-iologic and behavioral cues of the infant. Neonatal Netw. 2003;22:31–37.
45. Parker S, Zahr LK, Cole JCD, et al. Outcomes after developmentalintervention in the neonatal intensive care unit for mothers of pre-term infants with low socioeconomic status. J Pediatr. 1992;120:780–785.
14 Sweeney et al Pediatric Physical Therapy

46. Redshaw ME. Mothers of babies requiring special care: attitudes andexperiences. J Reprod Infant Psychol. 1997;15:109–121.
47. Als H, Lawhon G, Duffy FH, McAnulty GB, Gibes-Grossman R,Blickman JG. Individualized developmental care for the very low-birth-weight preterm infants. Medical and neurofunctional effects.JAMA. 1994;272:853–105.
48. Kleberg A, Westrup B, Stjernqvist K. Developmental outcome, childbehaviour and mother-child interaction at 3 years of age followingNewborn Individualized Developmental Care and Intervention Pro-gram (NIDCAP) intervention. Early Hum Dev. 2000;60:123–135.
49. Nugent JK, Brazelton TB. (2000). Preventive infant mental health:uses of the Brazelton Scale. In: Osofsky J, Fitzgerald HE, eds.WAIMH Handbook of Infant Mental Health. Vol. II. New York, NY:Wiley; 2000:159–202.
50. Sameroff AJ. Models of development and developmental risk. In:Zeanah CH, ed. Handbook of Infant Mental Health, New York, NY:Guilford; 1997:3–13.
51. Vandenberg KA. Individualized developmental care for high risknewborns in the NICU: a practice guideline. Early Hum Dev. 2007;83:433–442.
52. Sweeney JK. Physiological adaptation of neonates to neurologicalassessment. Phys Occup Ther Pediatr. 1986;6:155–167.
53. Sweeney JK. Physiological and behavioral effects of neurologicalassessment in preterm and full-term neonates [abstract]. PediatrPhys Ther. 1989;9:144.
54. Symington A, Pinelli J. Developmental care for promoting develop-ment and preventing morbidity in preterm infants. Cochrane Data-base Syst Rev. 2006;2:CD001814.
55. Westrup B, BohmB, Lagercrantz H, et al. Preschool outcome inchildren born very prematurely and cared for according to the New-born Individualized Developmental Care and Assessment Program(NIDCAP). Acta Paediatr. 2004;93:498–507.
56. White-Traut RC, Nelson MN, Silvestri JM, et al. Effects of auditory,tactile, visual, and vestibular intervention on length of stay, alert-ness, and feeding progression in preterm infants. Dev Med ChildNeurol. 2002;44:91–97.
57. Maguire CM, Veen S, Sprij A, et al. Leiden Developmental CareProject. Effects of basic developmental care on neonatal morbidity,neuromotor development, and growth at term age of infants whowere born at �32 weeks. Pediatrics. 2008;121:239–245.
58. Maguire CM, Walther FJ, Zwieten PH, et al. Follow-up outcomes at1 and 2 years of infants born less than 32 weeks after NewbornIndividualized Developmental Care and Assessment Program. Pedi-atrics. 2009;123:1081–1087.
59. Sweeney JK, Gutierrez T. Musculoskeletal implications of preterminfant positioning in the NICU. J Perinat Neonatal Nurs. 2002;16:58–70.
60. de Vries JI, Fong BF. Normal fetal motility: an overview. UltrasoundObstet Gynecol. 2006;27:701–11.
61. American Academy of Pediatrics Task Force on Sudden InfantDeath Syndrome. The changing concept of sudden infant death syn-drome: diagnostic coding shifts, controversies regarding the sleep-ing environment, and new variables to consider in reducing risk.Pediatrics. 2005;116:1245–1255.
62. Ferrari F, Bertoncelli N, Gallo C, et al. Posture and movement inhealthy preterm infants in supine position in and outside the nest.Arch Dis Child Fetal Neonatal Ed. 2007;92:F386–F390.
63. Van Vlimmeren LA, van der Graff Y, Boere-Boonekamp MM, et al.Risk factors for deformational plagiocephaly at birth and at 7 weeksof age: a prospective cohort study. Pediatrics. 2008;119:408–418.
64. Joint Committee on Infant Hearing, American Academy of Audiol-ogy, American Academy of Pediatrics, American Speech-Language-Hearing Association, and Directors of Speech and Hearing Programsin State Health and Welfare Agencies. Year 2000 position statement:principles and guidelines for early hearing detection and interven-tion programs. Pediatrics. 2000;106:798–817.
65. Vaivre-Douret L, Ennouri K, Jrad I, et al. Effect of positioning on theincidence of abnormalities of muscle tone in low-risk, preterm in-fants. Eur J Paediatr Neurol. 2004;8:21–34.
66. Vaivre-Douret L, Golse B. Comparative effects of 2 positional sup-ports on neurobehavioral and postural development in preterm ne-onates. J Perinat Neonatal Nurs. 2007;21:323–330.
67. Monterosso L, Kristjanson LJ, Cole J, et al. Effect of postural sup-ports on neuromotor function in very preterm infants to term equiv-alent age. J Paediatr Child Health. 2003;39:197–205.
68. McManus BM, Capistran PS. A case presentation of early interven-tion with dolichocephaly in the NICU: collaboration between theprimary nursing team and the developmental care specialist. Neona-tal Netw. 2008;27:307–15.
69. Monterosso L, Kristjanson L, Cole J. Neuromotor development andthe physiologic effects of positioning in very low birth weight in-fants. J Obstet Gynecol Neonatal Nurs. 2002;31:138–46.
70. Short MA, Brooks-Brunn JA, Reeves DS, et al. The effects of swad-dling versus standard positioning on neuromuscular developmentin very low birth weight infants. Neonatal Netw. 1996;15:25–31.
71. Schulzke SM, Trachsel D, Patole SK. Physical activity programs forpromoting bone mineralization and growth in preterm infants. Co-chrane Database Syst Rev. 2007;2:CD005387.
72. Cameron EC, Maehle V, Reid J. The effects of an early physical therapyintervention for very preterm, very low birth weight infants: a random-ized controlled clinical trial. Pediatr Phys Ther. 2005;17:107–119.
73. Girolami GL, Campbell SK. Efficacy of a neuro-developmental treat-ment program to improve motor control in infants born prema-turely. Pediatr Phys Ther. 1994;6:175–184.
74. Massaro AN, Hammad TA, Jazzo B, et al. Massage with kinestheticstimulation improves weight gain in preterm infants. J Perinatol.2009;29:352–357.
75. Vaivre-Douret L, Oriot D, Blossier P, et al. The effect of multimodalstimulation and cutaneous application of vegetable oils on neonataldevelopment in preterm infants: a randomized controlled trial.Child Care Health Dev. 2009;35:96–105.
76. White-Traut RC, Nelson MN, Silvestri JM, et al. Developmentalpatterns of physiological response to a multisensory intervention inextremely premature and high-risk infants. J Obstet Gynecol Neona-tal Nurs. 2004;33:266–275.
77. Fucile S, Gisel E, Lau C. Oral stimulation accelerates the transitionfrom tube to oral feeding in preterm infants. J Pediatr. 2002;141:230–236.
78. Boiron M, Da Nobrega L, Roux S, et al. Effects of oral stimulationand oral support on non-nutritive sucking and feeding performancein preterm infants. Dev Med Child Neurol. 2007;49:439–444.
79. Bragelien R, Rokke W, Markestad T. Stimulation of sucking andswallowing to promote oral feeding in premature infants. Acta Pae-diatr. 2007;96:1430–1432.
80. Pinelli J, Symington A. Non-nutritive sucking for promoting phys-iologic stability and nutrition in preterm infants. Cochrane DatabaseSyst Rev. 2005;4:CD001071.
81. Law-Morstatt L, Judd DM, Snyder P, et al. Pacing as a treatmenttechnique for transitional sucking patterns. J Perinatol. 2003;23:483–488.
82. Chang YJ, Lin CP, Lin YJ, et al. Effects of single-hole and cross-cutnipple units on feeding efficiency and physiological parameters inpremature infants. J Nurs Res. 2007;15:215–223.
83. Kirk AT, Alder SC, King JD. Cue-based oral feeding clinical pathwayresults in earlier attainment of full oral feeding in premature infants.J Perinatol. 2007;27:572–578.
84. McCain GC. An evidence-based guideline for introducing oral feed-ing to healthy preterm infants. Neonatal Netw. 2003;22:45–50.
85. McGrath JM, Medoff-Cooper B. Alertness and feeding competencein extremely early born preterm infants. Newborn Infant Nurs Rev.2002;2:174–186.
86. Beachy M. Premature infant massage in the NICU. Neonatal Netw.2003;3:39–45.
87. Vickers A, Ohlsson A, Lacy JB, et al. Massage for promoting growthand development of preterm and/or low birth-weight infants. Co-chrane Database Syst Rev. 2004;2:CD000390.
88. Harrison L, Oliver L, Cunningham K, et al. Effects of gentle humantouch on preterm infants. Neonatal Netw. 1996;15:35–42.
Pediatric Physical Therapy Neonatal PT Practice Guidelines: Part II 15

89. Ludington-Hoe SM, Anderson GC, Swinth JY, et al. Randomizedcontrolled trial of kangaroo care: cardiorespiratory and thermaleffects on healthy preterm infants. Neonatal Netw. 2004;23:39 –48.
90. Browne JV. Considerations for touch and massage in the neonatalintensive care unit. Neonatal Netw. 2000;19:61–63.
91. Hough JL, Flenady V, Johnston L, et al. Chest physiotherapy forreducing respiratory morbidity in infants requiring ventilatory sup-port. Cochrane Database Syst Rev. 2008;3:CD006445.
92. Sweeney JK. Neonatal hydrotherapy: an adjunct to developmentalintervention in an intensive care nursery setting. Phys Occup TherPediatr. 1983;3:39–52.
93. Sweeney JK. Feeding proficiency in preterm neonates followinghydrotherapy in the NICU setting [abstract]. Pediatr Phys Ther.2003;15:63.
94. Kaaresen PI, Rønning JA, Ulvund SE, et al. A randomized, controlledtrial of the effectiveness of an early-intervention program in re-ducing parenting stress after preterm birth. Pediatrics. 2006;118:e9 – e19.
95. Melnyk BM, Feinstein NF, Alpert-Gillis L, et al. Reducing prematureinfants’ length of stay and improving parents’ mental health out-comes with the Creating Opportunities for Parent Empowerment(COPE) neonatal intensive care unit program: a randomized, con-trolled trial. Pediatrics. 2006;118:e1414–e1427.
96. Field TM, Dempsey J, Hallock N, et al. Mothers’ assessments of thebehaviors of their infants. Infant Behav Dev. 1978;1:157–167.
97. Cardone LA, Gilkerson L. Family administered neonatal activities: afirst step in the integration of parental perceptions and newbornbehavior. Inf Mental Health J. 1990;11:127–131.
98. Das Eiden R, Reifman A. Effects of Brazelton demonstrations onlater parenting. J Pediatr Psych. 1996;21:857–868.
99. Goldstein LA, Campbell SK. Effectiveness of the Test of Infant Mo-tor Performance as an educational tool for mothers. Pediatr PhysTher. 2008;20:152–159.
100. Dusing SC, Murray T, Stern M. Parent preferences for motor devel-opment education in the neonatal intensive care unit. Pediatr PhysTher. 2008;20:363–368.
101. Scales LH, McEwen IR, Murray C. Parents’ perceived benefits ofphysical therapists’ direct intervention compared with parental in-struction in early intervention. Pediatr Phys Ther. 2007;19:196–202.
102. Byrne E, Constantinou J, Sweeney JK, et al. Comparison of neonatalphysical therapy instructional methods on parent competency in aneonatal intensive care setting [abstract 90]. Dev Med Child Neurol.2009;51 (suppl 5):35.
103. Lekskulchai R, Cole J. Effect of a developmental program on motor perfor-mance in infants born preterm. Aust J Physiother. 2001;47:169–176.
104. Heathcock JC, Lobo M, Galloway JC. Movement training advances theemergence of reaching in infants born at less than 33 weeks of gesta-tional age: a randomized clinical trial. Phys Ther. 2008;88:310–322.
105. Oxford Centre for Evidence-Based Medicine. Levels of Evidence(March 2009). Available at http://www.cebm.net. Accessed Septem-ber 9, 2009.
16 Sweeney et al Pediatric Physical Therapy