national stroke research institute - nsri.org.au · petrolo, sandra nsri porritt, michele...
TRANSCRIPT
NNaattiioonnaall SSttrrookkee RReesseeaarrcchh
IInnssttiittuuttee
SSiixxtthh AAnnnnuuaall
SSttrrookkee RReesseeaarrcchh RReettrreeaatt
2277tthh ttoo 2299tthh JJuullyy 22000077,, BBaallllaarraatt LLooddggee,, BBaallllaarraatt..


A lesson in fun
A penumbral moon
A satisfied delegate

Annual Stroke Research Retreat
2007
Facilitator
Dr. ALAN SIMON FINKEL, Ph.D, AM, FTSE
Executive Publisher Cosmos Magazine

Biography –Alan Finkel
Alan received his PhD in Electrical Engineering from Monash University in 1980 then worked for two years as a neuroscience Research Fellow at the John Curtin School of Medical Research. In 1983 Alan founded Californian company Axon Instruments, which rose to international pre-eminence as a supplier of electronic and robotic instruments and software for cellular neurosciences, genomics and pharmaceutical drug discovery. In March 2000 Axon listed on the Australian Stock Exchange (ASX) in what was described as the most successful Initial Public Offering ever on the ASX. In 2004 Axon was acquired by the US company Molecular Devices Corporation and Alan became the Senior Vice President for Global Engineering, the Chief Technology officer and a member of the Board of Directors. A highlight of his time at Molecular Devices, was his invention of the Population Patch Clamp, a seminal and novel technology that enables rapid drug discovery at pharmaceutical companies. Since Axon, Alan’s interests have converged on public benefit endeavours in two key areas: education and neuroscience research. In support of community-oriented research, he serves as the chairman of the National Research Centre for the prevention of Child Abuse at Monash University. In support of neuroscience research, in 2004 he conceived the idea for, and provided the initial funding for the Australian Course in Advanced Neuroscience (ACAN), an organization that provides career-enabling research training for young scientists. In 2005 he was appointed to the Australian Academy of Technological Science and Engineering (ATSE) Clunies Ross foundation Board of Governors. The mission of this foundation is to promote awareness of science and technology in Australia. Currently he is taking a lead role in organizing a major new initiative for year 10 students known as the Extreme Science Experience. Another educational initiative for which he has been the principal architect is the Science and Technology Education Leveraging Relevance (STELR) program of the ATSE. This initiative aims to add relevance, excitement and inquiry-based science teaching in secondary schools in Australia by the introduction of context-based learning centred on a renewable-energy theme. Alan, his wife and two colleagues founded Cosmos Magazine, a popular magazine of science in society, and more recently G Magazine, a lifestyle magazine for sustainable living. In 2006, Cosmos won eight honours at the Bell Magazine Awards, including Magazine of the year. In 2006 Alan was invited to serve as Chair of the Amalgamation Committee to manage the merger of the Brain Research Institute, the Howard Florey Research Institute and the National Stroke Research Institute and the co-location of the Mental Health Research Institute. The merger contract was successfully finalized in July 2007 and Alan serves as a director on the Board of the new Florey Neuroscience Institutes. In 2007 Alan was appointed Chancellor of Monash University, a position he will begin in January 2008.
Contents
Sponsor Acknowledgment 2 Foreword 3 Participant List 4 Facilitator’s Report –Dr A. Finkel 6 Program 8 Session Summaries 9 Delegate Details 42 Retreat Awards 59 Memorable Quotes 62 Acknowledgments 63 NSRI 2007 Publications 64

2
Sponsors of the National Stroke Research Institute Sixth Annual Stroke Research Retreat
Bayer Schering Pharma (Georgia Rogers & Bevin Sweerts)
Boehringer Ingelheim
(Sian Jamison)
Bristol-Myers Squibb (Tina Dafnas)
Sanofi Aventis
(Samantha Shepherd)
Servier Laboratories (Peter Ellis)
Johnson & Johnson

Foreword
3
FOREWORD The purpose of each NSRI retreat is to encourage an active dialogue between individuals from a diverse range of backgrounds and to identify areas of common concern, designed to expediate and foster collaboration. This year’s 6th annual NSRI retreat, successfully achieved this purpose and was immensely enjoyable, and informative. We tested a new format, designed to strengthen discussion and incorporate the knowledge, experience and innovative ideas of an exceptional and diverse range of investigators. These individuals included; the basic scientist, the physicist, the clinician, the allied health professional and the health economist. The focus of the discussion was to reduce the stroke burden by driving scientific and technologically based discovery in an effort to ensure the delivery of earlier, better and faster acute care intervention. This whole process was greatly enhanced by our outstanding facilitator Alan Finkel, whose breadth of knowledge, exceptional technological expertise, and well defined interpersonal skills, strongly encouraged focus, participation and lively discussion. His enthusiasm, his spirited introductions and summaries, made the whole event immensely enjoyable. Much to my delight, the accomplishments of this year’s retreat have already begun to emerge. A committee is established, to specifically address the CT perfusion plan. Collaborations between NSRI, the Brain Research Institute and Auckland City Hospital, New Zealand are leading to further validation of the MRI tractography technology. Collaborative efforts between CSIRO and NSRI’s basic science division also continue to expand. This has proved to be a very challenging and rewarding retreat. I thank you all for your participation. GEOFFREY A. DONNAN

Participants
4
DELEGATE PARTICIPATION LIST
Delegate Affiliation Partner Aleksoska, Elena NSRI/University of Melbourne Antonic, Ana NSRI/University of Melbourne Bannister, Louise La Trobe University Barber, Alan Auckland City Hospital Beer, Christopher University of Western Australia Mark Etherton Ben-Shabat, Ettie NSRI Bernhardt, Julie NSRI Tony Cross Bladin, Chris Monash University Cadilhac, Dominique NSRI Calford, Michael University of Newcastle Carey, Leeanne NSRI Carter, Rob Deakin University Gail Younie Chambers, Brian NSRI Coia, Greg CSIRO Collier, Janice NSRI Connelly, Alan Brain Research Institute Cox, Susan NSRI/University of Melbourne Brook Sumner Craggs, Barbara Medical Student Dafnas, Tina Bristol-Myers Squibb De Silva, Deidre Royal Melbourne Hospital Dewey, Helen NSRI & Austin Health David Price Dhamija, Rajinder NSRI Donnan, Geoff NSRI Elizabeth Donnan Ebinger, Martin Royal Melbourne Hospital Johanna Gertler Ellis, Peter Servier English, Coralie University of South Australia Favaloro,Jenny NSRI/University of Melbourne Finkel, Alan Cosmos Magazine Elizabeth Finkel Hankey, Graeme Royal Perth Hospital Howells, David NSRI Hudson, Peter CSIRO James, Louise Austin Hospital Jamison, Sian Boehringer Ingelheim Jeffreys, Amy NSRI/University of Melbourne Judkins, Simon Austin Health Kelly, Roslyn NSRI Andrew Melling Kerr, Nicole NSRI/University of Melbourne Lalor, Erin National Stroke Foundation Lefevere, Kathy CCRE Neurosciences Martin Burd Leung, Jessica NSRI Loy, Candace NSRI/University of Melbourne

Participants
5
Delegate Affiliation Partner Ly, John NSRI Ma, Henry NSRI Mackay, Mark Royal Children's Hospital Manasseh, Richard CSIRO Markus, Romesh University of New South Wales Masci, Kevin Metropolitan Ambulance Service Mendelsohn, Fred Howard Florey Institute O'Collins, Tori NSRI/University of Melbourne Roger Smith
Parsons, Mark John Hunter and Mater Hospitals
Pearce, Dora NSRI Petrolo, Sandra NSRI Porritt, Michele NSRI/University of Melbourne Rewell, Sarah NSRI/University of Melbourne Rogers, Georgia Bayer Schering Rostas, John University of Newcastle Sena, Emily NSRI/University of Melbourne Shepherd, Samantha Sanofi Aventis Sidon, Kate NSRI/University of Melbourne Sitte, Karin NSRI Roger Meagher Spratt, Neil John Hunter Hospital Stinear, Cathy University of Auckland Sturm, Jonathan Gosford Hospital Sweerts, Bevin Bayer Schering
Tournier, Donald Brain Research Institute Joanna Stamogiannou
Trenberth, Robert NSRI, Board Member Judy Trenberth Udommongkol, Chesda NSRI Vogiagis, Daphne NSRI Peter Trimbos Wills, Taryn NSRI/University of Melbourne Young, Dennis NSRI Zavala, Jorge NSRI Margareth Zavala

Facilitator’s Report
6
POST-RETREAT REPORT FROM FACILITATOR DR ALAN FINKEL Our ability to expand scientific knowledge depends critically on advances in scientific instrumentation. Of all the classes of scientific instruments ever invented, the one that has had the most profound impact is the microscope and its imaging brethren. Images of molecules and galaxies, of proteins and brains, provide uniquely valuable insights into structure and function. Whether the imaging is direct, such as that provided by most microscopes, or indirect such as that provided by x-ray diffraction, the images invariably contribute to our present-day understanding and set the stage for the next generation of questions, inventions and knowledge accumulation. The 2007 National Stroke Research Institute retreat was a stage upon which a bountiful array of imaging technologies were paraded. Perfusion CT is an enhancement to conventional CT that advances the state of the art, by using time-based imaging to track a perturbation created by the introduction of a bolus of contrast agent. This leads to excellent visualisation of the infarct core and the penumbra. Along with the challenges inherent in setting thresholds and performing clinical trials, limitations such as radiation exposure, contrast agent load and cannulation were identified MRI Tractography’s main goal is to follow the white matter tracts. The tensor based technique used until recently is severely affected by crossing fibres. A new approach to MRI tractography based on constrained spherical deconvolution is much more accurate and provides the promise of a useful new clinical tool. However, functional studies to correlate the tractography images with clinical outcomes are needed. The third session challenged the audience to think of new uses for a large number of leading edge technologies, presently used in basic science laboratories. The cornucopia of technologies included:
• new PET ligands; managanese, • MRI, • phase contrast X-ray imaging using a synchrotron, • optical coherence tomography, • miniaturized confocal microscopes capable of
probing the brain at cellular resolution, • ultrasound targeting of microbubbles to image
blood flow and volume, • In vivo bioluminescence, optical spectroscopy, and • Doppler blood flow reperfusion.

Facilitator’s Report
7
This rich suite of technologies will surely provide gainful employment for neurologists and basic scientists for decades to come. Especially as these technologies are extended and supplemented in the future. Two of the major challenges that emerged from the pioneering technologies discussed at the retreat were: 1) To share and collate initial research data so that the combined expertise of like-thinking pioneers will: a) guide the evolution of research directions and b) identify clinical applications most likely to benefit from the new imaging modalities. 2) To run animal trials that will prove the accuracy and utility of these new techniques in guiding stroke treatment and thereby provide practical and ethical justification to test these new techniques in clinical trials. It was a privilege to be part of this exciting, challenging and dynamic retreat.
Program
8
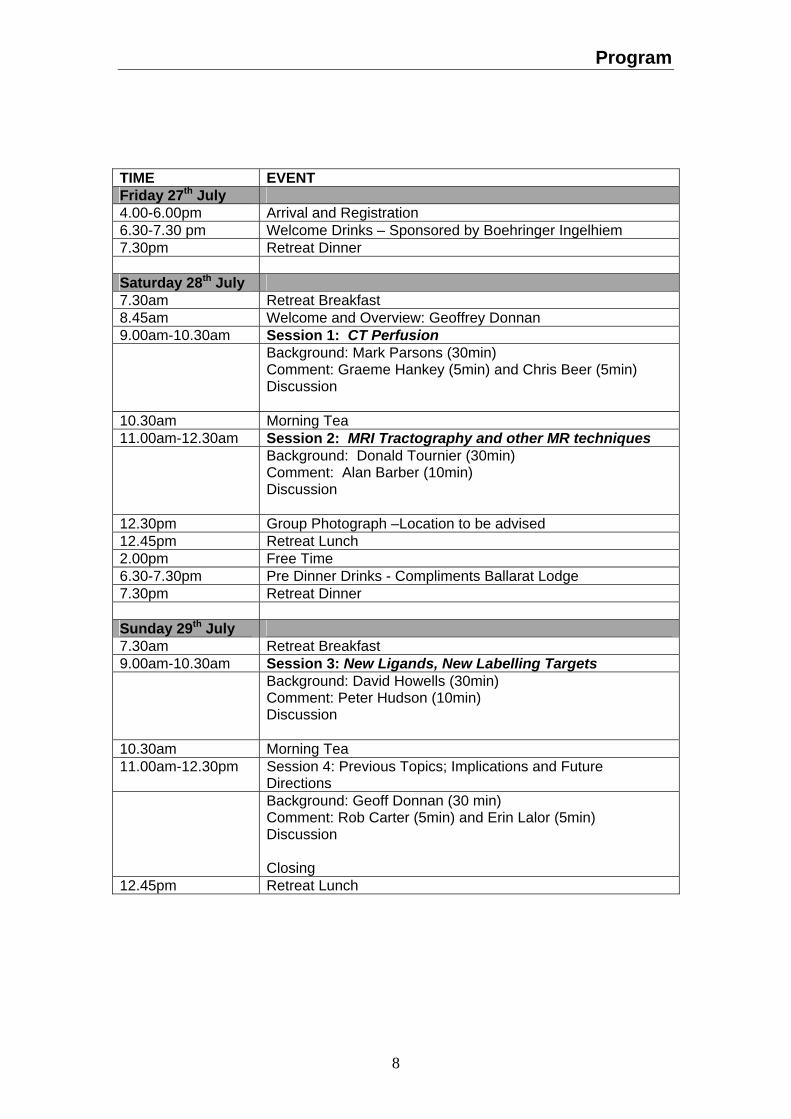
TIME EVENT Friday 27th July 4.00-6.00pm Arrival and Registration 6.30-7.30 pm Welcome Drinks – Sponsored by Boehringer Ingelhiem 7.30pm Retreat Dinner Saturday 28th July 7.30am Retreat Breakfast 8.45am Welcome and Overview: Geoffrey Donnan 9.00am-10.30am Session 1: CT Perfusion Background: Mark Parsons (30min)
Comment: Graeme Hankey (5min) and Chris Beer (5min) Discussion
10.30am Morning Tea 11.00am-12.30am Session 2: MRI Tractography and other MR techniques Background: Donald Tournier (30min)
Comment: Alan Barber (10min) Discussion
12.30pm Group Photograph –Location to be advised 12.45pm Retreat Lunch 2.00pm Free Time 6.30-7.30pm Pre Dinner Drinks - Compliments Ballarat Lodge 7.30pm Retreat Dinner Sunday 29th July 7.30am Retreat Breakfast 9.00am-10.30am Session 3: New Ligands, New Labelling Targets Background: David Howells (30min)
Comment: Peter Hudson (10min) Discussion
10.30am Morning Tea 11.00am-12.30pm Session 4: Previous Topics; Implications and Future
Directions Background: Geoff Donnan (30 min)
Comment: Rob Carter (5min) and Erin Lalor (5min) Discussion Closing
12.45pm Retreat Lunch

Session Summaries
9
Saturday 28th July 2007
Alan Finkel, Facilitator Basic research tends to occur from the bottom up. Clinical research tends to occur from the top down. There is always a problem if either of these approaches is used to the exclusion of the other. Clearly, we need a combination of both. At the NSRI the research groups span the entire spectrum, from basic and clinical research to allied health and public health outcomes. In addition to combining bottom up and top down approaches, this is a technologically orientated conference. This is exciting, as breakthroughs in science often ride on advances in instrumentation. The executive directors of the new FNI are determined people with a clear vision, and will be supportive of the research and clinical practice recommendations that emerge from this conference. Session 1: CT Perfusion
Background: Mark Parsons The Ischaemic penumbra CT imaging -practical to take penumbral imaging to the masses. If perfusion is not restored the infarct core will expand to occupy the penumbra. The Holy Grail of acute stroke involves the reperfusion of the penumbra. Currently we use tPA however, we do not image the penumbra in a patient. The current acute therapy selection is based on time and ‘negative’ imaging. We need to include penumbral imaging as part of the selection of TPA patients. Non-contrast CT often gives false negatives. Advanced Multi-modal CT can be used to track a contrast bolus and is similar to perfusion /diffusion MRI. Protocols vary from site to site due to differences in equipment.

Session Summaries
10
CT perfusion Questions What are the perfusion thresholds for infarct core and penumbra and how do they change over time? How much do values vary across manufacturers? Various values will give different results. Is multi-modal CT comparable to MRI? Multi-modal CT –limited brain coverage? We do not have whole brain coverage we have between 40-60mm coverage which is sufficient for therapy. New generation scanners will give better coverage. Third generation tenectoplase-has superior reperfusion. An ethical concern of using this technique is radiation exposure.

Session Summaries
11
Future directions: The penumbral selection or “enrichment”of population for phase III trials. The advantage is accessibility and practicality compared to MR. Do we need more observational data about CT predictors of response to acute therapy? This is also true for MR. What penumbral mismatch is the cut off? The greater the mismatch the more likely the patient will benefit. What about large core and large penumbra, if the patient does not have an obvious vessel occlusion? Do the patients need vessel occlusion as well as penumbra to be the ideal imaging target? Phase IIb “proof of concept” trials. Performed to assess biological effect and signal higher chance of success before proceeding to much larger and very expensive phase III trials Phase IIb trial – using penumbral selection with perfusion CT and randomisation of tPA use or a 3rd generation thrombolytic agent.

Session Summaries
12
Surrogate outcome marker: CBV lesion can be used as a baseline for infarct expansion Early reperfusion is a potent measure of biologic efficacy of thrombolytic agents and strongly predicts clinical outcome.
Animal studies There are very few centres that do perfusion CT on animals. Studies in New Zealand white rabbits, show that penumbra does exist.

Session Summaries
13
Session 1: CT Perfusion
Comment: Graeme Hankey and Chris Beer Graeme Hankey: Criteria for accepting studies for publication Is the study:
• Ethical? • Valid? • Important? • Novel? • Well presented?
How does the study that Mark Parsons described compare?
It is ethical? - Yes, but there is a small risk associated with radiation exposure with CT.
Is it valid? Yes, the measures of cerebral blood flow and volume, and mean cerebral transit time have been validated. However, the hypothesis that, in areas of reduced cerebral blood flow and increased transit time, reduced cerebral blood volume is a predictor of the infarct core and normal or increased cerebral blood volume is a predictor of the ischaemic penumbra, and response to reperfusion therapy, remains to be validated externally.
Is it novel? Yes, in areas of reduced cerebral blood flow and increased transit time, reduced cerebral blood volume has been shown for the first time to be a possible predictor of the infarct core and normal or increased cerebral blood volume the ischaemic penumbra. Is it important? Yes, identifying a valid imaging predictor of the infarct core and ischaemic penumbra, and response to reperfusion, can allow treatment to be targeted to those most likely to respond and avoid giving a potentially risky and costly treatment to those who are unlikely to benefit.
Chris Beer: ‘ASTART’, The Western Australian study using CT perfusion Originally Chris was doing research using statins and angiotensin receptor blockers and he wanted a clinical outcome using a safe technique. Reasons for choosing CT perfusion? 1) Access to MR very difficult in the acute setting.
Session Summaries
14
2) Convenience. We initially had some safety concerns; routine use of CT angiography was stopped, partly because of concerns about the radiation dose. Also, initially we used CT angiography which was later dropped due to radiation dose. This is a study in progress. Session 1: Discussion We need an enormous database of perfusion images to answer a number of questions. Why not collaborate with other centres worldwide? Limitations, considerable funding is required to do this. Currently, only a small number of centres perform these studies as there are quality control issues. How many Australian centres do CT perfusion? Can map acquisition be standardised? Yes, maps can be saved in a format that can be transferred by email (small file size). The software needs to be available to all centres participating. With MRI perfusion, the measures come from standard software MRI scanners and are unreliable. Using CT perfusion it may be advantageous to build up a whole body of data that determines the course of action over the following years without building questions into the study. Is this the right time to do a multi centre study? CT perfusion issues The major concern is the software variability between different manufacturers. Each manufacturer uses different methods of analysis and therefore this leads to different results. Validity is dependent on either pre or post processing. Inter-user variability also occurs. It would be useful to obtain the raw data and some basic information. Then build-up the repository for later analysis. Minimum data to be collected: Acute CT data. Clinical data. 3-Day data. The problem is that you need a feedback mechanism to improve the data which is collected at each centre. Is it possible to calibrate the instruments and get the same signal across sites? This is not an easy task with different manufacturers and acquisition methods.

Session Summaries
15
David Howells has some animal models that are robust enough to share, and are ready to test at other centres. A major initiative could be to get some order into standardising these parameters and to develop a system that the manufacturers would be interested in exploring. This would create a huge commercial opportunity. We need mixed audiences when these discussions occur at conferences. There are often meetings amongst technical people without input from clinicians and visa versa. Currently the software market is driven by radiologists who demand packages from manufacturers. Therefore, clinical sites put pressure on manufacturers to produce the packages. Who is driving the physics development of CT perfusion? Nobody in the scanner world. There is an enormous opportunity to drive this research technology from a clinical perspective. We need to expand on the evidence that Cerebral Blood Volume (CBV) correlates with infarct. There is a very good correlation on follow-up. Reduced CBV can be seen to be reversed (not if zero). CSIRO is starting to do 3D registrations of PET and MR – looking for new opportunities for cross registration of 2D and 3D neuroimaging. This presents a great opportunity for collaboration on software development. To what extent do researchers work as consultants to companies to provide algorithms? Alan Connelly’s group are doing this but the lead time to get this into production is very long. Who are the groups performing CT perfusion? Group Leaders: Chris Bladin Romesh Markus Graeme Hankey and Chris Beer Mark Parsons Geoff Donnan

Session Summaries
16
Session 2: MRI Tractography and other MR techniques Background: Donald Tournier
Tractography –acquiring a large number of diffusion weighted images. Diffusion tensor–represents how much diffusion occurs at various directions. Mean diffusivity –is used to measure acute stroke. Parameters –to look at the direction of diffusion. From the directions you can then form the actual tractography. The random thermal motion of particles is called diffusion. Diffusion of particles at around 5 microns is comparable to cells in a tissue. Diffusion provides information about tissue microstructure. Diffusion can be measured along a particular direction by labelling molecules according to their position. Molecules are allowed to diffuse, the gradient is reversed and the particles that do not move have a high signal and a low rate of diffusion. Particles which move will have a low signal and a high rate of diffusion.

Session Summaries
17
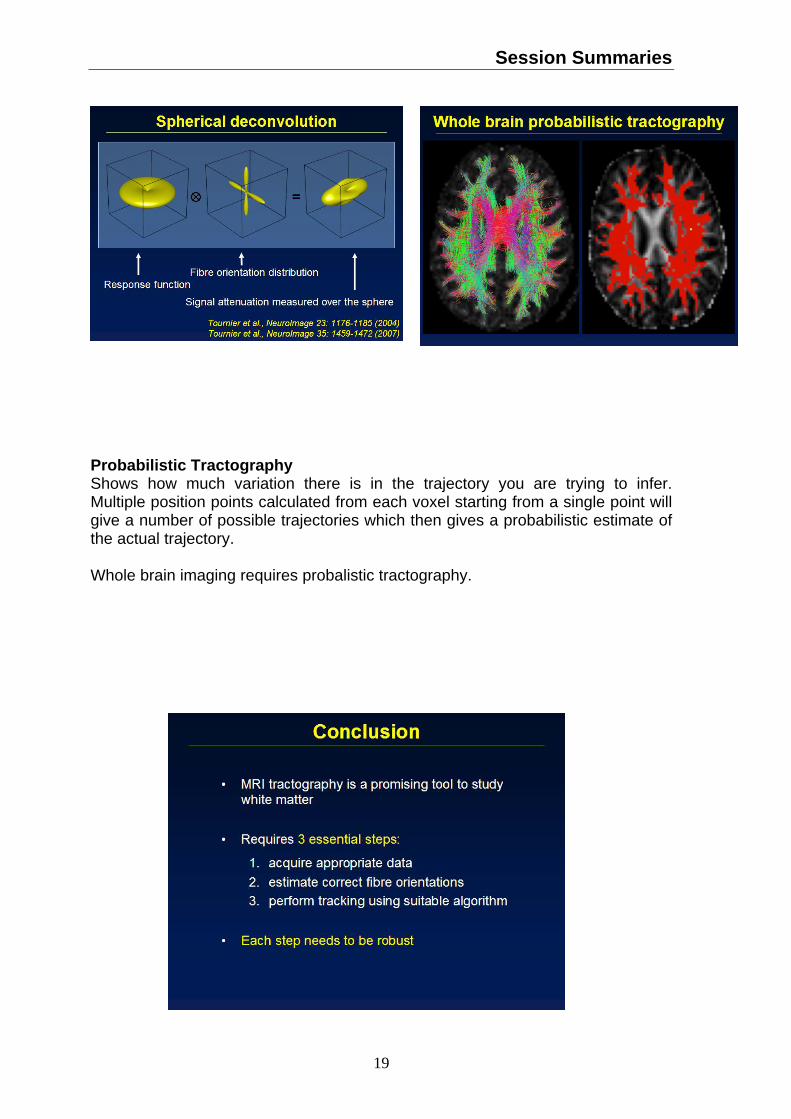
Tensor imaging Anisotropy – particles are restricted to where they can diffuse so they end up in an ellipsoid configuration. This occurs in white matter tracts. Additionally, you get directionality of diffusion in different planes (up/down, left/right). Isotropy- particles have freedom to diffuse anywhere – spherical shape, therefore get a low signal (grey matter, CSF). Fibre tracking can be used. Limitations Diffusion weighted imaging cannot be trusted if we have crossing fibres. (Example from slide) Crossing fibres, diffusion tensor model has two different orientations, therefore the object ends up between elliptic and spherical which is very difficult to interpret. Approx 1/3 of white matter voxels are affected by this problem. This causes problems with tracking as most fibres will reach a cross junction at some point and can end up in a different location than originally expected. How do you determine what is a real result and what is not? Constrained Spherical Deconvolution CSD Combined information from spherical and directional data needs to be split to determine both components. Therefore the directional component can be analysed on its own. This allows us to see the directions of the tracks when they cross over.

Session Summaries
18
Session Summaries
19
Probabilistic Tractography Shows how much variation there is in the trajectory you are trying to infer. Multiple position points calculated from each voxel starting from a single point will give a number of possible trajectories which then gives a probabilistic estimate of the actual trajectory. Whole brain imaging requires probalistic tractography.

Session Summaries
20

Session Summaries
21

Session Summaries
22
Session 2: MRI Tractography and other MR techniques
Comment: Alan Barber
We are conducting the following study: Patient upper limb weakness using a multimodel MRI study. The above slide shows a patient with a lacunar infarct (T1-W1). The fMRI image shows activation elsewhere. In this surviving patient diffusion tensor tractography DTT was used to demonstrate that there is damage to the descending fibres in the aortic spinal tract. Tractography is a great technique. When looking at tractography on its own you are only learning about the wires, this needs to be combined with functional information to have meaning. Alan’s team recently published a clinical study:

Session Summaries
23

Session Summaries
24

Session Summaries
25
Session 2: Discussion MRI tractography is a new technique and there has been an explosion of papers in the field, however not all papers are of good quality. Tractography, using microscopy has similar limitations to MRI because you need to reconstruct a 3D model from a number of slices. Dissections are also very difficult, however no technique is perfect. Managanese MRI (calcium analog). Very difficult to get only one tract to take up the dye. Best to use a combination of methods. If it were possible to get histological information, could you use it to guide tractography? Analogy, GPS in car is not really accurate but uses maps as well as satellite information to determine the exact location of the car. This has been suggested and tried, but nobody has done it in a convincing manner. Value of this method in the plasticity of stroke. It needs to be linked with fMRI as a starting point to seed the tractography. Need to exercise caution as the exact location of the voxel can affect the result. Probabilistic analysis how does it work? Can you be confident of the outcome? Usually, as you get further away from seed point you get more spreading out. Therefore, lower probability values which can prove difficult to control. How do you use this to include or exclude patients for certain types of treatments? This depends on the type of treatment. Try to use the technique to see if the patients would benefit from physical therapy. Tractography gives information on actual bundles of fibres from A to B. fMRI looks at point A and point B, where you have no information on synapses between these two points. Detection of unexpected tracts, if the middle part of the 3 step process goes wrong, this will result in the wrong connection. All 3 steps need to be robust before conclusions can be drawn about new tracts. Therefore, inclusions and exclusions of patients as a result of these must be approached with extreme caution. Where should this technology go? It is too premature to exclude patients for rehabilitation on the basis of tractography? We may need to look at different approaches, where you look at connections in the opposite hemisphere to the stroke.

Session Summaries
26
Sunday 29th July 2007 Session 3: New Ligands, New labelling targets
Background: David Howells What would we like to image? Vascular function Cellular injury Axonal injury Inflammatory processes Wound healing Regenerative processes Drug delivery
The vasoconstriction of green vessels (above), imaging of live brain under the microscope. How can we use this technique in a human setting?

Session Summaries
27
Axonal and dendritic injury Should we be looking at axonal and dendritic function as well as cell body and main axon injury? We need to look at changes in connectivity, as these local interconnections allow our brains to function.
Microglia/macrophages PK1195 ligands often used, but these do bind to other cell types. We need to be more imaginative and we need to use markers that give greater cell specificity. We need to be careful as macrophages fulfil many functions, some of which are not detrimental to neurons.

Session Summaries
28
Astrocytes and endothelium Glutamate transporters may be useful to image the astrocytic response to brain injury. Aquaporins are up regulated and vessels dilate to allow more blood into the area. Astrocytes regulate vasodilation. New uses of existing technologies: Pet MRI CT SPECT Ultrasound

Session Summaries
29
New uses for imaging techniques Thioflavine-S accumulates where axons have been damaged. PIB is an analog of thioflavine. Does PIB-PET image damage axons? Developing new ligands for PET is not trivial. FMISO was thought to be a penumbral marker. New ligand FSO101 binds better at the penumbral region as opposed to core. We must interpret these results with caution, as we don’t know for certain that the binding occurs in the penumbra.
Manganese MR Transported along axons and is structurally similar to calcium. Emerging technologies: Diffraction X-ray imaging Infra-red optical imaging Hand-held con-focal microscopy Contrast-enhanced ultrasound

Session Summaries
30
Phase contrast X-ray imaging X ray diffraction imaging in live animals is possible.
Optical coherence tomography – may develop to get greater penetration.

Session Summaries
31
Hand held confocal microscopy Fibred confocal fluorescence microscopy facilitates extended imaging in the field of microcirculation. A comparison with intravital microscopy. Microscope is on a 2mm long probe.
High-resolution ultrasound imaging Contrast enhanced ultrasound; can it be used to image inflammation? Can light imaging be coupled to ultrasound? As demonstrated in the above, slide it is possible to view apoptosis in a tumor by bioluminescence.

Session Summaries
32
Session 3: New Ligands, New labelling targets
Background: Peter Hudson Neurodegenerative disease, mental disorders and brain health
CSIRO is currently undertaking the $10 million AIBL study with NSA/NSV partner Institutes to follow neurodegenerative disease progression in 1000 volunteers over 2 years. This is the world’s largest study to include neuroimaging by PIB-PET and MRI and this will enable accurate biomarker diagnosis of Alzheimer’s disease progression. The AIBL study also includes accurate Alzheimers 3-D imaging technologies.

Session Summaries
33
CSIRO is also developing Microbubbles to deliver Contrast agents for improved vascular-imaging and deliver therapeutic agents (eg TPA) to break up clots.

Session Summaries
34
CSIRO has world-leading expertise in engineering Antibodies directed to diagnostic imaging and therapy of cancer and inflammatory diseases and is a member of HUPO (human proteomics) in an ambitioius attempt to map all human proteins against disease pathologies. CSIRO has spun-out antibody companies EvoGenix (EGX) and AviPep Pty Ltd and has assisted Agen (AGX) in the development of a D-dimer targeted antibody that is used to image thromboses and clots. Currently, CSIRO is attaching antibodies to novel nano-capsules for drug delivery or internal imaging.

Session Summaries
35
There are many opportunities for stroke researchers to partake in these studies. Session 3: Discussion Process for priority setting. Early detection and prevention of disease is a National priority and would make a huge impact in reducing health cost burden. Individual priority areas are segmented into disease indications and product development is driven by companies and limited government funding. CSIRO is now driven by the National Research priority for “Promoting Health” and the Neurodisease (Alzheimer’s) focus is directed to a major health benefit to the Australian population. . Conclusion: Begin with broad discussion for collaborative opportunities between NSRI and CSIRO and then focus into disease-specific indications and solutions. Fast-track small-scale collaborations which have already been identified (eg Sonar thrombolysis without antibody targeting).

Session Summaries
36
Session 4: Previous Topics; Implications and Future Directions
Comment: Rob Carter Priority setting is a multi disciplinary area of research, there are many contributors to this area which include clinicians and economists. There is also an International Society for Priority Setting. Which get together and discuss the contribution of health economics in relation to priority setting. Priority assessment. The starting point involves scientists talking to clinicians, to clearly identify areas of common concern and interest. There needs to be an active dialogue between the basic scientists and the medical professionals. There is a whole body of literature of technology assessment. The evaluation perspective involves a logical sequence of events. Questions that need to be considered include: Does it work? Is it value for money? Is it important to stakeholders ie patients? What is the feasibility of implementation? The natural set up of questions when you evaluate technology. From the Health Economist perspective, there are three questions: What do we do? How do we do it? Who gets it? Need to consider these three questions alongside the hierarchy of technology assessment. In the world of technology assessment; “It is always too early to evaluate until it is too late”. There is a need to start that process quite early and think about the broader issues, rather than leaving this until it is too late.

Session Summaries
37
Session 4: Previous Topics; Implications and Future Directions
Comment: Erin Lalor The questions that Erin would like to ask in relation to the discussions that took place today and yesterday are as follows: What are the possible clinical applications of the techniques? How might it be used to improve clinical outcomes and how can it be translated to clinical practice? The basis for these questions are as follows: There is now a shift in the NHMRC funding policy. The NHMRC has determined that much of the research that is occurring in Australia does not translate into improved outcomes for patients. It is important to note that basic/curiosity research is still considered significant by the NHMRC, but how this can be translated into practice is being explored. The NHMRC now has a program called the Practice and Policy Program PPP For example, a question asked could be: how can we be sure that the work funded by the NSF will change clinical practice? The NSF is also looking not only at research that creates new knowledge, but also at research, and how to translate this into practice Barriers to do this: We don’t use what works. We don’t know what works. We don’t have something that works. Need to explore these areas in the research presented here. It is important that we create a new assemblage of therapies, where we understand the mechanisms. The use of networks is important because it looks at the endpoint and not the start point. Session 4: Previous Topics; Implications and Future Directions
General Discussion: Geoff Donnan The new retreat format has worked incredibly well. Past formats have included the 10 minute talk with 3 slides. Or the 20 minute talk with 5 slides, in which Chris Levi managed to include 20 additional slides. His famous quote when asked about exceeding the 5 slide limit last year was, ‘they won’t notice”. Furthermore, even with a one hour discussion for each session there still does not seem to be enough time to cover all the information, ideas and insights.

Session Summaries
38
CT perfusion The three areas to highlight and discuss further are:
1) Setting up an Australian database, ie as Helen Dewey suggested. a) What sort of collaborating centres should we have? b) What sort of storage device should we use? ie MMIM project c) What would be the minimum data set required? It does not
matter what software we have, because software will get better and we can then apply it to the data set.
d) What funding should we aim for? 2) Should we be using animal CT? As it is too difficult to sort out all the
problems with CT in human studies. 3) Can we do CT perfusion in the posterior circulation.
Rob Trenberth’s comment I would like to propose the need to try to improve current alogarithms and get better insights into the data. Due to the continuing use of CT perfusion scanning, there will always be a role for it, so any investment made will deliver value. We must engage a small group to develop approaches to solve the software problem. As a next step a national workshop could be organised and may be funded by the NHMRC in view of their new priorities. Mark Parsons Need someone to champion the software development. Perfusion software issue will take some time to sort out. Need to collect the data and work on the software alongside. Gold standard for human or animal model? Currently there is no existing phantom. We may need to develop one of these, this should not be too difficult. Plastination technology could be used to create a cast of the whole body. Look at the vasculature and then use a polymer to get rid of the vessels, what you have left is the vasculature of the brain and skull. The protocol for CT perfusion could be as follows: 1) Initial perfusion CT 2) Follow up MR because of variation problems 3) Clinical outcome data for three months. 4) Minimal data set. Why are we collecting the data – the funding bodies will want to know this! Collecting data around intervention would give data which will answer questions on health outcome. Alan Connelly’s group cannot undertake solving the CT problems as they are already too committed to MRI. There are no other groups that are linked to the manufacturers. We need funding and personnel resources. Erin Lalor questions the clinical applications of the database. It may be better to look at: 1) How tPA is being used? 2) Why it is not used in some cases?

Session Summaries
39
3)How it can be used better? Should we identify patients that don’t get tPA because we don’t know when they had a stroke using sodium imaging? Could images from other diseases be included to broaden the research criteria? What proportion of cases get treated, who did not actually have a stroke? Question: Is animal CT possible and is it worthwhile? Answer: Yes, we have access to a single slice machine. Also we may get access to an ex-human machine (trying this out on Wednesday; D. Howells). The NHMRC funding switch to a more focused outcome is a concern. You can’t pick winners in this game. Moving away from the former model is dangerous because it could stifle basic research and great new ideas. CT Perfusion Action Plan: Set up a committee (chaired by Mark Parsons and Helen Dewey) to work through priorities (minimum data set, funding source etc). Develop a plan. Diffussion tensor imaging; Donald Tournier Spherical deconvolution model – Is it really the best? -When is it ready for prime time? -How should it be validated?
-In animal models? -In clinical studies?
-What is the best clinical application? -connactivity mapping in stroke? -evolution after acute stroke? -rehabilitation studies? Donald Tournier There are two main schools of thought. Many methods that are similar with performance overlap. There has been lots of interest in this method over other sytems. Validation – have done extensive simulations to get the answer. Have done phantom model work. There is no phantom for tracking and it would be very difficult to do. You cannot replicate white matter and the geometry. We are working on creating a numerical phantom with realistic geometry. We are interested in collaborating to establish an animal model. We could use sciatic nerve and contort it to see if it can be tracked. Is this realistic? Need to have lots of intersecting fibres, to challenge the model. We could use MR in rats to test tracking in animal models.

Session Summaries
40
If this technique is ready to use, how can we get the best value for its use? It is not really prime time in clinical stage, still in the phase of good research tool. Not useful for the acute stage. Strength is in the rehabilitation. In the future we may be able to individualise therapies for individual patients. The ability to detect injury in vivo and then target therapy. This would be a very powerful technique in animal models. MRI Tractography Action Plan: Collaborations between BRI and NSRI on validation Alan and Leanne already collaborate in the connectivity area. New Ligands, New labelling targets Objectives: To identify technology that is translatable and able to reduce the burden of stroke. Set up criteria:
1. Benefit in diagnosis and management of stroke. For instance, PIB PET very successful in Alzheimer’s. Study of very high risk vascular patients. Can use controls from AIBL study.
2. We need to have expertise in place at the NRSI along with the expertise of CSIRO (eg ultrasound)
3. We need to look at what might be early wins – translation early The two projects with the most rapid transition – micro-bubbles and d-dimer targeted antibody. In parallel imaging technologies can add value. D-dimer antibody is good at detecting fresh clots which may be an advantage for thrombolysis. Can identify 0.5 gram clots.
4. Things that might be blue sky and long term investments.

Session Summaries
41
Closing Remarks: Helen Dewey This is the 6th annual retreat and it has been the most successful so far. I particularly liked the format and the level of interaction between the groups. We have had some concrete outcomes which we will take forward. Our strength has been the range of people attending, from our collaborating centres to our core Melbourne group. It has been wonderful to have the CSIRO group contribute to the discussions and we look forward to fruitful collaborations with you. We thank all our interstate collaborators for attending; the Newcastle, Gosford, Sydney and Western Australian groups. We thank Fred Mendelsohn from HFI and our overseas guests from Auckland. For the first time we also have had representation from BRI. We also thank our facilitator, Alan Finkel who has done a wonderful job. Alan Finkel Fascinating, everything described at this retreat has involved a device or a technology. Technology often involves things we want to play with, but the broad debate has contributed a reality check that these things need to be useful. Introducing new technology at Axon Instruments was easier than introducing new technology into the clinic. We sold machines to researchers not only because they provided useful functionality, but partly because they were cool to have. Coolness does not enter into the equation in these stroke scenarios because of the ethical implications that they will be used in humans. It is clear, though, that many of the technologies described in the last two days show a lot of promise for translation into clinical practice. Thanked organisers and Geoff for chairing the last session.

Delegate Details
42
Delegate Details (alphabetically) MS ELENA ALEKSOSKA Position: Technical Assistant Institution: University of Melbourne and NSRI Contact details
Phone: 9496 5635 Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
MS ANA ANTONIC Position: PhD Student Institution: University of Melbourne and NSRI Contact details
Phone: 9496 5635 Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
MS LOUISE BANISTER Position: PhD Student Institution: Latrobe University Contact details
Phone: Address:
DR ALAN BARBER Position: Director & Neurologist, Auckland City Hospital Stroke Service Institution: Auckland City Hospital Contact details
Phone: Address: Level 8, Support Building, Auckland City Hospital
Park Rd, Grafton, Auckland 1001, New Zealand

Delegate Details
43
DR CHRISTOPHER BEER Position: Senior Lecturer and Geriatrician/Clinical Pharmacologist Institution: University of Western Australia and Royal Perth Hospital Contact details Phone: Address: Level 6 48 Murray St PERTH WA 6000 MS ETTIE BEN-SHABAT Position: PhD Student Institution: National Stroke Research Institute Contact details
Phone: 9496 2515
Address: National Stroke research Institute, Repatriation campus - Austin Health, 300 Waterdale Rd. Heidelberg Heights, Victoria 3081 Australia
A/PROF JULIE BERNHARDT Position: Director, AVERT Institution: National Stroke Research Institute Contact details
Phone: 9496 2783 Address: Level 1, Neurosciences building, Heidelberg Repatriation
Hospital , 300 Waterdale Rd, Heidelberg Heights, 3081 PROF CHRISTOPHER BLADIN Position: Co-chair, Australasian Stroke Trials Network
Director, Eastern Melbourne Neurosciences Institution: Box Hill Hospital Contact details
Phone: Address: Box Hill Hospital, Nelson Rd., Box Hill,
Melbourne, 3128, Australia

Delegate Details
44
MS DOMINIQUE CADILHAC Position: Manger Public Health Division, PhD Candidate Institution: NSRI Contact details
Phone: 03 9496 2078 Address: Level 1, Neurosciences building, Heidelberg
Repatriation Hospital, 300 Waterdale Rd, Heidelberg Heights, 3081
PROF MICHAEL CALFORD Position: Professor of Human Physiology and Pro Vice-Chancellor
(Health) Institution: The University of Newcastle
Contact details
Phone: (02) 4921 6378 Address: Faculty of Health, University of Newcastle, Australia Callaghan
Campus, Newcastle, NSW Australia 2308
A/PROF LEEANNE CAREY Position: Principal Research Fellow Institution: National Stroke Research Institute Contact details
Phone: 03 9496 2586 Address: Level 1, Neurosciences building, Heidelberg Repatriation
Hospital, 300 Waterdale Rd, Heidelberg Heights, 3081 PROF ROB CARTER Position: Chair in Health Economics at Deakin University in
the School of Health and Social Development, Institution: The University of Melbourne Contact details
Phone: Address: Deakin University, Faculty of Health Medicine,
Nursing and Science, 221 Burwood Highway, Burwood VIC 3125

Delegate Details
45
A/PROF BRIAN CHAMBERS Position: Head of Ultrasound Research Institution: NSRI Contact details
Phone: Address: Level 1, Neurosciences building, Heidelberg
Repatriation Hospital,300 Waterdale Rd, Heidelberg Heights, 3081
DR GREG COIA Position: Research Fellow Institution: CSIRO Contact details
Phone: Address: Molecular and Health Technologies 343 Royal Parade,
Parkville, Vic 3052 DR JANICE COLLIER Position: Research Fellow Institution: National Stroke Research Institute Contact details National Stroke Research Institute
Phone: 9496 2783 Address: Level 1, Neurosciences building, Heidelberg Repatriation Hospital , 300 Waterdale Rd, Heidelberg Heights, 3081 PROF ALAN CONNELLY Position: Deputy Director & Head MR Physics Institution: Brain Research Institute Contact details
Phone: 9496 4389 Address: Neurosciences Building, Austin Health, Waterdale
Road Heidelberg West, Victoria, 3081
MS SUSAN COX Position: Research Assistant Institution: University of Melbourne (Austin Health),
National Stroke Research Institute

Delegate Details
46
Contact details
Phone: (03) 9496 5635 Address: Howells Lab, Austin Health, Department of Medicine, Lance Townsend Building – Level 7, Studley Road, Heidelberg, VIC 3084 MS BARBARA CRAGGS Position: Medical Student Institution: Contact details
Phone: Address: MS TINA DAFNAS Position: Bristol-Myers Squibb, Representative Institution: Bristol-Myers Squibb Contact details
Phone: Address: Clinical Support Team, Bristol-Myers Squibb,
556 Princes Highway, Noble Park VIC 3174
DR DEIDRE DE SILVA Position: Clinical Research Fellow Institution: Royal Melbourne Hospital Contact details
Phone: Address: Royal Melbourne Hospital, Parkville Vic Australia 3050 A/PROF HELEN DEWEY Position: NHMRC Practitioner Fellow
Head, Inpatient Stroke Services, Austin Health Associate Director, National Stroke Research Institute Associate Professor, Department of Medicine, Austin Health, University of Melbourne
Institution: NSRI and Austin Health Contact details
Phone: 9496-2888 Address: National Stroke Research Institute, Heidelberg Repatriation Hospital, Heidelberg Heights VIC 3081

Delegate Details
47
DR RAJINDER DHAMIJA Position: Clinical Research Fellow Institution: National Stroke Research Institute Contact details: Phone:
Address: Level 1, Neurosciences building, Heidelberg Repatriation Hospital, 300 Waterdale Rd, Heidelberg Heights, 3081
PROF GEOFFREY DONNAN Position: Director, NSRI Institution: National Stroke Research Institute Contact details
Phone: 9496 2699 Address: Level 1, Neurosciences building, Heidelberg
Repatriation Hospital, 300 Waterdale Rd, Heidelberg Heights, 3081
DR MARTIN EBINGER Position: Clinical Research Fellow Institution: Royal Melbourne Hospital Contact details
Phone: Address: Royal Melbourne Hospital, Parkville Vic Australia 3050 MR PETER ELLIS Position: Servier Regional Manager, Victoria Institution: Servier Contact details Phone: Address: Servier Laboratories Pty Ltd, 8 Cato St,
Hawthorn VIC 3121
DR CORALIE ENGLISH Position: Lecturer in Physiotherapy Institution: University of South Australia

Delegate Details
48
Contact Details: Phone: (08) 8302 2552
Address: School of Health Sciences, University of South Australia, City East – Room C7-49,
DR JENNY FAVALORO Position: Senior Research Fellow Institution: Univeristy of Melbourne, Contact details
Phone: Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
DR ALAN FINKEL Position: Executive Publisher Cosmos Magazine Institution: Cosmos Magazine Contact Details: Phone: Address: Cosmos Magazine, Suite 1 level 3,
521 Toorak Rd, Toorak Vic 3142
PROF GRAEME HANKEY Position: Neurologist & Head of the Stroke Unit, Royal Perth Hospital, Clinical
Professor, School of Medicine and Pharmacology, University of Western Australia.
Institution: Royal Perth Hospital Contact Details: Phone: Address: Department of Neurology, Royal Perth Hospital
Wellington Street Campus, GPO Box X2213 Perth, Western Australia, 6847
A/PROF DAVID HOWELLS Position: Associate Director NSRI, Senior Research Fellow, Institution: NSRI
Delegate Details
49
Contact Details: Phone: 9496 3789 Email:
Address: Level 7, LTB Austin Health Studley Rd Vic, 3084
PROF PETER HUDSON Position: CSIRO Research Director for Neurosciences & Molecular
Imaging, Co-founder and Advisor EvoGenix Pty Ltd & AviPep Pty Ltd
Institution: CSIRO Contact Details: Phone: Email:
Address: Neurosciences & Molecular Imaging, 343 Royal Parade, Parkville, Vic 3052
MS LOUISE JAMES Position: Austin Hospital Acute Stroke Care Unit Liaison Nurse Institution: Austin Health Contact Details: Phone: Email:
Address: Austin Hospital Studley Road, Heidelberg, VIC, 3084
MS SIAN JAMISON Position: Boerhinger Ingelheim, Representative Institution: Boerhinger Ingelheim, Contact Details: Phone: Email:
Address: 85 Waterloo Road North Ryde New South Wales Australia 2113 MS AMY JEFFREYS Position: PhD Canditate

Delegate Details
50
Institution: Melb Uni, Dept. Medicine Austin Health, NSRI Contact details
Phone: 94963592 Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
MR SIMON JUDKINS Position: Institution: Austin Health Contact details
Phone: Address: Austin Hospital
Studley Road, Heidelberg, VIC, 3084 MS ROSLYN KELLY Position: Clinical Trials Co-ordinator Institution: National Stroke Research Institute Contact details
Phone Address: Level 1, Neuroscience Building, Heidelberg Repatriation Hospital, 300 Waterdale Rd, Heidelberg Heights, 3081
MS NICOLE KERR Position: Research Assistant Institution: Melb Uni, Dept. Medicine Austin Health Contact details
Phone: 94963592 Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
DR ERIN LALOR Position: CEO, National Stroke Foundation Institution: National Stroke Foundation Contact details
Phone: 9670 1000 Address: Level 8, 99 Queen St Melbourne, Victoria 3000
Delegate Details
51
DR KATHY LEFEVERE Position: CCRE Course and Postgraduate Co-ordinator Institution: Centre of Clinical Research Excellence in
Neurosciences, Department of Medicine, Austin Health, University of Melbourne
Contact details
Phone: (03) 9496 2990 Address: Epilepsy Research Centre, Level 1, Neurosciences
Building, Heidelberg Repatriation Hospital, Austin Health.
MS JESSICA LEUNG Position: Research Assistant Institution: National Stroke Research Institute Contact details: Phone:
Address: Level 1, Neurosciences building, Heidelberg Repatriation Hospital, 300 Waterdale Rd, Heidelberg Heights, 3081
MS CANDACE LOY Position: PhD Student Institution: Melb Uni, Dept. Medicine Austin Health Contact details
Phone: 94963592 Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
DR JOHN LY Position: Clinical Research Fellow, Institution: NSRI Contact details
Phone: Address: Austin Hospital, 3KZ building, Neurology department
DR HENRY MA Position: Clinical Research Fellow, PhD Student Institution: NSRI

Delegate Details
52
Contact details Phone: Address: Austin Hospital, 3KZ building, Neurology department
DR MARK MACKAY Position: Institution: Royal Children’s Hospital Contact details
Phone: Address: Royal Children’s Hospital, Flemington Road, Parkville 3052.
DR RICHARD MANASSEH Position: Research Fellow Institution: CSIRO Contact details
Phone: Address: CSIRO, 343 Royal Parade, Parkville, Vic 3052
DR ROMESH MARKUS Position: Neurologist,
Director, Stroke Care Unit Conjoint Senior Lecturer, University of New South Wales
Institution: St Vincent's Hospital Contact details
Phone: +61 2 8382 3306 Address: Department of Neurology, Level 4 Xavier, St Vincent's
Hospital, 390 Victoria Street, Darlinghurst, Sydney, NSW 2010
MR KEVIN MASCI Position: General Manager, Paramedic Education and Training Institution: Metropolitan Ambulance Service Contact details Phone 03 9840 3302 Address: Metropolitan Ambulance Service, PO Box 2000, Doncaster 3108

Delegate Details
53
PROF FRED MENDELSOHN Position: Director, Howard Florey Institute Institution: Howard Florey Institute Contact Phone: 83441809 Address: Howard Florey Institute, University of Melbourne Victoria 3010 MS TORI O’COLLINS Position: PhD Student Institution: University of Melbourne, NSRI Contact details
Phone: 9496 3257 Address: Neuroscience Lab, Department of Medicine, Level 7,
Lance Townsend Building, Austin Health, Heidelberg DR MARK PARSONS Position: Neurologist, Director of the Acute Stroke Unit at the
Newcastle Mater Hospital
Institution: John Hunter Hospital Contact details
Phone: Address: John Hunter Hospital, Deptartment of Neurology,
Locked Bag 1, Hunter Region Mail Centre NSW 2310. MS DORA PEARCE Position: Biostatistician, PhD Student Institution: NSRI Contact details
Phone: Address: Neurosciences Building, Austin Health, Repatriation
Campus, 300 Waterdale Rd, Heidelberg Heights, VIC 3081
MS SANDRA PETROLO Position: Clinical Trials Co-ordinator Institution: National Stroke Research Institute

Delegate Details
54
Contact details
Phone: 9496 2615 Address: Level 1, Neuroscience Building, Heidelberg
Repatriation Hospital, 300 Waterdale Rd, Heidelberg Heights, 3081
DR MICHELLE PORRITT Position: Research Officer Institution: University of Melbourne, NSRI Contact details
Phone: 9496-5635 Address: Level 7, Lance Townsend Building, Austin Health Studley Road, Heidelberg, VIC 3084
MS SARAH REWELL Position: PhD Student Institution: University of Melbourne and NSRI Contact details
Phone: 9496 5635 Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
MS GEORGIA ROGERS Position: Specialist Representative, Specialised Therapeutics,
Bayer Schering Pharma Institution: Bayer Schering Contact details
Phone: Address: Bayer Schering Pharma, PO Box 3411,
Burnley North Vic 3121 PROF JOHN ROSTAS Position: Professor of Biomedical Sciences, and Deputy Head of Faculty
(Research) Faculty of Health Institution: University of Newcastle Contact details
Phone: (02) 4921 5669 Address: The University of Newcastle, Callaghan, NSW 2308

Delegate Details
55
MS EMILY SENA Position: PhD Student Institution: University of Melbourne and NSRI Contact details
Phone: 9496 5635 Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
MS SAMANTHA SHEPHERD Position: Sanofi Aventis Representative Institution: Sanofi Aventis Contact details
Phone: Address: Sanofi Aventis, Level 1 31 Market Street, South Melbourne
Vic 3205
MS KATE SIDON Position: Research Assistant Institution: University of Melbourne and NSRI Contact details
Phone: 9496 5635 Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
DR KARIN SITTE Position: Business Manager Institute: National Stroke Research Institute Contact Details:
Phone: 9496 2948 Address: Neurosciences Building, Austin Health Repatriation Campus,
300 Waterdale Rd Heidelberg Heights, Vic 3081. DR NEIL SPRATT Position: Neurologist, & Conjoint Senior Lecturer University of Newcastle

Delegate Details
56
Institution: John Hunter Hospital Contact details
Phone: Address: John Hunter Hospital, Deptartment of Neurology,
Locked Bag 1, Hunter Region Mail Centre NSW 2310 DR KATHY STINEAR Position: Research Fellow Institution: University of Auckland Contact details
Phone: Address: Movement Neuroscience Laboratory, University of Auckland,
Private Bag 92019, Auckland 1142, New Zealand
DR JONATHAN STURM Position: Neurologist, Central Coast Health Institution: Gosford Hospital Contact details
Phone: Address: Central Coast Health, Dept of Neurology, Gosford Hospital
PO Box 351,Gosford, NSW 2250 MR BEVIN SWEERTS Position: Senior Specialist Representative, Specialised Therapeutics Institution: Schering Pty Ltd Contact details
Phone: Address: PO Box 3411, Burnley North, VIC, 3121
DR DONALD TOURNIER Position: Research Fellow Institution: Brain Research Institute Contact details
Phone: 9496 4169 Address: Neurosciences Building, Austin Health, Waterdale
Road Heidelberg West, Victoria, 3081
Delegate Details
57
MR ROBERT TRENBERTH Position: Florey Neuroscience Institutes, NSRI, Board Member Institute: National Stroke Research Institute & National Stroke
Foundation Contact details
Phone: Address: P.O. Box 523, Kew, Victoria
DR CHESDA UDOMMONGKOL Position: Clinical Research Fellow Institution: NSRI Contact details
Phone: Address: Austin Hospital, 3KZ building, Neurology department, Studley
Road, Heidelberg, VIC, 3084
DR DAPHNE VOGIAGIS Position: Business Manager Institute: National Stroke Research Institute Contact Details:
Phone: 9496 2948 Address: Neurosciences Building, Austin Health Repatriation Campus,
300 Waterdale Rd Heidelberg Heights, Vic 3081. MS TARYN WILLS Position: PhD Student Institution: University of Melbourne and NSRI Contact details
Phone: 9496 5635 Address: Department of Medicine, Austin Hospital
Level 7, Lance Townsend Building Studley Road, Heidelberg, VIC, 3084
MR DENNIS YOUNG Position: Clinical Trials Manager Institution: NSRI Contact details

Delegate Details
58
Phone: +613 9496 2648 Address: Level 1, Neurosciences Building, Austin Health, 300 Waterdale
Road, Heidelberg Heights, Victoria 3081 DR JORGE ZAVALA Position: Clinical Research Fellow Institution: National Stroke Research Institute Contact details
Phone: 9496 3114 Address: Austin Hospital, 3KZ building, Neurology department,
Studley Road, Heidelberg, VIC, 3084

Retreat Awards
59
The Alpaca Love Award Presented to: Jorge Zavala For demonstrating an undreamt knowledge of alpacas – “my father comes from Peru.”
Fran Drescher “The Nanny” Award Presented to: Leeanne Carey For hyperphasia
The Calvin Klein Award Presented to: Donald Tournier For sartorial splendour demonstrating fractional anisotropy of the shirt tail.
Retreat Awards
60
The Kerry O’Keefe Award Presented to: Alan Barber For saying what others may think but don’t verbalise – “fMRI didn’t add anything.”
The Olivia Newton-John “Let’s Get Physical” Award Presented to: Romesh Markus “I get a work-out nearly every morning.”
The Narcolepsy Award Presented to: Amy G For sustained gelastic seizure 8-12pm. Very long blink by 9am.
The Charlene Award Presented to: Daphne Vogiagis For reputed karaoke skills – “I’ve been to paradise…but I’ve never been to me…”

Retreat Awards
61
The Russel Crowe Gluteus Maximus Award Presented to: Geoff Donnan For observations about Christians and Lions (he only looks like a pussy cat!)
The Jillaroo Award Presented to: Helen Dewey For attempting to round up the speakers – “Do you want to stand on the other side Donald?”
The New Inventors Award Presented to:Alan Finkel For wanting to invent a GPS for the brain.

Memorable quotes
62
Memorable quotes “Do you want to stand on the other side Donald?” Helen Dewey. “I’m quite comfortable here”. Donald Tournier commenting on his position at the centre of the stage. Due to microphone interference from the next room our discussion is interrupted by an enthusiastic speaker commenting about the intricacies of alpaca maintenance. “Lunch today will be in a random location. The location for dinner tonight is also random”. Geoff Donnan, comments on the complication of finding the lunch and dinner venues. “Dinner tonight is where the alpaca people had dinner last night”, Michelle Porritt. “With all due respect Michelle this gives us no extra information, we may have heard from the alpaca people today, but we certainly have not seen them”, Geoff Donnan. “Just pretend that you are a karaoke singer Raj”. Mark Parsons tells Raj Dhamija to speak into the microphone. “My father comes from Peru, so I know all about alpacas”, Jorge Zavala. “This is wishful thinking, but it is going to keep us occupied for a while”, Alan Barber, in response to using white matter tracking to individualise therapies. “I’m surprised that Daphne has not had us at Sovereign Hill panning for gold to raise money for the retreat”, Peter Hudson. “Certainly we are going for world supremacy if possible”, Donald Tournier in response to Geoff challenging him to join the race for a good white matter model. “On your desks you will find a copy of the retreat satisfaction survey. Please fill in and hand in on your way out today. Otherwise, Daphne will be calling you at 6.00pm on Tuesday evening for your responses”, Alan Finkel.

Acknowledgments
63
Once again Prof. Geoff Donnan and A/Prof. Helen Dewey have organized a wonderful and informative retreat program. I thank them both for their direction and guidance. Thank you to our Pharmaceutical Sponsors, without their support this event would not be possible. A special thank you to our facilitator; Dr. Alan Finkel, to our speakers and commentators; Dr. Mark Parsons, Dr. Donald Tounrier, A/Prof. David Howells, Prof. Graeme Hankey, Dr. Chris Beer, Dr. Alan Barber, Prof. Peter Hudson, Dr. Erin Lalor and Prof. Rob Carter, for taking the time to make this year’s retreat program informative and enjoyable. Dr. Donald Tournier provided the front cover picture and Prof. Leeanne Carey sourced it. Ms. Li Chun Quang assisted with the front cover design. Dr. Karin Sitte assisted with the note taking during the retreat sessions. Our retreat photographers were Dr. Karin Sitte and Mr. Roger Meagher. Dr. Neil Spratt organized the retreat awards. Dr. Daphne Vogiagis, NSRI, Retreat Organizer and Commercial Manager.

Publications
64
NSRI 2007 Publications