national safe motherhood and (nsmnh-ltp)
TRANSCRIPT


National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
ANC Ante Natal CareANM Auxiliary Nurse MidwifeBCC Behaviour Change CommunicationBEOC Basic Emergency Obstetric CareCAC Comprehensive Abortion CareCBO Community Based OrganisationCBS Centre Bureau of StatisticsCDP Community Drug ProgrammeCEDAW Convention for the Elimination of Discrimination Against
WomenCEOC Comprehensive Emergency Obstetric CareCHD Child Health DivisionCTEVT Council for Technical Education and Vocational TrainingDACC District AIDS Coordination CommitteeDDA Department of Drug AdministrationDDC District Development CommitteeDHMC District Health Management CommitteeDHS Demographic and Health SurveyDoHS Department of Health ServicesDUDBC Department of Urban Development and Building
ConstructionEDP External Development PartnerEHCS Essential Health Care ServicesENC Essential Newborn CareEOC Emergency Obstetric CareFCHV Female Community Health VolunteerFHD Family Health DivisionFMIS Financial Management Information SystemHEFU Health Economics and Financing UnitHMIS Health Management Information SystemHP Health PostHURDEC Human Resource Development CentreHURIC Human Resource Information CentreIEC Information Education CommunicationIMCI Integrated Management of Childhood IllnessIOM Institute of MedicineKAP Knowledge Attitudes and PracticeLMD Logistics Management DivisionLMIS Logistics Management Information SystemLSGA Local Self Governance Act
List of Acronyms

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
LSI Livelihood and Social InclusionMBBS Bachelor of Medicine Bachelor of SurgeryMDG Millennium Development GoalMOF Ministry of FinanceMOGA Ministry of General AdministrationMoHP Ministry of Health and PopulationMOLD Ministry of Local DevelopmentMPPW Ministry of Planning and Physical WorksMRT Midwifery Refresher TrainingNAN Nursing Association of NepalNNC Nepal Nursing CouncilNEPAS Nepal Paediatric SocietyNESOG Nepal Society of Obstetricians and GynaecologistsNGO Non Government OrganisationNHEICC National Health Education Information Communication
CentreNHTC National Health Training CentreNHSP-IP Nepal Health Sector Programme-Implementation PlanNLSS National Living Standard SurveyNMC Nepal Medical CouncilNSMNH-LTP National Safe Motherhood Newborn Health -Long Term PlanPAC Post Abortion CarePCL Proficiency Certificate LevelPESON Perinatal Society of NepalPHCC Primary Health Care CentrePMTCT Prevention of Mother to Child TransmissionPNC Post Natal CarePPP Public Private PartnershipRH Reproductive HealthRHCC Reproductive Health Coordination CommitteeRHD Regional Health DirectorateRHTC Regional Health Training CentreSBA Skilled Birth AttendantSHP Sub Health PostSMNF Safe Motherhood Network FederationSMNH Safe Motherhood and Newborn HealthSMNSC Safe Motherhood and Neonatal Sub CommitteeSN Staff NurseSSMP Support to the Safe Motherhood ProgrammeTMIS Training Management Information SystemTT Tetanus ToxoidUNFPA United National Fund for Population ActivitiesUNICEF United Nations Children’s FundUSAID United States Agency for International DevelopmentVDC Village Development CommitteeWHO World Health Organisation

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
This revised National Safe Motherhood and Newborn Health Long Term Plan(NSMNH-LTP) 2006-2017 has been developed to be in line with the Second LongTerm Plan Health Plan (1997-2017), the Nepal Health Sector ProgrammeImplementation Plan and Millennium Development Goals (MDG). The revisiontakes into account recent developments such as the increased specific emphasison neonatal health, recognition of the importance of skilled birth attendance inreducing maternal and neonatal mortalities, health sector reform initiatives,legalisation of abortion, recognition of the significant levels of mother to childtransmission of HIV/AIDS and increased emphasis on equity issues in safemotherhood services.
The overall goal of this plan is to improve maternal and neonatal health and survivalespecially among poor and socially excluded communities, with indicators drawnfrom the MDGs. These include a reduction in the maternal mortality ratio to 134per 100,000 live births by 2017 and a reduction in the neonatal mortality ratio to 15per 1,000 live births by 2017.
The purpose is increased healthy practices and utilisation of quality maternal andneonatal health services, especially by the poor and excluded, delivered by awell-managed health sector. The indicators are an increase in the number ofdeliveries assisted by Skilled Birth Attendants (SBA) to 60 percent by 2017 andincrease in the number of deliveries in a health facility to 40 percent by 2017. Metneed for Emergency Obstetric Complication will be increased by 3 percent eachyear and the met need for Caesarean Section by 4 percent each year.
Eight key outputs have been identified, with individual indicators and key activities:
1. Equity and AccessThe purpose is to ensure that individuals, groups and networks are sociallyempowered to practise desired Safe Motherhood and neonatal Health (SMNH)behaviours, leading to increased equity of and access to health services. The keyactivity areas are in advocacy, social mobilisation and behaviour changecommunication.
2. ServicesThe purpose is to enhance equitable provision of quality SMNH services. Theseinclude: focused antenatal care, delivery and newborn care by skilled birthattendant, postnatal care, emergency obstetric care, comprehensive abortion careand referral services. Activity areas include strengthening and expansion of SMNHservices, improvement in quality of services, reaching socially excluded groups,creating an enabling environment for services and developing appropriate linkages.
Executive Summary

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
3. Public Private PartnershipThe purpose is to increase participation of the private sector, NGOs, communitybased organisations and professional/academic institutions in SMNH related publicservices to ensure consumers have equitable access to affordable services.
4. DecentralisationThe purpose is to enhance local government and partner capacity to plan andoversee SMNH services in line with the Local Self Governance Act (LSGA).
5. Human Resource Development: Skilled Birth Attendant StrategyThe purpose is to develop and implement a strategy and plan for human resourcedevelopment in safe motherhood and neonatal health, particularly skilled birthattendant training.
6. Information ManagementThe purpose is to develop a comprehensive sector wide SMNH information baseand to incorporate and utilise this within the Health Information System to supportpolicy, planning, monitoring, evaluation and advocacy at national and local levels.Key activity areas include information management, data collection and quality,access to information and monitoring.
7. Physical Assets and ProcurementThe purpose is to ensure adequate physical resources for SMNH services alongwith year round availability of SMNH related drugs and supplies. Key activity areasinclude construction and maintenance, planning and quality assurance anddistribution of drugs and commodities.
8. FinanceThe purpose is to ensure improved sustainable financing systems for SMNHservices. Key activity areas include mobilisation of resources, alternative financingsystems and formation of safety nets for the socially excluded.
Seven cross cutting issues and approaches were identified, which are commonto all the outputs. These are: social inclusion, gender, rights based approach,research and advocacy, enabling environment, public private partnership anddecentralisation.

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Preface
Acknowledgements
List of Acronyms
Executive Summary
1 Chapter: 1 Introduction and background 1
1.1 Introduction 1
1.2 Rationale for revision of the NSMNH-LTP 1
1.3 The revision process 2
1.4 Goal purpose and outputs 3
1.5 Definition of terms 4
1.6 Cross cutting issues and approaches 4
1.7 Risks and assumptions 6
2 Chapter: 2 Description of outputs 8
Output 1: Equity and access 8
Output 2: Services 9
Output 3: Public private partnerships 11
Output 4: Decentralisation 13
Output 5: Human resource development:
Skilled Birth Attendant Strategy 14
Output 6: Information management 15
Output 7: Physical assets and procurementOutput 8: Finance 16
3 Chapter: 3 The logframe 20
Annexes
Contents

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Introduction and Background
1.1 IntroductionThe overarching goal of development efforts in Nepal is to reduce poverty,as highlighted in the Tenth Plan (Poverty Reduction Strategy Paper) 2002-2007, and health sector development efforts are treated as an integral partof this strategy. The Ministry of Health and Population (MoHP, formerlyMinistry of Health) developed the Second Long Term Health Plan (1997-2017) as a sectoral perspective plan and the National Safe MotherhoodLong Term Plan (NSMLTP) (2002-2017) was based on this document as asub sector plan, in l ine with the Nepal Health Sector ProgrammeImplementation Plan (NHSP-IP) 2004-2009.
Within the health sector, safe motherhood has been a national priority programmefor the last decade, and is highlighted in all major health related policies andplans. The Tenth Plan, the Second Long Term Health Plan and the NSMLTP (2002-2017) all highlight the need to reduce the high levels of mortality among women,infants and children. The Millennium Development Goals (MDG) specify a twothirds reduction in the under-five mortality rate and 75 percent reduction in thematernal mortality ratio by the year 2015. The NHSP-IP draws on the MillenniumDevelopment Goals, with the stated purpose of improving the health status of theNepalese population through utilisation of essential health care services (EHCS),specifying maternal mortality and infant and child mortality reduction among otheressential health care indicators. Since safe motherhood and newborn health arenot purely health issues, they warrant a multi-sectoral approach, and the role ofother sectors is particularly important in enhancing access and promoting equity.This is acknowledged in the NSMLTP and outputs are related to programmes ineducation, information and communication, transport and local development, asappropriate.
The NSMLTP outlines strategic directions and defines the major outputs andgeneral areas of activity, but without a more specific set of activities, detailedcosting is beyond its scope. This will be included on a three-year rolling basis withimplementation planning.
1.2 Rationale for Revision of the National Safe Motherhood LongTerm Plan (NSMLTP 2002-2017)
In recent years many safe motherhood stakeholders, both government and non-government, at district, regional and national forums, have noted gaps in the originalNSMLTP and advocated for its revision and updating. In order to retain itseffectiveness as a guide to programming, the plan needs to be treated as a rollingdocument, and revised regularly, in line with the changing context of newdevelopments. A number of specific issues have been identified that highlight theurgent need for revision as follows:
Chapter 1:
1

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
MDGs and Neonatal health: The NSMLTP (2002-2017) was developed beforethe Millennium Development Goal Country Report was prepared, and so wasunable to fully take into account the recommendations it contained. For example,prior to this little attention had been paid to neonatal health in its own right, but theMDG report highlighted the growing recognition that safe motherhood shouldspecifically incorporate newborn health. The infant mortality rate in Nepal isdeclining but only slowly - child mortality declined by 34 percent between 1996and 2001, but during the same period infant mortality declined by only 18 percent.Since two thirds of infant deaths occur in the neonatal period, significant reductionof infant mortality rates depends on a decrease in the neonatal mortality rate.While it is understood that safe motherhood interventions do contribute to areduction of perinatal and neonatal mortality, in order to achieve the substantialinfant and child mortality reductions encompassed by the MDGs, additional specificnewborn health interventions need to be integrated with safe motherhoodprogramming. The National Neonatal Health Strategy and National Neonatal HealthLong Term Plan formulated in 2004 and 2005 respectively to address neonatalhealth issues had also not been incorporated into the previous plan.
Skilled birth attendance: The original NSMLTP (2002-2017) placed littleemphasis on the importance of skilled birth attendance in the drive to reducematernal and neonatal mortalities. Global standards for what constitutes skilledbirth attendance and how a skilled birth attendant (SBA) is defined have alsochanged significantly in the last few years. The National SBA Policy has been onlyrecently formulated and endorsed, and key points from this need to be incorporatedinto the current plan.
Health sector reform: The NSMLTP (2002-2017) pre-dated the recent work onhealth sector reform and strategy development, and the outputs of Nepal HealthSector Strategy and Nepal Health Sector Programme Implementation Plan (2004-2009) need to be included.
Abortion: The legalisation of abortion under specified conditions in 2002 hasresulted in an intensive programme to establish comprehensive abortion care(CAC) services in public hospitals from 2004 and a commitment to integratingCAC into safe motherhood programming. This important step acknowledges thesignificant effect of complications due to unsafe abortions on the high maternalmortality ratio in Nepal and was not included in the original NSMLTP (2002-2017).
Mother to child transmission of HIV is an increasing problem. As HIV infectionrates grow, this is likely to become major issue in the near future for serviceprovision As it is a recently acknowledged phenomenon, prevention activities arenot mentioned in the original NSMLTP. Prevention of mother to child transmission(PMTCT) needs to be incorporated in the current plan.
Equity issues in access and utilisation of safe motherhood and neonatal health(SMNH) services are not mentioned in the original NSMLTP and are of criticalimportance if the most needy members of society are to be targeted and theMDGs achieved.
1.3 The Revision ProcessRevision of the plan was carried out in three stages, with the participation of multiplestakeholders, both government and external development partners (EDP). Thelist of participants is shown in the annex.
1. A preparatory meeting of potential participants was held in November 2005,to share the rationale for revision and the proposed methodology for the
2

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
process. The meeting determined the parameters, boundaries and broadoutputs and assigned tasks. Working groups for different outputs were formedon the basis of professional expertise, and possible reviewers suggested.
2. In preparation for the first workshop, held in January 2006, consultantsreviewed existing national policies, strategies and plans, to identify the gaps,deficiencies and discrepancies, and prepared a background paper forpresentation at the workshop. Based on this review, an analysis of thestrengths, weaknesses, opportunities and threats of the existing plan wascarried out. The groups then worked to analyse and update the individualoutputs and associated activities for the plan, and presented their ideas in aplenary session for further discussion and refining. By the end of the workshopa first draft revision of the plan had been prepared.
3. Each group met at least twice before the second workshop, which was heldin March 2006. During this period they refined the output statements,developed a full set of activities under each output and agreed on indicatorsand their means of verification. Cross group sharing helped to avoid theduplication and ensure consistency in the plan, and groups consulted withother experts for technical inputs. At the second workshop groups presentedtheir work for comments and suggestions, on the basis of which the draftplan was refined and finalised. Risks and assumptions were developed andgroups drafted a brief narrative of their output.
1.4 Goal, Purpose and Outputs
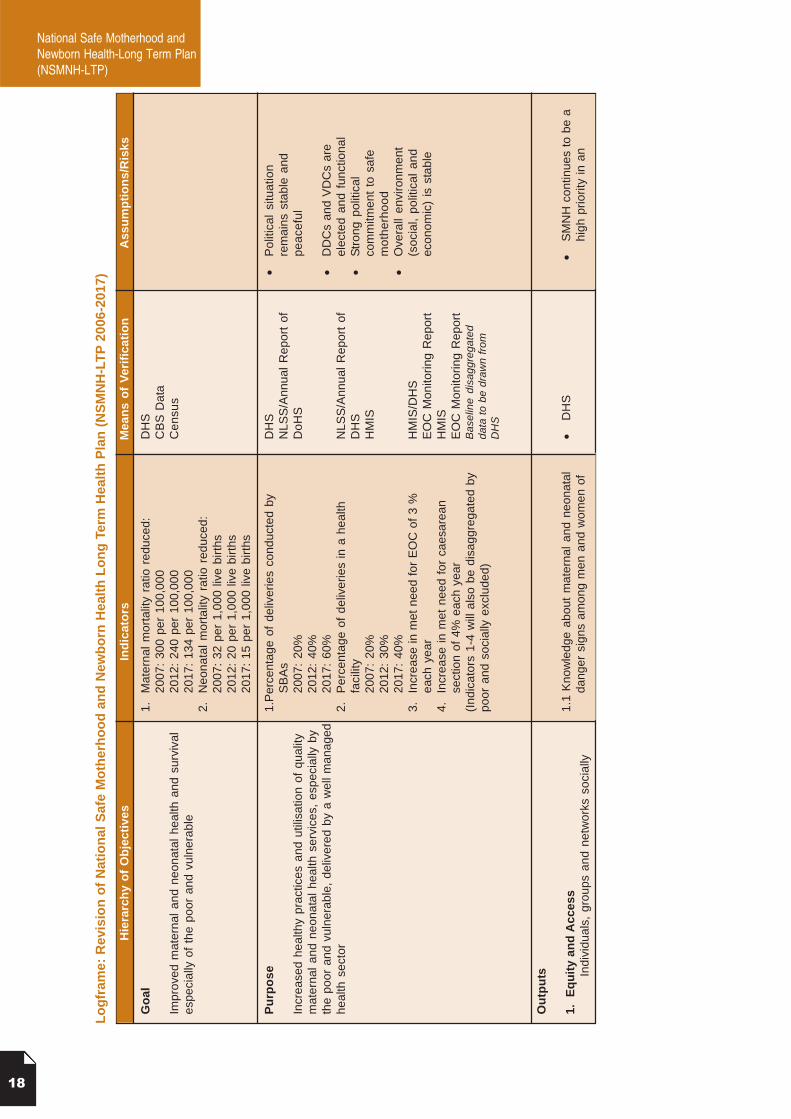
Goal: Improved maternal and neonatal health and survival, especially of thepoor and excluded.
The key indicators for this NSMNH-LTP goal are:
1. A reduction in the maternal mortality ratio from 539 per 100,000 livebirths1 to 134 per 100,000 by 2017
2. A reduction in the neonatal mortality ratio from 39 per 1,0002 to 15per 1,000 by 2017.
Purpose: Increased healthy practices, and utilisation of quality maternaland neonatal health services, especially by the poor and excluded,delivered by a well-managed health sector.
Key indicators for this include:
1. Increase in the percentage of deliveries assisted by an SBA to 60% by 20172. The percentage of deliveries taking place in a health facility increased to
40% by 20173. Increase in met need for emergency obstetric care of 3% per year4. Increase in met need for caesarean section of 4% per year.
Outputs: Eight outputs are specified in the plan, each withindividual indicators.
1. Equity and access2. Services3. Public private partnership4. Decentralisation5. Human resource development: Skilled birth attendant
strategy6. Information management7. Physical assets and procurement8. Finance
1 Nepal Family HealthSurvey 1996
2 Demographic andHealth Survey 2002
3
National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
1.5 Definition of termsIn order to ensure consistency and clarity, technical terms used regularly amongsafe motherhood stakeholders are defined below, as used in this document.
Poor: Classification of poverty is based on the annual expenditure on food andnon-food items. The official poverty line developed for the year 2003/4 by the NepalCentral Bureau of Statistics is a total real per capita consumption of NRs.7,696(approximately US$102) per year3. The food poverty line is based on an energyintake of 2,144 Kcal per person, per day.
Social exclusion; A process and state that prevents individuals or groups fromfull participation in social, economic and political life and from asserting their rights.It derives from exclusionary relationships based on power and may relate to caste,ethnicity, religion or gender status.
Social Inclusion: The removal of institutional barriers and enhancement ofincentives to increase the access of diverse individuals and groups to developmentopportunities (World Bank).
Social empowerment: Improvements in knowledge, attitudes, behaviours,confidence, legal and social status and access to resources, including transportand finance schemes, among individuals, groups and networks. The World Bankdefines empowerment as: The enhancement of assets and capabilities of diverseindividuals and groups to function and to engage, influence and hold accountablethe institutions that affect them.
Enabling environment: The existence of support (physical and social/attitudinal)that promotes and enables desired behaviours or service provision.
Comprehensive abortion care (CAC): Legally available elective induced abortionservice that includes safe techniques (manual vacuum aspiration and effectivepain management), counselling and post procedure contraception services.
1.6 Cross cutting issues and approachesSocial inclusionSocial exclusion, due to caste, ethnicity, age, religion or gender, is a major causeof poverty, affecting access to and utilisation of essential health care services(EHCS). A number of institutional barriers have been identified related to accessand utilisation by these groups, and the Vulnerable Community Development Planwas developed as a part of the Nepal Health Sector Implementation Plan (2004-2009) to directly address these and ensure poor and excluded people haveequitable access to EHCS. This includes increasing the coverage and raising thequality of EHCS, with special emphasis on improved access for poor and excludedgroups. Thus social inclusion has emerged as a major social, economic and politicalpolicy issue, which is high on the agenda of policy makers and planners. SinceSMNH services are a major component of EHCS, the NSMNH-LTP mainstreams socialinclusion as a cross cutting issue in its goal, purpose and all outputs. Related annual planswill specifically address the needs of socially excluded groups, and progress in reachingthem will be monitored by means of disaggregated indicators. Priority will be given toinfrastructural and resource needs in areas serving socially excluded groups, andcommunities will be encouraged to identify and support the training of women from thesegroups as SBAs and create an enabling environment for them to serve their communities.Access activities will encourage self-confidence, voice and agency, especially amongwomen and other socially excluded and vulnerable groups and will engage them in aninclusive and empowering way.
3 Adjusted toNRs.11,057 forKathmandu,NRs.7,901 for otherurban areas,NRs.8,902 for ruralwestern hills,NRs.8,070 for ruraleastern hills,NRs.7,418 for ruralwestern terai,NRs.6,079 for ruraleastern terai.
4

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
GenderAs an excluded group in themselves, and as the key beneficiary targeted by safemotherhood interventions, the needs of women are treated as paramountthroughout the NSMNH-LTP, not simply as individuals, but as members of familiesand communities functioning within complex relationships and social expectations.Gender issues are included as a cross cutting issue and an important part of allthe outputs, but particularly in human resource development and deployment,management approaches and access activities.
Rights based approachHuman rights standards relevant to maternal health include, but are not limited to:
• The right to life and survival• The right to the highest attainable standard of health• The right to decide freely the number and spacing of one’s children• The Convention for the Elimination of Discrimination Against Women
(CEDAW).
The right to life and health through access to essential health care services, andspecifically SMNH services, is thus a basic human right, and one that is denied tocountless women in Nepal. Behind every preventable maternal death lies a failureto assure women’s rights, linked to social issues such as the low status of women,their lack of decision-making power, poor access to information and care, restrictedmobility, early age of marriage, and the low priority and resources given to theirhealth. There are also marked disparities by social group in women’s access toskilled birth attendance and to essential obstetric care. Achieving improved andmore equitable maternal survival will thus require political, social, legal andeconomic actions as well as scaling up technical strategies. Traditional publichealth and health systems approaches must therefore be combined with a humanrights-based approach.
Rights based approaches are therefore included as fundamental and cross-cuttingto all outputs of the NSMNH-LTP, with the aim of increasing accountability formaternal and neonatal health, strengthening local capacity of duty-bearers to fulfilwomen’s rights, strengthening women’s voices and their ability to demand theirrights to maternal health and transforming the distribution of power and resourcesthat maintain inequalities across society, in families, communities and healthsystems.
Research and advocacyImproving the quality and utilisation of evidence in policy and practice can helpsave the lives of mothers and their newborns. Research provides the scientificevidence needed to improve the quality and safety of SMNH services, reducecosts and broaden access. It also informs advocacy, which at central level playsvital role in developing favourable policies and plans and at community level isimportant in raising public awareness of key health and social issues and creatingdemand for services Thus research and advocacy are incorporated as importantcross cutting issues in all outputs of the NSMNH-LTP.
Enabling environmentSimply providing training and facilities or undertaking access activities, are not enoughto ensure women receive high quality SMNH services. An enabling environment isimportant in supporting staff in facilities and motivating them to provide high qualityservices. This means that human resource development must go hand in hand withupgrading of infrastructure, provision of equipment and supplies. An enabling
5

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
environment is also important at community level to support women in making healthyreproductive health choices and carrying them through. It encourages people toutilise health services within any given social context, using local knowledge,perceptions and values, relevant traditional practices, preferences and beliefs toenhance knowledge and awareness. Sensitivity to the effects of the armed conflict,which has already been reported to negatively impact women’s access to SMNHservices will also be important.
1.7 Risks and assumptions
Key assumptions on which the NSMNH-LTP is based include:1. Continuing political commitment to safe motherhood and neonatal care as a
high priority in both policy and programming, including allocation of resources2. Effective and timely execution of the Nepal Health Sector Programme
Implementation Plan3. Social, political and economic stability, enabling activities to be carried out as
planned and resources accessed as needed4. Resolution of the conflict and/or development of effective strategies for working
safely and effectively in conflict affected areas, such as using locally acceptablecommunity workers as bridging people and using rights based messagesand approaches
5. Elected leaders in place in functional district and village developmentcommittees, able to facilitate devolved decision-making, local ownership andaccountability
6. Commitment to local level capacity building and support, combined withdecentralisation, to ensure quality services.
6

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Chapter 2:
Description of the Outputs
The outputs are derived from NHSP-IP and so are closely linked with it. Thisplan however, elaborates the outputs with a focus on maternal and newbornhealth concerns.
Output 1: Equity and Access
Purpose: Individuals, groups and networks socially empowered to practisedesired SMNH behaviours, leading to increased equity of andaccess to health services.
Lead Agency: This output will be led by National Health Education, Informationand Communication Centre (NHEICC) mainly in collaborationand coordination with the Family Health Division (FHD) and ChildHealth Division (CHD) and other relevant Divisions within theDepartment of Health Services, development partners, NGOs,civil society, networks, federations, groups and individuals.
BackgroundIncreasing equity of and access to SMNH services requires changes in national,community and household level behaviours and expectations. This is not onlytrue for preventative and promotive services, but also for timely treatment ofcomplications in which dangerous delays are common. A combination of mutuallyreinforcing approaches - advocacy, social mobilisation and BCC - has provedsuccessful in addressing barriers to services in Nepal. These three approaches,combined with the provision of quality services, will be critical to improving thehealth of mothers and newborns and reducing the three delays responsible for somany maternal and neonatal deaths.
This output will seek to promote gender and social inclusion as cross cuttingissues, and to address equity issues in order to expand the reach of services tothe poor and socially excluded. Specific localised advocacy, social mobilisationand BCC activities, linked to increased availability of services, will address barriersto health services among poor and socially excluded groups. Access activities willwork to encourage self-confidence, voice and agency, especially among womenand other disadvantaged groups and to engage poor and socially excludedcommunities in inclusive and empowering way.
Equity and access outputs will seek to create an enabling environment thatencourages people to utilise health services within any given social context.Activities will advantageously use local knowledge, perceptions and values, relevanttraditional practices, preferences and beliefs to enhance knowledge and awarenessand will be sensitive to conflict issues. Access embraces financial, institutionaland infra-structural factors including, but not limited to, funding, transportation
7

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
and education. It also relies upon positive and welcoming service provider attitudes,trust, honesty, responsiveness, accountability and quality service delivery both atestablished facilities and through outreach programmes.
Activity areas A. AdvocacyAdvocacy will be a key component for increasing equitable access to SMNHservices. In order to ensure coordinated, supported and sustained advocacyactivities, action forums (existing if possible) at national and district levels andcomprising a wide range of government and NGO partners, journalists andthe private sector will be mobilised to develop and implement specific actionplans. Activities will include lobbying for the formation or updating of appropriatepolicies for social empowerment, increased resources for SMNH programmesand provision of at least one telephone in each health facility. The actionforums will raise the profile of SMNH through a range of activities, such aspublishing articles and organising public events. Advocacy will focus at differentlevels through partnerships and collaboration with relevant stakeholders toincorporate the voices of users and providers. This output will be closely linkedwith Output 8, Finance.
B. Social MobilisationSocial mobilisation activities are important for ensuring the involvement of peopleat all levels and obtaining support for safe motherhood activities. Activities will becarried out at national, district and community levels, in collaboration with safemotherhood partners and stakeholders from other sectors (inter and intraministerial, divisional, NGO) and line agencies. The programme will useparticipatory approaches to encourage communities to take ownership of the driveto improve the health of the mothers and newborns. Safe motherhood programmeimplementers will support the strengthening of existing committees. The capacityof community groups and networks will be enhanced to create and utilisesustainable emergency funds and transportation schemes. Referral systems willbe supported at all levels (linking with Output 2, Services).
C. Behaviour Change Communication (BCC)BCC informs people about safe motherhood and neonatal health issues and theservices available and promotes positive behaviours. Mass media, local mediaand inter-personal communication will be used to disseminate and reinforcemessages. BCC strategies will ensure that consistency of messages is retainedthrough all channels used, so that people are able to understand messages withintheir own context and act on the information received. There will be a strong focuson using localised approaches to cater to the needs of different target audiences,particularly reaching out to poor and socially excluded communities. BCCinterventions will need to go hand in hand with service availability, and will thereforebe closely linked with Output 2, Services.
The Safe Motherhood Information Education Communication (IEC) strategy (2003-2008) will be updated to incorporate research-based and standardised messages.It will be implemented through focused communication interventions that reachout to poor and socially excluded groups. Rights-based approaches will be usedto promote service utilisation, especially skilled attendance at childbirth, and reduceviolence against women. There will be an increased emphasis on birthpreparedness and complication readiness as well as renewed attention toenhancing positive non-discriminatory interpersonal communication betweenproviders and clients. Cost sharing initiatives will be promoted as appropriate,linked with Output 8, Finance.
8

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Output 2: Services
Purpose: Enhanced and equitable provision of quality maternal andneonatal health services
Lead agency: This output will be led by FHD, with support from the LogisticsDivision, Management Division, National Health Training Centre(NHTC), NHEICC, CHD, hospitals and PHCCs, concerned lineministries, external development partners and relevantprofessional organisations.
BackgroundThe aim of Output 2 is to make quality essential SMNH services equitablyaccessible for all women and their newborns, through functioning and well-managed public health facilities that provide services at all levels (from tertiaryreferral hospitals to community based outreach services) and are linked througheffective referral services. Essential SMNH services include: focused antenatalcare; skilled attendance at birth; newborn care; post-natal care, including familyplanning services; Basic and Comprehensive Emergency Obstetric Care (B/CEOC), including post-abortion care; comprehensive abortion care; and effectivereferral services. Close linkages will be established with Output 1, Equity andAccess activities in order to meet the needs of poor and socially excludedpopulations. Decentralisation of responsibilities to district and community levelsand development of appropriate public/private partnerships will be key strategiesin planning and programming. Professional organisations, such as the NepalSociety for Obstetricians and Gynaecologists (NESOG), Nursing Association ofNepal (NAN), Nepal Medical Association and Nepal Medical Council (NMC), willbe important partners, and linkages with other reproductive health related initiativeswill be developed as appropriate.
Advocacy efforts, through community level health service providers, will focusparticularly on the importance of skilled birth attendance and healthy practices formothers and newborns. At policy level, evidence based lobbying techniques willbe used to influence decision-makers in addressing issues related to equitableaccess to quality SMNH services for all women, particularly those in remote anddisadvantaged areas.
Activity AreasA. Strengthening and expansion of quality SMNH servicesA strategy will be developed and implemented for the phased strengthening andexpansion of quality SMNH services at all levels (especially the number and qualityof B/CEOC sites and birthing centres), including monitoring of services with five-yearly reviews.
It is recognised that the majority of women still give birth at home and are not ableto travel to health facilities for delivery or other essential SMNH services, and thiswill continue to be the case for some time. It is therefore essential to ensure thatSMNH care is available at community level through home visits and outreachclinics, and appropriate health posts and sub health posts are developed aseffective local facilities, with support provided for community level initiatives.
B. Linkages and integration with other reproductive health initiativesTo ensure the provision of complete SMNH services for all women and theirnewborns, neonatal care, family planning services, CAC, PMTCT and malariatreatment will be integrated with safe motherhood services through the developmentof improved linkages between relevant government ministries, divisions andprogrammes (the Female Community Health Volunteer (FCHV), Family Planning,HIV/AIDS and Malaria programmes) and appropriate external developmentpartners. Close links will also be maintained with health related IEC/BCC activities
9

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
under the NHEICC (Output 1, Equity and Access). Joint planning, implementationand monitoring of activities at all levels will be promoted.
C. Quality of servicesThe quality of care provided in health facilities (including private and NGO) and atcommunity level will be improved through a range of interventions that focus ondevelopment and implementation of national standards, training and capacitybuilding for staff and community workers, effective monitoring and support systemswith on site coaching and development of an enabling environment to supportstaff and community volunteers in their work. Institutionalisation of monitoring willbe addressed through local quality of care teams.
D. Enabling environmentThe development of an enabling environment that encourages health workers atall levels to strive for high standards and take responsibility for the services theyprovide will be promoted through: evidence-based lobbying for appropriate policiesand programmes; improving logistic support, infrastructure quality and humanresource deployment; supporting and capacity building local health managementcommittees; encouraging socially inclusive local participation in health facilitymanagement; and promoting the concepts of accountability and the pursuit ofexcellence. Links with the SBA policy and programme will be improved.
E. Poor and socially excluded groupsSocially and economically excluded groups are also the hardest to reach because,in addition to their poverty and low education levels, they often live in areas thatare geographically remote and/or severely affected by the armed conflict. Thesegroups will be identified through equity and access programmes and communitybased volunteers and organisations, and innovative approaches used to prioritisethem in planning appropriate SMNH activities, such as cost sharing and subsidysystems, which increase their access to services. The use of facilities by sociallyexcluded groups will be monitored and the results used in programme planning(linked with Output 1, Equity and Access).
F. Referral systemsWhen complications occur, an effective referral system is essential to enablewomen and their newborns to receive appropriate and high quality emergencycare as quickly as possible. At service level, efforts to improve the effectiveness ofthe system will focus on ensuring 24-hour availability of skilled staff with essentialdrugs and equipment, good community and inter-facility linkages and feedbacksystems to promote further improvements. Remote areas present an even greaterchallenge and require additional focused efforts, which will be covered by districtspecific strategies.
Output 3: Public Private Partnership
Purpose: Increased participation of the private sector, NGOs, communitybased organisations and professional/academic institutions inSMNH related public services to ensure consumers haveequitable access to affordable services.
Lead agency: This output in relation to SMNH will be led by Department ofHealth Services with the shared responsibilities of Family HealthDivision and Child Health Division (for SMNH services),Management Division (regulation, and information) and NationalHealth Training Centre (for trainings) Other support Agencieswill include: Federation of Nepal Chamber of Commerce andIndustries (FNCCI), the Organisation of Private Hospitals andNursing Homes, Universities and the NGO CoordinationCommittee (NGOCC).
10

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
BackgroundIn recognition of the limitations posed by financial and human resource constraintswithin the public health sector, the government is actively promoting the formationof new partnerships between the public and private or NGO sectors andprofessional/academic institutions, in order to ensure the provision of the widestpossible choice of high quality health services and effective human resourcedevelopment. In this way a range of different skills and resources can be madeavailable to support government efforts to improve the health status of womenand their newborns across the country. Public private partnership is a cross cuttingapproach, which can contribute to all other outputs in this plan.
Activity areasDespite the stated policy promoting public private partnerships within the healthsector, the lack of appropriate legal regulatory frameworks and guidelines meansthere has been little discernable progress. This is particularly important to ensurepartnerships are able to contribute to increased SMNH service provision and accessfor poor and socially excluded groups, who will be a key target. Activities for thisoutput will therefore focus on mainstreaming public private partnership initiativesat both policy and implementation level through the establishment of arepresentative regulatory body at MoHP. Appropriate legal frameworks andprotocols will be developed and mechanisms for joint planning and monitoringestablished. District level institutions will be encouraged to identify and establishlocal partnerships.
Output 4: Decentralisation
Purpose: Enhanced local government and partner capacity to plan andoversee SMNH services in line with the Local Self GovernanceAct (LSGA).
Lead agency: This output will be led by the Policy, Planning and InternationalCooperation Division (PPICD) of MoHP. Other support agenciesinclude the Ministry of Local Development and the District andVillage Development Committee Federations.
BackgroundSince most people access health services at local level, devolution of decision-making and promotion of local accountability is the most effective way of ensuringthat high quality services are available and accessible when needed for all sectorsof society. This requires the active involvement of local communities and enhancedcapacity of responsible local institutions, combined with effective communicationand information sharing. Decentralisation is a cross cutting issue, with the potentialto positively contribute to all other outputs in this plan, but its achievement will relyheavily on the overall decentralisation of health services.
Activity areasThe current decentralisation policy is expected to enhance the participation oflocal stakeholders in SMNH service provision and monitoring and increaseequitable access to these services. The activities of this output will aim to clarifythe roles and responsibilities of stakeholders in local level SMNH service provision,raise public awareness of the devolution of services and facilitate informationsharing to promote public accountability and coordination at all levels. Capacitybuilding will be provided for local institutions and line agencies to ensure maximumefficiency. There will be a particular focus on issues relating to poor and sociallyexcluded groups.
12

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Output 5: Human Resource Development: Skilled BirthAttendant Strategy
Purpose: Strategy/plan for human resource development in safemotherhood and neonatal health, particularly skilled birthattendant training, developed and implemented.
Lead agencies: This output will be lead by NHTC and MoHP. Support will beprovided by the Human Resource Development/Skilled BirthAttendant forum, which has representation from FHD, NepalNursing Council (NNC), NMC, NAN, NESOG, JHPIEGO,WHO, UNFPA, Support to the Safe Motherhood Programme(SSMP), Institute of Medicine (IoM), Council for TechnicalEducation and Vocational Training (CTEVT) and other keystakeholders involved in human resources development.
BackgroundGlobal evidence shows that skilled attendance during childbirth is a critical factorin saving the lives of mothers and their newborns. National human resourcedevelopment efforts in SMNH are therefore focusing on increasing the number ofhealth care providers competent to provide skilled birth attendance across Nepaland ensuring they possess the internationally defined set of skills required for askilled birth attendant. In order to promote service availability for poor and sociallyexcluded groups, efforts will be made to support the training of women from minoritygroups and remote areas and encourage them to serve their communities.Otherhealth workers, such as health assistants and auxiliary health workers, who alsoplay a key role at local level in saving the lives of mothers and newborns will betrained and encouraged to provide obstetric first aid. All training curricula willincorporate client friendly and gender sensitive approaches in order to promotean enabling environment for women to access SMNH services. Human resourcedevelopment needs to be combined with upgrading of Health infrastructure,provision of equipments and supplies to ensure quality service delivery, and forthis links will be made with Output 7, Physical Assets and Procurement. Publicprivate partnership approaches (link with Output 3) will also be explored forcontracting out of human resource development retention where appropriate.
Activity areas A. Human Resource Development PlanNHTC will take a lead role in developing an up coming Periodic Human ResourceDevelopment Plan to support National Periodic Plan. The aim of this plan will beto ensure 24-hour availability of SBAs, with required human resource mix for qualitySMNH services. The plan will also look at broader human resource managementrelated issues including geographical considerations for deployment, retentionand career advancement of staff. The plan will also encourage health facilitymanagement committees to recruit the required number of staff, including SBAs,to deal with the increased number of births and the demands for other reproductivehealth services and ensure continuum of care. Appropriate human resource foranaesthesia will be developed for CEOC services.
B. Skilled Birth Attendant Development StrategyThe SBA Development Strategy will identify, upgrade and accredit SBA trainingsites in order to produce the required number of SBAs as quickly as possible. Apublic-private-community partnership approach will be promoted to identify potentialSBAs, support their training, deploy and retain them through the creation of anenabling environment for them in the community. The Nepal Medical Council and
12

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Nursing Council will approve an updated SBA training package (in-service andpre-service) in order to formalise the accreditation and licensing of SBAs. Specialconsideration will be given to recruiting and training health workers from the poorand socially excluded groups. Upgrading the skills of medical graduates (MBBS)for caesarean section will be done considering the importance and availability ofCEOC services at district level.
Output 6: Information Management
Purpose: A comprehensive sector wide SMNH information basedeveloped, incorporated and utilised within the HealthInformation System to support policy, planning, monitoring,evaluation and advocacy at national and local levels.
Lead agencies: This output will be led by the Health Management InformationSystem (HMIS) Section working with the Management Divisionand FHD of the DoHS and with support from the PPICD andMonitoring and Evaluation Division of the MoHP.
BackgroundThe HMIS provides an essential link in the work of all other divisions and sectionswithin the DoHS and MoHP and other stakeholders in the health sector. Theinformation stored underpins and supports all the other outputs within this plan, andforms basis for developing an understanding of cross cutting issues, such as ethnicity,caste, poverty and the effects of the armed conflict. In order to play this vital roleeffectively, the database needs to be comprehensive in its coverage, well managedand accessible, with reliable and accurate information collected from a range ofsources, such as facility based data, surveys and other research. It is also importantto ensure that this resource is known about so that it can be utilised to supportadvocacy efforts and ensure key issues and linkages are identified.
Activity areasA. Information Management StrategyAn Information Management Strategy for SMNH will be developed to improve thecollection of and access to reliable SMNH related data, and its use in evidence-based policy making, planning and advocacy work.
B. Data collection and qualityThrough the HMIS and/or surveys, health and service utilisation data will becollected and analysed in relation to ethnicity, cast and wealth. To supplementquantitative data, additional information will be collected through qualitative studiesusing a range of different tools, such as key informant monitoring. Exercises toverify data and increase its reliability will be designed and implemented. Informationwill be collected for maternal and newborn deaths from health institutions incollaboration with FCHVs.
C. Access to informationEfforts will be made to ensure that information is available to stakeholders at alllevels, including within communities, and orientation and capacity building will beprovided to increase their understanding of key SMNH issues. Public privatepartnerships and relationships will be explored to increase the flow of informationboth to and from HMIS.
D. MonitoringThe quality of monitoring will be improved through the provision of training in SMNHprogramme monitoring approaches. New and innovative monitoring tools, such askey informant monitoring, will be designed and implemented as appropriate.Strengthening of monitoring SMNH services at health institution level will be initiated.
13

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Output 7: Physical Assets and Procurement
Purpose: Adequate physical resources for SMNH services with year roundavailability of MNH related drugs and supplies.
Lead agency: This output will be led by the Director General of the DoHS andRegional Health Directorates (RHD).
BackgroundAvailability of and access to high quality SMNH services is strongly dependent onthe provision of adequate physical resources and infrastructure, which also impactson staff morale and performance and on public perceptions of quality of service.Output 7 is therefore an important pillar on which other efforts rest. In the pastthere have been shortcomings in both infrastructural development/maintenanceand in the management of resources and essential supplies. This will be addressedthrough the establishment of improved systems for planning, monitoring and recordkeeping, and development of appropriate linkages with other relevant outputsand stakeholders.
Activity areasA. Inventory of MNH facilities and equipmentAn inventory of all government health facilities, by district, will be prepared, includingzonal, regional and district hospitals, Primary Health Care Centres (PHCC), HealthPosts and Sub Health Posts (SHP). Details of land ownership, age of buildings,type of construction and area, existing condition and available support serviceswill be recorded. A separate equipment inventory, stating the type, quantity andcondition of equipment, will be prepared for each facility.
B. Development, renovation and maintenance of physical resourcesSelection of sites for infrastructure development and upgrading will be need basedrather than resource based, taking into account equity and efficiency concernsand using agreed and approved criteria. Priority will be given to upgrading SHPsto birthing centres in order to promote community level service availability. Allphysical resources development work will be closely linked with Output 5, HumanResource Development.
A building and equipment maintenance policy will be developed, with coordinationbetween the DoHS and the Department of Urban Development and BuildingConstruction (DUDBC) and support from external development partners. This willguide the annual plan for infrastructure development and equipment.
C. Planning, implementation and quality assuranceNeed assessment, planning, design and implementation of health facilityimprovements will be carried out in consultation with users and other stakeholders,including inputs from expert advisers. Regular monitoring will be included in theprocess through a monitoring committee comprising representatives from relevantgovernment divisions, external development partners, users and otherstakeholders, chaired by the Director General, DoHS to assure quality ofconstruction and equipment.
Quality assurance procedures and compliance testing of drugs (through DDA,LMD and private laboratories) will be strengthened. Commodity distribution willbe improved through decentralised decision-making and strengthenedmanagement systems. Where possible, commodities will be delivered directly tosites, rather than through central stores.
14

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
A joint planning mechanism between FHD, LMD and CHD will be developed forequipment, drug and commodity procurement planning, implementation andmonitoring. A similar joint planning mechanism between MoHP, Ministry of Planningand Physical Works (MPPW) and MD will be developed for infrastructuredevelopment and maintenance work. Procurement mechanisms will be improvedby reforming MoHP procurement policies and capacity building at local and centrallevels.
D. Database, protocols and distribution channels for drugs and commoditiesA national level database of SMNH drug suppliers will be prepared, incorporatingdistribution channels such as means of transportation and storage facilities. Theauthority for purchasing commodities will be transferred to districts (where privatesuppliers can guarantee price and availability) while maintaining nationallynegotiated prices, both for government and sanctioned NGO and externaldevelopment partner facilities. This will gradually reduce the need for LMD todistribute drugs to districts.
In order to improve resource utilisation and information systems available todecision-makers, the Logistics Management Information System (LMIS) will bestrengthened through selective decentralisation of data processing to the districtlevel, inclusion of all SMNH commodities in the LMIS and a review of reportingmechanisms.
Rational use of drugs will be promoted through the use of the SMNH treatmentprotocol and drug financing schemes will be supported, linked with Outputs 2 and8 respectively.
Output 8: Finance
Purpose: Sustainable financing system improved for Safe Motherhood andNeonatal Health Services.
Lead agency: This output will be led by the Health Economics and FinancingUnit (HEFU), of the MoHP.
BackgroundThe emphasis of this output is on establishing a system to support a sustainablefinancing base for SMNH activities. This includes identifying and mobilising financialresources, ensuring their effective utilisation, looking at innovative approaches tofinancing, particularly at local level, and encouraging users and other partners todevelop supportive linkages that may include financing or other cost saving inputs.Where possible, initiatives promoting self sufficiency will be promoted, but specificsystems will be put in place to ensure the needs of poor and socially excludedgroups are catered for.
Activity areas A. Increasing and mobilising resources for SMNHWith assistance from the health sector support programme, financial resourcegaps will be identified, and the evidence used for lobbying and advocacy to increaseresource allocation for SMNH (linked with Outputs 1 and 6, Equity Access andInformation respectively). Resource allocation formula, capacity building/trainingand financial management information systems will be improved through thecollaborative efforts of HEFU the Finance Section DoHS, and HMIS. The privatesector (both for profit and not for profit) will be encouraged to increase inputs toMNH services (linked with Output 3, Public Private Partnerships), under appropriateregulation. The cost-sharing scheme will be implemented and promoted with theactive participation of local bodies, civil society, and NGOs.
15

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
B. Promoting alternative financing schemesThe community health insurance scheme developed under the health sectorsupport programme, which includes safe delivery and emergency obstetric andneonatal care services, will be expanded, and health cooperatives will be promotedwith the collaboration of HEFU, Management Division and FHD. Alternativefinancing schemes will be promoted, such as revolving community emergencyfunds to increase access to services for maternal and neonatal emergency cases(linked with Output 1, Equity Access). District based external development partnerprogrammes, community organisations and other local bodies will facilitate andmonitor emergency funds with the support of MoHP, Ministry of Local Development(MoLD), and Ministry of Women Children and Social Welfare.
C. Safety net for poor and socially excluded groupsSystems are necessary to protect poor and socially excluded groups and ensuretheir ability to access services. Mechanisms to achieve this will be furtherdeveloped and improved, working with the health sector support programme totest new mechanisms of financing (linked with Output 1, Equity Access). MoHPwill provide guidelines regarding user fees and safety net arrangements for poormothers and their newborns. The DoHS will monitor implementation, with supportfrom the Regional and District Health Offices (link with Output 2, Services).
Explanatory notesBasic Emergency Obstetric CareThis includes, administering parental antibiotics, oxytocic drugs andanticonvulsants, performing manual removal of placenta, use of manual vacuumaspiration and assist vaginal delivery with vacuum /forceps
Comprehensive Emergency Obstetric CareThis includes all the six components of BEOC and provision of surgery (caesareansection) and blood transfusion.
Essential SMNH servicesThese include: focused antenatal care; skilled attendance at birth; newborn care;post-natal care, including family planning services; Basic and ComprehensiveEmergency Obstetric Care (B/CEOC), including post-abortion care; comprehensiveabortion care; and effective referral services.
Definition of skilled birth attendant (SBA)“An accredited health professional-such as a midwife, doctor or nurse-who hasbeen educated and trained to proficiency in the skills needed to manage normal(uncomplicated) pregnancies, childbirth and the postnatal period and in theidentification, management and referral of complications in women and newborns(WHO)
16

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Chapter 3: Logframe
National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Lo
gfr
ame:
Rev
isio
n o
f N
atio
nal
Saf
e M
oth
erh
oo
d a
nd
New
bo
rn H
ealt
h L
on
g T
erm
Hea
lth
Pla
n (
NS
MN
H-L
TP
200
6-20
17)
Go
al
Impr
oved
mat
erna
l and
neo
nata
l hea
lth a
nd s
urvi
val
espe
cial
ly o
f th
e po
or a
nd v
ulne
rabl
e
1.M
ater
nal
mor
talit
y ra
tio r
educ
ed:
2007
: 30
0 pe
r 10
0,00
020
12:
240
per
100,
000
2017
: 13
4 pe
r 10
0,00
02.
Neo
nata
l m
orta
lity
ratio
red
uced
:20
07:
32 p
er 1
,000
live
birt
hs20
12:
20 p
er 1
,000
live
birt
hs20
17:
15 p
er 1
,000
live
birt
hs
DH
SC
BS
Dat
aC
ensu
s
Pu
rpo
se
Incr
ease
d he
alth
y pr
actic
es a
nd u
tilis
atio
n of
qua
lity
mat
erna
l an
d ne
onat
al h
ealth
ser
vice
s, e
spec
ially
by
the
poor
and
vul
nera
ble,
del
iver
ed b
y a
wel
l man
aged
heal
th s
ecto
r
1.P
erce
ntag
e of
del
iver
ies
cond
ucte
d by
SB
As
2007
: 20
%20
12:
40%
2017
: 60
%2.
Per
cent
age
of d
eliv
erie
s in
a h
ealth
faci
lity
2007
: 20
%20
12:
30%
2017
: 40
%3.
Incr
ease
in m
et n
eed
for
EO
C o
f 3
%ea
ch y
ear
4.In
crea
se in
met
nee
d fo
r ca
esar
ean
sect
ion
of 4
% e
ach
year
(Ind
icat
ors
1-4
will
als
o be
dis
aggr
egat
ed b
ypo
or a
nd s
ocia
lly e
xclu
ded)
DH
SN
LSS
/Ann
ual
Rep
ort
ofD
oHS
NLS
S/A
nnua
l R
epor
t of
DH
SH
MIS
HM
IS/D
HS
EO
C M
onito
ring
Rep
ort
HM
ISE
OC
Mon
itorin
g R
epor
tB
asel
ine
disa
ggre
gate
dda
ta t
o be
dra
wn
from
DH
S
•P
oliti
cal
situ
atio
nre
mai
ns s
tabl
e an
dpe
acef
ul
•D
DC
s an
d V
DC
s ar
eel
ecte
d an
d fu
nctio
nal
•S
tron
g po
litic
alco
mm
itmen
t to
saf
em
othe
rhoo
d•
Ove
rall
envi
ronm
ent
(soc
ial,
polit
ical
and
econ
omic
) is
sta
ble
Ou
tpu
ts
1.
Eq
uit
y an
d A
cces
sIn
divi
dual
s, g
roup
s an
d ne
twor
ks s
ocia
lly
1.1
Kno
wle
dge
abou
t m
ater
nal
and
neon
atal
dang
er s
igns
am
ong
men
and
wom
en o
f•
DH
S•
SM
NH
con
tinue
s to
be
ahi
gh p
riorit
y in
an
Hie
rarc
hy
of
Ob
ject
ives
Ind
icat
ors
Mea
ns
of
Ver
ific
atio
n
Ass
um
pti
on
s/R
isks
18

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
empo
wer
ed t
o pr
actis
e de
sire
d S
MN
H b
ehav
iour
sle
adin
g to
incr
ease
d eq
uity
of,
and
acce
ss t
ohe
alth
ser
vice
s.
(Soc
ial
empo
wer
men
t in
clud
es i
mpr
ovin
g kn
owle
dge
attit
udes
, be
havi
ours
, co
nfid
ence
, le
gal
and
soci
alst
atus
and
acc
ess
to r
esou
rces
, in
clud
ing
tran
spor
tan
d fin
ance
sch
emes
, of
indi
vidu
als,
gro
ups
and
netw
orks
)
repr
oduc
tive
age,
inc
ludi
ng d
isad
vant
aged
grou
ps,
incr
ease
d to
80%
by
2017
.1.
2 M
en a
nd w
omen
of
repr
oduc
tive
age,
incl
udin
g di
sadv
anta
ged
grou
ps,
able
to
iden
tify
B/C
EO
C s
ites
and
SB
As
incr
ease
dto
80%
by
2017
1.3
Des
ired
chan
ge in
tar
gete
d K
AP
am
ong
men
and
wom
en o
f re
prod
uctiv
e ag
e(r
elat
ed t
o fo
cuse
d A
NC
, P
NC
EO
C,
EN
C,
PA
C a
nd C
AC
)1
1.4
Per
cent
age
of p
eopl
e pr
actis
ing
birt
hpr
epar
edne
ss a
nd c
ompl
icat
ion
read
ines
sin
crea
sed
to 7
0% b
y 20
171.
5 C
omm
uniti
es (
war
ds)
havi
ng s
usta
inab
leem
erge
ncy
fund
s an
d tr
ansp
orta
tion
sche
mes
incr
ease
d to
70%
by
2017
•P
erio
dic
surv
eys
both
qua
litat
ive
and
quan
titat
ive
•H
MIS
•D
HS
•D
oHS
ann
ual
repo
rt
Nat
iona
l KA
P S
urve
y2
emer
ging
sec
tor
wid
e fr
amew
ork
even
afte
r 20
09•
Har
mon
isat
ion
and
coor
dina
tion
amon
gS
MN
H s
take
hold
ers
2.S
ervi
ces
Enh
ance
d an
d eq
uita
ble
prov
isio
n of
qua
lity
SN
MH
serv
ices
(Ess
entia
l S
MN
H s
ervi
ces
incl
ude:
foc
used
AN
C,
deliv
ery
by s
kille
d bi
rth
atte
ndan
t w
ith n
ewbo
rn c
are,
PN
C,
EO
C,
CA
C s
ervi
ces
and
refe
rral
ser
vice
s)
2.1
Per
cent
age
of H
Ps
prov
idin
g no
rmal
deliv
ery
serv
ices
and
new
born
car
e in
line
with
nat
iona
l st
anda
rds
2007
: 10
%20
09:
15%
2012
: 3
0%20
17:
70%
2.2
Per
cent
age
of P
HC
Cs
prov
idin
g B
EO
C,
incl
udin
g ne
wbo
rn c
are
and
CA
Cse
rvic
es.
(Bas
elin
e: 9
% i
n 20
04/5
)20
07:
20%
2009
: 40
%20
12:
60%
2017
: 80
%
2.3
Num
ber
of d
istr
icts
pro
vidi
ng C
EO
C,
new
born
car
e an
d C
AC
ser
vice
s(in
clud
ing
priv
ate
sect
or)
(B
asel
ine:
26
in20
04/5
)20
07:
3120
09:
3720
12:
47
•Adm
inis
trative r
eco
rds
•Periodic
superv
isio
nre
port
s•
HM
IS•
DH
S•
DoH
S a
nnual re
port
s•
FH
D r
eco
rds
•Stu
dy/S
urv
ey r
eport
s
�Continuin
g p
olit
ical
com
mitm
ent
and
reso
urc
es
for
safe
moth
erh
ood a
s a
priority
�Com
mitm
ent
and
reso
urc
es
for
loca
lca
paci
ty b
uild
ing in
health m
anagem
ent
as
a p
art
of
dece
ntr
alis
ation e
ffort
s
�D
evelo
pm
ent
of
safe
and e
ffect
ive w
ays
of
work
ing in c
onflic
t-aff
ect
ed a
reas
1 S
pe
cifi
c in
dic
ato
rs r
ela
ted
to
th
e i
nd
ica
tors
are
: A
NC
- %
of
pre
gn
an
t w
om
en
wh
o r
ece
ive
4 f
ocu
sed
AN
C c
he
cku
ps
(wit
h T
T,
iro
n s
up
ple
me
nta
tio
n,
de
-wo
rmin
ga
nd
co
un
sell
ing
fo
r d
an
ge
r si
gn
s);
EO
C –
kn
ow
led
ge
of
da
ng
er
sig
ns,
id
en
tifi
cati
on
of
loca
l S
BA
an
d w
he
re t
o g
o i
n c
ase
of
em
erg
en
cy;
PN
C -
% o
f w
om
en
wh
ore
ceiv
e a
t le
ast
3 f
ocu
sed
PN
C c
he
cku
ps
(iro
n s
up
ple
me
nta
tio
n,
vita
min
A,
cou
nse
llin
g f
or
da
ng
er
sig
ns
an
d c
on
tra
cep
tive
se
rvic
es)
; E
NC
- %
of
po
stn
ata
l w
om
en
wh
o k
no
w t
o w
ait
fo
r a
t le
ast
24
ho
urs
to
ba
the
th
eir
ne
wb
orn
an
d t
o k
ee
p i
t w
rap
pe
d a
nd
wa
rm;
PA
C -
% a
cce
pta
nce
of
po
st p
roce
du
re c
on
tra
cep
tio
n;
CA
C-
% o
fw
omen
who
kno
w le
gal c
ondi
tions
for
saf
e ab
ortio
n an
d w
here
to
go f
or s
ervi
ces.
2 N
atio
nal K
AP
Sur
vey
2006
, N
HIE
CC
19

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
2017
: 60
2.4
CA
C s
ervi
ces
avai
labl
e in
all
dist
rict
hosp
itals
by
2009
3.P
ub
lic P
riva
te P
artn
ersh
ip
Incr
ease
d pa
rtic
ipat
ion
of p
rivat
e se
ctor
, N
GO
s, C
BO
san
d pr
ofes
sion
al /
aca
dem
ic i
nstit
utio
ns i
n pu
blic
serv
ices
(S
MN
H r
elat
ed)
whi
ch e
nsur
es c
onsu
mer
sha
ve e
quita
ble
acce
ss t
o af
ford
able
ser
vice
s.
3.1
Num
ber
of S
MN
H s
ervi
ces,
hum
anre
sour
ce d
evel
opm
ent
and
acce
ss r
elat
edco
ntra
cts
with
NG
Os,
CB
Os,
prof
essi
onal
/aca
dem
ic i
nstit
utio
ns a
ndpr
ivat
e se
ctor
inc
reas
ed3.
2S
trat
egic
pla
n an
d im
plem
enta
tion
guid
elin
es o
n P
PP
join
tly d
evel
oped
and
endo
rsed
by
the
MoH
P b
y th
e en
d of
200
73.
3P
rivat
e, N
GO
, C
BO
sec
tors
and
prof
essi
onal
/ a
cade
mic
ins
titut
ions
with
SM
NH
ser
vice
s in
crea
sed
by 2
0 pe
rcen
tby
the
yea
r 20
17.
•D
oHS
Ann
ual
Rep
ort
•P
lan
and
guid
elin
eson
PP
P•
DoH
S A
nnua
lR
epor
t
•C
ondu
cive
pol
icy
envi
ronm
ent
for
part
ners
hip
with
NG
O,
CB
O a
nd p
rivat
e se
ctor
cont
inue
s
4.D
ecen
tral
isat
ion
Enh
ance
d lo
cal
gove
rnm
ent
and
part
ner
capa
city
to
plan
and
ove
rsee
SM
NH
ser
vice
s in
line
with
Loc
alS
elf
Gov
erna
nce
Act
4.1
Ann
ual h
ealth
pla
ns d
evel
oped
by
DD
Cs
that
cov
er S
MN
H a
nd s
ocia
l inc
lusi
on,
and
invo
lve
loca
l st
akeh
olde
rs4.
2 In
crea
sed
shar
e of
SM
NH
fro
m 5
% t
o 8%
of d
istr
ict
annu
al b
udge
t
•A
nnua
l he
alth
pla
ns•
DD
C p
lan
•D
istr
ict
budg
et
•C
ondu
cive
pol
icy
envi
ronm
ent
onde
cent
ralis
atio
n•
Str
ong
polic
y an
dfin
anci
al c
omm
itmen
tsfr
om g
over
nmen
t, E
DP
s•
Prio
rity
give
n to
SM
NH
and
soci
al in
clus
ion
bylo
cal
bodi
es c
ontin
ues
•Lo
cal
bodi
es r
emai
nre
spon
sive
to
loca
lvo
ices
5.H
um
an R
eso
urc
e D
evel
op
men
t: S
kille
d B
irth
Att
end
ant
Str
ateg
y
Str
ateg
y/P
lan
for
Hum
an R
esou
rce
Dev
elop
men
t in
rela
tion
to S
MN
H a
nd f
or S
kille
d B
irth
Atte
ndan
tsde
velo
ped
and
impl
emen
ted
5.1
HR
D s
trat
egy/
plan
for
SM
NH
(20
07-2
012)
deve
lope
d, i
ncor
pora
ted
in n
ext
perio
dic
Hea
lth P
lan
and
impl
emen
ted
5.2
Hea
lth f
acili
ties
(Dis
tric
t an
d P
HC
C)
fully
staf
fed
by S
BA
s (w
ith s
kill
mix
, bo
thnu
mbe
r an
d ty
pes)
:20
07:
25%
2012
: 50
%20
17:
80%
•Tr
aini
ng r
epor
t fr
omac
cred
ited
trai
ning
site
s by
NN
C•
11th F
ive
year
Hea
lthP
lan
•H
UR
IC d
ata
•H
UR
IC,
TM
IS a
ndM
oHP
dat
a
•S
MN
H H
RD
str
ateg
y/p
lan
refle
cted
in t
he 1
1th
Fiv
e Y
ear
Pla
n
6.In
form
atio
n
Key
SM
NH
rel
ated
in
form
atio
n, in
clud
ing
6.1
95 p
erce
nt o
f pu
blic
and
25%
hea
lthin
stitu
tions
of
priv
ate
sect
ors
and
NG
Os
repo
rt t
heir
SM
NH
ser
vice
dat
a to
HM
IS b
y
•H
MIS
•D
HS
•D
oHS
ann
ual
repo
rt
20

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
200
8, 5
0% b
y 20
12,
and
100%
by
2017
6.2
Dis
aggr
egat
ed S
MN
H d
ata
gene
rate
d by
2008
6.3
Use
ND
HS
, N
LSS
sur
veys
info
rmat
ion
inpl
anni
ng a
nd p
olic
y fo
rmul
atio
n pr
oces
s.
7.P
hys
ical
Ass
ets
and
Pro
cure
men
t
Ade
quat
e ph
ysic
al r
esou
rces
for
SM
NH
ser
vice
s w
ithye
ar r
ound
ava
ilabi
lity
of S
MN
H r
elat
ed d
rugs
and
supp
lies
ensu
red
7.1
Num
ber
of d
istr
icts
with
at
leas
t on
e fu
llyeq
uipp
ed C
EO
C f
acili
ties
incr
ease
d fr
om28
to
31 b
y en
d of
200
7 an
d to
60
dist
ricts
by e
nd o
f 20
177.
2 P
erce
ntag
e of
PH
CC
s w
ith f
ully
equ
ippe
dB
EO
C f
acili
ties
incr
ease
d fr
om 9
% t
o 20
%20
07 a
nd 4
0 %
by
the
year
200
9, 6
0 %
by
the
year
201
2 an
d 80
% b
y 20
177.
3 H
Ps
with
birt
hing
cen
tres
2007
: 10
%20
09:
15%
2012
: 3
0%20
17:
70%
7.4
Year
rou
nd a
vaila
bilit
y of
SM
NH
dru
gs a
ndco
mm
oditi
es in
crea
sed
to 1
00%
by
2012
7.5
Dru
g fin
anci
ng s
chem
es i
mpl
emen
ted
asst
ated
in N
HS
P-I
P (
8)
•D
oHS
ann
ual
repo
rt•
LMIS
Rep
ort
•F
inan
cial
sup
port
fro
mE
DP
s co
ntin
ues
disa
ggre
gatio
n by
eth
nici
ty,
cast
e an
d w
ealth
,de
velo
ped,
inco
rpor
ated
with
in t
he H
MIS
, an
d o
ther
sour
ces
of in
form
atio
n (N
DH
S,
NLS
S e
tc)
used
at
natio
nal
and
loca
l le
vels
8.F
inan
ce
Sus
tain
able
fin
anci
ng s
yste
m f
or S
MN
H s
ervi
ces
impr
oved
8.1
At
leas
t 15
% o
f pu
bic
expe
nditu
re o
n he
alth
sp
ent f
or S
MN
H a
t the
end
of
2012
fro
m 1
0% a
nd 2
0% b
y 20
178.
2 A
t le
ast
45%
of
SM
NH
pub
lic e
xpen
ditu
rew
ill b
e sp
ent
for
the
bene
fit o
fdi
sadv
anta
ged
grou
ps3
by 2
012
and
50%
by t
he 2
017
8.3
At
leas
t 45
% o
f th
e w
omen
ben
efiti
ng f
rom
the
cost
sha
ring
sche
me
will
be
from
disa
dvan
tage
d gr
oups
(D
alit
and
Janj
ati)
by20
12 a
nd 5
0% b
y 20
178.
4 A
t le
ast
50%
of
villa
ges
will
hav
efu
nctio
nal r
evol
ving
SM
NH
em
erge
ncy
fund
s by
201
2 an
d 60
% b
y 20
17.
•S
urve
y re
port
•F
MIS
•LS
I M
onito
ring
/Ass
essm
ent
repo
rts
•N
LSS
•LS
I M
onito
ring
/Ass
essm
ent
repo
rts
•A
nnua
l rep
ort
DoH
S
•S
MN
H s
hare
of
heal
thbu
dget
inc
reas
ed a
spl
anne
d•
Loca
l bod
ies
are
func
tiona
l•
Leve
l of
reso
urce
sre
mai
ns t
he s
ame
aspl
anne
d
3 S
peci
fical
ly t
his
incl
udes
Dal
its (
low
cas
te o
r oc
cupa
tiona
l ca
ste)
and
Jan
jatis
(et
hnic
min
ority
gro
ups)
21

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
1.E
qu
ity
and
Acc
ess
A.
Ad
voca
cy1.
Lobb
y po
licy
mak
ers
and
influ
entia
l peo
ple
at n
atio
nal,
dist
rict
and
com
mun
ity le
vels
, in
corp
orat
ing
user
and
pro
vide
r vo
ice,
to
have
app
ropr
iate
pol
icie
s in
pla
ce f
or s
ocia
l em
pow
erm
ent
of w
omen
, fa
mili
es a
nd c
omm
uniti
es (
incl
udin
g pr
otec
tion,
sec
urity
,rig
hts,
end
ing
disc
rimin
atio
n, i
mpr
ovin
g st
atus
)2.
Lobb
y at
all
leve
ls f
or e
quita
ble
dist
ribut
ion
of s
ervi
ces
and
infr
astr
uctu
re,
incl
udin
g ro
ads,
brid
ges
and
one
func
tioni
ng t
elep
hone
in e
ach
faci
lity
B.
So
cial
Mo
bili
sati
on
1.In
volv
e co
mm
uniti
es i
n pa
rtic
ipat
ory
plan
ning
, in
clud
ing
cond
uctin
g so
cial
map
ping
, im
plem
entin
g, m
onito
ring
(incl
udin
g vo
ice)
of
SM
NH
pro
gram
mes
and
tak
ing
a co
mm
unity
-bas
ed lo
calis
ed a
ppro
ach.
Wom
en a
nd m
en s
houl
d be
invo
lved
esp
ecia
lly w
omen
of r
epro
duct
ive
age,
mot
hers
-in-la
w a
nd in
fluen
tial f
amily
mem
bers
, an
d di
spla
ced
wom
en a
nd t
heir
fam
ilies
incl
uded
2.M
obili
se h
ealth
wor
kers
, tr
aditi
onal
hea
lth c
are
prov
ider
s, l
ocal
med
ia,
yout
h gr
oups
, co
mm
unity
vol
unte
ers/
FC
HV
s, p
rivat
epr
actit
ione
rs,
mot
hers
’ gro
ups,
sch
ool t
each
ers,
loca
l rep
rese
ntat
ives
and
dut
y ho
lder
s (f
rom
sch
ools
, fo
rest
and
wat
er u
ser
and
savi
ngs
and
cred
it) g
roup
s to
pro
mot
e S
MN
H3.
Pro
vide
sup
port
to
stre
ngth
en c
oord
inat
ion
foru
ms
(RH
CC
/SM
NF
/SM
NS
C/
and
sub-
com
mitt
ees)
at
all l
evel
s to
impl
emen
t S
MN
Hpr
ogra
mm
es,
espe
cial
ly t
arge
ting
the
RH
IE
C t
echn
ical
com
mitt
ee4.
Bui
ld c
omm
uniti
es’ c
apac
ity t
o cr
eate
and
util
ise
sust
aina
ble
emer
genc
y fu
nds
and
tran
spor
tatio
n sc
hem
es (
link
with
Out
put
2,S
ervi
ces)
5.P
rom
ote
cros
s-se
ctor
al (
inte
r an
d in
tra-
min
iste
rial,
divi
sion
al,
NG
Os)
col
labo
ratio
n fo
r in
tegr
atin
g S
MN
H
Beh
avio
ur
Ch
ang
e C
om
mu
nic
atio
n (
BC
C)
1.C
ondu
ct n
atio
nal
base
line
rese
arch
2.U
pdat
e an
d im
plem
ent
inte
grat
ed s
afe
mot
herh
ood
and
new
born
hea
lth c
omm
unic
atio
ns s
trat
egy,
inc
ludi
ng s
tand
ardi
sing
mes
sage
s an
d m
akin
g th
em a
vaila
ble
at a
ll le
vels
3.D
evel
op a
nd i
mpl
emen
t fo
cuse
d re
sear
ch b
ased
com
mun
icat
ion
inte
rven
tions
(lin
ked
with
ser
vice
im
prov
emen
t) t
o re
ach
disa
dvan
tage
d an
d vu
lner
able
gro
ups
incl
udin
g di
spla
ced
peop
le4.
Pro
mot
e S
MN
H r
elat
ed h
ealth
y be
havi
ours
, in
clud
ing
birt
h pr
epar
edne
ss,
by c
ondu
ctin
g B
CC
act
iviti
es a
nd u
sing
rig
hts
base
dap
proa
ches
, sp
ecifi
cally
red
ucin
g al
l vi
olen
ce a
gain
st w
omen
5.P
rom
ote
posi
tive,
non
-dis
crim
inat
ory
inte
r-pe
rson
al c
omm
unic
atio
n be
twee
n pr
ovid
ers
and
clie
nts
•C
oord
inat
ed e
ffort
to
impl
emen
t th
ede
cent
ralis
atio
n ac
t•
Com
mun
ities
will
ingl
ypa
rtic
ipat
e in
SN
MH
prog
ram
mes
•C
onfli
ct d
oes
not
limit
the
mob
ility
and
gath
erin
g of
peo
ple
atdi
stric
t le
vel a
nd b
elow
•In
ter
Min
istr
yco
ordi
natio
n su
ppor
tses
tabl
ishm
ent
offu
nctio
ning
pho
ne l
ines
Maj
or
Act
ivit
y A
reas
Ass
um
pti
on
s
2. S
ervi
ces
1.S
tren
gthe
n an
d ex
pand
qua
lity
SM
NH
ser
vice
s at
all
leve
ls in
a p
hase
d m
anne
r, in
clud
ing
C/B
EO
C,
deliv
ery
and
CA
C s
ervi
ces,
2.Im
prov
e lin
kage
s an
d in
tegr
atio
n w
ith o
ther
rep
rodu
ctiv
e he
alth
and
chi
ld h
ealth
initi
ativ
es (
such
as
IMC
I, P
MT
CT,
Mal
aria
, C
AC
,F
CH
V p
rogr
amm
es)
�R
esou
rces
con
tinue
to
be a
vaila
ble
for
impr
ovin
g ph
ysic
alfa
cilit
ies,
mai
ntai
ning
adeq
uate
sta
ffing
and
22

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
3.Im
prov
e th
e qu
ality
of
serv
ices
thr
ough
dev
elop
men
t of
qua
lity
assu
ranc
e an
d m
onito
ring
syst
ems
with
on-
site
coa
chin
g an
dlo
gist
ic s
uppo
rt,
in c
oord
inat
ion
with
app
ropr
iate
div
isio
ns4.
Cre
ate
an e
nabl
ing
envi
ronm
ent
for
SM
NH
ser
vice
s th
roug
h ad
voca
cy a
t al
l lev
els,
cap
acity
bui
ldin
g of
loca
l man
agem
ent
bodi
esan
d in
volv
emen
t of
civ
il so
ciet
y an
d pr
ivat
e se
ctor
in c
oord
inat
ion
with
app
ropr
iate
div
isio
ns5.
Prio
ritis
e th
e ne
eds
of p
oor
and
vuln
erab
le g
roup
s, f
ocus
ing
on s
uppo
rtin
g co
mm
unity
car
e in
mar
gina
lized
are
as a
nd d
evel
opin
gst
rate
gies
for
red
ucin
g se
rvic
e co
sts
for
poor
wom
en6.
Impr
ove
the
func
tioni
ng o
f re
ferr
al s
yste
ms
by d
evel
opin
g si
mpl
e re
ferr
al p
roto
cols
, st
reng
then
ing
mec
hani
sms,
orie
ntin
gco
mm
unity
wor
kers
and
ens
urin
g 24
-hou
r av
aila
bilit
y of
ser
vice
s7.
Ava
il an
aest
hesi
a se
rvic
e(S
ee A
nnex
for
mor
e de
taile
d ac
tiviti
es)
prov
idin
g su
ppor
t�
Oth
er R
H in
itiat
ives
will
ing
to c
oope
rate
�C
onfli
ct d
oes
not
limit
activ
ities
�Lo
cal
Man
agem
ent
bodi
es a
re c
omm
itted
to
SM
NH
ser
vice
s
4.
Dec
entr
alis
atio
n1.
Ens
ure
clar
ity a
bout
rol
es a
nd r
espo
nsib
ilitie
s of
sta
keho
lder
s fo
r de
liver
ing
devo
lved
SM
NH
ser
vice
s2.
Rai
se p
ublic
aw
aren
ess
abou
t de
volu
tion
of S
MN
H s
ervi
ces
to c
omm
unity
leve
l3.
Fac
ilita
te q
uart
erly
pub
lic d
isse
min
atio
n of
SM
NH
bud
gets
and
am
ount
spe
nt4.
Str
engt
hen
man
agem
ent
capa
city
at
loca
l le
vel
5.S
uppo
rt d
istr
ict
and
faci
lity
leve
l pla
nnin
g an
d m
onito
ring
rela
ted
to S
MN
H,
with
foc
us o
n eq
uity
and
acc
ess
and
soci
al in
clus
ion
6.D
evel
op a
nd im
plem
ent
a st
anda
rd m
onito
ring
chec
klis
t fo
r S
MN
H s
ervi
ces,
incl
udin
g eq
uity
and
acc
ess
and
soci
al in
clus
ion
issu
es7.
Est
ablis
h a
syst
em o
f re
war
ds a
nd in
cent
ives
for
tho
se p
rovi
ding
ef
ficie
nt
non-
disc
rimin
ator
y S
MN
H s
ervi
ces
at lo
cal l
evel
8.Tr
ack
the
outc
ome
and
impa
ct o
f de
volu
tion
on lo
cal S
MN
H in
dica
tors
9.D
evel
op m
etho
ds f
or g
reat
er p
ublic
acc
ount
abili
ty o
f lo
cal h
ealth
ser
vice
s10
.Inc
reas
e tr
ansp
aren
cy a
nd p
ublic
acc
ess
to S
MN
H r
elat
ed i
nfor
mat
ion
on:
budg
et,
spen
ding
, hu
man
res
ourc
es,
logi
stic
s,su
pplie
s, s
ervi
ces
avai
labl
e an
d pr
ovid
ed a
nd i
ndic
ator
s11
.Enh
ance
coo
rdin
atio
n am
ong
key
bodi
es s
uch
as R
HC
C,
DH
MC
, D
AC
C,
CD
P a
nd I
SC
.
•Lo
cal
bodi
es r
emai
nre
spon
sive
to
loca
lvo
ices
•M
ater
nal
heal
th r
emai
nsa
prio
rity
for
the
loca
lbo
dies
•Lo
cal
gove
rnm
ent
isac
com
mod
ativ
e in
plan
ning
and
mon
itorin
g
3.
Pu
blic
Pri
vate
Par
tner
ship
1.E
stab
lish
an e
ffect
ive
regu
lato
ry b
ody
at M
oHP
with
rep
rese
ntat
ion
from
the
priv
ate
sect
or,
NG
Os
and
CB
Os
2.D
evel
op a
lega
l fra
mew
ork,
pro
toco
ls a
nd g
uide
lines
to
enco
urag
e an
d re
gula
te P
PP,
incl
udin
g tr
ansf
er o
f pu
blic
res
ourc
es t
oN
GO
s, C
BO
s an
d th
e pr
ivat
e se
ctor
3.E
stab
lish
and
stre
ngth
en jo
int
annu
al p
lann
ing
and
revi
ew m
echa
nism
s w
ith r
epre
sent
atio
n fr
om p
rivat
e se
ctor
, N
GO
s, C
BO
ssu
ppor
t fr
om e
xper
ts4.
Incl
ude
NG
O,
CB
O a
nd p
rivat
e se
ctor
SM
NH
pla
ns a
nd p
rogr
ess
in h
ealth
sec
tor
mon
itorin
g5.
Pro
vide
cap
acity
bui
ldin
g on
SM
NH
ser
vice
del
iver
y fo
r N
GO
s, C
BO
s an
d th
e pr
ivat
e se
ctor
6.H
arm
onis
e P
PP
pro
cedu
res
for
impl
emen
tatio
n to
ens
ure
cons
iste
ncy
with
tho
se o
f G
over
nmen
t an
d E
DP
s7.
Enh
ance
the
cap
acity
of
dist
rict
RH
CC
s to
add
ress
ser
vice
pro
visi
on,
equi
ty a
nd a
cces
s an
d so
cial
incl
usio
n is
sues
in S
MN
H8.
Trai
n do
ctor
s on
C/S
•S
tron
g po
licy
and
finan
cial
com
mitm
ent
from
Gov
ernm
ent,
ED
Ps
and
priv
ate
sect
or
23

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
5.
Hu
man
Res
ou
rce
Dev
elo
pm
ent:
Ski
lled
Bir
th A
tten
dan
ts’ S
trat
egy/
PL
an
A.
Hu
man
Res
ou
rce
Str
ateg
y1.
Dev
elop
a 5
-yea
r H
RD
str
ateg
y fo
r S
MN
H s
ervi
ces
2.D
evel
op a
nd m
aint
ain
a da
taba
se o
f hu
man
res
ourc
es a
nd s
kills
the
ir ut
ilisa
tion
3.D
evel
op t
ools
for
und
erta
king
pos
t tr
aini
ng o
nsite
sup
ervi
sion
and
mon
itorin
g4.
Dev
elop
mec
hani
sms
for
unde
rtak
ing
perf
orm
ance
ass
essm
ent
of t
rain
ed h
ealth
car
e pr
ovid
ers
5.E
stab
lish
a na
tiona
l aw
ard
syst
em f
or ‘
’saf
e m
othe
rhoo
d ch
ampi
on’’
in c
olla
bora
tion
with
pro
fess
iona
l or
gani
satio
ns
B.
Ski
lled
Bir
th A
tten
dan
ts’ S
trat
egy
1.D
evel
op a
5-y
ear
SB
A in
-ser
vice
tra
inin
g st
rate
gy/p
lan
2.D
evel
op g
ener
ic (
27 c
ore
skill
s) c
ompe
tenc
y ba
sed
SB
A t
rain
ing
pack
age
3.R
evie
w a
nd d
evel
op a
ccre
dita
tion
stan
dard
s fo
r tr
aini
ng in
stitu
tions
, sc
ope
of p
ract
ices
and
cer
tific
atio
n st
anda
rds
for
SB
As
4.Id
entif
y ga
ps in
the
exi
stin
g B
EO
C in
-ser
vice
cur
ricul
um a
nd a
dapt
for
in-s
ervi
ce S
BA
tra
inin
g (A
NM
s, S
N a
nd M
BB
S)
5.S
cree
n ex
istin
g he
alth
car
e pr
ovid
ers
(AN
Ms,
SN
s an
d do
ctor
s) w
ho h
ave
rece
ived
MR
T a
nd B
EO
C t
o as
sess
whe
ther
the
yre
quire
ref
resh
er t
rain
ing
6.U
pgra
de S
BA
tra
inin
g si
tes
7.C
ondu
ct p
lann
ing
mee
ting
with
5 R
HT
CS
s to
mak
e ar
rang
emen
ts f
or b
egin
ning
SB
A t
rain
ing
8.Tr
ain
serv
ice
prov
ider
s to
ens
ure
they
hav
e co
re S
BA
com
pete
ncie
s an
d ce
rtify
the
m9.
Ada
pt t
he g
ener
ic p
acka
ge f
or p
re-s
ervi
ce t
rain
ing
10.S
tren
gthe
n th
e ca
paci
ty o
f pr
e-se
rvic
e tr
aini
ng in
stitu
tions
(A
NM
, P
CL)
11.E
nsur
e al
l new
AN
M g
radu
ates
hav
e co
re S
BA
com
pete
ncie
s an
d ce
rtify
the
m
•11
th F
ive
year
Hea
lthP
lan
appr
oved
by
MoF
,M
oGA
, P
ublic
Ser
vice
Com
mis
sion
and
Nat
iona
l P
lann
ing
Com
mis
sion
•O
bste
tric
com
pone
nt o
fpr
e-se
rvic
e cu
rric
ulum
for
MB
BS
upd
ated
•S
uffic
ient
num
ber
ofA
NM
, P
CL
trai
ning
site
sac
cred
ited
by N
NC
•S
uffic
ient
num
ber
ofA
NM
gra
duat
es c
ertif
ied
as S
BA
s by
NN
C
6.In
form
atio
n M
anag
emen
t
A.
Info
rmat
ion
man
agem
ent
stra
teg
y1.
Dev
elop
a s
trat
egy
to in
corp
orat
e ke
y S
MN
H in
form
atio
n w
ithin
an
inte
grat
ed m
atrix
(di
sagg
rega
ted
by e
thni
city
, ca
ste,
and
wea
lth)
B.
Dat
a co
llect
ion
an
d q
ual
ity
2.Im
prov
e th
e qu
ality
of
data
col
lect
ed3.
Con
duct
dat
a ve
rific
atio
n ex
erci
ses
4.D
esig
n an
d im
plem
ent
rese
arch
and
stu
dies
for
gen
erat
ing
addi
tiona
l inf
orm
atio
n th
at is
not
inco
rpor
ated
in H
MIS
C.
Acc
ess
to I
nfo
rmat
ion
5.In
crea
se a
cces
s to
SM
NH
info
rmat
ion
at a
ll le
vels
(co
mm
unity
to
cent
re)
6.B
uild
rel
atio
nshi
ps w
ith p
ublic
, pr
ivat
e an
d N
GO
sec
tors
, an
d in
trod
uce
mec
hani
sms
for
regu
latin
g th
e flo
w o
f in
form
atio
n to
HM
IS7.
Pro
vide
orie
ntat
ion
to b
uild
cap
acity
of
SM
NH
sta
keho
lder
s to
gen
erat
e un
ders
tand
ing
on S
MN
H is
sues
at
all l
evel
s (c
omm
unity
to c
entr
e)
•C
ompr
ehen
sive
HM
IS i
sfe
asib
le•
A f
unct
iona
l bod
y is
inpl
ace
to r
egul
arly
rev
iew
and
reco
mm
end
chan
gein
HM
IS t
o re
spon
d to
prog
ram
me
need
s
24

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
D.
Mo
nit
ori
ng
8.P
rovi
de t
rain
ing
and
refr
eshe
r tr
aini
ng o
n S
MN
H p
rogr
amm
e m
onito
ring9
. D
esig
n an
d im
plem
ent
Key
Inf
orm
ant
Mon
itorin
gsy
stem
10.
Des
ign
and
impl
emen
t co
nflic
t m
onito
ring
syst
em
7.P
hys
ical
Ass
ets
and
Pro
cure
men
t
1.D
evel
op a
n in
vent
ory
of S
MN
H s
ervi
ce f
acili
ties,
equ
ipm
ent
and
inst
rum
ents
2.Im
plem
ent
a sy
stem
for
crit
eria
bas
ed d
istr
ict
sele
ctio
n fo
r ex
pans
ion/
exte
nsio
n/re
nova
tion
of p
hysi
cal
faci
litie
s3.
Dev
elop
and
im
plem
ent
need
bas
ed p
artic
ipat
ory
plan
ning
, m
onito
ring
and
impl
emen
tatio
n m
echa
nism
s4.
Dev
elop
and
im
plem
ent
a m
aint
enan
ce p
olic
y5.
Dev
elop
int
er-m
inis
teria
l an
d in
ter-
depa
rtm
enta
l co
ordi
natio
n m
echa
nism
s fo
r ph
ysic
al r
esou
rce
and
com
mod
ities
pla
nnin
g,m
onito
ring
and
impl
emen
tatio
n6.
Est
ablis
h a
data
base
of
supp
liers
and
dis
trib
utio
n ch
anne
ls f
or d
rugs
and
com
mod
ities
7.S
tren
gthe
n th
e qu
arte
rly L
MIS
rep
ortin
g sy
stem
for
con
sum
ptio
n of
SM
NH
rel
ated
dru
gs a
nd o
ther
com
mod
ities
8.Im
plem
ent
MN
C t
reat
men
t pr
otoc
ols
with
rat
iona
le u
se o
f dr
ugs
(ref
er t
o O
utpu
t 2,
Ser
vice
s)
•Tr
ansp
ort
bottl
enec
ksar
e no
t si
gnifi
cant
lyin
crea
sed
•E
DP
com
mitm
ent
offu
ndin
g su
ppor
t do
es n
otde
clin
e•
Situ
atio
n al
low
sm
onito
ring
of p
hysi
cal
faci
lity
cons
truc
tion
•C
onfli
ct s
ituat
ion
does
not
affe
ctim
plem
enta
tion
activ
ities
2.F
inan
ce
A.
In
crea
sin
g r
eso
urc
es f
or
SM
NH
1.C
ondu
ct e
vide
nce
base
d ad
voca
cy t
o in
crea
se a
vaila
bilit
y of
fin
anci
al r
esou
rces
for
SM
NH
ser
vice
s2.
Red
esig
n th
e re
sour
ce a
lloca
tion
form
ula
3.C
arry
out
cap
acity
bui
ldin
g/tr
aini
ng f
or t
imel
y sp
endi
ng o
f av
aila
ble
finan
cial
res
ourc
es4.
Impr
ove
Fin
anci
al M
anag
emen
t In
form
atio
n S
yste
m (
in li
ne w
ith t
he N
HS
P-I
P)
5.Im
plem
ent
and
refin
e th
e co
st s
harin
g sc
hem
e6.
Dev
elop
and
im
plem
ent
a su
stai
nabi
lity
plan
B.
Pro
mo
tin
g a
lter
nat
ive
fin
anci
ng
sch
emes
7.C
ondu
ct o
pera
tiona
l re
sear
ch o
n su
stai
nabl
e fin
anci
ng8.
Dev
elop
nat
iona
l gui
delin
es a
nd p
rovi
de c
omm
unity
mat
chin
g fo
r S
MN
H e
mer
genc
y fu
nds
C.
Saf
ety
net
fo
r p
oo
r an
d v
uln
erab
le g
rou
ps9.
Con
trib
ute
to t
he u
ser
char
ge p
olic
y, a
ddin
g ex
empt
ion
crite
ria f
or t
he m
ost
vuln
erab
le g
roup
s10
.Mon
itor
and
eval
uate
fin
anci
ng s
chem
es
•Le
vel o
f de
man
d fo
rhe
alth
res
ourc
es d
oes
not
grow
mas
sive
lybe
caus
e of
the
con
flict
•A
ll di
stric
ts h
ave
func
tioni
ng t
elep
hone
s•
Insu
ranc
e sc
hem
eex
pand
s as
pla
nned
•S
ituat
ion
allo
ws
regu
lar
mon
itorin
g an
dev
alua
tion
25
National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
An
nex
1:
Det
aile
d a
ctiv
itie
s u
nd
er m
ajo
r ca
teg
ori
es f
or
serv
ices
(O
utp
ut
2)
2.1
S
tren
gth
en a
nd
exp
and
qu
alit
y S
MN
H s
ervi
ces
at a
ll le
vels
in a
ph
ased
man
ner
, in
clu
din
g B
/CE
OC
, del
iver
y an
d C
AC
ser
vice
s
a)D
evel
op a
ppro
pria
te s
elec
tion
crite
ria f
or B
/CE
OC
site
s an
d bi
rthi
ng c
entr
es.
b)D
evel
op a
nd i
mpl
emen
t a
need
bas
ed p
lann
ing
and
mon
itorin
g sy
stem
and
a p
hase
d ex
pans
ion
plan
for
B/C
EO
C s
ites
in d
istr
ict
hosp
itals
and
PH
CC
s, a
nd fo
r bi
rthi
ng c
entr
es in
app
ropr
iate
HP
s an
d S
HP
s, a
ccor
ding
to a
gree
d cr
iteria
. The
min
imum
req
uire
men
t for
CE
OC
and
BE
OC
site
s ac
cord
ing
to t
he U
N s
tand
ard
is f
our
BE
OC
site
s an
d on
e C
EO
C s
ite p
er 5
00,0
00 p
opul
atio
n. H
owev
er,
the
spar
se p
opul
atio
n di
strib
utio
n in
the
hill
and
mou
ntai
n ar
eas
and
asso
ciat
ed p
oor
tran
spor
t ava
ilabi
lity
mea
ns th
at N
epal
may
nee
d m
ore
C/B
EO
C s
ites
than
spe
cifie
d by
this
crit
erio
n, o
r a
stre
ngth
ened
ref
erra
l sys
tem
in th
ose
dist
ricts
whe
re C
EO
C s
ervi
ces
are
not f
easi
ble
or c
ost
effe
ctiv
e.c)
Enc
oura
ge t
he c
omm
unity
, E
DP
s an
d pr
ivat
e/N
GO
sec
tor
to d
evel
op d
eliv
ery
cent
res
and
EO
C s
ervi
ces
(incl
udin
g es
sent
ial n
ewbo
rnca
re)
to c
ompl
emen
t go
vern
men
t se
rvic
es a
nd c
onfo
rm w
ith n
atio
nal s
tand
ards
.d)
Ens
ure
skill
ed b
irth
atte
ndan
ts a
re a
vaila
ble
at H
Ps
and
SH
Ps
and
in c
omm
uniti
es. E
ncou
rage
wom
en to
use
an
SB
A fo
r ho
me
birt
hs if
they
are
not
abl
e to
go
to a
hea
lth f
acili
ty (
link
with
Out
puts
1,
Equ
ity a
nd A
cces
s, a
nd 5
, H
uman
Res
ourc
e D
evel
opm
ent)
.e)
Enc
oura
ge h
ealth
wor
kers
to
prov
ide
early
PN
C c
are
(with
in 7
2 hr
s of
the
birt
h) a
t ho
me
or in
the
hea
lth f
acili
ty.
Enc
oura
ge F
CH
Vs
topr
ovid
e po
stna
tal h
ome
visi
ts t
o ad
vise
new
mot
hers
and
the
ir fa
mili
es a
bout
car
ing
for
mot
her
and
baby
, an
d lin
k th
is w
ith t
he F
CH
Vpr
ogra
mm
e to
ens
ure
mot
hers
’ gro
ups
are
info
rmed
abo
ut t
he im
port
ance
of
PN
C.
f)S
tren
gthe
n ca
re f
or lo
w b
irth
wei
ght
and
sick
new
born
s in
hea
lth f
acili
ties
and
in c
omm
uniti
es/
fam
ilies
.g)
Str
engt
hen
post
part
um f
amily
pla
nnin
g co
unse
lling
and
ser
vice
s (li
nk w
ith f
amily
pla
nnin
g se
rvic
es).
h)D
evel
op C
AC
ser
vice
s in
all
dist
rict h
ospi
tals
and
app
ropr
iate
PH
CC
s, a
nd e
ncou
rage
priv
ate/
NG
O s
ecto
rs to
exp
and
CA
C s
ervi
ces
inlin
e w
ith th
e C
AC
pol
icy.
2.2
Im
pro
ve l
inka
ges
an
d i
nte
gra
tio
n w
ith
oth
er r
epro
du
ctiv
e h
ealt
h a
nd
ch
ild h
ealt
h i
nit
iati
ves
a)N
ewbo
rn c
are:
•In
tegr
ate
esse
ntia
l ne
wbo
rn c
are
in s
afe
mot
herh
ood
and
child
hea
lth c
are
prog
ram
mes
at
all
leve
ls i
n or
der
to c
reat
e sy
nerg
y an
dm
axim
ise
outp
uts.
•In
tegr
ate
neon
atal
car
e in
the
IM
CI
prog
ram
me.
•Li
nk w
ith C
hild
Hea
lth D
ivis
ion
to p
rovi
de m
icro
nutr
ient
sup
ply
and
TT
im
mun
isat
ion
for
preg
nant
wom
en a
s pa
rt o
f A
NC
and
PN
Cse
rvic
es.
•B
uild
link
ages
with
IE
C/B
CC
and
acc
ess
prog
ram
mes
to
ensu
re in
form
atio
n an
d se
rvic
es a
re m
atch
ed.
26

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
b)H
IV/A
IDS
: Li
nk w
ith N
CA
SC
to p
rovi
de P
MT
CT
and
car
e of
HIV
pos
itive
pre
gnan
t wom
en in
sel
ecte
d hi
gh r
isk
dist
ricts
acc
ordi
ng to
the
HIV
/A
IDS
pol
icy
and
prog
ram
me.
c)M
alar
ia:
Pro
vide
ant
i-mal
aria
l tr
eatm
ent
to p
regn
ant
wom
en i
n en
dem
ic a
reas
, ac
cord
ing
to n
atio
nal
stan
dard
s, t
hrou
gh l
inki
ng w
ith t
hem
alar
ia s
ectio
n of
the
Epi
dem
iolo
gy D
ivis
ion.
2.3
Im
pro
ve q
ual
ity
of
serv
ices
th
rou
gh
dev
elo
pm
ent
of
qu
alit
y as
sura
nce
an
d m
on
ito
rin
g s
yste
ms
wit
h o
n-s
ite
coac
hin
g a
nd
log
isti
csu
pp
ort
, in
co
ord
inat
ion
wit
h a
pp
rop
riat
e d
ivis
ion
s
a)C
oord
inat
e w
ith M
anag
emen
t D
ivis
ion
to d
evel
op a
nd i
mpl
emen
t a
com
preh
ensi
ve q
ualit
y as
sura
nce
syst
em f
or s
afe
mot
herh
ood
and
new
born
car
e, c
over
ing
all l
evel
s an
d in
clud
ing
priv
ate/
NG
O s
ecto
rs:
•D
evel
op/u
pdat
e an
d im
plem
ent
SM
NH
Sta
ndar
ds,
prot
ocol
s gu
idel
ines
and
too
ls f
or m
ater
nal a
nd n
ewbo
rn c
are
at a
ll le
vels
of
serv
ice.
•W
ork
with
Man
agem
ent
Div
isio
n to
dev
elop
qua
lity
of c
are
mon
itorin
g te
ams
at c
entr
al,
regi
onal
and
dis
tric
t le
vels
for
tec
hnic
al a
ndm
anag
emen
t su
perv
isio
n.•
Dev
elop
the
cap
acity
of
dist
rict
heal
th m
anag
emen
t co
mm
ittee
s, h
ealth
ser
vice
pro
vide
rs a
nd p
ublic
hea
lth n
urse
s an
d in
stitu
tiona
lise
qual
ity a
ssur
ance
, in
line
with
qua
lity
mon
itorin
g gu
idel
ines
.•
Sup
port
the
inc
lusi
on o
f th
e pr
ivat
e/N
GO
sec
tor
unde
r th
e na
tiona
l sy
stem
for
qua
lity
assu
ranc
e, t
o en
cour
age
them
to
adop
t na
tiona
lst
anda
rds
and
QO
C g
uide
lines
.•
Ens
ure
suffi
cien
t lo
gist
ic s
uppo
rt is
ava
ilabl
e (li
nk w
ith o
utpu
t 7,
pro
cure
men
t).
b)
Dev
elop
, pl
an a
nd im
plem
ent
regu
lar
mon
itorin
g an
d su
perv
isio
n sy
stem
s at
diff
eren
t le
vels
:•
Inst
itutio
nalis
e th
e E
OC
mon
itorin
g sy
stem
in H
MIS
and
in s
afe
mot
herh
ood
dist
ricts
incl
udin
g pr
ivat
e/N
GO
sec
tor
faci
litie
s.•
Incr
ease
the
cap
acity
of
publ
ic h
ealth
nur
ses/
dis
tric
t su
perv
isor
s to
pro
vide
effe
ctiv
e m
onito
ring
and
supe
rvis
ion
and
on-s
ite c
oach
ing.
•D
evel
op s
uper
visi
on c
heck
lists
and
gui
delin
es.
c)Im
plem
ent a
nd e
xpan
d m
ater
nal a
nd p
eri-n
atal
dea
th a
udits
in h
ospi
tals
in a
pha
sed
man
ner,
acco
rdin
g to
gui
delin
es a
nd in
volv
ing
prof
essi
onal
orga
nisa
tions
suc
h as
NE
SO
G,
NE
PA
S,
PE
SO
N a
nd N
AN
.d)
Car
ry o
ut p
erio
dic
asse
ssm
ent a
nd re
sear
ch in
the
field
of S
MN
H, i
nclu
ding
com
mun
ity p
erce
ptio
n of
qua
lity
of c
are
thro
ugh
use
of te
chni
ques
such
as
clie
nt e
xit
inte
rvie
ws
and
inte
ract
ion
with
com
mun
ities
, in
ord
er t
o im
prov
e po
licy
deve
lopm
ent
and
prog
ram
min
g.
2.4
C
reat
e an
en
ablin
g e
nvi
ron
men
t fo
r S
MN
H s
ervi
ces
thro
ug
h a
dvo
cacy
at
all l
evel
s, c
apac
ity
bu
ildin
g o
f lo
cal m
anag
emen
t b
od
ies
and
in
volv
emen
t o
f ci
vil
soci
ety
and
pri
vate
sec
tor
in c
oo
rdin
atio
n w
ith
ap
pro
pri
ate
div
isio
ns
a)A
dvoc
ate
and
lobb
y at
all
leve
ls fo
r ap
prop
riate
nee
d ba
sed
SM
NH
pol
icie
s, p
rogr
amm
es a
nd r
esou
rce
allo
catio
n, to
ens
ure
the
avai
labi
lity
ofqu
ality
SM
NH
ser
vice
s an
d re
spon
d to
loca
l rea
litie
s (li
nk w
ith O
utpu
t 1,
Equ
ity a
nd A
cces
s).
27

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
b)C
oord
inat
e w
ith M
anag
emen
t Div
isio
n to
str
engt
hen
the
capa
city
of l
ocal
hea
lth m
anag
emen
t com
mitt
ees,
coo
rdin
atio
n fo
rum
s an
d co
mm
uniti
esin
fluen
tial i
n th
e m
anag
emen
t of S
MN
H s
ervi
ces
at d
iffer
ent l
evel
s of
hea
lth fa
cilit
y, a
s pa
rt o
f the
dec
entr
alis
atio
n ef
fort
. Ens
ure
the
part
icip
atio
nof
civ
il so
ciet
y, N
GO
/ pr
ivat
e se
ctor
s an
d D
alit
and
Janj
ati g
roup
s in
the
pro
cess
.c)
Dev
elop
mec
hani
sms
to p
rom
ote
acco
unta
bilit
y an
d te
am s
pirit
in h
ealth
fac
ility
man
agem
ent
com
mitt
ees
and
staf
f fo
r th
e de
liver
y of
qua
lity
SM
NH
ser
vice
s, u
sing
app
reci
ativ
e an
d pa
rtic
ipat
ory
man
agem
ent
proc
esse
s an
d in
volv
ing
com
mun
ities
and
civ
il so
ciet
y.d)
Wor
k w
ith N
HT
C t
o en
sure
ade
quat
e hu
man
res
ourc
es a
re in
pla
ce n
urse
s ar
e le
gally
pro
tect
ed w
hen
deal
ing
with
em
erge
ncie
s in
out
lyin
gar
eas
(link
with
out
put
5, h
uman
res
ourc
e de
velo
pmen
t).
e)W
ork
with
Log
istic
s M
anag
emen
t D
ivis
ion
to d
evel
op e
ssen
tial S
MN
H r
elat
ed d
rugs
and
equ
ipm
ent
lists
and
mak
e th
em a
vaila
ble
(link
with
Out
put
7, P
hysi
cal A
sset
s an
d P
rocu
rem
ent)
.f)
Dev
elop
infr
astr
uctu
re s
tand
ards
for
SM
NH
ser
vice
s (li
nk w
ith O
utpu
t 7,
Phy
sica
l Ass
ets
and
Pro
cure
men
t).
g)E
mpo
wer
fem
ale
staf
f in
hea
lth in
stitu
tions
as
chan
ge a
gent
s, t
hrou
gh o
n-si
te s
uppo
rt,
lead
ersh
ip a
nd m
anag
emen
t tr
aini
ng.
Incr
ease
the
irpa
rtic
ipat
ion
in p
lann
ing
prog
ram
min
g, d
ecis
ion-
mak
ing
and
supe
rvis
ion.
2.5
Pri
ori
tise
th
e n
eed
s o
f p
oo
r an
d v
uln
erab
le g
rou
ps, f
ocu
sin
g o
n s
up
po
rtin
g c
om
mu
nit
y ca
re in
mar
gin
aliz
ed a
reas
an
d d
evel
op
ing
stra
teg
ies
for
red
uci
ng
ser
vice
co
sts
for
po
or
wo
men
a)
Prio
ritis
e an
d ta
rget
hea
lth f
acili
ties
whi
ch p
rovi
de S
MN
H s
ervi
ces
for
poor
and
vul
nera
ble
grou
ps.
b)D
evel
op a
str
ateg
y fo
r re
duci
ng t
he c
ost
of d
eliv
ery
and
EO
C t
hat
ensu
res
key
serv
ices
are
affo
rdab
le (
cost
s ar
e tr
ansp
aren
t, in
clud
ing
ratio
nal p
roto
cols
for
dru
gs),
and
sub
sidi
es a
re a
vaila
ble
for
poor
peo
ple.
c)E
nsur
e th
at th
e co
st-s
harin
g sc
hem
e, w
hich
aim
s to
enc
oura
ge a
ll w
omen
to u
se a
n S
BA
for
child
birt
h, is
kno
wn
abou
t and
acc
essi
ble
to p
oor
and
vuln
erab
le w
omen
(lin
k w
ith O
utpu
t 1,
Equ
ity a
nd A
cces
s).
d)M
onito
r util
isat
ion
of S
MN
H s
ervi
ces
by v
ulne
rabl
e gr
oups
to g
ain
a be
tter u
nder
stan
ding
of w
hat w
orks
, and
app
ly th
ese
less
ons
to p
rogr
amm
ing.
2.6
Im
pro
ve th
e fu
nct
ion
ing
of r
efer
ral s
yste
ms
by
dev
elo
pin
g s
imp
le re
ferr
al p
roto
cols
, str
eng
then
ing
mec
han
ism
s, o
rien
tin
g c
om
mu
nit
yw
ork
ers
and
en
suri
ng
24-
ho
ur
avai
lab
ility
of
serv
ices
a)
Str
engt
hen
the
resp
onsi
vene
ss o
f re
ferr
al m
echa
nism
s.b)
Est
ablis
h lin
kage
s be
twee
n he
alth
faci
litie
s, p
erip
hera
l hea
lth c
are
prov
ider
s an
d vo
lunt
eers
, tra
ditio
nal p
ract
ition
ers
and
NG
O/C
BO
coo
rdin
atio
nfo
rum
s.c)
Dev
elop
a r
efer
ral p
roto
col (
incl
udin
g co
nditi
ons
for
patie
nts
to b
e re
ferr
ed a
nd s
tabi
lisat
ion
with
obs
tetr
ic fi
rst a
id b
efor
e an
d du
ring
tran
spor
t)an
d sl
ip, w
ith m
echa
nism
s fo
r co
mm
unic
atin
g w
ith h
ighe
r ce
ntre
s an
d lin
ks w
ith e
mer
genc
y fu
nds
and
tran
spor
t sch
emes
to a
ssis
t in
refe
rral
of p
oor
wom
en (
link
with
Out
put
1, E
quity
and
Acc
ess)
.d)
Dev
elop
a s
peci
al s
trat
egy
for
rem
ote
dist
ricts
and
con
flict
affe
cted
are
as,
such
as
esta
blis
hmen
t of
mat
erni
ty w
aitin
g ho
mes
nea
r re
ferr
alho
spita
ls f
or p
regn
ant
wom
en w
ho a
re n
ear
term
.e)
D
evel
op a
nd p
ilot
mat
erni
ty w
aitin
g ho
me
oper
atio
nal g
uide
lines
.f)
D
evel
op a
saf
ety
net
and
subs
idy
syst
em f
or p
oor
wom
en (
link
with
Out
put
8, F
inan
ce).
28

National Safe Motherhood and
Newborn Health-Long Term Plan
(NSMNH-LTP)
Published byFamily Health DivisionDepartment of Health ServicesMinistry of Health & PopulationTeku, Kathmandu
Printed in Nepal bySagun Printing PressTeku, Kathmandu
Design and Layout byPrism Color ScanningKuleshwor, Kathmandu