national organ donation committee, 28.01014 objectives –welcome new members / attendees...
TRANSCRIPT

National Organ Donation Committee, 28.01014
• Objectives– Welcome new members / attendees– Feedback on the proposed revisions to the pregnancy
policy– Review the educational activities of the Committee– Contribute to the understanding of the current
increases in deceased donation– Advise ODT of the likely impact of any reduction in
investment on donation-related activities– Report on work in regional collaboratives– Consider the future working arrangements of NODC

Matters arising
a) Extended DCD project (Roberto Cacciola)
b) St John’s Award (Dale Gardiner)
c) Clinical microsite (John Richardson / James Neuberger)
c) Pregnancy and Organ Donation (Huw Twamley / Liz Waite)
d) Regional on-call nurses (Sri Nagaiyan)
e) Club 32 (Dale Gardiner)
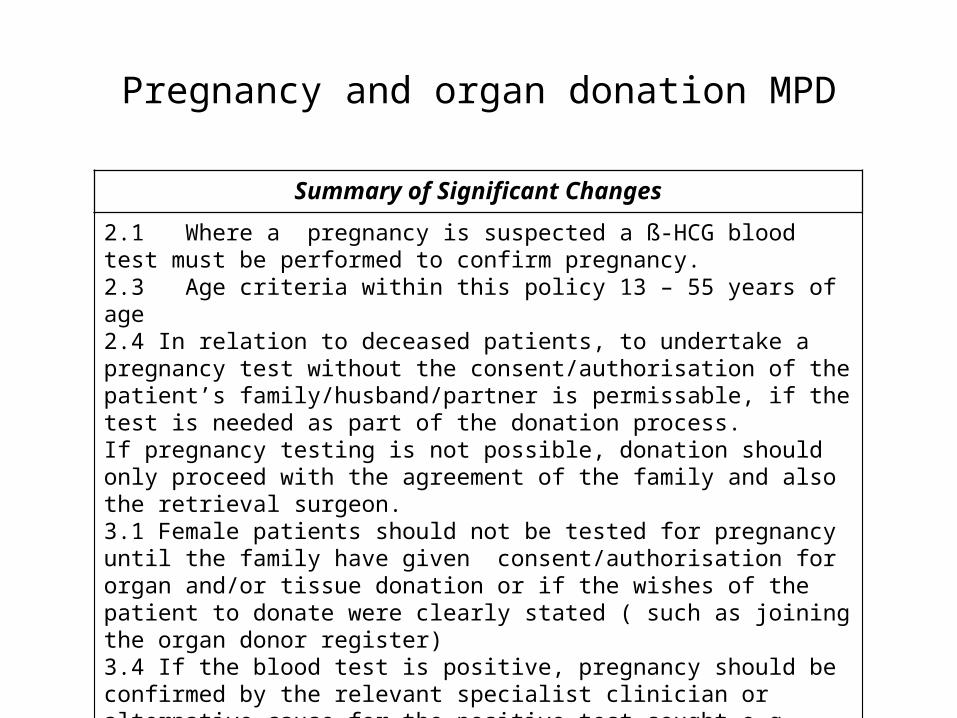
Pregnancy and organ donation MPD
Summary of Significant Changes
2.1 Where a pregnancy is suspected a ß-HCG blood test must be performed to confirm pregnancy. 2.3 Age criteria within this policy 13 – 55 years of age2.4 In relation to deceased patients, to undertake a pregnancy test without the consent/authorisation of the patient’s family/husband/partner is permissable, if the test is needed as part of the donation process.If pregnancy testing is not possible, donation should only proceed with the agreement of the family and also the retrieval surgeon.3.1 Female patients should not be tested for pregnancy until the family have given consent/authorisation for organ and/or tissue donation or if the wishes of the patient to donate were clearly stated ( such as joining the organ donor register)3.4 If the blood test is positive, pregnancy should be confirmed by the relevant specialist clinician or alternative cause for the positive test sought e.g. Choriocarcinoma ( which would be a contra-indication to organ or tissue donation).

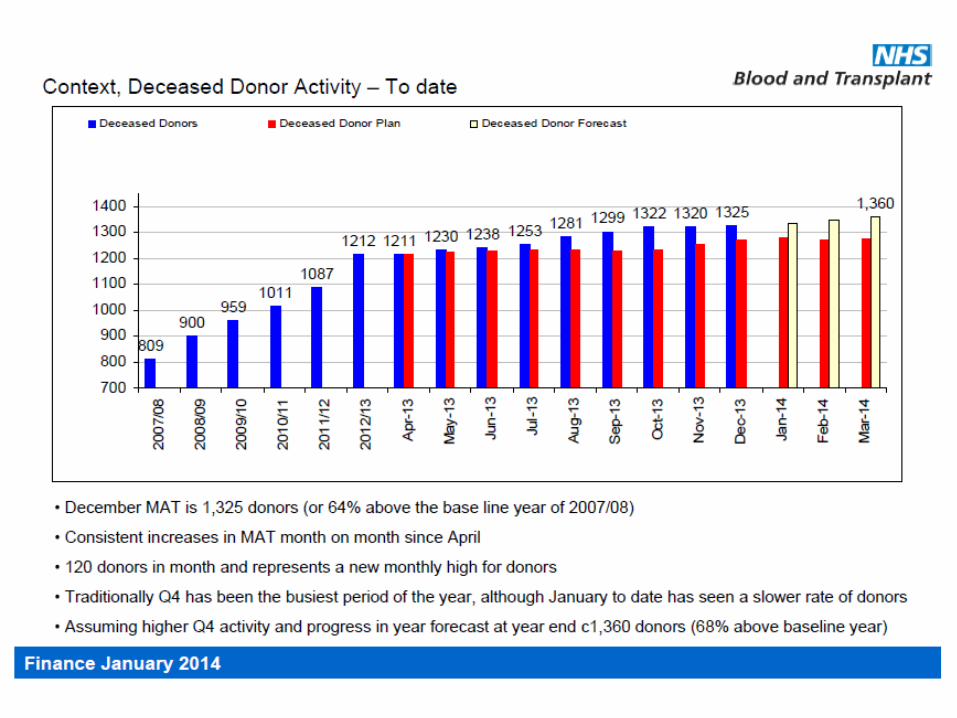
Current UK donor and transplant activity
Current year(01.04.13 – 12.01.14)
Previous year(01.04.12 – 12.01.13)
% ChangePrevious full financial year(2012/2013)
ORGAN DONORS
Donors after brain death 611 532 14.8 705
Donors after circulatory death
438 387 13.2 507
Total deceased donors 1049 919 14.1 1212
Deceased donors (DD) transplants
Kidney 1543 1320 16.9 1750
Pancreas 20 29 -3.1 37
Kidney/pancreas 151 123 22.8 166
Pancreas islets 27 27 0 30
Heart 155 106 46.2 142
Lung(s) 167 145 15.2 188
Liver 678 591 14.7 775
Total DD transplants 2711 2363 17.3 3113

Number of donors, April 1st to January 12th
2003/4 – 2013/4
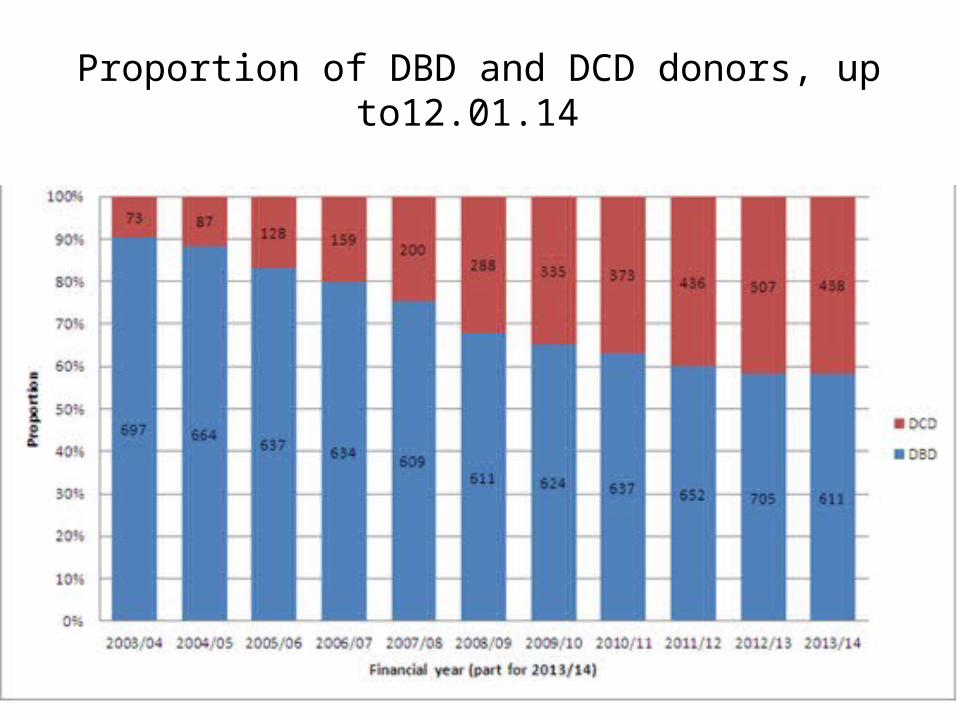
Proportion of DBD and DCD donors, up to12.01.14

Key DBD rates

Number of patients at each stage of pathway

Age proportions of actual donors

Age distributions along the DBD organ donation pathway (1)

Age distributions along the DBD organ donation pathway (2)

Key DBD rates for 18 to 34 year olds

Education and Training
NODC Terms of ReferenceTo lead the design and delivery of training and development opportunities for clinical staff involved in the care of potential deceased organ donors, including (but not limited to)
– refresher courses for CLODs and Donation Committee Chairs
– the National Donation Congress,
– relevant areas of the NHSBT organ donation microsite and organ donation toolkit
– the Map of Medicine organ donation pathways

Education and Training
a) Evaluation of doctors/nurses attitudes, knowledge & training towards organ and tissue donation (Tim Collins)
b) National Donation and Transplantation Congress (Paul Murphy / Olive McGowan)
c) Training course for ICM trainees (Dale Gardiner)
d) Role of NODC in education and training (all)

Updates
a) ACCORD (Paul Murphy / Sally Johnson)
b) DePPart (Dale Gardiner)
c) NICE Guidance (Gus Vincent)
d) Scout Pilot (Gerlinde Mandersloot)
e) UK DEC (Dale Gardiner / Paul Murphy)
i. Heparin in DCD
ii. Draft Guidance in DBD
iii. Workshop on future workstreams (7th March, London)
f) TOT2020 (Sally Johnson / James Neuberger)
i. Workforce review (Anthony Clarkson for Ella Poppitt)
g) Substitution Study (Alex Manara / James Neuberger)
h) Statistics Group (Jo Allen)

ACCORD
• EU funded programme• UK leading workstream 5
– Promoting cooperation between ICUs and donor transplant coordination
– Impact of end of life care on organ donation• 17 participating member states
• 66 participating hospitals
• WS5 design– Audit of ≥ 20 consecutive patients dying of brain injury in 6
month study period (1670 completed patient Qs) – Change methodology training and action plans– Re-evaluation

ACCORD: country questionnaire
•DCD programme
•Legal definition of death
•Guidance for
–diagnosis of brain death
–care of potential donors
–ethical guidance
–withdrawal of life sustaining treatments
–donor identification and referral
–family approach
•Training
•National and / or regional OPOs
•Regulatory authority
Donor rate by number of positive national indicators for organ donation
Portugal
GermanyHungary
Slovenia
Croatia
Lithuania
Rep. Ireland
Greece
Italy
Netherlands
Spain
LatviaEstonia
France
UK
0
5
10
15
20
25
30
35
40
5 6 7 8 9 10 11
Number of positive indicators
Do
no
r ra
te p
mp
(20
11)
No DCD programme
DCD programme

Care paradigms of study patients
0% 20% 40% 60% 80% 100%
CROATIA (66)
ESTONIA (94)
FRANCE (87)
GERMANY (40)
GREECE (28)
HUNGARY (56)
IRELAND (31)
ITALY (75)
LATVIA (12)
LITHUANIA (81)
PORTUGAL (43)
SLOVENIA (18)
SPAIN (413)
NETHERLANDS (95)
UK (531)
ALL MS (1670)
A: Full active treatment on CCU until the diagnosis of BD
B: Full active treatment until unexpected cardiac arrest from which the patient could not be resuscitated
C: Admitted to CCU to incorporate organ donation into end-of-life care
D: Full active treatment on CCU until the decision of withdrawal or limiting life sustaining therapy was made, withan expected final cardiac arrestE: Not admitted, or admitted to CCU but subsequently discharged

proceeding DCD, n = 35
0
50
100
150
200
250
300
1 7 13 19 25 31 37 43 49 55 61 67 73 79 85 91 97 103 109 115
time after withdrawal (min)
sy
sto
lic
BP
(m
mH
g)
Heparin and DCD
Time from SBP< 50 to asystole (min):
median 5
minimum 1
maximum 26
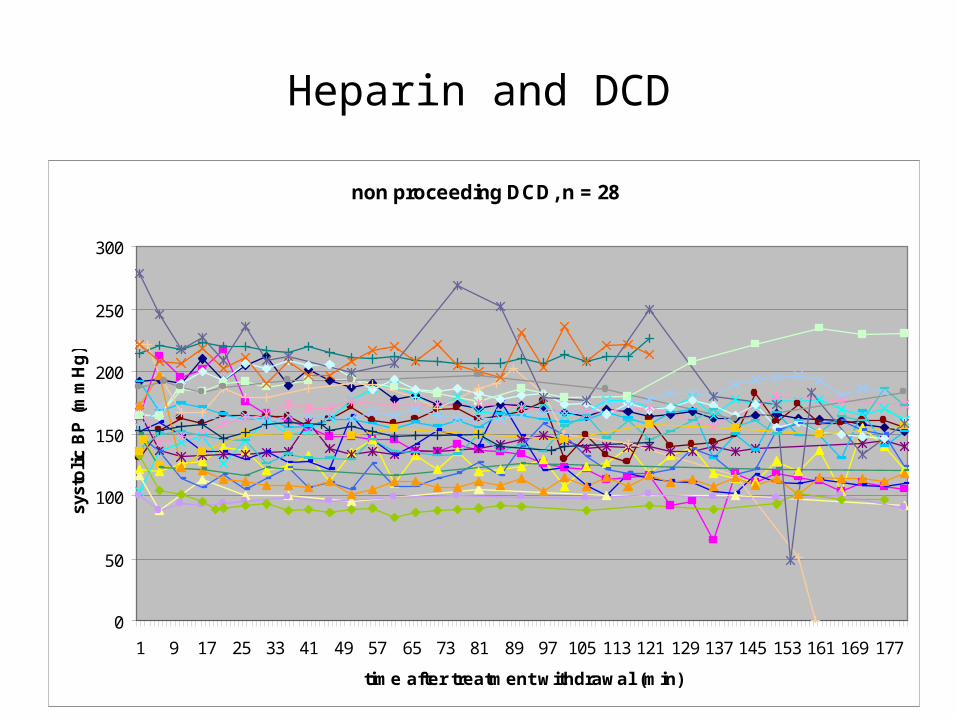
Heparin and DCD
non proceeding DCD, n = 28
0
50
100
150
200
250
300
1 9 17 25 33 41 49 57 65 73 81 89 97 105 113 121 129 137 145 153 161 169 177
time after treatment withdrawal (min)
syst
oli
c B
P (
mm
Hg
)

Regional Collaboratives
a) Vision for regional collaboratives (Dale Gardiner)
b) Reports from regional collaboratives, outcomes from this
year’s work, priorities for 2014/15 and update on the
promotion of the family approach material (Regional
Managers / Regional CLODs)
c) Overview (all)

National Donation Committee – Terms of Reference
• Service development
– To act as a source of advice and assistance to NHSBT in the development and implementation of strategies to increase organ, corneal and tissue donation
– To provide a forum for identifying and spreading best practice across the UK
– To assist NHSBT to improve and optimise all aspects of donation to enable more transplants to take place,
• Representative and performance
– To represent, lead and support the UK wide network of Donation Committees and Regional Collaboratives ensuring that regional issues are raised and shared at a national level
• Education and training
– To lead the design and delivery of training and development opportunities for clinical staff involved in the care of potential deceased organ donors
• Consultative
– To promote effective dialogue and collaboration between relevant professional groups and the Colleges and Societies that may represent them,
• Research
– To sponsor and support research, development and audit relevant to deceased donation, including (but not limited to) the analysis and future development of the Potential Donor Audit
• To commission a small number of working subgroups that will deliver the key objectives of the committee

National Donation Committee – membership
National Clinical Lead for Organ DonationDeputy National Clinical Lead for Organ DonationNational Clinical Lead for Donor OptimisationNational Clinical Lead for Governance
Associate Medical Director for Organ Donation and Transplantation
Regional Clinical Leads – Scotland– Midlands – Yorkshire and Humber– South East Coast – East of England – North West – London – Northern – South Central– South East– South West– South Wales
Donation Committee Chair
Director, Organ Donation and TransplantationAssistant Director for Operations, Organ DonationHead of Service DevelopmentHead of Service DeliveryLead Nurse for Health Informatics
Regional Managers for Organ Donation– London and Northern Ireland– South East and Eastern England– South West and South Wales– Northern and Scotland– Midlands and South Central– North West and Northern
Statistics and Clinical Studies, NHSBT
Professional representatives – Royal College of Anaesthetists– Faculty of Intensive Care Medicine – Intensive Care Society– British Association of Critical Care Nursing– College of Emergency Medicine– Royal College of Child Health and Paediatrics /
Paediatric Intensive Care Society – British Transplantation Society– Society of British Neurological Surgeons

National Donation Committee - contributions
• Donor identification and referral policy
• Family approach Best Practice Guide and DVD
• National Donation Congress 2012 and National Donation and Transplantation Congress 2013
• Review of Map of Medicine pathways
• National pilot of simulation training for ICM trainees
• St John Award
• Scout pilot
• Club 32
• Taking Organ Transplantation to 2020
• Development of the clinical microsite
• Regional Organ Donation Roadshows 2013
• DBD / DCD substitution study

National Donation Committee – proposals
• Option 1 – streamlined status quo
Accept the reality of the landscape for deceased donation in the UK, but reconsider the need for both the Regional Manager and Regional Clinical Lead to attend all meetings.
• Option 2 – disentangle the various responsibilities of the National Donation Committee and support each separately
Limit the National Organ Donation Committee to the original advisory and consultative roles of the Donation Advisory Group, reducing frequency of meetings accordingly. Fulfill other responsibilities of the National Donation Committee through separately supported groups and pathways
• Option 3 – hybrid option
Reduce frequency and objectives of full meetings of the National Donation Committee. Formally establish subgroups with the following responsibilities:
–Consultative
–Education and training
–Research, statistics and audit
–Service development
–Performance