national mental health intelligence network introduction to network and profiling tools cam lugton...
TRANSCRIPT
National Mental Health Intelligence Network
Introduction to network and profiling tools
Cam LugtonHead of Intelligence – Mental Health (NMHDNIN)

About us • National Mental Health Intelligence Network (NMHIN) is part of
the National Mental Health Dementia and Neurology Intelligence Network (NMHDNIN)
• Launched in June 2014; came into being 6 months earlier
• One of 5 Health Intelligence Networks led by PHE
• Core staff – MH: 8 people, 6wte – MHDN 13 people, 11wte. But the network is everyone that’s interested
• PHE funded but support the whole system / care pathways
• Each area (i.e. MH, Dementia) chaired by the relevant NHS National Clinical Director

Our remit: PHE intelligence networks remit
• Turn data into meaningful health intelligence to inform the planning and delivery of high quality, cost-effective services
• Work with partners and stakeholders to agree priorities, increase efficiency, drive innovation, and deliver effectively
• Ensure intelligence is understood and used to improve the health and wellbeing of the population and reduce inequalities
• Practical support to strategic clinical networks and other local partners
• Eyes on the long term prize:
– Data linkage across clinical pathways and external agencies
– Translation of research findings
– shift in resources towards primary and secondary prevention
– Better outcomes and reduced health inequalities
Where to access the Network:• http://www.yhpho.org.uk/mhdnin
Where to access the tools:• http://fingertips.phe.org.uk/profile-group/mental-health/

Demonstration of NMHIN tools:
using the Suicide Prevention Profile

Introduction


Profile structure: data held in 3 domains
Note: ‘Suicide data’ is presented at local authority level only, ‘Related risk factors’ and ‘Related service contacts’ include data presented at both local authority and CCG level

Suicide data
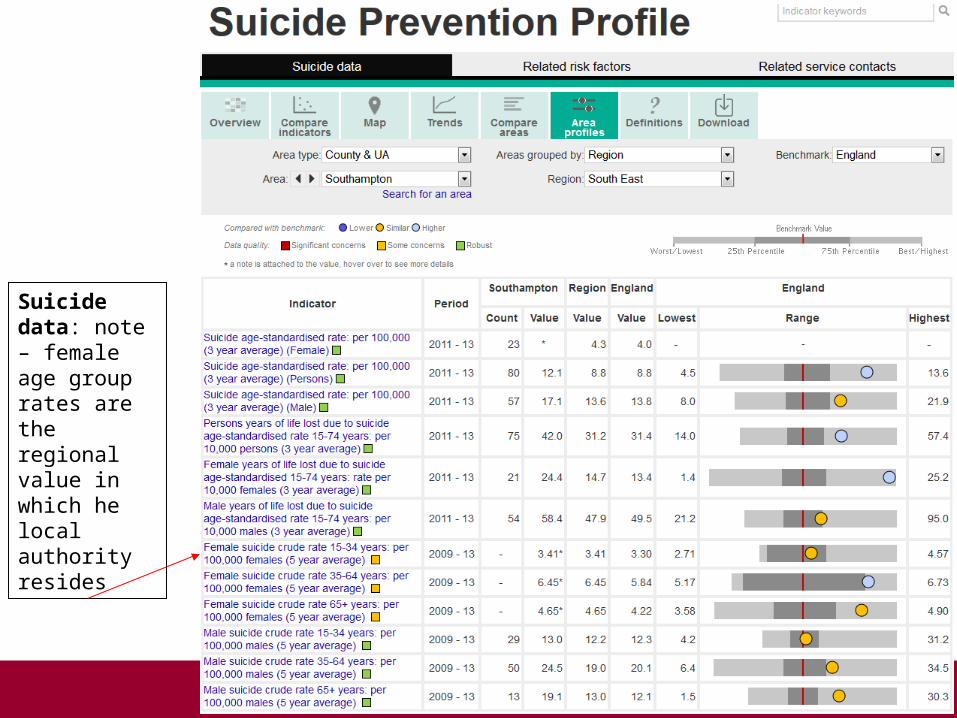
Suicide data: note – female age group rates are the regional value in which he local authority resides
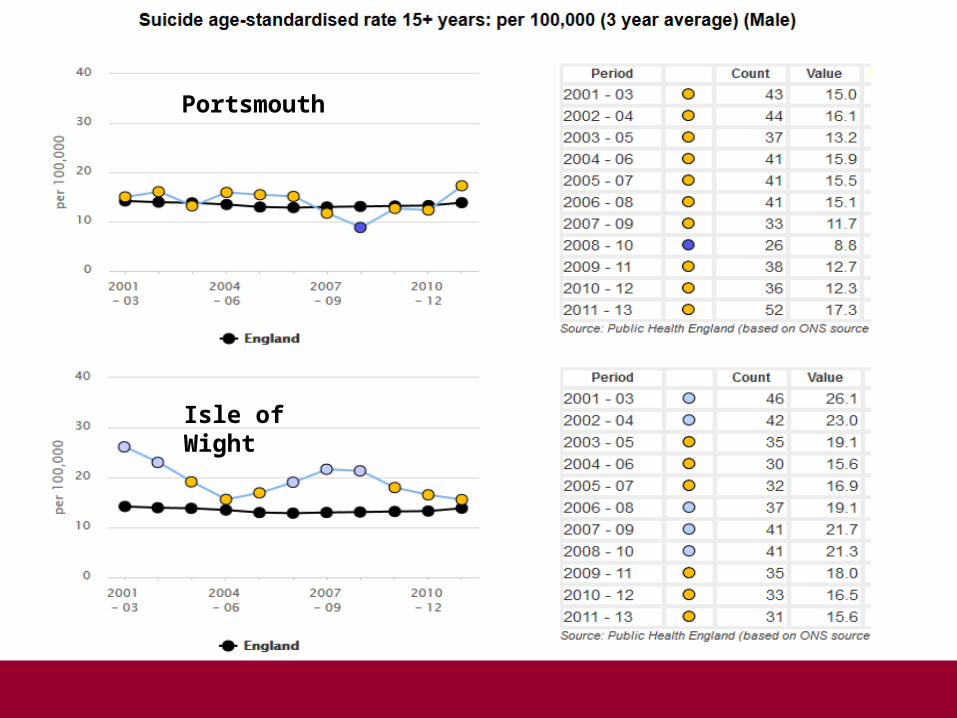
Portsmouth
Isle of Wight
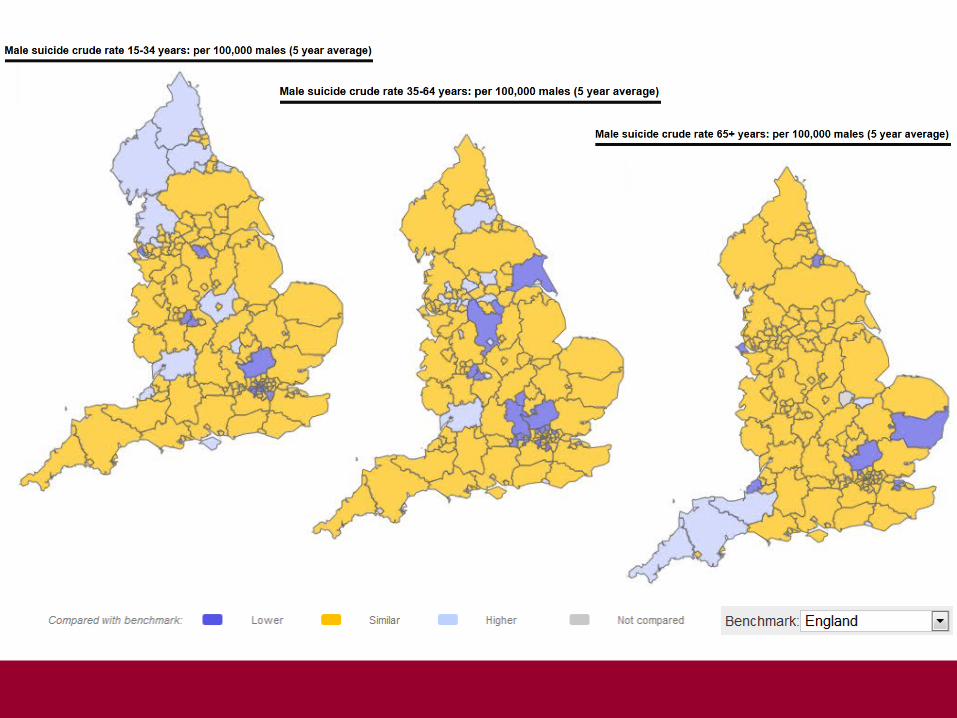

South East– male age specific crude suicide rates per 100,000 (5 year average)

Female years of life lost due to suicide: age standardised rate 15 – 74 years: per 10,000 males (3 year average)

Related risk factors
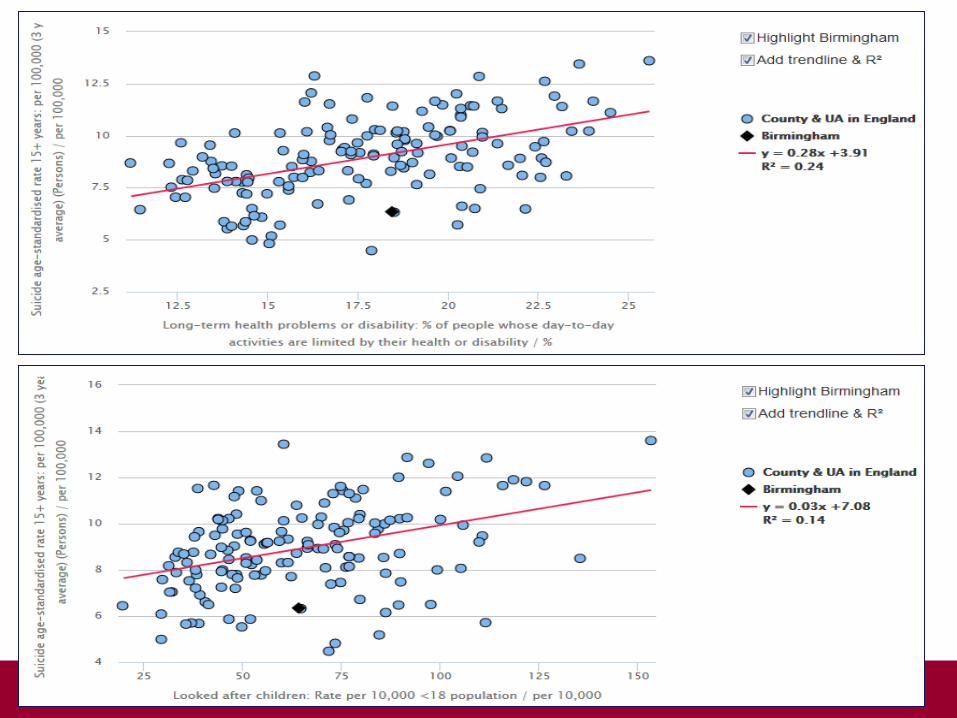

Related risk factors
Portsmouth 11.6 per 100,000 East Sussex 11.0 per 100,000

Related service contacts


Related service contacts – local authority data
Portsmouth 11.6 per 100,000 East Sussex 11.0 per 100,000

Related service contacts – CCG data
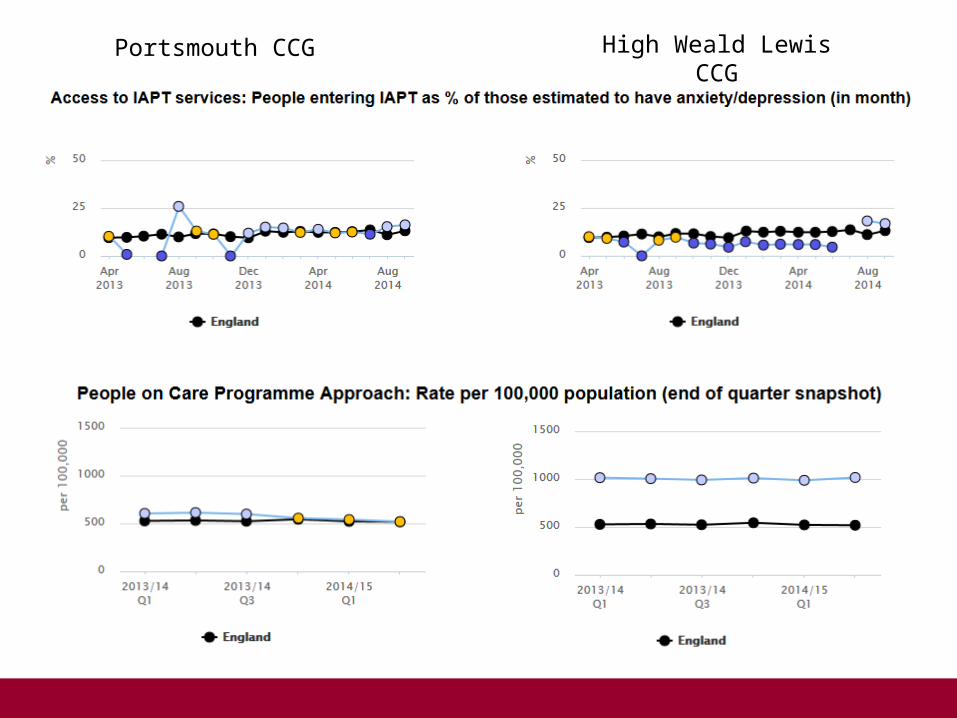
Portsmouth CCG High Weald Lewis CCG

And rest…
Any questions / comments?

SMI profiling tool:
building a profile – an example using Brighton and Hove
condition counts / estimates and
comparison methodology
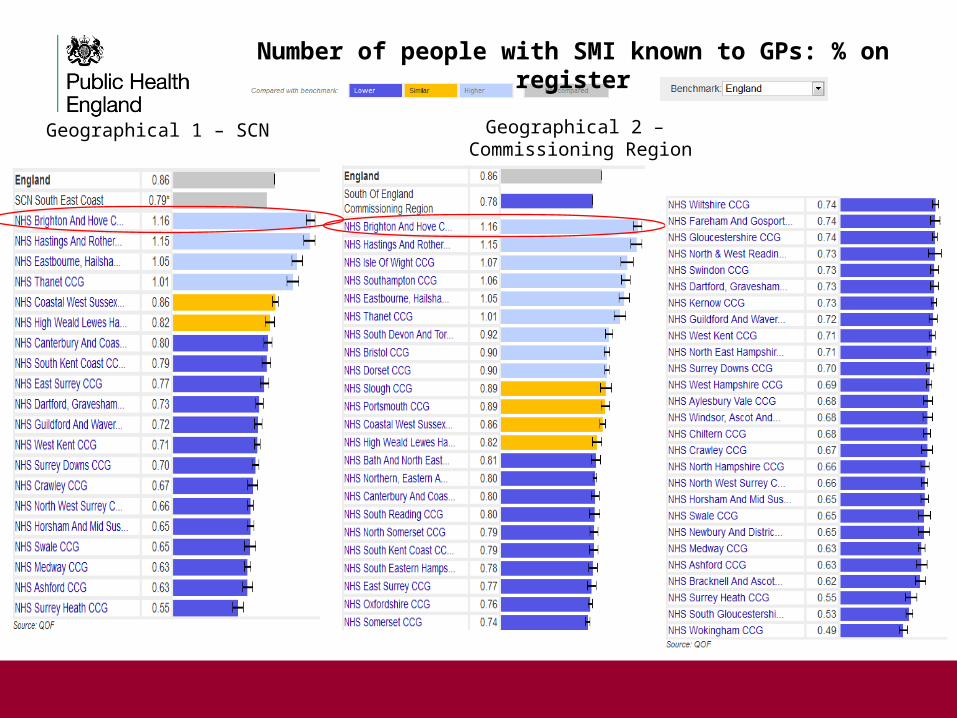
Geographical 1 – SCN Geographical 2 – Commissioning Region
Number of people with SMI known to GPs: % on register

Statistical 1 – deprivation decile
Statistical 2 – CCG Cluster
Number of people with SMI known to GPs: % on register

Geographical neighbours Statistical neighbours: deprivation
Risk Profiling


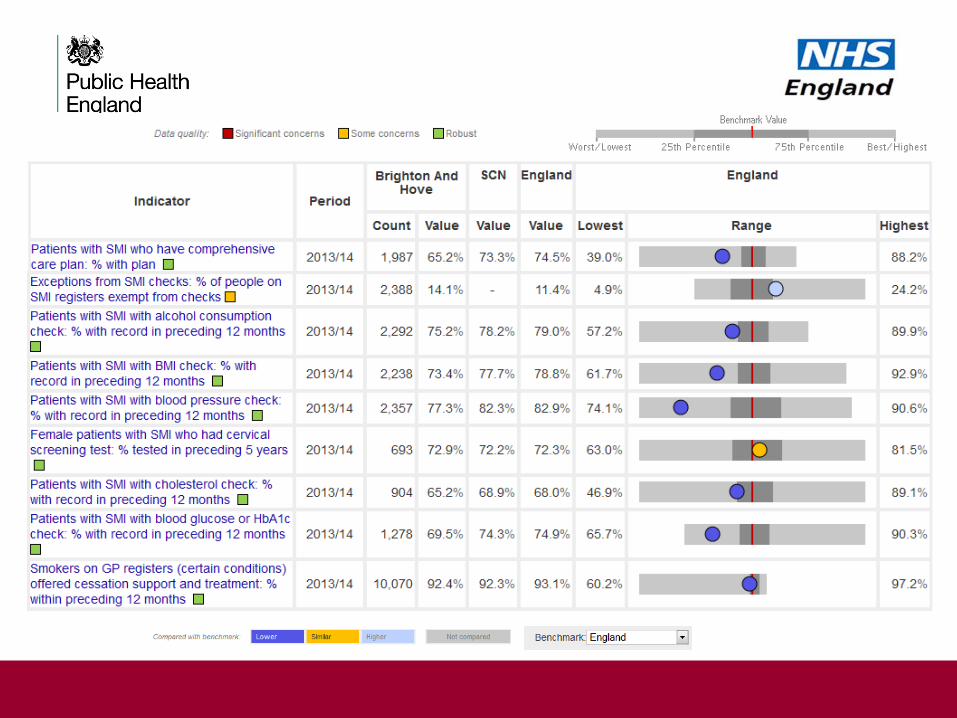
Care in Primary Care:
1. proportion of SMI exceptions 2. Health checks

Geographical neighbours Statistical neighbours: deprivation

Accessing care:
1. Early Intervention in Psychosis 2. Use of Mental Health Act
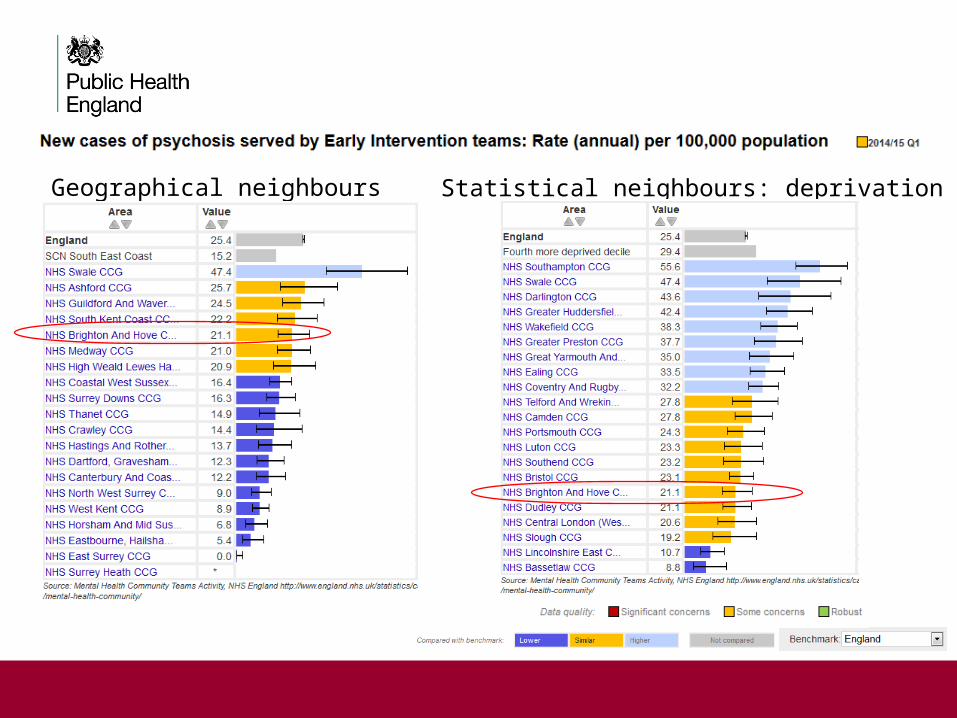
Geographical neighbours Statistical neighbours: deprivation

Geographical neighbours Statistical neighbours: deprivation
B&H Trend
Whole system assessment:

Common Mental Health Disorders
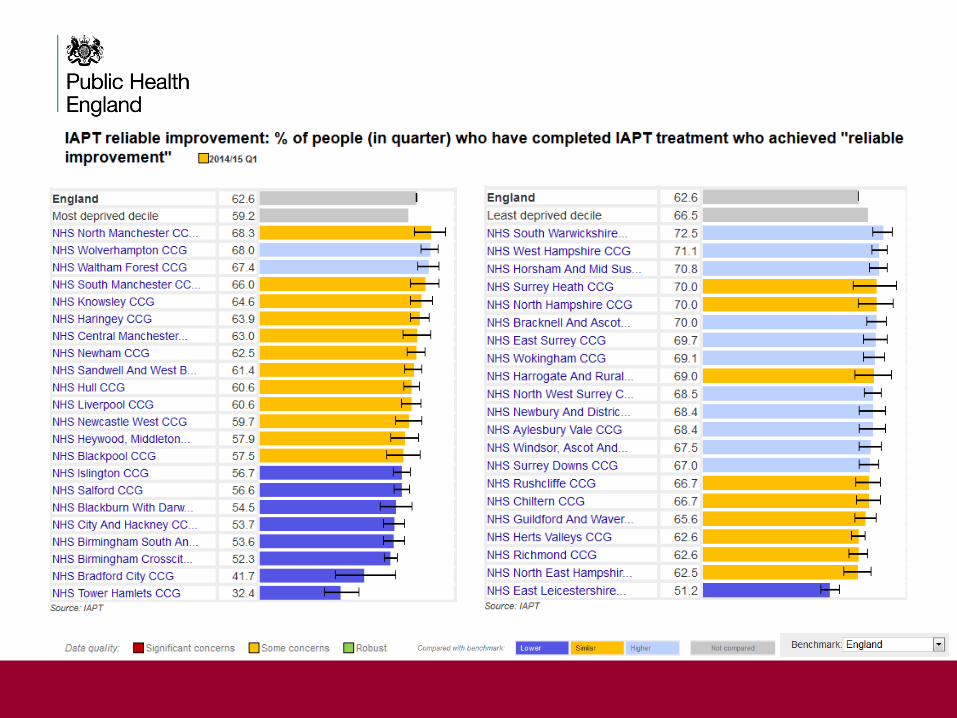
Use of Improving Access To Psychological Therapies
Statistical group comparison



Moving Forward
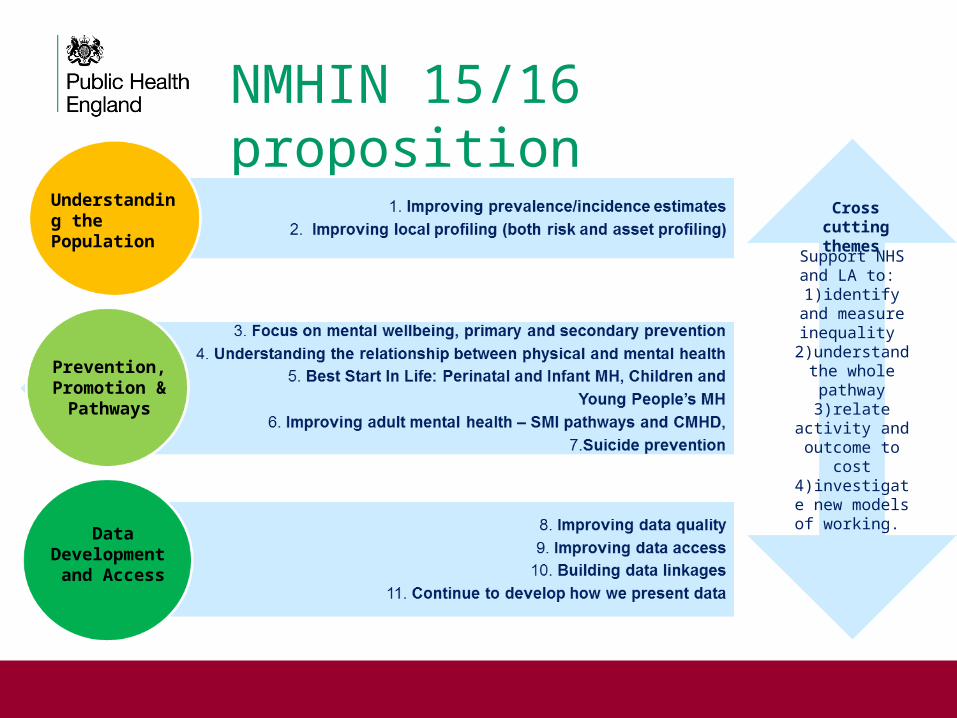
NMHIN 15/16 proposition
Understanding the Population
Prevention, Promotion &
Pathways
Data Development and Access
Support NHS and LA to:
1)identify and measure
inequality 2)understand
the whole pathway
3)relate activity and outcome to
cost4)investigate
new models of working.
Cross cutting themes

In terms of what we will deliver, that means:
1)Support product use
2)Product outputs:
a. Profiling tools
b. Intelligence products
c. Website
3)Data development
4)Measure impact & seek feedback
NMHIN 15/16 proposition

Products Process
User guides: general and product specific. •Priority is to develop a JSNA toolkit
Deliver programme of promotional and product use presentations and workshops
Video aids – current: Intro to network, intro to profile tools planned: product and process specific items
Support PHE Local Contribution Leads and Knowledge Transfer Facilitators to present / train NMHIN products
Promotional presentations: general and product specific Support appropriate SCN staff / members to use and encourage use / train on MHIN products
Encouraging use presentations: topic and product specific Run series of product and process focussed webinars
Training materials: feed into existing programmes / develop MHIN specific modules
Routine engagement with knowledge facilitators (PHE, SCNs) to provide updates and receive feedback
Effectively measure impact
Support product use
No point in intelligence products unless people know about & use them.
To ensure that happens we will deliver the following:
Stakeholder engagement is essential.
We need to know that: people know about products, products are used well, products are fit for purpose, users tell us what else is required.

Tool Planned development Potential development
SMI Provider level view of data – NHSBN + moreLA view of MHLDDS dataAdd new psychosis prevalence estimatesFlow waiting time & access pathway metrics
Condition based data – through C&P file or diagnosis dataAdd high level pathwaysData split by age group
CMHD Condition based view of IAPTAverage number of sessionsRange of service available
Specialist care role in CMHD Better use of benefits and carer dataIAPT employment metrics
CYPMHW Preparation for major expansion in response to forthcoming CAMHs dataset (inc CYP IAPT)
CESMMHI Update routinely and review content
Suicide prevention
Review / add to current contentAdditional data items at MH Trust level
Across tools Improve metrics for prevention & finance Improve non health care provider content
Profiling tools
• More tools? If so on what topics? Perinatal MH, Crisis, AMH pathway specific
• More data? What topics / organisations are missing? Police, CJS
• Less data? Fewer data items but more ‘indicators’?
• In tool guidance / interpretation? Rationale for inclusion, evidence base, triangulation
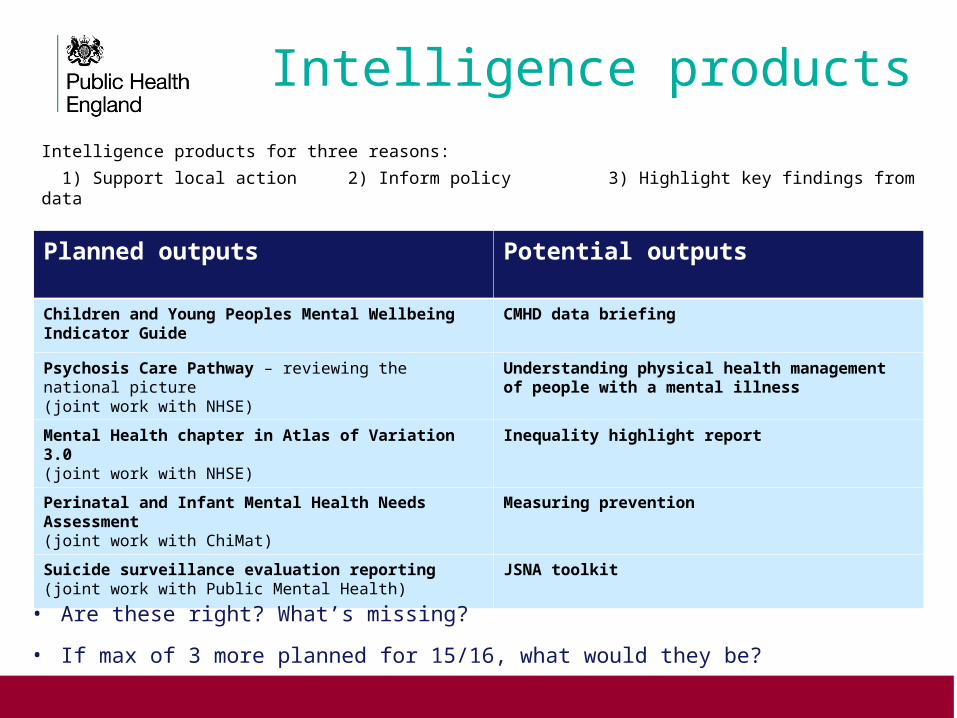
Planned outputs Potential outputs
Children and Young Peoples Mental Wellbeing Indicator Guide
CMHD data briefing
Psychosis Care Pathway – reviewing the national picture (joint work with NHSE)
Understanding physical health management of people with a mental illness
Mental Health chapter in Atlas of Variation 3.0(joint work with NHSE)
Inequality highlight report
Perinatal and Infant Mental Health Needs Assessment (joint work with ChiMat)
Measuring prevention
Suicide surveillance evaluation reporting(joint work with Public Mental Health)
JSNA toolkit
Intelligence productsIntelligence products for three reasons:
1) Support local action 2) Inform policy 3) Highlight key findings from data
• Are these right? What’s missing?
• If max of 3 more planned for 15/16, what would they be?

Work area
Planned action Potential action
New data • Prevalence: psychosis and CMHD?• Flow waiting times & access metrics• Flow outcome & improvement measures
• Develop pathway prevalence estimates (Perinatal, PD, ED) + flow APMS & CAMHS
• Develop / flow prevention metrics• Flow new data sources (police, CJS)
Data use • Improve efficiency of data flow e.g. combine months, rates at source
• Improve use of existing sources (C&P, NHSBN, Programme Budget & other finance)
• Review / revise Fingertips population methodology
Data quality • Aim for all ‘green’ data items• Focus on topic specific areas of concerns• Issue resolution e.g. MH LD data split• Review use of best data (e.g. carers, social care)
• Join work to resolve diagnosis issues• Role in validation of QOF data / fill gaps on
stepped down data items
Data access • Access MHLDDS & HES to add data items
Data linkage
• Link primary & secondary care data – work with key areas and prep for care.data
• Link MHLDDS & HES: outputs to include perinatal MH and understanding physical health
Data development
This work area has defined outputs but needs the space to be developmental
How much does the data quality agenda sit with NMHIN and how much elsewhere?

If you would like a video introduction to the network or a guide to using the tools please go to:
http://www.yhpho.org.uk/resource/view.aspx?RID=207312.