my work: bledsoe brace custom order form
TRANSCRIPT
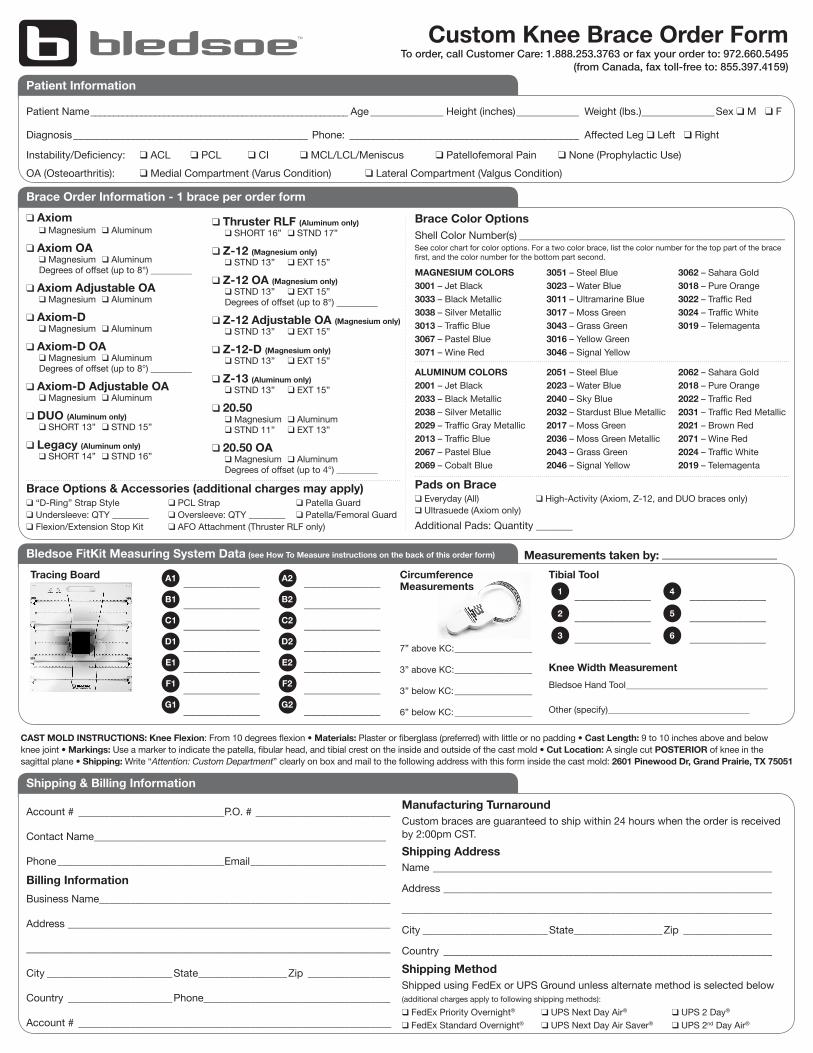
Brace Order Information - 1 brace per order form
Shipping & Billing Information
Account # ____________________________P.O. # __________________________
Contact Name ________________________________________________________
Phone ________________________________Email __________________________Shipping AddressName _________________________________________________________________
Address _______________________________________________________________
_______________________________________________________________________
City ________________________State _________________Zip _________________
Country _______________________________________________________________
MAGNESIUM COLORS3001 – Jet Black3033 – Black Metallic3038 – Silver Metallic3013 – Traffic Blue3067 – Pastel Blue 3071 – Wine Red
3051 – Steel Blue3023 – Water Blue3011 – Ultramarine Blue3017 – Moss Green3043 – Grass Green3016 – Yellow Green3046 – Signal Yellow
3062 – Sahara Gold3018 – Pure Orange3022 – Traffic Red3024 – Traffic White3019 – Telemagenta
See color chart for color options. For a two color brace, list the color number for the top part of the brace first, and the color number for the bottom part second.
Shell Color Number(s) ___________________________________________________
ALUMINUM COLORS2001 – Jet Black2033 – Black Metallic2038 – Silver Metallic2029 – Traffic Gray Metallic2013 – Traffic Blue2067 – Pastel Blue2069 – Cobalt Blue
2051 – Steel Blue2023 – Water Blue2040 – Sky Blue2032 – Stardust Blue Metallic2017 – Moss Green2036 – Moss Green Metallic2043 – Grass Green2046 – Signal Yellow
2062 – Sahara Gold2018 – Pure Orange2022 – Traffic Red2031 – Traffic Red Metallic2021 – Brown Red2071 – Wine Red2024 – Traffic White2019 – Telemagenta
Manufacturing TurnaroundCustom braces are guaranteed to ship within 24 hours when the order is received by 2:00pm CST.
Billing Information
Business Name _________________________________________________________
Address _______________________________________________________________
_______________________________________________________________________
City ________________________State _________________Zip _________________
Country ____________________Phone ____________________________________
Account # ____________________________________________________________
Shipping MethodShipped using FedEx or UPS Ground unless alternate method is selected below (additional charges apply to following shipping methods):q FedEx Priority Overnight® q UPS Next Day Air® q UPS 2 Day®
q FedEx Standard Overnight® q UPS Next Day Air Saver® q UPS 2nd Day Air®
q Axiom q Magnesium q Aluminum
q Axiom OA q Magnesium q Aluminum Degrees of offset (up to 8°) _________
q Axiom Adjustable OA q Magnesium q Aluminum
q Axiom-D q Magnesium q Aluminum
q Axiom-D OA q Magnesium q Aluminum Degrees of offset (up to 8°) _________
q Axiom-D Adjustable OA q Magnesium q Aluminum
q DUO (Aluminum only) q SHORT 13” q STND 15”
q Legacy (Aluminum only) q SHORT 14” q STND 16”
q Thruster RLF (Aluminum only) q SHORT 16” q STND 17”
q Z-12 (Magnesium only) q STND 13” q EXT 15”
q Z-12 OA (Magnesium only) q STND 13” q EXT 15” Degrees of offset (up to 8°) _________
q Z-12 Adjustable OA (Magnesium only) q STND 13” q EXT 15”
q Z-12-D (Magnesium only) q STND 13” q EXT 15”
q Z-13 (Aluminum only) q STND 13” q EXT 15”
q 20.50 q Magnesium q Aluminum q STND 11” q EXT 13”
q 20.50 OA q Magnesium q Aluminum Degrees of offset (up to 4°) _________
Brace Options & Accessories (additional charges may apply)q “D-Ring” Strap Style q PCL Strap q Patella Guardq Undersleeve: QTY ________ q Oversleeve: QTY ________ q Patella/Femoral Guardq Flexion/Extension Stop Kit q AFO Attachment (Thruster RLF only)
Brace Color Options
Pads on Braceq Everyday (All) q High-Activity (Axiom, Z-12, and DUO braces only)q Ultrasuede (Axiom only) Additional Pads: Quantity _______
CAST MOLD INSTRUCTIONS: Knee Flexion: From 10 degrees flexion • Materials: Plaster or fiberglass (preferred) with little or no padding • Cast Length: 9 to 10 inches above and below knee joint • Markings: Use a marker to indicate the patella, fibular head, and tibial crest on the inside and outside of the cast mold • Cut Location: A single cut POSTERIOR of knee in the sagittal plane • Shipping: Write “Attention: Custom Department” clearly on box and mail to the following address with this form inside the cast mold: 2601 Pinewood Dr, Grand Prairie, TX 75051
Bledsoe FitKit Measuring System Data (see How To Measure instructions on the back of this order form)
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________
_____________7” above KC: _________________
3” above KC: _________________
3” below KC: _________________
6” below KC: _________________
Knee Width MeasurementBledsoe Hand Tool _______________________________
Other (specify) _______________________________
Measurements taken by: ____________________Tibial ToolTracing Board Circumference
MeasurementsA1 A2
1 4B1 B2
2 5C1 C2
3 6D1 D2
E1 E2
F1 F2
G1 G2
Custom Knee Brace Order FormTo order, call Customer Care: 1.888.253.3763 or fax your order to: 972.660.5495
(from Canada, fax toll-free to: 855.397.4159)
Patient Information
Patient Name ________________________________________________________ Age ______________ Height (inches) ____________ Weight (lbs.) ______________Sex q M q F
Diagnosis _____________________________________________ Phone: ____________________________________________ Affected Leg q Left q Right
Instability/Deficiency: q ACL q PCL q CI q MCL/LCL/Meniscus q Patellofemoral Pain q None (Prophylactic Use)OA (Osteoarthritis): q Medial Compartment (Varus Condition) q Lateral Compartment (Valgus Condition)

Note: Make sure the base of the Tracing Guide is on the Tracing Board and one side of the Tracing Guide is against the leg.
Circumference Measurements1. With the patient’s foot dorsi flexed and quad muscles tightened, use the Tape Measure to take circumference measurements at the four locations
marked on the patient’s leg in step B1. 2. Record the four leg circumferences on the Order Form.
Positioning the Leg1. Attach the Knee Pillow to the Tracing Board.2. Center the patient’s knee over the Knee Pillow.
1
Mark the Patient’s Leg1. Using the reference marks on the Tracing Board and the Marker provided, mark the patient’s leg at 3” and 7” above mid-patella and 3” and 6” below mid-patella.
1
B
C Trace the Leg1. Insert the Marker into the Tracing Guide.
2. With the patient’s foot dorsi flexed and quad muscles tightened, making light contact with the leg simply mark the profile of the leg at each point where the leg intersects the horizontal lines. 3. Repeat step D2 for the other side of the leg. 4. Record the values from the Tracing Board where the marked spot crosses each of the scales on the Order Form.
1 2
4
3D
Tibial Hand Tool1. Have patient stand for measuring.2. Visually align your sight with the
patient’s knee.3. Measure 6 inches below mid patella and mark. Align the upper surface of the measuring tool with the mark.4. Take Knee Width Measurement: Place the Tibial Hand Tool at the knee joint line, located where the leg crosses over D1/D2 of the tracing board. Compress the device so the front paddle is lightly touching the knee cap and the side paddles lightly touch the sides of the knee joint. Record the value from the #6 position onto Knee Width Measurement section of the Custom Brace Order Form.
E Measure the Tibia1. Loosen the lock knob on the underside of the Tibial Hand Tool. Grasp
the two finger rings and open the tool wider than the leg. With the tool aligned with the front to back axis mark, slide the two finger rings together until all three vertical positioning plates touch the leg without indenting the soft tissue. All should contact at the front and both sides of the leg.2. Tighten the lock knob to secure this position without indenting.
1F
Record Measurements1. Hold the Tibial Hand Tool in position and slide each pin in towards the front of the leg until it touches the soft tissue without indenting.
2. Remove the Tibial Hand Tool by sliding it outwards from the front of the leg.3. Hold the Tibial Hand Tool level and read the position of each scale numbered 1 through 6. 4. Record measurements on Order Form.
G 1
2
2
2
3
How To MeasureFor trained personnel only
For more information, call Customer Care: 1.888.253.3763
A
CP010120 Rev G 01/12