mutation - cftrscience | clinician's guide to cftr · patients having a class i, ii, or iii...
TRANSCRIPT
A Quick Guide to the
MutationR117H
C F T R S C I E N C E
© 2016 Vertex Pharmaceuticals Incorporated | VXR-HQ-02-00045a(1) | 03/2016

Loss of CFTR activity is the underlying cause of cystic fibrosis (CF)1
• People with 2 CFTR mutations resulting in loss of CFTR activity generally have a CF phenotype, which may include1-3,6
– Elevated sweat chloride (>60 mmol/L)
– Pancreatic insufficiency
– CBAVD a
– Lung function decline over time
– Pseudomonas aeruginosa colonization
aCBAVD, congenital bilateral absence of the vas deferens.
References: 1. Davis PB et al. Am J Respir Crit Care Med. 1996;154(5):1229-1256. 2. Rowe SM et al. Proc Am Thorac Soc. 2007;4(4):387-398. 3. Zielenski J. Respiration. 2000;67(2):117-133. 4. Sheppard DN et al. Nature. 1993;362(6416):160-164. 5. Welsh MJ, Smith AE. Cell. 1993;73(7): 1251-1254. 6. Castellani C et al. J Cyst Fibros. 2008;7(3):179-196.
Some CFTR mutations result in little to no CFTR activity3-5
0% 100%
Total CFTR Activity
0% 100%
Total CFTR Activity
Some CFTR mutations result in residual or partial CFTR activity3-5
Spectrum of Phenotypes Associated With Total CFTR Activity1,2
Total CFTR Activity
% of Normal
No CF Disease
CFTR-relatedDisorders
Cystic Fibrosis
Individuals with 2 normal alleles and CFTR mutation carriers
Clinical entities associated with CFTR dysfunctionthat do not fulfill diagnostic criteria for CF, e.g., CBAVD, acute recurrent or chronic pancreatitis and bronchiectasis
Typical phenotype: sinopulmonary disease, sweatchloride >60 mmol/L, pancreatic insufficiency, appearing early in life. In some patients, progressionof disease is delayed or not all features are present
100%
0%
Clinical Phenotype
2

Levels of CFTR activity affect survival in CF1
References: 1. McKone EF et al. Chest. 2006;130(5):1441-1447. 2. The World Bank. http://data.worldbank.org/indicator/SP.DYN.LE00.IN?page=2. Accessed November 12, 2015. 3. MacKenzie T et al. Ann Int Med. 2014;161:233-241.
1.00
0.75
0.50
0.25
0.00
0 10 20
Risk Time (Age)
Surv
ival
Pro
babi
lity
30 40 50
Residual CFTR activity (Class IV, V): R117H, R334W, R347P, 3849+10KbC–›T, 2789+5G–›A, A455E
Severely reduced CFTR activity (Class I, II, III): G542X, R553X, W1282X, R1162X, 621-IG–›T, 1717-1G–›A, 1078delT, 3659delC, I507del, N1303K, S549N, G85E, F508del, G551D, R560T
n=1126
n=14,525
• Life expectancy in Western countries (general population born in 2000) is ~79 years2
• Between 1993 and 2002, median survival for US patients with genotypes associated with little to no CFTR activity was 36.3 years (95% CI, 35.5 to 37.6 years), while median survival for those having genotypes associated with residual CFTR activity was 50 years (95% CI, 47.1 to 55.9 years)1
– In this study, R117H was considered only as a Class IV CFTR mutation and patients were part of the residual CFTR activity group
• More recent US data (2000-2010) suggest median survival across genotypes continues to improve3
Survival Curves by CFTR Activity During a 10-Year Follow-Up (1993-2002) of Patients From the US CFF Registrya
a Data are from a retrospective study of patients enrolled in the Cystic Fibrosis Foundation patient registry measuring risk of death over a 10-year observation period from 1993 to 2002. Patients were grouped as having a high-risk or low-risk genotype based on the functional effects of their class of CFTR mutation on phenotype and mortality. Patients having a Class I, II, or III mutation on both alleles were considered high-risk, while patients having at least 1 Class IV or V mutation were categorized as low-risk. A total of 15,651 patients had a CFTR genotype of a known functional class; 14,525 (93%) had a high-risk CFTR genotype and 1126 (7%) had a low-risk CFTR genotype.1
These data represent population-based outcomes.1 Individual outcomes in cystic fibrosis are variable.
Adapted with permission from McKone EF et al. Chest. 2006;130(5):1441-1447.
3

• In the CFTR2 global database, ~2% of patients with CF have at least 1 copy of the R117H mutation2
References: 1. Sheppard DN et al. Nature. 1993;362-3):160-164. 2. US CF Foundation, Johns Hopkins University, The Hospital for Sick Children. The Clinical and Functional TRanslation of CFTR (CFTR2). http://www. cftr2.org. Accessed November 12, 2015. 3. Cystic Fibrosis Foundation. Cystic Fibrosis Foundation Patient Registry 2013 Annual Data Report. Bethesda, MD. © 2014; Cystic Fibrosis Foundation. 4. Cystic Fibrosis Trust. UK Cystic Fibrosis Registry Annual Data Report 2014. © 2015; Cystic Fibrosis Trust; London, UK. 5. The Cystic Fibrosis Registry of Ireland. 2013 Annual Report. © CFRI, 2015; Dublin, Ireland. 6. French Cystic Fibrosis Registry. Annual Report 2013. © Vaincre la Mucoviscidose and Ined, 2015; Paris, France. 7. Belgisch Mucoviscidose Register – Registre Belge de la Mucoviscidose. The Belgian Cystic Fibrosis Registry. Summary Report 2011. © 2014; Institute of Public Health (WIV-ISP), Brussels, Belgium. 8. Nederlandse Cystic Fibrosis Stichting. Dutch Cystic Fibrosis Patient Registry. Report on the Year 2014. © 2015; NCFS: Baarn, Netherlands. 9. Mukoviszidose e.V. und Mukoviszidose Institut gemeinnützige Gesselschaft für Forschung und Therapienntwicklung mbH. Beriichtsband Qualitätssicherung Mukoviszidose 2012. © 2013, Bonn, Germany. 10. Cystic Fibrosis Australia. Australian Cystic Fibrosis Data Registry 2013–16th Annual Report. © 2015; Cystic Fibrosis Australia; Baulkham Hills NSW, Australia. 11. Cystic Fibrosis Association of New Zealand. PORT CFNZ National Data Registry, 2014 Registry Report. Christchurch, New Zealand. 12. Bobadilla JL et al. Hum Mutat. 2002;19(2):575-606. 13. World Health Organization. The molecular genetic epidemiology of cystic fibrosis: report of a joint meeting of WHO/ECFTN/ICF(M)A/ECFS; June 19, 2002; Genoa, Italy. © World Health Organization; 2004.
Aus10: 4%
US3: 3%
Prevalence of the R117H Mutation in Patients With Cystic Fibrosis (% of Patients With at Least 1 Allele)
3%
1%
0.7%
0.6%
0.5%
0.5%
Norway12
Greece12
Austria13
Canada13
Denmark13
Switzerland13
Country % of Alleles
Additional sources report frequency of the R117H mutation on CF alleles
R117H is the most common residual function CFTR mutation and the fifth most common CFTR mutation in the world1,2
Europe:UK4: 4% Ireland5: 4%France6: 2%Belgium7: 2%Netherlands8: 2%Germany9: 0.5%
New Zealand11: 2%
4

The R117H mutation results in reduced channel- opening and conductance of the CFTR protein1-4
References: 1. Welsh MJ, Smith AE. Cell. 1993;73(7):1251-1254. 2. Castellani C et al. J Cyst Fibros. 2008;7(3):179-196. 3. Zielenski J. Respiration. 2000;67(2):117-133. 4. Sheppard DN et al. Nature. 1993;362(3):160-164.
• R117H is a missense mutation. R117H-protein channels reach the apical cell surface, but their function is decreased1-4
– R117H produces a CFTR protein with reduced channel-open probability (or gating), characteristic of a Class III mutation
– R117H also results in decreased chloride conductance, typical of a Class IV mutation
CFTR Processing
CFTR Synthesis
CFTR Trafficking
DNA
mRNA
mRNA
Transcription
CFTR
Trafficking
Translation
Immature CFTR
Posttranslationalmodification
Illustrative Example of Class III Defect With Class IV Defect
CFTR Turnover
CFTR Function
5

CF disease in patients with the R117H mutation is influenced by the CFTR poly-T tract variant1-8
• R117H-5T: Causes the greatest reduction of functional CFTR at the apical cell surface.
Typically, 5T in cis with R117H (i.e., on the same allele) is associated with a CF phenotype2-5,9,10
• R117H-7T: Less likely than R117H-5T to result in CF, however, individuals can develop CF. Patients who have 7T in cis with R117H may still need to be monitored for the development of CF 5-10
• R117H-9T: Highly unlikely to result in CF4,5
References: 1. Castellani C et al. J Cyst Fibros. 2008;7(3):179-196. 2. Claustres M. Reprod Biomed Online. 2005; 10(1):14-41. 3. Chu C-S et al. Nat Genet. 1993;3:151-156. 4. Kiesewetter S et al. Nat Genet. 1993;5:274-278. 5. Massie RJ et al. Eur Respir J. 2001;17(6):1195-2000. 6. O’Sullivan BP et al. Pediatrics. 2006;118(3):1260-1265. 7. Lording A et al. J Cyst Fibros. 2006;5:101-104. 8. Peckham D et al. J Cyst Fibros. 2006;5:63-65. 9. Zielenski J. Respiration. 2000;67(2):117-133. 10. US CF Foundation, Johns Hopkins University, The Hospital for Sick Children. The Clinical and Functional TRanslation of CFTR (CFTR2). http://www.cftr2.org. Accessed November 12, 2015.
8Intron 7
Exon Exon Exon
CFTR gene
Full-length CFTR mRNA
Exons Exons
TGmTTTTTTTTTAAACAGTGmTTTTTTTAAACAGTGmTTTTTAAACAG
9T7T5T
Number of thymidineresidues
Normal CFTR protein
Longer poly-T lengthMore channelsMore chloride transport
Shorter poly-T lengthFewer channelsLess chloride transport
No CFTR protein
mRNA without exon 9
Intron 8 Intron 99 10
7 8 7 8 109 10
Adapted with permission from Claustres M. Reprod Biomed Online. 2005;10(1):14-41.
Intron 8 Poly-T Variant Length Affects Splice Efficiency During R117H-CFTR Protein Synthesis1-3
6
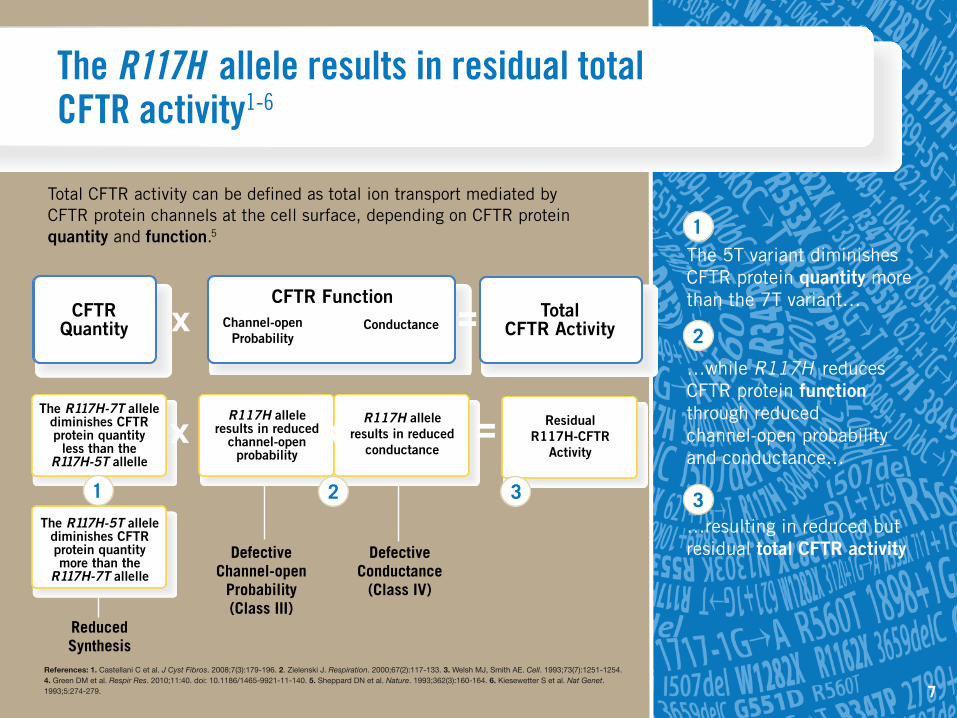
Defective Channel-open
Probability(Class III)
Reduced Synthesis
Defective Conductance
(Class IV)
The R117H allele results in residual total CFTR activity1-6
The R117H-7T allele diminishes CFTR protein quantity
less than the R117H-5T allelle
The R117H-5T allele diminishes CFTR protein quantity more than the
R117H-7T allelle
R117H allele results in reduced
channel-open probability
R117H allele results in reduced
conductance
ResidualR117H-CFTR
Activity
The 5T variant diminishes CFTR protein quantity more than the 7T variant…
…while R117H reduces CFTR protein function through reduced channel-open probability and conductance…
…resulting in reduced but residual total CFTR activity
References: 1. Castellani C et al. J Cyst Fibros. 2008;7(3):179-196. 2. Zielenski J. Respiration. 2000;67(2):117-133. 3. Welsh MJ, Smith AE. Cell. 1993;73(7):1251-1254. 4. Green DM et al. Respir Res. 2010;11:40. doi: 10.1186/1465-9921-11-140. 5. Sheppard DN et al. Nature. 1993;362(3):160-164. 6. Kiesewetter S et al. Nat Genet. 1993;5:274-279.
1
1
2
2
3 3
Total CFTR activity can be defined as total ion transport mediated by CFTR protein channels at the cell surface, depending on CFTR protein quantity and function.5
x x =
Channel-openProbability
Conductance
CFTR FunctionTotal
CFTR ActivityxCFTR Quantity x =
7

Both CFTR alleles play a role in determining phenotype or disease severity1-7
• An R117H allele results in residual CFTR activity. The phenotype of a particular patient is also influenced by the mutation on the other allele. The R117H allele results in variable phenotypes1-7
• R117H typically results in the indicated phenotypes
References: 1. US CF Foundation, Johns Hopkins University, The Hospital for Sick Children. The Clinical and Functional TRanslation of CFTR (CFTR2). http://www.cftr2.org. Accessed November 12, 2015. 2. deGracia J et al. Thorax. 2005;60(7):558-563. 3. Cystic Fibrosis Genotype-Phenotype Consortium. N Engl J Med. 1993;329(18):1308-1313. 4. Davis PB et al. Am J Respir Crit Care Med. 1996;154(5):1229-1256. 5. Castellani C et al. J Cyst Fibros. 2008;7(3):179-196. 6. Zielenski J. Respiration. 2000;67(2):117-133. 7. Massie RJH et al. Eur Respir J. 2001;17:1195-1200.
No CF DiseaseNormal individuals and CF carriers
Cystic Fibrosis
CFTR-related DisorderClinical entities associated with CFTR dysfunction that do not fulfill diagnostic criteria for CF
Normal Normal Normal
Normal Residual
Residual Residual
Residual
Littleto None
Littleto None
Littleto None
Littleto None
Allele 1Total CFTR Activity
Allele 2Total CFTR Activity
TotalCFTR
Activity
0%
100%
Adapted from Zielenski J. Respiration. 2000;67(2):117-133.
8

R117H in combination with another allele that produces little to no CFTR activity can result in CF symptoms that may emerge later in life1-6
References: 1. US CF Foundation, Johns Hopkins University, The Hospital for Sick Children. The Clinical and Functional TRanslation of CFTR (CFTR2). http://www.cftr2.org. Accessed November 12, 2015. 2. deGracia J et al. Thorax. 2005;60(7): 558-563. 3. Cystic Fibrosis Genotype-Phenotype Consortium. N Engl J Med. 1993;329(18):1308-1313. 4. Davis PB et al. Am J Respir Crit Care Med. 1996;154(5):1229-1256. 5. Castellani C et al. J Cyst Fibros. 2008;7(3):179-196. 6. Massie RJH et al. Eur Respir J. 2001;17:1195-2000.
CF Phenotype In patients registered in the CFTR2 database with an R117H mutation on 1 allele and a pancreatic insufficient mutation on the second allele1
• Sweat chloride (average): 60 mmol/L
• A range of pulmonary phenotypes, including classic CF, delayed onset of pulmonary symptoms, or no pulmonary symptoms6
• Pseudomonas colonization: 28% of patients
• Pancreatic insufficiency: 23% of patients
ResidualTotal
CFTR Activity
EnvironmentalFactors
Modifier Genes
Residual CFTR Protein Activity
Allele #1: R117H
Little to NoCFTR Protein
Activity
Allele #2
CFTR Genotype
9

Summary• Loss of CFTR activity is the underlying cause of CF
• Levels of CFTR activity affect survival in CF
• R117H is the most common residual function CFTR mutation and the fifth most common CFTR mutation in the world
• The R117H mutation results in reduced channel-opening and conductance of the CFTR protein
• CF disease in patients with the R117H mutation is influenced by the CFTR poly-T tract variant
• The R117H allele results in residual total CFTR activity
• Both CFTR alleles play a role in determining phenotype or disease severity
• R117H in combination with another allele that produces little to no CFTR activity can result in CF symptoms that may emerge later in life
10