mucinous cystadenoma arising 3 years after ovarian-sparing surgery for mature teratoma in a child
TRANSCRIPT
www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2010) 45, E9–E12
Mucinous cystadenoma arising 3 years after ovarian-sparingsurgery for mature teratoma in a child☆
Benoit Parmentier a, Emmanuelle Vaz b, Maud Chabaud-Williamson c, Sylvie Fasola d,Henri Kotobi a, Aurore Coulomb-L'herminé e,f, Frédéric Auber c,⁎
aService de Chirurgie Pédiatrique Viscérale et Urologique, Centre Hospitalier Général Robert Ballanger, 93602 Aulnay SousBois Cedex, FrancebService d'Anatomie et Cytologie Pathologiques, Centre Hospitalier Général Robert Ballanger, 93602 Aulnay Sous BoisCedex, FrancecService de Chirurgie Pédiatrique Viscérale et Néonatale, AP-HP–Groupe Hospitalier Armand Trousseau–La Roche-Guyon,75571 Cedex 12, Paris, FrancedService d'Oncologie Pédiatrique, AP-HP–Groupe Hospitalier Armand Trousseau–La Roche-Guyon, 75571 Cedex 12, Paris,FranceeService d'Anatomie et Cytologie Pathologiques, AP-HP–Groupe Hospitalier Armand Trousseau–La Roche-Guyon, 26 Avenuedu Dr Arnold Netter, 75571 Cedex 12, ParisfUniversité Pierre et Marie Curie, Paris, France
Received 26 February 2010; revised 8 May 2010; accepted 10 May 2010
0d
Key words:Mucinous cystadenoma;Ovarian-sparing surgery;Mature teratoma;Adolescent
AbstractWe report the case of a 15-year-old girl diagnosed with mucinous cystadenoma 3 years afterovarian-sparing surgery for a mature teratoma located in the same ovary. Ovarian teratoma is themost common ovarian neoplasm in children, whereas mucinous cystadenoma is extremely rareduring childhood.© 2010 Elsevier Inc. All rights reserved.
Ovarian teratoma is the most common ovarian neoplasm an adolescent. The patient and both parents consented to the
in children and is usually mature [1,2]. Surgical excision isthe standard treatment [3]. Mature or immature recurrencemay occur during follow-up [1-3]. Synchronous ovarianteratoma with mucinous cystadenoma has been reported in afew patients [4-9]. Mucinous cystadenoma is extremely rareduring childhood [10]. Here, we report a case of metachro-nous mature ovarian teratoma and mucinous cystadenoma in☆ Conflict of interest statement: none.⁎ Corresponding author. Tel.: +33 1 44 73 65 90; fax: +33 1 44 73 69 79.E-mail address: [email protected] (F. Auber).
022-3468/$ – see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2010.05.024
publication of this report.
1. Case report
A 12-year-old premenarchal girl with an unremarkablemedical history came to the emergency department for acutesevere abdominal pain without fever or vomiting. Ultraso-nography of the abdomen and pelvis at admission visualizeda left ovarian cyst measuring 65 × 50 × 45 mm with thinwalls, several septa, and a few vegetations. The plainabdominal radiograph revealed a pelvic calcification.
E10 B. Parmentier et al.
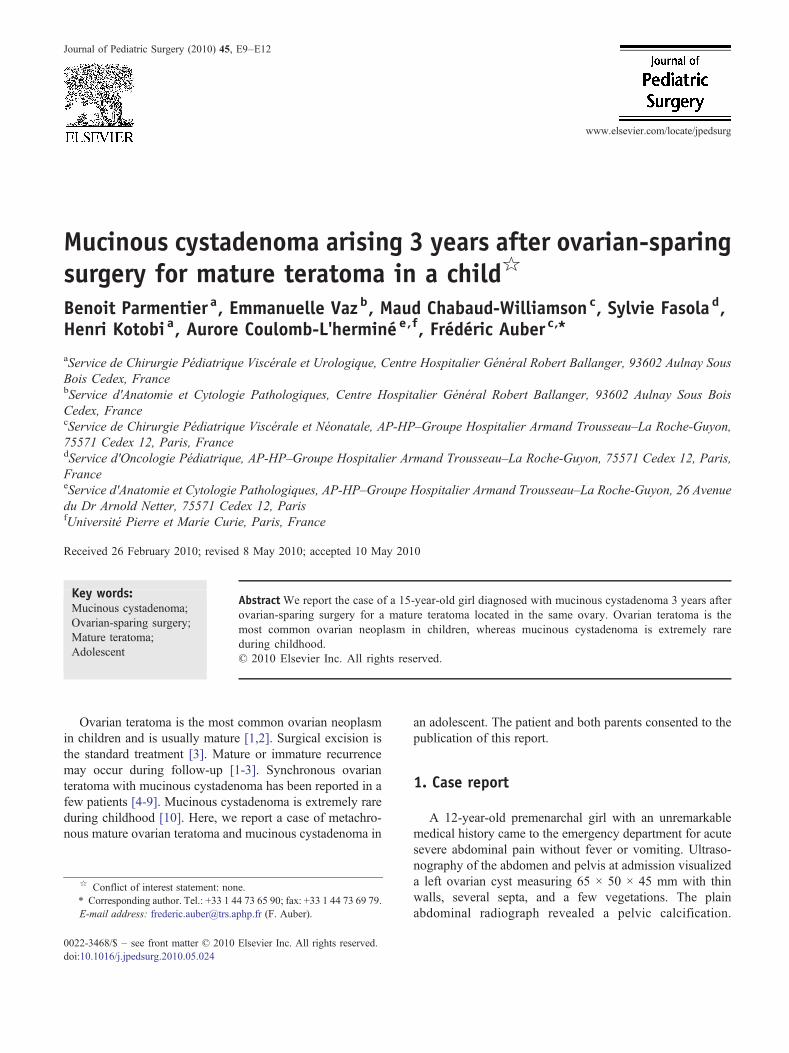
Findings were normal from laboratory tests including tumormarker assays (α-fetoprotein and human chorionic gonado-tropin). Computed tomography showed a left ovarian tumorwith features suggesting localized teratoma. Surgery wasthrough a transverse suprapubic incision. The left ovariancyst had the typical appearance for mature teratoma, withhair within the cyst. The right ovary was normal. Partial leftoophorectomy preserving a strip of ovarian tissue wasperformed. Histologic examination of the operative speci-men showed a mature cystic teratoma and tumor-freemargins (Fig. 1). The postoperative course was uneventful.Follow-up consisted of a physical examination and ultraso-nography of the abdomen and pelvis every 6 months. Normalmenstrual cycles began 11 months after surgery.
Three years after surgery, routine follow-up ultrasonog-raphy showed a multilocular image in the left ovarymeasuring 57 × 28 × 42 mm. The right ovary was normal,with follicles. The patient was symptom free and reported aregular menstrual cycle. The suggested diagnosis wasfunctional cyst or teratoma recurrence. Computed tomogra-phy visualized a persistent bilocular cyst measuring 70 ×50 mm in the left ovary with no tumoral componentor calcification. The right ovary was normal. Findingswere normal from serum assays of the tumor markers α-fetoprotein, carcinoembryonic antigen, human chorionicgonadotropin, and CA-125.
Combined oral contraception was started.Ultrasonography 2 months later showed a persistent
fluid-filled cyst measuring 72 × 67 mm with a thintransversal septum and no tissue component or calcification.Conservative cyst removal was performed via the transverse
Fig. 1 Ovarian teratoma composed of mature tissues including epidermmature glial tissue (dotted arrow in A), and mature glial tissue with cere
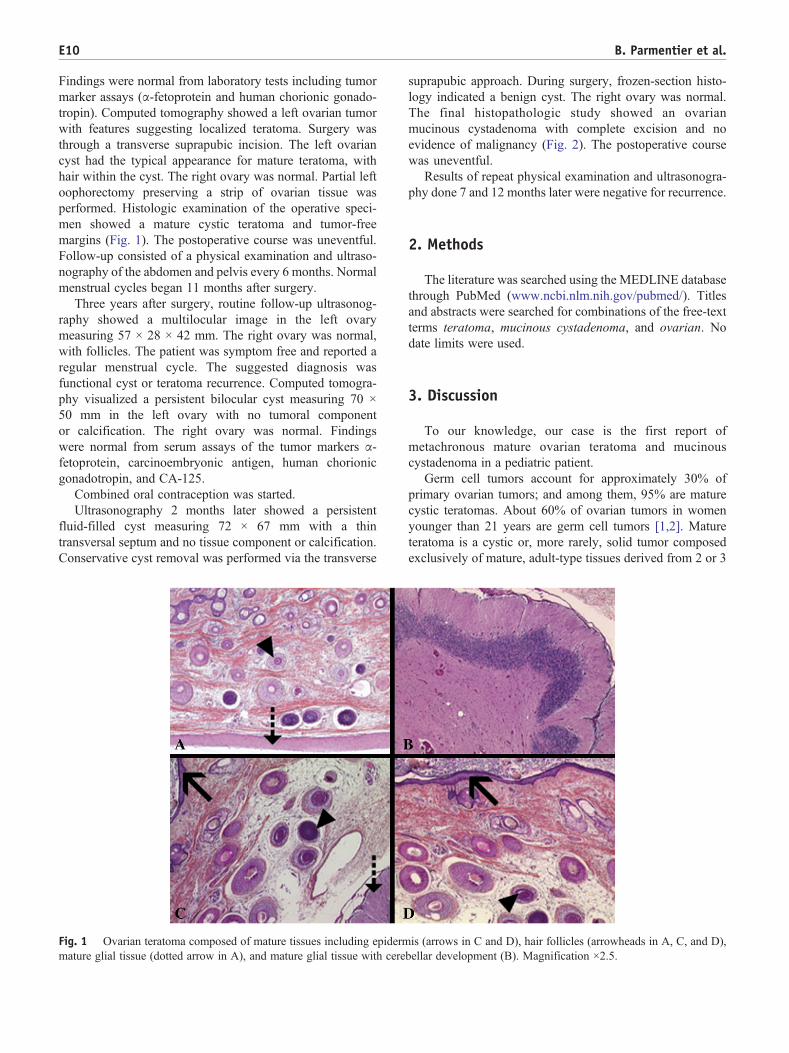
suprapubic approach. During surgery, frozen-section histo-logy indicated a benign cyst. The right ovary was normal.The final histopathologic study showed an ovarianmucinous cystadenoma with complete excision and noevidence of malignancy (Fig. 2). The postoperative coursewas uneventful.
Results of repeat physical examination and ultrasonogra-phy done 7 and 12 months later were negative for recurrence.
2. Methods
The literature was searched using the MEDLINE databasethrough PubMed (www.ncbi.nlm.nih.gov/pubmed/). Titlesand abstracts were searched for combinations of the free-textterms teratoma, mucinous cystadenoma, and ovarian. Nodate limits were used.
3. Discussion
To our knowledge, our case is the first report ofmetachronous mature ovarian teratoma and mucinouscystadenoma in a pediatric patient.
Germ cell tumors account for approximately 30% ofprimary ovarian tumors; and among them, 95% are maturecystic teratomas. About 60% of ovarian tumors in womenyounger than 21 years are germ cell tumors [1,2]. Matureteratoma is a cystic or, more rarely, solid tumor composedexclusively of mature, adult-type tissues derived from 2 or 3
is (arrows in C and D), hair follicles (arrowheads in A, C, and D),bellar development (B). Magnification ×2.5.
Fig. 2 Ovarian mucinous cystadenoma with regular mucinousendocervical-type cells lining the cyst (arrow). Magnification ×20(A) and ×2.5 (B).
E11Metachronous mucinous cystadenoma and ovarian teratoma
embryonic layers (ectodermal, mesodermal, and endodermallayers) [1,2,11]. The diagnosis is usually established duringthe reproductive years, mainly during the first 2 decades oflife, although cases have been reported in premenarchal girls[2]. A dermoid cyst is a mature teratoma composedpredominantly of a cyst that is completely or partially linedby an epithelium resembling the epidermis with itsappendages. Mesodermal, endodermal, and other ectodermalderivatives are also present in most cases [1]. Matureteratoma may manifest as an abdominal mass, pelvic pain, oracute complications such as torsion, rupture, or infection. Inmost cases, the diagnosis is readily confirmed based on thetypical gross appearance and presence of calcifications [12].Oophorectomy is the standard treatment [3]. However,ovarian-sparing surgery has been advocated recently [5].Although our patient has been operated on through atransverse suprapubic incision, a laparoscopic approach tothe management of benign ovarian tumors has become anaccepted option [5,13]. Expertise in laparoscopic surgery iscrucial to minimize the risk of tumor spillage. Recurrence ofeither a mature or an immature teratoma is possible, makinglong-term follow-up mandatory [1,2].
Benign mucinous cystadenoma is an epithelial ovariantumor whose incidence peaks between 30 and 50 years ofage. Pediatric cases are extremely uncommon. A retrospec-tive study of 240 ovarian masses showed that epithelial-derived tumors contributed 16.6% of cases and that, amongthem, 47% were serous cystadenomas and 16% weremucinous cystadenomas (3/240, 1%) [14]. A literaturereview conducted by Sri Paran et al [10] in 2006 foundonly 13 cases of mucinous cystadenoma in perimenarchalgirls, to which the authors added 6 cases. Thus, the casereported here is highly unusual. Furthermore, we are notaware of previous pediatric reports of metachronous maturecystic teratoma and mucinous cystadenoma.
Mucinous cystadenomas are often large and usuallycystic, with 76% being multilocular and 24% unilocular[1,2,6]. They are composed of multiple smooth-walled cystsof various sizes filled with mucus-rich fluid produced bygastrointestinal- or endocervical-type cells [6]. They arebilateral in 5% to 10% of cases [15,16]. Mucinouscystadenomas are divided into benign, borderline, andmalignant types; and they can progress to cystadenocarci-noma [15]. However, 77% to 87% of all mucinous ovarianneoplasms are benign. The manifestations are typicallynonspecific symptoms, such as increasing abdominal girth,abdominal or pelvic pain, emesis, asthenia, constipation, orurinary symptoms. The treatment consists of completesurgical excision, which should be conservative whentechnically possible [15,17]. Careful follow-up is importantbecause some tumors recur, especially if not completelyremoved by surgery [16,17].
Our literature search retrieved several reports of mucinouscystadenoma occurring synchronously with other ovariantumors such as endometrial cyst and dermoid cyst [4],anaplastic carcinoma [18], clear-cell carcinoma [19], cho-riocarcinoma [20], granulosa cell tumor, and matureteratoma [21]. Morris et al [22] suggested that somemucinous tumors may derive from germ cells, for instance,in mature teratoma; and our report supports this hypothesis.
The proportion of mucinous tumors among malignantepithelial neoplasms is higher in childhood than in adulthood(39% vs 12%) [23]. Childhood and adulthood ovariancarcinomas differ substantially, and at least some mucinousneoplasms seem to represent a type of monophyleticteratoma. A case of ovarian tumor combining a mucinouscystadenoma, a granulosa cell tumor, and a mature cysticteratoma has been reported [21]. The authors suggested thatthe totipotency of the tissues within teratomas may give riseto a combination of different tumors [21]. Hart [6] pointedout that 3% to 5% of mucinous tumors were associated withdermoid cysts, suggesting that some pure mucinous tumorsmay be in fact monodermal teratomas. The synchronousoccurrence of a mucinous tumor and dermoid cyst has beeninvestigated in 3 studies performed in the general population.A 1960 retrospective review of 1019 benign ovarianneoplasms identified 9 (5%) dermoid cysts among 171mucinous cystadenomas [7]. In 1953, a retrospective study

E12 B. Parmentier et al.
of 355 patients with ovarian mucinous cystadenoma andmucinous cystadenocarcinoma found a coexisting teratomain 4.5% of cases [8]. Finally, a 1979 study of 293 benignmucinous cystadenomas of the ovary showed a synchronousdermoid cyst in 11 (4%) cases (10 ipsilateral and 1contralateral) [9]. In these studies, the association wasalways synchronous. No cases of metachronous associationhave been reported previously.
We suggest 3 hypotheses to explain the unusualassociation in our patient. The occurrence of the 2 tumorsmay be ascribable to chance alone. However, this possibilityis unlikely given the low incidence of both tumors inpediatric patients. Two unrelated tumors may have devel-oped metachronously in a tumor-prone ovary. Indeed,several cancer predisposition syndromes with gonadaltumor development have been described [24]. However,the ovarian parenchyma adjacent to the tumor was normal inour patient, who had no clinical evidence of cancerpredisposition syndrome or familial history of cancer. Thethird hypothesis is recurrence of the mature cystic teratomaas a mucinous cystadenoma. This possibility is consistentwith previous reports of synchronous dermoid cyst andmucinous cystadenoma. Pathologists and clinicians shouldbe aware of this possibility when they identify an ovariantumor recurrence after complete surgical excision of a matureteratoma in a child. Long-term regular clinical andultrasonographic monitoring is essential in children treatedfor either tumor type.
Acknowledgment
We thank Antoinette Wolfe for her assistance forpreparation of the manuscript.
References
[1] Scully RE, Young RH, Clement PB. Tumors of the ovary,maldeveloped gonads, fallopian tube, and broad ligament. In: RosaiJ, editor. Atlas of tumor pathology. Third series, fascicle 23.Washington DC: Armed Forces Institute of Pathology; 1998.
[2] Tavassoli FA, Devilee P, editors. World Health Organizationclassification of tumours pathology and genetics of tumour of thebreast and female genital organs. Lyon: IARC Press; 2003. p. 163-71.
[3] Cass DL, Hawkins E, Brandt ML, et al. Surgery for ovarian masses ininfants, children, and adolescents: 102 consecutive patients treated in a15-year period. J Pediatr Surg 2001;36:693-9.
[4] Hata K, Hata T, Kitao M, et al. Endometrial cyst, dermoid cyst andmucinous cystadenoma sonographically evidenced in the same ovary.Gynecol Obstet Invest 1989;27:160-3.
[5] Templeman CL, Hertweck SP, Scheetz JP, et al. The management ofmature cystic teratomas in children and adolescents: a retrospectiveanalysis. Hum Reprod 2000;15:2669-72.
[6] Hart WR. Mucinous tumors of the ovary: a review. Int J GynecolPathol 2005;24:4-25.
[7] Beck RP, Latour JP. Review of 1019 benign ovarian neoplasms.Obstet Gynecol 1960;16:479-82.
[8] Cariker M, Dockerty M. Mucinous cystadenomas and mucinouscystadenocarcinomas of the ovary; a clinical and pathological study of355 cases. Cancer 1954;7:302-10.
[9] Russell P. The pathological assessment of ovarian neoplasms. I:introduction to the common ‘epithelial’ tumours and analysis of benign‘epithelial’ tumours. Pathology 1979;11:5-26.
[10] Sri Paran T, Mortell A, Devaney D, et al. Mucinous cystadenoma ofthe ovary in perimenarchal girls. Pediatr Surg Int 2006;22:224-7.
[11] Hong SR, Chun YK, Kim YJ, et al. Ovarian mucinous cystadenomawith mural node of anaplastic carcinoma. J Korean Med Sci 1998;13:680-4.
[12] Vacher-Lavenu MC. Histology of benign borderline ovarian cysts andsubperitoneal dystrophic cysts. J Gynecol Obstet Biol Reprod (Paris)2001;30:S12-S19.
[13] Savasi I, Lacy JA, Gerstle JT, et al. Management of ovarian dermoidcysts in the pediatric and adolescent population. J Pediatr AdolescGynecol 2009;22:360-4.
[14] Morowitz M, Huff D, Von Allmen D. Epithelial ovarian tumors inchildren: a retrospective analysis. J Pediatr Surg 2003;38:331-5discussion 331-5.
[15] Mittal S, Gupta N, Sharma AK, Dadhwal V. Laparoscopicmanagement of a large recurrent benign mucinous cystadenoma ofthe ovary. Arch Gynecol Obstet 2008;277:379-80.
[16] Vizza E, Galati GM, Corrado G, et al. Voluminous mucinouscystadenoma of the ovary in a 13-year-old girl. J Pediatr AdolescGynecol 2005;18:419-22.
[17] Baksu B, Akyol A, Davas I, et al. Recurrent mucinous cystadenoma ina 20-year-old woman: was hysterectomy inevitable? J Obstet GynaecolRes 2006;32:615-8.
[18] Hong SR, Chun YK, Kim YJ, et al. Ovarian mucinous cystadenomawith mural node of anaplastic carcinoma. J Korean Med Sci 1998;13:680-4 (9).
[19] Dutt N, Berney DM. Clear cell carcinoma of the ovary arising in amucinous cystadenoma. J Clin Pathol 2000;53:938-9.
[20] Ozaki Y, Shindoh N, Sumi Y, et al. Choriocarcinoma of the ovaryassociated with mucinous cystadenoma. Radiat Med 2001;19:55-9.
[21] Farah Y, Moid FY, Jones RV. Granulosa cell tumor and mucinouscystadenoma arising in a mature cystic teratoma of the ovary: a uniquecase report and review of literature. Ann Diagn Pathol 2004;8:96-101.
[22] Morris HB, La Vecchia C, Draper GJ. Malignant epithelial tumors ofthe ovary in childhood: a clinicopathological study of 13 cases in GreatBritain 1962-1978. Gynecol Oncol 1984;19:290-7.
[23] Deprest J, Moerman P, Corneillie P, Ide P. Ovarian borderlinemucinous tumor in a premenarchal girl: review on ovarian epithelialcancer in young girls. Gynecol Oncol 1992;45:219-24.
[24] Lee PA, Houk CP, Ahmed SF, et al. Consensus statement onmanagement of intersex disorders. Pediatrics 2006;118:488-500.