mp state plan report feb 11, 2012 - vision2020 india gajiwala, medical director, divya jyoti trust,...
TRANSCRIPT

1
COMPREHENSIVE EYE CARE STRATEGIC PLAN
MADHYA PRADESH
Organised by Directorate of Health Services, Bhopal, MP
February 8th-9th, 2012
Technical Support
Dr. Rajendra Prasad Centre for Ophthalmic Sciences, AIIMS, New Delhi
Facilitated by
VISION 2020:The Right to Sight-India

2
ORGANISERS Directorate General of Health Services, Madhya Pradesh 1. Dilip Kumar Samantaray Principal Secretary, Health & Family Welfare, Madhya Pradesh 2. Dr. AN. Mittal Director, Directorate of Health Services, Madhya Pradesh 3. Dr. V.A. Joshi Joint Director& State Programme Officer (NPCB) Directorate of Health Services, Madhya Pradesh 4. Dr. Dhanila Narayan Deputy Director (NPCB), Directorate of Health Services, Madhya Pradesh
TECHNICAL SUPPORT Dr. R. P. Centre for Ophthalmic Sciences, AIIMS, New Delhi 1. Dr. Praveen Vashist
Additional Professor and Head, Deptt of Community Ophthalmology 2. Dr. Noopur Gupta
Scientist grade III (Ophthalmologist), Deptt of Community Ophthalmology
FACILITATORS VISION 2020:The Right to Sight - India 1. Col.( Retd.) M. Deshpande, President, VISION 2020:The Right to Sight -India 2. Dr. G. V. Rao, Chief Executive Officer, VISION 2020:The Right to Sight -India
REPORT WRITING 1. Dr. Praveen Vashist
Additional Professor and Head, Deptt of Community Ophthalmology 2. Dr. Noopur Gupta
Scientist grade III (Ophthalmologist), Deptt of Community Ophthalmology 3. Dr. G. V. Rao, Chief Executive Officer, VISION 2020: The Right to Sight - India OTHER RESOURCE PERSONS AND PARTICIPANTS 1. Dr. Uday Gajiwala, Medical Director, Divya Jyoti Trust, Surat 2. Mr. Anand Sudan, SSSN, Chitrakoot, Satna 3. Representatives, Sight Savers International 4. Representatives, CBM 5. Representatives, RIO Bhopal and Medical College Indore 6. District Program Managers 7. Local NGOs

3
ACRONYM EXPANSION
AWW Anganwadi Worker
AIIMS All India Institute of Medical Sciences
ASHA Accredited Social Health Activist
ANM Auxiliary Nurse Midwife
CHC Community Health Centre
CSR Cataract Surgical Rate
DPM District Programme Manager
DBCS District Blindness Control Programme
GOI Government of India
GIA Government of India Aid
IEC Information Education Communication
INGO International Non Government Organization
IOL Intra Ocular Lens
ISO International Organization for Standardization
HR Human Resource
HOD Head of Department
HIMS Healthcare Information & Management System
LV Low Vision
MIS Management Information System
MP Madhya Pradesh
MSW Medical social Worker
NABH National Accreditation Board for hospitals
NRHM National Rural Health Mission
NPCB National Programme for Control of Blindness
NGO Non Government Organization
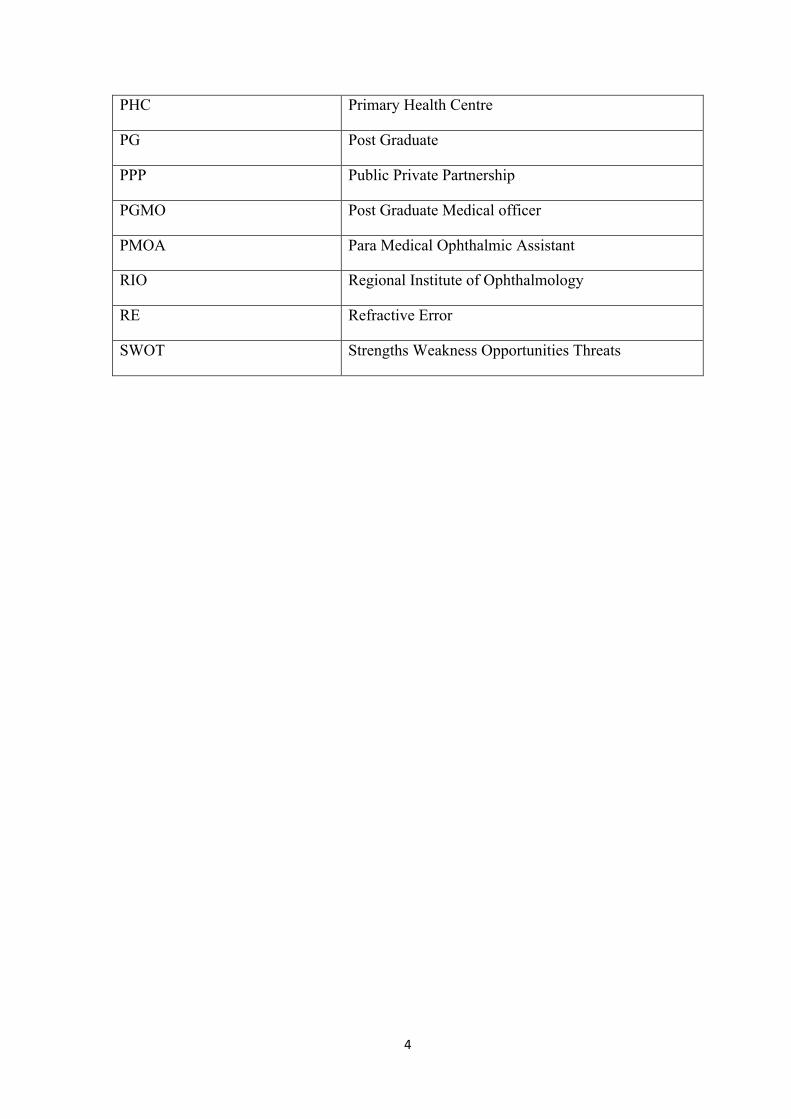
4
PHC Primary Health Centre
PG Post Graduate
PPP Public Private Partnership
PGMO Post Graduate Medical officer
PMOA Para Medical Ophthalmic Assistant
RIO Regional Institute of Ophthalmology
RE Refractive Error
SWOT Strengths Weakness Opportunities Threats

5
Table of Contents
S No Content Page Number
1 Executive Summary, Objectives, Key Strategies & Recommendations for the State Plan
6
2 Profile of Madhya Pradesh 11
3 National Programme for Control of Blindness, Madhya Pradesh: Current Status
13
4 Need Assessment: Eye Care Services 17
5 Group Work 21
5.1 Group Work 1: SWOT analysis 21
5.2 Group Work 2: Division wise discussion and suggestions by the groups
26
6 Recommendations by the groups 28
7 Annexures 31

6
1. Executive Summary, Objectives, Key Strategies and Recommendations
1.1 Executive Summary:
National Programme for Control of Blindness (NPCB) was launched in India in the year 1976 with the aim to reduce the prevalence of blindness from 1.4 percent to 0.3 percent by the year 2020. The strategies implemented by NPCB for this purpose are:
• Developing human resources and infrastructure, ensuring optimal utilization • Promoting outreach activities and public awareness • Improving Quality Eye Care services and visual outcome following medical and
surgical management.
For the past 4 years, the target set by the NPCB were 4,50,000 cataracts and almost 95% was achieved last year with IOL implementation was reported at 98%. The MP State thus, gained widespread acclaim for successfully attaining set targets by the NPCB over the past 4 years. Various eminent International and national Non-Governmental Organizations (INGOs) working in the State, contribute significantly in decreasing the blindness burden in the state.
The State of MP has been striving persistently for its growth in eye care service provision. In order to expand to reach to the unreached, improve the quality and specialties eye care services, it is time for having a strategic direction with 5 year plan. With this vision, Dr. R. P. Centre and VISION 2020: the Right to Sight- India partnered with State Blindness Control Society to provide technical assistance (by Dr. R. P. Centre) and facilitate in developing a State Plan for strengthening Comprehensive Eye Care Services and Resources.
With the active participation from the top and mid level management and clinical & non-clinical staff of District Hospitals, DPMs, RIO, Medical Colleges, Mobile Units, NGOs, the workshop facilitated the development process of a Five-year Eye Care State Plan (2012-2017) for MP. Prior to the workshop, a thorough study of the eye care capacity & services was studied by the team by obtaining necessary secondary data from the State. The team facilitated a workshop on 8th and 9th February 2012.
7
1.2. Objectives:
• To develop a State plan for affordable, accessible and effective quality eye care services in the state of Madhya Pradesh
1.3. Keys strategies:
• High volume cost effective Cataract, Refractive Errors and pediatric eye care services
• Strengthen Community Outreach and service marketing • Patient satisfaction and Quality enhancement of services. • Strengthen other specialty services like glaucoma, retina etc.
With efficient processes & systems put in place and improved human resource management the State Blindness Control Society can reach to a level of high performance state for comprehensive eye care services. It is projected that if strategies are implemented, the State can perform nearly 24,48,148 cataract surgeries from 2012- 2017 and will be able to generate sufficient resources from patient revenues for its management and future growth.
1.4. Recommendations 1.4.1. Programme management:
1. More emphasis is required for infrastructure development and human resource availability in the low performing districts, the districts in remote areas or difficult areas. The low performing districts Annupur, Sidhi, Sheopurkala, Harda, Dindori, Alirajpur. The INGOs, local NGOs should be promoted to strengthen the service delivery in these districts.
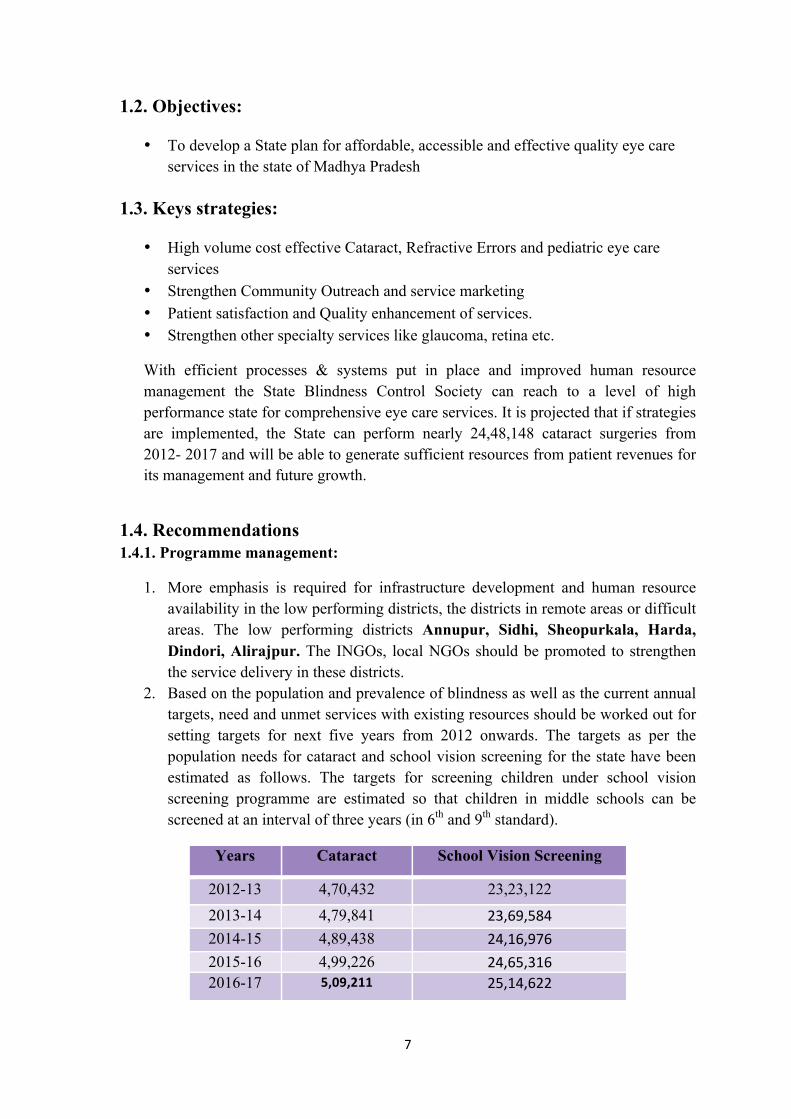
2. Based on the population and prevalence of blindness as well as the current annual targets, need and unmet services with existing resources should be worked out for setting targets for next five years from 2012 onwards. The targets as per the population needs for cataract and school vision screening for the state have been estimated as follows. The targets for screening children under school vision screening programme are estimated so that children in middle schools can be screened at an interval of three years (in 6th and 9th standard).
Years Cataract School Vision Screening
2012-13 4,70,432 23,23,122 2013-14 4,79,841 23,69,584 2014-15 4,89,438 24,16,976 2015-16 4,99,226 24,65,316 2016-17 5,09,211 25,14,622
8
3. Mapping of eye care services specifically the specialty services should be undertaken in the State. It is suggested that specialty services should be made available to all divisions.
4. It is suggested that appraisal should be conducted for ophthalmologists and optometrists with respect to their individual targets as well as the quality of services.
5. Currently, cataract surgical records are not maintained in most of the hospitals. HMIS needs to be implemented in all districts and data needs to be verified by the DPM for its accuracy and reliability. Short-term training of the district programme managers on MIS and record management is necessary. The record keeping should be shifted from manual to MIS.
6. In addition to NPCB funds, state government should earmark funds for training, IEC and assessment and monitoring of blindness control programme in the State.
1.4.2. Regional Institute of Ophthalmology, Bhopal and Medical Colleges:
Strengthening of Regional Institute of Ophthalmology, Bhopal and Medical colleges in MP to provide technical support of high efficiency in ophthalmic services:
1. They should be an integral part of the Blindness Control Programme: The Blindness Control Programme under the Director Health Services and Director Medical Education should work in coordination for blindness control activities in the State. The RIO, Bhopal should be an autonomous agency instead of part of a Medical College for better delivery of eye care services and capacity building.
2. There is a need to the assess the current capacity of RIO, Bhopal in order to further strengthen it as a Centre of Excellence for research, training and service delivery in eye care for this region. This may be taken with NPCB or Dr. R.P. Centre for necessary technical support.
3. All speciality eye care services like Paediatric Ophthalmology Unit, Vitreo-Retina clinic, Low Vision clinic, rehabilitation of the blind etc should be available in the RIO with high output and good quality services. The RIO should have trained ophthalmologists in all the subspecialties. It is essential that the specialty services should be expanded so that these services should be available in all the divisions.
4. RIO should provide facilities for the training and demonstrate the organisation and research in Eye Bank procedures including implantation and grafts.
5. The RIO and Medical colleges should be responsible for training of ophthalmologists and optometrists all over the State. Currently, most of the ophthalmologists have to go to other States for speciality training.

9
6. RIO and Medical colleges should be accountable for the referred cases from the district hospital. There should be some feedback information to the district hospital for referred cases.
7. RIO and Medical colleges should stimulate and provide facilities in research at a high level of competence. There is need for conducting surveys on blindness, Vitamin A deficiency, blind school survey etc.
8. The training in Phaco-surgery and availability of Phaco-machines may be considered in all Medical colleges and also at the district hospitals, as well.
1.4.3. District Hospitals and secondary level hospitals
Currently, around 350 ophthalmologists are available in Madhya Pradesh. This includes 227 in the government sector. One third of these posts are vacant and another 40% are non-surgical ophthalmologists. The vacant posts of ophthalmologists should be filled. There is a need to initiate motivation among non-surgical ophthalmologists for pursuing comprehensive medical ophthalmology that should include conducting screening camps, follow up services, Retina, Glaucoma and Low Vision Clinics.
1. The ophthalmologists are not showing interest in specialty training for skill transfer. It is suggested that short-term hospital based programme should be conducted with support of voluntary faculty/ faculty posted in RIO, Bhopal. Agencies like VISION 2020 – INDIA can be one of the resources for such programme.
2. As per NPCB guidelines, 1400 PMOA are required in the State. There is a need to develop training centres either through medical universities or other recognised centres to meet the future demand. All the vacant posts of the PMOA should be filled. Equitable distribution of PMOA, especially in underserved and difficult areas, should be ensured.
3. Team building workshops should be organised for motivation, commitment and improved performance among human resources at all levels of eye care service delivery. This may be done with the support of VISION 2020 - INDIA resources.
4. District mobile unit should be available in all the 50 districts. Currently they are available in 30 districts only.
5. It is recommended that the outreach surgical camps (make shift operation theatres) should be strictly prohibited in the entire State as per the guidelines of NPCB.
6. Regular maintenance of equipment should be undertaken. For this purpose, PMOA or NGO representative may be trained for 6 weeks in equipment maintenance from reputed institutes.

10
7. The information about cataract surgical outcomes is not available in most of the hospitals. It is suggested that records maintenance should be ensured at all level. Short-term training of the district programme managers on MIS and record management is necessary. The record keeping should be shifted from manual to MIS.
8. The follow up and monitoring of the operated cases should be ensured; NPCB recommend monitoring of at least 5% of the postoperative cases by DPM. It is not practiced in most of the districts.
1.4.4. Primary Level
1. All CHCs (catering to a population of 50,000 to 100,000 in Madhya Pradesh) should have well equipped Vision Centre with adequate space for refraction facility. A full time Para Medical Ophthalmic Assistant (PMOA) should be posted in each CHC accountable for the screening camps for cataract and school vision screening programme in the CHC.
2. Training of ASHA workers in primary eye care should be adopted at the Vision Centre level to improve awareness, identification and referral of blind patients and children with visual impairment. It is suggested that state government should earmark funds for training and output-based honorarium for these workers as done in other National Programmes. NGOs like Sightsavers may be utilised for effective implementation of this programme.

11
2. Profile of Madhya Pradesh Madhya Pradesh often called the Heart of India is a state in central India. Its capital is Bhopal and Indore is the largest city. Madhya Pradesh is the second largest state by area and with over 75 million inhabitants, the sixth largest state in India by population. It borders the states of Uttar Pradesh to the northeast, Chhattisgarh to the southeast, Maharashtra to the south, Gujarat to the west, and Rajasthan to the northwest.
2.1 Districts Madhya Pradesh state is made up of 50 districts, which are grouped into 10 divisions: -
Bhopal, Indore, Jabalpur, Gwalior, Ujjain, Rewa, Sagar, Chambal, Shahdol and Hoshangabad.

12
Districts:- Anuppur, Alirajpur, Ashoknagar, Balaghat, Barwani, Betul, Bhind, Bhopal, Burhanpur, Chhatarpur, Chhindwara, Damoh, Datia,Dewas, Dhar, Dindori, Guna, Gwalior, Harda, Hoshangabad, Indore, Jabalpur, Jhabua, Katni, Khandwa, Khargone, Mandla, Mandsaur,Morena, Narsinghpur, Neemuch, Panna, Raisen, Rajgarh, Ratlam, Rewa, Sagar, Satna, Sehore, Seoni, Shahdol, Shajapur, Sheopur,Shivpuri, Sidhi, Singrauli, Tikamgarh, Ujjain, Umaria, Vidisha.
2.2 Government and politics
Madhya Pradesh has a 230-seat state Legislative Assembly. The state also sends 40 members to the Parliament of India: 29 are elected to the Lok Sabha (Lower House) and 11 to the Rajya Sabha (Upper House).
The Madhya Pradesh's Legislative assembly

13
2.3 Demographics
Madhya Pradesh is a medley of ethnic groups and tribes, castes and communities. The population of Madhya Pradesh includes indigenous people and migrants from other states. According to census of 2000, 92% followed Hindu religion while others are Muslim(6%), Jain(0.9%), Christians(0.30%), Buddhists(0.30%), and Sikhs(0.20%).The scheduled castes and scheduled tribes constitute a significant portion of the population of the State. The scheduled castes are 13.14% while scheduled tribes were 20.63%.
No. of Districts – 50
No. of Sub Districts – 342
No. of Towns – 476
No. of Statutory Towns – 364
No. of Census Towns – 112
No. of Villages – 54903
Total Rural Urban
Population Persons 72,597,565 52,537,899 2,005,966
Male 37,612,920 27,142,409 10,470,511
Female 34,984,645 25,395,490 9,589,155
Population (0-6 yrs) Persons 10,548,295 (14.5%)
8,132,745
(15.5%)
2,415,550
(12.0%)
Male 5,516,957
(14.7%)
4,242,585
(15.6%)
1,274,372
(12.2%)
Female 5,031,338
(14.4%)
3,890,160
(15.3%)
1,141,178
(11.9%)
Literates Persons 43,827,193
(70.6%)
28,991,005
(65.3%)
14,836,188
(84.1%)
Male 25,848,137
(80.5%)
17,549,814
(76.6%)
8,298,323
(90.2%)
Female 17,979,056
(60.0%)
11,441,191
(53.2%)
6,537,865
(77.4%)
Sex Ratio 930 936 916
14
3. National Programme for Control of Blindness, Madhya Pradesh: Current Status
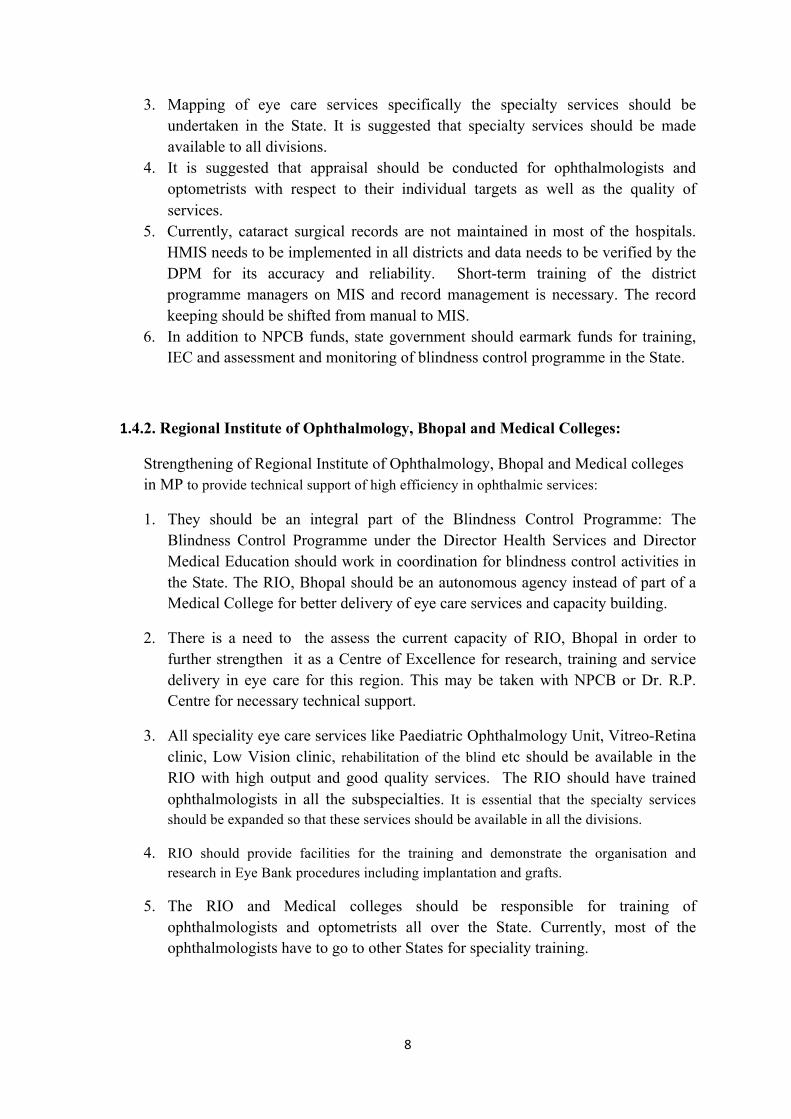
The National Programme for Control of Blindness was launched in the state of Madhya Pradesh in 1978 as a centrally sponsored programme. For the purpose of health, the State has been divided into seven divisions namely Bhopal, Indore, Jabalpur, Gwalior, Ujjain, Rewa and Sagar. Madhya Pradesh has 50 districts, 313 blocks and 52117 villages. Health care services are being provided in the State by 48 district hospitals, 56 civil hospitals, 333 community health centres, 1156 primary health centres and 8860 sub-centres.
3.1 Organizational Setup of Blindness Control Programme Madhya Pradesh
In the non-government set up, 150 NGOs, 56 private institutions and 91 private practitioners are functional to provide eye care services in the state.
3.2 Human Resource and Infrastructure for eye care
3.2.1 Human Resources in Blindness Control Programme in Madhya Pradesh
Working Vacant Total
Class I (Eye Surgeon) 44 56 100
Post Graduate Medical Officer in
Ophthalmology 113 14 127
Ophthalmic Assistant 434 163 598

15
3.2.2 Training of Human Resource in Madhya Pradesh
IOL Trained Phaco Trained
Class I Eye Surgeon 14 1
PGMO 67 18
Total 81 19
Ophthalmic Assistant Refresher Trained
85
3.2.3 Infrastructure & Equipments The current status of the equipments available in the government hospitals is shown in the table below:
Equipment name From GOI
From State
Total Working Not working
Functional equipments (%)
Operating Microscope
55 7 62 52 10 83.9
A scan Biometer 53 6 59 49 10 83.1 AV Unit 35 - 35 32 3 91.4 Indirect Ophthalmoscope
48 - 48 48 0 100.0
Cryo Unit 42 - 42 40 2 95.2 Fumigator 32 - 32 23 9 71.9 Auto clave 50 - 50 42 8 84.0 Keratometer 53 8 61 60 1 98.4 Slit lamp 54 6 60 58 2 96.7 Yag Laser 20 - 20 19 1 95.0 Streak Retinoscope
42 50 92 89 3 96.7
Tonometer 91 50 141 140 1 99.3 Direct Ophthalmoscope
67 50 117 113 4 96.6
3.3 Cataract Surgical Performance in Madhya Pradesh
In the year 2008-09, 376143 cataract surgeries were performed in the entire State (84% achievement according to target) and 429695 surgeries were conducted in 2010-11. The NGO sector contributes to nearly 47% cataract surgeries performed in the State while the private sector, district hospitals and medical colleges contribute to 37%, 12% and 4%

16
cataract surgeries respectively. 32 districts are performing very well while 8 districts show less than 50% performance.
3.4 School Vision Screening Programme
In the year 2010-11, 37791 schools were covered and 3490087 children were reported to be screened by school teachers. Out of these, a total of 72142 students were diagnosed with refractive error and 35990 were provided with free spectacles. Five districts did not provide any spectacles to children diagnosed with refractive error in 2010-11.
3.5 Districts having eye banks
There are around 25 eye banks in the State. In 2010-11, 906 eyes were collected and 454 keratoplasty were performed. The following districts reported having eye bank(s):
Government Sector NGO Sector
Gwalior Bhopal
Indore Sagar
Ratlam Chindwara
Indore
Neemuch
Satna
In the State, all the sub- specialties like Cataract (Phaco, SICS), Cornea, Glaucoma, Squint and Pediatric ophthalmology, Retina, Retinopathy of Prematurity (ROP), Orbit & Oculoplasty, Contact Lens & Low Vision Clinic and emergency services are available however limited to few centres only. There is a huge gap in these eye care specialties services in several parts of the state, and therefore, necessary training to HR, equipment would be required besides the focus on cataract program.

17
4. Need assessment for the eye care services
4.1 Magnitude and causes of Blindness in Madhya Pradesh
There is a huge estimated need for all kind of eye care services in the catchments area. For instance, the annual estimated need for eye care services of cataract and refractive errors itself is 3,13,621 blind people (48% of total blind population) and 2,28,682 persons (35% of total blindness burden) respectively. Considering the current capacity in terms of infrastructures, human resources, equipments and current estimated eye care needs in the catchment State of MP (and its respective 50 districts), the State Health Services and State Blindness Control Society has a great potential to tap into the wider market within its catchment areas and offer high volume, high quality and low cost eye care services to meet the need and demand of the area. In addition, State Blindness Control Society may continue its efforts to mobilize resources through grants and donations from NPCB, it may also make proposals for funding from State Government, INGOs where possible. While increasing the service capacity, the State of MP has to strengthen its Human Resource Management Capacity, Quality Improvement of its Services and Outcomes, Systems & Processes for efficient and effective service delivery, optimum utilization of existing NPCB’s Hospital Management Information System (HIMS) for data monitoring, increased community outreach and involvement of satisfied patients, improved IEC campaign using local media customized to the local culture.
4.2: Need for diseases control:
4.2.1 Gaps in Cataract Surgical Performance in Madhya Pradesh
In the year 2010-11, 429695 cataract surgeries were performed in the entire State with more than 80% of surgeries were conducted by NGOs and private sector. The performance from the ophthalmologists in district hospitals was around 12% with an average cataract surgery of less than 200 cataract surgeries per ophthalmologists per year.
Proportion of Blindness Numbers Total number of Blind people in Madhya Pradesh (0.9% of total population) 653378
Cataract 48% 313621 Refractive error 35% 228682 Glaucoma 5.1% 33322 Posterior segment including DR 3% 19601 Corneal Blindness including trachoma 1.1% 7187 Others 7.8% 50963

18
There is need to increase the cataract surgical outputs by around 10% to meet the population need for the cataract surgery for eliminating avoidable blindness in the State. There is need to give more emphasis on blind patients especially in the remote and underserved areas.
With the available strength of 300 ophthalmologists in the State, the targets can only be achieved if on an average more than 1500 surgeries are performed by each ophthalmologist in the State. Currently, the ophthalmologists in NGO sector are performing surgeries as per this target. There is need to improve the performance in the government sector.
4.2.1.1 Cataract Surgeries: Gaps & Targets as per the population need in MP
Total Population 7,25,97,565 Cataract surgeries 2010-11( against Targets of 450,000) 4,29,695 Cataract surgery required (as per population need) per year 4,70,432 Gap in annual surgeries 40,737 Cataract surgeries required per Million population per year 6,480
4.2.1.2 Cataract surgery targets as per Human Resource Capacity
No. of eye surgeons 300 No. of cataract surgeries per surgeon/week 35 No. of potential cataract surgeries per week 10500 No. of working weeks in a year 45 Human Resource Potential for no. of cataract surgeries per year 472500
4.2.2 Refractive Error Services and School Vision Screening programme
The 17.9% of the population in Madhya Pradesh is estimated of having any type of refractive error including presbyopia in 45 and above age group. The screening of school children is a priority under the National Programme. The programme recommends that the school teachers in the middle schools 3490087? should be trained to screen vision in children. The estimated children enrolled in middle school 6th to 10th standard are around 58 million. Out of these, more than 23 million children should be screened annually assuming that children are screened at the time of entry in 6th standard and then in 9th standard. As per the NPCB reports for the year 2010-11, near 35 million children were screened in Madhya Pradesh in one year. The number is very much higher than the estimated targets. This may be due to more frequent examinations or coverage of even primary classes in some districts.
4.2.2.1 Magnitude of Refractive errors in Madhya Pradesh

19
Population Proportion of Population (%)
Prevalence of Refractive error
0-4 years 12% 1% 5-9 years 11% 2% 10-14 years 10% 3% 15-44 years 47% 10% 45+ years 21% 25% 45+ (Presbyopia) 60%
4.2.2.2Refractive errors targets and gaps in Madhya Pradesh
Total Population 7,25,97,565 Estimated number of people with refractive error in all age group including presbyopia 1,30,24003
Estimated number of school children in school (6th-10th standard) 58,07,805
Estimated number of children to be screened by teachers annually
23,23,122
Estimated number of school children requiring spectacles annually
69, 694
4.2.3. Magnitude of Childhood Blindness in Madhya Pradesh
Total Population 7,25,97,565
Population under 15 years 32% 2,32,31,220
Prevalence of Childhood Blindness 0.8/1000 18585
4.2.4. Magnitude of Diabetic retinopathy (DR) cases in Madhya Pradesh
No. of Persons with Diabetes
14,51,951
DR amongst the diabetics 2,90,390
20
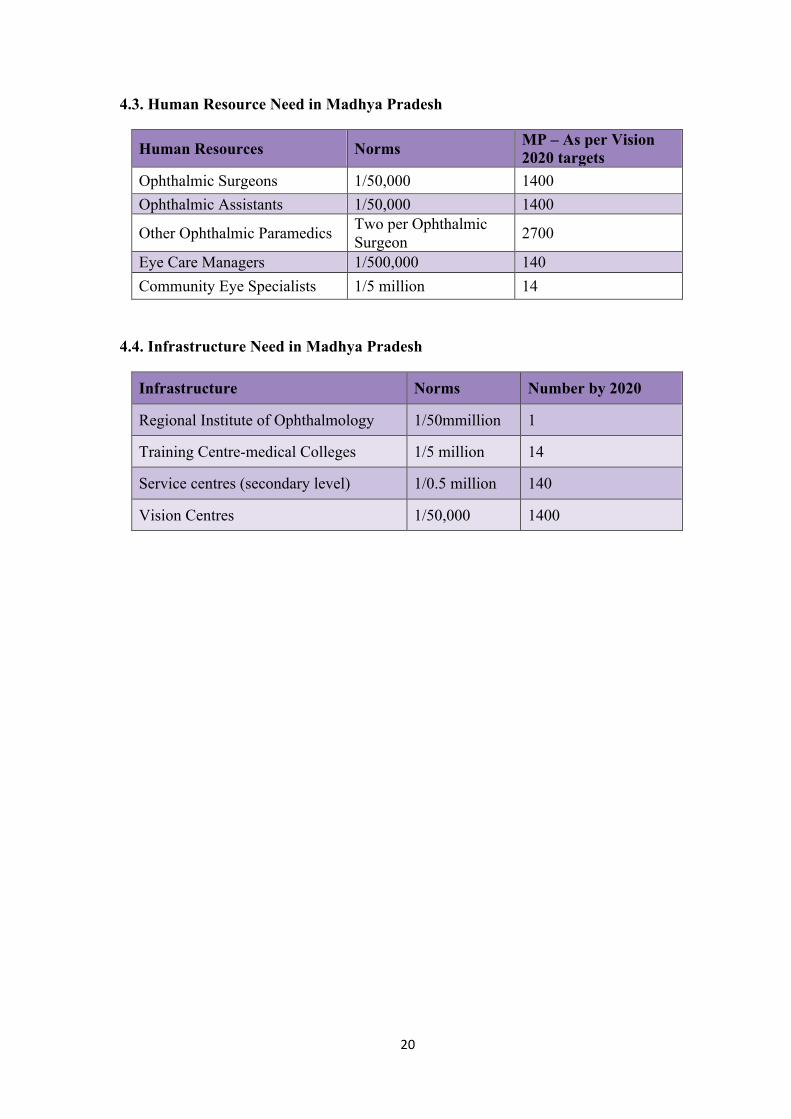
4.3. Human Resource Need in Madhya Pradesh
Human Resources Norms MP – As per Vision 2020 targets
Ophthalmic Surgeons 1/50,000 1400 Ophthalmic Assistants 1/50,000 1400
Other Ophthalmic Paramedics Two per Ophthalmic Surgeon 2700
Eye Care Managers 1/500,000 140 Community Eye Specialists 1/5 million 14
4.4. Infrastructure Need in Madhya Pradesh
Infrastructure Norms Number by 2020
Regional Institute of Ophthalmology 1/50mmillion 1
Training Centre-medical Colleges 1/5 million 14
Service centres (secondary level) 1/0.5 million 140
Vision Centres 1/50,000 1400

21
5. Group Work
5.1 Group Work 1: SWOT Analysis
During the 2nd day (9th February 2012) of the workshop, a SWOT (Strengths, Weakness, Opportunities and Threats) analysis was done for focusing on strengths and minimizing weaknesses. Key areas included in this group work were human resource optimization & management, infrastructure, service delivery and quality assurance including monitoring, finance, governance, MIS etc.
Strengths and weaknesses (internal environment)
n Strengths
• What are our existing strengths? • What do we do really well? • What makes us different from others?
n Weaknesses
• What areas of work we are not satisfied with? • What can be eliminated? • Complaints about our work?
Threats and opportunities (external environment)
n Threats
• Do we perceive any obstacles in our work from external sources?
• Apprehensions about Funding, Staffing, Technology?
• Political/social/economic opposition to our work?
n Opportunities
• What are the recent favourable trends in our environment?
• Government regulations, Social Patterns, Lifestyle Changes, New Technology
• Are we making use of our expertise and capacity to our best advantage?

22
5.1.1. SWOT Analysis by Government Sector (District Hospitals & Medical Colleges)
Strengths Weaknesses General General
Readymade platform for patients to walk in Policy and programmes in place Budgetary provision Free of cost services to needy segment
Lack of motivation & commitment Attitude towards NGOs Bureaucratic procedures Lack of proper accountability Lack of awareness about policies and guidelines at primary levels
Human Resource Human Resource Graded system of having specialist Government Policy on training employees
Disproportionate and inadequate staff Burden of non-ophthalmic work Non-optimal utilization of staff Poor team work & in-coordination amongst staff & other departments Posts vacant Lack of continuous trainings Job Turnover (Attrition) Misuse of manpower Performance review systems Promotion system based on seniority rather than performance No dedicated managerial staff
Infrastructure Infrastructure Buildings - well known and accessible Vehicle pool available
Space for dark rooms, DBCS office Building maintenance OT complex-quality and standardization norms only on paper facility for proper sterilization
Quality Quality ISO certified Population survey
Equipment supply Improper record keeping and analysis of data Waiting time for patients more
Management Management Hierarchical structure Planned programmes MIS Funding Various meeting (Purchase committee, HOD, Quarterly) Lateral linkages with other Government department Utilization of resources
Administrative powers with managers Sanctioning system Funds utilization
Marketing & Outreach Marketing & Outreach Funds available for IEC No well defined system

23
Field units of health and other departments Service Delivery Service Delivery Government schemes Scope of PPP Sub-specialty department & Eye bank/collection centre Government provides funds for expensive treatment Mobile Van Supporting Satellite vision centre Services Quality affordable & food
Personal rapport with patients Improper Counseling Communication with Pts of Doctor/MSW’s Overcrowding Fire fighting approach
Opportunities Threats Collaboration with NGOs , PPP Human Resource Training – MTs through Medical colleges, Through MTS to District persons ASHA , ANM, AWW & teachers training Recruitment Promotions Job responsibilities and allocation
Political and media interference Human Resource Lack of Trained staff – All types Lack of working hands at all levels Misuse of trained staff
Infrastructure Infrastructure AMC-Repair and maintains policy needs to strengthen
Out dated and out of order equipment
Quality Quality Protocols restricted to Cataract & RE Introduction to Legal protection/ Doctor Indemnity will help Quality measurement tools- NABH, ISO
Quality considerations vs targets vs guidelines Protocols not available for other diseases DR, Glaucoma etc. Medico legal proceedings Research (drug trials)
Management Management Dedicated Clinical Managers In-service Management training
To hire the professionals
Marketing & Outreach Marketing & Outreach Grievance redress committees Tie-up with private Practitioners and organization, specialty camps, marketing, corporate approach
Media
Service Delivery Service Delivery Changes in Govt. Policies Overcrowding

24
5.1.2. SWOT Analysis by Non-Government Sector (INGO & Local NGO of MP)
Strengths and Weaknesses
STRENGTHHRAvailability of skilled manpower
Retaining skilled manpower in rural areas
Spirit of volunteerismInfrastructureState of art infrastructure/Good
Equipments
QualityAvailability of good MIS
WEAKNESSHRNon-‐availability of trained
ophthalmic nurse Lack of second-‐line leadership Using Ayurvedic doctorsLack of HR
policies/implementationInfrastructureOne OT one Microscope QualityImproper documentationImproper follow-‐up
Strengths and Weaknesses
STRENGTHManagementPreparation of operational planMarketing & OutreachEmpanelment corporate Service DeliveryCommunity supportTiered pricing systemCapability to deliver
comprehensive eye care services
High volume extensive outreach program
WEAKNESSManagementImplementation of planMarketing & OutreachImpression as free service
provider
Service DeliveryLess walk-‐in patientsGIA for cataract lessLow priority for eye donation

25
Opportunities and Threats
OPPORTUNITIESHROpportunity for collaboration with in
NGOsCollaboration with GovernmentInfrastructureBurden of problem and expansion
opportunities
QualityGood clinical and surgical approachQuality measurement tools-‐
NABH/AIOSResearch
THREATS HRFew training institute Retention of ophthalmologists Not cooperating with leadership in
quality and system issuesInfrastructureAvailability of regular electricity Lack of fund for building and
equipment maintenanceQualityPerforming surgeries in make-‐shift
OTs Medico legal proceedings
Opportunities and Threats
OPPORTUNITIESManagementDevelop second-‐line leadershipTo develop HR policy having
specialized person for specialist job.
Gen. Insurance schemesMarketing & OutreachCollaboration with corporateRegular publicity from
government Competition
THREATS ManagementChange in leadershipAcceptance to change is very
low Marketing & OutreachBranding as charity hospitalMisuse of name of the
institute

26
Opportunities and Threats
OPPORTUNITIESService DeliveryGovernment aid to support
specialist services Strengthen referral system To open eye donation centers
in rural areas and in medical colleges/district hospitals
Collaboration for transporting corneas with railways/pvtairlines.
THREATS Service DeliveryDelayed GIA reimbursement Dependent of external fundingLack of system for financial
sustainability
5.2 Group Work 2: Division wise discussion and suggestions of the groups
5.2.1 Human Resources 1. Lack of trained staff-training and refresher trainings to PMOAs 2. Optimise resources-disease load of administrative works : exempt from other
duties from the months of October to March 3. Number of ophthalmologists are less in number and doing other non-ophthalmic
jobs 4. Non-operating surgeons, identify non-operating ophthalmologists and allocate
work accordingly 5. Training in all eye care disease priorities such as DR, Pediatric, Glaucoma,
Retina, Cornea, LV 6. Motivation, commitment and reluctance in human resources-performance based
appraisal and team work may be a solution 7. PMOAs should be under the supervision of ophthalmologists 8. PMOA should be at the level of vision centres 9. Awareness about proper record keeping, quality of services, answerability 10. Training of ASHA workers 11. increase PMOA-vacant posts to be filled 12. Inequitable distribution of PMOA

27
5.2.2. Infrastructure and Equipment 13. Vision Centres should be developed in PHCs, however adequate space needs to be
provided. 14. Operating microscopes and Phaco machines may be considered after doctors have
undergone Phaco training 15. Regular maintenance of equipment should be undertaken. For this purpose,
maintenance of equipments-PMOA or NGO representative may be trained for 6 weeks in equipment maintenance
16. Lack of office space, administrative powers and managerial staff for DPM. 17. Easy procurement of equipments without delay.
5.2.3. Disease Control 18. Based on the population and prevalence of blindness as well as the current annual
targets, need and unmet services with existing resources should be worked out for setting targets for each district for 2012 onwards
19. Mapping of eye care services in the State including NGOs/private organizations should be done on a priority for better monitoring and referral network
20. Specialty eye care services to be made available to all divisions. 21. Mapping of specialty eye care services in Madhya Pradesh as information is
available to all DPMs
5.2.4. Quality Monitoring 1. No CSR records are maintained and hence a suggestion that such data should be
kept 2. Ensure follow up ; 5% post operative cases to be monitored by DPM 3. HMIS, developed by NPCB, need to be implemented by all DPMs and data need
to be verified by the DPM for its accuracy and reliability. 4. Problems in opening the HMIS and in passwords for the systems. Will be taken up
with NPCB by the SPO for a solution.
5.2.5. Sustainability 5. Co-ordination between NRHM and NPCB 6. Early disbursements of DBCS funds to all NGOs.

28
6. Recommendations by the groups
6.1. Human Resources
1. Ophthalmologists: Currently 350 ophthalmologists are available in Madhya Pradesh. This includes 227 in Government sector. One third of these posts are vacant and another 40% are non-surgical ophthalmologists. The vacant posts need to be filled. Majority of the ophthalmologists are posted under PG-Medical Officer cadre and have to conduct general duties in the hospital. There is need to initiate motivation among non-surgical ophthalmologists for non-surgical ophthalmic including screening camps, follow up services and retina and glaucoma clinics.
2. The ophthalmologists are not showing interest in specialty training for skill transfer. It is suggested that short-term hospital based programme should be conducted with support of voluntary faculty/ RIO faculty with - in their own hospitals. The agencies like VISION 2020 - INDIA can be one of the resources for such programmes. In the long term, RIOs and medical college in Madhya Pradesh should play mentoring role for the training programmes for the ophthalmologists.
3. As per the NPCB guidelines, 1400 PMOA are required in the State. There is need to develop training centres either through Medical Universities or other recognized centres to meet the future demand. All the vacant posts of the PMOA should be filled.
4. Training in all eye care disease priorities such as DR, Pediatric, Glaucoma, Retina, Cornea, Low Vision should be arranged.
5. Team building workshops should be organized for motivation, commitment and improved performance among human resources. This may be done with the support of VISION 2020 – INDIA resources.
6. Training of ASHA workers in primary eye care should be adopted at the Vision Centre level to improve the awareness, identification and referral of blind patients and children with visual impairment. It is suggested that state government should earmark funds for training and output-based honorarium for these workers as done in other National Programmes. NGOs like Sight savers may be utilized for effective implementation of this programme.
6.2. Infrastructure and Equipment
1. Strengthening of Regional Institute of Ophthalmology, Bhopal and Medical colleges in MP a. They should be an integral part of the Blindness Control Programme: The
Blindness Control Programme under Director Health services and Director Medical Education should work in coordination for blindness control activities
b. There is need to assess the current capacity of RIO, Bhopal in order to further strengthen it as centre of excellence for research, training and service delivery in

29
eye care. This may be taken with NPCB or Dr. R.P. Centre for necessary technical support.
c. The RIO, Bhopal should be a separate agency instead of part of Medical College. d. All the speciality eye care services like Paediatric Ophthalmology Unit, Vitreo-
Retina clinic, Low Vision clinic etc should be available in the RIO with high output and good quality services. The RIO should have trained ophthalmologists in all the subspecialties.
e. The RIO and Medical colleges should be responsible for training of ophthalmologists and optometrists all over the State. Currently most of the ophthalmologists have to go to other States for speciality training.
f. RIO and medical colleges should be accountable for the referred cases from the district hospital. There should be some feedback information to the district hospital for referred cases.
g. RIO and medical colleges should be involved in research and surveys in the State. There is a need for conducting survey on blindness, Vitamin A deficiency, blind school etc.
h. The training in Phaco-surgery and availability of Phaco-machines may be considered in all medical colleges and also at the district hospitals.
2. District mobile unit should be available in all the districts. 3. It is recommended that the outreach surgical camps should be strictly prohibited in
the entire State as per the guidelines of NPCB. 4. More emphasis is required for infrastructure development and human resource
availability in the low performing districts, the districts in remote areas or difficult areas. The low performing districts Annupur, Sidhi, Sheopurkala, Harda, Dindori, Alirajpur. The INGOs, local NGOs should be promoted to strengthen the service delivery in these districts.
5. All the CHCs (in Population 50,000 to 100,000) should have well equipped Vision Centres with adequate space for refraction facility. A full time Paramedical Ophthalmic Assistant(PMOA) should be posted in each CHC accountable for the screening camps for cataract and school vision screening programme in the CHC.
6. Regular maintenance of equipment should be undertaken. For this purpose, maintenance of equipments-PMOA or NGO representative may be trained in equipment maintenance.

30
6.3 Disease Control
1. Based on the population and prevalence of blindness as well as the current annual targets, need and unmet services with existing resources should be worked out for setting targets for 2012 onwards. The targets as per the population needs for cataract and school vision screening have been estimated as follows. The district wise targets are also given in the annexure. The district authorities may use these targets for the districts. These targets may be modified for individual districts depending upon other factors like availability of ophthalmologists, NGOs in the area, difficult areas etc.
Years Cataract School Vision Screening
2012-13 4,70,432 23,23,122
2013-14 4,79,841 23,69,584
2014-15 4,89,438 24,16,976
2015-16 4,99,226 24,65,316 2016-17 5,09,211
25,14,622
2. Mapping of eye care services specifically the specialty services should be undertaken in the state. It is suggested that Specialty services should be made available to all divisions.
6.4 Quality & Monitoring
1. Currently cataract surgical records are not maintained in most of the hospitals. The information about cataract surgical outcomes are not available in most of the hospitals. It is suggested that records maintenance should be ensured at all level. HMIS, developed by NPCB, needs to be implemented in all districts and data need to be verified by the DPM for its accuracy and reliability. Short-term training of the district programme managers on MIS and record management is necessary. The record keeping should be shifted from manual to MIS.
2. The follow up of the operated cases should be ensured; NPCB recommend
monitoring of at least 5% of the postoperative cases by DPM. It is not practiced in most of the districts.
6.5 Budget allocation:
1. In addition to NPCB funds, state government should earmark funds for training, IEC and assessments and monitoring of blindness control programme.

31
7. Annexures 1. MP_Cataract surgery– Population based Targets
2. School Vision screening – Population based Targets
3. MP_Meeting Agenda
4. List of participants

32
Annexure 1: MP Cataract surgery– Population based Targets
S.No District Population
Target CSR
Annual Target surgery required as per the population need
2012-13
2013-14
2014-15
2015-16 2016-17
1 Sheopur 687,952 6,480 4,458 4,547 4,638 4,731 4,825
2 Morena 1,965,137 6,480
12,734
12,989
13,249
13,514 13,784
3 Bhind 1,703,562 6,480
11,039
11,260
11,485
11,715 11,949
4 Gwalior 2,030,543 6,480
13,158
13,421
13,689
13,963 14,243
5 Datia 786,375 6,480 5,096 5,198 5,302 5,408 5,516
6 Shivpuri 1,725,818 6,480
11,183
11,407
11,635
11,868 12,105
7 Tikamgarh 1,444,920 6,480 9,363 9,550 9,741 9,936 10,135
8 Chhatarpur 1,762,857 6,480
11,423
11,652
11,885
12,123 12,365
9 Panna 1,016,028 6,480 6,584 6,716 6,850 6,987 7,127
10 Sagar 2,378,295 6,480
15,411
15,720
16,034
16,355 16,682
11 Damoh 1,263,703 6,480 8,189 8,353 8,520 8,690 8,864
12 Satna 2,228,619 6,480
14,441
14,730
15,025
15,325 15,632
13 Rewa 2,363,744 6,480
15,317
15,623
15,936
16,255 16,580
14 Umaria 643,579 6,480 4,170 4,254 4,339 4,426 4,514
15 Neemuch 825,958 6,480 5,352 5,459 5,568 5,680 5,793
16 Mandsaur 1,339,832 6,480 8,682 8,856 9,033 9,214 9,398
17 Ratlam 1,454,483 6,480 9,425 9,614 9,806
10,002 10,202
18 Ujjain 1,986,597 6,480
12,873
13,131
13,393
13,661 13,934
19 Shajapur 1,512,353 6,480 9,800 9,996
10,196
10,400 10,608
20 Dewas 1,563,107 6,480
10,129
10,332
10,538
10,749 10,964
21 Dhar 2,184,672 6,480
14,157
14,440
14,729
15,023 15,324
22 Indore 3,272,335 6,480
21,205
21,629
22,061
22,503 22,953
23 Khargone 1,872,413 6,480
12,133
12,376
12,623
12,876 13,133
24 Barwani 1,385,659 6,480 8,979 9,159 9,342 9,529 9,719

33
25 Rajgarh 1,546,541
6,480
10,022
10,222
10,426
10,635 10,848
26 Vidisha 1,458,212
6,480 9,449 9,638 9,831 10,028 10,228
27 Bhopal 2,368,145
6,480
15,346
15,652
15,966
16,285 16,611
28 Sehore 1,311,008
6,480 8,495 8,665 8,839 9,015 9,196
29 Raisen 1,331,699
6,480 8,629 8,802 8,978 9,158 9,341
30 Betul 1,575,247
6,480
10,208
10,412
10,620
10,832 11,049
31 Harda 570,302
6,480 3,696 3,769 3,845 3,922 4,000
32 Hoshangabad 1,240,975
6,480 8,042 8,202 8,366 8,534 8,704
33 Katni 1,291,684
6,480 8,370 8,538 8,708 8,882 9,060
34 Jabalpur 2,460,714
6,480
15,945
16,264
16,590
16,921 17,260
35 Narsimhapur 1,092,141
6,480 7,077 7,219 7,363 7,510 7,660
36 Dindori 704,218
6,480 4,563 4,655 4,748 4,843 4,939
37 Mandla 1,053,522
6,480 6,827 6,963 7,103 7,245 7,390
38 Chhindwara 2,090,306
6,480
13,545
13,816
14,092
14,374 14,662
39 Seoni 1,378,876
6,480 8,935 9,114 9,296 9,482 9,672
40 Balaghat 1,701,156
6,480
11,023
11,244
11,469
11,698 11,932
41 Guna 1,240,938
6,480 8,041 8,202 8,366 8,533 8,704
42 Ashoknagar 844,979
6,480 5,475 5,585 5,697 5,811 5,927
43 Shahdol 1,064,989
6,480 6,901 7,039 7,180 7,324 7,470
44 Anuppur 749,521
6,480 4,857 4,954 5,053 5,154 5,257
45 Sidhi 1,126,515
6,480 7,300 7,446 7,595 7,747 7,902
46 Singrauli 1,178,132
6,480 7,634 7,787 7,943 8,102 8,264
47 Jhabua 1,024,091
6,480 6,636 6,769 6,904 7,042 7,183
48 Alirajpur 728,677
6,480 4,722 4,816 4,913 5,011 5,111
49 Khandwa 1,309,443
6,480 8,485 8,655 8,828 9,005 9,185
50 Burhanpur 756,993
6,480 4,905 5,003 5,103 5,206 5,310
Madhya Pradesh 72597565
6,480
470,432
479,841
489,438
499,226 509,211

34
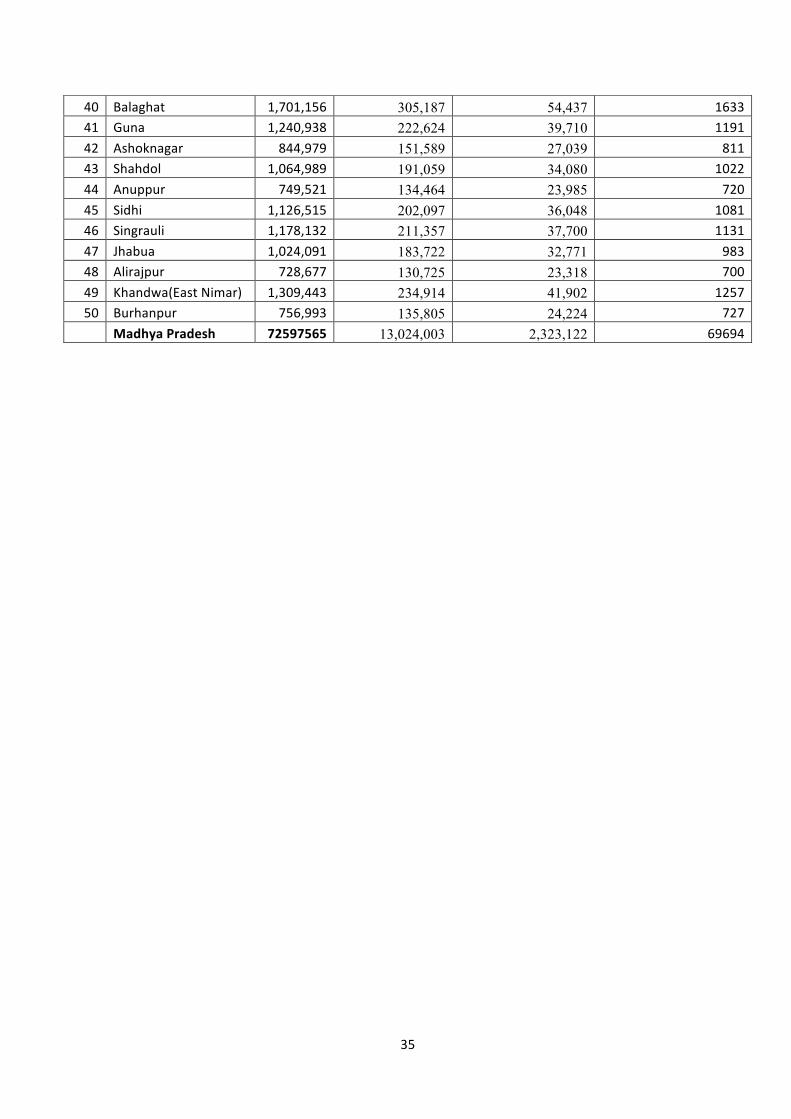
Annexure 2: Annual Targets of School Vision Screening in Madhya Pradesh
S.No District Population district
Total RE including presbyopia all age
Children that need to be screened annually
Estimated Refractive error cases in middle schools
1 Sheopur 687,952 123,419 22,014 660 2 Morena 1,965,137 352,546 62,884 1887 3 Bhind 1,703,562 305,619 54,514 1635 4 Gwalior 2,030,543 364,279 64,977 1949 5 Datia 786,375 141,076 25,164 755 6 Shivpuri 1,725,818 309,612 55,226 1657 7 Tikamgarh 1,444,920 259,219 46,237 1387 8 Chhatarpur 1,762,857 316,257 56,411 1692 9 Panna 1,016,028 182,275 32,513 975
10 Sagar 2,378,295 426,666 76,105 2283 11 Damoh 1,263,703 226,708 40,438 1213 12 Satna 2,228,619 399,814 71,316 2139 13 Rewa 2,363,744 424,056 75,640 2269 14 Umaria 643,579 115,458 20,595 618 15 Neemuch 825,958 148,177 26,431 793 16 Mandsaur 1,339,832 240,366 42,875 1286 17 Ratlam 1,454,483 260,934 46,543 1396 18 Ujjain 1,986,597 356,395 63,571 1907 19 Shajapur 1,512,353 271,316 48,395 1452 20 Dewas 1,563,107 280,421 50,019 1501 21 Dhar 2,184,672 391,930 69,910 2097 22 Indore 3,272,335 587,057 104,715 3141
23 Khargone(West Nimar) 1,872,413 335,911 59,917 1798
24 Barwani 1,385,659 248,587 44,341 1330 25 Rajgarh 1,546,541 277,449 49,489 1485 26 Vidisha 1,458,212 261,603 46,663 1400 27 Bhopal 2,368,145 424,845 75,781 2273 28 Sehore 1,311,008 235,195 41,952 1259 29 Raisen 1,331,699 238,907 42,614 1278 30 Betul 1,575,247 282,599 50,408 1512 31 Harda 570,302 102,312 18,250 547 32 Hoshangabad 1,240,975 222,631 39,711 1191 33 Katni 1,291,684 231,728 41,334 1240 34 Jabalpur 2,460,714 441,452 78,743 2362 35 Narsimhapur 1,092,141 195,930 34,949 1048 36 Dindori 704,218 126,337 22,535 676 37 Mandla 1,053,522 189,002 33,713 1011 38 Chhindwara 2,090,306 375,001 66,890 2007 39 Seoni 1,378,876 247,370 44,124 1324
35
40 Balaghat 1,701,156 305,187 54,437 1633 41 Guna 1,240,938 222,624 39,710 1191 42 Ashoknagar 844,979 151,589 27,039 811 43 Shahdol 1,064,989 191,059 34,080 1022 44 Anuppur 749,521 134,464 23,985 720 45 Sidhi 1,126,515 202,097 36,048 1081 46 Singrauli 1,178,132 211,357 37,700 1131 47 Jhabua 1,024,091 183,722 32,771 983 48 Alirajpur 728,677 130,725 23,318 700 49 Khandwa(East Nimar) 1,309,443 234,914 41,902 1257 50 Burhanpur 756,993 135,805 24,224 727
Madhya Pradesh 72597565 13,024,003 2,323,122 69694

36
Annexure 3: Meeting Agenda
MADHYA PRADESH STATE LEVEL PLANNING MEETING
VENUE: Bhopal, Madhya Pradesh
DATE & TIME:
8th February 2012, 4:00 PM – 6:00 PM
9th February 2012, 9:00 AM to 5:00 PM
AGENDA FOR 8TH FEBRUARY 2012, 4:00 PM – 6:00 PM:
1. WELCOME NOTE – 10 MINUTES Dr. V.A. Joshi/ M.P. government representative to address the delegates and briefly discuss the purpose and agenda of the meeting.
2. INTRODUCTION TO VISION 2020: THE RIGHT TO SIGHT – INDIA -‐ 10 MINUTES Dr. Col Deshpande
3. MAGNITUDE OF BLINDNESS AND STATUS OF EYE CARE SERVICES IN MADHYA PRADESH – 30 MINUTES PRAVEEN VASHIST WILL TALK ABOUT THE PREVALENCE OF BLINDNESS, MAJOR CAUSES AND KEY
STRATEGIES OF PREVENTABLE BLINDNESS. This session would also involve a situational analysis on the state of eye care services in Madhya Pradesh focusing on current and required human resources, training, finances & budgets, infrastructure needs. The situational analysis would be performed based on the study done in 2008/ 09.
4. BRAINSTORMING SESSION – 60 MINUTES Dr. V.A. Joshi, Dr. Praveen Vashist, Col. Deshpande and Dr. G.V. Rao would lead this session. SETTING TARGETS FOR DISEASE, INCREASING PRODUCTIVITY-‐ DEMAND AND HR TRAINING, INFRASTRUCTURE,
5. CONCLUDING REMARKS-‐ 10 MINUTES Dr. V.A. Joshi, Col. Deshpande
AGENDA FOR 9th February 2012, 9:00 AM to 5:00 PM
1. REGISTRATION10.00 AM – 10.30 AM
2. INTRODUCTION OF PARTICIPANTS AND BRIEFING OF DAY ONE ACTIVITIES-‐ DR. G.V.RAO-‐ 10.30-‐10.45
3. INTRODUCTION TO VISION 2020: THE RIGHT TO SIGHT – INDIA AND COMPONENTS OF A STATE ACTION PLAN –10.45-‐10.50 AM– COL. DESHPANDE
5. Disease burden assessment-‐ using templates–Dr. Praveen Vashist 10.50-‐11.05
6. QUALITY ASSURANCE AND MONITORING INDICATORS FOR STATE ACTION PLAN-‐ DR. UDAY GAJIWALA
11.05-‐11.20

37
7. IEC, Integration and sustainability in eye care -‐11.20-‐11.50
• IEC including social marketing for eye care in M.P.-‐ 10 minutes Mr. Anand Sudan
• Integrated eye care in M.P.-‐ 10 minutes-‐ Ms. Archana Bhambhal • Sustainability in eye care-‐ 10 minutes-‐ Mr. Prateep Chakrarvati
This will be followed by group discussion facilitated by various speakers where the following topics will be discussed and based on the inputs received; a state plan for Madhya Pradesh would be developed by participants. – 2 hours 30 minutes ( 11.50-‐ 1.00 PM)
a. Disease burden and various strategies to disease control– Facilitated by Praveen Vashist
b. Human resources and training needs –Facilitated by Mr. Ananad Sudan c. Infrastructure and equipment maintenance – Facilitated by Col. Deshpande d. Quality assurance, reporting, Monitoring and accountability– Facilitated by Dr. Uday
Gaziwala, Mr. Sarfaraj e. IEC, Integration and sustainability in eye care –D. Joshi, Ms. Archana Bhambhal, Mr.
Prateep Chakrarvati Lunch-‐1.00 PM to 2.00PM
2. PRESENTATION OF GROUP WORK AND DISCUSSION– 10 MINUTES FOR GROUP PRESENTATION AND
DISCUSSION (2.00PM TO 4.00 PM) MODERATORS-‐ DR.V.A JOSHI, DR. PRAVEEN VASHIST, COL. DESHPANDE, DR. GV RAO, DR. UDAY
GAJIWALA 3. COMPILATION OF WORKSHOP REPORT-‐ DR. NOOPUR GUPTA 4. DR.V.A JOSHI, DR. PRAVEEN VASHIST, COL. DESHPANDE will present a brief summary of the
compiled report in State Secretariat.
38
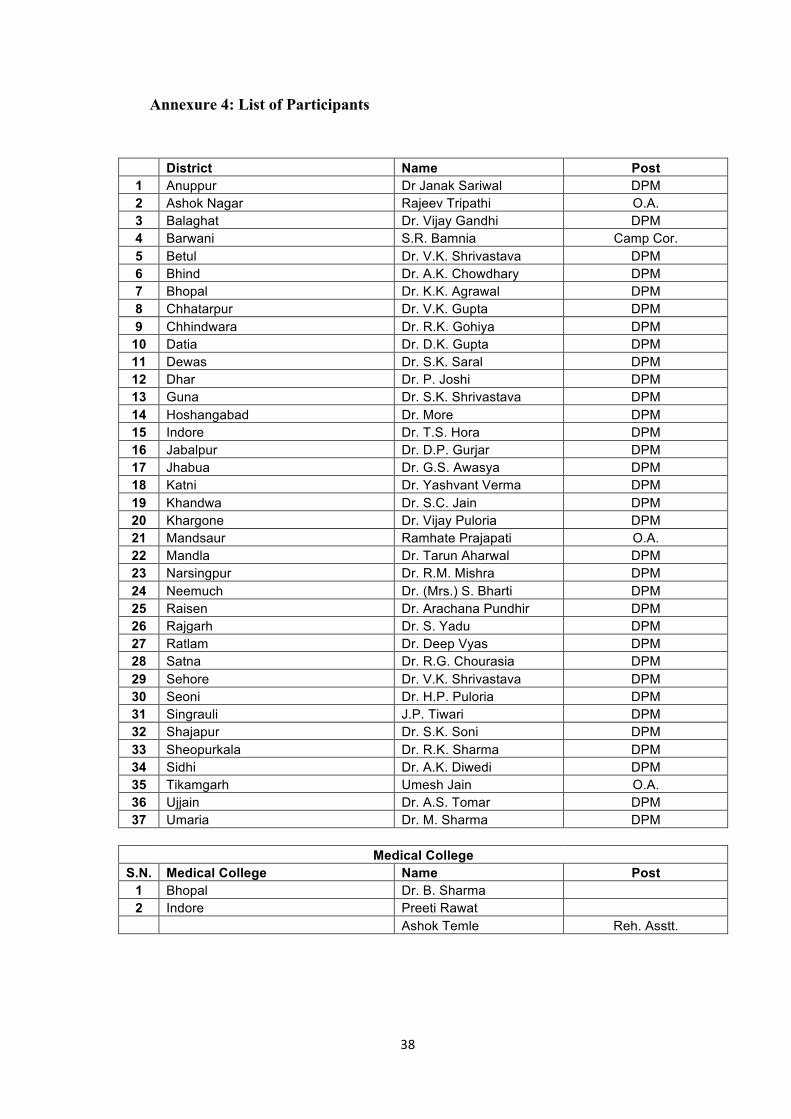
Annexure 4: List of Participants
District Name Post 1 Anuppur Dr Janak Sariwal DPM 2 Ashok Nagar Rajeev Tripathi O.A. 3 Balaghat Dr. Vijay Gandhi DPM 4 Barwani S.R. Bamnia Camp Cor. 5 Betul Dr. V.K. Shrivastava DPM 6 Bhind Dr. A.K. Chowdhary DPM 7 Bhopal Dr. K.K. Agrawal DPM 8 Chhatarpur Dr. V.K. Gupta DPM 9 Chhindwara Dr. R.K. Gohiya DPM
10 Datia Dr. D.K. Gupta DPM 11 Dewas Dr. S.K. Saral DPM 12 Dhar Dr. P. Joshi DPM 13 Guna Dr. S.K. Shrivastava DPM 14 Hoshangabad Dr. More DPM 15 Indore Dr. T.S. Hora DPM 16 Jabalpur Dr. D.P. Gurjar DPM 17 Jhabua Dr. G.S. Awasya DPM 18 Katni Dr. Yashvant Verma DPM 19 Khandwa Dr. S.C. Jain DPM 20 Khargone Dr. Vijay Puloria DPM 21 Mandsaur Ramhate Prajapati O.A. 22 Mandla Dr. Tarun Aharwal DPM 23 Narsingpur Dr. R.M. Mishra DPM 24 Neemuch Dr. (Mrs.) S. Bharti DPM 25 Raisen Dr. Arachana Pundhir DPM 26 Rajgarh Dr. S. Yadu DPM 27 Ratlam Dr. Deep Vyas DPM 28 Satna Dr. R.G. Chourasia DPM 29 Sehore Dr. V.K. Shrivastava DPM 30 Seoni Dr. H.P. Puloria DPM 31 Singrauli J.P. Tiwari DPM 32 Shajapur Dr. S.K. Soni DPM 33 Sheopurkala Dr. R.K. Sharma DPM 34 Sidhi Dr. A.K. Diwedi DPM 35 Tikamgarh Umesh Jain O.A. 36 Ujjain Dr. A.S. Tomar DPM 37 Umaria Dr. M. Sharma DPM
Medical College S.N. Medical College Name Post
1 Bhopal Dr. B. Sharma 2 Indore Preeti Rawat Ashok Temle Reh. Asstt.
39
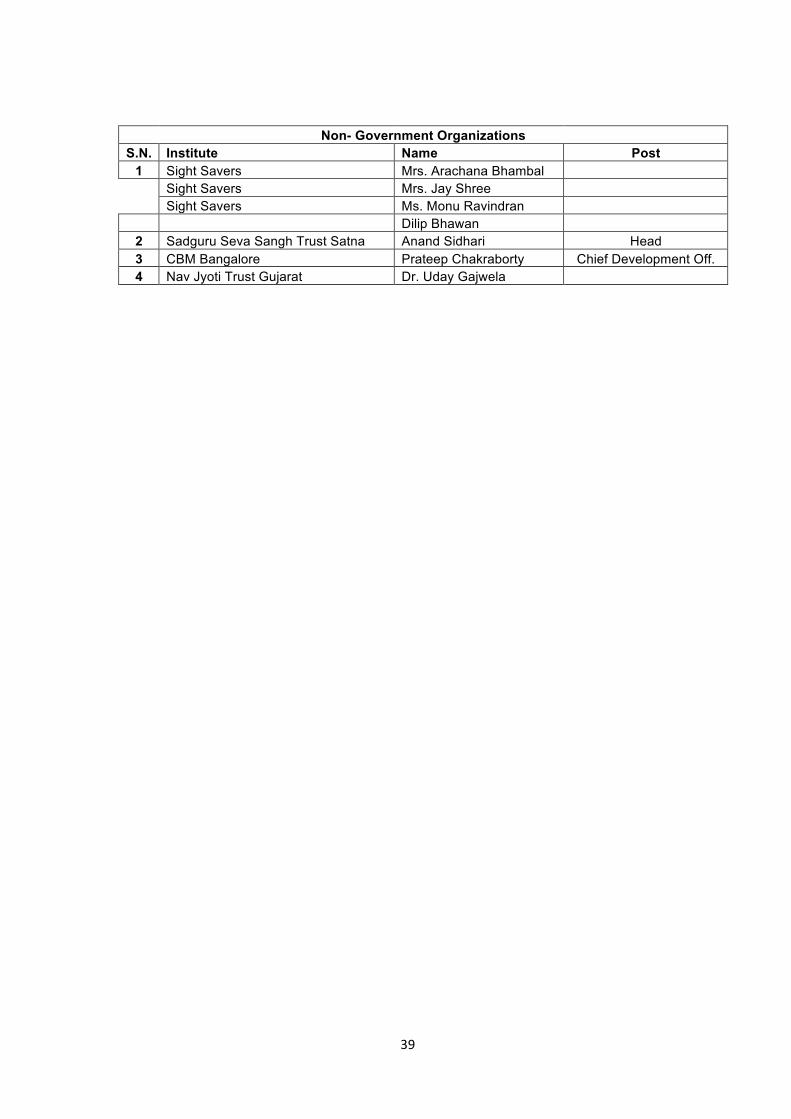
Non- Government Organizations S.N. Institute Name Post
1 Sight Savers Mrs. Arachana Bhambal
Sight Savers Mrs. Jay Shree
Sight Savers Ms. Monu Ravindran
Dilip Bhawan 2 Sadguru Seva Sangh Trust Satna Anand Sidhari Head 3 CBM Bangalore Prateep Chakraborty Chief Development Off. 4 Nav Jyoti Trust Gujarat Dr. Uday Gajwela