modeling flow through a normal and calcified coronary artery
TRANSCRIPT

Modeling Flow through a Normal and Calcified Coronary
Artery
BME 429 Fluids Module Report Lab Group 5
Alex Thomason, Sarea Recalde Phillips, Thaddeus Schlamb
This lab investigates the hemodynamics of a normal and diseased coronary artery through
simulation and experimentation. The diseased artery experiences calcification around the
artery wall, decreasing the diameter of the artery creating a stenosis that affects blood flow
through the artery. Normal and calcified coronary arteries were extracted from patient
specific MRI images through Mimics. Through the use of COMSOL, particle visualization
flow was modeled and compared in both arteries. To validate the COMSOL fluid flow
models, hollowed arteries were created in 3Matics and 3D printed for benchtop testing.
The results of the particle tracing were based off the results of a time-dependent laminar
flow physics study that gave us the velocity profile through the normal and diseased model.
Hollow 3D models of the diseased and normal coronary arteries were printed and polished
so a dyed fluid with similar viscous properties of blood could be pumped through the
models. The fluid was pumped at the same velocity and pressure that was used in the
COMSOL simulations to provide consistency of boundary conditions. The fluid flow was
videotaped to capture how the fluid flowed through the diseased and normal arteries. Flow
through the benchtop experiment was similar to the COMSOL model, validating the
computational simulation.
Keywords - Coronary artery, stenosis, calcification, COMSOL, Mimics, CVD,
hemodynamic
I. Introduction
Cardiovascular disease (CVD), which narrows
blood vessels, causes strokes, heart attacks, and
various other heart maladies. This medical malady
is a growing concern across the world. In America
alone, 11.5% or 27.6 million adults have some form
of heart disease. In America the mortality rate has
become 221.9 per 100,000 afflicted with CVD. [1]
While over 7 million people in the United Kingdom's
are affected with CVD; with a new death every 8
minutes. [2] CVD can be prevented by reducing risk
factors, and by improving one’s diet and exercise
regiment. [3] Yet, CVD is currently irreversible, so
while preventable measures are important the
effects of the disease must be studied.[4]
The most common variation of CVD is coronary
artery disease, which can go without detection until
a heart attack. [5] Coronary artery disease occurs
when low-density lipoprotein (LDL) cholesterol
adhere to the vascular wall near areas of high shear
stress and turbulent flow. Behind the vascular wall,
macrophages consume the LDL cholesterol and
converts it to a foam cell. These foam cells thicken
with time into plaque starting the stenosis in the
artery. [6] As the stenosis grows it can constrict
blood flow leading to a heart attack. In addition, if
the pressure and shear stress is large enough the
vascular walls can rupture, allowing plaque to enter
blood flow and potentially damaging blood cells and
creating a blockage leading to a stroke. [7]

There are various methods to treat and manage
coronary artery disease. This includes medications
such as angiotensin-converting enzyme (ACE)
inhibitors, which dilates the blood vessels and
reduces high pressure gradients in the coronary
artery. [8] The more severe treatments include
coronary bypass surgery and balloon angioplasty
surgery. Coronary artery bypass grafting is when an
exterior vein is applied around the stenosis
improving blood flow while reducing pressure near
the stenosis.[9] Coronary angioplasty surgery is
when a catheter is positioned within the stenosis,
and a balloon inflates and compresses the stenosis.
A stent is placed in the reduced stenosis to
preventing decompression. [10] With the severity of
treatments and its high mortality rate coronary
artery disease has become a central point of
biomedical research.
Recently, efforts have been centralized around
modeling fluid flow paths within the cardiovascular
system. Until the advancements in computational
modeling, most fluid studies were restricted to
benchtop animal models or artificial models. With
the new use of computer modeling and its inherent
ability to solve complex differential equations
through finite element analysis, complex
hemodynamic studies can be solved. This allows
for improved fluids research in complex vessel
designs and potential treatments. This improved
computational method saves time and money
before a single prototype is produced. Therefore,
our concern for this project centered around
validating our computational model.
This fluid module began by extracting normal and
diseased models of two different coronary arteries
from two different MRI images in Mimics. The
purpose of this was simply to establish a 3D model
of each both arteries. It was important to obtain an
accurate model of the diseased artery with a visible
stenosis due to calcifications. In theory, the normal
artery model should have a clear path for blood
flow. After a rough model is obtained, it can be
smoothed using a wrapping tool, which will help
yield more accurate results later in the module.
Once the models were obtained in Mimics, they
were imported to 3Matics. The solid models were
smoothed, remeshed, and processed to import to
COMSOL. Additionally, secondary models of the
diseased and healthy arteries were hollowed and
remeshed to be 3D printed for benchtop
experimentation.
Once the solid models of the normal and
diseased arteries were meshed properly, they were
imported to COMSOL. The purpose of the
COMSOL simulations was to complete two, time-
dependent physics studies (laminar flow and
particle tracing) for the normal and diseased artery.
The laminar flow study yielded the velocity and
pressure profiles for both models as the fluid flowed
from the inlet to the outlet. The particle tracing study
used the results from the laminar flow study to trace
3,000 particles through the diseased stenosis and
normal model.
Each member’s diseased stenosis model of the
coronary artery was 3D printed so that a physical
experimental study could be performed to compare
the results of the particle tracing to the actual flow
in the 3D printed hollow models. In total the group
had three diseased models and one provided
normal hollow model to test.
After completion of the simulation, the benchtop
experiment was prepared. 3D printed samples of
the arteries were sanded to improve visibility. An
analogous blood fluid was created with added food
dye to improve visibility. The analogous blood fluid
was pumped through the 3D printed model using a
at a rate resembling conditions exhibited in the
body. Finally, videos were taken of fluid flow
through the 3D models and compared to the
simulation.
In total, the goals of this experiment:
1. Complete a time-dependent laminar flow
physics study for the normal coronary
artery and the three diseased coronary
arteries.
a. Compare how the velocity profile
differs between the normal and
diseased models.
b. Compare how the velocity in the
diseased model (stenosis) with the
theoretical trends that should occur
in a stenosis, according to
Bernoulli's equation.
2. Compare the average velocity of the actual
model to the corresponding COMSOL
model from the time-dependent laminar
flow physics study.

3. Complete a time-dependent particle
tracking physics study for the normal
coronary artery and the three diseased
coronary arteries.
4. Compare the particle tracking simulation to
the flow of the glycerine/water solution in
the actual models.
II. Methods and Materials
This project was broken into two sections. The
first half of this section focuses on the
computational simulation of fluid flow, while the
second half focuses on the bench top
experimentation. Both section evaluated healthy
and diseased coronary arteries.
A. Computational Simulation
i. Mimics
Structural hydrogen MRI images of heart with
healthy and calcified coronary arteries were
accessed in Mimics. By selecting the images’
voxels based on their grayscale intensity the
coronary artery could be transformed into a 3D
model. This was easily accomplished through the
growing region tool in Mimics, and then by hand
editing the Mask. After the 3D models were
produced, they were wrapped and smooth to
reduce the rough edges from the cubic voxels and
edited for discontinuities. This process was used to
create 3D models of the healthy and diseased
coronary arteries. It is important to note, that the
calcification could be seen around diseased artery
due to the bright grayscale value.The calcification
was not selected, resulting in the stenosis seen in
the disease models. After 3D models were created
they were exported to 3Matics for further
processing.
ii. 3Matics
After exporting the 3D models from Mimics to
3Matics, the trim tool was utilized to create clear
inlets and outlets. The 3D model was then
remeshed, using the autoremesh feature,
equalizing the mesh dimension across the model
and further smoothing the model. Then the three
dimensional mesh was converted to a volumetric
surface mesh. To ensure surface selection of the
inlets and outlets in COMSOL, the mark smooth
region was applied to simplifying the mesh at the
inlet and outlet. After these steps were completed
the meshes of the healthy and diseased arteries
were exported to COMSOL as mesh files
(.MPHTXT).
iii. COMSOL
The full setup of the comsol simulation is listed in
Appendix A. To determine the type of fluid flow,
laminar or turbulent, literature values of average
coronary blood flow velocity, blood density, blood
viscosity, and the 3D models’ diameter were used
to calculate the Reynolds number using the
equation
𝑅𝑒 = 𝜌𝑉𝐿
𝜇.
Density, flow velocity, and viscosity were based on
typical values for blood, and length was based on
arterial length. For both healthy and calcified
arteries, it was found to be laminar flow. In
COMSOL, a 3D time-dependent laminar flow study
was selected. The imported mesh was given
density and dynamic viscosity values of blood found
from literature. At the inlet, a steady inflow velocity
was used as a boundary condition, while at the
outlet the average physiological blood pressure of
100 mmHg was used. A no slip condition was set at
the walls and an initial value of 100 mmHg was set.
After solving for pressure and velocity fields across
the healthy and diseased artery, a second time
dependent study was added.
The second time-dependent physics was particle
tracing flow. The drag force was calculated using
Stoke’s law, and linked to the velocity field,
viscosity, and density from the initial study. The
walls and outlet of both models were set to freeze.
Particle properties were solid with a diameter of
0.5μm, with 3000 particles release. In this second
physics a video was created to show particle
trajectory fields through the artery.
B. Benchtop Experiment
i. 3Matics
The same 3D models created in Mimics were
imported into 3Matics. This time the model was
hollowed, using the hollow tool. Then the trim tool
was used to create inlets and outlets on the models.
The hollowed diseased model was saved as an
.STL file. The normal hollow model was provided by
the course.
ii. 3D Printing and Finishing

The diseased and healthy models were 3D
printed by a Formlabs Form 2 stereolithography
3D printer (Formlabs Inc, Somerville, MA). The
printing material was composed of a polypropylene
mimic. After printing, models were covered in
isopropyl alcohol and heat treated. To improve flow
visualization, healthy and diseased arteries
underwent wet sanding with 800-,1500-, and 2000-
grade sandpaper. Finally the models were
immersed in water to remove any excess debris.
iii. Solution Preparation
Water and glycerin, and blue food dye were
materials used to create the analogous blood
solution. A 20mL solution with a 40/60 ratio of
glycerin and water was mixed with addition of food
dye to improve visibility through the arteries. This
specific ratio was created to match the dynamic
viscosity of blood at body temperature of 2.78
mPa*s [11]. At room temperature, a 41%
glycerin/water mix yields a dynamic viscosity of
0.0027889 Ns/m2 [12]
iv. Experimental Setup and Data
Acquisition
A 16G, 1” needle syringe (SAI Infusion
Technologies) was attached to a syringe pump
(NE-300 Just InfusionTM Syringe Pump), the former
being 11.43cm from the base. A 21.59cm-long
plastic tube (SILASTICTM Laboratory Tubing) was
attached to the tip of the syringe needle and placed
in the entrance of the 3D healthy and diseased
models.
The flow rate of the syringe pump was calculated
in proportion to the dimensions of the 3D models
using the equation
𝑉1𝐴1 = 𝑉1𝐴2,
where V1, A1, and A2 were established to be blood
flow velocity, the area of an artery, and the area of
the syringe, respectively. Given the parameters, the
flow rate of the syringe pump was calculated to be
7.35 mm/sec.
Models were placed on a flat surface where a
ruler was placed with respect to the model’s most
longitudinal orientation. The glycerin-water solution
was pumped . Video recordings were performed on
an iPhone 8 (Apple Inc, Cupertino, CA) at 60
frames/second.
III. Results
A. Benchtop Results
Figure 1. Fluid flow before stenosis in 3D models.
Figure 1 depicts the flow profile of the dyed liquid
before the stenosis. Note that the normal coronary
artery does not have a stenosis. Figure 1A has an
irregular flow profile at 0.40 seconds. Figures 1A
and 1B have an even flow profile, the latter reaching
the stenosis at 0.95 seconds. Figure 1C has a
narrower pre-stenosis region than the normal
model, as well as Figures 1A and 1B, and reached
the stenosis at 0.70 seconds. Figure 1D has a more
constant wide diameter because there are no
calcifications to obstruct the flow and reached a
distance where a stenosis would have occurred at
0.75 seconds.
Figure 2. Fluid flow at stenosis in 3D models.
Figure 2 shows the flow profile of the dyed liquid
before the stenosis. Note that the normal coronary
artery does not have a stenosis. Figure 2A has a
more abrupt, narrow stenosis compared to the rest
of the cross section, and reached stenosis at 1.13
seconds. The flow profile of the fluid is slightly
irregular as it passes through the stenosis. Figure
2B, which reached the stenosis after 1.90 seconds
has the narrowest stenosis of the diseased models
but has a somewhat irregular, curved flow profile
when the fluid passes through the narrowed region.
Figure 2C depicts more of a constant narrowed
stenosis as opposed to an abrupt narrowing of the
fluid pathway and reached the stenotic area after
2.10 seconds. However, there is an irregular flow
profile when the fluid passes through the narrowest
region. Figure 2D continues to have a normal flow
profile because there were no calcifications to
create a stenosis. This figure reached what would
have been the stenotic point after 1.75 seconds.

Figure 3. Fluid flow after stenosis in 3D models.
In Figures 3A-3C, the cross section of the fluid
pathway increases after the stenosis. Figure 3A
achieved a concave flow profile after the stenosis
and reached this point after 2 seconds. Both the
second and third diseased model has an irregular
flow profile, both passing the stenosis after 2.70
and 2.60 seconds, respectively. Figure 3D, normal
model, has a regular flow profile since it has the
same cross section as the rest of the model, and
passed where the stenotic area would be after 2.48
seconds.
The average velocity of each 3D printed model
was calculated by timing how long it took for the
dyed fluid solution to pass from the inlet to the outlet
and dividing that time by the length of the model. As
seen in Table 1, aside from model 1 (Sarea), the
diseased models’ velocity values were higher than
the normal model’s.
Model Label Average Velocity [cm/s]
A (Ted) 1.38
B (Sarea) 1.04
C (Alex) 1.5
D (Normal) 1.12
Table 1. Average velocities of 3D models
B. COMSOL RESULTS
Figure 4. Particle tracing of diseased and normal
coronary arteries.
The goal of the particle simulation is to obtain a
qualitative computational results in regards to the
particle tracing physics study. Each figure shows
the trend of how 3,000 particles flow through the
three diseased models and the normal model. The
first diseased model is shown to have a very narrow
passageway for the blood to flow. The middle blue
section is where the stenosis is most prominent.
The blood crosses the stenosis with a velocity of
approximately 0.05 m/s. The particles just before
and after the stenosis have an approximate velocity
from 0.1 - 0.2 m/s. The second diseased model
simulation shows the particles as they are entering
the stenosis. The particles flow from a wider cross
section to a considerably narrower cross section.
The particles start to pick up a velocity of about
25E-3 - 30E-3 m/s when traveling through the
stenosis. The particles just before and after the
stenosis have an approximate velocity of 5E-3 -
20E-3 m/s. The third diseased model shows
particles traveling through a relatively steady cross
section with a stenosis towards the end. The
particles travel through the stenosis from
approximately 0.06 - 0.07 m/s. The particles just
before and after the stenosis have a velocity from
0.03 - 0.05 m/s.
Figure 5. Developed velocity field.
This fully developed velocity shows the velocity
of the fluid at various points in the models. It is
interesting to note the normal velocity profile has a
relatively steady velocity throughout the entire
model. When comparing the relatively normalized
slices of the healthy model to the three diseased
models it is polar opposite; as with the disease
models the average flow varies significantly due to
the slice location in reference to the stenosis. The
highest velocity are often seen within the stenosis
with lower velocity profiles before and after the
stenosis. In Figure 5 B, the velocity profile near the
stenosis is almost zero, with a very tiny area of
high velocity in the center.
IV. Discussion
A. Mimics and 3Matics
The models were converted into .STL files and
.MPHTXT files through Mimics and 3Matics,
respectively. Extracting the 3D model in Mimics
was challenging due to the large field of view of the
MRI images, and the low contrast between the
artery and heart muscle. If the contrast noise was
improved through histogram equalization or some
other imaging processing it would have improved
the accuracy of the 3D model. Therefore, it is

possible that the healthy model and disease model
were not fully anatomically correct. This explains
how the three diseased models, which were all
taken from the same image, are very different. For
more accurate results, higher contrast images are
needed for more anatomically correct arteries.
B. COMSOL
According to the particle tracing study, the
healthy model displayed straight, undisturbed flow,
while the diseased model had a general trend of
slower fluid. The diseased model was expected to
have slow velocity regions of recirculation and
eddies, especially after the stenosis. The slower
velocities in the diseased models create more
stagnation of the blood and increase the chance of
clot formation. Calcifications in the diseased
arteries restrict blood flow and further increase the
chance of thrombus formation. This can be seen at
the end of the particle tracing study, as some
particles adhere to areas that restrict blood flow.
The inefficiencies of the diseased coronary arteries
reduce the amount of oxygen that is delivered to the
cardiac muscle, which will cause other
physiological problems.
The laminar flow study shows that the velocity of
the normal model is relatively constant throughout
the whole model. This is expected since there is no
stenosis in a healthy coronary artery. Alternatively,
this study shows that the velocity of each diseased
models have higher velocity of blood in the stenotic
region of the model and lower velocities before and
after the narrowed region. This is expected
because of the Bernoulli's equation calculation,
which proves that the narrow region of a stenosis
should have an increase in velocity. The steps of
this proof can be seen below:
An exception of this is the stenosis of the first
diseased COMSOL model since the velocity of the
fluid slows in the stenotic area. The other diseased
models follow the expected result.
The computational model mostly agrees
with the bench top simulations and will be
discussed in the following section.
C. Benchtop Experiment
Due to the available equipment and
structure of this project the benchtop model yielded
more qualitative than quantitative results. The
average velocity profile was determined for each
disease model with a timer and a ruler, hindering
the accuracy of the results obtained. This is due to
the complex shape and bend of the model which
affects the measurement, and the accuracy of the
tubing connection between inlet and outlet. What
could be visually seen, was the turbulent flow and
eddies produce by the disease models. The healthy
models had smoother and more laminar flow. In
addition, while the video cannot be shown, the flow
rate through the stenosis of all disease model was
always larger than the flow rate before and after the
stenosis. As discussed above, this makes logical
sense due to Bernoulli’s Equation. Because the
turbulent flow, eddies, and proper velocity profiles
were verified through videos, the results of the
benchtop model validate the results seen within the
COMSOL simulation.
D. Errors and Improvement

The first and most obvious improvement that
could have been made to this experiment was the
comparison of the 3D printed normal artery model
and the normal COMSOL model. Due to lack of time
and resources, one normal model was printed per
group and didn’t match the COMSOL model that it
was compared to. Therefore, determining if the
discrepancies are due to different geometries or
another factor was difficult. The 3D printed models
could have also been sanded to be clearer. This
could have been accomplished by sanding longer
with both the rough and fine sand paper under
water. Although the dye is visible through the
models, it is hard to get a finer perspective on how
the flow field actually looks like. This could include
backflow, eddies, and stagnant flow. It would also
be easier to compare the flow between the 3D
printed models and the COMSOL particle tracking
simulation. There is likely error in the calculations
for the average velocities during the benchmark
experiment because the time that it took for the
liquid to go from the inlet to the outlet was manually
timed. The displacement of the fluid was also
difficult to measure because of the complex
geometry. Lastly, there could have been some
resolution error from the 3D printing process, which
could cause the geometry of the printed models to
vary slightly from the computer models. Making
these improvements would add value and accuracy
to the results.
V. Conclusion
The purpose of the experiment .was to convert
medical images into useable 3D models to study
coronary artery disease fluid flow. Computational
modeling allows for a faster analysis on factors that
can contribute to blood flow in healthy and diseased
arteries, as well as provide insight on how flow is
affected by blockage of the artery. From this study,
COMSOL models of diseased models
demonstrated a less developed parabolic flow and
decreased flow velocity when in the presence of a
blocked arterial area.
Benchtop analysis further supported the
information obtained from COMSOL simulations
pertaining to flow rate. Using 3D models and
documenting flow in real time allowed for average
flow over the entire model. This data suggests that
not only is flow affected and inhibited near blocked
arterial regions, but the flow overall is affected.
This trend is essential in understanding the
health effects that blocked arteries have in real
scenarios; a diseased coronary artery inhibits blood
flow and increases the chance for blood to
accumulate, thereby increasing risk of heart attacks
and even death in humans. Cardiovascular disease
is a reversible healthcare problem, and utilizing
computational and benchtop analysis helps
contribute more solutions in healthcare before
fatalities occur in the human population.
References
[1] Benjamin EJ, Virani SS, Callaway CW, et al.
Heart disease and stroke statistics - 2018 update:
A report from the American Heart Association.
Circulation.2018.
doi:10.1161/CIR.0000000000000558
[2] Statistics BHFH. Cvd Statistics – Bhf Uk
Factsheet Deaths From Cvd and Numbers Living
With Cvd. Br Hear Found. 2018
[3] Statistics BHFH. Cvd Statistics – Bhf Uk
Factsheet Deaths From Cvd and Numbers Living
With Cvd. Br Hear Found. 2018.
[4] Nissen S. Is Heart Disease Curable? Health
Essentials from Cleveland Clinic.
https://health.clevelandclinic.org/is-heart-disease-
curable/. Published September 6, 2018. Accessed
November 5, 2018.
[5] Coronary Artery Disease: Causes, Diagnosis &
Prevention. Centers for Disease Control and
Prevention.
https://www.cdc.gov/heartdisease/coronary_ad.ht
m. Published August 10, 2015. Accessed
November 5, 2018.
[6] Bhatia SK. Coronary Artery Disease. In:
Biomaterials for Clinical Applications. New York,
NY: Springer; 2010:23-49. ISBN: 978-1-4419-
6919-4
[7] Falk E. Plaque rupture with severe pre-existing
stenosis precipitating coronary thrombosis.
Characteristics of coronary atherosclerotic plaques
underlying fatal occlusive thrombi. Heart. 1983.
doi:10.1136/hrt.50.2.127

[8] Izzo JL, Weir MR. Angiotensin-converting
enzyme inhibitors. J Clin Hypertens. 2011.
doi:10.1111/j.1751-7176.2011.00508.x
[9] Coronary Artery Bypass Grafting. National Heart
Lung and Blood Institute.
https://www.nhlbi.nih.gov/health-topics/coronary-
artery-bypass-grafting. Accessed November 5,
2018.
[10] Coronary angioplasty and stents. Mayo Clinic.
https://www.mayoclinic.org/tests-
procedures/coronary-angioplasty/about/pac-
20384761. Published December 30, 2017.
Accessed November 5, 2018
[11] Pop GA, Duncker DJ, Gardien M, et al. The
clinical significance of whole blood viscosity in
(cardio)vascular medicine. Neth Heart J.
2002;10(12):512-516.
[12] Calculate density and viscosity of
glycerol/water mixtures. Calculate density and
viscosity of glycerol/water mixtures.
http://www.met.reading.ac.uk/~sws04cdw/viscosity
_calc.html. Published April 4, 2018. Accessed
November 4, 2018.

A1. COMSOL Setup (Ted)
Table 2. Setting Up Laminar Flow Study
Define Space Dimension
Select Physics
Choose Laminar Flow
Select Study
Choose Time Dependent Study
Import Mesh
Right click on Mesh, select import, Change source to COMSOL Multiphysic file and import either the diseased or healthy model.
Create Material
Right click on Materials, select Blank Material.
Define Material
Select the Blank Material. Under Material Properties Select Density and Dynamic Velocity.

Define the Material properties Values under material content. Note the dynamic viscosity and density is equivalent to literature values of normal blood.
Define Fluid Properties
Under Fluid Properties, select the density to be from the material and the dynamic viscosity to be from the material.
Define Initial Values
Under the Initial Values set the pressure to be 11600 Pa which is equivalent to blood pressure in the coronary artery.
Define Wall Condition
Under Wall 1, select all surfaces except the inlet and outlet. Under the boundary condition tab change the wall condition from No Slip to Slip Velocity.

Define Inlet Conditions
Under Inlet 1, select the inlet surface of the model. Under Boundary Condition change it from Velocity to Laminar Flow. Select the Average velocity button. Define Average Velocity to be 0.233 m/s and entrance length to 0.2m to verify laminar flow. The average velocity value was determined from coronary artery research paper.
Define Outlet Conditions
Under Outlet 1, first select the outlet surfaces of the model. Under Boundary condition select Pressure. Under Pressure Conditions define the pressure to 11600 Pa and select the suppress backflow button.

Solve and Compute
The study settings can be selected as shown below. Once selected hit compute.
Results
Under Results the velocity field can be seen. To adjust the amount and location of slices the slice 1 settings can be Adjusted.
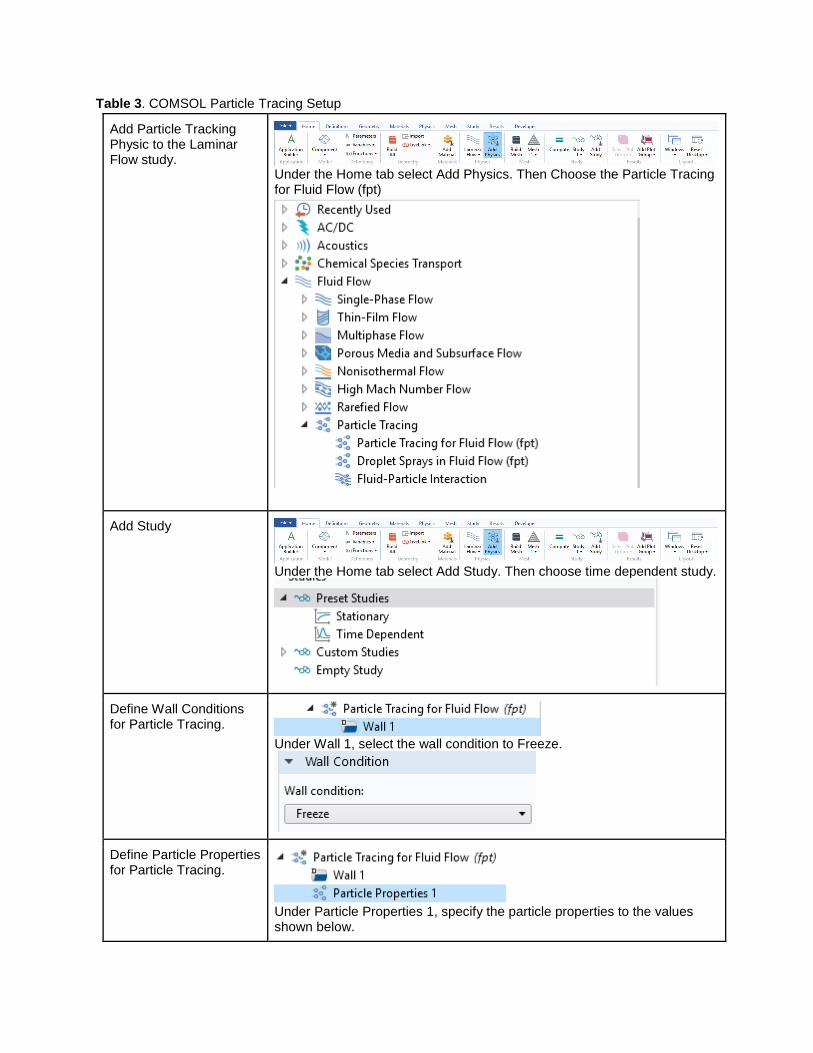
Table 3. COMSOL Particle Tracing Setup
Add Particle Tracking Physic to the Laminar Flow study.
Under the Home tab select Add Physics. Then Choose the Particle Tracing for Fluid Flow (fpt)
Add Study
Under the Home tab select Add Study. Then choose time dependent study.
Define Wall Conditions for Particle Tracing.
Under Wall 1, select the wall condition to Freeze.
Define Particle Properties for Particle Tracing.
Under Particle Properties 1, specify the particle properties to the values shown below.

Define the Inlet Conditions for Particle Tracing
Under Inlet 1, select the initial position and initial velocity settings shown below. Make sure the inlet surface is selected.

Define Outlet conditions for Particle Tracing
Under Outlet 1, make sure to select the outlet surface. Define the outlet wall condition to freeze.
Define Drag Force conditions for Particle Tracing
Under Drag force, in the drag force tab, make the selections below.

Define Study 2 Time dependent solver configurations.
Adjust the Values of dependent variables as seen below then hit compute. A Direct Solver should be used for computation. Make sure the first study has been computed, or the second study will not compute.

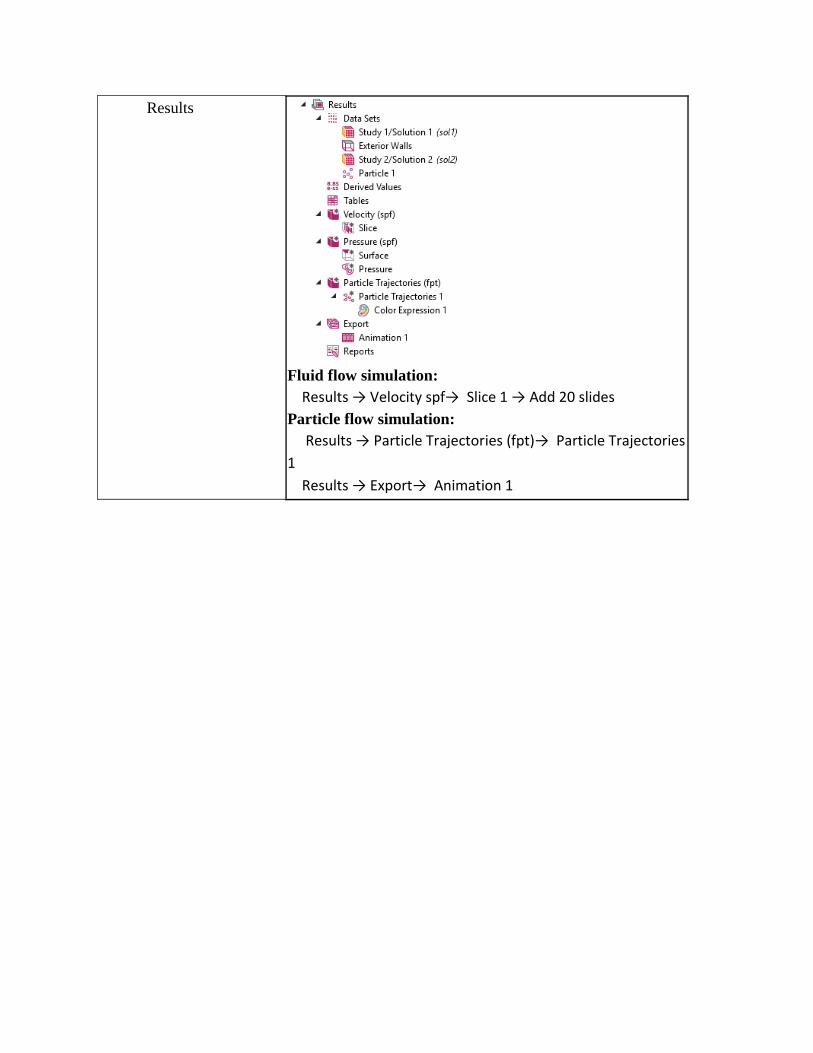
Results
Under Particle Trajectories the various time points of the particles and their velocities can be plotted. All the time points can be exported to a video by hitting the animation button, located in the particle trajectories tab.

A2. COMSOL Setup (Alex)
Table 4. Alex’s Comsol Table Including Laminar and Particle Tracing Physics Study:
Define the space
dimension
Start COMSOL Multiphysics. Model wizard>Select Space Dimension>2-D
axisymmetric>click on “next” arrow
Define the physics There are two physics studies performed in this module:
1. Time-Dependent Laminar Flow
2. Time -Dependent Particle Tracing for Fluid Flow
Define the study type Both physics studies are time-dependent.
Define the geometry The geometry was obtained by extracting a healthy and diseased
coronary artery using Mimics.
Define the material
type
The material of the fluid was blood. The density and dynamic viscosity
were 1060 kg/m^3 and 0.0032 Pa*s, respectively.
Physical Settings, initial
conditions
Laminar Flow Study
● The inlet pressure = 9,332.57 Pa (pressure of the blood inside the
coronary artery)
● outlet pressure = 9,332.57 Pa (pressure of the blood inside the
coronary artery)
● Inlet velocity = 0.029 m/s
Particle Tracing
● Drag law = stokes
● Inlet = 3000 particles released
Physical Settings
Boundary Conditions
● Wall condition for laminar flow study - no slip
● Wall condition for particle tracing - freeze
● Particle density = 2200 [Kg/m^3]
● Particle diameter = 5E-7 [m]
Mesh The mesh was created using 3 Matics program. The geometry of the
elements are triangles that were adjusted to make a finer mesh to get
more accurate result in the physics studies.
Study: Solve ● Laminar Flow Study - solving for velocities throughout model as a
function of time
● Particle Tracing - solving for particle displacements and velocities
throughout model as a function of time. This study uses results from
the laminar flow study.
Compute Click study 1 --

A3. COMSOL Setup (Sarea)
Table 5. Table Including Laminar and Particle Tracing Physics Study:
Define the space
dimension
Start COMSOL Multiphysics. Model wizard>Select Space
Dimension>2-D axisymmetric>click on “next” arrow
Define the physics
Fluid flow → Single-Phase Flow → Laminar Flow (spf)
Define the study type
Preset studies → Time Dependent
Define the geometry N/A - models were imported through the mesh
Define the material
type
Materials → Right-click Materials → select Blank Materials
→ select “Density”,”Dynamic Viscosity” under Materials
Content section
Physical Settings,
initial conditions
Fluid flow simulation:
Initial values: Pressure = 11600 Pa
Particle-tracking simulation:
Physical Settings
Boundary Conditions
Fluid flow simulation:
Fluid properties: dynamic viscosity = 3.2E-3 Pa*s density =
1060 kg/m3
Wall condition: no slip
Normal inflow velocity: Vo = 0.029 m/s
Outlet: P0 = 11600 Pa with suppressed backflow
Particle-tracking simulation:

Mesh
Mesh 1 → Import 1
Performed for healthy and diseased models
Study: Solve Fluid flow simulation:
Study 1 → Study 1: Time Dependent
Particle flow simulation
Study 2 → Study 2: Time Dependent → de-select “Solve
for” check for Laminar flow under the Physics and Variable
Selection subsection
Compute
Fluid flow simulation:
Study 1 → Solver Configurations → Solution 1 → Time-
Dependent Solver 1 → study type should be “Direct 1”
Particle flow simulation:
Study 2 → Solver Configurations → Solution 2 → Time-
Dependent Solver 1 → study type will be “Iterative 1”
Results
Fluid flow simulation:
Results → Velocity spf→ Slice 1 → Add 20 slides
Particle flow simulation:
Results → Particle Trajectories (fpt)→ Particle Trajectories
1
Results → Export→ Animation 1