mlab 2401: clinical chemistry keri brophy-martinez pathophysiology of renal function
TRANSCRIPT

MLAB 2401: Clinical MLAB 2401: Clinical ChemistryChemistryKeri Brophy-MartinezKeri Brophy-Martinez
Pathophysiology of Renal Function

Glomerular DiseasesGlomerular DiseasesAssociated with damage to the
glomeruli of the nephronLead to tubular dysfunctionCan be acute or chronic

Acute Glomerulonephritis Acute Glomerulonephritis (AGN)(AGN)Characterized by rapid onset of
symptoms that indicate damage to the glomeruli.
Population affected includes children and young adults

Acute Glomerulonephritis Acute Glomerulonephritis (AGN)(AGN)Causes of:
◦AGN often follows a group A streptococcal infection Circulating immune complexes trigger an
inflammatory response in the glomerular basement membrane
◦Toxin/Drug-related exposures◦Acute kidney infections◦Systemic diseases

Acute Glomerulonephritis Acute Glomerulonephritis (AGN)(AGN)• Symptoms–Hematuria– Proteinuria–Oliguria– Fever–Malaise– Rapid Onset– Edema–Hypertension– Sodium & water
retention
• Laboratory Findings–Decreased GFR– Increased BUN &
creatinine–Hyaline, granular,
RBC casts– Increased protein
in urine– Blood in urine

Chronic Glomerulonephritis Chronic Glomerulonephritis (CGN)(CGN)Associated with the end stage of
persistent glomerular damageIrreversible loss of renal tissue Can result in renal failureSymptoms of CGN include:
◦ edema, fatigue, hypertension, metabolic acidosis, proteinuria, decreased urine volume
Nephrotic SyndromeNephrotic SyndromeCauses of:
◦Complications of glomerulonephritis ◦Circulatory disorders affecting
kidneys
Hallmark◦Increased permeability of glomerular
basement membrane Allows for proteins & lipids to enter GFR
Nephrotic SyndromeNephrotic SyndromeSymptoms:
◦Massive proteinuria (>3 g/day)◦Albuminuria (>1.5 g/day)◦Pitting edema◦Hyperlipidemia◦Hypoalbuminemia◦Lipiduria: oval fat bodies

Urinary Tract InfectionUrinary Tract Infection• Causes of:–Pyelonephritis (kidneys)• Acute: no permanent damage• Chronic: permanent damage, possible
renal failure–Cystitis (bladder)
• Lab Findings–Positive nitrite on dipstick–Hematuria–Pyuria–WBC casts
ObstructionsObstructionsCauses of:
◦Renal calculi Calcium oxalate most common
◦Tumors◦Urethral strictures
Leads to chronic renal failure

Renal FailureRenal FailureAcute
◦Sudden decline in renal function◦GFR < 10 mL/minute◦Caused by nephrotoxic agents,
necrosis, hemorrhaging Hemolytic transfusions reactions Burns Cardiac failure Antifreeze ingestions

Renal Failure: Chronic Renal Failure: Chronic (CKD)(CKD)
Chronic◦ Gradual decline in function◦ Associated with hypertension and diabetes◦ Risk factors
Autoimmune diseases Urinary tract and systemic infections Some medicationsoComplications from CKD• Anemia• Hyperparathyroidism• Vitamin D deficiency/insufficiency• Mineral and bone disorders
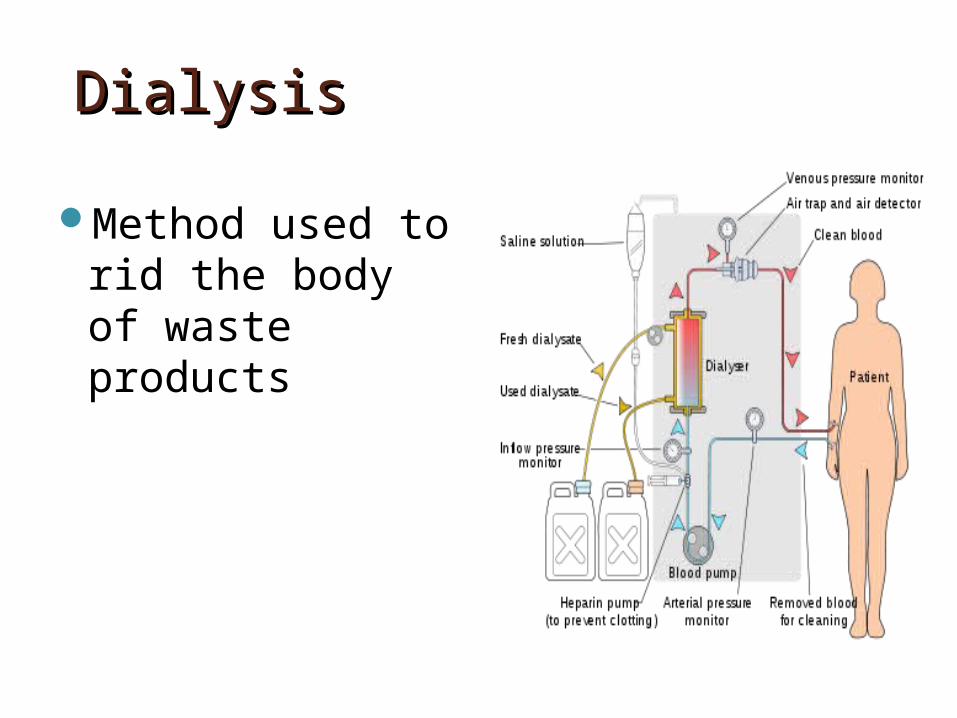
DialysisDialysis
Method used to rid the body of waste products

ReferencesReferences Bishop, M., Fody, E., & Schoeff, l. (2010). Clinical
Chemistry: Techniques, principles, Correlations. Baltimore: Wolters Kluwer Lippincott Williams & Wilkins.
Sunheimer, R., & Graves, L. (2010). Clinical Laboratory Chemistry. Upper Saddle River: Pearson.
Vassalotti, MD, J. A., & Kaufman, MD, H. W. (2013, July). New Guidelines to Evaluate and manage Chronic Kidney Disease. MLO, 24-26.
14