minocycline pigmentation 2
DESCRIPTION
oral pigmentationTRANSCRIPT

Minocycline-Induced PigmentationIncidence, Prevention and Management
Drore Eisen1 and Miriam D. Hakim2
1 Dermatology Research Associates of Cincinnati, Cincinnati, Ohio, USA2 University of Cincinnati Medical Center, Cincinnati, Ohio, USA
ContentsSummary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4311. Tetracyclines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 432
1.1 Minocycline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4321.2 Pigmentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 432
2. Minocycline-Induced Pigmentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4332.1 Skin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4332.2 Nails . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4342.3 Oral Cavity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4352.4 Thyroid and Other Viscera . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4362.5 Breastmilk . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4372.6 Skeleton and Cartilage . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4372.7 Ocular . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 437
3. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 437
Summary Pigmentation is a well recognised adverse effect of minocycline therapy. Var-ious body sites, most notably the skin, nails, bones, thyroid, mouth and eyes areaffected and the pigmentation may appear at multiple sites. In general, pigmen-tation results from long term administration of minocycline at cumulative dosesgreater than 100g, although cutaneous or oral mucosal pigmentation may appear,regardless of dose or duration of therapy. When the skin is involved, the blue-black pigmentation develops most frequently on the shins, ankles and arms. Otherpatterns of skin involvement include pigmentation that is either generalised andsymmetrical, or that develops at sites of inflammation. The bones of the oralcavity are probably the most frequently affected sites of pigmentation affectinggreater than 20% of patients taking minocycline for more than 4 years. In contrast,the oral mucous membranes and teeth are infrquently pigmented from minocyc-line. Ocular, thyroid and visceral pigmentation is also relatively uncommon andusually develops only with high doses and long term minocycline use. Whereaspigmentation of the skin and oral mucosa is generally reversible when the drugis discontinued, the pigmentation is often permanent when other sites are in-volved. Although minocycline-induced pigmentation is not harmful, the drugshould be discontinued when the adverse effect is recognised. All patients receiv-ing minocycline, especially those treated for longer than 1 year, require screeningfor the development of pigmentation.
PHARMACOEPIDEMIOLOGY Drug Safety 1998 Jun; 18 (6): 431-4400114-5916/98/0006-0431/$05.00/0
© Adis International Limited. All rights reserved.

1. Tetracyclines
The tetracyclines, antibacterials with antimicro-bial, anti-inflammatory and immunosuppressiveproperties, are widely employed for the treatmentof acne, rosacea and a variety of other dermatolog-ical conditions.[1] Although once considered theantibacterials of choice for selected Gram-positiveand Gram-negative infections, their broad antimi-crobial spectrum make them valuable for the treat-ment of many infections such as atypical pneumo-nias, sexually transmitted diseases, traveller’sdiarrhoea, rickettsial infections, periodontal dis-ease and methicillin-resistant Staphylococcus au-reus (MRSA) colonisation.[2] In addition, a double-blind study has confirmed efficacy in rheumatoidarthritis.[3]
1.1 Minocycline
Minocycline is a semi-synthetic broad-spectrumtetracycline antimicrobial agent that was intro-duced in 1967. It is a popular member of the tetra-cycline class because of several advantages thedrug has compared with other tetracyclines. Inaddition to achieving peak serum concentrationswithin several hours after administration, it is wellabsorbed and possesses greater antimicrobial ac-tivity than other tetracyclines.[4] Also, orally ad-ministered minocycline hydrochloride is highlybound to plasma proteins and is lipid soluble, thusfacilitating penetration into body fluids (such assaliva, bile and breastmilk) and tissues (includingthe skin, brain, thyroid, fat and liver).[4,5] Bacterialresistance to minocycline is minimised by the highliphophilicity of the drug. Minocycline resistanceis mediated through chromosomally located Tetgenes, and occurs less frequently than resistance totetracycline which is mediated through Tet geneswithin a plasmid locus.[6]
1.2 Pigmentation
Pigmentation is a well recognised adverse reac-tion associated with all tetracyclines, with the ex-ception of doxycycline. For example, methacycline,a tetracycline used infrequently in the treatment of
acne, may, with prolonged administration, result ingrey-black pigmentation of nails, conjunctiva andsun-exposed skin.[7,8] Tetracycline hydrochloridehas also been reported to cause pigmentation ofteeth and nails[9,10] and osteoma cutis.[11]
However, of all of the tetracyclines, minocycl-ine is most often associated with the adverse effectof pigmentation, potentially affecting various or-gans and body fluids (table I). Although minocyc-line is a yellow crystalline material, its black deg-radation product may be deposited in varioustissues.[12] The accumulation of high concentra-tions of minocycline at various sites may, in part,explain the pigmentation that results with its use.
Although the safety of long term high-dosage(200 mg/day) minocycline for the treatment ofacne has recently been demonstrated, cutaneouspigmentation was the most frequently observed ad-verse reaction.[13] Failure to recognise this rela-tively common cause of pigmentation of the skinand other body sites may lead to unnecessary test-
Table I. Minocycline-induced pigmentation: sites of involvement(after Dummett and Barens,[44] with permission)
CutaneousSkin
Nails
Oral cavityTeeth
Mucous membranes
Alveolar bone and hard palate
OcularSclerae
Conjunctiva
Skeleton and cartilageVertebrae
Costal cartilage
Parietal bone
Alae nasi
Viscera and body fluidsThyroid
Substantia nigra
Aortic and mitral valves
Atherosclerotic plaques
Breastmilk
432 Eisen & Hakim
Adis International Limited. All rights reserved. Drug Safety 1998 Jun; 18 (6)

ing and confusion with other causes of pigmenta-tion.
2. Minocycline-Induced Pigmentation
As mentioned in section 1.2, minocycline canbe associated with the development of pigmenta-tion in a number of body areas.
2.1 Skin
2.1.1 Types of PigmentationMinocycline-induced pigmentation of the skin
is readily identifiable and 3 patterns of involve-ment have been well described (type I, type II andtype III).
Type IType I cutaneous pigmentation is characterised
by blue-black macules that are localised to sites ofscarring or inflammation.[14] Although the pigmen-tation appears predominantly on the face withinacne scars (fig. 1), it has also been reported at othersites of inflammation on the chest and legs. Thisdistribution was emphasised by Fleming et al.[15]
who described a patient with lepromatous leprosywho developed multiple blue-black lesions at var-ious sites of inflammation.
Pigmentation from minocycline followingsclerotherapy has also been reported, highlightingthe localisation of type I pigment to sites of inflam-mation.[16] Additionally, minocycline, like tetracy-cline, may cause pigmentation of post-acne oste-oma cutis.[17] These osteomas, which representmetaplastic bone formation, are rare complicationsof chronic acne and typically develop on the face.
Microscopically, pigment granules in type I pig-mentation, free within macrophages, have beenidentified in the dermis and consist of minocyclineor a minocycline degradation product chelatedwith haemosiderin, ferritin or iron.[14]
Type IIType II cutaneous pigmentation appears as
blue-black, brown or slate-grey pigmentation anddevelops on healthy skin, primarily the skin of theshins, ankles and arms (fig. 2). The staining mayappear to be either well circumscribed or diffuse.
The pigment is found in the dermis and subcu-tis, often in macrophages, where it may be mem-brane bound or freely scattered among dermal col-lagen fibres.[18] Although microanalysis hasrevealed the presence of sulphur, chlorine and cal-cium, the cutaneous pigment is thought to consistof insoluble complexes of minocycline or a mino-cycline oxidation product chelated to iron.[19-21]
Type IIIType III cutaneous pigmentation appears as
muddy-brown in hue and develops on healthy skinin a generalised and symmetrical pattern, accentu-ated in sun exposed areas.[22] The pigmentresembles a persistent, deep brown tan and mayresult from increased melanisation of the basal celllayer. Melanin or a minocycline-melanin complexwithout iron may be demonstrated microscopicallyin the epidermis and papillary dermis.[22]
Additional TypesA fourth type of cutaneous pigmentation has
been proposed by Chu and Van,[23] who describeda patient taking minocycline who developed darkbrown macular pigmentation of the lips. Micro-scopically, post-inflammatory changes were con-sistent with a resolving fixed drug eruption. Ridg-way and Reizner[24] observed similar clinical andmicroscopic features in a patient taking minocycl-ine.
Pigmentation can also be classified according toits distribution as either: (i) local, corresponding to
Fig. 1. Minocycline–induced type I cutaneous pigmentation de-velops most commonly on the face within acne scars.
Minocycline-Induced Pigmentation 433
Adis International Limited. All rights reserved. Drug Safety 1998 Jun; 18 (6)

Pigmentation can also be classified according toits distribution as either: (i) local, corresponding totype I; or (ii) diffuse, which typifies types II andIII. Patients may display features of several typesat a given time, and cutaneous pigmentation mayalso be accompanied by pigmentation involvingother organs.
2.1.2 IncidenceThe incidence of pigmentation resulting from
minocycline appears to be related to several fac-tors. Whereas the duration of therapy and total cu-mulative dose do not influence the onset of type Ipigmentation, types II and III pigmentation de-velop predominantly in patients who are treated forprolonged periods with high dosages of thedrug.[25] This is evidenced by reports of type I pig-mentation developing after only a few weeks ofminocycline therapy.[15,16] In contrast, types II andIII pigmentation generally do not develop until pa-tients have received a cumulative dose of minocyc-line exceeding 70 to 100g.[26,27] The intensity of thepigmentation does not appear to correlate with thetotal dose of minocycline or the duration of treat-ment.
Patients treated for rosacea develop pigmenta-tion from minocycline more often than thosetreated for acne.[25] This may be related to the olderage of patients with rosacea, who demonstrategreater age-related solar elastosis and receivehigher cumulative doses of minocycline than pa-
tients with acne. In the study by Dwyer andCuddihy[25] of 54 patients treated with minocyclinefor a mean duration of 17 months for acne or rosa-cea, approximately 15% (8 patients) developedpigmentation. Six of the 8 identified patients weretreated for rosacea and the remaining 2 for acne.These figures are in agreement with others whohave reported an incidence of pigmentation of 3%in patients with acne who were treated with mino-cycline for prolonged periods.[28]
2.1.3 ManagementPatients undergoing therapy with minocycline
should be informed of the possible adverse effectof cutaneous pigmentation and should be appropri-ately screened for its development. This is espe-cially true for patients treated for extended periodsof time with cumulative doses greater than 100g.
Fortunately, both type I and II pigmentation isharmless, but it may be unsightly and darken sig-nificantly if the drug is not withdrawn. In almostall cases, the pigmentation resolves after the drugis stopped; however, several months may elapsebefore complete resolution is achieved. In contrast,the diffuse muddy brown pigmentation observedwith type III pigmentation may persist indefi-nitely,[25,29] although, based on paucity of reportsin the literature and our own observations, this typeis the most rare.
Successful treatment of minocycline-inducedpigmentation without scarring or hypopigmenta-tion has been reported with a Q-switched laser.[30]
Management of pigmented osteoma cutis involvessurgical removal of the epidermal nodules or theuse of tretinoin cream for dermal osteomas.
2.2 Nails
Nail pigmentation caused by minocycline is un-usual and far less common than skin involvement.Although a number of colour changes have beenreported, a slate-grey discoloration of the proximalnail bed appears to be the most frequent type (fig.3).[31] Even more rare are longitudinal melan-onychia, diffuse nail pigmentation and photo-onycholysis.[32,33]
Fig. 2. The ankle is a common location for the development oftype II cutaneous minocycline-associated staining.
434 Eisen & Hakim
Adis International Limited. All rights reserved. Drug Safety 1998 Jun; 18 (6)

Generally, nail pigmentation develops concom-itantly with other sites of involvement and it israrely an isolated finding. Stimulation of nail ma-trix melanocytes with increased melanin deposi-tion in the nail plate has been described as the causeof pigmentation in longitudinal melanonychia.[34]
This is similar to the mechanism in type III cuta-neous pigmentation.
Pigmentation of the nail may persist for pro-longed periods despite withdrawal of the drug. Therecognition of these changes may avoid unneces-sary biopsy.
2.3 Oral Cavity
Minocycline may cause pigmentation of theteeth, the oral mucosal surfaces and the underlyingbones of the oral cavity.
2.3.1 TeethAlthough the incidence of tooth discoloration in
the erupted permanent dentition has been reportedto be as high as 6% in 1 retrospective study,[35] ourown experience and that of others reveal a muchlower rate.[36] In fact, we have only observed thistype of pigmentation in a few cases after treatingseveral hundred patients with minocycline, andonly when therapy was administered for an ex-tended period of years. When present, the discol-oration is greyish-blue. Unlike staining caused bytetracycline, which primarily affects the proximalthird of the tooth, minocycline staining is most ev-
ident in the middle portion of the tooth and occa-sionally involves the lower incisal third. The bluepigmentation is generally permanent, unless it ap-pears shortly after the initiation of minocyclinetherapy and the drug is promptly withdrawn.[37]
Some have suggested that the pigmentation ofthe teeth may be caused by either demineralisationand etching of the enamel by minocycline resultingin a persistent extrinsic stain[38] or deposition ofminocycline in dentin which becomes visiblethrough the enamel.[39] Since the concentration ofsystemically administered minocycline in the gin-gival fluid is 5 times that of serum,[40] pigmenta-tion near the gingival margin would be expected.Additionally, after the teeth erupt, dentin forma-tion is greatly reduced. Thus, both theories are in-sufficient to explain why minocycline but not tet-racycline cause erupted teeth to discolour.
Staining of the roots of teeth has been well doc-umented.[41,42] Indeed, our oral surgeons have fre-quently observed this during extraction of thirdmolars (wisdom teeth) from patients with acnewho were treated with minocycline during root de-velopment.
2.3.2 Oral Mucosal SurfacesReports of minocycline-induced pigmentation
affecting the oral mucous membranes are equallyrare and have included the buccal mucosa, gingiva,lips and tongue.[36,43,44] Although minocycline is theonly tetracycline associated with oral mucosal pig-mentation, its cause remains unknown. It has beensuggested that either a minocycline-metabolitecomplex or melanin, iron and calcium-containinggranules are the source of the pigment.[41] We haveobserved that the oral pigmentation develops atsites predisposed to oral trauma such as the tongueand buccal mucosa. The pigmentation appears tobe unrelated to the duration of minocycline therapyor the cumulative dose, and resolves completelywhen the drug is discontinued. These features areidentical to those described for type I cutaneouspigmentation (see section 2.1.1).
2.3.3 Bones of the Oral CavityWithout question, almost all cases of intraoral
pigmentation represent minocycline staining of theFig. 3. Minocycline–induced slate-grey pigmentation of the prox-imal nail bed.
Minocycline-Induced Pigmentation 435
Adis International Limited. All rights reserved. Drug Safety 1998 Jun; 18 (6)
underlying bones without involvement of the over-lying oral mucosal surfaces. As we recently re-ported, the incidence of intraoral bone pigmenta-tion from minocycline, at dosages of 100 to 200mg/day, is 10% after 1 year of therapy.[45] The in-cidence increases to 20% in patients taking mino-cycline for 4 years.
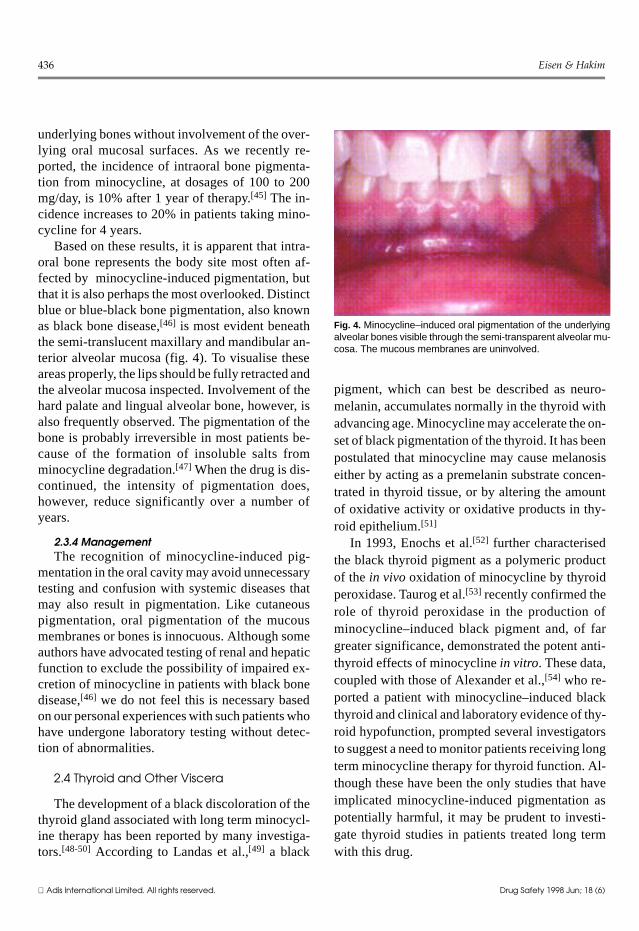
Based on these results, it is apparent that intra-oral bone represents the body site most often af-fected by minocycline-induced pigmentation, butthat it is also perhaps the most overlooked. Distinctblue or blue-black bone pigmentation, also knownas black bone disease,[46] is most evident beneaththe semi-translucent maxillary and mandibular an-terior alveolar mucosa (fig. 4). To visualise theseareas properly, the lips should be fully retracted andthe alveolar mucosa inspected. Involvement of thehard palate and lingual alveolar bone, however, isalso frequently observed. The pigmentation of thebone is probably irreversible in most patients be-cause of the formation of insoluble salts fromminocycline degradation.[47] When the drug is dis-continued, the intensity of pigmentation does,however, reduce significantly over a number ofyears.
2.3.4 ManagementThe recognition of minocycline-induced pig-
mentation in the oral cavity may avoid unnecessarytesting and confusion with systemic diseases thatmay also result in pigmentation. Like cutaneouspigmentation, oral pigmentation of the mucousmembranes or bones is innocuous. Although someauthors have advocated testing of renal and hepaticfunction to exclude the possibility of impaired ex-cretion of minocycline in patients with black bonedisease,[46] we do not feel this is necessary basedon our personal experiences with such patients whohave undergone laboratory testing without detec-tion of abnormalities.
2.4 Thyroid and Other Viscera
The development of a black discoloration of thethyroid gland associated with long term minocycl-ine therapy has been reported by many investiga-tors.[48-50] According to Landas et al.,[49] a black
pigment, which can best be described as neuro-melanin, accumulates normally in the thyroid withadvancing age. Minocycline may accelerate the on-set of black pigmentation of the thyroid. It has beenpostulated that minocycline may cause melanosiseither by acting as a premelanin substrate concen-trated in thyroid tissue, or by altering the amountof oxidative activity or oxidative products in thy-roid epithelium.[51]
In 1993, Enochs et al.[52] further characterisedthe black thyroid pigment as a polymeric productof the in vivo oxidation of minocycline by thyroidperoxidase. Taurog et al.[53] recently confirmed therole of thyroid peroxidase in the production ofminocycline–induced black pigment and, of fargreater significance, demonstrated the potent anti-thyroid effects of minocycline in vitro. These data,coupled with those of Alexander et al.,[54] who re-ported a patient with minocycline–induced blackthyroid and clinical and laboratory evidence of thy-roid hypofunction, prompted several investigatorsto suggest a need to monitor patients receiving longterm minocycline therapy for thyroid function. Al-though these have been the only studies that haveimplicated minocycline-induced pigmentation aspotentially harmful, it may be prudent to investi-gate thyroid studies in patients treated long termwith this drug.
Fig. 4. Minocycline–induced oral pigmentation of the underlyingalveolar bones visible through the semi-transparent alveolar mu-cosa. The mucous membranes are uninvolved.
436 Eisen & Hakim
Adis International Limited. All rights reserved. Drug Safety 1998 Jun; 18 (6)

In addition to the thyroid gland, minocycline-associated pigmentation has been reported in thesubstantia nigra and atherosclerotic plaques,[49] aswell as in aortic and mitral valves.[55] In all of thesecases, pigmentation was found incidentally, andadditional information regarding any harmful ef-fects of the pigmentation was not reported.
2.5 Breastmilk
Because of its lipophilic nature, minocycline ishighly soluble in body fluids and may be excretedin breastmilk. We know of only 2 cases that reportblack galactorrhoea in patients taking minocycl-ine.[56,57] The first patient developed galactorrhoeafrom phenothiazine, and after 4 years of takingminocycline 200 mg/day developed black breast-milk. The second patient, who had completedbreast feeding 18 months prior to her presentation,had been treated for only 4 weeks with minocycl-ine at a dosage of 150 mg/day before she notedsmall amounts of black milk. The milk of bothpatients demonstrated macrophages containingparticles that stained positive for iron. It was pos-tulated that the pigmentation consisted of an ironchelate of minocycline or one of its derivatives.[56]
2.6 Skeleton and Cartilage
Rumback et al.[58] reported a case of blackenedthoracic vertebrae discovered incidentally duringan elective neurosurgical procedure, without evi-dence of pigmentation elsewhere. The pigmenta-tion occurred in a woman who had a cumulativeingestion of minocycline of greater than 220g.Other patients who had been administered smallercumulative doses were noted to have pigmentedbones, usually in association with pigmentation ofthe skin and nails.[59]
Minocycline-staining involving other portionsof the skeleton, including costal cartilage, parietalbones and alae-nasi, were reported in a single pa-tient.[48] These findings occurred simultaneouslyafter treatment with minocycline 200 mg/day forover a year and were found concurrently with auniformly black thyroid.
The dark pigment in bone may represent a deg-radation product or a drug complex, and has beenshown to consist of a deposit containing iron andcalcium and resemble haemosiderin.[58,60]
The effect of minocycline on bone metabolismis unknown, although no adverse effects of mino-cycline on the structure or function of bone havebeen reported. Tetracycline is known to chelate cal-cium phosphate and bind loosely to polypeptidesin bone, but despite considerable accumulation ofthe drug in adult bone, no adverse consequenceshave been noted.[61] The metabolic effects of mino-cycline on bone require further investigation.
2.7 Ocular
Minocycline staining of the ocular structures in-cluding the conjunctiva and the sclera has been re-ported by several investigators.[18,62-64] Distinctpigmented changes involving the sclera include ablue-grey, 3 to 5mm band starting at the limbus,which is usually enhanced in the palpebral aper-ture.[65] Diffuse blue discoloration of the sclera hasalso been observed.[18] It has been noted that al-most all patients who report scleral pigmentationalso display pigmentation of the nails. Further-more, in addition to taking high dosages of mino-cycline for prolonged periods (exceeding 2 years),all patients exhibited type III, diffuse muddy-brown cutaneous pigmentation.
Subconjunctival, densely pigmented spots lo-cated on the inferior tarsal plate, hypothesised tobe conjunctival cysts, have also been noted in pa-tients taking minocycline.[18,66] These pigmentedabnormalities have been reported in both the pres-ence and absence of skin changes.
Pigmentation involving the ocular structuresmay resolve within years or it may persist indefi-nitely. Fortunately, no harmful effects of the pig-mentation have been reported.
3. Conclusion
Minocycline has been demonstrated to causedark pigmentation of various body sites, mostprominently the skin, nails, bones, thyroid and
Minocycline-Induced Pigmentation 437
Adis International Limited. All rights reserved. Drug Safety 1998 Jun; 18 (6)

eyes. Table II provides an overview of this adverseeffect.
In general, with the exceptions of type I cutane-ous pigmentation and intraoral mucous membranepigmentation which develop independent of doseor duration of therapy, all other minocycline-induced pigmentations develop after long term ad-ministration of the drug and high cumulative doses.Multiple sites of pigmentation are frequently de-tected. Since almost all cases of pigmentation de-velop in patients with acne and rosacea who havebeen treated long term, minimising the cumulativedose of minocycline by discontinuing the drug af-ter 6 months will avoid this common adverse ef-fect.
The pigmentation may lead to confusion if notproperly recognised and may result in unnecessarytesting to exclude other causes of pigmentation. Allpatients receiving minocycline therapy should becarefully screened for the development of pigmen-tation. In addition to a twice yearly examination ofthe skin, nails, eyes and oral cavity, some authorsadvocate thyroid function testing for those patientstreated with minocycline for longer than 1 year, orfor those receiving cumulative doses of greaterthan 100g. Additional research on the effects ofminocycline on thyroid function is required beforeroutine testing can be recommended.
Once pigmentation has been identified, the drugshould be promptly discontinued and substitutedwith an alternative antibacterial. Pigmentation ofthe skin usually resolves within months or years,although pigmentation of other body sites is morelikely to be permanent.
With proper monitoring, minocycline remainsan invaluable drug for the treatment of acne and avariety of other conditions.
References1. Humbert P, Treffel P. The tetracyclines in dermatology. J Am
Acad Dermatol 1991; 25: 691-72. Klein NC, Cunha BA. Tetracyclines. Med Clin North Am 1995;
79: 789-8013. O’Dell JR, Haire CE, Palmer W, et al. Treatment of early rheu-
matoid arthritis with minocycline or placebo: results of a dou-ble-blind, placebo-controlled trial. Arthritis Rheum 1997; 40:842-8
4. Saivin S, Houin G. Clinical pharmacokinetics of doxycyclineand minocycline. Clin Pharmacokinet 1988; 15: 355-66
5. Siller G, Marcus A. Minocycline-induced oral pigmentation. JAm Acad Dermatol 1994; 30: 350-4
6. Eady EA, Cove JH, Holland KT, et al. Superior antibacterialaction and reduced incidence of bacterial resistance in mino-cycline compared to tetracycline-treated acne patients. Br JDermatol 1990; 122: 233-44
7. Dysler-Aas K, Hansson H, Miorner G, et al. Pigment depositsin eyes and light-exposed skin during long-term methacyclinetherapy. Acta Derm Venereol 1974; 54: 209-22
8. Moller H, Rausing A. Methacycline hyerpigmentation: a five-year follow-up. Acta Derm Venereol 1980; 60: 495-501
9. Wallman IS, Hilton HB. Teeth pigmented by tetracycline. Lan-cet 1962; I: 112
10. Hendricks A. Yellow lunulae with flourescence after tetracy-cline therapy. Arch Dermatol 1980; 116: 438-40
Table II. An overview of minocycline-induced pigmentation
Organ involvement Clinical features of pigmentation Effects of dose and duration of drug therapy
Skin
type I At sites of inflammation on face, chest and legs Does not influence onset
type II On healthy skin of shins, ankles and arms Cumulative dose >70-100g
type III Generalised, symmetrical on sun-exposed areas Cumulative dose >70-100g
Nails Slate-grey discoloration of the proximal nail bed Usually with prolonged therapy
Oral cavity
teeth Middle of tooth, occasionally the incisal third After years of therapy
mucous membranes Sites predisposed to trauma, e.g. tongue and buccal mucosa Does not influence onset
alveolar bone Beneath the semitranslucent maxillary and mandibularalveolar mucosa, and hard palate
Evident after 1 year of therapy; incidenceincreases with prolonged therapy
Thyroid Black discoloration of the thyroid gland Usually after long term therapy
Skeleton/cartilage Thoracic vertebrae, costal cartilage, parietal bones andalae-nasi
Usually after long term therapy
Ocular Blue-grey scleral pigmentation and subconjunctivalpigmented spots
After high doses for extended periods
438 Eisen & Hakim
Adis International Limited. All rights reserved. Drug Safety 1998 Jun; 18 (6)

11. Walter JF, Macknet KD. Pigmentation of osteoma cutis causedby tetracycline. Arch Dermatol 1979; 115: 1087-8
12. Hendrix J, Greer K. Cutaneous hyperpigmentation caused bysystemic drugs. Int J Dermatol 1992; 3: 458-66
13. Goulden V, Glass D, Cunliffe WJ. Safety of long-term high-dose minocycline in the treatment of acne. Br J Dermatol1996; 134: 693-5
14. Fenske N, Millns J, Greer K. Minocycline-induced pigmenta-tion at sites of cutaneous inflammation. JAMA 1980; 244:1103-6
15. Fleming C, Hunt M, Salisbury ELC, et al. Minocycline-in-duced hyperpigmentation in leprosy. Br J Dermatol 1996;134: 784-7
16. Leffell DJ. Minocycline hydrochloride hyperpigmentationcomplicating treatment of venous ectasia of the extremities.J Am Acad Dermatol 1991; 24: 501-2
17. Moritz D, Elewski B. Pigmented postacne osteoma cutis in apatient treated with minocycline: report and review of theliterature. J Am Acad Dermatol 1991; 24: 851-3
18. Sabroe R, Archer C, Harlow D. Minocycline-induced dis-colouration of the sclerae. Br J Dermatol 1996; 135: 314-6
19. Argenyi Z, Finelli L. Minocycline-related cutaneous hyper-pigmentation as demonstrated by light microscopy, electronmicroscopy and x-ray energy spectroscopy. J Cutan Pathol1987; 14: 176-80
20. Okada N, Sato S, Sasou T. Characterization of pigmented gran-ules in minocycline-induced cutaneous pigmentation: obser-vations using flourescent microscopy and high-performancechromatography. Br J Dermatol 1993; 129: 403-7
21. Gordon C, Sparano B, Iatropoulos M. Hyperpigmentation ofskin associated with minocycline therapy. Arch Dermatol1985; 121: 618-23
22. Simons J, Morales A. Minocycline and general cutaneous pig-mentation. J Am Acad Dermatol 1980; 3: 244-7
23. Chu P, Van S. Minocycline hyperpigmentation localized to thelips: an unusual fixed drug reaction? J Am Acad Dermatol1994; 30 (5): 802-3
24. Ridgway H, Reizner GT. Acquired pseudo-mongolian spot as-sociated with minocycline therapy. Arch Dermatol 1992; 128:565-6
25. Dwyer CM, Cuddihy AM. Skin pigmentation due to minocyc-line treatment of facial dermatoses. Br J Dermatol 1993; 129:158-62
26. Layton A, Cunliffe W. Minocycline-induced pigmentation inthe treatment of acne: a review and personal observations. JDermatol Treatment 1989; 1: 9-12
27. Hutchinson S, Burrows DJ. Minocycline-induced pigmenta-tion. Br J Dermatol 1992; 127: 47-8
28. Layton AM, Cunliffe WJ. Minocycline induced pigmentationin the treatment of acne – a review and personal observations.J Dermatol Treat 1989; 1: 9-12
29. Eedy D, Burrows P. Minocycline-induced pigmentation occur-ring in two sisters. Clin Exp Derm 1991; 16: 55-7
30. Collins P, Cotterill J. Minocycline-induced pigmentation re-solves after treatment with the Q-switched ruby laser. Br JDermatol 1996; 136: 317-9
31. Liu TT, May N. Pigmentary changes due to long term minocyc-line therapy. Cutis 1985; 35: 254-5
32. Daniel C, Scher R. Nail changes caused by systemic drugs oringestants. Dermatol Clin 1985; 3: 491-500
33. Kestel J. Photo-onycholysis from minocycline: side-effects ofminocycline therapy. Cutis 1981; 28: 53-4
34. Mallon E, Dawber R. Longitudinal melanonychia induced byminocycline. Br J Dermatol 1994; 130: 794-801
35. Poliak SC, DiGiovanna JJ, Gross EG. Minocycline-associatedtooth discoloration in young adults. JAMA 1985; 254: 2930-2
36. Berger R, Mandel E, Hayes T. Minocycline staining of the oralcavity. J Am Acad Dermatol 1989; 21: 1300-1
37. Rosen T, Hoffmann T. Minocycline-induced discoloration ofthe permanent teeth. J Am Acad Dermatol 1989; 21: 569
38. Salman R, Salman D, Glickman R. Minocycline-induced pig-mentation of the oral cavity. J Oral Med 1985; 40: 154-7
39. Westbury LE, Najera A. Minocycline-induced intraoral phar-macogenic pigmentation: case reports and review of the lit-erature. J Periodontol 1997; 68: 84-91
40. Ciancio S, Mather M, McMullen J. An evaluation of minocyc-line in patients with periodontal disease. J Periodontol 1982;51: 530-4
41. Siller GM, Tod MA, Savage NW. Minocycline-induced oralpigmentation. J Am Acad Dermatol 1994; 30: 350-4
42. Cohen BD, Abrams BL. An unusual case of stained roots ofunerupted third molars. Gen Dent 1989; 37: 342-3
43. Meyerson M, Cohen P, Hymes S. Lingual hyperpigmentationassociated with minocycline therapy. Oral Surg Oral MedOral Pathol 1995; 79: 180-4
44. Dummett C, Barens G. Pigmentation of the oral tissues: a re-view of the literature. J Periodontol 1967; 38: 360-78
45. Eisen D. Minocycline-induced oral hyperpigmentation. Lancet1997; 349 (9049): 400
46. Odell E, Hodgson R, Haskell R. Oral presentation of minocyc-line-induced black bone disease. Oral Surg Oral Med OralPathol 1995; 79: 459-61
47. Kelly R, Kanegis L. Metabolism and tissue distribution of ra-dioisotopically labelled minocycline. Toxicol Appl Phar-macol 1967; 11: 171-83
48. Atwood HD, Dennett X. A black thyroid and minocycline treat-ment. BMJ 1976; 2: 1109-10
49. Landes S, Schelper R, Fermin T, et al. Black thyroid syndrome:exaggeration of a normal process? Am J Clin Pathol 1986; 85:411-8
50. Folson D, Gauderer M, Dahms W. Nodular hyperplasia, blackthyroid and chronic minocycline ingestion in a teenager. ArchSurg 1992; 127: 1476-7
51. Benitz KF, Roberts G, Vusa A. Morphologic effects of mino-cycline in lab animals. Toxicol Appl Pharm 1967; 11: 150-70
52. Enochs W, Nilges M, Swartz H. The minocycline-induced thy-roid pigmentation and several synthetic models: identifica-tion and characterization by electron paramagnetic resonancespectroscopy. J Pharm Exp Ther 1993: 266: 1164-76
53. Taurog A, Dorris M, Doerge D. Minocycline and the thyroid:anti-thyroid effects of the drug and the role of thyroid perox-idase in minocycline-induced black pigmentation of thegland. Thyroid 1996; 6 (3): 211-9
54. Alexander CB, Herrara GA, Jaffe K, et al. Black thyroid: clin-ical manifestations, ultrastructural findings, and possiblemechanisms. Hum Pathol 1985; 16: 72-8
55. Butler J, Marks R, Sutherland R. Cutaneous and cardiac valvu-lar pigmentation with minocycline. Clin Exp Dermatol 1985;10: 432-7
Minocycline-Induced Pigmentation 439
Adis International Limited. All rights reserved. Drug Safety 1998 Jun; 18 (6)

56. Hunt M, Salisbury E, Grace J, et al. Black breast milk due tominocycline therapy. Br J Dermatol 1996; 134: 943-4
57. Basler RSW, Lynch PJ. Black galactorrhea as a consequence ofminocycline and phenothiazine therapy. Arch Dermatol 1988;121: 417-8
58. Rumback M, Pitcock JA, Palmieri GMA, et al. Black bonesfollowing long-term minocycline treatment. Arch Pathol LabMed 1991; 115: 939-41
59. Wolfe I, Reichmister J. Minocycline hyperpigmentation: skin,tooth, nail and bone involvement. Cutis 1984; 33: 457-8
60. Basler R. Minocycline-related hyperpigmentation. ArchDermatol 1985; 121: 606-8
61. Okland S, Prolo DJ. The significance of yellow bone. JAMA1981; 246: 761-3
62. Angeloni V, Salasche S, Ortiz R. Nail, skin, and scleral pigmen-tation induced by minocycline. Cutis 1987; 40: 229-33
63. Messmer E, Font R, Sheldon G, et al. Pigmented conjunctivalcysts following tetracycline/minocycline therapy. Ophthal-mology 1983; 90: 1462-8
64. Morrow GL, Abbott RL. Minocycline-induced scleral, dental,and dermal pigmentation. Am J Ophthalmol 1998; 125: 396-7
65. Fraunfelder FT, Randall JA. Minocycline-induced scleral pig-mentation. Ophthalmology 1997; 104: 936-8
66. Brothers D, Hidayat A. Conjunctival pigmentation associatedwith tetracycline medication. Ophthalmology 1981; 88:1212-5
Correspondence and reprints: Dr Drore Eisen, DermatologyResearch Associates of Cincinnati, 7691 Five Mile Road,Cincinnati, OH 45230, USA.
440 Eisen & Hakim
Adis International Limited. All rights reserved. Drug Safety 1998 Jun; 18 (6)