mild cognitive impairment in patients with carotid disease irena martinic popovic 1, m.d, arijana...
TRANSCRIPT
MILD COGNITIVE IMPAIRMENT MILD COGNITIVE IMPAIRMENT IN PATIENTS WITH CAROTID IN PATIENTS WITH CAROTID
DISEASEDISEASEIrena Martinic Popovic1, M.D, Arijana Lovrencic-Huzjan1, M.D, Ph. D,
Ana-Maria Simundic2, Ph.D, Vida Demarin1, M.D, Ph.DUniversity Department of Neurology1 and Clinical Institute of Chemistry2,
“Sestre milosrdnice” University Hospital Center Zagreb, Croatia
1Referal Centre for Neurovascular Disorders of Croatian Ministry of HealthReferal Centre for Neurovascular Disorders of Croatian Ministry of Health1Referal Centre for Headaches of Croatian Ministry of HealthReferal Centre for Headaches of Croatian Ministry of Health

Conflict of Interest DisclosureConflict of Interest Disclosure
Irena Martinic PopovicIrena Martinic Popovic, , M.D.M.D.Arijana Lovrencic-Huzjan, M.D, Ph.DArijana Lovrencic-Huzjan, M.D, Ph.D
Ana-Maria Simundic, Ph.DAna-Maria Simundic, Ph.DVida Demarin, M.D, Ph.DVida Demarin, M.D, Ph.D
Have no real or apparent conflicts of interest
to report.

CAROTID DISEASECAROTID DISEASE
• Risk factor for TIA/stroke
• Each 10% increase in the degree of CS 26% increase in risk of TIA/stroke
• “Severe carotid disease” advanced stenosis (>70%) and /or occlusion of the internal carotid artery (ICA) – ICA s/o
• Associated with silent cerebral infarctions

• Narrowing or occlusion of carotid arteries (ICA)• State of increased risk for cerebrovascular incident• Increased risk for cognitive decline
ASYMPTOMATIC CAROTID DISEASEASYMPTOMATIC CAROTID DISEASE

ASYMPTOMATIC ASYMPTOMATIC CAROTID DISEASE & VASCULAR RISKCAROTID DISEASE & VASCULAR RISK
• associated with multiple VRFs (arterial hypertension, diabetes, hyperlipoproteinaemia, increased body-mass index (BMI) and cigarette smoking)
• VRFs the risk for atherosclerotic disease and for brain injury
• VRFs detrimental effects on cognitive abilities

CVINCIDENT
(STROKE/TIA)
CAROTID DISEASE
VASCULAR RISK FACTORS
COGNITIVE FUNCTIONING

THE AIMS OF THE STUDYTHE AIMS OF THE STUDY
Besides standard MMSE, we used MoCA to investigate the association of ICA s/a and cognition in asymptomatic ICA s/o
Assessment of predicitive value of ICA s/o and vascular risk factors with respect to performance on cognitive domains (covered by MoCA)

• Clinical history
• Data on vascular risk factors
• Brain CAT scan (patients)
• Color Doppler Flow Imaging (CDFI) of carotid arteries
• Cognitive testing (MMSE and MoCA)
STUDY PROTOCOLSTUDY PROTOCOL

Variable PATIENTS(n=70)
CONTROLS(n=70)
p
Age/years (median, min-max) 67.5 (43 -85) 67.0 (42-82) 0.675**
Females (proportion, n) 0.37 (26) 0.44 (31) 0.640
Education/years (mean, SD) 11.58 (2.45) 11.78 (3.24) 0.681
Hypertension (proportion, n) 0.83 (58) 0.81 (57) 0.959
Diabetes (proportion, n) 0.26 (18) 0.29 (20) 0.867
Hyperlipidaemia (proportion, n) 0.74 (52) 0.41 (29) 0.009*
Coronary disease (proportion, n) 0.39(27) 0.27 (19) 0.356
Current smoking (proportion, n) 0.23 (16) 0.29 (20) 0.995
Ex-smoking (proportion, n) 0.31 (22) 0.19 (13) 0.238
Obesity (proportion, n) 0.23 (16) 0.19 (13) 0.792
DEMOGRAPHIC & VASCULAR RISK DATADEMOGRAPHIC & VASCULAR RISK DATA
* sign. difference (z-test)
** t-test

INCLUSION CRITERIA• PATIENTS:
• Asymptomatic (stroke/TIA free) patients; right-handed
• CAT scan normal• Diagnosed with severe ICA
stenosis (>70%) or with ICA occlusion
• CONTROLS
• Asymptomatic (stroke/TIA free) patients; right-handed
• Without severe ICA stenosis (>70%) or with ICA occlusion
EXCLUSION CRITERIA
• BOTH PATIENTS AND CONTROLS:
• A history or presence of stroke/TIA
• Dementia (DSM-IV) • Depressive disorder (DSM-IV) • Inability to perform the
cognitive testing
CRITERIA FOR THE STUDYCRITERIA FOR THE STUDY
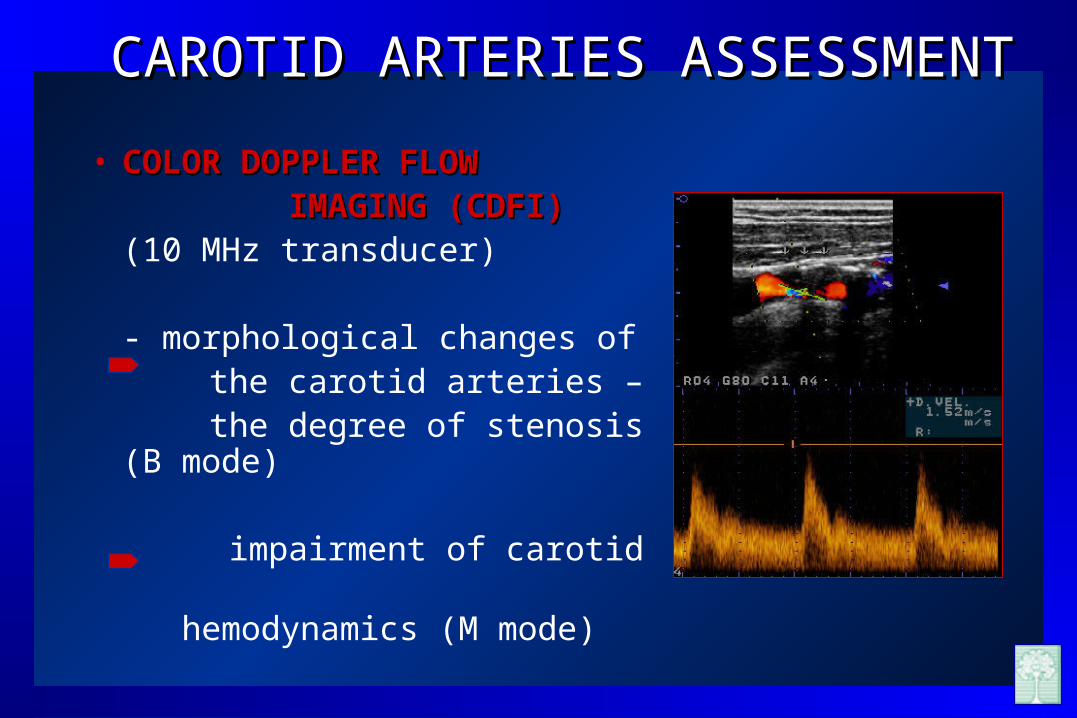
CAROTID ARTERIES ASSESSMENTCAROTID ARTERIES ASSESSMENT
• COLOR DOPPLER FLOW COLOR DOPPLER FLOW IMAGING (CDFI)IMAGING (CDFI)
(10 MHz transducer)
- morphological changes of the carotid arteries – the degree of stenosis (B mode)
impairment of carotid hemodynamics (M mode)

Proportion (n)PATIENTS
Left ICA advanced stenosis 0.38 (27)
Right ICA advanced stenosis 0.4 (28)
Billateral ICA advanced stenosis 0.04 (3)
Left ICA occlusion 0.03 (2)
Right ICA occlusion 0.07 (5)
Billateral ICA occlusion 0.03 (2)
Left ICA occlusion and right ICA advanced stenosis
0.03 (2)
Right ICA occlusion and left ICA advanced stenosis
0.01 (1)
CAROTID PATHOLOGY: CAROTID PATHOLOGY: THE SIDE & THE DEGREE OF STENOSIS THE SIDE & THE DEGREE OF STENOSIS
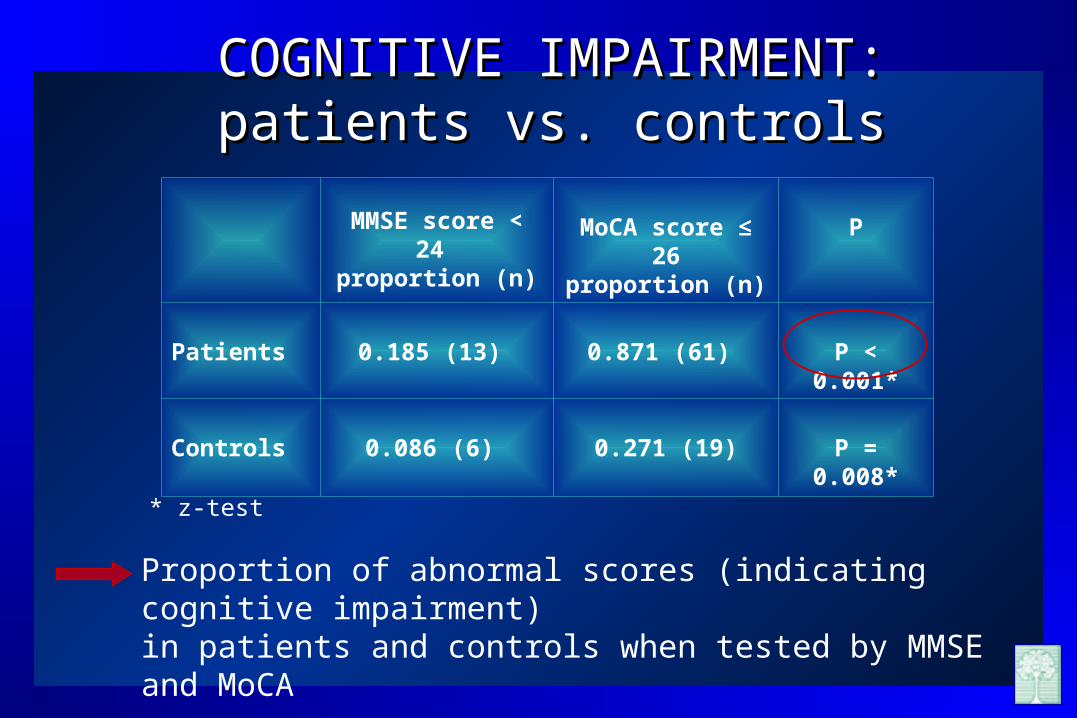
MMSE score < 24 proportion (n)
MoCA score ≤ 26proportion (n)
P
Patients 0.185 (13) 0.871 (61) P < 0.001*
Controls 0.086 (6) 0.271 (19) P = 0.008*
Proportion of abnormal scores (indicating cognitive impairment) in patients and controls when tested by MMSE and MoCA
* z-test
COGNITIVE IMPAIRMENT:COGNITIVE IMPAIRMENT:patients vs. controlspatients vs. controls

PATIENTS(n=70)
CONTROLS (n=70)
pMedian Q1 Q3 Median Q1 Q3
MoCA(total score)
23 20 25 24.5 23 26 <0.001**
MMSE 27.5 25 29 27 26 28 0.575
Patients and controls did not differ significantly in MMSE scores.
Median total MoCA scores were significantly lower in patients.
TOTAL COGNITIVE TESTING SCORES: TOTAL COGNITIVE TESTING SCORES: patients vs. controlspatients vs. controls

MoCA
subtests
scores
PATIENTS
(n=70)
CONTROLS
(n=70)
PMedian Q1 Q3 Median Q1 Q3
VSE* 3 2 4 4 3 5 0.018**
Naming 3 3 3 3 3 3 0.662
Attention 5 4 6 5 4 6 0.723
Language 2 2 3 2 2 3 0.204
Abstraction 1 1 1 2 1 2 <0.001**
Delayed recall 2 0 3 3 2 4 <0.001**
Orientation 6 6 6 6 6 6 0.451
MoCA SUBTESTS SCORES: MoCA SUBTESTS SCORES: patients vs. controlspatients vs. controls

Parameter Univariate regressionanalysis
Multivariate regressionanalysis
OR (95% CI) P OR (95% CI) P
Age 0.87 (0.794 - 0.955) 0.0034 0.86 (0.780 - 0.956)
6.41 (1.277 - 32.220)
0.004
0.024
Gender 1.85 (0.482 - 7.152) 0.3682
Hypertension 0.80 (0.147 - 4.343) 0.7960
Diabetes 6.00 (1.458 - 24.687) 0.0130
Hyperlipidemia 3.56 (0.418 - 30.271) 0.2453
Coronary disease
1.73 (0.449 - 6.638) 0.4262
Smoking 1.26 (0.552 - 2.879 0.5824
Obesity 0.95 (0.672 - 1.352) 0.7907
Left ICA s/o 1.18 (0.415 - 3.339) 0.7582
Right ICA s/o 0.96 (0.335 - 2.752) 0.9391
Regression model for prediction of cognitive impairment (defined as MoCA cutoff score ≤26) with respect to vascular risk factors and the side of ICA s/o
COGNITIVE IMPAIRMENT & VASCULAR RISKCOGNITIVE IMPAIRMENT & VASCULAR RISK

Patients with ICA s/o AND diabetes performed worse (p <0.001) at delayed recall
Patients with ICA s/o AND increased BMI performed worse at delayed recall (p=0.02)*
Patients with diabetes had lower attention (p=0.065)* and naming (p=0.06)* MoCA subtests scores
Hyperlipemic patients scored worse at attention (p=0.064)* Patients with hypertension scored lower at naming MoCA
subtests (p=0.04)* The side of stenosis was not associated with lower
performance on MoCA subtests
COGNITIVE IMPAIRMENT & VASCULAR RISKCOGNITIVE IMPAIRMENT & VASCULAR RISK
* Differences not statistically significant

No neuroimaging in controls ?
Influence of potential cofounders (antihypertensive drugs, statin therapy...) not analyzed ?
Duration of exposure to vascular risk factors ?
What were What were THE LIMITATIONS OF OUR STUDY?THE LIMITATIONS OF OUR STUDY?

• Patients with severe carotid disease often do have subtle cognitive abnormalities
• MoCA is far more suitable for cognitive assessment in patients with carotid disease than MMSE
• Decreased median MoCA scores in controls is probably due to the presence of vascular risk and likely to the silent brain injury (no neuroimaging was done in controls!)
What are What are OUR PRINCIPAL FINDINGS?OUR PRINCIPAL FINDINGS?
• Patients with severe carotid disease had impaired multiple cognitive domains when MoCA subtests were analyzed:
...VISUOSPATIAL, EXECUTIVE, ATTENTION...
• Our results are similar to those of other researchers (who mostly used extensive neuropsychological testing batteries!)
What are What are OUR PRINCIPAL FINDINGS?OUR PRINCIPAL FINDINGS?

• Decreased total MoCA scores in older patients with ICA s/o
• Decreased total MoCA scores in diabetic patients with carotid disease in line with previous research (diabetes is well known indipendent factor for cognitive decline)
What are What are OUR PRINCIPAL FINDINGS?OUR PRINCIPAL FINDINGS?

• Stroke/TIA free patients with advanced carotid disease are routinely considered asymptomatic
• Cognitive impairment in patients with ICA s/o is not questioned during routine clinical visits
• The use of MoCA could facilitate early recognition of cognitive problems in patients with carotid disease
What can we CONCLUDE ?What can we CONCLUDE ?

THANK YOU!THANK YOU!
