michigan department of health and human services federally ... · conz of cervix w/scope leep...
TRANSCRIPT

Code Short Description Modifier Age Range Rate Effective Date**10021 Fna W/O Image $68.7410022 Fna W/Image $79.2410040 Acne Surgery $62.0110060 Drainage Of Skin Abscess $66.9610061 Drainage Of Skin Abscess $116.2810080 Drainage Of Pilonidal Cyst $101.4310081 Drainage Of Pilonidal Cyst $152.1410120 Remove Foreign Body $86.7710121 Remove Foreign Body $155.1110140 Drainage Of Hematoma/Fluid $92.9110160 Puncture Drainage Of Lesion $73.5011000 Debride Infected Skin $30.9011042 Deb Subq Tissue 20 Sq Cm/< $66.3611055 Trim Skin Lesion $27.1411056 Trim Skin Lesions 2 To 4 $33.0811057 Trim Skin Lesions Over 4 $37.4411100 Biopsy Skin Lesion $59.4311101 Biopsy Skin Add-On $18.4211200 Removal Of Skin Tags <W/15 $50.5211201 Remove Skin Tags Add-On $10.9011300 Shave Skin Lesion 0.5 Cm/< $55.2711301 Shave Skin Lesion 0.6-1.0 Cm $67.7511302 Shave Skin Lesion 1.1-2.0 Cm $79.8311303 Shave Skin Lesion >2.0 Cm $88.1511305 Shave Skin Lesion 0.5 Cm/< $55.8611306 Shave Skin Lesion 0.6-1.0 Cm $68.9411307 Shave Skin Lesion 1.1-2.0 Cm $81.8211308 Shave Skin Lesion >2.0 Cm $85.3811310 Shave Skin Lesion 0.5 Cm/< $64.3811311 Shave Skin Lesion 0.6-1.0 Cm $63.0011312 Shave Skin Lesion 1.1-2.0 Cm $90.7311313 Shave Skin Lesion >2.0 Cm $105.1911400 Exc Tr-Ext B9+Marg 0.5 Cm< $70.9211401 Exc Tr-Ext B9+Marg 0.6-1 Cm $84.5911402 Exc Tr-Ext B9+Marg 1.1-2 Cm $94.3011403 Exc Tr-Ext B9+Marg 2.1-3cm $108.9611404 Exc Tr-Ext B9+Marg 3.1-4 Cm $123.4211406 Exc Tr-Ext B9+Marg >4.0 Cm $178.0911420 Exc H-F-Nk-Sp B9+Marg 0.5/< $69.3411421 Exc H-F-Nk-Sp B9+Marg 0.6-1 $88.7511422 Exc H-F-Nk-Sp B9+Marg 1.1-2 $99.8411423 Exc H-F-Nk-Sp B9+Marg 2.1-3 $113.7111424 Exc H-F-Nk-Sp B9+Marg 3.1-4 $132.1311426 Exc H-F-Nk-Sp B9+Marg >4 Cm $189.3811440 Exc Face-Mm B9+Marg 0.5 Cm/< $76.66
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 1 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
11441 Exc Face-Mm B9+Marg 0.6-1 Cm $95.0911442 Exc Face-Mm B9+Marg 1.1-2 Cm $106.3811600 Exc Tr-Ext Mal+Marg 0.5 Cm/< $109.3511601 Exc Tr-Ext Mal+Marg 0.6-1 Cm $129.3611602 Exc Tr-Ext Mal+Marg 1.1-2 Cm $140.2511603 Exc Tr-Ext Mal+Marg 2.1-3 Cm $160.6611604 Exc Tr-Ext Mal+Marg 3.1-4 Cm $178.0911606 Exc Tr-Ext Mal+Marg >4 Cm $254.7611620 Exc H-F-Nk-Sp Mal+Marg 0.5/< $110.1411621 Exc S/N/H/F/G Mal+Mrg 0.6-1 $129.9511622 Exc S/N/H/F/G Mal+Mrg 1.1-2 $145.0111623 Exc S/N/H/F/G Mal+Mrg 2.1-3 $170.1711640 Exc F/E/E/N/L Mal+Mrg 0.5cm< $113.5111641 Exc F/E/E/N/L Mal+Mrg 0.6-1 $134.3111642 Exc F/E/E/N/L Mal+Mrg 1.1-2 $153.3311720 Debride Nail 1-5 $18.6211721 Debride Nail 6 Or More $25.5511730 Removal Of Nail Plate $59.6311732 Remove Nail Plate Add-On $17.8311740 Drain Blood From Under Nail $28.3311750 Removal Of Nail Bed $86.5711755 Biopsy Nail Unit $74.2911760 Repair Of Nail Bed $105.9811765 Excision Of Nail Fold Toe $94.4911900 Inject Skin Lesions </W 7 $31.7011901 Inject Skin Lesions >7 $39.8211976 Remove Contraceptive Capsule $81.2211981 Insert Drug Implant Device $80.2311982 Remove Drug Implant Device $89.7411983 Remove/Insert Drug Implant $129.5612001 Rpr S/N/Ax/Gen/Trnk 2.5cm/< $51.3112002 Rpr S/N/Ax/Gen/Trnk2.6-7.5cm $62.4012004 Rpr S/N/Ax/Gen/Trk7.6-12.5cm $72.9012011 Rpr F/E/E/N/L/M 2.5 Cm/< $62.6012013 Rpr F/E/E/N/L/M 2.6-5.0 Cm $65.5712031 Intmd Rpr S/A/T/Ext 2.5 Cm/< $134.3112032 Intmd Rpr S/A/T/Ext 2.6-7.5 $170.5612041 Intmd Rpr N-Hf/Genit 2.5cm/< $134.1112042 Intmd Rpr N-Hf/Genit2.6-7.5 $163.2312051 Intmd Rpr Face/Mm 2.5 Cm/< $145.8012052 Intmd Rpr Face/Mm 2.6-5.0 Cm $166.2116000 Initial Treatment Of Burn(S) $38.8316020 Dress/Debrid P-Thick Burn S $46.5517000 Destruct Premalg Lesion $37.2417003 Destruct Premalg Les 2-14 $2.9717004 Destroy Premal Lesions 15/> $81.4217110 Destruct B9 Lesion 1-14 $63.0017111 Destruct Lesion 15 Or More $74.49
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 2 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
17250 Chem Caut Of Granltj Tissue $45.3617340 Cryotherapy Of Skin $29.7219000 Drainage Of Breast Lesion $63.3920526 Ther Injection Carp Tunnel $43.7820527 Inj Dupuytren Cord W/Enzyme $47.7420550 Inj Tendon Sheath/Ligament $29.9120551 Inj Tendon Origin/Insertion $34.2720552 Inj Trigger Point 1/2 Muscl $31.1020553 Inject Trigger Points 3/> $35.8620600 Drain/Inj Joint/Bursa W/O Us $27.1420604 Drain/Inj Joint/Bursa W/Us $40.6120605 Drain/Inj Joint/Bursa W/O Us $28.5320606 Drain/Inj Joint/Bursa W/Us $45.1720610 Drain/Inj Joint/Bursa W/O Us $34.0720611 Drain/Inj Joint/Bursa W/Us $51.1120612 Aspirate/Inj Ganglion Cyst $34.0723500 Treat Clavicle Fracture $124.2123650 Treat Shoulder Dislocation $178.6924640 Treat Elbow Dislocation $56.2626010 Drainage Of Finger Abscess $150.1626011 Drainage Of Finger Abscess $221.4826341 Manipulat Palm Cord Post Inj $56.2626600 Treat Metacarpal Fracture $167.0026750 Treat Finger Fracture Each $104.6028190 Removal Of Foot Foreign Body $147.9828470 Treat Metatarsal Fracture $124.8028510 Treatment Of Toe Fracture $70.7229530 Strapping Of Knee $16.8429540 Strapping Of Ankle And/Or Ft $14.8629550 Strapping Of Toes $10.7029580 Application Of Paste Boot $34.6729584 Appl Multlay Comprs Arm/Hand $44.5729700 Removal/Revision Of Cast $36.8529705 Removal/Revision Of Cast $37.6430300 Remove Nasal Foreign Body $99.4530901 Control Of Nosebleed $76.6630903 Control Of Nosebleed $117.8730905 Control Of Nosebleed $182.2530906 Repeat Control Of Nosebleed $189.1931579 Laryngoscopy Telescopic $100.8336415 Routine Venipuncture $2.7036591 Draw Blood Off Venous Device $13.4741010 Incision Of Tongue Fold $114.3043760 Change Gastrostomy Tube $279.3246083 Incise External Hemorrhoid $101.4346320 Removal Of Hemorrhoid Clot $105.1951700 Irrigation Of Bladder $41.8051701 Insert Bladder Catheter $26.74
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 3 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
51702 Insert Temp Bladder Cath $36.2551705 Change Of Bladder Tube $51.9051725 Simple Cystometrogram $106.3851725 Simple Cystometrogram 26 $43.5851725 Simple Cystometrogram TC $62.8051736 Urine Flow Measurement $8.7251736 Urine Flow Measurement 26 $4.7551736 Urine Flow Measurement TC $3.9651741 Electro-Uroflowmetry First $8.9151741 Electro-Uroflowmetry First 26 $4.7551741 Electro-Uroflowmetry First TC $4.1651784 Anal/Urinary Muscle Study $39.2251784 Anal/Urinary Muscle Study 26 $21.3951784 Anal/Urinary Muscle Study TC $17.8351798 Us Urine Capacity Measure $8.9154050 Destruction Penis Lesion(S) $75.8754056 Cryosurgery Penis Lesion(S) $81.0254060 Excision Of Penis Lesion(S) $103.0154065 Destruction Penis Lesion(S) $124.8054150 Circumcision W/Regionl Block $88.7554160 Circumcision Neonate $125.6055250 Removal Of Sperm Duct(S) $220.2956405 I & D Of Vulva/Perineum $61.4156420 Drainage Of Gland Abscess $68.7456441 Lysis Of Labial Lesion(S) $81.6256501 Destroy Vulva Lesions Sim $74.2956515 Destroy Vulva Lesion/S Compl $127.7756605 Biopsy Of Vulva/Perineum $46.1656606 Biopsy Of Vulva/Perineum $21.3956820 Exam Of Vulva W/Scope $63.3956821 Exam/Biopsy Of Vulva W/Scope $83.2057061 Destroy Vag Lesions Simple $64.1857065 Destroy Vag Lesions Complex $109.9557100 Biopsy Of Vagina $50.3257160 Insert Pessary/Other Device $42.5957170 Fitting Of Diaphragm/Cap $33.8857420 Exam Of Vagina W/Scope $66.5657421 Exam/Biopsy Of Vag W/Scope $88.7557452 Exam Of Cervix W/Scope $61.2157454 Bx/Curett Of Cervix W/Scope $85.3857455 Biopsy Of Cervix W/Scope $80.0357456 Endocerv Curettage W/Scope $75.4857460 Bx Of Cervix W/Scope Leep $157.8957461 Conz Of Cervix W/Scope Leep $178.6957500 Biopsy Of Cervix $71.5157505 Endocervical Curettage $57.6557510 Cauterization Of Cervix $73.8957511 Cryocautery Of Cervix $81.62
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 4 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
57520 Conization Of Cervix $173.3457522 Conization Of Cervix $147.9857800 Dilation Of Cervical Canal $33.6858100 Biopsy Of Uterus Lining $61.0158110 Bx Done W/Colposcopy Add-On $27.1458120 Dilation And Curettage $145.4158300 Insert Intrauterine Device $41.4058301 Remove Intrauterine Device $53.4958340 Catheter For Hysterography $67.3558353 Endometr Ablate Thermal $562.8058356 Endometrial Cryoablation $1,048.5458555 Hysteroscopy Dx Sep Proc $150.5658558 Hysteroscopy Biopsy $763.0858562 Hysteroscopy Remove Fb $190.5758563 Hysteroscopy Ablation $890.4658565 Hysteroscopy Sterilization $1,043.5958579 Hysteroscope Procedure M59000 Amniocentesis Diagnostic $71.5159020 Fetal Contract Stress Test $40.0259020 Fetal Contract Stress Test 26 $21.2059020 Fetal Contract Stress Test TC $18.8259025 Fetal Non-Stress Test $27.3459025 Fetal Non-Stress Test 26 $17.0459025 Fetal Non-Stress Test TC $10.3059160 D & C After Delivery $116.2859425 Antepartum Care Only $426.9659426 Antepartum Care Only $762.2859430 Care After Delivery $172.4859812 Treatment Of Miscarriage $180.4759820 Care Of Miscarriage $215.7364405 N Block Inj Occipital $58.0464450 N Block Other Peripheral $45.1764455 N Block Inj Plantar Digit $26.9465205 Remove Foreign Body From Eye $32.0969000 Drain External Ear Lesion $104.9969005 Drain External Ear Lesion $119.4569200 Clear Outer Ear Canal $46.1669209 Remove Impacted Ear Wax Uni $7.9269210 Remove Impacted Ear Wax Uni $27.3469220 Clean Out Mastoid Cavity $45.9670015 Contrast X-Ray Of Brain $81.0270015 Contrast X-Ray Of Brain 26 $33.6870015 Contrast X-Ray Of Brain TC $47.3570030 X-Ray Eye For Foreign Body $15.6570030 X-Ray Eye For Foreign Body 26 $4.7570030 X-Ray Eye For Foreign Body TC $10.9070100 X-Ray Exam Of Jaw <4views $18.4270100 X-Ray Exam Of Jaw <4views 26 $5.15
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 5 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
70100 X-Ray Exam Of Jaw <4views TC $13.2770110 X-Ray Exam Of Jaw 4/> Views $21.2070110 X-Ray Exam Of Jaw 4/> Views 26 $7.1370110 X-Ray Exam Of Jaw 4/> Views TC $14.0770120 X-Ray Exam Of Mastoids $18.6270120 X-Ray Exam Of Mastoids 26 $5.1570120 X-Ray Exam Of Mastoids TC $13.4770130 X-Ray Exam Of Mastoids $30.3170130 X-Ray Exam Of Mastoids 26 $9.7170130 X-Ray Exam Of Mastoids TC $20.6070134 X-Ray Exam Of Middle Ear $27.9370134 X-Ray Exam Of Middle Ear 26 $9.7170134 X-Ray Exam Of Middle Ear TC $18.2370140 X-Ray Exam Of Facial Bones $16.6470140 X-Ray Exam Of Facial Bones 26 $5.9470140 X-Ray Exam Of Facial Bones TC $10.7070150 X-Ray Exam Of Facial Bones $23.1870150 X-Ray Exam Of Facial Bones 26 $7.5370150 X-Ray Exam Of Facial Bones TC $15.6570160 X-Ray Exam Of Nasal Bones $18.4270160 X-Ray Exam Of Nasal Bones 26 $4.9570160 X-Ray Exam Of Nasal Bones TC $13.4770170 X-Ray Exam Of Tear Duct $30.5970170 X-Ray Exam Of Tear Duct 26 $8.5270170 X-Ray Exam Of Tear Duct TC $21.5170190 X-Ray Exam Of Eye Sockets $20.0170190 X-Ray Exam Of Eye Sockets 26 $6.3470190 X-Ray Exam Of Eye Sockets TC $13.6770200 X-Ray Exam Of Eye Sockets $23.7770200 X-Ray Exam Of Eye Sockets 26 $8.1270200 X-Ray Exam Of Eye Sockets TC $15.6570210 X-Ray Exam Of Sinuses $16.6470210 X-Ray Exam Of Sinuses 26 $4.9570210 X-Ray Exam Of Sinuses TC $11.6970220 X-Ray Exam Of Sinuses $21.0070220 X-Ray Exam Of Sinuses 26 $7.1370220 X-Ray Exam Of Sinuses TC $13.8770240 X-Ray Exam Pituitary Saddle $17.2370240 X-Ray Exam Pituitary Saddle 26 $5.5570240 X-Ray Exam Pituitary Saddle TC $11.6970250 X-Ray Exam Of Skull $20.4070250 X-Ray Exam Of Skull 26 $7.1370250 X-Ray Exam Of Skull TC $13.2770260 X-Ray Exam Of Skull $25.5570260 X-Ray Exam Of Skull 26 $9.9170260 X-Ray Exam Of Skull TC $15.6570300 X-Ray Exam Of Teeth $8.3270300 X-Ray Exam Of Teeth 26 $3.37
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 6 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
70300 X-Ray Exam Of Teeth TC $4.9570310 X-Ray Exam Of Teeth $20.8070310 X-Ray Exam Of Teeth 26 $4.5670310 X-Ray Exam Of Teeth TC $16.2470320 Full Mouth X-Ray Of Teeth $29.5270320 Full Mouth X-Ray Of Teeth 26 $6.9370320 Full Mouth X-Ray Of Teeth TC $22.5870328 X-Ray Exam Of Jaw Joint $17.0470328 X-Ray Exam Of Jaw Joint 26 $5.1570328 X-Ray Exam Of Jaw Joint TC $11.8970330 X-Ray Exam Of Jaw Joints $26.3570330 X-Ray Exam Of Jaw Joints 26 $6.9370330 X-Ray Exam Of Jaw Joints TC $19.4170355 Panoramic X-Ray Of Jaws $11.6970355 Panoramic X-Ray Of Jaws 26 $6.3470355 Panoramic X-Ray Of Jaws TC $5.3570360 X-Ray Exam Of Neck $15.8570360 X-Ray Exam Of Neck 26 $4.7570360 X-Ray Exam Of Neck TC $11.0970370 Throat X-Ray & Fluoroscopy $40.2170370 Throat X-Ray & Fluoroscopy 26 $8.9170370 Throat X-Ray & Fluoroscopy TC $31.3070380 X-Ray Exam Of Salivary Gland $18.0370380 X-Ray Exam Of Salivary Gland 26 $4.7570380 X-Ray Exam Of Salivary Gland TC $13.2770390 X-Ray Exam Of Salivary Duct $52.6970390 X-Ray Exam Of Salivary Duct 26 $10.7070390 X-Ray Exam Of Salivary Duct TC $42.0071045 X-Ray Exam Chest 1 View $11.0971045 X-Ray Exam Chest 1 View 26 $5.1571045 X-Ray Exam Chest 1 View TC $5.9471046 X-Ray Exam Chest 2 Views $17.0471046 X-Ray Exam Chest 2 Views 26 $6.1471046 X-Ray Exam Chest 2 Views TC $10.9071047 X-Ray Exam Chest 3 Views $21.7971047 X-Ray Exam Chest 3 Views 26 $7.9271047 X-Ray Exam Chest 3 Views TC $13.8771048 X-Ray Exam Chest 4+ Views $23.3871048 X-Ray Exam Chest 4+ Views 26 $9.1171048 X-Ray Exam Chest 4+ Views TC $14.2671100 X-Ray Exam Ribs Uni 2 Views $18.6271100 X-Ray Exam Ribs Uni 2 Views 26 $6.3471100 X-Ray Exam Ribs Uni 2 Views TC $12.2871101 X-Ray Exam Unilat Ribs/Chest $21.3971101 X-Ray Exam Unilat Ribs/Chest 26 $7.7371101 X-Ray Exam Unilat Ribs/Chest TC $13.6771110 X-Ray Exam Ribs Bil 3 Views $22.3971110 X-Ray Exam Ribs Bil 3 Views 26 $8.32
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 7 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
71110 X-Ray Exam Ribs Bil 3 Views TC $14.0771111 X-Ray Exam Ribs/Chest4/> Vws $26.3571111 X-Ray Exam Ribs/Chest4/> Vws 26 $9.3171111 X-Ray Exam Ribs/Chest4/> Vws TC $17.0471120 X-Ray Exam Breastbone 2/>Vws $16.6471120 X-Ray Exam Breastbone 2/>Vws 26 $5.7471120 X-Ray Exam Breastbone 2/>Vws TC $10.9071130 X-Ray Strenoclavic Jt 3/>Vws $20.2171130 X-Ray Strenoclavic Jt 3/>Vws 26 $6.3471130 X-Ray Strenoclavic Jt 3/>Vws TC $13.8772020 X-Ray Exam Of Spine 1 View $12.4872020 X-Ray Exam Of Spine 1 View 26 $4.3672020 X-Ray Exam Of Spine 1 View TC $8.1272040 X-Ray Exam Neck Spine 2-3 Vw $18.6272040 X-Ray Exam Neck Spine 2-3 Vw 26 $6.3472040 X-Ray Exam Neck Spine 2-3 Vw TC $12.2872050 X-Ray Exam Neck Spine 4/5vws $25.3672050 X-Ray Exam Neck Spine 4/5vws 26 $8.9172050 X-Ray Exam Neck Spine 4/5vws TC $16.4472052 X-Ray Exam Neck Spine 6/>Vws $31.3072052 X-Ray Exam Neck Spine 6/>Vws 26 $10.3072052 X-Ray Exam Neck Spine 6/>Vws TC $21.0072070 X-Ray Exam Thorac Spine 2vws $19.0272070 X-Ray Exam Thorac Spine 2vws 26 $6.3472070 X-Ray Exam Thorac Spine 2vws TC $12.6872072 X-Ray Exam Thorac Spine 3vws $19.4172072 X-Ray Exam Thorac Spine 3vws 26 $6.1472072 X-Ray Exam Thorac Spine 3vws TC $13.2772074 X-Ray Exam Thorac Spine4/>Vw $21.7972074 X-Ray Exam Thorac Spine4/>Vw 26 $6.1472074 X-Ray Exam Thorac Spine4/>Vw TC $15.6572080 X-Ray Exam Thoracolmb 2/> Vw $18.8272080 X-Ray Exam Thoracolmb 2/> Vw 26 $6.3472080 X-Ray Exam Thoracolmb 2/> Vw TC $12.4872081 X-Ray Exam Entire Spi 1 Vw $21.5972081 X-Ray Exam Entire Spi 1 Vw 26 $7.5372081 X-Ray Exam Entire Spi 1 Vw TC $14.0772082 X-Ray Exam Entire Spi 2/3 Vw $34.8772082 X-Ray Exam Entire Spi 2/3 Vw 26 $9.1172082 X-Ray Exam Entire Spi 2/3 Vw TC $25.7572083 X-Ray Exam Entire Spi 4/5 Vw $42.0072083 X-Ray Exam Entire Spi 4/5 Vw 26 $10.3072083 X-Ray Exam Entire Spi 4/5 Vw TC $31.7072084 X-Ray Exam Entire Spi 6/> Vw $48.9372084 X-Ray Exam Entire Spi 6/> Vw 26 $12.0872084 X-Ray Exam Entire Spi 6/> Vw TC $36.8572100 X-Ray Exam L-S Spine 2/3 Vws $19.6172100 X-Ray Exam L-S Spine 2/3 Vws 26 $6.34
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 8 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
72100 X-Ray Exam L-S Spine 2/3 Vws TC $13.2772110 X-Ray Exam L-2 Spine 4/>Vws $27.3472110 X-Ray Exam L-2 Spine 4/>Vws 26 $8.9172110 X-Ray Exam L-2 Spine 4/>Vws TC $18.4272114 X-Ray Exam L-S Spine Bending $34.4772114 X-Ray Exam L-S Spine Bending 26 $9.3172114 X-Ray Exam L-S Spine Bending TC $25.1672120 X-Ray Bend Only L-S Spine $22.7872120 X-Ray Bend Only L-S Spine 26 $6.3472120 X-Ray Bend Only L-S Spine TC $16.4472170 X-Ray Exam Of Pelvis $17.8372170 X-Ray Exam Of Pelvis 26 $4.9572170 X-Ray Exam Of Pelvis TC $12.8872190 X-Ray Exam Of Pelvis $21.2072190 X-Ray Exam Of Pelvis 26 $6.1472190 X-Ray Exam Of Pelvis TC $15.0672200 X-Ray Exam Si Joints $15.8572200 X-Ray Exam Si Joints 26 $4.9572200 X-Ray Exam Si Joints TC $10.9072202 X-Ray Exam Si Joints 3/> Vws $18.4272202 X-Ray Exam Si Joints 3/> Vws 26 $5.3572202 X-Ray Exam Si Joints 3/> Vws TC $13.0772220 X-Ray Exam Sacrum Tailbone $15.8572220 X-Ray Exam Sacrum Tailbone 26 $4.9572220 X-Ray Exam Sacrum Tailbone TC $10.9072240 Myelography Neck Spine $54.8772240 Myelography Neck Spine 26 $25.5572240 Myelography Neck Spine TC $29.3272255 Myelography Thoracic Spine $55.0772255 Myelography Thoracic Spine 26 $26.1572255 Myelography Thoracic Spine TC $28.9272265 Myelography L-S Spine $51.5172265 Myelography L-S Spine 26 $23.1872265 Myelography L-S Spine TC $28.3372270 Myelogphy 2/> Spine Regions $71.7172270 Myelogphy 2/> Spine Regions 26 $38.0472270 Myelogphy 2/> Spine Regions TC $33.6872275 Epidurography $64.7872275 Epidurography 26 $21.9972275 Epidurography TC $42.7972285 Discography Cerv/Thor Spine $62.8072285 Discography Cerv/Thor Spine 26 $33.6872285 Discography Cerv/Thor Spine TC $29.1272295 X-Ray Of Lower Spine Disk $54.4872295 X-Ray Of Lower Spine Disk 26 $24.3772295 X-Ray Of Lower Spine Disk TC $30.1173000 X-Ray Exam Of Collar Bone $15.6573000 X-Ray Exam Of Collar Bone 26 $4.75
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 9 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
73000 X-Ray Exam Of Collar Bone TC $10.9073010 X-Ray Exam Of Shoulder Blade $17.0473010 X-Ray Exam Of Shoulder Blade 26 $5.1573010 X-Ray Exam Of Shoulder Blade TC $11.8973020 X-Ray Exam Of Shoulder $12.8873020 X-Ray Exam Of Shoulder 26 $4.5673020 X-Ray Exam Of Shoulder TC $8.3273030 X-Ray Exam Of Shoulder $16.4473030 X-Ray Exam Of Shoulder 26 $5.3573030 X-Ray Exam Of Shoulder TC $11.0973040 Contrast X-Ray Of Shoulder $56.6673040 Contrast X-Ray Of Shoulder 26 $15.4573040 Contrast X-Ray Of Shoulder TC $41.2073050 X-Ray Exam Of Shoulders $20.0173050 X-Ray Exam Of Shoulders 26 $5.9473050 X-Ray Exam Of Shoulders TC $14.0773060 X-Ray Exam Of Humerus $16.2473060 X-Ray Exam Of Humerus 26 $4.7573060 X-Ray Exam Of Humerus TC $11.4973070 X-Ray Exam Of Elbow $15.2573070 X-Ray Exam Of Elbow 26 $4.5673070 X-Ray Exam Of Elbow TC $10.7073080 X-Ray Exam Of Elbow $17.6373080 X-Ray Exam Of Elbow 26 $4.9573080 X-Ray Exam Of Elbow TC $12.6873085 Contrast X-Ray Of Elbow $53.6973085 Contrast X-Ray Of Elbow 26 $16.2473085 Contrast X-Ray Of Elbow TC $37.4473090 X-Ray Exam Of Forearm $14.4673090 X-Ray Exam Of Forearm 26 $4.7573090 X-Ray Exam Of Forearm TC $9.7173092 X-Ray Exam Of Arm Infant $15.2573092 X-Ray Exam Of Arm Infant 26 $4.5673092 X-Ray Exam Of Arm Infant TC $10.7073100 X-Ray Exam Of Wrist $17.6373100 X-Ray Exam Of Wrist 26 $4.9573100 X-Ray Exam Of Wrist TC $12.6873110 X-Ray Exam Of Wrist $19.6173110 X-Ray Exam Of Wrist 26 $4.9573110 X-Ray Exam Of Wrist TC $14.6673115 Contrast X-Ray Of Wrist $59.8373115 Contrast X-Ray Of Wrist 26 $16.0573115 Contrast X-Ray Of Wrist TC $43.7873120 X-Ray Exam Of Hand $15.8573120 X-Ray Exam Of Hand 26 $4.7573120 X-Ray Exam Of Hand TC $11.0973130 X-Ray Exam Of Hand $17.8373130 X-Ray Exam Of Hand 26 $4.95
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 10 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
73130 X-Ray Exam Of Hand TC $12.8873140 X-Ray Exam Of Finger(S) $18.0373140 X-Ray Exam Of Finger(S) 26 $3.9673140 X-Ray Exam Of Finger(S) TC $14.0773501 X-Ray Exam Hip Uni 1 View $16.8473501 X-Ray Exam Hip Uni 1 View 26 $5.3573501 X-Ray Exam Hip Uni 1 View TC $11.4973502 X-Ray Exam Hip Uni 2-3 Views $23.1873502 X-Ray Exam Hip Uni 2-3 Views 26 $6.3473502 X-Ray Exam Hip Uni 2-3 Views TC $16.8473503 X-Ray Exam Hip Uni 4/> Views $28.9273503 X-Ray Exam Hip Uni 4/> Views 26 $8.1273503 X-Ray Exam Hip Uni 4/> Views TC $20.8073521 X-Ray Exam Hips Bi 2 Views $21.0073521 X-Ray Exam Hips Bi 2 Views 26 $6.3473521 X-Ray Exam Hips Bi 2 Views TC $14.6673522 X-Ray Exam Hips Bi 3-4 Views $27.3473522 X-Ray Exam Hips Bi 3-4 Views 26 $8.5273522 X-Ray Exam Hips Bi 3-4 Views TC $18.8273523 X-Ray Exam Hips Bi 5/> Views $31.7073523 X-Ray Exam Hips Bi 5/> Views 26 $9.1173523 X-Ray Exam Hips Bi 5/> Views TC $22.5873525 Contrast X-Ray Of Hip $57.8573525 Contrast X-Ray Of Hip 26 $16.4473525 Contrast X-Ray Of Hip TC $41.4073551 X-Ray Exam Of Femur 1 $15.6573551 X-Ray Exam Of Femur 1 26 $4.7573551 X-Ray Exam Of Femur 1 TC $10.9073552 X-Ray Exam Of Femur 2/> $18.4273552 X-Ray Exam Of Femur 2/> 26 $5.3573552 X-Ray Exam Of Femur 2/> TC $13.0773560 X-Ray Exam Of Knee 1 Or 2 $17.4373560 X-Ray Exam Of Knee 1 Or 2 26 $4.7573560 X-Ray Exam Of Knee 1 Or 2 TC $12.6873562 X-Ray Exam Of Knee 3 $20.0173562 X-Ray Exam Of Knee 3 26 $5.3573562 X-Ray Exam Of Knee 3 TC $14.6673564 X-Ray Exam Knee 4 Or More $22.1973564 X-Ray Exam Knee 4 Or More 26 $6.3473564 X-Ray Exam Knee 4 Or More TC $15.8573565 X-Ray Exam Of Knees $20.0173565 X-Ray Exam Of Knees 26 $4.9573565 X-Ray Exam Of Knees TC $15.0673580 Contrast X-Ray Of Knee Joint $65.5773580 Contrast X-Ray Of Knee Joint 26 $16.2473580 Contrast X-Ray Of Knee Joint TC $49.3373590 X-Ray Exam Of Lower Leg $16.0573590 X-Ray Exam Of Lower Leg 26 $4.75
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 11 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
73590 X-Ray Exam Of Lower Leg TC $11.2973592 X-Ray Exam Of Leg Infant $15.2573592 X-Ray Exam Of Leg Infant 26 $4.5673592 X-Ray Exam Of Leg Infant TC $10.7073600 X-Ray Exam Of Ankle $16.6473600 X-Ray Exam Of Ankle 26 $4.7573600 X-Ray Exam Of Ankle TC $11.8973610 X-Ray Exam Of Ankle $17.6373610 X-Ray Exam Of Ankle 26 $4.9573610 X-Ray Exam Of Ankle TC $12.6873615 Contrast X-Ray Of Ankle $59.8373615 Contrast X-Ray Of Ankle 26 $16.2473615 Contrast X-Ray Of Ankle TC $43.5873620 X-Ray Exam Of Foot $14.6673620 X-Ray Exam Of Foot 26 $4.3673620 X-Ray Exam Of Foot TC $10.3073630 X-Ray Exam Of Foot $16.4473630 X-Ray Exam Of Foot 26 $4.7573630 X-Ray Exam Of Foot TC $11.6973650 X-Ray Exam Of Heel $15.2573650 X-Ray Exam Of Heel 26 $4.5673650 X-Ray Exam Of Heel TC $10.7073660 X-Ray Exam Of Toe(S) $15.8573660 X-Ray Exam Of Toe(S) 26 $3.7673660 X-Ray Exam Of Toe(S) TC $12.0874018 X-Ray Exam Abdomen 1 View $15.2574018 X-Ray Exam Abdomen 1 View 26 $5.1574018 X-Ray Exam Abdomen 1 View TC $10.1074019 X-Ray Exam Abdomen 2 Views $18.6274019 X-Ray Exam Abdomen 2 Views 26 $6.5474019 X-Ray Exam Abdomen 2 Views TC $12.0874021 X-Ray Exam Abdomen 3+ Views $21.7974021 X-Ray Exam Abdomen 3+ Views 26 $7.7374021 X-Ray Exam Abdomen 3+ Views TC $14.0774022 X-Ray Exam Series Abdomen $24.9674022 X-Ray Exam Series Abdomen 26 $9.1174022 X-Ray Exam Series Abdomen TC $15.8574190 X-Ray Exam Of Peritoneum $43.8974190 X-Ray Exam Of Peritoneum 26 $13.2774190 X-Ray Exam Of Peritoneum TC $29.2374400 Contrst X-Ray Urinary Tract $61.4174400 Contrst X-Ray Urinary Tract 26 $13.8774400 Contrst X-Ray Urinary Tract TC $47.5474410 Contrst X-Ray Urinary Tract $62.2074410 Contrst X-Ray Urinary Tract 26 $13.8774410 Contrst X-Ray Urinary Tract TC $48.3474415 Contrst X-Ray Urinary Tract $76.2774415 Contrst X-Ray Urinary Tract 26 $13.87
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 12 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
74415 Contrst X-Ray Urinary Tract TC $62.4074420 Contrst X-Ray Urinary Tract $69.8374420 Contrst X-Ray Urinary Tract 26 $9.9174420 Contrst X-Ray Urinary Tract TC $58.6874425 Contrst X-Ray Urinary Tract $40.3974425 Contrst X-Ray Urinary Tract 26 $9.9174425 Contrst X-Ray Urinary Tract TC $29.2374430 Contrast X-Ray Bladder $21.3974430 Contrast X-Ray Bladder 26 $9.1174430 Contrast X-Ray Bladder TC $12.2874440 X-Ray Male Genital Tract $44.9774440 X-Ray Male Genital Tract 26 $10.3074440 X-Ray Male Genital Tract TC $34.6774445 X-Ray Exam Of Penis $60.5674445 X-Ray Exam Of Penis 26 $31.5074445 X-Ray Exam Of Penis TC $25.2074450 X-Ray Urethra/Bladder $42.9474450 X-Ray Urethra/Bladder 26 $9.3174450 X-Ray Urethra/Bladder TC $32.6574455 X-Ray Urethra/Bladder $46.1674455 X-Ray Urethra/Bladder 26 $9.3174455 X-Ray Urethra/Bladder TC $36.8574470 X-Ray Exam Of Kidney Lesion $44.4074470 X-Ray Exam Of Kidney Lesion 26 $14.8674470 X-Ray Exam Of Kidney Lesion TC $28.0174485 X-Ray Guide Gu Dilation $51.9074485 X-Ray Guide Gu Dilation 26 $14.6674485 X-Ray Guide Gu Dilation TC $37.2474710 X-Ray Measurement Of Pelvis $20.4074710 X-Ray Measurement Of Pelvis 26 $9.7174710 X-Ray Measurement Of Pelvis TC $10.7074712 Mri Fetal Sngl/1st Gestation $276.5574712 Mri Fetal Sngl/1st Gestation 26 $84.7974712 Mri Fetal Sngl/1st Gestation TC $191.7674713 Mri Fetal Ea Addl Gestation $133.7274713 Mri Fetal Ea Addl Gestation 26 $52.5074713 Mri Fetal Ea Addl Gestation TC $81.2274740 X-Ray Female Genital Tract $41.8074740 X-Ray Female Genital Tract 26 $10.7074740 X-Ray Female Genital Tract TC $31.1074742 X-Ray Fallopian Tube $40.5474742 X-Ray Fallopian Tube 26 $17.4374742 X-Ray Fallopian Tube TC $29.7074775 X-Ray Exam Of Perineum $51.7874775 X-Ray Exam Of Perineum 26 $17.6374775 X-Ray Exam Of Perineum TC $32.6575600 Contrast Exam Thoracic Aorta $112.3275600 Contrast Exam Thoracic Aorta 26 $13.67
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 13 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
75600 Contrast Exam Thoracic Aorta TC $98.6575605 Contrast Exam Thoracic Aorta $77.2675605 Contrast Exam Thoracic Aorta 26 $31.3075605 Contrast Exam Thoracic Aorta TC $45.9675625 Contrast Exam Abdominl Aorta $76.8675625 Contrast Exam Abdominl Aorta 26 $31.5075625 Contrast Exam Abdominl Aorta TC $45.3675630 X-Ray Aorta Leg Arteries $95.4875630 X-Ray Aorta Leg Arteries 26 $49.5375630 X-Ray Aorta Leg Arteries TC $45.9675705 Artery X-Rays Spine $142.0475705 Artery X-Rays Spine 26 $64.9875705 Artery X-Rays Spine TC $77.0675710 Artery X-Rays Arm/Leg $96.4775710 Artery X-Rays Arm/Leg 26 $48.5375710 Artery X-Rays Arm/Leg TC $47.9475716 Artery X-Rays Arms/Legs $109.5575716 Artery X-Rays Arms/Legs 26 $54.2875716 Artery X-Rays Arms/Legs TC $55.2775726 Artery X-Rays Abdomen $83.6075726 Artery X-Rays Abdomen 26 $31.1075726 Artery X-Rays Abdomen TC $52.5075731 Artery X-Rays Adrenal Gland $96.4775731 Artery X-Rays Adrenal Gland 26 $32.2975731 Artery X-Rays Adrenal Gland TC $64.1875733 Artery X-Rays Adrenals $103.6175733 Artery X-Rays Adrenals 26 $35.8675733 Artery X-Rays Adrenals TC $67.7575736 Artery X-Rays Pelvis $89.5475736 Artery X-Rays Pelvis 26 $30.9075736 Artery X-Rays Pelvis TC $58.6475741 Artery X-Rays Lung $83.9975741 Artery X-Rays Lung 26 $35.4675741 Artery X-Rays Lung TC $48.5375743 Artery X-Rays Lungs $94.4975743 Artery X-Rays Lungs 26 $45.3675743 Artery X-Rays Lungs TC $49.1375746 Artery X-Rays Lung $84.9875746 Artery X-Rays Lung 26 $31.3075746 Artery X-Rays Lung TC $53.6975756 Artery X-Rays Chest $96.6775756 Artery X-Rays Chest 26 $32.0975756 Artery X-Rays Chest TC $64.5875774 Artery X-Ray Each Vessel $48.5375774 Artery X-Ray Each Vessel 26 $9.7175774 Artery X-Ray Each Vessel TC $38.8375801 Lymph Vessel X-Ray Arm/Leg $147.4675801 Lymph Vessel X-Ray Arm/Leg 26 $25.16
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 14 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
75801 Lymph Vessel X-Ray Arm/Leg TC $121.1975803 Lymph Vessel X-Ray Arms/Legs $156.7275803 Lymph Vessel X-Ray Arms/Legs 26 $33.8875803 Lymph Vessel X-Ray Arms/Legs TC $121.1975805 Lymph Vessel X-Ray Trunk $161.9675805 Lymph Vessel X-Ray Trunk 26 $22.1975805 Lymph Vessel X-Ray Trunk TC $136.6975807 Lymph Vessel X-Ray Trunk $242.9575807 Lymph Vessel X-Ray Trunk 26 $31.8975807 Lymph Vessel X-Ray Trunk TC $205.0375809 Nonvascular Shunt X-Ray $55.4775809 Nonvascular Shunt X-Ray 26 $13.4775809 Nonvascular Shunt X-Ray TC $42.0075810 Vein X-Ray Spleen/Liver $315.9275810 Vein X-Ray Spleen/Liver 26 $30.7175810 Vein X-Ray Spleen/Liver TC $281.2475820 Vein X-Ray Arm/Leg $64.7875820 Vein X-Ray Arm/Leg 26 $19.6175820 Vein X-Ray Arm/Leg TC $45.1775822 Vein X-Ray Arms/Legs $76.0775822 Vein X-Ray Arms/Legs 26 $29.3275822 Vein X-Ray Arms/Legs TC $46.7575825 Vein X-Ray Trunk $75.4875825 Vein X-Ray Trunk 26 $31.5075825 Vein X-Ray Trunk TC $43.9875827 Vein X-Ray Chest $77.8575827 Vein X-Ray Chest 26 $31.7075827 Vein X-Ray Chest TC $46.1675831 Vein X-Ray Kidney $78.6575831 Vein X-Ray Kidney 26 $31.1075831 Vein X-Ray Kidney TC $47.5475833 Vein X-Ray Kidneys $93.1175833 Vein X-Ray Kidneys 26 $41.0175833 Vein X-Ray Kidneys TC $52.1075840 Vein X-Ray Adrenal Gland $83.2075840 Vein X-Ray Adrenal Gland 26 $32.2975840 Vein X-Ray Adrenal Gland TC $50.9175842 Vein X-Ray Adrenal Glands $99.6475842 Vein X-Ray Adrenal Glands 26 $42.2075842 Vein X-Ray Adrenal Glands TC $57.4575860 Vein X-Ray Neck $80.8275860 Vein X-Ray Neck 26 $31.5075860 Vein X-Ray Neck TC $49.3375870 Vein X-Ray Skull $83.2075870 Vein X-Ray Skull 26 $32.2975870 Vein X-Ray Skull TC $50.9175872 Vein X-Ray Skull Epidural $83.2075872 Vein X-Ray Skull Epidural 26 $32.29
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 15 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
75872 Vein X-Ray Skull Epidural TC $50.9175880 Vein X-Ray Eye Socket $70.5275880 Vein X-Ray Eye Socket 26 $19.8175880 Vein X-Ray Eye Socket TC $50.7175885 Vein X-Ray Liver W/Hemodynam $87.7675885 Vein X-Ray Liver W/Hemodynam 26 $38.4375885 Vein X-Ray Liver W/Hemodynam TC $49.3375887 Vein X-Ray Liver W/O Hemodyn $87.9675887 Vein X-Ray Liver W/O Hemodyn 26 $38.4375887 Vein X-Ray Liver W/O Hemodyn TC $49.5375889 Vein X-Ray Liver W/Hemodynam $80.4375889 Vein X-Ray Liver W/Hemodynam 26 $30.7175889 Vein X-Ray Liver W/Hemodynam TC $49.7275891 Vein X-Ray Liver $81.0275891 Vein X-Ray Liver 26 $31.1075891 Vein X-Ray Liver TC $49.9275893 Venous Sampling By Catheter $67.3575893 Venous Sampling By Catheter 26 $15.2575893 Venous Sampling By Catheter TC $52.1075894 X-Rays Transcath Therapy $580.0275894 X-Rays Transcath Therapy 26 $40.6175894 X-Rays Transcath Therapy TC $539.3375898 Follow-Up Angiography $73.9675898 Follow-Up Angiography 26 $50.7175898 Follow-Up Angiography TC $23.5675901 Remove Cva Device Obstruct $100.4475901 Remove Cva Device Obstruct 26 $13.2775901 Remove Cva Device Obstruct TC $87.1675902 Remove Cva Lumen Obstruct $40.4175902 Remove Cva Lumen Obstruct 26 $10.7075902 Remove Cva Lumen Obstruct TC $29.7276010 X-Ray Nose To Rectum $14.6676010 X-Ray Nose To Rectum 26 $5.1576010 X-Ray Nose To Rectum TC $9.5176080 X-Ray Exam Of Fistula $30.7176080 X-Ray Exam Of Fistula 26 $14.6676080 X-Ray Exam Of Fistula TC $16.0576098 X-Ray Exam Surgical Specimen $9.5176098 X-Ray Exam Surgical Specimen 26 $4.5676098 X-Ray Exam Surgical Specimen TC $4.9576100 X-Ray Exam Of Body Section $51.3176100 X-Ray Exam Of Body Section 26 $17.8376100 X-Ray Exam Of Body Section TC $33.4876101 Complex Body Section X-Ray $59.6376101 Complex Body Section X-Ray 26 $16.0576101 Complex Body Section X-Ray TC $43.5876102 Complex Body Section X-Rays $95.4876102 Complex Body Section X-Rays 26 $19.61
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 16 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
76102 Complex Body Section X-Rays TC $75.8776506 Echo Exam Of Head $66.1776506 Echo Exam Of Head 26 $18.0376506 Echo Exam Of Head TC $48.1476510 Ophth Us B & Quant A $77.0676510 Ophth Us B & Quant A 26 $40.4176510 Ophth Us B & Quant A TC $36.6576511 Ophth Us Quant A Only $46.1676511 Ophth Us Quant A Only 26 $24.1776511 Ophth Us Quant A Only TC $21.9976512 Ophth Us B W/Non-Quant A $42.2076512 Ophth Us B W/Non-Quant A 26 $24.1776512 Ophth Us B W/Non-Quant A TC $18.0376513 Echo Exam Of Eye Water Bath $53.8876513 Echo Exam Of Eye Water Bath 26 $20.2176513 Echo Exam Of Eye Water Bath TC $33.6876514 Echo Exam Of Eye Thickness $8.7276514 Echo Exam Of Eye Thickness 26 $5.5576514 Echo Exam Of Eye Thickness TC $3.1776516 Echo Exam Of Eye $35.6676516 Echo Exam Of Eye 26 $14.0776516 Echo Exam Of Eye TC $21.5976519 Echo Exam Of Eye $41.8076519 Echo Exam Of Eye 26 $17.6376519 Echo Exam Of Eye TC $24.1776529 Echo Exam Of Eye $45.1776529 Echo Exam Of Eye 26 $18.6276529 Echo Exam Of Eye TC $26.5576536 Us Exam Of Head And Neck $65.7776536 Us Exam Of Head And Neck 26 $15.8576536 Us Exam Of Head And Neck TC $49.9276604 Us Exam Chest $50.3276604 Us Exam Chest 26 $15.2576604 Us Exam Chest TC $35.0676641 Ultrasound Breast Complete $60.6276641 Ultrasound Breast Complete 26 $20.6076641 Ultrasound Breast Complete TC $40.0276642 Ultrasound Breast Limited $49.7276642 Ultrasound Breast Limited 26 $19.2276642 Ultrasound Breast Limited TC $30.5176700 Us Exam Abdom Complete $69.1476700 Us Exam Abdom Complete 26 $22.7876700 Us Exam Abdom Complete TC $46.3676705 Echo Exam Of Abdomen $51.7076705 Echo Exam Of Abdomen 26 $16.6476705 Echo Exam Of Abdomen TC $35.0676706 Us Abdl Aorta Screen Aaa $53.2976706 Us Abdl Aorta Screen Aaa 26 $15.65
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 17 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
76706 Us Abdl Aorta Screen Aaa TC $37.6476770 Us Exam Abdo Back Wall Comp $63.9976770 Us Exam Abdo Back Wall Comp 26 $20.8076770 Us Exam Abdo Back Wall Comp TC $43.1976775 Us Exam Abdo Back Wall Lim $32.6976775 Us Exam Abdo Back Wall Lim 26 $16.2476775 Us Exam Abdo Back Wall Lim TC $16.4476776 Us Exam K Transpl W/Doppler $88.5576776 Us Exam K Transpl W/Doppler 26 $21.3976776 Us Exam K Transpl W/Doppler TC $67.1676800 Us Exam Spinal Canal $82.2176800 Us Exam Spinal Canal 26 $33.6876800 Us Exam Spinal Canal TC $48.5376801 Ob Us < 14 Wks Single Fetus $69.7376801 Ob Us < 14 Wks Single Fetus 26 $28.1376801 Ob Us < 14 Wks Single Fetus TC $41.6076802 Ob Us < 14 Wks Addl Fetus $36.6576802 Ob Us < 14 Wks Addl Fetus 26 $23.9776802 Ob Us < 14 Wks Addl Fetus TC $12.6876805 Ob Us >/= 14 Wks Sngl Fetus $80.4376805 Ob Us >/= 14 Wks Sngl Fetus 26 $28.5376805 Ob Us >/= 14 Wks Sngl Fetus TC $51.9076810 Ob Us >/= 14 Wks Addl Fetus $52.6976810 Ob Us >/= 14 Wks Addl Fetus 26 $28.3376810 Ob Us >/= 14 Wks Addl Fetus TC $24.3776811 Ob Us Detailed Sngl Fetus $103.4176811 Ob Us Detailed Sngl Fetus 26 $55.2776811 Ob Us Detailed Sngl Fetus TC $48.1476812 Ob Us Detailed Addl Fetus $115.4976812 Ob Us Detailed Addl Fetus 26 $51.9076812 Ob Us Detailed Addl Fetus TC $63.5976813 Ob Us Nuchal Meas 1 Gest $68.9476813 Ob Us Nuchal Meas 1 Gest 26 $34.2776813 Ob Us Nuchal Meas 1 Gest TC $34.6776814 Ob Us Nuchal Meas Add-On $45.7676814 Ob Us Nuchal Meas Add-On 26 $29.1276814 Ob Us Nuchal Meas Add-On TC $16.6476815 Ob Us Limited Fetus(S) $47.7476815 Ob Us Limited Fetus(S) 26 $18.4276815 Ob Us Limited Fetus(S) TC $29.3276816 Ob Us Follow-Up Per Fetus $65.3776816 Ob Us Follow-Up Per Fetus 26 $24.7676816 Ob Us Follow-Up Per Fetus TC $40.6176817 Transvaginal Us Obstetric $54.8776817 Transvaginal Us Obstetric 26 $21.3976817 Transvaginal Us Obstetric TC $33.4876818 Fetal Biophys Profile W/Nst $69.7376818 Fetal Biophys Profile W/Nst 26 $30.71
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 18 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
76818 Fetal Biophys Profile W/Nst TC $39.0376819 Fetal Biophys Profil W/O Nst $50.7176819 Fetal Biophys Profil W/O Nst 26 $22.1976819 Fetal Biophys Profil W/O Nst TC $28.5376820 Umbilical Artery Echo $27.1476820 Umbilical Artery Echo 26 $14.4676820 Umbilical Artery Echo TC $12.6876821 Middle Cerebral Artery Echo $52.6976821 Middle Cerebral Artery Echo 26 $20.4076821 Middle Cerebral Artery Echo TC $32.2976825 Echo Exam Of Fetal Heart $157.0976825 Echo Exam Of Fetal Heart 26 $47.3576825 Echo Exam Of Fetal Heart TC $109.7576826 Echo Exam Of Fetal Heart $92.7176826 Echo Exam Of Fetal Heart 26 $23.3876826 Echo Exam Of Fetal Heart TC $69.3476827 Echo Exam Of Fetal Heart $42.5976827 Echo Exam Of Fetal Heart 26 $16.2476827 Echo Exam Of Fetal Heart TC $26.3576828 Echo Exam Of Fetal Heart $30.1176828 Echo Exam Of Fetal Heart 26 $16.0576828 Echo Exam Of Fetal Heart TC $14.0776830 Transvaginal Us Non-Ob $68.9476830 Transvaginal Us Non-Ob 26 $19.6176830 Transvaginal Us Non-Ob TC $49.3376831 Echo Exam Uterus $67.5576831 Echo Exam Uterus 26 $20.8076831 Echo Exam Uterus TC $46.7576856 Us Exam Pelvic Complete $62.2076856 Us Exam Pelvic Complete 26 $19.4176856 Us Exam Pelvic Complete TC $42.7976857 Us Exam Pelvic Limited $27.3476857 Us Exam Pelvic Limited 26 $14.0776857 Us Exam Pelvic Limited TC $13.2776870 Us Exam Scrotum $38.2376870 Us Exam Scrotum 26 $18.0376870 Us Exam Scrotum TC $20.2176872 Us Transrectal $54.4876872 Us Transrectal 26 $19.0276872 Us Transrectal TC $35.4676873 Echograp Trans R Pros Study $97.6676873 Echograp Trans R Pros Study 26 $43.9876873 Echograp Trans R Pros Study TC $53.6976881 Us Compl Joint R-T W/Img $57.2576881 Us Compl Joint R-T W/Img 26 $17.8376881 Us Compl Joint R-T W/Img TC $39.4276882 Us Lmtd Jt/Nonvasc Xtr Strux $32.4976882 Us Lmtd Jt/Nonvasc Xtr Strux 26 $13.87
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 19 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
76882 Us Lmtd Jt/Nonvasc Xtr Strux TC $18.6276885 Us Exam Infant Hips Dynamic $81.6276885 Us Exam Infant Hips Dynamic 26 $21.0076885 Us Exam Infant Hips Dynamic TC $60.6276886 Us Exam Infant Hips Static $59.6376886 Us Exam Infant Hips Static 26 $17.6376886 Us Exam Infant Hips Static TC $42.0076941 Echo Guide For Transfusion $75.9476941 Echo Guide For Transfusion 26 $38.4376941 Echo Guide For Transfusion TC $34.0976942 Echo Guide For Biopsy $33.6876942 Echo Guide For Biopsy 26 $18.2376942 Echo Guide For Biopsy TC $15.4576945 Echo Guide Villus Sampling $54.5376945 Echo Guide Villus Sampling 26 $19.2276945 Echo Guide Villus Sampling TC $34.0976946 Echo Guide For Amniocentesis $18.4276946 Echo Guide For Amniocentesis 26 $11.0976946 Echo Guide For Amniocentesis TC $7.3376977 Us Bone Density Measure $4.1676977 Us Bone Density Measure 26 $1.5876977 Us Bone Density Measure TC $2.5877053 X-Ray Of Mammary Duct $32.6977053 X-Ray Of Mammary Duct 26 $10.1077053 X-Ray Of Mammary Duct TC $22.5877054 X-Ray Of Mammary Ducts $42.7977054 X-Ray Of Mammary Ducts 26 $12.8877054 X-Ray Of Mammary Ducts TC $29.9177065 Dx Mammo Incl Cad Uni $75.8777065 Dx Mammo Incl Cad Uni 26 $22.9877065 Dx Mammo Incl Cad Uni TC $52.8977066 Dx Mammo Incl Cad Bi $95.8877066 Dx Mammo Incl Cad Bi 26 $28.3377066 Dx Mammo Incl Cad Bi TC $67.5577067 Scr Mammo Bi Incl Cad $77.2677067 Scr Mammo Bi Incl Cad 26 $21.3977067 Scr Mammo Bi Incl Cad TC $55.8677071 X-Ray Stress View $27.1477072 X-Rays For Bone Age $12.8877072 X-Rays For Bone Age 26 $5.3577072 X-Rays For Bone Age TC $7.5377073 X-Rays Bone Length Studies $20.2177073 X-Rays Bone Length Studies 26 $8.1277073 X-Rays Bone Length Studies TC $12.0877074 X-Rays Bone Survey Limited $36.0577074 X-Rays Bone Survey Limited 26 $12.8877074 X-Rays Bone Survey Limited TC $23.1877075 X-Rays Bone Survey Complete $48.93
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 20 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
77075 X-Rays Bone Survey Complete 26 $15.2577075 X-Rays Bone Survey Complete TC $33.6877076 X-Rays Bone Survey Infant $53.6977076 X-Rays Bone Survey Infant 26 $19.8177076 X-Rays Bone Survey Infant TC $33.8877077 Joint Survey Single View $20.8077077 Joint Survey Single View 26 $9.1177077 Joint Survey Single View TC $11.6977080 Dxa Bone Density Axial $23.5777080 Dxa Bone Density Axial 26 $5.7477080 Dxa Bone Density Axial TC $17.8377081 Dxa Bone Density/Peripheral $15.8577081 Dxa Bone Density/Peripheral 26 $6.1477081 Dxa Bone Density/Peripheral TC $9.7178265 Gastric Emptying Imag Study $231.5878265 Gastric Emptying Imag Study 26 $27.1478265 Gastric Emptying Imag Study TC $204.4478266 Gastric Emptying Imag Study $275.9578266 Gastric Emptying Imag Study 26 $30.1178266 Gastric Emptying Imag Study TC $245.8480047 Metabolic Panel Ionized Ca $11.3780048 Metabolic Panel Total Ca $8.6480051 Electrolyte Panel $7.1780053 Comprehen Metabolic Panel $10.8080055 Obstetric Panel $48.8780061 Lipid Panel $13.6980069 Renal Function Panel $8.8880074 Acute Hepatitis Panel $48.6980076 Hepatic Function Panel $8.3580081 Obstetric Panel $76.5280156 Assay Carbamazepine Total $14.8980162 Assay Of Digoxin Total $13.5780163 Assay Of Digoxin Free $13.5780164 Assay Dipropylacetic Acd Tot $13.8480165 Dipropylacetic Acid Free $13.8480170 Assay Of Gentamicin $16.7480171 Drug Screen Quant Gabapentin $17.9480175 Drug Screen Quan Lamotrigine $13.5580176 Assay Of Lidocaine $15.0280177 Drug Scrn Quan Levetiracetam $13.5580178 Assay Of Lithium $6.7680184 Assay Of Phenobarbital $12.6780185 Assay Of Phenytoin Total $13.5580186 Assay Of Phenytoin Free $14.0780197 Assay Of Tacrolimus $14.0480198 Assay Of Theophylline $14.4680200 Assay Of Tobramycin $16.4980201 Assay Of Topiramate $12.19
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 21 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
80202 Assay Of Vancomycin $13.8480299 Quantitative Assay Drug $15.4380305 Drug Test Prsmv Dir Opt Obs $11.1480306 Drug Test Prsmv Instrmnt $14.8780307 Drug Test Prsmv Chem Anlyzr $59.4880500 Lab Pathology Consultation $13.0780502 Lab Pathology Consultation $41.6081000 Urinalysis Nonauto W/Scope $3.3381001 Urinalysis Auto W/Scope $3.2581002 Urinalysis Nonauto W/O Scope $2.8881003 Urinalysis Auto W/O Scope $2.2981005 Urinalysis $2.2181015 Microscopic Exam Of Urine $3.1181025 Urine Pregnancy Test $7.1381099 Urinalysis Test Procedure M81528 Oncology Colorectal Scr $421.3481539 Oncology Prostate Prob Score $629.2882009 Test For Acetone/Ketones $4.6282010 Acetone Assay $8.3582024 Assay Of Acth $39.4882040 Assay Of Serum Albumin $5.0682042 Other Source Albumin Quan Ea $6.4482043 Ur Albumin Quantitative $5.9182044 Ur Albumin Semiquantitative $5.1682085 Assay Of Aldolase $9.9382088 Assay Of Aldosterone $41.6682105 Alpha-Fetoprotein Serum $17.1582120 Amines Vaginal Fluid Qual $4.9682128 Amino Acids Mult Qual $14.1882140 Assay Of Ammonia $14.9082150 Assay Of Amylase $6.6282157 Assay Of Androstenedione $29.9282164 Angiotensin I Enzyme Test $14.9382175 Assay Of Arsenic $19.3982232 Assay Of Beta-2 Protein $16.5482239 Bile Acids Total $17.5082240 Bile Acids Cholylglycine $27.1782247 Bilirubin Total $5.1382248 Bilirubin Direct $5.1382270 Occult Blood Feces $3.6382271 Occult Blood Other Sources $4.4082272 Occult Bld Feces 1-3 Tests $3.5082274 Assay Test For Blood Fecal $16.2682308 Assay Of Calcitonin $27.3982310 Assay Of Calcium $5.2782330 Assay Of Calcium $13.9882340 Assay Of Calcium In Urine $6.1682360 Calculus Assay Quant $13.16
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 22 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
82365 Calculus Spectroscopy $13.1882374 Assay Blood Carbon Dioxide $4.9982375 Assay Carboxyhb Quant $12.5982378 Carcinoembryonic Antigen $19.3882380 Assay Of Carotene $9.4382384 Assay Three Catecholamines $25.8282390 Assay Of Ceruloplasmin $10.9882435 Assay Of Blood Chloride $4.7082436 Assay Of Urine Chloride $5.1482465 Assay Bld/Serum Cholesterol $4.4582525 Assay Of Copper $12.6882530 Cortisol Free $17.0882533 Total Cortisol $16.6682540 Assay Of Creatine $4.7482565 Assay Of Creatinine $5.2482570 Assay Of Urine Creatinine $5.2982575 Creatinine Clearance Test $9.6682595 Assay Of Cryoglobulin $6.6182607 Vitamin B-12 $15.4182626 Dehydroepiandrosterone $25.8382627 Dehydroepiandrosterone $22.7382652 Vit D 1 25-Dihydroxy $39.3582668 Assay Of Erythropoietin $19.2182670 Assay Of Estradiol $28.5682671 Assay Of Estrogens $33.0282672 Assay Of Estrogen $22.1782677 Assay Of Estriol $24.7282679 Assay Of Estrone $25.5182693 Assay Of Ethylene Glycol $15.2482696 Assay Of Etiocholanolone $24.1182710 Fats/Lipids Feces Quant $17.1882728 Assay Of Ferritin $13.9482731 Assay Of Fetal Fibronectin $65.8482746 Assay Of Folic Acid Serum $15.0382784 Assay Iga/Igd/Igg/Igm Each $9.5182800 Blood Ph $9.1182803 Blood Gases Any Combination $21.5982805 Blood Gases W/O2 Saturation $65.2282810 Blood Gases O2 Sat Only $8.9282941 Assay Of Gastrin $18.0382946 Glucagon Tolerance Test $15.4182947 Assay Glucose Blood Quant $4.0282948 Reagent Strip/Blood Glucose $4.1782950 Glucose Test $4.8582951 Glucose Tolerance Test (Gtt) $13.1682952 Gtt-Added Samples $4.0182955 Assay Of G6pd Enzyme $9.9182960 Test For G6pd Enzyme $6.19
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 23 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
82962 Glucose Blood Test $2.7282977 Assay Of Ggt $7.3682985 Assay Of Glycated Protein $15.4183001 Assay Of Gonadotropin (Fsh) $18.9983002 Assay Of Gonadotropin (Lh) $18.9383003 Assay Growth Hormone (Hgh) $17.0483010 Assay Of Haptoglobin Quant $12.8683014 H Pylori Drug Admin $8.0383015 Heavy Metal Qual Any Anal $19.2583020 Hemoglobin Electrophoresis $13.1683020 Hemoglobin Electrophoresis 26 $10.3083021 Hemoglobin Chromotography $18.4683036 Glycosylated Hemoglobin Test $9.9383037 Glycosylated Hb Home Device $9.9383045 Blood Methemoglobin Test $5.3783050 Blood Methemoglobin Assay $7.4983090 Assay Of Homocystine $17.2583497 Assay Of 5-Hiaa $13.1883498 Assay Of Progesterone 17-D $27.7783525 Assay Of Insulin $11.6883540 Assay Of Iron $6.6283550 Iron Binding Test $8.9383605 Assay Of Lactic Acid $10.9283615 Lactate (Ld) (Ldh) Enzyme $6.1783625 Assay Of Ldh Enzymes $13.0883633 Test Urine For Lactose $9.3283655 Assay Of Lead $12.3883690 Assay Of Lipase $7.0583695 Assay Of Lipoprotein(A) $13.2383700 Lipopro Bld Electrophoretic $11.5183704 Lipoprotein Bld Quan Part $32.2583718 Assay Of Lipoprotein $8.3883719 Assay Of Blood Lipoprotein $11.8983721 Assay Of Blood Lipoprotein $9.7583735 Assay Of Magnesium $6.8583825 Assay Of Mercury $16.6283835 Assay Of Metanephrines $17.3283861 Microfluid Analy Tears $18.6183874 Assay Of Myoglobin $13.2183880 Assay Of Natriuretic Peptide $34.6983930 Assay Of Blood Osmolality $6.7683935 Assay Of Urine Osmolality $6.9783945 Assay Of Oxalate $13.1683970 Assay Of Parathormone $42.1983986 Assay Ph Body Fluid Nos $3.6683987 Exhaled Breath Condensate $3.6684075 Assay Alkaline Phosphatase $5.2984080 Assay Alkaline Phosphatases $15.11
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 24 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
84100 Assay Of Phosphorus $4.8484105 Assay Of Urine Phosphorus $5.2984132 Assay Of Serum Potassium $4.7084133 Assay Of Urine Potassium $4.4084134 Assay Of Prealbumin $14.9184140 Assay Of Pregnenolone $21.1384144 Assay Of Progesterone $21.3384145 Procalcitonin (Pct) $27.3984146 Assay Of Prolactin $19.8184153 Assay Of Psa Total $18.8084154 Assay Of Psa Free $18.8084155 Assay Of Protein Serum $3.7584165 Protein E-Phoresis Serum $10.9884165 Protein E-Phoresis Serum 26 $10.3084166 Protein E-Phoresis/Urine/Csf $18.2284166 Protein E-Phoresis/Urine/Csf 26 $10.3084181 Western Blot Test $17.4084181 Western Blot Test 26 $10.3084182 Protein Western Blot Test $24.1984182 Protein Western Blot Test 26 $10.3084238 Assay Nonendocrine Receptor $37.3884244 Assay Of Renin $22.4884295 Assay Of Serum Sodium $4.9284300 Assay Of Urine Sodium $4.9784305 Assay Of Somatomedin $21.7484402 Assay Of Free Testosterone $26.0484403 Assay Of Total Testosterone $26.3984410 Testosterone Bioavailable $52.4384432 Assay Of Thyroglobulin $16.4284436 Assay Of Total Thyroxine $7.0284439 Assay Of Free Thyroxine $9.2284442 Assay Of Thyroid Activity $15.1184443 Assay Thyroid Stim Hormone $17.1884445 Assay Of Tsi Globulin $51.9884450 Transferase (Ast) (Sgot) $5.2984460 Alanine Amino (Alt) (Sgpt) $5.4284466 Assay Of Transferrin $13.0584478 Assay Of Triglycerides $5.8784479 Assay Of Thyroid (T3 Or T4) $6.6184480 Assay Triiodothyronine (T3) $14.5084481 Free Assay (Ft-3) $17.3284484 Assay Of Troponin Quant $10.3384520 Assay Of Urea Nitrogen $4.0484540 Assay Of Urine/Urea-N $4.8584550 Assay Of Blood/Uric Acid $4.6284560 Assay Of Urine/Uric Acid $4.8584585 Assay Of Urine Vma $15.8484590 Assay Of Vitamin A $11.87
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 25 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
84600 Assay Of Volatiles $16.4484630 Assay Of Zinc $11.6484681 Assay Of C-Peptide $21.2884702 Chorionic Gonadotropin Test $15.3984703 Chorionic Gonadotropin Assay $7.6984704 Hcg Free Betachain Test $15.3984999 Clinical Chemistry Test M85002 Bleeding Time Test $4.6185004 Automated Diff Wbc Count $6.6185007 Bl Smear W/Diff Wbc Count $3.5185008 Bl Smear W/O Diff Wbc Count $3.5185013 Spun Microhematocrit $5.8085014 Hematocrit $2.4385018 Hemoglobin $2.4385025 Complete Cbc W/Auto Diff Wbc $7.9485027 Complete Cbc Automated $6.6185044 Manual Reticulocyte Count $4.4085045 Automated Reticulocyte Count $4.0885046 Reticyte/Hgb Concentrate $5.7085048 Automated Leukocyte Count $2.5985049 Automated Platelet Count $4.5885097 Bone Marrow Interpretation $51.5185220 Blooc Clot Factor V Test $18.0485240 Clot Factor Viii Ahg 1 Stage $18.3085245 Clot Factor Viii Vw Ristoctn $23.4585246 Clot Factor Viii Vw Antigen $23.4585247 Clot Factor Viii Multimetric $23.4585250 Clot Factor Ix Ptc/Chrstmas $19.4785300 Antithrombin Iii Activity $12.1185301 Antithrombin Iii Antigen $11.0585302 Clot Inhibit Prot C Antigen $12.2885303 Clot Inhibit Prot C Activity $14.1485305 Clot Inhibit Prot S Total $11.8785306 Clot Inhibit Prot S Free $15.6785345 Coagulation Time Lee & White $4.4085347 Coagulation Time Activated $4.3685379 Fibrin Degradation Quant $10.4085380 Fibrin Degradj D-Dimer $10.4085384 Fibrinogen Activity $8.6985390 Fibrinolysins Screen I&R $12.8285390 Fibrinolysins Screen I&R 26 $10.3085460 Hemoglobin Fetal $7.9185461 Hemoglobin Fetal $7.7585576 Blood Platelet Aggregation $21.9685576 Blood Platelet Aggregation 26 $10.3085610 Prothrombin Time $4.0285611 Prothrombin Test $4.0385613 Russell Viper Venom Diluted $9.80
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 26 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
85651 Rbc Sed Rate Nonautomated $3.6385652 Rbc Sed Rate Automated $2.7685660 Rbc Sickle Cell Test $5.6385705 Thromboplastin Inhibition $9.8485730 Thromboplastin Time Partial $6.1485732 Thromboplastin Time Partial $6.6185810 Blood Viscosity Examination $11.9385999 Hematology Procedure M86003 Allg Spec Ige Crude Xtrc Ea $5.3386005 Allg Spec Ige Multiallg Scr $8.1586008 Allg Spec Ige Recomb Ea $18.3386038 Antinuclear Antibodies $12.3586060 Antistreptolysin O Titer $7.4686063 Antistreptolysin O Screen $5.9086140 C-Reactive Protein $5.2986141 C-Reactive Protein Hs $13.2386148 Anti-Phospholipid Antibody $16.4386153 Cell Enumeration Phys Interp 26 $19.4186162 Complement Total (Ch50) $20.7786200 Ccp Antibody $13.2386215 Deoxyribonuclease Antibody $13.5486225 Dna Antibody Native $14.0586235 Nuclear Antigen Antibody $18.3386255 Fluorescent Antibody Screen $12.3286255 Fluorescent Antibody Screen 26 $10.3086256 Fluorescent Antibody Titer $12.3286256 Fluorescent Antibody Titer 26 $10.3086300 Immunoassay Tumor Ca 15-3 $21.2886304 Immunoassay Tumor Ca 125 $21.2886308 Heterophile Antibody Screen $5.2986316 Immunoassay Tumor Other $21.2886318 Immunoassay Infectious Agent $14.9886320 Serum Immunoelectrophoresis $24.7786320 Serum Immunoelectrophoresis 26 $10.3086325 Other Immunoelectrophoresis $22.8686325 Other Immunoelectrophoresis 26 $10.3086334 Immunofix E-Phoresis Serum $22.8486334 Immunofix E-Phoresis Serum 26 $10.3086335 Immunfix E-Phorsis/Urine/Csf $30.0086335 Immunfix E-Phorsis/Urine/Csf 26 $10.3086337 Insulin Antibodies $21.8886340 Intrinsic Factor Antibody $15.4186341 Islet Cell Antibody $20.2386356 Mononuclear Cell Antigen $27.3786386 Nuclear Matrix Protein 22 $18.0386403 Particle Agglut Antbdy Scrn $10.4286430 Rheumatoid Factor Test Qual $5.8086431 Rheumatoid Factor Quant $5.80
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 27 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
86481 Tb Ag Response T-Cell Susp $82.8086485 Skin Test Candida $6.5586486 Skin Test Nos Antigen $2.7786510 Histoplasmosis Skin Test $3.5786580 Tb Intradermal Test $4.5686592 Syphilis Test Non-Trep Qual $4.3686593 Syphilis Test Non-Trep Quant $4.5086701 Hiv-1antibody $9.0886702 Hiv-2 Antibody $13.8286703 Hiv-1/Hiv-2 1 Result Antbdy $14.0186704 Hep B Core Antibody Total $12.3286705 Hep B Core Antibody Igm $12.0486706 Hep B Surface Antibody $10.9886707 Hepatitis Be Antibody $11.8286708 Hepatitis A Antibody $12.6686778 Toxoplasma Antibody Igm $14.7286780 Treponema Pallidum $13.5386803 Hepatitis C Ab Test $14.5886804 Hep C Ab Test Confirm $15.8486812 Hla Typing A B Or C $26.3886813 Hla Typing A B Or C $59.2886849 Immunology Procedure M86850 Rbc Antibody Screen $8.0986880 Coombs Test Direct $5.5186886 Coombs Test Indirect Titer $5.2986900 Blood Typing Serologic Abo $3.0686901 Blood Typing Serologic Rh(D) $3.0687045 Feces Culture Aerobic Bact $9.6587070 Culture Othr Specimn Aerobic $8.8187075 Cultr Bacteria Except Blood $9.6887076 Culture Anaerobe Ident Each $8.2687077 Culture Aerobic Identify $8.2687081 Culture Screen Only $6.7787084 Culture Of Specimen By Kit $22.4187086 Urine Culture/Colony Count $8.2587088 Urine Bacteria Culture $8.2787101 Skin Fungi Culture $7.8787102 Fungus Isolation Culture $8.5987106 Fungi Identification Yeast $10.5587109 Mycoplasma $15.7387110 Chlamydia Culture $20.0387116 Mycobacteria Culture $11.0587140 Culture Type Immunofluoresc $5.7087147 Culture Type Immunologic $5.2987177 Ova And Parasites Smears $9.1087181 Microbe Susceptible Diffuse $4.8587184 Microbe Susceptible Disk $7.0587186 Microbe Susceptible Mic $8.83
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 28 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
87205 Smear Gram Stain $4.3687206 Smear Fluorescent/Acid Stai $5.5187207 Smear Special Stain $6.1387207 Smear Special Stain 26 $10.3087209 Smear Complex Stain $18.3787210 Smear Wet Mount Saline/Ink $4.8287220 Tissue Exam For Fungi $4.3687252 Virus Inoculation Tissue $26.6587255 Genet Virus Isolate Hsv $34.6287270 Chlamydia Trachomatis Ag If $12.2587272 Cryptosporidium Ag If $12.2587276 Influenza A Ag If $13.3187280 Respiratory Syncytial Ag If $12.2587299 Antibody Detection Nos If $13.3387324 Clostridium Ag Ia $12.2587328 Cryptosporidium Ag Ia $12.2587338 Hpylori Stool Ia $14.7187340 Hepatitis B Surface Ag Ia $10.5687350 Hepatitis Be Ag Ia $11.7887380 Hepatitis Delta Ag Ia $16.7887389 Hiv-1 Ag W/Hiv-1 & Hiv-2 Ab $24.6287390 Hiv-1 Ag Ia $19.9287391 Hiv-2 Ag Ia $18.1387420 Resp Syncytial Ag Ia $12.2587425 Rotavirus Ag Ia $12.2587430 Strep A Ag Ia $13.9287449 Ag Detect Nos Ia Mult $12.2587450 Ag Detect Nos Ia Single $9.8087661 Trichomonas Vaginalis Amplif $35.8887804 Influenza Assay W/Optic $13.7087807 Rsv Assay W/Optic $12.2587808 Trichomonas Assay W/Optic $12.6687809 Adenovirus Assay W/Optic $18.0287810 Chylmd Trach Assay W/Optic $29.2287850 N. Gonorrhoeae Assay W/Optic $20.3487880 Strep A Assay W/Optic $13.6987905 Sialidase Enzyme Assay $12.4988141 Cytopath C/V Interpret $18.2388142 Cytopath C/V Thin Layer $20.7188143 Cytopath C/V Thin Layer Redo $20.7188147 Cytopath C/V Automated $41.8688148 Cytopath C/V Auto Rescreen $15.5388155 Cytopath C/V Index Add-On $12.1388164 Cytopath Tbs C/V Manual $12.1388165 Cytopath Tbs C/V Redo $34.9688166 Cytopath Tbs C/V Auto Redo $12.1388167 Cytopath Tbs C/V Select $12.1388174 Cytopath C/V Auto In Fluid $21.84
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 29 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
88175 Cytopath C/V Auto Fluid Redo $27.0888187 Flowcytometry/Read 2-8 $26.5588188 Flowcytometry/Read 9-15 $36.6588189 Flowcytometry/Read 16 & > $48.9388233 Tissue Culture Skin/Biopsy $143.8688237 Tissue Culture Bone Marrow $129.1188262 Chromosome Analysis 15-20 $127.4188264 Chromosome Analysis 20-25 $127.4188271 Cytogenetics Dna Probe $21.8988274 Cytogenetics 25-99 $35.5988275 Cytogenetics 100-300 $42.3988291 Cyto/Molecular Report $18.6288299 Cytogenetic Study M88371 Protein Western Blot Tissue $22.7288371 Protein Western Blot Tissue 26 $10.3088738 Hgb Quant Transcutaneous $5.1389050 Body Fluid Cell Count $4.8389051 Body Fluid Cell Count $5.6389055 Leukocyte Assessment Fecal $4.3689060 Exam Synovial Fluid Crystals $7.3189060 Exam Synovial Fluid Crystals 26 $10.3089190 Nasal Smear For Eosinophils $4.8589220 Sputum Specimen Collection $9.1189230 Collect Sweat For Test $1.9890281 Human Ig Im M90283 Human Ig Iv M90284 Human Ig Sc M90296 Diphtheria Antitoxin M90371 Hep B Ig Im $117.1290375 Rabies Ig Im/Sc $295.8290376 Rabies Ig Heat Treated $305.4490378 Rsv Mab Im 50mg M90384 Rh Ig Full-Dose Im $125.0890385 Rh Ig Minidose Im $58.6290396 Varicella-Zoster Ig Im M90399 Immune Globulin M90460 Im Admin 1st/Only Component $7.0090461 Im Admin Each Addl Component $0.0090471 Immunization Admin $7.0090472 Immunization Admin Each Add $7.0090473 Immune Admin Oral/Nasal $3.0090474 Immune Admin Oral/Nasal Addl $3.0090620 Menb-4c Vacc 2 Dose Im 10 to 19 years $0.0090620 Menb-4c Vacc 2 Dose Im 19 to 26 years $169.6090621 Menb-Fhbp Vacc 2/3 Dose Im 10 to 19 years $0.0090621 Menb-Fhbp Vacc 2/3 Dose Im 19 to 26 years $121.9090630 Flu Vacc Iiv4 No Preserv Id $20.3490632 Hepa Vaccine Adult Im $56.69
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 30 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
90633 Hepa Vacc Ped/Adol 2 Dose Im $0.0090636 Hep A/Hep B Vacc Adult Im $96.4690644 Hib-Mency Vacc 6wk-18m0 Im $0.0090647 Hib Prp-Omp Vacc 3 Dose Im $0.0090648 Hib Prp-T Vaccine 4 Dose Im $0.0090651 9vhpv Vaccine 2/3 Dose Im 19 to 27 years $172.0890651 9vhpv Vaccine 2/3 Dose Im 9 to 19 years $0.0090653 Iiv Adjuvant Vaccine Im $54.67 Effective: 08/01/201890654 Flu Vacc Iiv3 No Preserv Id $18.9290655 Iiv3 Vacc No Prsv 0.25 Ml Im $0.0090656 Iiv3 Vacc No Prsv 0.5 Ml Im 19 to 124 years $19.77 Effective: 08/01/201890656 Iiv3 Vacc No Prsv 0.5 Ml Im 3 to 19 years $0.0090657 Iiv3 Vaccine Splt 0.25 Ml Im $6.0290658 Iiv3 Vaccine Splt 0.5 Ml Im $11.3790661 Cciiv3 Vac No Prsv 0.5 Ml Im $22.2990662 Iiv No Prsv Increased Ag Im $53.37 Effective: 08/01/201890670 Pcv13 Vaccine Im 19 to 124 years $205.1190670 Pcv13 Vaccine Im 42 days to 19 years $0.0090673 Riv3 Vaccine No Preserv Im $40.6190674 Cciiv4 Vac No Prsv 0.5 Ml Im 19 to 124 years $24.0590674 Cciiv4 Vac No Prsv 0.5 Ml Im 4 to 19 years $0.0090675 Rabies Vaccine Im $288.9690676 Rabies Vaccine Id $287.5590680 Rv5 Vacc 3 Dose Live Oral $0.0090681 Rv1 Vacc 2 Dose Live Oral $0.0090682 Riv4 Vacc Recombinant Dna Im $53.37 Effective: 08/01/201890685 Iiv4 Vacc No Prsv 0.25 Ml Im $0.0090686 Iiv4 Vacc No Prsv 0.5 Ml Im 19 to 124 years $19.0390686 Iiv4 Vacc No Prsv 0.5 Ml Im 6 months to 19 years $0.0090687 Iiv4 Vaccine Splt 0.25 Ml Im $0.0090688 Iiv4 Vaccine Splt 0.5 Ml Im 19 to 124 years $17.8490688 Iiv4 Vaccine Splt 0.5 Ml Im 6 months to 19 years $0.0090691 Typhoid Vaccine Im $111.5290696 Dtap-Ipv Vaccine 4-6 Yrs Im $0.0090698 Dtap-Ipv/Hib Vaccine Im $0.0090700 Dtap Vaccine < 7 Yrs Im $0.0090702 Dt Vaccine Under 7 Yrs Im $0.0090707 Mmr Vaccine Sc 1 to 19 years $0.0090707 Mmr Vaccine Sc 19 to 124 years $53.1790710 Mmrv Vaccine Sc $0.0090713 Poliovirus Ipv Sc/Im 19 to 124 years $29.0990713 Poliovirus Ipv Sc/Im 42 days to 19 years $0.0090714 Td Vacc No Presv 7 Yrs+ Im 19 to 124 years $23.7290714 Td Vacc No Presv 7 Yrs+ Im 7 to 19 years $0.0090715 Tdap Vaccine 7 Yrs/> Im 19 to 124 years $30.9590715 Tdap Vaccine 7 Yrs/> Im 7 to 19 years $0.0090716 Var Vaccine Live Subq 1 to 19 years $0.0090716 Var Vaccine Live Subq 19 to 124 years $88.10
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 31 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
90717 Yellow Fever Vaccine Subq $91.0690723 Dtap-Hep B-Ipv Vaccine Im $0.0090732 Ppsv23 Vacc 2 Yrs+ Subq/Im 19 to 124 years $107.7590732 Ppsv23 Vacc 2 Yrs+ Subq/Im 2 to 19 years $0.0090734 Mcv4 Menacwy Vaccine Im 19 to 56 years $122.5090734 Mcv4 Menacwy Vaccine Im 2 months to 19 years $0.0090736 Hzv Vaccine Live Subq $208.9590739 Hepb Vacc 2 Dose Adult Im $131.1090740 Hepb Vacc 3 Dose Immunsup Im $130.2590744 Hepb Vacc 3 Dose Ped/Adol Im 0 to 19 years $0.0090744 Hepb Vacc 3 Dose Ped/Adol Im 19 to 20 years $26.1490746 Hepb Vaccine 3 Dose Adult Im $65.1290747 Hepb Vacc 4 Dose Immunsup Im $130.2590749 Vaccine Toxoid M90750 Hzv Vacc Recombinant Im $148.4090756 Cciiv4 Vacc Abx Free Im 19 to 124 years $22.7990756 Cciiv4 Vacc Abx Free Im 4 to 19 years $0.0090785 Psytx Complex Interactive $8.1290791 Psych Diagnostic Evaluation $75.0890792 Psych Diag Eval W/Med Srvcs $83.9990832 Psytx W Pt 30 Minutes $36.4590833 Psytx W Pt W E/M 30 Min $38.0490834 Psytx W Pt 45 Minutes $48.7390836 Psytx W Pt W E/M 45 Min $47.9490837 Psytx W Pt 60 Minutes $73.1090838 Psytx W Pt W E/M 60 Min $63.3990839 Psytx Crisis Initial 60 Min $76.2790840 Psytx Crisis Ea Addl 30 Min $36.4590847 Family Psytx W/Pt 50 Min $61.2190853 Group Psychotherapy $14.6690887 Consultation With Family $49.5392002 Eye Exam New Patient $46.7592004 Eye Exam New Patient $84.5992012 Eye Exam Establish Patient $49.1392014 Eye Exam&Tx Estab Pt 1/>Vst $70.7292015 Determine Refractive State $11.0992020 Special Eye Evaluation $15.0692025 Corneal Topography $21.3992025 Corneal Topography 26 $11.2992025 Corneal Topography TC $10.1092060 Special Eye Evaluation $36.4592060 Special Eye Evaluation 26 $21.5992060 Special Eye Evaluation TC $14.8692065 Orthoptic/Pleoptic Training $30.3192065 Orthoptic/Pleoptic Training 26 $10.1092065 Orthoptic/Pleoptic Training TC $20.2192071 Contact Lens Fitting For Tx $21.2092072 Fit Contac Lens For Managmnt $74.68
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 32 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
92081 Visual Field Examination(S) $19.4192081 Visual Field Examination(S) 26 $9.3192081 Visual Field Examination(S) TC $10.1092082 Visual Field Examination(S) $27.1492082 Visual Field Examination(S) 26 $12.2892082 Visual Field Examination(S) TC $14.8692083 Visual Field Examination(S) $36.0592083 Visual Field Examination(S) 26 $15.6592083 Visual Field Examination(S) TC $20.4092100 Serial Tonometry Exam(S) $45.5692132 Cmptr Ophth Dx Img Ant Segmt $17.6392132 Cmptr Ophth Dx Img Ant Segmt 26 $9.3192132 Cmptr Ophth Dx Img Ant Segmt TC $8.3292133 Cmptr Ophth Img Optic Nerve $21.2092133 Cmptr Ophth Img Optic Nerve 26 $12.6892133 Cmptr Ophth Img Optic Nerve TC $8.5292134 Cptr Ophth Dx Img Post Segmt $23.3892134 Cptr Ophth Dx Img Post Segmt 26 $14.6692134 Cptr Ophth Dx Img Post Segmt TC $8.7292136 Ophthalmic Biometry $44.1892136 Ophthalmic Biometry 26 $17.6392136 Ophthalmic Biometry TC $26.5592145 Corneal Hysteresis Deter $9.9192145 Corneal Hysteresis Deter 26 $5.3592145 Corneal Hysteresis Deter TC $4.5692225 Special Eye Exam Initial $15.2592226 Special Eye Exam Subsequent $14.0792227 Remote Dx Retinal Imaging $8.3292228 Remote Retinal Imaging Mgmt $19.0292228 Remote Retinal Imaging Mgmt 26 $11.4992228 Remote Retinal Imaging Mgmt TC $7.5392230 Eye Exam With Photos $32.4992235 Fluorescein Angrph Uni/Bi $48.3492235 Fluorescein Angrph Uni/Bi 26 $24.5692235 Fluorescein Angrph Uni/Bi TC $23.7792240 Icg Angiography Uni/Bi $117.8792240 Icg Angiography Uni/Bi 26 $26.3592240 Icg Angiography Uni/Bi TC $91.5292242 Fluorescein Icg Angiography $128.3792242 Fluorescein Icg Angiography 26 $30.9092242 Fluorescein Icg Angiography TC $97.4792250 Eye Exam With Photos $32.0992250 Eye Exam With Photos 26 $12.2892250 Eye Exam With Photos TC $19.8192260 Ophthalmoscopy/Dynamometry $10.3092265 Eye Muscle Evaluation $49.5392265 Eye Muscle Evaluation 26 $26.5592265 Eye Muscle Evaluation TC $22.98
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 33 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
92270 Electro-Oculography $52.3092270 Electro-Oculography 26 $23.1892270 Electro-Oculography TC $29.1292275 Electroretinography $84.1992275 Electroretinography 26 $30.7192275 Electroretinography TC $53.4992283 Color Vision Examination $30.9092283 Color Vision Examination 26 $5.1592283 Color Vision Examination TC $25.7592284 Dark Adaptation Eye Exam $35.2692284 Dark Adaptation Eye Exam 26 $7.1392284 Dark Adaptation Eye Exam TC $28.1392285 Eye Photography $11.6992285 Eye Photography 26 $1.7892285 Eye Photography TC $9.9192286 Internal Eye Photography $21.5992286 Internal Eye Photography 26 $12.4892286 Internal Eye Photography TC $9.1192287 Internal Eye Photography $77.8592287 Internal Eye Photography 26 $26.3592287 Internal Eye Photography TC $51.5192310 Contact Lens Fitting $54.6892311 Contact Lens Fitting $57.2592312 Contact Lens Fitting $66.3692313 Contact Lens Fitting $54.2892326 Replacement Of Contact Lens $20.6092340 Fit Spectacles Monofocal $20.0192341 Fit Spectacles Bifocal $22.9892342 Fit Spectacles Multifocal $24.5692352 Fit Aphakia Spectcl Monofocl $22.7892353 Fit Aphakia Spectcl Multifoc $26.5592370 Repair & Adjust Spectacles $17.4392371 Repair & Adjust Spectacles $6.5492507 Speech/Hearing Therapy $43.9892508 Speech/Hearing Therapy $12.8892511 Nasopharyngoscopy $61.2192520 Laryngeal Function Studies $43.1992521 Evaluation Of Speech Fluency $63.9992522 Evaluate Speech Production $51.5192523 Speech Sound Lang Comprehen $110.9492524 Behavral Qualit Analys Voice $49.3392526 Oral Function Therapy $48.1492537 Caloric Vstblr Test W/Rec $22.7892537 Caloric Vstblr Test W/Rec 26 $17.8392537 Caloric Vstblr Test W/Rec TC $4.9592538 Caloric Vstblr Test W/Rec $11.6992538 Caloric Vstblr Test W/Rec 26 $8.9192538 Caloric Vstblr Test W/Rec TC $2.77
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 34 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
92541 Spontaneous Nystagmus Test $13.8792541 Spontaneous Nystagmus Test 26 $11.8992541 Spontaneous Nystagmus Test TC $1.9892542 Positional Nystagmus Test $15.8592542 Positional Nystagmus Test 26 $14.0792542 Positional Nystagmus Test TC $1.7892544 Optokinetic Nystagmus Test $9.5192544 Optokinetic Nystagmus Test 26 $8.1292544 Optokinetic Nystagmus Test TC $1.3992545 Oscillating Tracking Test $8.9192545 Oscillating Tracking Test 26 $7.5392545 Oscillating Tracking Test TC $1.3992546 Sinusoidal Rotational Test $58.6492546 Sinusoidal Rotational Test 26 $8.5292546 Sinusoidal Rotational Test TC $50.1292547 Supplemental Electrical Test $3.3792548 Posturography $55.4792548 Posturography 26 $14.6692548 Posturography TC $40.8192550 Tympanometry & Reflex Thresh $12.0892551 Pure Tone Hearing Test Air $6.9392552 Pure Tone Audiometry Air $17.8392553 Audiometry Air & Bone $21.3992555 Speech Threshold Audiometry $13.4792556 Speech Audiometry Complete $21.3992557 Comprehensive Hearing Test $21.2092561 Bekesy Audiometry Diagnosis $21.9992562 Loudness Balance Test $26.1592563 Tone Decay Hearing Test $17.4392564 Sisi Hearing Test $14.6692565 Stenger Test Pure Tone $8.7292567 Tympanometry $8.1292568 Acoustic Refl Threshold Tst $8.9192570 Acoustic Immitance Testing $18.0392571 Filtered Speech Hearing Test $15.4592575 Sensorineural Acuity Test $26.5592576 Synthetic Sentence Test $21.2092577 Stenger Test Speech $8.1292579 Visual Audiometry (Vra) $25.7592582 Conditioning Play Audiometry $38.2392587 Evoked Auditory Test Limited $12.0892587 Evoked Auditory Test Limited 26 $10.3092587 Evoked Auditory Test Limited TC $1.7892588 Evoked Auditory Tst Complete $18.4292588 Evoked Auditory Tst Complete 26 $16.2492588 Evoked Auditory Tst Complete TC $2.1892590 Hearing Aid Exam One Ear $45.0292591 Hearing Aid Exam Both Ears $45.02
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 35 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
92594 Electro Hearng Aid Test One $13.0492595 Electro Hearng Aid Tst Both $26.1092597 Oral Speech Device Eval $40.4192601 Cochlear Implt F/Up Exam <7 $92.7192602 Reprogram Cochlear Implt <7 $57.4592603 Cochlear Implt F/Up Exam 7/> $85.9892604 Reprogram Cochlear Implt 7/> $50.9192607 Ex For Speech Device Rx 1hr $73.5092608 Ex For Speech Device Rx Addl $29.5292609 Use Of Speech Device Service $61.6192610 Evaluate Swallowing Function $48.1492612 Endoscopy Swallow (Fees) Vid $107.1792614 Laryngoscopic Sensory Vid $81.0292616 Fees W/Laryngeal Sense Test $116.0992625 Tinnitus Assessment $39.4292626 Eval Aud Rehab Status $50.5292627 Eval Aud Status Rehab Add-On $12.6892630 Aud Rehab Pre-Ling Hear Loss $32.6892633 Aud Rehab Postling Hear Loss $32.6892700 Ent Procedure/Service M92950 Heart/Lung Resuscitation Cpr $171.1692960 Cardioversion Electric Ext $89.7493000 Electrocardiogram Complete $9.5193005 Electrocardiogram Tracing $4.7593010 Electrocardiogram Report $4.7593040 Rhythm Ecg With Report $7.1393041 Rhythm Ecg Tracing $3.1793042 Rhythm Ecg Report $3.9693224 Ecg Monit/Reprt Up To 48 Hrs $51.1193225 Ecg Monit/Reprt Up To 48 Hrs $14.8693226 Ecg Monit/Reprt Up To 48 Hrs $21.2093227 Ecg Monit/Reprt Up To 48 Hrs $15.0693228 Remote 30 Day Ecg Rev/Report $14.6693229 Remote 30 Day Ecg Tech Supp $409.0893260 Prgrmg Dev Eval Impltbl Sys $36.6593260 Prgrmg Dev Eval Impltbl Sys 26 $24.3793260 Prgrmg Dev Eval Impltbl Sys TC $12.2893261 Interrogate Subq Defib $33.2893261 Interrogate Subq Defib 26 $21.2093261 Interrogate Subq Defib TC $12.0893268 Ecg Record/Review $115.4993270 Remote 30 Day Ecg Rev/Report $5.1593271 Ecg/Monitoring And Analysis $96.0893272 Ecg/Review Interpret Only $14.2693278 Ecg/Signal-Averaged $17.4393278 Ecg/Signal-Averaged 26 $7.1393278 Ecg/Signal-Averaged TC $10.3093279 Pm Device Progr Eval Sngl $27.73
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 36 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
93279 Pm Device Progr Eval Sngl 26 $18.2393279 Pm Device Progr Eval Sngl TC $9.5193280 Pm Device Progr Eval Dual $32.6993280 Pm Device Progr Eval Dual 26 $21.5993280 Pm Device Progr Eval Dual TC $11.0993281 Pm Device Progr Eval Multi $35.4693281 Pm Device Progr Eval Multi 26 $24.1793281 Pm Device Progr Eval Multi TC $11.2993282 Prgrmg Eval Implantable Dfb $34.2793282 Prgrmg Eval Implantable Dfb 26 $23.9793282 Prgrmg Eval Implantable Dfb TC $10.3093283 Prgrmg Eval Implantable Dfb $43.7893283 Prgrmg Eval Implantable Dfb 26 $32.4993283 Prgrmg Eval Implantable Dfb TC $11.2993284 Prgrmg Eval Implantable Dfb $47.7493284 Prgrmg Eval Implantable Dfb 26 $35.4693284 Prgrmg Eval Implantable Dfb TC $12.2893285 Ilr Device Eval Progr $23.9793285 Ilr Device Eval Progr 26 $14.8693285 Ilr Device Eval Progr TC $9.1193286 Peri-Px Pacemaker Device Evl $16.8493286 Peri-Px Pacemaker Device Evl 26 $8.5293286 Peri-Px Pacemaker Device Evl TC $8.3293287 Peri-Px Device Eval & Prgr $21.3993287 Peri-Px Device Eval & Prgr 26 $13.0793287 Peri-Px Device Eval & Prgr TC $8.3293288 Pm Device Eval In Person $21.5993288 Pm Device Eval In Person 26 $12.0893288 Pm Device Eval In Person TC $9.5193289 Interrog Device Eval Heart $30.5193289 Interrog Device Eval Heart 26 $21.0093289 Interrog Device Eval Heart TC $9.5193290 Icm Device Eval $20.6093290 Icm Device Eval 26 $12.2893290 Icm Device Eval TC $8.3293291 Ilr Device Interrogate $18.4293291 Ilr Device Interrogate 26 $10.3093291 Ilr Device Interrogate TC $8.1293292 Wcd Device Interrogate $20.6093292 Wcd Device Interrogate 26 $12.0893292 Wcd Device Interrogate TC $8.5293293 Pm Phone R-Strip Device Eval $29.9193293 Pm Phone R-Strip Device Eval 26 $8.5293293 Pm Phone R-Strip Device Eval TC $21.3993294 Pm Device Interrogate Remote $17.2393295 Dev Interrog Remote 1/2/Mlt $30.9093296 Pm/Icd Remote Tech Serv $14.8693297 Icm Device Interrogat Remote $14.86
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 37 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
93298 Ilr Device Interrogat Remote $15.0693299 Icm/Ilr Remote Tech Serv $72.9793303 Echo Transthoracic $135.7093303 Echo Transthoracic 26 $35.8693303 Echo Transthoracic TC $99.8493304 Echo Transthoracic $90.3393304 Echo Transthoracic 26 $20.6093304 Echo Transthoracic TC $69.7393306 Tte W/Doppler Complete $117.6793306 Tte W/Doppler Complete 26 $41.2093306 Tte W/Doppler Complete TC $76.4793307 Tte W/O Doppler Complete $80.0393307 Tte W/O Doppler Complete 26 $25.3693307 Tte W/O Doppler Complete TC $54.6893308 Tte F-Up Or Lmtd $59.4393308 Tte F-Up Or Lmtd 26 $14.4693308 Tte F-Up Or Lmtd TC $44.9793320 Doppler Echo Exam Heart $30.5193320 Doppler Echo Exam Heart 26 $10.3093320 Doppler Echo Exam Heart TC $20.2193321 Doppler Echo Exam Heart $15.4593321 Doppler Echo Exam Heart 26 $4.1693321 Doppler Echo Exam Heart TC $11.2993325 Doppler Color Flow Add-On $14.4693325 Doppler Color Flow Add-On 26 $1.7893325 Doppler Color Flow Add-On TC $12.6893350 Stress Tte Only $116.6893350 Stress Tte Only 26 $40.0293350 Stress Tte Only TC $76.6693668 Peripheral Vascular Rehab $10.9093880 Extracranial Bilat Study $115.1093880 Extracranial Bilat Study 26 $22.5893880 Extracranial Bilat Study TC $92.5193922 Upr/L Xtremity Art 2 Levels $49.7293922 Upr/L Xtremity Art 2 Levels 26 $7.1393922 Upr/L Xtremity Art 2 Levels TC $42.5993923 Upr/Lxtr Art Stdy 3+ Lvls $77.0693923 Upr/Lxtr Art Stdy 3+ Lvls 26 $12.4893923 Upr/Lxtr Art Stdy 3+ Lvls TC $64.5893924 Lwr Xtr Vasc Stdy Bilat $95.8893924 Lwr Xtr Vasc Stdy Bilat 26 $13.8793924 Lwr Xtr Vasc Stdy Bilat TC $82.0193925 Lower Extremity Study $147.5893925 Lower Extremity Study 26 $22.3993925 Lower Extremity Study TC $125.2093926 Lower Extremity Study $86.3793926 Lower Extremity Study 26 $13.6793926 Lower Extremity Study TC $72.70
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 38 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
93930 Upper Extremity Study $118.2793930 Upper Extremity Study 26 $22.5893930 Upper Extremity Study TC $95.6893931 Upper Extremity Study $73.5093931 Upper Extremity Study 26 $13.8793931 Upper Extremity Study TC $59.6393970 Extremity Study $111.1393970 Extremity Study 26 $19.4193970 Extremity Study TC $91.7293971 Extremity Study $68.1593971 Extremity Study 26 $12.6893971 Extremity Study TC $55.4793975 Vascular Study $160.0693975 Vascular Study 26 $32.6993975 Vascular Study TC $127.3893976 Vascular Study $93.1193976 Vascular Study 26 $22.3993976 Vascular Study TC $70.7293978 Vascular Study $108.5693978 Vascular Study 26 $22.3993978 Vascular Study TC $86.1793979 Vascular Study $68.5493979 Vascular Study 26 $14.0793979 Vascular Study TC $54.4893980 Penile Vascular Study $71.1293980 Penile Vascular Study 26 $34.8793980 Penile Vascular Study TC $36.2593981 Penile Vascular Study $43.3893981 Penile Vascular Study 26 $12.2893981 Penile Vascular Study TC $31.1094010 Breathing Capacity Test $20.2194010 Breathing Capacity Test 26 $4.7594010 Breathing Capacity Test TC $15.4594060 Evaluation Of Wheezing $34.0794060 Evaluation Of Wheezing 26 $7.3394060 Evaluation Of Wheezing TC $26.7494070 Evaluation Of Wheezing $34.0794070 Evaluation Of Wheezing 26 $16.2494070 Evaluation Of Wheezing TC $17.8394150 Vital Capacity Test $14.4694150 Vital Capacity Test 26 $2.1894150 Vital Capacity Test TC $12.2894200 Lung Function Test (Mbc/Mvv) $15.4594200 Lung Function Test (Mbc/Mvv) 26 $3.1794200 Lung Function Test (Mbc/Mvv) TC $12.2894250 Expired Gas Collection $15.8594250 Expired Gas Collection 26 $3.1794250 Expired Gas Collection TC $12.68
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 39 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
94375 Respiratory Flow Volume Loop $22.3994375 Respiratory Flow Volume Loop 26 $8.3294375 Respiratory Flow Volume Loop TC $14.0794400 Co2 Breathing Response Curve $32.4994400 Co2 Breathing Response Curve 26 $11.0994400 Co2 Breathing Response Curve TC $21.3994450 Hypoxia Response Curve $40.2194450 Hypoxia Response Curve 26 $11.2994450 Hypoxia Response Curve TC $28.9294617 Exercise Tst Brncspsm $53.4994617 Exercise Tst Brncspsm 26 $18.8294617 Exercise Tst Brncspsm TC $34.6794618 Pulmonary Stress Testing $19.2294618 Pulmonary Stress Testing 26 $12.8894618 Pulmonary Stress Testing TC $6.3494621 Cardiopulm Exercise Testing $92.7194621 Cardiopulm Exercise Testing 26 $38.8394621 Cardiopulm Exercise Testing TC $53.8894640 Airway Inhalation Treatment $10.5094667 Chest Wall Manipulation $15.0694668 Chest Wall Manipulation $18.0394669 Mechanical Chest Wall Oscill $18.4294680 Exhaled Air Analysis O2 $32.8894680 Exhaled Air Analysis O2 26 $7.1394680 Exhaled Air Analysis O2 TC $25.7594681 Exhaled Air Analysis O2/Co2 $32.0994681 Exhaled Air Analysis O2/Co2 26 $5.7494681 Exhaled Air Analysis O2/Co2 TC $26.3594690 Exhaled Air Analysis $31.3094690 Exhaled Air Analysis 26 $2.1894690 Exhaled Air Analysis TC $29.1294726 Pulm Funct Tst Plethysmograp $30.9094726 Pulm Funct Tst Plethysmograp 26 $6.9394726 Pulm Funct Tst Plethysmograp TC $23.9794727 Pulm Function Test By Gas $24.7694727 Pulm Function Test By Gas 26 $6.9394727 Pulm Function Test By Gas TC $17.8394728 Pulm Funct Test Oscillometry $23.1894728 Pulm Funct Test Oscillometry 26 $7.1394728 Pulm Funct Test Oscillometry TC $16.0594729 Co/Membane Diffuse Capacity $30.7194729 Co/Membane Diffuse Capacity 26 $5.1594729 Co/Membane Diffuse Capacity TC $25.5594750 Pulmonary Compliance Study $46.3694750 Pulmonary Compliance Study 26 $6.1494750 Pulmonary Compliance Study TC $40.2194772 Breath Recording Infant M94772 Breath Recording Infant 26 $40.54
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 40 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
94772 Breath Recording Infant TC M94776 Ped Home Apnea Rec Downld $93.0394777 Ped Home Apnea Rec Report $30.6595004 Percut Allergy Skin Tests $2.9795012 Exhaled Nitric Oxide Meas $11.2995017 Perq & Icut Allg Test Venoms $4.3695018 Perq&Ic Allg Test Drugs/Biol $11.8995024 Icut Allergy Test Drug/Bug $4.5695027 Icut Allergy Titrate-Airborn $2.5895028 Icut Allergy Test-Delayed $7.3395044 Allergy Patch Tests $3.1795052 Photo Patch Test $3.7695056 Photosensitivity Tests $25.7595060 Eye Allergy Tests $19.8195065 Nose Allergy Test $14.0795070 Bronchial Allergy Tests $17.4395071 Bronchial Allergy Tests $19.8195076 Ingest Challenge Ini 120 Min $67.1695079 Ingest Challenge Addl 60 Min $47.1595115 Immunotherapy One Injection $4.9595117 Immunotherapy Injections $5.7495145 Antigen Therapy Services $14.4695146 Antigen Therapy Services $26.5595147 Antigen Therapy Services $28.3395148 Antigen Therapy Services $40.4195149 Antigen Therapy Services $53.0995165 Antigen Therapy Services $7.3395180 Rapid Desensitization $76.4795199 Allergy Immunology Services M95249 Cont Gluc Mntr Pt Prov Eqp $30.9095250 Cont Gluc Mntr Phys/Qhp Eqp $86.1795251 Cont Gluc Mntr Analysis I&R $20.2195812 Eeg 41-60 Minutes $181.4695812 Eeg 41-60 Minutes 26 $32.6995812 Eeg 41-60 Minutes TC $148.7795813 Eeg Over 1 Hour $228.0195813 Eeg Over 1 Hour 26 $48.9395813 Eeg Over 1 Hour TC $179.0895816 Eeg Awake And Drowsy $204.6495816 Eeg Awake And Drowsy 26 $32.6995816 Eeg Awake And Drowsy TC $171.9595819 Eeg Awake And Asleep $237.9295819 Eeg Awake And Asleep 26 $32.6995819 Eeg Awake And Asleep TC $205.2395822 Eeg Coma Or Sleep Only $214.3495822 Eeg Coma Or Sleep Only 26 $32.6995822 Eeg Coma Or Sleep Only TC $181.6695824 Eeg Cerebral Death Only M
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 41 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
95824 Eeg Cerebral Death Only 26 $22.3995824 Eeg Cerebral Death Only TC M95827 Eeg All Night Recording $352.4295827 Eeg All Night Recording 26 $31.8995827 Eeg All Night Recording TC $320.5395851 Range Of Motion Measurements $11.2995852 Range Of Motion Measurements $10.3095857 Cholinesterase Challenge $30.3195860 Muscle Test One Limb $69.3495860 Muscle Test One Limb 26 $29.3295860 Muscle Test One Limb TC $40.0295861 Muscle Test 2 Limbs $98.2695861 Muscle Test 2 Limbs 26 $46.7595861 Muscle Test 2 Limbs TC $51.5195863 Muscle Test 3 Limbs $125.4095863 Muscle Test 3 Limbs 26 $56.4695863 Muscle Test 3 Limbs TC $68.9495864 Muscle Test 4 Limbs $140.2595864 Muscle Test 4 Limbs 26 $60.2295864 Muscle Test 4 Limbs TC $80.0395865 Muscle Test Larynx $82.8195865 Muscle Test Larynx 26 $47.3595865 Muscle Test Larynx TC $35.4695866 Muscle Test Hemidiaphragm $75.8795866 Muscle Test Hemidiaphragm 26 $38.0495866 Muscle Test Hemidiaphragm TC $37.8495867 Muscle Test Cran Nerv Unilat $57.2595867 Muscle Test Cran Nerv Unilat 26 $23.9795867 Muscle Test Cran Nerv Unilat TC $33.2895868 Muscle Test Cran Nerve Bilat $76.2795868 Muscle Test Cran Nerve Bilat 26 $35.6695868 Muscle Test Cran Nerve Bilat TC $40.6195869 Muscle Test Thor Paraspinal $52.6995869 Muscle Test Thor Paraspinal 26 $11.2995869 Muscle Test Thor Paraspinal TC $41.4095870 Muscle Test Nonparaspinal $53.4995870 Muscle Test Nonparaspinal 26 $11.2995870 Muscle Test Nonparaspinal TC $42.2095872 Muscle Test One Fiber $111.1395872 Muscle Test One Fiber 26 $87.3695872 Muscle Test One Fiber TC $23.7795873 Guide Nerv Destr Elec Stim $41.4095873 Guide Nerv Destr Elec Stim 26 $11.2995873 Guide Nerv Destr Elec Stim TC $30.1195874 Guide Nerv Destr Needle Emg $42.2095874 Guide Nerv Destr Needle Emg 26 $11.2995874 Guide Nerv Destr Needle Emg TC $30.9095885 Musc Tst Done W/Nerv Tst Lim $33.28
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 42 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
95885 Musc Tst Done W/Nerv Tst Lim 26 $10.7095885 Musc Tst Done W/Nerv Tst Lim TC $22.5895886 Musc Test Done W/N Test Comp $51.5195886 Musc Test Done W/N Test Comp 26 $26.1595886 Musc Test Done W/N Test Comp TC $25.3695887 Musc Tst Done W/N Tst Nonext $45.5695887 Musc Tst Done W/N Tst Nonext 26 $21.5995887 Musc Tst Done W/N Tst Nonext TC $23.9795907 Nvr Cndj Tst 1-2 Studies $55.0795907 Nvr Cndj Tst 1-2 Studies 26 $30.3195907 Nvr Cndj Tst 1-2 Studies TC $24.7695908 Nrv Cndj Tst 3-4 Studies $71.3295908 Nrv Cndj Tst 3-4 Studies 26 $38.2395908 Nrv Cndj Tst 3-4 Studies TC $33.0895909 Nrv Cndj Tst 5-6 Studies $84.9895909 Nrv Cndj Tst 5-6 Studies 26 $45.5695909 Nrv Cndj Tst 5-6 Studies TC $39.4295910 Nrv Cndj Test 7-8 Studies $111.9395910 Nrv Cndj Test 7-8 Studies 26 $60.8295910 Nrv Cndj Test 7-8 Studies TC $51.1195911 Nrv Cndj Test 9-10 Studies $133.5295911 Nrv Cndj Test 9-10 Studies 26 $75.8795911 Nrv Cndj Test 9-10 Studies TC $57.6595912 Nrv Cndj Test 11-12 Studies $148.1895912 Nrv Cndj Test 11-12 Studies 26 $90.1495912 Nrv Cndj Test 11-12 Studies TC $58.0495913 Nrv Cndj Test 13/> Studies $170.9695913 Nrv Cndj Test 13/> Studies 26 $106.7895913 Nrv Cndj Test 13/> Studies TC $64.1895921 Autonomic Nrv Parasym Inervj $46.9595921 Autonomic Nrv Parasym Inervj 26 $25.5595921 Autonomic Nrv Parasym Inervj TC $21.3995922 Autonomic Nrv Adrenrg Inervj $54.8795922 Autonomic Nrv Adrenrg Inervj 26 $27.3495922 Autonomic Nrv Adrenrg Inervj TC $27.5495923 Autonomic Nrv Syst Funj Test $73.1095923 Autonomic Nrv Syst Funj Test 26 $25.9595923 Autonomic Nrv Syst Funj Test TC $47.1595924 Ans Parasymp & Symp W/Tilt $84.9895924 Ans Parasymp & Symp W/Tilt 26 $50.3295924 Ans Parasymp & Symp W/Tilt TC $34.6795925 Somatosensory Testing $74.4995925 Somatosensory Testing 26 $15.6595925 Somatosensory Testing TC $58.8495926 Somatosensory Testing $73.1095926 Somatosensory Testing 26 $15.4595926 Somatosensory Testing TC $57.6595927 Somatosensory Testing $76.66
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 43 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
95927 Somatosensory Testing 26 $15.4595927 Somatosensory Testing TC $61.2195928 C Motor Evoked Uppr Limbs $119.8595928 C Motor Evoked Uppr Limbs 26 $45.1795928 C Motor Evoked Uppr Limbs TC $74.6895929 C Motor Evoked Lwr Limbs $123.2295929 C Motor Evoked Lwr Limbs 26 $45.5695929 C Motor Evoked Lwr Limbs TC $77.6695930 Visual Ep Test Cns W/I&R $39.2295930 Visual Ep Test Cns W/I&R 26 $10.7095930 Visual Ep Test Cns W/I&R TC $28.5395937 Neuromuscular Junction Test $46.1695937 Neuromuscular Junction Test 26 $19.4195937 Neuromuscular Junction Test TC $26.7495938 Somatosensory Testing $194.1495938 Somatosensory Testing 26 $26.1595938 Somatosensory Testing TC $167.9995939 C Motor Evoked Upr&Lwr Limbs $285.2695939 C Motor Evoked Upr&Lwr Limbs 26 $67.7595939 C Motor Evoked Upr&Lwr Limbs TC $217.5195981 Io Anal Gast N-Stim Subsq $18.8295982 Io Ga N-Stim Subsq W/Reprog $30.3195990 Spin/Brain Pump Refil & Main $52.5095991 Spin/Brain Pump Refil & Main $67.1696101 Psycho Testing By Psych/Phys $46.1696102 Psycho Testing By Technician $34.4796103 Psycho Testing Admin By Comp $15.4596110 Developmental Screen W/Score $9.2096111 Developmental Test Extend $75.8796116 Neurobehavioral Status Exam $52.5096118 Neuropsych Tst By Psych/Phys $54.2896119 Neuropsych Testing By Tec $44.5796120 Neuropsych Tst Admin W/Comp $26.7496127 Brief Emotional/Behav Assmt $3.5796150 Assess Hlth/Behave Init $9.3696151 Assess Hlth/Behave Subseq $9.0696152 Intervene Hlth/Behave Indiv $8.6296153 Intervene Hlth/Behave Group $1.9396154 Interv Hlth/Behav Fam W/Pt $8.3296160 Pt-Focused Hlth Risk Assmt $2.1896161 Caregiver Health Risk Assmt $2.1896360 Hydration Iv Infusion Init $26.1596361 Hydrate Iv Infusion Add-On $7.7396365 Ther/Proph/Diag Iv Inf Init $40.8196366 Ther/Proph/Diag Iv Inf Addon $12.2896367 Tx/Proph/Dg Addl Seq Iv Inf $17.6396368 Ther/Diag Concurrent Inf $11.6996372 Ther/Proph/Diag Inj Sc/Im $11.49
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 44 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
96374 Ther/Proph/Diag Inj Iv Push $25.9596375 Tx/Pro/Dx Inj New Drug Addon $10.1096377 Applicaton On-Body Injector $11.4997012 Mechanical Traction Therapy $8.3297014 Electric Stimulation Therapy $8.7297016 Vasopneumatic Device Therapy $8.9197018 Paraffin Bath Therapy $4.9597022 Whirlpool Therapy $10.7097024 Diathermy Eg Microwave $3.9697026 Infrared Therapy $3.5797028 Ultraviolet Therapy $4.5697032 Electrical Stimulation $8.7297033 Electric Current Therapy $11.6997034 Contrast Bath Therapy $8.5297035 Ultrasound Therapy $7.5397036 Hydrotherapy $20.0197039 Physical Therapy Treatment M97110 Therapeutic Exercises $17.2397112 Neuromuscular Reeducation $19.6197116 Gait Training Therapy $17.0497124 Massage Therapy $17.2397139 Physical Medicine Procedure M97140 Manual Therapy 1/> Regions $15.6597161 Pt Eval Low Complex 20 Min $47.1597162 Pt Eval Mod Complex 30 Min $47.1597163 Pt Eval High Complex 45 Min $47.1597164 Pt Re-Eval Est Plan Care $31.8997165 Ot Eval Low Complex 30 Min $50.9197166 Ot Eval Mod Complex 45 Min $50.9197167 Ot Eval High Complex 60 Min $50.9197168 Ot Re-Eval Est Plan Care $34.6797530 Therapeutic Activities $22.7897533 Sensory Integration $19.2297535 Self Care Mngment Training $19.4197542 Wheelchair Mngment Training $18.8297597 Rmvl Devital Tis 20 Cm/< $46.9597760 Orthotic Mgmt&Trainj 1st Enc $26.3597761 Prosthetic Trainj 1st Enc $22.7897763 Orthc/Prostc Mgmt Sbsq Enc $27.1497799 Physical Medicine Procedure M98925 Osteopath Manj 1-2 Regions $17.8398926 Osteopath Manj 3-4 Regions $25.7598927 Osteopath Manj 5-6 Regions $33.6898928 Osteopath Manj 7-8 Regions $40.8198929 Osteopath Manj 9-10 Regions $48.7398940 Chiropract Manj 1-2 Regions $16.0598941 Chiropract Manj 3-4 Regions $22.9898942 Chiropractic Manj 5 Regions $29.91
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 45 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
99151 Mod Sed Same Phys/Qhp <5 Yrs $43.5899152 Mod Sed Same Phys/Qhp 5/>Yrs $28.9299153 Mod Sed Same Phys/Qhp Ea $6.1499188 App Topical Fluoride Varnish $6.9399201 Office/Outpatient Visit New $24.9699202 Office/Outpatient Visit New $42.0099203 Office/Outpatient Visit New $60.4299204 Office/Outpatient Visit New $92.1299205 Office/Outpatient Visit New $115.8999211 Office/Outpatient Visit Est $12.0899212 Office/Outpatient Visit Est $24.5699213 Office/Outpatient Visit Est $40.8199214 Office/Outpatient Visit Est $60.2299215 Office/Outpatient Visit Est $81.2299241 Office Consultation $26.5599242 Office Consultation $49.9299243 Office Consultation $68.3499244 Office Consultation $102.2299245 Office Consultation $124.6099304 Nursing Facility Care Init $51.1199305 Nursing Facility Care Init $73.1099306 Nursing Facility Care Init $93.5099307 Nursing Fac Care Subseq $24.9699308 Nursing Fac Care Subseq $38.8399309 Nursing Fac Care Subseq $51.3199310 Nursing Fac Care Subseq $76.2799315 Nursing Fac Discharge Day $40.8199316 Nursing Fac Discharge Day $59.4399318 Annual Nursing Fac Assessmnt $53.8899324 Domicil/R-Home Visit New Pat $30.9099325 Domicil/R-Home Visit New Pat $44.9799326 Domicil/R-Home Visit New Pat $78.0599327 Domicil/R-Home Visit New Pat $104.4099328 Domicil/R-Home Visit New Pat $122.2399334 Domicil/R-Home Visit Est Pat $33.6899335 Domicil/R-Home Visit Est Pat $53.0999336 Domicil/R-Home Visit Est Pat $75.8799337 Domicil/R-Home Visit Est Pat $108.3699341 Home Visit New Patient $30.7199342 Home Visit New Patient $44.5799343 Home Visit New Patient $73.1099344 Home Visit New Patient $102.4299345 Home Visit New Patient $124.4199347 Home Visit Est Patient $30.9099348 Home Visit Est Patient $47.1599349 Home Visit Est Patient $72.1199350 Home Visit Est Patient $100.2499354 Prolong E&M/Psyctx Serv O/P $73.10
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 46 of 62
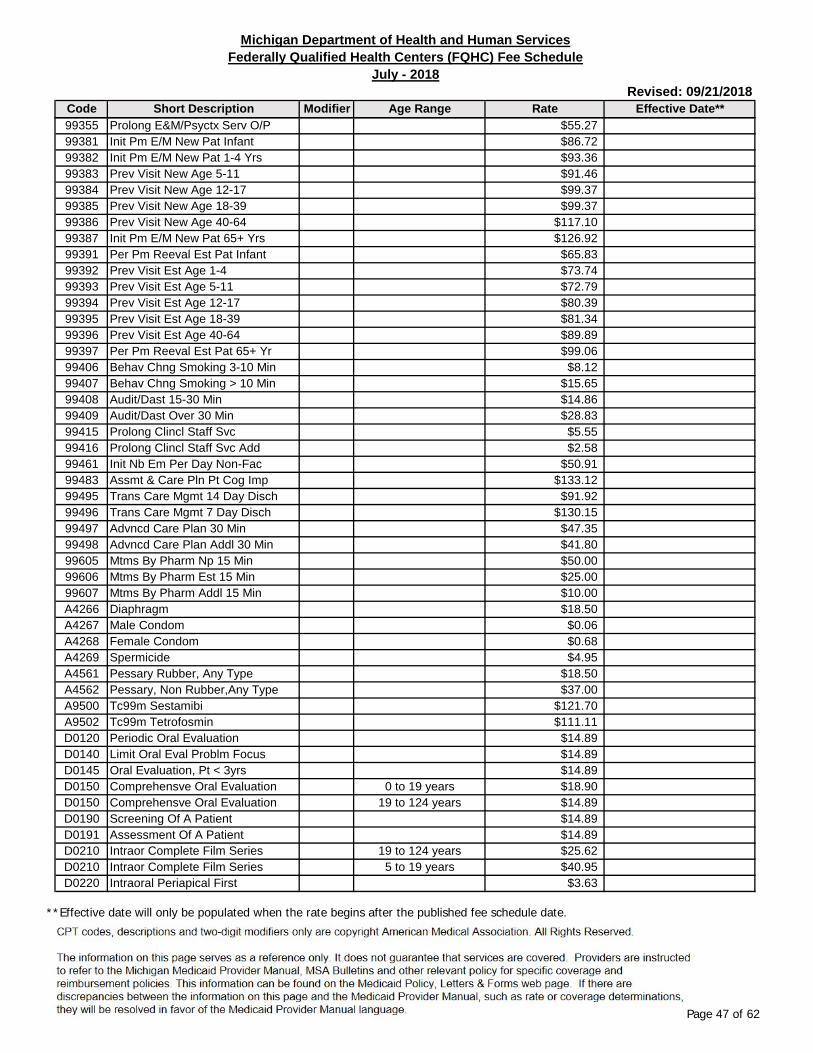
Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
99355 Prolong E&M/Psyctx Serv O/P $55.2799381 Init Pm E/M New Pat Infant $86.7299382 Init Pm E/M New Pat 1-4 Yrs $93.3699383 Prev Visit New Age 5-11 $91.4699384 Prev Visit New Age 12-17 $99.3799385 Prev Visit New Age 18-39 $99.3799386 Prev Visit New Age 40-64 $117.1099387 Init Pm E/M New Pat 65+ Yrs $126.9299391 Per Pm Reeval Est Pat Infant $65.8399392 Prev Visit Est Age 1-4 $73.7499393 Prev Visit Est Age 5-11 $72.7999394 Prev Visit Est Age 12-17 $80.3999395 Prev Visit Est Age 18-39 $81.3499396 Prev Visit Est Age 40-64 $89.8999397 Per Pm Reeval Est Pat 65+ Yr $99.0699406 Behav Chng Smoking 3-10 Min $8.1299407 Behav Chng Smoking > 10 Min $15.6599408 Audit/Dast 15-30 Min $14.8699409 Audit/Dast Over 30 Min $28.8399415 Prolong Clincl Staff Svc $5.5599416 Prolong Clincl Staff Svc Add $2.5899461 Init Nb Em Per Day Non-Fac $50.9199483 Assmt & Care Pln Pt Cog Imp $133.1299495 Trans Care Mgmt 14 Day Disch $91.9299496 Trans Care Mgmt 7 Day Disch $130.1599497 Advncd Care Plan 30 Min $47.3599498 Advncd Care Plan Addl 30 Min $41.8099605 Mtms By Pharm Np 15 Min $50.0099606 Mtms By Pharm Est 15 Min $25.0099607 Mtms By Pharm Addl 15 Min $10.00A4266 Diaphragm $18.50A4267 Male Condom $0.06A4268 Female Condom $0.68A4269 Spermicide $4.95A4561 Pessary Rubber, Any Type $18.50A4562 Pessary, Non Rubber,Any Type $37.00A9500 Tc99m Sestamibi $121.70A9502 Tc99m Tetrofosmin $111.11D0120 Periodic Oral Evaluation $14.89D0140 Limit Oral Eval Problm Focus $14.89D0145 Oral Evaluation, Pt < 3yrs $14.89D0150 Comprehensve Oral Evaluation 0 to 19 years $18.90D0150 Comprehensve Oral Evaluation 19 to 124 years $14.89D0190 Screening Of A Patient $14.89D0191 Assessment Of A Patient $14.89D0210 Intraor Complete Film Series 19 to 124 years $25.62D0210 Intraor Complete Film Series 5 to 19 years $40.95D0220 Intraoral Periapical First $3.63
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 47 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
D0230 Intraoral Periapical Ea Add $3.15D0240 Intraoral Occlusal Film $3.63D0270 Dental Bitewing Single Image 0 to 19 years $10.29D0270 Dental Bitewing Single Image 19 to 124 years $6.93D0272 Dental Bitewings Two Images 0 to 19 years $12.60D0272 Dental Bitewings Two Images 19 to 124 years $9.35D0273 Bitewings - Three Images 0 to 19 years $15.12D0273 Bitewings - Three Images 19 to 124 years $11.69D0274 Bitewings Four Images 0 to 19 years $17.64D0274 Bitewings Four Images 19 to 124 years $14.02D0330 Panoramic Image $17.56D0340* 2d Cephalometric Image $28.39D1110 Dental Prophylaxis Adult 14 to 19 years $27.72D1110 Dental Prophylaxis Adult 19 to 124 years $22.10D1120 Dental Prophylaxis Child $19.53D1206 Topical Fluoride Varnish 0 to 3 years $9.00D1206 Topical Fluoride Varnish 3 to 16 years $13.23D1208 Topical App Fluorid Ex Vrnsh $13.23D1351 Dental Sealant Per Tooth $15.12D1352 Prev Resin Rest, Perm Tooth $15.12D1354 Int Caries Med App Per Tooth $13.23D1510 Space Maintainer Fxd Unilat $110.25D1515 Fixed Bilat Space Maintainer $173.25D1550 Recement Space Maintainer $21.42D1555 Remove Fix Space Maintainer $21.42D1575 Dist Space Maint, Fixed Unil $110.25D2140 Amalgam One Surface Permanen 0 to 19 years $38.22D2140 Amalgam One Surface Permanen 19 to 124 years $15.59D2150 Amalgam Two Surfaces Permane 0 to 19 years $48.41D2150 Amalgam Two Surfaces Permane 19 to 124 years $31.21D2160 Amalgam Three Surfaces Perma 0 to 19 years $60.12D2160 Amalgam Three Surfaces Perma 19 to 124 years $41.22D2161 Amalgam 4 Or > Surfaces Perm 0 to 19 years $69.93D2161 Amalgam 4 Or > Surfaces Perm 19 to 124 years $48.45D2330 Resin One Surface-Anterior 0 to 19 years $46.94D2330 Resin One Surface-Anterior 19 to 124 years $25.62D2331 Resin Two Surfaces-Anterior 0 to 19 years $60.48D2331 Resin Two Surfaces-Anterior 19 to 124 years $36.77D2332 Resin Three Surfaces-Anterio 0 to 19 years $74.13D2332 Resin Three Surfaces-Anterio 19 to 124 years $49.02D2335 Resin 4/> Surf Or W Incis An 0 to 19 years $98.28D2335 Resin 4/> Surf Or W Incis An 19 to 124 years $59.05D2390 Ant Resin-Based Cmpst Crown 0 to 19 years $154.75D2390 Ant Resin-Based Cmpst Crown 19 to 21 years $131.25D2391 Post 1 Srfc Resinbased Cmpst 0 to 19 years $38.23D2391 Post 1 Srfc Resinbased Cmpst 19 to 124 years $15.59D2392 Post 2 Srfc Resinbased Cmpst 0 to 19 years $48.41D2392 Post 2 Srfc Resinbased Cmpst 19 to 124 years $31.21
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 48 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
D2393 Post 3 Srfc Resinbased Cmpst 0 to 19 years $60.12D2393 Post 3 Srfc Resinbased Cmpst 19 to 124 years $41.22D2394 Post >=4srfc Resinbase Cmpst 0 to 19 years $66.52D2394 Post >=4srfc Resinbase Cmpst 19 to 124 years $48.45D2710 Crown Resin-Based Indirect 0 to 19 years $232.05D2710 Crown Resin-Based Indirect 19 to 21 years $175.49D2712 Crown 3/4 Resin-Based Compos 0 to 19 years $232.05D2712 Crown 3/4 Resin-Based Compos 19 to 21 years $175.49D2740* Crown Porcelain/Ceramic $432.92D2750* Crown Porcelain W/ H Noble M $411.60D2751* Crown Porcelain Fused Base M $393.23D2752* Crown Porcelain W/ Noble Met $404.25D2790* Crown Full Cast High Noble M $404.25D2791* Crown Full Cast Base Metal $363.83D2792* Crown Full Cast Noble Metal $367.50D2794* Crown-Titanium $367.50D2799* Provisional Crown $232.05D2910 Recement Inlay Onlay Or Part $11.69D2915 Recement Cast Or Prefab Post $11.69D2920 Re-Cement Or Re-Bond Crown $11.69D2930 Prefab Stnlss Steel Crwn Pri 0 to 19 years $84.00D2930 Prefab Stnlss Steel Crwn Pri 19 to 21 years $46.80D2931 Prefab Stnlss Steel Crown Pe $85.62D2933 Prefab Stainless Steel Crown 0 to 19 years $90.83D2933 Prefab Stainless Steel Crown 19 to 21 years $58.49D2934 Prefab Steel Crown Primary $90.83D2940 Protective Restoration $11.69D2950 Core Build-Up Incl Any Pins $116.13D2951 Tooth Pin Retention $22.79D2952 Post And Core Cast + Crown $155.82D2954 Prefab Post/Core + Crown $150.68D2999 Dental Unspec Restorative Pr MD3110 Pulp Cap Direct 0 to 19 years $18.38D3110 Pulp Cap Direct 19 to 21 years $12.82D3220 Therapeutic Pulpotomy $66.15D3221 Gross Pulpal Debridement $66.15D3222 Part Pulp For Apexogenesis 19 to 21 years $35.10D3222 Part Pulp For Apexogenesis 5 to 19 years $66.15D3230 Pulpal Therapy Anterior Prim $102.77D3240 Pulpal Therapy Posterior Pri $102.77D3310 End Thxpy, Anterior Tooth 0 to 19 years $239.40D3310 End Thxpy, Anterior Tooth 19 to 21 years $134.54D3320 End Thxpy, Premolar Tooth 0 to 19 years $283.50D3320 End Thxpy, Premolar Tooth 19 to 21 years $157.93D3330 End Thxpy, Molar Tooth 0 to 19 years $378.00D3330 End Thxpy, Molar Tooth 19 to 21 years $204.73D3346 Retreat Root Canal Anterior 0 to 19 years $246.58D3346 Retreat Root Canal Anterior 19 to 21 years $138.57
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 49 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
D3347 Retreat Root Canal Premolar 0 to 19 years $292.00D3347 Retreat Root Canal Premolar 19 to 21 years $162.66D3348 Retreat Root Canal Molar 0 to 19 years $389.34D3348 Retreat Root Canal Molar 19 to 21 years $210.87D3351 Apexification/Recalc Initial $63.21D3352 Apexification/Recalc Interim $63.21D3353 Apexification/Recalc Final $404.25D3410 Apicoectomy - Anterior 0 to 19 years $312.90D3410 Apicoectomy - Anterior 19 to 21 years $81.89D3421 Root Surgery Premolar $349.13D3425 Root Surgery Molar $374.85D3426 Root Surgery Ea Add Root $374.85D3430 Retrograde Filling $73.50D3999 Endodontic Procedure MD4355 Full Mouth Debridement $43.26D5110 Dentures Complete Maxillary $341.25D5120 Dentures Complete Mandible $341.25D5130 Dentures Immediat Maxillary $341.25D5140 Dentures Immediat Mandible $341.25D5211 Dentures Maxill Part Resin $157.93D5212 Dentures Mand Part Resin $157.93D5213 Dentures Maxill Part Metal $380.22D5214 Dentures Mandibl Part Metal $380.22D5225 Maxillary Part Denture Flex $157.93D5226 Mandibular Part Denture Flex $157.93D5410 Dentures Adjust Cmplt Maxil $36.75D5411 Dentures Adjust Cmplt Mand $36.75D5421 Dentures Adjust Part Maxill $36.75D5422 Dentures Adjust Part Mandbl $36.75D5511 Rep Broke Comp Dent Base Man $66.15D5512 Rep Broke Comp Dent Base Max $66.15D5520 Replace Denture Teeth Complt $70.35D5611 Rep Resin Part Dent Base Man $66.15D5612 Rep Resin Part Dent Base Max $66.15D5621 Rep Cast Part Frame Man $70.35D5622 Rep Cast Part Frame Max $70.35D5630 Rep Partial Denture Clasp $89.24D5640 Replace Part Denture Teeth $63.00D5650 Add Tooth To Partial Denture $70.35D5660 Add Clasp To Partial Denture $99.75D5710 Dentures Rebase Cmplt Maxil $146.24D5711 Dentures Rebase Cmplt Mand $146.24D5720 Dentures Rebase Part Maxill $87.74D5721 Dentures Rebase Part Mandbl $87.74D5730 Denture Reln Cmplt Maxil Ch $66.15D5731 Denture Reln Cmplt Mand Chr $66.15D5740 Denture Reln Part Maxil Chr $66.15D5741 Denture Reln Part Mand Chr $66.15
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 50 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
D5750 Denture Reln Cmplt Max Lab $105.85D5751 Denture Reln Cmplt Mand Lab $105.85D5760 Denture Reln Part Maxil Lab $116.99D5761 Denture Reln Part Mand Lab $116.99D5810 Denture Interm Cmplt Maxill $146.24D5811 Denture Interm Cmplt Mandbl $146.24D5820 Denture Interm Part Maxill $105.28D5821 Denture Interm Part Mandbl $105.28D5899 Removable Prosthodontic Proc MD5982* Surgical Stent $627.00D5988* Surgical Splint $627.00D6010* Odontics Endosteal Implant $1,468.00D6055* Implant Connecting Bar $1,949.00D6056* Prefabricated Abutment $300.00D6057* Custom Abutment $300.00D6058* Abutment Supported Crown $675.00D6059* Abutment Supported Mtl Crown $675.00D6062* Abutment Supported Mtl Crown $675.00D6065* Implant Supported Crown $975.00D6066* Implant Supported Mtl Crown $975.00D6067* Implant Supported Mtl Crown $975.00D6068* Abutment Supported Retainer $675.00D6069* Abutment Supported Retainer $675.00D6072* Abutment Supported Retainer $675.00D6075* Implant Supported Retainer $975.00D6076* Implant Supported Retainer $975.00D6077* Implant Supported Retainer $975.00D6080* Implant Maintenance $112.00D6081* Scale & Debride, Single Imp $112.00D6090* Repair Implant MD6091* Repl Semi/Precision Attach MD6092* Recement Supp Crown $65.00D6093* Recement Supp Part Denture $70.00D6094* Abut Support Crown Titanium MD6095* Odontics Repr Abutment MD6100* Removal Of Implant MD6110* Implnt/Abut Remov Dent Max $1,719.00D6111* Implnt/Abut Remov Dent Mand $1,719.00D6112* Imp/Abut Rem Dent Part Max $1,719.00D6113* Imp/Abut Rem Dent Part Mand $1,719.00D6114* Implnt/Abut Fixed Dent Max $2,919.00D6115* Implnt/Abut Fixed Dent Mand $2,919.00D6116* Imp/Abut Fixed Dent Part Max $2,919.00D6117* Imp/Abut Fixed Dent Part Man $2,919.00D6194* Abut Support Retainer Titani $675.00D6199* Implant Procedure MD6205* Pontic-Indirect Resin Based $232.05D6210* Prosthodont High Noble Metal $396.90
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 51 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
D6211* Bridge Base Metal Cast $382.20D6212* Bridge Noble Metal Cast $389.55D6214* Pontic Titanium $422.63D6240* Bridge Porcelain High Noble $422.63D6241* Bridge Porcelain Base Metal $374.85D6242* Bridge Porcelain Nobel Metal $393.23D6245* Bridge Porcelain/Ceramic $417.90D6253* Provisional Pontic $232.05D6710* Crown-Indirect Resin Based $232.05D6740* Crown Porcelain/Ceramic $417.90D6750* Crown Porcelain High Noble $422.63D6751* Crown Porcelain Base Metal $374.85D6752* Crown Porcelain Noble Metal $393.23D6790* Crown Full High Noble Metal $396.90D6791* Crown Full Base Metal Cast $382.20D6792* Crown Full Noble Metal Cast $385.88D6793* Provisional Retainer Crown $232.05D6794* Crown Titanium $422.63D6930 Recement/Bond Part Denture $28.61D6980* Fixed Partial Repair MD7111 Extraction Coronal Remnants $23.39D7140 Extraction Erupted Tooth/Exr 0 to 19 years $44.47D7140 Extraction Erupted Tooth/Exr 19 to 124 years $25.62D7210 Rem Imp Tooth W Mucoper Flp 0 to 19 years $99.23D7210 Rem Imp Tooth W Mucoper Flp 19 to 124 years $33.43D7220 Impact Tooth Remov Soft Tiss 0 to 19 years $117.60D7220 Impact Tooth Remov Soft Tiss 19 to 124 years $52.65D7230 Impact Tooth Remov Part Bony 0 to 19 years $158.03D7230 Impact Tooth Remov Part Bony 19 to 124 years $87.74D7240 Impact Tooth Remov Comp Bony 0 to 19 years $190.37D7240 Impact Tooth Remov Comp Bony 19 to 124 years $116.99D7250 Tooth Root Removal 0 to 19 years $43.37D7250 Tooth Root Removal 19 to 124 years $23.39D7260 Oral Antral Fistula Closure $257.25D7261 Primary Closure Sinus Perf $171.50D7270 Tooth Reimplantation $147.00D7280* Exposure Of Unerupted Tooth $176.40D7282* Mobilize Erupted/Malpos Toot $120.40D7283* Place Device Impacted Tooth $120.40D7310 Alveoplasty W/ Extraction $99.23D7320 Alveoplasty W/O Extraction $124.95D7471 Rem Exostosis Any Site $87.74D7472 Removal Of Torus Palatinus $113.58D7473 Remove Torus Mandibularis $113.58D7485 Surg Reduct Osseoustuberosit $113.58D7510 I&D Absc Intraoral Soft Tiss $9.46D7970 Excision Hyperplastic Tissue $113.58D7971 Excision Pericoronal Gingiva $55.13
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 52 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
D7972 Surg Redct Fibrous Tuberosit $87.74D8050* Intercep Dental Tx Primary $1,260.00D8060* Intercep Dental Tx Transitn $1,470.00D8070* Compre Dental Tx Transition $1,460.00D8080* Compre Dental Tx Adolescent $1,775.00D8090* Compre Dental Tx Adult $1,880.00D8660* Preorthodontic Tx Visit $107.09D8670* Periodic Orthodontc Tx Visit $600.00D8692* Replacement Retainer $78.75D8999* Orthodontic Procedure MD9110 Tx Dental Pain Minor Proc $13.92D9248 Sedation (Non-Iv) $40.56D9310 Dental Consultation $29.24D9930 Treatment Of Complications $17.56D9940* Dental Occlusal Guard $229.00G0008 Admin Influenza Virus Vac $7.00G0009 Admin Pneumococcal Vaccine $7.00G0010 Admin Hepatitis B Vaccine $7.00G0101 Ca Screen;Pelvic/Breast Exam $21.39G0102 Prostate Ca Screening; Dre $11.89G0103 Psa Screening $18.80G0104 Ca Screen;Flexi Sigmoidscope $95.29G0105 Colorectal Scrn; Hi Risk Ind $178.49G0105 Colorectal Scrn; Hi Risk Ind 53 $88.95G0117 Glaucoma Scrn Hgh Risk Direc $30.31G0118 Glaucoma Scrn Hgh Risk Direc $24.17G0121 Colon Ca Scrn Not Hi Rsk Ind $178.69G0121 Colon Ca Scrn Not Hi Rsk Ind 53 $89.34G0130 Single Energy X-Ray Study $19.61G0130 Single Energy X-Ray Study 26 $6.34G0130 Single Energy X-Ray Study TC $13.27G0168 Wound Closure By Adhesive $58.24G0306 Cbc/Diffwbc W/O Platelet $7.94G0307 Cbc Without Platelet $6.61G0328 Fecal Blood Scrn Immunoassay $16.26G0432 Eia Hiv-1/Hiv-2 Screen $16.20G0433 Elisa Hiv-1/Hiv-2 Screen $15.14G0435 Oral Hiv-1/Hiv-2 Screen $12.25G0466 Fqhc Visit New Patient Clinic Specific RateG0467 Fqhc Visit, Estab Pt Clinic Specific RateG0468 Fqhc Visit, Ippe Or Awv Clinic Specific RateG0469 Fqhc Visit, Mh New Pt Clinic Specific RateG0470 Fqhc Visit, Mh Estab Pt Clinic Specific RateG0472 Hep C Screen High Risk/Other $38.38G0476 Hpv Combo Assay Ca Screen $35.88G0480 Drug Test Def 1-7 Classes $94.75G0481 Drug Test Def 8-14 Classes $129.66G0482 Drug Test Def 15-21 Classes $164.56
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 53 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
G0483 Drug Test Def 22+ Classes $204.45G0490 Home Visit Rn, Lpn By Rhc/Fq $80.98G0499 Hepb Screen High Risk Indiv $28.90G0515 Cognitive Skills Development $16.05G0516 Insert Drug Implant,>=4 $131.74G0517 Remove Drug Implant $144.81G0518 Remove W Insert Drug Implant $250.00H0001 Alcohol And/Or Drug Assess $61.48H0002 Alcohol And/Or Drug Screenin $42.50H0004 Alcohol And/Or Drug Services $22.37H0005 Alcohol And/Or Drug Services $13.02H0031 Mh Health Assess By Non-Md $91.21H2011 Crisis Interven Svc, 15 Min $50.25J0171 Adrenalin Epinephrine Inject $0.58J0520 Bethanechol Chloride Inject MJ0558 Peng Benzathine/Procaine Inj $10.93J0561 Penicillin G Benzathine Inj $13.94J0565 Inj, Bezlotoxumab, 10 Mg $40.28J0570 Buprenorphine Implant 74.2mg $1,250.92J0583 Bivalirudin $0.96J0588 Incobotulinumtoxin A $5.08J0600 Edetate Calcium Disodium Inj $5,594.42J0606 Inj, Etelcalcetide, 0.1 Mg $3.47J0610 Calcium Gluconate Injection $4.16J0620 Calcium Glycer & Lact/10 Ml MJ0630 Calcitonin Salmon Injection $2,606.13J0636 Inj Calcitriol Per 0.1 Mcg $0.56J0637 Caspofungin Acetate $13.60J0640 Leucovorin Calcium Injection $3.13J0690 Cefazolin Sodium Injection $0.78J0692 Cefepime Hcl For Injection $2.50J0694 Cefoxitin Sodium Injection $3.83J0695 Inj Ceftolozane Tazobactam MJ0696 Ceftriaxone Sodium Injection $0.59J0697 Sterile Cefuroxime Injection $1.99J0698 Cefotaxime Sodium Injection $1.53J0702 Betamethasone Acet&Sod Phosp $6.99J0710 Cephapirin Sodium Injection MJ0712 Ceftaroline Fosamil Inj $2.90J0713 Inj Ceftazidime Per 500 Mg $2.32J0714 Ceftazidime And Avibactam MJ0715 Ceftizoxime Sodium / 500 Mg MJ0735 Clonidine Hydrochloride $12.21J0743 Cilastatin Sodium Injection $6.96J0744 Ciprofloxacin Iv $3.22J0780 Prochlorperazine Injection $10.05J0840 Crotalidae Poly Immune Fab $3,231.94J0875 Injection, Dalbavancin $14.66
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 54 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
J0878 Daptomycin Injection $0.36J0881 Darbepoetin Alfa, Non-Esrd $3.84J0882 Darbepoetin Alfa, Esrd Use $3.84J0885 Epoetin Alfa, Non-Esrd $13.09J0887 Epoetin Beta Esrd Use $1.79J0888 Epoetin Beta Non Esrd $1.79J0895 Deferoxamine Mesylate Inj $20.16J1000 Depo-Estradiol Cypionate Inj $21.97J1020 Methylprednisolone 20 Mg Inj $4.18J1030 Methylprednisolone 40 Mg Inj $7.00J1040 Methylprednisolone 80 Mg Inj $13.51J1050 Medroxyprogesterone Acetate $0.56J1071 Inj Testosterone Cypionate $0.03J1094 Inj Dexamethasone Acetate $0.27J1100 Dexamethasone Sodium Phos $0.12J1130 Inj Diclofenac Sodium 0.5mg MJ1170 Hydromorphone Injection $1.37J1200 Diphenhydramine Hcl Injectio $0.59J1335 Ertapenem Injection $62.78J1364 Erythro Lactobionate /500 Mg $78.87J1380 Estradiol Valerate 10 Mg Inj $15.74J1410 Inj Estrogen Conjugate 25 Mg $310.39J1435 Injection Estrone Per 1 Mg MJ1438 Etanercept Injection $411.71J1439 Inj Ferric Carboxymaltos 1mg $1.07J1447 Inj Tbo Filgrastim 1 Microg $0.59J1450 Fluconazole $4.49J1455 Foscarnet Sodium Injection $13.25J1460 Gamma Globulin 1 Cc Inj $38.48J1555 Inj Cuvitru, 100 Mg $13.40J1556 Inj, Imm Glob Bivigam, 500mg $70.52J1557 Gammaplex Injection $55.77J1559 Hizentra Injection $9.85J1560 Gamma Globulin > 10 Cc Inj $384.81J1561 Gamunex-C/Gammaked $40.24J1562 Vivaglobin, Inj MJ1566 Immune Globulin, Powder $40.01J1568 Octagam Injection $33.16J1569 Gammagard Liquid Injection $46.33J1570 Ganciclovir Sodium Injection $68.53J1571 Hepagam B Im Injection $67.89J1572 Flebogamma Injection $35.16J1573 Hepagam B Intravenous, Inj $51.29J1575 Hyqvia 100mg Immuneglobulin $14.34J1580 Garamycin Gentamicin Inj $1.36J1599 Ivig Non-Lyophilized, Nos MJ1627 Inj, Granisetron, Xr, 0.1 Mg $3.89J1630 Haloperidol Injection $0.99
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 55 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
J1631 Haloperidol Decanoate Inj $17.98J1670 Tetanus Immune Globulin Inj $277.59J1675 Histrelin Acetate MJ1700 Hydrocortisone Acetate Inj MJ1710 Hydrocortisone Sodium Ph Inj MJ1720 Hydrocortisone Sodium Succ I $13.18J1726 Makena, 10 Mg $32.40J1729 Inj Hydroxyprogst Capoat Nos MJ1741 Ibuprofen Injection MJ1750 Inj Iron Dextran $13.67J1756 Iron Sucrose Injection $0.23J1815 Insulin Injection $0.94J1826 Interferon Beta-1a Inj MJ1830 Interferon Beta-1b / .25 Mg $257.61J1833 Injection, Isavuconazonium MJ1840 Kanamycin Sulfate 500 Mg Inj $7.69J1850 Kanamycin Sulfate 75 Mg Inj $1.15J1885 Ketorolac Tromethamine Inj $0.57J1890 Cephalothin Sodium Injection MJ1940 Furosemide Injection $0.88J1942 Aripiprazole Lauroxil 1mg $2.46J1950 Leuprolide Acetate /3.75 Mg $1,196.91J1956 Levofloxacin Injection $1.25J2010 Lincomycin Injection $13.03J2020 Linezolid Injection $11.92J2175 Meperidine Hydrochl /100 Mg $3.77J2180 Meperidine/Promethazine Inj MJ2182 Injection, Mepolizumab, 1mg $27.30J2185 Meropenem $0.81J2265 Minocycline Hydrochloride MJ2270 Morphine Sulfate Injection $2.43J2278 Ziconotide Injection $7.58J2280 Inj, Moxifloxacin 100 Mg $9.73J2300 Inj Nalbuphine Hydrochloride $2.90J2310 Inj Naloxone Hydrochloride $23.87J2315 Naltrexone, Depot Form $3.26J2320 Nandrolone Decanoate 50 Mg MJ2360 Orphenadrine Injection $6.39J2405 Ondansetron Hcl Injection $0.08J2407 Injection, Oritavancin $25.62J2410 Oxymorphone Hcl Injection $2.85J2426 Paliperidone Palmitate Inj $10.88J2430 Pamidronate Disodium /30 Mg $10.05J2505 Injection, Pegfilgrastim 6mg $4,720.84J2510 Penicillin G Procaine Inj $29.30J2540 Penicillin G Potassium Inj $1.09J2543 Piperacillin/Tazobactam $2.73J2547 Injection, Peramivir M
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 56 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
J2550 Promethazine Hcl Injection $1.93J2650 Prednisolone Acetate Inj MJ2675 Inj Progesterone Per 50 Mg $1.10J2680 Fluphenazine Decanoate 25 Mg $13.94J2700 Oxacillin Sodium Injeciton $2.27J2780 Ranitidine Hydrochloride Inj $5.45J2786 Injection, Reslizumab, 1mg MJ2788 Rho D Immune Globulin 50 Mcg $25.38J2790 Rho D Immune Globulin Inj $82.44J2791 Rhophylac Injection $4.85J2792 Rho(D) Immune Globulin H, Sd $27.32J2794 Risperidone, Long Acting $9.40J2840 Inj Sebelipase Alfa 1 Mg MJ2860 Injection, Siltuximab MJ2916 Na Ferric Gluconate Complex $2.18J2920 Methylprednisolone Injection $4.81J2930 Methylprednisolone Injection $6.97J3000 Streptomycin Injection $16.46J3030 Sumatriptan Succinate / 6 Mg $51.89J3090 Inj Tedizolid Phosphate $1.44J3250 Trimethobenzamide Hcl Inj $32.24J3260 Tobramycin Sulfate Injection $3.00J3265 Injection Torsemide 10 Mg/Ml MJ3301 Triamcinolone Acet Inj Nos $1.77J3302 Triamcinolone Diacetate Inj MJ3303 Triamcinolone Hexacetonl Inj $3.61J3305 Inj Trimetrexate Glucoronate MJ3310 Perphenazine Injeciton MJ3315 Triptorelin Pamoate $262.10J3320 Spectinomycn Di-Hcl Inj MJ3358 Ustekinumab, Iv Inject, 1 Mg $12.55J3360 Diazepam Injection $6.96J3370 Vancomycin Hcl Injection $3.91J3380 Injection, Vedolizumab $19.62J3410 Hydroxyzine Hcl Injection $7.27J3411 Thiamine Hcl 100 Mg $2.91J3415 Pyridoxine Hcl 100 Mg $9.52J3420 Vitamin B12 Injection $1.91J3430 Vitamin K Phytonadione Inj $4.27J3465 Injection, Voriconazole $1.94J3471 Ovine, Up To 999 Usp Units $0.41J3472 Ovine, 1000 Usp Units $137.80J3473 Hyaluronidase Recombinant $0.36J3475 Inj Magnesium Sulfate $0.51J3480 Inj Potassium Chloride $0.12J3485 Zidovudine $1.51J3486 Ziprasidone Mesylate $18.07J3489 Zoledronic Acid 1mg $14.72
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 57 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
J7030 Normal Saline Solution Infus $2.50J7040 Normal Saline Solution Infus $1.26J7042 5% Dextrose/Normal Saline $1.01J7050 Normal Saline Solution Infus $0.62J7060 5% Dextrose/Water $2.28J7070 D5w Infusion $4.49J7100 Dextran 40 Infusion $17.77J7110 Dextran 75 Infusion MJ7120 Ringers Lactate Infusion $2.67J7121 5% Dextrose In Lac Ringers MJ7175 Inj, Factor X, (Human), 1iu MJ7179 Vonvendi Inj 1 Iu Vwf:Rco MJ7180 Factor Xiii Anti-Hem Factor $8.22J7181 Factor Xiii Recomb A-Subunit MJ7182 Factor Viii Recomb Novoeight $1.33J7183 Wilate Injection $1.03J7185 Xyntha Inj $1.25J7187 Humate-P, Inj $1.12J7188 Factor Viii Recomb Obizur MJ7189 Factor Viia $2.07J7190 Factor Viii $1.11J7191 Factor Viii (Porcine) MJ7192 Factor Viii Recombinant Nos $1.35J7193 Factor Ix Non-Recombinant $1.14J7194 Factor Ix Complex $1.43J7195 Factor Ix Recombinant Nos $1.51J7196 Antithrombin Recombinant MJ7197 Antithrombin Iii Injection $3.68J7198 Anti-Inhibitor $2.11J7199 Hemophilia Clot Factor Noc MJ7200 Factor Ix Recombinan Rixubis $1.35J7201 Factor Ix Alprolix Recomb $2.99J7202 Factor Ix Idelvion Inj MJ7205 Factor Viii Fc Fusion Recomb $2.01J7207 Factor Viii Pegylated Recomb MJ7209 Factor Viii Nuwiq Recomb 1iu MJ7210 Inj, Afstyla, 1 I.U. MJ7211 Inj, Kovaltry, 1 I.U. MJ7296 Kyleena, 19.5 Mg $909.83J7297 Liletta, 52 Mg $723.30J7298 Mirena, 52 Mg $858.33J7300 Intraut Copper Contraceptive $783.34J7301 Skyla, 13.5 Mg $757.58J7303 Contraceptive Vaginal Ring $149.38J7304 Contraceptive Hormone Patch $38.90J7307 Etonogestrel Implant System $943.70J7308 Aminolevulinic Acid Hcl Top $404.59J7309 Methyl Aminolevulinate, Top $83.69
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 58 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
J7315 Ophthalmic Mitomycin MJ7316 Inj, Ocriplasmin, 0.125 Mg $1,018.70J7320 Genvisc 850, Inj, 1mg $6.25J7321 Hyalgan Supartz Visco-3 Dose $83.18J7322 Hymovis Injection 1 Mg MJ7323 Euflexxa Inj Per Dose $143.73J7324 Orthovisc Inj Per Dose $140.34J7325 Synvisc Or Synvisc-One $11.70J7326 Gel-One $509.35J7327 Monovisc Inj Per Dose $796.56J7328 Gelsyn-3 Injection 0.1 Mg MJ7336 Capsaicin 8% Patch $3.15J7501 Azathioprine Parenteral $217.30J7504 Lymphocyte Immune Globulin $2,106.51J7511 Antithymocyte Globuln Rabbit $725.69J7516 Cyclosporin Parenteral 250mg $44.20J7525 Tacrolimus Injection $206.32J7999 Compounded Drug, Noc MJ8655 Netupitant Palonosetron Oral $340.62J9032 Injection, Belinostat, 10mg $37.26J9034 Inj., Bendeka 1 Mg $23.45J9039 Injection, Blinatumomab $109.92J9145 Injection, Daratumumab 10 Mg $50.95J9176 Injection, Elotuzumab, 1mg $6.42J9205 Inj Irinotecan Liposome 1 Mg $45.63J9212 Interferon Alfacon-1 Inj MJ9213 Interferon Alfa-2a Inj MJ9214 Interferon Alfa-2b Inj $34.38J9215 Interferon Alfa-N3 Inj $31.80J9216 Interferon Gamma 1-B Inj MJ9217 Leuprolide Acetate Suspnsion $218.17J9219 Leuprolide Acetate Implant MJ9225 Vantas Implant $3,452.33J9226 Supprelin La Implant $30,441.90J9271 Inj Pembrolizumab $48.57J9295 Injection, Necitumumab, 1 Mg $5.51J9299 Injection, Nivolumab $27.16J9308 Injection, Ramucirumab $57.67J9352 Injection Trabectedin 0.1mg $296.42L4350 Ankle Control Ortho Pre Ots $73.80L4360 Pneumat Walking Boot Pre Cst $197.46L4361 Pneuma/Vac Walk Boot Pre Ots $176.50L4370 Pneum Full Leg Splnt Pre Ots $179.50Q0091 Obtaining Screen Pap Smear $24.96Q0111 Wet Mounts/ W Preparations $1.54Q0112 Potassium Hydroxide Preps $1.54Q0113 Pinworm Examinations $1.54Q0114 Fern Test $1.54
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 59 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
Q0138 Ferumoxytol, Non-Esrd $0.96Q0139 Ferumoxytol, Esrd Use $0.96Q0144 Azithromycin Dihydrate, Oral $15.05Q2034 Agriflu Vaccine MQ2035 Afluria Vacc, 3 Yrs & >, Im $18.24 Effective: 08/01/2018Q2036 Flulaval Vacc, 3 Yrs & >, Im $8.58Q2037 Fluvirin Vacc, 3 Yrs & >, Im $17.69Q2038 Fluzone Vacc, 3 Yrs & >, Im $12.04Q2039 Influenza Virus Vaccine, Nos MQ3027 Inj Beta Interferon Im 1 Mcg $54.18Q4001 Cast Sup Body Cast Plaster $35.89Q4002 Cast Sup Body Cast Fiberglas $135.65Q4003 Cast Sup Shoulder Cast Plstr $25.78Q4004 Cast Sup Shoulder Cast Fbrgl $89.25Q4005 Cast Sup Long Arm Adult Plst $9.50Q4006 Cast Sup Long Arm Adult Fbrg $21.42Q4007 Cast Sup Long Arm Ped Plster $4.76Q4008 Cast Sup Long Arm Ped Fbrgls $10.71Q4009 Cast Sup Sht Arm Adult Plstr $6.34Q4010 Cast Sup Sht Arm Adult Fbrgl $14.28Q4011 Cast Sup Sht Arm Ped Plaster $3.17Q4012 Cast Sup Sht Arm Ped Fbrglas $7.14Q4013 Cast Sup Gauntlet Plaster $11.54Q4014 Cast Sup Gauntlet Fiberglass $19.48Q4015 Cast Sup Gauntlet Ped Plster $5.77Q4016 Cast Sup Gauntlet Ped Fbrgls $9.74Q4017 Cast Sup Lng Arm Splint Plst $6.68Q4018 Cast Sup Lng Arm Splint Fbrg $10.65Q4019 Cast Sup Lng Arm Splnt Ped P $3.34Q4020 Cast Sup Lng Arm Splnt Ped F $5.33Q4021 Cast Sup Sht Arm Splint Plst $4.94Q4022 Cast Sup Sht Arm Splint Fbrg $8.92Q4023 Cast Sup Sht Arm Splnt Ped P $2.48Q4024 Cast Sup Sht Arm Splnt Ped F $4.46Q4025 Cast Sup Hip Spica Plaster $27.72Q4026 Cast Sup Hip Spica Fiberglas $86.53Q4027 Cast Sup Hip Spica Ped Plstr $13.86Q4028 Cast Sup Hip Spica Ped Fbrgl $43.27Q4029 Cast Sup Long Leg Plaster $21.19Q4030 Cast Sup Long Leg Fiberglass $55.78Q4031 Cast Sup Lng Leg Ped Plaster $10.60Q4032 Cast Sup Lng Leg Ped Fbrgls $27.89Q4033 Cast Sup Lng Leg Cylinder Pl $19.76Q4034 Cast Sup Lng Leg Cylinder Fb $49.17Q4035 Cast Sup Lngleg Cylndr Ped P $9.89Q4036 Cast Sup Lngleg Cylndr Ped F $24.59Q4037 Cast Sup Shrt Leg Plaster $12.06Q4038 Cast Sup Shrt Leg Fiberglass $30.21
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 60 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
Q4039 Cast Sup Shrt Leg Ped Plster $6.04Q4040 Cast Sup Shrt Leg Ped Fbrgls $15.11Q4041 Cast Sup Lng Leg Splnt Plstr $14.66Q4042 Cast Sup Lng Leg Splnt Fbrgl $25.03Q4043 Cast Sup Lng Leg Splnt Ped P $7.33Q4044 Cast Sup Lng Leg Splnt Ped F $12.52Q4045 Cast Sup Sht Leg Splnt Plstr $8.51Q4046 Cast Sup Sht Leg Splnt Fbrgl $13.69Q4047 Cast Sup Sht Leg Splnt Ped P $4.25Q4048 Cast Sup Sht Leg Splnt Ped F $6.85Q4049 Finger Splint, Static $1.55Q4050 Cast Supplies Unlisted MQ4051 Splint Supplies Misc MQ4081 Epoetin Alfa, 100 Units Esrd $1.31Q4106 Dermagraft $33.05Q4131 Epifix Or Epicord $160.62Q5105 Inj Retacrit Esrd On Dialysi $1.17Q5106 Inj Retacrit Non-Esrd Use $11.69Q9951 Locm >= 400 Mg/Ml Iodine,1ml MQ9965 Locm 100-199mg/Ml Iodine,1ml $0.90Q9966 Locm 200-299mg/Ml Iodine,1ml $0.34Q9967 Locm 300-399mg/Ml Iodine,1ml $0.12Q9991 Buprenorph Xr 100 Mg Or Less $1,674.80Q9992 Buprenorphine Xr Over 100 Mg $1,674.80Q9993 Inj., Triamcinolone Ext Rel $18.88Q9995 Inj. Emicizumab-Kxwh, 0.5 Mg $49.48S0030 Injection, Metronidazole $0.02S0032 Injection, Nafcillin Sodium MS0074 Injection, Cefotetan Disodiu MS0077 Injection, Clindamycin Phosp $3.30S0080 Injection, Pentamidine Iseth $40.02S0145 Peg Interferon Alfa-2a/180 MS0148 Peg Interferon Alfa-2b/10 MS0164 Injection Pantroprazole $5.30S0166 Inj Olanzapine 2.5mg $11.37S0171 Bumetanide 0.5 Mg $0.53S0190 Mifepristone, Oral, 200 Mg MS0191 Misoprostol, Oral, 200 Mcg MS0199 Med Abortion Inc All Ex Drug MS0592 Comp Cont Lens Eval $28.72S0620 Routine Ophthalmological Exa $46.75S0621 Routine Ophthalmological Exa $49.13S2083 Adjustment Gastric Band $33.48S4989 Contracept Iud MS9024 Paranasal Sinus Ultrasound MS9152 Speech Therapy, Re-Eval $36.64S9443 Lactation Class $49.92
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 61 of 62

Code Short Description Modifier Age Range Rate Effective Date**
Michigan Department of Health and Human ServicesFederally Qualified Health Centers (FQHC) Fee Schedule
July - 2018Revised: 09/21/2018
*Covered benefit for CSHCS only: D0340, D2740, D2750, D2751, D2752, D2790, D2791, D2792, D2794, D2799, D5982, D5988, D6010, D6055, D6056, D6057, D6058, D6059, D6062, D6065, D6066, D6067, D6068, D6069, D6072, D6075, D6076, D6077, D6080, D6081, D6090, D6091, D6092, D6093, D6094, D6095, D6100, D6110, D6111, D6112, D6113, D6114, D6115, D6116, D6117, D6194, D6199, D6205, D6210, D6211, D6212, D6214, D6240, D6241, D6242, D6245, D6253, D6710, D6740, D6750, D6751, D6752, D6790, D6791, D6792, D6793, D6794, D6980, D7280, D7282, D7283, D8050, D8060, D8070, D8080, D8090, D8660, D8670, D8692, D8999, D9940
**Effective date will only be populated when the rate begins after the published fee schedule date.
Page 62 of 62