melanoma bridge 2014: molecular enhancement of...
TRANSCRIPT

Molecular Enhancement of Sentinel Node Evaluation
Departments of Pathology and Laboratory Medicine and Surgery,
David Geffen School of Medicine at UCLA.John Wayne Cancer Institute, Santa Monica.
Alistair Cochran, MD and Rong Huang MD
Grant Support: NCI CA 29605 (PI DL Morton) and Australian and New
Zealand Melanoma Trials Group.
Cochran Illustrations 060104

Donald Morton MDCochran Illustrations 060104

Lymphatic Mapping and Sentinel Node Biopsy for Melanoma: Status in December 2014.
• First described 30 years ago• 1 major clinical trial (MSLT1) completed and
results published (NEJM 2014)• 1 major clinical trial (MSLT2) in follow-up (1926
patients randomized) • 5 year follow up by 2019• Techniques widely practiced around the world• Techniques effectively applied to tumors other
than melanoma• Some issues remain unresolved• No viable alternative approach in sight
Cochran Illustrations 060104
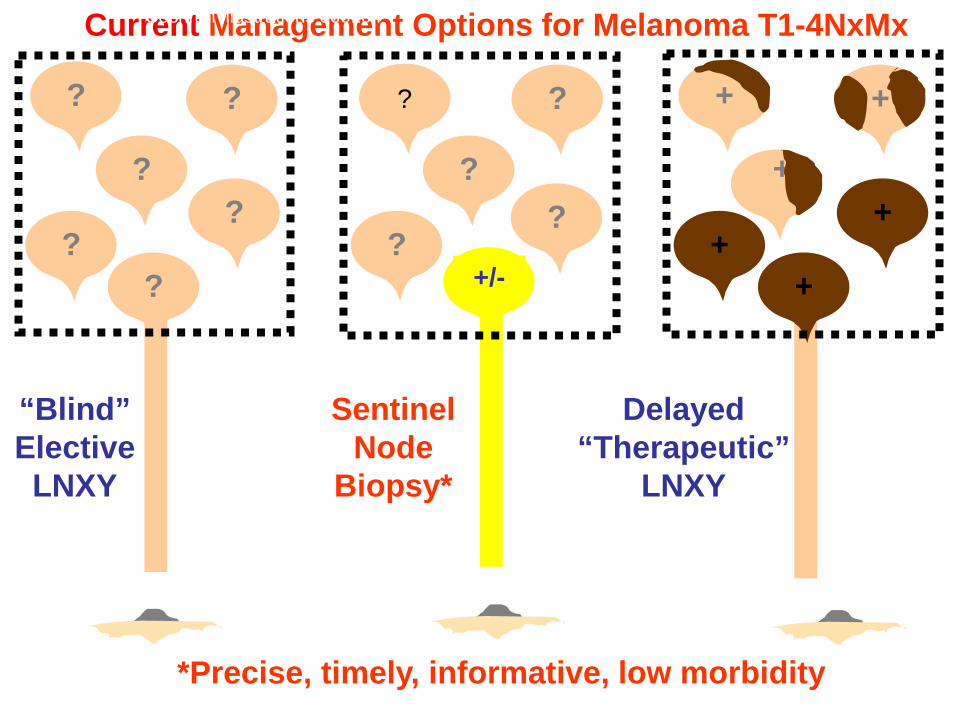
+/-
“Blind” Elective
LNXY
Delayed “Therapeutic”
LNXY
Sentinel Node
Biopsy*
?
?
??
??
?
??
??
+
++
++
+
Current Management Options for Melanoma T1-4NxMx
*Precise, timely, informative, low morbidity
Cochran Illustrations 060104

Summary – MSLT Data
• LM/SNB accurately stages regional nodes (up to 95-97% accuracy).
– Identifies patients with clinically occult metastatic melanoma in the sentinel node
– Identifies candidates for immediate CLND– During clinical observation small impalpable
metastases in SN become detectable and may spread to additional nodes (3.2 vs,1.4 P=0.001)
– SN metastases may also spread to distant sites HR–0.62 – P= 0.0152
•
Cochran Illustrations 060104

MSLT-1 at 10 years of follow up: Summary
• Data validate accuracy of biopsy-based staging of intermediate and thick melanomas
• Identifies patients with SN metastases who benefit from immediate CLND
• SNB/selective CLND prolongs disease free survival for all patients
• Prolongs distant disease free survival and melanoma specific survival for patients with SN metastases from intermediate (1.2-3.5mm.) primaries
• Early lymph node surgery associated with substantially less morbidity
Cochran Illustrations 060104

Primary Melanoma Subgroups
• Primary with risk of nodal metastases• a. =/> 1mm. Breslow• b. <1mm. Breslow with mitoses or ulceration• Treatment: consider for sentinel node biopsy• Primary with low/no risk of nodal metastases• <1mm. Breslow without mitoses or ulceration• Treatment: wide excision and follow up• Problem of false negative sentinel node• False negatives in experienced hands <5%

Primary Melanomas treated by Sentinel Node biopsy
• 80% SN microscopically negative• Optimally staged so follow up only• SNB justified as pt. spared CLND• 20% SN microscopically positive• SNB justified as optimally staged• consider for immediate CLND

SNB+ve patients receiving immediate CLND
• Negative Non-sentinel nodes (84%)• Evaluate for distant metastases and observation• ?Adjunctive therapy• ?surgically over-treated: how to identify these pts. and avoid CLND?• Evaluate primary and sentinel nodal metastases• Histology, Immunohistology, molecular and genetic analyses• Positive Non-sentinel nodes (16%)• Evaluate for distant met.• Adjunctive therapy• Extensive nodal surgery defensible in this sub-group• How are these patients to be identified?• Evaluate primary and sentinel nodal metastases• Histology, Immunohistology, molecular and genetic analysis
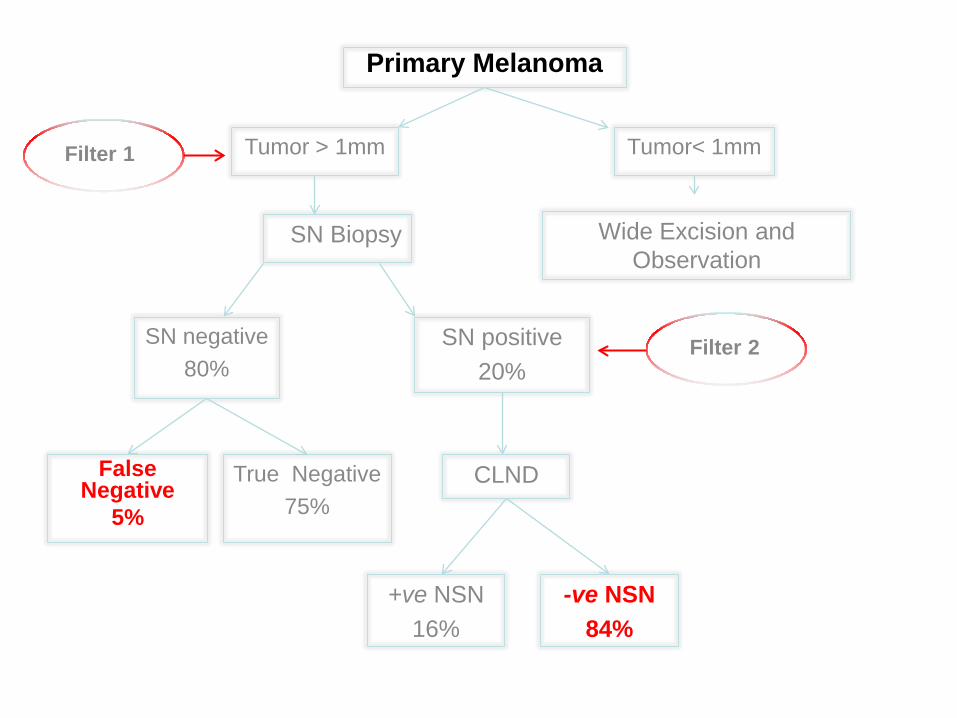
Primary Melanoma
Tumor > 1mm
SN Biopsy
SN negative80%
SN positive20%
False Negative
5%
True Negative75%
CLND
+ve NSN 16%
-ve NSN 84%
Tumor< 1mm
Wide Excision and Observation
Filter 1
Filter 2

Variables Estimated Odds Ratio (95% CI)
P-value
Age >50 vs. ≤50 0.62 (0.44, 0.87) 0.0060
Primary Site Trunk vs. other 1.74 (1.24, 2.44) 0.0015
Breslow ≤2.00 1.0 (reference)
2.01-4.00 2.42 (1.65, 3.53) <.0001
>4.00 3.80 (2.32, 6.22) <.0001
Clark level IV-V vs. I-III 1.46 (1.01, 2.12) 0.0429
Lymphatic invasion Y vs.N 2.88 (1.62, 5.12) 0.0003
Demographic/pathological features of primary melanomas predicting metastases in sentinel nodes (Filter 1) .

Staging Based on SN Tumor Status (Filter 2)
• Most accurate available staging technique• Identifies pts. with actual early nodal spread• Other predictors (Breslow, Clark, ulceration)
identify pts. likely to have nodal spread• SN status included in current AJCC
classification• SN evaluation greatly exceeds accuracy of
clinical staging and available adjunctive techniques
Cochran 6th World Congr on Melanoma
Vancouver 09080512

Evaluation of need for completion lymph node dissection in patients with sentinel node metastases
Aim. Spare 84% of patients unnecessary CLND1. Evaluate the number of sentinel nodes with
metastases2. Evaluate the site, size, frequency of
metastases and the percentage of node replaced by tumor
3. Molecular Pathology Assessment– Gene Expression Microarrays (GEM) to develop
Gene Signatures-under investigation

Amount and disposition of tumor in the SN predict
groups of patients at risk for NSN tumor, tumor
recurrence and death from melanoma.
Cochran Illustrations 060104

Survival prediction from SN tumor features
• Percent tumor burden- P=0.0023• Tumor diameter- P=0.0173• Tumor depth from capsule- P=0.0096• Number metastatic foci- P=0.0063• Tumor site in node- P=0.05• Extra-capsular extension- P=0.0148
Cochran Illustrations 060104

Evaluation of need for sentinel node biopsy in patients with primary melanoma
Aim: To confine sentinel node biopsy to patients with reasonable likelihood of nodal metastases1. Careful clinicopathological assessment: Age, site, Breslow,
Lymphatic invasion and Clark level2. Identify 5% of pts. with false -ve SNs-HOW? 3. Molecular Pathology Assessment
– CGH-likely adjunctive-currently applied clinically – FISH-likely adjunctive-currently applied clinically– RTPCR unfulfilled promises for SN– Gene Expression Microarrays/Gene Signatures-under investigation– Gene Sequencing to generate signatures-likely adjunctive-under
investigation

In a study of melanoma Primaries and SN metastases (Koh et al)
• DNA microarrays show:– differential gene expression patterns
between primaries and SN metastases.– clear distinction on hierarchical clustering
map– 576 significant genes identified at >=2 fold
and p<0.05 – most genes with greatest fold-change were
decreased rather than increased– Analysis of these data continues to
develop gene signatures
17

Supervised gene expression microarray (GEM)• to investigate metastatic melanoma in SN from 15
patients who had immediate CLND: 7 with nomelanoma in the non-sentinel nodes (NSN), and 8with metastasis-positive NSN.
• We found significantly different gene expressionprofiles comparing SN metastases from these twogroups of patients: -ve NSN-without melanoma inNSN; +ve NSN with metastasis in NSN.
• We developed two preliminary gene signatures
Molecular Pathology AssessmentSentinel Node

PCA: Significant Pattern of Expressed Genes in SN Metastases
(+ve NSN versus –ve NSN)

• Consideration of two preliminary gene signatures, withclinical and pathological features, will likely enhanceaccuracy of prediction of NSN tumor status, separatingpatients likely to benefit from CLND, from those unlikelyto derive benefit from CLND.
• This will spare relevant patients the morbidity ofextended surgery and significantly reduce medical costs.
• More accurate staging will also identify patients at highrisk of visceral metastases who may benefit fromrelatively aggressive adjuvant therapy.
Summary