mechanics of the pulmonary valve in the aortic...
TRANSCRIPT

Available online at www.sciencedirect.com
www.elsevier.com/locate/jmbbm
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7
1751-6161/$ - see frohttp://dx.doi.org/10
nCorresponding autE-mail address: a
Research paper
Mechanics of the pulmonary valve in theaortic position
A.L.F. Soaresa,n, D. van Geemena, A.J. van den Bogaerdtb, C.W.J. Oomensa,C.V.C. Boutena, F.P.T. Baaijensa
aEindhoven University of Technology, Eindhoven, The NetherlandsbHeart Valve Bank, Department of Cardio-Thoracic Surgery, Erasmus University Medical Center,Rotterdam, The Netherlands
a r t i c l e i n f o
Article history:
Received 15 April 2013
Received in revised form
2 July 2013
Accepted 4 July 2013
Available online 16 August 2013
Keywords:
Aortic valve
Pulmonary valve
Biomechanical properties
Remodeling
nt matter & 2013 Elsevie.1016/j.jmbbm.2013.07.009
hor. Tel.: þ31 40 247 [email protected] (A.L.F.
a b s t r a c t
Mathematical models can provide valuable information to assess and evaluate the
mechanical behavior and remodeling of native tissue. A relevant example when studying
collagen remodeling is the Ross procedure because it involves placing the pulmonary
autograft in the more demanding aortic valve mechanical environment. The objective of
this study was therefore to assess and evaluate the mechanical differences between the
aortic valve and pulmonary valve and the remodeling that may occur in the pulmonary
valve when placed in the aortic position. The results from biaxial tensile tests of pairs
of human aortic and pulmonary valves were compared and used to determine the
parameters of a structurally based constitutive model. Finite element analyzes were then
performed to simulate the mechanical response of both valves to the aortic diastolic load.
Additionally, remodeling laws were applied to assess the remodeling of the pulmonary
valve leaflet to the new environment. The pulmonary valve showed to be more extensible
and less anisotropic than the aortic valve. When exposed to aortic pressure, the pulmonary
leaflet appeared to remodel by increasing its thickness and reorganizing its collagen fibers,
rotating them toward the circumferential direction.
& 2013 Elsevier Ltd. All rights reserved.
r Ltd. All rights reserved.
.Soares).
1. Introduction
The mechanical function of cardiovascular tissue is mainlydetermined by the extracellular matrix (ECM) composition andstructure. The matrix defines the response of the tissue tomechanical load and can also remodel in response to changesin its environment. Thus, an improved understanding of theadaptation capabilities of cardiac valve ECM is essential forunderstanding both valve pathology and physiology and fordesigning materials for valve repair or replacement. Yet, the
events and mechanisms by which the matrix remodels andadapts are largely unknown since the collagen architectureand the local mechanical loading condition within the tissueare highly coupled. Mathematical models can give insight inthis interaction and in predicting the tissue's response andadaptation.
One particular case of a tissue undergoing a strong change inmechanical environment is the so called Ross procedure. Theoperation consists of replacing the aortic valve (AV) by thepulmonary autograft and the use of a homograft valve instead

j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7558
of the pulmonary valve (PV) (Ross, 1967). This procedure isparticularly attractive for children, athletes and women ofchildbearing age because it eliminates the need for antic-oagulation therapy and has the potential for somatic growth.
Usage of a pulmonary autograft has several advantages, inparticular its ability to grow and its improved hemodynamicsand durability (Elkins et al., 1994; Chambers et al., 1997; Santiniet al., 1997). There are, however, potential disadvantages.In adults, the AV and PV are known to differ in morphologyand structure, (Stradins et al., 2004; Vesely et al., 2000; Azadaniet al., 2012; Hokken et al., 1997) and after pulmonary autograftreplacement of the AV, the autograft is subjected to higherpressures. This mechanically more demanding environmentmay cause remodeling of the autograft. The valve explantsshow thickened leaflets and severe aneurysmal degeneration ofthe wall, which was characterized by intimal thickening, medialelastin fragmentation, and adventitial fibrosis (Schoof et al.,2006; Mookhoek et al., 2010). Concern exists, that these struc-tural and functional changes in the implanted autograft lead toprogressive aortic root dilatation and neoaortic regurgitation.
Another limitation of the technique is the lack of longterm results (Phillips, 2003; Kouchoukos, 2011). Somemidterm studies however, reported freedom from autograftreoperation between 93% and 98.6% at 10 years (Rabkin-Aikawa et al., 2004; Favaloro et al., 2008; Elkins et al., 2008;Takkenberg et al., 2009). This range of values may be depen-dent on the technique employed, the surgeon and the patientgroup selected. Therefore uncertainty remains regarding thesuitability of the autograft to potentially become a viablepermanent replacement.
The objective of this study was therefore to assess andevaluate the mechanical differences between the AV and PVleaflets and the remodeling that may occur in the PV leafletswhen placed in the aortic position. The mechanical propertiesof sets of PVs and AVs leaflets from the same donor wereassessed and evaluated. Next, a structurally based model forcollagenous cardiovascular tissues (Driessen et al., 2005) wasapplied to describe the mechanical behavior of the leaflets.Finite element analyzes (FEA) were performed to simulate themechanical response of both leaflets to a transvalvular aorticpressure load. Last, the previous model extended with remodel-ing equations for the collagen angular fiber distribution(Driessen et al., 2008) was applied to study the remodeling ofthe PV leaflets when subjected to the aortic valve diastolic load.
2. Materials and methods
2.1. Tissue preparation
Five sets of human aortic and pulmonary heart valves frompatients 11 to 51 years (mean 31.8716.1 years) of age wereobtained from Dutch postmortem donors, giving permiss-ion for research. The valves, which were assessed to be unfitfor implantation, were obtained from the Heart ValveBank (Erasmus University Medical Center, Rotterdam, TheNetherlands). All valves were structurally and mechanicallyunaffected. Previous studies suggest that the study of tissue(mechanical) properties can be done in cryopreservedheart valves since the structural integrity of collagen and
elastin (Gerson et al., 2009) and mechanical properties (ViruesDelgadillo et al., 2010) are not affected by the applied cry-opreservation protocol. Furthermore, valvular disease orconditions known to precede valvular disease were notrelated to the cause of dead of the donors.
The cryopreserved valves were stored at �80 1C. Priorto the ECM analysis and mechanical testing, the valves werethawed according to the guidelines of the Dutch HeartValve Bank. Briefly, the package containing the cryopreservedhomograft was gently agitated in warm saline (740 1C) todissolve ice-crystals and soften the graft. After thawing, thepackage containing the valve was opened and depositedin phosphate buffered saline (PBS; Sigma-Aldrich, St. Louis,USA) to allow dimethyl sulfoxide (DMSO) to dilute from thetissue into the solution. Immediately after thawing, the cuspswere carefully excised from the intact heart valves, using ascalpel. The specimens were cut in a square shape, usingparallel razor blades (n¼21 for the AV leaflets and n¼26 forthe PV leaflets, with n being the sample size). Each specimenhad a dimension of 6�6 mm and its edges were aligned withthe circumferential and radial axes. Mechanical testing wasperformed within 48 h after thawing. The leaflet specimenthickness distribution was obtained using a SensoFar PLμ 2300optical imaging profiler (SensoFar-Tech, Barcelona, Spain) andthe average thickness of each sample was measured.
2.2. Experimental protocol
The specimens were placed in aluminium foil and kepthydrated. The specimens were then mounted in a Bio-Tester5000 test device (CellScale, Canada) using a BioRakes mountingsystem with pins with 0.7 mm tine space. These BioRakes hadneglecting values of force due to pin deflection for stretcheslower than 200%. To produce visual surface texture, the tissuewas sprinkled with graphite particles. The samples were thentested while submersed in phosphate buffered saline (PBS) tomimic natural conditions.
The samples were biaxially tested to peak values ϵCC andϵRR, where subscripts C and R correspond to the circum-ferential and radial directions, respectively. The completebiaxial testing regime consisted of 6 groups of 5 protocols.The first group of protocols of strain ratios was defined asϵCC : ϵRR ¼ 0 : 60; 11:5 : 55;23 : 23;24 : 11:5; 25 : 0ð%Þ. The strainswere then sequentially increased during the next 5 groupof protocols in steps of 5% or 10% until the last group ϵCC :
ϵRR ¼ 0 : 110;49 : 105;78 : 78; 79 : 49; 80 : 0ð%Þ was performed.Preliminary studies showed that this particular biaxial stretchratio could capture the nonlinear mechanical behavior of theheart valve leaflets without damaging the tissue and takinginto account inter patient variability. The samples were left torecover for 1 min between protocols. Due to their viscoelasticproperties (Lee et al., 1984), the specimens were precondi-tioned, before each group of protocols, for 10 contiguous cyclesfirst to the maximum ϵCC and then to the maximum ϵRR of thegroup. The strain rate in the radial and circumferential direc-tion was defined as l0=min, with l0 being the sample edgelength. As the specimens were stretched, images werecaptured using a 1280�960 pixel charge-coupled device(CCD) camera at a sampling frequency of 5 Hz. The group ofprotocols that more closely achieved the valve working tension

j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7 559
was chosen for analysis. This was estimated to be approxi-mately 60 N/m for AV leaflets and 30 N/m for the PV (Mayneet al., 1989; Billiar and Sacks, 2000).
The software provided with the BioTester (CellScale,Canada) was used to define a grid of 25 points on the interiorportion of the specimen to track point motion. With theconfiguration of the grid in both undeformed and deformedsituations, the 2D deformation tensor F was determined foreach grid point, using a second-order method to computestrains from the discrete set of displacements (Geers et al.,1996). The undeformed situation was defined as the firstimage of the protocol.
Fig. 1 – Schematic representation of the angular fiberdistribution function. Indicated are the main fiber angle α,the dispersity β, and the local directions e
-1 and e
-2.
2.3. Constitutive equationsThe native heart valve was modeled as an incompressiblefiber-reinforced tissue (Lanir, 1983; Holzapfel et al., 2000). Thetotal Cauchy stress r consists of the hydrostatic pressure pand the extra stress τ:
r¼�pIþ τ: ð1Þ
The extra stress was split into an isotropic matrix contribu-tion and an anisotropic fiber contribution (van Oijen, 2003):
τ ¼ τ̂ þ ∑N
i ¼ 1ϕif ðψ i
f� e-i
f � τ̂ � e-i
f Þ e-i
f e-i
f ; ð2Þ
with τ̂ the isotropic matrix stress, ϕf the fiber volume fraction,ψ f the fiber stress, e
-
f the current fiber direction and N thenumber of fiber directions.
The isotropic matrix stress was modeled as a Neo-Hookeanmaterial with a shear modulus G. For the fibers, the followingconstitutive equation was used (Holzapfel et al., 2000):
ψ f ¼ k1λ2f ½ek2ðλ2f �1Þ�1�; ð3Þ
where k1 [N/mm2] and k2 [-] are material constants. The currentfiber direction e
-
f can be calculated from the fiber direction inthe undeformed configuration e
-
f0 with the relation:
λf e-
f ¼ F � e-f0 ð4Þ
with λf the fiber stretch λf ¼ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffie-
f0 � C � e-f0
qand C¼ FT � F the
right Cauchy-Green deformation tensor.The angular fiber distribution was incorporated into the
constitutive model by specifying an appropriate set of fiberdirections e
-
f0 and fiber contents ϕf . For that purpose, thefiber directions were defined as
e-
f0ðγiÞ ¼ cos ðγiÞv-
1 þ sin ðγiÞv-
2 ð5Þ
where γi was defined with respect to v-
1 in the plane spannedby v
-1 and v
-2 (Fig. 1). The vectors v
-1 and v
-2 are defined in
Section 2.7.For the fiber volume fraction a periodic version of the
normal probability distribution function was used (Gasseret al., 2006):
ϕif ¼A exp
cos ½2ðγi�αÞ� þ 1β
� �ð6Þ
with α the main fiber angle and β the dispersity of the fiberdistribution function. The scaling factor A was obtained by
defining the total fiber content to be equal to ϕtot.
A¼ ϕtot
∑Ni ¼ 1exp
cos ½2ðγi�αÞ�þ1β
h i ð7Þ
2.4. Collagen fiber remodeling
To model the fiber distribution, it was assumed that thepreferred main fiber direction αp is situated in between v
-1
and v-
2. Thus, stimulus functions g1 and g2 were introduced inthe direction of v
-1 and v
-2 (Driessen et al., 2008), and the
value of αp was then defined as
αp ¼ arctanðg2=g1Þ: ð8Þ
Two preferred main fiber orientations, situated at γ ¼7αpwere used to preserve material symmetry. The preferredvalue of fiber dispersity was given by
βp ¼
kðg1=g2Þ�1
if g1Zg2
kðg2=g1Þ�1
if g1og2
8>>><>>>:
ð9Þ
with k a scaling factor.Eqs. (8) and (9) imply that for g15g2 or g25g1 a uniaxial fiber
distribution (i.e. βp-0) is obtained with the preferred fiberdistribution close to v
-1 (i.e. αp-01) or v
-2 (i.e. αp-901), res-
pectively. Finally when g2≊g1 a uniform or sotropic fiberdistribution (i.e. βp-1) with the preferred fiber directionαp-451 is predicted (Fig. 2). The uniform and uniaxial fiberdistribution refers to a distribution with a maximum andminimum dispersity value, respectively (still to be specified).
The evolution of the main fiber direction and dispersity ofthe fiber distribution function were modeled by a first orderrate equation:
dαdt
¼ 1τa
ðαp�αÞdβdt
¼ 1τb
ðβp�βÞ ð10Þ
with τa and τb the time constants of the remodeling process.These parameters were set to 10 to guarantee small changes

Fig. 2 – (A) Definition of the preferred main fiber angle αp in respect to the stimulus functions g1 and g2 and (B) preferreddispersity βp as a function of the ratio of the stimulus function g1 and g2. (Modified from Driessen et al., 2008).
Fig. 3 – Finite element (FE) mesh of the heart valve leaflets(modified from Driessen et al., 2005).
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7560
in the collagen orientation in each time step that led tonumerical stable solutions.
2.5. Stimulus function
For the stimulus functions giði¼ 1;2Þ a strain-based and astress-based approach were adopted (Driessen et al., 2008).For the strain-based remodeling algorithm the stimulusfunctions were related to the stretch λi in the direction of v
-
i
gi ¼λχi �1 if λiZ1
0 if λio1
(ð11Þ
where χ is the power of alignment. For the stress-basedapproach the stimulus functions were set equal to the extrastresses τi in the direction of v
-
i
gi ¼τχi if τiZ0
0 if τio0:
(ð12Þ
with χ the power of alignment. The maximum and minimumvalues of the preferred dispersity were set to 1000 and 0.1, toprevent numerical problems with the expression of βp in Eq. (10).
Eqs. (8), (9), (11) and (12) result in an alignment of all fiberswith the major loading direction ðαp ¼ 01; βp ¼ 0Þ in case ofuniaxial loading conditions (g1a0 and gz¼0 or g1 ¼ 0 andg2a0). For biaxial loading conditions (g1a0 and g2a0), thefibers are situated in between v
-1 and v
-2 with the ratio
of the stimulus functions dictating the value of the mainorientation and dispersity. In case of an equibiaxial loadingcondition (g1 ¼ g2), the fibers are uniformly distributed in theplane of v
-1 and v
-2 (Fig. 2).
2.6. Balance equations
FEA was performed to simulate the mechanical response ofthe native valve during pressurization. Considering incom-pressibility, the continuity equation reduces to:
J�1¼ 0 ð13Þwhere the volume factor J¼ detðFÞ defines the ratio of thevolumes in the deformed and undeformed configuration. Thequasi-static balance of linear momentum, neglecting body
forces and inertia was written as
∇-
� r¼ 0-
ð14ÞThe balance equations were solved using the finite ele-
ment package SEPRAN (Segal, 1984). A mixed formulation wasused to account for incompressibility and the set of inter-polation functions for the displacement and pressure fieldhad to satisfy the Babuska–Brezzi condition. A hexahedralTaylor–Hood element was used, with a linear (continuous)interpolation for the pressure field and a quadratic interpola-tion for the displacement field.
2.7. Geometry and boundary conditions
Due to symmetry, 1/6 of a valve was used for the finiteelement analysis (Fig. 3). The radius was set to 12 mmand the thickness was obtained from the experimentalresults (0.82 mm for the AV and 0.62 mm for the PV). At thesymmetry surface the normal displacements were sup-pressed. The displacements at the bottom curve of the fixededge were also suppressed (stented valve). At the free edge,

Fig. 4 – Local direction v-
1 (left) and v-
2 (right) in theundeformed configuration of the valve leaflets
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7 561
a contact surface was defined to model contact between theleaflets (i.e. coaptation). On the top surface, a transvalvularpressure was applied. The pressure value was chosen torepresent the aortic valve pressure (12 kPa). To assure numer-ical stability a value of 5 kPa was added to the experimentallydetermined shear modulus G.
In the leaflets, the directions v-
1 and v-
2 were obtained fromthe stress based principal loading directions with isotropicmechanical properties (Driessen et al., 2008) (Fig. 4). The directionv-
1 was chosen to coincide with the major principal loadingdirection. The direction v
-2 is constructed perpendicular to the
direction v-
1 and to the normal to the plane of the leaflet ðn-Þ.When using the isotropic material response, the resulting v1 andv2 generally coincide with the circumferential and radial direc-tion, respectively. Furthermore, v
-1 enters the fixed edge radially,
consistent with observations from the literature that collagenfibers enter the aortic root perpendicular for an optimal transferof loads into the wall (Sauren, 1981).
2.8. Parameter estimation
Based on values in the literature for native heart valves (Basheyet al., 1967; Li et al., 2001) the total fiber volume fraction ϕtot wasset to 0.5. The results of a group of 5 protocols of independentbiaxial tensile tests (defined in Section 2.2) were fitted simulta-neously to estimate the material parameters (G, k1, k2, α and β)by minimizing the stress based nonlinear error function:
Error¼wc ∑nc
i ¼ 1ðsexp;ic �snum;i
c Þ2 þwr ∑nr
i ¼ 1ðsexp;ir �snum;i
r Þ2 ð15Þ
where s denotes the sample stress, w is a weighting factor andn is the number of data points. The subscripts c and r indicatethe circumferential and radial directions, respectively, where-as the superscripts exp and num refer to experimental data andthe values predicted by the constitutive model. The matrixparameter G was fit to the initial part of the curve while theremaining parameters to the complete curve. Per specimen allparameters were obtained and the averaged parameters of allspecimens were used for analysis. A nonlinear least-squaressolver is used from the software package MATLAB (The Math-Works, Inc, Natick, MA), to fit the numerical parameters to theexperimental data.
2.9. Statistical analysis
All data were presented as means and standard error of themean. The data was assumed to follow a normal distributionand therefore, a t-test was performed to check for significancein difference between the AV and the PV parameters. Statis-tical significance was assumed for a Po0:05.
3. Results
3.1. Mechanical properties
The constitutive model fitted the experimental data well Fig. 5and Fig. 6. The stress–stretch curves and the estimated valuesfor the model parameters indicated that the AV leaflets wereless extensible than the pulmonary tissues (Table 1). Results
also showed that the AV leaflets were more anisotropic thanthe PV leaflets. These differences were due to structural andmorphological variations between the AV and PV.
Structurally, the leaflets showed a collagen distributionwith a significantly different dispersity β ðPo0:05Þ. A largeror smaller value for β implies that the fibers are distributedmore or less uniformly and, consequently, the mechanicalresponses in the circumferential and radial directions aremore or less similar, respectively.
The matrix properties also differed for the leaflets,which had a significantly different G modulus ðPo0:05Þ. Thisparameter dictates the slope of the initial part of the curve.Morphologically, the leaflets of the AV were significantlythicker when compared to the PV ðPo0:01Þ.
3.2. Mechanical behavior
The simulated stress–stretch curves of a node in the bellyregion of the AV and PV leaflets after aortic pressurization areshown in Fig. 7. It is noticeable that both valves respondedsimilarly to the aortic diastolic pressure. Yet, the PV leaf-lets behaved less anisotropic than the AV leaflets, which wasa result of the large dispersity of the PV collagen distributioncompared to the AV. A larger value for the dispersity impliesthat the fibers are distributed more uniformly and, conse-quently, the mechanical responses in both directions are moresimilar. Furthermore, the PV leaflets appeared to be moreextensible and reach higher stresses than the AV leaflet.
The simulated evolution of the leaflets' symmetry line(Fig. 3) during pressure application is shown in Fig. 8. Dueto the collagen organization, the PV leaflets deflected more inthe radial direction than the AV leaflets. As a result, thedeformed configuration of the PV leaflets showed a smallercoaptation surface than the AV leaflets.
3.3. Remodeling
Both the observed increase in thickness of valve explants andthe importance of the collagen architecture in the leafletsmechanical properties were taken into account. Therefore, wheninvestigating the potential remodeling of the PV leaflets sub-jected to diastolic aortic pressure, 3 remodeling responses wereinvestigated:
Case 1
The thickness parameter T was increased whilemaintaining the total collagen volume fraction con-stant ðϕtot ¼ 0:5Þ.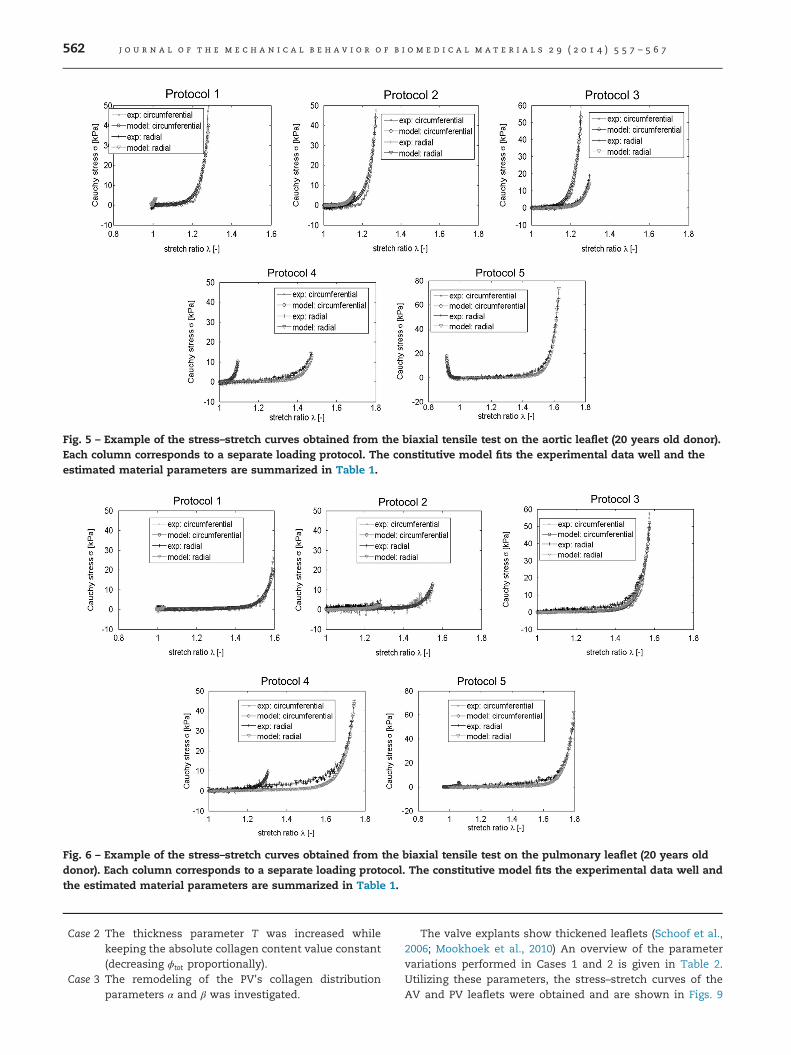
Fig. 5 – Example of the stress–stretch curves obtained from the biaxial tensile test on the aortic leaflet (20 years old donor).Each column corresponds to a separate loading protocol. The constitutive model fits the experimental data well and theestimated material parameters are summarized in Table 1.
Fig. 6 – Example of the stress–stretch curves obtained from the biaxial tensile test on the pulmonary leaflet (20 years olddonor). Each column corresponds to a separate loading protocol. The constitutive model fits the experimental data well andthe estimated material parameters are summarized in Table 1.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7562
Case 2
The thickness parameter T was increased whilekeeping the absolute collagen content value constant(decreasing ϕtot proportionally).Case 3
The remodeling of the PV's collagen distributionparameters α and β was investigated.The valve explants show thickened leaflets (Schoof et al.,
2006; Mookhoek et al., 2010) An overview of the parametervariations performed in Cases 1 and 2 is given in Table 2.Utilizing these parameters, the stress–stretch curves of theAV and PV leaflets were obtained and are shown in Figs. 9
Table 1 – Fitted parameters of the numerical model for the aortic valve and pulmonary valve leaflets. The data is presentedas means and the standard error of the mean, t-test.
Tissue G (kPa) α (deg) β (–) k1 (kPa) k2 (–) T (mm)
AV 1.5070.30a 14.8571.86 0.2170.03a 0.1670.06 15.1875.42 0.9070.05b
PV 0.9270.09a 21.6273.36 0.3070.03a 0.0670.04 13.8271.07 0.6270.02b
a Po0:05.b Po0:01.
Fig. 7 – Simulated stress–stretch curves in thecircumferential and radial directions for a node in the bellyregion of the aortic valve leaflets (black) and the pulmonaryvalve leaflet (grey).
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7 563
and 10, respectively. The stress–stretch curves were takenfrom a node in the AV and PV leaflets belly region duringpressurization. For the AV the experimentally obtained thick-ness was considered while for the PV the influence of anincreased thicknesses was investigated. Fig. 9 shows thatwhen the thickness of the PV increased, the nodal maximumstress is decreased. This trend is also observed in Fig. 10,when maintaining the absolute collagen content constant.Yet, the decrease in collagen volume fraction resulted in aslight decrease in the stiffness of the curves.
For Case 3, the remodeling parameter χ that better des-cribe the fitted collagen distribution parameters of the AVleaflets was first estimated for both the strain and stressdependent algorithms (Eqs. (11) and (12), respectively).Numerical simulations of the leaflet pressurization wereperformed and the collagen architecture parameters α and β
were left to remodel until stable values were obtained. Tostart with an isotropic fiber distribution, the initial α and β
were set to 14.851 and 100, respectively. For the straindependent algorithm χ ¼ 0:1 was obtained and for the stressdependent algorithm χ ¼ 1:0, respectively. The acquired col-lagen remodeling parameters α and β are summarized inTable 3. The values obtained with the stress dependentalgorithm approximated better the fitted collagen architec-ture parameters. This was also observed when comparing thestretch-stress curve of a node in the belly region (Fig. 11).Results showed that the stress–stretch curves obtained withthis algorithm (blue curve in Fig. 11) approximated better theAV leaflet stress–stretch curves (black curve in Fig. 11). Highervalues for the same parameters were obtained when a straindependent algorithm was applied. This was characteristic of
a more isotropic average collagen distribution that resulted ina more isotropic mechanical response (red curve in Fig. 11).
The remodeling of the PV in the aortic position was theninvestigated. The estimated χ values of the AV leaflet wereused and the initial values for α and β were set to 21.621 and100, respectively. The obtained α and β are shown in Table 3and the resulting stretch-stress curves of a node in the bellyregion are shown in Fig. 12. The stress dependent algorithmresulted in a decreased α, i.e. in the rotation of the collagenfibers toward the circumferential direction. In contrast, therotation of the fiber away from the circumferential directionwas predicted with the strain dependent algorithm. Observeddifferences in the final collagen architecture were due to thedifferent distribution of the principal strain and stress direc-tions in the leaflets (Fig. 13). Furthermore, the remodeledstress–stretch curves (blue and red curve in Fig. 12) and theAV leaflet stress–stretch curves (black curve in Fig. 12) werenot completely identical. This shows that collagen remodel-ing alone was not sufficient for a complete remodel of the PVleaflet toward an AV leaflet.
4. Discussion
In the present study, a structure-based numerical model wasapplied to assess and evaluate the mechanical propertiesof pairs of human aortic and pulmonary donor valves. Themodel was employed to evaluate and demonstrate valvularbehavior in the Ross procedure. Furthermore, numericalremodeling laws were applied to assess the change in proper-ties of the PV leaflet in the aortic position. The resultsfrom biaxial tensile tests were used to determine the modelparameters. Comparing the results from both valves it wasobserved that the PV leaflet were more extensible than theAV tissues. The PV leaflets was also less anisotropic than theAV leaflets. Results also showed that the AV leaflets werethicker than the PV leaflets. When subjected to the aorticdiastolic pressure, the simulated stresses in the PV leafletstissue were also higher and the simulated coaptation areawas smaller than in the AV leaflets. Furthermore, our studysuggested that the PV leaflets appear to remodel by increas-ing its thickness and rotating its fibers toward the circumfer-ential direction. However, these changes were not sufficientfor the complete remodel of the PV leaflet toward an AVstructure.
Previous studies comparing the AV and PV leaflets mec-hanical properties showed minimal differences betweenthese structures, both for human (Stradins et al., 2004) andporcine tissues (David et al., 1994). However, Joyce et al.
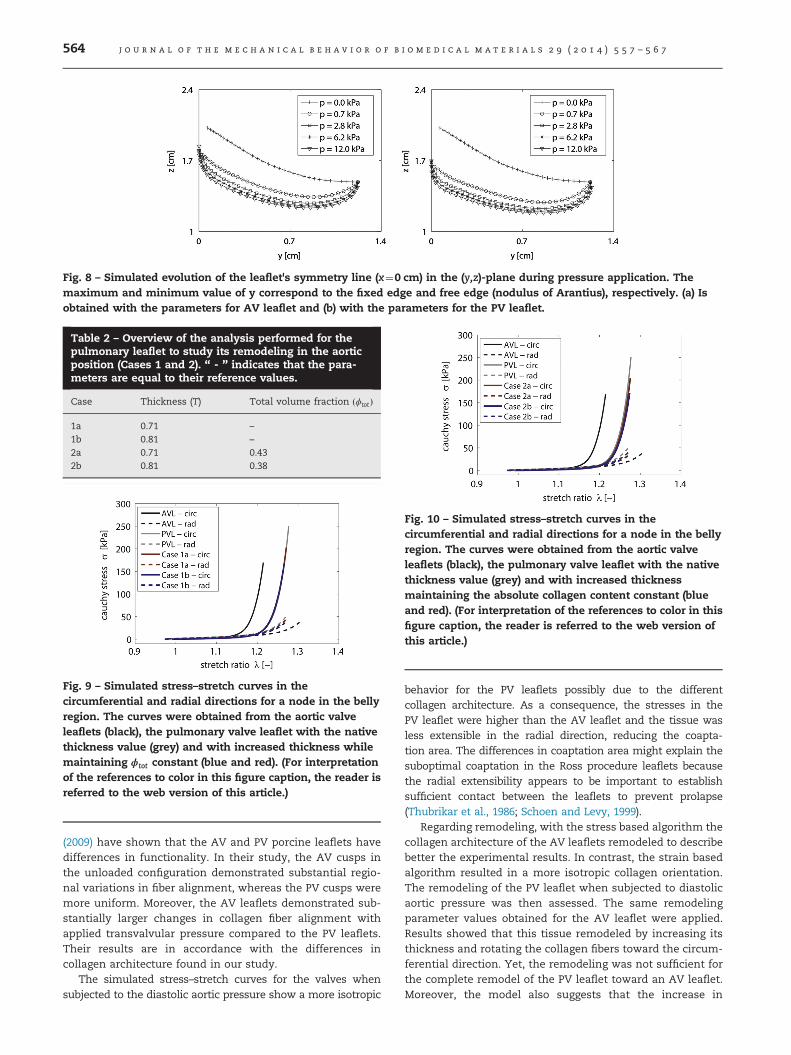
Table 2 – Overview of the analysis performed for thepulmonary leaflet to study its remodeling in the aorticposition (Cases 1 and 2). “ - ” indicates that the para-meters are equal to their reference values.
Case Thickness (T) Total volume fraction ðϕtotÞ
1a 0.71 –
1b 0.81 –
2a 0.71 0.432b 0.81 0.38
Fig. 9 – Simulated stress–stretch curves in thecircumferential and radial directions for a node in the bellyregion. The curves were obtained from the aortic valveleaflets (black), the pulmonary valve leaflet with the nativethickness value (grey) and with increased thickness whilemaintaining ϕtot constant (blue and red). (For interpretationof the references to color in this figure caption, the reader isreferred to the web version of this article.)
Fig. 8 – Simulated evolution of the leaflet's symmetry line (x¼0 cm) in the (y,z)-plane during pressure application. Themaximum and minimum value of y correspond to the fixed edge and free edge (nodulus of Arantius), respectively. (a) Isobtained with the parameters for AV leaflet and (b) with the parameters for the PV leaflet.
Fig. 10 – Simulated stress–stretch curves in thecircumferential and radial directions for a node in the bellyregion. The curves were obtained from the aortic valveleaflets (black), the pulmonary valve leaflet with the nativethickness value (grey) and with increased thicknessmaintaining the absolute collagen content constant (blueand red). (For interpretation of the references to color in thisfigure caption, the reader is referred to the web version ofthis article.)
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7564
(2009) have shown that the AV and PV porcine leaflets havedifferences in functionality. In their study, the AV cusps inthe unloaded configuration demonstrated substantial regio-nal variations in fiber alignment, whereas the PV cusps weremore uniform. Moreover, the AV leaflets demonstrated sub-stantially larger changes in collagen fiber alignment withapplied transvalvular pressure compared to the PV leaflets.Their results are in accordance with the differences incollagen architecture found in our study.
The simulated stress–stretch curves for the valves whensubjected to the diastolic aortic pressure show a more isotropic
behavior for the PV leaflets possibly due to the differentcollagen architecture. As a consequence, the stresses in thePV leaflet were higher than the AV leaflet and the tissue wasless extensible in the radial direction, reducing the coapta-tion area. The differences in coaptation area might explain thesuboptimal coaptation in the Ross procedure leaflets becausethe radial extensibility appears to be important to establishsufficient contact between the leaflets to prevent prolapse(Thubrikar et al., 1986; Schoen and Levy, 1999).
Regarding remodeling, with the stress based algorithm thecollagen architecture of the AV leaflets remodeled to describebetter the experimental results. In contrast, the strain basedalgorithm resulted in a more isotropic collagen orientation.The remodeling of the PV leaflet when subjected to diastolicaortic pressure was then assessed. The same remodelingparameter values obtained for the AV leaflet were applied.Results showed that this tissue remodeled by increasing itsthickness and rotating the collagen fibers toward the circum-ferential direction. Yet, the remodeling was not sufficient forthe complete remodel of the PV leaflet toward an AV leaflet.Moreover, the model also suggests that the increase in
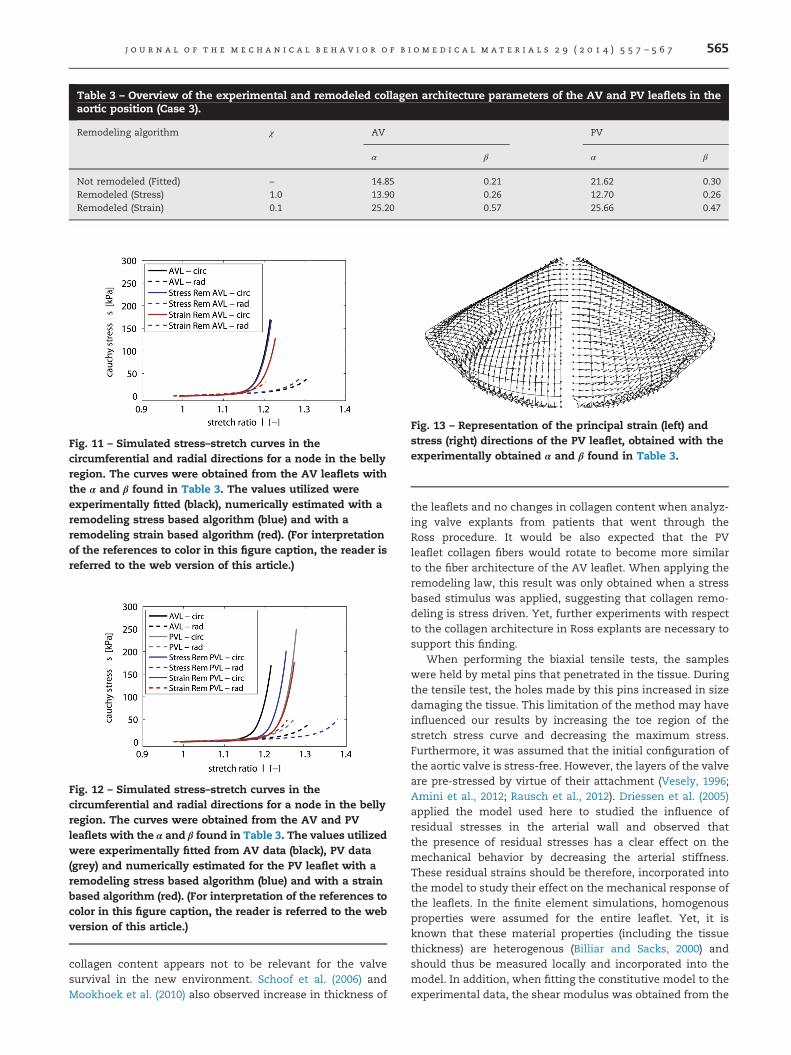
Table 3 – Overview of the experimental and remodeled collagen architecture parameters of the AV and PV leaflets in theaortic position (Case 3).
Remodeling algorithm χ AV PV
α β α β
Not remodeled (Fitted) – 14.85 0.21 21.62 0.30Remodeled (Stress) 1.0 13.90 0.26 12.70 0.26Remodeled (Strain) 0.1 25.20 0.57 25.66 0.47
Fig. 11 – Simulated stress–stretch curves in thecircumferential and radial directions for a node in the bellyregion. The curves were obtained from the AV leaflets withthe α and β found in Table 3. The values utilized wereexperimentally fitted (black), numerically estimated with aremodeling stress based algorithm (blue) and with aremodeling strain based algorithm (red). (For interpretationof the references to color in this figure caption, the reader isreferred to the web version of this article.)
Fig. 12 – Simulated stress–stretch curves in thecircumferential and radial directions for a node in the bellyregion. The curves were obtained from the AV and PVleaflets with the α and β found in Table 3. The values utilizedwere experimentally fitted from AV data (black), PV data(grey) and numerically estimated for the PV leaflet with aremodeling stress based algorithm (blue) and with a strainbased algorithm (red). (For interpretation of the references tocolor in this figure caption, the reader is referred to the webversion of this article.)
Fig. 13 – Representation of the principal strain (left) andstress (right) directions of the PV leaflet, obtained with theexperimentally obtained α and β found in Table 3.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7 565
collagen content appears not to be relevant for the valvesurvival in the new environment. Schoof et al. (2006) andMookhoek et al. (2010) also observed increase in thickness of
the leaflets and no changes in collagen content when analyz-ing valve explants from patients that went through theRoss procedure. It would be also expected that the PVleaflet collagen fibers would rotate to become more similarto the fiber architecture of the AV leaflet. When applying theremodeling law, this result was only obtained when a stressbased stimulus was applied, suggesting that collagen remo-deling is stress driven. Yet, further experiments with respectto the collagen architecture in Ross explants are necessary tosupport this finding.
When performing the biaxial tensile tests, the sampleswere held by metal pins that penetrated in the tissue. Duringthe tensile test, the holes made by this pins increased in sizedamaging the tissue. This limitation of the method may haveinfluenced our results by increasing the toe region of thestretch stress curve and decreasing the maximum stress.Furthermore, it was assumed that the initial configuration ofthe aortic valve is stress-free. However, the layers of the valveare pre-stressed by virtue of their attachment (Vesely, 1996;Amini et al., 2012; Rausch et al., 2012). Driessen et al. (2005)applied the model used here to studied the influence ofresidual stresses in the arterial wall and observed thatthe presence of residual stresses has a clear effect on themechanical behavior by decreasing the arterial stiffness.These residual strains should be therefore, incorporated intothe model to study their effect on the mechanical response ofthe leaflets. In the finite element simulations, homogenousproperties were assumed for the entire leaflet. Yet, it isknown that these material properties (including the tissuethickness) are heterogenous (Billiar and Sacks, 2000) andshould thus be measured locally and incorporated into themodel. In addition, when fitting the constitutive model to theexperimental data, the shear modulus was obtained from the

j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7566
initial 20% of the curve only considering the isotropic part ofthe model. This methodology provided a more representativevalue for G and a decrease in parameters when fitting to theexperimental curve. For the FEA simulations, the value usedfor the shear modulus was the lowest value possible that ledto stable solutions. Since the tissue mechanical behavior ismainly governed by the collagen fibers the increase in G is notexpected to affect our results. Furthermore, the instabilitymay be localized and may have no influence in the overallbehavior of the tissue. A Gaussian function was assumed forthe fiber distribution based on measurements obtained fromnative porcine leaflets (Billiar and Sacks, 2000) and the mainfiber angle α and standard deviation β were estimated by theparameter fitting algorithm. Several techniques exist to deter-mine the collagen architecture quantitatively and experimentson native tissues should be performed. Techniques such assmall angle light scattering (Billiar and Sacks, 2000; Sacks, 2003),polarized light microscopy (Finlay et al., 1995; Canham et al.,1997), confocal (reflection) laser scanning microscopy and two-photon microscopy, using fluorescent probes to label collagen(Rubbens et al., 2009; Soares et al., 2011) can be used to assessthe collagen architecture. It may then be possible to incorporatethe measured fiber distribution directly into the model, therebyfurther reducing the number of model parameters. At largerstrains, the experimentally measured mechanical responsestended to behave more linear than the exponential constitutivemodel for the fibers (Fig. 2). Models that account for fiberrecruitment (Sacks, 2003) might be more appropriate to describethis phenomenon. Furthermore, stress and stretch remodelingstimuli are widely used in the literature and their predictionsqualitatively agree with observations from the literature fornative tissues (Rodriguez et al., 1994; Taber and Eggers, 1996; Linand Taber, 1995; Cowin, 1996). Yet, the mechanism by whichcells remodeled the collagen fibers is not fully understood. It isknown that collagen fibrils align with cells in many nativetissues suggesting that cells remodeled the extracellular matrixin such a way that the collagen fibers aligned with the preferredfiber directions. This may either be the result of cells contractileforces deforming the matrix by reorienting the collagen fibers(Friedrichs et al., 2007). Or the collagen fibers increased resis-tance against enzymatic degradation with increasing strain orstress (Bhole et al., 2009). Further experimental work has to beperformed to further clarify the exact mechanisms of theseprocesses and to determine their relative contributions tocollagen reorganization. In addition, the current model focusedmainly on the collagen thickness and fiber orientation however,the effect of remodeling on other collagen fibers properties suchas cross-linking should also be addressed when studying theremodeling in native cardiovascular tissues. It is known that inresponse to environmental cues, collagen fibers can alsoincrease in size and become crosslinked (Clark, 1996; Rubinand Farber, 1998).
Despite the limitations, our study revealed structuraldifferences between the AV and PV. These variations resultedin a more extensible and less anisotropic behavior of the PVleaflet as compared to the AV leaflet. When exposed to aorticpressure, the PV leaflet appeared to remodel by increasing itsthickness and reorganizing its collagen, rotating it toward thecircumferential direction. Yet, this remodeling did not resultin properties that are completely identical to the AV leaflet.
Therefore, to fully elucidate the potential of the PV leaflet forthe Ross procedure, the adaptive remodeling of other matrixcomponents such as elastin should be taken into account.Also, a better understanding of the native tissue proper-ties and their adaptation capabilities to different mechanicalenvironments, as shown in this study, can be used to opti-mize mechanical conditioning protocols in heart valves TE.
r e f e r e n c e s
Amini, R., Eckert, C., Koomalsingh, K., McGarvey, J., Minakawa, M.,Gorman, J., Gorman, R., Sacks, M., 2012. Springer US; on thein vivo deformation of the mitral valve anterior leaflet: effects ofannular geometry and referential configuration. Annals ofBiomedical Engineering 40 (7), 1455–1467.
Azadani, A.N., Chitsaz, S., Matthews, P.B., Jaussaud, N., Leung, J.,Wisneski, A., Ge, L., Tseng, E.E., 2012. Biomechanicalcomparison of human pulmonary and aortic roots. EuropeanJournal of Cardio-Thoracic Surgery: Official Journal of theEuropean Association for Cardio-Thoracic Surgery 41 (5),1111–1116.
Bashey, R.I., Torii, S., Angrist, A., 1967. Age-related collagen andelastin content of human heart valves. Journal of Gerontology22, 203–208.
Bhole, A.P., Flynn, B.P., Liles, M., Saeidi, N., Dimarzio, C.A.,Ruberti, J.W., 2009. Mechanical strain enhances survivabilityof collagen micronetworks in the presence of collagenase:implications for load-bearing matrix growth and stability.Physical and Engineering Sciences 367 (1902), 3339–3362.
Billiar, K.L., Sacks, M.S., 2000. Biaxial mechanical properties of thenative and glutaraldehyde-treated aortic valve cusp: part ii – astructural constitutive model. Journal of BiomechanicalEngineering 122 (4), 327–335.
Canham, P., Finlay, H., Boughner, D., 1997. Contrasting structure ofthe saphenous vein and internal mammary artery used ascoronary bypass vessels. Cardiovascular Research 34 (3), 557–567.
Chambers, J.C., Somerville, J., Stone, S., Ross, D.N., 1997.Pulmonary autograft procedure for aortic valve disease: long-term results of the pioneer series. Circulation 96 (7),2206–2214.
Cowin, S.C., 1996. Strain or deformation rate dependent finitegrowth in soft tissues. Journal of Biomechanics 29 (5), 647–649.
Clark, R.A.F., 1996. The Molecular and Cellular Biology of WoundRepair, New York, Plenum press.
David, H., Boughner, D.H., Vesely, I., Gerosa, G., 1994. Thepulmonary valve. Is it mechanically suitable for use as anaortic valve replacement? ASAIO Journal 40 (2), 206–212.
Driessen, N.J.B., Bouten, C.V.C., Baaijens, F.P.T., 2005. A structuralconstitutive model for collagenous cardiovascular tissuesincorporating the angular fiber distribution. Journal ofBiomechanical Engineering-Transactions of the ASME 127 (3),403–494.
Driessen, N.J.B., Cox, M.A.J., Bouten, C.V.C., Baaijens, F.P.T., 2008.Remodelling of the angular collagen fiber distribution incardiovascular tissues. Biomechanics and Modeling inMechanobiology 7 (2), 93–103.
Elkins, R.C., Knott-Craig, C.J., Ward, K.E., McCue, C., Lane, M.M.,1994. Pulmonary autograft in children: realized growthpotential. The Annals of Thoracic Surgery 57 (6), 1387–1394.
Elkins, R.C., Thompson, D.M., Lane, M.M., Elkins, C.C., Peyton, M.D.,2008. Ross operation: 16-year experience. Journal of Thoracicand Cardiovascular Surgery 136 (3), 623–630 630.e1-5.
Favaloro, R.R., Roura, P., Gomez, C., Salvatori, C., 2008. Aorticvalve replacement: ten-year follow up of the Ross procedure.Journal of Heart Valve Disease 17 (5), 501–507.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 2 9 ( 2 0 1 4 ) 5 5 7 – 5 6 7 567
Finlay, H., Mccullough, L., Canham, P., 1995. 3-Dimensional collagenorganization of human brain arteries at different transmuralpressures. Journal of Vascular Research 32 (5), 301–312.
Friedrichs, J., Taubenberger, A., Franz, C.M., Muller, D.J., 2007.Cellular remodelling of individual collagen fibrils visualized bytime-lapse AFM. Journal of Molecular Biology 372 (3), 594–607.
Gasser, T.C., Ogden, R.W., Holzapfel, G.A., 2006. Hyperelasticmodelling of arterial layers with distributed collagen fibreorientations. Journal of the Royal Society Interface 3 (6), 15–35.
Geers, M.G.D., deBordt, R., Brekelmans, W.A.M., 1996. Computingstrain fields from discrete displacement fields in 2D solids.International Journal of Solids and Structures 33 (29),4293–4307.
Gerson, C., Goldstein, S., Heacox, A.E., 2009. Retained structuralintegrity of collagen and elastin within cryopreserved humanheart valve tissue as detected by two-photon laser scanningconfocal microscopy. Cryobiology 59 (2), 171–179.
Hokken, R.B., Bartelings, M.M., Bogers, A.J., deGroot, A.C.G., 1997.Morphology of the pulmonary and aortic roots with regard tothe pulmonary autograft procedure. The Journal of Thoracicand Cardiovascular Surgery 113 (3), 453–461.
Holzapfel, G.A., Gasser, T.C., Ogden, R.W., 2000. A new constitutiveframework for arterial wall mechanics and a comparative studyof material models. Journal of Elasticity 61 (1–3), 1–48.
Joyce, E.M., Liao, J., Schoen, F.J., Jr. J.E.M., Sacks, M.S., 2009.Functional collagen fiber architecture of the pulmonary heartvalve cusp. The Annals of Thoracic Surgery 87 (4), 1240–1249.
Kouchoukos, N.T., 2011. Should we still do the Ross operation inadults? Current Opinion in Cardiology 26 (2), 94–98.
Lanir, Y., 1983. Constitutive-equations for fibrous connectivetissues. Journal of Biomechanics 16 (1), 1–12.
Lee, J.M., Courtman, D.W., Boughner, D.R., 1984. Theglutaraldehyde-stabilized porcine aortic valve xenograft. I.Tensile viscoelastic properties of the fresh leaflet material.Journal of Biomedical Materials Research 18 (1), 61–77.
Li, J., Luo, X., Kuang, Z., 2001. A nonlinear anisotropic model forporcine aortic heart valves. Journal of Biomechanics 34 (10),1279–1289.
Lin, I.E., Taber, L.A., 1995. A model for stress-induced growth inthe developing heart. Journal of Biomechanical Engineering-Transactions of the ASME 117 (3), 343–349.
Mayne, A., Christie, G., Smaill, B., Hunter, P., Barratt-Boyes, B.G.,1989. An assessment of the mechanical properties of leafletsfrom four second-generation porcine bioprostheses withbiaxial testing techniques. Journal of Thoracic andCardiovascular Surgery 98, 170–180.
Mookhoek, A., deHeer, E., Bogers, A.J.J.C., Takkenberg, J.J.M.,Schoof, P.H., 2010. Pulmonary autograft valve explants showtypical degeneration. Journal of Thoracic and CardiovascularSurgery 139 (6), 1416–1419.
Phillips, J.R., 2003. Long-term outcomes of the Ross operation inchildren and adults. Progress in Pediatric Cardiology 16 (2),149–154.
Rabkin-Aikawa, E., Aikawa, M., Farber, M., Kratz, J.R., 2004.Clinical pulmonary autograft valves: pathologic evidence ofadaptive remodeling in the aortic site. The Journal of Thoracicand Cardiovascular Surgery 128 (4), 552–561.
Rausch, M., Famaey, N., Shultz, T., Bothe, W., Miller, D., Kuhl, E.,2012. Springer-Verlag; Mechanics of the mitral valve.Biomechanics and Modeling in Mechanobiology, 1–19.
Rodriguez, E.K., Hoger, A., Mcculloch, A.D., 1994. Stress-dependent finite growth in soft elastic tissues. Journal ofBiomechanics 27 (4), 455–467.
Ross, D.N., 1967. Replacement of aortic and mitral valve with apulmonary autograft. The Lancet 290 (7523), 956–958.
Rubin, E., Farber, J.L., 1998. Pathology, Philadelphia: Lippincott-Raven publishers.
Rubbens, M.P., Mol, A., vanMarion, M.H., Hanemaaijer, R., Bank, R.A.,Baaijens, F.P.T., Bouten, C.V.C., 2009. Straining mode-dependentcollagen remodeling in engineered cardiovascular tissue. TissueEngineering Part A 15 (4), 841–849.
Sacks, M., 2003. Incorporation of experimentally-derived fiberorientation into a structural constitutive model for planar-collagenous tissues. Journal of Biomechanical Engineering-Transactions of the ASME 125 (2), 280–287.
Santini, F., Dyke, C., Edwards, S., Stavri, G., Feccia, M., Khan, H.,Birks, E., Yacoub, M.H., 1997. Pulmonary autograft versushomograft replacement of the aortic valve: a prospectiverandomized trial. The Journal of Thoracic and CardiovascularSurgery 113 (5), 894–900.
Sauren, A.A.H.J., 1981. The Mechanical Behavior of the AorticValve. Eindhoven University of Technology, The Netherlands.
Schoen, F.J., Levy, R.J., 1999. Tissue heart valves: currentchallenges and future research perspectives. Journal ofBiomedical Materials Research 47, 439–465.
Schoof, P.H., Takkenberg, J.J., vanSuylen, R.J., Zondervan, P.E.,Hazekamp, M.G., Dion, R.A., Bogers, A.J., 2006. Degenerationof the pulmonary autograft: an explant study. TheJournal of Thoracic and Cardiovascular Surgery 132 (6),1426–1432.
Segal, A., 1984. SEPRAN User Manual, Standard Problems andProgrammers guide. The Netherlands: Leidschendam:Ingenieursbureau SEPRA.
Soares, A.L.F., Stekelenburg, M., Baaijens, F.P.T., 2011.Remodelling of the collagen fiber architecture due tocompaction in small vessels under tissue engineeredconditions. Journal of Biomechanical Engineering 7 (133).
Stradins, P., Lacis, R., Ozolanta, I., Purina, B., Ose, V., Feldmane, L.,Kasyanov, V., 2004. Comparison of biomechanical andstructural properties between human aortic and pulmonaryvalve. European Journal of Cardio-Thoracic Surgery 26 (3),634–639.
Taber, L.A., Eggers, D.W., 1996. Theoretical study of stress-modulated growth in the aorta. Journal of Theoretical Biology180 (4), 343–357.
Takkenberg, J., Klieverik, L., Schoof, P., Suylen, R.J.V., Herwerden,L.V., Zondervan, P., Roos-Hesselink, J., Eijkemans, M., Yacoub,M., Bogers, A., 2009. The Ross procedure: a systematic reviewand meta-analysis. Circulation (Baltimore) 119 (2), 222–228.
Thubrikar, M.J., Aouad, J., Nolan, S.P., 1986. Comparison of the invivo and in vitro mechanical properties of aortic valve leaflets.Journal of Thoracic and Cardiovascular Surgery 92, 29–36.
van Oijen, C.H.G.A., 2003. Mechanics and Design of Fiber-Reinforced Vascular Protheses. Eindhoven University ofTechnology, The Netherlands.
Vesely, I., Casarotto, D., Gerosa, G., 2000. Mechanics ofcryopreserved aortic and pulmonary homografts. Journal ofHeart Valve Disease 9 (1), 27–37.
Vesely, I., 1996. Reconstruction of loads in the fibrosa andventricularis of porcine aortic valves. ASAIO Journal 42,M739–M746.
Virues Delgadillo, J., Delorme, S., El-Ayoubi, R., DiRaddo, R.,Hatzikiriakos, S., 2010. Effect of freezing on the passivemechanical properties of arterial samples. Journal ofBiomedical Science and Engineering 3, 645–652.