mechanical ventilation, sedation and neuromuscular blockade dr. mohammad aljawadi pharmd, msc, phd...
TRANSCRIPT

Mechanical Ventilation, Sedation and Neuromuscular Blockade
Dr. Mohammad Aljawadi PharmD, Msc, PhD
PHCL 478
Clinical Pharmacy Department
College of Pharmacy
King Saud University
APRIL 2015
1

A disclaimer and an acknowledgment:
Part of these slides was prepared by
Dr. Rashid Amin Pharm D., BCPS
Clinical Pharmacy Specialist- Adult Critical Care
King Faisal Hospital & Research Centre
and have been used with his permission
2

Respiratory System Overview
http://en.wikipedia.org/wiki/Respiratory_system
3

Causes for Inadequate Ventilation and Respiratory Failure
4

First Steps
Oxygen Supplementation B2-Agonists Ipratropium Corticosteroids
5

First Steps
Oxygen Supplementations:
6

B2-Agonists
Stimulation of β2-adrenergic receptors causes bronchial and vascular smooth-muscle relaxation
Metered-dose inhaler or by intermittent or continuous nebulization
No role for long acting agents
7

Anticholinergic Agents
Ipratropium bromide competes with acetylcholine at the bronchial receptor site, resulting in bronchial smooth-muscle relaxation.
Metered-dose inhaler or by intermittent or continuous nebulization
More delayed onset of action than β2-agonists The addition of ipratropium to albuterol appears to have an
additive benefit in approximately 30% of asthma patients.
8

Corticosteroids The benefit from aggressive corticosteroid use in asthmatic patients
with ARF is well documented. Decrease β-receptor tachyphylaxis. Limited consensus exists on dosing schedules in asthma.
Doses of methylprednisolone of 80 mg/24 h have been as effective as >360 mg/24 hr. OR 1 mg/kg/24 h, adjusting as patient response dictates.
The intravenous and oral routes are equally effective. Routine use of inhalational agents is not recommended in the setting of acute
severe bronchospasm. Myopathies with moderate to high doses
9

10

If First Steps Fail then Mechanical Ventilation is the Way to Go
A ventilator is a device used to assist or replace the work of the respiratory system.
Mechanical Ventilation: Positive pressure ventilation
Air is pushed into the lungs Negative Pressure ventilation (Less used nowadays)
Air is sucked into the lungs
11
Mechanical Ventilation
Non-Invasive Noninvasive Positive Pressure Ventilation (mainly)
A form of mechanical ventilation that provides respiratory assistance without an invasive artificial airway
Invasive
12

Noninvasive Positive Pressure Ventilation
fear of having no escape or being closed-in
13

Noninvasive Positive Pressure Ventilation14

Invasive Mechanical Ventilation 15

THE IRON LUNG16
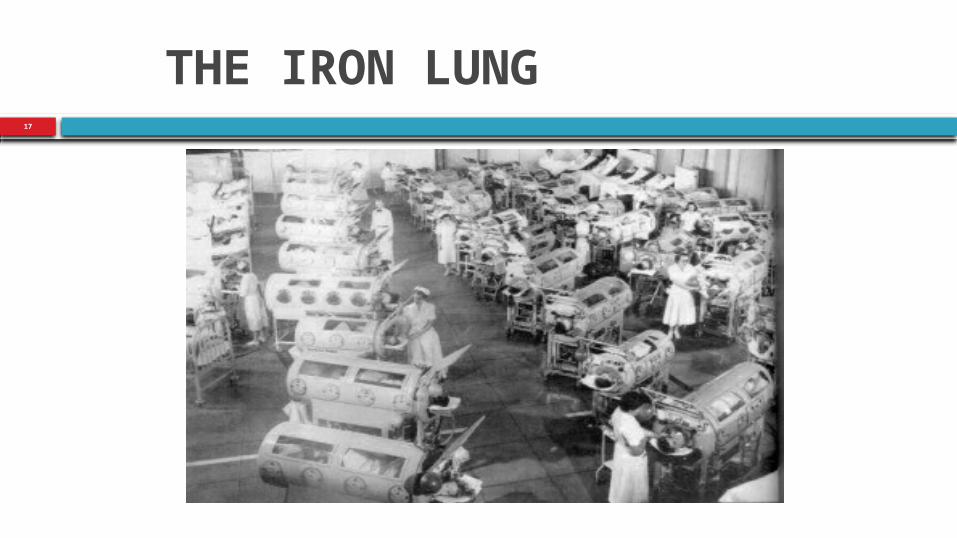
THE IRON LUNG17
18
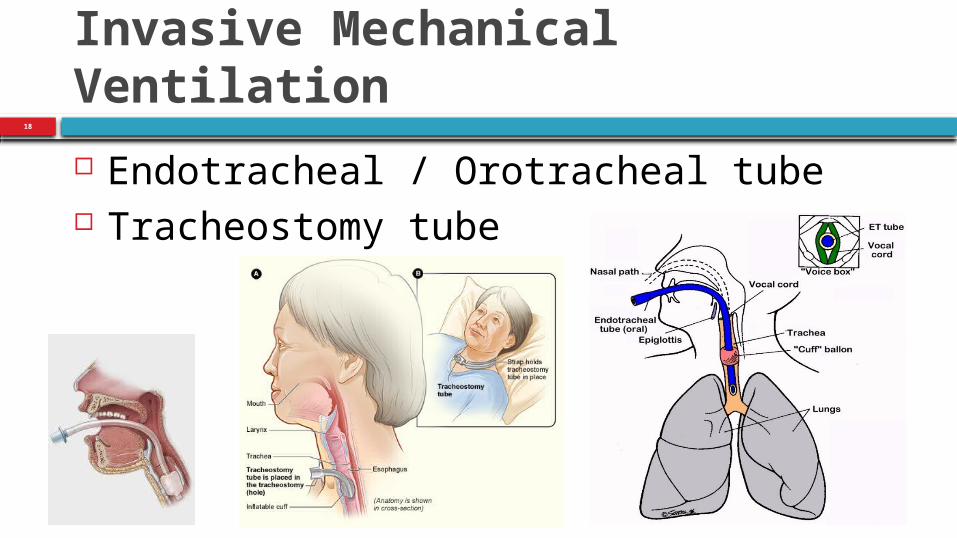
Invasive Mechanical Ventilation
Endotracheal / Orotracheal tube Tracheostomy tube

19
Tracheostomy
Surgically created passage into the trachea for long term MV Do not necessitate any use of sedative drugs.
Inserted early: In patients with pre-existing severe respiratory disease Patients expected to be difficult to wean from mechanical
ventilation, i.e., patients with little muscular reserve.

Tracheostomy Advantages and Disadvantages
Advantages Reduced sedation requirement (greater
comfort than endotracheal intubation) Airway protection while unconscious Allows gradual weaning of ventilatory
support (reduced work of breathing) Enhanced communication (written or
phonation) Enhanced nursing care (mouth care and
mobility) Avoids laryngeal injury Can facilitate transfer to the ward Possibly reduces VAP (studies conflicting)
Disadvantages
Requirement for a surgical procedure with inherent risk of complications
Longterm benefit not shown (studies conflicting)
20

21
Ventilator Complications Pulmonary barotrauma
Pneumothorax (abnormal collection of air in the pleural space) Pneumomediastinum (air in chest cavity) Bronchopleural fistula (fistula between the pleural space and the lung)
Diaphragm atrophy Air embolism Motility of mucocilia in the airways
↑ Ventilator Associated pneumonia (VAP)

22
Weaning from mechanical ventilation When should we start thinking about weaning?
The day we intubate the patient (always plan ahead)
Should not be delayed unnecessarily, nor should it be done prematurely.
Patients should have their ventilation considered for withdrawal if they are able to support their own ventilation and oxygenation, and this should be assessed continuously.
Trials of spontaneous breathing
23
Factors which Lead to failed extubation
Underlying chronic cardiac or respiratory disease Time on ventilator Anything that contributes to muscle weakness:
High dose and prolonged use of steroids Neuromuscular blockade agents High dose opioids, benzodiazepines Insufficient caloric intake

24
Things to Remember
Every failed extubation and subsequent re-intubation has shown to increase mortality
Must have the followings: Cardiovascular stability No atelectasis (collapse or closure of the lung) Resolution of Pneumonia Good cough reflex Minimal tracheal secretions

25
Summary Mechanical ventilation can be life saving Start thinking about extubation from the day you intubate the patient Assess patient frequently by giving them Trials of spontaneous
breathing Be aware of complications such as Ventilator Associated Pneumonia,
pneumothorax etc.. Use non-invasive ventilation whenever possible Use the lowest doses and shortest duration of medications such as
steroids, opiods, benzodiazepine, and neuromuscular blockers.

SEDATION IN THE ICU26

Indication for Sedation in the ICU Many causes for anxiety:
Continuous audible alarms Poor lighting Interactions with medical and nursing staff Pain Immobility Interruptions in the normal sleep cycle.
Approximately 52% to 71% of all patients in the ICU may develop at least one episode of agitation.
Agitation can arise from anxiety, delirium, medications, pain, metabolic defects, hypoxia, and drug or alcohol withdrawal.
27

28
What We Know About ICU Agitation/Discomfort
Immediate sequelae of agitation: • Patient-ventilator dyssynchrony• Increased oxygen consumption • Self (and health care provider) injury• Family anxiety
Long-term sequelae: chronic anxiety disorders and post-traumatic stress disorder (PTSD)

29
Recall in the ICU
Some degree of recall occurs in up to 70% of ICU patients.• Anxiety, fear, pain, panic, agony, or nightmares reported in 90% of those who did have recall.
Potentially cruel:• Up to 36% recalled some aspect of paralysis.
Associated with PTSD in ARDS? • 41% risk of recall of two or more traumatic experiences.
Associated with PTSD in cardiac surgery

30
Appropriate Recall May be Important
Factual memories (even unpleasant ones) help to put ICU experience into perspective
Delusional memories risk panic attacks and PTSD
The optimal level of sedation for most patients is that which offers comfort while allowing for interaction with the environment.

31
Goals of Sedation in ICU Patient comfort and Control of pain Anxiolysis and amnesia Blunting adverse autonomic and hemodynamic responses Facilitate nursing management Facilitate mechanical ventilation Avoid self-extubation Reduce oxygen consumption The optimal level of sedation for most patients is that which offers comfort while
allowing for interaction with the environment.

32
Characteristics of an ideal sedation agents for the ICU
Lack of respiratory depression Analgesia, especially for surgical patients Rapid onset, titratable, with a short elimination
half-time Sedation with ease of orientation and arousability Anxiolytic Hemodynamic stability

33
The Challenges of ICU Sedation
Assessment of sedation Altered pharmacology Tolerance Delayed emergence Withdrawal Drug interaction

34
Correctable Causes of Agitation Full bladder Uncomfortable bed position Inadequate ventilator flow rates Mental illness Uremia Drug side effects Disorientation Sleep deprivation Noise Inability to communicate

35
Causes of Agitation Not to be Overlooked
Hypoxia Hypercarbia Hypoglycemia Endotracheal tube malposition Pneumothorax Myocardial ischemia Abdominal pain Drug and alcohol withdrawal

36
Daily Goal is Arousable, Comfortable Sedation
Sedation needs to be protocolized and titrated to goal: Lighten sedation to appropriate wakefulness daily. Effect of this strategy on outcomes:
One- to seven-day reduction in length of sedation and mechanical ventilation needs
50% reduction in tracheostomies Three-fold reduction in the need for diagnostic evaluation of
CNS

37
Assessment of Sedation
Many scales are used to assess the level of sedation and agitation of patients in ICU: Ramsay scale Riker Sedation-Agitation Scale Motor activity assessment scale Glasgow Coma Scale Richmond Agitation-Sedation Scale (RASS)

38
FYI

39
FYI

40
Riker Sedation-Agitation Scale FYI

41
FYI

42
Required

43
What Sedation Scales Do
Provide a semi-quantitative “score” Standardize treatment endpoints Allow review of efficacy of sedation Facilitate sedation studies Help to avoid over-sedation
44
What Sedation Scales Don’t Do
Assess anxiety Assess pain Assess sedation in paralyzed patients Predict outcome Agree with each other

45
Sedating/Analgesia Options
Rule out reversible causes of discomfort/anxiety such as hypoxemia, hypercarbia, and toxic/drug side effect.
Assess comorbidities and potential side effects of drugs chosen.
Target irreversible etiologies of pain and agitation.

46
Strategies for Patient Comfort
Set treatment goal Quantitate sedation and pain Choose the right medication Use combined infusion Reevaluate need Treat withdrawal

Sedative Agents
Benzodiazepines Propofol Dexmedetomidine
47

Benzodiazepines
benzodiazepines bind γ-aminobutyric acid receptors results in the opening of a chloride channel, causing hyperpolarization and stabilization of the neuronal membrane
48
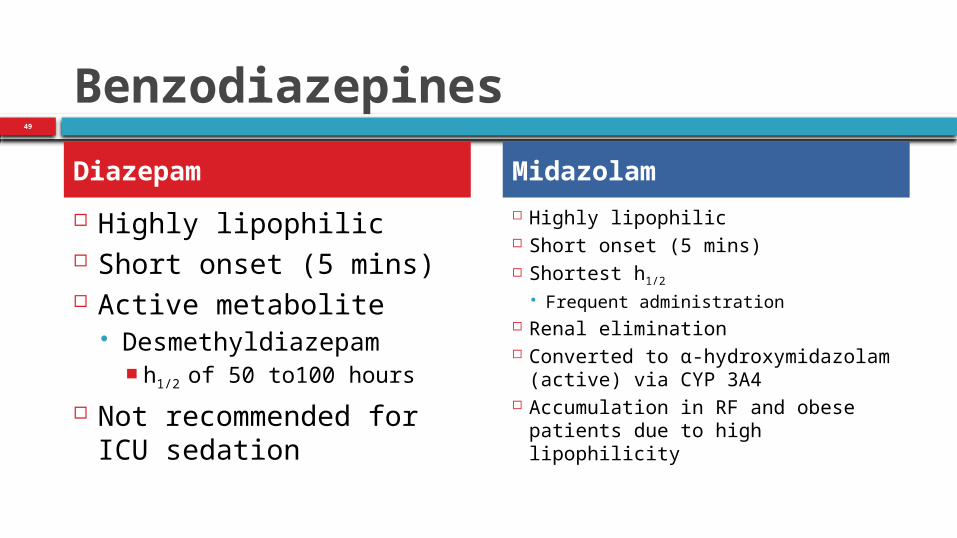
Benzodiazepines
Highly lipophilic Short onset (5 mins) Active metabolite
Desmethyldiazepam h1/2 of 50 to100 hours
Not recommended for ICU sedation
Highly lipophilic Short onset (5 mins) Shortest h1/2
Frequent administration Renal elimination Converted to α-hydroxymidazolam
(active) via CYP 3A4 Accumulation in RF and obese patients
due to high lipophilicity
Diazepam Midazolam
49

Benzodiazepines
Lorazepam is less lipophilic than the other benzodiazepines slower onset of action (5-20 minutes). Intermediate duration of action (6-8 hours)
Less frequent adminstration than midazolam. Lorazepam is eliminated by glucuronidation
no significant enzymatic drug interactions and it has no active metabolites.
50

51

PropofolPharmacology: GABA agonist
Pharmacokinetics/dynamics: onset 1 - 2 minutes, terminal half-life 6 hours, duration 10 minutes, hepatic metabolism
Benefits• Rapid onset and offset and easily titrated
• Hypnotic and antiemetic
• Can be used for intractable seizures and elevated intracranial pressure
Risks• Not reliably amnestic, especially at low doses
• NO analgesia!
• Hypotension
• Hypertriglyceridemia; lipid source (1.1 kcal/ml)
• Respiratory depression
• Propofol Infusion Syndrome
- Cardiac failure, rhabdomyolysis, severe metabolic acidosis, and renal failure
- Caution should be exercised at doses > 80 mcg/kg/min for more than 48 hours
- Particularly problematic when used simultaneously in patient receiving catecholamines and/or steroids
52

53
Propofol Dosing
3-5 g/kg/min antiemetic 5-20 g/kg/min anxiolytic 20-50 g/kg/min sedative hypnotic >100 g/kg/min anesthetic

54

55
DexmedetomidineAlpha-2-adrenergic agonist like clonidine but with much less imidazole activity
Has been shown to decrease the need for other sedation in postoperative ICU patients
Potentially useful while decreasing other sedatives to prevent withdrawal
Benefits• Does not cause respiratory depression
• Short-acting
• Produces sympatholysis which may be advantageous in certain patients such as postop cardiac surgery
Risks• No amnesia
• Small number of patients reported distress upon recollection of ICU period despite good sedation scores due to excessive awareness
• Bradycardia and hypotension can be excessive, necessitating drug cessation and other intervention

56

57

58
Dexmedetomidine (α-2 agonist)
Advantages: No respiratory depression Has sedative, anxiolytic and some analgesic properties Light sedation allows for it to be used as a bridge agent
Disadvantages: Can cause hypotension (especially with bolus dose) Expensive

59

60
Things to remember Overdose (prolonged infusion)
pK derived from healthy patients Drug interaction Individual variation
Delayed elimination Liver (Cp450) Kidney dysfunction Active metabolites
Quick onset and short t1/2 are desired characteristics for sedatives and analgesics (making midazolam and fentanyl a good choice)

Neuromuscular blocking agents (NMBA)61

62
Neuromuscular blocking agents (NMBA)
MOA: mimic acetylcholine as they bind with cholinergic receptors and block neuromuscular transmission at the neuromuscular junction causing paralysis.
63
Classification
Non-depolarizing blocking agents (majority) Rocuronium Vecuronium Pancuronium
Depolarizing blocking agents Succinyl-Choline

64
Clinical Use NMB are used adjunctively to anesthesia to produce paralysis,
firstly to paralyse the vocal cords, and permit intubation of the trachea, and secondly to optimize the surgical field by inhibiting spontaneous ventilation, and causing relaxation of skeletal muscles.
Because the appropriate dose of neuromuscular-blocking drug may paralyze muscles required for breathing (i.e., the diaphragm), mechanical ventilation should be available to maintain adequate respiration

65
Adverse effects
cause paralysis of the diaphragm facilitate histamine release, which causes hypotension,
flushing, and tachycardia Reversal
reversed with anticholinesterase inhibitors, neostigmine, and edrophonium.
Sugammadex is a newer drug for reversing neuromuscular block by rocuronium in general anesthesia.
66

Questions
67