maternal & newborn health resource center
TRANSCRIPT

Maternal & Newborn Health Resource Center01
Process Document
An implementation model towards improved clinical practices and patient safety through standardization of clinical protocols
Maternal & Newborn Health Resource Center

Enhancing Efficiency of Pneumonia Management02

ContentsAcronyms .................................................................................................................04
executive summAry ................................................................................................05
mnH QuAlity of cAre ...............................................................................................06
role of meDicAl colleges in rmncH QuAlity imProvement .............................06
Vriddhi imPlementAtion moDel .............................................................................07
objectives of tHe imPlementAtion moDel .........................................................09
trAnsition to online mentoring During coviD-19 PAnDemic ............................ 15
outcome: results AnD AnAlysis in lAbor room PrActices ............................. 17
outcome: results AnD AnAlysis in sncu PrActices ......................................... 19
cHAllenges fAceD by mnH resources centre ..................................................22
WAy forWArD AnD sustAinAbility ........................................................................23
Annexures ...............................................................................................................24Annexure 1: letter from rims to secretary, Health for institutionalization
of jharkhand state maternal and newborn Health resource center ........ 24
Annexure 2A: standard checklist for maternal Health mentoring visits ...................... 25
Annexure 2b: standard checklist for newborn Health mentoring visits ...................... 34
Maternal & Newborn Health Resource Center04
AD Aspirational DistrictADMO AssistantDivisionalMedicalOfficerCDMO ChiefDistrictMedicalOfficerDH District Hospitals DHS Directorate of Health servicesFBNC facility based newborn careFPC family Participatory careFRU first referral unitGoI government of indiaHoD Head of DepartmentIP infection PreventionLR labor roomMCH maternal and child HealthMNCH maternal newborn child HealthMNHRC maternal and newborn Health resource centerMO I/C MedicalOfficerIn-chargeNBCC newborn care cornerNFHS national family Health surveyNHM national Health missionNSSK navjaat shishu suraksha KaryakramOT operation theatrePIP Program implementation PlanPMSMA Pradhan mantri surakshit matritva AbhiyanPPH Postpartum HemorrhagePSM Preventive and social medicineQI Quality improvementQoC Quality of careRCH reproductive child HealthRIMS rajendra institute of medical scienceRMNCHA reproductive, maternal, newborn, child and Adolescent HealthRoP record of ProceedingsSDG sustainable Development goalsSNCU special newborn care unitsSOP standard operating ProceduresSUMAN surakshit matritva AashwasanUSAID united states Agency for international DevelopmentWHO World Health organization
Acronyms

Maternal & Newborn Health Resource Center05
Every health system strives to provide effi-cient and effective healthcare services, in line with latest clinical care standards and practic-es. Apart from the infrastructure, the level of services depends on the competence of pro-viders with respect to the latest procedures and technologies to improve patient care and patient safety. A healthcare professional competency for standardized clinical proto-cols builds through pre-service education, in-service trainings, and work experience. However, evidences show sub-optimal qual-ity of most of these learnings. Additionally, unprecedented challenges like the COVID-19 pandemic test the ability of health system to provide efficient and effective care without being overwhelmed.
To bring standardization as per standards of clinical care and adoption of evidence sup-ported SOPs in a structured way, the Mater-nal and Newborn Health Resource Center (MNHRC) was started in the state of Jharkhand by USAID Vriddhi project. The MNHRC im-plementation pilot model involved linking a mentor facility (A medical college, here RIMS, Ranchi) with mentee facilities (Selected Dis-trict Hospitals & high case load FRUs) using a hub and spoke model.
Executive SummaryThe program is unique as it combines two Na-tional programs, ‘LaQshya focusing on Labor Room strengthening practices’ and ‘Facility Based Newborn Care’, prioritizing clinical case management beyond infrastructure and logis-tics, and aims every woman to receive routine, evidence-based care as a norm.
The program has focused QI supportive su-pervision and hand holding tools for maternal and newborn care. There are total 13 stand-ards comprising of 76 variables. The case im-provement is assessed on a score card. The results are promising as the improvement in case management practices during 2nd Stage of labor improved by 52%, during 3rd Stage of labor by 30% and in immediate postpartum period by 3.5%.
The resource centre is a viable and feasible model buttressing the suboptimal quality of pre-service education and in-service train-ings of many public health service providers with the latest knowledge and standards.
Maternal & Newborn Health Resource Center06
India is constantly working to enhance facili-ty-based care for pregnant women and new-borns to promote quality and respectful care under LaQshya and Facility based newborn care (FBNC). Concurrently, there has been several initiatives in terms of strengthening of health infrastructure and service quali-ty improvement initiatives under Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA) and Surakshit Matritva Aashwasan (SUMAN). In addition, various, mechanisms and innova-tions have been put in place to improve sup-ply chain. Despite these various efforts, the improvement in case management practices has been slow and poor. This low compliance towards clinical guidelines and protocols poses a continuous challenge in early identi-
MNH Quality of Care fication of those cases which require special and urgent attention and subsequently, pro-vision of appropriate care to such mothers and newborns.
The Reproductive, Maternal, Newborn, Child and Adolescent Health (RMNCHA)-India strat-egy identifies various ways to enhance quality of healthcare services to make it equitable, acceptable, effective, and safe for every wom-an and newborn. One such RMNCHA strategy suggests to utilize expertise available within medical colleges by setting up of technical support units in terms of ‘Regional Resource Centers’ to extend required technical support and mentor their respective state Reproduc-tive Child Health (RCH) programs1.
The emphasis to use Medical College for qual-ity improvement is because they are the hub of knowledge and clinical excellence and are usually well versed in latest clinical protocols, implementation practices and challenges. Hence, using peer mentoring approach where Medical College mentor other public health facilities like District Hospitals (DH) and First Referral Unit (FRU) seemed a feasible idea.
After a broader strategy decision on how to improve clinical case management using Med-ical Colleges, the next set of questions were:
i) Are there any existing learning resource center model/s in the country which can be used as reference/s?
Role of Medical Colleges in RMNCH Quality Improvement
The Government of India (GoI) had issued a guidance note on establishing Newborn Health Resource Centers in leading Medical Colleges of the states in the year 2018. The success of these Newborn Resource Centers in the states of Odisha, Madhya Pradesh and others can surely be considered as a learning experience.
ii) The ‘Newborn Health Resource Center’ model had a much narrower focus – would it be feasible to include clinical case-management of pregnancy, childbirth and related maternal cases to newborn survival and safety? This was indeed a challenge, but the National Family Health Survey (NFHS) data and other ev-idences pointed towards need for an Integrated model of Maternal and Newborn care - not only
1 Chapter 13: Technical Support for RMNCHA service delivery, RMNCHA strategy, MoHFW
Maternal & Newborn Health Resource Center07
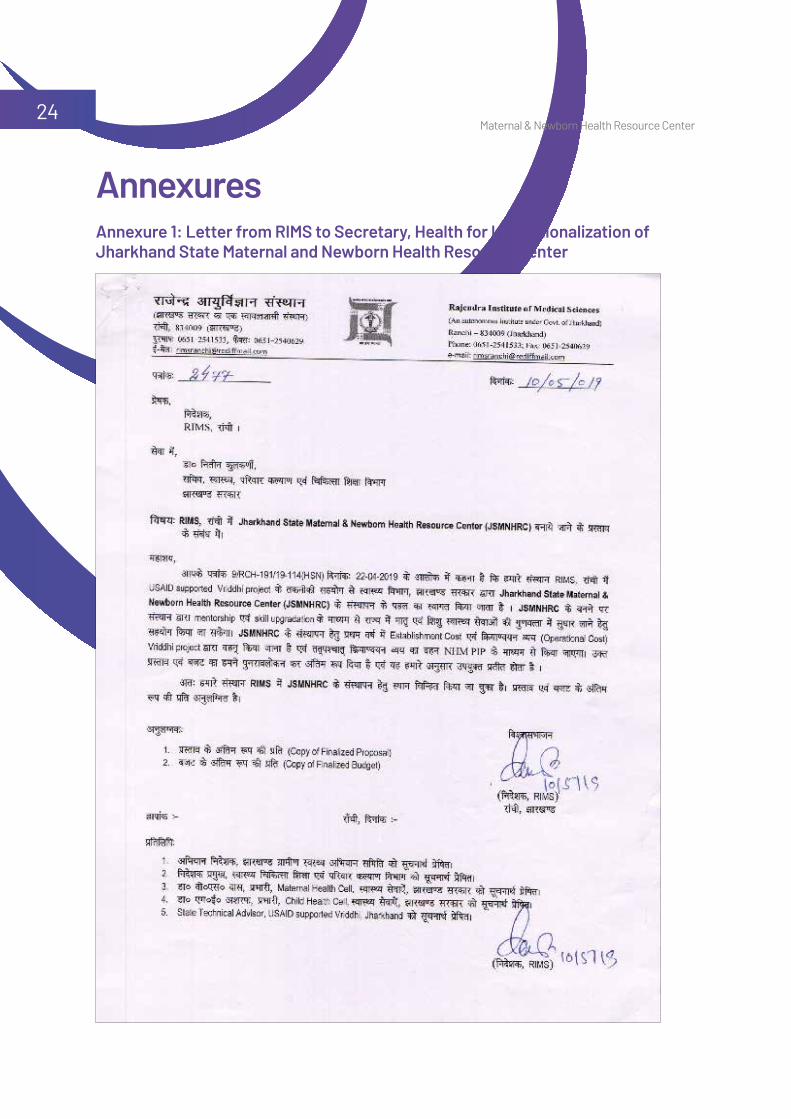
for newborns. Hence, it was decided to name this project as ‘Maternal and Newborn Health Resource Center’ (MNHRC) and advocacy to State Government was initiated on institution-alizing integrated model of resource center (A letter in this regard from RIMS to Secretary, Health – NHM Jharkhand for institutionalizing MNHRC has been appended as an Annexure 1).
iii) Which criteria should be used to select the Medical College which shall act as the Resource Hub for clinical mentorship in the state? It was decided that the main selection criteri-on shall be their willingness to host the insti-tutional structure of repute and agree to men-tor the facilities.
iv) Medical Colleges are themselves stressed - running low on resources and overloaded with patient services. How then will they find time and resources for travel, co-ordination with mentee facilities, document their findings, and provide appropriate clinical mentorship?
This is where USAID Vriddhi project came in as a support and interface mechanism which helped make this resource center model a re-ality. The role of medical colleges as clinical mentors in public healthcare is of great val-ue – and Project Vriddhi, in concurrence with the state government and medical college au-thorities, was determined to enable this and address any issues that may arise.
The USAID supported Vriddhi Project active-ly worked with the National Health Mission (NHM), Jharkhand and the ‘Rajendra Institute of Medical Science’ (RIMS), Ranchi to establish the first state ‘Maternal and Newborn Health Resource Centre’ (MNHRC) which would serve as a mentoring center of clinical excellence for the state of Jharkhand.
The state MNHRC, a Quality Improvement (QI) initiative was envisaged as a step to improve focus on standardized clinical care by adop-tion and adherence to Standard Operating Procedures (SOP) and Protocols.
The standards of care from current global guidance and those adapted by the Govern-ment of India were used as part of this quality improvement initiative.
The implementation model primarily address-es the root-cause of the problem – the case
Vriddhi Implementation Modelmanagement practices. The technical capacity of every care provider is different and demands customized and need based mentoring. Thus, a human centered design focusing on individ-ual needs was selected to appropriately utilize available expertise with Medical College RIMS.
The state of Jharkhand was selected to host this unique initiative as part of USAID support-ed state and because the state has maximum number of Aspirational Districts (AD).
RIMS was selected because of its strength as an institute of clinical repute, willingness to host the MNHRC and NHM approval. In addi-tion, the positive attitude and willingness of the departments of Obstetrics & Gynecology, Pediatrics and Preventive and Social Medi-cine (PSM) at RIMS helped to finalize RIMS to host of the state MNH Resource Centre. The previous experience of the RIMS faculty (Who were involved in the Facility Based Newborn

Maternal & Newborn Health Resource Center08
Care Programs and the LaQshya – Labor Room Strengthening Program, Government of India) could also be leveraged in this new initiative. Last but not the least, this was the only Medi-cal College in the state implementing and sup-porting state RCH programs.
The methodology required Mentor Facilities (I.E. the Medical College) to provide guidance, handholding, and troubleshooting to mentee facilities (I.E. selected District Hospitals & high case load FRUs) in a structured way. It utilized the ‘hub-and-spoke’ model to promote stand-ardized mentoring using standardized formats.
The Standards of Care define the ‘Do’s and Don’ts’ of clinical care practice and how this would ensure a satisfying positive experience – for both the care provider and care seeker. The key aspect of this initiative was to shift the focus and encourage ‘evidence supported’ practices and discourage ‘harmful practices’ for the mother and newborn.
To support this Checklist of Do’s and Don’ts, a reference manual was prepared which provid-ed justification of each variable under stand-ards of care.
For mentoring visits, use of standard based tools, and different methods of data collection e.g. Direct Observation, Provider Interview, Re-cord Review, and simulation were considered. The preferred method remained direct observa-tion of how a particular case is managed. How-ever, considering the unpredictable occurrence of complications during childbirth, other men-toring methods were also considered.
The newly developed maternal and newborn health tools (Refer to Annexure 2) prepared especially for this initiative captures the cur-
rent clinical practices of mentee facility and guides the mentee facility to move towards robust and resilient health system by adopt-ing latest ‘evidence-based’ practices. The new tools have 13 standards comprising of 76 variables for maternal and newborn care and these case practices are assessed on a score card (Refer to Annexure 2: Maternal and New-born health tools with score card).
To keep the focus on clinical case management practices only, the collection of data on infra-structure, human resource and logistics re-quirements was purposely excluded from this intervention. However, this did not preclude the mentors from emphasizing availability of critical drugs, promoting use of appropriate uterotonics during Postpartum Hemorrhage (PPH) or stressing upon judicious use of antibi-otics for sick newborn management.
Maternal and Newborn Health Resource Center in Ranchi, Jharkhand
Maternal & Newborn Health Resource Center09
The overall vision of the state MNH Resource Center is to be clinical mentors to the state RCH programs and facilitate the state health departments to improve quality of Maternal Newborn Child Health (MNCH) care and help achieve Sustainable Development Goals (SDG).
Specific Objectives • Sustain Government of India MNH Quality Im-
provement programmes such as◆ LaQshya- for improved clinical care practic-
es during labor, initial management of Post-partum Hemorrhage & Eclampsia and other clinical protocols of GoI under the LaQshya framework.
◆ Facility Based Newborn Care through ca-pacity building and mentoring of ongoing and other newer trainings and concepts like Family Participatory Care (FPC).
• Analyse data and provide actionable feed-back to Special Newborn Care Units (SNCUs) and District Hospitals on performance to strengthen Quality of Care (QoC).
• Provide clinical guidance– for ongoing and newer interventions under the maternal and newborn space.◆ Analyze data and provide actionable feed-
back to SNCUs and DHs on performance to strengthen Quality of Care
• Provide clinical & technical guidance to state for improved maternal and new-born outcomes
Steps in operationalizing State Ma-ternal and Newborn Health Resource Center to Improve Quality of Care
The state Maternal and Newborn Health Re-source Center is a physical entity, situated in the mentor facility (I.E. RIMS, Ranchi), acting as an interface between the mentor (RIMS) and mentee facilities (I.E. DH and FRUs). The MNHRC liaises with the three concerned de-partments of RIMS and facilitates the phys-ical visit of technical experts. Physical visit to each mentee facility happens 1-2 times in a period of 3 months - after which data is re-corded, compiled, and analyzed. The report is shared with concerned stakeholders for ap-propriate action.
The MNHRC provides precision clinical super-vision to the mentee facilities in terms of gaps identified during each visit. At the same time, it liaises with the mentor facility for next visit for continuous mentoring.
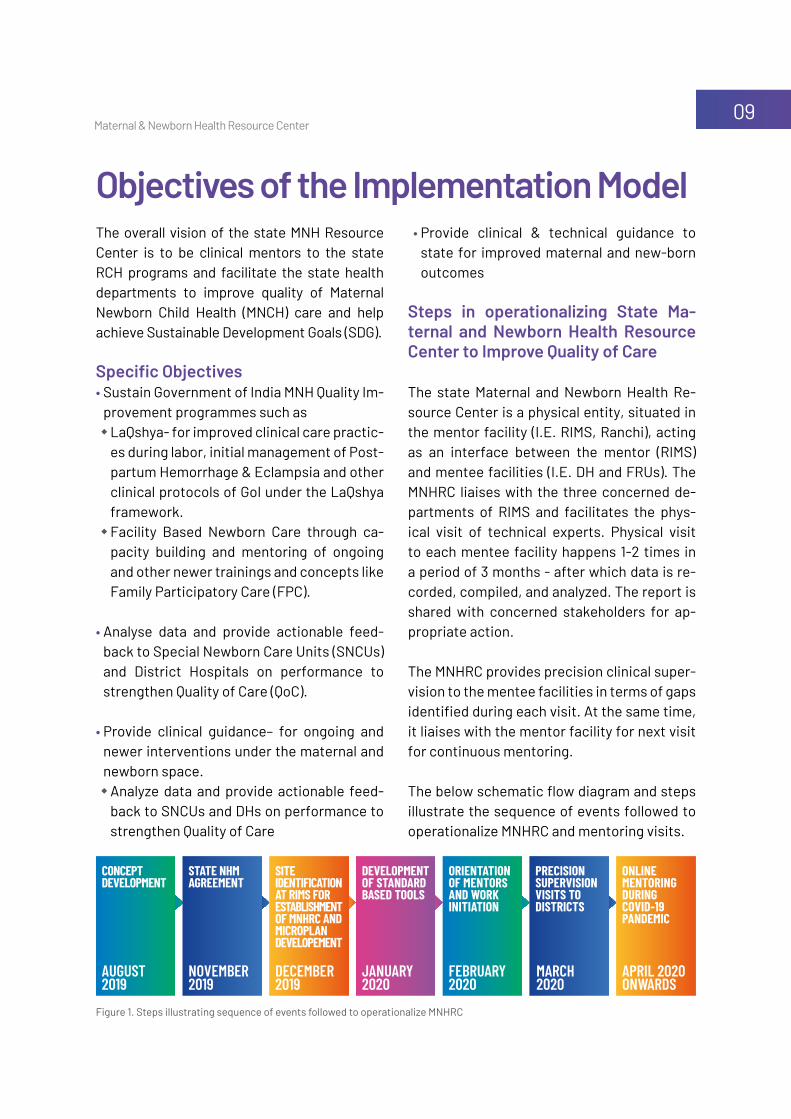
The below schematic flow diagram and steps illustrate the sequence of events followed to operationalize MNHRC and mentoring visits.
Objectives of the Implementation Model
Figure 1. Steps illustrating sequence of events followed to operationalize MNHRC
ConCept Development
orientation of mentors anD work initiation
state nHm agreement
preCision supervision visits to DistriCts
site iDentifiCation at rims for establisHment of mnHrC anD miCroplan Developement
online mentoring During CoviD-19 panDemiC
Development of stanDarD baseD tools
December 2019
november 2019
august 2019
january 2020
february 2020
march 2020
april 2020onwards

Maternal & Newborn Health Resource Center10
Step 1: Concept DevelopmentPreliminary information gathering revealed that the state was already going ahead to es-tablish a Resource Center for newborn health as per GoI guidelines. The Vriddhi Project team shared their vision with state NHM technical division and proposed an integrated approach of developing a combined Maternal and New-born Resource Center. Towards this, a draft concept note was developed.
Step 2: State NHM AgreementThis draft concept was discussed with the Secretary Health, Jharkhand Health Services and with the Maternal and Child Health (MCH) Program officers at the Program level. The State health administration finalized the con-cept and suggested to develop a detailed work plan. The concept was then finalized with the key authorities at RIMS which was identified as the partner to host the MNH Resource Center establishment.
The project proposal was developed jointly by Vriddhi Project team and RIMS – then worked towards seeking concurrence of all concerned parties for setting up the resource center. The proposal was approved by the State Adminis-tration and sent to the state NHM for ratifica-tion. The NHM on further review with the ma-ternal and child health cells sought approval from the Mission Director, NHM. The other important processes that were taking shape meantime were as follows:
Site Selection for the Resource CenterAccording to the final proposal, the Medical College would provide space to set up the Resource Center. The main criteria for site selection was to posit it near the involved de-partments of ‘Obstetrics & Gynecology’ and ‘Pediatrics’. The selected site was earmarked
by the Head of Department (HoD) - Obstetrics and Gynecology, RIMS and handed over to the newly selected MNHRC Project staff.
Finalizing the Finances and Administration of state MNH Resource CenterFor operational management (Including fi-nances and administration) of the MNHRC, the Superintendent of RIMS was made In-charge and would oversee all operational and finan-cial matters. To support him, any one of the 3 involved Head of Departments could hold an additional charge of the Resource Center. The MNHRC would submit a monthly activity report to the NHM and Superintendent In-charge and HoDs of RIMS.
Hiring of Staff for the Resource CenterThe RIMS (Medical College) recruited, with financial support from USAID Vriddhi pro-ject, the following staff for the Resource Center:• One MNHRC program coordinator – A Pro-
gram management person with data analysis and documentation capacities
• One clinical nurse mentor
After the termination of financial support of the USAID Vriddhi project, these 2 posts would be continued through NHM support.
Funding of establishment and running of the resource centerThe financial requirements of initial setting up of MNHRC physical space and line items re-quired to demonstrate clinical practices was done using Project Vriddhi funds. The required items like Mannequins, Air conditioner, furni-ture consisting of tables, chairs, almirah, desk top computer, printer, photocopier, etc. were installed in the resource center prior to the in-auguration.

Maternal & Newborn Health Resource Center11
Vriddhi Project proposal provided for funding support of the Resource Center for the first year after which NHM funds would be used for its continuity. The recurring costs would be re-viewed by the state NHM and suitable amount proposed in the upcoming NHM Program Im-plementation Plan (PIP) 2020-21 and beyond.
Identification of Mentee FacilitiesThe mentee district hospitals were selected by mutual discussion with the Head of Depart-ments aided by dashboards like the SNCU Quali-ty of Care Index (SQCI) and District Hospital Qual-ity of Care Index (DQCI), with a minimum of 1 visit per quarter to one facility. These four district hospitals were chosen for mentoring of health staffs of Labor Room (LR), maternity Operation Theater (OT), and SNCU to promote standardiza-tion of case management practices.
Four Aspirational District hospitals namely Latehar, Giridih, Palamu and Ranchi with high delivery case load were selected to receive guidance and technical support from experi-enced and senior professionals of RIMS on pe-riodic basis. A mechanism for regular support to the secondary/district/FRU level facilities by the MNH Resource Center was established.
Step 3: Development of Standard based Tools and Scoring Criterion Two separate mentoring checklists (Refer to Annexure 2) were prepared by the Vriddhi National team for Labor Room, Maternity OT and SNCU. The checklists supported with a manual provided explanation and references of all standards of clinical care enlisted in the checklist.
standards were developed for the following: • Case management practices during 2nd
stage of labor
• Case management practices during 3rd stage of labor
• Case management practices of mother & newborn during immediate post-partum period
• Case management practices during PPH• Case Management Practices during Hyper-
tensive Disorder during childbirth• Case Management Practices of Sick new-
born at SNCU• Case Management Practices or Care at New-
born Care Corner (NBCC)
scoring criterion of selected standards: Next, each standard and sub-standard was to be scored on a 1-5 scale as follows: 5 - Being good practice complying with stand-
ards of care4 - Little need for improvement to reach stand-
ard of care3 - Some need for improvement to reach stand-
ards of care2 - Considerable need for improvement to reach
standards of care 1 - Services not provided, totally inadequate care
For each clinical skill, the mentor assigned marks based on observation. After each sec-tion, average marks are calculated (Shown in Annexure 2). This helped in locating current deficiencies as per World Health Organiza-tion (WHO) standards of clinical case man-agement and provided customized guidance to each level. Based on this ‘baseline’, sub-sequent visits could help track the improve-ment from previous visit. The scoring could hence show the trend of improvement in standards of care.
The checklists were piloted by the faculty of the RIMS in their respective departments be-fore finalization.

Maternal & Newborn Health Resource Center12
Step 4: Orientation of Mentors and work initiationThe steps in identifying, orienting and sup-porting the mentors were as follows:• List of willing, nominated mentors from De-
partment of Obstetrics & Gynecology, De-partment of Pediatrics and Department of PSM were sought from respective HoDs. This list of nominated mentors were approved by NHM for mentoring purposes of District Hos-pitals and FRU facilities.
• Inauguration of the Resource Center: MNHRC was inaugurated by Mission Director (MD), NHM in the presence of Director RIMS, Super-intendent RIMS, Mission Director, USAID/In-dia, Health Office Director, and Project Direc-tor, USAID Vriddhi/IPE Global Ltd on the 2nd of March 2020. The inauguration was imme-diately followed by orientation of identified mentors by the faculties of the departments of Neonatology, Obstetrics & Gynecology and Preventive and Social Medicine of RIMS.
• Orientation of Mentors on newly developed standards based mentoring formats (Concur-rent Step): The clinical experts/ faculty from the departments of Obstetrics and Gynecolo-gy, the Neonatology, and the Preventive and Social Medicine RIMS were trained on the cog-nitive aids i.e. standards based tools and man-ual to guide users through SOPs for accurate task completion. These tools are inspired by the two National programs, ‘LaQshya focusing on labor room strengthening practices’ and ‘Facility Based Newborn Care’. With the be-lief that adult education is about stimulation of curiosity and provision of right knowledge, and the human centered approach of provid-ing customized mentoring, the faculty initiat-ed the field visits to mentee facilities.
• Travel Itinerary and support to mentors: The frequency of mentoring visits is decid-ed by the resource center. However, at least
one visit per quarter to each mentee facil-ity is mandatorily planned. The travel plan is coordinated by the staff at the MNHRC in consultation with NHM and concerned HoDs of RIMS. Additionally, mentoring vis-its were well aligned and coordinated with state Maternal Health Cell, Child Health Cell, the state health department, and district health officials. The mentors were informed beforehand about the mentoring plan and based on their availability; the mentoring visits were scheduled.
Guidelines for travel and reimbursement were developed. A facility pre-visit information sheet was shared with mentee facilities so that basic information is collected before-hand. This ensured that maximum on-site time of mentors is utilized for problem solv-ing. The next mentoring visits are also sched-uled at the end of the visit in the facility.
After the visit, the data is analyzed, and re-ports are shared with concerned authorities including the respective civil surgeons of the districts. So far, MNHRC has consistently shared the reports and minutes with the state health officials of NHM and the district health officials which has helped them to understand the progress on action points made during the mentoring visits/online mentoring. After the visit, the mentors submitted their trav-el claims as per the NHM norms with the Re-source Center, along with reports.
Step 5: Precision supervision visits to Districts: Physical and online visits Four aspirational districts were chosen – Pal-amu, Latehar, Giridih and Ranchi. Official gov-ernment letters were sent to the respective facilities prior to the mentoring visit for coor-dination and support.
Maternal & Newborn Health Resource Center13
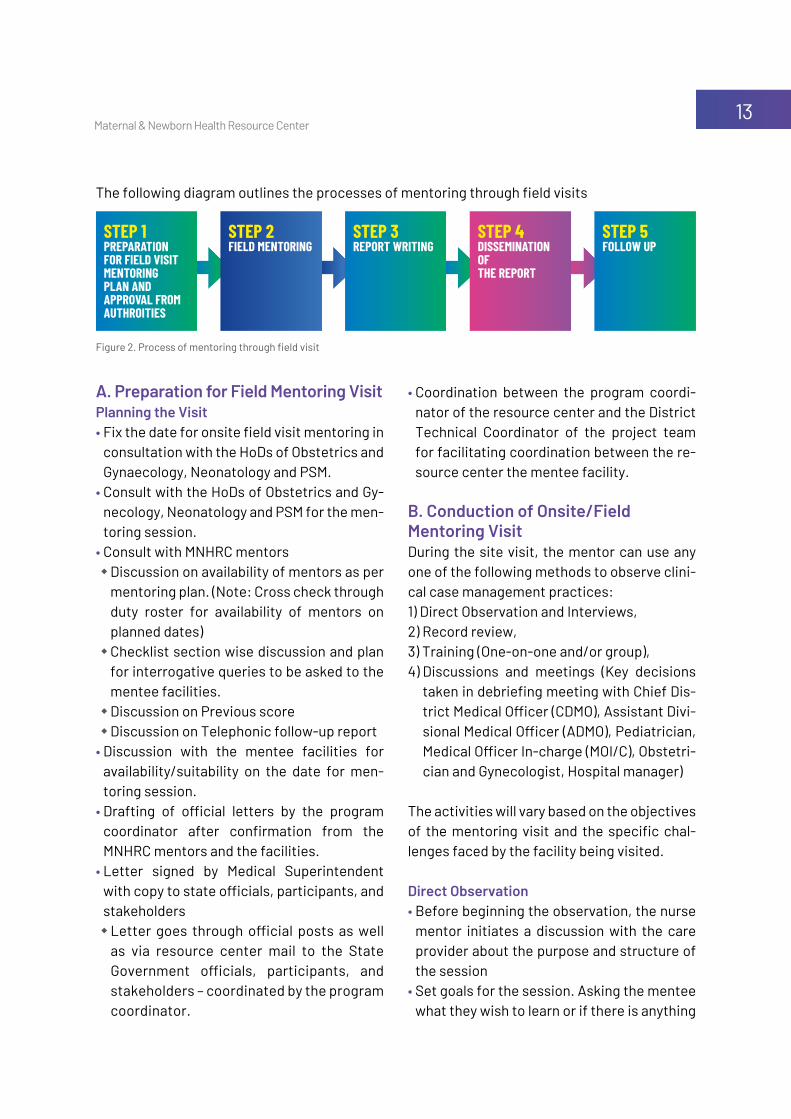
The following diagram outlines the processes of mentoring through field visits
A. Preparation for Field Mentoring VisitPlanning the Visit• Fix the date for onsite field visit mentoring in
consultation with the HoDs of Obstetrics and Gynaecology, Neonatology and PSM.
• Consult with the HoDs of Obstetrics and Gy-necology, Neonatology and PSM for the men-toring session.
• Consult with MNHRC mentors ◆ Discussion on availability of mentors as per
mentoring plan. (Note: Cross check through duty roster for availability of mentors on planned dates)
◆ Checklist section wise discussion and plan for interrogative queries to be asked to the mentee facilities.
◆ Discussion on Previous score◆ Discussion on Telephonic follow-up report
• Discussion with the mentee facilities for availability/suitability on the date for men-toring session.
• Drafting of official letters by the program coordinator after confirmation from the MNHRC mentors and the facilities.
• Letter signed by Medical Superintendent with copy to state officials, participants, and stakeholders◆ Letter goes through official posts as well
as via resource center mail to the State Government officials, participants, and stakeholders – coordinated by the program coordinator.
Figure 2. Process of mentoring through field visit
step 1 preparation for fielD visit mentoring plan anD approval from autHroities
step 5 follow up
step 2fielD mentoring
step 3report writing
step 4Dissemination of tHe report
• Coordination between the program coordi-nator of the resource center and the District Technical Coordinator of the project team for facilitating coordination between the re-source center the mentee facility.
B. Conduction of Onsite/Field Mentoring VisitDuring the site visit, the mentor can use any one of the following methods to observe clini-cal case management practices:1) Direct Observation and Interviews, 2) Record review, 3) Training (One-on-one and/or group), 4) Discussions and meetings (Key decisions
taken in debriefing meeting with Chief Dis-trict Medical Officer (CDMO), Assistant Divi-sional Medical Officer (ADMO), Pediatrician, Medical Officer In-charge (MOI/C), Obstetri-cian and Gynecologist, Hospital manager)
The activities will vary based on the objectives of the mentoring visit and the specific chal-lenges faced by the facility being visited.
Direct Observation• Before beginning the observation, the nurse
mentor initiates a discussion with the care provider about the purpose and structure of the session
• Set goals for the session. Asking the mentee what they wish to learn or if there is anything

Maternal & Newborn Health Resource Center14
they are concerned about or want to practice• Observe facility layout, patient flow, systems
and procedures, information sharing, and counseling. Try to get a sense of the big picture about how the health care facility operates
• Using mentoring checklists to guide, obser-vation and document information for fol-low-up and for sharing in meetings and re-ports. Check for compliance with guidelines and protocols. If guidelines are not being fol-lowed, MNHRC mentors provide training and instruction on to use the guidelines
Record Review• Review registers, patient records, and sum-
mary forms. Check to see if they are up to date, whether data are being entered cor-rectly, whether appropriate care is being provided (To the extent possible given the in-formation collected on the records), and how the documents are being stored.
TrainingDepending on what issues arise during the site visit, mentors conduct training sessions for life saving critical skills for health care provid-ers. This might take the form of a case discus-sion, grand rounds or a discussion session on a specified topic. Skills demonstrated or taught during the visit are documented in the mentor-ing checklist used by the MNHRC mentors.
Discussions and MeetingsGive feedback to the health care facility staff at the completion of onsite mentoring visit:• Describe gaps in knowledge among health
care workers that mentor observed.• Note problems in record-keeping or other
systems that mentor observed.• Suggest ways to improve clinic organization.• Note major barriers to effective delivery of
services.
• Answer any questions that may arise during discussion.
Develop a plan including action items and per-sons responsible to address issues of concern identified. This plan should be revisited during subsequent visits to track progress.
C. Sharing Observations with State and Mentee FacilitiesThe field observations made by the mentors are recorded in the checklists by the nurse mentor of the resource center at the facility. Based on the observations and the checklist, a summary report of the field findings is prepared by the resource center and shared with the HoDs and mentors for review and upon finalization, is shared with the Medical Superintendent.
The final report is countersigned by the Pro-gram Coordinator of resource center, the mentor and the Medical Superintendent and shared with mentee facilities, state govern-ment officials and all the stakeholders and participants (Via post as well as through re-source center email).
The Results and Improvements section is di-vided into two: a) improvement in Labor Room practices and b) Improvement in neonatal care.
D. Adapting to COVID-19 Restrictions First onsite visit was at Palamu. Mentors from RIMS along with Vriddhi team visited Palamu Medical College Hospital on 7th March 2020 with checklists for SNCU, LR and Maternity OT. There was a meeting with the officials of Palamu hospital regarding the objective and methodology of mentoring. The SNCU and LR visit was followed by a joint discussion with the clinical staff. The mentees readily accept-ed the structured mentoring methodology.

Maternal & Newborn Health Resource Center15
The initial field visits results were promising and inspiring.
The project activities took a learning pause during the initial phase of COVID-19 pandemic but the belief in ‘Never waste a good crisis’ led the Project Vriddhi team to explore and move ahead with digital solutions for continued clin-
ical mentorship. The transition to digital online mentoring proved to be useful during COVID-19 pandemic from June - September 2020.
During the Pandemic, the digital platform was utilized to renew and improve focus towards safety standards and Infection Prevention (IP) practices.
Step 1: Preparation for Online Mentoring (Preparatory Phase)• The preparatory phase of organizing a
physical or online mentoring and process-es after conduction of the mentoring ses-sion remains largely the same (Details of the same are given above in Step 1: Prepa-ration for field visit mentoring and Step 3: Sharing observations with state and men-tee facilities). So, the additional steps or steps which were different during online mentoring session have been described below:
• Challenges: Setting up an online mentoring platform and getting both the mentor – ment-ee facilities oriented to how to use online plat-form initially was challenging for the Vriddhi state team, but it was made possible under constraints of pandemic situation as well.
• Advantages of online mentoring: ◆ More providers from mentee facilities were
able to join an online platform and peer ad-dressing of most obstetric and newborn sit-uations could be done
◆ Senior and experienced mentors were able to join the mentoring session who were ei-
ther overtly busy with clinical duties earlier or unfit to travel
◆ Online mentoring was started through IT platform in July 2020. Prior official letter was sent for preparedness for the online mentoring of medical officers and staff nurses of SNCU, LR and maternity OT. On-line mentoring and review has been carried out through the structured checklist.
Step 2: Conduction of Online Mentoring How the online mentoring was conducted - Process overview: Entire process was facili-tated by the MNHRC Nurse Mentor (Confirma-tion and gentle reminder to everyone before the mentoring session):
• Welcoming the State Government officials, RIMS staff (HoDs and Mentors), District Hos-pital staff, National and State Vriddhi team
• Opening remarks by State Government officials• Briefing on objectives for online mentoring
session by State Vriddhi Team• Online mentoring by MNHRC Mentors using
the checklist• Experience sharing and discussion on ex-
pectation of the Mentees• Concluding remarks and Vote of thanks
Transition to Online Mentoring During COVID-19 Pandemic
Maternal & Newborn Health Resource Center16
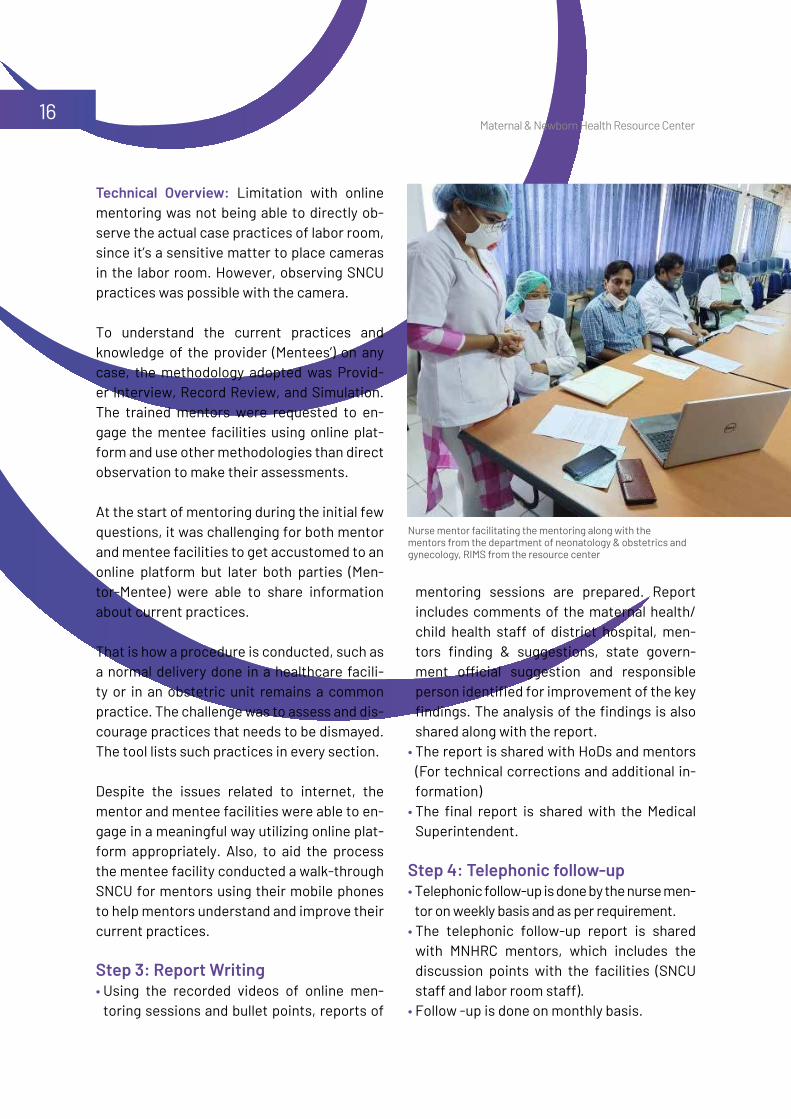
Technical Overview: Limitation with online mentoring was not being able to directly ob-serve the actual case practices of labor room, since it’s a sensitive matter to place cameras in the labor room. However, observing SNCU practices was possible with the camera.
To understand the current practices and knowledge of the provider (Mentees’) on any case, the methodology adopted was Provid-er Interview, Record Review, and Simulation. The trained mentors were requested to en-gage the mentee facilities using online plat-form and use other methodologies than direct observation to make their assessments.
At the start of mentoring during the initial few questions, it was challenging for both mentor and mentee facilities to get accustomed to an online platform but later both parties (Men-tor-Mentee) were able to share information about current practices.
That is how a procedure is conducted, such as a normal delivery done in a healthcare facili-ty or in an obstetric unit remains a common practice. The challenge was to assess and dis-courage practices that needs to be dismayed. The tool lists such practices in every section.
Despite the issues related to internet, the mentor and mentee facilities were able to en-gage in a meaningful way utilizing online plat-form appropriately. Also, to aid the process the mentee facility conducted a walk-through SNCU for mentors using their mobile phones to help mentors understand and improve their current practices.
Step 3: Report Writing• Using the recorded videos of online men-
toring sessions and bullet points, reports of
mentoring sessions are prepared. Report includes comments of the maternal health/ child health staff of district hospital, men-tors finding & suggestions, state govern-ment official suggestion and responsible person identified for improvement of the key findings. The analysis of the findings is also shared along with the report.
• The report is shared with HoDs and mentors (For technical corrections and additional in-formation)
• The final report is shared with the Medical Superintendent.
Step 4: Telephonic follow-up • Telephonic follow-up is done by the nurse men-
tor on weekly basis and as per requirement. • The telephonic follow-up report is shared
with MNHRC mentors, which includes the discussion points with the facilities (SNCU staff and labor room staff).
• Follow -up is done on monthly basis.
Nurse mentor facilitating the mentoring along with the mentors from the department of neonatology & obstetrics and gynecology, RIMS from the resource center
Maternal & Newborn Health Resource Center17
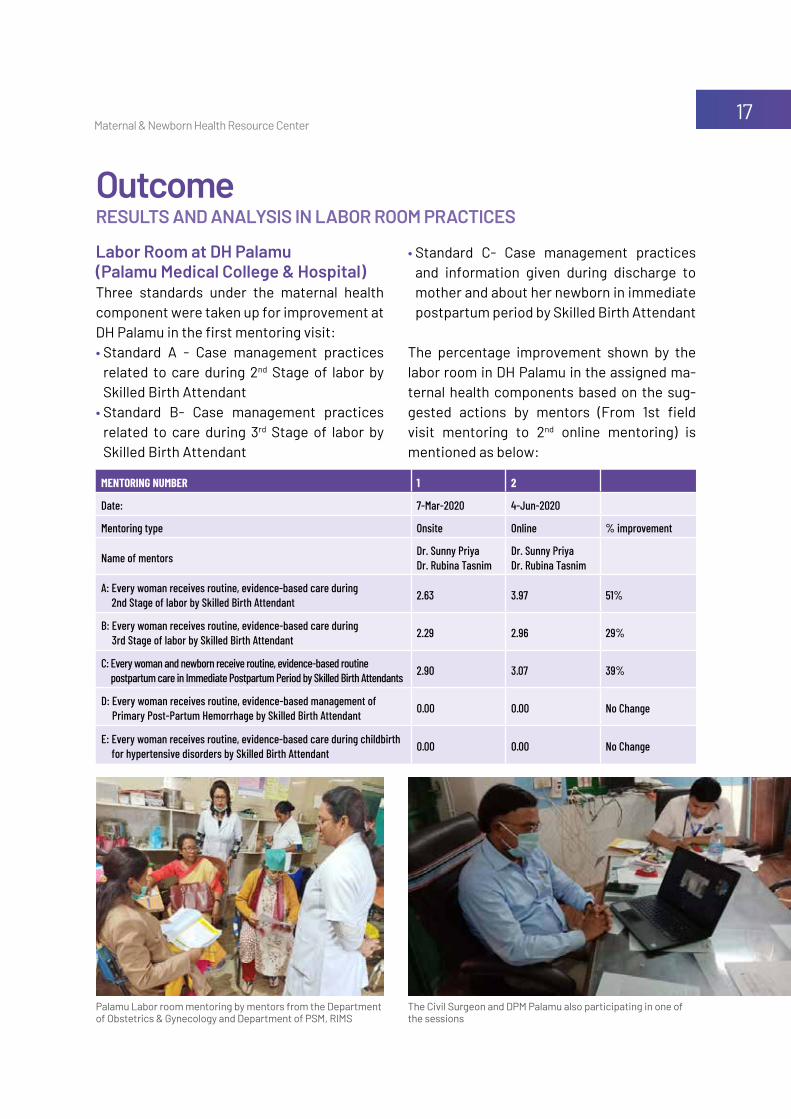
Labor Room at DH Palamu (Palamu Medical College & Hospital)Three standards under the maternal health component were taken up for improvement at DH Palamu in the first mentoring visit:• Standard A - Case management practices
related to care during 2nd Stage of labor by Skilled Birth Attendant
• Standard B- Case management practices related to care during 3rd Stage of labor by Skilled Birth Attendant
OutcomeRESULTS AND ANALySIS IN LABOR ROOM PRACTICES
mentoring number 1 2
Date: 7-Mar-2020 4-Jun-2020
Mentoring type Onsite Online % improvement
Name of mentors Dr. Sunny Priya Dr. Rubina Tasnim
Dr. Sunny Priya Dr. Rubina Tasnim
A: Every woman receives routine, evidence-based care during 2nd Stage of labor by Skilled Birth Attendant 2.63 3.97 51%
B: Every woman receives routine, evidence-based care during 3rd Stage of labor by Skilled Birth Attendant 2.29 2.96 29%
C: Every woman and newborn receive routine, evidence-based routine postpartum care in Immediate Postpartum Period by Skilled Birth Attendants 2.90 3.07 39%
D: Every woman receives routine, evidence-based management of Primary Post-Partum Hemorrhage by Skilled Birth Attendant 0.00 0.00 No Change
E: Every woman receives routine, evidence-based care during childbirth for hypertensive disorders by Skilled Birth Attendant 0.00 0.00 No Change
• Standard C- Case management practices and information given during discharge to mother and about her newborn in immediate postpartum period by Skilled Birth Attendant
The percentage improvement shown by the labor room in DH Palamu in the assigned ma-ternal health components based on the sug-gested actions by mentors (From 1st field visit mentoring to 2nd online mentoring) is mentioned as below:
Palamu Labor room mentoring by mentors from the Department of Obstetrics & Gynecology and Department of PSM, RIMS
The Civil Surgeon and DPM Palamu also participating in one of the sessions
Maternal & Newborn Health Resource Center18
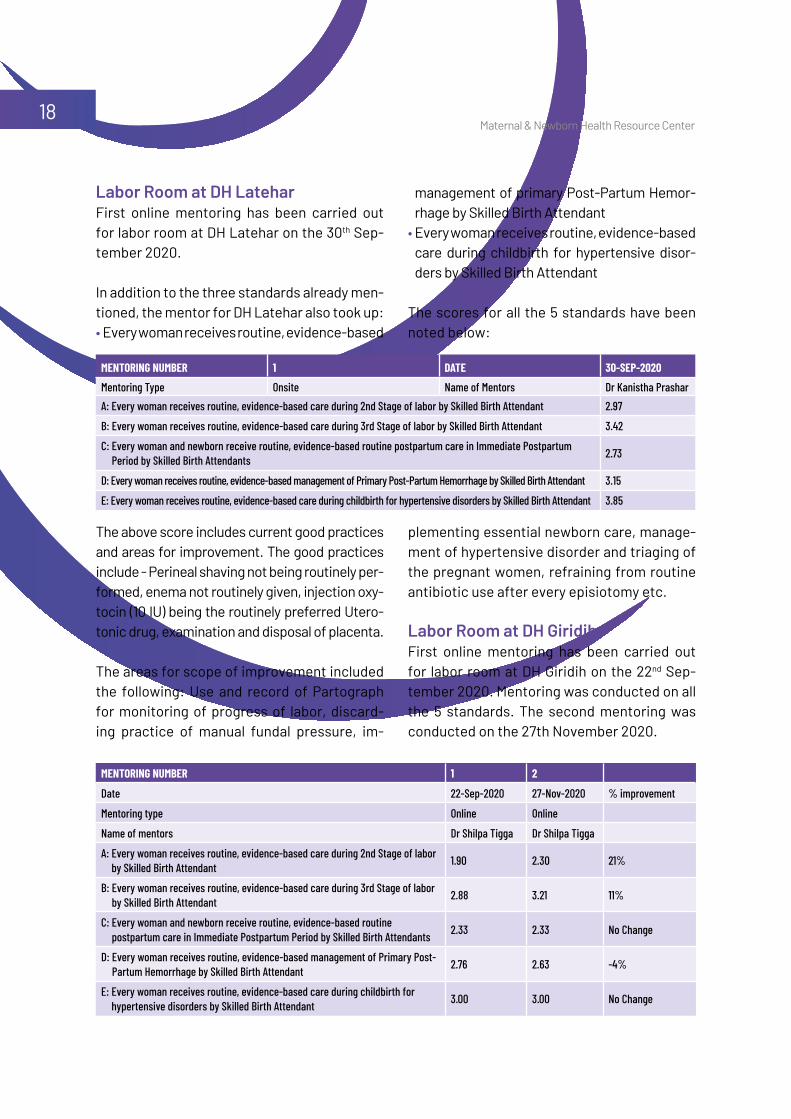
Labor Room at DH LateharFirst online mentoring has been carried out for labor room at DH Latehar on the 30th Sep-tember 2020.
In addition to the three standards already men-tioned, the mentor for DH Latehar also took up:• Every woman receives routine, evidence-based
mentoring number 1 Date 30-sep-2020Mentoring Type Onsite Name of Mentors Dr Kanistha PrasharA: Every woman receives routine, evidence-based care during 2nd Stage of labor by Skilled Birth Attendant 2.97
B: Every woman receives routine, evidence-based care during 3rd Stage of labor by Skilled Birth Attendant 3.42
C: Every woman and newborn receive routine, evidence-based routine postpartum care in Immediate Postpartum Period by Skilled Birth Attendants 2.73
D: Every woman receives routine, evidence-based management of Primary Post-Partum Hemorrhage by Skilled Birth Attendant 3.15
E: Every woman receives routine, evidence-based care during childbirth for hypertensive disorders by Skilled Birth Attendant 3.85
management of primary Post-Partum Hemor-rhage by Skilled Birth Attendant
• Every woman receives routine, evidence-based care during childbirth for hypertensive disor-ders by Skilled Birth Attendant
The scores for all the 5 standards have been noted below:
The above score includes current good practices and areas for improvement. The good practices include - Perineal shaving not being routinely per-formed, enema not routinely given, injection oxy-tocin (10 IU) being the routinely preferred Utero-tonic drug, examination and disposal of placenta.
The areas for scope of improvement included the following: Use and record of Partograph for monitoring of progress of labor, discard-ing practice of manual fundal pressure, im-
plementing essential newborn care, manage-ment of hypertensive disorder and triaging of the pregnant women, refraining from routine antibiotic use after every episiotomy etc.
Labor Room at DH GiridihFirst online mentoring has been carried out for labor room at DH Giridih on the 22nd Sep-tember 2020. Mentoring was conducted on all the 5 standards. The second mentoring was conducted on the 27th November 2020.
mentoring number 1 2
Date 22-Sep-2020 27-Nov-2020 % improvement
Mentoring type Online Online
Name of mentors Dr Shilpa Tigga Dr Shilpa Tigga
A: Every woman receives routine, evidence-based care during 2nd Stage of labor by Skilled Birth Attendant 1.90 2.30 21%
B: Every woman receives routine, evidence-based care during 3rd Stage of labor by Skilled Birth Attendant 2.88 3.21 11%
C: Every woman and newborn receive routine, evidence-based routine postpartum care in Immediate Postpartum Period by Skilled Birth Attendants 2.33 2.33 No Change
D: Every woman receives routine, evidence-based management of Primary Post-Partum Hemorrhage by Skilled Birth Attendant 2.76 2.63 -4%
E: Every woman receives routine, evidence-based care during childbirth for hypertensive disorders by Skilled Birth Attendant 3.00 3.00 No Change
Maternal & Newborn Health Resource Center19
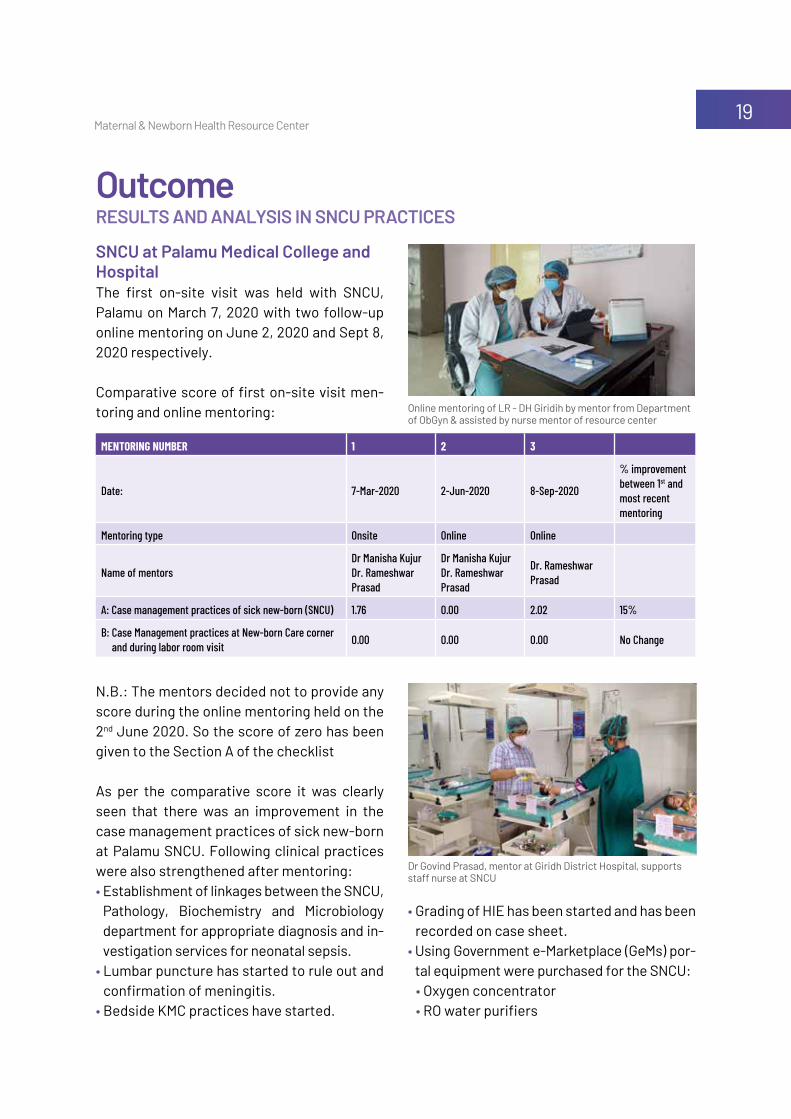
SNCU at Palamu Medical College and Hospital The first on-site visit was held with SNCU, Palamu on March 7, 2020 with two follow-up online mentoring on June 2, 2020 and Sept 8, 2020 respectively.
Comparative score of first on-site visit men-toring and online mentoring:
N.B.: The mentors decided not to provide any score during the online mentoring held on the 2nd June 2020. So the score of zero has been given to the Section A of the checklist
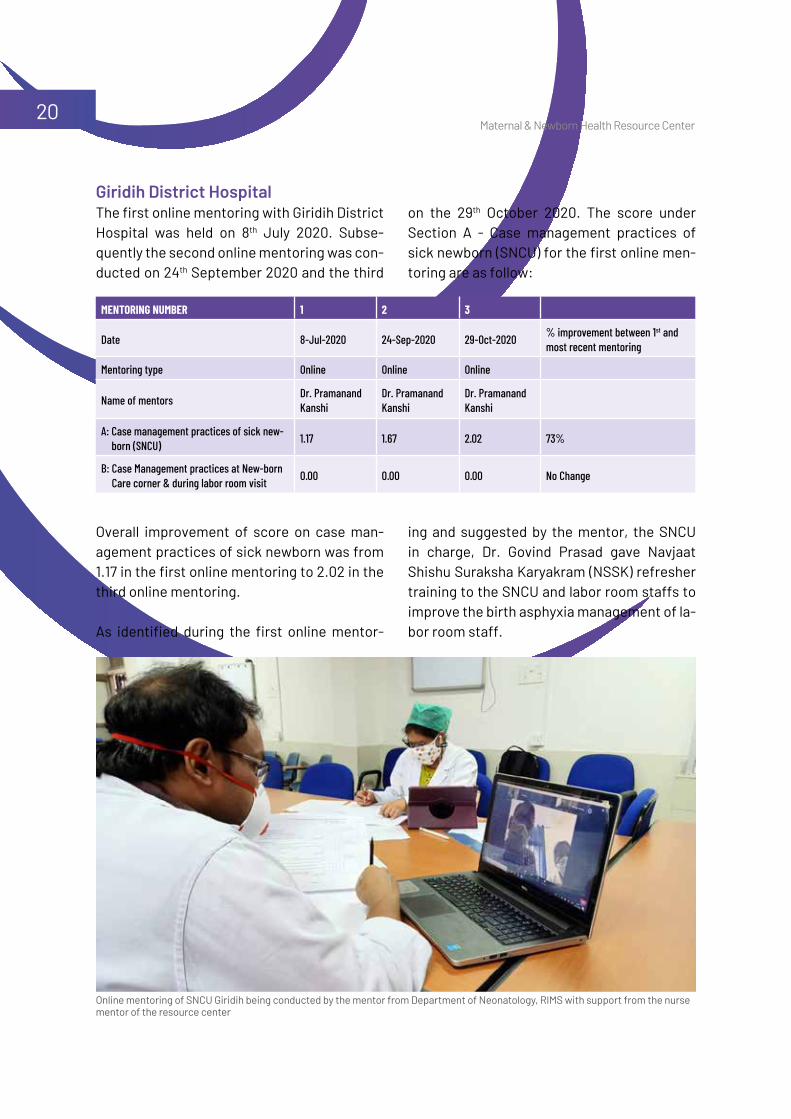
As per the comparative score it was clearly seen that there was an improvement in the case management practices of sick new-born at Palamu SNCU. Following clinical practices were also strengthened after mentoring:• Establishment of linkages between the SNCU,
Pathology, Biochemistry and Microbiology department for appropriate diagnosis and in-vestigation services for neonatal sepsis.
• Lumbar puncture has started to rule out and confirmation of meningitis.
• Bedside KMC practices have started.
mentoring number 1 2 3
Date: 7-Mar-2020 2-Jun-2020 8-Sep-2020
% improvement between 1st and most recent mentoring
Mentoring type Onsite Online Online
Name of mentorsDr Manisha Kujur Dr. Rameshwar Prasad
Dr Manisha Kujur Dr. Rameshwar Prasad
Dr. Rameshwar Prasad
A: Case management practices of sick new-born (SNCU) 1.76 0.00 2.02 15%
B: Case Management practices at New-born Care corner and during labor room visit 0.00 0.00 0.00 No Change
• Grading of HIE has been started and has been recorded on case sheet.
• Using Government e-Marketplace (GeMs) por-tal equipment were purchased for the SNCU: • Oxygen concentrator• RO water purifiers
OutcomeRESULTS AND ANALySIS IN SNCU PRACTICES
Online mentoring of LR - DH Giridih by mentor from Department of ObGyn & assisted by nurse mentor of resource center
Dr Govind Prasad, mentor at Giridh District Hospital, supports staff nurse at SNCU
Maternal & Newborn Health Resource Center20
mentoring number 1 2 3
Date 8-Jul-2020 24-Sep-2020 29-Oct-2020 % improvement between 1st and most recent mentoring
Mentoring type Online Online Online
Name of mentors Dr. Pramanand Kanshi
Dr. Pramanand Kanshi
Dr. Pramanand Kanshi
A: Case management practices of sick new-born (SNCU) 1.17 1.67 2.02 73%
B: Case Management practices at New-born Care corner & during labor room visit 0.00 0.00 0.00 No Change
Giridih District HospitalThe first online mentoring with Giridih District Hospital was held on 8th July 2020. Subse-quently the second online mentoring was con-ducted on 24th September 2020 and the third
on the 29th October 2020. The score under Section A - Case management practices of sick newborn (SNCU) for the first online men-toring are as follow:
Online mentoring of SNCU Giridih being conducted by the mentor from Department of Neonatology, RIMS with support from the nurse mentor of the resource center
Overall improvement of score on case man-agement practices of sick newborn was from 1.17 in the first online mentoring to 2.02 in the third online mentoring.
As identified during the first online mentor-
ing and suggested by the mentor, the SNCU in charge, Dr. Govind Prasad gave Navjaat Shishu Suraksha Karyakram (NSSK) refresher training to the SNCU and labor room staffs to improve the birth asphyxia management of la-bor room staff.
Maternal & Newborn Health Resource Center21
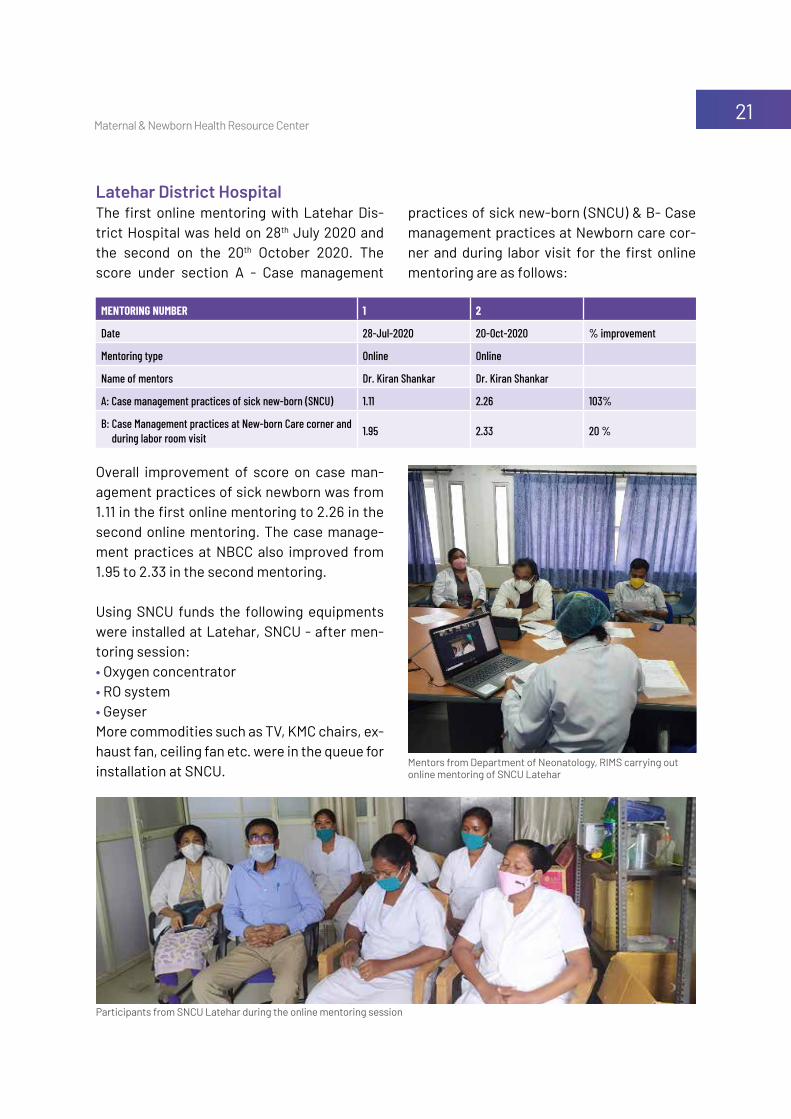
Overall improvement of score on case man-agement practices of sick newborn was from 1.11 in the first online mentoring to 2.26 in the second online mentoring. The case manage-ment practices at NBCC also improved from 1.95 to 2.33 in the second mentoring.
Using SNCU funds the following equipments were installed at Latehar, SNCU - after men-toring session:• Oxygen concentrator• RO system • Geyser More commodities such as TV, KMC chairs, ex-haust fan, ceiling fan etc. were in the queue for installation at SNCU.
mentoring number 1 2
Date 28-Jul-2020 20-Oct-2020 % improvement
Mentoring type Online Online
Name of mentors Dr. Kiran Shankar Dr. Kiran Shankar
A: Case management practices of sick new-born (SNCU) 1.11 2.26 103%
B: Case Management practices at New-born Care corner and during labor room visit 1.95 2.33 20 %
Latehar District HospitalThe first online mentoring with Latehar Dis-trict Hospital was held on 28th July 2020 and the second on the 20th October 2020. The score under section A - Case management
practices of sick new-born (SNCU) & B- Case management practices at Newborn care cor-ner and during labor visit for the first online mentoring are as follows:
Participants from SNCU Latehar during the online mentoring session
Mentors from Department of Neonatology, RIMS carrying out online mentoring of SNCU Latehar
Maternal & Newborn Health Resource Center22
During Preparatory Phase• RIMS Ranchi is an autonomous medical col-
lege which comes under the preview of the Directorate of Health Services (DHS). The pro-cess to develop a collaboration on this issue between DHS and the National Health Mission, Jharkhand took time in the initial phase.
• Transfer of funds from the project to the Medical College (an autonomous institution) for establishing the Resource Center was an-other deterrent. There was no way to transfer the funds from Project Vriddhi funds to RIMS. However, the determination to drive the agenda of setting standard based case man-agement practices led to Project Vriddhi team to recruit human resources, procure com-modities and establish the state of art MNHRC from its own resources instead of waiting to transfer funds to RIMS as per the initial plan.
• Though not difficult but it was challenging to bring the maternal health cell and the child health cell, NHM Jharkhand together to drive this agenda forward.
• To improve accountability of the MNHRC host – i.e. RIMS – it was suggested to nominate a fac-ulty as ‘Head’ of MHNHRC. However, this met with a lot of resistance as most faculty remain extremely busy round the year. As a solution, the Medical Superintendent was made ‘Officer in Charge’ of the Resource Center along with one of the HoDs of three concerned depart-ments on term by term basis.
Challenges Faced by MNH Resources Centre
• The synchronizing of a common date and date for the 3 departments – i) Obstetrics & Gy-necology ii) Pediatrics and iii) P&SM - for the launch and ToT of the mentors was an issue.
• Coordination between the departments and the Resource Center for the mentoring dates remains a challenge. Hence, the mentoring visits for SNCUs and LRs have been sepa-rately scheduled to avoid need for additional co-ordination.
During the Mentoring Session:• Poor audio/video conferencing quality dur-
ing online mentoring• Handholding of mentors and mentee facili-
ties is required while conducting online men-toring due to lack of exposure and appropri-ate technology.
• Lack of sufficient internet bandwidth• MNHRC mentors’ emergency COVID-19 duty
clashed with planned dates for online men-toring.
• Mentors on sudden leave. (Since the mentors are fixed for every district (To facilitate bet-ter understanding and continuity), they can-not be replaced)
• Sudden scheduling of departmental meet-ings which clash with the online mentoring dates and timing.
• Due to technology hiccups, the mentors of-ten cannot complete the whole checklist in one sitting.
Maternal & Newborn Health Resource Center23
The mentoring model has proved to be simple and effective in public health setting with min-imal external support. The Medical College fac-ulty are useful mentors to high case load facil-ities like DH and FRUs and is evident from the initial visits only. The Resource Center is slowly pushing both the mentor and mentee facilities towards an efficient healthcare system where every women and newborn would have access to quality and positive healthcare.
One of the positive side-effects of this exer-cise is that the mentors have improved and upgraded their own knowledge and practice of clinical care standards and started looking for more clinical updates to mentor the ment-ee facilities better.
Way Forward and SustainabilityTaking advantage of the clinical expertise from the medical college and creating a channel for the knowledge and skill to flow to other facili-ties is a fruitful way of leveraging existing ex-pertise and works within available resources.
Considering the viable nature and feasible model of MNHRC, the state of Jharkhand has included its running cost in the proposed State National Health Mission PIP 2020-21. This proposal was accepted by Government of India as per Record of Proceedings (ROP) 20-21. USAID Vriddhi and MNHRC agreement is up to 31st December 2020 and after which the GoI approved funding will drive the agenda of standardization of clinical care in RMNCHA in the state of Jharkhand.
Maternal & Newborn Health Resource Center24
Annexures Annexure 1: Letter from RIMS to Secretary, Health for Institutionalization of Jharkhand State Maternal and Newborn Health Resource Center
Maternal & Newborn Health Resource Center25
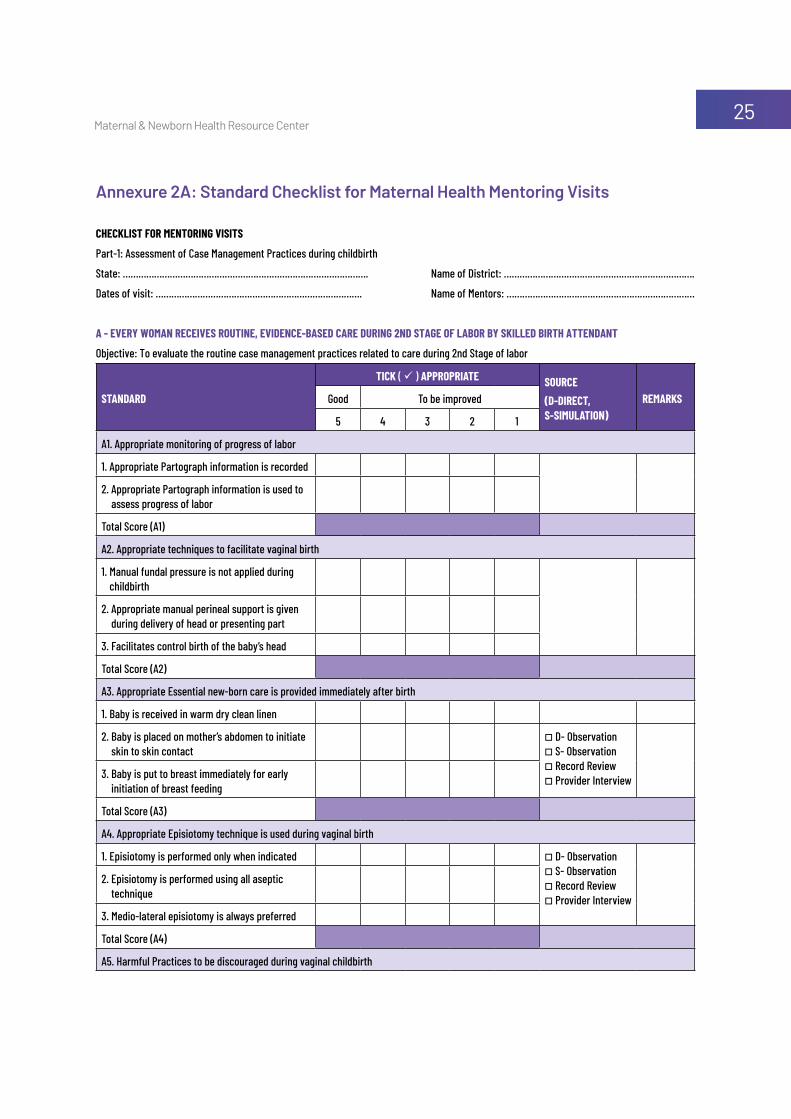
Annexure 2A: Standard Checklist for Maternal Health Mentoring Visits
CHeCklist for mentoring visits
Part-1: Assessment of Case Management Practices during childbirth
State: …………………………………………………………………………………. Name of District: ……………………………………………………………….
Dates of visit: ……………………………………………………………………. Name of Mentors: ………………………………………………………………
a - every woman reCeives routine, eviDenCe-baseD Care During 2nD stage of labor by skilleD birtH attenDant
Objective: To evaluate the routine case management practices related to care during 2nd Stage of labor
stanDarD
tiCk ( ü ) appropriate sourCe(D-DireCt, s-simulation)
remarksGood To be improved
5 4 3 2 1
A1. Appropriate monitoring of progress of labor
1. Appropriate Partograph information is recorded
2. Appropriate Partograph information is used to assess progress of labor
Total Score (A1)
A2. Appropriate techniques to facilitate vaginal birth
1. Manual fundal pressure is not applied during childbirth
2. Appropriate manual perineal support is given during delivery of head or presenting part
3. Facilitates control birth of the baby’s head
Total Score (A2)
A3. Appropriate Essential new-born care is provided immediately after birth
1. Baby is received in warm dry clean linen
2. Baby is placed on mother’s abdomen to initiate skin to skin contact
o D- Observationo S- Observationo Record Review o Provider Interview3. Baby is put to breast immediately for early
initiation of breast feeding
Total Score (A3)
A4. Appropriate Episiotomy technique is used during vaginal birth
1. Episiotomy is performed only when indicated o D- Observationo S- Observationo Record Review o Provider Interview
2. Episiotomy is performed using all aseptic technique
3. Medio-lateral episiotomy is always preferred
Total Score (A4)
A5. Harmful Practices to be discouraged during vaginal childbirth

Maternal & Newborn Health Resource Center26
stanDarD
tiCk ( ü ) appropriate sourCe(D-DireCt, s-simulation)
remarksGood To be improved
5 4 3 2 1
1. Perineal shaving is not routinely performed o D- Observationo S- Observationo Record Review o Provider Interview
2. Enema is not routinely given
3. Vaginal examination is not done (in less than 4 hours)
4. Augmentation of Labor is not routinely performed
5. Routinely antibiotics are not prescribed after vaginal birth
Total Score (A5)
Summary Table: A. Case management practices related to care during 2nd Stage of labor by Skilled Birth Attendant
stanDarD sCore
A1. Appropriate Monitoring of progress of labor
A2. Appropriate techniques to facilitate vaginal birth
A3. Appropriate Essential new-born care is provided immediately after birth
A4. Appropriate Episiotomy technique is used during vaginal birth
A5. Harmful Practices to be discouraged during vaginal childbirth
Average Score = (A1+A2+A3+A4+A5)/5
Main areas of strengths & Good practices
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Main areas where strengthening is required
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
b - every woman reCeives routine, eviDenCe-baseD Care During 3rD stage of labor by skilleD birtH attenDant

Maternal & Newborn Health Resource Center27
Objective: To evaluate the routine case management practices related to care during 3rd Stage of labor
stanDarD
tiCk ( ü ) appropriate sourCe(D – DireCt, s – simulation)
remarksGood To be improved
5 4 3 2 1
B1. Appropriate practices during third stage of labor
1. Oxytocin (10 IU, IM) is the routinely preferred uterotonic drug
o D- Observationo S- Observation o Record Review o Provider Interview2. Controlled cord traction is provided
appropriately by SBA
3. Uterine massage is not routinely performed
Total Score (B1)
B2. Appropriate examination and disposal of Placenta
1. Appropriately examines placenta and membranes for completeness and abnormality
o D- Observationo S- Observation o Record Review o Provider Interview
2. Appropriately disposes placenta (as per the Infection Prevention Protocol)
Total Score (B2)
B3. Appropriate monitoring to prevent Post-Partum Hemorrhage
1. Appropriately monitors maternal vitals, uterine tonus, fundal height and vaginal bleeding (to identify early signs of hypovolemic shock)
o D- Observationo S- Observation o Record Review o Provider Interview
Total Score (B3)
B4. Appropriate examination and repair of Episiotomy / Tear
1. Examines perineum under good light following childbirth for any tear / laceration
o D- Observationo S- Observation o Record Review o Provider Interview
2. Appropriately, repairs all tear
3. Antibiotics are not prescribed routinely after episiotomy
Total Score (B4)
Summary Table: B. Case management practices related to care during 3rd Stage of labor by Skilled Birth Attendant
stanDarD sCore
B1. Appropriate practices during third stage of labor
B2. Appropriate examination and disposal of Placenta
B3. Appropriate monitoring to prevent Post-Partum Hemorrhage
B4. Appropriate examination and repair of Episiotomy / Tear
Average Score = (B1+B2+B3+B4)/4
Maternal & Newborn Health Resource Center28
Main areas of strengths & Good practices
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Main areas where strengthening is required
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
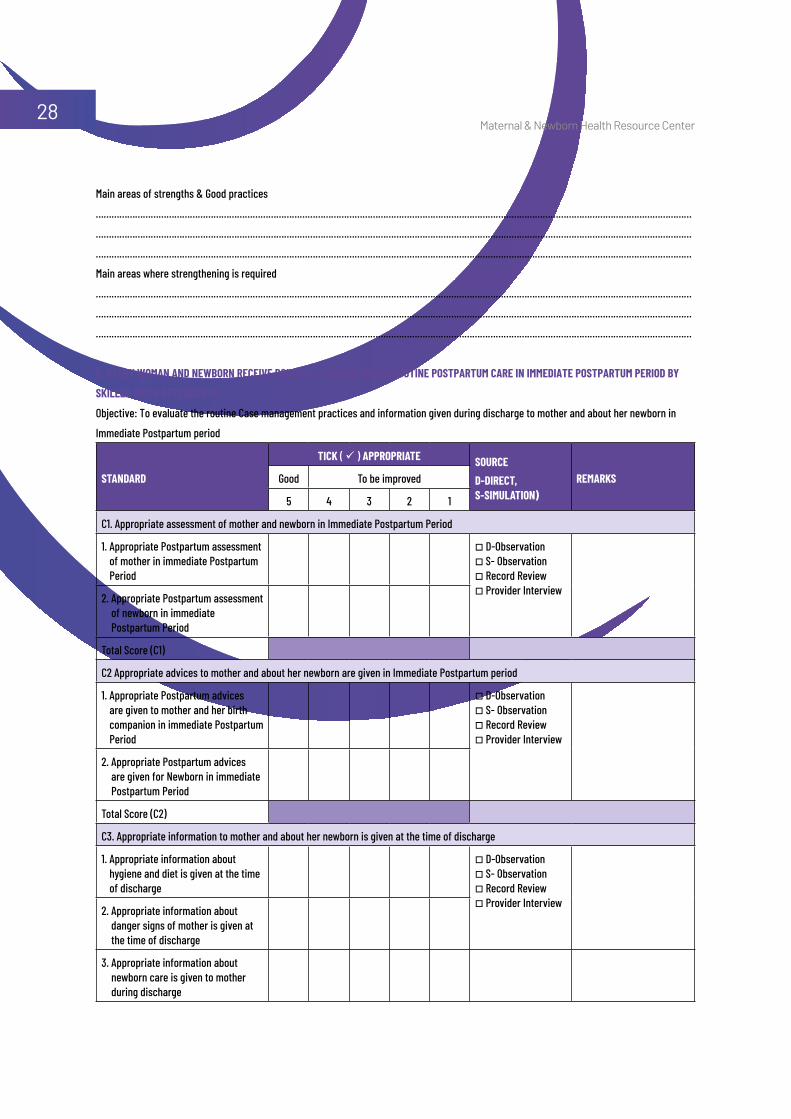
C: every woman anD newborn reCeive routine, eviDenCe-baseD routine postpartum Care in immeDiate postpartum perioD by
skilleD birtH attenDants
Objective: To evaluate the routine Case management practices and information given during discharge to mother and about her newborn in
Immediate Postpartum period
stanDarD
tiCk ( ü ) appropriate sourCe D-DireCt, s-simulation)
remarksGood To be improved
5 4 3 2 1
C1. Appropriate assessment of mother and newborn in Immediate Postpartum Period
1. Appropriate Postpartum assessment of mother in immediate Postpartum Period
o D-Observationo S- Observationo Record Review o Provider Interview
2. Appropriate Postpartum assessment of newborn in immediate Postpartum Period
Total Score (C1)
C2 Appropriate advices to mother and about her newborn are given in Immediate Postpartum period
1. Appropriate Postpartum advices are given to mother and her birth companion in immediate Postpartum Period
o D-Observationo S- Observationo Record Review o Provider Interview
2. Appropriate Postpartum advices are given for Newborn in immediate Postpartum Period
Total Score (C2)
C3. Appropriate information to mother and about her newborn is given at the time of discharge
1. Appropriate information about hygiene and diet is given at the time of discharge
o D-Observationo S- Observationo Record Review o Provider Interview
2. Appropriate information about danger signs of mother is given at the time of discharge
3. Appropriate information about newborn care is given to mother during discharge

Maternal & Newborn Health Resource Center29
4. Appropriate information regarding care of low birth weight babies is given at the time of discharge
5. Appropriate information about danger signs of newborn is given to mother/ family members at the time of discharge
Total Score (C3)Summary Table: C. Case management practices and information given during discharge to mother and about her newborn in Immediate
Postpartum period by Skilled Birth Attendant
stanDarD sCore
C1. Appropriate assessment of mother and newborn in Immediate Postpartum Period
C2. Appropriate advices to mother and about her newborn are given in Immediate Postpartum period
C3. Appropriate information to mother and about her newborn is given at the time of discharge
Average Score = (C1+C2+C3)/3
Main areas of strengths & Good practices
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Main areas where strengthening is required
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Maternal & Newborn Health Resource Center30
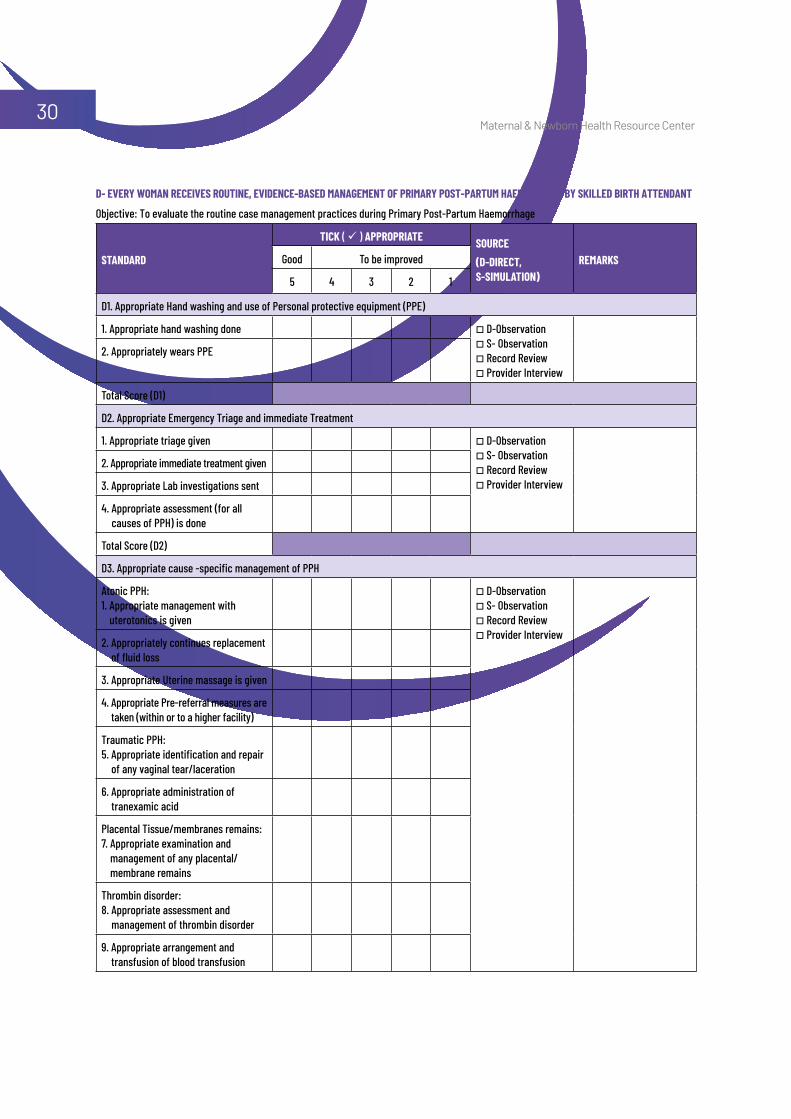
D- every woman reCeives routine, eviDenCe-baseD management of primary post-partum HaemorrHage by skilleD birtH attenDant
Objective: To evaluate the routine case management practices during Primary Post-Partum Haemorrhage
stanDarD
tiCk ( ü ) appropriate sourCe(D-DireCt, s-simulation)
remarksGood To be improved
5 4 3 2 1
D1. Appropriate Hand washing and use of Personal protective equipment (PPE)
1. Appropriate hand washing done o D-Observationo S- Observationo Record Review o Provider Interview
2. Appropriately wears PPE
Total Score (D1)
D2. Appropriate Emergency Triage and immediate Treatment
1. Appropriate triage given o D-Observationo S- Observationo Record Review o Provider Interview
2. Appropriate immediate treatment given
3. Appropriate Lab investigations sent
4. Appropriate assessment (for all causes of PPH) is done
Total Score (D2)
D3. Appropriate cause -specific management of PPH
Atonic PPH: 1. Appropriate management with
uterotonics is given
o D-Observationo S- Observationo Record Review o Provider Interview
2. Appropriately continues replacement of fluid loss
3. Appropriate Uterine massage is given
4. Appropriate Pre-referral measures are taken (within or to a higher facility)
Traumatic PPH:5. Appropriate identification and repair
of any vaginal tear/laceration
6. Appropriate administration of tranexamic acid
Placental Tissue/membranes remains:7. Appropriate examination and
management of any placental/ membrane remains
Thrombin disorder: 8. Appropriate assessment and
management of thrombin disorder
9. Appropriate arrangement and transfusion of blood transfusion
Maternal & Newborn Health Resource Center31
stanDarD
tiCk ( ü ) appropriate sourCe(D-DireCt, s-simulation)
remarksGood To be improved
5 4 3 2 1
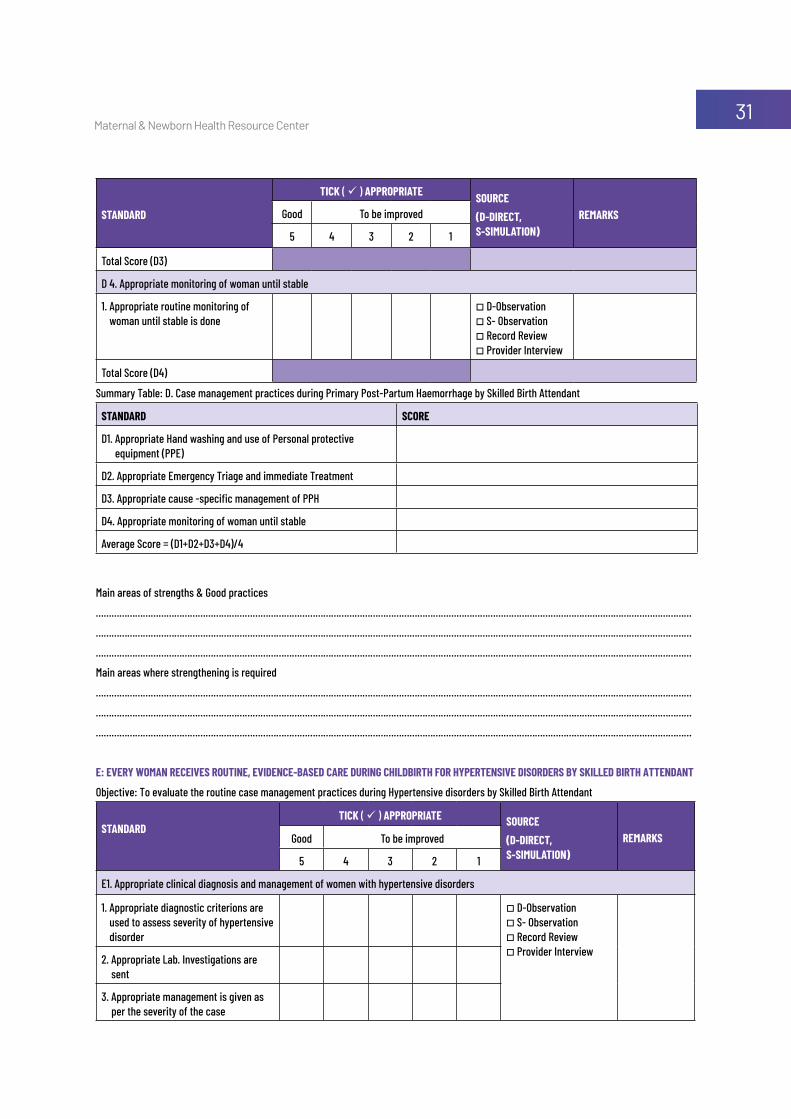
Total Score (D3)
D 4. Appropriate monitoring of woman until stable
1. Appropriate routine monitoring of woman until stable is done
o D-Observationo S- Observationo Record Review o Provider Interview
Total Score (D4)
Summary Table: D. Case management practices during Primary Post-Partum Haemorrhage by Skilled Birth Attendant
stanDarD sCore
D1. Appropriate Hand washing and use of Personal protective equipment (PPE)
D2. Appropriate Emergency Triage and immediate Treatment
D3. Appropriate cause -specific management of PPH
D4. Appropriate monitoring of woman until stable
Average Score = (D1+D2+D3+D4)/4
Main areas of strengths & Good practices
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Main areas where strengthening is required
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
e: every woman reCeives routine, eviDenCe-baseD Care During CHilDbirtH for Hypertensive DisorDers by skilleD birtH attenDant
Objective: To evaluate the routine case management practices during Hypertensive disorders by Skilled Birth Attendant
stanDarD tiCk ( ü ) appropriate sourCe
(D-DireCt, s-simulation)
remarksGood To be improved
5 4 3 2 1
E1. Appropriate clinical diagnosis and management of women with hypertensive disorders
1. Appropriate diagnostic criterions are used to assess severity of hypertensive disorder
o D-Observationo S- Observationo Record Review o Provider Interview
2. Appropriate Lab. Investigations are sent
3. Appropriate management is given as per the severity of the case
Maternal & Newborn Health Resource Center32
stanDarD tiCk ( ü ) appropriate sourCe
(D-DireCt, s-simulation)
remarksGood To be improved
5 4 3 2 1
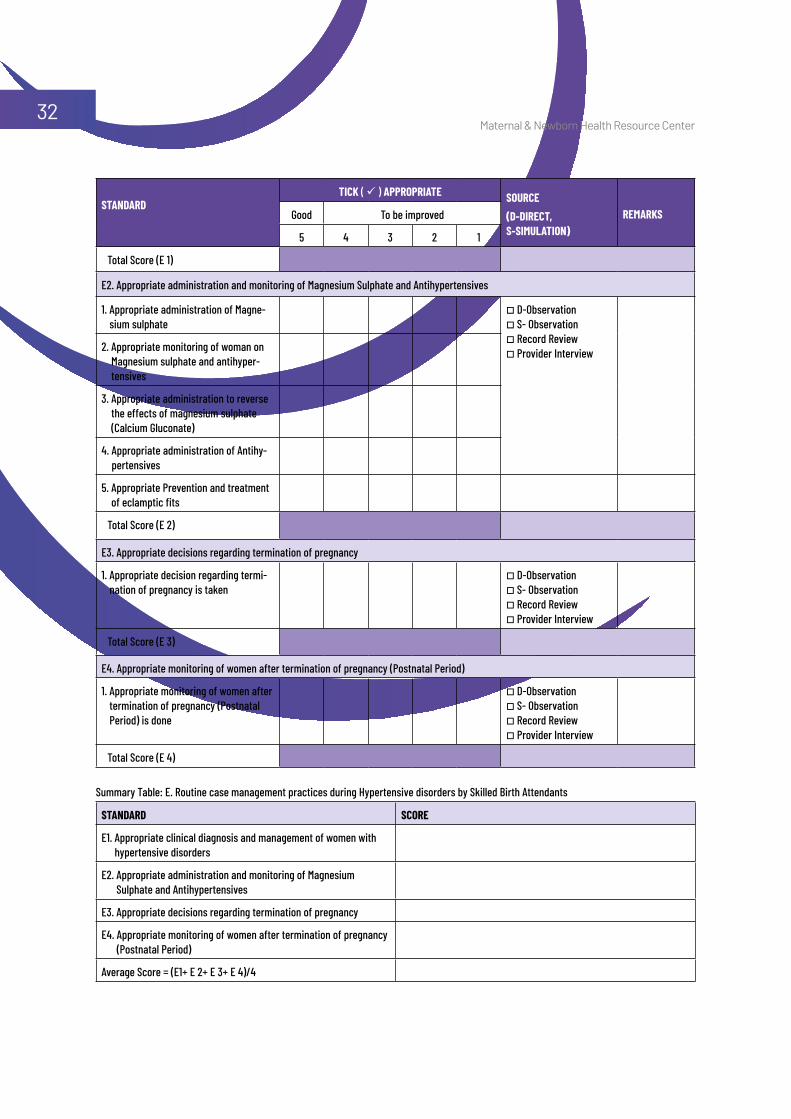
Total Score (E 1)
E2. Appropriate administration and monitoring of Magnesium Sulphate and Antihypertensives
1. Appropriate administration of Magne-sium sulphate
o D-Observationo S- Observationo Record Review o Provider Interview2. Appropriate monitoring of woman on
Magnesium sulphate and antihyper-tensives
3. Appropriate administration to reverse the effects of magnesium sulphate (Calcium Gluconate)
4. Appropriate administration of Antihy-pertensives
5. Appropriate Prevention and treatment of eclamptic fits
Total Score (E 2)
E3. Appropriate decisions regarding termination of pregnancy
1. Appropriate decision regarding termi-nation of pregnancy is taken
o D-Observationo S- Observationo Record Review o Provider Interview
Total Score (E 3)
E4. Appropriate monitoring of women after termination of pregnancy (Postnatal Period)
1. Appropriate monitoring of women after termination of pregnancy (Postnatal Period) is done
o D-Observationo S- Observationo Record Review o Provider Interview
Total Score (E 4)
Summary Table: E. Routine case management practices during Hypertensive disorders by Skilled Birth Attendants
stanDarD sCore
E1. Appropriate clinical diagnosis and management of women with hypertensive disorders
E2. Appropriate administration and monitoring of Magnesium Sulphate and Antihypertensives
E3. Appropriate decisions regarding termination of pregnancy
E4. Appropriate monitoring of women after termination of pregnancy (Postnatal Period)
Average Score = (E1+ E 2+ E 3+ E 4)/4
Maternal & Newborn Health Resource Center33
Main areas of strengths & Good practices
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Main areas where strengthening is required
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Key decisions taken in Debriefing Meeting (with CDMO/ ADMO (Med); SNCU / Ped. I/C, O&G Specialist, Hospital manager):
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Signature, Mentor Signature, ADMO Signature, In charge
Date: Date: Date:
Maternal & Newborn Health Resource Center34
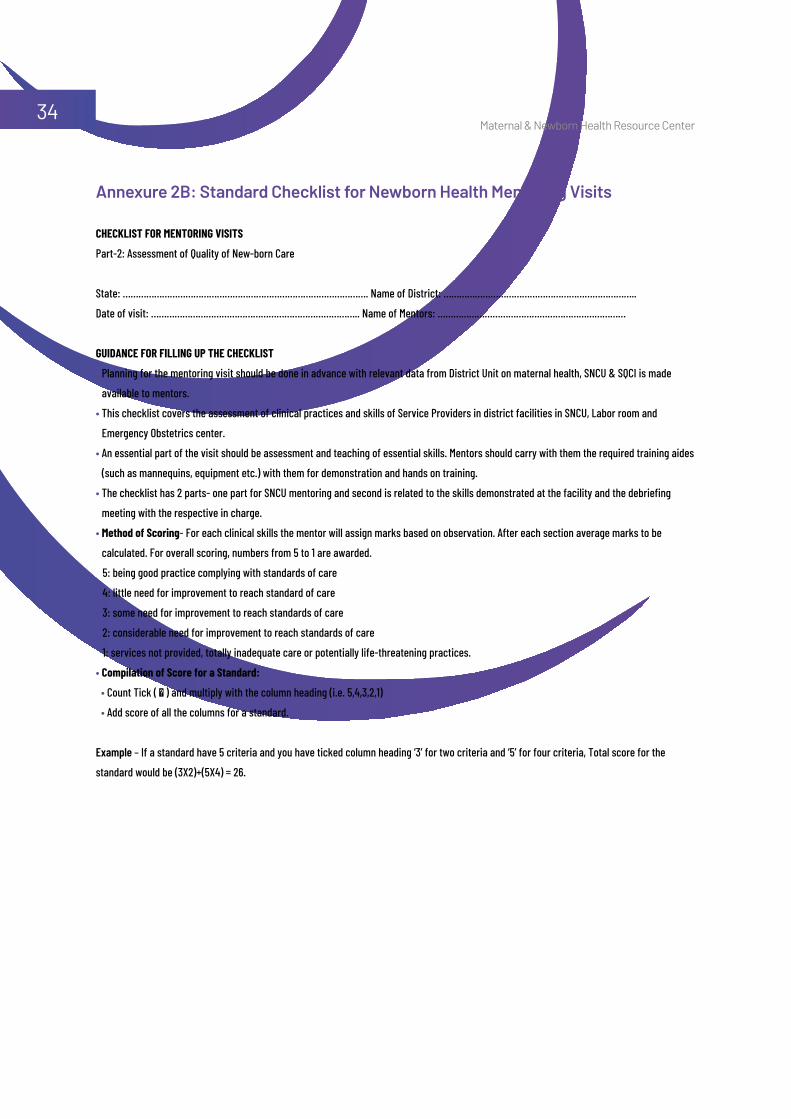
CHeCklist for mentoring visits
Part-2: Assessment of Quality of New-born Care
State: …………………………………………………………………………………. Name of District: ………………………………………………………………..
Date of visit: …………………………………………………………………….. Name of Mentors: ………………………………………………………………
guiDanCe for filling up tHe CHeCklist
• Planning for the mentoring visit should be done in advance with relevant data from District Unit on maternal health, SNCU & SQCI is made
available to mentors.
• This checklist covers the assessment of clinical practices and skills of Service Providers in district facilities in SNCU, Labor room and
Emergency Obstetrics center.
• An essential part of the visit should be assessment and teaching of essential skills. Mentors should carry with them the required training aides
(such as mannequins, equipment etc.) with them for demonstration and hands on training.
• The checklist has 2 parts- one part for SNCU mentoring and second is related to the skills demonstrated at the facility and the debriefing
meeting with the respective in charge.
• method of scoring- For each clinical skills the mentor will assign marks based on observation. After each section average marks to be
calculated. For overall scoring, numbers from 5 to 1 are awarded.
5: being good practice complying with standards of care
4: little need for improvement to reach standard of care
3: some need for improvement to reach standards of care
2: considerable need for improvement to reach standards of care
1: services not provided, totally inadequate care or potentially life-threatening practices.
• Compilation of score for a standard:
• Count Tick ( ) and multiply with the column heading (i.e. 5,4,3,2,1)
• Add score of all the columns for a standard.
Example – If a standard have 5 criteria and you have ticked column heading ‘3’ for two criteria and ‘5’ for four criteria, Total score for the
standard would be (3X2)+(5X4) = 26.
Annexure 2B: Standard Checklist for Newborn Health Mentoring Visits
Maternal & Newborn Health Resource Center35
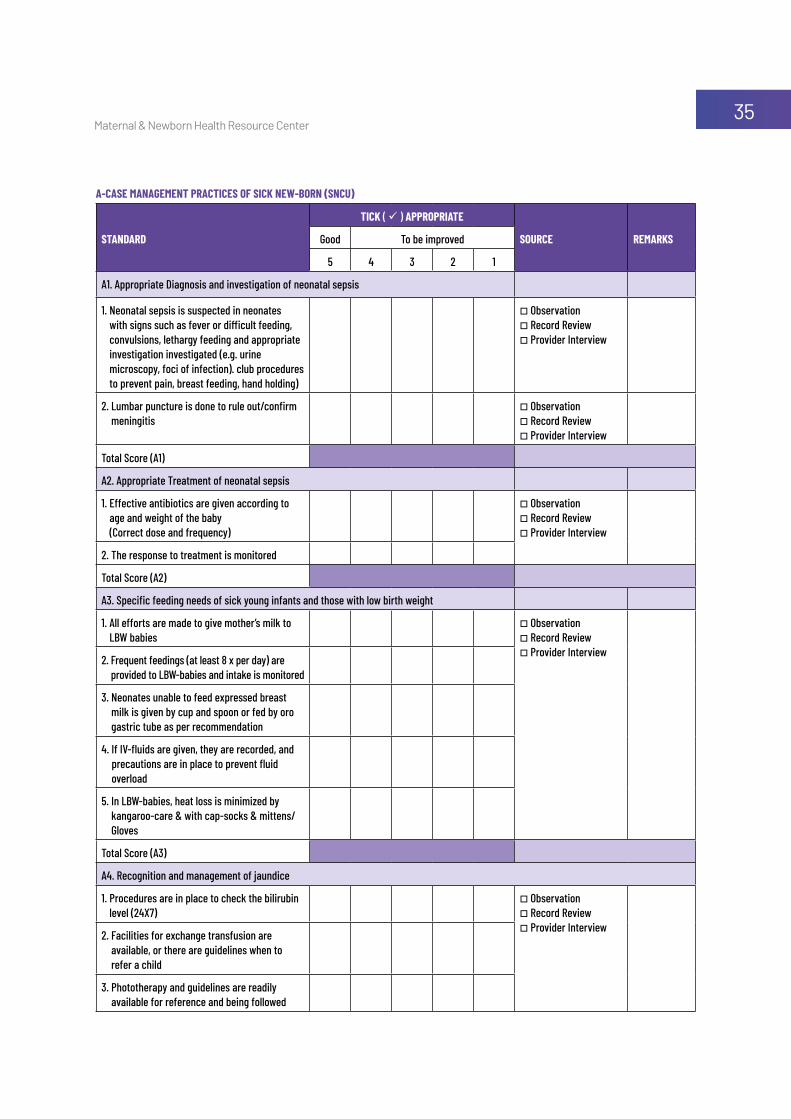
a-Case management praCtiCes of siCk new-born (snCu)
stanDarD
tiCk ( ü ) appropriate
sourCe remarksGood To be improved
5 4 3 2 1
A1. Appropriate Diagnosis and investigation of neonatal sepsis
1. Neonatal sepsis is suspected in neonates with signs such as fever or difficult feeding, convulsions, lethargy feeding and appropriate investigation investigated (e.g. urine microscopy, foci of infection). club procedures to prevent pain, breast feeding, hand holding)
o Observation o Record Review o Provider Interview
2. Lumbar puncture is done to rule out/confirm meningitis
o Observation o Record Review o Provider Interview
Total Score (A1)
A2. Appropriate Treatment of neonatal sepsis
1. Effective antibiotics are given according to age and weight of the baby (Correct dose and frequency)
o Observation o Record Review o Provider Interview
2. The response to treatment is monitored
Total Score (A2)
A3. Specific feeding needs of sick young infants and those with low birth weight
1. All efforts are made to give mother’s milk to LBW babies
o Observation o Record Review o Provider Interview
2. Frequent feedings (at least 8 x per day) are provided to LBW-babies and intake is monitored
3. Neonates unable to feed expressed breast milk is given by cup and spoon or fed by oro gastric tube as per recommendation
4. If IV-fluids are given, they are recorded, and precautions are in place to prevent fluid overload
5. In LBW-babies, heat loss is minimized by kangaroo-care & with cap-socks & mittens/Gloves
Total Score (A3)
A4. Recognition and management of jaundice
1. Procedures are in place to check the bilirubin level (24X7)
o Observation o Record Review o Provider Interview
2. Facilities for exchange transfusion are available, or there are guidelines when to refer a child
3. Phototherapy and guidelines are readily available for reference and being followed
Maternal & Newborn Health Resource Center36
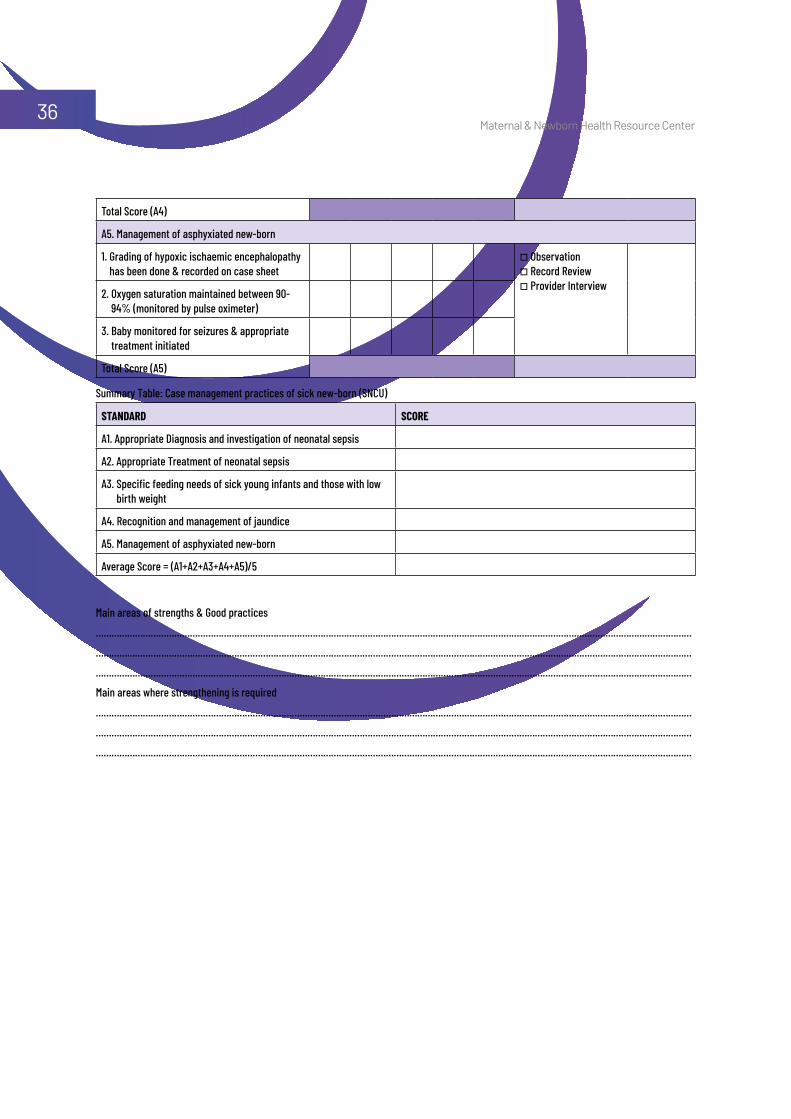
Total Score (A4)
A5. Management of asphyxiated new-born
1. Grading of hypoxic ischaemic encephalopathy has been done & recorded on case sheet
o Observation o Record Review o Provider Interview
2. Oxygen saturation maintained between 90-94% (monitored by pulse oximeter)
3. Baby monitored for seizures & appropriate treatment initiated
Total Score (A5)
Summary Table: Case management practices of sick new-born (SNCU)
stanDarD sCore
A1. Appropriate Diagnosis and investigation of neonatal sepsis
A2. Appropriate Treatment of neonatal sepsis
A3. Specific feeding needs of sick young infants and those with low birth weight
A4. Recognition and management of jaundice
A5. Management of asphyxiated new-born
Average Score = (A1+A2+A3+A4+A5)/5
Main areas of strengths & Good practices
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Main areas where strengthening is required
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Maternal & Newborn Health Resource Center37
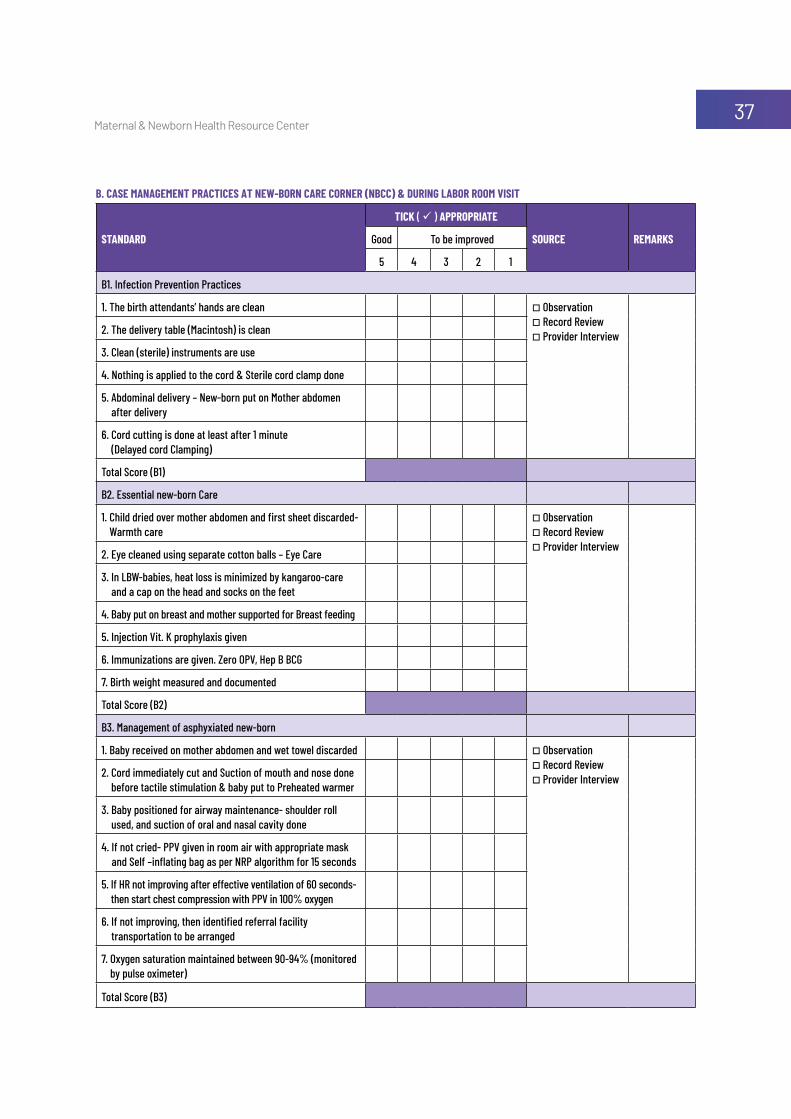
b. Case management praCtiCes at new-born Care Corner (nbCC) & During labor room visit
stanDarD
tiCk ( ü ) appropriate
sourCe remarksGood To be improved
5 4 3 2 1
B1. Infection Prevention Practices
1. The birth attendants’ hands are clean o Observation o Record Review o Provider Interview2. The delivery table (Macintosh) is clean
3. Clean (sterile) instruments are use
4. Nothing is applied to the cord & Sterile cord clamp done
5. Abdominal delivery – New-born put on Mother abdomen after delivery
6. Cord cutting is done at least after 1 minute (Delayed cord Clamping)
Total Score (B1)
B2. Essential new-born Care
1. Child dried over mother abdomen and first sheet discarded- Warmth care
o Observation o Record Review o Provider Interview
2. Eye cleaned using separate cotton balls – Eye Care
3. In LBW-babies, heat loss is minimized by kangaroo-care and a cap on the head and socks on the feet
4. Baby put on breast and mother supported for Breast feeding
5. Injection Vit. K prophylaxis given
6. Immunizations are given. Zero OPV, Hep B BCG
7. Birth weight measured and documented
Total Score (B2)
B3. Management of asphyxiated new-born
1. Baby received on mother abdomen and wet towel discarded o Observation o Record Review o Provider Interview2. Cord immediately cut and Suction of mouth and nose done
before tactile stimulation & baby put to Preheated warmer
3. Baby positioned for airway maintenance- shoulder roll used, and suction of oral and nasal cavity done
4. If not cried- PPV given in room air with appropriate mask and Self –inflating bag as per NRP algorithm for 15 seconds
5. If HR not improving after effective ventilation of 60 seconds- then start chest compression with PPV in 100% oxygen
6. If not improving, then identified referral facility transportation to be arranged
7. Oxygen saturation maintained between 90-94% (monitored by pulse oximeter)
Total Score (B3)
Maternal & Newborn Health Resource Center38
Summary Table: Case Management practices at New-born Care corner (NBCC) & during labor room visit
summary sCore Case management of nbCC sCore
B1. Infection Prevention Practices
B2. Essential new-born Care
B3. Management of asphyxiated new-born
Average Score= (B1+B2+B3)/3
Main areas of strengths & Good practices
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Main areas where strengthening is required
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
List down the skills demonstrated or taught during the visits
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Key decisions taken in Debriefing Meeting (with CDMO/ ADMO (Med); SNCU / Ped. I/C, O&G Specialist, Hospital manager):
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………………………………………………………
Signature, Mentor Signature, ADMO Signature, In charge
Date: Date: Date:

Maternal & Newborn Health Resource Center39

DISCLAIMER: This document is made possible by the generous support of the American People through the United States Agency for International Development (USAID). The contents are the responsibility of IPE Global Limited and do not necessarily reenact the views of USAID or the United States Government.
IPE Global HouseB-84, Defence Colony, New Delhi - 110024Tel: +91 11 4075 5900 | Fax: +91 11 2433 9534Email: [email protected]
Desi
gn ©
Pea
liDez
ine,
pea
li.du
ttag
upta
@gm
ail.c
om