manju mehta behavioural sciences in medical practice, 2nd edition from simsonians.blogspot.com
TRANSCRIPT

Behavioural Sciences inMedical Practice


Behavioural Sciences inMedical Practice
Second Edition
JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTDNew Delhi • Ahmedabad • Bengaluru • Chennai • Hyderabad • Kochi
Kolkata • Lucknow • Mumbai • Nagpur • St Louis (USA)
®
Manju Mehta MA DM & SP PhD
Professor of Clinical PsychologyDepartment of Psychiatry
All India Institute of Medical Sciences (AIIMS)New Delhi, India

Published by
Jitendar P VijJaypee Brothers Medical Publishers (P) Ltd
Corporate Office4838/24 Ansari Road, Daryaganj, New Delhi - 110 002, India, +91-11-43574357 (30 lines)
Registered OfficeB-3 EMCA House, 23/23B Ansari Road, Daryaganj, New Delhi 110 002, IndiaPhones: +91-11-23272143, +91-11-23272703, +91-11-23282021, +91-11-23245672,Rel: +91-11-32558559 Fax: +91-11-23276490, +91-11-23245683e-mail: [email protected], Website: www.jaypeebrothers.com
Branches• 2/B, Akruti Society, Jodhpur Gam Road Satellite
Ahmedabad 380 015 Phones: +91-79-26926233, Rel: +91-79-32988717Fax: +91-79-26927094 e-mail: [email protected]
• 202 Batavia Chambers, 8 Kumara Krupa Road, Kumara Park EastBengaluru 560 001 Phones: +91-80-22285971, +91-80-22382956, +91-80-22372664Rel: +91-80-32714073, Fax: +91-80-22281761 e-mail: [email protected]
• 282 IIIrd Floor, Khaleel Shirazi Estate, Fountain Plaza, Pantheon RoadChennai 600 008 Phones: +91-44-28193265, +91-44-28194897,Rel: +91-44-32972089 Fax: +91-44-28193231 e-mail: [email protected]
• 4-2-1067/1-3, 1st Floor, Balaji Building, Ramkote Cross RoadHyderabad 500 095 Phones: +91-40-66610020, +91-40-24758498, Rel:+91-40-32940929Fax:+91-40-24758499 e-mail: [email protected]
• No. 41/3098, B & B1, Kuruvi Building, St. Vincent RoadKochi 682 018, Kerala Phones: +91-484-4036109, +91-484-2395739, +91-484-2395740e-mail: [email protected]
• 1-A Indian Mirror Street, Wellington SquareKolkata 700 013 Phones: +91-33-22651926, +91-33-22276404, +91-33-22276415Rel: +91-33-32901926, Fax: +91-33-22656075, e-mail: [email protected]
• Lekhraj Market III, B-2, Sector-4, Faizabad Road, Indira NagarLucknow 226 016 Phones: +91-522-3040553, +91-522-3040554 e-mail: [email protected]
• 106 Amit Industrial Estate, 61 Dr SS Rao Road, Near MGM Hospital, ParelMumbai 400012 Phones: +91-22-24124863, +91-22-24104532, Rel: +91-22-32926896Fax: +91-22-24160828 e-mail: [email protected]
• “KAMALPUSHPA” 38, Reshimbag, Opp. Mohota Science College, Umred RoadNagpur 440 009 (MS) Phone: Rel: +91-712-3245220, Fax: +91-712-2704275 e-mail: [email protected]
USA Office1745, Pheasant Run Drive, Maryland Heights (Missouri), MO 63043, USA, Ph: 001-636-6279734e-mail: [email protected], [email protected]
Behavioural Sciences in Medical Practice© 2009, Jaypee Brothers Medical Publishers
All rights reserved. No part of this publication should be reproduced, stored in a retrieval system, or transmitted in any formor by any means: electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of theauthor and the publisher.
This book has been published in good faith that the material provided by author is original. Every effort is made toensure accuracy of material, but the publisher, printer and author will not be held responsible for any inadvertenterror(s). In case of any dispute, all legal matters to be settled under Delhi jurisdiction only.
First Edition: 1998Second Edition: 2009
ISBN 978-81-8448-629-2
Typeset at JPBMP typesetting unitPrinted at

ToMy parents


Medical practice and medical education, at the end of twenty first century, are being driven byseveral factors. Behavioural Sciences can be considered as one of the most influential of thesefactors. There was a time when medicine was equated with the study of pathophysiology, diagnosisand treatment of diseases. We are now beginning to understand that the diseased individual isa part of the complex human ecosystem, with several levels of organisation ranging from themolecular to psychosocial and culture. Our recognition of the limitations of curative biomedicine
has also opened up alternative strategies such as behavioural and cognitive therapies, which haveenriched the field of medicine.
There has been a paradigm shift in the disease pattern of the society. While the age-old infectiousdiseases and poverty-related illnesses are still haunting us, there has been sudden upsurge inthe lifestyle-related illnesses such as cardiovascular diseases, cancers, trauma and chronic degenerativedisorders, which cannot be tackled by biomedical sciences alone. The trauma of a terminally-
ill patient, the tale of an ill-fated HIV/AIDS positive individual or even a victim of stress in a fastmoving society have their genesis in the behavioural aspects of medicine.
The need for introducing behavioural science components in the curriculum of undergraduatemedical students has been keenly felt but hardly implemented. Many of the committees on medicaleducation and other forums have strongly expressed the need for introducing behavioural sciences.A study conducted by the consortium of medical institutions, adopting inquiry-driven strategies
for innovation in medical education has clearly revealed that the young graduates are deficientin communication and interpersonal skills, and humanistic aspects of medicine. Though the needfor incorporating behavioural sciences has been keenly felt, the attempts to formulate a well-structured programme have been few and sporadic. This is mainly because of dearth of goodtextbooks and resource materials. The present book is an attempt to bridge this void.
The contents of this book have been divided in six parts. The first part is an introduction
to the subject. The second part deals with basis of behaviour, which are core psychological processesthat determine human behaviour. These processes like learning, memory, stress are not onlyrelevant to medical practice, but an understanding of these processes can be of great importanceto the students themselves. Many psychosocial problems are related to the developmental process;thus, the third part of the book is on development of behaviour from birth to death. A specialemphasis is given to adolescence and oldage as these periods are concerned with new emerging
specialities: adolescent psychiatry, medicine and geriatrics. A chapter has been devoted to enhancethe skills of medical students to deal with difficult situations like dying patients, breaking newsof death to the family members and to understand the bereavement process. The fourth partis primarily related to social issues important in patient care, these being the attitudes, family andcompliance behaviour. Qualitative as well as quantitative research in any medical speciality often
Preface

viii Behavioural Sciences in Medical Practice
borrows methods and tools from behavioural sciences; hence fifth part deals with assessmentmethods and various psychological methods of management; the most important of these beingcounselling. A chapter on behavioural medicine has been included, as behavioural methods havebeen integrated in management of certain disorders. The sixth part deals with special applications
of behavioural skills like communication skills, understanding illness behaviour and psychologyof pain.
The overwhelming response to the first edition of this book has encouraged me to work forthe second edition, which brings additions in some chapters. I hope these additions would behelpful for the students. Behavioural Sciences need human dimensions, thus an attempt has beenmade to explain the concepts and theories in simple manner. Real case studies with fictitious
names have been given in the beginning of each chapter, and clinical applications are discussedto make the students comprehend, relate and use this information in their practical work. It wasnot feasible to include some other important aspects of health care like economics, ethics, etc.simply to keep the volume of information at a readable level. Again, not much emphasis hasbeen given on latest research finding as the objective of this book is to help the students understandthe relevance of behavioural sciences to medicine.
It is impossible to acknowledge all the sources of inspiration and information that I used whilewriting this book. But first of all, I must thank my patients, whom I have met over the last threedecades; the experiences I have gained from them have helped me understand the clinical applicationsof behavioural sciences. I am also grateful to Professor NN Wig, former Regional Director, WHO,for stimulating my achievement motivation. I am greatly indebted to Mrs Roxana Samuel, MsRenuka Dutta, Ms Anubha Dhal and my students for the help provided to me, with their valuable
suggestions and the editing of this book.Mrs Nani Gangadharan has painstakingly typed and retyped manuscript of this book, and
she deserves my whole-hearted gratitude. I also appreciate the enthusiasm of Sameer and Aditiin making graphic illustrations on computer.
Last but not the least, this work would not have been possible without the patience, supportand encouragement that I received from my husband, Dr Anil Mehta and other members of
my family.
Manju Mehta

PART 1: Introduction
1. Behavioural Sciences ................................................................................................. 1
PART 2: Basis of Behaviour
2. Sensory Processes and Perception ............................................................................ 7
3. Attention ................................................................................................................... 19
4. Memory... .................................................................................................................. 24
5. Learning and Studying ............................................................................................ 35
6. Intelligence ................................................................................................................ 48
7. Thinking ................................................................................................................... 58
8. Motivation ................................................................................................................ 67
9. Emotion .................................................................................................................... 77
10. Stress and Coping .................................................................................................... 88
11. Personality .............................................................................................................. 100
PART 3: Development of Behaviour
12. Development—Infancy to Adolescence .................................................................. 111
13. Adulthood to Ageing .............................................................................................. 124
14. Dealing with Death and Bereavement .................................................................. 132
PART 4: Social Behaviour
15. Attitudes ................................................................................................................. 138
16. Family ..................................................................................................................... 146
17. Compliance with Health Care ............................................................................... 155
Contents

x Behavioural Sciences in Medical Practice
PART 5: Assessment and Management
18. Assessment in Behavioural Sciences ..................................................................... 161
19. Counselling ............................................................................................................. 177
20. Behaviour Therapy ................................................................................................ 185
21. Cognitive Behaviour Therapy ................................................................................ 196
22. Behaviour Medicine ............................................................................................... 206
PART 6: Applications of Behavioural Sciences to Health
23. Communication Skills ............................................................................................ 212
24. Illness Behaviour .................................................................................................... 222
25. Psychology of Pain ................................................................................................. 229
Bibliography ........................................................................................................... 243
Index ....................................................................................................................... 253

While taking ward rounds you examine Mr Raged fifty-five years on bed no. 5, and Mr Saged forty-eight years on bed no. 6, both thepatients have similar symptoms and have beendiagnosed as carcinoma of lungs. From physicalpoint of view you have knowledge of humananatomy, physiology, and learning of pharmaco-logy helps you to prescribe medicines. Yet youfind that both the patients are reacting to illnessand responding to the medical treatmentdifferently. How do you explain thesedifferences? Mr S is restless, gets irritated easily,is always complaining of other staff working inthe ward. On the other hand Mr R is accommo-dating and is grateful for whatsoever care is givento him. They are not only patients of bed no.5 and bed no. 6, but are two human beingswith their unique personalities, abilities to copewith stress and varied family responsibilities.These differences in behaviour are due to one’sown personality and reactions to illness. It is notsufficient to have knowledge about the biologicaland organic aspects of the disease only, it isimportant to understand the person having thedisease and his psychosocial background.
Definition
The branch of science, which can help you inunderstanding your patients as unique
individuals, is known as Behavioural Sciences.This term has been used to denote the studyof human behaviour both of the individual andof groups of people, small or large. It emphasiseson individual behaviour and on the applicationof such basic knowledge to medical and allieddisciplines.
Thus behavioural sciences have become partof the undergraduate medical education all overthe world. Though this course is fairly well-established in many developed countries, it isincluded in some medical schools in India also.The Indian Medical Council has recommendedits inclusion in all the undergraduate medicalschools. Behavioural Sciences draws uponvarious disciplines and sciences related to thestudy of human behaviour like: psychology,sociology, anthropology, economics and statistics(Fig. 1.1). Psychology is the study of humanindividual behaviour. Sociology is more aboutsocial and group behaviours. Anthropology dealswith culture and natural history of mankind ofdifferent races and their development. Econo-mics has to do with the distribution of scarceresources within a society. The statistics helps intesting hypotheses and measurement. Thetreatment to all these branches cannot be givenat par in this book more concentration is givenon the understanding of the individual patient.
1BehaviouralSciences
PART 1: Introduction

2 Behavioural Sciences in Medical Practice
Need for Behavioural Sciences
The aim of this book is to help the students todevelop an understanding of human behaviour,and its relationship with medical practice. Theunderstanding of conceptual and methodo-logical basis is required for subsequent clinicalinstructions. An understanding of human beha-viour is desirable in most branches of clinicalpractice; it is especially important in medicine,psychiatry, community medicine, pediatrics andgeriatrics. There are ample examples to illustratethe need for the disciplines of behaviouralsciences (which mainly consists of psychologyand sociology) to provide a systematic academicfoundation in the preclinical period for theseclinical subjects.
Developments in medical education havecome about mainly as a response to scientificand technological advances made in the fieldof medicine. There is a growing danger that thestudent may become so preoccupied with theminutiae of the specialities and with the techno-logies of the laboratory that he loses sight of thepatient as a “whole person”, functioning in asocial context. Moreover little attention is paidto changes in community patterns of disease orto changes in the social functions of medicine.
This has led some medical educators to searchfor a counter-balancing element to build intothe medical curriculum. It seems that behaviouralsciences can provide this element. They can havea significant effect on the outlook and attitudesof medical students, both through their subjectmatter (human behaviour and social processes)and through their central premise that theproblems they deal with are susceptible toscientific investigation and explanation.
Behavioural Sciences can be of more directmedical relevance also. In medical practice thedoctor’s main concern is individual patient. Oftenone encounters differences in response to pain,illness, hospitalisation, and other stresses; theinfluence of personality and social class on illness.Patient’s personalities and relationships may beimportant factors in the disease process and inmedical care. A doctor also needs tocommunicate effectively with patients, theirrelatives, with colleagues-doctors, and nurses.He faces resistance to attitude and behaviourchange in the context of preventive medicine—these are a few examples of everyday problemsof medical care, which require the doctor to formjudgement and make decisions based on anunderstanding of human behaviour andinstitutions. Biological training alone does notprepare a doctor to deal with such situations.
Furthermore, psychological knowledge canbe valuable in developing the effectiveness ofthe student’s and doctor’s own cognitiveprocesses. Clinical practice involves complexroutines of observations, discrimination, andinterpretation, acquiring and retaining factualinformation, of problem-solving and decision-making. There is an extensive body of psycho-logical knowledge concerning these processesand the variables which influence them (e.g. theeffects of fatigue, attitudes, and expectancy onaccuracy of perception and recall); and it isbelieved that students can profit from awarenessof these problems and of the principlesunderlying them.
Fig. 1.1: Subject content in behavioural sciences

Behavioural Sciences 3
Culture as Determinant of Health
Culture is shared learned behaviour that istransmitted from one generation to another forpurposes of human adjustment, adaptation, andgrowth. Culture has both external and internalreferents. External referents include roles andinstitutions. Internal referents include attitudes,values, beliefs, expectations, and consciousness.
Culture is something that mediates andshapes virtually all aspects of human behaviour.It is the way in which human beings define andexperience reality. It includes their sense ofmorality and personhood. These dimensions ofhuman behaviour are not inborn but rather areshaped by the socialisation process. An ethnocultural group’s language and its religion,economic, political, and social systems areinstitutional reflections of culture and help toshape the internal referents as part of a reciprocalor interdependent system.
As children are reared, they are conditioneddirectly and indirectly to think, feel, and act incertain ways. These ways constitute their reality.Their language helps to shape reality and is alsoin turn shaped by it. Culture is a criticaldeterminant of human behaviour, to the extentthat culture varies, human behaviour must alsovary. Compare the two adolescent males grownup in two different places like one in North Indiaand the second in down South, you would findthat their differences in the appearance, food,dress, and rituals also produce differences in theway they think and define reality. The individualis the representative product of biological,psychological, social and cultural determinants.Figure 1.2 presents this conceptualisation ofhuman behaviour.
The illness behaviour is also influenced bythe cultural determinants, e.g. in many culturesmales are not likely to cry or express pain orsuffering, during an illness. If you are not awareof these determinants, then probably yourassessment of that patient’s pain and sufferingwill be biased.
Scope of Behavioural Sciences
Training in the behavioural sciences is essentialfor the appropriate education of physicians asmajor health problems of today can lead topremature death or disability. Cardiovasculardisease, substance abuse, AIDS, cancer, andadolescent pregnancy are directly caused by risk-taking behaviour and can be prevented bypeople only by modifying their lifestyle andbehaviour. Many diseases require majormodifications of lifestyle to ensure benefits oftherapy. The primary purpose of teachingbehavioural science in medical schools is toprepare physicians to understand the role ofsocial and psychological factors in the aetiologyand course of disease. The knowledge can beapplied to reduce the burden of disease bychanging the patient’s behaviour. Some othercauses of illness stem from sociocultural forces,such as poverty, low socioeconomic status, andindustrialisation. These factors are very commonin developing countries, though they lie beyondthe realm of the individual doctor-patientrelationship; yet understanding these factors canhelp physicians plan appropriate medical servicesand preventive efforts.
The scope of behavioural sciences isenvisaged in the following areas of medicine.
The Doctor-Patient Relationship
The clinical knowledge base now includes alarge amount of research on doctor-patient
Fig. 1.2: Determinants of behaviour

4 Behavioural Sciences in Medical Practice
relationships which has been demonstrated tobe important to patient care outcomes. It includesinformation about the understanding ofintimacy-relations of trust and power betweendoctors and patients, and how interpersonalinfluence works in doctor-patient transactions.
Effective interviewing techniques are amongthe most essential skills that all physicians needto learn. Many studies have demonstrated thatphysicians who fail to obtain accurate informa-tion may misdiagnoses or recommend inap-propriate therapies. Examples of successfuloutcomes due to skillful inquiry provide usefulstimulus for students to learn behaviouralsciences.
Social Class and Health Behaviour
Social class is broadly associated with almostevery indicator of morbidity, disability andmortality. Factors associated with lower socialclass increase susceptibility to illness and injury.Understanding specific risks and vulnerabilitiesassociated with social status provides physiciansopportunities for more effective communicationand therapy, and for preventive initiatives.
Several investigators have demonstrated thatdisadvantaged social environments increase therisk of serious health problems especially inchildren and adolescents. One of the examplesis the low birth weight child when reared indisadvantaged environment, has an increasedprevalence of acute and chronic illness for aslong as eleven years after birth.
Physicians often underestimate the extent towhich the patients of lower socioeconomic statusdesire information. Such patients are often lessexpressive and less questioning than the bettereducated patients and physicians commonly givethem less treatment relevant information.
Human Development: Life Cycle,Health and Illness
Physicians need to understand how life expe-riences at one stage of development influence
later behaviour, susceptibility to illness, and useof medical services. Previous life experiences alsomodify physiologic and immunologic responses.Longitudinal studies of life span in humans haveilluminated the cause-and effect relationships ofearly nutrition to later heart disease and the effectof early life stress on later immunologic response.
Psychophysical Relations
This is one of the most rapidly advancing fieldsis in the mind-body relationship. Parents witha child who is dying from leukaemia havemarkedly different cortisol and T-lymphocyteresponses, depending on whether they cangrieve openly or not. Those who cannot grievehave greater elevation of cortisol and more illnessin the year after the death of a child than thosewho can.
Data from primate laboratories have demo-nstrated that about twenty per cent of monkeysare shy and withdrawn from birth, and if lefton their own, grow up to have low status in thegroup. These studies not only demonstrate thebiological basis of such behaviour but thepossibilities of modification by early experience.
Children who are taught self-imaging (i.e.self-hypnosis) respond with greater secretory IgAin their pharynges than those who are not, andself-imaging has been shown to be as effectivein treatment of migraine headaches in childrenas standard pharmacologic treatments.
There are marked individual differences incortisol and neuroimmunologic response to stressfrom early life. Physicians need to recognise themind-body relationship, which has beenextensively documented. Physical disease causebehavioural changes. Psychological stresses causephysical changes.
Health and Illness Behaviour
Differences in behaviour account for much ofthe variation in the health of different popu-lations. These include not only personal healthbehaviours such as smoking, diet, substance

Behavioural Sciences 5
abuse and exercise but also exposure toenvironmental risks and interpersonal, work-related and community-related stresses. Risks tohealth are often inadvertent consequences ofpersonal choices and routine activities. Under-standing these risks and developing strategicapproaches for intervention enhance physician’sopportunities to assist their patients in leadinghealthier lives controlling many extremelyserious risks to health and to life itself such asHIV infection depends exclusively on successfulmodification behaviour and exposure to risk.
The Impact of Social Support
Many studies show that the presence of socialsupport, the quality of social networks, and thedegree of participation in them have substantialeffects on coping health status, and longevity.
The Importance of Self Efficacy
A large literature now attests to the importanceof self efficacy in supporting social adaptationand health. The deterioration of frail elderlypersons who move to new environments is oftenlinked to their sense of loss of control. Haggertyet al (1993) have quoted experiments carriedout in nursing homes, which show that increa-sing the elderly person’s sense of control resultsin enhancement of health. Similar finding havebeen reported on patients with chronic pain, thatexperience of pain is less in patients who thinkcontrolling power is with the person himself (seeChapter 25). While there is still much to belearned, several areas of research converge indemonstrating the importance of a person’ssense of control over his or her immediateenvironment.
The Hole of Self-Attentionon Symptom Amplification
Numerous lines of investigation show howfocussed attention on physical states amplify the
intensity of experience and concern about healthstatus (see Chapter 3). Understanding of thiswork has relevance for pain management andfor understanding symptom prevention andresponse.
The Illness-Disability Perception
Disability caused by the illness depends on arange of factors that intervene between theoccurrence of illness and disability. These factorsinclude personal variables such as attitudes andmotivation; aspects of the social context, suchas opportunities for participation, stigma, andphysical accessibility; and the health workers’management of the initial condition over itslongitudinal course. The understanding of thesefactors is crucial in the appropriate care ofpersons with physical impairments, the elderly,and individuals with chronic disease.
Adult Sexuality, Loss, Grief, Mourning, Aging,and Death These issues are concernedprimarily with the interaction of psychologic andsociologic aspects of individual behaviour andneed few specific examples to demonstrate theirimportance. Behavioural science seeks tounderstand the social organisation of thecommunities in which patients live, theinstitutions involved in the provision of medicalcare, and their influence on health.
Selye described the general adaptationsyndrome and developed the general conceptof stress and the neuroendocrine mechanismsinvolved, particularly the role of catecholaminesand the steroids. Since that time, steady progresshas been made toward working out step-by-stepthe biological mechanisms involved, wherebystress can lead to cardiovascular changes thatcause heart attacks and stroke or have profoundeffects on the immune system for example, westill have a long way to go in learning the detailsof these mechanisms, but we know enoughalready to begin to see how behaviours suchas smoking and high fat/high calorie diets, for

6 Behavioural Sciences in Medical Practice
example, affect these same mechanisms andexacerbate them and how exercise canameliorate them. We also know that behaviouralchange leading to prenatal care, good nutrition,and immunisation will make the difference inimproving our infant mortality rates. Further-more, violence, teenage high-risk behaviours,and suicide are major cause of mortality andmorbidity. Finally, we know that adherence tomedication, especially in the adult and theelderly, remains a major problem in managingchronic diseases.
With chronic diseases such a major portionof modern medicine and so dependent onlifestyles, behaviour modification and copingstrategies, health-promoting and disease-preventing behaviours become of greatimportance in the practice of medicine not onlyfor their value in cost containment but also forthe general welfare of our society.
SUMMARYBehavioural sciences is the branch of sciencewhich can help you in understanding yourpatients as unique individuals. This term has beenused to denote the study of human behaviourboth of the individual and of groups of people,small or large. It emphasises on individualbehaviour and on the application of such basicknowledge to medical and allied disciplines.Behavioural sciences draws upon variousdisciplines and sciences related to the study ofhuman behaviour like psychology, sociology,anthropology, economics, and statistics.
An understanding of human behaviour isdesirable in most branches of clinical practice,especially in medicine, psychiatry, communitymedicine, paediatrics and geriatrics. Behaviouralsciences are of direct medical relevance, as inmedical practice the doctor’s main concern isindividual patient. To understand variations inresponse to pain, illness, hospitalisation, andother stresses; the influence of personality andsocial class on illness, knowledge of normal rangeof behaviour should be known. Patientspersonalities and relationships may be impor-tant factors in the disease process and inmedical care. A doctor also needs to developcommunication skills to deal effectively withpatients, their relatives, with colleagues-doctors,and nurses.
Psychological knowledge can be valuable indeveloping the effectiveness of the one’s owncognitive processes. Clinical practice involvescomplex routines of observations, discrimination,and interpretation, acquiring and retaining factualinformation, of problem-solving and decision-making.
Culture shapes not only the normal beha-viour but it also influences illness behaviour. Thusthe patient’s behaviour and his symptoms shouldbe understood in their cultural context.
Thus the scope of behavioural sciences rangesfrom doctor-patient relationship to variousaspects of health care such as, social class andhealth behaviour, developmental life cycle,psychophysical relations, social support, selfefficacy, aging and bereavement.

2Sensory Processesand Perception
PART 2: Basis of Behaviour
Ranjeet, a young man comes to you with severeanxiety, Ranjeet is a music teacher in a privateschool, he is blind due to congenital defect, andhe is married but does not have children. Hiswife has normal vision, but she is not educated.The anxiety was precipitated after a neighboursuddenly passed away following cardiac arrest.The incident has caused concern and fear inRanjeet’s mind that being blind, how can hehandle such a situation if the need be. Anysensory defect can have negative psychologicalimpact on the individual’s personality andadjustment.
We live in a world of objects and peoples—a world that constantly bombards our senses withstimuli, bringing us information and presentingus with decisions, first on how we’ll perceive thesestimuli and then on how we’ll behave in response.The sensory organs—vision, hearing, smell,touch and taste are highly complex systems andthey do not make a straightforward responseto each stimulus encountered. The knowledgecomes to each one of us through our senses.We know about the world around us from whatwe learn directly about it, using our bodilysensations. We can understand the external worldonly from what our senses can detect of it.
Therefore, sensation becomes the primarysource of all human knowledge. In human beingunlike simple organism, sensation is only a smallpart of much more complicated informationprocessing systems.
Let us define some terms here. A stimulusis any form of energy to which we can respond(light waves, sound waves, and pressure on theskin). A sense is a particular physiologicalpathway for responding to a specific kind ofenergy. Sensation is the feeling we have inresponse to information that comes in throughour sensory organs. Perception is the way ourbrain organises these feelings to make sense outof them. This involves recognition of objects thatcomes from a combination of sensations and thememory of previous sensory experiences.
SENSATION
Sensations contain both a ‘quantity’ element(size, hardness, coldness), and a ‘quality’ element(attractive, bad or dangerous). For example if youget burnt from a hot pressure cooker, you maythink of all pressure cookers as being dangerousequipment. The physical property of heat maytherefore, take on the psychological propertyof dangerousness. Thus the physical and

8 Behavioural Sciences in Medical Practice
physiological events are collectively called‘sensation’. That is the way in which the bodyresponds to energy impinging upon it from theenvironment.
PERCEPTION
Sensation refers to the process of receivinginformation, whereas to perceive means tointerpret and understand. Perceiving is not seeing,believing. Perception refers to what is immediatelyexperienced by a person. Sensory events aretranslated into patterns of activity in the sensorychannels and the central nervous system. Someof what we perceive is very closely linked to theseactivity patterns. Perception is the process ofknowing the world outside you, by forming somemental representation. Perception is a complexprocess, extending far beyond the mereregistering of light, sound, and other impulsesfrom the external world. This external informationmust be internally coded and transformed beforeanyone can know what is really out there. Oftenyour beliefs and expectations about someexternal stimulus prove to be more important indetermining your behaviour than the physicalcharacteristics of that external object. Perceptionis like solving a complicated puzzle. You musttake bits and pieces of information that arepresent in the external world and fit them togethersomehow to form a comprehensive internalpicture.
It may at first appear that every object in theexternal world makes direct contact with the brainvia the sense organs: the eyes, ears, skin, andso on. But this view of perception is much toosimple. There is no direct one-to-one relationshipbetween the image formed by your eye and yourperception of that image. The situation is indeedeven more complex, since many physicalarrangements in the external world can produceexactly the same image upon the eye. Forexample, it follows from elementary principlesof geometry that a small triangle near you will
produce the same image in the eye as that ofa large triangle further away. Since any singleexternal cue is likely to prove insufficient tonarrow down the possibilities about the externalworld, we are forced to rely upon variouscombinations of cues. Although each cue by itselfmay be unreliable, if we consider enough cuestogether, we can often come up with an accuratemental picture of the external situation.
However, for much of what we perceive, thesensory patterns merely provide the ‘raw data’for experience. The sensory information is trans-formed elaborated and combined with memoriesto create what we actually experience or perceive.
Perceptual Processes
We do not perceive world as loud sounds, brightlights or patches of colours. We perceive the worldaround us as objects like, book, glass, and plants.We hear doorbell, footsteps and songs. Thatmeans the sensory inputs at the focus of ourattention have form and meaning. Perceptualprocesses which provide meaning to what we seeor hear are classified as—form, visual depth,constancy, movement perception, plasticity andindividual differences. We shall very brieflyexamine these processes.
Form Perception
The sensory inputs we receive come into ourawareness as shapes, pattern and form. The basicelement needed for visual form perception is thepresence of contour. A contour is an area withinthe visual array where there is an abrupt changein luminance. The normal optic array is filled withcontour information and an area completelyenclosed by a contour is usually seen as distinctand separate form.
Another fundamental process in form per-ception is the recognition of a figure on a ground.We see objects as standing against a background.The words on this book are figures against thebackground of the page. We must be able to

Sensory Processes and Perception 9
differentiate between the figure and these back-grounds, from which they are emerging. But ina reversible figure ground stimulus; perceptionof figures is a psychological act of interpretationsand not necessarily, directly predictable from thestimulus array. Reversible figure groundrelationship illustrates the multistability ofperceptual organisation, i.e. some stimulus inputscan be organised differently in perception.
Organisation in perception partially explainsour perception of complex patterns as unitaryforms or objects. We see objects as objects onlybecause grouping process operate in perception.Some laws of organisation are:1. Law of proximity—items close together in
space or time tend to be perceived asbelonging together.
2. Similarity—similar objects tend to be groupedtogether.
3. Symmetry—there is a tendency to organisethings to make a balanced or symmetricalfigure that includes all the parts.
4. Continuation—there is a tendency to perceivea time that starts in one way as continuingin the same way.
5. Common fate—elements, which are per-ceived as moving together from an organisedgroup.
6. Law of closure—refers to perceptual processsees, which organize the perceived world byfilling gaps in stimulation.
Depth Perception
Artists, philosophers, and psychologists have longbeen challenged by the everyday fact of 3Dseeing. The problem is set by the very structureof eye, which forms an optical image on a 2-dimensional surface, the retina. We make use ofinformation, or cues in the sensory input togenerate the 3D perception. The depth cues, werefirst studied by artist Leonardo da Vinci (1452-1519) to keep artists portray depth and distanceon a flat canvas. We use monocular andbinocular cues to create such effect.
Monocular cues: These operate when only oneeye is looking. The artist to give us depthexperience from a flat painting generally usesthese. The depth perception is created by-Linearperspective (the distances operating the images),clearness, interposition (one object obstructs viewof another), shadows, gradients of texture(change without abrupt transition) and move-ment.
Binocular cues: Many of the cues for depthperception require only one eye. Individuals withvision in one eye have adequate depth perceptionin most conditions. When we observe with two-eye vision, at the world we add binocular cuesto the depth perception to the monocular cues.As the two eyes receive slightly different view ofthe world thereby producing binocular cues.
Nonvisual cues of depth and distance: There aretwo possible cues to the perception of depthnamely convergence and accommodation. Theconception was that subject adjusted thisaccommodation and convergence until he hada sharp and single image of the object.
Visual Pattern Perception
When we consider all the processes that underliethe recognition of complex, everyday pattern, wefind they can be classified in two ways:1. Data-driven processing—begins with the
arrival of sensory information reaching thereceptors (data). This input is said to drivea series of analyses, beginning with regis-tration of luminance differences in image,colours, lines, angles, etc. This analysisproceeds from retina up through various levelsof visual pathways, until it reaches highercentres of brain.
2. The other type is called “conceptually-drivenprocessing—it uses higher level conceptualprocesses including memories of pastexperiences; general organisational strategies;knowledge of world and expectations basedupon surrounding context or situation. Both

10 Behavioural Sciences in Medical Practice
type of analyses can be occurring simul-taneously, or they may occur one after theothers.
Constancy of perception: Our perceptualexperiences are not isolated; they build a worldof identifiable things. This world as we perceiveis a stable world. An object that has beenconstituted perceptually as a permanent andstable thing is perceived as such regardless of theillumination on it; the position from which it isviewed; or the distance at which it appears. Thisstability of environment as we experience istermed as ‘perceptual constancy’.
Size constancy refers to the fact that as anobject is moved further away we, tend to correctit for distance and still see it as more or less normalin size, when we, see an object at a distance,we might judge its size in one of the 3 ways:1. Perspective size: According to the geometry
of perspective, i.e. size inversely proportionalto distance. This size would correspond to sizeof image on retina.
2. Object size: If object constancy is perfect wemight judge an object by its known size.
3. Compromise between perspective size andobject size: It might compromise and see theobjects smaller at a distance, but not as muchsmaller as geometry of perspective indicates.Size constancy develops largely as the result
of experience. Similarly, the tendency to see anobject, as of standard shape regardless of theviewing angle is shape constancy. The tendencyto see an object as of normal colour regardlessof light and shadow is called ‘colour constancy’and brightness respectively, finally, the fact thatobjects retain their same positions, even as wemove about is known as ‘location constancy’.Although the word constancy is an exaggeration,but it dramatises our relatively stable perceptionof objects.
Movement Perception
When we perceive movement, we sense actionin space taking place over time. We usually
explain the perception of movement accordingto the stimulation of successive parts of sensorysurface. Adaptive behaviour requires that weperceive movement accurately; otherwise onewould land up in the hospital following anaccident. Perceived motion also occurs withoutany energy movement across the receptor surfaceor without a successive pattern of stimulation,and is called apparent motion. In contrast to thisthere is real motion, the perception of the actualphysical movement of the objects.
Apparent motion It is movement perceived inthe absence of physical movement of an imageacross the retina. This is caused by the followingfactors:a. Autokinetic effect—if we stare at a single spot
of light in a completely dark room, after afew seconds light will appear to move in anerratic manner. This apparent movement ofstationary light is called Autokinetic effect.
b. Stroboscopic motion—This illusion of motionis created, when separated stimuli, not inmotion are presented in succession. Thismotion is used in making of cartoon films.Each frame of a film is slightly different fromthe preceding one, but when frames arepresented rapidly enough, the picture blendsinto a smooth motion. A simple form ofstroboscopic motion is called “Phi-Phenomenon”, according to this, in a darkroom if these are four lights and one of thesefour lights blinks on and off, followed shortlyby another, there is an illusion of a single lightmoving from first position to the second.When all four lights flash on and off in a rapidsequence, it appears that single light istravelling in a circle, but the perceived sizeof the circle is smaller; than would be the caseif lights were actually rotating.
Real motion: The perception of real motiondepends upon relations between objects withinthe visual field. Whenever there is movement,the brain has to decide what is moving and whatis stationary with respect to some frame of

Sensory Processes and Perception 11
reference. We generally tend to assume that largeobjects are stationary and, smaller objects aremoving. “Induced movement” is experiencedwhen we look at the moon through a thin coverof moving clouds. In a clear sky, the moonappears to be stationary. When framed bymoving clouds the moon will appear to raceacross the sky, while clouds appear stationary.
Plasticity: Visual deprivation or plasticity isrestriction of the visual output. This is generallycaused during the development stage in earlyinfancy. Individuals born with congenital cataractface this type of problem.
Individual differences: Individuals differ in theways they process sensory inputs to give rise towhat they experience. Two individuals watchingsunset in the western coast beach may have verydifferent perceptions of the sunset. One mayreport it was breath taking or pure magic, whereasthe other may report a red circle graduallydescending. These differences in the perceptionare the result of the following factors.
Perceptual learning: Eleanor Gibson (1969) hasdefined perceptual learning as “increase in theability to extract information from the environ-ment as a result of experience or practice withthe stimulation coming from it”. This learninginfluences behaviours and experiences; and alsodetermines the focus of attention. There aremany examples to show that learning can mouldperception. The one common example that wecommonly encounter is the competence ofindividuals trained in various professions, ascompared to untrained individuals. Skills in anyvariety are result of perceptual learning, whichis achieved only through practice. Another veryrelevant example of perceptual learning is thatblind persons learn to extract information fromthe environment, which generally the sightedpeople can not do, e.g. very sensitive discrimina-tion of auditory sounds.
Related with learning one often wonderswhether the perception is inborn or is influenced
by the environmental factor. Those who advocatenature’s role, say that brain organisation isdetermined by genetic codes and is so innate.The perception that depends upon this organi-sation is thus also innate. They say that sensorydeprivation or special sensory experience duringcritical period results in a loss of brain connectionsthat were genetically determined, because theyneeded environmental input, or nurture, for theirmaintenance. On the other hand, supporters ofenvironment, argue that while genetic codes mayprovide a rough blueprint nurture interacts withthe genetic outline during critical periods to directgrowth and cause the proper brain connectionsto be made, so according to them alterationsin the environment during critical period actuallychange the way the brain grows and theconnections are made.
Perceptual set: We frequently perceive an eventor object because we were mentally preparedfor a particular object or event to arise. Set refersto the idea that we are ready to receive certainkinds of sensory input. Such set or expectanciesvary from individual-to-individual. Imagine thetime when you were expecting your result foradmission to a medical college, you will be ableto recollect that you were able to spot the resultin the newspaper in no time whereas yourfriends who were not expecting did not evenlook at this news. Perceptual sets are related tothe actual physical environment of the stimulusitself or to the internal factors, such as emotionor motivation.
Motives and needs: Several experiments havebeen conducted to study the effect of need andmotive on perception. We attend to and organisesensory inputs in ways that match our needs.When you are hungry or thirsty, you are likelyto pay more attention to places that would satisfyyour need.
Illusions: Visual illusions are a dramatic exampleof how perceptual cues can be assembledincorrectly. Many illusions do not support the

12 Behavioural Sciences in Medical Practice
traditional view of perception that we infer fromwhat we see. An illusion is any figure that givesrise to a bizarre interpretation of reality. Theillusions demonstrate that what we perceive oftendepends on processes that go far beyond the ‘rawdata’ of sensory input. Illusions show thatperception results from transformation,elaboration and combination of sensory inputs.Specific instances in which the apparent curvatureor length of a perceived line are not predictablefrom the curvature or length of its stimuluspattern, have been called the “Geometricalillusions”. But this does not mean that they occuronly with regular lines and patterns; they can alsobe demonstrated with quite irregular drawingsand with real objects in normal environment. Theillusions are important because they may provideclues for our understanding of processes of shapeperception.
We shall examine some illusions that havea direct basis in our perception of ordinary objectsand scenes. In these cases it may be that oursenses have become so used to interpreting aparticular stimulus in a given way that they cannotreadily be dispensed with the ‘stereo type’. Thefamous Muller-Lyer illusion (Fig. 2.1) shows thatpeople usually perceive the vertical lines ofdifferent lengths. In reality both the vertical lines
Fig. 2.1: Which of the lines is longer?The Muller-Lyer illusion
Fig. 2.2: Measure the space between the twosets of arrowheads at their point
are equal in length. This illusion arises becauseof the architectural perspective implied in thesetwo arrangements of lines.
However, Figure 2.2 shows, even when thevertical lines are removed from the figure theillusion still persists; the inward pointingarrowheads still seem to be further separatedat the point than are those in the outwardpointing version. The reason for this illusion isthat even in normal circumstances we do notutilise all the available information when weperceive objects.
Same illusion is evoked even when arrowsare replaced by circles (Fig. 2.3). In this presenceof the circles now generate the illusion of oneline being longer than the other.
Fig. 2.3: Which of the straight lines is longer
Lines that converge suggest an appearanceof distance. The common example of this is astretch of long road or railroad tracks that remainparallel and equally wide as they disappear intothe distance (Fig. 2.4). The Ponzo illusion alsooccurs due to the converging lines suggest depth(Fig. 2.5).
Illusions make clear that the context in whicha given stimulus appears will determine how it

Sensory Processes and Perception 13
is perceived. Figure 2.6 demonstrates theimportance of context in determining perceptionthat we cannot ignore. In spite of our knowingthat we do not perceive accurately, still we areunable to prevent the false interpretation arisingout of these figures. These illusions show that ourperception is independent of our conscious will.Information reaching us in normal circumstancesmay frequently contain inaccuracies imposed bythese unconscious processes even though weare unaware of it happening.
At times the illusions can have serious effects.The Poggendorf Illusion can cause serious tragedylike, crashing aeroplanes, or misguiding thesurgeons while operating. This is the simple
illusion, which occurs when there are two parallellines and a third line intersects them (Fig. 2.7).As you can see that the diagonal lines do notappear to intersect, though in reality they areextensions of the same line. The Poggendorfillusion can be explained by a combination ofphysical and cognitive factors. These factors arecalled structural effects and processing strategies.The structural effect depends upon the biologicaland optical construction of the eye. The process-ing strategy depends upon the cognitive decisionsthat are shaped by learning, experience andmotivation.
Perception as Developmental Process
Is perception a developmental process? Like anyother psychological processes, perception is alsodifferent in children as compared to the adults.
Fig. 2.4: Converging railroad
Fig. 2.5: Ponzo illusion
Fig. 2.6: Perceive these circles. The context of thecircles that surround the centre circles influences ourperception
Fig. 2.7: The Poggendorf illusion

14 Behavioural Sciences in Medical Practice
Moreover, throughout the life span of anindividual some changes occur in the perceptualprocesses. Basic perceptual functions in childrenmay continue to mature during first year due tothe actual normal functioning of the visual system.At behavioural level, we can find some responsesin newborns to the direction, distance ormovement of stimuli. Infants are capable ofdirecting their age movements toward targets.Neonates tend to make convergent and divergenteye movements. Even repetitive eye movementsequence in the presence of a moving patterncalled optikinetic nystagmus, is seen. But visualacuity of neonates is quite poor. Infants candiscriminate between patterns. Fontz (1963)found that infants younger than one month,repor ted a looking preference for stimulicontaining facial features; but could notdifferentiate between normal and a scrambledface. This suggests they are discriminatingpatterns on basis of simple elements rather thanon the basis of total stimulus organisation. How-ever, by 4 months, there is definite preferencefor unscrambled face; indicating they can identifyhuman face. Process of habituation can be seenfrom the very first days of life. So, the newbornchild does have a reasonable set of perceptualcapacities, quite soon after the birth.
One of the most informative ways to monitorchanges in perceptual discrimination, recognitionand information processing is to observe the wayin which child selects information from externalstimuli. By monitoring eye movement patternsin children we can determine the manner inwhich they are viewing and hence constructing.As child becomes older there is gradualmovement toward a consideration of more globalaspects of a pattern and its elements. Olderchildren are more efficient at extracting details.But there is one form of pattern discriminationerror, which is characteristic of young children.This involves mirror reversals (common around3 year and gradually decrease, until child is about10 or 11 years). Letter reversals, in children
suggest that a child is relatively insensitive toorientation of a stimulus.
Perceptual change in adults involve basicsensory function especially like dark adaptationwhich tend to diminish with age, response tomore complex visual problems becomes better,or more accurate with age.
As we grow older, there seems to be gradualdecrease in efficiency of sensory structures. Thisis, however accompanied by gradual improve-ment in our abilities to perform complex,perceptual integrations and discriminations.
Extrasensory Perception (ESP)
You would have heard that some persons havereported correctly about their previous birth, orcan predict about some event which is about tooccur in very near future, like some accident isto take place or such a person sitting 500 kmswould be doing a particular task. Theseextraordinary types of perceptions require nosense organ stimulation whatsoever. Though,ESP is a controversial issue, yet some researchhas been carried out even in India. ESP stimulatesalso called as parapsychological phenomenon isof two main kinds—1. ESP
a. Telepathy or thought transference fromone person to another.
b. Clairvoyance or, perception of objects orevents not influencing the senses (e.g.telling the details of the contents sealedin an envelope.
2. Psychokinesis (PK) or mentally manipulatingobjects without touching them.There is skepticism about ESP, one of the
chief reasons being that no method has beenformed for reliably demonstrating the pheno-mena. Also, the results do not vary systematicallywith the introduction of different experimentalmanipulation. But still, it is desirable to keep anopen mind about issues that permit empiricaldemonstration, as some ESP phenomena do.

Sensory Processes and Perception 15
Social Perception
We meet someone for the first time and talk withor observe him or her for a few minutes. Evenin this short space of time we make judgementsabout a number of characteristics. Socialperception is concerned with our interpretationof behaviour in social settings and generally refersto how we perceive others, favourably orunfavourably. Social perception is of greatrelevance to medical profession. How the patientperceives the physician determines his trust forphysician’s healing power. Similarly physician’sperception of the patient, his illness, agony andpain influences physician’s involvement andefficacy of treatment. In the present era ofconsumer protection social perception of boththe physician and the patient has gained evenmore importance. We form opinion of otherpersons by means of initial impression formed,the reasons for prejudice and discrimination, andalso the development of liking and relationshipswith specific individuals through interpersonalattraction.
Attribution
As we do not have access to the personalthoughts, motives, or feelings of others, we makeinferences about the traits based on the behaviourwe observe. If we infer that something about theperson is primarily responsible for the behaviourour inference is called “dispositional attribution.”But if we include that some external force is,primarily responsible for the behaviour, it is called“situational attribution”.
Basic tendency to ascribe causes to eventsis believed to be an inherent part of how peopleprocess information in both their social andphysical world. A particular behaviour is consi-dered to be caused by environmental forces pluspersonal forces, which is further divided intomotivation and ability. Motivation involves bothan intention to do something and an exertion
of efforts to accomplish it. There is also relationbetween personal force of ability and environ-mental forces such as task difficulty. Together,these qualities form the perception of ‘can’ ifthe personal force of ability outweighsenvironmental force, then individual can doaction.
Behaviour is seen as involving choices andintended effects on the part of the individual. Aperceiver is said to take into account not onlywhat other person does but also what the personmight have done. What a person does is a chosenaction. Some of the effects of chosen andunchosen actions are same, but other effects areuncommon to both chosen or unchosen actions.It is these uncommon effects, which yield cluesregarding the intentions of another person. Aperceiver gains most of the information aboutpersonal characteristics of another person, froma small number of uncommon effects, which havelow valance.
According to Kelley (1967) the observersevaluate the motives for the behaviour of othersusing a number of criteria. Observers use thisinformation to form a casual schema with whichthey make sense of things happening aroundthem.
Attribution theory and social cognition hasbeen applied in a number of different settings.Of our relevance is cognitive theory of depressionby Beck (see Chapter 21). This theory describesthe faulty inferences people make when in adepressed state. These depressed persons blamethemselves when something goes wrong, thinkothers have interfered and nothing can be goodfor them even in the future.
Self-perception: We use, much the sameprocesses for self-attribution, as that for otherattribution. When we want to make attributionsabout our own behaviour, we become observersof that behaviour and make attributions muchas if we were observing someone else. Therefore,with our behaviour we would first determine

16 Behavioural Sciences in Medical Practice
whether the environment, has caused thebehaviour through some strong external force.If this does not seem likely, we then, assume,the behaviour occurred because of some internalmotives or personality traits. Internal states areinferred by ruling out external forces.
Errors in attribution: We underestimate thesituational causes of behaviour, jumping toconclusions about dispositions of person. Thisbias toward disposition rather than situationalattributions is called fundamental attributionerror. Due to the expectation people tend to see,what they want to see and hear what they wantto, our motives and emotions may also lead usto expect to perceive certain things. Projectivetests, capitalise on these influences of motivationand emotion on perception. Perhaps, the greatestinfluence of motivation on perception is to befound in perception of such complex events associal and interpersonal relationships. This is so,because social situations are often indefinite andambiguous. Our perception of them are less,definite and stable than our perceptions ofphysical objects. Expectancy or set, refers to theidea that we may be ‘ready’ and ‘prepared for’certain kind of sensory input. Expectancy hasmuch to do with selection of what we perceiveor attend to. It also has a large role to play inthe way, we perceive ambiguous situations.
Clinical Applications
Sensory Defects
When sensory apparatus is damaged or partiallydestroyed the impairment of perception may notbe an accurate reflection of sensory damage. InHemianopia, for example destruction in visualcortex of brain can render one half of visualreceptor apparatus inactive, so that patient’svisual field is cut in half vertically. Surprisinglypatient may not report this as a handicap to hiseveryday activities, as he has been able toreadjust or compensate for it. Gestalt psycho-logists investigated such patients to demonstrate
their principle of closure in perception. A circlepresented to such a patient, so that it overlappedthe functioning and blind areas was reported asa complete circle. As in other situation where,closure operates hemianopic perceived thewhole figure when the amount presented wassufficient to determine the nature of whole.Similar closure effects have been seen in patientssuffering from deafness; affecting only certainsound frequencies, and in patients with disorderof tactile sensations.
A more elaborate instance of this tendencyto closure after defect occurs in phenomenonknown as “phantom limbs”. Following amputa-tion the patient may continue to experiencerealistic sensations in missing limb for sometimeeven for years. This odd phenomenon is relatedto the “perception of bodily self” or bodily imagederived from sensations in muscles, tendons,joints and balancing mechanism, as well as fromvision, hearing, taste, touch and smell.
Perceptual Function
Perceptual functions have been tested whichbasically are based on Gestalt principles. TheIshihara test for colour blindness is one of theexamples, the subject is shown the series of cards,and each contains a mosaic made up of hundredsof little dots of different colours. Embedded inmosaic might be a numeral, which can bepresented on the basis of the principle ofsimilarity. A normal person will use colour, asbasis of similarity but colour blind, will usebrightness as basis of similarity.
Pain Perception
Melzack and Wall (1965) have proposed a “Gatecontrol” theory of pain, which takes into accountpsychological variables as well as sensory inputs(see Chapter 25). Perception of intensity of pain,tolerance and its impact on the global functioningof the individual is dependent on perception ofpain.

Sensory Processes and Perception 17
Hallucinations
Hallucinations are defined as percepts, whichoccur without an external stimulus. They canoccur, in any of the senses and have all charactersof normal perception, yet there is nothing in envi-ronment, which stimulate the sense receptors toproduce experience. It is different from illusion,as in an illusion some of the sensory features ofstimulus are identified but recognition of wholeis incorrect. Hallucinations occur in patientswith psychotic disorders especially chronicschizophrenics and in patients having organicpsychosis. They can be classified in terms ofparticular sense through which they are appa-rently experienced, visual, auditory or tactile.
Sensory Deprivation
Sensory deprivation can lead to considerablepsychological disturbance. Such disturbances arealso known to occur in patients admitted for avery long duration in the hospital especially thosepatients confined for long periods or indefinitelyin respirators, those restricted by attachment tovarious pieces of recording equipment and life-support systems in intensive care units, and thosedeprived of sight for a period after eye surgery.Even more generally, we may note that themanifestations of impairment of consciousnessin delirious states are commonly at night, whichmay in part be due to the lower level of sensoryand perceptual stimulation at that time. Theactive modification of the sensory input isrequired in certain clinical situations.
SUMMARY
The sensory organs—vision, hearing, smell,touch and taste are highly complex systems andthey do not make a straightforward response toeach stimulus encountered. The knowledgecomes to each one of us through our senses.Sensation is the primary source of all humanknowledge. In human being unlike simple
organism, sensation is only a small part of muchmore complicated information processingsystems.
A stimulus is any form of energy to whichwe can respond (pressure on the skin), a senseis a particular physiological pathway for respon-ding to a specific kind of energy. Sensation isthe feeling we have in response to informationthat comes in through our sensory organs.Perception is the way our brain organises thesefeelings to make sense out of them. This involvesrecognition of objects that comes from acombination of sensations and the memory ofprevious sensory experiences. Sensation containsboth qualitative as well as quantitative element,and both physical and physiological events arecollectively called ‘sensation’. Sensation refers tothe process of receiving information, whereas toperceive means to interpret and understand.Perception is the process of knowing theworld outside you, by forming some mentalrepresentation. Perception is a complex process,extending far beyond the mere registering of light,sound, and other impulses from the externalworld. This external information must beinternally coded and transformed before anyonecan know what is really out there.
Since any single external cue is likely to proveinsufficient to narrow down the possibilities aboutthe external world, we are forced to rely uponvarious combinations of cues. Much of what weperceive, the sensory patterns merely provide the‘raw data’ for experience. The sensory infor-mation is transformed elaborated and combinedwith memories to create what we actuallyexperience or perceive.
Perceptual processes, which provide mean-ing to what we see or hear, are classified as—form, visual depth, constancy, movementperception, plasticity and individual differences.
Visual illusions are a dramatic example ofhow perceptual cues can be assembledincorrectly. An illusion is any figure that givesrise to a bizarre interpretation of reality. The

18 Behavioural Sciences in Medical Practice
illusions demonstrate that what we perceive oftendepends on processes that go far beyond the‘raw data’ of sensory input. Specific instancesin which the apparent curvature or length of aperceived line are not predictable from thecurvature or length of its stimulus pattern, havebeen called the “Geometrical illusions”. But thisdoes not mean that they occur only with regularlines and patterns; they can also be demonstratedwith quite irregular drawings and with realobjects in normal environment. The illusions areimportant because they may provide clues forour understanding of processes of shapeperception. Throughout the life span of anindividual some changes occur in the perceptualprocesses.
Extrasensory perception or ESP, stimulatesalso called as parapsychological phenomenonis of two main kinds:1. ESP
a. Telepathy or thought transference fromone person to another.
b. Clairvoyance or, perception of objects orevents not influencing the senses.
2. Psychokinesis or mentally manipulatingobjects without touching them.Social perception is concerned with our
interpretation of behaviour in social settings andgenerally refers to how we perceive others,favourably or unfavourably. Social perception isof great relevance to medical profession. Howthe patient perceives the physician determineshis trust for physician’s healing power. Attributionis making inferrences of others behaviour. Basictendency to ascribe causes to events is believedto be an inherent part of how people processinformation in both their social and physicalworld. Sensory deprivation, phantom limb,hallucinations, perception of pain and perceptualdisorders are some of the examples of clinicalapplication of understanding of perceptions.Social perception and attribution are importantfor physicians as these are related to theirinterpersonal relationship with the patients.

3Attention
Vimal, a college going student complains ofdecline in his academic performance for the lasttwo months, he wants to get a college degreebut whenever he sits to study, his mind wandershe is not able to comprehend, and is laggingbehind. Similarly you would encounter numberof patients: children, adolescents, adults and oldaged, complaining of poor attention and difficultyin concentration.
Definition
Attention is the perceptual processing of selectedinputs for inclusion in our conscious experience,or awareness, at any given time. We do not reactequally to all stimuli that impinge upon us; wefocus upon only a few. In other words, thisperceptual focussing is called attention.Concentration is the ability to sustain attentionfor a specific period, on a particular object orsubject.
The processes of attention divide our field ofattention. Consider being in the sports stadiumwatching a cricket match. While your focus ofattention is on the batting of the player, yet youare also aware of the scoreboard, you would alsobe trying to focus on the commentary and youalso would be dimly aware of other observerssitting next to you, or occupying front rows. Herethough your focus was on the player, the marginalinputs (awareness of other events) illustratecharacteristic of attention that it is constantlyshifting. What is at the focus one moment may
be in the margin the next moment and theobjects being in the margins may become thefocus.
Attention is needed for the efficientassimilation of information and generation ofcoordinated behaviour. It is like a computersystem that gets stuck if it tries to process at eachlevel a large number of simultaneous events. Theattentional limitation is not necessarily one ofresponse in compatibility though this mightsometimes be a factor. You can understand thisby an example that in an experiment onconditional salivation reflects to a sound new lightcan suppress processing of the sound as indexedby inhibition of salivation. This is a competitionfor a limited processing capacity rather thanmotor output (Rizzolatti, 1983).
A basic process in attention is considered tobe a kind of filtering of the sensory informationwe receive. We cannot process all the informationin our sensory channels, so we filter out, or blockirrelevant information (Broadbent 1958). Thereis evidence, that stimuli to which we are notactively attending still register in some form inour perceptual system, even though we may notrecognised them at that time. There are two typesof processing, known as parallel processing andserial processing. The parallel processing is whenwe are able to pick up information from twodifferent conversations or sources simultaneously.On the other hand serial processing is when wepick up information in a serial order fromdifferent sources.

20 Behavioural Sciences in Medical Practice
Factors Facilitating Attention
There are certain factors, which are either externalor internal factors, which direct and facilitate ourfiltering of inputs.
External Factors
There are many external factors, which attractour attention more easily than other stimuli. Thefeatures that call for selection of focus of attentionare stimuli, which are of higher intensity, like loudmusic, or lecture delivered with microphone.Stimuli of larger size generally arouse attention,thus you would experience that in seminars orconferences emphasis is placed on bold and largelettering for audiovisual presentation. Contrastand novelty are other characteristics of the stimuli,which easily catch attention. These principles areoften used in making of commercial advertise-ment, designing fashion clothes, architecture ofa building. You also use these methods in youracademic presentations. Repetition and move-ment of stimuli are also used by the media tofacilitate attention, as moving objects are moreattended to, as when compared to static objects.
Internal Factors
The internal factors are those present within theindividuals that cause them to attend to one eventinstead of other. One of them is ‘motive’ or need,if you want to buy a car, your attention wouldgo more easily on advertisements related toselling of cars, similarly if you are hungry, youattend more to the eating places. Preparatingset, i.e. a person’s readiness to respond to onekind of sensory input, but not to other kinds, isanother factor, which determines attention andwas dicussed in Chapter 2 (Sensation andPerception). Interest, also influences the selectivityof attention. These internal factors may be thetemporary or permanent state of our mind at agiven time, e.g. motives keep changing interestmay be more or less permanent as interest in
sports. These factors provide us with a certainamount of consistency in the events to whichwe pay attention. So they give our experience,or perception of the world some direction andstability.
Types of Attention
Attention can be subdivided into different sub-systems. These are based on somewhat differentbrain regions. Perry and Hodges classify attentionas follows:
Selective Attention
Imagine you are in the library preparing for yourseminar. While you are going through the latestresearch in the journal, you also hear some ofyour fellow students talking to each other, theattendant helping someone to find a book, thetelephone ringing, noise of hammers comingfrom one corner of the library where thecarpenters are at work. Despite all these potentialdistractions you are probably still able to focusyour thoughts on the article that you werereading. Our ability to attend one main eventwhilst being remotely conscious of othersprovides us with the paradox of how attentioncan be both a selective and a divided processsimultaneously. The restriction of mental pro-cessing to one event at a time is called ‘selectiveattention’.
This type of attention provides the means bywhich we reduce the workload on our mentalsystems. Schizophrenic patients have been foundconsistently deficit in their ability to focus on aparticular task. They show marked impairmentinability to avoid distracting stimuli.
Broadbent (1958) has explained howattention is controlled by a filter. According tohim, the information that becomes filtered outof the system (consciously unattended) willreceive only a low level of analysis. How we selectwhat to select, and on what criterion, is decidedvery early in the processing of information.

Attention 21
Selection is based upon the physical propertiesof the stimulus and is also referred to as sensoryselection. Broadbent’s filter theory of attentionhas been used in number of experiments withnormal individuals as well as with schizophrenicpatients and this still holds a popular place intheories of attention.
Generally most of the individuals cannotperform more than one task without taking theirmind off the other. However, there is someevidence that people may be able to be trainedto perform two difficult tasks at the same time.
Divided Attention
It is our every day experience that we are ableto divide our attention between two or moreevents or tasks, such as listening to music whilestudying, knitting while watching television, orengaging in conversation while driving.Psychologists studying the selective aspects ofattention have always emphasised how limitedour ability is for diverse attention. In the typicalexperiment of dichotic listening it was alwaysfound that subjects were unable to attend morethan one thing at a time. However, in theseexperiments generally the tasks given were veryintellectually demanding, hence subjects had verylittle mental power left for attending to anothertask.
It is fairly recently that more attention is beingfocussed on the divided attention. Kahneman(1973) proposed the ‘resource allocation’ theoryof attention.’ Resources’ refer to a reservoir ofmental energy from which is drawn theappropriate amount when dealing with specifictasks. The more difficult the task, the greater willbe the demands of the mental resources requiredto complete it. The less energy one particular taskdemands then the more of that energy will beavailable for allocation to other things being donesimultaneously. It is not the task themselves thatdetermine the allocation of the resources but theperson who performs them. For instance, eventhough a particular task may require a lot of
resources we may perform poorly on the tasksimply by not putting enough effort into it. Thisallocation of cognitive resources to the task, isunder conscious control and we are free at anytime to switch our attention to other events.
Our capacity for dividing attention betweentasks increases with practice on them. It has beensuggested that our mental resources do not havelimited capacity but may actually expand withpractice. It may, therefore, be possible to developour cognitive resources in more efficient ways,once the principles are more clearly understood.
Sustained Attention
Sustained attention or vigilance is required toprocess stimuli of long duration. Sustainedattention underlies the capacity to detect a signalover long periods (Perry and Hodges 1999), forexample to inspect a screen and report when asignal appears. Sustained attention can beassessed on continuous performance test. Thetest consists of rapidly presented set of task withvaried spacing and timing of target and nontargetstimuli.
Automatic and Conscious Processing
Compare a person who has been driving for longto that of a novice. One notices that afteracquiring the skill a person can drive and con-verse or listen to the music at the same time,whereas the novice will have to put in all hismental resources in driving, e.g. his concentra-tion on the road, on the steering wheel, accele-rator, brakes, etc. This fundamental differencebetween our ability to perform a complex taskas a beginner and later as a skilled person is thatof degree of mental effort involved. The way thata skilled person applies a little effort in order toperform a task fluently is a source of constantfrustration to the struggling novice. Skilledperformance seems to require few cognitiveresources such as that involving attention todetail. Shiffrin and Schneider (1977) proposed

22 Behavioural Sciences in Medical Practice
that attention occurred in two domains, whichthey named ‘dom A’ and ‘dom B’. Dom Aprocessing describes general, undivided atten-tion, the features of which are that it is passive,automatic, has a relatively large capacity andmakes a multilevel analysis of the attendedinformation. Conversely, dom B processing isconsciously controlled and is an active systemhaving limited capacity and having no controlover the processing that occurs in dom A. Thedom A system continuously receives input aboutthe environment that it processes unconsciously.Tasks that are well learnt have their elementsstored in long-term memory, so they areavailable during the automatic processing ofevents when such tasks are subsequentlyperformed.
Clinical Applications
Attention and concentration are the psychologicalprocesses, which are the first to get affected inillness and especially in psychiatric disorders. Thepatients with schizophrenia exhibit deficits inattention, which is evident even from the casualclinical contact with these patients. Someschizophrenics lack the capacity to perceive andrespond to situations objectively, due to theirinability to achieve a major ‘set’. The schizo-phrenic is characterised by segmental set, inwhich response preparation is compromised dueto an inappropriate focus on minor or irrelevantaspects of the stimulus array. The attentionaldeficits in schizophrenic have been assessed onimmediate serial recall tasks, span of appre-hension, reaction time, dictomic listening,backward masking and continuous performancetests. Assessment of attention and concentrationhas been discussed in Chapter 18, on assessment.
Undue preoccupation with memories ofrecent and/or past events associated, for example,with bereavement, an anxiety state or adepressive disorder, results in diminishedattention to the external world, so that
information is not registered and the individualbecomes forgetful and unable to pursue a taskrequiring sustained attention such as reading.
In some patients who complain of physicalsymptoms for which no organic cause can bediscovered, it is probable that their complaintsare, at least in part, due to an excessive focussingof attention on the site of the symptom and thatwhat they are experiencing is a bodily sensationwhich does not normally reach the level ofawareness. Just as in some patients input maybe selectively enhanced, so in others it may beblocked for psychological reasons. There arepatients who, though free from organic disease,present with a loss of skin sensation in part ofthe body, or of a special sense such as visionor hearing. Such complaints usually do notcorrespond with those produced by organicdisease and they are commonly described ashysterical. It has for long been suggested that themechanism by which they occur is a process ofinvoluntary dissociation between a limited partof consciousness (e.g. that concerned with skinsensation from a particular area or with visualor auditory perception) and the rest ofconsciousness. Thus these parts are dissociatedor shut off from the rest of awareness and theindividual no longer experiences the appropriatesensations or perceptions.
Some of the phenomena produced by hyp-nosis may be related to alterations of attention,and indeed the fundamental basis for the processmay be a highly selective focussing of attentionby the subject on the hypnotist with acorresponding lowering of attention to all otherstimuli. Thus in a suitable subject the hypnotistis able to suggest a selective inattention toparticular stimuli, resulting in, for example, anarea of skin anaesthesia or a loss of a specialsense such as vision or hearing.
Diseases affecting the brainstem (i.e. includingthe reticular formation), such as inflammation(e.g. encephalitis lethargic or sleeping sickness)or pressure from a tumour, can cause

Attention 23
drowsiness, sleep or complete loss of conscious-ness. Conditions affecting the functioning of thebrain more generally (e.g. through lack of oxygenor blood supply) may cause a state of delirium,with impairment or ‘clouding’ of consciousness;the patient may become confused, or dis-oriented—not knowing the present time or placeand hallucinated, may have difficulty inconcentration and subsequently have little or nomemory for events at the time. Finally, episodesof unconsciousness occur in some forms ofepileptic seizure, a condition associated with anelectrical discharge in the brain which, in someindividuals, ‘epileptics’, arises spontaneouslyfrom time-to-time, but can be provoked inanyone by chemical or electrical means (e.g.electroconvulsive therapy or ECT). Attentiondeficit hyperactive disorder is a common clinicalcondition in children. This disorder has onsetbefore seven years of age, is four to five timesmore common in boys than girls. Attentiondisturbances are manifested as failing to finishthe tasks that were started, easy distractibility,and difficulty in tasks requiring sustainedattention. Children with poor attention may haveaverage intelligence yet their school performanceis very poor. These children often have comorbidproblem of conduct disorder or specific learningdisability.
SUMMARY
Attention refers to the perceptual focussing oncertain stimuli with the aim of including themin the conscious awareness. Ability to sustainattention for some time is called concentration.
Attention is influenced by external and internalfactors. The former includes intensity and sizeof the stimulus, novelty, contrast and movement.The internal factors include motivation andinterest. Attention is of three types, namely,selective attention, sustained attention and
divided attention. Selective attention refers tothe ability to focus the thoughts on a particularstimulus, despite the presence of other factors.Sustained attention refers to the ability to holdattention over considerable period of time(vigilance). Divided attention implies focussing
attention on two or more tasks simultaneously.Attention also involves automatic and consciousprocessing. Study of attention is important sinceattentional deficits are commonly seen in patients,especially those having anxiety, schizophrenia,somatic complaints and certain neurological
conditions. Poor attention and difficulty insustaining concentration is the primary complaintin children diagnosed as attention deficithyperactivity disorder.

4Memory
Fifty-eight years old, male, senior executive ina good company comes to you with thecomplaints of not being able to remember hisappointments. At times he has difficulty inrecalling names of his colleagues, but remembersall the details of his past life. Otherwise he is ableto carry on his work quite effectively.
Just before the exams, many studentscomplain about forgetting everything that theyhave learnt. You would have wondered why oneforgets in these situations. Though you wouldhave read about the neurophysiology of memory,here we shall examine the psychological andclinical aspects of memory.
You would have realised learning emphasisesthat one must also remember the informationor skill learned. Imagine, if you were unable toretain or remember all that you ‘have earlierlearned. Even animals have some system bywhich they remember. Memory plays a very
important role in our learning and psychologicalgrowth. Through memory of our past expe-riences, we handle new situation, it helps us inour relearning, problem solving and thinking.
Memory ProcessMemory is the storage of learned behaviouralpotentials over time. It brings a persistent changein the central nervous system brought about byenvironmental input and by the activities of theorganism. Memory process can be divided intostages for the purpose of understanding (Fig. 4.1).Memory starts with the sensory input or stimulusfrom the environment. The input is throughsensory channels, like vision, hearing or touchand is held briefly (seconds) in a sensory register.Information is passed through sensory registerto short-term memory (STM) store where it isheld for 20-30 seconds. Some part of theinformation from STM is further processed in
Fig. 4.1: Memory process

Memory 25
rehearsal buffer that is information is repeated,and in some way linked with other informationalready stored in memory. From the rehearsalbuffer processed information is passed on to long-term memory store (LTM) where it is organisedin categories and stored for years. Informationnot so processed is forgotten. This process canbe compared with your day-to-day experiences.To learn new technical words, or names, youhave to rehearse several times.
Memory is viewed by cognitive theorist as anattempt to isolate some of the processes that actbetween the input of the stimulus and theresponse output. Memory is divided into threestages, encoding, storage, and retrieval. Encodingmeans transforming the sensory input into a formthat can be processed by the memory system.The encoded information is transferred tostorage. Retrieval involves locating memorisedinformation when needed. Figure 4.2 summa-rises this model.
Input→→→→→Encoding→→→→→Storage→→→→→Retrieval→→→→→Output
Fig. 4.2: Information processing model of memory
This could be compared with your expe-rience of attending a particular class. You hearlecture and make notes that is you encode thelecture, then the notes are stored in some fileusing date or topic name. When later thisinformation is required you retrieve by searchingthat particular file by it’s topic name. Thus anymemory system must perform three functions—a. Input—allow information to be fed into the
systemb. Storage—to maintain informationc. Retrieval—to access information when
required.There is another way of looking at the way
the memory works. Craik and Lockhart (1972)disagree with the concept of memory as a divisioninto three completely separate memory struc-tures—sensory, short-term, and long-term
memory. They identify only one kind of memoryand maintain that the ability to remember isdependent on how deeply we process infor-mation. We process material along a continuumof ever-increasing depth, running it through onlevels that range from quite shallow to very deep.The deeper we process it, the longer it lasts.
This concept of memory sees it as more ofan active than a reactive process with memoryperformance a direct result of the learner’s mentalactivity. The shallowest level of processing,according to this model, involves your awarenessof a sensory feature-what a word or number lookslike or sounds like, what a food smells or tasteslike, and so forth. As you recognise some kindof pattern in your sensory impression, you willprocess it more deeply. And when you make anassociation, that is give a meaning, to yourimpression, you will be at the deepest level ofprocessing of all, the kind that will form thestrongest and most enduring memory trace(Fig. 4.3).
Fig. 4.3: Levels of processing memory
Memory Systems
Recall of information is most often required indaily activities and especially in educationalperformances. We also recognise the material,or persons or places by acknowledging it.

26 Behavioural Sciences in Medical Practice
Familiar material can be learned more rapidlythan the unfamiliar material. There are at leastthree distinct ways of classifying memory. Theseare based on (1) neurological structure of thebrain, (2) experimental model of psychology and(3) clinical practices of mental examination. Onthe basis of neurological, theory, memory isdivided into verbal and non-verbal. On the basisof experimental model, memory is divided intosensory memory, short-term memory and long-term memory. On the basis of clinical practice,memory can be divided into remote, recent andimmediate. Their levels of processing alsodifferentiate short-term and long-term memory.Some detail of these memories is as follows:
Sensory Memory
Sensory memory is the first stop of an incomingstimulus. All sensory modalities (visual andauditory, tactile, olfactory and kinesthetic) areinvolved in receiving these first impressions.These impressions are either lost with time orprocessed further for later remembering. Theduration of sensory memory is very short andit varies in time for different sensory modalities.Iconic memory or visual sensory memory maylast from 250 msec to 500 msec, echoic orauditory sensory memory from 2 to 10 sec tactualmemory about 4 sec and motor memory(kinesthetic) as long as 80 sec.
Short-term Memory
You have just seen that information from sensoryregister is passed on to short-term memory(STM). This is also known as primary memoryand can be called as immediate memory. Whileyou have no voluntary control over whathappens to information in sensory storage, youcan control what is stored in STM by rehearsal.Information is held; in STM store upto about30 seconds, but the length can vary dependingupon many factors. Short-term memory has verylimited storage capacity; six to seven items can
be stored at one time. With new stimulus input,the original items get erased or fade away. Thestorage capacity ran be increased by chunking,i.e. combining several items. Unfamiliar itemsfade out faster than familiar items. Items can berecalled at will while the information is in short-term store.
Coding for short-term memory involvesspeech sounds, visual images and words. Gene-rally visual stimuli is translated into sounds, forexample, if a card of unfamiliar letters is flashedfor half a second after 15 seconds and you areasked to repeat it, chances are that you wouldreproduce the sound resembling that letter.
Some experiments have also demonstratedthat the material presented in the beginning ofthe next and at the end are recalled relativelywell than those appearing in the middle. This iscalled serial position effect. When recall is betterin the beginning of the text then it is known asprimacy effect while if the recall is better for thelast part of the text then it is called recency effect.
Working MemoryWorking memory is at times used as an alter-native term to STM. The concept of workingmemory is similar to STM with the only diffe-rence on its processing as well as its. storagefunctions. Working memory occurs between theshort time of sensory memory and the long-termmemory. A number of characteristics distin-guished this memory processing phase.• Working memory has very limited capacity.• Retains material for a very short duration of
time, for 18 to 20 seconds unless one triesto hold consciously.
• Material is consciously processed andretention last as long as it is held in attention.This system is called working memory
because the material transferred either in sensorymemory or long-term memory has to be workedon, thought about and mentally organised.Working memory provides a mental workingspace to help in sorting and processing new

Memory 27
information (Shiffrin, 1993). You can under-stand process of working memory by recallingthat you tend to remember the telephonenumbers till you have to dial it, after using thenumber it is discarded and it is no longer in thememory.
Rehearsal
Rehearsal means repeating items of information,silently or aloud and it helps to keep these itemsof information in the centre of attention.Experiments have shown that rehearsal could bemaintenance rehearsal where in information isjust repeated as it is. This is not very helpful inremembering for a longer duration. Elaborativerehearsal organises the material and givesmeaning while rehearsing. This is an activeprocess of transferring material from short-termmemory to long-term memory. The amount ofrehearsal given to items is important in thetransfer of information from short-term to long-term memory, the more an item is rehearsed,and the more likely it is to become part of long-term memory. In elaborative rehearsal, peopleuse strategies that give meaning and organisationto the material so that it can be fitted in withexisting organised long-term memories.
Long-term Memory
Long-term memory also known as secondarymemory seems to be very complex as it storesmany different aspects of our experiences. Thestorage capacity has no known limits and onecan remember information for days, months, andyears. It records the salient features of sensoryinputs and files these according to variousmemory categories. It also creates an auditoryrepresentation of the input and it also recordshow to reproduce the information whenrequired.
Long-term memory is of two types—procedural and declarative. Each one holdsdifferent kind of information. Procedural memory
stores memory for how things are done. It is usedto acquire retain and use perceptual cognitiveand motor skills. Procedural memory is relatedto action sequence, you recall skill memories likeswimming, driving, giving an injection. Theinteresting characteristic of this memory is thatyou remember the initial phase of learning. Onceyou have acquired the skill, you may performwithout consciously thinking about the task.Declarative memory is for remembering explicitinformation. It is also known as ‘fact memory’.Declarative memory contains two differentcategories of information.
Semantic Memory
Conains meaning of words and concepts, rulesof using these in language. Semantic memoryis not easily forgotten, as the information is storedin highly organised way in logical hierarchies,from general to specific ones. Such organisationmakes it possible for us to make logical inferen-ces from the information stored in semanticmemory.
Episodic Memory
Contains personal experiences of long-termmemories. It is a record of what has happenedto us, or remembrances of past things. Episodicmemory seems to be organised with respect tocertain events that happened in our lives. Theepisodes do not have to have a logical organi-sation. It is less organised, episodic memoryseems more susceptible to being forgotten thansemantic memory.
Long-term memory is highly organised.Information is categorised in number of ways.One of the evidence of organisation is seen in‘tip of the tongue phenomenon’. You all wouldhave experienced while trying to retrieve aperson’s name you cannot quite remember it butthe name is at your tongue. If we look at thistip-of-the-tongue (TOT) phenomenon in greaterdetail, we find evidence for the organisation of

28 Behavioural Sciences in Medical Practice
long-term memory. The search through thememory store in the TOT state is not random.If the name we are looking for is Shalu, we maycome up with Shalini or Shobha, but not Meena.If you try to experiment within this phenomenon,you would observe that when the subjects arein the TOT state, on hearing the definition butnot able to hit the “target” word, they would tendto retrieve words from their long-term memoriesthat (1) sounded like the target word, (2) startedwith the same letter as the target word, (3) containthe same number of syllables as the target word,and/or (4) have a meaning similar to that of thetarget word. The TOT phenomenon indicatesthat information is organised in long-termmemory. Types of memory are summarised inFigure 4.4.
Fig. 4.4: Types of memory
FORGETTING
Forgetting is failure to retrieve information fromlong-term memory store. Much of theinformation is lost but enough remains, so thatwe have sketchy record of our lives. Sometimeswhat we think is forgotten in real sense is notforgotten because it was never encoded andstored in the first place. Many students complainthat they do not remember the contents afterattending the class or forget after reading thetext. This happens due to lack of attention. Someinformation does not reach short-term memoryfrom the sensory register or due to inadequate
encoding and rehearsal; the information maynot have been transferred from short-term tolong-term memory. Information was not storedin long term memory because rehearsal was notsufficiently elaborate.
Many times we forget, as memory does notmatch events, which had occurred. This happensdue to the constructive processes, i.e. duringencoding, the to-be-remembered information,especially if it is a complex life event or somethingyou have read, is modified. Certain details areaccentuated, the material may be simplified, orit may be changed in many other ways so thatwhat is encoded and stored is far from a literalcopy of the input. Constructive processes ofencoding distort what is stored in the memoryand distortions are remembered. We rememberthe gist, or meaning of what we have read orheard but not the actual words themselves;inferences constructed at the time the informationwas encoded for storage is remembered, orportions of the to-be-remembered informationsis encoded. Besides the faulty memory processes,some of the other common factors of forgettingare as following.
Interference
According to this explanation, what we do in theinterval between learning and recall, determinesthe course of forgetting. Experimental studieshave shown that learning new things interfereswith memory of what is learned earlier and priorlearning interferes with memory of things learnedlater.
Retroactive inhibition: This is a technical namefor new learning that may interfere with materialpreviously learned. This has been demonstratedin experiments as following.
Activity
Group I II III
Experimental Learn A Learn B Recall AControl Learn A Unrelated Recall A
activity

Memory 29
As an example you may learn one chapterof physiology in activity I, then learn one topicof Anatomy in activity II, then try to recall whatyou had learned in physiology. The amount ofinformation you forget would be due to inter-ference caused by learning anatomy. Comparedto this, if you learn a topic from Physiology, restfor sometime, then recall physiology you wouldfind that your recall is better than that of theprevious chapter.
Proactive inhibition: When prior learninginterferes with the learning and recall of newmaterial, it is called proactive inhibition. Todemonstrate this type of interference experimentis designed as following.
Activity
Group I II III
Experimental Learn A Learn B Recall AControl Rest or Learn B Recall A
unrelatedactivity
Supposing you learn English, then learnFrench and recall French, you would find thatstudy of English interferes with your recall ofFrench. Here what you have learned earlier,interferes with the subsequent memory.
Even though lots of experiments have beenconducted, yet the process of interference is notvery clear. One idea is that the interferencesdisrupts the various kinds of associationsbetween stimuli and responses formed duringlearning. Another idea is that interference hasits greatest effect on the memory of retrieval cues.You have seen in the earlier section that memorydepends on retrieval cues, so if interferenceresults in problems with these cues, forgettingwill result.
In both types of interference it has beenfound that the effect of interference is less withmeaningful material and after attaining somemastery in the subject. In initial period of yourcourse you should try to allot different studytimes to similar subjects.
Encoding, Organisation and Retrieval Prob-lems If the stored information is not encodedwell or organized at the time it was learned, itis forgotten. Retrieval cues are also importantin memory, as we may not be able to recall someinformation in one situation but mayspontaneously remember in the other situation.Retrieval is facilitated by organisation of thestored material and the presence of retrieval cuesthat can guide our search through long-termmemory for stored informations. In the absenceof proper retrieval cues, the sought for itemsstored in long-term memory are not found. Manytimes you would have experienced that youcannot recall something while actively searchingfor it, but after giving up that search while doingsomething else, you recall that object. The newactivity in which you engaged, or the new contextgives another set of reminders, which helps toretrieve that information. It is a good idea to giveup and do something else in order to generatenew retrieval cues.
Motivated Forgetting
Emotional factors also play an important role inforgetting. If we encode information while in oneemotional state and try to recall it while inanother, recall suffers. Many lapses of memoryin daily life illustrate motivated forgetting. We mayforget the names of people we do not like.Repression theory holds that we forget becausethe retrieval of memories would be painful orunacceptable in some way to the person. Freud,in his book “The Psychopathology of EverydayLife” had illustrated many examples of repres-sion in forgetting. Repression includes retrievalfailure for the association of the threatening,anxiety-provoking information.
Anxiety or guilt producing material is moreoften forgotten than pleasant experiences.Supposing in a particular class you were scoldedby the teacher, chances of forgetting whathappened in that class would be higher.Psychologist have also found that some personscannot forget unpleasant experiences easily, they

30 Behavioural Sciences in Medical Practice
have related this phenomenon with personality.Some stored information is so threatening andanxiety arousing that it’s retrieval is possible onlyunder special circumstances like hypnosis, freeassociations.
Zeigarnik Effect
A Russian psychologist demonstrated throughexperiments that incomplete tasks areremembered better than the completed tasks.This is sometimes called “Zeigarnik effect”, “Ego-oriented” persons remember more of completedtasks as incomplete tasks generate more anxiety.On the other hand task-oriented personsremember more of incomplete tasks, as for themthe incomplete task is more painful whilecompleted tasks are not so.
Amnesia—Forgetting during Sickness
Amnesia refers to loss of memory due to disease.Amnesia is a general “disorder of memory”. Theperson may forget his past experiences or mayhave impaired ability to encode, store and toretrieve, thus forming of new memory is difficult.Amnesia is a profound memory deficit due toeither the loss of what has been stored or to theinability to form new memories. Amnesias areclassified under two categories: (i) biological and(ii) psychological.
Biological amnesias: Forgetting could be due toany of following reasons—diseases of the brainlike senile dementia, Korsakoff syndrome, con-cession from blows on head, brain damage, braininfections, tumour, stroke, temporary dis-turbances in the blood supply or effect of highdose of alcohol and drug abuse.
Senile dementia: It is characterised by deficitsin many intellectual abilities like memory, atten-tion, judgement, and abstract thought, that couldoccur in aged people. The person has troubleremembering events that happened after theonset of the disease. Thus the person with thisdisorder has trouble learning and cannot recall
well what happened last month, yesterday, oreven a few hours ago. Senile dementia is usuallythe result of a reduction in blood flow to the brain.
Transient global amnesia: These are profoundmemory problem with no loss of consciousness.It comes on suddenly without any obvious cause,and it typically lasts for only a few hours or daysbefore memory becomes normal again.Fortunately, most people who experience suchamnesia have it only once. This type of amnesiais called global because much of what has alreadybeen stored in memory is forgotten and becauseeven though the person is conscious and can goabout the routine business of daily life, no newmemories are formed while the attack is inprogress.
Alcohol and drug abuse: These also causeamnesia, a person may have amnesia for theevents occurring while under the influence ofalcohol because encoding and storage processeshave been disrupted by the effects of the alcoholon the brain. Heavy drinking over a period ofyears however, can result through vitamin-Bdeficits and other chemical imbalances, inirreversible brain damage and a pattern ofsymptoms known as the Korsakoff syndrome.Interograde amnesia the inability to form newmemories is one of the prominent symptoms ofthis syndrome.
Psychological amnesia: These types of amnesiasoccur due to psychiatric diseases where theperson forgets his identity also. There may notbe a permanent loss.
Childhood amnesia: is due to the differences inthe ways young children and older peopleencode and store information. As adults, muchof our memory is encoded verbally and tied intonetworks, or schemata, that are based onlanguage. But the young child without langu-age encodes memories in a nonverbal form,perhaps storing information as images orfeelings. Early childhood memories are thus saidto be stored in forms no longer available to us

Memory 31
as adults. Our language-dominated memories,do not have retrieval cues appropriate forgaining access to the image and feeling memo-ries of early childhood. Perhaps the memorymachine is just not able to store long-termmemories until its maturation is essentiallyfinished. Language ability and memory developtogether because both depend on brainmaturation. You all experience that dreams areforgotten on waking up. Dream amnesia mayactually have a biological basis. The dreamingbrain seems to be in a special state different fromthat of the waking brain.
Defensive amnesia: People with defensiveamnesia may forget their names, where they havecome from, who their spouses are, and manyother important details of their past lives.
It is called defensive because this type ofamnesia is usually considered to be a way ofprotecting oneself from the guilt or anxiety thatcan result from intense, intolerable life situationsand conflicts. Defensive amnesia is thus anextreme form of repression.
Normal aging: has its problems too, but thetypical forgetfulness of old age is hardly severeenough to be called amnesia. In normal aging,the memory problem, centres largely on thestorage of relatively recent events; it isanterograde in nature. But, in marked contrastto senile dementia patients, normal old peopleare able to compensate for their mild memoryproblems. They try to do less and thus put asmaller burden on their information-processingsystems, they provide themselves with remindercues, perhaps by writing down what is to beremembered, and they organise their lives intoroutines so that fewer new things need to beremembered. In other words, normal old peopleadopt adaptive memory strategies.
Methods to Improve Memory
With training, practice and motivation memorycan be improved. Some well-practiced methods,
verbal as well as visual mediators to improvememory are listed in this section.
Mnemonics
You can recall when a list of difficult technicalwords in pharmacology or unfamiliar words inforeign language is to be remembered. Mne-monics are devices that facilitate the learning andrecall of many such forms of difficult material.One of the method is to associate whatever youwant to recall with something already establishedin your memory bank, e.g. colours of rainboware associated with name “Roy G. BIV”, i.e. Red.Orange, Yellow, Green, Blue, Indigo and Violet.
Method of Loci
You visualise a scene and fit the items to beremembered in that scene. The scene can be astreet, a building with rooms, the layout of acollege campus, a kitchen, or just about anythingthat can be visualised clearly and contains anumber of discrete items in specific locations toserve as memory pegs. Supposing you want toremember for examination classical conditioning,then start by imagining a dog, experimentalroom, food, bell and any person as anexperimenter. Rehearse this image over and overuntil it is well-established in your mind. After youhave formed your image, associate the events,the stimulus substitution, and extinction with this.The trick is to make associations with as manyconcepts as needed.
Pegword Method
Pegword method is another technique throughwhich a list of items and their relative positionscan be learned effectively. To establish the mainidea in your long-term memory, a well-organized set of images to which the to-be-remembered items could be linked. For lettersystems you can establish mnemonic pegs byforming strong distinctive images of words thatstart with the sounds of the letter of the alphabet.

32 Behavioural Sciences in Medical Practice
In number systems, you form an image witheach number.
Rhyming
Rhyming can be used for learning of long listinvolving numbers like the numbers 1 through10. You can organize or arrange the first lettersof words in such a way that it rhymes. In Anatomymany students use rhyming to remember namesof the different bones.
Making a Story
Making a story in this you can fit the facts in thestory like you read in elaborative rehearsal.
Chunking
This technique illustrates systematic ways ofencoding information. If you want to remembera long list of digits, e.g. 1989609065 you canbreak the numbers into chunks, the first four digitscould be remembered as the year you passedyour school or associated with any significantthing that happened in that year. Next three digitscould also be taken as date, e.g. for someone’sbirthday. The last 3 digits can be an address code.Like this chunks can be associated with someimportant thing for lasting memory.
Remembering Names and Faces
As first steps in establishing a good memory fornames and faces, we should: (i) be sure we hearthe name clearly when introduced, (ii) repeatthe name when acknowledging the introduction,and (iii) if the name is unusual, politely ask thenew acquaintance to spell it. While we are makingsure we have heard and rehearsed the name,we should be paying close attention to theindividual’s face.
The important thing for good memory is yourmotivation and ability to organise the material.One strategy in remembering things well is to
organise, or arrange the input so that it fits intoexisting long-term memory categories, is groupedin some logical manner, or is arranged in someother way that makes sense. The organisationalencoding may be inherent in the input itself orit may be supplied by individuals as they learnand remember new things.
Here are some tips to help you to improveyour memory.1. Plan your study content and make a time
schedule to cover that content. Stick to thisschedule firmly.
2. For academic and nonacademic activities.One can make use of methods that help usto study better for the exams and do well.These methods are listed in the section below.
3. As you have seen rehearsal is important totransfer information into long-term memory,and elaborative rehearsal is more effectivethan maintenance rehearsal. So make notesof important points as all the details ofinformation cannot be remembered. Revisethese notes.
4. You can use imagery to visualise the materialyou are learning and give auditory stimu-lation by reading aloud. For example whilestudying nervous system, visualise thestructure of nervous system with minutestdetails and also read loudly. Multi-channelstimulation would improve your memory.
5. Try to organise your material with retrievalcues or reminders. Make a map of contentsin your mind.
6. Give a feedback to yourself by testing yourmemory. Revise areas where you could notremember.
7. Review before examination. Try to learn butdo not get anxious as you have seen highanxiety level would interfere with yourremembering.
8. Give some short rest pauses between yourstudy times. It would help to consolidate thematerial you are learning.

Memory 33
Clinical Assessment of Memory
Measurement of memory is a complex taskbecause a number of variables interact in recall.All these variables can be divided in three groups:(i) nature of the material, (ii) the methods usedfor testing the recall, and (iii) characteristics ofthe individual. A combination of these threefactors is necessary for testing the memory.Methods to assess memory are given in Chapter18.
The method employed for testing the memoryincludes, immediate recall, delayed recall,sequential recall, associative recall, recons-truction, recognition both filled and unfilledinterval between presentation of material andtheir recall. Recall is also affected by individual’scharacteristics. A person who is more attentiveand receptive can recall better. The physical stateof the individual taking test, his motivation, age,sex, education, do play role in the recall;irrespective of the material and methods usedfor testing the memory.
We are much more concerned about memorydisturbances and its quantification. There are twotypes of memory disturbances—period specificmemory disturbances and generalised slowingin memory. The former includes retrogradeamnesia and anterograde amnesia. Retrogradeis a defect of recall whereas anterograde amnesiais a defect of registration/retention, from thepoint of occurrence of a significant life event.
Longer the time duration of washout ofprevious traces in case of retrograde and thedifficulty in forming the images for subsequentrecall in case of anterograde amnesia forms thedegree of severity of memory disturbances.Conventional techniques of memory testing donot quantify these period specific memorydisturbances.
The generalised slowing in the formation andretrieval of the traces however, can be quantifiedfrom the available psychological tests of memory.
Clinical Applications
Memory is the most recognised cognitive func-tion. It is markedly sensitive and easily influen-ced by emotionality, problems of daily life,psychiatric disturbances, sleep deprivation, overwork, fatigue, consumption of intoxicants,electroconvulsive therapy (ECT), exposure toanaesthetic gases, head injury, etc.
In your clinical practice you shall come acrossmany patients having minor memory distur-bances, but you may also come across patientswith very severe memory disturbance, wherethe patient may even forget his name, to whichplace he belongs. He may go from one placeto another and have total loss of memory forthe incident. In memory loss due to normal agingsometimes the individual may remembereverything of the past, but is unable to form newmemories. Memory problems are very commonamongst students. Children with below averageintelligence also have memory problems.Similarly poor memory is reported in childrenwith attention deficit disorders. High anxietystate in students during examination impairsretention.
Psychological strategies for enhancingmemory or aids to rehabilitation especially forpatients with neurological problems have beendeveloped. These are of special importance inrehabilitation of patients with head injury, andamnesias of all types. As any memory processincludes three functions namely—encoding,storage and retrieval thus the strategies toenhance these processes are given in brief inthe following section.
Encoding
To improve encoding of the information advisepatients/family members to:
i. Simplify informationii. Reduce the amountiii. Make sure he has understood

34 Behavioural Sciences in Medical Practice
iv. Repeat the informationv. Make associations
vi. Encourage to organise and group theinformation
vii. Process at deeper levels—think aboutmakes it meaningful.
StorageTo improve storage process first of all rate offorgetting should be objectively assessed. Thenattempts should be made to rehearse, then testand retest the memory. Use method of expandedor reconstruction rehearsal method as this is moreeffective than repetition.
RetrievalAs retrieval is better in context where the patientis learning, so advise patients to go to the situationin which retrieval is required. Retrieval can bedone by:
i. First letter promptsii. Alphabetical searchingiii. Mental retracing of events.
In addition to this certain other strategies canbe used for rehabilitation of patients with memoryimpairment. Environmental adaptations forpatients having very impaired memory can bemade by using labels, sign post, or colour coding.External aids can be used. These are of two types:(1) those aids that we use to store informationexternally, e.g. lists, plans, diaries, and (2) cueingdevices. Also some of the methods listed aboveto improve memory can be used, likemnemonics. While helping such patients it isalso important to advise family members not tomake fun or laugh at these patients. Anencouraging attitude towards the patient shouldbe adopted.
SUMMARY
Memory is an ability to remember, this is a veryimportant cognitive process for our learning. The
memory process is divided into three mainstages—encoding, storage and retrieval. Thereare three distinct ways of classifying memory:(i) neurological structure of the brain, whichdivides memory into verbal and nonverbal,(ii) on the basis of experimental model, memoryis divided into sensory memory, short-termmemory and long-term memory, and (iii) onthe basis of clinical practice, memory can bedivided into remote, recent and immediate.Their levels of processing also differentiate short-term and long-term memory. The two primaryand secondary types of memory are, short-termmemory wherein information is stored formaximum 30 seconds and has limited capacity.In long-term memory store, information isorganised in semantic memory or in episodicmemory.
There are four main causes of forgetting:(i) interference due to similar material, (ii) faultyencoding, storage and retrieval. If the sensoryregistration or input of information is faulty thenmemory will not be established. Similarly eachof these stages are important for good memory,(iii) motivated forgetting, and (iv) amnesias whichcould be biological, due to diseases of the brainor psychological.
Memory could be improved with goodplanning, organisation, review and feedback. Theother methods to improve memory aremnemonics, method of loci, pegword method,rhyming, making a story, and chunking. Somestrategies have been developed to help andrehabilitate patients with severe memory defectssuch as head injury, dementias, normal aging.These strategies provide steps to enhancememory at different stages of processing.
There are several methods to assess memory,which have been given in Chapter 18.
Clinical applications of memory extend fromvarious psychiatric; child psychiatric disorders toneurological disorders especially head injury anddementia. Methods to improve memory are ofrelevance to the students themselves.

5Learning andStudying
Try to remember the first time you tried to solveproblem on Rubrik’s Cube or played badminton.Probably now you will laugh at that behaviour,as at that time you found that difficult to performor play because of the errors made one afteranother. But you can also recall that with gradualpractice, you got better and better at each time.This illustrates an important principle of‘Learning,’ the capacity to ‘profit’ from experienceand practice. Learning is an important processas it has applications not only to learn new things,but also to modify maladaptive behaviours. Fora student, learning also has relevance as it canhelp in understanding one learning process, andmethods to improve learning styles.
Definition
Learning is the central process to all ourbehaviour, as we learn to do various activitieslike speak, write, think, or play. Our attitudes andemotional expressions are also learnedbehaviours. All our adaptive as well asunadaptive, cognitive as well as affectivebehaviour are formed by learning processes.These are of vital importance in helping theperson to adapt to his changing environment.
Learning is the acquisition through insight ofcognitive structure. It is an internal process, notnecessarily observable, in which information isintegrated into the structure of what studentalready knows and understands. Learning is aprocess resulting in some modification, relatively
permanent, of the way of thinking, feeling, anddoing of the learner. The characteristics oflearning is producing a behavioural change inthe learner, leading to a relatively permanentchange, that is also gradual, adaptable andselective resulting from practice, repetitions andexperience, and not directly observable. Thereare three important factors in learning:1. Learning brings change in behaviour.2. Change takes place through practice or
experience. It emphasises that all changesdue to growth or maturation or by drugs,brain injury, are not learning.
3. The change in behaviour should bepermanent, to be called as learning.Learning is not only acquisition of a body
of knowledge, but it governs our total behaviourfrom simple to complex. There are a variety ofways by which we learn, which are detailed inthe following section:
How do we Learn?
There are a number of theoretical explanationsabout the process of learning. Some theoriesemphasise on stimulus response (S-R) relation-ships, and interpret learning as an associativeprocess. Classical conditioning and operantconditioning are based on associative learning.Other psychologists argue that all types oflearning cannot be explained on simple formsof S-R relationships. They give importance toperception and understanding for learning

36 Behavioural Sciences in Medical Practice
complex forms of learning. Cognitive theoriesare an offshoot of this explanation. However,we are social beings and we learn number oftasks in social context, so another group oftheorists have given the social learning model.In the following section, all these methods oflearning shall be examined in detail.
Classical Conditioning
Classical conditioning is the simplest form oflearning based on experiments of Pavlov, aRussian physiologist. Conditioning is a term usedto describe the process by which the previouslyneutral stimulus (CS) gains the power to elicitthe conditioned response (CR). Pavlov hadnoticed during the experiments that hisexperimental dogs salivated not only to the sightof food, but also to the sound of experimenter’sfootsteps. To study this phenomenon systemati-cally, he associated the presentation of food tothe dog with another stimulus, such as the soundof bell. After giving some trials in which the bellpreceded the presentation of food, the dogstarted salivating at the sound of the bell. Toexplain this phenomenon, some technical termsare used; food is called unconditioned stimulus(US), and salivation elicited for food is calledunconditioned response (UR). The sound of bellin the experiment was conditioned stimulus(CS). It was initially a neutral stimulus becauseexcept for an alerting or attentional responseduring the first few times it is presented; it doesnot evoke a specific response. The response ofsalivation to bell is called conditioned response,as it was originally a neutral conditioned stimulus;it evoked a specific response due to learning (Fig.5.1) the conditioning procedure.
Fig. 5.1: Classical conditioning procedure
The acquisition of a conditioned response isgradual and becomes stronger with repeatedtrials. There are certain acts of classicalconditioning which require consideration.
Acquisition: Each paired presentation of the CSand the US should be presented a number oftimes, and the interval between CS and USshould be short. In simultaneous conditioning,the CS begins a little earlier than the onset ofUS and continues along with it until the responseoccurs. In delayed conditioning, the CS beginsmuch before the onset of US. In trace condi-tioning, the CS is presented and then removedbefore the US starts.
Stimulus substitution: An association or pairingof CS with US acquires the capacity to substitutefor the US in evoking a response. Withconditioning, a link or bond is formed betweenthe CS and US, and as a result of this CS becomesequivalent to US in eliciting a response. Stimulussubstitution occurs if CS is similar to US. But therecent theorists do not agree with this simpleprocess of stimulus substitution. According totheir viewpoint, CS becomes a signal for the US;when CS is presented, the US is expected andthe learner responds due to expectation.
Stimulus generalisation and discrimination: Whenthe conditioned response to a stimulus has beenacquired, other similar stimuli can also evokethe same response. This is known as stimulusgeneralisation. In Pavlov’s experiments, the doggave CR to slightly different bell also. It has alsobeen demonstrated that the closer the similarityto US with other stimuli, the greater is the CR.
Discrimination is to make one response toone stimulus and a different response, or noresponse to another. This process is comple-mentary to generalisation. In experiments it isdemonstrated by using two different tones CS1and CS2. On some trials CS1 is paired with USand on other trials CS2 is given alone withoutUS. The subject learns to respond only to CS1,after learning takes place (Fig. 5.2).

Learning and Studying 37
Extinction and spontaneous recovery: If theunconditioned stimulus (US) does not follow theconditioned stimulus CS repeatedly, theconditioned response gradually diminishes.Repetition of the conditioned stimulus withoutunconditioned stimulus is called extinction; thisis not forgetting, as a specific procedure isinvolved in this.
Extinction is used for modification of prob-lem behaviours in clinical practice. A responsethat has been extinguished, does recur later onits own, this is called spontaneous recovery. Ifthere is a period of rest after extinction, the CRtends to re-emerge. This tendency is moremarked after continuous than distributed practiceof the response during extinction. At this stage,if reinforcement or US is not presented with CS,the response extinguishes permanently.
Operant Conditioning
Operant conditioning, a term coined by BFSkinner, means that the likelihood of a behaviourdepends on the significance of the eventimmediately following it to person showing thebehaviour. If the event following the behaviouris positively reinforcing or rewarding, then it willrecur. If it is not reinforced or is punished, thenit is less likely to recur and eventually stopscompletely, a process known as ‘extinction’. Analternative related approach is ‘stimuluscontrol’—changing the preceding event. Whena response operates on the environment, it mayhave consequences that can affect the likelihoodof the response occurring again. This form oflearning is also known as instrumentalconditioning, because some action or behaviour
of the learner is instrumental in bringing abouta change in the environment, that makes theaction more or less likely to occur again in thefuture. For example, putting food in your mouth(an operant) is likely to be repeated because ofits pleasant consequences (Fig. 5.3).
This is an effective method for teaching newbehaviour patterns and for modifying undesir-able behaviours. A number of treatment strate-gies used in behavioural therapy and behaviouralmedicine are derived from this method (seeChapters 20, 22). The basics of operant condi-tioning are reinforcement and punishment. Thus,use of reinforcement and punishment shall beexamined in detail.
Reinforcement: The basic principles of operantconditioning are that when a behaviour occursand is followed by reinforcement, it is more likelyto occur again in the future. A great deal of ourbehaviour has been learned because it has beenrewarded. For example, you study because youmay find it reinforcing in terms of marks attainedor praise from your colleagues. Many responsescan be made to occur more frequently byfollowing it with reinforcement. The behaviourcan be shaped and moulded by appropriatearrangements of responses and reinforcers.
Nature of reinforcers: Whether something ispositively reinforcing or punishing, depends onthe effect it has on behaviour. What may bepositively reinforcing to one child may not beso for another. For example, usually food willbe positively reinforcing, but to an anorexic girl,who hates the sight of food, it may be punishing.Pain is usually punishing, but to a child preoc-cupied with guilt with masochistic tendencies, it
Fig. 5.2: Generalisation anddiscrimination learning
Fig. 5.3: Operant conditioning process

38 Behavioural Sciences in Medical Practice
will be positively reinforcing or rewarding.Further, the strength and direction of rein-forcement will depend to some degree on thechild’s relationship with the person administeringor involved in it. A game of football is likely tobe more positively reinforcing for a boy if itinvolves his father than his mother. A star chartfor bed-wetting worked out in cooperation witha mother with whom a 6 years old has a goodrelationship, is likely to be more effective thanif the mother and child are in serious conflict.
Reinforcements are divided into two types:(i) primary or material rewards, such as snacks,sweets, food, etc. and (ii) secondary or socialrewards, such as praise, smile. Events orconsequences, which strengthen behaviour whenthey are presented, are called positive reinforcers.In negative reinforcement, the response causesthe termination of a painful event. Removal ofpainful or unpleasant consequences can alsostrengthen or reinforce behaviour. For instance,offering a screaming child an ice cream may resultin a child stopping screaming. The adult is likelyto continue to give ice cream (operant) to stopthe child from screaming (negative reinforcementfor the adult).
In children, the most common form ofpositive reinforcement is praise and attention.Children are likely to repeat behaviour, whichgives pleasure to those whom they are fond of.Usually their parents and teachers are the mostimportant people to give positive reinforcement;as they get older, other children/peers increa-singly take on this role. If a teacher plays gratifyingattention to bad behaviour (even if the attentiontakes form of shouting at the child), then badbehaviour will recur. Material rewards such asmoney, sweets, chocolates, other favouritefoods, and watching television are also used asreinforcers.
Schedule of reinforcement: According toSkinner, at the beginning of training you shouldreward each and every move the child makes
toward the goal. However, once the child hasmastered a given response in the chain, you maybegin slowly fading out the reward by reinforcingthe response intermittently. Continuousreinforcement is necessary at first, both to keepthe individual to perform and to let him knowthat he is doing something right. However, oncethe child learns what that “something” is, youmay begin reinforcing the response every secondtime, then every third or fourth time, thenperhaps every tenth time. If you fade out thereward very gradually, you can get a child tomake a simple response several times, for eachreinforcement.
During the fading process, the exact schedu-ling of the reward is crucial. If you reinforceexactly every tenth response, the child will soonlearn to anticipate which response will gain himreward. Skinner calls this fixed ratio reinfor-cement, because the ratio between the numberof responses required and the rewards given isfixed and never varies. Instead of reinforcingexactly the tenth response, we can vary theschedule, so that sometimes the third responseyields reward, sometimes the twentieth or anyresponse in between. A hundred responses willyield about 10 rewards, but the child will neverknow when the next reward is coming. Whentrained on variable ratio schedules, individualsrespond at a fairly constant pace.
Extinction generally occurs most rapidlyfollowing withdrawal of things that are positivereinforcers. Thus the withdrawal of love frompeople of whom the child is fond is often themost effective way of achieving extinction of theundesirable behaviour. In other children, thewithdrawal of material goods, such pocketmoney, special food or drink, and opportunityto watch television are more important.
Shaping: Refers to the gradual forming of thebehaviour. Desirable new behaviour can be builtup through successive reinforcement of asequence of components parts of that behaviour.

Learning and Studying 39
It is commonly used in teaching skills to mentallysubnormal.
Punishment: When we wish to eliminate anunadaptive behaviour, punishment tends todecrease the likelihood of occurrence of theresponses. Any unpleasant consequence ofbehaviour, which makes that behaviour lesslikely to occur, can be seen as punishing. Physicalpunishment by parents is the most frequentlyused, but many children do not respond to itby a reduction in their undesirable behaviour.Probably, the attention they get when they arepunished has a positive reinforcing rewardingeffect, and this result overrides negativeexperiences of physical pain. The experience ofnegative emotional states like anxiety, depressionand a sense of failure, are like strong punishment.In other words, punishment decreases thefrequency of a response and stops thebehaviours leading to it. Some of the commonmethods based on principle of punishment aretime out from reinforcement, overcorrection andresponse cost. These methods, if used con-sistently and systematically, have been found to
be very effective in modifying problembehaviour in children (Mehta, 1989).
Comparison between ClassicalConditioning and Operant Conditioning
Both classical and operant conditioning are theimportant methods of learning, but you wouldhave observed that these two types of condi-tioning are different in their process of learningfrom each other. These differences have beenhighlighted in the following Table 5.1.
Cognitive Learning
In learning more complex tasks, perception andknowledge or cognitive processes play animportant role. Cognitive theorists state thatlearning cannot be satisfactorily explained interms of stimulus response association. Theypropose, that a learner forms a cognitive struc-ture in memory, which organizes information intorelationships and meaning. Without any knownreinforcement, new associations are formed andnew relationships are perceived among events,
Table 5.1: Comparison between classical conditioning and operant conditioning
Classical conditioning Operant conditioning
1. Stimulus oriented Response oriented2. UCS is given irrespective of the organism’s behaviour Organism’s own behaviour determines whether or not the
UCS will be presented3. Time interval between the CS and the UCS is rigidly Time interval depends on the organism’s own fixed
behaviour4. CR is reflexively forced by UCS Response is more voluntary and spontaneous5. CR and UCR are similar but not identical Similarity is the exception rather than rule6. Responses involuntarily medicated by autonomic Responses under voluntary control, mediated by the
nervous system like eye blink central nervous system7. The unconditioned stimulus (UCS) occurs without The reward is contingent upon the occurrence of
regard to the subject behaviour response8. Association between stimulus response (S-R) is on the Association between stimulus response (S-R) is on the
basis of law of contiguity (things occurring closer basis of law of in effect (effect of reward and punishment)time and space get associated)
9. Reinforcement comes first, as food is presented first Reinforcement is provided after the response is madeto elicit the response by the organism
10. Stress is laid on time control Place of motivation and reward is stressed11. The essence of learning is stimulus substitution The essence of learning is response modification

40 Behavioural Sciences in Medical Practice
simply as a result of having experienced theseevents. Links are made among stimuli, so thatstimulus-stimulus (S-S) associations are learned.These theories take account of concept forma-tion, in which the learner actively tests his ideas,rules and principles, in order to make sense ofincoming information. Bruner et al (1966)hypothesised that the learner interprets andtransforms any incoming stimulus in the light ofprevious experience. Gagne suggested thatlearning is an eight stage hierarchical process,involving events both internal and external tothe learner and which incorporate many differenttypes of learning (see Box 5.1).
Box 5.1: STAGES OF LEARNING• Motivation (desire to learn new things)• Apprehending or attending (perceiving the
relevant information)• Acquisition (the learner codes the infor-
mation)• Retention (the information is stored in
memory)• Recall (the information is retrieved from
memory)• Generalisation (the information is applied
to novel situations)• Performance (or practice of what has been
learned)• Feedback (The learner receives knowledge
of their performance)
Cognitive learning includes some of thefollowing methods of learning.
Insight learning: Kohler, a German psychologist,on the basis of this experiments on chimpanzees,emphasised that while working on a problem,one grasps three inner relationships throughinsight, not through mere trial and error, butby perceiving the relationships essential tosolution. In his typical experiment, a chimpanzeein the bars was given two unequal sizes of sticksand the fruit was kept outside the bars, whichcould not be reached by one stick alone. Afterseveral trials, the animal all of a sudden joined
the two sticks together to make it a single longstick, and with that he could reach the fruit.
Insight is often used in problem solving,puzzles and riddles. To emphasise the sudden-ness of the solution, it is also called by some as“Aha experience” (see Chapter 7).
Sign learning: It is an acquired expectation thatone stimulus will be followed by another in aparticular context. What we learn is a set ofexpectations or a cognitive map of the environ-ment, rather than specific responses.
Toleman believed that some learning is signlearning. We develop a sort of cognitive mapor structure, instead of learning a sequence ofthe task. On the basis of understanding, we tendto make spatial relationships.
Social LearningThere are many forms of learning, which cannotbe explained through conditioning or throughcognitive learning. We also learn through obser-vation. Social learning theorists stress uponobservational learning or modeling, in which aperson acquires a response to a specific situation,by watching others make a response (Bandura,1969).
Imitation is one of the important methodsbased on this theory, which could be appliedin learning of many skills. For example, manyof your skills like giving an injection, measuringblood pressure, dressing of a wound or surgicalskills, are learned by simply observing seniorsperforming those skills. Even maladaptivebehaviours, like aggression are learnt throughimitation. The learner acquires and stores inter-nal (representations) response through imagesand verbal coding, which may be expressed later.Social learning methods are also applied inbehaviour therapy (see Chapter 20).
Observational Learning
Imagine the following events:1. A student watches a consultant surgeon
operating on an infant for diaphragmatic

Learning and Studying 41
hernia. In this way, he begins to acquire thecomplex skills needed for this type of surgery.
2. A group of young men and women listento a detailed account of an unusual, buthighly successful bank robbery on theevening news. Later, they plan and carry outa similar robbery themselves.These two situations are different, yet they
share one important feature of learning throughobservation. In each case, new forms ofbehaviour were acquired simply by observingothers’ actions.
There has been rising recognition of the keyrole played by observational learning in thebehaviour of young children. Many experimentssuggest that youngsters acquire a wide range ofresponses, including attitudes, values, and self-control, through exposure to their parents orother persons that is, through exposure to socialmodels (Rushton, 1976; Bandura, 1977). Inseveral early studies, Albert Bandura and hiscolleagues exposed children to brief films, inwhich an adult model acted aggressively towardan inflated plastic doll. Observational learningis increased when we pay close attention to theactions of others, but is reduced when suchattention is absent. It is also increased when weattempt to first summarise or code others’behaviour in some manner, and then rehearseit (Bandura, 1977; Berger et al 1979).
Latent Learning
This type of learning refers to any changes thatare not evidenced by behaviour at the time ofthe learning. It occurs without any reinforcementfor particular responses, and seems to involvechanges in the way in which information isprocessed. You can get ample examples of latentlearning from your own experiences. This isdifferent from observational learning, as you havenot consciously put an effort to learning, but lateryou can perform that particular skill or responses.
Biological Learning
You would have seen that in spite of using similarmethods of learning, devoting similar time, yetall persons are not able to learn in a same way.Some people take more time to learn ascompared to others. Thus, important process oflearning cannot be fully understood without somegrasp of the biological functioning of differentpeople. We possess different capacities to receiveand process different abilities to learn. The studyof learning has acquired a new perspective, onein which the impact of biological factors is givenincreased emphasis. The most important conceptthat emerged out of this perspective is conceptof preparedness, proposed by Seligman (1970).According to this concept, persons are preparedby their biological structure and function, toaccomplish certain kinds of learning but notothers. Learned behaviour can be divided intodistinct categories.
Prepared: These actions are closely related tothe survival of the persons and very little trainingis required.
Unprepared: The tasks are learned slowly as andwhen required by the person. These are notrelated to the survival.
Contraprepared: These are responses, which arecontrary to the persons’ natural tendencies, forexample, fears.
These findings seem to suggest that as humanbeings, we are prepared to acquire fears of somestimuli, e.g. snakes, lizards, etc. but not others,e.g. houses, flowers. This possibility is also seenin clinical practice. While individuals come forhelp in over-coming fears of some animals,objects and situations, but not on others.
Principles of Learning
Learning is primarily controlled by the learner.It is unique and individual. It is affected by the

42 Behavioural Sciences in Medical Practice
total state of the learner. It can be cooperativeand collaborative, it is an evolutionary process.It is a consequence of experience and is notdirectly observable. There are four principles oflearning:
Individuality of the Learner
Each learner is a unique individual in terms ofthe style of learning and rate of learning.However, given adequate time and flexibility inapproach all individuals can attain required levelof competence.
All Learning is Contextual
Learning takes place when a person ‘interacts’with a problem/situation, and ‘processes’information in the light of his/her own previouslearning and experience. By providing real lifeexperience or using simulated situation, learningcan be made more meaningful. Participatorytraining techniques, in which the trainee activelyparticipates in the learning process, should beused, such as group discussions, case studies,demonstration, role play, games, exercises,projects, field work, etc. New learning shouldbe built on the previous experience of thetrainees. Asking questions about previouslearning, not only activates the learner, but alsohelps in proper understanding of the subject.
Role of Motivation
Motivation holds the key for all learning.Motivation depends upon the needs felt by theindividual, which varies from individual-to-individual, and from one situation to the other.However, one can make following generalisa-tions regarding the factors motivating an adultlearner:• Physiological needs: (self-preservation/
existence, hunger, sex)• Security: job security, living conditions, etc.• Social status: recognition, fellow feeling
• Esteem: ego fulfillment• Self-actualisation: working for the sake of
excellence.These are organised in a hierarchical manner.
Unless the lower level need is met, the higherones usually do not operate; e.g. an under-paidnursing orderly is more concerned about his pay,perks and making living. A doctor whose suchneeds are fulfilled might work for esteem orrecognition.
Positive reinforcement of the correct responsein course of learning greatly facilitates learning.The reinforcement could be in the form of verbalresponse (e.g. excellent, fantastic, ideal, that isgreat, etc.); it could be a nonverbal gesture (e.g.a pat, or a smile, etc.). Rewards have a positiveeffect on motivation and the punishment hasnegative influence. While promotion, higher pay,perks, awards medals, etc. represent extrinsicform of motivation; self-satisfaction, working forsake of work, pursuit of excellence representintrinsic motivation. Intrinsic motivation lastslonger than extrinsic motivation.
Motivation is heightened, when a person hasclear idea of the ‘goals’, and when he perceivesvalue of reaching the goal. If the goal is not clearor not achievable at all, a person is not likelyto put in efforts. Adult learners always think: isit worth pursuing? What do I get out of it? Doesthis task help in any way in my present or futurejob performance? The extent to which the answeris ‘yes’, the person is likely to put in effort. If thegoal is not clear or not achievable at all, a personis not likely to put in efforts.
Motivation calls for a ‘nonthreatening’environment in learning. Though learning is acognitive activity, it is also an emotionalexperience. People learn when they are happy,cheerful. The training atmosphere must becordial. The attitude of the trainer to a large extentdetermines this factor. A democratic and friendlytrainer is more effective than an authoritarian,conservative trainer.

Learning and Studying 43
Feedback
Learning is very much facilitated, when indivi-duals are helped to set the goals and givencontinuous feedback on their progress. Theknowledge of success or failure includes not onlythe extent of achievement or failure, but also thelogic and the cause of failure. Successfulperformance of tasks increases confidence, whichagain breeds success. The failure may either leadto frustration or may enthuse the person to takealternate approach leading to success.
How is Learning Facilitated?
Over the last few years, research studies havebeen focussed on how students learn. Learningprocess is influenced by a host of factors suchas ability to concentrate, memory, organisationof learning material. Some of the students havedifficulties with their studies, arising not just fromlack of application or psychosocial problems, butfrom specific problems with the way they studyand learn. There seems little doubt that goodstudy skills contribute to academic success. Withthe skills, the student should have a positiveattitude and motivation to the subject. It is veryimportant to organise the time and resourcesavailable to the learner. Here are some tips bywhich you can learn more effectively.
Definite Goal
In any learning, student should have clear goalin view, as with a goal in mind, one works towardsa definite and sure purpose. Students should getspecific, immediate and achievable goals, as theyenhance your motivation to learn and ensurebetter learning.
Knowledge of Results orPsychological Feedback
The learner must also have conscious assu-rance that he is making progress towards his
achievement. Frequent and regular review ofthe amount of progress being made toward thegoal, act as a strong motive to promotecontinuing effort on the part of the learner.
Distribution of Practice Periods
A number of experiments have demonstratedthose shorter practice periods are moreeconomical than longer periods, and whendistributed over several days; they yield betterreturns that when they are concentrated into asingle sitting.
Whole versus Part Method
Whether the entire topic should be learned allthe way through in each trial, or by breakingit into small portions and learning in turns? Theformer is known as whole method and latter aspart method. With easy units, whole methodshould be adopted. If material is difficult inrelation to the learner’s ability, smaller unitsshould be learnt; but they still are as large wholesas a learner can manage efficiently. Try to learnin natural units.
Logical Learning
This means that instead of learning by heart,rote memorisation, you should try to graspmeaning and idea of the text. Logical learningcalls for an arrangement and assimilation withother ideas in mind.
Rest Pauses
Take brief rest pauses in between your studiesas mental fatigue blocks your ability to rememberand think.
Avoid undue Anxiety
Worry, apprehension or nervousness interfereswith good performance. Forgetting is more instate of anxiety.

44 Behavioural Sciences in Medical Practice
Rhyming
To improve memory, rhyming can be helpful,as it is well known that certain kind of material(poems Vs. prose) can be learnt better byrhyming.
Rational use of Media
When information is given through multiplechannels (viz. audio and visual), it makes strongermemory traces. Moreover, in medical education,the students need to understand and developability to see relationship among various topics.With the use of media (e.g. video films of self-instructional programmes), a learner can gothrough the material at his own pace.
Overlearning
Continuing repetitions of stimulus responselearning, even after 100% reproductions, helpretain learned material over a longer period oftime.
Reading Aloud
Better learning can be ensured at times withreading aloud than silent reading, especially ifone has habit to get into day dreaming. Thismethod of learning can be applied to manyclinical situations like treatment of speechdisorders.
LEARNING STYLES
Kirti studies day and night, yet barely managesto pass. Ravi can learn better through groupdiscussions, whereas Amit learns better by self-learning. These differences in learning reportedby these students as well as by some others,indicate that all students do not have the samemethod of learning. They have differentmethods of reading, interpreting and coding theinformation. There are individual differences ina student’s ability to assimilate, retain and
reproduce at the required time. Often, theirstrategies or methods of processing informationare useful. However, some students may developpathological learning strategies.
Different students describe their learningexperience differently. Some students describelearning as the retention of knowledge achievedthrough repetition and recitation, while othersdescribe it as an interpretative process aimed atunderstanding reality. Several studies have ledto elucidation of the concept of learningstrategies.
How does Students Learn?
Every student implements a set of proceduresfor accomplishing learning. These proceduresdenote that learning strategies are determinedby student’s perception and personal attributes.Two basic approaches to learning have beenidentified, namely, the “surface” and the “deep”approach.
The students with surface approach tend tomemorise important parts of the text, from whichthey anticipate questions in assessment. Thelearning outcome is essentially a reproductionof the words from the textbook. Their focus ofattention is limited to the specific facts, ordisconnected information, which is rote, learned.Furthermore, the surface approach does notinclude perception of the holistic structure ofinformation, but instead atomises it intodisconnected bits and pieces that are memorisedthrough repetition. This means that studentstaking a surface approach fail to derive fullmeaning, including implications and connectionsfrom information they have gone through.
On the other hand, students with deepapproach try to understand the meaning of thematerials and relate it to previous knowledge,concepts and experiences. A deep approachinvolves perception of the holistic organisationof the material studied, organised in a hierarc-hical manner. A student using this approach is

Learning and Studying 45
able to extract the meaning from words, notfocussing on words as an end in themselves. Thelearner is sensitive to relationships among topicsand to the structure.
A medical student needs to have a versatileapproach. He should be able to use both deepas well as surface approaches as required, fora particular learning task. It is also important thathe looks for the meaning and comprehends thelearning material. In a study at AIIMS, it has beenobserved that in the 1st semester, undergraduatestudents adopt the surface approach. But by thetime they reach the 7th, 8th semester, theirapproach changes towards deep. This changeis linked to the demands of the curriculumassessment, teaching style and learningenvironment (Fig. 5.4).
Fig. 5.4: Factors affecting learning outcome
Student Autonomy
Medical students ultimately need to become moreeffective learners, to enable themselves torespond to the variety of situations faced by themduring their medical profession. A medicalstudent learns a great deal on his own pace.Student autonomy refers to student indepen-dence and responsibility with regard to hislearning. A medical student needs to develop anability to decide which areas of study require
more focus than others, and also which type ofapproach should be used in learning specific skillsor subject matter.
Ability to think independently can be pro-moted by developing certain skills like choos-ing, deciding, deliberating, reflecting planningand judging. Cognitive and emotional develop-ment of the students also have a bearing on thedevelopment, which leads to increasing differen-tiation of perceptual categories revealing theuniqueness of events. On the emotional side,self-esteem and self-confidence in the studenthelps in the development of autonomy.
Skills Requisites of anAutonomous Learner
Autonomy in learning does not come naturallyto all students; it is a capability, which needs tobe developed. If the student is exposed to theautonomous methods of learning withoutinternalising the values of autonomy, then it willnot result in the change of his approach. To bean autonomous student, one needs to have anability and willingness to approach a situationwith an open mind, to suspend critical judge-ment, and to act in accordance with rules andprinciples which are the product of the autono-mous person’s own endeavours and expe-riences.
Certain attributes of an autonomous learnerneed to be inculcated, in order to be an effectivelearner in higher education. The most impor-tant characteristic is that students should takeresponsibility for their own learning. Followingare some steps to initiate autonomous learningin medical students (Table 5.2).
Table 5.2: Steps in autonomous learning
• Identifying learning needs• Setting goals and planning learning activities• Finding resource learning material• Conjuring up problems to tackle• Using teachers as guide• Undertaking additional nonteacher guidance• Self-assessment and reflection on their learning process

46 Behavioural Sciences in Medical Practice
In the setting of medical education, autonomousapproaches to learning are of great relevance.One such approach is in the form of problem-based learning. The basic idea here is that thestarting point for learning should be a problem,a query or a puzzle that the learner wishes tosolve. Organized forms of knowledge andacademic disciplines should be introduced,when the demands of the problems requirethem.
Role of Teachers in Facilitating Learning
The teachers should help the students to beautonomous learners. This can be achieved byguiding them to learn to focus in meanings ofthe contents. This can also be achieved by usingadvance organizers. Prior to teaching a newtopic, the student goes through the main pointsof the study and gets a clearer idea of the subject.According to Ramsden, the factors influencinginclude teaching methods, the degree ofenthusiasm/commitment of the teachers, thestructure, pace and the level at which informationis presented. The teachers need to provideopportunities for students to learn in a way, whichsuits the students preferred style of learning. Thus,teachers have an important role in helpingstudents to learn successfully, control theircognitive processes, including learning to learn,to remember and to think.
But a student has a major responsibility inlearning by developing skills to use learningstrategies judiciously according to the topic, anddevelop motivation to learn and to handle hisemotions.
Clinical Applications of Learning
Learning is fundamental to the development andmodification of behaviour; knowledge con-cerning the process may be usefully applied tomany clinical situations, not only for the patientsbut also for the students and professionals. Many
of our subjective feelings, emotions and attitudesare probably conditioned responses. Throughgeneralisation, it becomes difficult to identify theorigin of our emotional responses. Both ouradaptive emotional responses as well asunadaptive responses are learned and can beunlearned through principle of learning.
Behaviour modification or behaviour therapyis a group of techniques commonly used in thetreatment of various psychiatric disorders, andin the training of mentally handicapped children.Cognitive learning methods are also applied inclinical settings.
Learning methods have wide applications ineducational setting. In programmed learning, thematerial to be learned is broken up into smalleasy steps, so that the learner can accomplishwithout frustrations. Also with programmedlearning, learner can master the task at his ownpace. With versatile and flexible learning youcan improve your learning style. Use ofreinforcement principles can often, increaseproductivity, both in studies as well as in vocation.
The principles of operant conditioning havealso been applied to various clinical problems.One example concerns the attempt to improvethe social behaviour of long-stay patients inpsychiatric hospitals.
Other conditions of clinical interest, whereoperant conditioning principles may beimportant—both in causation and treatment—are those disorders of behaviour, for example,excessive gambling, smoking, over eating andaddictions. These behaviours are maladaptive inthe sense of being harmful to the individual, yetbecome habitual. Other examples of maladaptivebehaviour familiar to general medicine areabnormal illness behaviour, and noncomplianceof treatment, can also be modified usingbehavioural techniques.
Learning theories have not only been appliedto clinical problems of patients, but have alsobeen applied in development of techniques to

Learning and Studying 47
acquire clinical skills by health professionals.Some of these skills are related to interpersonalrelationships. These skills are required for‘bedside’ examination of patients, dealing withfamily members of the patients, and withcolleagues, seniors and junior staff. Althoughpersonality differences may contribute tovariation in this respect, clinical skills have to bedeveloped through the process of learning.Many of such skills are learnt through imitation,modelling and role-playing.
There are certain disorders in whichindividual’s ability to acquire new informationis impaired (e.g. clouded consciousness,dementia). There are psychological tests to detectand measure the extent of impairment oflearning. These are generally based on speedwith which new material can be learned by thepatient.
SUMMARY
Learning is defined as any relatively permanentchange in behaviour that occurs as a result ofpractice or experience. Methods of learning areclassified as: classical conditioning, operantconditioning, cognitive learning and sociallearning, observational learning, latent learningand biological learning. In classical conditioning,a neutral stimulus CS is presented before theunconditioned stimulus (US), that evokes anunconditioned response (UR). As a result ofassociation, the previously neutral stimulusbegins to elicit a conditioned response (CR). Inoperant conditioning, an action of the learneris instrumental in bringing about a change in
the environment that makes the action more orless likely to occur again in the future.Reinforcement is basic in this form of learning.Cognitive learning refers to changes in the wayinformation is processed as a result of experiencea person has had. Insight learning and signlearning are examples of cognitive learning.Social learning emphasises the role ofobservation, imitation and modelling in learning.Biological learning places emphasis on differencesin the capability of individuals. There are fourprinciples of learning, namely, individualdifferences in the learner, all learning iscontextual, motivation and feedback is importantfor learning to progress. Learning can befacilitated by defining a definite goal, givingfeedback, spacing your study time, learning unitsize that is easily grasped, understanding thematerial rather than rote learning and byavoiding anxiety.
There are different learning styles used bythe students. These are surface, deep andversatile; these learning styles also influence thelearning outcome. In medical education, thestudents need to adopt their own autonomousapproaches to learning. Teachers and educationenvironment play a crucial role in helpingstudents to develop the learning styles.
Clinical applications of learning are relatedto development of phobias, depression andother maladaptive behaviours. Behaviourtherapy, social skills training and cognitivetherapy are offshoot of learning theories.Learning pathologies cause failure and learningstyles determine the learning outcome. Thusfaulty learning styles can be modified.

6Intelligence
Ramesh had recently celebrated his fifth birthday.His joyous parents got him admitted in a publicschool. Ramesh enthusiastically started going tothe school. He had made one friend in his class.Gradually, Ramesh’s mother got complaints fromthe teachers that he was NOT able to cope upwith the task in the class, which other childrenwere doing quite well. His parents startedteaching the child at home, and also arrangedan extra tuition class for him after the schoolhours. Yet Ramesh was either making too manyspelling mistakes, or was not able to memorise,his handwriting was also very poor. Ramesh wasno longer keen to go to the school. Ramesh’sparents were advised to get his intelligenceassessed. On standardised intelligence testRamesh got a score of 70, borderline intelligence.He was advised admission in a special schoolfor slow learners. Ramesh’s parents could notjudge his intelligence because it cannot beobserved like height or weight, it can only beinferred from behaviour.
Intelligence as a concept is used verycommonly in our day-to-day life. We often makecomments that this person seems to be veryintelligent or seems to be dull. But what is thisintelligence? Different people would give differentmeaning to intelligence. Similarly psychologistshave attributed a variety of factors to the conceptof intelligence.
Definition
Most commonly accepted view is that intelligenceis a general capacity for comprehension andreasoning that manifests itself in various ways.The most widely accepted definition is,“Intelligence is the global capacity of an indivi-dual to act purposefully, to think rationally andto deal effectively with his environment”(Weschler 1944). It includes the power ofadaptation of an individual to his milieu, hisability to learn and for abstract thinking.
Difference between Intelligenceand Aptitude
A distinction has to be made between intelligenceand aptitude. Intelligence is the capacity or thepotentiality that a person has, whereas aptitudeis a combination of characteristics indicative ofan individual’s capacity to acquire some specificknowledge, or skill. Aptitude means anindividual’s aptitude for a given type of activity,the capacity to acquire proficiency underappropriate conditions.
Nature of Intelligence
Different theories have been proposed tounderstand the nature of intelligence.

Intelligence 49
Two Factor Theory
Charles Spearman (1927) proposed thatindividuals possess general intelligence factor (G)in varying amounts (degree). This determinesthe individual’s overall ability. In addition to G,individuals also possess specific abilities, (S) Gis universal inborn ability, and it is general mentalenergy. The amount of ‘G’ differs from indivi-dual-to-individual. Higher the ‘G’ in anindividual, higher is the success in life. ‘S’ islearned and acquired in the environment, itvaries from activity-to-activity even in the sameindividual: the individuals themselves differ inthe amount of ‘S’ ability (Fig. 6.1).
Two individuals in a class may be comparableon their G factor, yet one may be very goodwith numbers while the other possesses highermusical ability.
Multifactor Theories
a. Thurstone (1936) felt that intelligence couldbe broken down into a number of primarymental abilities. He had derived 7 primarymental abilities on the basis of factor analy-ses. These abilities, as shown in the Table 6.1are represented in items in test construction.
b. Guilford has broadened the concept ofintelligence. According to him there are twotypes of thinking: (a) convergent thinking—solving a problem that has a defined correctanswer and (b) divergent thinking—arriving
at many possible solutions to a problem. Thisis predominantly creative thinking. Hehad proposed a three dimensional theoryrepresented in a cubical model shown inFigure 6.2. Guilford maintained that intelli-gence test items should distinguish in termsof the operations performed upon thecontent and the product that results. Thismodel provides for 120 factors of intelligence,which is a combination yield of 4 contents,5 operations and 6 products. Assume thata subject is asked to rearrange jumble ofwords, e.g. CEIV, NERTE, to form a familiarwords (VICE, ENTER). The content issymbolic; since the test involves a set of lettersymbols; the operation is ‘cognition’ becauseit requires recognition of information and theproduct unit is a word.
Process Oriented Theories
These theories have focussed on intellectualprocesses—the pattern of thinking that peopleuse when they reason and solve problems. Thesetheorists prefer to use the term cognitiveprocesses in place of intelligence. They are oftenmore interested in how people solve problemsand how many get the right solution. They havefocussed on the development of cognitiveabilities. Piaget’s work is a significant contributionin this area (see Chapter 12). He viewedintelligence as an adaptive process that involvesinterplay of biological maturation and interactionwith environment.Fig. 6.1: Two factor theory
Table 6.1: Primary mental abilities
Ability Description
Verbal comprehension Understanding meaning of words.Word fluency Ability to think rapidlyNumber Perform calculationsSpace Visualise space form relationshipMemory Recall verbal stimuliPerceptual speed Grasp of visual detailsReasoning Ability to find a general rule,
logical thinking.

50 Behavioural Sciences in Medical Practice
Information Processing Theories
These theories break intelligence down intovarious basic skills that people employ to takein information, process it, and then use it toreason and solve problems. These basic skills maybe simple or complex. Robert Sternberg (1984),distinguishes between information processing“components” and “metacomponents”. Com-ponents are the steps to solve a problem andmetacomponents are the basics of knowledgethat one has to know to solve the problem. Theinformation processing theory has often beencompared with computers in which attention andmemory have been designated as the intellectualhardware whereas the action schemes (Piagetiannotion) are similar to specific, repeatableintellectual sequences, and executive schemes,similar to plans and strategies. The neo Piagetiansare of the opinion that people’s softwarebecomes more sophisticated as they mature,with their schemes expanding in complexity andtheir amount of available mental energy
increasing. Such changes in their view, promotethe growth of intelligence. Other approachesfocus on the rules involved in intelligentbehaviour or the skills required for various tasks.
Hebb (1966) has distinguished two meaningsof intelligence on neurological basis. IntelligenceA is the innate potential based on the develop-mental process. This type of intelligence isdependent upon ‘the possession of a good brainand a good neural metabolism’. Intelligence Binvolves the functioning of the brain, and isobservable indirectly from the individual’sbehaviour. Intelligence A is not observable andcannot be measured, whereas intelligence B ismeasured through tests.
Cattell (1971) on the basis of factor analysis,has divided general factor of intelligence (G) intotwo parts—fluid intelligence (GF) and crystallisedintelligence (GC). The former being innate,biologically or genetically determined and thelatter is acquired based on cultural andeducational experience. Fluid intelligence isrelated to ability to solve problems, thus isassessed on intelligence test like block design teston progressive matrices. Crystallised knowledgethus is measured on tests of information,arithmetic and vocabulary.
Eysenck (1973) distinguishes between speedand power components of intelligence. Speedis measured by the time required to completethe task and power is measured through test ofreasoning.
Jensen (1980) splits intelligence into twolevels. Associative ability being the capacity tolearn, remember and recall information. ltrepresents the lower level of continuum.Cognitive ability is concerned with reasoning andis located at the higher level. Cognitive abilitydepends upon associated ability but not viceversa.
Earl Hunt (1983) proposed that individualdifferences in intelligence are due to the differentprocesses people use in solving problems. Huntidentifies these ways of cognitive processes that
Fig. 6.2: Guilford’s model of intelligence

Intelligence 51
makes difference in people. These are: (1) wayto internally represent a problem, (2) strategiesfor manipulating mental representation and(3) abilities necessary to execute basic infor-mation processing steps, according to thestrategy requirement.
Howard Gardner (1983) has proposed seventypes of intelligence, each one of those isimportant. The seven intelligences identified byGardner are—1. Linguistic ability2. Logical-mathematical ability3. Spatial ability (navigating in space, using
mental images)4. Musical ability5. Bodily-kinesthetic ability6. Interpersonal ability (understanding others)7. Intrapersonal ability (understanding oneself).
Robert Sternberg (1986) has suggestedtriarchic (three points of origin) components inintelligence—in this knowledge acquisition,performance and metacognition is for learningnew facts, for problem solving strategies andtechniques for selecting a strategy andmonitoring process towards success. Accordingto Sternberg individuals can improve theirexperimental, contextual intelligence andcomponential intelligence by practice and effort.
Emotional Intelligence (EI)
Emotional intelligence refers to the way wehandle the each other and ourselves. PeterSalovey and John Mayer (1990) coined the termemotional intelligence. Later Daniel Goleman(1995) did extensive work on the concept ofemotional intelligence. Though personalintelligence is important for academic abilities yetemotional intelligence contributes towards abalanced personality. Emotional intelligencehelps ‘to be angry with a right person, to the rightdegree, at the right time, for the right purposeand in the right way’ (Aristotle). The compe-tencies of the emotional intelligence are crucial
for success in work and in interpersonalrelationships. It trains people to manage emotionsand develop to skills to handle relationships. Thefive domains of emotional intelligence are—• Knowing one’s emotions• Managing emotions• Motivating oneself• Recognising emotions in others• Handling relationships.
It is feasible to enhance emotional intelligencethrough training. Currently attempts are beingmade to include training in emotional intelligencein the school curriculum.
Intelligence Quotient (IQ)
IQ is a commonly used term, which was firstsuggested by Stern and Kuplmann in 1912. Onindividuals, Intelligence quotient is expressed asa ratio of mental age (MA) to the chronologicalage (CA).
MAIQ = __________ × 100
CA
The ratio is multiplied by 100 to remove thedecimal. If the child has an average mental age,then a correlation of his mental age (MA) andthe chronological age (CA) will form a straightline. In case the individual’s mental age (MA)is higher than the chronological age (CA) thenthe curve will be different as shown in Figure6.3.
An individual with an average intelligence hasan IQ of 100. If the mental development fallsbehind the individual will have an IQ less than100 and if the rate of development is faster theindividual will have an IQ more than 100. If twochildren six and eight years old obtain a MA ofseven years on an intelligence test then theyounger child has a higher intellect.
MA 7If Child - A __________ × 100 = 88
CA 8
MA 7Child - B __________ × 100 = 117
CA 6

52 Behavioural Sciences in Medical Practice
Fig. 6.3: Correlation of mental ageand chronological age
Child A with an IQ of 88 is dull in compari-son to child B who has superior intelligence withan IQ of 117. Descriptive terms are also appliedto individuals whose intelligence test scores fallwithin the various bands under the normal curve(Atkinson et al. 1993). These are given in Table6.2.
Table 6.2: Classification of IQ scores
IQ score Descriptive term
130+ Very superior120–129 Superior110–119 Bright normal90–109 Normal80–89 Low normal70–79 Borderline50>~ 69 Mild mental subnormal35–49 Moderate mental subnormal20–34 Severe mental subnormal0–19 Profound
These terms are used into determine whatlevel of remedial treatment or care is requiredby those with mental subnormality.
Growth of Intelligence
Generally the growth of intelligence is rapidduring early childhood and then slows down in
teens (Fig. 6.4). Longitudinal studies usingWechsler’s tests have shown that mental abilityincreases upto the age of twenty-six, after whichit levels off and remains unchanged till latethirties. There is a gradual decrease in the intel-lectual ability after forty with a sharp decline aftersixty. But it must be noted that decline in abilitydepends both on the person and the type ofability tested. Individuals engaged in activestimulating working environments with goodphysical health show little decrease in intellectualability upto age seventy. Physical disabilities,particularly those resulting from strokes orprogressive reduction of blood circulation to thebrain usually result in a significant decrease inintellectual ability.
Mental abilities that require speed and short-term memory decline earlier than generalknowledge. The rate of decline of specific abili-ties is related to one’s occupation, like peoplein literary work or professionals do not declinein mental ability as early as others. Experienceand accumulated knowledge compensates fordiminished speed in old age.
Fig. 6.4: Growth of intelligence

Intelligence 53
Stability of Intelligence
The stability of intelligence or IQ has receiveda great deal of attention from the educationalpsychologists because of its usefulness ineducation. There are two opinions. One holdsthat the IQ remains relatively stable over theyears changing only very slowly. Another opinionis that if determined effort is made, a changein IQ can be obtained. There is a considerableevidence to indicate that stability in IQ is notabsolute but only a small range of scores wouldchange.
An extensive body of data accumulated,shows that intelligence test performance is quitestable. Studies have reported high correlationsranging from .72 to .83 on retest of intelligencescales. Bradway, Thompon and Cravensconducted a follow up on children originallytested between the age of 2 and 5.5 years aspart of the 1937 Stanford Binet standardisationsample. Initial IQs correlated .65 with 10 yearsretests and .59 with 25 years retests. The corre-lation between 10-year retest mean age 14 yearsand mean age 29 years (25 year retest) was .85.If the initial assessment is done in late childhoodor after that then the correlations are found tobe very high. The instability of IQ may occuras a result of drastic environmental changes. Itcan increase with stimulation and training butcan decrease due to prolonged or severe illness,head injury, brain damage, high fevers, epilepsy,meningitis and adverse environmental factorslike conflict at home, death of parent,malnutrition. Instability of scores could also bedue to fast or slow development of the childthan that of the normative sample population.Generally children in continually disadvantagedenvironments tend to lose and those instimulating environments gain in IQ with age.The relationship between IQ, educationalattainment, and later occupational achievementis positive. Many highly intelligent peopleperform disappointingly, while many with
average IQ may do remarkably well. This isbecause factors other than intelligence, such asdrive, persistence, attention, useful socialcontacts, and highly-developed social skills, areof major importance in the achievement in laterlife.
Determinants of Intelligence
The question of relative importance of ‘nature’and ‘nurture’ as a determinant of intelligence hasbeen controversial. The role of genetics orheritability and environment has been exten-sively studied. Their comparative roles in deter-mining intelligence are as follows:
Heredity
Evidence pointing to the influence of heredityon intelligence comes mainly from family andthe twin studies. A heritability index shows theproportional contribution of genetic or heredityfactors of a particular trait in a given populationunder existing conditions. A frequent procedureto compute heritability index is to utilise intelli-gence test correlations of monozygotic (identical)and dizygotic (fraternal) twins. Correlationsbetween monozygotic twins reared together andbetween monozygotic twins reared apart in thefoster homes, have also been used. Table 6.3summarises the results of a large number ofstudies (Bouchard et al 1990), indicating thatcloser the genetic relationship, the more similaris the tested intelligence.
Table 6.3: Correlation of intelligencewith heredity
Relationship Correlation
Parents and natural children .40Parents and adopted children .31Dizygotic twin .60Monozygotic twin
Reared together .86Reared apart .72
Cousins .15

54 Behavioural Sciences in Medical Practice
Heritability estimates for intelligence haveranged from .40 to .86. The lower estimate isbased on the assumption that a sizeable portionof variation in IQ scores can be attributed to agenetic environmental covariation. Parents caninfluence their offspring both by direct genetictransmission and by the kind of environmentthey provide.
EnvironmentEven though intelligence has a significant gene-tic component, environmental conditions canalso be crucially important. The influence of theenvironment begins from the moment of con-ception. The development of the foetus, espe-cially at critical times, may be affected by variousphysical factors including mother’s diet, smoking,disease such as rubella and certain drugs.Subsequent environment especially duringchildhood, socioeconomic status, nutrition,health and educational influences of the familyare very important determinants of IQ.
It has been recognised that children fromlower social class families generally perform lesswell on intelligence tests than those from highersocial classes. Studies of family influences suggestthat greater parental attention received bychildren of smaller families and the first-born mayresult in higher scores. The use of media andthe educational toys provide the rightenvironment for intellectual stimulation. Similarlyurban and rural set up, type of school attendedlead to differential stimulation and type ofexperience which in turn affects the intelligencescores. Effect of education not only influencesthe test scores, but teacher’s expectation mayspeed up or slow down the development ofindividual child.
One of the most convincing evidence for theinfluence of the environment comes from suc-cessful attempts, through intensive stimulationand education, to improve the IQs in high-riskchildren and mentally handicapped. Similarly IQ
scores have been found to increase, whenchildren are transferred from poor institutionsto good foster homes.
To sum up, both heredity and environmentplay an important role in determining intelli-gence. These can be compared to land and seedsused to grow crop. Seed is like heredity and theland is like environment. If the land is not fertile,then even with good seed one cannot have agood crop. Similarly with a fertile land if poorquality seeds are used, the crop will not achievegood results. Thus just as for good crop, bothfertile land and good quality seeds arerequired, similarly both heredity and stimulatingenvironments are required for higher intelli-gence.
Extremes of Intelligence
Mental Subnormality
Mental subnormality refers to subaveragegeneral intellectual functioning, which originatesin the developmental period and is associatedwith impairment in adaptive behaviour. A personis regarded as mentally subnormal if: (i) the IQattained is below 70 on standard psychologicaltests of intelligence; (ii) their adaptive skills areinadequate to cope up with the daily routines.Adaptation skills are those behaviours by whichan individual makes adjustments and indepen-dent living in the society. In childhood these arethe self help activities such as eating and dressingindependently. Later on the adaptive behavioursare concerned with basic academic skills, copingskills such as telling time, using money andassuming social responsibilities. Slowness inintellectual development may be widespread andaffect all aspects of cognition. Only rarely willa child’s functioning be retarded to the samedegree over the entire range of skills, but wheresuch skills are significantly impaired, it isreasonable to think of the child as showinggeneral mental subnormality.

Intelligence 55
In our country the problem of mental sub-normality is quite significant. The studies haveshown an incidence of 4-5 per 1000 individuals.Mental subnormality is categorised in fourlevels—mild, moderate, severe and profound.Table 6.4 gives the characteristics of each of theselevels.
Clinical features: Mental subnormality may firstbe identified by delay in their motor milestonesin the first few months of life. The child will beslow to obtain head control, sit unsupported.Large number of moderately retarded childrenhowever, shows normal motor development andpresent for the first time with language delay.The child may be thought to be deaf becausehe fails to take notice of sounds or shows lackof single words or word combinations at theappropriate age. Mildly retarded children maynot be detected until they enter school whenfailure of educational progress may be foundto be due to a general slowness of developmentrather than to a specific learning disability. Usuallyhowever, it will be found that the early
development of the mildly retarded especiallytheir early language development has been slow.Occasionally mental retardation arises as a resultof some postnatal event, such as a head injuryor cerebral infection. In these cases the timecourse of the condition will, of course bedifferent.
Once diagnosed, the clinical features ofchildren with mental retardation will dependmore especially on:1. The severity of the condition2. The presence of associated physical and
psychiatric conditions3. The quality of care and education the child
receives.
Management: Management should begin withan explanation to the parents of the diagnosis,its probable cause, the way in which the childcan be helped, and the likely outcome. It isimportant to reassure parents that their beha-viour has not produced the condition, thoughthis does not mean that, in the future, there isnot much they can do to help the child.
Table 6.4: Characteristics of persons with various degrees of mental subnormality
Description Mild Moderate Severe
Preschool Can develop social and Can talk, learn to communicate: Poor motor development,0-5 yrs. communication skills, poor social awareness; fair motor speech minimal; general
minimal retardation in development, profits from training unable to profit fromsensory-motor areas, in self-help; can be managed self-help; little or nooften not distinguished with moderate supervision. communication skillsfrom normal until late age.
School age Can learn academic skills upto Can profit from training in social can talk or learn to6-20 yrs. approximately 6th grade level and occupational skills; unlikely communicate, can be trainedTraining and by late teens; can be guided to progress beyond 2nd grade elemental healthEducation toward social conformity level in academic subjects; may habits, profits from
learn to travel alone in systematic habit trainingfamiliar environment.
Adult Can usually achieve social and May achieve self-maintenance May contribute partially to21 and over vocational skills, adequate unskilled or semiskilled work self maintenance undersocial and to minimum self-support under sheltered conditions, complete supervision;vocational but may need guidance and needs supervision and guidance can develop self-protectionadequacy assistance when under unusual when under mild social or skills to a minimal
social or economic stress. economic stress. useful level in controlledenvironment.

56 Behavioural Sciences in Medical Practice
Retarded children take longer to learn newmaterial and once they have learned somethingnew, they usually forget more easily than thenormal. Consequently they need more help, andmore systematic help from parents, teachers, andother in the acquisition of skills. In particular,they often fail to learn by observation, andtherefore, need more structured teaching. Thehelp needs to be provided at an appropriatelevel for the child. It is useless to try and teachskills too far ahead of the child present mentalage. Parents play an important role in trainingthese children (also see Chapter 20).
In the preschool period the main role forprofessionals such as clinical psychologist, specialeducators, speech therapists, etc. is in helpingparents to find ways to stimulate their child’sdevelopment.
The Mentally Gifted
In distribution of intelligence, the right extremeof the bell-shaped curve represents the giftedor the genius (Fig. 6.5). These are the individualswith IQs of 140 or higher. About one out of every100 children has an IQ of 140-160. Less thanone out of every 1000 has an IQ above 160.In the early childhood, a gifted child is generallyfound to be misfit in his class because the level
of teaching in a normal classroom is for anaverage child, whereas the gifted child is ableto comprehend much faster. As a consequence,they often indulge in behavioural irregularities.They have been found to be gross under achie-vers and extremely unhappy. One problem seemsto be that such extremely bright children findthemselves intellectually misfit with children oftheir own age, and physically misfit with the olderpeople who are their intellectual equals. Butthings improve by adulthood and they appearto be happier and better adjusted than mostothers of their age. These days there are separateschools for the gifted children. With the righttype of training their superior potential ischannelised in constructive tasks.
Clinical Applications
Assessment (see Chapter 18) and understandingof intellectual functions is helpful in your clinicalwork as with this knowledge, you can diagnosea patient with mental subnormality or with verysuperior intelligence. Assessment of intelligenceis discussed in detail in Chapter 18. Yourexplanations or guidance to the patient wouldbe according to his intellectual level. In somediseases like neuropsychiatric disorders, epilepsy,and psychiatric disorders and in some of theendocrinological disorders, assessment ofintelligence is of great assistance in theirmanagement. Physical and/or mental ill healthmay temporarily impair intellectual performance.Distressing physical symptoms may obviouslyinterfere with mental concentration, while greatanxiety, deep depression or the thought disorderof schizophrenia may make it extremely difficultfor a patient to respond adequately to testmaterial.
The influence of motivation may be quiteprofound on performance on intelligence test.If the individual sees no relevance of the intelli-gence testing to his current situation or prob-lems he may make little attempt to cooperateFig. 6.5: Normal distribution of intelligence

Intelligence 57
with the tasks involved, and may then achievea much lower score than would have been thecase if he had been more highly motivated.
It is generally organic disease affecting thefunctioning of the brain that is likely to impairintellectual performance; so that it is in the fieldof neuropsychiatry particularly that intelligencetesting may be of greatest assistance. Not onlymay there be evidence of a general falling offin intellectual functioning compared with anactual previous measurement, or an estimatebased on past educational or occupationalhistory, but more specific cognitive impairmentsmay indicate lesions of particular parts of thebrain.
The assessment of an individual’s intellectualabilities can be of value in other clinical situationswhere psychological problems may be arising inan educational or vocational context.
Knowledge of intellectual functioning is alsouseful for yourself as a student and later as ateacher. Teaching method, content of the subjectmatter and expectations from students shouldbe based on student’s intellectual functioning.
SUMMARY
Intelligence is not a unitary concept, it is a globalcapacity of an individual to act purposefully,comprehend and think rationally. Varioustheories have been put forth to understand thenature of intelligence. Different theories haveexplained nature of intelligence. According toSpearman, intelligence has two factors, generaland specific factors, the multifactor theories of
Thurstone, provides seven primary abilities.Guilford has classified structure of intelligencein products, contents and operations; their com-bination produces 120 factors of intelligence,Guilford has also made distinction betweenconvergent and divergent intelligence. Cattell hasclassified intelligence as fluid and crystallisedintelligence acknowledging role of heredity andenvironment. Gardner has advocated seventypes of intelligence. According to Sternberg,individuals can improve their experimental,contextual intelligence and componentialintelligence by practice and effort.
Emotional intelligence is a term used forability to control emotions and ability to handleinterpersonal relationship. EI is consideredimportant for success in later life. Scores are moreor less stable, as the test scores of the early yearshave been found to correlate highly with thescores obtained in late adolescence. Heredity andenvironment both play an important role indetermining the intelligence.
Intelligence can be assessed through verbalor performance test. Intelligence quotient is theratio between mental age and chronological age.Average IQ scores range from 90 to 110(obtained on standard tests of intelligence).Those having an IQ below 70 are consideredas mentally subnormal, while those with an IQabove 160 are considered as mentally gifted.Knowledge of intellectual functioning and itsassessment, is of a great importance in clinicalpractice, especially in neuropsychiatry, psychiatry,endocrinology and paediatrics.

7Thinking
Imagine yourself examining a patient in theemergency ward with an unusual to plan sometreatment strategy immediately because if youdo not deteriorate fast and he may even die.There is no other doctor in the casualty so youhave to think, plan and start the treatment entirelyon your own. Similarly, you can take anothersituation where you are driving home late in thenight. You see a big crowd on the road due tosome accident. Being a doctor you stop the carand go near the site of the accident. You findthat the victim is lying in a pool of blood. Whatshould you do? How should you do? Thesewould be the common questions coming to yourmind. You arrive at the solution for theseproblems based on thinking process.
Definition
Thinking is the mental activity that makes humanbehaviour complex and fascinating. It is somekind of ongoing mental activity with internalrepresentation of the outside world of which thesubject is aware but which is unobservable byanother person. It must be inferred from thebehaviour of the individual. It may or may nothave been induced by an external stimulus andit may or may not result in some psychologistdefine thinking as a response to any stimuli.According to them thinking is more complicatedthan responding. For example, a mathematicalproblem at times can be solved by two different
methods, with the same result. So thinking isnot responding but a process by which onearrives at the solutions. These processes ofsolving problems can be different in differentindividuals and different situations.
Human thought process is like informationprocessing sequences, building from basicinformation such as pattern recognition andperceptual analysis. Thinking is mental processof forming a new representation by transformingavailable information. Thinking involves atten-tion, memory, reasoning, imagination, decisionmaking and judging. Thinking has three charac-teristics—• Thinking occurs in the mind but is inferred
from observable behaviour.• Thinking is a process that manipulates
knowledge in a person’s cognitive system.• Thinking is directed toward finding solutions
to problems facing the individual (Mayer,1981).
How do we Think?We store information from our experience withpeople and things; we make mental representa-tion of these experiences in our minds. At timeswe generalise our experiences like learning isbetter early in the morning, all students whowear spectacles are studious. Thinking relies ona variety of mental structures to form a thought.These are symbols, concept, schema, imagery,cognitive maps and language.

Thinking 59
Symbols
Thinking has also been defined as themanipulation of symbols. Symbol is an objectthat can represent other objects. For example,a triangle can represent family planning or ×in a mathematical equation can stand formultiplication. Thus the red triangle and × aresymbols. Though words form important symbolsin our thinking, yet symbols are not limited tothe familiar language of words. There are othersymbolic languages, such as language ofmathematics; Tangible symbols include suchsymbols as a stop sign, a cross on the church,a red cross on the ambulance. We think insymbols as verbal language is a rich symbolicprocess. A symbol conveys a meaning, it providesinformation about some object or event to whichit refers and thereby suggests appropriate actionto the persons who perceives it. Symbolic stimuliproduce reactions appropriate to some stimulusother than themselves, e.g. sign DANGER alertssomeone to take necessary action. Thoughthinking is private and invisible yet we can studythe result of simple manipulation and then workbackwards making guesses about what kind ofsymbols might have been manipulated and abouthow this manipulation is performed. The studyof the process of thinking is dependent uponintrospection and verbal report by the subject.
Concepts
When symbol stands for a class or group ofobjects with common properties, it refers to aconcept, like green, women, injection. Conceptsare labels one gives to a group of objects; it isthe organisation of a variety of different objectsor events into categories. Some concepts caneasily be formed as they are basic, whereas otherconcepts are difficult to form. Concept learningis based on principles of generalisation anddiscrimination (see Chapter 5). A child learningthe concept of dog may generalise all small
animals as dog. Later with parental correctionand with personal experience the child is ableto discriminate dog from other small animals.Language ability helps us to form concepts fromconcrete to the abstract ones. Piaget’s stages ofintellectual development indicate that the childfirst learns object concepts and develops moreabstract concepts only as he grows older (seeChapter 12). The inability to form abstractsis characteristic of certain disorders like,schizophrenia, mental subnormality and someneurological disorders. Normal individuals havecapacity to treat new stimuli as familiar andremembered categories. This ability to categoriseindividual experiences is regarded as one of themost basic abilities of thinking organisms (Mervisand Rosch, 1981).
Psychologist have identified a level in concepthierarchies at which people best categories andthink about objects. The basic level can beretrieved from memory, e.g. chair is identifiedas piece of furniture. The basic levels of conceptsare the fundamental of thought.
Schemas
Schemas are general conceptual frameworksregarding certain people objects and situationsone’s life. You correlate ‘exams’ with studyingmost of the time, anxiety to finish the course,lots of books and cutting down on social activities.This visual representation provides expectationabout the features likely to be found in a particularsituation. Whenever incomplete or ambiguousinformation is available, we make inferences.Schemas are the primary units of meaning inthe human information processing systems. Wecomprehend new information by integratingnew inputs and what we already know.
We also have schemas of events; these arereferred to as script. A script is a cluster ofknowledge about sequences of interrelated,specific events and actions expected to occur ina certain way in particular settings. We have a

60 Behavioural Sciences in Medical Practice
script for going to a picnic, traveling in train,making presentations. Scripts may depend uponthe culture, e.g. traveling in train in India isdifferent from traveling in train in Japan.
Imagery
Supposing you have joined a hostel and youhave an empty room. You are supposed toarrange the room. What will you do? How willyou plan the places for your things like bed, studytable, books, music system and other accessories?For this you need an imagery to plan thearrangement and setting of your things. Imageryis the mental picture which is usually notcomplete. Imagery is an important tool forsolving many problems. Mental imagery is theability, which varies between individuals, toexperience ‘internally’ something resembling butnot identical with a percept, visual, auditory,olfactory, etc. These mental images may bememories of previous events, scenes, etc. orapparently original as, for example, in the caseof some creative artists. The ability to experiencevivid and details images which are then projectedinto the environment and perceived as if externalis known as eidetic imagery. The images mayoccur spontaneously in some situations, whileon other occasions they may result from aconscious effort on the part of the individual.These may be referred to as autonomous andcontrolled imagery respectively. This differencemay be extended to all thinking so that adistinction is made between what may bedescribed as purposive and fantasy thinking—the difference depending essentially on thedegree of control exercised by the thinker.
Cognitive Maps
A cognitive representation of a physical spaceis called a cognitive map. These are internal mapsthat guide future actions towards desired goals.Cognitive maps help people to visualise a
situation like one draws a visual route to reacha particular destination. Visual thought and verbalthought differ in the ways information isprocessed and stored. Visual thought increasescomplexity and richness to our thinking. Visualthinking can be useful in solving problems relatedto special or geographical relationship.
Culture influences the cognitive maps dueto the subjective impression of physical reality.The maps often mirror our personal or culturallyegocentric perspective. If you are asked to drawa female figure that would be different in featuresand dress as compared to a figure drawn by anAmerican.
Language
Thinking involves the manipulation of internalor covered representations of external and overtevents or behaviour, but that is because of theexistence of language. Language serves twomajor functions, it helps us to communicate withone another and it provides system of symbolsand rules that facilitate thinking. Language likeany other external behaviour may be representedinternally, and much human thinking involves akind of internal speech. There are also manyexamples of nonlinguistic thought as whencomposer ‘hears’ in his mind music that he iscreating or an artist ‘sees’ a painting he will puton to canvas.
Neurological Basis of Thinking
Luria, the Russian psychologist, on the basis ofstudies of children, has regarded the inter-nalisation of speech as the major factor in thedevelopment of thinking. He has also shown thatpatients with lesions of the frontal lobes maysuffer from loss of speech control as well as moregeneral disorganisation of behaviour, andpresumably of the thinking process underlyingit. Milner (1963) has also found that frontal lobepatients show impairment on a card-sorting task
Thinking 61
in which cards can be categorised in terms ofcolour, form of number. If the principle waschanged (e.g. from form to colour), the patientscontinued to sort cards according to the originalprinciple, showing preservation of behaviour.There are also other disturbances associated withfrontal lobe damage, including motivationaldeficit, so that the association of frontal lobe andthe process of thinking can only be regarded astentative.
Types of Thinking
Thinking has been classified in number of ways.Some of the important types of thinking arediscussed here.
Purposive and Fantasy Thinking
Our thought can go to extremes from purposive,realistic thinking to fantasy or autistic thinking.Autistic thinking is a personal, idiosyncraticinvolving fantasy day dreaming being in yourown world. This type of indivisualised thoughtscan be important for creative acts. But in extremecases it can be abnormal as it generates delusionsand hallucinations. Realistic thinking is logical,takes account of external reality and, clearly, isinvolved in reasoning and problem-solving.Autistic thinking in contrast, is primitive, non-logical in its association of ideas and is not subjectto correction by reference to reality.
Convergent and Divergent Thinking
Another dichotomy between two forms ofpurposive thinking as suggested by Guilford(1956) and later developed by Hudson (1966).Convergent thinking applies to problem solvingwhich involves focussing on to the one and onlycorrect answer—the sort of problem that hascommonly been used in conventional tests ofintelligence (e.g. ‘fat is to think as tall is to …..?)Divergent thinking requires the production ofas many answers as possible (e.g. ‘how many
uses can you think of for a flower pot?) and hasbeen considered to be important in relation tocreativity.
Functions of Thinking
Thinking has various functions that help us inour day-to-day activities requiring reasoning,problem solving, and decision making andjudging.
Reasoning
Reasoning is a process of realistic, goal directedthinking in which conclusions are drawn froma set of facts. In reasoning information both storedand collected from the environment are usedaccording to the set rules. Reasoning is classifiedas deductive and inductive.
Deductive reasoning involves drawing aconclusion that follows logically established rulesfrom two or more statements. Examples of thisreasoning is that A has high blood sugar, so hehas diabetes.
Inductive reasoning uses available evidenceto generate a conclusion about the likelihoodof something. For inductive reasoning oneconstructs a hypothesis based on availableevidence and then test it against other evidence.Inferences are accomplished by integratingpast experiences, weighted value of the impor-tance of the evidence and creativity. Examplesof this type of thinking are probing into a murdercase.
Most scientific reasoning is inductive as oftena medical diagnosis is made on the inferencesdrawn from the case history of the patient.Inductive reasoning plays a key role in our livesin solving many problems, like misplacing certainobject and then trying to find that.
Problem Solving
Problem solving is thinking that is directedtowards solving specific problems. This is the

62 Behavioural Sciences in Medical Practice
important part of our thinking that moves froman initial state to a goal state by means of a setof mental operations. Solving a problem impliesthat the organism is faced with a task the solutionto which is not immediately apparent, but whichit is able to solve after an interval during whichthe problem-solving activity including thinking orreasoning has occurred. In other words, problem-solving involves the acquisition of an appropriateresponse to a novel situation.
The ability to find an answer to the questionthat is to solve a problem is a cognitive abilitywhich has a goal. Goal can be achieved byvarious methods for which the psychologists haveexplained on the basis of different theories.These are—learning theory, Gestalt theory andinformation processing theory.
Learning theory : The learning theory approachto problem solving is illustrated by work of Pavlov,Watson, Thorndike. According to Thorndike thecats placed in the puzzle boxes learned to pullthe string that got them out of the trial and errorprocess. Here the cats were only learning a newhabit because of the reward and reinforcementof getting out of the box. The cats did notunderstand the mechanism of pulling the stringled to the escape.
Gestalt theory : The work of German psycho-logist Kohler (1927) is an example of Gestaltapproach where famous experiments of insightlearning were conducted on the chimpansee,Sultan. The bananas were placed outsideSultan’s cage, out of reach, and he was givena stick, he would use the stick to pull the bananasto him. Sultan’s problem occurred when neitherof the two sticks he had was long enough toreach the bananas. He tried to get the bananaswith one of the sticks but was not successful andwalked away. Suddenly, he went back and bychance combined the two sticks together, makea single long stick. With this he could immediatelyreach to the bananas. According to Kohler,
Sultan used insight which is often known as an‘aha’ experience. He came up with a completelynew creative solution to his problem which hecontinued to use in the similar situations.
The Gestalt approach to solving problem isbased on rearranging the situation to gain oninsight into its fundamental nature. Here is aproblem for you to answer.
These are nine sticks, try to make them tenwithout adding another stick
Problem-solving occurs through a process oftrial and error. You would have experiencedmany such incidents where the initial methodto solve the problem was based on trial and errorbut later on the solution comes through insight.It may come suddenly to your mind while youwere doing something different. The Gestalt viewof problem-solving, is a more holistic one.Instead of a solution proceeding gradually bysmall steps as proposed by Thorndike, the Gestaltschool considered that the problems are solvedefficiently when organised into a good structure.This is also called reproductive thinking as itduplicates or reproduces old habits. Theproductive thinking.
Information processing : According to thisapproach problem-solving is a complex activitycomprising several processes. These processesinclude—registering information, retrievinginformation from memory and using both kindsof knowledge in a purposeful way. The studyof information processing has grown along withthe use of computers and at times it has beenequated to artificial intelligence.

Thinking 63
Stages of problem-solving : Whenever you haveto solve a problem try to think what all isrequired. Supposing you have been asked tomake a research proposal, what necessary stepswould you take ? Generally, whenever they haveto solve a problem, we go through three hourstages, we prepare, we produce and weevaluate.
Preparation: The first step to problem solvingis to understand the problem as our inter-pretation can be affected by the way the problemis presented. At times, there is a problem of fixedor rigid mental set which can interfere inunderstanding and thereby working on theproblem.
Production: We need to generate possiblesolution. Simple problems may be solved justby collecting correct information either fromlong-term memory or from other sources likebooks, advice from others, etc. The morecomplicated problems require complexstrategies. The two basic kinds of solutionstrategies are algorithms and heuristics.
An algorithm is a strategy that exhausts everypossible answer till it comes up with the correctsolution used diligently, it guarantees a correctsolution. Algorithms are rarely used because theydo not exist for many problems and they arevery time-consuming. A heuristic is a “rule ofthumb” that can lead to a very quick solutionto no solution at all. Heuristics may involveplanning that ignores some of the probleminformation while focussing on other informationor it may involve means end analysis that testsfor a difference between the state that currentlyexist and one that desired and doing somethingto reduce the difference. Heuristics may alsoinvolve working backward to review the idealsituations and then determining what steps willlead to the ideal situation.
Evaluation: We have to decide how good is oursolution. It may be easy for some solutions but
many problems have less precise goals and areharder to judge may have many solutions tothe problem in which we have to decide whichis the best solution. When a problem is solvedby insight learning the evaluation is very quickbut in information processing and associationtype of problem-solving one may move up anddown and gradually come to the solution of theproblem. Hence, the evaluation process is alsodifferent than that of insight.
Mental blocks can hinder problem-solvingability. Mental blocks are functional fixedness,i.e. one may find it hard to perceive a newfunction for an object that was previouslyassociated with some other purpose. Some otherfactors like habitual strategy, past experiencesor conditioning, actor-Observer bias and mentalset may interfere with finding right solutions.Mental set is a tendency to respond to a newproblem in the same manner used to solveprevious problem. These factors function as“Black Box” in our thinking.
If you want to avoid pitfalls in problem-solving follow these guidelines—• Formulate a plan by making a outline• Work in a organised manner• Begin working with easy options• Mentally rehearse taking the right action• Involve yourself completely in the problem,
try to get maximum information on that• Be enthusiastic, think positively• Anticipate the challenge.
Decision Making
In our day-to-day living there are many incidentsin which we have to make decisions. It may bea simple decision as to which dress to wear, orcomplex decisions like whether to join Paediatricsor to take up Radiology for postgraduation.Similarly, we have to take number of decisionsrelated to patient care like diagnosis andtreatment. Decision making is an important partof all science-based professions. This is a cognitive

64 Behavioural Sciences in Medical Practice
process leading to the selection of a course ofaction among alternatives, it produces a finalchoice and is an action or an opinion.
Decision making is a kind of problem-solving.In which we are presented with several alter-natives among which we must choose. Whiletaking decisions one tries to optimise utility—perceived benefit or psychological value. Mostdecisions are risky in the sense that we cannotbe sure of the outcome for example, whiletreating a patient with intestinal carcinoma, youare not sure whether the patient would benefitwith chemotherapy, radiotherapy or surgery. Youtake the risk of deciding one type of treatmentthat is to be given.
The problem arises when we have to decideand choose between several alternatives. Whenthere are no fixed rules of deciding then thereis a risk of making errors in decision making dueto subjective bias. We often make use of theheuristic of representativeness to arrive atsubjective probabilities, we decide whether thecurrent situation is similar to one we haveencountered before, and then we act accordingly.While in some situations it may be useful todecide according to the past experience, but thisapproach can at times cause problems as it mayinterfere with new way of thinking. While decidingone also considers availability of options andweighing the relative advantages and disadvan-tages of a particular decision.
Decision making style have been suggestedby MBTI (Myers-Briggs Type Indicator).
According to this there are four dimensions—thinking and feeling, introversion and extro-version, judgement and perception, sensing andintuition. People high on intuition, judgementand thinking tend to take better decisions.
Decision frame is a structure of a problempresentation. Decisions are influenced by decisionframe that is how the facts are presented fordecision making. The oncologist in favour ofradiotherapy as compared to chemotherapy maypresent morbidity rate with chemotherapy.
Personal Biases in Decision Making
There are several personal bias which interferewith correct decision making. These are:• Selective search for evidence• Premature termination of search for evidence
unwillingness to share a view• Experiential limitations• Selective perception• Wishful thinking or optimism• Choice-supportive bias—when we distort our
memories of chosen and rejected options tomake the chosen options seem relatively moreattractive
• Recency—tendency to place more attentionon recent information and either ignore orforget more distant information
• Repetition bias• Influences of initial information• Inconsistency• Role-fulfillment• Faulty generalisations.
Judging
Judgement is a process by which we formopinions reach conclusions and make criticalevaluations of events and people on the basisof available information. Sometimes we makespontaneous judgments based upon ourattitude. Often decision making and judgementare considered as two sides of a coin. Judge-ments are based on inference, the reasoningprocess of drawing a conclusion on the basis ofevidence or prior beliefs.
Blocks in Cognitive Process
“We may try to see things as objectively as weplease. Nonetheless, we can never see them withany eyes except our own”.
Sometimes we may make wrong judgementsdue to over-generalised stereotypes based onminimal or faulty information. There are severalfactors which cause mental blocks in our thinking.

Thinking 65
The unconscious prejudice may bias our thinkingdue to which one may not arrive at impartialand neutral judgement. The past experienceshidden in our unconscious mind may interferewith our judgement. Prejudices like racism andsexism are commonly witnessed in thejudgements.
Cognitive bias is a systematic error in infe-rence, decision and judgement. Apprehensionof bias is inevitable as decision making processdepends on different experiences and pers-pectives. This can occur when we perceiverandom events and nonrandom, when we makeshort cuts to solve a problem, perceiving peopleas causing rather than being victimised byevents, not exploring a range of possiblesolutions. The reasons for cognitive biases arefirst and last impression, self-esteem at stake,personal need, ego enhancing bias, beliefs andstereotypes. Often mental state of a person likeanxiety, depression, frustration and irritabilitymay lead to wrong judgements. Somepsychologist have studied how complexjudgements are made. They have suggested thatthere two main heuristics (mental short cuts) thatare responsible for mistakes made in judgement.These are availability heuristic and represen-tativeness heuristic. The availability heuristicmeans that we make judgement based upon howeasily we can come up with a similar example.It is a cognitive strategy that estimatesprobabilities based on personal experience. Youestimate the likelihood of an outcome based onhow easily you can imagine similar outcomes.As example of this strategy recall that you werein a hurry, you decided to take a particular routeto reach a particular destination. On the contrary,you had encountered more obstacles on thisroute or would have taken longer to reach yourdestination. The representativeness heuristic is acognitive strategy that assigns items to categoriesbased on whether they possess some repre-sentative characteristics of the category. Thedanger of this strategy is oversimplified thinking.
We look for common features found in a typicalcategory member for example; we assumecertain characteristics for vegetarian people.
Clinical ApplicationsIn recent years, with the development ofcomputer technology in clinical decision-makingthe process of diagnosis, prognosis and treatmentmay be represented in the form of ‘decision tree’.The decision is taken based on elements ofevidence or ‘indicants’, such as answers by thepatient to a question, the presence of a physicalsign on examination or the result of a laboratorytest. Later, a comparative evaluation is done ofthe computer programme of the diagnosticprogramme with diagnosis formed by clinicians.A similar procedure is used in the experimentalstudy of thinking by computer stimulation, butit has been shown that clinicians themselves differwidely in their diagnostic behaviour. A furtherapplication has been the construction ofcomputer programmes actually to aid diganosisin specific clinical areas such as congenital heartdisease and thyroid disease.
Disorders of thinking are one of the primeconcerns in psychiatric patients. Many psychiatricdisorders specially schizophrenia and someneurological disorders like dementia, deliriumcause disorders of thinking, the examples, lackof association, neologisms (coining new words),circumstantiality, flight of ideas and delusions. Indepressive illness aim of cognitive therapy is tomodify negative thinking in terms of not beingliked by others, rejection by others and bleakfuture.
Decision making is not only important forthe physician who is treating but is also importantfor the patient and his relatives. Imagine asituation where a patient is on the ventilator fortwo months and the doctor provides the optionsto the family to continue or to wean off thepatient from the ventilator. Similarly, the patientmight have to decide whether he wants to betreated for angina by pharmacotherapy or he

66 Behavioural Sciences in Medical Practice
should undergo surgery. Similarly while dealingwith patients with substance abuse decision tostop abuse of the substance is entirely patient’sresponsibility. To help individuals who are poorin making decisions, programmes have beendeveloped to provide skills training, which isbased on cognitive and behavioural theories.
SUMMARY
Thinking is a mental activity in which oneresponds to the problem by cognitive rearrange-ment or manipulation of both information fromthe environment and the information stored in
a long-term memory. We think by means ofsymbols, concepts, schema, scripts, imagery andcognitive maps. Thinking has important functionin problem solving, decision making and judging.Problem-solving has been explained on the basisof learning theory, Gestalt theory andinformation processing. To solve a problemgenerally we take three steps like we prepareor plan, we produce and we evaluate thesolution. Decision making is important in clinicalpractice for the physicians as well as the patients.Cognitive bias may interfere with impartialrational judging. Problem-solving and decisionmaking are used in every step in patient care.

8Motivation
Mansi, a singer has developed hoarseness ofvoice and is not able to sing. The doctors treatingher feel that it will not be possible for Mansi tosing again. Music is Mansi’s life and without beingable to sing there is no meaning in life for Mansi.
The sheer motivation helps Mansi to singagain which is surprising to the doctors. You willcome across many patients in your medicalpractice who fight with the illness and survivedue to their motive to live.
Definition
Motivation means ‘to move’ and is defined asan internal process that provides energy forbehaviour and directs it towards a specific goal.Motive in a person helps to infer, explain andpredict his behaviour. Motivation is a general termfor all the processes involved in starting directingand maintaining physical and psychologicalactivities, it can be understood by studying theunderlying urges, wants, needs, desires and goals.Drive refers to biological motivation like hunger.Motives refer to psychological and social needsthat are assumed to be learned through personalexperience.
Indicators of Motivation
The following are some of the measurablequalities and events that indicate motivationunderlying behaviour:• The more motivated an organism is, the
higher will be its level of activity.
• Strong motivation increases an individual’srate of learning.
• Motivation enables one to attain a higherlevel of performance.
• Once learned, a motivated response will bemore resistant to extinction.
• Being motivated in one task can disruptefforts in other activities.
Models of Motivation
Various models have been proposed tounderstand motivation. Some of the importantmodels are drive and homeostatic model.
Drive Model
It is assumed that each organism is born withor later develops a variety of biological needs.A need is something that is required physiolo-gically, for example, the need for food, water,and the elimination of bodily wastes. When asufficient amount of time passes during whicha need is not satisfied, a relevant drive is aroused.Subjectively, we decide that we are hungry orthirsty and are directed to act in order toovercome the unpleasant state.
Once the individual is in a high drive state,there is a readiness to respond to external stimulithat are related to the aroused drive. These stimuliare known as incentives. When our drives areactivated, we move toward such incentives asthe food or water, in the refrigerator or thekitchen. Much of our behaviour is directed by

68 Behavioural Sciences in Medical Practice
incentives. An incentive may be thought of asan appropriate object or activity for satisfying aneed. Once the incentive has been obtained, theindividual engages in consummatory behaviour.That is, he eats or drinks. Such activity satisfiesthe need in question and is said to be the goalof the motivated behaviour. Obtaining such agoal reduces the aroused drive, and this drivereduction acts as a reward or positive reinforce-ment. Once a need is satisfied, the organismbecomes relatively inactive again. The generalcycle of events is illustrated in Figure 8.1. Itmay be seen, then, that motivation energisesthe organism to seek an appropriate goal byapproaching relevant incentives. Motivation alsoaccounts for the tendency to be persistent in thisbehaviour until the need is satisfied.
Fig. 8.1: Drive cycle
Within this general model, drive is often saidto be a stimulus for behaviour. That is, whena need is unsatisfied, various internal stimuli areactivated, and these stimuli lead to responses.Any strong, persistent stimulus can haveproperties to be a drive for example, a verybrightlight or an unpleasant loud noise will causean individual to close his or her eyes or coverhis or her ears, and if possible to move awayfrom the annoying stimulus. In such instances,there is no need deprivation in the usual sensebut rather an external stimulus that acts as adrive. It has been suggested that individuals actto avoid intense external stimulation aremotivated by the ‘need to avoid pain’.
The Homeostatic Model
Homeostasis refers to the regulatory process thatimpels us to eat when we are hungry and tostop eating when we have had enough, to drinkwhen we are thirsty and to stop drinking whenthat need is satisfied, and so on. There is a naturaltendency toward balance that serves to keep ourinternal environment at a relatively constant statewith respect to the various needs.
Both the drive model and the homeostaticmodel are based on a common assumption,namely that an organism when aroused strivesto return to a quiet, stable state. A more inclu-sive view suggests that drive induction and drivereduction can each be reinforcing underappropriate circumstances.Anxiety as a drive The concept of anxiety asa drive was based on the assumption that thisis a relatively stable characteristic in which indivi-duals differ. Anxiety has been classified as a traitand as a state. Trait anxiety is considered as apersonality variable. Those who were anxiouswould be expected to experience anxiety in avariety of situations. State anxiety refers to atemporary condition of arousal in response toparticular situations. For example, even if youare not a particularly anxious person (trait), youmight feel very upset as you sit in a dentist’swaiting room (state).
It has been proposed that individuals whoare characteristically anxious and tense mustordinarily experience a higher drive level thancalm, placid individuals. If so, those high inanxiety should, when compared with those lowin anxiety, demonstrate greater response strengthwith respect to various habits. As an exampleof such effects, consider what happens when anexperienced driver sees a small child suddenlycoming in front of his car. The well-learned, well-practiced habit of stepping on the brake is muchstronger than any competing habit, so it is verylikely to occur. If such a driver were extremelyanxious, the braking response would be even

Motivation 69
more likely to occur—more quickly and withgreater force. Imagine the same situation withsomeone who is just learning to drive. Many newhabits are being learned, and they are aboutof equal strength. If a child dashes in front ofthe car, a new driver may be equally inclinedto step on the brake, step on the accelerator, orhonk the horn. If that person were highlyanxious, it would only complicate matters sinceall of the responses (both appropriate andinappropriate) would be strengthened by sucha drive state. Extremely bright individuals do welleven if they are anxious. Those who areextremely dull do badly even if their anxiety islow. In the middle range, though, it is clear thathighly anxious students do less well on exams,obtain lower grades and are more likely to leaveschool (Spielberger, 1966). Students with highanxiety can be helped by assessing the severityof anxiety and then providing therapy to reducetheir anxiety (see Chapter 20).
Humanistic Model
Some theorists have proposed more complexsystem of categorising needs. Abraham Maslow(1970) has classified motivation into a hierarchyconsisting of seven separate needs. As shownin Figure 8.2, these range from the mostnecessary requirements for survival to the mostimportant expressions of the human potential.Let us look briefly at each of the five levels.
Fig. 8.2: Hierarchy of needs
Physiological needs: These are the primarymotives that serve to keep the individual aliveand to permit the continuation of the species.
Safety needs: In addition to mere survival, thereis the need to avoid pain, to obtain bodilycomforts, and to be free from fear and insecurity.These are said to be powerful, lower-orderneeds.
Need to belong and to love: The higher-orderneeds begin with the desire to obtain securityby means of identification with a group? For thisreason, we seek to identify with our families, withour school, our organisation, our religion, ournation, our race, and so forth. Somehow, wefeel better about ourselves as individuals whenwe are able to find our roots in a larger bodyof people, i.e. experience love. Besides, havinga lower-order need for sexual release, we havea higher-order need for the feelings of affectionand love - both to give and to receive.Establishing at least a loving relationship withone individual.
Esteem needs: Each of us wants to feel that heis a worthwhile individual who counts forsomething. This includes the feeling ofcompetence or mastery of the environment, andalso the need to accomplish and achieve. Inaddition, self-esteem is said to be highest if wecan be independent and free.
Cognitive needs: Individuals have an innate needto make sense of various aspects of their externalenvironment. This forms the need for know-ledge and understanding.
Aesthetic needs: These constitute the needs fororder and beauty, which individuals strive forin their lives and external environment.
Self-actualisation needs: The highest of all needsare met if an individual can achieve self-actualisation. This is a rather complex conceptinvolving the need to know all that we can, aboutourselves and about the world around us, theneed to create and to appreciate beauty, and

70 Behavioural Sciences in Medical Practice
the tendency to be a spontaneous and inner-directed achiever.
In Maslow’s view, each of us would progresssmoothly up this hierarchy as each set of lowerneeds is met. We would each become secure,creative ‘self-actualisers’. However, harsh envi-ronmental conditions can force people to spendtheir entire lives working very hard just to meetthe lower-order needs.
In addition, changes in the solution can veryquickly propel an individual back down thehierarchy. Many times, a person will have a lower-order need that is not met, and higher-orderneeds will be ignored as the person is stronglymotivated to eat, to obtain sexual gratification,or to find a bathroom. There also can be aserious disruption of one’s life that can force atotal concentration on the basic needs. Forexample, a painful illness or some natural orman-made disaster can turn even the most crea-tive, self-actualised person into an individualconcerned only with safety and survival. In therecent past many well-established Kashmiriimmigrants both intellectuals and businessmenwere seen to be having such basic survivalproblems.
Social Cognitive Model
Social cognitive model of motivation share theconcept that human motivation comes not fromobjective realities but from our subjectiveinterpretation of them. You often experience thatif you think that achieving a particular goal isimportant for you then under any circumstancesyou work to reach that goal. That means whatwe do is controlled by what we think isresponsible for causing our action, what webelieve we can do and anticipate the outcomeof our efforts. Social cognitive model givesimportance to higher mental processes thatcontrol motivation rather than physiologicalarousal or biological mechanism. Locus of controlis another concept given by Julian Rotter to
understand social learning model. According tothis model an individual will engage in a givenbehaviour is determined by two factors. One isexpectations of attaining a goal and the otheris the personal value of that goal. Expectationsof a future occurrence are based on our pastexperience, which helps in developing a personalsense of locus of control. Often we find thatstudent’s who are poor in studies do not havemotivation to study because they do notanticipate a positive outcome of their studies.Locus of control can be internal or external.When a person thinks the outcome of our actionscan be controlled by our efforts that is internalcontrol. On the contrary, if one believes that theoutcome is controlled by external factors forexample, a student thinks that his poor marksare due to teacher’s bias that is called externalcontrol.
Classification of Motives
Needs are often an important component instudying motivation. They are classified intoprimary and secondary motives, the primary orphysiological necessities are: hunger, thirst, adesire for sex, temperature regulation, sleep, painavoidance and need for oxygen. The secondaryor learned, acquired desires are: achievement,power, affiliation, aggression, autonomy,nurturance and play. The secondary motives arealso called as social motives because they arelearned in social groups, in the family, in theschool, and with peer group. The social motivesare general, persisting characteristics of a personand they differ in strength from individual-to-individual because they are learned. Thisclassification of motives is a useful one, but thedistinction can become somewhat blurred. Thatis, learned appetites and aversions influence thesatisfaction of primary motives, and thesatisfaction of secondary motives can becomeclosely tied to biological processes. For example,does your desire to earn money involve the

Motivation 71
instrumental use of money to buy somethingbasic such as food? Is it used instead to buy someproduct that would provide you instantpopularity in the hostel? Or, is the money to beacquired purely for its own sake, because youhave learned to enjoy a huge bank balance. Itseems that much of what we do can be identifiedas a mixture of primary and secondarymotivation.
Hunger Motive
While most of us take for granted the daily activityof eating, food means more than fuel for thebody with symbolic associations. Food maysymbolise love, social bonding, and the displayof affluence. The way we eat may reflect ourattitudes toward our families, our society, andourselves.
How does our body tell us we need food?We are more likely to feel the stirrings of appetite,but very poor persons have the pangs of a bodydepleted by hunger. In either case, however, theunderlying mechanism is probably the same. Abasic signal for hunger is the presence of stomachcontractions. When the stomach is empty,contractions occur and are sensed. More recentlythe research in this field has indicated that levelsor rates of use of dissolved nutritive substancescirculating in the blood are crucial for theactivation of feeding. Low level of glucose (sugar)in the blood is now believed to be an importantcause in the initiation of hunger motivation.Hypothalamus is also involved in hungermotivation, as indicated by some experiments.However we all are aware that hunger motivationis not entirely governed by the internalstimulation. A host of external factors are alsoresponsible in initiating hunger motivation.
Achievement Motive
People are very different from one another intheir desire to compete and to win at whatever
they undertake. It has been proposed that diffe-rences reflect variations in the learned motiveto achieve (Atkinson, 1977). Achievement is task-oriented behaviour that allows the individual’sperformance to be evaluated according to someinternally or externally imposed criterion.Achievement motivation can be seen in manyareas of human endeavour such as school, job,sports or art performance such as painting,singing, dancing. Achievement motivation islearned, children copy from their parents andother important persons in their lives. The expec-tations of the parents from their children areimportant in development of this motivation. Ithas been found that high achievers generally havehigh achieving mothers.
Achievement motive has been associated withthe behaviour. High achievement orientedbehaviour expresses in many ways such as,persistence, taking challenges, high aspirations,constant need for feedback and control over theenvironment. These individuals are generallymost successful in their profession provided theirneed for competition is not very strong.
Aggression Motive
An aggression is intended to hurt someone orsomething. In most places aggression leads toviolence, destructive action against people orproperty. At other times the aggressive impulseis confined to competition, verbal attack, or someother expression of hostility short of physicalinjury. When we talk about aggression, then, weare talking about behaviour that the doer engagesin with the intention of doing harm. It could bein the form of verbal attack, physical injury,violence or destructive action against people orproperty only.
Hormones and chemicals do not produceaggressive behaviour itself. What they do is tolower our threshold for expression of aggression.Very often aggression is the response to frustration(the thwarting of some goal directed behaviour),

72 Behavioural Sciences in Medical Practice
insults, and negative evaluations. Frustrationdoes not always bring about aggression;however, it is likely to lead to aggression onlywhen it is intense and unexpected or arbitrary.You are less likely to become angry when youare refused a job if you had not counted ongetting it and if you think the interview was fair.Furthermore, frustrated individuals are not likelyto become aggressive, no matter how angry theyget, unless the stage is set for aggression. Thisstage setting may consist of cues for aggression,such as an atmosphere that promotes violence(communal riots, setting fire to religious places),the presence of weapons that remind you howthey can be used to hurt someone, or a previousdislike for the person who frustrated you(Berkowitz, 1967).
Children learn from an early age that callingpeople names is almost sure to make themangry, and laboratory researchers have confir-med the aggression-eliciting power of insults byacting rudely toward subjects, sometimes ques-tioning their intelligence. Negative evaluationgiven by teachers has often resulted in frustrationin the students.
How do we learn to be aggressive? We learnaggressive behaviour from the people aroundus. Parents usually teach their children not tohit other children especially smaller children, andother adults. But when parents themselvesbehave aggressively, they become role modelsfor their children. Parents exert a great deal ofinfluence over children’s aggressiveness. Onemajor study found that the parents of childrenwho were aggressive in school were less nurtu-rant and accepting, punished their children foraggression at home, and, in general, gave themlittle support (Eron, 1980).
We learn aggression from television serials.At present there are many programmes bothmeant for adults and children like WWF in whichchildren see lots of aggression and violence. Laterthey try to imitate these aggressive stunts. While
some people argue that viewing aggression oreven acting it out to a limited degree helps todrain off aggressive energy. But actingaggressively is likely to make someone more,rather than less, aggressive. And the bulk of theresearch on viewing aggression indicates thatchildren who watch a lot of television learn thatwe live in a society that condones aggression inmany situations, and they learn what to do whenthey feel aggressive themselves (Bandura, 1973).But when parents let their children know thatviolence is not an acceptable means of settlingdisputes, then watching TV does not lead tomore aggression.
Arousal and Curiosity
Most psychologists believe that a basic motiva-tional system underlies exploratory behaviourand curiosity and arousal are related in importantways. Anyone who has ever spent much timein the company of a three year old knows thathuman beings are very curious creatures froma very early age. We want to know abouteverything in our lives—why people act as theydo, why events occur, how things work, what ison the other side of a hill, a mountain, and anocean. To satisfy our curiosity we begin as infantsto touch, to put new objects in our mouths. Aswe grow older, we continue to process theinformation that comes in through all our senses,we explore our surroundings, we ask questions,we study, we think. We seem to do many thingsfor no intrinsic reward other than satisfying ourcuriosity.
Motives and Conflict
You would have experienced some time in yourlife that you have to choose one between twoattractive offers, both of them being motivatingto some degree. Motivation researchers haveclassified such competing motives into thefollowing four categories.

Motivation 73
1. Approach approach conflicts occur when youare simultaneously attracted to two desirableoutcomes or activities, as in a situation whenyou are trying to decide which of two goodcourses you should take up for career.
2. Avoidance avoidance conflicts arise when youare repelled by two or more undesirableoutcomes or activities. Suppose there is arequired course in computers that you haveto take and that clashes with your mostimportant clinical posting or clashes with yourexam time. Still, you know that if you wantto graduate, you have to choose one of theseunwanted alternatives.
3. Approach avoidance conflicts come up whena single option has both positive and negativeelements. Suppose you are asked to speakto a group that can be influential in helpingyou to get a good job, but you are terrifiedof speaking in public. In this kind of conflict,individuals sometimes adopt unhealthymeans to combat anxiety.
4. Multiple approach avoidance conflicts are theones we most often face in life. These involvesituations in which several options exist, witheach one containing both positive andnegative elements. Not surprisingly, these arethe hardest to resolve, and the most stressful.
Clinical Applications
There can be two major applications of knowle-dge of motivation to clinical field. First, it canbe of help in understanding the wide range ofbehaviours of patients in relation to their illnessand treatment. Psychological response of patientsto their disabling illness is likely to differ accordingto the degree of dependency or dominance needsof the patient. Second, it is concerned with theproblems, which arise directly from abnormalitiesof drives of their goals. The aggressive driveappears to be expressed to a pathological degreein some individuals, who may thereby be a
danger to others a so-called aggressivepsychopath. Sexual deviations occur in whichthe aim of the sex drive departs to varyingdegrees from the usual goal of heterosexualintercourse, sometimes with an admixture ofaggression as in sado-masochism. Suchabnormalities are seen in patients havingpsychological disorders. One of the explanationsfor such behaviour is based on approach-avoidance model where, possibly owing toearlier experience, the ‘normal’ sexual object isboth attractive and frightening, so that either anintermediate position between approach andavoidance is chosen, (e.g. voyeurism or indecentexposure) or a less aversive object (e.g. smallgirls instead of adult women).
Importance of motivation is of prime impor-tance in psychiatric disorders. Schizophrenia, acommon feature, particularly in the later stagesof a chronic illness, is a loss of motivation so thatthe patient becomes apathetic and generallyinactive. Current trends of treatment arefocussed on enhancing motivation in thesepatients. Seligman (1975) has given a conceptof’ Learned Helplessness’, which has beenapplied to aetiology of depressive disorders.Learned helplessness means that the depressedperson is convinced that he is out of control,nothing he can do would make any differencein changing an important feature of his life. Sincethey believe they can’t do anything to changea situation, they don’t have any motivation evento try. Learned helplessness is a traumaticexperience as one who feels powerless to escapefrom stressful situations often gives up and die.Learned helplessness is also reported at timesby patients with chronic illness, elderly andinstitutionised persons.
Other disorders of motivation are found insuch conditions as alcohol and drug dependenceand over-eating leading to obesity. Since thesedisorders are on the increase thus shall bediscussed at length later in this section. Motivation

74 Behavioural Sciences in Medical Practice
for apparently self-injurious behaviour can beunderstood in terms of the needs that it satisfiesor the rewards that it brings—though often inthe short term. The child who repeatedly getsinto trouble, through ‘misbehaviour’ knowingfully well that he will be punished, may bemotivated (though without being aware of it) bythe fact that only by so doing will he receive moreattention from others.
The degree of control exerted over the overtexpression of basic drives—such as sex andaggression may be weakened by organic diseaseaffecting the functioning of the brain. The firstsigns of such disease may sometimes be theappearance of behaviour quite ‘out of characterfor the individual. Such a change of personalitymay therefore, be an important in dictation forclinical assessment for neurological disease.
Motivational Basis of Addictive Behaviour
Alcoholism is a condition in which heavy drinkinginterferes with an individual’s ability to functioneffectively in dealing with other people and inworking. Similar problems are also present inpatients with drug addiction. There has been agreat deal of research directed to discover theway in which we acquire this powerful and oftendangerous motive. Three major factors seem tobe involved.
First, there are the basic learning processesthat underlie the acquisition of any motive. Ifan individual grows up in a society in whichadults drink whenever they want to celebratesomething and whenever they want to relax andhave fun, such activity clearly is associated withpositive feelings. Individuals tend to model theirbehaviour after that of others. Experimentalsubjects have been found to drink more whenexposed to a stranger who drinks heavily thanwhen the stranger is a light drinker or does notdrink at all. In addition, by adolescence thereare often strong peer pressures to drink.
Second, in addition to external sources ofrewards for drinking, alcohol itself can providea powerful reinforcement. It is a depressant drugthat acts on the central nervous system to bringfeelings of relaxation and reduced anxiety. Thefact that a few drinks can very quickly relievetension and fears means that drinking is easilylearned as a method of dealing with stress.
Third, ‘alcoholic’ individuals may have aspecial physiological weakness that results in acraving for alcohol. Several biological differen-ces between alcoholics and nonalcoholic havebeen identified. For example, problem drinkersfeel less physical pain when they consumealcohol, but social drinkers actually feel morepain after a few drinks. The fact that it is possibleto breed animals that drink alcohol readily whileothers of the same species avoid it suggests thata genetic factor is involved.
A complex combination of cultural, psycho-logical, and physiological factors contributes todrinking behaviour and to alcoholism.
Eating DisordersRaju aged 12, weighing 88 kgs was referred fromendocrinology OPD. All his investigations werenormal; no physiological or endocrinologicalcause for his abnormal weight could be elicited.During psychological assessment his father’smotive to get the child’s name in Guiness Bookof World Record was noted. Through this hewanted to get a large amount of money. Fatheralways reported that the child has normalappetite and a small amount of food was givento him, but in reality the child was alwaysoverfed. This is an example of motivation forone type of problem related to eating. In Indiaobesity has always been present but was notconsidered a problem. Now with awarenessabout its harmful effects, as it prevents a normallife and is a menace to health, people havebecome concerned about it and more and morepeople are seeking treatment for obesity.

Motivation 75
It is not uncommon to find that the excessiveintake is due to actual feelings of hunger thanto eating, becoming associated with needs otherthan the food itself to reduce feelings of anxietyor unhappiness, for example in a depressed statepeople tend to eat more.
Two other kinds of eating disorders, whichseem to have become more common in recentyears, especially among young women, areanorexia nervosa, a form of self-starvation thatcan actually lead to death, and bulimia, in whichan individual regularly eats vast quantities of foodand then purges the body of them either byinduced vomiting or laxative use.
Losing Weight by Applying MotivationalPrinciples
1. Eat only at one place at regular times: Thiswill help you cut down on snacking, bylimiting the number of places and times thathave associations with eating.
2. Eat slowly: This helps you get the mostpleasure from the least amount of food, helpsyou fool yourself into thinking you are eatingmore than you actually are, and gives yourbody time to give you feedback on whenyou have had enough.
3. Do not do anything else while you are eatingsuch as reading or watching television, so thatyou can concentrate on your food and bemore responsive to your body’s internal cues.
4. Reduce the availability of fattening foods. Ifyou cannot resist seine high calorie food ofyour choice, do not bring them home. If youbuy nuts, buy them with their shells on soyou will have to expend more effort to eatthem, you will eat less.
5. Allow for some variety in your diet, if youdeprive yourself of all the foods you love,you will binge when you get the chance soit is better to incorporate a small serving ofhigh-calorie food into your menu planinstead of avoiding it completely. However,
since people eat more food when faced witha large variety, limit your meals to a few basicdishes instead of wide choice.
6. Avoid fatty and rich-tasting foods as the look;smell, and taste seem to stimulate theappetite.
7. Eat in the company of other people who aremoderate eaters themselves, you will beinclined to eat more moderately when otherpeople are witnesses to what you eat. Alsoyou will be able to guide your intake by theirs.
8. Use small serving plates; food heaped on asmall plate looks more than the sameamount on a large plate. Take advantage ofthis visual illusion to fool you into eating less.
9. Incorporate exercise into your daily schedule.Aside from the direct expenditure of energyin the activity itself, exercise seems to reduceappetite. Programmes that combine dieting,changes in behaviour, and exercise result inmore weight loss than any one of thesechanges alone. The most effective exerciseschedules include sessions of at least 20minutes each, three times a week, of activitiesthat are strenuous enough to expend 300calories per session or to raise the heart rateto 60 to 70 per cent of its maximum (Thomp-son et al 1982). This generally means likeswimming, running, bicycling, dancing, orsome other kind of aerobic activity (requiringhigh consumption of oxygen for a sustainedperiod of time) rather than a more staticexercise like weight lifting or sit-ups.
SUMMARY
Motivation is the force that energies and givesdirection to behaviour and that underlies thetendency to persist. According to drive model,once the individual is in high drive state, thereis a readiness to respond to external stimuli thatare related to the arousal drive. Once the incen-tive is achieved that satisfies the drive. Amongthe models, the homeostatic model discusses a

76 Behavioural Sciences in Medical Practice
natural tendency of the body towards main-taining balance that serves to keep our internalenvironment at a relatively constant state withrespect to various needs.lt proposes thatindividuals who are characterised anxious andtense must ordinarily experience a high drivelevel than calm, placid individuals. Maslow hasgiven humanistic model of motivation, whereinfive stages are given namely—physiological,safety needs, belongingness, esteem needs andself-actualisation. The cognitive social modelemphasises on the expectations an individual hasabout himself to reach to goal and the meaningof that goal for the individual. Locus of controlcan be internal (conditions are within the controlof the person) or external (Conditions arecontrolled by other people or situations).
Motives are classified as primary motive, thephysiological secondary motive, the learned oracquired desires. A low level of glucose in blooddoes not only indicate hunger motives but alsoinclude symbolic content of the food as love andsharing. People are different from one anotherin their desire to compete and win at whateverthey undertake. Achievement motivation may belearned, there may be a dominant pattern withhigh achieving motives and is also associated withindividual’s behaviour as being persistent,challenging, high aspirant, etc.
Aggression motive is inclusive of thebehaviour that the doer engages with anintention of doing harm in form of verbal attack,physical injury, violence or destructive actionagainst people or property. Very often aggres-sion is a response to intense frustration. We learnto be aggressive by observing our parents, theattitudes prevalent in the society and byobserving television. Most psychologists’ believethat a basic motivational system underliesexploratory behaviour and curiosity and arousalbeing related in important ways.
Frustration is the result of conflict betweenthe competing motives. The conflicts are classifiedas: approach- approach, approach - avoidance,avoidance - avoidance, and multiple approach- avoidance conflict.
The shady of motivation has two majorclinical applications: firstly, it can be of help inunderstanding the wide range of behaviours ofpatients in relation to their illness and treatment.Secondly, it is concerned with the problems,which arises directly from abnormalities of drives(sexual deviations and aggression). Motivationenhancement is becoming an important aspectin all treatments regimens as it relates tocompliance. The outcome of some treatmentintervention depends to some degree on themotivation of the patient.

9Emotion
Bharati aged 48 years, is married and has twochildren. Bharati has been referred for herasthmatic attacks, which have recently becomevery severe and also occur more frequently. Hermedication has been increased but Bharati hasnot got any relief. Bharati and her whole familyare very upset due to her severe attacks, whichat times even require hospitalisation. What couldbe the reason for Bharati’s problem? One of thecommon causes in such situations is emotionaldistress. A detail history of psychosocial factorsrevealed that lately Bharati has been very upset,as her young daughter wanted to marry a boyfrom other caste. Bharati had tried to dissuadeher daughter, but the daughter had her ownperspective. Bharati has been worrying aboutthis, has not been able to sleep, and has notdiscussed her problem with any one else. It iswell known that the emotional state of the personhas a great impact on the physical health;emotions can precipitate or aggravate an illness.
Emotion is one of the important aspects ofhuman relationship. Emotions have a psycho-logical aspects also related to behaviour andcognition, which influences the physiologicalaspects of the emotion. When you are screamingat someone’s behaviour, it arouses sympatheticnervous system and your body reactsaccordingly. An emotion involves a subjectiveawareness of a particular state of mind, whichis recognised as happiness or fear, and anobjective physiological change, like change in
heart rate, and expressive motor behaviour(over activity, running away), which is observableand can be measured. Emotions are closelyassociated to health and sickness, thus anunderstanding of emotions is of great impor-tance.
Definition
The dictionary gives many definitions of“emotion”, most of which have to do withagitated movement of some kind. And most ofthis “agitated movement” has to do with goals.You often feel joy and happiness, when you reacha goal. You often feel angry and frustrated, whenyou perceive a barrier between you and a goal.And you may experience pain and depression,when you believe you cannot possibly get whatyou want or need. The emotional experience hasnot been much emphasised in the scientificdefinitions of emotion.
According to biologically oriented psycho-logists, emotion is primarily a physical reactionthat involves rather special parts of your nervoussystem. The purpose of emotions is to arousebody for some kind of specific action (such asfighting), or to depress physical responses, so thatbody can regain itself.
To other psychologists, emotion is primarilyan intrapsychic experience that involves “innerfeelings” rather than physiological reactions(for overt behaviours). Some of these experts

78 Behavioural Sciences in Medical Practice
divide emotions into various types of mentalexperiences such as fear, anger, love, hate, andlust. Other intrapsychic psychologists viewfeelings as being bipolar either “pleasant” or“unpleasant”. Still other group of psychologistsperceives emotions as being behaviouralresponses. They are concerned with fearfulreactions, rather than fears, and of inactivity orunresponsiveness rather than depression.
Cutting across this debate about whatemotions are, is the age-old controversy aboutwhere emotions come from. Some psychologistsbelieve that all cultures share similar emotionalreactions. Other behavioural scientists view theemotions as being mostly learned reactionsacquired through experience. These psycho-logists believe you had to be carefully taught tolove the things you love, and to hate the thingsyou despise.
The Physiology of Emotions
Emotionality has been viewed by somephysiologists as primarily a biological event, andthey tend to focus on arousal and depression.Emotional reactions are perceived by them asbeing one’s way of preparing to respond to somekind of physical or psychological challenge.Imagine you are about to be attacked by somerobbers. Then you must prepare yourself eitherto fight or to get out of the threatening situation.Your physiological emotional responses will takeplace without your conscious volition or desire;you do not have to “will” your sweat glands tosecrete water or your teeth to start chattering,when you are frightened or cold. These activitiesare handled for you automatically by theunconscious parts of your brain and nervoussystem.
Autonomic Nervous System
Autonomic nervous system is that part of bodywhich controls emotional reactions. It isconnected to most of the glands and many ofthe muscles in the body. Autonomic nervous
system has two major parts: (1) the sympatheticnervous system, whose activity tends to exciteor arouse and (2) the parasympathetic nervoussystem, which tends to depress or slow downmany of the bodily functions. Both parts of thenervous systems work together in a coordinatedfashion to control bodily activities. When oneneeds to relax, parasympathetic system increasesits neural activities, while sympathetic systemslows down. It is the joint action of the twosystems, which allows responding appropriatelyto most of the physical and psychologicalchallenges one meets in life.
Sympathetic Nervous System
Your sympathetic nervous system consists of agroup of 22 neural centres, lying on or closeto your spinal cord. From these 22 centres,axonic fibers run to all parts of your body, tothe salivary glands in your mouth, to the irisesin your eyes, to your heart, lungs, liver, andstomach, and to your intestines and genitals.Your sympathetic nervous system is alsoconnected with your sweat glands, your hair cells,and with the tiny blood vessels near the surfaceof your skin.
Whenever you encounter an emergency ofsome kind—something that enrages you, makesyou suddenly afraid, creates strong desire, orcalls for heavy labour on your part, yoursympathetic nervous system swings into actionin several ways:• The pupils in your eyes open up to let in
more light.• Your heart pumps more blood to your brain,
muscles and to the surface of your skin.• You breathe harder and faster.• Your blood sugar level is elevated.• Your digestion is slowed down to a crawl.• Your skin perspires to flush out the waste
products created by the extra exertion andto keep you cool.
• The sympathetic nervous system also controlsorgasm and ejaculation during sexual excite-ment.

Emotion 79
In short, activity in your sympathetic nervoussystem prepares you for fighting, fleeing, feeding,or sexual climax.
Parasympathetic Nervous System
Your parasympathetic nervous system connectsto most (but not all) parts of your body, as doesthe sympathetic. In general, parasympatheticstimulation produces physiological effects that arethe opposite of those induced by sympatheticstimulation. Activity in your parasympatheticsystem does the following things:1. It closes down or constricts the irises in your
eyes.2. It decreases the rate at which your heart
beats.3. It slows down your breathing.4. It lowers your blood sugar level.5. It increases salivation, stimulates the flow of
digestive juices, and promotes the processesof excretion.
6. It retards sweating.7. It induces penis erection in the male and
nipple erection in the female during sexualactivity.Generally speaking, activity in your para-
sympathetic nervous system conserves or buildsup your body’s resources.
Homeostatic BalanceIncreased neural excitement in the sympatheticsystem tends to inhibit activity in the para-sympathetic, and vice versa. But the two systemsare not really antagonists or competitors. Rather,they function together smoothly in a coordinatedfashion to maintain an optimum balance betweenover-arousal and under-arousal. The sympatheticsystem gears the organism for energy output. Asthe emotion subsides, the parasympatheticsystem, the energy-conserving system, takes overand returns the organism to its normal state.
An example of joint activity of these twosystems is the sexual act, where parasympathetic
stimulation is necessary for erection to occur.However, orgasm and ejaculation are controlledby sympathetic excitation. Thus, sexual activitymust begin with relaxation (parasympatheticstimulation) but typically goes on to arousal andclimax (sympathetic stimulation). Too muchsympathetic arousal or inhibition early in the sexact, leads to impotence in the male and disinterestor frigidity in the female. And too muchparasympathetic stimulation will prevent orgasmin both sexes. Under normal circumstances, inmost of the activities there is a normal balancebetween parasympathetic and sympatheticstimulation. On the contrary, individuals who areunder stress or are angry, agitated, the balancebetween the two systems is disturbed and thesympathetic nervous system becomes moreactive.
The Adrenal Glands
There are two adrenal glands, one sitting atopeach of the kidneys. Adrenals produce hormonesthat influence sexual development and thatmonitor bodily functions such as urineproduction. But these glands also produce twochemicals that are referred to as the “arousal”hormones. Earlier, these two hormones werecalled as adrenalin and noradrenalin, now theseare more commonly referred as “epinephrine”and “norepinephrine.”
When epinephrine and norepinephrine arereleased into the bloodstream by adrenal glands,these hormones bring about all of thephysiological changes associated with strongemotions such as fear, anger, hostility and sexualaggressiveness. These two hormones act toprepare blood pressure and heart rate, speedingup breathing, widening the pupils in eyes, andincreasing perspiration. The release ofepinephrine and norepinephrine is under thecontrol of sympathetic nervous system, whoseactivities are imitated by the hormones. Whenyou encounter an arousing situation, your

80 Behavioural Sciences in Medical Practice
sympathetic nervous system goes into action first,mobilising your body’s energy resources and alsocausing the secretion of the two “arousal”hormones. As you secrete epinephrine, thearousal process by chemically stimulating thesame neural centres that the sympathetic nervoussystem has stimulated electrically.
But the hormones also increase the firingrate of the nerve cells in the sympathetic nervoussystem itself. This stimulation causes you tosecrete more of the hormones, which increasesactivity in the sympathetic system, and so onuntil the emergency has passed or you collapsein exhaustion.
General Adaptation Syndrome
Hans Selye (1976) outlined the three states thatbody seems to go through when its resourcesmust be mobilised to meet situations of exces-sive physiological stress. According to Selye,biological reaction to stress almost always followsthe same adaptive pattern. Selye calls this patternthe General Adaptation Syndrome, or GAS andhas three main stages or parts: (i) Alarm stage,(ii) resistance or counteraction and (iii)exhaustion. Suppose you suffer from a severephysical or emotional trauma. Your body willimmediately respond with the alarm reaction,which is the first stage of the General AdaptationSyndrome. During this stage, your body andmind are in a state of shock. Your temperatureand blood pressure drop, your tissues swell withfluid, and your muscles lose their tone. You maynot think clearly and ability to file things awayin long-term memory may be disrupted.
The second part of the GAS is the stage ofresistance, or countershock. During this stage,your body begins to repair the damage it hassuffered, and your mind begins to function moreclearly. ACTH hormone is released by the brain,which acts on your adrenal glands, causing themto release their own hormones. These adrenalhormones counteract the shock in several ways,
primarily by raising temperature and bloodpressure. However, you pay a price for resistingthe shock, for your body uses up its availablesupply of ACTH and adrenal hormones at a rapidpace. If the stress continues, your adrenal glandswill swell as they strive to produce enoughhormones to neutralise the stress.
During the first two GAS stages, your sym-pathetic nervous system is intensely aroused.However, if the emergency continues for toolong, an overwhelming counter-reaction mayoccur in which your parasympathetic systemtakes over. You may fall into the third state—the stage of exhaustion. During this stage, yougo into shock again because your body has beenover-stimulated for so long, that it is depletedof ACTH and adrenal hormones. Further expo-sure to stress at this time can lead to depression,psychophysiological disorders or even death.
Theoretical Explanation of Emotion
Psychologists and physiologists have tried toformulate some general principles to explainemotions. These theories are concerned with therelationship between individuals’ bodily states theemotions they feel, and how emotions areinvolved in behaviour.
The James-Lange Theory of Bodily Reactions:The most famous physiological theory ofemotionality was proposed by William James in1884. According to James, body always takesthe lead in emotional situations; “feelings” aremerely mental responses to the changes that haveoccurred in nervous system, muscles and glands.
An example of this could be, suppose youare walking through the woods one day andyou almost step on a huge rattlesnake. Chancesare, you will momentarily go into shock. Then,almost immediately, your heart will startpounding, your hair will stand on end, and youwill breathe more rapidly. And if you are wise,you will slowly back away and then run for your

Emotion 81
life. Moments later, usually after you are out ofdanger, you will notice these physiologicalreactions and realise that you are scared.
You may think that you saw the snake,became frightened, and then ran. But accordingto James, this is not the case. For he presumesthat your bodily reactions precede and thus causeyour feelings. According to this theory, we areafraid because we run; we do not run becausewe are afraid. Later, similar explanation wasgiven based on independent research by Langeand this is often called the James-Lange theoryof emotions.
The Cannon-Bard Theory of Central NeuralProcesses: Some objections were pointed out tothe James-Lange theory by the physiologistWalter B Cannon. First, James-Lange assumedthat feelings are dependent upon activity in thesympathetic nervous system. However, peoplewho (through accident or disease) have lost useof their sympathetic systems still feel emotionsand show emotional behaviours. Second, thebodily changes associated with emotions gene-rally occur after the “feelings and behaviours”have started, not before they take place. Third,the same physiological changes occur in verydifferent emotional states and in nonemotionalstates as well.
Cannon believed that emotional inputs wereprocessed almost simultaneously by two differentparts of the brain, the thalamus and thehypothalamus; the thalamus controlled emo-tional feelings, while the hypothalamus control-led bodily responses. You would experienceconscious “fear” of a snake, even if your bodywere totally paralysed because “fear” and“running” are mediated by different centres inyour brain. Bard advanced almost the sameviewpoint later in 1937, since then this approachto the explanation of emotionality is called theCannon-Bard theory.
The Lasarus-Schachter Theory ofEmotional Arousal
Sensory experiences lead to emotion only whenthe stimuli are cognitively appraised as havingpersonal significance. Richard Lasarus (1984)advocated cognitive appraisal view, thatemotional experience ‘grows out of ongoingtransactions with the environment that areevaluated’. According to Stanley Schachter(1971) the experience of emotion is the jointeffect of the physiological arousal and cognitiveappraisal. All arousal is assumed to be generaland undifferentiated and it comes first in theemotion sequence. Cognition serves todetermine how this ambiguous inner state willbe labeled. This theory is also known as two factortheory of emotion. This approach has beenchallenged, as awareness of once physiologicalarousal is not a necessary condition for emotionalexperience.
Other Physiological Viewpoints: Karl Lashley(1960) noted that people with damagedthalamuses still experienced emotional feelings,and people with damaged hypothalamuses stillshowed emotional responses. At about the sametime, other scientists showed that both the limbicsystem and the right hemisphere were involvedin mediating emotional feelings and behaviours.
The recent theorists have pointed out thatbodily reactions do play an important role increating and sustaining emotions. However, ourfeelings are so frightfully complex, that we simplycannot reduce them to mere hormonal neuralactivity. To gain a more complete understandingof emotionality, therefore, we must look at intra-psychic variables as well.
Intrapsychic Aspects of Emotionality
Intrapsychic psychologists believe contrary to thebiological psychologists that how you perceive

82 Behavioural Sciences in Medical Practice
and feel about a situation determines your bodilyreactions. An intrapsychic viewpoint emphasisesthe reverse.
For example, you can tell the difference(subjectively) between your emotions and youdifferentiate between such emotional states ashunger, fear, and anger. You apparently do soon the basis of intrapsychic cues rather thanbiological states. The physical changes that occurin your body are pretty much the same, nomatter what type of emotional upheaval youare undergoing.
There is some recent evidence that adrenalglands produce more epinephrine when you areafraid, but secretes more norepinephrine whenyou are angry. However, both hormones arereleased to some degree in all arousal situations.Thus, we cannot tell objectively whether you areangry or afraid just by measuring the relativeamounts of epinephrine and norepinephrinefloating around in your bloodstream.
The importance of psychological factors inemotions has been supported by a study, inwhich human volunteers were injected with largeamounts of epinephrine or norepinephrine, theyoften reported feeling as if they were “about tobecome emotional”, but they could not say why.The “arousal” they experienced did not seem“real” somehow, because it was not focussed ordirected toward any given object. Many of thevolunteers described the experience as “coldrage”.
Cognitive Factors in Emotion
Bodily sensations, particularly the activity of theautonomic nervous system, are important tofeelings of emotion, but different emotions showpretty much the same physiological patterns.People are usually aware that something is goingon internally when they are angry, or excited,or afraid, but they do not discriminate their heartrate or blood pressure or what is happening intheir stomach very well. The individual identifies
and labels his state of physiological and psycho-logical arousal in terms of the immediate circum-stances, what angered them, or pleased themor frightened them. They go on to describe someof their bodily reactions and this determineswhether he is, angry, fearful or happy. They donot define the emotion solely in terms of theirown internal feelings.
These results support cognitive-physiologicaltheory of emotion. According to Schachter(1971), emotion is internal physiological arousalin interaction with cognitive processes. Feedbackto the brain from physiological activity gives riseto an undifferentiated state of affect, but the feltemotion is determined by the “label” the subjectassigns to that aroused state. The assignment ofa label is a cognitive process; the subject usesinformation from past experiences and hisperception of what is going on around him toarrive at an interpretation of his feelings. Thisinterpretation will determine how he acts and thelabel that he uses to define his emotional state.According to Lasarus (1966), the individualcognitive appraisal of any situation determinesthe emotional response, including its accom-panying physiological changes. Appraisal isinfluenced by past experience and currentavailability of strategies for coping with threat.
Learning to label bodily sensations in termsof emotional tone (i.e. as pleasant or unplea-sant) is relevant to some of the differencesobserved between experienced and inexperien-ced users, of alcohol, marijhuana, and otherdrugs. First, sensations are often unpleasant butmuch of the pleasure associated with the useof such drugs comes from cognitive and socialfactors. Initial users have to learn to label thephysical sensations as enjoyable.
Modifying Arousal by Altering Cognitions: If ourstate of emotional arousal is determined by ourcognitive evaluation of the emotion-producingsituation, then it should be possible to alterarousal level by changing one’s cognitions.

Emotion 83
Indeed, you can think of instances where initialemotional responses to stimuli change as thesituation is reappraised as threatening or benign.You are awakened by the telephone at midnight.Your initial fear reaction aroused by the thoughtthat some catastrophe has happened to a lovedone changes to relief as you discover it is a wrongnumber. A potentially emotion-producingsituation has become neutral because of achange in your appraisal of it.
Types of Emotions
How many different types of emotions have youexperienced? You would include love and hate,joy and sadness, anxiety and calmness, guilt andrelief, anger and friendliness, fear and security,elation and depression. There are variousclassifications of the emotions. There are threebasic innate emotions: fear, rage and love. Fromthese, all other emotions are derived throughconditioning process. McDougall (1908) listedseven primary emotions: flight-fear, repulsion-disgust, curiosity-wonder, pugnacity-anger, selfabasement-subjective, self-assertion-elation andparental care-tenderness. There are complexemotions such as admiration, envy andsentiments (e.g. love, hate, respect). Sentimentsare regarded as habitual responses to an object,involving a persistent disposition to respond ina particular way.
Emotions are generally measured on thescale with two extremes on either side; it mayalso be referred as positive pole or negative pole.An illustration of this would be—
Positive Negative
Arousal InhibitionJoy SadnessLove Hate
Verbal descriptions of emotions are at bestpoor descriptions of complex psychologicalprocesses. Is your love for material things, thesame sort of intrapsychic experience as your love
for your mother or for your country? And whenyou say, you are “somewhat afraid of lizards”,is that merely a weaker form of the fear someoneelse feels when he says, “I despise those creepy-crawly things.” We seldom experience emotionsin a vacuum. Rather, emotions are tied to specificevents, situations, and objects. Thus, it seldommakes much sense to talk about “love” inabstract terms. Rather, we should probably speakof “love of” something, or “the love for”something.
Some emotions are not only positive andarousing, they give us a pleasant feeling as well.
Other emotions are not only negative anddepressing, they are also downright unpleasant.But again, things are not as simple as they seem.Some love makes us happy, whereas others arefrustrating and unrewarding. Some hatred isdepressing, while others stimulate us topleasurable accomplishments.
Karl Pribram has attempted to explain theconcept of “feeling tone”. He believes that thereare two types of positive affect: gratification andsatisfaction. There are also two types of negativeaffect or feeling tone, which Pribram calls distressand dissatisfaction. You experience “gratification”,whenever your needs are satisfied or yourphysiological drives are reduced. The feelingsthat accompany this gratification are relief,calmness, and tranquility. “Satisfaction” goesbeyond mere calmness, it occurs when youreduce your uncertainty about things. Thefeelings associated with satisfaction are those ofdelight, relish, joy, and exhilaration.
Role of Learning in Emotional Arousal
Some situations appear to be innately emotionproducing. Anger tends to be provoked byrestraint against the carrying out of a motivatedsequence of behaviour. Fear can be aroused bypain, a loud noise, or sudden loss of support inany young individual. The fear-arousing elementseems to be strangeness, and we can postulate

84 Behavioural Sciences in Medical Practice
that the important factor is the ability todiscriminate the new from the familiar.
Fear of something strange seems to be largelyinnate, but maturation and learning may berequired as a background. At about eight months,human infants show an intense fear of strangers.No matter how sociable the child has been priorto this time, or how many different people hehas been exposed to, the onset of “strangershyness” is usually abrupt and intense? The mostplausible interpretation is that maturation ofperceptual abilities has enabled the child todiscriminate familiar from strange adults.
Emotions may also be associated with newobjects or situations by learning. In the classicexperiment by Watson, the founder of Beha-viourism, a boy named Albert was conditionedto fear, a previously neutral object, a white rat.When eleven-month-old Albert was shown awhite rat, he reached for it, evidencing no fear.But every time he touched the rat he wasfrightened by a loud sound. He soon becameafraid of the rat. The originally neutral rat becamea “conditioned stimulus” to fear. Albert alsoshowed fear of his mother’s fur neckpiece andof other furry objects. Albert’s fear generalisedto objects that were similar in some respect tothe rat but not to toys, such as rubber balls orblocks, that were unlike rat in appearance(Watson and Rayner, 1920).
It is probably that some irrational fears areacquired in this relatively automatic way. Youwould have experienced that children are veryfearful of the hospitals because of their associationof hospital with injections. Similarly, fear ofthunder can be understood because lightningprecedes thunder, the child may come to fearthe lightning as much as the thunder, althoughthe loud sound of thunder is the primary reasonfor fright. But most fears are probably learnedin a more complex way, some through actualcontact with harmful objects, but more throughimitation of parental fears.
Emotional Expression
How emotions are expressed? Are there indivi-dual differences in expression of emotions? Thedifferent research finding have pointed out thatthere are some emotions, which are universallyexpressed in the similar way, these have beentermed as innate emotional expression. There aresome emotional expressions, which areinfluenced by learning, culture and individualstyle.
Innate Emotional Expression
The basic ways of expressing emotion are innate.Children all over the world cry when hurt orsad, and laugh when happy. Studies of childrenblind and deaf from birth, indicate that manyof the facial expressions, postures, and gesturesthat we associate with different emotionsdevelop through maturation, they appear at theappropriate age even when there is noopportunity to observe them in others. Certainfacial expressions do seem to have a universalmeaning regardless of the culture in which theindividual is raised, like facial expressions ofhappiness, anger, sadness, disgust, fear, andsurprise.
Hole of Learning in Emotional Expression:Although certain emotional expressions may belargely innate, many modifications occurthrough learning. Anger, for example, may beexpressed by fighting, by using abusivelanguage, or by leaving the room. Leaving theroom is not an expression of emotion that isknown at birth, and certainly the abusive lan-guage has to be learned. Certain facialexpressions and gestures are taught by one’sculture as ways of expression emotion. As youwould have observed that laughter is restrainedin some cultures.
Even gender differences in expression ofemotions are seen, females are supposed to

Emotion 85
suppress expression of emotions. Thus, super-imposed upon basic expressions of emotion,which appear to be universal, are conventionalor stereotyped forms of expression, whichbecome a kind of ‘language of emotion’,recognised by others within a culture. Skilledactors are able to convey to their audiences anyintended emotion by using facial expressions,tone of voice, and gestures, according to thepatterns the audience recognises.
Arousal Level and Effectiveness of Performance:A mild level of emotional arousal tends to pro-duce alertness and interest in the task at hand.When emotions become intense, however,whether they are pleasant or unpleasant, theyusually result in some decrement in perfor-mance. The curve in Figure 9.1 represents therelation between the level of emotional arousaland the effectiveness of performance. At verylow levels of arousal (for example, when oneis just waking up), the nervous system may notbe functioning fully and sensory messages maynot get through. Performance is optimal atmoderate levels of arousal. At high levels ofarousal, performance begins to decline.Presumably, the central nervous system is soresponsive, that it is responding to too manythings at once; thus, preventing the appropriateset of responses from dominating. Individualsdiffer in the extent to which their behaviour isdisrupted by emotional arousal. Observationsof people during crises, such as fires or suddenfloods, suggest that about 15 per cent showorganised, effective behaviour. The majority, 70per cent, shows various degrees of disorgani-sation but are still able to function with someeffectiveness. The remaining 15 per cent are sodisorganised that they are unable to functionat all. They may race around screaming orexhibit aimless and completely inappropriatebehaviour.
Emotions, when sufficiently intense, canseriously impair the processes that controlorganised behaviour.
Clinical Applications
Emotions according to their intensity can beadaptive or disruptive. Here, emotions arerelated to stress and individual’s ability to copewith stresses. Sometimes emotions are notquickly discharged but continue to remainunexpressed or unresolved. Perhaps, thesituation that makes one angry (e.g. prolongedconflict with one’s employer) or mat makes onefearful (e.g. worry over the chronic illness of aloved one) continues for a long period of time.The state of heightened arousal can take its tollof the individual’s ability to function efficiently.Sometimes, continual emotional tension canimpair physical health. In a psychophysiologicaldisorder, the symptoms are physical, but thecause is primarily psychological. A number ofdifferent types of illness, e.g. ulcers, asthma,migraine headaches, chronic fatigue, high bloodpressure and skin eruptions, are related toemotional stress. Long-term emotional stress canimpair a person’s physical health as well as hismental efficiency.
The physiological changes accompanyingintense emotions are the basis for use of thepolygraph, commonly known as the “liedetector”, in checking the reliability of anindividual’s statements. The polygraph does notdetect lies; it simply measures some of thephysiological accompaniments of emotion. The
Fig. 9.1: Arousal and performance

86 Behavioural Sciences in Medical Practice
measures most frequently recorded are alterna-tions in heart rate, blood pressure, respirationand the galvanic skin response, or GSR (the GSRis a change in the electrical conductivity of theskin).
Feelings involve the expenditure of physical,mental, or behavioural energy. Learning to copewith emotions, therefore, requires learning howto handle the stresses and strains of life. Anxietyand phobias are result of intense emotionalexperience. Apprehension of panic attack oranxiety is related to the James-Lange theory.Even if the autonomic changes are not the causeof the emotional state, awareness of them, actslike a positive feedback to many patients.Another clinical condition of interest in relationto emotions is epilepsy originating in the temporallobes. The electric discharge in that part of thebrain may give rise to a transient state of intensefear.
Emotions and the accompanying physiolo-gical changes are considered by many to be ofgreat importance in relation to psychosomaticmedicine. The psychosocial factors may contri-bute to the causation of, or affect the course andprognosis of, organic disease.
In psychopharmacology, study of emotionshas become important, as many factor influencethe effect of a drug on behaviour such as dosage,route of administration and the presence ofmultiple effects. Even the placebo effect is dueto the psychological influences arising from thepatient’s perception of the situation in which thedrug is administered.
SUMMARY
Emotion is an important aspect of humanrelationship. Emotions have a psychologicalaspect related to behaviour and cognition, whichinfluences the physiological aspect of emotion.It is a subjective awareness as happiness or fear,and an objective physiological change like heartrate and expressive motor behaviour.
Emotion has been viewed as a biologicalevent. Emotional reactions are controlled byautonomic nervous system, which has two parts:sympathetic nervous system and para-sympathetic nervous system. It is the joint actionof the two systems, which allows one to respondappropriately. When the individual is in a relaxedstate, the parasympathetic nervous systemincreases its neural activities, while sympatheticnervous system slows down. A homeostaticbalance is maintained between over arousal andunder arousal. The physiological changes dueto strong emotions are associated with arousalhormones produced by adrenal glands, namely,epinephrine and norepinephrine. The releaseof epinephrine and norepinephrine is under thecontrol of sympathetic nervous system. GeneralAdaptation Syndrome theory advocates thatduring excessive stress, the body goes throughthree stages mobilising its resources for anemergency. These three stages are the stage ofalarm, the resistance and exhaustion.
James-Lange theory of emotion states thatthe emotions we experience result from ourperception of the changes taking place in thebody during emotion. However, the Cannon-Bard theory believes that emotional inputswere processed almost simultaneously by twodifferent parts of the brain, the thalamus andthe hypothalamus. The emotional feelings werecontrolled by the thalamus and the hypotha-lamus controlled bodily responses. Otherphysiological viewpoints do not agree withCannon-Bard theory as the individuals withdamaged thalamus also experience emotions.Thus, psychologists have given intrapsychicexplanations; they view emotions as experiencesthat involve inner feelings, than physiologicalreactions. The cognitive-physiological theory ofemotion states that the individual’s cognitiveappraisal of any situation determines theemotional response, including its accompanyingphysiological changes. Appraisal is influenced by

Emotion 87
past experience and current availability ofstrategies for coping with threat. Thoughemotional reactions are shared by all cultures,but some emotional reactions are also learnedthrough experience. Different research findingshave pointed out that there are some emotions,which are universally expressed, these aretermed as innate expressed emotion. There aresome emotions, which are learned throughculture and individual styles. The relationshipbetween the arousal level and the performancedetermines its effectiveness. Performance isoptimal at moderate levels. At low levels, thenervous system may not be fully functioning,and at high levels the performance declines.
Sometimes, continual emotional tension canimpair physical health. In a psychophysiologicaldisorder, the symptoms are physical, but thecause is primarily psychological. A number ofdifferent types of illness, e.g. ulcers, asthma,migraine, headaches, chronic fatigue, high bloodpressure and skin eruptions, are related toemotional stress. Long-term emotional stress canimpair a person’s physical health as well as hismental efficiency. Emotions and the accompany-ing physiological changes are considered bymany to be of great importance in relation topsychosomatic medicine.
Negative emotions can be quite stressful;learning to cope with emotions requires learninghow to handle the stresses and strains of life.

10Stress and Coping
Vijay, 45 years old, is a company executive ina multinational firm. Being in the top position,Vijay leaves home at seven thirty every morningand returns back late in the evening. He has notime to rest, or able to enjoy leisure time activities.Every day he has to meet dead lines in work,attend official meetings and take decisions. Hehas not been able to take off from work evenfor a single day for the last two years. However,lately Vijay has been having some physicalproblems, like he never feels fresh, is tired allthe time, is not able to have sound sleep, hasoften indigestion of food and his appetite hasreduced. All the laboratory test has failed to geta cause for his problems. Such physical problemsdo occur as a result of persistent stress.
We all experience stress in some or the otherform, such as meeting time-bound targets,competitions, getting stuck in a traffic jam whileon the way to attend an urgent task, noise, socialpressures, etc. We differ in the extent to whichwe get affected by stressors as we all havedifferent ways of dealing with these situations.
Definition
Hans Selye (1974), the pioneer in stress research,defined stress as a stimulus event of sufficientseverity to produce disequilibrium in thehomeostatic physiological systems. We feel stresswhen our responses to even disrupt or threatento disrupt our physical or psychologicalfunctioning. Positive stresses called ‘Eustress’, like
shifting to a new house, promotion in job. Whenstress has negative effect on the individual, it isdistress, for example, failure in examination,chronic illness, break-up with loved ones. Thestimulus that evokes a stress response is calleda stressor. A stimulus becomes a stressor by virtueof the cognitive interpretation or meaning thatthe individual assigns to the stimulus or by virtueof the fact that the stimulus affects the individualby way of same sensory or metabolic process,which is in itself inherently stressful. Inphysiological terms stress is the body’s responseto any stressful demand. Lazarus defined it inpsychological terms as an Individual’s cognitivejudgement that his or her personal resources willbe taxed or incapable of dealing with thedemands posed by a particular event. Accordingto Reuben Hill a stressor event is one that makesdemands on the family system, rather than onthe individual.
Components of Stress
Stress comprises of stressor, the sources causingthe stress and stress response, which is how theindividual copes with the stressful situation, hiscoping resources like person’s skills and socialsupport systems (Fig. 10.1).
Stressor represents stimulus events requiringsome form of adaptation or adjustment. Stressorcan be internal stimuli like cognitions or thoughtsor external stimuli like crowd, noise, andinterpersonal difficulties. The stressed person

Stress and Coping 89
shows several stages: (i) Stage of alarm, (ii) Stageof appraisal, and (iii) Stage of reaching for acoping strategy.
The stress response is a complex reactionpattern that consists of physiological, cognitiveand behavioural components. The physiologicalcomponent of the stress response activates thesympathetic and parasympathetic autonomicnervous system and elicits a set of physiologicalreactions. The stress response has threecomponents namely the tonic—the resting orbasal level of activity, the phasic—the reactionto the given stressor and recovery—return tothe tonic level.
Sylve had described a three-stage reactionto stress consisting of alarm, resistance andexhaustion known as general adaptionsyndrome (GAS). The three stages are asfollowing:a. Alarm reaction, subdivided in two phases,
shock and counter-shock. Shock phase isinitial and immediate response. Countershock is how the body rebounds to mobiliseits defenses.
b. Stage of resistance: This is adaptation whereyou try to fight back.
c. Stage of exhaustion: This is extreme fatigueone feels after fighting against stress.
As an example imagine you are in a building,which has caught fire. The place is full of peopleand there is only one exit door. Your first reactionwould be of shock. For some time you are numb,but in no time you try to size up the situation.According to the second stage of resistance, youlook for an alternative way to get out; you breakopen the window glass, jump into the balconyand finally get out of the building. In the processof getting out you may also help others to escapefrom fire. Finally when you are out from thisstressful situation then there is extreme exhaustionand fatigue.
The first two phases of GAS prepare one’sbody to respond to stress in one of the twoways—either attacking the threatening force(fight) or escaping to safety (flight). Thesephysiological responses result from the action ofthe adrenal gland which has been stimulated toincrease the body’s production of adrenalinhormone that gives body the required energyneeded to adapt to the demands of the stressor.
The cognitive components of stress responserepresents the conscious appraisal of the stimu-lus, the individual’s evaluation or perception ofthe situation. This also includes mood state,ranging from elation to tension, depression,difficulty in concentration and fatigue. Copingstyles are also an example of cognitive coping.The behavioural component represents overtbehavioural response to the stressor. Behaviourcan range from withdrawal to aggression, andviolence. Facial expressions also indicatebehavioural reactions. Frequent outbursts ofanger, competitiveness and sexual dysfunctionsare manifestation of stress response.
Types of Stress
Stress is not only desirable but also essential tolife. A certain amount of stress is essential fornormal health. Stresses can be positive ornegative. The positive stress is called ‘eustress’,and the negative stress is termed as ‘distress’
Fig. 10.1: Components of stress

90 Behavioural Sciences in Medical Practice
(Selye 1974). Some events are associated withpositive emotions, while others are associatedwith negative emotions, which in turn determinethe quality of the stress experiences. We usuallythink of negative events or situations as the causesof stress. Some positive changes like constructinga house, a new job, promotion, marriage orbecoming a parent may be stressful due toincreased pressure and responsibilities. As theseare associated with positive feelings likeexcitement, happiness, love and joy, theyincrease our resistance to stress. On the otherhand, negative situations such as death of thespouse, parents illness, interpersonal problems,difficulty at the place of work, financial losses,etc. are all associated with negative feelings suchas sadness, dissatisfaction, conflict, irritation andconfusion. These feelings lower our resistanceto stress and make us more vulnerable to mentaldisturbances and diseases. The negative aspectsof stress can produce harmful effects on the bodyespecially if they are continuing for a long time.Stress produces tension and exerts a greatpressure on the body systems. It is like the bodybeing in a state of constant preparedness to meeta challenge. This tension disturbs the mental andthe physical health. Stress can also preventhealthy and smooth functioning of differentorgans of the body and accelerates the agingprocess.
Stressful Life Events
Research suggests that experiencing an excessivenumber of ‘life events’ in a particular period oftime can lead to increased ill-health. Holmes andRahe (1967) have indicated the relation of lifeevents to our health. These events are normalevents that occur in everyone’s life over alifetime—birth, death, marriage, divorce, newjob, retirement, moving house or going for aholiday. The important factor is how often youexperience these changes, whether they occurtogether at the same time or in a short span of
time and whether they are positive or negative.The greater the amount of social readjustmentrequired, greater the likelihood of developingan illness. Paykel showed that loss events suchas loss of job or death are more likely to beassociated with illness than gain events such asnew addition in the family or buying a newhouse. The variety of illnesses that have beenlinked with life events range from heart disease,cancer and depression to the less life-threateningcommon cold or migraine.
Daily Hassles
Major life events are rare occurrences for mostof us. One does not generally get married morethan once or have more than two or three child-ren, or change jobs frequently. Usually most ofus are able to cope with these events quiteeffectively without being under too muchpressure.
What could actually be more stressful are thesmall daily hassles or events which appear trivial,like standing in long bus queues, getting stuckin a traffic jam, arguments and fights with anuncooperative colleague at work, tensionbetween family members or a very sick, agingparent. These daily tensions can produce acumulative effect and may result in your havinga breakdown one day.
Chronic stress from such daily hassles orstressors can cause physiological damage andalso lead to the development of certain psycho-somatic illnesses such as arthritis, irritable bowelsyndrome, bronchial asthma, hypertension,migraine and other chronic illness.
Stressful Life Events in Children: Children alsoexperience stress and they have different stressfulevents than those of adults. An excess of lifeevents was noted in adolescents attendingoutpatient clinics with recurrent abdominal pain(Green et al 1985). Children tend to report painthat is associated with tension and worry aboutspecific situations—usually academic tests or new

Stress and Coping 91
situations. Vulnerable children who developpsychiatric symptoms, especially those havingpsychogenic pains, demonstrate a directassociation of a traumatic loss and illness event(Mehta et al 1993).
Singh et al (1994) studied the relationshipbetween stressful family life events and somaticcomplaints in 77 school children, and found asignificant association between life event andsomatic complaints, these increasing in almostdirect proportion to the number of stressful familylife events. Occurrence of symptoms was morein girls. The most frequent stressful life events werefinancial problems, moving house, death of arelative, chronic illness in the family and frequentchange in job of parents.
Robinson et al (1988) studied adolescentswith functional somatic complaints (chest pain,recurrent abdominal pain, limb pain, andhyperventilation syndrome). Patients reportedsignificantly more negative life events, a lowerself-esteem, more psychophysiological symptomsand a lower self-evaluation than controls. Theysuggested that functional somatic complaints inadolescents might be associated with poorpsychosocial adjustment and reaction to negativelife events.
Maloney (1980) stressed that grief reactionis often an important precipitant of symptoms.Pantel and Goddman (1972) studied 100adolescents with recurrent chest pain. 31 percent subjects reported occurrence of significantnegative life events within 6 months of onset ofpain.
Scharrer, Ryan-Wenger and Nancy (1991)found that children with RAP had higher meanstress under the parameters of frequency,severity and total stress. Stresses includedparental arguments, not spending enough timewith parents and falling sick. Mean scores forcoping efficacy and total coping were higher innon RAP group.
Rangaswamy and Kamakshi (1983) studiedthe role of stress in 30 adolescent hysterics aged
13-17 years using the social readjustment ratingscale of Coddington for 12-16 years old. Thisstudy was the first systematic study in the fieldof life events in children in India and reportedthat the majority (85%) of hysterics had a signi-ficant life stress before the onset of symptoms.Malhotra et al (1992) found that sick children(hysteria/emotional disorders, hyperactive/conduct disorders, enuresis and miscellaneouscategory) scored higher on life events and stressscores when compared to normal children.
Daily hassles often have more adverse effectthan major stresses. Mehta and Singh (1995)reported that the relatively minor life events, i.e.daily hassles and major life events weresignificantly associated with persistence ofrecurrent abdominal pain (RAP). These childrenexperienced greater incidence of stressful lifeevents like change in school (66%), beginninga new level in school (50%), increase inarguments between parents (43%), change infinancial status of parent (33%), change infather’s occupation (23%), loss of a job of aparent (20%), hospitalisation of sibling (16%),death of grandparent (10%), hospitalisation ofa parent (6%), and mother beginning work(10%). RAP children and control had more orless similar problems but the appraisal (howmuch an event disturbs) was different in the twogroups. Due to poor coping strategies RAPchildren perceived greater negative impact ofstressful events. Children’s perception of stressfulevents was different than that of their parents.Problems related to the personal lives in schoolas well as in the family had more negative impacton them.
Family StressAll of us who live in families, however, have alsoexperienced the kind of stress that we share withothers in our households. Family stress can takemany forms. Many stressors obviously affect theentire family—such events as theft, sickness,marriage or childbirth. In India we have a large

92 Behavioural Sciences in Medical Practice
number of extended families and joint familiesthus family stress is the common problem. If onemember of the family has chronic illness orfinancial loss, the rest of the family members arealso affected.
Executive Stress
The office culture at all levels causes lot ofproblems related to stress. Number of organisa-tions are experiencing that at higher ladderpeople have more and more of stress-relatedproblems, often manifesting in physical problemslike high blood pressure, short temper, insomnia,chronic fatigue syndrome, low back pains,headaches and migraines and increasedconsumption of alcohol and smoking. Theseproblems are now known as executive stress asbesides long hours of work, these people areinvolved in decision making, given lot ofresponsibilities and have result-oriented tasks.They have to meet competitions and challenges.A study conducted at NIMHANS (1996), on thepolice officers revealed that police officers incertain cadres have ‘burnt out’ syndrome—emotional exhaustion, depersonalisation andreduced personal accomplishment. Manyestablished organisations have expressed theirconcerned and have started stress managementprogrammes for their employees.
Test Anxiety
Test anxiety is stress-related factor commonlyseen in students. Virtually all students experiencesome anxiety before a test. But students withexcessive test anxiety feel ‘frozen up’ and panicbefore exams. Due to high level of anxiety theiracademic performance is also affected, even withhard work and high intelligence they are unableto get good results.
Stress-esteem
Pearlin (1989) has observed, that coping styleand social support have effect on stress outcomes.
Self-esteem has been linked to elements of thestress process. According to Rosenberg (1965,1986), self-esteem is “the evaluation which theindividual makes and customarily maintains withregard to himself or herself: it expresses anattitude of approval or disapproval towardoneself”. The process of self-esteem formationis said to involve the principles of “reflectedappraisal”, “social comparison”, and “selfattribution”. Reflected appraisal involves theindividual’s interpretation of how he or she isviewed by others, whereas social comparisonholds that “in the absence of objectiveinformation about themselves people judgethemselves on the basis of comparison withothers”. Self-attribution refers to the tendency todraw conclusions about oneself from observingone’s own actions, including the success or failureof efforts. It is clear that self-esteem is potentiallymodifiable by future social experience.Accordingly, to the extent it is relevant topsychological distress and disorder, it representsone obvious target for prevention and earlyintervention efforts in the service of mental health.The goal of such efforts would be to increasethe individual’s capacity to maintain self-esteemin the face of adversity and, especially, lossevents.
A positive and resilient self-image (in contrastto a negative or labile self-esteem) representsa crucial resource for combating the negativeimplications for self that are the frequentaccompaniments of stressful events. Presumably,the stability and extent of self-esteem is deter-mined by the nature and consistency of one’scumulative experiences of reflected appraisals,social comparisons, and self-attributions.
Self-esteem and Psychological Distress: It hasbeen noted that poor self-esteem can lead todepression. Low self-esteem represents avulnerability factor that increases risk of depres-sion three-fold in the presence of stress. Thesignificance of self-esteem as a mediator of the

Stress and Coping 93
impact of unemployment on psychologicaldistress has been demonstrated by studiesinvolving diverse populations and designs. It hasbeen reported that individuals high in self-esteemappear to be more resistant to the negativeeffects of unemployment than individuals lowin self-esteem.
Low self-esteem is generally taken as a key-defining characteristic of depression. This viewis associated with the cognitive theory ofdepression, which suggests that low esteem maybe state dependent, arising out of depressiveaffect rather than contributing to it. Thus, it canbe concluded that some important part of thecausation involved in the self-esteem-depressionrelationship goes from esteem to depression,and that self-esteem may be especially significantamong the disadvantaged and in high-stresscircumstances. One implication of this conclusionis that prevention or intervention efforts shouldbe made to enhance self-esteem to reduce therisk of psychological distress.
Personality and Stress
Certain personality types are prone to specificillnesses. This understanding helps us to modifya behavioural pattern to prevent the onset ofrelated illness. People who are perfectionists, self-sacrificing, conforming, self-conscious, inhibited,shy and nervous, sensitive, get easily worked up,are more prone to get physical diseases ifexposed to prolonged and severe stress.
Type A personality has often been associatedwith stress and illness. As you will read in Chapter11, that these people are intensely ambitious,competitive and impatient. They are always pre-occupied with deadlines and want to achievethings in the shortest possible time. Type Aperson expends enormous energy in pursuit ofhis goals. Migraine and tension headaches arealso associated with this personality type.
COPING WITH STRESS
There is no way that we can escape stressthroughout life. Stress whether good or bad, isan all-prevailing facet of life. It is unavoidableand inescapable. So, what everyone attemptsis to cope with stress and maintain it at mana-geable levels. We all learn to cope with tensions.
Coping strategies in managing stress requirechange in yourself, others and the environment.You may have to use one of these accordingto the problem or situation. Coping means theways and means you adopt to keep stress atmanageable levels. If you are getting stressedbecause of overwork, you will need to learn torelax, change your working style, bring aboutcertain changes in yourself, so that you perceivethe stressor as not so threatening, or find waysto convert it into a motivating or driving force.If the stress is due to interpersonal problems thenone can discuss with colleagues, similarlyenvironment can be modified by reducing noiselevel, rearranging the things or going for a shortholiday.
It is our reaction to stress that determines theeffect of stress on our life. Cognitive appraisalor our perception of a stressor is the mostimportant aspect of our coping ability, forexample, for some people frequent travelling ispleasurable whereas a person with negativecognitive appraisal would think travelling as verytiring, monotonous, and waste of time. The waywe feel depends to a great extent on the waywe think about the events in our lives. Lazarussees stress as a result of a transaction betweenperson and environment. The way peopleappraise or construe their relationship with theenvironment is a function of cognition, orthought. These thoughts influence the waypeople feel. On the contrary individual’s emo-tions affect the way they make sense out of theworld around them. Thus, emotion (feeling)follows cognition (thought), and vice versa.

94 Behavioural Sciences in Medical Practice
The way we all feel, think and act is a productof the way we as individuals interact with events.All experiences—the good and the bad: arefiltered through one’s unique personalities,personal histories, and viewpoints on life. By andlarge, we determine which of these experienceswill be uplifting and which will be degrading.We do this partly in the way we act to shapeour own lives and partly in the way we reactto the shapes our lives assume.
Coping skills are an individual’s attempt toresolve life stressors and emotional pain. Copingcan be thought of as having two components,the methods used and the focus of the copingresponse. In terms of method of coping, theindividual can utilise either an active responseto resolve the stressful event or choose to avoidthe stressor. The focus of the coping responsemay be directed at the problem itself (problem-focussed) or the emotional consequences of thestressor (emotion-focussed). Active cognitivecoping responses manage one’s appraisal of thestressfulness of the problem itself or its emotionalconsequences. Avoidance cognitive copingresponses include those attempts to avoid havingto confront the problem, like denying a heartattack, and claiming it to be just a severe caseof indigestion.
Coping can be positive and negative. Someof the negative coping techniques are drinkingalcohol, taking drugs, escaping from the stressfulsituation. There are certain ways to cope withthe day-to-day stress in positive way. These arephysical and mental exercises to reduce tension,diversion in various hobbies and activities toavoid negative thoughts, nutrition and healthyeating habits, lifestyle and congenial interpersonalrelationship. The coping strategies usuallyemployed by majority of people are distraction,situation redefinition, direct action, catharsis,acceptance, seeking social support, relaxation,and religion.
In cases where stress is severe and has conse-quently manifested in physical or psychological
problems, help from the professionals shouldbe taken. Stress inoculation training can help incoping with the stress.
Stress-Inoculation Training
Rajeev, a first-year college student, always breaksout in a cold sweat before taking an examination,is so tense and nervous that he forgets all thematerial and goes on to get a low grade on thetest. Since Rajeev wants to do well at theuniversity, he knows he will have to do somethingto overcome this debilitating test anxiety.
One thing Rajeev might do is to seek out aprogramme of stress-inoculation training. Thisapproach uses techniques of behaviour modifi-cation to prevent stress in a variety of specificareas. These programmes educate individualsabout their stressful reactions through an activegive-and-take between leader and participants,give them a chance to rehearse ways to copewith the specific stressor being discussed, andthen have them practice these coping skills ona variety of stressors, from mild to severe. In oneprogramme geared to test anxiety, students areencouraged to learn new, helpful statements thatthey can say to themselves to replace the formeranxiety-producing ones.
Stress-inoculation training has many otherapplications. It can help people overcomephobias, cope with pain, and control anger. Oneinnovative way to use this same basic approachis to prevent stress before it occurs. Cognitivebehavioural approaches have been used verysuccessfully to manage problems arising fromstress. Cognitive behavioural approaches aredescribed in detail in Chapter 21.
Family Coping
The event that affects one human being—illness,a job promotion that requires a move out of town,the loss of a job, any major triumph ordisappointment is likely to affect everyone in thatperson’s family. Not only does the affected

Stress and Coping 95
individual have to cope with the stress, the entirefamily must deal with it. Researchers who havestudied family stress have found that familiescope by the same basic means as individual’sdo by taking actions and changing their attitudes,both to solve the problems and to makethemselves feel better.
Assessment of Stress and Coping
There are various methods to assess stress, thesecan be physiological measures or can be assessedon self-report, questionnaires, checklist andrating scales. One of the examples of rating scaledeveloped for Indian population is given here.For children different scales are used as theirstressors are different than those of adults (Table10.1).
While psychological inventories and tests arealso available that measure how the individualcopes, clinical practice necessitates immediateempirical evaluation of the problem, thevulnerability level, and the coping strategies inuse. The following list suggests guidelines of agenerally useful approach to the assessment ofpatients, whether the predominant problem isward-centred, and illness-related, or personality-related.
1. Do not use a set speech because eachpatient is different.
2. Introduce yourself, even to stuporous orconfused patients.
3. Sit down and try to establish eye contact.4. Avoid asking questions that can be
answered ‘yes’ or ‘no’.5. Learn how to listen and observe.6. Respond as seems appropriate, but make
sure that the patient has the opportunityto talk, too.
7. Monitor your own thoughts because theymay mirror those of the patient, or helpexplain your difficulties in getting across.
8. Modulate and measure your answersaccording to the needs of the patient.
9. Always ask yourself what the patient waslike before becoming ill.
10. Clarification, control and cooling off areusually carried out simultaneously, just asperception, behaviour, and emotion are aunit.
11. Use the most timely, informative, andevocative questions, such as:
a. What has bothered you most about thisillness?
b. How has it been a problem for you?c. What have you done (or are you doing)
about the problem?d. What has been the most difficult thing you
have had to face until now?e. What did you do then?f. Whom do you rely on most, or expect
will be most helpful to you?g. In general, how do things usually turn
out for you?h. Tell me what you think about this whole
situation.
Clinical Applications
Effect of Stress on Health Coping is a problem-solving behaviour designed to bring about reliefand equilibrium. The common denominator ofcoping is to have a problem. The common taskof physicians and patients is to solve problemsrelated to being sick, that is, the medical plightbeyond mere physical changes and conse-quences. Coping, therefore, is an integral partof medical practice as well as illness. With thesame disease at comparable stages, and withmore or less equivalent treatment, patients mayhave different problems, and physicians maythemselves respond with a wide variety ofreactions, diagnoses and management.
Coping means that one has to overcome athreat or master a risky situation. How patientscope is a complicated mixture of cognitiveappraisal and reappraisal, initial responses andcorrected responses. Being sick is a problem in
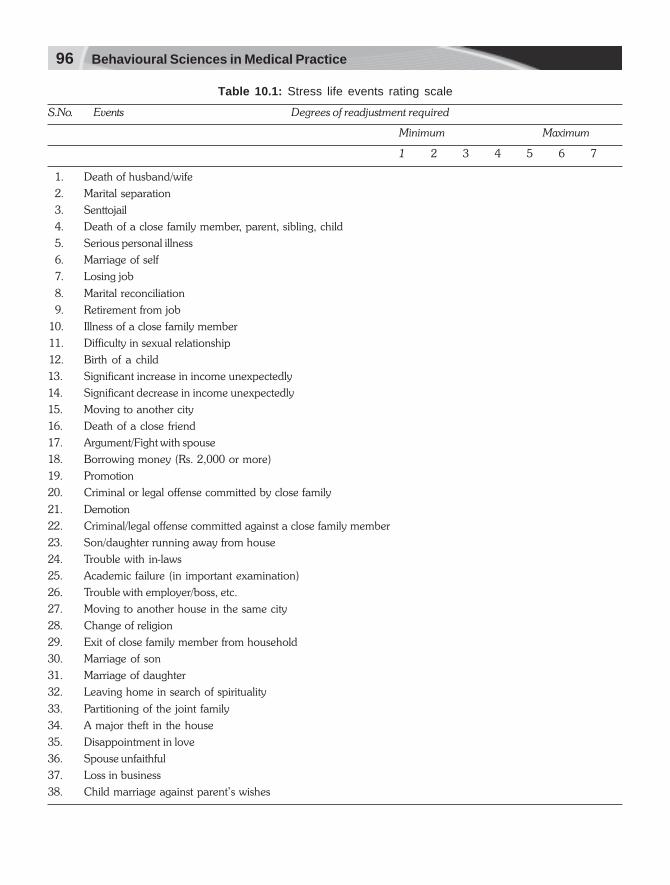
96 Behavioural Sciences in Medical Practice
Table 10.1: Stress life events rating scale
S.No. Events Degrees of readjustment required
Minimum Maximum
1 2 3 4 5 6 7
1. Death of husband/wife
2. Marital separation
3. Senttojail
4. Death of a close family member, parent, sibling, child
5. Serious personal illness
6. Marriage of self
7. Losing job
8. Marital reconciliation
9. Retirement from job
10. Illness of a close family member
11. Difficulty in sexual relationship
12. Birth of a child
13. Significant increase in income unexpectedly
14. Significant decrease in income unexpectedly
15. Moving to another city
16. Death of a close friend
17. Argument/Fight with spouse
18. Borrowing money (Rs. 2,000 or more)
19. Promotion
20. Criminal or legal offense committed by close family
21. Demotion
22. Criminal/legal offense committed against a close family member
23. Son/daughter running away from house
24. Trouble with in-laws
25. Academic failure (in important examination)
26. Trouble with employer/boss, etc.
27. Moving to another house in the same city
28. Change of religion
29. Exit of close family member from household
30. Marriage of son
31. Marriage of daughter
32. Leaving home in search of spirituality
33. Partitioning of the joint family
34. A major theft in the house
35. Disappointment in love
36. Spouse unfaithful
37. Loss in business
38. Child marriage against parent’s wishes

Stress and Coping 97
itself. But the fact of being sick sends waves intothe far reaches of a patient’s life, undoingpsychosocial balance, and even initiating illnessin significant others (family and friends).
Disease-related problem: Different diseases havetheir own special complications with whichalmost every victim must cope. A disfiguring scar,ataxia, a colostomy, a restrictive diet, and so forthrequire some form of primary rehabilitation andretraining that entails coping processes.Behavioural scientist in a general hospital dealswith psychosocial problems. Some of these arecomplications of rehabilitative procedures. Forexample, it is not uncommon for an elderlyperson to prefer a wheelchair to a prosthesis aftera leg amputation. The patient may be able towalk well with assistance in the hospital, but bereluctant to venture beyond his room when hereturns home. The treating doctor can talk aboutthe amputation with the patient, and then aboutthe living arrangements, the emotional supportreceived or not received from others, and fearsabout walking unaided or alone on a crowdedstreet. Behavioural Scientist is now being askedmore often to help patients suffering from“diseases of progress”. Almost every advance-ment in medicine is followed by an unexpectedcomplication. Treatments that save patients fromone disease may expose them to several others.The secondary problems of immunosuppressionare prominent examples that require psycho-social intervention.
Sickness-related problems: Illness have itsinterpersonal and intrapsychic qualities that mayundo medical and surgical efforts. When thelimits of medicine and surgery have beenreached, psychosocial problems may just begathering momentum. For example, a youngfather who develops carcinoma of the lung isnot just physically sick. He worries about his jobas well as about other psychosocial compli-cations of illness and its treatment. He maycomplain about the physicians, argue with his
wife, and even blame his children for his plight.All these objectionable results may conceal deeppessimism about survival and fear of abandoningpeople closest to him.
For some people, patienthood is easier thanfunctioning in the outside world. A person whosubmits courageously to a series of operationsmay not be able to work when recovered andthereby becomes an even greater liability thanbefore the surgery began. Every illness shouldbe presumed to carry a balance of gains andlosses for the individual. An unexpectedimprovement or recovery in a patient who hasbecome accustomed to invalidism and the sickrole may induce relative ego impairment if toomany psychosocial responsibilities are thrust onthe patient too quickly. Survival, support andself-esteem are only three important problemsfaced by chronically-ill patients, including thosewho are rescued from invalidism through newermedical and surgical treatments.
Vulnerability
Vulnerability refers to the emotional distress thatis the most personal aspect of illness. It reflectsimpairment of competence, control andconsciousness. Consequently, vulnerability notonly signifies distress in the here-and-now, buta disposition to behave or conduct oneself at lessthan full efficiency. The ways in which the humanbeing is vulnerable are both endless andunexpected.
Manifestation of poor coping: While dealing withother people you would meet people who arenot good in coping with the daily hassles orstresses. Here are some behavioural patterns thatcan be observed in these individuals.
Vulnerability: Hopelessness -Patient believes thatall is lost; effort is futile; there is no chance forrecovery.
Turmoil/perturbation: Patient is tense, agitated,restless, indicating inner distress.

98 Behavioural Sciences in Medical Practice
Frustration: Patient is angry about inability toresolve problems and get relief.
Despondent/depressed: Patient is dejected,withdrawn, tearful, and often inaccessible tointeraction.
Helplessness/powerlessness: Patient feels unableto initiate positive action; complains of being tooweak to struggle; surrenders and defaultsdecisions.
Anxiety/fears: Patient has specific fears or dreads;feelings of panic or impending doom.
Exhaustion/apathy: Patient feels depleted andworn out; expresses indifference to outcome.
Worthlessness/self-rebuke: Patient feels no good,defective; blames self for weakness, short-comings, and failures,
Painful isolation/abandonment: Patient feelslonely, ignored, alienated from others whoallegedly do not care.
Denial/avoidance: Patient speaks or acts as ifunwilling to recognise threatening aspects ofillness; minimises complaints or findings.
Truculence/annoyance: Patient is embittered,feeling victimised or mistreated by someone orsomething outside, beyond control.
Repudiation of significant others: Patient rejects,turns away from, or antagonises sources ofpotential help and support, usually a familymember or friend.
Closed time perspective: Patient foresees a verylimited future; day-to-day existence.
Vulnerability and the variations of copinghave a somewhat reciprocal relationship, at leastfrom the clinical viewpoint. Few patients use onlyone or two strategies to cope with very importantproblems, because in coping with importantproblems patients recall past experiences andapprehend future obstacles. Given a suitablecombination or sequence of strategies, the
patient who copes effectively will experiencereduction of distress, relief, and perhaps evenresolution of problems. Of the three principalparts of a patient’s plight, coping is by far themost difficult to detect. The distress ofvulnerability is usually far more obvious becausehigh levels of vulnerability are what promptedconsultation in the first place.
Good copers also have good doctor-patientrelationships. They are optimistic and resourceful,can directly confront problems, and then canrevise them in “cope-able” terms. Suppressionand denial are only temporarily effective. Goodcopers are flexible in using all available options,just as they faced difficult situations in the past,even though the illness is the unique problemfor every patient.
In contrast, patients who are poor coperstend to have higher emotional distress and donot clearly recognise pertinent psychosocialproblems. The habits of avoiding, nullifying anddisguising problems as well as the failure to beclear and communicative are diagnostic signs ofpoor coping. Blaming others or themselves isalso an indication of poor coping potential. Itis usually important to ask about timeperspective and anticipated recovery, since thesegive a clue to how pessimistic or realistic thepatient’s view of the illness is. The doctor whoworks with patients needs experience in interviewskills to deal with medical and surgical patientswho are not primarily motivated to seek or usepsychotherapeutic interventions.
SUMMARY
Stress is a stimulus event of sufficient severityto produce disequilibrium in the homeostaticphysiological systems. The stimulus that evokesa stress response is called a stressor. A stimulusbecomes a stressor either by the cognitiveinterpretation or meaning that the individualassigns to the stimulus or by the fact that thestimulus affects the individual by way of some

Stress and Coping 99
sensory or metabolic process, which is stressful.In physiological terms stress is the body’sresponse to any stressful demand. In psycho-logical terms stress is an individual’s cognitivejudgement that his or her personal resources willbe taxed or incapable of dealing with thedemands posed by a particular event.
Stress comprises of stressor, stress responseand the individual’s coping resources like skillsand social support systems. Stressor representsstimulus events requiring some form of adapta-tion or adjustment. Stressor can be internalstimuli like cognitions or thoughts or externalstimuli like crowd, noise, and interpersonaldifficulties.
Stresses are classified as positive or negativestresses.
An excessive number of ‘life events’ in aparticular period of time can lead to increaseill health. The variety of illnesses that have beenlinked with life events range from heart disease,cancer and depression to the less life-threateningcommon cold or migraine.
Major stressful life events and daily hassleshave been reported to have association with illhealth. In children a significant association hasbeen found between stressful life event andsomatic complaints. The most frequent stressfullife events were financial problems, movinghouse, death of a relative, chronic illness in thefamily and frequent change in job of parents.
Self-esteem has relevance to psychologicaldistress and disorder. In many psychiatricproblems self-esteem is one of the componentsfor prevention and early intervention efforts in
the service of mental health. Poor self-esteemis three times more in depressed patients.
Coping strategies in managing stress requirechange in yourself, others and the environment.Coping means the ways and means you adoptto keep stress at manageable levels. Coping hastwo components, the methods used and thefocus of the coping response. Coping can bepositive and negative. Some of the negativecoping techniques are drinking alcohol, takingdrugs, escaping from the stressful situation. Thereare certain ways to cope with the day-to-daystress in positive way.
There are various methods to assess stress,these can be physiological measures or can beassessed on self-report, questionnaires, checklistand rating scales. One of the examples of thecommon task of physicians and patients is tosolve problems related to being sick. Coping isan integral part of medical practice as well asillness. Different diseases have their own specialcomplications with which almost every victimmust cope. A disfiguring scar, ataxia, a colostomy,a restrictive diet, require some form of primaryrehabilitation and retraining that entails copingprocesses. Sickness-related problems haveinterpersonal and intrapsychic qualities that mayundo medical and surgical efforts.
Vulnerability refers to the emotional distressthat is the most personal aspect of illness. Itreflects impairment of competence, control andconsciousness. Consequently, vulnerability notonly signifies distress in the here-and-now, buta disposition to behave or conduct oneself atless than full efficiency.

11Personality
Sivati, 24 years old female, is pursuing a careerin town planning. She is elder of two sisters ina nuclear family. She has had an outstandingacademic record. She is very conscientious,overdutiful, perfectionist and rigid which ismanifested in all forms of behaviour fromhandwriting to keeping clothes, things, dressingand other tasks. As she adheres to very highstandards of performance, she expects similarstandards of performance from others too. Thisexpectation from others often causes angeroutburst and creates problems in interpersonalrelationship. She is always in a hurry to completetasks, is not able to relax and often gets severeheadache. This is an example of how personalitydetermines behaviour of a person and itsrelationship in developing illness.
In our everyday lives we are accustomed tomaking some kind of assessment of other people.If we are asked to describe someone we know,we are likely to say something about hisappearance and other aspects of behaviour,which characterise him as an individual who isdifferent from others. There are always varia-tions in individual’s personality development, andfunctioning which results in a unique personality.
Definition
Personality is a stable, characteristic way a personfeels and behaves in a variety of situations.Personality as a concept is difficult to define andpsychologists also differ in their explanation of
personality, some mention it in terms of qualities,some as characteristics of person’s behaviour ormay be both. RB Cattell, (1965) defines it, asthat which determines behaviour in a definedsituation and a defined mood. The assumptionhere is that the behaviour of the individual willdepend not only on the situation in which hefinds himself but also on his emotional state atthat time. It is the stability during this period,which allows behaviour to be predictable withinlimits. Gorctn Allport, a pioneer in personalityresearch has defined personality ‘ as a dynamicorganisation within the individual, of psycho-logical systems that determine his uniqueadjustments to his environment’. According toMischel (1976) personality consists of distinctivepatterns of behaviour that characterise eachindividual’s adaptation to his life. Reference mustalso be made to two other terms usedsynonymously with personalities, character andtemperament. Character is a word that tendsto be used in a morally judgemental way; theindividual is evaluated in terms of cultural normsagainst which he is seen ‘good’ or ‘bad’.Temperament refers to the emotional respon-siveness of a person, such as hot tempered-placid,fearful-unworried.
Determinants of Personality
Every child is born with certain potentialities. Thedevelopment of these potentialities dependsupon maturation and upon experiences

Personality 101
encountered in growing up. The determinantsthat shape personality are viewed from differentperspectives. The major distinction is drawnbetween biological influences, most likely to begenetically determined and environmentalinfluences determined by family, school, peergroup and culture.
Heredity
The relative contributions of heredity in theformation of adult personality have been studiedby twin studies and statistical methods.
Eysenck studied personality dimensions inidentical twins and nonidentical twins and foundthat the score on the dimensions of extra-versionand neuroticism showed no significantcorrelation between the nonidentical twins butwere closely related for the identical twins.
Physique: Further evidence of importance ofbiological factors in personality comes fromindividual differences to variation of physique.Kretschmer has given concept of personalitytypes based on physique. The two types beingschizothymic and cyclothymic personalities.These two types were correlated to majorpsychiatric disorders schizophrenia and manic-depressive psychosis respectively. The schizo-thymic is shy, inward looking with long andnarrow body build. This type corresponds toJung’s introvert personality. This cyclothymic issociable, outward looking, but liable to swingsof mood have muscular or fat body build. Thistypes corresponds to Jung’s extrovert perso-nality.
Sheldon identified three types of physiquefrom a large number of photographs of malecollege students. According to him there arethree personality types associated with functionsof, the body organ and systems developedfrom the embryonic layers. The three types are:(i) the endomorphic, the viscerotonic persona-lity is characterised by a love of comfort and of
food, (ii) the mesomorphic, muscular buildindividuals with a somatotonic personality, arevigorous, active and assertive, (iii) theectomorphic the cerebrotonic personality isdominated by the central nervous system withinhibition, restraint and little social contact. Thesephysical body types and personality typesrepresent the extreme dimensions rather thancategories.
Environment
Personality characteristics are the result ofinteraction between the individual and the socialand physical conditions of the situation. Theenvironmental factors advocate that personalitycan be acquired. In the process of personalitydevelopment psychosocial determinants play acrucial role.
Family: A family fulfils the basic physical andpsychological needs of children as also seen inChapter 16. During the early years of develop-ment the parents are the role models andthrough them various behaviours are learned,try to recall the time when you behaved just likeyour own mother or father. Family also transmitscultural values and norm, which influences yourthinking process.
School and peer group: School environment isdifferent in various schools; some emphasisecompetition, some high academic achievement,and some schools place greater importance tooverall development and some devote moretime on creativity. The differences in schoolenvironment contribute towards personalitydevelopment of their students. Similarly the peergroup influences are well known in thedevelopment of adaptive as well as maladaptivepersonality traits. If you are in the company ofhigh achievers, you are also motivated to dowell.
Culture: There has been a considerable amountof research on influence of culture on

102 Behavioural Sciences in Medical Practice
personality. Some cross-cultural studies havebeen conducted to study the effect of cultureon various personality traits. McClelland founddifferences between ratings of achievementimagery in TAT stories of school boys in Japan,Germany, Brazil and India. Measures of field-dependence have also shown cross-culturalvariations in many studies. The differences havebeen found in cognitive style and different childrearing practices. It has been found that aperceptual skill required for the performance ontest of field-dependence depends upon pastexperience of similar task and which will varyfrom one culture to another. Cattell’s 16 PF testhas also been used to study cultural influences.If we apply cultural differences to study perso-nality differences in our country, you wouldobserve characteristic differences in individualsreared in urban or rural backgrounds. In someof the Indian studies conducted on dis-advantaged children, it was found that learningof psychomotor skills was delayed in childrenwith rural background. Similarly, culturaldifferences on personality can be seen in ourcontext in individuals belonging to differentcommunities like Punjabis, Bengalis, Biharis,Tamilians, etc.
Theories of Personality
Personality has been studied in a number of ways.The explanation of how people acquire andchange the relative aspects of their behaviourcomes from different theories of personality.Each personality theory has characteristicimplications regarding the meaning of adjust-ment and deviance. However, two differentapproaches to study the concept are, theideographic and the nomothetic—the formeremphasises the uniqueness of the individual withintensive investigation of single cases and the latterwith generalisation in the form of universal laws.Different theories may adopt any one of theapproaches.
There are different schools of psychologicalthought about development of personality.There are number of different approaches tostudy personality. Cattell (1965) describes threehistorical phases in the understanding ofpersonality. The oldest, though still continuingto the present day, is the prescientific or literaryand philosophical phase. Many of the greatpoets, novelists and playwriters have, in theirwritings and especially in the characters havecreated and conveyed seemingly brilliant insightsinto the complexities of human nature. Thesecond historical stage is called by Cattell theprotoclinical, since it was based largely onobservation of psychiatrically sick people by‘founding fathers’ of psychiatry like EmilKraepelin in Germany and Pierre Janet inFrance, but more especially Sigmund Freud andhis early associates Carl Jung and Alfred Adler.Among the personality theories of psycho-dynamic approach, only the latter theoristswould be discussed here. Two major limitationsto this essentially descriptive historical phase inpsychology are; first, the fact that it was derivedfrom the study of psychological abnormalityrather than the ‘normal’; and second, the virtualabsence of any attempt at measurement.
The characteristics of the third stage areevident from Cattell’s description of it asquantitative and experimental. In other words,the scientific study of personality based on actualbehavioural measurements. Four major theoriesof personality, psychodynamic, trait and type,social learning and humanistic theories arediscussed in this section.
Psychodynamic Theories
The psychodynamic approach is ideographic,arising from observations made, during thecourse of treatment of psychologically disturbedpatients. Psychodynamic approach has receivedconsiderable recognition on the basis of Freud’swork. According to him, the structure of mind

Personality 103
is seen as functionally differentiated into threeparts; Id, ego and superego. The unconsciousid energises primitive instincts or drives, whichare satisfied, by wish-fulfilling fantasies. Id isgoverned by pleasure principles. The largelyconscious ego, gradually develops in order tomediate between the demands of the id andthe constraints of the outside world in accordancewith the reality principle and guided by the thirdstructure, the superego, which represents thevalues and controls of society and other controlsof society through early identification with theparents and other figures of authority (Fig. 11.1).
The instinctual energy of the id, mainly inthe form of libido is concerned with sex and self-preservation attached to different erogenousareas of the body—oral, anal and phallic—though as a result of excessive gratification orfrustration it may become fixated at a particularstage. Later the libido becomes more outwardlydirected as erotic feelings toward the parent ofthe opposite sex, with rivalry and fear of theparent of the same sex develops into an Oedipusor Electra conflict which should be successfullyresolved by identification with the same-sexedparent and repression of the sexual drive duringthe latency period, until its reawakening atpuberty in the final genital stage of development.
Another important aspect of psychodynamictheoryconcerns with the defense mechanisms
used by the ego to reduce or avoid anxiety. Theego has several defense mechanisms at itsdisposal to protect itself from being traumatisedby the stress arising from these conflicts. But theego is not always aware of what the needs ofthe id and superego are, because many of theseneeds are unconscious. The occurrence of signalanxiety warns the ego that libidinal tensions havebecome so strong that it must either handle themor be disabled by stress.
All the defense mechanism has threecharacteristics in common: (i) they reduce stressand anxiety, (ii) they deny or distort reality, and(iii) they operate at unconscious level. Some ofthe common defense mechanisms are: repres-sion, denial, rationalisation, displacement andsublimation, and identification.
Repression: It is the most important defensemechanism. It is the process by which the egoblocks off threatening thoughts or desires andthus keeps them from sweeping into the spotlightof consciousness. Most of these experienceshave undischarged libidinal energy attached tothem in some way. In repressing theseexperiences, the ego has to use up some of itsown energy sources. And the more painful thememory, or the stronger the unacceptable urge,the more energy the ego must expend in orderto keep the material repressed. Eventually theego may run out of steam, and bits and piecesof the repressed material may leak though toconsciousness as slips of the tongue, or assymbols in dreams.
Denial: As you would see during your clinicalpractice that many patients deny having anillness. Denial is a defense mechanism by whichthe ego shuts itself off from certain realities,especially which is painful facts.
Rationalisation: Again you would see patientswho would give rationalisation for their non-compliance of treatment, e.g. a chronic alcoholicmay rationalise for his drinking by saying thatFig. 11.1: Relation of Id, ego and superego

104 Behavioural Sciences in Medical Practice
the drink provides him energy to earn moneywhich is very important for bringing up of hischildren. Rationalisation is offering elaboratejustifications for behaviours that are illogical orimmature.
Displacement and sublimation: The child’s egogains the ability to displace the flow of libidinalenergy from one object to another. But the egomay use this ability inappropriately, as a defensemechanism. If the child gets angry with its mother,it dares not hit her because it will be punished.Therefore, it displaces its anger towards a safeobject—such as a doll—that cannot retaliate ifthe child strikes it.
Sublimation is a form of displacement andmost mature of the defense mechanisms. In thisthe energy is channeled away from unaccep-table to socially acceptable acts. For example,an unmarried female may sublimate her sexualdrives in form of painting or art work.
Reaction formation: in reaction formation theego changes unacceptable love into acceptablehate or vice-versa. If a mother hates a child—a feeling she must deny conscious awareness of—the mother may pat the child with affection. Orthe mother’s ego may indulge in projection bypretending that the child actually hates her. Shethus projects her unacceptable emotions ontothe child.
Identification: In the next Chapter 12 onDevelopment—Infancy to Adolescence you willread about psychosexual development theory,which describes Oedipus complex and Electracomplex. Many people resolve their Oedipus orElectra crisis by taking on the characteristics oftheir same-sex parent. The young girl identifieswith her mother. In adolescence, the girl identifieswith other women and strengthens the consciousportion of her superego. Ego-ideals help toreduce anxiety by allowing the person to releaselibidinal energy in socially approved ways.
Early splits with Freudian psychoanalysisresulted in Alfred Adler’s school of individual
psychology and Carl Jung’s analytical psycho-logy, Adler claimed that even in normalcircumstances a child feels helpless and beginsto develop a particular strategy or lifestyle, tocompensate for feelings of inferiority and to reachthe goal of superiority. Adler drew attention tothe importance of the ego and nonsexual factorsin the personality. Jung also reacted againstFreud’s emphasis on sex. The motivating forcein Jung’s view, although still called the libido,was nonsexual and more in the nature of a lifeforce. Jung postulated not only a conscious mindand a personal unconscious, but in addition amuch larger collective or racial unconscious con-taining the beliefs and myths of the individual’srace and at a still deeper level, a universalunconscious shared with all humanity. Jungcalled the collective unconscious archetypes.Psychosocial developmental theory of ErikErikson (see Chapter 12) who, with ErichFromm, Karen Horney and Harry Stack Sullivan,comprised the sociologically oriented groupknown as the neo-Freudians that developed inUSA during 1930s. Emphasis was placed on theinterpersonal rather than the intrapsychicdimension and on the conflicts, which may arisein relationships between the individual andothers as well as within himself. More recentlyobject relations theory, describes ‘object’ in thesense of a psychologically significant person orpart of a person, has stressed the relationshipof the individual to such objects. The stages ofdevelopment are then seen as different meansof achieving such relationships (e.g. throughfeeding at the oral stage), and adult personalityas being much influenced by the nature of theseearly relationships.
Trait and Type Theories
These theories focus on internal influences onpersonality. According to this viewpoint, perso-nality is consistent from situation-to-situation notbecause of an emotional outlook coloured byearly experience, nor because of universal

Personality 105
needs. Rather these explanations focus onspecific attributes peculiar to the individual, insome cases physical and in others psychological.Some of these theories divide individuals intodistinct categories as being of one type or another.Jung’s introverts and extroverts are types.Sheldon’s classification according to the physiqueis also an example of personality types. Traittheories look at individuals not so much in termsof extremes of one type or another but as blendsof many different characteristics that individualshave to a greater or lesser extent.
Allport differentiated between individual andcommon traits. A term trait was reserved forcommon traits and a new term personal disposi-tion was introduced for individual trait. Theimplication is that a trait may be shared by anumber of individuals. According to Allport, aspecific act is always the product of manydeterminants not only of lasting sets, but alsoof momentary pressures on the person and inthe situation. It is the repeated occurrence ofacts that allow one to make necessary referenceof traits and personal dispositions later on Allportdistinguished traits and types in terms of theextent to which they are tailored to the indivi-dual. Allport maintained that each of us has apersonal disposition made up of a cardinal,central and secondary traits. A cardinal trait isso dominant that it colours virtually every aspectof a person’s behaviour and attributes. Centraltraits are handful of characteristic tendencies thatwe would ordinarily use to describe a person.The secondary traits are displayed by us fromtime-to-time, but are not strong enough to beregarded as integral parts of our personality.
Cattell assumes that there are natural ele-ments of personality, which can be discoveredusing the technique of multivariate analysis.Cattell began his researches by taking trait namesused in everyday language to describe humanbehaviour. He then rated individuals on the traitdescription and inspection of the ratingssuggesting that about 40 basic dimensions are
involved. The 16 first order or primary factors,which make up 16 PF questionnaires, have beenmost intensively considered by Cattell and hisassociates. These factors are called ‘source traits’.We all have same traits but to different degreesand in this way, no two individuals are exactlyalike.
Eysenck (1990) stated that each type is madeup of a set of personality characteristics. Threemajor personality types or dimensions havebeen listed by Eysenck, namely extroversion,neuroticism and psychoticism. For examplepeople who fit Eysenck’s extroverted type aresaid to be characterised as sociable, lively andexcitable. Each one of these characteristics canbe broken into a habitual response, which canfurther be broken down to specific responseswithin specific situations. This progression frombroad to specific responses made Eysenck’sapproach into a hierarchical theory.
The big Five: There are five basic dimensions,theorised to underlie the many traits used todescribed human behaviour, known as big five.Each of the dimensions is bipolar, one of theends of the dimension describes the ‘high’ poleand the opposite end describes the ‘low’ pole.These five dimensions are—• Openness to experience: creative intellectual
and open minded vs. simple, shallow andunintelligent.
• Conscientiousness: organised responsible andcautious vs. careless frivolous, irresponsible.
• Extroversion: talkative, energetic and assertivevs. quite reserved and shy.
• Agreeableness: sympathetic, kind andaffectionate vs. cold, quarrelsome and cruel.
• Neuroticism: emotionally stable, calm andcontented vs. anxious, unstable andtemperamental.The big five theory is a comprehensive
descriptive system. This approach accommodatesmany scientific approaches to personality. Thesefive factors have been included in a personalityassessment instrument, the NEO-pi (Caprara

106 Behavioural Sciences in Medical Practice
et al 1993). This inventory has been used tostudy personality characteristic in clinical andresearch studies (Costa and McCrae, 1992).
Social Learning TheoriesThe social learning approach to personality hasderived its main impetus from the behaviouralmovement in psychology and partly from dis-satisfaction with trait approaches. Behaviouralpsychologists take quite a different approach.Generally speaking, they see personality deve-lopment as being a set of learned responses.Thus, according to BF Skinner, you became whoyou are primarily because that is what your socialenvironment has conditioned you to be.
Skinner believes that behaviour is, above allelse, lawful. By this he means that your actions(and hence your thoughts and emotionalresponses) are predictable because they areprimarily under the control of external, measur-able influences. You do not eat because you are“hungry”, but rather because you have beenconditioned to eat in the presence of certainenvironmental stimuli. Indeed, “hunger” has nomeaning to Skinner because it refers to a subjec-tive “inner state” rather than to an objective setof behaviours. Your “psychic energy” comes notfrom dynamic forces working deep within yourunconscious mind, but from external inputs.
Skinner rejects not only all intrapsychicaspects of personality development, but mostbiological influences as well. Innate reflexes arealways modified by experience. If you wish tostudy personality development, you shouldfocus entirely on how a given society trains itschildren. For if you change the pattern of“parenting behaviours” in a culture, Skinnerbelieves, you will completely alter thepersonalities of children reared in that culture.Social learning theories, especially that ofBandura and Walters postulated that all learningneed not be direct (see Chapter 5). Imitationaccording to Bandura and Walters, plays aprominent role in learning. We try to imitate
what we observe especially, when we identifywith certain models in our environment. Theselection of a model again depends on the age,sex, motives, etc. For example A child usuallytakes mother as a model. They have also pointedout how wrong models could set bad examplesto the individual.
Situational determinants of behaviour havealso been considered in social learning approach.Situations by themselves do not evoke anybehaviour but it is given a meaning by theperson. Different situations have their ownmeanings to people. Thus, situations influenceone’s behaviour in unique manner, on the basisof one’s previous learning experience. Tosummarise, the social learning viewpoint placesa great emphasis on the importance of learningand situations in personality. Human behaviouris only a resultant of person, situation variablesand their interaction.
Humanistic Approach
A number of theorists have focussed on theconcept of ‘self ’ in personality. Self has twodistinct sets of feelings. One set has to do withpeople’s attitude about themselves, their selfconcept and second set relates to the processesby which the individual copes, remembers, thinksand plans. Self concept are central to humanistictheories. Carl Rogers and Abraham Maslow aretwo most influential humanistic theorists.
Rogers believes we are born with no self-concept, and no self—but we do have an innateurge to become fully functioning and actualisedpeople. At birth, all we have is a confusing setof sensory impressions, physiological processes,and motor activities. Rogers calls this sum totalof our experience the phenomenal field. As wemature, the outside world imposes a kind oforder or logic onto this field. And, as we becomeaware of this logic, our self emerges anddifferentiates itself from the phenomenal field.The self is thus the conscious portion ofexperience.

Personality 107
Rogers believes you are most likely to run intodevelopmental problems when society wants youto become something that conflicts with your owninternal values or standards. If you yield to thedemands of society too much, your psychologicalexperience is distorted and your self-conceptsuffers accordingly. Most of your experiences areunconscious, i.e. below the threshold ofawareness. But you can bring almost anyexperience above threshold if you merely givethe experience a name or a label. That is, youmake an unconscious experience conscious bydeveloping word-symbols that allow you todescribe (and hence think about) the experience.If a particular event threatens your self concept,then you may refuse to symbolise this even inwords or thoughts. But if you cannot toleratesome of your own behaviours, you will haveproblems achieving full actualisation because youare continually hiding some of your own valuesor motivations from conscious expression.
When you can accept yourself completely,you become what Rogers’s calls a fully function-ing individual. You are open to all experienceand you defend against nothing. You are awareof both your faults and your virtues, but youhave a high positive regard for yourself. And,most of all, you maintain happy and humanerelationships with others.
Abraham Maslow took his ideas abouthuman behaviour from studying highly creativeand psychologically healthy people. Maslowassumed these individuals had achieved a highdegree of self-fulfillment or they would not havebeen so prominent and demonstrated suchleadership. By determining the similarities amongthe members of this noted group, he arrivedat the characteristics of a truly “self-actualised”person.
Most psychoanalytical theories focus on whatcan go wrong during the developmental years.That is, they emphasise the possibility of sickness,not the probability of success. Maslow’sapproach is different, for he looks primarily at
the healthy side of human nature. As we notedin Chapter 8, Maslow has created a hierarchyof needs, of which self-actualisation is thehighest. Maslow acknowledges the strength ofour physiological instincts, but sees them as being“basic needs” easily satisfied in most civilisedsocieties. Our drives for food and sex are partof a more impelling intrapsychic urge-an active“will toward health”—that drives us up thedevelopmental ladder toward self-actualisation.
Humanistic theories emphasise the impor-tance of people’s subjective attitudes feelings andbeliefs, especially with regard to self. Theoriesof this type are often criticised for their heavyreliance on subjective self report data but suchdata can provide one with respectable insightsinto people.
Personality Related to Illness
The idea that personality traits and psycholo-gical characteristics play a role in the aetiologyof physical disease has its roots in medicine andphilosophy before Descartes. Early physiciansbelieved that intense emotions could produceimbalances in bodily function, culminating invarious forms of physical pathology. In the firsthalf of this century, the role of chronic emotionalconflicts in the aetiology of physical disorderswas emphasised. Based on observations ofclinical groups, correlations between particulardiseases and personality types were reported,and striking psychological similarities amongpatients suffering from the same organic diseasewere described. These similarities wereformulated and linked to specific disorders suchas coronary heart disease (CHD), peptic ulcer,and asthma. Later trait approaches suggestedthat certain dispositions, such as giving up,depression, and inability to express feelings wererelated to general susceptibility to illness. Recentstudies suggest that epidemiological evidence fora link between Type A and CHD is no longerunequivocal. A number of studies have

108 Behavioural Sciences in Medical Practice
quantified the degree of coronary artery diseasepresent in patient, undergoing coronaryangiography and have correlated disease seve-rity with measures of Type A behaviour. Patientswith Type A personality were likely to have severecoronary artery disease in comparison to TypeB patients. However, subsequent studies foundthat Type A was not associated with extensivecoronary artery disease.
Behaviour Patterns andCoronary Heart Disease
Behaviour patterns and its relationship to healthhas been described in our ancient Indian systemof medicine, Ayurveda. The fundamentals forprevention of disease and promotive health carewere related to the following tenets:• Achaar (conduct)• Vichaar (thought)• Vyavahaar (interpersonal dealings)• Ahaar (nutrition).
These four tenets are components ofpersonality and variations in these cause illnessboth physical and mental. While some of youwould not agree that there seems to be anapparent relationship between physical healthand our actions, but in all cultures it has beenobserved that the spiritual component energisesand helps in coping with stress. A relaxed mindis certainly more productive than an agitated andtensed one. Tension and stress may lead to wrongdecisions, thus to prevent and control stressrelaxation exercises should be practiced (Wasir1995).
Considerable attention has been devoted tothe study of “coronary-prone” behaviourpatterns, and two general patterns have beenidentified. The first consists of negative, distur-bing emotions such as life dissatisfaction, anxietyand depression. Given generally fairly highcorrelations between these dysphonic cha-racteristics seems reasonable to incorporate theminto the broad rubric of “neuroticism”. A second
example of a “coronary prone behaviour”conceptualisation is the Type A behaviourpattern, which is the most extensively researchedpsychosocial risk factor of CHD. Individuals withthe Type A behaviour pattern are characterisedby action emotion complex, struggle to achievemore in short time, autonomous, statusconscious, power hungry, inpatience, free-floating hostility. These individuals are intenselyambitious, competitive, short tempered and havetime urgency. In contrast, type B individuals arerelatively relaxed and easy-going.
Type A can be assessed by the structuredinterview in which individuals are asked toindicate how they usually respond in situationsthat is likely to elicit competitiveness, impatienceand hostility in certain individuals. The evaluationof Type A is primarily based on speech stylistics,such as loudness and explosiveness, content ofthe answers. A number of questionnaires forassessing Type A exist; the Jenkins Activity Survey(JAS) (Jenkins, 1976) is the most commonlyused. Studies that have correlated various TypeA measures with other psychological scales. Selfreport measures correlate more highly withnegative emotional states. In a classical studyknown as the Framingham Heart Study (Haynes,Feinleib and Kannel, 1980) an adhoc scale wasused to measure Type A behaviour. Individualswho were classified as Type A were more likelyto have developed CHD at the follow up eightyears later than were Type B subjects. Theframingham scale predicted the development ofmyocardial infarction alone, angina alone andmyocardial infarction with angina.
Type A and Physiological Reactivity
Since associations between Type A and ischaemicheart disease cannot be explained solely by thestandard coronary risk factors, research hasattempted to determine physiologic mechani-sms linking Type A to disease. Most explanationsfor this link suggest that behaviours exhibited

Personality 109
by Type A individuals are accompanied bysympathetic neuroendocrine and cardiovascularresponses, which might promote the develop-ment of coronary atherosclerosis or precipitateits clinical symptoms of ischaemic heart disease.
The results of this study suggest that theremay be an underlying psychobiological or“constitutional” basis for Type A behaviour incardiac patients. The impatience, hostility andspeech patterns exhibited by Type A patients withmanifest disease may, in part, reflect underlyingsympathetic nervous system hyperactivity. Thisview is different from, but not necessarilycontradictory with, the idea that Type A appraisalsor behaviours produce elevated sympatheticresponses. If Type A is a consequence ofsympathetic hyperactivity, then Type A behaviourmight be suppressed by treatment techniquesthat decreased sympathetic responsiveness.Beta-blockers such as propranolol are commonlyused to treat cardiovascular disorders. Thesedrugs antagonise certain sympathetic nervoussystem responses that would otherwise beactivated by epinephrine. These responses occurprimarily in organs such as the heart, and insmooth muscle of the blood vessels and lungs.
Clinical Applications
Personality has been of great clinical importance,as you would recall that no two patients evenwith a similar disease are same. The reactionsto the illness have been found to be related topersonality. An extrovert and an introvert mayreact differently to the restrictions imposed byillness. Someone with poor self-concept and self-esteem may feel further threatened by an illnessas it produces feeling of failure to meet thedemands of coping with illness. On the otherhand, an individual habitual of using defensemechanism of projection may tend to blameothers for his illness and find faults with thehospital system. The way a patient construes
illness in general, and his own in particular, inrelation to other aspects of life, will determinehis response to it; an individual’s strength ofachievement motivation may be significant inrelation to any disability threatening his career;that a sensation seeker would find any degreeof sensory deprivation from illness particularlystressful; that those whose locus of control isinternal may be vulnerable to the dependenceon others often entailed by illness. Thus anunderstanding of patient’s personality can helpthe physicians in providing specific treatmentstrategies. For example, when you realise thatthe patient X is taking secondary gains from herillness and thus is not showing any improvement,then providing attention to the healthybehaviour and ignoring illness behaviour wouldhelp the patient to recover soon.
From a more psychiatric standpoint, someknowledge of a person’s ‘normal’ or ‘previous’personality can be important in order to detectchanges, which may have occurred as a conse-quence of disease either organic or psycholo-gical and also to assess the degree of recoveryfrom such illness. An individual’s personality willalso ‘colour’ the clinical picture of any psychiatricdisorder that he develops, so that it will neverbe identical with that of another patient.According to Eysenck the personality typedetermined the nature of illness for example,introverts are more prone to depression, anxiety,schizophrenia. The extroverts are more proneto disorders like somatoform and hypomania.Similarly personality has influence on thepsychophysiological disorders. Studies have triedto correlate personality patterns of individualswith disorders such as irritable bowel symptoms,ulcerative colitis, headaches, etc.
There are some people whose personalitiesdepart, in various ways, from the norm to suchan extent that they experience difficultiesthemselves, resulting in anxiety or depression,or cause difficulties to others in their attempts

110 Behavioural Sciences in Medical Practice
to cope with the normal pressures andresponsibilities of life; they may therefore bediagnosed as having a personality disorder.
Personality disorders themselves are classi-fied into a number of types in a way that isgenerally quite different from that of thepersonality theories we have been considering.The definitions of the various personality dis-orders are essentially derived from clinicalexperience often being seen as personality‘equivalents’ of particular psychiatric disorders(e.g. the ‘schizoid’ personality and schizophre-nia, the ‘hysterical’ personality and hysteria).
Personality has been correlated with thestudying skills. As a student you would beinterested in knowing that certain personalitycharacteristic predict greater academic success.Introverted boys and extroverted girls generallyperform better in the academic performances.Since personality also influences which isinteractional abilities hence in a workingenvironment like hospitals where teamwork ofmultiple disciplines is required, understandingof personality is of greater relevance.
SUMMARY
Personality is a stable characteristic way a personfeels and behaves in a whole variety of situations.Different psychologists view personality differentlybut many agree to the view that it is aninteraction between the behaviour and a givensituation. Character and temperament thoughdifferent are terms used synonymous withpersonality.
Every child is born with certain potentialities.The determinants, which shape personality, areviewed from different perspectives. A distinctionis drawn between biological influences, i.e.genetically determined and environmentalinfluences determined by family, school, peergroup and culture.
Personality has been studied in a number ofways by different theorists. These are psycho-dynamic theoretic by Freud, Jung, Adler andErikson. According to Freud the interactionbetween the id, ego and superego results inpersonality development. Various defensemechanisms help to reduce stress and anxiety.The type and trait theories classify individualsaccording to types like introvert, extrovert andtraits are personal dispositions. The traits can becardinal, central and secondary. The big fivefactor theory includes five basic traits whichbroadly cover different traits given by all othertheorists. The social learning theories emphasiserole of learning and environmental situation inpersonality development. According toHumanistic theorists, self-concept, self-esteemand self-actualisation are related to success.
Early, physician believed that intenseemotions could produce imbalances and bodilyfunction, culminating in various forms of physicalpathology. Specific disorders as coronary heartdisease (CHD), peptic ulcer and asthma havebeen linked to personality. Epidemiologicalevidence is suggestive of link between Type Aand CHD. Type A patients are more likely tohave severe coronary artery disease incomparison to type B patients.
The study of personality has been of greatclinical importance as one would recall that notwo patients even with similar disease are same.An extrovert and an introvert may reactdifferently to the instructions imposed by illness.People with poor self-concept, self-esteem andlow motivation feel threatened by illness.Knowledge of a person’s normal or previouspersonality can be important in order to detectchanges, which occur as consequences ofdisease—organic or psychological, and alsoto assess the degree of recovery from suchillness.

12Development—Infancyto Adolescence
PART 3: Development of Behaviour
Sanjay, a 15 years old adolescent, has frequenttemper outbursts, he does not get along with hisparents, he has occasional fights with his parentsand his younger sister. He frequently demandsmoney from his parents, which the parents cannotafford. His parents feel that his academicperformance is also going down, as he spendslot of time in looking at himself in the mirror,and is interested in talking to girls. Though heis a terror at home, but on the other hand, heis very popular amongst his friends. Sanjay isnot suffering from any psychiatric problem, butis passing through an adolescent period. Tounderstand normal deviations in behaviour, oneshould be aware of the normal developmentalprocess.
The human life cycle influences health andillness at all its stages. Human development startsat the time of birth and continues till death.Development passes through important stagesof life. These can be understood in terms ofInfancy, Childhood, Adolescence, Adulthoodand Old age. In this chapter, developmentalprocess from infancy to adolescence shall bediscussed, and in the next chapter, developmentprocess in adulthood and old age would bediscussed.
INFANCY AND CHILDHOOD
The human infant has a number of adaptivereflexes, including the grasping and suckingreflexes. Infants are social creatures from the daythey are born. Early social development, laysa foundation for later relationships with parents,siblings, friends and relatives. Self-awareness andsocial referencing (increased awareness of others)are two important elements of social develop-ment. Self-awareness is seen around 15 monthsof age. The core of social development lies inthe emotional bonds that babies form with theircaregivers. Infant attachment is reflected byseparation anxiety, which appears around 8-12months of age. Separation anxiety refers to thedistress displayed by infants, when separatedfrom their parents or caregivers.
Language proceeds from control of cryingto loosing, to babbling, followed by use of singlewords and then to telegraphic speech. Pre-language communication between parents andchild involves shared rhythms, nonverbal signals(in the form of touch, vocalising, gazing orsmiling). Turn taking is the tendency of parentand child to alternate in the sending andreceiving of signals and messages.

112 Behavioural Sciences in Medical Practice
Stages of Development
Development occurs along multiple lines, it isoverall physical development, cognitive, per-sonality, social and neurological development.The personal experiences, organisational styles,coping strategies, feelings and thoughts, allcontribute to create one’s unique experience oflife.
Development moves in a fixed, predictablemanner, with minor variations in all individuals.Some of the important milestones of develop-ment are given in Table 12.1.
Table 12.1: Milestones of development
Age Motor Social
0-3 Lateral head movement Fixes eyes and holds gazemonths Arms and legs thrust in Smiles at nodding head,
play high voiceEye coordination First social smileHead erect and steady Discriminate between
mother and others3-6 Rolls over Gives first laughmonths Head steady Expresses wariness
Elevates on armsEquilateral movements Responds to mother
differentlyTurns from back to sideSits with support
6-12 Pulls to sit Babblesmonths Bangs in play Laughs at incongruity
Sits alone steadily Fear of strangersPulls to stand Interacts sociallyStands alone Follow simple instructionsStarts walking
Cognitive Development
Jean Piaget (1896 to 1980) focussed on howchildren and adolescents think and acquireknowledge. His theory is referred to as geneticepistemology, which means to study of acquisi-tion, modification and growth of abstract ideasand abilities on the basis of an inheritive orbiological substrate.
The concept of schemata lies at the core ofhis theory. He defined it as a specific cognitivestructure that has a behavioural pattern. As an
individual grows, the schema becomes more andmore complex. Later schemas are referred to asoperations, which include imitation, abstractionand higher intelligence. Piaget spoke of twoprocesses: (a) assimilation, and (b) accommoda-tion. The former refers to taking in of newexperience, through one’s own system of know-ledge. The latter implies modification of existingschemas to the demands of the environment.These two processes give rise to the—conceptof adaptation, which is the individual’s ability toadjust to the environment and interact with it.
Piaget gave four stages of cognitive deve-lopment.
Sensory Motor StageIt occurs in the first two years of life. It ischaracterised by learning that occurs throughsensory observation. The child is concerned withlearning to coordinate purposeful movementswith the information from his senses. Objectpermanence is an important achievement thatoccurs during this period. It implies that objecthave an existence independent of child’sinvolvement with them. The child is able tomaintain a mental image of an object eventhough it is not visible.
Preoperational Stage
It occurs during the second and the seventh year.The child uses language and symbols extensively.Thinking and reasoning are at an intuitive level.The child lacks a sense of cause and effect. Thecharacteristic feature of the stage is egocentricthinking that is, having a limited point of viewand inability to take the role of other person.Animistic thinking, the tendency to endowphysical events and objects with life like psycho-logical attributes is also seen during this stage.
Concrete Operational Stage
It is the stage that occurs between the seventhand eleventh year. In this stage, the child ope-rates and acts on concrete, real and perceivable

Development—Infancy to Adolescence 113
world of objects and events. Operational thinkingreplaces egocentric thinking, which means thatthe child is able to attend and deal with a widearray of information and is able to take othersperspective. In this stage, the child is able to forma logical conclusion from two premises and thisis known as syllogistic reasoning. The child is ableto reason and follow rules and regulationsdevelop moral sense and a code of values.Children who become overly invested in viewsmay show obsessive-compulsive behaviour, andchildren who resist a code of value often seemwillful and inactive.
Conservation and reversibility are the othertwo characteristics of this stage. Conservation isthe ability to recognise that the shape and formof objects may change but the mass remains thesame. Reversibility is the capacity to understandthe relations between things, to understand thatone thing can turn into another and back again.For example, ice and water.
Stage of Formal Operations
This stage occurs from 11 years onwards throughthe end of adolescence. The adolescent is ableto think abstractly, reason deductively, defineconcepts and deal with permutation andcombination. Hypotheticodeductive thinking,which is the highest organisation of cognition,occurs during this time. The individual is ableto make a hypothesis and test it against reality.
Psychosexual Development Freud wasprobably the first psychologist, to emphasise thedevelopmental aspects of personality and inparticular to stress the decisive role of the earlyyears of infancy and childhood in laying downthe basic character structure of the person. Freudfelt that personality was well-formed by the endof the fifth year, and that the subsequent growthconsisted for the most part of elaborating thisbasic structure.
Freud’s notions about personality develop-ment came from many sources. But mostly histheory sprang from his observations of his own
patients. Freud was fascinated by the fact thatmost of his patients seemed to have gonethrough very similar developmental crises aschildren. Freud believed that “the child is thefather of the man”. Eventually, he decided thatone passes through various psychosexual stagesof development, which correspond to thematurational stage of ones body at various timesin the life. Each stage is associated with a uniquecrisis of some kind.
Oral Stage
Oral stage is the period which lasts from birthto about one year of age. The first crisis is thatof birth, when one is thrust out into the worldand becomes dependent on others to meet theneeds. You had innate reflexes that help to surviveby creating libidinal energy that had to be dis-charged; but the manner in which you releasethis energy changes as body matures. When youwere newborn, the brain centres, which controlmouth movements were physically, the mostdeveloped so libidinal energy released easilythrough such oral activities as sucking andswallowing.
Freud saw many child—like oral behaviourpatterns in his patients, such as talking too much,over-eating, excessive smoking and so forth. Hepresumed that this “residue of their infantileexperiences” remained locked away in theirunconscious minds because of some traumaticexperience they had while in the oral stage. Thesepatients had problems because they were stilltrying to release libidinal energy through adultoral activities. Therapy for these patients wouldobviously involve some form of “catharsis” toallow the patients to discharge the libidinal energythat had been repressed while they were still inthe oral stage.
Anal Stage
The second crisis occurs when parents beginmaking demands, which conflicted with instinc-tual need to obtain immediate gratification of all

114 Behavioural Sciences in Medical Practice
biological and psychological needs. The secondcrisis reaches a peak during toilet training, whenparents insist that you learn to delay gratification.Freud assumed you resolved this crisis by creatingan “ego” or conscious self that could respondto reality by gaining voluntary control over therelease of libidinal energy through anal activities.
Some of Freud’s patients were excessivelyneat, obstinate, and miserly. These three traitsmake up what Freud called the “anal character”,and he saw all the three as attempts to punishthe mother for the trauma of toilet training. Themother demanded that the child ”be clean”, sothe patient became unreasonably tidy. Themother demanded the child to “produce”, sothe child rebelled by withholding its feces, andbecame fixated at the anal stage. As an adult,the patient still rebels by obstinately refusing topart with single paise. Again, catharsis and givingthe patient insight into the roots of the problem-seemed to Freud to be the best therapy.
Phallic Stage
At stage three or so, sex organs began to mature,and did the centres in the brain associated withsexual activity. Thus, one acquires a new avenuefor discharging instinctual energies. During thisphallic period, boys build up a warm and lovingrelationship with their mothers, which Freudcalled the Oedipus complex. At the same age,girls experience an intense “emotional attach-ment” for their fathers, called the Electracomplex. Freud stated that, during the phallicstage, boys experience incestual desires topossess their mothers and compete with (or evenkill) their fathers, while girls like their fathers andfear or hate their mothers.
Latency Period
According to Freud, one enters the latencyperiod at about age five or six. At this time, onestarts to move out of the home more frequently,
and friendships with peers taken on greaterimportance on one’s emotional and intellectualdevelopment. Freud believed this was naturalhomosexual period during which boys found‘heroes’ among older male friends and peers, andgirls developed ‘crushes’ on other girls and olderwomen.
Psychosocial Development (Erikson)
Erikson proposed a psychosocial theory ofdevelopment. This means that the stages of aperson’s life from birth to death are formed bysocial influences, interacting with a physically andpsychologically nurturing organism. In Erikson’swords, there is a mutual fit of individual andenvironment that is, of the individual’s capacityto relate to an over expanding life space of peopleand institutions, on the one hand, the readinessof these people and institutions to make him partof an enjoying cultural concern (Erikson, 1975).
Eight Developmental Stages: According to thePsychosocial theory, development proceeds instages—eight in all; the first four stages occurduring infancy and childhood, the fifth stageduring adolescence and last three stages duringthe adult years including old age. Erikson hasplaced particular emphasis on the adolescentperiod because it is then that the transitionbetween childhood and adulthood is made.
These consecutive stages are not laid outaccording to a strict chronological timetable,because Erikson feels that a given child has itsown timetable, and therefore, it would be mis-leading to specify an exact duration for eachstage. Moreover, each stage is not passedthrough and then left behind. Instead, each stagecontributes to the formation of the total perso-nality. Each of these stages is characterised byits own type of crisis, or conflict. Erikson sawthese crises as being eight great tests of yourcharacter.

Development—Infancy to Adolescence 115
Trust Vs Mistrust
Erikson called the first developmental stage the“sensory stage”, which corresponds to Freud’soral stage. To Erikson, the crisis at the sensorystage is that of learning basic trust or mistrustof other people. At this point in life, the infantis totally dependent on others for its needs. Ifhis mother (or someone else) meets these needs,the infant learns to depend on others in later life.If for any reason, the mother is inconsistent insatisfying the infant’s needs, the infant may carrysuspicion and doubt through the rest of its years.
Autonomy vs Shame, Doubt
The second of Erikson’s stage, similar to the analstage, is that of muscular development. Duringtoilet training the child learns to control its ownmuscles and begins to assert its individuality. Thecrisis here is that of autonomy, or the ability tocontrol one’s own bodily functions. The childeither learns autonomy, or if it is unsuccessful,develops shame and doubt about its own abilities.
Initiative vs Guilt
The third stage, that of locomotors control, issimilar to Freud’s phallic stage. Now the childattempts to develop its own way of asserting itsneeds and gaining its rewards. Urged by itsinstincts to possess its opposite-sex parent (at leastin fantasy) and to rival its same-sex parent, thechild faces the crisis of inner desires versussociety’s demands. Erikson believed that if thechild could channel its sexual needs into sociallyacceptable behaviours, the child acquiredinitiative. If not, the child might build up a strongsense of guilt that would haunt it the rest of itsdays.
Industry vs Inferiority
Both Freud and Erikson called the fourthdevelopmental stage that of latency. During these(typically) school years, the crisis the child faces
is that of competence or failure. If the child doeswell in school, he learns that he can succeedand thus becomes industrious. If he does poorly,it gains a sense of inferiority.
Identity vs Indentity Confusion
At puberty, Freud thought sexual interest returnsand the individual must make the finaladjustment, that of heterosexuality. Erikson sawthe puberty crisis as that of either finding youridentity, or of developing what he called roleconfusion. You must decide what the future willhold and who you will become. Although thesocial roles available may vary from one societyto another, you must decide which of these rolesto adopt. By discovering who and what you wantto be, you are able to plan your life as aworking, functioning adult.
Intimacy vs IsolationErikson postulated three final stages of maturationbeyond the five that Freud spoke of. The firstof these stages, which occurs in young adulthood,presents you with the crisis of intimacy versusisolation. If you have “found” yourself by now,you can then go on to the delightful task of“finding” someone else to share life’s intimacieswith. If you fail to resolve your identity crisis,however, you will remain isolated from the closestforms of psychological “sharing” with others.
Generativity vs StagnationSocieties often pass through a period of rapiddevelopment, then settle into complacencywhen growth stops and stagnation sets in.Erikson believed that adults often experience thesame “growth” crisis during their middle years.Human beings need more than intimacy. Wemust be productive and helpful to our fellowhumans, and we must make a contribution tosociety. The crisis decision here then is, thatbetween what Erikson called generativity andstagnation.

116 Behavioural Sciences in Medical Practice
Integrity vs DespairErikson’s final stage is that of maturity. If youlive long enough, you have to face squarely thefact that you are mortal, and that some day youwill die. By resolving your prior crises, you gainthe strength to integrate even death into thepattern of your existence, You come to termswith yourself, content with the knowledge thatyou have done the best that you could underthe circumstances. Knowing that your life hasbeen successful, you can die as you lived, withintegrity. But, if you fail to solve the earlier crises,you may see your life as having been useless,incomplete, and wasted. And thus, you maysuccumb to feelings of despair at the futility ofexistence.
Summary of these eight stages is given inTable 12.2.
AdolescenceAdolescence is a period (ranging from 11-19years), during which a growing person makesa transition from childhood to adulthood. Thebiological, psychological, cognitive, emotionaland social changes taking place in the years
around puberty are greater than at any otherage since the second year of life. Adolescenceperiod has its importance in preparing a youngindividual to meet challenges of social andeconomic world. In the recent years, there havebeen tremendous changes in our Indian socialenvironment and economic conditions, whichhas influenced the psychological development ofan adolescent. Emotional and psychologicaldevelopment of an adolescent needs understan-ding and careful handling by adults as this periodis the most sensitive period in an individual’s life.
The late adolescent period is marked byselecting a career. Career development consistsof four broad phases:a. Exploration phase Possibilities are made an
initial search for career.b. Establishment phase The individual finds a
job, enters a career, develops competenceand gains status.
c. Mid career phase is a time of highproductivity and acceptance by co-workers.
d. Later career phase The individual serves asa respected expert and a guide/role modelfor young workers.
Table 12.2: Stages of psychosocial development
Stage and Age Psychosocial crisis Major concern
Infancy 0-l yr. Trust vs mistrust The infant develops a sense of trust/mistrust that basic needslike warmth, physical contact will/will not be fulfilled.
Early child- Autonomy vs shame, doubt Learn self-control as a means of being self-sufficient, e.g.toilethood 1-3 yrs. training, shame and doubt about the ability to be autonomous.Play age Initiative vs guilt Anxious to investigate adult activities, may have feelings of3-6 yrs. guilt about trying to be independent and daring.School age Industry vs inferiority Learns about imagination and curiosity, develops learning skills7-11 yrs. or feelings of inferiority if they fail to master task.Adolescence Identity vs identity confusion Try to figure out who they are, how they are unique, how they12-20 yrs. can establish, sexual ethnic and career identity. Confusion can
arise over these decisions.Young adult- Intimacy vs isolation Seek companionship and intimacy with significant others orhood 20-30 yrs avoid relationship and become isolated.Adulthood Generativity vs stagnation Need to be productive—create products/ideas/32-65 yrs children or become stagnated.Mature age Integrity vs despair Efforts to make sense of one’s life. Reflecting on completed goals65 + or despair about unreached goals and desires.

Development—Infancy to Adolescence 117
Emotions Experienced duringAdolescence
To understand the adolescent, it is important toknow what he does and thinks but it is even moreimportant to know what he feels. Duringadolescence, emotion is involved in everythingin which the adolescent is involved. Differentemotions are expressed by an adolescent whenhis desires are fulfilled, or when he is blockedor thwarted, in his efforts, or when he is harmedor threatened with harm.
Adolescent Love
To achieve the tasks of loving, an adolescentneeds to achieve emotional independence ofparents. The need to love and to be loved issupremely important in their lives. Examples oflove are also seen in devotion towards group bydelinquents and impulse for doing idealisticthings. With adolescence, one is faced with newdemands, new situations, in which the task oflove and sex must be faced. The capacity orability to love serves function to fulfill andbroaden the potential for enjoying one’s life. Aperson who is unable to love, for psychologicalor social reasons starts comparing himself withother peers and feels depressed.
Sexuality
Adolescents engage in range of sexual beha-viours. Experimentation with sex is becomingvery common with adolescents due to the effectof media. At times, these involvements lead tounwanted teenage pregnancies, abortions andguilt feelings. If these guilt feelings are nothandled appropriately, it can lead to negativerepercussions for future sexual relationship.Some adolescents engage in homosexual activi-ties, both as active and passive partners.
Anger
Adolescent’s temper flares often and easilybecause he is overly sensitive, he tends to feel
abused, and his self-esteem and confidence areshaky partly due to the occurrence of physicaland hormonal changes.
It is through his anger that an adolescent mostsharply asserts his demands and interests. Thebasic conditions that arouse anger remain muchthe same throughout life, but there are changeswith age in the particular circumstances thatprovoke it. When we try to understand angerin the adolescent, it is easier to identify what itis that makes him angry than to tell why it makeshim angry.
During adolescence, persons rather thanthings most often provoke anger. There aremany unavoidable frictions in the give and takeof everyday life. Many adolescents are annoyed,not only by specific parental practices but alsoby parental traits and habits. It is often observedthat anger is frequently aroused by unjustcriticism by parents, being treated like a childat home, clashes of opinion with parents, andtroubles with brothers and sisters.
Anxiety
Many adolescents may experience a vaguefeeling of uneasiness, a feeling of being on edge,other feelings such as fear, anger, restlessness,irritability, or depression. The underlying conflictsprings from a clash between incompatibleimpulses, desires, or values. Such a conflictprevails when a person is angry but is afraid ofgiving offense. Likewise, it exists when a personis eager to be popular but has strong scruplesagainst doing what is necessary to becomepopular.
Anxiety-producing Stresses inAdolescence
Everything that an adolescent for the first timerecognises about himself, every venture that heaccepts or declines, every decision he makes,may threaten earlier ideas, perceptions, andattitudes he has acquired regarding himself.

118 Behavioural Sciences in Medical Practice
The course of physical growth itself has manyemotional repercussions in adolescence, such asthe stresses connected with early or latematuring, adolescent obesity, concern aboutdevelopment of the genitals and secondary sexcharacteristics. In the sphere of sex, he has urgesand faces temptations, choices, and hasards,which are more critical than his earlier experi-ences with sex. In his interpersonal relations, hefaces problems of independence-dependence,conformity-nonconformity, and self-assertion-self-negation.
Anxiety and self-determination: Planning forcareer is the preoccupation of this period. Someadolescents work very hard to achieve theirgoals. But some, with high achievement driveface anxiety either in achieving their targets,which might have been set very high or due tohurdles and delay coming in the way of success.Currently, many adolescents have the urge toearn lots of money in no time; when they findthat it is not an easy task, they feel frustratedand depressed.
Anxiety-producing stresses in adolescence: Theneed for intimacy normally first appears in pre-adolescence. Intimacy means emotionalcloseness and it involves mutuality. It maybecome anxiety provoking for an adolescent,if due to a slower rate of development, he hasno need for intimacy when most of the otherpersons of his age have this need.
Relationship with parents and siblings: There isa general agreement that adolescence is achallenging and sometimes trying time for boththe young and the parents. The rapid rate ofsocial change, which we are currently under-going means that the adolescents and the parentshave grown up in markedly in different worlds.When the developmental experiences that shapeour personalities and social changes that mustbe confronted are very different, a generationalgap may be expected. The adolescents develop
different cultural values and outlooks. Differencesin their knowledge tend to magnify the conflictbetween parents and adolescents.
Parental support and guidance, in additionto meeting the basic needs of developing youngpeople for nurturance, are especially crucial inthe face of stressful nature of adolescenttransition. The parent-child relationship affectsthe relative ease with which the young personadjusts to the changed role a new demands ofadolescence.
Relationship with Peers
Peer group provides the adolescent with thearena for much of the learning and developingthat occurs in all the life tasks. Peers play crucialrole in the psychological and social developmentof most adolescents, especially in age segregated,technological societies like our own, whereentrance into adult world of work and familyresponsibility is increasingly delayed. The peergroup provides opportunities to learn how tointeract with others, to control social behaviour,to develop age relevant scales and interest andto share similar problems and feelings. Roleplayed by peers in adolescence is especiallycritical. Relationship between both same andopposite sex peers during the adolescent yearscome closer to serving as prototype for later adultrelationship—in social relations, in work and ininteraction with members of opposite sex. Theyoung man or woman who has not learned howto get along with other of the same sex and toestablish satisfactory heterosexual relationship,by the time he or she reaches adulthood is likelyto face serious obstacle in the years ahead.
Adolescents are also dependent on peerrelationships, simply because ties to parentsbecome progressively looser, as the adolescentgains greater independence. In addition, rela-tion with family members are likely to becomecharged with conflicting emotions in the earlyyears of adolescents-dependent yearnings, exist

Development—Infancy to Adolescence 119
along side independent striving, hostility is mixedwith love and conflict occur over cultural valuesand social behaviour. Consequently, many areasof adolescent’s inner life and outward behaviourbecome difficult to share with parents.
During this vulnerable stage of developmentrelationship with peers may also be harmful.Adolescents may be pressurised by a group oftheir peers into suspending their own betterjudgement and engaging in behaviour they maylater regret. These may range from relativelyminor improprieties to more serious, sometimestragic incidence.
Finally, the role of the peer group in helpingan individual to define his or her own identitybecomes particularly important, during adole-scence because at no other stage of develop-ment is one’s sense of identity so fluid.
Social isolation and alienation: The prevalenceof reported loneliness, shyness and social anxietyamong adolescents appears to be rather high.Research investigating correlates of adolescentloneliness and social isolation, has focussed onseveral factors that seem to contribute to theseinteraction difficulties. Occasional feeling ofloneliness, isolation, and awkwardness areprobably normal. Among more seriouslyadolescents, the investigations have identifieddeficits in certain social skills, social participationand cognitive behavioural characteristics andsocial outlook problems.
There are powerful forces in the culture thatlead adolescents to disguise or repress theiremotions. The most common example isrepression of sexual feelings in traditional andconservative families.
Ego and Identity
The adolescent “search for identity” leads toincreased conflict with parents. Increasedidentification with peer groups is commonly seenduring this period.
An essential problem of adolescence is thatof finding a workable answer to the question,“Who am I?” As you have seen, that Eriksonhas pointed out a strong sense of ego identityin the adolescent, so he sees himself or herselfas a separate, distinctive individual. Indeed, thevery word individual, as a synonym for person,implies a universal need to perceive oneself assomehow separate from others, no matter howmuch one may share motives, values, andinterests with others.
The individual needs to have a sense ofpsychosocial reciprocity—a consistency“between that which he conceives himself to beand that which he perceives others to see in himand expect of him”. Erikson’s assertion that one’ssense of identity is tied, at least partly, to socialreality is important, it emphasises the fact thatsocietal or individual rejection can seriouslyimpair an adolescent’s chances of establishinga strong, secure sense of personal identity. Anydevelopmental influences that contribute toconfident perceptions of oneself as separate anddistinct from others, consistent and integrated,having a continuity over time, and similar to theway one is perceived by others, contributes tooverall sense of ego identity. By the same token,influences that may impair any of these self-perceptions, fosters what Erikson calls “identityconfusion”.
Due to difficult transition from childhood toadulthood, and of sensitivity to social andhistorical changes, the adolescent during thestage of identity formation is likely to suffer moredeeply that ever before or even again from aconfusion of roles, or identity confusion. Thisstage can cause one to feel isolated, empty,anxious, and indecisive. Adolescents may feelthat society is pushing them to take decisions,thus they become even more resistant. They aredeeply concerned with how others view them,and are apt to display a lot of self-consciousnessand embarrassment.

120 Behavioural Sciences in Medical Practice
Adolescent might feel he is regressing ratherthan progressing. The term identity crisis refersto the necessity to resolve the transitory failureto form a stable identity, or a confusion of roles.Each successive stage in fact, “is a potential crisisbecause of radical change in perspective”(Erikson, 1968).
Negative identity is a sense of possessing aset of potentially bad or unworthy characteristics.The most common way of dealing with one’snegative identity is to project the badcharacteristics onto others. It can lead to a lotof social pathology, including prejudice andcrime, but it is also an important part of theadolescent’s readiness for ideological involve-ment.
Personality and Social Development
Change in self, or sense of self, is an importantissue in adolescence. The sudden changes in theirbodies bewilder young people and make themquestion who they have been and who they arebecoming. “Am I the same person I used to be?”they wonder. “What will be like from now on?”As teenagers continue to question and puzzleover their greatest preoccupation, their life’swork, they are in danger of becoming confused.This confusion can show itself by the individual’staking an excessively long time to settle on acareer.
Inconsistency and impulsiveness in behaviourinterferes temporarily in achieving uniquepersonality. In some manner, the distinctivecharacteristic that differentiates one individualfrom others in the psychological and behaviouralrealms must be consistent over time so that theindividual can psychologically and be “himself”to himself and others. During adolescence, withpeer group identity one sees changes in valuesystem, beliefs, attitudes and behaviour, whichare an integral part of personality. Stability infamily relationship and role modelling is equallyimportant in the formation of personality at thisstage.
Clinical Applications
Understanding of normal child developmenthelps in identification, management of mentalsubnormality and specific developmental delays.As a part of normal growth and development,children commonly undergo the psychologicalproblems. Problems like specific fears sleepdisturbances, regression, sibling rivalry andrebellion. However, if these normal problemsworsen or last for long periods, it may be a signalfor more serious disturbances. The seriousdisturbances are in the form of toilet training(enuresis and encopresis), feeding disturbances(overeating, anorexia nervosa and pica), speechdisturbances (delayed speech and stuttering),learning disabilities, attention-deficit hyperactivitydisorder and autism.
Adolescent period is a very sensitive periodhence maintaining positive mental health is veryimportant. Many adjustment problems of minornature and psychiatric problems of major/ severenature develop during this period. Psychiatricproblems and substance abuse have been dealtin detail in other chapters of this book.Adjustment problems mainly occur due to lotsof factors like unresolved conflicts, misunder-standing with parents, impulsiveness, angeroutburst, aggressive behaviour and increasedinterest in sexuality. There has been an increasein awareness of adolescent problems so someadolescents seek psychological help, but still alarge number of adolescents experience anxietyof growing within themselves.
Many adjustment problems occur due to lackof information on sex. As masturbation is acommon experience for adolescent boys, butthere are many misconception associated withthat, dating behaviour is increasing in presentgeneration adolescents, which is not acceptableto many of the parents, especially in case of girls.So conflict and interpersonal problems arise. Forgirls, the problems begin with demand forautonomy. For girls conflicts are generally relatedto type of dresses, they want to wear, visit to

Development—Infancy to Adolescence 121
beauty parlors and attending late night parties.Environment has a key role in increasing mentalhealth problems. To some extent, media isresponsible for their increase. Violence,aggressiveness and sexual liberties shown on TV.Screens, movies and songs instigate adolescentsto behave in similar ways. The changing valuesof our society are different. Pressures andchallenges to the adolescents like show-off ofwealth, smoking, drinking, driving recklessly, latenight parties and free mixing of both sexes insome sections of societies becomes a reason ofconflict for others due to peer group pressures.
During the last few years, adolescentmedicine has started to deal with a number ofsocial problems experienced by youths such astobacco, alcohol and drug abuse. Inadequateresilience to stress and adversity, and sexuallytransmitted diseases. Indeed, alcohol is the mostwidely used psychoactive drug among adoles-cents (32) and initiation of the use of tobacco(at the age of >11) has increased rapidly,especially in girls. Almost half of adolescents haveused an illicit drug before they finish high school,and 25 percent have consumed an illegal drugother than marijuana (30). Moreover, approxi-mately half of fatal motor vehicle accidents andhomicides, as well as substantial proportion ofsuicides among adolescents, are associated withthe use of alcohol and other drugs (33). Thehigh incidence of adolescents affected withsexually transmitted diseases also has beenpointed out.
A fairly common medical subject such asadequate nutrition for proper growth andpubertal development has become an obsessiveproblem for many teenagers, whose greaterawareness of their physical appearance causesdissatisfaction with their body weight and phy-sical image. Excessive dieting and inappropriateweight loss in girls usually interfere with normalgrowth and menstrual cycles. Most of theseadolescents are not excessively overweight.Many, are most concerned over the localisation
of subcutaneous fat on their hips, thighs, waistand buttocks. Most young girls, with theseconcerns diet without medical supervision. Theybegin by skipping breakfast or lunch, and prolongfasting. They often take diuretics, laxatives andappetite suppressants and end up withunexpected secondary health problems.Inappropriate preoccupation over weight andpoor diets may be predisposing factors to moreserious eating disorders, such as anorexia nervosaand bulimia, with all the psychological,gynaecologic and metabolic sequelae associatedwith these conditions.
Medical doctors also have to deal with an-other fairly common eating disorder, i.e. someforms of obesity. Excessive overweight inpubertal boys and girls, not only causes importantpsychological problems, which affect social,educational and sport activities, but also is apredisposing factor for hypertension and eleva-ted cholesterol with a greater risk of cardio-vascular diseases later in adulthood. Excessivefood intake, sedentary lifestyles, excessivetelevision viewing habits, and poor physicalactivities are among the main causes of obesityin childhood and adolescence.
The relationship between overweight duringadolescence and subsequent educational achie-vement, marital status, household income, andself-esteem on 370 obese patients aged 16 to24 years, was studied by Gortmaker et al. Theseauthors concluded in a seven year follow-up thatthis condition had important negative social andeconomic consequences, which were moreadverse than those of many individuals withother chronic diseases. Practically all adolescentsare over sensitive about body image, and fatteenagers are especially vulnerable to socialdiscrimination. Medical doctors must see and talkto these adolescents without the presence of theirparents, carrying out a private dialogue, evenat ages of 10 or lower. Youngsters on their ownusually become more friendly, open, receptiveand cooperative than in the presence of their

122 Behavioural Sciences in Medical Practice
parents. Adequate counselling and properlybalanced dieting, not fancy commercial diets,should be prescribed with a periodic weightcheck. No drugs for weight reduction should beadministered. These patients should becounselled that while they are modifying theirbody to reach their final physical shape late inpuberty, they are developing their personality;their self-assurance, and their self-control. Theirefforts therefore, are not only directed tomodifying their physical aspects but also tobuilding up their personality.
Adolescent growth proceeds at an astonish-ing pace, the most rapid of any postnatal time(average weight increment during the adoles-cent growth spurt is 16 g/day for females and19 g/day for males). It is also during adolescenceand young adulthood that the skeletal mineralaccretion is completed, the peak bone massbeing critical for skeletal maintenance andprevention of osteoporosis. Lesions of arterio-sclerosis also begin to accelerate at this age andpeak incidence of anorexia and bulimia nervosais in adolescence. Moreover, overweight andobese conditions occurring at this age showpersistent health effects decades later. Further-more, food habits which develop as the adoles-cent enjoys increasing independence andresponsibility for his or her own dietary intakeare believed to persist into adulthood, makingthis a critical time for preventive health inter-ventions.
SUMMARYThe human infant has a number of adaptivereflexes, including the grasping and suckingreflexes. Early social development lays afoundation for later relationships with otherpeople. Development occurs along multiplelines, it is overall physical development, cogni-tive, personality, social and neurological deve-lopment. The motor development is mainly inthe first few years of life. Cognitive developmentaccording to Piaget, occurs in four stages, sensory
motor stage, preoperational stage, concreteoperational stage, and stage of formal operations.
According to Freud, the personality deve-lopment passes through various stages ofpsychosexual development. These stages areoral stage, anal stage, phallic stage and latencyperiod. Erikson has proposed a psychosocialtheory of personality development, whichconsists of eight stages. The first four stages occurduring infancy and childhood, the fifth duringadolescence and the last three stages during theadult years including old age.
Adolescents are a transition period in one’slife from childhood to adulthood. Psychologicaland emotional development reaches its peakduring this period. The changes occurring in anindividual are varied and rapid which if nothandled carefully can disturb the mental healthof an individual.
Constitutional delay of the onset of pubertyis a fairly common reason for adolescents (14and 16 years of age) and for their parents toseek a clinical consultation. While the age ofpuberty onset varies, the delayed initiation ofpubertal changes and of the growth spurtfrequently worries a large number of adolescents,especially boys, because of the social dimensionof perceived delays. Some who perceive thattheir development is abnormal, start havingproblems in school, stop participating in sports,are no longer willing to participate in social events,etc.
Most girls with delayed puberty accept theexplanation offered, especially when one cangive approximate dates when these processeswill start taking place. Conversely, boys are moredifficult to manage, because most of them arequite upset over their sexual infantilism and shortstature. Boys usually seek clinical help becausetheir growth velocity has not increasedsignificantly, at a time when their peers aregrowing faster than they. Boys often show aconsiderable difference in height from one yearto the next. Frequently, they do not mention

Development—Infancy to Adolescence 123
their main concern, i.e. that they are shorter thantheir school friends and are often ridiculed bypeers. Such patients should be assured that thepresent situation is transient. They should beprovided with an approximate date for the onsetof their growth spurt based on testicularvolument and their bone age and an estimateof final adult height. Some boys with delayedpuberty are also quite concerned over theirsexual infantilism. This concern often leads themto abandon sports activities because they do notwant to undress with their more sexually maturepeers. Some respond by making efforts to obtainbetter physical development. They perform
strenuous exercises at the gymnasium, two tothree hours daily, using heavy weights tostimulate muscle development. Physicians shouldadvise them that such efforts will have verylimited results due to a transient lack of sufficienttestosterone to stimulate muscle mass growth.A useful metaphor is to compare their effortsto a man who wishes to move a car by pushingit, without the car having gasoline; he will beable to move the car, but slowly; igniting theengine would be better but this is impossiblewithout gasoline; in sense, testosterone is thegasoline needed by the muscle for it to developwhen stimulated by exercise.

13Adulthood to Ageing
A senior government executive, around 45 yearsold was referred for obsessive rumination. Thisproblem was very severe and it interfered withhis work, he felt insecure, so his wife, also anexecutive had to be with him always. Behaviouralassessment revealed that besides his ruminationabout girl, he also was afraid to see gray hair,had intense anxiety as well as apprehensionabout his growing old. He had negative thoughtsrelated to old age as nobody cares for, personbecomes lonely and the life in old age isworthless. This case is not unique, as many ofus can have problems of adjustment to agespecific roles, illness, failing abilities and so on.On the other hand, we meet many people fromvarious stages of life enjoying every bit ofexperience. This chapter shall help you tounderstand various developmental changes,which occur with the advancement of age sothat you can identify the deviations and thusprovide help.
According to the ancient Hindu literature, thedevelopment period was divided into four stagesnamely: Brahmacharya ashram, Grihasthashram, Vanprasth ashram, and Sanyas ashram.The first two stages correspond to early periodof childhood through adolescence andadulthood where the individual settles in job,gets married and has family responsibilities. TheVanprasth is equivalent to the middle age wherethe person after fulfilling some of the primaryresponsibilities of family, works for his self-actualisation joins religious organisations works
for social cause; and finally, the sanyas beingthe old age where the individual retires andoccupies himself with religious activities. Similarsystem of development has been adopted bythe modern thinkers. Many of the developmentaltasks described in ancient Hindu books aresimilar in nature with those described by modernthinkers.
Adulthood
The adulthood has been divided into three parts,namely, young adulthood (20 to 40-45 years);middle adulthood (40-45 to about 65 years);and old age (from 65 or 70 years onwards).This classification is only for the convenience ofstudying the developmental process in adult age,which is fairly a longer period than other stageslike childhood or adolescence.
Stages in Adult Development
It is only recently that due attention has beengiven to the developmental process from earlyadulthood to middle adulthood. Thus, somelongitudinal studies have been carried out tostudy this process. The findings of these studiesare as follows:
The Early Adult Transition (17 to 22years)
People feel halfway out of the family and sensea great need to get all the way out. They have

Adulthood to Ageing 125
a tenuous sense of their own autonomy and feelthat real adult life is just around the corner.
Entering the Adult World (22 to 28 years)
People now feel like adults. They are establishedin a chosen lifestyle; independent of theirparents, and pursuing immediate goals withoutquestioning themselves about whether they arefollowing the right course.
The Age 30 Transition (28 to 34 years)
People ask themselves, “What is this life all aboutnow that I am doing what I am supposed to?”and “Is what I am, the only way for me to be?”They often reassess both work and familypatterns. At this time, for example, careerwomen think about having a baby, andhomemakers begin to work outside the home.
Settling Down (33 to 43 years)
People make deeper commitments to work,family, and other important aspects of their lives,setting specific goals with set timetables. Towardsthe end of this period, is the state which Levinsoncalls “becoming one’s own man”, when menbreak away from the authorities in their livesand work at attaining senior status in their ownright.
Midlife Transition (40 to 45 years)
People question virtually every aspect of theirlives and values with an increasing awarenessthat time is limited. They may bridge thetransition to the second half of life. They cometo terms with the fact that the first part of adultlife is over, and they will not be able to do allthat they had planned before they grow old anddie. The transition may be smoothly managedor it may assume crisis proportions, dependingon their personalities and the specific situationsthey find themselves in.
While biology shapes much of what we doin childhood, culture and individual personalityplay a much larger role in adult life. The olderwe grow, the less our age tells about us. Forexample, two 45-year-old women may resem-ble each other physiologically, but the one whohad two children in her twenties, remained athome would have a different outlook on life fromthat of her age-mate with a well-establishedcareer.
Traditionally, most adults have had strongfeelings about the time in life, when certainactivities are considered acceptable. People arekeenly aware of their own timing and describethemselves as “early”, “late”, or “on time”,regarding the time they got married, settled ina career, had children, or retired. This sense oftiming seems to be shaped by environmentalexpectations, often affected by social class.
In recent years, however, as affluence hasfiltered down, as medical advances have keptpeople vigorous, and as the life span haslengthened, age-based expectations havebecome more flexible. We are more acceptingof 40-year-old first time parents and 40-year-old grandparents, 50-year-old retirees and 75-year-old workers. As Bernice Neugarten andGunhild Hagestad (1976) point out, we seemto be moving in the direction of what might becalled an age-irrelevant society; and it can beargued that age, like race or sex, is diminishingin importance as a regulator of behaviour.
In adulthood, generally people are well-settled in their careers barring a few. We aremuch more flexible in dealing with the basicdevelopmental tasks of adulthood. These areyears of good health and energy, especially inour twenties and thirties, with very slight, gradualchanges not becoming noticeable till about age50. We are at the peak of our muscular strengthand our manual dexterity at about 25 or 30.We see and hear most sharply in our earlytwenties, gradually there is a decline in these

126 Behavioural Sciences in Medical Practice
senses, as majority of the people becomefarsighted around forty years. Taste, smell, andsensitivity to pain, touch, and temperatureremain stable until at least 45 or 50.
Certain relatively consistent events markadulthood in our society. These range fromescaping parental dominance in the late teens,to a noticeable acceptance of one’s lot in lifeduring the 50’s. Research indicates that midlifeaffects many people in the 37-41 ranges, butthis is not universal. Midlife crisis is characterisedby feeling of instability and anxiety.
Biological ageing begins between 25 and 30years, but peak performance in specific pursuitsmay come at various parts throughout life. Mostof the health changes from young adulthoodto middle age are relatively minor. The organsystems are not as efficient as they had been,tending to lose some of their reserve capacity.Men’s sexual capacity declines, and high bloodpressure becomes a problem. Metabolismchanges, and both sexes tend to put on weight.
How do individuals cope with physicalchanges, and therefore, with the awareness oftheir ageing? Past health history, family attitudes,and individual personalities play a large part.Women tend to be more health conscious, bothfor themselves and their families. This may havesomething to do with the fact that pregnancyand childbirth have involved them more closelywith medical care, as well as with their traditionalrole as guardian of the family’s health. Whilemen often turn to diets and exercise, they tendto ignore symptoms (Lewis and Lewis, 1977).
Middle Adulthood
Physical Changes
The ratio of the physical and the psychologicalchanges in midlife vary, with the former affec-ting women universally and the latter becomingincreasingly recognised syndrome among men.
Menopause: It is a biological event in everywoman’s life, when she stops menstruating and
can no longer bear children. There are varia-tions in the age at which it may come. It canoccur any time between 38 and 60 years of age,with the average between 48 and 52 (Upjohn,1983). At one time, a number of psychologicalproblems, especially depression, were blamedon the menopause, but recent research showsno reason to attribute psychiatric illness to thephysical changes in a woman’s body. Suchproblems are more likely caused by environ-mental pressures against ageing, which reminda woman that menopause marks the end of heryouth. In those cultures that value the olderwoman, few problems are associated with themenopause (Ballinger, 1961). A society’s attitudetoward ageing seems to influence a menopausalwoman’s well-being far more than the level ofhormones in her body.
The male climacteric: Despite the fact that mencontinue to father children till quite late in life,there are some biological changes in middle-agedmen. These include decreased fertility andfrequency of orgasm, and an increase in impo-tency (Beard, 1975). Furthermore, men seemto have cyclic fluctuations in the production ofhormones. About five per cent of middle-agedmen are said to experience symptoms such asdepression, fatigue, sexual inadequacy, andvaguely defined physical complaints. Sinceresearchers have found no relationships betweenhormone levels and mood changes (Doering,Kraemer; Brodie and Hamburg), it is probablethat most men’s complaints are just as subjectto environmental pressures as women’s are.Some of the problems may be related todisturbing life events, such as illness of the manor his wife, business or job problems, his childrenleaving home, or the death of his parents.
Intelligence and Memory
For many years, it was believed that generalintellectual activity peaked at about age 20 andthen declined. We have strong evidence show-ing that certain types of intelligence continue to

Adulthood to Ageing 127
develop throughout life. We have discussed inChapter 6 about two types of intelligence, fluidand crystallised. Verbal abilities, a type ofcrystallised intelligence, appear to increasethroughout adulthood and old age. Performancein solving new problems such as spatial-relationstasks, an aspect of fluid intelligence, peaks in thelate teens and then begins a slow, steady decline.Furthermore, the accumulated wisdom thatcomes with adulthood may offset any declinein fluid abilities. Wisdom, the ability to exercisegood judgement about important but uncertainmatters of life, also affects our relationships withother people.
Personality
Few of us hold the same outlook on life at 40that we did at 20, showing the growth anddevelopment that takes place during adulthood.This growth comes about from many sources—the people we meet, the reading we do, theexperiences we undergo, the challenges we faceup to. Recent longitudinal studies of adults havedramatically illustrated the kinds of deve-lopmental tasks we deal with over the years.
Yet despite the changes that occur-in our livesand our thinking, we are still the same people.And we do tend to carry certain basic traits withus in all the twists and turns of life’s pathways.The two threads of stability and change areintertwined throughout all our lives, with someof us showing more change and others morecontinuity.
One personality change, common in midlifeis the tendency to express aspects of our persona-lities that we had repressed during our youngeryears. Sometimes, the repressed personality traitsget a chance to manifest in middle age. Withthe recognition at this stage of life that some ofour basic goals have already been achieved—the children reared, the career established, theidentity in large measure achieved—both menand women feel freer to change from the
stereotypical male or female role they hadmodelled themselves in younger age. They allowthemselves to express long-buried aspects of theirpersonalities, as many women become moreassertive, competitive, and independent andmany men allow themselves to be passive anddependent. You may find many men enjoyingcooking in this age, which was never evendreamt in their young age. The significant aspectof such change is not of “contrasexual” naturebut the fact that any trait that has been repressedfor the first half of life may now flower, with theincreased self-confidence and relaxation thatoften accompany middle age.
One other common personality change,which may help uncover such buriedcharacteristics, is a tendency for people tobecome more introspective as they grow older.While younger people invest more of theirenergies in action rather than in thought, peopleat midlife and beyond tend to think aboutthemselves more, analysing what they have donein their lives and why they have done it(Cytrynbaum).
Parenthood and Development
Parenthood can be a creative self-growth expe-rience as parents go through its several stages:anticipating ahead of time what parenthood willbe like, adjusting to new demands and learninghow to meet them at every stage of theirchildren’s growth, and then disengaging fromthe active parental role as children mature. Aschildren grow, parents get a second chance torelive their own childhood experiences and towork out issues they had not resolved with theirown parents. In addition, their children, whobring their own unique personalities anddemands to this intimate, intensely emotionalrelationship, influence them. This is the periodwhen children settle in own professions, getmarried and leave home. The parents especiallymothers may feel lonely in the house. This

128 Behavioural Sciences in Medical Practice
phenomenon has been called “empty nestsyndrome”. Persons with poor coping ability orwith too much of dependency on children finddifficult to adjust with the new circumstances.
Old Age or the Senescence
The interface between the body systems and theenvironment as it exists in senescence requiresone to look at the older person in a special light.Most significantly, later life is marked by a numberof progressive losses. For example, health,vocation, financial security, status, beauty,friendship, and even-eventually-life itself are allat risk for older people.
Abnormal development occurs when theelderly individual is unable to cope successfullywith the large number of losses that he or sheis apt to experience in the course of a life time.The symptoms that the elderly individualexhibits in the face of these stresses are likelyto represent exacerbations of long-standing orwell-established patterns of behaviour. Sene-scence leads to diverse physical and psychosocialchanges that may affect the functioning of theolder adult.
Developmental Tasks of Old Age
Gerontologists have proposed two theories ofageing. The disengagement theory holds thatwithdrawal from society is necessary and desir-able in old age. The activity theory counters thatoptimal adjustment to ageing is tied to conti-nuing activity and involvement. According to areport, well being in old age is characterised byself-acceptance, positive relations with others,autonomy, environmental mastery, a purposein life and continued personal growth.
Those who do achieve a sense of wholenessand integrity may develop one of the hallmarksof successful ageing, wisdom. Our culture tradi-tionally relies on selected elderly people foradvice about complex life problems. One reasonmay be that older people who have been attentive
to their life experience, often have a perspectiveon reality that is richer and more informed thanthe view most younger people take.
Health Changes
Physical functioning and health decline in oldage. Although ageing does not affect the entireorganism uniformly, we observe negative chan-ges in nine body systems; they are musculo-skeletal, cardiovascular, respiratory, nervous andspecial senses, gastrointestinal, urinary,integumentary, reproductive, and endocrine.Whether we look at the thinning of muscularfibres, loss of muscle tone in the bladder, ordecreased basal metabolic rate, we discover adecline in the older person’s vital functions. Itis of special importance to the behaviouralscientist, to recognise that all five senses sufferloss in even normal ageing, thereby skewingperception. For the most part, these conditionsare more like chronic, debilitating illnesses, asopposed to acute episodes as seen earlier in life.The following pictures show physical changes thatoccur from adulthood to old age (Fig. 13.1).
Psychological Changes
Intelligence
Some intellectual abilities do not decline withage, while other abilities decline at different rates.In general, verbal abilities tend to be maintainedwhile psychomotor speed and problem solvingtend to decline. Studies using the Wechler AdultIntelligence Scale (WAIS), indicated the elderlydo best on information, vocabulary, andcomprehension subtests; less well on arithmeticand picture completion subtests; and worst ontests of object assembly, block design, and picturearrangement.
Learning and MemoryBecause learning and memory are closelyintertwined and both are crucial to intellectual

Adulthood to Ageing 129
functioning, it is important to find out how thetwo operate in old age. Many investigators haveworked at this task, and some general trendsare emerging from their work. First, though olderadults can certainly learn via classical andinstrumental conditioning.
Second, in verbal learning—learning lists ofwords, for example, adults over 60 generallydo not perform as well as do young adults, butexperts are now debating whether these perfor-mance differences reflect real differences inlearning ability. Some attribute the inferiorperformance of older adults to pacing problems.It is on timed tasks that older people performmost poorly.
Third, overcaution and pacing problems mayalso contribute to some of the memory—performance deficits older people demonstrate.These deficits are not found in all aspects of theirmemory but are largely confined to processingof information.
Older people show deficits in the encodingand retrieval processes. They are less effectivethan are younger adults in coming up with goodstrategies for organising and rehearsing thememories they are encoding, and they oftentake longer than do younger adults to draw
memories out of storage (Erber, 1982).Memories—be they words, pictures, or con-cepts—seem to be recognised about as effectivelyby older as by younger adults; it is recall,remembering from scratch or from partial cues,that tends to suffer with old age. As we haveseen in Chapter on Memory that the memoriesare rarely lost, it just takes longer to find themin the file or takes longer to retrieve. The abilitiesmay vary in the various components ofmemory—registration, storage and retrieval ofinformation. Bellak (1976) reports that elderlyindividuals may remember better wheninformation is personally meaningful, offered insmall amounts, and presented in a way that iseasy to code for storage.
Personality Changes
Adult development from early adulthood tomiddle adulthood and to later life has been alargely neglected area of study. Recently, someattention has been given to the study ofpersonality in later years, by adopting adevelopmental approach. Thus, as during theformative childhood and adolescent years, theadult is viewed as passing through various lifephases. During these phases, the individual’s
Fig. 13.1: Physical changes according to aging

130 Behavioural Sciences in Medical Practice
perspective on life and death, personal accomp-lishments, and interpersonal relationships areever evolving. The many changes faced by theelderly quite often call for a team approach todeal with their problems. Mental health prob-lems may be one of many issues confrontingthe older person.
Stressful Life Events
There is an increasing evidence that life eventsassociated with older persons are higher due todeath of the spouse, change in living conditions,at times rejection from children, lack of friends,restriction in financial condition and mobility. Thephysical disabilities like loss of hearing, poorvisions, difficulty in walking, etc. may causeadditional stress on the older person. Thesestressful events should be taken into con-sideration while understanding the problems ofthe aged, because the presence of stress candelay the recovery process of physical diseases(Chapter 10).
Indeed mental health conditions may beinextricably tied to other physical or social pro-blems in the older person’s life. An understandingof the role of body systems as well as needs forcare and support are necessary, in order to beable to provide effective treatment to an olderpatient. Even the manner in which you com-municate with the older patient is important indeveloping trust and good doctor-patientrelationship. At times, it is good to integratemental health treatment into the ovrall care planfor the older patient.
Social Changes
Social losses among the elderly are a majorconcern. Widowed elders lose the psychosocialrole of being a spouse and are much more likelyto experience isolation and loneliness. Peoplewho experience isolation and loneliness aredocumented as being at high risk for mentalillness.
The economical problems in old age oftenresult in the biopsychosocial crises experiencedby the elderly. The elderly persons from loweror middle economic class may live on relativelyfixed incomes. During illness, if expensivemedication is prescribed, many of these elderlypersons are not even able to buy them. Lackof mobility, limited public transportation, poorintergenerational relationships, loss of status dueto retirement, society’s prejudice can result insynergistic blend of conditions that lead to a highrate of psychopathology and need for servicesamong the old.
Gerontologists have proposed two theoriesof ageing. The disengagement theory holds thatwithdrawal from society is necessary anddesirable in old age. The activity theory countersthat optimal adjustment to ageing is tied to conti-nuing activity and involvement. According to Ryft(1989), well being in old age is characterisedby self-acceptance, positive relations with others,autonomy, environmental mastery, a purposein life and continued personal growth.
Clinical Applications
Ageing brings difficulties of adjustment and thesemay be of sufficient severity to lead topathological states of anxiety or depression,which required treatment. Middle adulthood isa period of productivity, being on the highestscales of the career and thus more prone to stress.As we have seen earlier in the Chapter of Stress,that it can give rise to number of physicalproblems. Coping with these physical problemsand fulfilling the aspirations and ambitions mayget into conflict. Understanding the varyingreactions to such situations can be used in themanagement of physical problems.
With the advancement in medicine, the lifeexpectancy has increased. Thus, in any countrythe population of the elderly people is growing.With advancement of age, not only the physicalproblems increased but the psychological

Adulthood to Ageing 131
problems are also greater. Since memoryproblems are a frequent complaint of elderlypeople who are depressed, discriminatingbetween memory problems that are organicversus functional in nature is of primeimportance. Amongst the psychologicalproblems, depression is the most commonproblem encountered in the aged population.The depressive feeling may be associated withloneliness, physical illness or simply due to thedecline of abilities due to normal ageing.Understanding the family circumstances, socialsupport system and coping resources of thesepeople can enhance the efficacy of the treatment.
SUMMARY
The period of adulthood has primarily beendivided into three periods, namely, early, middleand late adulthood. Depending upon the perso-nality, attitude and lifestyle the differentiationbetween these three stages is not very clear-cut.Generally, there are not many physical or
psychological changes in the early adulthood.The physical changes start showing up after theage of 50 years (middle age).
The middle age is the period, which can showsome personality changes like the womenbecoming more assertive and the men takingthe reverse role. The physical changes due tomenopause can be associated with somepsychological problems in some women. Thesebeing, who have negative attitude towardsageing or have not achieved what they wantedare more prone to depression at this age. Theold age is generally considered around 65 yearsand above. In old age there are problems inlearning new materials and deficits in memoryprimarily due to the difficulty in retrieval. Therecan be some personality changes as old agedemands adjustment with retirement, limitedresources and decline in functioning of the vitalorgans. Death of the spouse and children stayingaway can result in loneliness. Older people areat risk to develop mental health problems,especially depression.

14Dealing with Deathand Bereavement
A 3 years old child admitted in paediatric ICU,is in very critical condition. The patient is restless,crying with pain and has very little chance ofsurvival. His parents are constantly enquiringabout his condition. As a doctor attending uponthe child, what should you do? Tell the parentsabout his critical condition or just do not talkto them. Often patients and family membershave been ignored and not informed about thecondition. Now more and more patients andfamily members wish to know all about thedisease process, prognosis and treatment plans.In such cases, where the illness is fatal, thedoctors’ role in comforting the patient and familyis very vital.
The care of the dying patient and the com-fort of the bereaved are major responsibility ofthe doctor. It is as important as providingtreatment. These areas have only in recent yearsbeen studied systematically. Death evokes fearand embarrassment among most people, as theyhave not experienced death till late in their lives.The medical professions also do not encounterdeath as frequent as it was in the past. With theimprovement of life expectancy in this century,death has become less well known andtherefore, perhaps, more frightening. Yet deathis inevitable in many conditions and doctors haveto be prepared to deal with such situations. Theyshould be able to offer help in easing the processof dying. For doctors, it may also now evokemore of a sense of professional failure since the
expectation is increasingly one of the cure fromlife-threatening diseases—a fact which coloursthe doctor’s attitude to the death. It is ofconsiderable value to understand and therebyhelp, both the dying and the bereaved.
The reactions of family members to deathvary according to the nature of death. Theending of life may take a variety of forms—sometimes sudden and unexpected as with afatal accident or heart attack, sometimes slowand expected following a period of ‘terminal’illness. Many healthy elderly people diepeacefully in their sleep without warning; deathbeing simply due to ‘old age’. Determinants ofthe psychological response to dying areassociated with its cause (e.g. due to ageing ordisease, and if so its nature), with the individualand with his environment. Fears of death areat times focussed less on the thought of deathitself, and more on the process of dying.Sometimes, death is disturbing as it may resultin extreme physical distress.
Many factors influence an individual’s res-ponse to death. One of the common significantresponse is the presence of religious faith, sincethis often holds out the promise of eternal life.It has been observed in hospitalised patients, thatthose who had a firm religious faith have leastanxiety. Consoling power of religion is seen inall types of patients, with different religiousbackground. Sudden death due to accidents orcardiac arrest, are more difficult to accept thandeath due to chronic illness.

Dealing with Death and Bereavement 133
Another factor that influences responses todeath is, age in the younger patient as the anxietyis further aroused by parenthood with appre-hension concerning dependent children.Depression is also frequently seen among thedying. While this may by partly related tophysical discomfort in some illnesses, it may alsostem from feelings of isolation resulting from atendency to avoidance or emotional withdrawalon the part of others when a person is knownto be dying. At the same time, this disengage-ment may sometimes be a two-way process, withthe dying person himself withdrawing, perhapsin anticipation of the final parting. Depressionmay additionally be explicable as part of a kindof anticipatory grief or mourning by theindividual for the losses that he is experiencingor expecting by loss of life.
The patient (if conscious) and family mem-bers face a very difficult time as the deathapproaches. Many problems arise at this timedue to lack of communication and doctors’ abilityto handle such situations. Often the doctors takedeath of the patient as a matter of fact and thepatient may just be a bed no. 2 for them. Thisattitude and manner of communicating causeslots of harsh feeling in the family members. Itis thus important for the doctors to understanddifferent types of reactions and responses todeath and thereby deal accordingly.
Methods to Deal with Dying PatientsRobert, a 43-year-old businessman, and his wifehad two sons. Doctors had given him six monthsto live, but offered and even encouraged himto undergo chemotherapy which would give hima ten per cent chance of recovery. Thechemotherapy had wrecked his body and madehim physically much weaker. In spite of this, hisfamily and his doctor desired him to continue.When he was asked as to what he wanted todo, that was the first time that he said that hewanted the treatment stopped and that he only
wanted to spend the rest of the day of his lifewith his family and with as much peace aspossible.
This incident supports the fact that the qualityof time spent in the last days of life is mostimportant for all concerned. The family membersshould be encouraged to support patient’sattempts to remain as independent as possible.He can be involved in making decisionsconcerned with the family. In our culture thereis a tendency to hide facts from the patient.When we do not talk about death with thepatient, it does not mean that the patient is notaware of it. Rather, they conceal their anxietiesand other thoughts to themselves, which mightbe more painful. If the patient is in a consciousstate, talking about death, at least warning ofimpending death can help the patient to beprepared for it. Surely it is better to face deaththan to die suddenly. We need to be there willingto listen to the thoughts, feelings, fears anddoubts about dying. Do not brush aside thetopic, so as not to cause any unnecessary upsetsor avoid the subject because you cannot copeup with the patients, and family’s reaction. Insome situations, the patient may not want totalk about the pending death. In those situationswe should not push this subject. Chapter 23 givesdetails of communicating with dying patients.
There are two areas of decision making thatconcern the dying patient. One has to do withthe treatment and the other has to do withpractical needs and plans for the immediatefuture such as organising finances, making willfor legal matters, seeking spiritual readiness andrekindling relationships. Lack of information isone of the primary causes of anxiety among theterminally ill. We should therefore take all thingsinto consideration before deciding to withholdany information about the patient. It would betragic if one were to die without fulfilling orexpressing one’s wishes regarding areas of one’swishes.

134 Behavioural Sciences in Medical Practice
If the family members are well-informedabout the pending death, they can either fulfilltheir certain religious rituals or mend theirrelationship with the dying person, if it wasdisturbed.
By not warning the family members, we oftengenerate guilt feelings in them. I haveencountered a situation, where the wife wheninformed about her husband’s death said thatif she was informed earlier, at least she couldhave offered some prayers to improve herhusband’s next life (a Hindu belief).
There are many practical and thoughtfulthings that we can do to help the patients intheir final days. Life is precious, even when deathis near. We should do all that can make themcomfortable.
Bereavement
The effect of death on those who are still alivehas also received systematic investigation inrecent years. A fairly consistent pattern ofmourning has been identified (Parkes, 1965).Typical or uncomplicated grief is usually seenfollowing the death of a parent, child, sibling orfirst-degree relative with whom there has beenat least a moderate amount of social contactwithin the preceding year.
Stages of Bereavement
Bereavement involves several stages. The firstresponse to an unexpected death is one of shockand disbelief—a period of denial, which maylast from a few hours to a fortnight. A 42 yearsold woman lost her husband while he wasundergoing angioplasty. When the news wasconveyed to her by the relative, she becameabsolutely shocked, did not cry, and kept sayingthat ‘Deepak is feeling better, he has sent mehome to look after children. Tomorrow he willbe discharged from the hospital.’ She was notable to give any reasons why the other relatives
were crying. She came out of this state after halfan hour. During this period, bereaved personfeels numbed but is able to carry on with theusual routine, as well as coping witharrangements for the funeral.
Gradually however, this protective denialbegins to give way to a full realisation of the lossand is associated with feelings of despair. Attacksof yearning may be accompanied by greatdistress, with reminders of the deceased (suchsymptoms may include feelings of tightness, etc.).Between these waves of distress, there is ageneral state of depression, apathy and senseof futility. Sleep is disturbed and appetite poor.There is a preoccupation with thoughts of thedeceased and often a characteristic restlessnesswhich may appear aimless but probablyrepresents a searching for the dead—sometimesacknowledged by the bereaved person, whoconsciously looks in places previously frequen-ted by the dead person. Irritability and angerare as responsible for the death. Often in thehospital, sometimes the medical staff is blamed,and at times the relatives become very aggres-sive and abusive towards the doctors. On theother hand, there may be feelings of guilt andself-blame for past behaviour towards thedeceased, whose memory tends to be idealised.In the earlier part of this stage, however, thereis a tendency to think of the dead person as stillalive to feel his presence or to actually see orhear him but gradually this is replaced by fullrealisation of the loss. Another frequent charac-teristic is the appearance of traits of the deceasedin the behaviour of the bereaved including oftenthe symptoms of the last illness. Finally, theintensity of this stage begins to decline after afew weeks and is generally minimal by aboutsix months, with full acceptance of the death.For several years thereafter, however, there maybe occasional brief periods of depression andyearning, usually precipitated by reminders ofthe loss and especially by anniversaries.

Dealing with Death and Bereavement 135
A great deal of mental activity is involved inthe process of grieving. Freud (1917) describedhis mental activity as grief work and Lindemann(1944) subdivided this into three components:(1) emancipation from bondage to the deceased(2) readjustment to the environment from whichthe deceased in missing, and (3) formation ofnew relationships. The first of these tasks is themost crucial and depends upon the bereavedperson remembering, often repeatedly, themany shared experiences that formed the basisof the relationship with the deceased. Thisprocess is initially extremely distressing butbecomes progressively less, so with passage oftime such recollections do not bring pain butpleasure. Table 14.1 summarises the stages ofbereavement.
Table 14.1: Stages of bereavement
• Shock and disbelief• Protective denial• Preoccupation with thoughts (Feeling of guilt and self-
blame)• Tendency to think of dead people alive• Appearance of traits (of the deceased person in the
bereaved)• Depression• Full acceptance
A person’s mourning does not of course takeplace in isolation, but within a socioculturalcontext, which includes the particular beliefs andrituals of his culture Anthropological studies haveshown that these vary widely between differentsocieties, each of which seems to have developedits own beliefs about the meaning of deathtogether with a set of rituals concerning thedisposal of the bereaved. Now, the ritualassociated with bereavement has declined, andGorer (1965) claims that this loss of recognitionand support for the expression of the grief isresponsible for increased psychologicaldisturbance among bereaved people today. Inthis respect, the Orthodox way of ritual mourning
appears to provide a more favourable environ-ment. In our culture, there is also a tendencyto encourage the strict control of feelings on thepart of the mourner.
Religious beliefs are also important inbereavement. Just as belief in an ‘after -life’ cancolour the attitudes of the dying to theircondition, so too it affects those who are leftbehind. The idea of ultimate reunion can be agreat comfort to the bereaved, though itsometimes leads to suicide in order to hastenthe process.
Children also have problems in acceptingdeath of their dear ones. Children develop theconcept of death around seven years of age.Due to the incomplete understanding, veryyoung children often cannot accept the absenceof the person due to death. As children do notopenly express their fears regarding death, theyoften develop emotional problems, which aremanifested in a sudden drop in their academicperformance, sleep disturbances, developmentof fears, depression and insecurity. Childrenshould be helped to talk out their fears andanxieties.
Clinical Applications
The care of the dying is also one of the respon-sibilities of the doctor. A great deal can be doneto provide relief from physical discomfort, andespecially pain; but care of the whole personincludes consideration of his psychologicalwelfare, and this is a matter which has receivedmore systematic attention in recent years.
One of the most frequently discussedproblems, is how much information should begiven to dying patients, in particular, whetherand if so when, they should be made aware ofthe fact that their illness is fatal. This questionis often put in relation to cancer—should thepatient be told? the implication being that thisis like pronouncing a death sentence. In fact,the matter is nowhere near as simple at this. By

136 Behavioural Sciences in Medical Practice
no means all patients diagnosed as having cancerwill have their lives shortened by the disease,while there are obviously many of other diseasesthat can threaten life. Nor in the presence ofa fatal disease, is the doctor usually able to predictwith any degree of accuracy when death willoccur. For their part, patients often suspect andsometimes are sure that they are dying beforebeing told so. Doctors vary in their attitudes totelling patients the truth about fatal illness,ranging from those who consider it never rightto do so, to those who believe in always pro-viding such information. Most, probably take aposition somewhere between these two extremesand try to judge what is best for each individualpatient.
Most dying patients ultimately come to anawareness of the truth, whether or not they askfor and are given it. Greater stress should begiven on listening to what patients have to sayand ask than on what should be said to them.If they are given the opportunity to talk abouttheir situation, to voice their concerns and toexpress their wishes, it is usually possible to judgethe best response to any question aboutprognosis. Some indicate quite openly that theydo not want to know if their illness is fatal, andthis wish should be respected. Others, ask thequestion in such a way that it indicates the needfor reassurance, or at least hope (‘It’s not cancer,is it doctor?’). In this event, rather than givingan immediate denial and perhaps untruthfulreply, which will be of more lasting value to thepatient than a consoling but false picture of thefuture; by allowing him to talk freely andrepeatedly in this way, and by giving simpleexplanations of his disease, the patient’sawareness of dying may gradually grow in anatmosphere of sympathetic understanding.
Attitude towards death, namely, the sense offailure felt by medical and other staff in the faceof a fatal illness. This may sometimes lead to atendency to withdraw from contact with thedying, which may be sensed by the patient.
Many patients are sensitive to this difficulty onthe part of some doctors and feel unable to talkopenly to them about their illness, for fear ofcausing embarrassment. However, that a shiftmay be occurring within the medical professiontowards greater frankness, and this is associatedwith an increasing emphasis on the care of thedying in medical education.
An awareness of the normal sequence ofevents in typical grief, together with an under-standing of the psychological processes involved,should be of assistance to those who areconcerned with advising and helping thebereaved, and indeed it has become recognisedthat bereavement counselling requires morethan common sense if it is to be effective.
During the early stage of numbness, thebereaved person needs a certain amount ofassistance with simple decisions and practicalmatters to do with the registration of the death,funeral arrangements, etc. Once the initial phaseof shock has passed, sharing of the feelings ofgrief may be most helpful, while advice to ‘stopthinking about it’ can be positively harmful.Expression of emotions should be allowed butnot forced by insensitive probing. Individuals willvary in the degree to which they actually expresstheir grief—what is important is that they shouldbe able to feel it. This means rejecting thecustomary social attitude, which seems to implythat grief can be avoided by not talking aboutit, and by restricting conversation to trivialitiesinstead. The bereaved person needs sympatheticunderstanding but not pity, and at this time,social support system provided by relatives andfriends in our culture is very helpful in copingwith the loss. Bereavement sometimes leads toabnormal reactions, which may be of clinicalimportance, both physically and psychologically.There is evidence for an increased incidence ofboth morbidity and mortality from organicdisease, following bereavement. Bereavementmay also result in a psychiatric illness such aneurotic illness, depression, schizophrenia, or

Dealing with Death and Bereavement 137
mania, for example. In this case, the actualnature of the psychological disturbance isprobably not determined by the bereavement,which simply acts as a nonspecific precipitatingstress.
Sometimes you may encounter abnormalgrief reactions, which may be seen as variantsof the normal process, and are thus ‘stress-specific’, i.e. they only occur following a loss.Parkes (1965) describes three types of abnormalgrief. Chronic grief represents an intensificationand prolongation of the typical form, and isfrequently associated with recurrent ideas of guiltand self-blame, and with physical symptoms,similar to those of the final illness of the deceased.Inhibited grief tends to occur in the very youngor the very old, and is characterised by theprolonged inhibition of a large part of the totalpicture of typical grief, with substitution of othersymptoms instead. Delayed grief is typical orchronic grief occurring after a delay of monthsor years.
Parkes reviewed the evidence, mostly fromstudies of bereaved women, concerning thedeterminants of severe grief reactions, andconcluded that the high-risk case would havethe following characteristics; a young widow withchildren and no close relatives nearby; a timid,dependent personality, history of depressiveillness; a relationship with her husband whichwas closely dependent or ambivalent with nopreparedness for his unexpected death; andfinally, a family and cultural tradition whichinhibits the expression of grief.
SUMMARY
The care of dying patient and comfort of thebereaved are major responsibility of doctor andas important as providing treatment. Determi-nants of psychological response to dying are
associated with its cause (e.g. due to aging ordisease), and with the individual and his enviro-nment. Fears of death are at times focussed lesson the thought of death itself, and more on theprocess of dying. Sometimes, death is disturbingand may result in extreme physical distress.Some measures can be taken by the clinicianin consultation with the family members, tomake the dying person more comfortable bytalking to them, listening to their wish andreducing their apprehensions and anxiety.
The effect of death on those who are stillalive has also received systematic investigationin the recent years. A fairly consistent patternof mourning has been identified. Typical oruncomplicated grief is usually following deathof a parent, child, sibling, or first-degree relative,with whom there has been at least moderatedegree of social contact within preceding year.Bereavement involves several stages, includingthe shock following the death within few hoursto six months, till the individual has a fullacceptance of death. Children also haveproblems in accepting death of their dear ones.As children do not openly express their fearsregarding death, they often develop emotionalproblems, which are manifested in sudden dropin their academic performance, sleep distur-bances, development of fears, depression andinsecurity.
Attitude towards death, on part of medicalstaff and how the matter is conveyed is of utmostimportance. On awareness of the normalsequence of events, in typical grief together withan understanding of the psychological processesinvolved, should be of assistance to those whoare concerned with advising and helping thebereaved, and indeed it has become recognisedthat bereavement counselling requires morecommon sense, if it is to be effective.

15Attitudes
PART 4: Social Behaviour
Dr Krishan Kant, is taking history of a patient,admitted in surgery ward. The patient has pasthistory of abusing illicit drugs, he is not employed,and his appearance is not good. Presently thepatient is having fever and has an infectedwound on his right thigh. When this case historyis presented, the consultant is surprised that inspite of being a good resident doctor, Dr Kanthas neglected to elicit some common details,which were important to diagnose this patient.This incomplete case history was not due to lackof competence, but due to negative attitudestowards patients with substance abuse.
There is an increasing awareness of theimportance of the role that attitudes and abilityto communicate play, in the delivery of effectiveclinical services. It is extremely important for adoctor to be a congenial person who has thesincerity and tact to strike a good relationshipwith the health care team, his patients and theirfamilies. Attitudes related to patient care, takingresponsibility and working in a team developduring the training of the medical students.Hence, it is necessary to assess attitudes ofstudents from time-to-time.
Nature of Attitudes
An attitude is a tendency to behave in a pre-ferential manner. It denotes certain constant traitsin an individual’s ways of feeling and thinking,and his predispositions towards action with regardto another person such as, a patient Attitudesare our expressions of likes and dislikes towardsthe people and objects. They determine andguide our behaviour in different social situations.One may have noticed that a doctor’s behaviouris different while treating an elderly person ascompared to an adolescent, or if treating acritically-ill patient. These differences in behaviourare because of his attitudes towards old peopleand adolescents. Our attitude towards a critical,terminally-ill patient determines how we interactwith him or his family members. An attitude hasthree components:• Cognitive what a person knows and his belief
about the attitude object.• Affective how he feels about the attitude
object.• Conative behavioural tendency towards the
object, both verbal and nonverbal (Fig.15.1).

Attitudes 139
Fig. 15.1: Components of attitudes
Let us take an example to illustrate thesethree components of an attitude. Consider theviews of an imaginary person named Dr ArvindVerma on the issues of drug addiction. Dr Vermahas some beliefs about persons taking illegaldrugs, the conditions under which they are takenand the problems these persons can create. Allof these beliefs constitute cognitions about drugaddiction. Dr Verma also has some feelings aboutdrug addiction. Whenever he comes across sucha person, he feels sorry and has sympathy forthe family members of the addicted person.What does Dr Verma do to help these personsreflects his behavioural tendencies towards drugaddicts. Thus attitudes are more than the mereknowledge of the subject matter. There is feelingassociated with it and this determines the actionthat the person would take in that particularsituation.
Attitudes are predisposed ‘tendencies torespond in a particular way and not a fixedresponse. These are not innate. The whole per-sonality structure of an individual and his beha-viour are constituted by a complex of interlinkedattitudes. Attitudes are influenced by a numberof factors. Attitudes are preferences towards awide variety of attitudinal items such as likes ordislikes, anti or pro, positive or negative.Anything that arouses evaluative feelings can becalled an object of attitude, e.g. an attitudetowards assessment of teachers. A distinction iscommonly made between attitude and opinion.An opinion is a belief that one holds about someobject in his environment. It differs from attitude,being relatively free of emotion. It lacks theaffective component central to attitude.
Role of Attitudes in Nursing
In medical, students’ attitudes vary according topatient’s characteristics, quality of teaching andattitudes of teachers. A significant relationshiphas been reported between attitudes and thelearning material. The choice towards a‘particular medical speciality’ plays significant rolein determining the ultimate career choice.Attitudes influence the behavioural responses ofthe individuals. The professional attitude of thedoctor is not only concerned with his feelings,beliefs and behaviour towards the patients, butalso towards other elements of professionalfunctioning like health care delivery, scientificinterest and collaboration with other pro-fessionals. Importance of the assessment ofattitudes for doctors can be related to thefollowing factors:
Patient care: Any negative attitude towards race,community or disease results in a prejudicialbehaviour that affects the patients.
Formation of attitudes of peers or juniors: Seniordoctors has a significant impact on the studentsfor the formation of opinions concerning health-related issues.
Acceptance of new technology: In the presenttimes, many new innovations in techniques,equipment and methods of health care deliveryare taking place. Our attitudes can biasacceptance of new technology and high profilespecialities.
Interpersonal skills: Studies have shown thatduring training of undergraduate students thereis a gradual decline in their interpersonal skills.This affects skills of history taking and elicitationof information from the patient.
Curriculum planning: While planning a newcurriculum or revising the existing curriculum ineducational courses, one needs to identify theattitudes of the students and teachers.
Effects of attitudes on meaningful learning andretention: Attitudinal bias has a differential effect

140 Behavioural Sciences in Medical Practice
on the learning of controversial things. With afavourable attitude, one is highly motivated tolearn, puts greater effort and concentrates better.Negative attitude leads to close-minded view toanalyse new material and hence, learning isimpaired. Attitude structure exerts an additionalfacilitating influence on retention that isindependent of cognition and motivation.
Effect of attitudinal bias on training/learning:Attitudinal bias often causes loss of objectivityin a clinical setting. This is encountered insituations where either a relative patient is beingexamined or a patient revealing a historyresembling the student’s own life. Class or racialdifferences also impair a student’s ability to relateeffectively.
Marcotte and Held (1978) have suggesteda set of responses that reveal attitudinal bias whileexamining the patients. These are:1. Premature closure and dogmatic response—
an early referral is made prior to taking acomplete history, a simplistic solution maybe provided in the initial contact.
2. Evasion—student misses the patient’s historyand directs the conversation under his control.
3. Premature reassurance—here the studentnegates the concerns of the patient andreassures the patient without havingsubstantial evidence.
4. Rejection—student may avoid conflict areasand reject patient’s concerns by neglect.
5. Condescension—Value-laden language isused so as to shame, embarrass or humiliatethe patient.
6. Too many technical jargons are used by thestudent that confuses the patient.
Developments of Attitudes
Attitudes can develop through different modes.Heredity may play only a very small partthrough differences in the physical characteristicsand intelligence. It is mainly the environmentalfactors that are responsible for development of
attitudes. These are through family, peers,conditioning in sociocultural environment (Fig.15.2).
Fig. 15.2: Development of attitudes
Family
Family is the first place for formation of attitu-des. Parents begin the information flow thatforms beliefs and attitudes about things.Categories are formed in our head on the basisof early information.
Sullivan has observed that the informationprovided by the parents in the earliest stages oflife is very difficult to undo. Erroneous andnonadaptive attitudes moulded from parentalfeedback have tremendous implications forfurther personality development.
As we grow, we tend to be influenced byother sources such as friends and group mem-bers. They serve as reference group in the deve-lopment of attitudes. One identifies oneself withfriends and moulds one’s attitudes in relationto the prevailing norms of the group concerned.
Peers
Just as we learn from family in the early child-hood, later our peer group has a tremendousinfluence on the development of attitudes. Onemay form very different or opposing attitudesin the company of friends, e.g. attitudes towardspatients with AIDS or addictions, etc.
Conditioning in Sociocultural Environment
There are ample examples in our socioculturalenvironment, which are responsible forconditioning our attitudes. One such exampleis words, which have acquired effective meaning.

Attitudes 141
They can create positive or negative attitudes.Many attitudes developed on the basis of classicalconditioning are found to be irrational, as theyhave been paired with an emotion producingunconditioned stimulus either accidentally or ina quite extraneous situation. Similarly theappropriate attitudes can be developed throughclassical conditioning.
An attitudinal response can be learnt throughinstrumental conditioning by reinforcing aresponse that occurred in the presence of adiscriminated stimulus. Any responses, whichhave a reinforcing consequence, are learnt morereadily than those without reinforcement. Inter-racial and intercaste attitudes are prevalent inour culture, so if your interaction with personsfrom other caste is satisfactory, you tend todevelop positive attitudes towards persons ofthat caste.
How to FacilitateDevelopment of Attitudes?
The problems of ensuring teaching as well asthe development of attitudes may be ideallyresolved by selection of medical students whowill pay attention to humanistic concerns andby recruiting faculty members who can serve asrole models for the younger students. However,a more realistic approach would be to buildlearning opportunities, and to ensure periodicalassessment of the same. One needs to organiseeducational methods that cut across disciplinesand provide the right setting for developingattitudes besides imparting knowledge.
Teachers motivate and facilitate the deve-lopment of attitudes in students. Attitudes ofsenior students and peers also help in shapingthose of future students. Though there are noguaranteed methods of teaching attitudes, yetteachers must be aware of all learningexperiences that facilitate the development ofworthwhile attitudes.
Providing Information
Information can bring changes in attitudes. Forexample, information about smoking as a causefor cancer and heart diseases is likely to bringabout changes in attitudes towards smoking. Itmay not work in all cases, but it is generally foundto be helpful. Information about attitudes maybe imparted through lectures, or audiovisualaids, especially, video and films. The attitude ofeven health professionals towards AIDS patientscan be changed dramatically, by effectiveutilisation of video films and other audiovisualmedia.
Providing Examples or Models
Most advertising is designed to change attitudes.A common technique is to show an ideal personusing a certain product. The advertiser aims toprovide a model or an example, which will befollowed by the reader. Many students considertheir teachers as a role model and often emulatetheir teacher’s behaviour. If the teachers are rudeto patients, then their students will tend to dolikewise. It is therefore, essential to set goodexamples for the students.
Providing Experience
Medical training provides a number of experi-ences, which shape the attitudes of the students.They may see patients with sores that have notbeen treated and that have become septic andpossibly disabling. This direct experience ofseeing the patient’s suffering will have far moreimpact on shaping students attitudes than awhole lot of theoretical information about theneed for early treatment of sores and superficialwounds.
Discussions
Discussions in small groups are generally thoughtto be helpful in shaping student’s attitudes.

142 Behavioural Sciences in Medical Practice
Discussion also helps to make the previous threemethods more effective. For example, it ishelpful for students to describe and discuss theexperiences that they have had with theirpatients. During the discussion, they can sharetheir experiences with other members of thegroup. Discussions also help to change students’attitudes by the process in which a student giveshis opinion and sees the reactions of otherstudents. Discussions are more effective in smallgroups.
Role-play
Role-playing is an exercise in which the studentsplay roles of suffering patients, doctors, para-medicals, etc. and begin to experience differentkind of behavioural attributes. In a role-play, theparticipants exaggerate a situation or anincidence so that the audience can betterappreciate the gravity of the situation. Not onlythe participants benefit from the role-play, butalso the audience who can empathies with thecharacters of the role-play. The job of the teacheris just to play a theme for the role-play and briefthe participants on the theme. A group discussioncan be conducted at the end of the role-playto analyse the theme and to identify the ‘takehome message’.
Attitudes to be Developed byUndergraduate Medical StudentsIt has been felt that medical students need todevelop more humanistic attitudes towardspatients and their relatives. It is difficult to listall the attitudes that one would like students tohave. Some of the essential and primary attitudesexpected from the medical student are givenbelow.1. Eliciting psychosocial aspects of the illness.2. Giving due respect to the patient’s age; com-
municating patiently with older patients.3. Examination of female patients in privacy.4. Informing the relative about the patient’s
condition.
5. Breaking the news of death to the relatives.6. To elicit history concerning very personal
aspects of patient’s life, like sexual history.7. Informing the patient before giving an
injection or doing a procedure.8. Understanding individual differences and
reactions to illness.
Methods to Change Attitudes
During the development stage if a student hasdeveloped certain negative attitudes, which laterinterfere with his professional competence, thenit is desirable for the student to modify thenegative attitudes. It is not an easy task to changeattitudes, as they are consistent ways of reactingtowards object. Attitudes can be changed underdifferent conditions. It is necessary to modifyunhealthy or irrational attitudes for learning newthings.
Attitude change is influenced by both factorsthat are external as well as internal to the person.One should pay attention/consider the com-municator, communication and the audience tobring about a change in attitude (Fig. 15.3).a. Source or the communicator should be very
effective and highly credible. He should betrustworthy and an expert to produce thechange. Communicators, if they are similarto the target audience, their message is welltaken, that means the communicator shouldis be someone from your profession, specialityand should be considered as a role modelby you.
b. Content of communication has also beensubjected to research. The findings are thatcommunications, which discuss both the prosand cons to the point, are more effective insituations where there is initial resistance toaccept. Communications associated withpleasant emotions can also enhanceeffectiveness.
c. Personality characteristics of the audiencehave been linked with attitude change.However, self-esteem and intelligence do not

Attitudes 143
play a very important role in changingattitudes. Increased discrepancy between theaudience’s attitudes from the target’s positioncan help in change of attitudes. Committingthe audience to take challenges or dosomething has proven to be an effectivetechnique for attitude change. Generalsusceptibility or suggestibility of an individualwill also determine their tendency to accept/reject new information.Similarly role playing, bringing change
through smaller steps, distracting the audienceare some other methods which have been usedto change attitudes.
Fig. 15.3: Methods to change attitudes
ASSESSMENT OF ATTITUDES
In the studies conducted by the consortium(Verma et al 1993), it has been revealed thatsome departments discussed attitudes at timeswhile imparting the news of illness to the patientsand their families, but no one assessed them.Medical educators assess the acquisition ofstudent’s skills but not attitudes. Assessment ofattitudes seems to be ignored because of thefollowing reasons:1. Attitudes are often vague and ill-defined
entities.2. The teachers frequently differ on what
attitudes are really desirable.3. Our instruments for measuring attitudes are
not really good. Hence many teachers consi-der it inappropriate to use these instrumentsof poor reliability and validity for thepurposes of grading certification.
Measuring an attitude is a difficult task, asit has to be measured in an indirect way. Onecannot see the attitude directly; it must bemeasured from what the individual says or does.Even when one talks about the behaviouralcomponent of an attitude, the predisposition toact in a particular way is concerned with thepreparation to act rather than with the act itself.Attitudes do refer to internal aspects of behaviourbut there are also external manifestations ofattitudes, as they are often expressed in actions.What a person does, and the manner in whichhe or she does it, most directly expresses aperson’s behavioural tendency. Actions may alsoexpress beliefs or feelings, though not so directlyas they do the behavioural component.Occasionally, physiological indicators may beused, but even these are only indirect by-products of the internal arousal associated withan attitude.
The most common approach in attitudemeasurement is to find out how favourable orunfavourable is the individual to an idea. Thereare different methods of measuring attitudes.Some of these are very simple while others arecomplex. Broadly, attitudes can be measuredby self-report methods, attitude scales and invo-luntary behaviour methods. Attitude scales aremore often used because of their reliability. Thecommonly used scales are the Likert scale andthe Osgood’s semantic differential scale.
The various instruments in current use forassessment of attitudes are:
Rating ScalesA series of statements concerning attitudes beingmeasured are made, and the answer is expectedon a 3-7 point scale. The most commonly usedscales are Likert scale which ask the rater to ratethe attribute on a five point scale viz. stronglyagree/agree/undecided/disagree/stronglydisagree. Osgood’s semantic differential scale isanother commonly used scale.
Likert scale: In Likert scale, an attitudinal objectis assessed on a five point scale ranging from

144 Behavioural Sciences in Medical Practice
extremely positive to extremely negative. It formsa continuum extending between two extremesof a scale. Each pole of the scale is representedby the attitude intended to be assessed. Thescores are given from 5 to 1. Some of theexamples of this type of scale are given below:
Behavioural science is of A B C D Eminimum relevance in UGmedical curriculum
Knowledge of behavioural A B C D Esciences helps in under-standing psychosocialaspects of illness
Each patient needs an A B C D Edifferent way of communication to explain hisproblems.(A: strongly agree, B: agree, C: cannot decide,D: disagree, E: strongly disagree).
Monchy et al (1988) had developed a scaleto measure professional attitudes of students ondoctor-patient relationship. Some of its items areas follows:
The emotions Strongly Agree Neutral Disagree Stronglyof the doctor agree disagreeshould agreeideally neverplay a role inhis dealingswith patients.Only a small Strongly Agree Neutral Disagree Stronglynumber of agree disagreepatients areable to under-stand complexhealth problems.
Osgood scale: In Osgood’s scale, two oppositeadjectives are given with gradations. Followingare some examples of this scale:
Behavioural Sciences course in medicalcurriculum is:Useful --------------------------- Not useful.Informative -------------------- Not informative.Interesting ---------------------- Uninteresting.Relevant ------------------------ Irrelevant.
Observational Rating Scales
In clinical settings, the students’ attitudes canoften be assessed through observational ratingscales. This requires repeated and standardiseddirect observation of student’s behaviour(activity) over a long period and in natural pro-fessional situations such as in the ward with olderpatients, outpatient clinic or in primary healthcentre. Attitudes are assessed on a standardisedrating scale. If the rating is not done carefullyit can lead to various errors in the measurement.One example of this type is as follows.
If a student is being observed when he isexamining a patient, and an evaluation is neededof how he gains the patient’s confidence, thefollowing rating scale may be used:
The student has:Taken all the necessary precautions, andthe patient appears completely relaxed 5Taken the necessary precautions and hasreassured the patient several times 4Made an effort, and has followed it up 3Made an effort, without following it up 2Seems to be quite unaware of the problem 1
Though assessment of attitudes is a difficulttask it is worth taking the trouble, as it wouldensure positive development of attitudes inmedical students. This can be integrated withassessment of skills and knowledge.
Indirect MethodsOne of the methods is based on the principlethat people remember better the things that theyconsider to be important. A group of studentmight be shown a filmed interview with a patientfollowed by a series of multiple choice questions,some of them relating to biomedical aspects andothers to the social aspects of the case. Theanswers to questions relating to social aspectswould indicate the attitudes of the candidate.
Construction of an attitude scale: One oftenfaces difficulties in deciding what aspect of anattitude is to be measured. We cannot measure

Attitudes 145
everything at one time, so we must chooseprecisely what we wish to measure or examine.Often attitude scale needs to be constructed fora particular aspect that one wishes to measure.Following are the steps in construction of anattitude scale:1. Specify attitude variable that is to be
measured.2. Collect wide variety of statements.3. Edit the statements.4. Sort out the statements into (an imaginary)
scale.5. Calculate the scale value.
Writing of the statements is difficult yet mostimportant aspect of constructing an attitude scale.Some of the guidelines for writing the statementsare given in the box.
Reliability and validity: Since most of the time,attitude scales are constructed for the specificaspect of behaviour, one should do item vali-dation of the statements and estimate reliabilityand content and construct validity of the scaleusing standard procedures, such as test retestmethod, split half method, etc.1. The statements should be brief.2. Each statement should convey one complete
thought.3. The statement should belong to the attitude
variable that is to be measured.4. Care should be taken on language:
- use simple sentences- avoid double negatives- avoid “all, always, none or never”- use with care “only, just, merely”- avoid words with more than one mean-
ing.5. The statements should cover the entire range
of the effective scale of interest.6. Statements should be such that they can be
endorsed or rejected (agreed/disagreed).7. Acceptance and rejection should indicate
something about the attitude measured.
SUMMARY
An attitude is a tendency to behave in apreferential manner. It denotes certain traits inan individual’s ways of feeling and thinking, andhis predispositions towards action with regardto another person such as a patient. Attitudesare our expressions of like and dislikes towardsthe people and objects. They determine andguide our behaviour in different social situations.
An attitude has three components, Cogni-tive—What a person knows and his belief aboutthe attitude object, Affective—How he feelsabout the attitude object and Conative—Behavioural tendency towards the object, bothverbal and nonverbal.
Attitude development in itself is a long process.The formation occurs on three different modes.The family, peers and the conditioning processesboth operant and instrumental provide expla-nation for formation of rational and irrationalattitudes. Balance theory tries to explain howattitudes change to create a balanced structure.However, if a imbalance exists, there is atendency to move towards this balance.
Once we understand our attitudes we workin the direction of change especially modifyingirrational and unhealthy attitudes. Attitudechange is influenced by both internal andexternal factors. It involves a communicator, thequality of communication, the content of themessage and the receiver’s personality. Forfacilitation of development of new attitudes insuch clinical settings we need to provide moreinformation, a model, have more discussions,look into experiences of medical students andexact patient-doctor role plays. A list of essentialand primary attitudes expected from medicalstudents has been given at the end of thechapter. Thereby correct attitudes would bringin satisfaction of needs bringing in satisfactionof work.

16Family
Ms S, 16 years old, weighing 25 kg, five feettall, was diagnosed as having an eating disorder—anorexia nervosa. She presented withcomplaints of loss of weight, poor appetite,irritability, acting out aggressively, both at homeand at school. On detail history taking, it wasnoted that her family consisted of hergrandmother, parents and four siblings. Out ofthe four siblings, she was the eldest girl with theyoungest child a brother. There was maritaldisharmony between her parents. The motherperceived her husband as extremely harsh andcommunicated more with the patient. Thoughthe family was very well off, yet the mother oftenborrowed money from her parents to fulfill theneeds of the children. Grandmother was punitiveand abusive to children, and they often hadverbal fights in the family. This caused anxietyin the patient. Her problems reflected instability,erratic, unpredictable environment in the house.The mother was afraid to face uncontrollabletemper-tantrums of the patient and gave in easilyto fulfill, even irrational demands by her. As aresult, the homeostasis of family as a system wasdisturbed, with poor understanding of the needsof the family members.
This is an example of how family canpredispose, precipitate and reinforce the illness.In this chapter, you will learn the importanceof studying family, their relationships, communi-cations and developments of psychopathology,and role of these factors in therapy.
Structure of Family
The family is a system of social relationships,which trains its young in different dealings in thesociety. A family cares, protects and educates itsyoung, not only in the ways of its culture butalso in ways that helps to establish identity, self-concept and functioning of its children. Thefamily is the most powerful force for the pro-motion of health, as well as for the productionof disturbance in members. Ackerman (1966)has described the disturbed family as one, inwhich the members sacrifice one of their ownmembers in order that their needs are gratified.Assessment of presenting quality of familyinteraction are essential components in itsunderstanding.
The family structure may be nuclear, exten-ded or joint. As shown in Figure 16.1, the nuclearfamily consists of a married couple and theirchildren; extended family has parents, their sonand his wife and children. The joint family is akin group, which may contain 3 or moregenerations within one household. It may haveparents, all their children with their families, andin some households it may extend further, i.e.children of the third generation may also livein the same house. All the family members sharea common kitchen. The joint family system wasvery prevalent in our culture, but now this systemis breaking for extended and nuclear familysystem. The nuclear family is a product ofmodern culture and values. In other words, the
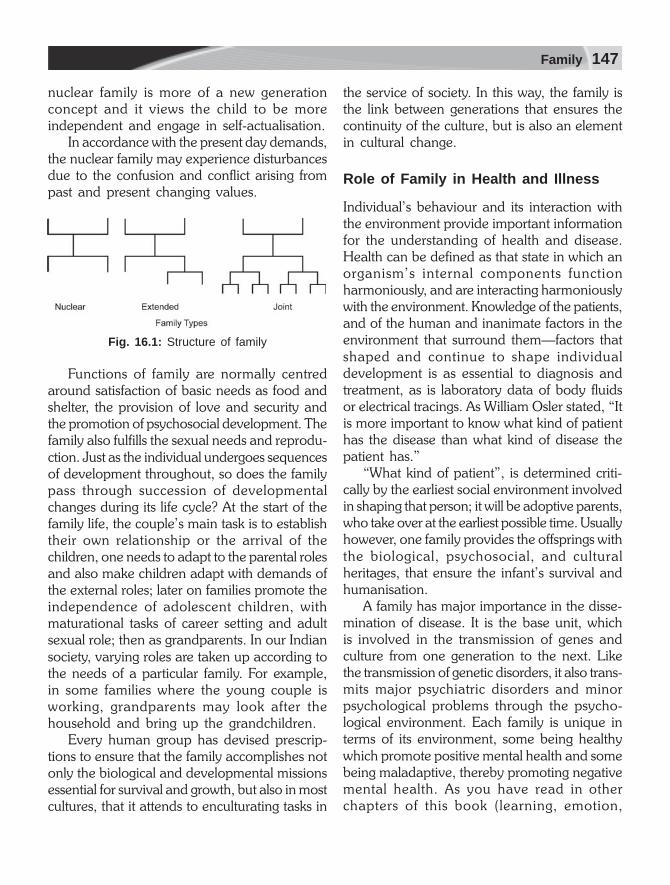
Family 147
nuclear family is more of a new generationconcept and it views the child to be moreindependent and engage in self-actualisation.
In accordance with the present day demands,the nuclear family may experience disturbancesdue to the confusion and conflict arising frompast and present changing values.
Fig. 16.1: Structure of family
Functions of family are normally centredaround satisfaction of basic needs as food andshelter, the provision of love and security andthe promotion of psychosocial development. Thefamily also fulfills the sexual needs and reprodu-ction. Just as the individual undergoes sequencesof development throughout, so does the familypass through succession of developmentalchanges during its life cycle? At the start of thefamily life, the couple’s main task is to establishtheir own relationship or the arrival of thechildren, one needs to adapt to the parental rolesand also make children adapt with demands ofthe external roles; later on families promote theindependence of adolescent children, withmaturational tasks of career setting and adultsexual role; then as grandparents. In our Indiansociety, varying roles are taken up according tothe needs of a particular family. For example,in some families where the young couple isworking, grandparents may look after thehousehold and bring up the grandchildren.
Every human group has devised prescrip-tions to ensure that the family accomplishes notonly the biological and developmental missionsessential for survival and growth, but also in mostcultures, that it attends to enculturating tasks in
the service of society. In this way, the family isthe link between generations that ensures thecontinuity of the culture, but is also an elementin cultural change.
Role of Family in Health and Illness
Individual’s behaviour and its interaction withthe environment provide important informationfor the understanding of health and disease.Health can be defined as that state in which anorganism’s internal components functionharmoniously, and are interacting harmoniouslywith the environment. Knowledge of the patients,and of the human and inanimate factors in theenvironment that surround them—factors thatshaped and continue to shape individualdevelopment is as essential to diagnosis andtreatment, as is laboratory data of body fluidsor electrical tracings. As William Osler stated, “Itis more important to know what kind of patienthas the disease than what kind of disease thepatient has.”
“What kind of patient”, is determined criti-cally by the earliest social environment involvedin shaping that person; it will be adoptive parents,who take over at the earliest possible time. Usuallyhowever, one family provides the offsprings withthe biological, psychosocial, and culturalheritages, that ensure the infant’s survival andhumanisation.
A family has major importance in the disse-mination of disease. It is the base unit, whichis involved in the transmission of genes andculture from one generation to the next. Likethe transmission of genetic disorders, it also trans-mits major psychiatric disorders and minorpsychological problems through the psycho-logical environment. Each family is unique interms of its environment, some being healthywhich promote positive mental health and somebeing maladaptive, thereby promoting negativemental health. As you have read in otherchapters of this book (learning, emotion,

148 Behavioural Sciences in Medical Practice
motivation, illness behaviour and pain), thatfamily also plays a crucial role in teachingadaptation to physical illness. It also provides theimmediate environment for the sharing of genes,diet, toxins, infections, stress, emotions and socialattachments that may interact to affect expres-sion of underlying physical and behaviouraltraits, and also to cause various mental disordersand to influence the outcome of these disorders.
This is specially true for children’s beha-vioural disorders, which are related not only togenetic factors (inherited from parents andshared with other family members) but also tofamily environmental factors as the family formsthe earliest, immediate and most persistent socio-psychological environment for the infant andsmall child and shapes its behaviour and atti-tudes. Even when child comes out of the family,its subsequent experiences are perceived, under-stood and emotionally reacted according to thefoundations established within the family. Therole of family in causation and outcome ofvarious mental illnesses has been proved byvarious studies showing positive or negativeassociation between specific behaviouraldisorders on one side and certain types of familypsychopathology on the other side. We are moreconcerned with the psychological dysfunctions,so we shall limit our discussion on family dys-functions rather than positive aspects of thefamily.
There have been various studies in whichillness has been correlated with the family. Familycan transmit illness through heredity, both inphysical and psychiatric disorders, for example,diabetes, coronary disorders, blindness, andmood disorders. A family can also transmit illnessthrough its psychological environment forexample, inconsistency in disciplining, maritaldiscords, broken homes, financial problems,chronic illness and so on. Perception andexperience of pain (see in Chapter 25) is alsoinfluenced by the family members. Familyenvironment is very important in the causation
of childhood psychiatric disorders. Some of thestudies conducted have shown that abdominalcomplaints in the immediate family members ofthe children with recurrent abdominal pain(RAP) was six times higher than the matchedcontrols. Out of this, mothers accounted for 2/5th of the family members affected by RAP.
Psychological problems in family membershave been reported by several authors. Friedman(1972) noted that children with RAP experiencestressors such as psychological illness in one onboth parents, parental discord, parental absenceand unsatisfactory parent-child relationships.Hodges et al (1985) emphasised that bothparents of a child with RAP demonstratedsignificant anxiety levels, with mothers out num-bering fathers - 25 to 40 percent of the mothershad mild depression also.
Families represent more than mere collectionof individuals. There are patterned regularitiesin transactions among individual family mem-bers, and between the family and the largercommunity, that may have important impli-cations for their health and well-being. Familytheorists have sometimes underestimated thelarge areas of autonomy in the lives of familymembers, and their ability to transcend the limitsof the family’s influence. Nonetheless, they havealerted us to the need to observe howinvolvement in a family regulates and constrainsor facilitates the coping of the individuals.
It should be made clear, that no argumentis made that only the family transactions causethe psychosomatic problems occurring in a givenfamily member. Instead in some families, symp-toms may foster the development of problematicfamily organisation.
Weakland (1977) has coined the term ‘familysomatic’, to indicate the family’s involvement inhealth and illness. He argues that it is importantto describe concretely how both illness, and themaintenance of health pose problems for a givenindividual and other members of the family, andhow they cope with it.

Family 149
Affective Involvement
Optimally the family meets emotional needs ofall members and provides cohesion, security andsense of being valued that contribute to thedevelopment of trust, self-esteem and indepen-dence.
The degree of affective involvement variesin the families, with some having more intenseand involving family relationships. The qualityof involvement determines, whether the relation-ship is nurturing and supportive or destructiveand self-serving (Epstein and Bishop, 1981). Inthe uninvolved family, both the degree and thequality of involvement are low. Such familiesencourage premature emotional separation,often resulting in pseudoindependence thatmarkedly impairs the capacity to tolerate trueintimacy. Families whose intensity and quality ofinvolvement are only slightly greater than thoseof unemotional family, may be described asshowing interest which is devoid of feelings.Some families still show a still higher intensityof affective involvement, but withdraw theiracceptance as soon as any member fails to satisfythe others’ needs. Such parental narcissisticinvolvements are destructive in quality andusually excessive in degree.
Intense but destructive involvement occurswhen two or more members are enmeshed(Minuchin, 1974). The concept of enmeshmentis identical to those of symbiotic relationships(Solnit, 1978). It has pseudomutuality,undifferentiated family ego, and too richly cross-jointed system. Enmeshments are alwaysreciprocal. They are destructive as they areincompatible with the development ofautonomy and usually involve tolerance, andreinforcement by other family members. Thoseinvolved are overly sensitive and react withpanic or rage to any attempt by the otherpartner at withdrawing.
Control Styles
Family members influence each other to ensurethe accomplishment of the instrumental tasks androle requirements of daily life. Families vary inpredictability and constructiveness, and eachfamily has its own prototypical control styles.Generally control styles have been classified intofour types: (i) rigid, (ii) flexible, (iii) laissez-faireand (iv) chaotic.
Rigid families are quite successful at main-tenance control, but their rigidity interferes withsuccessful adaptation and assumption of personalresponsibility.
A flexible control style combines moderatepredictability with high constructiveness. In aflexible style, task accomplishment is relativelyeasy to achieve because its supportive andeducational tone encourages family membersto participate and to identity with the rules ofthe family.
In laissez-faire style, members do as theyplease so long as to avoid bothering others andas little responsibility is assumed or expected.Because of their constant disorganisation, roleintegration is rarely achieved, task accomplish-ment is haphasard and communication isfrequently insufficient, unclear and indirect.
A chaotic style is extremely low, both inpredictability and constructiveness. Changesdepend more on the mood of the dominantmembers in the family than situational demands.Instability and inconsistency typify these familiesand the overall effect is destructive.
Values and Norms
Every aspect of the family functioning, directlyor indirectly reflects ‘the family’s values andnorms’. The way in which roles are defined, theforms of communication considered acceptable,the predominant patterns of affective involve-ment and the control style are all shaped by

150 Behavioural Sciences in Medical Practice
values derived partly from the references of theparent’s families of origin, to partly from theculture and subgroups to which a family belongs.
Family Temperament
As any clinician is aware, families vary dramati-cally in the character and flavour of their inter-nal environments. Family temperament mea-sures the underlying regulatory principle infamilies. Family temperament, is a product ofthree properties of family personality—family’senergy level, preferred interaction distance, andcharacteristic behaviour change.
The family sets various guidelines and limitsfor it’s functioning. The family’s energy levelestablishes guidelines about behavioural activity,the family’s preferred interactional distanceestablishes guidelines, regarding boundarypermeability and their behaviour rangeestablishes guidelines about the degree ofvariability, that the family manifests in its patternsof interactional behaviour.
Pathology and Communicationin Families
Disturbances in the communication pattern arecharacteristic of the ‘emotionally disturbed’families. Family psychopathology generallyrevolves around two concepts, which are centralin understanding of psychopathology and usedin therapy; these being the double-bind and thefamily homeostasis.
The double-bind form of communication hasbeen labelled by Bateson et al (1968). Thedouble-bind messages are peculiar to families,in which one of the members is schizophrenic.This type of communication may also be foundin other families and may be induced in manycommon interpersonal situations.
The family as the social system is seen asmaintaining a cooperative balance or homeo-stasis. In a disturbed family, the members inter-act with one another in ways that are exploitative
or disturbing: “The emotional give and take” offamily relationships is crucial in the developmentof mental health. The family determines theemotional fate of the child; it affects the emotionaldevelopment of the adolescent and adultmembers as well (Ackerman, 1966).
The goal of communication amongst thefamily members is towards the achievement ofa mutual understanding, which is possible onlywhen the messages sent are clear, direct, andsufficient and the receivers are psychologicallyavailable.
In content, communication can be an affec-tive (i.e. expression of feeling) instrument, whichis either related to the ongoing tasks of everydaylife or neutral (neither instrumental nor affective).At the same time, communication can be clearor masked (vague), disguised or ambiguous. Themore masked is the message, the more likelyit is to arouse confusion, anxiety and subsequentdistortion in the receiver. The directedness andthe indirectedness of the message depend onwhether the message was received appropriatelyby the receiver, especially in indirect communi-cation. The components of communication arepresented in Table 16.1.
In disturbed families there may be parado-xical communication, which moves in twoopposite and internally inconsistent directions atthe same time.
Research on family interaction represents oneaspect of the broader field of inquiry, referredto as Family Studies of psychopathology. Thetheoretical and methodological perspective,which we refer to as family interaction embodiestwo major commitments: (a) to identify familypatterns and processes that are precursors,concomitants and consequences of disorderedbehaviour, (b) to the integration of this know-ledge into the broader family studies literature,concerned with the independent and inter-dependent effects of genetic, socioculturaland personality factors on the developmentof perpetuation of psychopathology. These

Family 151
interactions in greater depth with respect to thelevel of emotions is reviewed in the followingsection.
Systems Theory
Systems theory is a general theory to explainthe interactions and relationships between theindividual components comprising a larger struc-ture. This theory provides a framework tounderstand the behaviour of the individualsubsystems of the family such as the childrenor the parents, as well as their relationships tothe outside world. This theory has gained popu-larity as it not only explains how families workand function, but also provides a method ofanalysing faults and flaws in the daily activitiesof family life. For instance, poor delineation ofthe boundaries between the parental and childsubsystems can be responsible for problems ofcontrol and discipline with the children. The fourother concepts in the general system theory thathave influenced mainstream thinking about thefamily include:
Wholeness
It states that the system cannot be understoodby dissection and study of its individual parts.
We study the system as a whole. If one memberin the system changes, then all the members ofthat system will change because of that onemember’s behaviour in terms of response to thatchange.
Equifinality
The concept of equifinality implies that there aremany paths to the same destination. Applied tothe family system, it means that the particularpath a family takes as it evolves, its form is lesssignificant than the final form itself. This isbecause there are more than a set of eventsleading to a certain end state and therefore,studying the events will not produce much usefulinformation as studying the end state.
Feedback
Feedback refers to how individual units in thesystem communicate with each other. Feedbackis circular rather than linear. In a systems theory,we understand the network in terms of a circularfeedback loop, i.e. a change in A may producea change in B and subsequently A again. Eachperson’s behaviour becomes a reinforcingfeedback for the behaviour of the other.
Homeostasis
Feedback either reflects change (positive feed-back) or reinstates stability (negative feedback).The tendency of a system to seek stability andequilibrium is referred to as homeostasis. Thehomeostatic balance may be achieved byreducing deviations in process. This concepthas been enormously helpful for family thera-pists in understanding a family’s reluctance tochange.
The system theory is different from traditionalpsychoanalytic theory, where the intrapsychicdisturbances in the individual disrupt familyfunctioning. The key differences in the twotheories are highlighted below:
Table 16.1: Components of communication
Essential ProcessesExchanging information mutual understanding
verbal verbalnonverbal nonverbal
Critical aspectsSender Receiverclarity availabilityDirectedness opennesssufficiency
ContentsInstrumental regarding the mechanics of day-to-day life.Affective regarding the emotional aspects of family
lifeConsider: range and intensity of affect timingand duration of affect
Neutral neither instrumental nor affective

152 Behavioural Sciences in Medical Practice
Past vs Present
Psychoanalytic therapists use their knowledge ofthe past to help the patient better understandwhat is going on in the present. Systemictherapists, view behaviour within the currentinteractions in the family.
Content vs Process
When family members come to therapy theyfocus on the content. Parents may say that theirchild does not come home on time. A couplemay describe about their relationship being‘empty’. Although the therapist listens to whatfamily members say about each other (concept),he is chiefly interested in how family membersinteract with each other (process). Differentemphasis is given to the process of family therapyin various approaches.
Intrapsychic vs Interpersonal Context
The psychoanalyst focusses on the individualspast to encourage insight (intrapsychic), whereassystemic approaches focus on the current intera-ctions (interpersonal) to alleviate symptomaticbehaviour. Most of the systemic approaches dealwith other significant contexts also. Transgene-rational therapists include extended familymembers (grandparents) to change interactionsin the nuclear family.
Model of Individual Psychopathologyand Family Dysfunction
The fundamental tenet of a systems theoryperspective is that traditional problems in andother psychiatric disorders as schizophrenia,depression, drug abuse and anxiety are bestunderstood as manifestations of disturbances inthe family (Haley, 1976; Minuchin, 1974;Stanton, 1981; Watzlawick, Weakland and Fish,1974). The family member with “symptom” islittle more than a messenger or family scapegoat;
his/her symptoms serve to cover up thegeneralised family disturbance. In this sense, thesymptoms of the identified “patient” are viewedas serving a function for the family as a whole,despite the overt distress that may occur as aconsequence of these symptoms, e.g. adisruptive or delinquent child may consume aninordinate amount of attention from other familymembers, and thereby prevent parents fromattending to the emptiness and lack of intimacyin their own marital relationship. As long as thechild continues to engage in delinquent acts; theparents are protected from having to focus ontheir marriage. The functional value of the child’ssymptoms is usually beyond the awareness ofall family members.
The notion that symptoms are functionalreflects a view of families as complex interper-sonal systems. The family system is relativelystable and organised according to implicit rulesgoverning the behaviour of all family membersin their inter-relationships with one another. Theroles and the functions of family membersbehaviour are associated through a series ofinterconnected feedback loops that defy simplelinear causal explanation. These behaviourpatterns are repetitive and tend to occur inparticular sequences. We can consider thefollowing example:
Spouse A is driving and spouse B is in a hurryto get to their destination (also conveys thisbefore starting). A accelerates and moves fastwith a jerk, B holds on to the glass and criticisesA, B protests more loudly, A shouts back andthe child C starts to cry. At this point, theargument stops while B attends to C and A slowsdown.
This sequence exemplifies one form of arepetitive dysfunctional family process, where thechild behaves in such a way that attention iswithdrawn from the conflict between the spousesand refocussed onto the child. Thereby, whenwe discuss homeostasis in families the behaviour

Family 153
of the identified patient must be understood asbeing a part of that system. Despite the expressedconcern with the patients’ symptoms on the partof all family members, the family is inherentlymotivated to maintain homeostasis and willthereby resist any effort on the part of thetherapist to modify the symptomatic behaviourof the identified patient. This makes the task ofthe family therapist exceedingly difficult.
Many of the prominent family theorists haveidentified triangles (e.g. mother, father, son) asthe basic unit of family transactions. A thirdperson is brought into diffuse to eliminate tensionbetween the other two. According to Haley(1976), most behaviour problems in childrenare brought about by a cross-generationalalliance between the child and over involvedparent (usually the mother). The third party inthe triangle is the absent parent (usually thefather). It is a safe assumption that symptomaticbehaviour on the part of the child is maintainedby both parents, with the child serving as a bufferbetween the parents and saving them from amore direct relationship.
Family Therapy
If symptoms serve to stabilise the family andmaintain homeostasis, it follows that theindividual cannot be expected to change unlessfundamental changes occur in the family system.This notion that family members will persist thetherapists change attempts, has led to thedevelopment of this strategic therapy calledfamily therapy. The model also implies thatchanges in individuals will effectively come aboutonly when the structure of the family undergoesa change. Therefore, whether the therapist istreating one client or the entire family, the targetof change is the family system.
Family Counselling
Family counselling is widely used in medicalpractice. You come across a family with Down’s
syndrome, and the family wants to have anotherchild. You have to provide genetic counsellingto this family. Similarly, role of family counsellingin patients with AIDS, addictions, child psychia-tric problems, development delays, patientundergoing painful procedures, all require familycounselling. More details of counselling processare given in Chapter 19.
Clinical Application
The importance of understanding family inrelation to medicine is best understood whenyou are working in community medicine andyou make family visits. In all the hospitals, aconcept of family medicine is emerging and hasled to creation of separate departments of familymedicine. The significance of the family in relationto health and illness lies in the fact that almostevery patient or potential patient, is a memberof a family and the interaction within the familyis a two way process. The family may beconsidered from two points of view, one aspossible causative or modifying agent in thepatient’s illness, and on the other hand as moreimmediate social environment within which theillness occurs—including the reaction of the otherfamily members to it. Family provides socialsupport, which has been considered veryimportant in the recovery of the patient. Inpatients where there is no social support, thephysicians have to work out in providing socialsupport through nonvoluntary organisations.Family pathology, or sickness of the family itselfmay lead to codependence; this means that inchronic illness, the spouse may also developsimilar symptoms. In some cases, chronic illnesscan lead to family breakdown, separation ordivorce. This is especially true in patients havingaddictions or chronic mental illness. Theseparation or divorce between parents, due tothe social changes prevalent in the present timeis also giving rise to psychological problems inchildren. In patients with AIDS, the relevance

154 Behavioural Sciences in Medical Practice
of understanding family and providing counsel-ling cannot be understated. The difficultiesextended to the family members in looking afterthe sick patient also often calls for familycounselling, to provide support and help to theentire family in the crisis situation.
Cultural factors may also be important inimmigrant families, where conflict arises betweenthe first and the second generations owing tothe influence of different values. At times, socialmobility causes conflict in children related to thevalues.
SUMMARY
The family is a social system, which cares, protectsand educates its members to establish identity,self-concept and adapt to various stressfulsituations. The family is the most powerful forcefor the promotion of health as well as for theproduction of disturbance in members.
A family has major importance in thedissemination of disease. It transmits genes andculture from one generation to the next. Familyis responsible in transmitting genetic disorders;it also transmits major psychiatric disorders andminor psychological problems through thepsychological environment. Each family is unique
in terms of its environment, some being healthywhich promote positive mental health and somebeing maladaptive, thereby promoting negativemental health.
There are four types of controlling methodsadopted by the families, these are—rigid,flexible, laissez- faire and choatic. The values andnorms are also learned through family.Emotionally disturbed families have double-bindcommunication, in which no clear messages aregiven. Family psychopathology evolves aroundthe concept of homeostasis, which reinforcesillness in some member of the family to maintainits homeostasis. Systems theory has provided theframework to understand the relationships withinthe family and has also provided a model forfamily therapy.
Family counselling is the need of the presentday medicine. Family members want to beinformed about the illness and are being involvedin the management, especially where child is thepatient. To prevent certain diseases which havehigh genetic loading is a prime field for familycounselling.
Understanding of family behaviour is of greatrelevance to medicine, as a result of this familymedicine is emerging as a specialised field ofmedicine.

17Compliance withHealth Care
You are examining patients in endocrinologyOPD. You come across an eighteen years oldfemale, 5.1 feet tall, weighing 84 kg. All herinvestigations have been reported to be normal.The consultant seeing this patient advises dietrestriction and vigorous activity. After onemonth’s follow up, the patient reports no lossof weight. Why this girl has not lost any weight?Is her diagnosis wrong or she has not compliedwith the consultant’s advice. Most likely her causeof not losing weight is noncompliance of theadvice.
One of the significant problems in health careis patient’s noncompliance or lack of adherenceto medical treatment. Interest in adherence tohealth regimen has proliferated in recent yearsand has been directed to medication taking,where reports indicate that 33-80 per cent ofpatients do not follow or err in following theirregimens (Garb et al, 1974). More recent reportssuggest that other health regimens fare as poorly.Dropout rate in weight loss programmes reachas high as 70 per cent within two years anddietary compliance is about 50 per cent (Dunbarand Stunkard, 1997). Patients with postmyo-cardial infarction dropout of exercise pro-grammes. The increasing professional interest inthe area of compliance can probably beaccounted for by an influence of several factors.
Thus, a substantial portion of individuals failto receive maximum benefit from healthregimens. The problem is further compounded,
when one realises that good adherence is neces-sary and that knowledge of the degree of patientadherence is required to monitor treatmentefficacy, safety and side effects. This is not onlycrucial to the evaluation of treatment for theindividual patient, but also to the interpretationof clinical research involving self-administeredregimen.
From a biomedical perspective, noncomp-liance in a patient means that they are ignorant,lazy or willfully neglectful. For example, you mayhave a patient with diabetes who does notcomply with diet restriction. Similarly, in anumber of other medical conditions, complianceis required not only related to drug in-take butalso related to restrictions in diet, activities,smoking, drinking and change in lifestyle. Thehealth care provider may not be aware of theantecedent environmental conditions for apatient’s symptoms, his/her decision to seektreatment and also the failure to comply withtreatment. At times, it may become difficult forthe doctor to decide whether the treatment pre-scribed is not effective or the patient does notshow improvement because of noncompliance.
The role a patient plays in his own therapyhas subtly changed from a largely passive oneto a largely active one. The life-threatening disea-ses have moved from those of infectious diseasesto those of chronic diseases or diseases in whichthe person’s lifestyle is implicated. This hasresulted in the need for a long and continuous

156 Behavioural Sciences in Medical Practice
adherence to medical regimens and changes inpatterns of living. Under these conditions, theperson assumes more responsibility for the healthoutcome because of the very nature of thehealth problem and the long duration of thetherapy. Patients need to continue the therapy,even if long periods of time intervene betweentheir contacts with physicians.
Another reason that patients assume a moreactive role in therapy is because chronic disea-ses have a direct and potent effect on their healthstatus. Recommendations for the maintenanceof health extend beyond those of taking drugs,to those of changing habits such as modifyingsmoking or eating patterns. Since there are alarge number of examples in which healthoutcome is not determined by the doctor’sactions alone, but rather that of the doctor’s andpatient actions jointly, the health provider mightat first feel less responsible for the outcome. Theremay, for example, be some professionalresistance accepting this different kind ofresponsibility, which includes gaining the patient’scooperation. Doctors and their coworkers areassuming greater responsibility to protect healthhence the interest in helping the patients tocomply has increased. When one remembersthat recommendations to nonhospitalised peopleconstitute to be the bulk of the practice ofmedicine, one realises that concern about patientcompliance is unavoidable. It is quite reasonableto believe that future doctors will assume thattheir responsibility encompasses minimising thosefactors such as patient’s educational level andunderstanding those which influence com-pliance.
The problem of compliance focusses on theenvironmental conditions promoting adherenceto a structured treatment programme. Forexample, in case of evaluating adherence toweight reduction programme for obese indi-viduals, the questions to be addressed would
include frequency, quantity and type of foodeaten, stimuli preceding eating, nature ofeating—fast or slow, the consequences of eating.The research is being focussed on changingbehaviour of the patient for long-term adhe-rence of treatment. Behavioural scientist havedeveloped strategies to resolve long-term adhe-rence by understanding patient’s behaviour andusing behavioural strategies to bring change inpatient’s lifestyle.
Most of the doctors feel confident that theycan identify noncompliers; but in reality, it is adifficult task. Several studies have been con-ducted on the degree of accuracy with whichhealth care providers can identify noncompliantpatients—usually with respect to medication.Since the physician’s subjective assessment of aperson’s compliance seems to be inadequate,one begins to consider other ways of measuringcompliance as well as to look more closely atwhat is meant by the term compliance.
The compliance or recommendations forhealth ranges from advice about periodic healthexaminations, to making radical changes in dailyhabits such as abstinence from alcohol. With alittle reflection, one would certainly expectcompliance with some recommendations to behigher than with others, and this proved to betrue in several studies. For example: (1) thegreater the change in the person’s long-standingpersonal habits, the less likely he is to comply;(2) the more complex the drug regimen, theless compliance is obtained; and (3) the longerthe duration of therapy, the lesser is thecompliance.
Types of ComplianceCompliance varies according to the type ofhealth recommendation: (1) making a contactwith a health provider, (2) adhering to a drugregimen, or (3) making lifestyle changes (Fig.17.1).

Compliance with Health Care 157
Contact with Health Provider
Perhaps the most pervasive type of behaviourinvolving compliance, is that in which the patientis asked to either initiates or continue contactwith a health provider. This request involves thesimplest form of compliance. It is a truism thatnothing can be done if the patient does notpresent himself for help. Still the seriousconsequences of such a non compliance is oftenseen when a person does not seek help at allor waits until his disease has crossed beyond thepoint of intervention. There have been manyattempts to find the reasons for such delay.
The factors found to be related to delay inor failure to seek health care are—fear,ignorance, level of education, cultural beliefs,financial status, and convenience of location.Almost half of all missed appointments arerelated to ineffective communication. Differencesin the effectiveness of communication mayaccount for some of the variation in rates ofmissed appointments that have been reported.
To sum up, there is a substantial amount ofevidence that suggests that very simple effortswill increase compliance with all types ofappointments.
Medication Compliance
The patient himself, his support system, his rela-tionship with the clinician, and his experience
with the clinic itself, all contribute to his abilityand willingness to follow a medical regimen. Butperhaps the single most important determinantof compliance is the regimen itself.
It has been found that on an average, thereis about 50 per cent compliance with medicationrecommendations. Compliance to medicationis related to the degree of complexity. There isa poor compliance if the medication regimenis complex and a large number of medicines areto be taken in a single day. It has also beenobserved that if the medication does not haveany benefit, the patients on their own stop takingit.
Medication compliance is an issue in anyhealth problem and has been found in suchwidely varying cases as—prescribed for pregnantwomen with anaemia, to antihypertensivemedication for those with elevated bloodpressure. There is some suggestion that olderpatients have more trouble than younger onesin complying. It has been suggested that it ispossible to increase drug adherence by assistingpatients with the establishment of the requiredroutine. Education of hospitalised patients to taketheir medication when they are dischargedshould be used more extensively.
Lifestyle Changes
The most difficult compliance to achieve is relatedto changing personal habits such as eatingpatterns, exercise, or alcohol intake. Althoughthese types of behaviours are known to relateto health status, patients have proved to berefractory when doctors have tried to changethem. This type of health behaviour changeseems to be particularly resistant to mere advice,which is left to be implemented by the patienton his own. Perhaps, part of the lack of successis that health providers themselves are somewhathesitant to give advice about personal habits.
The physician might well be most effectivein initiating health advice and reinforcing
Fig. 17.1: Types of compliance

158 Behavioural Sciences in Medical Practice
successful health habit change—that his effortscan be strengthened by working with other per-sonnel who see patients more often. This seemsto be the most effective method in helpingpatients with health recommendations, whichinvolve making changes in lifestyle.
Factors Related to Compliance
Studies on the identification of factors thatpredict compliance behaviour have focussed onpsychological characteristics of the person suchas attitudes and perception of illness and healthbehaviour; environmental factors such as familyinstability, living alone, the therapeutic regimenitself and finally the doctor-patient interaction.Davidson (1982) reported that there was norelationship between therapeutic complianceand factors like education, socioeconomic status,family interaction, and distance to the clinic orhospital or the diagnosis. Research examiningattitude and perception of the patient is relatedto health belief system, which the person learnsfrom his sociocultural environment.
There are three general categories of factorsthat have been studied (Gillum and Barsky,1974), which determine relation to thecompliance behaviour of patients: the personnelcharacteristics of patients, the personalcharacteristics of providers and the structuralcharacteristics of the health care setting.
Patient Characteristics
Considerable effort has been expended to asse-mble information about the types of individuals,who are noncompliant. Unfortunately, there arelarge numbers of studies, which taken as a whole,have reported contradictory information aboutthe sociodemographic variables of sex, age, andeconomic status. The most ambitious attemptto synthesise knowledge in this area has beenby Sackett and his colleagues. What emergesfrom this and similar attempts is that it is difficult
to identify noncompliers on the basis of knowingtheir sociodemographic characteristics. Onephysician, who studied noncompliance inconsiderable detail concluded that each personshould be considered a potential noncomplier.Noncompliance should be assumed, especiallywhen no evidence of benefit from therecommendation is seen. This should not beinterpreted as recommending an adversaryrelationship; quite the reverse is necessary.
Despite the lack of an easy method ofidentifying noncompliers, there are certainpersonal characteristics, including attitude,towards therapy and disease, which should alertthe physician that the patient may be at a greaterrisk of noncompliance, for example, those wholive alone. This is consistent with the finding thatnoncompliance increases, depending onwhether the individual is an inpatient, daypatient, or ambulatory patient. In other words,lesser the support the patient has or the morehe is on his own, the greater is the likelihoodof noncompliance.
Persons who understand the therapeuticbenefit of the recommendation and who haveimmediate negative feedback if they fail tocomply are more likely to have bettercompliance.
There are some persons, for example, whodeny their illness and are therefore unable tocomply with the health recommendations, sincedenial and compliance are incompatible. Usually,the denial stems from being unable to deal witha “weakness” or with the fear that accompaniesbeing told of the illness. There are other patientswho, because of a lack of trust, do not acceptthe validity and truth of the illness or theprescribed treatment. These are persons, whofor a variety of reasons, are convinced they arenot ill, and therefore there is no rationale forcompliance with any treatment.
On the other hand, there are those whoaccept the fact that they are ill but are

Compliance with Health Care 159
noncompliant because they are motivated toremain ill. They, for instance, get either attentionor tolerance because of their illness or are givenspecial dispensation from work or otherdemands.
Provider Characteristics
There have not been as many studies to identifypersonal characteristics of the provider relatedto compliance, as there have been to identifypatient’s characteristics. This may, however, bemisleading, for the provider-patient encounteris an interaction in which both persons’characteristic contribute to the process, and toseparate these characteristics is in some waysarbitrary.
There have been a few studies of the relationbetween the quality of the doctor-patientrelationship and patient compliance. Severalstudies have shown acceptance and satisfactionwith practitioners and paramedical assistants,which seems to be related to the ability of theseproviders to establish rapport and continuity ofcontact with the patient as with physicians.
There are other studies that show thatimproved compliance is related to a long-timerelationship with the physician (Charney, 1967)and that private physicians are better able toobtain compliance than clinic physicians. It is notpossible, of course, to study these characteristicswithout considering the patients’ characteristics.Nevertheless, studies do suggest that a goodpatient-physician relationship, which ismaintained over a fairly long time, increases thechances of compliance. It has been found thatthe physician’s attitudes toward treatment andmedication are important in determining thepatient’s compliance behaviour. The physician’sdegree of conviction in the treatment is alsorelated to the patient’s cooperation. If theprescribing physician believes in the efficacy ofthe treatment, he is much more apt to obtainpatient compliance than is his counterpart, who
is unconvinced about the benefits. Seemingly,this conviction is, intentionally or unintentionally,communicated to the patient. Several authorsattribute all noncompliance problems to failurein communication between the provider and thepatient. Those physicians or providers, whospend time establishing the patient’s under-standing of the reason for the required regimen,do get better compliance.
Assessment of Compliance
Compliance can be measured by number ofmethods, for example, interviews, pill count,clinician rating, biochemical indicators and self-report. Since each of these methods has theirown limitations, thus a combination of two ormore forms of assessment should be used.Biochemical procedures provide a directmeasure, whether or not the treatment has beencarried out, but provides no knowledge of thedegree of compliance. The pill count offersinformation on the degree of compliance overtime, but does not offer any information on theproblems encountered or side effects. The self-report can be insufficient due to the memorylapses. Self-monitoring can provide a continuousrecord on compliance, as well as patterns andproblems specific to regimen. It is not suggestedto use physiological outcomes as measure ofcompliance, as there is individual variability inresponse to treatment that allows some patientsto achieve a therapeutic goal with poorcompliance rates.
Clinical Application
Recently some approaches and techniques havebeen developed to facilitate compliance. Theseinclude patient education, accommodation,modification of environmental and social factors,change in therapeutics regimen, and enhance-ment of doctor-patient interaction.1. Education—Patient education can have a
greater impact, if education about the illness

160 Behavioural Sciences in Medical Practice
is provided in an active way, for example,making the patient read the informationhimself through handouts or self-helpbooks.
2. Accommodation—The personality charac-teristics, which interfere with compliance, areunderstood and the treatment is planned outin terms of negotiations. This makes theperson an active participant in the treatment.This type of treatment negotiations, havebeen found to be very useful, especially inde-addiction of drugs and substance abuse.
3. Modification of environmental and socialfactors—The family members and friends canbe included in the treatment and they canbe oriented to reinforce compliantbehaviours. Any interpersonal problems athome interfering with the treatment can alsobe resolved with the family members.
4. Change in therapeutic regimen—Theregimen can be made as simple as possible,and the patient should be involved in theplanning. Compliance can be shaped by: first,giving simple components of the treatmentregiment and reinforcing success, andgradually adding the other components ofthe regimen.
5. Enhancement of doctor-patient relation-ship—Good communication between thedoctor and patient can resolve some of theproblems of noncompliance. By under-standing patient’s expectation, his viewpointand problems encountered in adhering tothe treatment regimen, the doctor and thepatient can work out schedule for treatment.
SUMMARYOne of the significant problems in health careis patient’s noncompliance or lack of adherenceto medical treatment. A substantial portion ofindividuals fails to receive maximum benefit fromhealth regimens. The problem is further
compounded, when one realises that goodadherence is necessary and that knowledge ofthe degree of patient adherence is required tomonitor treatment efficacy, safety and sideeffects.
From a biomedical perspective, noncomp-liance in a patient means that they are ignorant,lazy or willfully neglectful. For example, you mayhave a patient with diabetes who does notcomply with diet restriction. Compliance isrequired not only for the intake of medicationbut also for compliance with restrictions in diet,activity or lifestyle.
The average person in our country has alarger number of contacts with the health caresystem than ever before. He has found thatthere are more and more ways in which suchcontacts can give him relief in times of illnessor even prevent its occurrence. As knowledgehas continued to be accumulated, curativemedicine has become possible for an increasingnumber of diseases; knowledge about thepathogenesis of disease has resulted in theprevention or control of some diseases at an earlystage.
Compliance is of three types: first, makinga contact with health provider; second, adheringto the medication regimen; and third, makinglifestyle changes. There are various factors relatedto compliance, these are primarily related topatient characteristic and characteristic of theprovider.
In the present day medical context, whenmore of psychosocial factors are playing role inthe aetiology of illness, compliance to treatmenthas become one of the important aspects of totalhealth care system. Motivating the patients tocomply specially in disorders, like substanceabuse, AIDS, coronary heart diseases, diabeteshas become important for the physicians.Behavioural therapy techniques are used tointervene with noncompliance patients.

18Assessment inBehavioural Sciences
PART 5: Assessmentand Management
Assessment methods used in behaviour sciencesare very comprehensive and have a variety ofinstruments. Both qualitative and quantitativemethods are used in the assessment. Thesemethods are being employed not only inpsychiatry but in all clinical disciplines, especiallyto understand the role of psychosocial factors,e.g. to rule out depression in patient with lowback pain, or to rule out possibility of secondarygains in the same patient with low back pain.
Assessment refers to the procedures andprocesses employed in collecting informationabout or evidence of human behaviourAssessment, a broader term, refers to the entireprocess involved in collecting information aboutpersons and using it to make importantpredictions and inferences.
Goals of Assessment
The goal of assessment is to identify and under-stand the individual’s symptoms within thecontext of his or her overall level of functioningand environment. This includes determining thenature and severity of any maladaptivebehaviour and understanding the conditions thatmay have caused and/or be maintaining it. Todo this, the clinician must gather, weigh, and
synthesise as much information as possible aboutthe patient, usually within a brief period of timeand often with limited information. Theindividual may manifest a perplexing array ofpsychological problems, and his or her medicaland social history may be unknown. In addi-tion, there may be seemingly unsolvable prob-lems in the individual’s life situation. Equallyimportant to evaluate are the individual’sstrengths and resources, including such personalfactors as motivation for treatment capacity forchange, ability to participate in the treatment,programme, and available support from familyand others. With all this information in hand,the clinician must then arrive at a workingformulation concerning what can be done topromote the individual’s well being. It is anawesome but necessary task.
The assessment provides a basis for makingdecisions concerning the best treatmentprogramme, be it hospitalisation, the use ofmedication or psychotherapy, the modificationof family patterns, or some other approach. Theinitial assessment also provides a baseline forcomparison, later with other measures obtainedduring and following treatment. This is impor-tant but sometimes forgotten aspect of assess-ment. It makes it possible to check on the

162 Behavioural Sciences in Medical Practice
effectiveness of an ongoing treatment pro-gramme, to see if modifications may be needed;it also allows for comparison of the relativeeffectiveness among different therapeutic andpreventive approaches. This is important notonly in treating the individual, but also inconducting the research that can advance ourunderstanding of the disorders themselves, aswell as the development of new and moreeffective assessment and treatment techniques.All of which ultimately, will enhance the prog-nosis for individuals suffering from psychologicaldisorders. Furthermore, the importance ofassessment has increased dramatically as thedemand for accountability in therapy has grown.Assessment is not necessarily a onetime venture,it is an ongoing process.
The foremost goal of assessment is to identifythe problem. Is it a situational problem,produced by an environmental stressor, or is ita more pervasive and long-term disorder? Howis the individual dealing with the problem?
For many clinical purposes, a formal dia-gnostic classification is much less important thanhaving a basic understanding of the individual’shistory, intellectual functioning, personalitycharacteristics, and environmental pressures andresources.
It is also important to understand the personand his problems in the social context in whichthe individual operates. What kinds ofenvironmental demands are typically placed onthe individual, and what supports or specialstressors exist in the individual’s life situation?
Assessment helps to understand why theperson is behaving in maladaptive ways. Thediverse and often conflicting bits of informationabout the individual’s personality traits,behaviour patterns, environmental demands,must then be integrated into a consistent andmeaningful picture. The formulation shouldallow the clinician to develop hypotheses aboutthe patient’s future behaviour as well, e.g. whatis the likelihood of improvement or deterioration
if the individual’s problems are left untreated?Which behaviours should be the focus of changeand what treatment methods are most likely tobe successful? How much change mightreasonably be expected from a particular typeof treatment?
Sources of Assessment
Since a wide range of factors can play importantroles in causing and maintaining maladaptivebehaviour, assessment may involve the variousassessment procedures like physical, psycho-logical, and environmental assessment pro-cedures.
Physical Evaluation
In some situations or with certain psychologicalproblems, a medical examination is necessaryto rule out physical abnormalities or to deter-mine the extent to which physical problems areinvolved. The medical evaluation may includeboth general physical and special neurologicalexaminations. A common example of this isrecurrent abdominal pain, headache, or panicattacks.
Psychosocial Assessment
Psychosocial assessment attempts to provide arealistic picture of the individual in interactionwith the environment. This picture includesrelevant information concerning the individual’spersonality makeup and present level offunctioning, as well as information about thestressors and resources in his or her life situation.For example, early in the process, clinicians mayact like puzzle solvers, absorbing as muchinformation about the client as possible—presentfeelings, attitudes, memories, demographic facts,and so on—and trying to fit the pieces togetherinto a meaningful pattern. They typicallyformulate hypotheses and discard or confirmthem as they proceed. Starting usually with a

Assessment in Behavioural Sciences 163
global technique, such as the clinical interview,clinicians may later select more specificassessment tasks or tests. The following are someof the psychosocial procedures that may beused.
Assessment Interviews
The assessment interview usually involves a face-to-face conversation conducted in such a waythat the clinician obtains information aboutvarious aspects of the patient’s situation,behaviour, and personality makeup. The inter-view may vary from a simple set of questionsto a more formal format.
In order to minimise sources of error, anassessment interview is often carefully structuredin terms of goals, content to be explored, andthe type of relationship the interviewer attemptsto establish with the subject. Here, the use ofrating scales may help focus and score theinterview data. For example, the subject maybe rated on a three-point scale with respect toself-esteem, anxiety, and various othercharacteristics. Such a structured interview isparticularly effective in giving an overallimpression of the subject and his or her lifesituation and in revealing specific problems orcrises—such as marital difficulties, drugdependence, or suicidal fantasies that mayrequire immediate therapeutic intervention.
In recent years, several researchers haveattempted to improve further the reliability ofthe clinical interview by eliminating the humanfactor and using computers instead to actuallyconduct the interview. Highly sophisticatedcomputer programmes have been written to“tailor-make” a diagnostic interview for thepatient. One of the examples is ComputerisedDiagnostic Interview for Children that can con-duct a standard psychiatric interview. Severalmore specific clinical assessment tasks have beenadopted for computer administration.
Self-Assessment
A type of assessment that is related to theinterview is the self-report. This approachrecognises that individuals are an excellentsource of information about themselves.Assuming that the right questions are asked andthat people are willing to disclose informationabout themselves, the results can be quitevaluable. One of the most efficient instrumentsfor obtaining specific information about anindividual’s problem area is the self-reportschedule or problem checklist. Such checklistsmay include items that measure fears, problems,moods, and conditions that may be operatingas reinforcers in the person’s life. Thus they canprovide useful information for structuring abehavioural treatment plan. Quality of life is alsoassessed on self-reports.
Clinical Observation
Direct observation of the individual’s charac-teristic behaviour has always been an importantmethod of psychosocial assessment. The mainpurpose of direct observation is to find out moreabout the person’s psychological makeup andlevel of functioning; though such observationswould ideally occur within the individual’s naturalenvironment, or they are typically confined tohospital settings. For example, a brief descriptionis usually made of the patient’s behaviour at thetime of admission in the hospital and moredetailed observations are made periodically inthe ward. These descriptions include relevant in-formation about the subject’s personal hygiene,emotional behaviour, delusions or hallucinations,anxiety, sexual behaviour, aggressive or suicidaltendencies, and so on.
Psychological Tests
Interviews and behavioural observations aredirect attempts to determine the individual’s

164 Behavioural Sciences in Medical Practice
beliefs, attitudes, and problems. Psychologicaltests, on the other hand, are a more indirectmeans of assessing psychological characteristics.A psychological test is essentially an objective andstandardised measure of a sample of behaviour.Psychological tests are like tests in any otherscience, as observations are made on a smallbut carefully chosen sample of an individual’sbehaviour. In this respect, the psychologistproceeds in much the same way as thebiochemist that tests a patient’s blood. Thediagnostic or predictive value of psychologicaltests depends on the degree to which it servesas an indicator of a relatively broad andsignificant area of behaviour. The psychologicaltest is a standardised measure that impliesuniformity of procedure in administering andscoring the test. The testing conditions are alsocontrolled for scientific observation. The tests areevaluated for their reliability and validity. Manytimes, a battery of psychological tests is admi-nistered to assess wide range of behaviours.
Objectives of Psychological Tests
Psychological testing is done primarily with fourobjectives.
Screening of certain traits or behaviour: Certainpersonality traits like psychopathy, extroversion,neuroticism, poor coping resourses, emotionallylabile individuals, are more prone to acquirebehavioural or emotional disorders. Psycho-logical tests are used for screening individualswho are at high risk to develop these disorders.The screening is often required when a researchis to be carried out or for early identification of‘at risk’ population.
To assess psychopathology and to help inmaking diagnosis: Patients often have comorbidconditions such as schizophrenia, depression,anxiety, personality disorder or organic brainsyndrome. The clinical presentation of thesecomorbid conditions often are not presented in
the clear cut manner and thus cause problemsin making the diagnosis. In these situationspsychological test finding can help by providingevidence for psychopathology, thought disorder,signs of organicity or personality profile.
To elicit factors that are causative as well asmaintaining maladaptive behaviours: There is acomplex interaction of psychosocial and biolo-gical factors in the aetiology of many psychiatricdisorders as in any other medical disorder. Atpresent there is shift of focus on understandingand treating the underlying causes, and factorsthat could maintain the maladaptive behaviourlike addiction. Often the underlying aetiologi-cal factors are psychosocial factors operating atan individual level or in the family dynamics,or in the job situation. These factors are oftennot reported by the patient, as they do notrecognise an association between psychosocialproblems and addiction. Moreover, the conflictsmay not be operating at the conscious level.Psychological tests help in digging out thisinformation from both conscious as well as sub-conscious level systematically. After determiningand assessing the impact of these factors on theaddictive behaviour of the patient, they can bethe foundation for planning treatment. If theunderlying factors are treated then the relapserate can also be reduced considerably.
In planning of rehabilitation assessment ofcognitive ability and aptitude: Planning ofrehabilitation for patients with psychiatric illnessor neurological disorders, handicaps, head injurypatients, is as important as the treatment. Ifrehabilitation plans are not made and executedthen chances of relapse or developing psychiatricproblems are higher. At present in most of themedical centres more attention is being focussedin helping patients to rehabilitate. This requiresan understanding of patient’s level of cognitivefunctioning, i.e. attention, memory, intelligence,aptitude, interest and adaptability. The psycho-logical testing can provide valuable information

Assessment in Behavioural Sciences 165
on all of these aspects, which can be used inplanning the rehabilitation.
Types of Psychological Assessment
Psychological assessment generally is classifiedas neuropsychological tests, personality tests andtests for assessment of psychopathology. The testsare selected according to the aim of assessment,e.g. diagnosis, rehabilitation or research.
In a clinical setting these tests are given onan individual basis. Observation of behaviourduring testing is as important as the test perfor-mance, as the nonverbal clues indicate usefulinformation like motivation, persistence,concentration and manipulativeness.
Neuropsychological Assessment: Neuro-psychological assessment comprises of cognitivefunctions, namely, attention, concentration,perception, memory and intelligence. Some ofthe examples of these tests are as follows:
Attention and concentration: All cognitivefunctions are dependent on attention span andability to sustain attention. Clinically attentioncan be assessed through observation duringhistory taking and in interview sessions. Formallyit can be assessed by asking the patient to repeatdigits forward and backward. Forward digits arestarted from 3 and continued till 8-9 digits. Thetest is stopped after two consecutive failures.Backward digits are given from 2 to 8. The digitsshould not be presented either very fast or veryslow. The ideal rate of presentation should beone digit per second. These can also be assessedon the subtest of Wechsler’s Adult IntelligenceScale namely Digit Span and Digit Symbol test.
The other methods used for formal andobjective tests include letter cancellation, colourcancellation, counting 20 to 1 backwards andserial subtraction 40–3.
Perception: Bender Visual Motor Gestalt test(Fig. 18.1) is a simple and short method of
assessing organicity and visuomotor co-ordination, useful for both children and adults.This test consists of simple 9 designs printedagainst a white background on a separate card,which are to be copied by the patient on unlinedpaper. Objective scoring system is available.Evaluation of the protocol depends both in theform of the reproduced figures and on theirrelationship to each other. Probably the mostfrequent clinical use for the test with adults isas a screening device for detecting signs oforganicity.
Memory assessment: Memory tests help to assessdegree of impairment in memory functions. Theyalso provide a baseline on which treatmentprogramme can be planned specifically toenhance memory. An ideal test of memoryshould estimate deficits in all types of memoryprocesses and should suggest anatomicallocalisation as well as the aetiological nature ofthe pathology. There are no biological tests thatindicate memory deficits. The currently availableneuropsychological tests are also far from meetingthis ideal goal.
Fig. 18.1: Bender visual-motor Gestalt test

166 Behavioural Sciences in Medical Practice
Most of the tests used at present may begrouped under the following categories:1. Single tests of memory
a. Verbal tests.b. Nonverbal tests.
2. Test batteries for memory.3. Neuropsychological test batteries including
tests for memory.4. Questionnaires to assess memory.5. Clinical examinations of memory.6. Specific rating scales and inventories.
Digit span tests: The Wechsler’s Adult IntelligenceScale includes a digit span subtest in which anincreasing number of digits are presented forimmediate verbal recall. The digits are recalledboth in a forward and a reverse order. The rateof presentation for all digits is 1/sec.
In the Number Span technique, the patientis given increasingly longer number of sequences.However, each succeeding sequence differs fromthe one before it in its last number, e.g. 6-2,6-2-4, 6-2-4-8, and so forth. It is reported thatyoung adults could recall an average of 9.06numbers, whereas older persons (> 65 years)could retain only 5.87 numbers.
Letter span tests: These tests are similar to thedigit span tests except that letters are substitutedfor digits. The norms for letter span are 6.7 lettersfor people in their 20s and 6.5 letters for peoplein their 50s.
Memory for sentences: An average adult cancorrectly recall sentences of 24 or 25 syllablesin length. The Stanford-Binet Scales include asentence memory test at several age levels,beginning with 12 syllable sentences for 4-year-old, 16 to 19-syllable sentences for 11-year-old,and 20-syllable sentences for 13-year-old. Thesyntax and vocabulary become more complexat higher age levels.
Memory for paragraph and stories: It is generallynot possible to memorise a paragraph or a storyword by word. However, most people can recallthe ideas presented in the paragraph using someof their own words and some from the actual
presentations, omissions, additions, elaborations,and shifts in the story’s sequence. Severalmethods of scoring have been suggested.Rapaport et al (1968) developed a system inwhich they scored all segments of the story ascorrect in which “the change does not alter thegeneral meaning of the story or its details”. Theyalso included a four-point “distortion score” thatreflects the extent of minor alterations as accurate“meaningful memories”.
Several of the paragraphs and stories thathave been standardised for testing immediateand delayed recall include stories in the Stanford-Binet Test, the Wechsler Memory Scale, theBabcock Story Recall Test, and the Cowboy story.
Test batteries for memory Wechsler memory scaleis a rapid, simple and practical memoryexamination. This test is used all over the world.lt consists of the following seven subtests.
1. Personal and current information—The sub-ject is asked for age, date of birth, and identi-fication of current and recent public officials.
2. Orientation is assessed by questions aboutthe time and place.
3. Mental control—This subcategory is designedto test automatism such as repeating thealphabet and simple conceptual tracking asin counting by fours from 1 to 53.
4. Logical memory—This subtest includesimmediate recall of verbal ideas from twoparagraphs. The examiner first reads the twoparagraphs but stops after each paragraphto get the subject’s immediate recall.Paragraph A contains 24 memory units orideas and paragraph B contains 33. Thesubject is given one point of credit for eachcorrect idea recalled. The total score is theaverage recalled and extends upto 23.
5. Digit span—This subtest differs from the DigitSpan Subtest of the Wechsler’s AdultIntelligence Scale by omitting the three-digittrial of digit forward and the two-digit trialof digit backward and not giving score creditsfor performance of nine or eight backward.

Assessment in Behavioural Sciences 167
6. Visual reproduction—Each of the three cardswith a printed design is shown for 5 sec.following each exposure, the patient drawswhat he remembers of the design. This is animmediate recall test but some examiners alsorecommend a delayed trial.
7. Associate learning test—This subtest consistsof ten words, of which six are called “easy”as they have common associations such as“baby-cries” and the other four pairs areuncommon or “hard” associations such as“cabbage-pen”. The list of the word pairs isread three times. The subject tries to recallas many pair associates as he can rememberafter each reading. The total score is on halfthe sum of all correct associations to the easypairs plus the sum of all correct associationsto the hard pairs. The highest possible scoreis 21.
PGI memory scale: This scale has beenstandardised by Pershad for Indian population.It is used on both literate and illiterate adultsand older persons. It has ten subtests, namelyremote memory, recent memory, mentalbalance, attention and concentration, delayedrecall, immediate recall, verbal retention forsimilar pairs, verbal retention for dissimilar pairs,visual retention, and recognition. Figure 18.2is the stimulus card for recognition test. The testeehas to identify these objects from the larger objecttable (Fig. 18.3). This test has objective scoring,and norms according to age and sex have beendeveloped.
Memory questionnaires: For assessment ofworking memory simple questionnaires can alsobe used. The content of these questionnaires isrelated to historical facts, salient life events, andmemory of specific situations on the basis ofrepeated experience with every day memorytasks. Generally immediate recent and remotememory is assessed. These terms also arereferred to as short-term and long-term memory.
Clinical examination of memory: Most neuro-psychiatric examinations includes a mental statusexamination to determine the patient’s neuro-logical and psychiatric status. Memory assessmentis an important part of a comprehensive mentalstatus examination. However, in order to reachsome conclusion about memory deficits, it isnecessary to assess other mental functionssuch as the patient’s level of awareness,verbal functions, attention and concentration,emotional status, and intellectual potential. Adeficit in any one of these areas is likely to affectfunctions in other areas as well as memory. Infact, most mental functions overlap with eachother and a separation of such functions isartificial.
Brief cognitive rating scale (BCRS) (Reisberget al, 1983): Patients with Alzheimer’s diseaseshow a fairly uniform decline on BCRS, whichutilises seven, rating categories for each of thefive axis. Several other diagnostic categories suchas mania and acute anxiety will cause somedeficits on the concentration axis. The five axesinclude the following: concentration andcalculating ability, recent memory, past memory,orientation, functioning and self-care. Items ineach axis are scored from information obtainedduring a clinical interview with the patient in thepresence of spouse or the caretaker.
Global deterioration scale (GDS) (Reisberg et al,1982): The Global Deterioration Scale is a clini-cal scale that describes clinical characteristics ofAlzheimer’s disease in seven stages thatcorrespond to seven clinical phases as follows:
GDS stages Clinical phases
1. No cognitive decline Normal2. Very mild cognitive decline Forgetfulness3. Mild cognitive decline Early confusion4. Moderate cognitive decline Late confusion5. Moderately severe decline Early dementia6. Severe cognitive decline Middle dementia7. Very severe cognitive decline Late dementia

168 Behavioural Sciences in Medical Practice
Intelligence: Assessment of intelligence is the mostcommon referral received by the psychologist.Intelligence tests are divided into verbal tests andperformance tests.1. Wechsler’s adult intelligence scale (WAIS)—
is the most widely used intelligence scale. Itconsists of verbal performance scales of whichare further subdivided into subscales. Thedetails of these subscales are as following:
Verbal Performance
Information Block design
Comprehension Picture completion
Arithmetic Picture arrangement
Similarities Object assembly
Digit Span Digit symbol
Vocabulary
Figs 18.2 and 18.3: Recognition tests in PGI memory scale

Assessment in Behavioural Sciences 169
Indian Adaptation of both of these verbal(Pershad and Verma) and performance(Ramalingaswamy) scales are available. Figure18.4 is an example of picture completion test,and Figure 18.5 is example of object assemblytest.2. Bhatia’s battery of performance test of
intelligence—The test was devised byDr CM Bhatia in India. This test measuresperformance intelligence. The test consists offive subtests that are loaded with the generalfactor (G) and a specific factor (S). Theseare:a. Kohs block design test consisting of 10
designs. The time limit for the first 5designs is 2 minutes and for the next 5,it is 3 minutes. The test is the measureof perceptual motor coordination, mentalcoordination and ability for analysis andsynthesis.
b. Alexander’s Passalong test, which consistsof 8 designs. The time limit for the firstfour designs is 2 minutes and for the nextfour is 3 minutes. It provides with the
measure of spacial, perceptual and motorcoordination.
c. Pattern drawing test consists of 8 itemsstarting from a simple square (Fig. 18.6).The subject should draw each pattern without lifting the pencil and without re-tracing. It measures motor coordination,perceptual motor ability, imagery andspacial component.
d. Immediate memory subtest has 2subparts, in part 1 the subject is to recallthe digits as provided to him whereas inthe second the subject is to recall thembackwards.
e. Picture construction test consists of 5items. lt measures the ability to apprehendrelations, mental imagery and concep-tualise part of the whole.
3. Standard progressive matrices (SPM)—thistest was developed by Raven and has threeforms. Besides standard progressive matrices(Fig. 18.7), the other two are Colouredprogressive matrices and advance matrices.SPM has five sets of matrices, with 12patterns in each set. The age range on whichthe test can be administered is ≥ 12 years.This test is considered a culturally fair test,as familiarity with any specific language is notrequired. This has an objective scoring and
Fig. 18.4: Picture completion test item Fig. 18.5: Object assembly test

170 Behavioural Sciences in Medical Practice
intelligence is expressed in terms of percentileranks. The task is to choose the missing insertfrom the given alternatives. The easier itemsrequire accuracy of discrimination, the moredifficult items involve analogies, permutationsand alternations of pattern and other logicalrelations.
Personality Tests
Clinical assessment of personality and psycho-pathology is a complex task, and it is one of themost critical aspects of working with emotionallydisturbed individuals. Personality testing is donefor many reasons. Its aim is to assess what theperson is usually like in thoughts, feelings andbehaviour patterns. Personality tests tapindividual differences of reacting to certainsituations.
The thoroughness and accuracy of assess-ment can determine the extent to which anindividual’s problems are understood and howwell his or her needs are met through therapy.In recent years, objective assessment has grownmore popular and important due to its variedapplications and advantages, e.g. quantificationin improvement, research, consumer protection,etc.
Personality test most often refers to measuresof emotional states, personality type and traits,e.g. introversion-extroversion, interpersonalrelations, interests, motivation and attitudes.Personality tests are in form of: (a) rating scales,(b) questionnaires, (c) semiprojective tests, and
(d) projective tests. All these tests have their ownadvantages as well as disadvantages. Generallya test is selected according to the aim of theassessment. Some of the commonly usedpersonality tests are as following:
Rating Scales
To measure psychopathology objectively ratingscales can be used. Rating scales enable theobserver to indicate not only the presence orabsence of a trait or behaviour, but also itsprominence. The rating scales are generally oftwo types—self-rating scales and observer ratingscales. Beck’s depression rating scale andHamilton rating scales are commonly used tomeasure depression. Anxiety can be measuredon state and trait anxiety scale and hamiltonanxiety scale.
Brief psychiatric rating scale (BPRS): This is themost widely used rating scale for recordingobservations in clinical practice and in psychia-tric research. The BPRS provides a structuredand quantifiable format for rating clinical symp-toms such as somatic concern, anxiety, emotional
Fig. 18.6: Pattern drawing test
Fig. 18.7: Standard progressive matrices

Assessment in Behavioural Sciences 171
withdrawal, guilt feelings, hostility, suspiciousness,and unusual thought patterns. It contains 18scales that are scored from ratings made by theclinician following an interview with the patient.The distinct patterns of behaviour reflected inthe BPRS rating, enable clinicians to make astandardised comparison of their patients’symptoms with the behaviour of other psychiatricpatients. The BPRS has been found to be anextremely useful instrument in clinical research,especially for the purpose of assigning patientsto treatment groups on the basis of similarity insymptoms.
Questionnaires
1. The Minnesota Multiphasic Personality Inven-tory (MMPI)—is certainly among the mostwidely used psychodiagnostic instruments.The test consists of 550 unique items whosecontent ranges from psychiatric symptomsto political and social attitudes. As such,many researchers have felt that the MMPIcan be a particularly useful diagnostic measurein instances where there is a denial ofproblems. The ten basic clinical scales ofMMPI include—HS: Hypochondriasis, D:Depression, HY: Hysteria, Pd. Psychopathicdeviate, Mf. Masculinity-femininity,pa: Paranoia, Pt. Psychasthenia, Sc:Schizophrenia, Ma: Hypomania, Si. SocialIntroversion scale.
2. Eysenck’s Personality Questionnaire—Compared to MMPI, Eysenck’s PersonalityQuestionnaire measures only three dimen-sions of personality namely, introversion-extroversion, neuroticism, psychoticism andlie score. This questionnaire consists of 86items and has been commonly used inresearch studies in India.
Semiprojective TestSentence Completion Test (SCT): Responses onthis test are often most helpful in establishinglevel of confidence regarding predictions of overt
behaviour. The SCT is designed to tap thepatient’s, conscious associations to areas like self-relationship with father, mother, opposite sexand superiors. It is composed of series ofsentence stems, such as, “I like...” “SometimesI wish....:” which patients are asked to completein their own words. The SCT usually elicitsinformation that the patient is quite willing togive, the level of inference is usually less thanin the Rorschach Test or TAT interpretations.
Projective tests: These test are based on theprojective hypnothesis derived from Freud’spsychoanalytic theory. The basic idea is that thetest taker responds to a relatively unstructuredstimuli and much of meaning to the responsescomes from within the person. Thereby,revealing the hidden aspects of the personality.It is a prolonged, intensive and extensiveassessment of that individual’s personality. It isfrom these responses that deductions are madeabout the personality dynamics includingunderlying conflicts and ego defenses.a. The Rorschach inkblot technique was
developed by Herman Rorschach (1921 /1941). He produced a set of 10 inkblots.The blots, 5 are black and white (Fig. 18.8),2 grey and red and 3 multicoloured andappear on separate cards. Subjects arepresented with one card at a time and askedquestion as ‘what might this be?’ or ‘whatdoes this remind you of?’ After writing downthe first response the tester goes back througheach response asking for more details. Thefirst phase of the test is called the free-association phase, and the second is calledthe inquiry. Scoring combines objective andsubjective procedures looking into the areaof the stimulus, and other properties of theblot as form, content, etc.
b. Thematic apperception test Another pro-jective approach was taken by ChristinaMorgan and Henry Murray (1938) indeveloping TAT. It is based on Murray’stheory of needs, which come-up in the storiesgiven by the patient.

172 Behavioural Sciences in Medical Practice
The Indian adaptation of this test is available.A set of 10 cards is selected (Fig. 18.9). To guidestory production, tester instructs while giving apicture, that based on the picture a story hasto be made by incorporating who all are in thepicture, what had happened before, what is goingto happen and what are the people involvedthinking and feeling. Trained psychologists pickup themes coming out from each story andthereby make personality inferences.
Assessment of Alcoholism andSubstance Abuse
CAGE questionnaire: The CAGE questionnairehas become one of the most widely usedscreening devices for alcoholism. It derives itsname as an acronym, for the following fourquestions that are asked of patients:1. Have you ever felt you ought to CUT DOWN
on your drinking?2. Have people ANNOYED you by criticising
your drinking?3. Have you ever felt bad or GUILTY about
your drinking?4. Have you ever had a drink first thing in the
morning to steady your nerves or get rid ofa hangover (EYE OPENER)?
Michigan Alcoholism Screening Test (MAST):The Michigan alcoholism screening test, or MAST(Selzer 1971), is a widely used 25-items, true/false questionnaire that contains questions about
alcohol consumption and consequences ofalcohol use. The test can be administered eitheras a self-report questionnaire or as a structuredinterview. The items are differentially weighted,resulting in a summary score that ranges from0 to 50. Although different cut-off scores foridentifying alcoholism have been recom-mended, these scores generally range between5 (the original cut-off) and 7, with higher scoresreflecting greater impairment and a higherlikelihood of significant alcoholism.
Drug Abuse Screening Test ( DAST): The drugabuse screening test, or DAST (Skinner 1982),is a 28-item, true/false self-administeredquestionnaire that contains questions about theextent and consequences of substance use. Theitems were selected to parallel items from theMAST. Unlike the standard scoring of the MAST,each DAST item is equally weighted so thatsummary scores ranges from 0 to 28. Skinner(1982) emphasised that the DAST score is bestconceptualised as a quantitative index ofsubstance abuse problems.
Alcohol Dependence Scale (ADS): The ADS(Skinner and Horn, 1984; Skinner and Allen,1982) was designed to provide a brief measureof the extent to which alcohol use has progressedfrom psychological involvement to the point of
Fig. 18.8: Rorschach inkblot test
Fig. 18.9: TAT stimulus card

Assessment in Behavioural Sciences 173
impaired control over drinking. The scale ispatterned after the concept of the alcoholdependence syndrome described in a WorldHealth Organisation (WHO) Task Force Report,which portrays alcohol dependence as existingin degrees rather than as an all-or-nonephenomenon.
The ADS consists of 25 multiple choice items,pertaining directly to alcohol use and itsconsequences; scores on the scale range between0 and 47.
Assessment Motivation:Readiness to Change
Outcome of any intervention is primarilydependent on motivation of the patient and hiswillingness to change. Often it is difficult to obtainthe correct information about the patient’s,motivation on direct interview due to responsebias and manipulative behaviour of the patient.Indirect assessment of motivation to seektreatment and to bring positive change inbehaviour can be assessed through projectivetests like Thematic Aperception test and SentenceCompletion Tests.
The use of Psychological Tests inPersonnel Screening
Many people who experience personal problemsor extreme psychological distress are not ableto function well enough in their job. In someorganisations, where the job demands are high,the employers get the psychological screeningdone through experts handing psychologicaltests. The high stress producing jobs like armypersonnel, police officers and firefighters, airtraffic controllers, and nuclear power plantworkers, require a consistently higher level ofpsychological performance or greater emotionalstability than others and allow for less personalvariations in the performance of the job.Emotional problems in some employees can beextremely dangerous to the employees and to
society as a whole. For example, an individualwho holds a key position in a nuclear powerplant control room and who is experiencingsymptoms of severe depression can have his orher ability to function significantly impaired,possibly resulting in a failure to recognise criticalproblems. In India, various organisations havepsychological screening as a regular feature. Forexample, members going to Antarctica for win-ter time for sixteen months are also psycho-logically examined.
Psychological Assessment of Children
Childhood disturbances are rarely as clear-cutas adult psychiatric disorders, and there are oftentoo many explanations for child’s problembehaviours in current family interactions, or inchild’s school experiences. Modern day psyc-hological assessment is likely to contribute to builda plan of management. There may be a needfor assessing the cognitive functioning andacademic achievements. It may be important tostudy the personality characteristics and the waythe child is perceived by others. Or it may bevaluable to get a family account of presentsymptoms and the problem within. Keeping theabove in view we may use one or a combinationof tests depending on the problem as mentionedbelow.
Intellectual Assessment: In infant’s develop-mental schedules are used to assess intelligence.Adaptive behaviour is considered very importantin young children.
Vineland Social Maturity Scale: This test wasdeveloped to assess the individual’s develop-mental level. It is most often used on mentallyretarded children, extending within an age rangefrom birth to 25 years. The test gives a patternanalysis on eight different areas, such as self-help in eating, dressing, socialisation, etc. Thistest is also useful in screening and in assessmentfor uncooperative children. This scale has beenstandardised for our population.

174 Behavioural Sciences in Medical Practice
Wechsler Intelligence Scale for Children-R(WISC-R): This test is similar in its format toWIAS, and its Indian standardised version isknown as Malin’s intelligence scale for Indianschool children. The subtests are classified intoverbal and performance scales yielding verbal,performance and full scale IQs. There is anothertest for children in the age range of two andhalf years to six years, Wechsler Preschool andPrimary Scale of Intelligence (WPPSI).
Coloured Progressive Matrices (CPM): This testis used for younger children within an age rangeof 5½ to 11½ years. It is a nonverbal test withpercentile norms by half years and supplemen-tary norms for mentally retarded children. It isa culture fair test with simple, easy to compre-hend instructions. It consists of 36 items dividedover 3 subtests reflecting on abstract andreasoning abilities.
Assessment of Specific Learning Disability (SLD):A battery of tests have been developed atNIMHANS, to assess children having specificlearning disability. This consists of the followingsubtests:1. Test of general abilities2. Attention3. Perceptual motor abilities4. Visual discrimination5. Auditory discrimination6. Memory7. Language skills8. Arithmetic skills.
Personality Tests
Projective tests are commonly used with child-ren to assess their needs, conflicts and generalpersonality. Some of the commonly used testsare:
Children, apperception test (CAT): This test isdesigned for children in the age range of 3 to10 years. The CAT cards have pictures ofanimals, more like in human situations relating
to problems of feeding, sibling rivalry, parent-child relations, aggression, toilet-training andother childhood experiences (Fig. 18.10). TheIndian version of CAT is also available. CATsupplementary cards depict different situationslike classroom, interaction in the playground,and reactions to illness.
Fig. 18.10: CAT card
Ravens Controlled Projection Test (RCPT): Thisprojective test can be administered in the agerange of 6½ and 12½ years. The child is askedto draw whatever he wishes to and constructa story for which a set of questions are askedby the examiner. The child’s concerns over lies,worries, dreams, friendships, etc. are elicited,which provides a better understanding of thechild.
Draw-A-person Test: This test (Good enough)assesses both intelligence and the personalitycharacteristics. The child is given two sheets ofpaper, and asked to draw a child followed bya figure of opposite sex to the one drawn. Aset inquiry is carried out by putting up questionson ambition, family, friends, attitude toward sexand marriage, etc. bringing out hidden meaningsfollowed by psychoanalytic interpretation.
House-Tree-Person Test: This test is used forchildren of 5 years age and older. The child isrequired to draw a house, a tree and a person
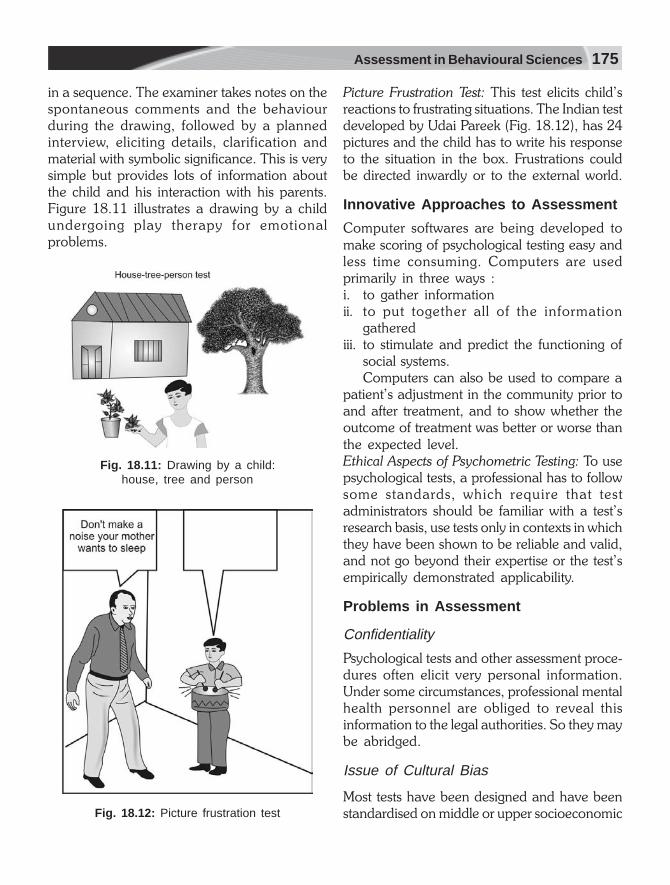
Assessment in Behavioural Sciences 175
in a sequence. The examiner takes notes on thespontaneous comments and the behaviourduring the drawing, followed by a plannedinterview, eliciting details, clarification andmaterial with symbolic significance. This is verysimple but provides lots of information aboutthe child and his interaction with his parents.Figure 18.11 illustrates a drawing by a childundergoing play therapy for emotionalproblems.
Fig. 18.11: Drawing by a child:house, tree and person
Fig. 18.12: Picture frustration test
Picture Frustration Test: This test elicits child’sreactions to frustrating situations. The Indian testdeveloped by Udai Pareek (Fig. 18.12), has 24pictures and the child has to write his responseto the situation in the box. Frustrations couldbe directed inwardly or to the external world.
Innovative Approaches to Assessment
Computer softwares are being developed tomake scoring of psychological testing easy andless time consuming. Computers are usedprimarily in three ways :i. to gather informationii. to put together all of the information
gatherediii. to stimulate and predict the functioning of
social systems.Computers can also be used to compare a
patient’s adjustment in the community prior toand after treatment, and to show whether theoutcome of treatment was better or worse thanthe expected level.Ethical Aspects of Psychometric Testing: To usepsychological tests, a professional has to followsome standards, which require that testadministrators should be familiar with a test’sresearch basis, use tests only in contexts in whichthey have been shown to be reliable and valid,and not go beyond their expertise or the test’sempirically demonstrated applicability.
Problems in Assessment
Confidentiality
Psychological tests and other assessment proce-dures often elicit very personal information.Under some circumstances, professional mentalhealth personnel are obliged to reveal thisinformation to the legal authorities. So they maybe abridged.
Issue of Cultural Bias
Most tests have been designed and have beenstandardised on middle or upper socioeconomic

176 Behavioural Sciences in Medical Practice
groups. Persons from other backgrounds mightbe handicapped in taking such tests and theirscores would not be a fair measure of theirpotential. A great deal of effort has gone intoattempts to develop tests of intelligence and otherabilities that are “culture fair”.
Criticism of Psychological Test Theory: An evenmore basic challenge has stemmed from thequestioning of the assumption that maladjustivebehaviour can best be understood by lookingwithin the individual, at his traits and charac-teristics. The development of tests to assess thesecontinuing inner characteristics was a logicalextension of this concept. However, much ofthe behaviour observed does not fit anywherein the established classification scheme, and theresult is a further disenchantment with classi-fication and labelling in general.
What can be done is to improve the existingprocedures of psychological testing and erectsafeguards to prevent the misuse of suchassessment data.
SUMMARY
As assessment is the primary step in any treat-ment, thus there have been attempts to refineassessment instruments. The technologies thathave been developed in the course of studiesinclude structured interviews, observationalrating scales, and self-report inventories. Thesemethods have a place in daily clinical practice.
The large repertoire of instruments givesclinicians greater flexibility. They can select theparticular method or instrument that suits theirparticular assessment needs. However, such alarge quantity of tests can only leave the naiveclinician feeling overwhelmed and uncertainabout what should be used in any given clinicalsituation. An introduction to the generalprinciples of how to use research instrumentsin clinical settings is necessary, along with some
examples of how they may be used, and ahistorical review of the changes in psychiatry thathave permitted this development.
Psychological tests are standardised measuresof behaviour. The most common psychologicaltests are those, which assess intelligence orpersonality. Intelligence is commonly assessedon Wechsler Adult Intelligence scale.
Rating scales, questionnaires and protectivetests, such as Rorschach Inkblot test, and TAT,can assess personality. There are differentpsychological tests for children.
Methods of personality assessment areessentially similar to those used previously like:Interview, Rating Scales, Questionnaires andProtective tests. Of late Standardised InterviewSchedules are being used more often. There hasbeen tremendous growth in rating scales espe-cially for measurement of psychopathology.Similarly, as newer diagnostic classificationsystems are introduced, application of personalitytypes is being applied to various medicalconditions, and many new questionnaires aredeveloped.
As in the case of interviews, the use of ratingscales in clinical observation helps not only toorganise information but also to encouragereliability and objectivity. That is, the formalstructure of the scale is likely to keep unwar-ranted observer inferences to a minimum. Thetest findings provide valuable information aboutpatient’s current psychological functioning andhis premorbid level of functioning. lt providesthe baseline on which intervention programmescan be evaluated and outcome can be objectivelymeasured. The test finding can also help indeciding type of intervention useful to a givenpatient, e.g. patient having psychosocialproblems, poor social skills, poor decisionmaking, would benefit more from psychologicalintervention. Testing is time consuming thus ajudicious and focussed assessment should bedone for cost effectiveness.

19Counselling
Counselling has wider applications in health care,and is not only restricted to the mental healthproblems. You are probably aware about careercounselling, marriage counselling; and in healthcare, genetic counselling, family counselling andparent counselling are often practiced. The scopeof counselling is becoming wider, as physicaldiseases with psychosocial aetiological factors, e.g.AIDS, substance abuse, are on increase. Thischapter deals with the counselling process andskills that must be developed by any clinician.
Definition
Counselling is a process involving an interactionbetween a counsellor and a client, with the aimof helping the client change his behaviour.Counselling helps by explaining how thebehaviour is learnt and how personality changesoccur. Counselling can be explained as:1. It influences change in voluntary behaviour
of the client.2. The purpose is to provide conditions, which
facilitate a behaviour change of the clients.3. As in all relationships, limits are imposed upon
clients.4. Conditions facilitating behaviour change are
provided through interviews.5. Listening is an important component.6. Counsellor understands the client.7. Counselling is conducted in privacy and
discussion is confidential.
Activities Appearing Differentbut Similar to CounsellingTo understand the characteristics of counselling,we should examine some of the controversies,relationships and helping activities that resemblecounselling. There are also some activities thatmay appear different from counselling but havethe same intentions. These range from friendlyadvice giving to more sharper differencesbetween counselling and psychotherapy.
Advising and InfluencingCounselling has historically been associated withadvice giving in every day life. Advice can beconveyed in strong terms as ‘my advice to youis to get a job immediately’, or ‘I would adviseyou to consider my options before you act’. Anadvice can be acted upon or ignored. There areoccasions when we all need instructions oradvice. For example, we may ask about a travelroute to somebody who is more familiar withthat. But the final route X or Y is chosen by us.If one encounters a bad experience in that routewe may blame the adviser. Daily life may befilled with more examples like asking for adviceas what to wear, what to eat or buy.
Counselling is then not advice giving, but istelling clients what they should do, facilitatingtheir efforts to arrive at their own decisions withpersonal and psychological issues. Generally ourpatients want the clinician to decide for them,or provide solutions to their problems.

178 Behavioural Sciences in Medical Practice
Friendship
Friendship implies an acceptance, safety andloyalty. A real friend will come to your aid, ifyou need him. A real friend will not talk aboutyou behind your back. He will understand youand your problems. But your counsellor is notyour friend. Counsellors make clear boundariesbetween the counselling relationship and anyother kind of relationship. Traditionally, coun-sellors and psychotherapists do not offer theirservices to close personal friends, but today theblurring of boundaries between friendship andcounselling would lead to a compromise ordamage both kinds of relationship. Somecounsellors do not consider counselling distinctfrom relationships like friendship at all. We allhelp our friends by listening and respondinghelpfully to their problems. Though friendshipcannot be disciplined the way counselling is, yetthe importance of social support and listeningby a friend cannot be undermined. In thedeveloped western countries, patients with HIVand AIDS are assigned to a supportive friendon a long-term basis. Another example of thisis Alcoholic Anonymous groups. There arefellow recovering alcoholics who offer com-.mitted support.
Friendship probably may help people morewith their problems than formal counselling. Butsometimes people do not want to be burdenon their friends or they may feel their friendsdo not want to listen about their depression, onemay have few or real geographically accessiblefriends or relatives. Some people may not beable to make good friends. Then the counsellorsmay functionally replace close friends teachingthem how to seek secure friendships.
Teaching
Counselling is not teaching. It is rarely a didacticteaching, but counselling helps individuals tounderstand their values, and coping resources.
Counsellors working with certain models oftenexplicitly teach their clients new ways of lookingat matters in the form of psychological concepts.Transactional Analysis, Cognitive AnalyticTherapy, Rational Emotive Therapy, CognitiveBehavioural Therapy, all teach skills to modifymaladaptive behaviour and effective functioning.Familiarity with the basic parent-adult-childmodel of transactional analysis, progressiverelaxation techniques, social skills, assertivenesstraining are taught to the clients.
Distinctions Between Counsellingand Psychotherapy (Table 19.1)Psychotherapy and counselling are the two termsyou often use while referring to psychologicalforms of treatment. These two are not the same,though both forms of therapy share manyfeatures in common. Psychotherapy is apsychological approach to treatment of emo-tional disorders as opposed to pharmacologicalor physical (ECT) approaches. This form oftreatment involves an interaction between twopeople or more individuals.
Table 19.1: Difference between counsellingand psychotherapy
Counselling Psychotherapy
1. Education, career, 1. Supportive, reconstructivehealth related
2. Situational 2. Depth rooted3. Problem-solving 3. Analytical4. Focusses on present 4. Focusses on past5. Deals with normal 5. Deals with severe emotional
age—appropriate problemdevelopmental tasks
6. Short-term 6. Long-term7. Emphasis on preven- 7. Emphasis on present
tive mental health mental health problems
The distinction between these two forms oftherapy is not always clear-cut. Instead of viewingthem as distinct forms of therapy, these shouldbe viewed on a continuum with regard to

Counselling 179
various elements like goals, clients, setting,practitioner and method. In therapy, it iscustomary to designate the person, receivinghelp as “patient” and in counselling as “client”although this distinction is only superficial. In thischapter, patient refers to the person havingphysical illness, and client refers to persons havinga problem rather than an illness. In comparingthe goals of counselling to the goals of therapy,it seems apparent that a frequent goal ofcounselling is to help individual deal with thedevelopmental tasks appropriate to their age.Counselling is more concerned with preventivemental health and therapy with remediation.Counsellor’s deal with individuals who are notnecessarily ill, but who have encounteredproblems, which may well be temporarilygenerating unhappiness.
Goals of Counselling
There are five major goals of counselling,namely:1. Facilitating behaviour change2. Enhancing coping skills3. Promoting decision making4. Improving relationships5. Facilitating client potential.
These goals are not mutually exclusive, norare they equally appropriate for every client. Amore appropriate classification of counsellinggoals has been given by Byrne (1963). Theseare:a. Ultimate: Goals which appear to be ideals
and we could achieve the desired outcomefrom counselling.
b. Intermediate: These relate to reasons forseeking counselling and usually requireseveral sessions to achieve this. The firstfour counselling goals mentioned above areintermediate goals i.e. they are outcomes,which can reasonably be achieved.
c. Immediate: These goals are moment bymoment intentions of counseling, e.g.
encourage a client to verbalize an un-expressed feeling.
Skills of Counselling
Most people probably agree that the kinds ofskills, which form the basis of practical counsellingtraining are not entirely distinguishable from thekinds of interpersonal and communication skillsused in everyday settings. While impartingtraining in counselling skills, it is necessary thatthe clinicians should also be trained incommunication skills (see Chapter 23) andshould be motivated, as counselling requires timeand patience. The counselling skills are:1. Listening2. Attending3. Perceiving4. Responding5. Initiating6. Summarising.
Passive Listening
Possibly the most basic of all skills is listeningwithin the counselling interview. Patients needopportunities to explore their feelings, attitudes,values and behaviours; initially they needsomeone to listen, even passively, to what theywish to share. New counsellors are typicallyuncomfortable with time lapses during theinterview, but if the counsellor can becomesensitive to the various meanings of silence andskillful at handling these pauses, these silencescan prove very useful. First, silence lets patientsknow that the responsibility for the interview lieson their shoulders. Too often counsellors rushinto fill up the space, thus assuming inappropriateresponsibility for the session. Second, silenceallows patients to delve further into thoughtsand feelings and to ponder the implications ofwhat has transpired during the session, patientsneed this time to reflect and process withoutfeeling pressured to verbalise every thought andfeeling.

180 Behavioural Sciences in Medical Practice
Listening is the process of tuning in carefullyto the client’s messages and responding accu-rately to the meaning behind the message. Thistype of listening is crucial in moving socialconversation to different levels of communi-cation, and it is the core of effective counselling.Listening at its simplest level calls on thecounsellor to reframe the content and feelingsthat the patient has expressed.
Listening is a synthesis of the skills ofrestatement of content and reflection of feeling.It promotes within the patient, the feeling ofbeing understood. It must be emphasised, thatlistening, though has an important role in thecounselling process, is not sufficient to producethe desired growth and change in the patient.
Attending
Attending refers to the physical behaviours youuse while listening to the patient. Posture, eyecontact, facial expression, tone of voice, andgestures, all communicate without the use ofwords. Attending makes it easier to listen andremember, it enhances self-respect of thepatient, it also helps to build good doctor-patientrelationship. On the other hand, poor attendingbehaviour distracts from the relationship.
Perceiving
Perceiving as a skill differs from listening andattending, as in this listening and attendinginvolve collecting all the cues the patientprovides: words, meaning, tones, expressionsand gestures. Perceiving is bringing all the cuesto personal awareness in an attempt to compre-hend the patient’s compliance.
It is important to develop skills to be ableto put meaning to the cues provided and theability to listen to self. The therapist should tryto be aware of the feelings and thoughts goingthrough the patient’s mind at the time ofconsultation.
Responding
Responding is essentially the culmination oflistening, attending, and perceiving. Respondingmeans communicating to the patient all that hehas said that has been heard. To achieve this,the therapist has to restate the content. The abilityto restate the content of the client’s message orto paraphrase a client’s statement is beginningin the process of learning to listen. Restatementof contents serves three purposes: a) to conveyto the patient that you are with him, that youare trying to understand what he is saying, b) tocrystallise a patient’s comments by repeatingwhat he has said in a more concise manner, andc) to check the interviewer’s own perception tomake sure he really does understand what thepatient is describing.
Reflection of feeling is another skill requiredfor responding. This differs from restatement ofcontent in terms of emphasis. In reflecting ona patient’s feeling, the counsellor listens carefullyto the patient’s statement and responds byparaphrasing the content of the message, buthe places the emphasis on the feeling, the patientexpressed. By responding to the patient’sfeelings, the counsellor is telling the patient thathe is trying to perceive and understand thepatient accurately from the patient’s internalframe of reference. The counsellor tries to identifythe feeling accurately by listening not only towhat the patient says, but also to how the patientsays it.
Initiating
Initiating skills refer to those skills the counselloruses to summarise and clarify the patients’problems and his deficits. With these skills youwould be able to elicit more information, solveproblems related to diagnosis and management.
Summarising
Summarising enables the counsellor to condenseand crystallise the essence of the patient’s
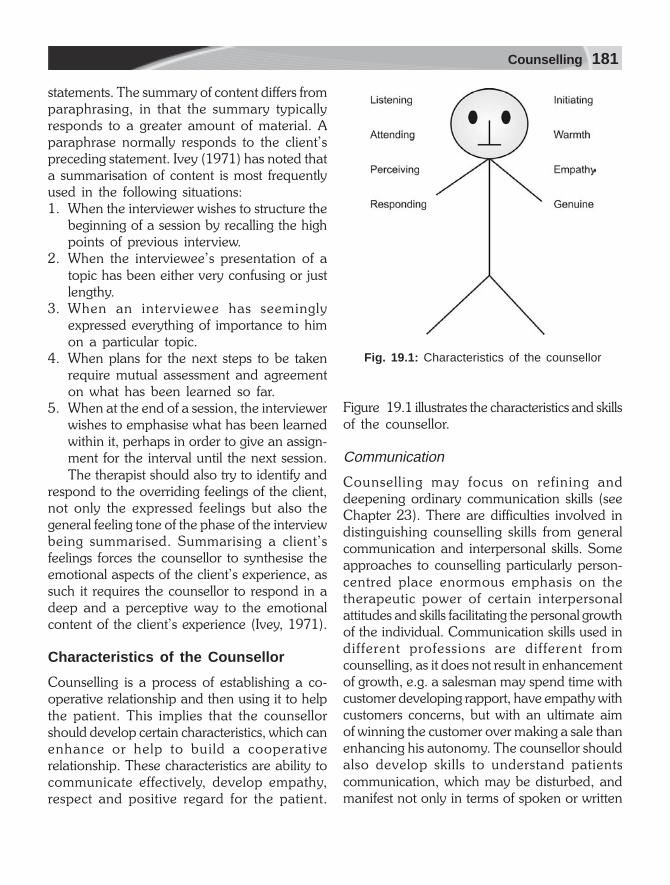
Counselling 181
statements. The summary of content differs fromparaphrasing, in that the summary typicallyresponds to a greater amount of material. Aparaphrase normally responds to the client’spreceding statement. Ivey (1971) has noted thata summarisation of content is most frequentlyused in the following situations:1. When the interviewer wishes to structure the
beginning of a session by recalling the highpoints of previous interview.
2. When the interviewee’s presentation of atopic has been either very confusing or justlengthy.
3. When an interviewee has seeminglyexpressed everything of importance to himon a particular topic.
4. When plans for the next steps to be takenrequire mutual assessment and agreementon what has been learned so far.
5. When at the end of a session, the interviewerwishes to emphasise what has been learnedwithin it, perhaps in order to give an assign-ment for the interval until the next session.The therapist should also try to identify and
respond to the overriding feelings of the client,not only the expressed feelings but also thegeneral feeling tone of the phase of the interviewbeing summarised. Summarising a client’sfeelings forces the counsellor to synthesise theemotional aspects of the client’s experience, assuch it requires the counsellor to respond in adeep and a perceptive way to the emotionalcontent of the client’s experience (Ivey, 1971).
Characteristics of the Counsellor
Counselling is a process of establishing a co-operative relationship and then using it to helpthe patient. This implies that the counsellorshould develop certain characteristics, which canenhance or help to build a cooperativerelationship. These characteristics are ability tocommunicate effectively, develop empathy,respect and positive regard for the patient.
Figure 19.1 illustrates the characteristics and skillsof the counsellor.
Communication
Counselling may focus on refining anddeepening ordinary communication skills (seeChapter 23). There are difficulties involved indistinguishing counselling skills from generalcommunication and interpersonal skills. Someapproaches to counselling particularly person-centred place enormous emphasis on thetherapeutic power of certain interpersonalattitudes and skills facilitating the personal growthof the individual. Communication skills used indifferent professions are different fromcounselling, as it does not result in enhancementof growth, e.g. a salesman may spend time withcustomer developing rapport, have empathy withcustomers concerns, but with an ultimate aimof winning the customer over making a sale thanenhancing his autonomy. The counsellor shouldalso develop skills to understand patientscommunication, which may be disturbed, andmanifest not only in terms of spoken or written
Fig. 19.1: Characteristics of the counsellor

182 Behavioural Sciences in Medical Practice
word but in all interplay of hidden gestures,feelings, bodily reactions, glances, etc. which areconstantly going on in human beings. Thereby,an awareness of both verbal and nonverbalfactors is essential in order to arrive at a completeunderstanding of each patient.
Warmth
Warmth is the caring for and accepting of anindividual. Warmth is communicated throughnonverbal behaviour, such as smile, tone ofvoice, etc. Warmth does not denote approvalor disapproval of the patient, but a caringattitude.
Empathy
Empathy means accurately understanding theindividual within that person’s frame ofreference. This means that you transposeyourself in imagination into your patient’sthinking, and feeling, so that you structure theworld similar to that of your patient. For example,you have a malnourished child and you arecounselling the parents on his food intake,quality, as well as quantity of food that you thinkthat the child should have, may not be feasiblefor the parents due to poverty, rural set up, etc.If in this case you were able to imagine theircontext of living, then probably your nature andcontent of counselling would be entirelydifferent, yet relevant to the patient. This alsohelps to improve compliance to treatment.
Empathy is feeling with others, not feelingfor other. It is communicating an understandingat the deepest level. If we are not able to under-stand the patient from his internal frame ofreference, we will be unable to help thatindividual.
Respect
Respect is closely related to warmth and caring.Respect can be related to unconditional positiveregard, or the patient also has potential, he is
worthy of changing himself. Respect should beexpressed especially when dealing with elderlypatients, women, and colleagues.
Genuineness
Genuineness is the ability to be real and notartificial, to be oneself in a relationship. A majorpart of genuineness is self-awareness, aboutyourself and how much help can be provided.It is better to be honest in the relationship withthe patient.
Client Expectations
It is important to note whether or not a parti-cular counselling experience will be worthwhileto the client, which will depend on the client’sexpectations. The counsellor must be aware ofher/his expectations and should encourageclients to talk about their expectations. Manyclients expect to have something done to/forthem as part of the counselling process.Counsellors must communicate to the clients thatultimately it is the client who acts, decides,changes and becomes what he or she shouldbe. In addition, clients often seek counselling incrisis situations, hoping to find remediation. Inthese situations, counsellors must learn torespond to the immediate needs and workingwith the client toward some intermediate/ultimate goals through the counselling process.
Influence of counsellors values on the client: Ourgoals are influenced by our values and whichin turn may affect the therapeutic goals.
Therapists should be aware of their valuesand those of the society (class-caste) and culturein which they live, and must avoid pressing themupon the patient. The values are communicatedthrough direct suggestions, interpretations orbuilding the nature of relationship between thetwo. The mannerisms of the counsellor indicatethe favourable or unfavourable attitude towardspatients verbal productions through operantconditioning, e.g. trace of a smile, a pleased look,

Counselling 183
nod of head, etc. The counsellor must try to beneutral, recognising his morals and values, atthe same time express them if he/ she feels thatthe relationship would improve.
Process of Counselling
The goals of counselling can be introduced inthe initial session and if acceptable to the client,the counsellor can work toward bringing an endto counselling as soon as clear direction is esta-blished. The duration of counselling determines,how long the relationship lasts. This is animportant area as it is related to the success ofcounselling. The processes involved incounselling to bring the minimum change in theperson include:
Change of Utilisation
Counselling attempts to bring about the bestpossible utilisation of what the person alreadyhas. We in each case help a person to discoverhis/her anxieties and conflicts, and graduallymove forward. In counselling, the person canbe made aware of the directional shifts that arepossible for him.
Emphasis on Strength
By and large, our diagnostic thinking rests onthe concepts taken from psychopathology. Wepoint out a person’s weak spots. Instead, onemust place emphasis on ‘positive diagnosis’. Aperson who knows about his/her real strengthsand values will be better able to cope withanxieties about certain aspects in life. We canenlist those by asking the patient, throughobservations from family and friends, etc. Thiswill make the individual aware of assets allowingone to by-pass difficulties.
Counselling Structure
One must try to structure the situation for theclient and must take into account his/her
expectations and goals, as well as ones own. Acounsellor’s job is to help the person find outwhat his/her personality is like, and decide howhe can use the assets he has and get rid ofobstacles that are blocking his progress. Anythinga person wishes to bring up can be consideredand analysed.
Necessary Support
Support the patient to look into new possibilities.Support does not mean pep talks, shallowreassurance or encouragement of dependence,but lending one’s strength to the patient duringwhich he can be certain about his moves. Oncethe client has established new direction forhimself, one can schedule interview hours amonth apart to maintain his/ her confidence.
The Closing Phase
Once a clear-direction is established in the client’slife, improvement in emotional ties with one’sfamily and a greater willingness to assumeresponsibility, is an indication of developmentand time to think about termination, whetherit takes two hours or 200, if he succeeds theeffort will have been very much worthwhile.
Counselling in Health Care
Counselling is a leading inherent technique inexplaining the prevention and management ofany illness. Social and psychological factors needto be recognised besides physical problems. Dueto increasing health awareness today, educatedpatients are not satisfied with simple prescription,they wish to discuss about factors that canpromote health and prevent further advance-ment of the disease. One encourages positivebehaviours related to change in lifestyle, e.g.eating a balanced diet or exercising regularly.Health education programmes can be giventhrough counselling to provide informationrelated to health, to change attitudes and health

184 Behavioural Sciences in Medical Practice
relating behaviours, which are conducive to thesame. Counselling is an important adjunct tomedical intervention. The role of the counsellingin medical settings is twofold.1. Counselling patients and their relations2. Work with health professional.
When the individual becomes ill, the con-cerns, preoccupations and worries have beenshown to change dramatically, focussing aroundthe illness and the effect it may have on the dailyactivities, their work and their family. The mostcommon reaction to an illness is distress andanxiety. Recognising patient’s distress isimportant, as the presence of psychologicaldistress has been found to have a negative effecton recovery from illness. Distress at all stages ofillness can be reduced by providing informationabout the illness and treatment. It is the periodof uncertainty, not knowing, which is mostdifficult to bear. With counselling skills physiciancan handle the sensitive aspects of theinformation to be provided, e.g. explanation oftreatment of cancer, its side effects andprognosis.
Counselling is increasingly being used todescribe a less directive way of helping peopleespecially in dealing with HIV patients.Counselling has been accepted as the controlcomponent in the management of AIDS. Indeveloping countries like ours, treatment of AIDSis very expensive; moreover, the prognosis beingvery poor, prevention is very important. Thiscan be achieved by counselling patients, theirrelatives, especially the spouses, and high-riskpopulation. The primary prevention of AIDSmay involve:a. Educating people about AIDSb. Strategies to reduce riskc. Injecting drug used. Promoting safer sex.
The initial sessions one can set goals andgradually provide support directing theindividual to recognise and look into his/herbehaviour. Counselling process should involveclient’s expectations, values and motivate
patients to aim for improvement in the directionof resolution.
SUMMARY
Counselling is viewed as a relationship, as wellas a process. It is designed to help people makechoices and resolve problems. It influenceschange in voluntary behaviour of the client. Thepurpose is to provide conditions, which facilitatea behaviour change of the clients. As in allrelationships, limits are imposed upon clients.Conditions facilitating behaviour change areprovided through interviews. Listening is animportant component. Counselling is conduc-ted in privacy and discussion is confidential.
Counselling is different from advising,friendship, teaching or psychotherapy. Thedistinction between these two forms of therapyis not always clear-cut. Instead of viewing themas distinct forms of therapy, these should beviewed on a continuum, with regard to variouselements like goals, clients, setting, practitionerand method.
There are five major goals of counselling,namely: facilitating behaviour change, enhan-cing coping skills, promoting decision making,improving relationships, and facilitating clientpotential.
The counselling skills include passive listening,accurate understanding, ability to understand theview point of another person, as if from theirown perspective, an ability to articulate what onehas heard and understood, to summarise theconcerns expressed in the conversation and anability to engage emotionally with others.
Counselling is an important adjunct to medi-cal intervention. The role of the counselling inmedical settings is twofold: (i) Counsellingpatients and their relations, and (ii) work withhealth professional. Counselling is being usedin the prevention of AIDS. The primaryprevention of AIDS may involve: (i) educatingpeople about AIDS, (ii) strategies to reduce risk,(iii) injecting drug use and (iv) promoting safersex.

20Behaviour Therapy
All behavioural approaches to therapy have asa common aim the direct modification of obser-vable behaviours, which have been identifiedas in need of change. These approaches sharea common premise, namely, that mostbehaviour is learned according to basic principlesof learning. Behaviour serves as a function intheir current context and is maintained by theevents, which precede and follow them. Thesemay or may not be the same factors, which gaverise to them in the first place. Behaviour therapytherefore, addresses to those factors that are seento be maintaining problems rather than thosewhich may have originally caused them toappear. It does not postulate underlying causes,as psychodynamic therapies do, but regards theobserved behaviour itself as ‘the problem’.
This view of behaviour therapy regardsbehaviour as functional or goal oriented. Therelevant goals are the observable or reportableconsequences of the behaviour, which maintainit. Behaviour, which includes thoughts, istherefore, a sample of the difficulties faced bythe patient and not merely a symptom of theunderlying pathology. These characteristics ofbehaviour therapy are described as:
i. Behaviour therapies attempt to modify theproblematic behaviours themselves.
ii. Like the social behaviour theories that guidethem, behaviour therapies emphasise theindividual’s current behaviours rather thanthe historical origins of his problems.
iii. Most behaviour therapists assume thatdeviant behaviour can be understood andchanged using the same learning principlesthat govern normal behaviour.
Though behaviour therapy has been appliedsince ages for disciplining children’s behaviour,rewarding and providing feedback for goodacademic work, etc. The application of learningprinciples to the problems occurring within thecontext of a clinical disorder has been in practicesince late fifties in some developed countries. InIndia, this form of therapy is being practiced sinceearly seventies, and at present this form oftherapy is the most popular amongst allpsychological therapies.
Foundation of Behaviour TherapyThe historical roots of behaviour therapy arebased in the two fundamental learning theoriesof classical and operant conditioning, (seeChapter 5). The social learning theory ofBandura (1969), which significantly contributedto the recognition of the role of cognitions onovert patterns of behaviour, was followed by theintroduction of various therapeutic techniqueswhich affected a change in observable behaviourby focussing on the mental processes or hiddenbehaviours referred to by Bandura. The role ofthe mediational processes and the subsequentdevelopment of covert treatment strategies areviewed by many practitioners as a comple-mentary extension of traditional behaviouralconcepts.

186 Behavioural Sciences in Medical Practice
In recent years, adopting a behaviouralperspective to management of psychiatric pro-blems has grown in popularity. There is the focuson the here-and-now, observable behaviour andthe avoidance of dynamic formulations. This formof therapy is objective, structured and can bepracticed by nurses, parents, spouse andteachers as cotherapists.
The limitations of the classical and operantmodels, in terms of their reliance on external,observable phenomena, focussed attention onthe role of internal behaviours, thinking,reasoning and imagining, for example, and theway in which such covert processes influencethe performance of behaviour. The resultantmediational theories of learning propose thatenvironmental stimuli do not in themselvesinitiate overt behavioural responses; rather, thenature of the response is additionally influencedby cognitive or information processing elements.
An important feature of Bandura’s sociallearning theory is the suggestion that learningcan take place indirectly and not just throughdirect experience, as proposed by earlier theorists(Bandura, 1969). Indirect or vicarious learningcan occur through the observations andexperiences of others. The mimicry ability ofchildren is well known and often a cause of adultembarrassment and amusement. Young girlslearn how to apply make-up by observing andthen imitating their mother, boys through thesame process, can replicate their father’s shavingritual. Moreover, as every parent knows, childrendo not just learn crude approximations, or themere mechanics of behaviour. Their imitationswill include subtle changes in facial expressionor body posture; similarly desirable behaviourpatterns or maladaptive responses can also beacquired. A child who observes his mother’sanxiety response to certain situations is likely todemonstrate equivalent behaviour when facedwith analogous situations. Vicarious learning,however, involves more than simply watching.Bandura describes four cognitive processes,
while acknowledging that there may be others,which mediate between the external event andthe behavioural response, namely, attention,retention, reproduction and motivation. Thechild for example, must be able to focus hisattention on his father’s behaviour; he must thenretain what he sees, so that he can reproducethe action. Finally, but just as importantly, thechild must be motivated to perform thebehaviour.
The prominence given by Bandura to theinternal or hidden processes generated prolificdevelopments in clinical techniques explicitlydirected at these covert behaviours. Mahoney(1974), for example, examined the relationshipbetween perception and behaviour. Hesuggested that the interpretation of an eventmight not represent the reality of the situation.A train passenger who thinks an alteration inengine vibration means that the train is aboutto crash has not authentically interpreted whatis happening. The concomitant effective andphysiological responses are a consequence ofhis unrealistic perception of events. A few yearslater, Meichenbaum (1977) demonstrated howpsychotic patients could learn to control dis-ruptive cognitions. Advances in the therapeuticmanipulation of these mental processes not onlyenhanced contemporary knowledge of humanbehaviour, but also expanded the clinician’s skillsrepertoire. The contemporary practice ofbehaviour therapy recognises the contributionto individual problems of living of distorted orunhelpful cognitive functioning. Cognitivetreatment approaches are increasingly combinedwith the more traditional behavioural methodsof intervention to help people improve theirquality of life.
Characteristics of Behaviour Therapy
Genuineness, warmth, empathy and the thera-peutic relationship that are important for thecounsellors, (see Chapter 19) are also important

Behaviour Therapy 187
to behaviour therapists and full recognition isgiven to their significance as determinantvariables of treatment efficacy. The therapeuticapproach is based on a model, which viewshuman behaviour largely as a function of theindividual’s interaction with his environment.Furthermore, it suggests that maladaptivebehaviours, are primarily acquired through theprocess of learning, in the same way as adaptivebehaviours are learned. It is the behaviour itself,which is the focus of attention rather than anyunderlying psychopathology, with the emphasison the here and now of the problem, whichdetracts from the individual’s quality of life. Thecharacteristics of behaviour therapy can besummarised as follows:1. Behaviour therapy is an empirical, scientific,
client-centred approach to an individual’sproblems.
2. There is a rigorous systematic assessmentprocess, which precisely defines in ope-rational terms the patient’s problem andidentifies environmental factors, whichinfluence the problem behaviour.
3. Explicit treatment goals are agreed upon anddefined prior to treatment intervention. Thedegree to which these targets are met allowsfor accuracy in progress evaluation andtreatment outcome.
4. The treatment techniques of behaviourtherapy are effective because they are deri-ved from clinical and experimental research.Behaviouralists place great emphasis onscientific validation of their practices and onthe individual appropriateness of the treat-ment methods selected.
5. During the assessment periods, observationsare made of the problems behaviour, whichprovide baseline measurements. Thesemeasurements are repeated at regularintervals during the treatment phase andagain on completion of the interventionprogramme. This progress is rigorouslymonitored from start to end. They are
indicators for continuance or modification ofthe treatment package.
6. The collaborative nature of this style oftherapy and the active participation of thepatient is strongly emphasised from the verybeginning.
7. Change, to have any real value to theindividual, must be socially significant.Therapy cannot be said to be therapeuticallyeffective if, on a practical everyday level, thepatient experiences no real improvement inhis quality of life.
8. It is a fairly common practice of behaviouralinterventions, to involve the use of cothera-pists who will assist in the delivery of thetreatment programme. Cotherapists may beparents, nursing staff, spouses, friends orcolleagues, who with the agreement of theclient, make a structured contribution to theresolution of the problem.
Process of Behaviour Therapy
Behaviour therapy aims to facilitating behaviourchange, to achieve this aim the first step is toidentify the specific nature of his problem, toidentify possible factors that precipitate andmaintain the problem behaviour, to assess thebaseline functioning of the patient, degree ofdistress caused by the problem, patients moti-vation to change his maladaptive behaviour andreadiness of key family member to’ act as a co-therapist. Behavioural assessment is summarisedin the Table 20.1.
Table 20.1: Behavioural assessment
1. Defines problem Functional analysis2. Helps Selection of treatment, e.g.
relaxation therapy exposure3. Assesses Change in behaviour through
self reportParent’s observationCognitive functioningPsychosocial factorsBaseline and ongoing assessment,e.g. frequency, intensity of panic attacks

188 Behavioural Sciences in Medical Practice
Observations made in clinical settings bytrained observers can provide useful behaviourdata. The programme includes evaluating thebehaviour of chronic patients and monitoringthe activities of staff members working with them.
In other situations, where observation in thenatural setting is not possible, the clinician mayconstruct an artificial observational situation thatcan provide information about the individual’sresponse to a particular situation. For example,an individual who has a phobia for snakes mightbe placed in a situation where snake-like objectsand pictures are presented.
An often-used procedure that enables theclinician to observe the patient’s behaviourdirectly is role playing. The patient is instructedto play a part, for example, someone asking forhis rights. Role-playing in a situation like this notonly can provide assessment information for theclinical assessment but also can serve as a vehiclefor new learning for the patient.
A type of self-observation which serves as atherapeutic strategy as well as an assessmentprocedure is self-monitoring. With this techni-que, patients are asked to observe and recordtheir own problem behaviour. In case of childpatient, parents can record the particularbehaviour. For example, they might be askedto record the number of times during the weekpatient had severe anxiety attack.
Treatment Methods inBehavioural Therapy
To modify or change maladaptive behaviours,various treatment methods are used. Somemethods help to decrease the maladaptivebehaviour, e.g. anxiety, while others tend toincrease adaptive behaviours, e.g. assertiveness,some methods build new adaptive responses,e.g. shaping language in mentally subnormalchildren, others eliminate maladaptive responses,e.g. temper tantrums. Some of the commonlyused treatment methods are discussed in thissection.
Relaxation Training
Relaxation training is the most effective methodof controlling anxiety. Though there are somedifferent methods used in relaxation training likeyoga, meditation, autogenic training, butJacobson’s progressive muscle relaxationprocedure is used more commonly. The musclerelaxation training involves progressively tensingand then relaxing major muscle groups in thebody. This procedure requires about 20 minutesto practice. Initial few sessions are given underthe therapist’s instructions, later the patient learnson his own and practices at home. At times,audiocassettes are provided to the patient forhome practice. The patient continues practicingthe relaxation procedure until he or she can relaxall the muscles in the body through the recallof the relaxed state. The goal then is to teachthe patient to discriminate between tension andthe relaxed stage. Relaxation exercises arecommonly done in the supine state withoutpillow. It can also be done while sitting on thechair.
The variations to this form of relaxation are‘savasana’ (yoga), brief relaxation, and cuerelaxation. Cue relaxation is also used as anadjunct to the standard procedure; it involvesimagination of a neutral scene, or listening tosome soft musical tune that is relaxing for aparticular patient, after the patient has finishedrelaxation exercises. Later this cue acts as aconditioned response to decrease anxiety.
Biofeedback TrainingBiofeedback training typical involves providinginformation about physiological functions thatare normally not in the patient’s awareness. Thephysiological functions used in biofeedback are:GSR, EMG, respiratory, and temperature. Aspecified target response, such as cervical muscletension is electronically monitored andinformation about changes in the functioning ofthe targeted response is relayed to the patientvia various feedback devices, such as a meter

Behaviour Therapy 189
reading or an auditory signal or visual signal inform of light. The goal is to use the feedbackto teach the patient to relax.
Hypnosis
Hypnosis is also used to decrease anxiety. Theactual hypnotic procedure typically varies,depending on therapist or patient, but the goalsare generally similar. Goals can include alteringthe patient’s negative perception of the problem,e.g. pain, shifting it to a neutral or a positiveone, enhancing positive self-statements, andimproving health-related attitudes. Hypnosis isalso used in patients with somotoform disorders.
Exposure
Exposure is the main technique used for treat-ment of phobias. The patient is exposed toanxiety provoking stimuli to decrease his anxiety.It is also used in conditions where anxiety isrelated to specific situations e.g. anxiety onseeing patients of leprosy. In theory, phobias canbe overcome by facing the things that are feared.The therapist should explain the model, usingthe patient’s individual symptoms to illustrate howvicious circles maintain symptoms. For example,an agoraphobic patient described having felt hotand fainted in a bus one day (a physiologicalsymptom), and then taking an alternative modeof transport, walking or hiring taxi to go to workthe next day for fear of going on the bus again(an avoidance reaction that maintains theanxiety). Gradually she began to dread journeys(anticipatory anxiety, another reaction), andpersuaded her husband or friends to take herto work (behaviour of others maintained heravoidance). With explanation of what hashappened, it becomes clear that if the avoidanceis reversed, gradually, in manageable steps, thenthe fear will subside. The patient should beencouraged to think actively about what to do.
The self-help rationale of treatment is thatthe vicious circle cannot be broken without the
active participation of the patient. The therapistshould explain that treatment involves learninghow to work on the problem effectively andindependently. Treatment sessions shouldtherefore, be backed up by regular homework,and improvement will be the result of acollaborative effort. It is necessary to keep arecord of practice, and to use this both to monitorprogress, and to identify stumbling blocks. Thefunction of practice is the same as when learninga physical skill.
Graded exposure: In practice, it is not alwayseasy to stick precisely to the guidelines forexposure described above, and treatmentdemands much creativity from both patient andtherapist. Various other procedures can becombined with exposure, such as relaxationexercises, distraction, role playing, rehearsal, andmodelling.
Devising practice tasks: It is frequently difficultto draw up a graduated list of tasks. A numberof useful strategies are available when thishappens. If the phobia is circumscribed, as inanimal phobias or fears of specific illness, anymeans of communication can be used as a basisfor practice. The patient may thus be able toextend the range of tasks by reading, writing,or talking about the phobic object; by watchingrelevant television programmes or films, or bylistening to radio programmes, and so on.
The greater the variety of available practicetasks the better, even though practice is hardwork, and may be boring. Greater varietyincreases motivation, confidence, and theprobability that improvement in one aspect ofthe phobia will generalise to other aspects (e.g.from waiting in the queue at the bus stand, towaiting in the hospital for the physician, andwaiting for someone who is late returning home).Strategies can also be used to break tasks downinto smaller steps when the next item on thehierarchy is too difficult. Encouraging patientsto search for opportunities to approach instead

190 Behavioural Sciences in Medical Practice
of avoid, helps them to overcome disruptivetypes of avoidance. These include feelingreluctant to do something, postponing activities,not thinking about the phobia, and givingexcuses or rationalisations.
Real life exposure: A major goal of treatmentis to give patients the confidence to face thethings they have been avoiding. This is whystrong emphasis is placed on homework, andon the realistic setting of practice. Nevertheless,it can be useful to accompany a patient duringexposure to begin with. This may reduce anxietyand/or make it easier to move faster up thehierarchy. It may also be a way of demonstratingparticular skills, for instance in managing anxietyor social interactions.
Imaginal exposure: In some cases, for examplethunder phobia or fear of travelling in trains,it is not easy to arrange real-life exposure, andimaginal exposure has to be used instead.Imaginal exposure should be graduated in thesame way as real-life exposure, and the twoshould be combined whenever possible. So thetravelling phobic may have to prepare for ajourney in imagination, but will also benefit fromreading or talking about train journey, from visitsto railway station, and, of course, from regulartravel by train. The patient starts by imaginingthe item vividly enough to induce anxiety, andgoes on thinking about it in as much detail aspossible until anxiety subsides. Items should berepeated until they provoke little anxiety, beforemoving on to the next item on the list. Thereis much variation in the ability to use imagery,so some patients may need a little promptingbefore they can get a clear image, and othersneed the therapist to describe the scene to them.For this reason, much of the exposure takes placeduring part of the treatment, and if the patientnotes down the imaginal scenes used, and isshown how to keep a record of anxiety and howit changes during imaginal exposure, it should
be possible to continue the exercise at home forhalf an hour each day.
Audio exposure: It is also used in the treatmentof obsessive compulsive disorders, with thesepatients audio exposure has been found to besuccessful. In audio exposure the patient isrequired to write a script about the worstscenario that he fears. Each scenario is like astory and runs for 1-2 minutes. Several suchscenarios are written. Then the patient is askedto record the script on an audiotape in his ownvoice. The patient is required to listen to thistape over and over again, several times in a daytill his anxiety related to a particular obsessionis reduced. The patient is instructed to listen tothe tape as long as it triggers off anxiety. Thistape should be listened in the place where heis less likely to be distracted. This is further helpedby listening to the tape using a headphone. Aninpatient setting, is not likely to be more beneficialthan encouraging a self-controlled reduction ofrituals (Skeketee et al, 1993).
Procedure
Exposure can be applied in many ways. Astreatment has to be adapted to the patient’sneeds, phobics are frequently treated indi-vidually, and about an hour per session is usedto review progress, practice of exposure, andplanning of tasks to be completed outside thesession.
Home-based treatment, in which the part-ner or a relative of the patient is also taught abouttreatment and cooperates with the therapist toencourage, motivate, and advise the patient, hasbeen found to be particularly successful withagoraphobics (Mathew et al, 1981). It is alsoextremely economical of therapist’s time, goodand lasting results having been obtained duringresearch trials in five brief sessions. Generally,in order to be effective, exposure should provokeanxiety. These techniques do not undermine

Behaviour Therapy 191
exposure by removing anxiety completely, butfacilitate it by developing skills for controllingsymptoms.
Operant Conditioning
Operant conditioning procedure is based onSkinner’s principles (see Chapter 5). The basicnotion in operant conditioning is that behaviouris determined, in part, by its consequences. Ifa behavioural response of crying with abdominalpain in a child is followed by parental attention,not going to school or getting demands fulfilled,then it tends to be strenghtened and occur morefrequently under the same environmentalcircumstances, as shown in Figure 20.1. On theother hand, if the response is followed by anaversive stimulus (punishment) or by no stimulusat all (extinction), it tends to be weakened andoccurs less frequently under the sameenvironmental circumstances. This kind ofconditioning occurs continuously in daily life,because most behaviour operates on theenvironment; that is, has consequences in it.Behaviour is continually altered and shaped asa result.
Fig. 20.1: Operant conditioning model
The procedural steps in operant condition-ing are given in detail in management of mentallysubnormal children, in the later part of thischapter.
Token Economy is for management ofpsychotic patients in the ward. The systematicapplications of this method were first demons-trated by Ayllon and Azrin. This method is basedon the principles of operant conditioning, theonly difference being in the delivery of rewards.In token economy as the name suggests tokensare given as a consequence of positive response,
these tokens are later exchanged for therewards. This method has also been applied totrain mentally retarded adults.
Social Skills Training
Deficits in social skills are frequently seen inpsychiatric patients. The indications of social skillstraining are for those patients who have neverlearned appropriate social behaviour (ASB) likea severe adolescent stutterer, patient with impulsecontrol disorder. The other type of patients inwhom social skills training is indicated, whereappropriate social behaviour is not available dueto disuse, like chronic schizophrenia. Patients withfaulty cognitive evaluative appraisal and highlevel of anxiety are known to have interpersonaland interactional problems. Thus these individualsalso benefit from social skills therapy.
This method places an emphasis on perfor-mance not on causation of the problem. Hence,the technique of social skills training consists of,training in assertiveness, personal effectiveness,behavioural rehearsal and structured learningtherapy. Modelling, reinforcement prompts,homework assignments feedbacks, instructionsand role-play are used to build or enhancesocially appropriate behaviours.
This method holds a great promise for a widerange of psychiatric disorders in adults andchildren both. A very shy adolescent girl havingsocial phobias, or a withdrawn schizophrenic,or a drug addict requiring rehabilitation are someexamples for its applications.
Aversion Therapy
Aversion therapy is used to control inappropriatebehaviours, such as addictions, and sexualattractions to inappropriate stimuli. A smallbattery operated apparatus is used to giveelectrical aversion. In some cases chemical aver-sion is also used, e.g. antabuse for alcoholics.This technique has also been used by Despandeand Mehta (1990) for controlling tricotillomania.

192 Behavioural Sciences in Medical Practice
Contingency Contracting
The contingency contracting is based on theoperant conditioning principles. In this methoda contract is made between the client (as thisis applicable for modification of all types ofmaladaptive behaviour) and the therapist, thaton the achievement of the target behaviour,client receives a reward and on failing to achievethe target, he does not receive a reward andlike negative marking, he loses one reward fromthe earlier gained reward. The client maintainsa contigeney chart to monitor his progress. Thismethod is very effective for self-managementprogrammes, like cessation of smoking,controlling aggressiveness, enuresis, habitdisorders, etc.
Applications of Behavioural Therapy
Behaviour therapy has very wide applicationsto clinical problems; these have been appliednot only to the psychiatric problems but also toother fields of medicine. Its application inmedicine are dealt in Chapter 22. In psychiatricdisorders, this form of therapy is the first choiceof treatment for phobias and mental subnorma-lity. It is being used as an independent modeof treatment of anxiety disorders, obsessivecompulsive disorders, sexual disorders andaddictions. At present, social skills training is givenas an adjunct treatment to schizophrenics.
Behaviour therapy has been very effectivein the treatment of child psychiatric disorders.In Indian setting, these techniques have beenapplied for the management of behaviouralproblems in normal children and in mentallyhandicapped, habit disorders, enuresis andencopresis, specific learning disability, somato-form disorders, attention deficit hyperactivitydisorders, abdominal pain, headache, andinfantile autism.
Behavioural Training for MentallySubnormal Children
The effectiveness of behaviour modification intraining in mentally handicapped is now a longestablished fact. (Matson and Andrasik, 1983,Mehta et al, 1990). A wide range of behaviours,reflecting the diversity of age groups, levels ofretardation and treatment settings, have beenmodified using behavioural techniques. Mostlyattention has been devoted to training self-careskills, language, and social behaviour. Problembehaviours of all kinds have been found torespond readily to behavioural intervention.
Usually parents are involved in the manage-ment because of advantages such as theproximity and availability of the parents, thegreater feasibility of their being able to conductthe training in the home and for an adequatelylong period of time, and most of all theirpotential as powerful sources of reinforcement.In addition, behaviour modification techniquesare relatively simple and can be readily acquiredby almost anyone. The added benefits are alsoof easier generalisation and persistence oflearned behaviour.
In India, numerous programmes have beenexplored and developed. One of the models(Mehta et al, 1990) is represented in Figure 20.2.
This model of behaviour training can be usedby all those concerned with the mentallyhandicapped persons. The training programmeinvolves parents as cotherapist. The training isimparted in various steps listed in the Figure20.2.
Assessments of parents: It is important to carefullyassess parents before involving them in a trainingprogramme. This is not to say that a completepersonality profile is what is required butattitudes, traits or behaviour patterns likely tofacilitate training should be explored. The most

Behaviour Therapy 193
important of these are perception of the problemand motivation to train the child. Assessment ofthe parent’s daily routine and the home situationneeds to be made. Many parents would like tospend time training their children but in fact havebuilt up a routine, which does not allow for this.It would be pointless in such a case, to pushparents straight into a training programme unlesssome changes in routine are first established.
The measurement of such, parameters asperception of the problem and the motivationto deal with it is both difficult and timeconsuming. Moreover, measurement devices tosuit the varied situations likely to be encountereddo not exist and would need to be prepared.Despite this, it is pointless to proceed with trainingunless there is some previous knowledge of itslikely benefit with a particular set of parents. Itmay prove helpful to assess parental attitudetoward the problem by preparing a briefquestionnaire for this purpose. Motivation maybe rated by two or more persons, independentlywhile talking to the parents. A trial task may becarried out as a demonstration. A monitoring
task in which each parent in turn monitors targetbehaviour, or a neutral behaviour can be setup and the extent and quality of compliance beused as a rough indicator of the parent’s futurecompliance in training tasks. A similar task canbe set up for the parents to carry out at home.
Behavioural Training
Selection of target behaviours and reinforcers:This stage is best dealt within individual sessionswith the parents. It is recommended that morethan one target behaviour be selected so as toallow the parents to be trained in variedtechniques and be equipped to deal with avariety of target behaviours.
Obtaining baseline information: Importancemust be given to the necessity of baselining andmonitoring target behaviour. Baselining fordifferent kinds of behaviours must bedemonstrated using charts. The parent must trya baselining task in the clinic to ensure that theprocedure has been adequately learned. Theprocess of baselining and monitoring is importantfor assessing the effectiveness of the training.
The target behaviours to be worked withmust be recorded for a period of three days toone week depending, of course, on the apparentfrequency of the behaviour.
Teaching behavioural techniques: The varioustechniques used in the training are based onoperant conditioning. To build new behaviourscontigency management, task analysis, promp-ting, fading and shaping are used. To decreaseor eliminate undesirable behaviours, time outfrom reinforcement and overcorrection methodsare used. In task analysis, target behaviour isbroken in small steps, which are easy to learnfor the retarded child. Prompting is used to guideand help the child to learn and as the learningprogresses, the prompts are gradually faded.Shaping is gradual forming of behaviour through
Fig. 20.2: Treatment plan formentally retarded children

194 Behavioural Sciences in Medical Practice
establishing various chains of tasks. The commonexample for this is teaching dressing to a retardedchild. Each part of dressing, wearing under-garments, shirt, pants, socks, shoes and combingof hair can be developed step by step and thenchaining the entire process. Time out simplymeans depriving child from the reward. Themost effective time out from reinforcement isinattention froth parents. Overcorrection is usedwith children who have lesser degree ofretardation. The child is forced to do correctionsof his undesirable behaviours, like messing orthrowing things and the child is also forced tocorrect others things in the environment. Forseverely retarded children for maladaptivebehaviour at times restraint is also used.
Practical demonstrations of the use of varioustechniques appears more effective than lecturesor discussions as a training medium, particularlywhen training aids such as films, slides, posters,etc. are used.
Implementing the techniques: Training tasks mustbe allotted to the parents so as to give them theopportunity to implement the techniqueslearned.
Assessing the effectiveness of training: Both theprogress made by the parents, and that madeby the child must be assessed. Since a positivechange in the child’s target behaviour is thestrongest indicator of progress made by theparents, this must be assessed carefully byscrutinising, monitoring records and by obser-vation and ratings made separately by trainers.
Dealing with problems encountered: Groupsessions may be scheduled for handling thedifficulties with training encountered by theparents and to allow trainers to monitor theprogress made by parents and children. Suchgroup meetings must allow discussion, catharsisand sharing of experiences.
Home visits: Whenever possible home visits bytrainers should be made to ensure that parentaltraining is effective and is being generalised.
Duration of training: The duration of the trainingprogramme and the number of session willdepend on the availability of personnel, theconvenience of the parents and the numerousother considerations, and hence will have to betailored to suit each situation.
Follow-up: Ideally, follow up immediately afterthe training should be intensive and frequent,phasing out gradually. Ensuring follow up whenparents often come from distant places has alwaysposed a problem, which will often be the casesince help services are usually concentrated inthe larger cities. At times postal contact may haveto be resorted to for the lack of an alternative.
Limitations of behavioural techniques: Thoughbehavioural therapy may seem very simple andstraight forward process but in practice onecomes across problems like getting cooperationfrom the patient or his family members. Manyof our patients do not understand the value ofhome assignment, or regular practice, or keepingappointments. Majority of the patients get moresatisfaction by taking medicine, as they do notwish to put in any efforts. They want therapistto do magic to make them symptom-free.
As behaviour therapy has various appli-cations and it holds promise in successful treat-ment of many disorders, we need to developmethods to enhance generalisation of the learnedbehaviour, as once the schizophrenic patient haslearned to socially interact with other patientsin the ward, after going home he should alsobe able to interact with his family members.
There are not many trained personnel to takethe tremendous load of patients requiringbehaviour therapy. Development of differenttraining programmes, for professionals likepsychologist, psychiatrist, nurses, parents and

Behaviour Therapy 195
teachers is required. The training modules shouldbe made according to the need, intensity ofinvolvement, and duration of the training.
Documentation of improvement requiresmaintaining records, which is not very easy withall classes of patients, especially the illiterate.There are certain behaviours, which are easy torecord, some are not feasible as in case of childpatient, and behaviour occurring at schoolcannot be measured. In such cases the patient,his family and the therapist should try to findan alternative solution of recording.
SUMMARY
Behaviour therapy regards behaviour asfunctional or goal orientated. Most behaviouris learned according to basic principles of learningand behaviours serve a function in their currentcontext and are maintained by the events, whichprecede and follow them. Behaviour therapytherefore, addresses to those factors that are seento be maintaining problems.
The historical roots of behaviour therapy arebased in the two fundamental learning theoriesof classical and operant conditioning. Later it hasalso adopted techniques from the social learningtheory of Bandura.
In recent years, adopting a behaviouralperspective to management of psychiatricproblems has grown in popularity. Behaviourtherapy is an empirical, scientific, and a rigoroussystematic assessment process which preciselydefines in operational terms the patient’sproblem and identifies environmental factorswhich influence the problem behaviour.
Explicit treatment goals are agreed upon anddefined during the assessment periods, whereobservations are made of the problembehaviour, which provide baseline measure-ments. The collaborative nature of this style oftherapy and the active participation of the patientis strongly emphasised. Cotherapists may be
parents, nursing staff, spouses, friends orcolleagues, who with the agreement of thepatient, make a structured contribution to theresolution of the problem.
Behaviour therapy aims to facilitatebehaviour change, to achieve this aim the firststep is to identify the specific nature of theproblem, to identify possible factors that preci-pitate and maintain the problem behaviour, toassess the baseline functioning of the patient,the degree of distress caused by the problem,patients motivation to change his maladaptivebehaviour and readiness of key family memberto act as a cotherapist. Observations may bemade by trained clinicians or individuals maybe asked to maintain a type of self-observation.To modify or change maladaptive behaviours,various treatment methods are used. Some ofthe commonly used methods are relaxationtraining, biofeedback, hypnosis, exposure,operant conditioning, social skills training andaversion therapy.
Behaviour therapy has been very effectivein the treatment of a wide variety of psychiatricdisorders. Various studies have reported itsefficacy in the treatment of phobias, anxietydisorders, obsessive compulsive disorders, sexualdisorders and addictions. Social skills training aregiven as an adjunct treatment to schizophrenics.In severe problems, behaviour therapy is alsoused as an adjunct to pharmacotherapy. Thisform of treatment has been especially effectivein the management of child psychiatric disorders.lt has been used in the management ofbehavioural problems in normal children, thementally handicapped, in habit disorders,enuresis, encopresis, specific learning disablity,somatoform disorders, attention deficit hyper-activity disorders, abdominal pain, headache andinfantile autism. Behavioural methods are usedextensively in the management of mentallysubnormal children.
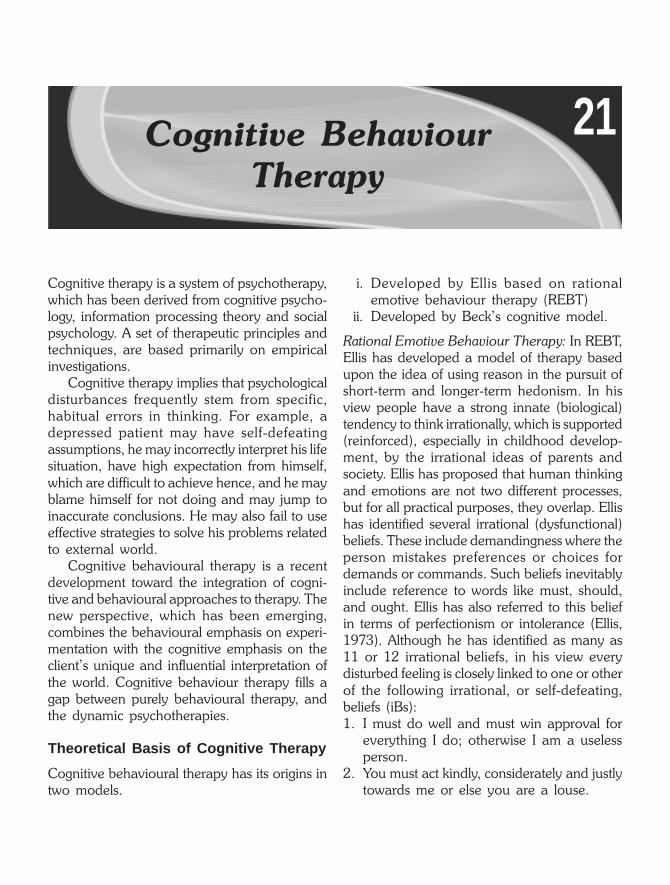
21Cognitive BehaviourTherapy
Cognitive therapy is a system of psychotherapy,which has been derived from cognitive psycho-logy, information processing theory and socialpsychology. A set of therapeutic principles andtechniques, are based primarily on empiricalinvestigations.
Cognitive therapy implies that psychologicaldisturbances frequently stem from specific,habitual errors in thinking. For example, adepressed patient may have self-defeatingassumptions, he may incorrectly interpret his lifesituation, have high expectation from himself,which are difficult to achieve hence, and he mayblame himself for not doing and may jump toinaccurate conclusions. He may also fail to useeffective strategies to solve his problems relatedto external world.
Cognitive behavioural therapy is a recentdevelopment toward the integration of cogni-tive and behavioural approaches to therapy. Thenew perspective, which has been emerging,combines the behavioural emphasis on experi-mentation with the cognitive emphasis on theclient’s unique and influential interpretation ofthe world. Cognitive behaviour therapy fills agap between purely behavioural therapy, andthe dynamic psychotherapies.
Theoretical Basis of Cognitive Therapy
Cognitive behavioural therapy has its origins intwo models.
i. Developed by Ellis based on rationalemotive behaviour therapy (REBT)
ii. Developed by Beck’s cognitive model.
Rational Emotive Behaviour Therapy: In REBT,Ellis has developed a model of therapy basedupon the idea of using reason in the pursuit ofshort-term and longer-term hedonism. In hisview people have a strong innate (biological)tendency to think irrationally, which is supported(reinforced), especially in childhood develop-ment, by the irrational ideas of parents andsociety. Ellis has proposed that human thinkingand emotions are not two different processes,but for all practical purposes, they overlap. Ellishas identified several irrational (dysfunctional)beliefs. These include demandingness where theperson mistakes preferences or choices fordemands or commands. Such beliefs inevitablyinclude reference to words like must, should,and ought. Ellis has also referred to this beliefin terms of perfectionism or intolerance (Ellis,1973). Although he has identified as many as11 or 12 irrational beliefs, in his view everydisturbed feeling is closely linked to one or otherof the following irrational, or self-defeating,beliefs (iBs):1. I must do well and must win approval for
everything I do; otherwise I am a uselessperson.
2. You must act kindly, considerately and justlytowards me or else you are a louse.

Cognitive Behaviour Therapy 197
3. The conditions under which I live must remaingood and easy, so that I get practicallyeverything I want without too much effortor discomfort, or else the world turns dam-nable, and life hardly seems worth living(Ellis, 1977).These three core beliefs are examples of what
Ellis has called ‘musturbation’. In Ellis’s view,there is no escape from individual responsibility.This approach aims to minimise the person’s self-defeating outlook, and to attain a more realistic,tolerant philosophy of life. His therapeutic tacticsemphasise disarming the patient on a conceptuallevel, often using punchy, direct language.
Beck’s Cognitive Model
The conceptual model upon which Beck’s cog-nitive therapy is based represents a synthesis offive distinct theoretical elements, each of whichhas been used to explain the genesis andmaintenance of specific problems of behaviour.Four functions within the individual (cognition,behaviour, mood and biology/biochemistry)interact with each other; all four interact withthe person’s environment. Such reciprocalinteractions can lead, from the perspective ofthis model, to the genesis of problems such asanxiety and depression.
This model acknowledges the role of pre-disposing and precipitating factors. Hereditarycharacteristics are accepted as potential pre-disposing factors, as are physical illness, whichmight generate neurochemical abnormalities.From a developmental perspective, inadequateexposure to experiences essential for the forma-tion of adequate coping mechanisms wouldconstitute a learning deficit, which might pre-dispose the person to psychological problemsin later life. Equally, the acquisition of rigid,dysfunctional belief systems, such as values andassumptions, would represent further predis-positions toward psychological problems in laterlife.
The cognitive triad or three specific thinkingpatterns are common in emotional disorders.These involved a negative view of self, a negativeinterpretation of life experiences (the world);and a tendency to take a negative view of futureevents. In the depressed patients, these thinkingpatterns appear to revolve around ideas of lossand deprivation. They perceive themselves asdeficient in important qualities, unworthy orgenerally inadequate. Such dysfunctionalthoughts intertwine with a range of fairly discretethinking errors, which involve faulty informationprocessing. Among the errors identified are:dichotomous reasoning (black-and-whitethinking): ‘If I do not succeed at everything Ido, then I am a total failure’, arbitrary inference(jumping to conclusions); ‘we had a fight, thismeans he does not love me any more’; selectiveattention (discounting the positive); ‘but I alwaysdo that anyway, that is not important’;magnification /minimisation (catastrophising);‘this is awful and there is nothing I can do aboutit’; personalisation; ‘why does this always happento me?’
The term schema designates relatively stablecognitive patterns. These form the basis of theperson’s interpretation or organisation ofexperience. Schemata represent the person’sinterpretation or organisation of experience, andthe person’s beliefs about himself. They arecommonly construed as unspoken premises,rather than conscious thoughts. Burns (1980)has classified seven discrete ‘silent assumptions’expressed in terms of needs. The need for:approval, love, achievement, perfectionism,entitlement, omnipotence, and autonomy.
Cognitive Approaches
Two broad categories of cognitive approachescan be distinguished: covert conditioningtherapies and cognitive learning therapies.
Covert Conditioning Therapies: As the nameimplies, the covert conditioning therapies

198 Behavioural Sciences in Medical Practice
attempt to apply a conditioning model to privateevents. Thoughts, mental images, and memoriesare viewed as covert behaviours, which conformto the same laws of learning that, were developedthrough observation of overt behaviours. Thus,thoughts are considered to be stimuli, responses,or consequences, and principles such asreinforcement, punishment, and extinction aresaid to affect their frequency and intensity.
A good example of a covert conditioningtherapy is Cautela’s technique of covert rein-forcement. In this procedure, the client isinstructed to imagine performing some difficulttask (e.g. refraining from drinking alcohol) andthen to reinforce himself by imagining somepleasant activity (e.g. watching a cricket match)A long involved task may be broken down intoa series of discrete steps, each of which is covertlyreinforced. A number of other covert condition-ing techniques are available, including exposureand thought stopping. By now most of theprinciples of learning, which have been appliedto overt behaviours, have been incorporated intosome covert technique.
Cognitive Learning Therapies
The second class of cognitive approaches is those,which have been labelled “the cognitive learningtherapies”. They are a much more hetero-geneous set of strategies, sharing a fewassumptions but differing widely in theirderivation and procedure. Though a precisemodel unifying these approaches has yet to bedeveloped, one or more of the principles appearto be fundamental to most of them.1. That human beings respond not to environ-
ments per se but to their cognitive represen-tations of those environments.
2. That thinking, emotion and behaviour areall causally interrelated.
3. That human learning involves the activeacquisition of complex rules and skills (deepstructural changes) rather than the passive
conditioning of simple habits or responses(surface structural manifestations).
4. That the task of the clinician is to teach skillsand offer experiences which replace mala-daptive cognitive representations with moreadaptive cognitive systems.
Process of CognitiveBehavioural Therapy
The process of cognitive therapy involves fivemain goals. The person learns to:1. Identify, evaluate and examine his thoughts
in relation to specific life events.2. Judge the validity of such thoughts using
objective evidence as a guide.3. Identify the silent assumptions (unspoken
schemata), which underpin his negativethoughts.
4. Practice a range of behavioural and cognitivestrategies, which can be applied in vivo whenconfronted by new or unexpected stresses.
5. Develop alternative, more adaptive, thoug-hts about himself, the world and the future,as well as less dysfunctional schemata.
Cognitive Behavioural Assessment: Assessmentin cognitive behaviour therapy is used to devisean initial formulation and treatment plan. Theformulation is tested out in subsequent home-work and treatment sessions, and modified ifnecessary. Cognitive behavioural approach islargely self-help, and that the therapist aims tohelp the patient develop skills to overcome notonly the current problems, but also any similarones in the future.
A cognitive-behavioural assessment also hasa general educational role and focusses thepatient on internal and external variables, whichmay not have been seen as relevant to theproblem. The patient is asked about situations,physiological states, cognitions, interpersonalfactors, as well as overt behaviour, and abouthow each of these groups of variables relatesto the problem.

Cognitive Behaviour Therapy 199
The assessment interview has an importantrole in beginning the process of therapy. Patientsfrequently present with an undifferentiated arrayof difficulties. As the therapist helps to clarify anddifferentiate between problems, so the difficultiesare frequently reduced to manageable propor-tions, and the patient begins to believe thatchange is possible. For example, a patient whopresents with a series of problems including mooddisturbance, self-dislike, hopelessness, feelsrelieved to learn that these are all commonsymptoms of one problem (i.e. depression), forwhich there are well-established treatmentapproaches.
The assessment emphasises the possibility ofchange, by helping the patient to think of whatmay be achieved, rather than dwellingcontinually on problems. It also sets reasonablelimits on what might be achieved throughtreatment; for example, it is unreasonable foran agoraphobic patient to aim never toexperience unpleasant emotions, but it shouldbe possible to undertake a train journey incomfort. The assessment also allows the patientto see that variations in the intensity of distressare predictable in terms of internal and externalevents, and are not just arbitrarily imposed byfate. It is implicit that if the variations arepredictable, they may also be controllable. Thetherapist should offer non-judgemental sympa-thy and concern about the patient’s problemsand distress; this may provide enormous relief,especially if the patient has felt embarrassed,guilty, or hopeless, as is often the case.
Finally, an important function of the assess-ment is to establish whether there is anything,which needs dealing with as an emergency. Forexample, if the patient is depressed, suicidal intentmust be assessed; if someone is complaining ofdifficulties in managing children, the possibilityof physical abuse must be explored.
In summary, the main goal of the cognitive-behavioural assessment is to agree a formula-tion and treatment plan with the patient. In
addition, it allows the therapist to educate thepatient about the treatment approach, and tobegin the process of change. It also allowsemergency factors to be assessed (Table 21.1).
Table 21.1: Methods of assessment
• Behavioural interview• Self-monitoring• Self-report (questionnaires, global rating scales)• Information from other family members.• Interviews and monitoring by key others (parents, spouse)• Direct observation of behaviour in clinical settings
– role-play– behavioural tests
• Behavioural by-products• Physiological measures.
Behavioural Analysis
To discover how the problem is currentlymaintained, in what way it is interfering with thepatient’s life, and whether the problem is servingany useful purpose for the patient. There aretwo commonly used approaches, first is themethod, which is also used in BehaviouralTherapy and discussed, in the previous chapter.In this method each problem can be analysedin terms of consequences. Each of these factorsmay increase or decrease the probability thatthe behaviour will occur.
Second approach though similar but morestraightforward way of carrying out a beha-vioural analysis is to describe the contexts inwhich the problems arise, to look at the factorswhich modulate the intensity of the problems,and to assess the consequences, includingavoidance, of them.
Detailed description of problem: As a first step,it is useful to ask the patient for a detaileddescription of a recent example of the problem.This gives more specific information than isobtained from a general description and providesclues about maintaining factors.
Context and modulating variables: A detailedassessment of contextual triggers is required

200 Behavioural Sciences in Medical Practice
because treatment plans often include manipu-lation of the contexts in which problems occur.In addition, treatment frequently involvesvariations in the modulating variables associatedwith particular cues. The range of possible triggersis almost infinite: for example, an obsessionalpatient may constantly ritualise at home butnever at work, an agoraphobic patient may beanxiety-free if in a town where she is unknown,a compulsive gambler may only gamble whenangry.
The patient may not be aware of the contextsin which the problem occurs, nor of themodulating variables. It is generally necessaryfor further information to be collected, eitherthrough self-monitoring or a behavioural test.These contexts and modulating variables couldbe situational, behavioural, cognitive, affective,interpersonal or physiological. Similarly, the samevariables could be responsible for maintaininga particular behaviour.
People differ in their methods of coping withproblems and distress, and in the extent to whichthey rely on themselves rather than on otherpeople. This ranges from the individual’sfamiliarity with specific strategies, like relaxingthe shoulders when tense, through to moregeneral assets, like being able to communicatedistress to others.
A description should be obtained of previoushistory, particularly of similar episodes. Thepatient’s response to previous treatment isparticularly important. This is partly because itmay predict current response to treatment, and,in the case of poor outcome, might giveinformation about pitfalls to avoid. Patients areunlikely to engage in treatment, if the approachthe therapist offers is not congruent with theirbeliefs about the nature of the problem.
Most cognitive-behavioural treatmentdemand a high level of commitment on thepatient’s part, and many treatments fail becausethe patient does not apply the agreedprocedures. It would be useful to identify those
people who are most likely to fulfill their sideof the treatment bargain. It is helpful to discusswith the patient some of the components, whichmake up a desire for change, correct anymisconceptions, and together make an informeddecision about whether it would be worthwhilecontinuing with treatment.
The assignment of homework and itscompletion is necessary component of cognitivebehaviour therapy. Hence, patient’s attitudetowards homework should be elicited andproblems should be discussed related toincompletion of homework.
Self-monitoring
These techniques involve monitoring or recor-ding of certain behaviour. Monitoring one’sbehaviour in this way also has a direct effect onthe behaviour itself. For example, individuals whorecord negative behaviours, such as overeating,usually reduce the amount of their food intakeover the period of self-observation. Thus, theassessment technique of self-monitoring hasbecome a major strategy in the treatment ofproblem behaviour.
Techniques used in CognitiveBehavioural Therapies
There are some specific therapeutic techniquesused in cognitive behaviour therapy.
Thought Stopping
To deal with intrusive thoughts, which are per-sistent patterns of negative thinking and disruptthe fulfillment of everyday living can beovercome by the procedure known as thoughtstopping. Thought stopping eliminates perse-verative thinking which characteristically isunrealistic, unproductive, anxiety provoking orotherwise disruptive. At times this procedure hasbeen used to control negative ruminativethoughts or auditory hallucinations. The

Cognitive Behaviour Therapy 201
procedure involves the patient to relax and thinkabout the negative thought. As soon as thenegative thought is produced the patient signalsthe therapist by raising his forefinger. Thetherapist shouts STOP. This interrupts thethinking process after few sessions the patientis asked to repeat this exercise on his own.Sometimes, the family members also can takethe role of the therapist when the trials are tobe practiced at home. Initially, the patient maysay STOP loudly on his own or he can use audiotape recorder. The patient is instructed togradually change from verbal STOP to subvocaland then to imagery of STOP.
Self-statements
Self-statements are thought which a patient hasabout specific events and their meaning for theperson concerned. The manipulation of nega-tive statements is used to enhance confidence,assertiveness and self-esteem in the patients. Thisis the simple and effective method, it involvesfollowing stages.1. The person is helped to recognise the
occurrence of such thoughts through use ofself-monitoring.
2. The person is helped to generate challengesto the negative thoughts, as well asproduction of alternative self-statements.
3. The person is helped to assess his reactionto be manipulation of self-statements, interms of his eventual behaviour andconcomitant emotions. This approach hasbeen used most successfully in depression,anger management, and impulse control inchildren.
Problem Solving
The focus upon the importance of cognition inunderstanding, mediating and resolvinginterpersonal and interpersonal problems.Problem-solving abilities are directly related toadjustment in children, adolescents and adults.People who do not have such skills have
problems like depression, anxiety, substanceabuse, and marital discord. Problem-solvingapproach has five stages.1. Recognition and understanding the nature
of interpersonal problems.2. Identifying the realistic targets and specific
goals. This involves problem definition andformulation.
3. Generation of a range of possible solutions.4. Arriving at a decision making out of the list
of possible solutions.5. Implementation and evaluation of the
selection solution.Problem-solving approach has been found
effective in management of number of psychia-tric problems both in children and adults. Thisapproach has a preventive value as oncelearned this strategy can be applied to the futureproblems also.
Distraction
A variety of distraction techniques can be usedas immediate symptom management strategies.Early in therapy, training in distraction can bea very useful way of combating patients’ beliefsthat they have no control over their anxiety.Later in therapy, distraction can be a usefulsymptom-management technique in situationswhere it is not possible to challenge automaticthoughts, for example, while talking to someone.In this situation, the distraction exercise wouldinvolve becoming outwardly directed, perhapsmoving closer to the person so that they feelthe patient’s field of view, and concentrating onthe conversation itself rather than on thoughtsconcerned with evaluation of his or her ownperformance. Distraction can also be used toprovide a potent demonstration of the cognitivemodel of anxiety.
Activity Schedules
In an activity schedule patients record their hour-by-hour activities, rating them (on 0-100 scales)for salient features such as anxiety, fatigue,

202 Behavioural Sciences in Medical Practice
pleasure, and mastery. Activity schedules intensetime pressure, they can be used to plan activitiesin such a way that they are likely to be able toengage in one task at a time (trying to do briefbreaks between tasks).
Time pressure and other anxious concernscan lead some patients to stop engaging in leisureand social activates which they previouslyenjoyed. Often these activities contributed to theirsense of worth and perceived control over theirenvironment. Therefore, dropping activitiesoften increases anxiety and perceivedvulnerability. Once this problem is identified, thetherapist and patient can use an activity scheduleto reintroduce pleasurable activities. Inspectionof activity schedules can also help to identifyperiods of anxious rumination, problems withperfectionism (suggested by highly polarisedmastery and pleasure rating—everything is eitherrated 10 or 0), and anxiety triggers.
Verbal Challenging of Automatic thoughts, Beliefsand Assumptions: In Beck’s model of depression,dysfunctional beliefs is cardinal feature ofdepression.
Challenging irrational or dysfunctional beliefsis important to bring change in the patient’scognition. Hence in cognitive behaviouraltherapy the patient is helped to identify,challenge and subsequently classify specific formsof thinking errors, in the form of specific self-statement. A series of questions are used to helppatients to evaluate negative automatic thoughtsand to substitute more realistic thoughts. Withinsessions, patients and therapist work collabo-ratively to identify rational responses toautomatic thoughts. Between sessions patientsattempt to put into practice the questioning skillsthey have learned in the sessions by recordingand challenging automatic thoughts as they arise.One particularly convenient way of doing thisis to use the daily record of dysfunctionalthoughts.
Behavioural Experiments: In addition todiscussing evidence for and against patients’
negative thoughts, therapists should also attemptto devise behavioural assignments, which helppatients to check out the validity of their negativethoughts. These assignments can be one of themost effective ways of changing beliefs.
Learning New Behaviours and Skills: For somepatients, part of the reason why they find socialsituations difficult is that they either lack, or havedifficulty using social and conversational skills.When this is the case, brief training in appropriatesocial skills can be helpful. Once a problematicsituation has been isolated, role-plays anddiscussion of what the patient actually did in thesituation are used to identify inappropriatebehaviours. Once these behaviours have beenidentified, alternatives are suggested, modelledby the therapist and then practiced by thepatient, initially in the safety of a role-play inthe therapy session and later in real-life situations.
Role-playing
Role playing and rehearsal are more often usedin the treatment of social phobias than of otherPhobias, and a role-play may itself be a typeof exposure. For example, a patient who findsit difficult to say no, or to be assertive, can practicebeing assertive during a role-play with thetherapist. This has many advantages. It mayreveal a lack of skill or knowledge, such asdifficulty in moderating responses, or beingunable to be assertive without being aggressive.The role-play can then be repeated in variousways, until the patient discovers how he or shewishes to change. Role-plays are particularlyuseful in preparation for events such as inter-views. Video (or audio) recordings, if available,allow patients to make the most of this type ofpractice. Watching the video provides accuratefeedback as well as new information: for instancethat they may feel much worse than they look.
Rehearsal
This is a way of preparing for exposure, manyphobics find that their minds go blank when they

Cognitive Behaviour Therapy 203
are faced with phobic objects or situations, orwhen feeling panicky. Techniques for managingthe symptoms of intense anxiety, especially panicattacks, should therefore be rehearsed. Whenthis ‘blankness’ occurs in social situations it createsawkwardness, which rapidly increases anxiety.It is less likely to happen if appropriate strategiesare rehearsed, and appropriate materialprepared, such as lists of questions to ask, ortopics to talk about. Social skills can be separatelyrehearsed and may improve with practice.Rehearsing difficult events, such as speaking inpublic, making a request, or introducingsomeone, both increases confidence and reducesanticipatory anxiety. Lastly, detailed rehearsalhelps to reveal ‘blocks’ that might preventexposure.
Modelling
This is a less direct technique, in which thetherapist demonstrates how to approach thephobic object, for example a snake or the edgeof a high building, while being observed by thepatient. Modelling is most effective when themodel exhibits, and overcomes, anxiety, and itis suggested that observation of such a ‘copingmodel’ facilitates the patient’s own coping skills.These might be poor either because patients donot know what to do, or because they are unableto think what to do at the time.
Clinical Applications
Cognitive approaches to treatment probablycame to the attention of most clinicians in themanagement of depressive disorders. However,cognitive behaviour therapy has much widerapplications, many of which relate to conditions,which often cannot be treated easily, andeffectively in other ways. These conditionsinclude anxiety and obsessional disorders, eatingdisorders, certain somatic problems, aspects ofthe disabilities of patients with chronic mentalillness, as well as sexual and marital problems.
Treatment of depression, anxiety and stressmanagement are dealt in some detail, in thissection.
Treatment of Depression: The main treatmentstrategies used in the treatment of depressionare given in Table 21.2. Depressed patients lackin activity, have no interest and do not derivepleasure from their activities. There are a numberof reasons that can explain the low rates ofpositive reinforcement and/or high rates ofpunishment experienced by depressed patient:(1) the limited availability of immediateenvironment; (2) the lack of skill that preventsthe individual from obtaining available positivereinforcing and/or coping effectively withaversive events; and (3) a diminishment of thepotency of positively reinforcing events and/ora heightening of the negative impact of punishingevents. Thus, the first step in the treatment isaimed towards increasing activity, and increasingsense of mastery. These aims are achieved usingthe first two strategies given in the table, cognitiveand behavioural strategies.
Table 21.2: Strategies for treatment of depression
1. Cognitive strategies Distraction techniquesCounting thoughts
2. Behavioural strategies Monitoring activities, pleasureand masteryScheduling activitiesGraded task assignment
3. Cognitive-behavioural Identifying negative automaticstrategies thoughts
Questioning negativeautomatic thoughtsBehavioural experiments
4. Preventive strategies Identifying assumptionsChallenging assumptionsUse of set-backsPreparing for the future
The patient may also be urged to identify,and question negative automatic thoughts.Patient may also try to elicit automatic thoughtsby imagining in detail the distressing situations

204 Behavioural Sciences in Medical Practice
that trigger the emotional response and thenrole-playing them with the therapist, forinstance, if they are interpersonal. Testingautomatic thought by operationally defining anegative construct, reattributing it, and gene-rating alternatives is the next stage of therapy.The therapist and patient define, in operationalterms, what the patient means by a particularword or expression (e.g. failure). Once thepatient and therapist agree upon the criterionfor “failure”, they examine past evidence toassess whether the label “failure”, is indeed avalid one. The goal of this procedure is to teachthe patient to recognise the arbitrary nature ofhis self-appraisal and to make the patient moreaware of more common-sense definition of thesenegative terms.
Another technique used in the therapy is thatof reattribution, whereby patient and therapistmay review the situations in which patient andtherapist may review the situations in whichpatients unrealistically blame themselves forunpleasant events and explore other factors thatmay explain what happened other than, or inaddition, the patients behaviour. Finally, aproblem-solving approach may be adopted,whereby the patient and therapist work togenerate solutions to the problems that had notbeen considered previously.
The therapist also attempts to identify, withthe patient’s help, underlying assumptionsresponsible for automatic thoughts. Underlyingassumptions may be viewed as the rules or the“rights”, and “wrongs” of the patient in judginghimself or herself and other people. One of themajor goals of therapy is to identify andchallenge these rules, which are typicallycouched in absolute terms are unrealistic, or areused inappropriately excessively. One strategy,for example, used in testing the validity ofmaladaptive assumptions may be for thetherapist and patients to generate lists of theadvantages and disadvantages of changing anassumption and then discuss and weigh these
lists, the patient is also assigned homework tofacilitate the transfer of learning of new skills fromtherapy sessions to the home environment.
Verbal challenging of automatic thoughts isfollowed by behavioural experiments throughwhich new ideas are put to test. The practiceof preventive strategies can reduce the risk ofrelapse.
Treatment of Anxiety
Cognitive behaviour therapy aims to reduceanxiety by teaching patients how to identify,evaluate, control and modify their negativedanger-related thoughts and associated beha-viours. A variety of cognitive and behaviourtechniques are used to achieve this aim.
Identifying negative thoughts: Some patients findit easy to identify their negative thoughts at thestart of therapy. However, others require sometraining before they can confidently identify theirkey anxiety-related thoughts. Shifts in moodduring a session can be particularly useful sourcesof automatic thoughts.
Finding alternatives: The Cognitive techniquesfor identifying and then examining the thoughtsassociated with anxiety can be used to controlsymptoms, for example of panic, as well as tochallenge thoughts about the phobia. They areparticularly useful for dealing with worries aboutfuture events or anticipatory anxiety, duringwhich patients often underestimate their capacityfor coping, and over-estimate the likelihood ordisaster.
Discussing a recent emotional experience:Patients are asked to recall a recent event orsituation which was associated with anxiety andfor which they have a fairly clear memory. Theevent is described in some detail and the therapistelicits the thoughts associated with the onset andmaintenance of the emotional reaction.
Distraction: Paying attention to symptoms ofanxiety perpetuates the vicious circle, and makes

Cognitive Behaviour Therapy 205
the symptoms worse. Distraction can reverse thisprocess. This is a useful short-term strategy, butcan be unhelpful in the long-term if used as away of avoiding symptoms, or of disengagingfrom exposure. There are many distractiontechniques, most of which involve focussing onexternal factors, and many patients like to devisetheir own.
Role-play or use of imagery: When simple directquestioning fails to elicit automatic thoughts, itcan be useful to ask patients to relive the recentemotional events by either replaying it in greatdetail using imagery or, if it is an interpersonalinteraction, by role-play.
Determining meaning of an event: Sometimes,skillful attempts to elicit automatic thoughts areunsuccessful. The therapist should then attemptto discern, through questioning, the specificmeaning of the event for the patient.
Modifying negative thoughts: A wide range ofprocedures are used to help patients evaluate,control, and modify their negative thoughts andassociated behaviours. When choosing specificprocedures to use with a particular patient, thetherapist is largely guided by the assessmentinterview and, in particular, by the hypotheseswhich he or she developed about the maincognitive and behaviour processes maintainingthe patient’s anxiety state.
As an adjunct to these cognitive strategies,relaxation exercises are also used with someanxious patients.
Management of Stress/Pain: Cognitive-beha-vioural approaches have been utilised in the formof stress/pain inoculation training (Meichenbaumand Turk, 1976), to help patients manage theirpain experience. Typically, a patient wouldinitially be given information to enhance his orher understanding of the pain and the stressorsthat accompany it. The patient would then betrained in a variety of coping strategies (e.g.relaxation, distraction, imagery techniques) andfinally would be asked to rehearse these
strategies while conceptualising the pain andstress at each phase of the total pain experience.Based on such a hypothesis, illness behaviouraccordingly is seen to develop as a result of: (1)vicarious learning through models, particularlyin childhood; (2) direct social reinforcement ofillness behaviour by family, friends, and physi-cians; and (3) avoidance learning (secondary toa social skill deficit or social anxiety).
Cognitive strategies for pain management areused for all types of pain, but these have beenreported to be especially very effective inmanagement of chronic pain, cancer pain, andpsychogenic pain.
SUMMARY
Cognitive therapies are an offshoot of cognitive,and social learning theories. They imply thatpsychological disturbances stem from specific,habitual errors in thinking. These theories haveoriginated from two models, Ellis’ Rationalemotive therapy and Beck’s cognitive model.Both the models have identified irrational beliefs,which are linked to depression or any maladaptivebehaviour. Beck has proposed a cognitive triad,which involves a negative view of self, others,and of future events. This model is commonlyreferred to, in the treatment of depression.
There are two broad approaches used incognitive therapy: Covert conditioning therapiesand Cognitive learning therapies. There arevarious specific techniques used in cognitivebehavioural therapies, such as thought stopping,problem solving, distraction, identifying negativeassumptions, automatic thoughts and theirmodification, role playing, rehearsal, modelling,etc.
Though cognitive behavioural therapy haswide applications, it has been specially claimedto be very effective in the treatment of milddepressive disorders, management of anxiety,pain and stress. This form of therapy is also beingused in medical disorders, which are discussedin the next chapter.

22Behaviour Medicine
Behavioural medicine is the interdisciplinary fieldconcerned with the development and integrationof the behavioural and biomedical science,knowledge and techniques relevant to health andillness. The application of this knowledge andthese techniques are used in prevention,diagnosis, treatment and rehabilitation.
As an interdisciplinary approach this sciencedraws the knowledge and skills from a varietyof research and clinical practitioner who bringto the analysis and treatment of health-relatedbehaviour their own perspective and expertiseand collaborate with one another. It includesdisciplines such as medicine, sociology, psycho-logy, epidemiology, nutrition, biochemistry, andmany other related fields.
Behavioural medicine emphasises the role ofpsychological factors in the occurrence,maintenance and prevention of physical illness.It extends our conception of disease beyond thetraditional medical preoccupation with physicalbreakdown of organs and organ systems. To putit simply, it seeks to understand the relationshipof behaviour and biology and effectivelypromotes individual’s health. In contrast topsychosomatic medicine, which is influenced bypsychodynamic theory and biological psychiatryand emphasises the aetiology and pathogenesisof disease; behavioural medicine is influencedby conditioning and learning theories, andemphasises the treatment and prevention ofdisease.
Examination of BiopsychosocialContexts of Problems
Behavioural medicine examines the broadbiopsychosocial context of the following problemareas.
AetiologyHow do critical life events, characteristicbehaviour and personality organisation predis-pose an individual to physical illness, e.g. aperson with anxious personality are more proneto hypertension.
Host ResistanceHow are the effects of stress mitigated byresistance resources like coping style, socialsupport and certain personality traits. Personswith good coping skills can manage stressfulsituations without many negative effects on theirhealth.
Disease MechanismHow is human physiology altered by stressors,particularly those arising from maladaptivebehaviour? For instance what effects areproduced in immune gastrointestinal andcardiovascular system due to stress?
Patient-Decision Making
What are the processes involved in the choicesindividuals make with respect to matters such

Behaviour Medicine 207
as hasardous lifestyles, excessive smoking andconsumption of alcohol, seeking of health-careand adherence to preventive regimens.
Compliance
Which factors like biomedical, behavioural, self-regulative, cultural, social and interpersonal(physician-patient relationship) determinecompliance with medical advice?
Intervention
How effective are psychological measures likehealth education and behaviour modification inaltering unhealthy lifestyles and in the directreduction of illness and illness behaviour atindividual and community levels.
Techniques used inBehavioural Medicine
Behavioural medicine is not restricted to a setof techniques or particular principles to changebehaviour. A wide variety of procedures areemployed like contingency management ope-rant conditioning, desensitisation, conditioningand cognitive-behavioural approaches. Detailsof these techniques you have already read inthe previous Chapters (20 and 21). Thecommon goal of all these techniques is to alterbad living habits, distressed psychological stateand aberrant physiological processes in order tohave a beneficial impact on are individual’sphysical condition.
As you read earlier that before focussing onthe treatment programme, one needs to do adetailed assessment. It is important to takeinformation from various sources into account.The medical problems along with the compli-cations they present need to be understood. Theeffects and side effects of the medications shouldalso be understood. Assessment of the disabilitystatus can provide a feedback about motivebehind patient’s illness, (also refer to chapter onIllness Behaviour).
In behavioural medicine, some of thecommon methods used to modify behaviour aredescribed here.
Self-monitoring
This is an effective treatment strategy and itinvolves systematic observation of behaviour.The patient is given instructions to maintaincomprehensive daily record of fluctuation ofsymptoms. This helps the patient to sharpen self-observational skills and become more aware ofthe symptoms. Self-monitoring helps the patientto receive immediate feedback regarding factorsthat contribute to an increase and/or decreaseof symptoms. lt can also help the patient todevelop internal performance standards thatguide behavioural change.
Stimulus Control
In this, the patient learns to identify the cues inthe environment that foster adaptive or mal-adaptive behaviour and then alter the environ-ment and behavioural routines. The attempt isto modify behavioural routines and eliminateemotional cues that maintain behaviouralproblems. This method is especially useful intreatment of obesity, addictive behaviours andinsomnia. Many obese individuals admit that theyeat more while watching TV, so by changingbehavioural routine of watching TV, like doingsome simple activity simultaneously can breakthe habit of eating with watching of TV.
Self-control of Internal States: Both relaxationtraining and biofeedback procedures are usedto achieve self-control of internal states, likeanxiety. Relaxation exercises are known asbehavioural aspirin. These are used as basic stepin almost all problems related to behavioralmedicine. Details of Jacobson’s ProgressiveMuscular Relaxation and biofeedback have beengiven in the previous chapter.
The behavioural scientists may also use cog-nitive restructuring, behavioural counselling,

208 Behavioural Sciences in Medical Practice
contingency management, stress managementand systematic desensitisation to bring about thedesired changes.
Applications of Behavioural Medicine
Behavioural medicine techniques have beenapplied to such diverse topics as alcohol andtobacco use, exercise, AIDS, diabetes, hyper-tension, stress and immunisation. It can also beapplied to diverse health problems like cancer,heart disease, infections and pain. Some of theimportant applications of behavioural medicineare in the management of headache, chronicpain, psychophysiological disorders, insomnia,and gastrointestinal disorders.
Headache
Headaches represent one of the two types:muscle-contraction headaches and migraineheadaches. The former are thought to be dueto increased levels of tension and latter due tochanges in cerebral blood flow.
Relaxation training and biofeedback techni-ques are commonly used for the treatment ofheadaches. EMG biofeedback is generally usedfor muscle-contraction headaches and is typicallyconducted by attaching electrodes to theforehead muscles.
In case of migraine headaches, thermalbiofeedback training is used more commonly.The procedure involves attaching a sensor tothe finger. The sensor measures the blood flowto the periphery.
Cognitive behavioural therapy has also shownsome promise in the treatment of headaches.Psychosocial factors, stressful life events and dailyhassles play an important role in the causationof headache. In children headache is related attimes to negative family environment.
Chronic Pain
Chronic pain is generally described as pain thatpersists for more than 6 months and has little
likelihood of remission. Thus it is important thatpatients learn to manage pain and pain-relatedimpairment effectively. Before starting thetreatment regimen it is necessary that thoroughassessment be done. It is essential to obtain adescription of pain and its onset, evaluation ofpain-related impairment, emotional distress andmarital and vocational factors. The assessmentis aimed to identify specific activity goals andappropriateness of the patient for rehabilitation.Most benefit is obtained from rehabilitationprogramme if the patient has pain-relatedimpairment, some emotional distress and asignificant other willing to attend treatmentsessions. The answer to the question ‘why isimpairment essential?’ is that the aim of thetreatment is to get the patient to engage inactivities in spite of pain. Treatment of chronicpain involves reconditioning through physicaltherapy, exercises, cognitive restructuring,reprogramming the patients’ environment andaddressing vocational issues. The aim of cognitiverestructuring is to help the patient and significantothers set reasonable goals and limits. Theenvironmental reprogramming involves includ-ing the significant others. The significant othersare involved so that they do not undermine thetreatment by prohibiting patients from engagingin health promoting behaviours or pushing thembeyond reasonable limits.
Psychophysiological Disorders: According toICD-10 psychophysiological disorders arephysical problems that have a known orsuspected pathophysiological mechanism andmay be influenced by psychological factors.1. Asthma—is a complex disorder of bronchial
tubes, caused by hyperreactivity to variousstimuli like exercises, cold air, respiratoryinfections. It leads to difficulty in breathing.Behavioural scientists have found thatemotions and certain situations trigger asthmaattack in some individuals. It also appearsthat asthma attacks are conditionable, i.e.having an asthma attack may predispose an

Behaviour Medicine 209
individual to have another attack whenexposed again to that particular situation.
Behavioural treatment of asthma includesEMG Biofeedback and relaxation training tohelp patients overcome fear and panic.Deconditioning of stimuli thought to produceasthma attack, has also been attempted.Asthmatics are taught about self manage-ment which includes gathering informationabout the attack, what prompts theiroccurrence, and management skills. Manage-ment skills emphasise that the patient shouldavoid triggering stimuli adheres to medicationregimen, and use positive coping strategies.Mehta and Chawla (1984) reportedeffectiveness of systematic desensitisation inthe management of frequent asthma attacks.
2. Insomnia—is a subjective feeling of nothaving obtained enough sleep along withobjective verification of sleeping difficultiesand/or daytime fatigue. Insomniacs maycomplain of difficulty falling asleep, frequentawakenings during night, awakening muchearlier in the morning and inability to sleepagain.
Behavioural medicine specialists empha-sise on sleep hygiene behaviour. It includesavoidance of caffeine, alcohol before sleep,avoidance of daytime napping and main-tenance of regular sleep schedule. Patientsare instructed to use the bed for sleeping only.Relaxation and biofeedback have also beenused as treatment procedures.
3. Raynaud’s disease—This disease is charac-terised by episodic attacks of vasospasm infinger and/or toes. Due to lack of bloodflowing to the periphery, the tips becomecold. Relaxation therapy and thermalbiofeedback are carried out in an effort toincrease flow of blood to the periphery.
4. Gastrointestinal disorders—These includeproblems associated with stomach and intes-tines. Peptic ulcers, irritable bowel syndrome,ulcerative colitis and Crohn’s disease are the
most common type of gastrointestinaldisorder, which are affected by emotionalstate of the individual. The interventionincludes stress management, anxiety mana-gement, assertiveness training, relaxation andbiofeedback. The effectiveness of thistreatment in case of Crohn’s disease isinconclusive. Bowel movement biofeedbackis found to be successful in management ofCrohn’s disease.
Health Promotion
Health promotion activities aim at reducing therisk of developing disease. It includes exerciseadherence, smoking cessation, weight manage-ment, stress management, medicationadherence and AIDS prevention.
Exercise Adherence
Physical activity is recognised as an acceptedform of treatment for a variety of disorders like—diabetes, obesity, hypertension, coronary heartdisease, depression and chronic pain conditions.Individuals may begin an exercise programmebut some find it difficult to adhere to it for longduration. Behavioural medicine specialists usethe following intervention techniques for exerciseadherence:
i. have the patient monitor the amount ofphysical exercise performed and establishsome kind of reward system for completionof a prescribed amount of exercise.
ii. use feedback and social support from familymembers, friends and treatment staff.
iii. focus on identification of primaryimpediments to maintenance of exerciseand develop ways to cope with suchimpediments.
Smoking Cessation
Addiction of smoking can be maintained byphysiological, social and behavioural condition-ing factors. Behavioural strategies for smoking

210 Behavioural Sciences in Medical Practice
cessation include use of self-monitoring andadministration of rewards. Patients set a criterionnumber of cigarettes to smoke and a reward formeeting that criterion. Patients generally reducethe number of cigarettes until total abstinenceis achieved. Use of social support increases thelikelihood of change and maintenance ofcessation. Relaxation training is incorporated tocombat the physiological arousal that may resultfrom craving. Efforts are also made to eliminatethe settings associated with smoking.
Management of Stress
Stress results in illness through two mechanisms:(a) directly by the effect of stress on immunesystem and other physiological function and(b) indirectly by reducing the likelihood ofengaging in healthy behaviours such asrelaxation, reading, and increasing the likelihoodof engaging in unhealthy behaviour, such asdrinking alcohol, smoking. The aim of stress-management programmes is to teach theindividuals to cope with daily demands in aneffective manner. To help cope with physiologicaleffects of stress, individuals are taught somemethod of physical relaxation-like progressivemuscle relaxation, yoga, meditation, orbiofeedback assisted relaxation. To reduce therelative importance attributed to potentiallynegative situations, cognitive therapies are used.It may also involve training in social skills orproblem-solving (refer to Chapter 10).
Medication Adherence
Behavioural medicine specialist help in impro-ving a patient’s nonadherence to prescribedmedication. Factors that contribute to non-adherence are lack of understanding aboutmedication, need for medication, potential sideeffects and benefits of adhering to treatmentregimen (also see Chapter 17). The behaviouralmedicine specialist focusses on: (1) enhancingpatient’s understanding about the need for and
benefit of medication (2) teaches the physiciansthe strategies that will increase patient adherence.He also helps him to develop effectivecommunication patterns. This involves:(a) Explaining to the patient, the physical andor psychological problems that they have, (b) tohelp the patient accept that they have a problemthat needs treatment. No acceptance may bedue to fear or denial or other factors, (c) explain-ing the specific treatment strategies, including theside effects, intended effects, benefits of adheringand possible complications of nonadhering, and(d) lastly the patient needs to adhere to thetreatment, and he may be provided withreinforcement for complying.
AIDS Prevention
As AIDS is becoming one of the major concernsfor health workers, and prevention of AIDS ison the top priority, behavioural medicine cancontribute significantly in the achievement of thistask. In this context behavioural medicinespecialists serves as a primary health careprofessional. HIV is transmitted via certain life-style behaviours, especially involvement in unsafesexual practices and use of infected needles forintravenous drug use.
AIDS prevention efforts include use ofeducational programmes emphasising theimportance of abstinence from high-riskbehaviour. Stimulus control procedures are usedwhich focus on identification of situations thatserve as cues to engage in high-risk behaviourand making attempts to avoid these situations.Modelling may also be used, since having amodel that is perceived to be similar to oneselfmay increase the likelihood of engaging in similarbehaviours.
Type A Behaviour and Hostility Reduction: TypeA behaviour has been described as consistingof competitiveness, achievement orientation,impatience, hostility, interpersonal dominanceand control. Research has shown that type A

Behaviour Medicine 211
behaviour pattern places an individual at riskfor coronary heart disease. Behaviour treatmentinvolves some kind of character procedure tocombat the physiological effects of cardiac hyper-reactivity. It may also include marital therapy,time management, stress management techni-ques or individual therapy aimed at reducingnegative attributions.
Diabetes
Behavioural medicine research emphasises onweight reduction, diet restriction and exercise toaid in diabetic control. The role of stress andefficacy of stress management techniques incontrolling blood glucose is also being examined.It is hypothesised that stress increases the amountof glucose in the blood. Biofeedback andrelaxation strategies have been used successfullyfor the treatment of diabetes. In a diabetic clinic(AIIMS) yoga has been introduced as an adjunctto medical treatment.
SUMMARY
Behavioural medicine is the diverse fieldconcerned with the development and integrationof the behavioural and biomedical techniquesrelevant to health and illness. This knowledgeand these techniques have been applied in
prevention, diagnosis, treatment and rehabili-tation. Behavioural medicine uses a wide varietyof behavioural techniques based on conditioningboth classical and operant, and cognitivebehavioural therapies. These include relaxationprocedures, continency management desensiti-sation techniques, stimulus control, self-moni-toring. Assessment is concerned with redefinitionof symptoms in observable and measurableterms and how the symptoms are experiencedand function in the life of the individual. Beha-vioural medicine has made significant advancesin treatment of psychophysiological disorders(asthma, chronic and acute pain, headache,diabetes, hypertension), behavioural and habitdisorders (smoking,overweight, addictivebehaviours). It has contributed to preventivemedicine through identification and counter-action of health risk factors involved in smoking,stress, Type A behaviour pattern. Behaviouralmedicine identifies factors that contribute tohealth or risk of illness and develop interventionto alter’ lifestyle in direction of health. Develop-ment of health promotion strategies especiallyin AIDS prevention, adherence to medicationand exercise regimen are also part of behaviouralmedicine. As life-threatening diseases arebecoming curable, rehabilitation of patients withsuch problems can be planned on thesebehavioural principles.

23CommunicationSkills
PART 6: Applications ofBehavioural Sciences to Health
When a patient seeks medical help, the clinician’sfirst task is to ensure that he behaves in sucha manner that the patient is able to trust himand disclose why he has presented, otherwisethe clinician may not determine the true natureand extent of the patient’s current difficulties.Once the diagnosis is made, the clinician has todiscuss that with the patient and explain anyaction he plans to take. Unless he does thisadequately, the patient will probably feeldissatisfied and fail to comply with advice ortreatment.
The patient may be extremely worried aboutthe possible diagnosis, investigations andtreatment. His fears can be allayed only if theclinician is able to clarify exactly what they areand reassure him. The history, physicalexamination and investigations may reveal apotentially life-threatening or fatal illness. Theclinician has then to decide whether, when andhow to break the news to the patient and closerelatives. Failure of the clinician to correctlyidentify what they wish to know about the diseaseand prognosis may hinder their attempts to copeand lead to serious psychological problems.Doctors can discharge these important taskseffectively only if they possess the relevant skills.
Unfortunately, many do not appear to acquirethem during their professional training.
Communication skills (Hess 1969; Ivey1983) are those skills by which—• The clinician-patient relationship is created
and maintained.• Verbal information relevant to the clarification
and solution of the patient’s problem isgathered.
• The solution to the problem is negotiated.The quality of the clinician-patient relation-
ship is positively related to the communicationskills using which the clinicians keep patientsinformed about the how and why of their actions.It is necessary to establish an effective workingrelationship. Communication skills are one ofthe most important skills that a clinician musthave. It is not enough to have the scientificknowledge alone, but also the skill to bring thatknowledge to bear in the diagnosis and treat-ment of illness. Clinicians must be able to com-municate not only with the patients, but alsowith colleagues, nursing staff and administrators.Difficulties in clinician-patient communication areoften reported as a major barrier to an effectivepatient care. It has been found (Evans et al,1991), that after taking part in a communication

Communication Skills 213
skills course, medical students were more efficientat detecting the patient’s verbal and nonverbalcues. They could elicit more relevant informationfrom the patients.
A fundamental requirement for effectivecommunication is an understanding of the patientas an individual. Since most of the medicalstudents are educationally and socially differentfrom their patients, they have difficulty inunderstanding their patient’s problems. In asurvey conducted at AIIMS by D’ Monte andPande (1990), students had expressed the needfor training in communication skills especially formanagement of outpatients. The patients expectthe clinicians to listen to their complaints, toencourage them to ask about their illness andadvise about their prognosis and subsequentpreventive measures.
Fletchner (1973) emphasised that foroptimal benefit, effective communication mustdepend on clinician’s understanding of thepatient, as an individual who has an illness, ratherthan as a disease process alone. Clinicians shouldcommunicate in such a manner that it matchesthe patient’s knowledge, social background,interests and needs.
It has also been shown that better informedpatients cope better with their disease, are morecompliant to treatment, less anxious and gene-rally more functional. On the basis of the avai-lable evidence, open communication appearsto be of great benefit, giving the patient anavenue for information and support.
Components of Communication Skills
A good communication in medical practicecomprises of certain skills. A basic level ofcompetence and consideration for the patientin the following areas can enhance effectivenessof clinician patient communication.
Appropriate Physical Environment: Anappropriate physical environment should be
established to enhance privacy, comfort andattentiveness. Even in the crowded room, asuitable environment can be created byarrangement of seating, or having a curtain. Asense of privacy tends to improve the outcomeof the interview.
Greeting Patients
Greeting patients in a manner acceptable withinthe cultural norms relating to age, sex, etc. willhelp maintain their dignity and encourage theirparticipation.
Listening
This involves using both verbal and nonverbalcommunication techniques. The clinician shouldclearly indicate that he is attentive to the patient,by looking at the patient, by offering acceptanceand nods. A willingness to listen actively is bestindicated by asking open-ended questions.
Empathy, and Warmth
The clinician should also learn to show empathy,warmth, respect, interest, and support. This willalso involve being nonjudgemental in attitude.Development of these skills is dependent uponthe attitude. Clinicians should clearly signal theirinterest in how the patient’s problem is perceivedby them, how it affects their life, what their hopesand expectations are.
Language
While communicating with the patients, cliniciansshould be careful in selecting words and the useof a particular language. If the patient is illiterate,use of english language and technical wordsshould be avoided. Similarly, for educatedpatients, if very simple language is used, thenthey feel offended. Most clinicians find difficultyin explaining diagnosis and the reasoning behindit and suggestions for management.

214 Behavioural Sciences in Medical Practice
Nonverbal communication: Skills in non-verbalcommunication like eye contact, physicalproximity, and facial expression need to bemonitored with feedback to the students, to helpthem improve their interactions. This shouldconvey to the patient that the clinician is attentiveand interested.
Closing the Interview
In addition to the skills of setting up, beginningand continuing an interview, the way of closingthe interview is also important. The clinicianshould close the interview by summarising whathas been said and what has been negotiated.
Communication Skillsin Specific Situations
Core communication skills can be taught as away to improve clinician-patient communicationin medical interviews. Communications skills arerequired to express oneself, and to be able tounderstand what patient is communicating.Often patients may not be able to communicateclearly, which creates problems in history taking.To be able to cope with such difficult situations,the clinician may require higher levels ofcompetence in core communication skills, forwhich additional training may be required.
Information Gathering
A critical part of all clinician-patient interactioninvolves eliciting information from the patient.The core skills, which are needed to facilitatethe process of information gathering, are skills,which help to facilitate the patient’s involvementin the medical interview in a way that enablesthe clinician to arrive at an accurate diagnosisof a patient’s problem or symptoms.
Deficiencies in History-taking Skills: Studies ofmedical students have found that theyexperience considerable difficulty when obtaining
a patients’ history, presenting either physical orpsychiatric problem. They generally assumed thatthe problem was more likely to be organic thanpsychological, despite the psychiatric setting inwhich they were conducting their interviews.Very few students followed a predictablesequence of questions, apart from those directedat a review of the major physical systems of thebody, there was not any consistency in the waythey began, conducted or terminated theirinterviews.
There was often little connection betweenconsecutive topics and it seemed more oftenmatter of chance which areas they covered. Onlyrarely did they try to establish how any problemshad affected the lives of their patients and theirfamilies.
Similar deficiencies were found by Heifer(1970), when he used stimulated parents of sickchildren to assess the interviewing skills of seniormedical students. He noted that they usedtechniques, which hindered the collection ofrelevant information, relied on leading questions,used unfamiliar medical jargon, cut off patients’communications and neglected to pursueimportant psychological and social aspects.
Over half the clinicians used complicatedmedical words, which the mother did notunderstand. They wasted much unnecessary timethrough needless repetition or getting intounhelpful battles with the mother. Many evenfailed to introduce themselves before they askedquestions and substantial proportion wereperceived by the mothers as cold and uncaring.
This failure of clinicians to respond to cuesgiven by patients or relatives about their mainconcerns was also found in a study ofcommunications between surgeons and womenattending a breast clinic. Although most (95%)of those who had rated themselves as verydistressed on a self-rating scale just before theconsultation gave clear verbal or nonverbal cluesthat they were upset, these were heeded and

Communication Skills 215
clarified in only 5 per cent. In 20 per cent ofcases, the surgeons appeared to have realisedthat the woman was worried, but dealt with itby bland general statements such as ‘Don’tworry, there is nothing to be bothered about’or ‘we will sort it all out for you’. In the remaining70 percent, there was no evidence that they hadpicked up the cues. Only rarely did any of thesurgeons inquire directly about how the womenhad reacted emotionally to the discovery of breastdisease and possible cancer. Consequently,many of these who had been distressed beforethe clinic were just as distressed afterwards(Maguire, 1980).
The failure of clinicians to enquire systema-tically how patients and relatives are adaptingpsychologically and socially to serious physicaldisease may partly explain why so much of theassociated psychiatric morbidity, remains hidden.In a recent study of patients who underwentmastectomy for cancer of the breast, thesurgeons detected only a fifth of those who haddeveloped psychiatric problems. They alsocommonly failed to realise the extent to whichwomen were suffering pain, swelling anddisability in the arm affected by surgery oradverse physical toxicity when treated withcytotoxic drugs (Maguire, 1980).
There has been much less study of the waysin which clinicians give patients information andadvice about their disease and treatment. Evenso, there is considerable indirect evidence thatmany clinicians are equally deficient in theseskills.
Survey of patients in hospital and thecommunity reveal that many feel dissatisfied withthe amount of information they are given abouttheir condition and treatment. They commonlycomplain that they did not understand what theirclinician said to them and had insufficientopportunity to ask questions and discuss anyworries. In hospital studies, the proportionexpressing dissatisfaction with the information
given has ranged from 5 to 65 per cent (Ley,1977). For example, even insulin, which couldbe life-saving for diabetics, was found to havebeen taken in the wrong dose by half of them.Moreover, 34 per cent had no knowledge ofhow to test their urine and so had no properbasis on which to estimate the insulin dose.
Inadequate Preparation for Major Investigativeand Surgical Procedures: These deficiencies inthe explanations given to patients have beenespecially apparent in patients undergoing majorinvestigations or surgery. They have complainedthat they were not given enough informationbeforehand, and that this made them muchmore fearful than they would otherwise havebeen. It has caused some patients to claim thatthey would not have agreed to surgery, had theyfully realised what it entailed. Inadequatepreparation has been commonly given as anexplanation by patients, who fail to adaptpsychologically to major surgery such asmastectomy or colostomy.
In patients who are diagnosed as havingcancer, there is commonly a serious mismatchbetween the patient’s wish for information andthe clinician’s willingness to provide it. Still, manyclinicians debate whether to share or not to sharethe diagnosis with the patient, it often dependson their judgement of the patient’s capacity tocope rather than on the patient’s own wishes,even when these are openly expressed. Doctorsmay also go against the patient’s wish to knowby agreeing with the relatives’ request that theyshould not be told.
Motivating Patients for Compliance: Informationgiving skills described earlier, will contribute topatient compliance to treatment plans by makingsure that the patient has understood the relevantinformation about the diagnosis and proposedtreatment. Poor compliance with advice andtreatment has been linked to perception of theclinician as business like rather than warm and

216 Behavioural Sciences in Medical Practice
friendly, neglect of psychological and socialaspects of illness, lack of feedback from theclinician, poor explanation of diagnosis andfailure to meet patients’ expectations. Itrepresents a major problem in medical practice,since it renders much of the offered treatmentand advice ineffective. Some of the strategiesto enhance patient compliance are skills for thepromotion of behaviour change, since realisticcompliance with treatment plans may requirepatients to make significant changes to their diet,lifestyle or daily routine on a short-term or long-term basis (also see Chapter 17). Table 23.1 listsstrategies for promoting compliance.
Table 23.1: Strategies for promoting compliance
• Provide a rationale for behaviour change• Tailor the treatment to suit the patient’s lifestyle• Counter barriers to change• Provide examples of role models• Allow opportunities for verbal rehearsal of the treatment• Feedback (positive reinforcement of constructive
behaviour changes)• Understanding how the patient explains the illness
Preparation for Major Investigation and Surgery:The systematic provision of information andsupport to patients, who are to undergo surgeryor special investigations appears to havebeneficial effects (Ley, 1977). Egbert et al (1964)compared a control group, who received onlythe care routinely given with patients, who werealso told what pain to expect, given instructionabout postoperative exercises and visited moreregularly by the anaesthetist. The experimentalgroup recovered sooner, required feweranalgesics and was discharged earlier. In anotherstudy, Schmitt and Wooldridge (1978) comparedthe effects of routine preparative care with thoseof giving information, advice and clarifying anyworries or misconceptions. The experimentalgroup was much less anxious, discharged soonerand showed less physiological disturbance thancontrol subjects.
These and other similar studies, which havefound a positive link between preoperativepreparation and outcome of surgery, have usedseveral approaches at once. It is therefore stillnot clear, what contributions of the ability toprovide needed information and support andto clarify and correct misconceptions beforesurgery make to this improved outcome.Moreover, the beneficial effects have so far beenshown only in relation to less serious surgery.Indeed, in a recent study of the effects ofproviding advice and information beforemastectomy it was found that while the womenwelcomed this help, it did not prevent the laterdevelopment of psychological and socialproblems (Maguire et al, 1980c).
Other work has suggested that whateverapproaches are used, they should be tailoredto the individual needs of the patient. Patientswho were experiencing low levels of anxiety wereactually harmed by the presentation of a leaflet,which told them about the surgical procedureswhich were shortly to be performed. Patientswho had high levels of anxiety benefitted fromthe leaflet. Patients, who cope by not facing theoutcome of their disease and its implications,may fare less well, if forced to accept information.Those who cope best by knowing about whatis happening to them may not improve fasterif information is withheld. Skills in assessmentare clearly required, if clinicians are to determinehow patients best cope. Communication skillsshould be applied in routine practice to improvepreparation of patients before surgery.
Communicating with the Dying and Bereaved:Studies of patients dying in hospitals or at homehave found that many of their problems continueunabated because they are not recognised bytheir clinicians or disclosed by the patients. Evenproblems like nausea, breathlessness, pain,anxiety, depression and mental confusion, whichcause much distress to patients and relatives, areoften unknown to the clinicians (Cartwright,

Communication Skills 217
et al, 1973). There has been little systematicstudy of how clinicians relate to the recentlybereaved. However, it seems likely that theyoften feel inadequate when called upon to doso, especially when faced with strong feelings ofsadness or hostility and when they feel upset bythe death.
There is no doubt that many clinicians feelespecially inadequate when confronted withcommunication with seriously ill patients, esp-ecially those suffering from cancer, the dying andbereaved. They have usually emphasised the useof listening skills, clarification of the patient’sfeelings, needs and wishes, and the importanceof being alert to verbal and nonverbal cues. Thus,training in this area is very important for allclinicians.
Recent work by Hinton (1979) suggests thatwillingness to communicate more frankly withpatients who are dying leads to a reduction intheir anxiety, depression and irritability. More-over, he found that patients prefer this opennessand appeared less troubled by thoughts of dyingand more prepared to discuss it than patientswho had been spoken to less honestly. Attemptsto counsel those bereaved people who are athigh risk of developing psychosomatic orpsychiatric illness have also had encouragingresults (Parkes, 1980). They appear to reducethe risk of a poor outcome to that of low-riskgroups. Therefore, it would seem worthwhile togive clinicians and medical students more trainingin the relevant skills (also see Chapter 14).
Breaking Bad News
Few responsibilities demand more of the clinicianthan that of breaking bad news to patients. Itcalls for sensitivity, gentleness, honesty andwillingness to be available and to be vulnerable,done in the right way, it can facilitate the patient’sadjustment to his/her situation by relief ofuncertainty, in itself therapeutic, and byclarification of what must be faced.
There is also evidence that although cliniciansmay think that they have broken the news, themessage may not have been received or at least,retained by the patient. The truth may be markedby language, may be too technical for the patientto understand. Again, a single communicationmay be insufficient for a listener distracted bypain or anxiety to take in. A recent study of agroup of dying patients who were aware of theircondition revealed that only 13 per cent hadreceived the news from their clinician. Anxietyand fear generated in patients when they weregiven insufficient information, and makes a pleafor better clinician-patient communication. Thus,there is reason to believe that clinicians may notbe communicating as much to patients as theliterature suggests or as they imagine themselvesto be.
Given that the communication of bad newsis an integral part of medical practice, how doesthe student or practicing physician acquire therequisite knowledge to manage these situations?A search of the literature in the area isdiscouraging; little seems to be known about theactual process of giving bad news. There is,however, much more information concerningthe needs and wants of patients and the effectthat receiving bad news has on them.
There are at least three distinct positions onwhat information to convey to patients who havea serious illness. The first position is that patientsshould always be given full information regard-less of their individual perceptions or needs.Second view states exactly the opposite; thatunder no circumstances should patients beinformed that they have acquired a fatal disease,and that falsehood and deception should be usedif necessary, on the basis that the patient needsprotection from the terrible reality of terminalillness. A third view suggests a more flexibleapproach, with a variety of psychological andsociological factors to be taken into consi-deration, but without guidelines as to how thismight be done.

218 Behavioural Sciences in Medical Practice
In difficult situations like informing about thefatal diagnosis, the clinicians often have doubtsregarding the manner, extent, place, and time,when the clinician should communicate with thepatients. Here are some guidelines forcommunication in such situations.
What to tell? The truth if at all possible. Establishthe diagnosis by histology (e.g. malignant disease)or radiological or biochemical evidence. Try touse clear nontechnical language. Tell the truthcalmly while sitting at the same levels as theperson to whom you are speaking. Also discusstreatment options.
When to tell? When all relevant results areavailable, a full diagnosis with implications oftreatment and prognosis can be given. It maybe easier to give the diagnosis in stages; a clinicalimpression in the first stage, the results of relevantinvestigations or histology later when you havethe reports, and the operative findings once thepatient has recovered sufficiently to understand.Try to tell the patient and relatives as soon aspossible.
Whom to tell? Tell the patient but use discretionwhen the prognosis is very poor. Permit thepatient to ask questions, related to his illness,treatment, and stay in the hospital if required.He has a right to know what is happening tohim. Discuss the clinical implications of thediagnosis with the closest relatives. Reassure themthat a truthful approach will permit maximumcooperation from the patient and also justifyfuture admissions, treatments, or continuedfollow-up at hospital, etc.
Where to tell? Speak to the patient or hisrelatives in privacy not in the corridor. If in theopen ward, draw the screens and ask the nurseallocated to the patient’s care to accompany you.
Who tells? Junior resident, senior resident,consultants, or staff nurses. Every consultant hashis own policy of communicating to the patient,so it is advisable to follow his policy. Nurses are
often asked about the diagnosis or result of anoperation during the delivery of care, so theyshould be involved. After telling the patient, beprepared to talk to him again. When the initialshock has passed there may be many questions.Others may be relieved to have a diagnosis fortheir troublesome symptoms. Some may acceptthe situation without further discussion.
Communication skills to break bad news: In theabsence of formal training, it is likely that what-ever communication skills physicians haveacquired by the time they enter practice haveeither been self-taught or patterened on thoseof their clinical teachers. Opportunities to observeinstructors communicating bad news are rare.Furthermore, it is likely that these teacherslearned their skills in the same way onegeneration earlier. Considering the issues in thisperspective, it may not seem quite so unreason-able that patients do not see their physicians aspossessing adequate communication skills.
Without formal training or an awareness ofthe scientific information that exists in the area,there is little else left to do than improvise anddevelop strategies based on personal socialexperiences acquired before becoming a profes-sional. Physicians approach communication withpatients in different manner from their approachto clinical problems-solving, the latter is muchmore likely to be managed through the use ofrational strategies that depend on the consciousmobilisation of scientific knowledge than theformer. Professional communications are oftenmanaged in the same way as social communi-cations that were developed prior to professionaltraining and without reference to scientificinformation.
Strategies to communicate bad news1. Have a plan in mind before starting—The
communication of bad news is a difficultactivity and cannot be properly executed byrelying on the rules of communication utilisedin social encounters. Patients will almost

Communication Skills 219
certainly be handicapped to some degreeduring the encounter because of fear, andthe introduction of uncertainty into their lives.The patient will likely look to the physicianto provide support and guidance to a greaterdegree than usual. Indeed, a few patients mayrequire very directive advice until they regaintheir equilibrium. Emotions are contagious,and intense emotions interfere with clearthinking. In the face of a very upset patient,the physician who has not thought throughhis management plan before introducing thebad news begins to feel the pressure of havingto solve problems as well as attend to adistressed patient. Having a set of generalrules about how to manage communicationof bad news and having tentative manage-ment plan for the specific problem beforebeginning the process, leaves the physicianfree to deal with what happens in the hereand now, rather than having to think aboutroutine matters. It is however, probably veryimportant to provide the patient with amanagement plan of some kind during anencounter in which bad news is broken.Recent evidence suggests that health-relatedproblems favour emotion-focussed coping,and that situations assessed as unalterable—or where no action can be taken—also favourthis kind of response.
2. Give the patient control over the quantityand timing of the information he receives—Even the patient who wants to knoweverything usually does not want to hear itall at once. A strategy commonly used byexperienced physicians is to start thecommunication with very vague terms andbecome more specific as the patient asks formore information. It is also important to tailorinformation to each patient’s concerns,knowledge and experience, because thisreduces the risk of causing unnecessary worryor discomfort. A patient who is told he has
a carcinoma of the transverse colon, mayhave more concerns about having acolostomy than having cancer per se. It isonly by asking the patient about his specificconcerns that this can be determined.
3. Allow the patient time to integrate infor-mation—Even in situation where non-fatalillness is being discussed, there is a limit tothe amount of information that patients canincorporate at any given time. As theseriousness of the illness becomes greater, sodoes the potential impact on the patient,which in turn will diminish the individual’sability to hear and incorporate new infor-mation.
4. Soften the bad news with good news byproviding some hope—Patients want and areappreciative of any information that provideshope. Certainly, the more advanced thedisease the poorer the prognosis, but no onecan be sure which patient will do well in spiteof the severity of the disease. For eachindividual, the distance between being andnot being on this earth in infinite. Makingthe journey from immortality to mortality ispainful and takes time. One of the commonlyused mechanisms to better this process isdenial, which is an essential and normaladaptive mechanism under certain circum-stances. It can buy time and comfort for thepatient while he completes his underlyinggrief work and is thereby better able toconfront the realities of the situation.Supporting a patient’s denial while he isincorporating bad news may be not onlyhumanitarian, but also constructive.
5. Never tell the patient a falsehood—Patientsneed information to make intelligentdecisions about their own treatment, but theydo not need to know all the details aboutthe course, the prognosis of their disease todo so. Patients also need more generalinformation about their illness and how it

220 Behavioural Sciences in Medical Practice
might affect them, so that they can plan forthe future.Every patient physician and situation isdifferent. The flexible use of any strategy willbe the only appropriate basis on which toapproach the problem. The communicationof bad news will never be pleasant, but itcan be rewarding for the physician whoknows that his planning, and his communi-cation skills have made the situation a littleless unpleasant for the patient.
Communication in OtherImportant Situations
In a document prepared by WHO, there is alist of special situations where communicationskills play a very important role. These are:1. Special groups of population: with language
and cultural differences, with families orcouples.
2. Special groups of disorders: disabled (blind,deaf, paraplegic, etc.), mentally retarded,chronically ill, terminally ill, depressive and/or suicidal patients, AIDS, STDs, chronic pain,speech impediments, problems of addiction,somatoform disorders, neurotic disorders.
3. Special personality problems: noncoperativepatients, hostile patients, overdependentpatients, inhibited patients, overdefensivepatients.
4. Special clinical situations: giving bad news,dealing with sensitive issues (sexual, etc.),telephone contact, preparation for threaten-ing diagnostic, treatment procedures, vaginalexamination, surgery, etc. when speaking toothers (e.g. relatives) about a patient.
Assessment of Communication Skills
Assessment of communication skills comprisesan evaluation of the student’s:1. ability to understand his patient;2. ability to communicate his view point to the
patient and his family members;
3. ability to explore and answer patient’squestions keeping in mind the patient’s frameof reference which includes the psychologicalconnotations of patient’s complaints, hiswishes, expectations and fears, i.e. everythingthat patient has thought and felt about hisproblem.
4. ability to propose solution to the problemsand to motivate patients for compliance withtreatment.Assessment of communication skills has the
dual function of educational feedback for thestudent and evaluation of his skills or perfor-mance. Ideally, the assessment should be linkedwith the teaching of communication skills. Thecontext in which communication is to take place,should be kept into consideration during theassessment.
The commonly used strategies to assesscommunication skills are as follows:1. Observation in routine setting, e.g. during
clinical rounds.2. Observation in a structured situation: 10-15
minutes interview session on a preselectedtopic; a checklist can be prepared to assessthe various components of communicationused/unused by the candidate.
3. Listening triad: A role-play exercise in which3 students take the role of clinician, patientand an ‘observer’. The observer records theensuing interviews, which form the substancefor discussion and feedback.
4. In many Western Universities, closed circuitTV monitors are used to assess the mannerin which a student interviews the patient. Inour set up, use of this method would requirefew years to become feasible.
5. Communication skills have also been assessedthrough OSCE (Objective structured clinicalexamination) stations. OSCE may be usedto gather specific information from thepatient, or telling mother the advantages ofbreastfeeding to her newborn child.Simulated or real patients may be used in

Communication Skills 221
the OSCE stations. The assessment can beobjectivised using a rating scale or a checklist.
6. Students may be asked to maintain a ‘logbook’, recording write-up of the variousexercises and activates related to communi-cation. This is constantly supervised by theteaching staff.
7. The students may view the videotape of aninterview situation and point out or answerto the specific questions, such as nonverbalbehaviour of the patient.
SUMMARY
Communication is an act of imparting knowledgeor exchanging thoughts, feelings or ideas byspeech, writing or gestures. Communication inmedical practice means interaction between twopeople—the clinician and the patient. lt isrecognised that in some hospitals the amountof time a patient clinician have in contact witheach other is extremely limited. Constraints mayalso include lack of space and lack of privacy,with number of patients crowding a room orcrowding around the clinician’s table. Doctor-patient communication skills can help a clinicianbe more efficient and effective particularly whensuch constraints exist. Using communication skillsand being innovative can enhance the outcomeof the consultation, e.g. using a curtain/screen,
or a specific chair to single out the patientcurrently being seen, focussing full attention onthat patient, using appropriate nonverbalcommunication, and clarifying comments. Onemay have to priorities patients for additionalinterviewing and call them back at a more con-venient time. More effective use of parapro-fessional staff may promote better communi-cation.
Components of communication skills include:appropriate physical environment, greetingpatients, listening, empathy and warmth, respectand interest, language, nonverbal communi-cation and closing of the interview. Communi-cation is used for gathering information, but thestudies have shown lots of deficiencies in historytaking due to lack of communication skills.
There are specific situations in which com-munication skill are necessary, some of thesesituations are: motivating patients for treatmentcompliance, talking to seriously ill, dying patientsand bereaved, preparing patients for majorinvestigations, patients with specific disorders likesuicidal, depressed, breaking bad news to thefamily. Special training and use of strategies canbe helpful in developing these skills.
Assessment of communication skills can behelpful to students in providing feedback toimprove upon these skills.

24Illness Behaviour
A 50-years male patient is admitted with GIbleeding. On detailed examination, it is observedthat this patient has multiple painful disorderslike arthritis, diabetes, chronic renal failure, yetthis patient is very calm and does not complainof distress or pain. You find him cooperative andhis compliance to treatment is good.
A forty-five-year-old male has a minor injuryon left leg, he is screaming with pain. He ispreoccupied with his injury, and demands fullattention from his wife and children. He doesnot even look after his personal care and is alsofed by his wife.
These two cases illustrate the extreme typesof behavioural response to illness often encoun-tered in clinical practice. There would be manypatients responding in between these two extre-mes of behaviours. Responses to symptoms andillness can vary considerably in individuals. Illnessbehaviour is the manner in which personsmonitor their bodies, give meaning to theirsymptoms, and their perceptions of the illness.This has implication on utilisation of varioussources of help and health care system. Whenresponse to illness is disproportionate to theextent of symptoms or illness, a maladaptivebehaviour is presumed. This chapter will helpyou to understand variations in illness behaviour,how an individual develops an abnormal illnessbehaviour, its modification and preventionstrategies.
Illness Behaviour
The concept of illness behaviour, according toMechanic (1978), refers to the ways in whichan individual perceives, evaluates and reacts totheir symptoms. Pilowsky (1977) has definedillness behaviour as ‘the way in which individual’sreact to aspects of their own functioning, whichthey evaluate in terms of illness and health’.Illness behaviour also refers to any behavioursthat involves help seeking and contact with healthcare provider. As the help seeking behaviour isdifferent amongst patients and can influence thetreatment, so it is important to understand thevariety of responses to illness—both normal andabnormal. Understanding the nature of humanbehaviour in health and disease has greater utilityin clinical practice as no two patients respondto their illness in the same manner. By under-standing the patients’ interpretation of illness,his fears and anxieties associated with hisinterpretation of the illness can be reduced.There are several determinants of help seekingbehaviours. These are related to perception ofthe symptoms, individual needs, available alter-nate interpretations of the symptoms, treatmentavailability and cost. Mechanic has described twodifferent levels at which the determinants canoperate—‘other-defined ‘and ‘self-defined’.Other-defined refers primarily to situations inwhich other people evaluate the person’s illnessbehaviour. Like how family members and close

Illness Behaviour 223
associates evaluate abdominal pain in a six yearsold child. Usually, others defined is applied tochildren and people with major psychiatricproblem. Self-defined refers to situations in whichthe individual perceives and evaluates his or herown symptoms. When self-defined and other-defined levels differ significantly, then theconcerned individual may be forced intotreatment. The expression of illness behaviouris both influenced by cultural patterns or normsand social learning at home.
Sick Role
The sick role, a related term was formulated byParsons (1964). This involves an exemptionfrom normal duties and obligations, providedthat the sick person is neither responsible for hisdisability nor able to terminate it by an act ofwill. Pilowsky (1978) has defined illness as a ‘stateof the organism which fulfils the requirementsof an appropriate reference group for admissionto the sick role’. An appropriate reference groupmeans that group, which is most able or willingto meet the social cost of the illness. Disease onthe other hand, is the constellation of objectivedata, which doctors believe, ought to qualify asan illness. Illness is characteristic of an individualwith distinct social significance.
Whenever a person cannot fulfil social rolesadequately, he can adopt a sick role, e.g. whena person is not able to work, by adopting sickrole he gets an excuse from the society for notworking. There are four basic components tothe sick roles:1. Absence of responsibility—The patient’s
inability to perform social roles is notconsidered to be under that person’svolitional control, he needs some treatmentor curative process before he can engage inexpected social roles.
2. Exemption from performing social roles—The type of exemption depends on theseverity and nature of the illness. The person
suffering from cancer has different exemptionof social roles, as compared to person havingdiabetes.
3. Being sick is undesirable—So, the person isobligated to seek help and cooperate withothers to recover. He has a responsibility ofgetting well as soon as possible.
4. Seeking adequate help—The personadopting the sick role must seek out andcomply with the prescribed treatment.The sick role gives the possible benefit of
exemption from role obligations but in return,the person is expected to recover by seekinghelp and complying with treatment. At the onsetof illness, the individual may adopt the sick roleby resting and not performing his social roles.But if the illness is prolonged, it gradually affectsother family members, children, friends andwork associates. These other people also playa very important role in granting the sick role.Illness behaviour also includes the ways in whichindividuals react to aspects of their own function-ing, which they evaluate in terms of health andillness. In our Indian context, these factors playa very important role, as family members tendto overprotect and encourage sick role.
Abnormal Illness Behaviour
Abnormal illness behaviour is diagnosed whenindividual illness behaviour does not follow thesocially accepted sick role process. These aregenerally psychiatric illness where no apparentorganic cause is present or in cases in which thesick role is no longer adaptive. These disordersare generally labelled as somatoform disorders,conversion reaction or hypochondriasis.Pilowsky had classified abnormal illnessbehaviour (AIB) as “illness affirming” and “illness-denying syndromes”. Both of these categoriesare important as in illness affirming, the patientbecomes convinced of the disease underlyingthe disorder, e.g. for persistent cough patientassumes that he has tuberculosis or cancer. In

224 Behavioural Sciences in Medical Practice
contrast, patients with ‘illness denying’ type,minimise or negate the existence of a significantillness. A patient with heart attack presumes thatthe chest pain was due to gastric upset. The otherfactors important in classification are motivationfor AIB, which could be conscious or unconsciousin both the illness affirming and illness-denyingcategorists.
Causes of Maladaptive IllnessBehaviour
Why some individuals react to illness in anadaptive manner whereas others react in a mal-adaptive manner depends on various factors.These factors generally originate from interactionbetween personal and environmental factors.Some of the important causes of maladaptivebehaviour are disposition, sociocultural, psycho-dynamic and social learning (Fig. 24.1).
Fig. 24.1: Factors influencing illness behaviour
Disposition
Some patients seek care readily for even minorsymptoms; others are reluctant to seek care foreven life-threatening illnesses. There can also beconsiderable variability in an individual’s res-ponses from one situation to another and overtime.
Illness behaviour is related to patient’sappraisals of their symptoms, the assumptionsthey make about causes, and responses tomedical advice are conditioned by patientsunderstanding of their bodily responses. Studiesconsistently demonstrate major inconsistenciesbetween physicians’ expectations and assump-tions and patients’ responses, resulting in poor
communication and difficulties in treatment.Leventhal and his colleague (1985) found, forexample, that while physicians assume thatpatients with hypertension cannot make judge-ments of their blood pressure, many patientsfeel confident in their abilities to assess when theirblood pressure is high or low, and they adjusttheir treatment regimens accordingly. Knowingthe physicians view, they withhold communi-cating their assumption or information aboutmodifications or regimen. Understanding illnessby patient’s perspective offers potential forimproved communication and more appropriatetherapeutic instruction.
The variability in patient behaviour in a givensubculture despite similarity of symptoms alsoreflects major differences in psychologicalorientations and predispositions.
At a simple level, people vary in their tole-rance for discomfort, the knowledge, informationand understanding they have about the illnessprogress, and the specific ways bodily indicationsaffect needs and ongoing social roles. Peopleseem to vary great deal in their subjective res-ponse to pain and discomfort, although thereappears to be much less difference in physicalthresholds.
Sociocultural Influences
The extraordinary differences among culturesand characterisations, illness conceptions ofcausation, and modes of treatment are substan-tially documented in the anthropological litera-ture. Even in modern populations, one finds ablend of sophisticated scientific ideas and folkwisdom. Such cultural content affects the recog-nition and conceptualisation of symptoms, thevocabularies for communication, modes andcontent of expression, and the range of remedialefforts attempted.
Sociocultural influences on illness behaviourare transmitted through families. The expressionof illness through psychological and social

Illness Behaviour 225
vocabularies is a relatively modern phenomenoncoexistent with growth of personal self-awarenessand broad self-expression.
Psychodynamic
According to psychodynamic view, conceptuali-sation of illness behaviour relates to an uncons-cious gratification and measuring for bodilysymptoms and physical suffering. The symptomsand suffering can represent (1) an alternativechannel to deflect sexual, aggressive, or oraldrives or (2) an ego defense against guilt or lowself-esteem (Nemiah, 1980). Physical sufferingcan serve as a defense against guilt, providingwell-deserved punishment for past wrongdoing.Support for these mechanisms is searched forin the early developmental stages of life, andsuch factors as parental care during illness oridentification with a chronically disabled siblingor parent are important candidates for research.
Social Learning
Illness behaviour represents a complex set ofbehaviours that evolve and are maintainedthrough learning processes like modelling andreinforcement. The social learning model gene-rally conceptualises chronic illness as a functionof two major factors: the consequences of illnessbehaviour and the premorbid state of the indi-vidual. In terms of the consequences ofbehaviour, the concept of reinforcement orsecondary gain is crucial. The patient, whoadopts or develops the illness behaviour pattern,may receive environmental support for thiscontinuing disability or sick role. Another majorhypothesis that the social learning modelproposes is that abnormalities in the individualsbefore the report of the symptoms or disordermay play a role in maintaining the illnessbehaviour. That is, the premorbid state of theindividual or his or her behavioural style mayaffect the types of illness behaviour the individualsubsequently engages in. A common clinical
observation with patients experiencing chronicdisability uncorrelated with organic disease is thatthese patients very often lack the social skills thatwould assist in facilitating recovery.
Cognitive perceptual abnormalities have alsobeen suggested as the cause of abnormal illnessbehaviour. These possible mechanism areindicated by: (1) patients amplify and augmentnormal bodily sensations; (2) patients mis-interpret bodily symptoms of emotional arousaland normal bodily function; and (3) a constitu-tional predisposition to think and perceive inphysical and concrete terms in contrast toemotional terms, setting the stage for symptompreoccupation. According to Barsky andKlerman, these mechanisms suggest thatperceptual defect is the primary underlyingdisorder, not the illness behaviour itself.
Psychosocial Adaptation to Illness
Physical illness is perceived as a stress andindividuals differ in their ability to cope up withstress. Physical illness is considered as a majorlife crisis that causes physical and psychologicaldisorganisation. A crisis should be resolved inshort life span, as any illness makes the individualsensitive he loses key life roles and undergoeschanges in appearance and bodily functioning.He may feel helpless and develops unpleasantfeelings as anger, guilt and at times, depression.
Adaptation to illness depends on back-ground, personal characteristics, factors relatedto illness, and physical and social environment.The patient and his family face special problemsrelated to illness like dealing with pain, then theyhave to adjust to hospital environment and haveto develop relationship with the doctors andnurses. The patient has to cope with aversivetreatment like frequent pricks, waiting for andundergoing investigations, etc. Many patients donot express their feelings of sadness, anger andhopelessness; they keep these feelings tothemselves but it is manifested in their behaviour.

226 Behavioural Sciences in Medical Practice
Family members also do not know how to helpthe patient to overcome these feelings. Thepatient needs to achieve a reasonable emotionalbalance, perception of an adequate self-imageand feeling of competency. During serious illness,social support to the patient and the family isimportant. It helps the patient to recover fasterwith less medication.
During illness, various individuals use differenttypes of coping strategies, these may be adaptiveor nonadaptive. Moos and Tsu (1977) havedescribed several types of coping skills. Theseare: (1) denying or minimising the illness, e.g.heart attack is taken as gastric problem by thepatient, (2) seeking relevant information, e.g.learning about the seizures/cause and course ofa renal failure, can help the patient feel morein control and know better what to expect,(3) seeking reassurance and emotional supportfrom family, friends and health care professio-nals. Some patients join special group, nationalgroup for haemophiliacs, cancer, alcoholicanonymous, (4) learning specific illness relevantprocedures, setting concrete goals, rehearsingalternative outcomes and finding a generalpurpose or pattern of meaning are also skills thatcan help patients to cope with their illness.
The journey to recovery is influenced bymany factors like age, intelligence, beliefs, pastcoping experience, and personal characteristicsof the individual patient. Religious beliefs are verycrucial in Indian culture as a source of coping.Developmental factors should be considered incase of child patients.
Besides providing the medical/surgical illness,it is critical to evaluate the biopsychosocialenvironment of the patients, an individualassessment to understand the particular patient,is mandatory to develop a good doctor-patientrelationship understanding and application ofthese factors help in speedy recovery and canprevent many consumer protection problemsfor the physician.
Management of AbnormalIllness Behaviour
Abnormal illness can be modified by psycho-logical techniques. The use of cognitive thera-pies in the modification of illness behaviour isbased on the rationale that faulty or irrationalpatterns of thinking modulate maladaptiveemotions and behaviours. Wooley, Blackwell,and Winget (1978) reported a treatmentprogramme that focussed on enhancing thepatient’s ability to take independent action incoping with his or her illness. Wooley et al (1979)targeted specific goals to alter a patient’s illnessbehaviour. These goals included (1) having thepatient assume responsibility for his or her care,(2) decreasing the care-taking response byothers, especially physicians and family members,(3) altering the social contingencies thatsupported illness behaviour, (4) decreasing thefrequency of complains throughout hospitali-sation and increasing achievement orientation,and finally, (5) collecting one-year follow-up dataon the generalisation of success from target tonontarget behaviours. The treatment pro-gramme emphasised the elimination of socialreinforcement for illness behaviour (throughgroup therapy) by teaching the patient techni-ques directed at reducing physical symptoms(e.g. relaxation, distraction, biofeedback, andself-control programmes), initiating therapydirected at helping family members reconstructthe learning process that led to the developmentof illness behaviour in the patient, and establish-ing contingencies to support the patient’semerging sense of autonomy and independence.Anxiety and depression is often seen as a mani-festation of illness behaviour, and chronically illpatients may show many of the features of amajor depressive episode.
Rational emotive behaviour therapy isaimed at helping the patient identify irrationalthoughts or beliefs that have self-defeating orself-destructive consequences and testing or

Illness Behaviour 227
challenging these beliefs in therapy sessions andin actual extra therapeutic situations (Ellis, 1977).This heightened perceptual sensitivity to bodilysensations, and their subsequent misinterpre-tation by the patient, may lead the patient tobelieve that he or she is the victim of somedisease process (e.g. stomach cancer). Such aconviction may often precede the developmentof illness behaviour. Rational emotive behaviourtherapy, therefore, would focus on the therapistfirst eliciting the precipitating external stimulusevents, then determining the specific thoughtpatterns (and underlying beliefs) that constitutethe internal response to these events thatgenerate negative emotions (e.g. anxiety,depression), and finally helping the patientmodify these beliefs and thought patterns.
Lewinsohn et al (1982) have providedguidelines for implementing a treatmentprogramme that attempts to assist the patientin (1) decreasing the frequency and thesubjective aversiveness of unpleasant events inhis or her life and (2) increasing the frequencyof pleasant events in his or her life. The five stepssuggested in accomplishing this goal include(a) daily monitoring of unpleasant and pleasantevents, (b) relaxation training, (c) managingaversive events, (d) time management, and(e) increasing pleasant activities. The treatmentprogramme is presented to the patient asproblem solving, task oriented, and education.Compliance with the programme is facilitatedthrough the use of contingency contracts, andan effort is made throughout treatment to keepthe intermediate goal meaningful and specificfor the therapist and the patient. The final stageof the treatment programme involves thetherapist and patient planning tactics that wouldhelp the patient resist the pressure of the oldenvironment and facilitate the practice of newskills. In order to gradually fade out therapistsupport and to assist the patient in an easiertransition to the home environment, sessionstoward the end of the treatment programme
are spread out over several weeks. This latterapproach is a common procedure in clinicalbehaviour therapy.
The patient is faced with the task of adaptingto the numerous changes in his or her socialand physical functioning. Moos and Tsu (1977)have delineated a model of coping with chronicillness, in which psychosocial intervention maybe beneficial. These psychosocial interventionsmay be targeted at helping the patient both withillness related and general adaptive tasks. Oftenin the context of medical settings, psychosocialteams are consulted (consultation-liaison teams)to facilitate the patient’s coping within thisframework. Such an approach is believed toserve as a preventive measure for further medicalcomplications, as well as the occurrence of illnessbehaviour.
At times, some additional procedures mayalso be used in the management of maladaptiveillness behaviour. These techniques are primarilyrelated to decrease anxiety or stress and toenhance social and interpersonal skills. Thefamily should be included in the managementprogramme because many maladaptive illnessbehaviours are reinforced and maintained bythe family members.
Clinical Applications
The different perceptions, evaluations andresponses to illness have, at times, dramaticimpact on the extent to which symptoms interferewith usual life routines, chronicity, attainment ofappropriate care and cooperation of the patientin treatment. Variables affecting illness behaviourusually come into play well before any medicalscrutiny and treatment (Mechanic, 1978a).
An illness behaviour model permits thecompatible integration of current social andbehavioural science concepts regardingindividuals as social organisms. It also allows forthe future incorporation of new information ofthe interaction between biological state,

228 Behavioural Sciences in Medical Practice
psychological processes and social functioning.As these aspects of illness behaviour areconsidered an equally important dimension, withnone having a prior superiority in understandingthe nature of human behaviour in health anddisease. An illness behaviour model may havegreater utility for present and future interdis-ciplinary research, education and clinical practicethan that which exists at present.
Illness behaviour is a dynamic process inwhich the sick person defines problems, struggleswith them, and attempts to achieve a comfortableaccommodation. Such processes of adaptationare partly learned and partly shaped by the socialsituation and influences in the immediateenvironment. The health professional thus canhelp to guide the process by suggestingconstructive alternatives for the patient and byavoiding the reinforcement of distorted meaningsand maladptive responses.
SUMMARYIllness behaviour is a dynamic process in whichthe sick person defines problems, struggles withthem, and attempts to achieve a comfortableaccommodation. Illness behaviour involves themanner in which persons monitor their bodies,define and interpret their symptoms, take reme-dial action and utilise various sources of help.Whenever a person cannot fulfil social rolesadequately, he can adopt a sick role, e.g. whena person is not able to work, by adopting sickrole he gets an excuse from the society for notworking. The basic components to the sick roleare: (1) absence of responsibility, (2) exemptionfrom performing social roles, (3) being sick isundesirable, and (4) seeking adequate help.
Abnormal illness behaviour is diagnosedwhen individual illness behaviour does not follow
the socially accepted sick role process. Illnessexperience is shaped by disposition of the patient,sociocultural and social-psychological factorsirrespective of their genetic, physiological andother biological bases. Psychodynamic and sociallearning also influences illness behaviour.
Cultural definitions, social development andpersonal needs shape the experience of illnessand meanings attributed to physical factors thatserve as its basis. While magnitude, severity,persistence and character of symptoms all effectand establish limits for personal and socialdefinitions, there is great variability in what isperceived, how it is defined, the interventionsthat are considered and used, requests forsupport and special consideration and illnessoutcomes.
Physical illness is perceived as a stress andindividuals differ in their ability to cope up withstress. Physical illness is considered as a majorlife crisis that causes physical and psychologicaldisorganisation. A crisis should be resolved inshort life span as any illness makes the individualsensitive, he loses key life roles and undergoeschanges in appearance and bodily functioning.He may feel helpless and develop unpleasantfeelings as anger, guilt and at times depression.
Abnormal illness can be modified bypsychological techniques. The use of cognitivetherapies in the modification of illness behaviouris based on the rationale that faulty or irrationalpatterns of thinking modulate maladaptiveemotions and behaviours.
The different perceptions, evaluations andresponses to illness have, at times, dramaticimpact on the extent to which symptoms interferewith usual life routines, chronicity, attainment ofappropriate care and cooperation of the patientin treatment.

25Psychology of Pain
Try the following experiment in your class. Ask10 students to prick their left index finger witha fine needle. Observe each student’s facialexpression and rate intensity of pain experiencedby all the five. Some students would prickwithout feeling much pain, whereas some mightscream and may not even prick the finger. Afterthe prick, again observe the different behavioursof these students. Some may report pain longafter the prick, others may keep looking andpressing the finger, yet others may not evenbother about the prick. These differences in paincan be understood by learning psychology ofpain.
Pain varies greatly in terms of duration,severity, quality, and the degree to which it inter-feres with adaptive functioning. There are severalpatterns of pain: pain may be acute, chronic-periodic, recurrent, chronic intractable-benign,or chronic-progressive (Turk, Meichenbaum andGenest, 1983). This differentiation is importantbecause the pattern of pain may provide helpfulinformation in formulating hypotheses regardingmechanisms involved in the development,exacerbation, and maintenance of the painproblem, and the pain pattern also relates tointervention planning.
Not all individuals suffering with chronic orrecurrent pain find it impossible to cope withpersistent pain. Many individuals are able toaccept and cope with such disorders as arthritis,migraine, and back pain without abuse of
medication, invalidism, and overuse of the healthcare system. Others however, develop a complexcluster of symptoms independent of the type ofpathophysiology. These individuals display aconstellation of problems, including personal andsocial difficulties as well as patterns of health careuse that are quite consistent across pathologies.This cluster of problems has been called thechronic pain syndrome.
The recognition of the important role thatpsychological and social factors play in themaintenance of chronic pain complaints, has ledto the systematic investigation of the utility ofpsychosocial parameters as predictors of treat-ment response in a wide variety of chronic painconditions, and with different pain treatments.
It is commonly observed that chronic painpatients vary widely in their level of psychologicaland behavioural dysfunction. All too often,chronic pain becomes associated withpsychological distress, especially depression(Romano and Turner, 1985); martial difficulties(Maruta et al, 1981; Ahern et al, 1985),vocational dysfunction, decreased ability toperform normal activities. Yet some chronic painpatients do continue to work, have minimaldisruption of normal activities, and are notclinically depressed.
Now there is evidence that how a patientappraises and copes with his pain problem hasa major impact on his psychological distress andphysical disability. If causal relations between

230 Behavioural Sciences in Medical Practice
certain now pain-coping strategies and physicaland psychosocial adjustment can be identified,then treatment programme can work withpatients to increase the use of adaptive strategiesand decrease the use of maladaptive copingefforts.
Gate Control Theory
Pain signals can be altered by a variety ofpsychological processes as they are transmittedwithin the nervous system. Pain is more thana simple transmission of sensory signals from apain source ascending the spinal cord to thebrain. Rather, it is the net result of a series ofcomplex interactions of neurophysiological andneurochemical processes permitting such psyc-hological processes as motivation, emotion, andcognition to modulate the pain experience.Melzack and Wall (1965) proposed a model thathelps to explain the role of such psychologicalfactors in CNS modulation of pain. The gatecontrol theory of pain has had a profoundinfluence on the conceptualisation and treatmentof pain over the past two decades. It has beenparticularly important in stimulating interest inempirical research on psychological processes inpain and the use of psychological techniques inpain management. It has emphasised the needfor the use of an integrative psychobiologicalapproach to theory and practice in the area ofpain and pain control.
Physiological and PsychosocialModels of Pain
Scientists have proposed various models tounderstand pain perception and tolerance. Initialattempts to understand pain were mainly froma physiological perspective. Later models haveincluded the psychological or experiential aspectsin modelling the human experience of pain.
The specificity model, or stimulus responsemodel, was one of the original theories
proposed. This model claimed that whenperipheral sensory receptors are stimulated asa result of injury to the body, nerve impulsestravel through the spinal cord to the brain. Theintensity of pain is assumed to be a directreflection of the activation of ‘pain receptors’.Various treatment techniques that followed thismodel were effective for acute type pains, butnot chronic pains.
The learning theory of pain distinguishesbetween the initial psychological reaction to apainful stimulus and the resultant behaviours.Respondent pain behaviours are actions thatresult from the actual nociception. Operant painbehaviours are actions that develop when thepain experience is linked to forms of reinforce-ment such as receiving pain medication, orattention, or being allowed to avoid unpleasantsituation. The reinforcements encourage the painbehaviour to linger on and become separatedfrom the original painful stimulus. If respondentpain behaviours last long enough, learning willoccur and behaviours will then be controlled bythe operant pain behaviours. In chronic pain,both respondent and operant pain behavioursmay exist. Certainly, learning theory cancontribute much to our understanding of cross-sectional (birth cohort) differences in responseto stressors, including pain.
It is the psychological aspects of pain that addscomplexity to understanding pain mechanismsand is an area of current debate. Pain may beginwith the noxious stimulus that can lead to tissuedamage, but it does not stop there. There alsois cognitive appraisal of the stimulus as well asevaluation of the context in which the stimulusoccurs. Finally, there is the affective dimensionof pain.
Recently one pain model proposed thatthe affective dimension of pain is composed oftwo stages. The first of these stages is relatedto the immediate unpleasantness of the pain.The second is dependent upon subsequent

Psychology of Pain 231
ramifications of experiencing pain that arestrongly influenced by subject variables.
According to Loeser (1982), the pheno-menon of human pain can be divided into fourcategories: nociception, pain, suffering and painbehaviour. Nociception is the detection of tissuedamage by transducers in the skin and deeperstructures. Pain is the perception and interpre-tation of the nociceptive input by the highestparts of the brain. Suffering is the negative res-ponse to pain or to other emotion-laden eventssuch as fear, anxiety, isolation, or depression.Pain behaviour is what a person says or doesor does not do or say, which leads the observerto infer that the patient is suffering from pain.
The literature that addresses the psycholo-gical aspect of pain primarily examines peoplewho experience chronic pain, as opposed toacute pain. Regardless of the classification, painthat persists can inhibit the person’s functionalcapacities, emotional state, psychological con-dition, and socioeconomic status. The longer aperson experiences chronic pain, the more thepain is likely to affect the psychological and socialfactors. Psychological conditions that are oftenfound in people with chronic pain includedepression anxiety, adjustment disorder,dysthymia, and personality disorder. For peoplewith chronic pain of an organic nature, it isestimated that 20 to 40 per cent have majordepression and 40 per cent have dysthymicdisorder. Furthermore, the cause-effect rela-tionship between pain and depression may goin either direction. Being depressed may leadto higher levels of pain, and high levels of painmay cause a person to become depressed.
People who have an internal Locus of Control(LOC) believe that they can affect theirexperiences/outcomes by their own behaviour.Studies have shown that chronic pain patients,who have external LOC as perception of pain,are more depressed than are those people withinternal LOC (Skevington, 1983). In addition,locus of control in patients with chronic pain is
significantly correlated with the use of pain copingstrategies and psychological distress. People withmore external or chance LOC are more likelyto have increased pain and functional impair-ment because of ineffective use of copingstrategies and avoidance of activity. Beingsensitive to individual differences in personalityfactors may be beneficial in both the assessmentand treatment of pain.
How pain perception affects the person’sfunctional abilities. Research on people withspinal cord injuries has shown that the amountof distress associated with pain, is correlated tothe extent to which the pain interferes withexpected functional activities. Comparingparaplegic patients and quadriplegic patients withsimilar levels of chronic pain, paraplegicsperceived the pain as more unpleasant ordisturbing than did quadriplegic. This may reflectthe greater potential for self-care in relation tofunctional activities among paraplegic. Inanother study of the effect of pain associatedwith menstruation, it was found that pain-relatedemotional distress was positively correlated withthe perceived inference with functional activities.
Another factor that has been found to affecta person’s pain experience is social support.Overall, the presence of social support is viewedas beneficial for recovery, rehabilitation, andadjustment to chronic disease. Research on theinfluence of social support on pain behaviourhas demonstrated interesting results. Thenumber of people available for support was nota significant factor, but the level of satisfactionwith the support did influence pain behaviourof chronic pain patients. People who reportedhigh levels of satisfaction with their support,demonstrated higher level of pain behaviour.The social support for these patients worked asa reinforcement to continue pain behaviours.
Psychological models of pain are notadequate to explain why pain experience variesfrom one individual to another. Locus of control,interference with functional activities, and social

232 Behavioural Sciences in Medical Practice
support are examples of psychological and socialfactors that influence the affective dimension ofpain and pain behaviours. These examples arecertainly not the limit of psychosocial factorsinfluencing pain-related suffering and behaviour.Other examples include cognitive models,expectancies, socioeconomic status, culturalbackground, gender, religious beliefs, and socialroles. Any of these may be influenced by chrono-logical age in the later years of life. Furthermore,both actual and perceived social support arelikely to be factors mediating chronic pain-relatedsuffering resulting from degenerative processesin the elderly. This is likely as true in the long-term care setting as in the community dwelling.
Despite the great advances in our under-standing on mechanisms of pain, there is still nosingle model or schema which completelydescribes the nature of the human painexperience.
Coping with Chronic Pain
Research has shown that people appraise painin diverse ways and develop a variety ofcognitive and behavioural strategies to help themcope with pain. Pain-coping strategies that areadopted and used over prolonged time periods,may significantly affect physical and psychologicalfunctioning. Behaviour therapists have deve-loped treatment programmes designed todecrease maladaptive and increase adaptive pain-coping strategies. Such programmes have beendeveloped from theoretical and common senseperspectives on what is maladaptive and whatis adaptive, with little empirical testing of theseideas.
The Lazarus and Folkman (1984) model ofstress, appraisal and coping provides a focus forclinicians and researchers in the identification ofimportant variables to assess in studyingadjustment in chronic pain problems.
Turner et al (1987) conducted analyses tolearn more about how patients’ beliefs abouttheir pain related to the strategies they used for
coping with pain. Patients, who believed theymust accept their pain and that pain did notrequire them to hold back from what they wouldlike to do, were more likely to use problem-focussed coping. These beliefs may be associatedwith low frustration, which may in turn allowfar more objective and problem rather thanemotion-focussed coping. Accepting one’s painwas also associated with less seeking of socialsupport, and it may be that acceptance of thepain leads to less frustration and distress and thusless need for information or support. Patientswere also more likely to seek social support ifthey had not experienced previous episodes ofpain. This points out the importance of viewingcoping with a stressor as a process, with differentcoping strategies used at different phases.Seeking social support may be most useful inthe early stages of coping with a pain problem,when uncertainty and anxiety are likely to behighest. Finally, Turner et al (1987) found thatpatients, who believed their pain would beresolved in four years, used significantly lessavoidance. This is consistent with previousresearch indicating avoidance is expected whenone perceives few alternatives for resolution.
Methods to Assess Pain Profile
Recent advances on the pain have led to greaterappreciation of the multidimensional nature ofpain. The critical role of motivational, affectiveand environmental factors in determining thebehaviour of many chronic pain patients is beingrecognised. Learning and cognitive factors playan important role in changing human behaviourin response to environmental situation. Somemodels have been suggested that nociceptiveinput from tissue or the nervous system is notthe sole determinants of individual pain beha-viour. Motivational, affective, and environmentalevents should also be considered to be relevantfactors in all chronic pain patients; particularlythose in whom operant and psychologicalmechanisms are predominant.

Psychology of Pain 233
Assessment methods are similar for bothacute and chronic pain. Sometimes a distinctionbetween pain as a state and pain as a trait ismade. A state is a situation—specific conditionof pain like postoperative pain. On the otherhand, a trait is a relatively enduring tendencyto feel or behave in a certain way of most ofthe times and across all circumstances. Anexample of this is chronic low back pain. As thepatient endures pain for years, this pain affectshis behaviour and activities.
To understand the complex nature of painand successful remediation, good assessment isa prerequisite. One needs to quantify pain andalso requires assessing illness behaviour, whichmay be normal or abnormal. It is important toassess the disability, suffering, behavioural andpsychological factors involved in persistent, pain,in order to provide an appropriate interventionfor altering pain behaviour.
Patients with chronic pain problems requirecomprehensive and time consuming assessment.What a patient with pain thinks or feels orbehaves, might not be well-communicated tothe doctor. Assessment of pain profile might servethe following functions:1. To provide baseline material against which
the progress and treatment can be compared.2. To provide the therapist, with a detailed
information about the nature of patient’smedical condition, previous treatments,patient’s perceptions of their pain, expec-tations about treatment, and patient’sresources for handling pain.
3. To assist in the establishment of appropriateand objective treatment goals.
4. To examine the important role of significantfactors in the maintenance of maladaptivebehaviours and as resources in the changedprocess.There are various methods to assess pain,
depending upon the aim of the assessment, acombination of methods can be used, e.g. toassess the severity of pain one needs a method
which can quantify the pain, on the other handto understand the pain behaviour, psychologicaltests are used. List of all the methods used inthe assessment of pain are given in Table 25.1.
Table 25.1: Methods of pain assessment
History of pain Psychological evaluationQuantification of pain Life stressSelf-report Psychological dysfunctionQuestionnaire Depression, somatisationBehaviour analysis Family
History of Pain
History of pain should include onset and courseof pain, subjective feeling of distress and disability,finding of physical investigations, previoustreatments, drug and alcohol use as well as abuse;perception of pain by family members, theirexpectations and history of pain in other familymembers; presence of psychiatric problemshould be asked. Assessment of patient’s adjust-ment at home and at work can provide cluesregarding psychological implications for theindividual.
Quantification of Pain
The aim of quantification of pain is to assessobjectively severity intensity and duration of painperiods. Quantifiable scales are also used toevaluate the efficacy of different therapeutictreatments. Quantitative pain scales are broadlygrouped as self-report on single dimensionscales, which usually measures the intensity ofpain. These include category rating scales, bothverbal and facial scales, numerical scales andvisual analog scales. The second group of scalesintend to measure multidimensions of painincluding the experience of pain. McGill PainQuestionnaire is the example of this group ofscales.
Self-report: Patient’s subjective report of inten-sity, frequency and duration of pain is elicited.This is the most commonly used method in

234 Behavioural Sciences in Medical Practice
clinical practice, but it has its limitations becauseof memory lapses on the part of the patient toreport correctly.
Verbal descriptor scales: Verbal descriptors havebeen used for simple reporting of subjective pain.Melzack and Torgetson (1971) introduced thefollowing scale for pain intensity: Instructions:Choose the word below; which best describeshow your pain feels at this time.
Mild Discomforting Distressing HorribleExcruciating. Category judgement is not limitedto words only; facial expressions of pain ofvarying intensity are placed on eight-point scalefor assessment (Frank et al, 1982). The majoradvantage of such scales is that categories canbe formed in native languages and is easy touse in clinical setting. The disadvantage of thisscaling form is to remember or have a writtenform for the words and limited number ofresponse categories. It also lacks statisticalmanipulations of categories.
Numeric rating scale: The simplest and mostfrequently used approach to assessing subjec-tive pain is a numerical rating scale. Patients areasked to rate their pain on a scale from 0 to10 or 100, on which 0 represents no pain and100 indicates the worst pain. This approach isvery commonly used in clinical practice by allof us. It is easily understood by a majority ofour patients. By this approach, only intensity ofpain is measured. An example of this approachis as follows:
Instructions: Choose a number from 0 to 10,which indicates how strong your pain is rightnow.
Visual analog scale: The visual analog scale (VAS)is considered to be one of the best methodsavailable for the estimation of pain. It providesa continuous scale for magnitude estimation andconsists of a straight line, the ends of which aredefined as the extreme limits of pain. Havingthe patient mark the line to indicate pain intensity,and then measure the mark on either a 1-10
or 1-100 scale does scoring. An example of visualanalog scale is: Instructions: Mark on the linebelow how strong is your pain right now. Nopain the worst pain.
Pain maps: Measures of pain location can bemade using pain maps (Keele, 1948), which area simplified human outline. The patient is askedto shade those body areas in which pain isexperienced. Pain maps have been reported(Mooney et al, 1976) to help identify thosepatients who complain of anatomicallyimplausible pain and those who may exaggeratepain. As pain maps only help in locating the pain,additional scales to measure intensity of painshould be used.
It is important that the patients should clearlyunderstand the two end points and they are freeto indicate a response at any point in the scale.High correlation has been reported for VAS andnumerical/verbal scales and is considered validand sensitive. However, it has been reported thatthe completion of the scale is difficult for somepatients. The other disadvantages are thatmeasurement is too subjective, not suited forstatistical procedures—unidimensional in nature,yields estimates of pain intensity only.
The primary limitations of the above-mentioned, unidimensional subjective scaling ofpain resides in the strong risk of subjective biasand inability to assess the complex nature of theexperience of pain. These simple scales can failto yield reliable and valid measurement if careis not taken to ensure accurate reporting. In spiteof these limitations, pain intensity measurementsare the most commonly used tools as they aresimple, inexpensive, easily understood and withculture fairness.
Questionnaires
As an alternative to single or unidimensionalscales, multidimensional scales have beendeveloped. The most widely used scale of thiscategory is McGill Pain Questionnaire.

Psychology of Pain 235
McGill pain questionnaire (MPQ): This question-naire scales pain in three dimensions: sensory,affective, and evaluative (Melzack, 1975). Thetest consists of 20 sets of words that describepain. The first 10 sets represent sensory qualities,the next 5 are affective, only one set numbered16 is evaluative, and the last 4 sets aremiscellaneous words. Patients have to select thesets that are relevant to their pain and circle thewords that best describe it within each selectedset. Each set has 2 to 6 words in varying intensi-ty. One can score each dimension and a totalscore can also be obtained. It requires 5 to 15minutes to complete the questionnaire.
At times Dartmouth Pain Questionnaire(Corson and Schneider, 1984) is used as anadjunct to McGill Pain Questionnaire. Theadvantage of using Dartmouth Pain Question-naire is to get additional information on thequality of pain and on positive functioning orassets of the patient, instead of only deficits infunctioning. MPQ though statistically is a soundtool, yet in our culture many patients cannotunderstand the vocabulary. As a clinical tool,MPQ helps in understanding the quality of pain,both in sensory dimension and in its impact onthe affect (mood) of the patient.
Brief pain inventory (BPI): The Brief PainInventory has been reported as a quick, multi-dimensional, valid scale for measuring pain incancer and arthritis patients (Daul et al, 1983,Cleeland, 1985). It measures analgesic medica-tion, relief in pain, qualitative descriptions of painand beliefs about the cause of pain, and areasof interference with quality of life. It alsomeasures location of pain and intensity of painon scales from 0 to 10.
West Haven-Yale multidimensional paininventory (WHYMPI): This inventory is muchbriefer than McGill Pain Questionnaire (Kernset al, 1985). It has 52 items divided in threeparts:
i. Five general dimensions of the experienceof pain, suffering, interference with normalfamily and work functioning and socialsupport.
ii. Patient’s perceptions of the response ofothers to displays of pain and suffering.
iii. Frequency of engagement in common dailyactivities. This scale has a much broaderapproach in assessment than the otherscales. It is also linked to cognitive-behavioural theory and assesses on dimen-sions beyond subjective distress.
Pain perception profile (Tursky et al, 1982): Itmeasures sensation threshold, uses magnitude—estimation procedures to judge induced pain,measures pain on intensity, reaction andsensation dimensions using psychophysicalscaling of verban pain descriptions, and the threedimensions of psychophysically scaled verbaldescriptors in a diary format for repeatedassessment over time. This method is shorter andsimpler than MPQ and more valid than VAS.For research purposes this method requires morevalidation work.
Memorial pain assessment card (MPAC): TheMPAC scales pain, pain relief, and mood onvisual analog scales and adds a set of adjectivesreflecting pain intensity. Advantages of thismethod are that it is easily administered, takesno time and correlates highly with other scales.
Behavioural Analysis
In behavioural analysis, also known as Beha-vioural Assessment, pain is viewed as a set ofbehaviours. Pain states are characterised bycertain consistent patterns, e.g. sighing, guard-ing, movements. Pain behaviour is operationallydefined and measures are employed to assesspain by objectively recording the frequency,occurrence and setting of their pain-relatedbehaviours. Behavioural methods for assessingpain generally include observational procedures

236 Behavioural Sciences in Medical Practice
in which independent raters record patient’sphysical behaviours by tallying over time andscore in terms of frequency. Observations alsoinclude activities, which evoke pain.
Self-monitoring of pain related the patientsthemselves could do behaviours. Semi-illiteratepatients in our setting can be trained to recordintensity, frequency and duration of pain. In ourpsychosocial milieu, significant family membersshould also be involved in maintaining recordsof pain. The following information should beelicited during behavioural analysis: changes inpatient’s activities because of pain, changes insignificant persons (spouse/parent/children)activities because of pain, patient’s behaviourwhen in pain, family members responses to painbehaviours and well (no pain) behaviours, factorsthat increase or decrease pain, impact of painon patient’s personal, vocational, family, socialand leisure-time activities.
Pain diary is useful in maintaining records ofpain. A pain diary should include pain-relevantactivity broken down into small blocks of time,such as hourly segments. Activities are cate-gorised as walking, sitting, resting. Pain can berated on 0 to 10 scale. It is also useful to recordmedication taken. An example of pain diary isas follows:
Activity, Pain Assessment Record Form
Date Activities Pain Level
Time Sitting Walking Resting Thoughts Medication 1-10
The use of pain diary with pain patients offersseveral advantages:
i. It is not subject to distortion, as it is filledout at the time of pain.
ii. It provides information on patterns ofnormal activity related to pain.
iii. It is expensive.iv. It provides information about patient’s
behaviour at home and at work.
v. It provides feedback to the patient at homeas to which activities increase or decreasepain.
vi. It is possible to correlate behaviouralpatterns with severity of pain.
If systematic records are maintained, beha-vioural assessment can provide importantinformation on various dimensions. One can alsoget information regarding reinforcing factors forpain behaviours.
Psychological Evaluation
To understand any persistent pain problem, fora number of reasons, comprehensive psycho-logical evaluation is required. A pain problemoriginally can be caused by certain processes(e.g. trauma), but can persist for entirely diffe-rent reasons (Fordyce, 1983). With continuationof pain for a longer period, the chances ofpsychological and behavioural processesincrease, as pain and disability have profoundeffects on mood, vocational and interpersonalrelationship. The aim of a psychological evalua-tion is to determine specific psychological factorscausing pain and suffering. Psychosocial factorselicited can be correlated to the patient’s problemand can also be useful in the selection ofparticular therapeutic approaches for a givenpatient.
Psychological evaluations of chronic painpatients are indicated in the following situations:a. Medical evaluation fails to reveal a physical
cause of the pain.b. Physical findings are insufficient to explain
the degree of pain behaviour.c. Physical findings are only speculative or
inferred.A psychologic evaluation can be useful in all
those cases in which the pain interferes signi-ficantly with the patient’s ability to engage innormal activities or has disturbed interpersonalrelationships, shows sign of psychological distress

Psychology of Pain 237
like depression, or secondary gains out of illnessrederived.
Life Stress
Current stressors in the patient’s life cancontribute to psychophysiologic dysfunction,such as increased levels of muscle tension, illnessbehaviour and disability. Patient might usemaladaptive coping strategies such as use ofmedication or alcohol. Pain, inability to engagein normal social, recreational, vocational, house-hold activities and worry about the prognosisor cause of the pain often acts as a source ofmajor stress. These stresses affect the patient’semotional functioning and interpersonalrelationships.
Basic research is being directed to study theunderlying psychophysiological processes,adaptational and coping mechanisms thoughtto mediate stress responses. Often, an associationbetween pain and life stresses is seen in ourclinical experience, although patients can initiallydeny or minimise the contributions of stress totheir pain problems. The interview with the othersignificant family members frequently revealsinformation about stresses affecting the patient.It is difficult to identify stress factors in an initialinterview and many patients might not haveexperienced major stress in the recent past. Inter-view during subsequent visits should be directedto elicit stress in the patient’s work, marriage,children and other areas of his functioning.Treatment can be directed on the effects of stresson pain, suffering and family functioning.
Psychological Dysfunction: The emotional impactof chronic pain, disability, or progressive diseasescan result in changes in psychologic functioning.Identification of psychologic dysfunction is oftenmissed out in a large number of patients sufferingfrom pain. This is probably due to a host offactors such as lack of clinician’s knowledgeconcerning psychological disorders and lack oftime spent with patients in discussing psychosocial
issues. On the other hand, patients may denyor minimise psychological symptoms. The com-mon psychologic dysfunctions are depression,anxiety and somatisation disorders. Anotherimportant concept that has recently emerged inrelation to psychologic dysfunction is abnormalillness behaviour.
Depression: It is one of the commonest problemsseen in pain patients. Therefore, this should beroutinely assessed as part of the psychologicalevaluation. Assessment of depression should notbe limited to asking about depressed mood. Oneshould enquire about symptoms such aspersistent irritability, fatigue, insomnia, lack ofinterest in day-to-day activities, and inability toparticipate in entertainment and leisure timeactivities. At times depressive symptoms canoccur as a side effect of medication. Identificationof depression can be done on the basis of clinicalinterview and brief rating scales such as BeckDepression Rating Scale and Zung DepressionScale. Depression can be easily treated bymedication or cognitive therapy.
Anxiety: It is often associated with acute pain.If the patient has not been communicated bythe treating doctor about the cause, pathology,treatment and prognosis, he fails to make anaccurate appraisal of his condition. This oftengives rise to anxiety. Some patients are anxiousby temperament and acute pain symptoms areperceived as a threat to personal integration.
Somatisation disorders: The unconsciouslymotivated forms of abnormal illness behavioursare often manifested as somatisation disorders.These differ from hypochondriasis, as the patientdenies preoccupations or fears about illnesses,but rather complains of pain and the conse-quences of the symptom. Often, patient enjoyssecondary gains from pain, as he gets a sick role.Somatisation disorders can be assessed throughclinical interview and on MMPI. These disordersare best managed by behaviour therapy.

238 Behavioural Sciences in Medical Practice
Illness behaviour: This refers to the ways in whichindividuals think, feel and act in relation to theirhealth status. Illness behaviour constitutespatient’s total experiences in relation to pain,which are shaped by biological, psychological,and sociocultural influences. Illness behaviourcan manifest as abnormal psychopathologicalstate, in some patients. Abnormal illnessbehaviour (AIB) is defined as the persistence ofan inappropriate or maladaptive more ofperceiving, evaluating and acting in relation toone’s own state of health (Pilowsky, 1978).
Assessment if illness behaviour is not requiredfor acute pain problems. Illness behaviour isdetermined by psychological and behaviouralfactors operating upon the patient and hisenvironment.
Family
In India, because of our strong bonds, familyplays an important role in maintaining, reinfor-cing illness behaviour and also in providing asocial support system necessary for treatmentand rehabilitation of pain patients. To assess theprobability of social reinforcement of painbehaviours it is important to ask from familymembers how they respond to the patient’spain. If family members are frequently respon-ding to pain behaviours and providing ‘sick role’to the patient, then these problems should beaddressed in treatment. Research findings haveindicated the role of family as a model fortolerating pain (Mehta and Dutta, 1993). Themeaning of pain behaviours should beunderstood within the context of family andculture. Expectations of family regardingprognosis should also be elicited. In situationswhere patient activity is discouraged by familymembers, or excessive fear and anxiety areexperienced by the spouse or other significantfamily member then counselling to familymembers should be given.
The psychologic evaluation of chronic painproblems is highly complex task involving a broadrange of clinical questions and issues. Psychologicand behavioural factors involved in persistentpain disability and suffering, with a view toprescription of appropriate interventions foraltering these patterns are needed. The outcomeof this evaluation is a synthesis of the informationgathered resulting in a list of problems reflectingcontribution of specific psychologic andbehavioural processes to the maintenance ofsuffering and pain behaviours.
Psychological Approachesto Pain Control
Pain is a prevalent and costly health problem.When pain persists beyond the “natural” courseof an illness, extends beyond the typical timerequired for an injury to heal, or is associatedwith a progressive illness such as arthritis, thepain is designated chronic. Such costs are relatedto hospitalisation, outpatient treatment, medica-tion, health care, surgery, loss of work produc-tivity, and loss of income, disability paymentsand litigation settlements. The social impact ofpain is also considerable.
An increasingly greater number of psycho-logical treatments are available for the manage-ment of chronic pain. Different psychologicaltreatment approaches are based on differenttheories and attempt to intervene according tothose aspects emphasised by the theory. Inter-ventions can be grouped in one of the four majorareas: focus on pain behaviour, modulation ofthe pain experience, modulation of mood, andcognitive-behavioural functioning.
Operant Therapy
Operant therapy attempts to intervene at thelevel of pain behaviour and applies learningprinciples to the treatment of chronic pain.

Psychology of Pain 239
Fordyce (1976) pioneered the operanttreatment approach to chronic pain. The focusof this approach is on changing overt painbehaviours rather than on the patient’s subjectiveexperience of pain. Pain behaviours includeavoidance of physical activity, medication use,verbal pain complaints, grimacing, and groan-ing. Thus, behaviours that can be observed andmeasured are the targets of intervention.
Pain behaviours are not assumed to solelyreflect underlying pathophysiology, but ratherare subject to influence of a variety of factors,including systematic environmental conse-quences of the patient’s actions.
The goal of this form of treatment is to reducepain behaviours, while simultaneously increasingwell behaviours. Contingencies of pain behaviourare modified. Behaviours incompatible with painbehaviour, such as increased physical exercise,time spent on hobbies, and work are reinforced,and the patient’s well behaviours are praised andattended to. In approaching chronic pain patientswith this operant treatment procedure, it isrecognised that the patient is experiencingsubjective distress, but it is explained to thepatient that this focus on the pain (defined byeach individual’s pain behaviour observed andreported) will be reduced if physical and socialactivities are increased, despite the presence ofpain. The use of selective reinforcement for non-pain behaviour and extinction of pain behaviourby staff, in the case of inpatients, of family, inthe case of inpatient and outpatient cases, is amajor component of this approach.
The operant approach is also helpful for themanagement of medication abuse whereby apatient is taking narcotic analgesics contingentupon exacerbations of pain. The approachassumes that such a contingent relationship(increased pain-increased medication) reinfor-ces pain and pain behaviour because of thepositive consequence of the medication (painrelief or expected pain relief). The patient is,
therefore, given medication at fixed intervals(e.g. every four hours), regardless of pain level.
Biofeedback Training
Biofeedback training typically involves providinginformation about physiological functions thatare normally not in the patient’s awareness. Aspecified target response, such as cervical muscletension, is electronically monitored andinformation about changes in the functioning ofthe targeted response is relayed to the patientvia various feedback devices (see Chapter 20).The goal is to use the feedback to teach thepatient to pain problem.
Relaxation Training
Another treatment that attempts to modulatethe pain experience is relaxation training (seeChapter 20). The goal is to teach the patient todiscriminate between tension and thoughts thatcause muscular skeletal pain or contribute to painassociated with some other type of health problemwhen tense. The relaxation approach has beenused with a variety of chronic pain problems.
Hypnosis
Hypnosis is also used to modulate the painexperience. The actual hypnotic procedure typi-cally varies, depending on therapist or patient,but the goals are generally similar. Goals caninclude altering the patient’s negative perceptionof the pain, shifting it to a neutral or a positiveone, enhancing positive self-statements,improving health-related attitudes, and instillingfeelings of deep relaxation potentiallyincompatible with certain pain behaviours.
Cognitive-Behavioural Approach: PainInoculation
A cognitive-behavioural approach conceptua-lises chronic pain problems in terms of coping

240 Behavioural Sciences in Medical Practice
skill deficits in either the cognitive or behaviouraldomains. The goal is to help the patient developmore adaptive cognitive and behaviouralresponses to the physical problem. Whendiscussing the cognitive approach, the patientis taught to identify negative, habitual thoughtsrelated to pain; recognise the connectionbetween thoughts and consequent feelings andpain; substitute more adaptive thoughts; and usecoping strategies (such as relaxation, distraction,imagery), to reduce suffering. Often in con-junction with these cognitive strategies, the patientis introduced to operant conditioning principles,and a programme is established to reinforcenonpain-related behaviour, such as medicationuse. These methods have been reported to bevery effective in all types of pain, all ages andin all cultures (Mehta, 1993).
Pain in Elderly
The beliefs and attitudes of the elderly painpatient have an important effect in shaping rela-tionships with physicians. The patient’s beliefsabout his pain and its causes, perceptions of hisphysicians’ beliefs, and his general attitudestowards health professionals, all directly affectthe relationships and their outcomes. This isclearly reciprocal process: The physicians’ beliefs,perceptions, and attitudes are equally importantin determining the quality of the relationshipsand their outcomes. A commonly encounteredpopular belief is the linkage between aging,illness and impairment.
There is considerable variance in the beliefsof both elderly pain patients and their physi-cians. When there is a discrepancy in beliefsbetween the elderly patient and his physician,it influences the effectiveness of the patient-physician relationship. There is a substantialresearch literature in support of positive out-comes related to agreement between patient andphysician about the importance of variousaspects of an illness and its treatment. For chronic
pain, views about appropriateness of certainkinds of treatments are often closely associatedwith beliefs about the origins of the pain. Theredeeming effects of such patient-physicianagreement have been found to include positivehealth outcomes. Greater conformity toprescribed treatment regimens and greaterpatient satisfaction.
Pottes and Silverman (1990) demonstratedthe potency of physician beliefs and their effectson some areas of patient outcome. The patientsof physicians, who viewed psychologicalconcerns as important, were found to be lessdepressed and anxious than were patients ofphysicians who attached less importance to thesefactors. Similarly, patients of physicians whoviewed a broad range of treatment componentsas important were found to have experiencedless sleep disturbance and less general disability.
Many elderly pain sufferers have negativeand even contemptuous views of the health caresystem. These views can represent substantialbarriers to treatment if not addressed by thehealth professional. In a study of reasons forrefusal of hospitalisation among elderly patients,negative perceptions of the health care systemwere the primary reason given by the refusers(Barry, Crescenzi, Radovsky, Kern, and Steel,1988). These negative perceptions includedprevious negative experiences, fear of hospitals,and a mistrust of the medical system.
SUMMARY
There are individual differences in coping withpersistent pain. Many individuals are able toaccept and cope with such disorders as arthritis,migraine, and back pain without much ofmedication. Others however, develop a complexcluster of symptoms independent of the type ofpathophysiology. These individuals displaypersonal and social difficulties as well as patternsof health care use that are quite consistent across

Psychology of Pain 241
pathologies. This cluster of problems has beencalled the chronic pain syndrome.
Melzack and Wall (1965) proposed a modelthat helps to explain the role of such psycho-logical factors in CNS modulation of pain. It hasemphasised the need for the use of an integrativepsychobiological approach to theory and practicein the area of pain and pain control.
Analysis of patient’s appraisals and copingstrategies is useful in understanding functionaldisability and distress in chronic pain patients.Attempts have been made to measure appraisalsand coping strategies for chronic pain. Studieshave consistently yielded certain importantfindings. First, passive coping strategies,catastrophising, and little perceived control overpain are associated with greater pain, depressionand functional disability.
Psychological models of pain are notadequate to explain why pain experience variesfrom one individual to another. Locus of control,interference with functional activities, and socialsupport are examples of psychological and social
factors that influence the affective dimension ofpain and pain behaviours.
Patients with chronic pain problems requirecomprehensive and time consuming assessment.To understand the complex nature of pain andsuccessful remediation, good assessment is aprerequisite. One needs to quantify pain, assessillness behaviour, the disability, suffering,behavioural and psychological factors involvedin persistent pain, in order to provide an appro-priate intervention for altering pain behaviour.
Behavioural treatment for pain is related todecreases in patient catastrophising and increasesin perceived control over pain, and thesechanges are associated with decreases in painrating and disability. Finally, there is evidencethat attention-diversion techniques, which aretaught in many pain programmes, may not beuseful for chronic pain. These findings suggestthat the effectiveness of pain managementprogrammes may be increased by interventionstargeted at patient’s sense of control over pain.This may be more important than training inspecific coping strategies.


Bibliography
1. Ackerman NW. Treating the Troubled Family.New York: Basic Books 1966a.
2. Agras WS, Kazdin AE, William GT. BehaviorTherapy: Toward and Applied Clinical Science(Ed) W.H. Freeman & Co. San Francisco 1979.
3. Ahern DK, Adams AE, Follick MJ. Emotional andmarital disturbance in spouses of chronic low-back pain patients. Clin. J. Pain, 1985;1:69-74.
4. Allen KE, Harris FR. Elimination of a Child’sExcessive Scratching by Training the Mother inReinforcement Procedures. Behaviour Researchand Therapy, 1966;4:79-84.
5. Allport GW. Pattern and Growth in Personality.London: Holt, Rinehart and Winston 1961.
6. Aman U, Khan MD. Clinical Disorders ofMemory. New York: Plenum Medical BookCompany 1986.
7. American Psychiatric Association. Diagnostic andStatistical Manual of Mental Disorders (ThirdEdition Revised). Washington, DC: AmericanPsychiatric Association 1987.
8. Anastasi A. Psychological Testing. New York:Macmillan Publishing Company 1988.
9. Anderson and Anderson. An Introduction toProjective Techniques. New York: Prentice-Hall,Inc. 1951.
10. Anthony J, Marsella Velma A, Kameoka.Ethnocultural Issues in the Assessment ofPsychopathology in Measuring Mental Illness. InS. Weltzer, Psychometric Assessment for Clinicians(Eds). Washington, DC 2005.
11. Apley J. The Child with Abdominal Pains.Oxford: Blackwell Scientific Publications 1975.
12. Atkinson JW, Birch DC. An introduction tomotivation (2nd ed.). New York: D. Van Nostrand1978.
13. Atkinson RC, Shiffrin RM. Human memory: Aproposed system and its control processes. InK.W. Spence & J.T. Spence (Eds.), The psychologyof learning and motivation (Vol.2). New York:Academic Press 1968.
14. Ausubel DP, Novak JS, Hanesian H. EducationalPsychology: A Cognitive View (2nd Edition).NewYork: Holt, Rinehart, and Winston 1978.
15. Ausubel DP, Novak JS, Hanesian H. EducationalPsychology: A Cognitive View. New York: HoltRinehart Winston 1990.
16. Baile WF, Engel BT. A behavioural strategy forpromoting treatment compliance followingmyocardial infarction. Psychosomatic Medicine,1978;40(5):413-9.
17. Bandura A, Walters RH. Social learning andpersonality development. New York: Holt,Rinehart and Winston 1963.
18. Bandura A. A social learning interpretation ofpsychological dysfunction. In P. London & D.Rosenhan (Eds), Foundations of abnormalpsychology. New York: Holt, Rinehart andWinston 1968.
19. Bandura A. Aggression: A social learning analysis.EngleWood Cliffs, N.J: Prentice-Hall 1973.
20. Bandura A. Principles of Behaviour Modification.New York: Holt, Rinehart and Winston 1969.
21. Bandura A. Social learning theory. EnglewoodCliffs, NJ: Prentice-Hall 1977.
22. Baron RA. The reduction of human aggression:A field study of the influence of incompatiblereactions. Journal of Applied Social Psychology,1973;6:260-74.
23. Barrett J, Rose R. Mental Disorders in theCommunity. Progress and Challenge. New York:Guilford Press 1986.

244 Behavioural Sciences in Medical Practice
24. Bateson G. Mind and Nature: A Necessary Unity.New York: Dutton 1980.
25. Beck A, Ward H, Mendelson M, et al. Aninventory for measuring depression. Arch GenPsychiatry 1961;4:561-71.
26. Beck A, Weissman A, Lester D, et al. Measure-ment of Pessimism: The Beck Hopelessness Scale.J Consult Clin Psychol 1974;42:861-65.
27. Beck AT, Ward CH, Mendelson M, et al. Aninventory for measuring depression. Arch GenPsychiatry 1961;4:561-71.
28. Beck AT. Cognitive Therapy and the EmotionalDisorders. New York: International UniversitiesPress 1976.
29. Beck AT. The development of depression: acognitive model. In R.J. Friedman & M.M. Katz,The Psychology of Depression: ContemporaryTheory and Research. New York: Wiley 1974.
30. Becker MH, Haefiner DP, Kasl SV, Kirscht JP,Maiman LA, Rosenstock IM. Selectedpsychosocial models and correlates of individualhealth-related behaviours. Medical Care,1977;15 (Suppl.5) 27-46.
31. Bellak L. Psychological aspects of normal aging.In: Bellak L, Tosko BD (Eds). Geriatric Psychiatry.New York: Grune and Stratton 1976.
32. Benton A, Hamsher K, Varney N, et al. Contri-butions to Neuropsychological Assessment. NewYork: Oxford University Press 1983.
33. Berkowitz L, LePage A. Weapons as aggressioneliciting stimuli. Journal of Personality and SocialPsychology 1967;7:202-07.
34. Bigga JB. Learning strategies, student motivationpatterns and subjectively perceived success. In JRKirby (Eds). Cognitive Strategies and EducationalPerformance. Orlando: Academic Press 1984.
35. Billings AG, Moos RH. The role of copingresponses and social resources in attenuating thestress of life events. Journal of BehaviouralMedicine, 1981;4:139-57.
36. Blumer D, Hilbronn M. Chronic pain as a variantof depressive disease: The pain-prone disorder.The Journal of Nervous and Mental Disease,1982;170(7):381-406.
37. Bonivs JI. Importance of the problem. In JJBonica, V Ventafridda (Eds). Advances in painresearch and therapy (Vol. 2). New York: RavenPress 1979.
38. Bouchard TJ, Lykken DT, McGue M, Segal NL,Tellegen A. Sources of human psychological
differences. The Minnesota study of twins rearedapart. Science, 1990;250:223-28.
39. Bradley RH, Caldwell BM. Early homeenviron-ment and changes in mental testperformance in children from 6 to 36 months.Developmental Psychology, 1976;12:93-97.
40. Brink TL. Geriatric Psychotherapy. In E Busse, EPfeiffer (Eds). Behavior and adptation in later life(2nd ed.) Boston: Little, Brown 1977.
41. Broadbent D, Cooper P, Fitzgerald P, et al. Thecognitive Failures Questionnaire (CFQ) and itscorrelates. Br J Clin Psychol 1982;21:1-16.
42. Brown GK, Nicassio PM. Development of aquestionnaire for the assessment of active andpassive coping strategies in chronic pain patients.Pain, 1987;31:53-64.
43. Bruner JS. Toward a Theory of Instruction.Cambridge, Massachusetts: Harvard UniversityPress 1966.
44. Bush B, Shaw S, Cleary P, et al. Screening foralcohol abuse using the GAGE questionnaire.Am J Med 1987;82:231-35.
45. Butters N, Albert M. Process underlying failuresto recall remote events. In LS Cermak (Eds).Human Memory and Ammesia. Hillsdale, NJ:Lawrence Erlbaum Associates 1982.
46. Cannon WB. The The James - large theory ofquotions: A critical examination and an aternativetheory -American Journal of Psychology,1927;39:106-24.
47. Caprara GV, Barbaranelli C, Borgoni L, PeruginiM. The Big Five Questionnaire –a NewQuestionnaire for the measurement for the fivefactor model. Personality and Individualdifferences 193;15:281-88.
48. Carver CS, Scheier MF. Control theory: A usefulconceptual framework for personality-social,clinical, and health psychology. PsychologicalBulletin, 1982;92:111-35.
49. Cattell RB. Abilities: Their structure, growth andaction. Boston: Houghton Mifflin 1971.
50. Cattell RB. The Handbook for the 16 PersonalityFactor Questionnaire. Champaign, 1llionois:Institute for Personality and Ability Testing 1986.
51. Cattell RB. The Scientific Analysis of Personality.Penguin, Harmondsworth 1965.
52. Chambers WJ, Puig-Antich J, Hirsch M, et al. Theassessment of affective disorders in children andadolescents by semi-structured interview: Test-retest reliability of the Schedule for Affective
Bibliography 245
Disorders and Schizophrenia for School-agechildren, present episode version. Arch GenPsychiatry 1985;42:696-702.
53. Charney E, Bynum R, Eldredge D, et al. How welldo patients take oral penicillin? A collaborative
study in private practice. Pediatrics 1967;40:188-95.
54. Charney E. Patient-doctor communication:Implications for the clinician. Pediatr. Clin. North
Am. 1972;19:263-79.55. Chesney MA, Eagleston JR, Rosenman RH. The
Type A structured interview: A behaviouralassessment in the rough. Journal of Behavioural
Assessment, 1980;2:255-72.56. Cinciripini PM, Williamson DA, Epstein LH.
Behavioural treatment of migrain headaches. InJM Ferguson, C Barr Taylor (Eds). The
Comprehensive Handbook of BehaviouralMedicine (Vol. 2). New York: Spectrum Medicial,1981.
57. Copp LA. The spectrum of suffering. Am. J.
Nursing, 1974;74:491-95.58. Costa PT Jr, McCrac RR. Revised NEO Personality
Inventory (NEO-pi-R) and NEO-five factorinventory (NEO-FFI) Professional manual.
Odessa; FL; Psychological Assessment Resources1992.
59. Craig KD. Social modeling influences on pain.In RA Sternbach (Ed). The psychology of pain.
New York: Raven Press 1978.60. D’Monte B, Pande JN. The use of Inquiry-driven
strategies for innovations in medical education,AIIMS experience In: Verma K, D’Monte B, Adkoli
BV, Nayar U (Eds). Inquiry driven strategies forinnovations in medical education in India. AIIMS1991;49-53.
61. Davidson PD. Issues in patient’s compliance. In
TI Millon, C Green, R Meagher (Eds). Handbookof Clinical Health Physiology. New York: PlenumPress, 1982.
62. Davis MS. Physiologic, psychosocial, and
demographic factors in patient compliance withdoctors’ order. Medical Care, 1968;6:115-22.
63. De Benedittis G, Lorenzetti A, Fieri A. The roleof stressful life events in the onset of chronic
primary headache. Pain, 1990;40:65-75.64. Derogatis L, Lipman R, Covi L. SCL-90: An
outpatient psychiatric rating scale: Preliminaryreport. Psychopharmacol Bull 1973;9:13-27.
65. Derogatis LR. The Symptom Checklist-90
Manual. Towson, MD: Clinical Psychometric
Research 1983.
66. Despande SN, Nehta M. Aversion Therapy in the
treatment of tricollotomania J of Per and Clinical
Studies 1990;6(1):145-47.
67. Dowling J. Autonomic indices and reactive pain
reports on the McGill Pain Questionnaire. Pain,
1982;14:387-92.
68. Dunbar J, Stunkard A. Adherence to diet and
drug regimen. In R Levy, B Rifkind, B Dennis,
N Ernst (Eds). Nutrition, Lipids, and Coronary
Heart Disease. New York: Raven Press, in press.
69. Eaton W. The epidemiology of Schizophrenia
(Volume 1). G Burrows, T Norman, G Rubinstein
(Eds). Epidemiology, Etiology, and Clinical
Features. New York, Elsevier 1986.
70. Edelbrock C, Costello AJ, Dulcan MK, et al.
Parent- child agreement on child psychiatric
symptoms assessed via structured interview.
Child Psychol Psychiatry 1986;27:181-90.
71. Edwards PW, Zeichner A, Kuczmierczyk AR,
Boczkowski J. Familial pain models: The
relationship between family history of pain and
current pain experience. Pain, 1985;21:379-84.
72. Egbert LD, et al. Reduction of postoperative pain
by encouragement and instruction of patients. J
Med 1964;270:825-27.
73. Ellis A. Humanistic Psychotherapy: The Rational-
Emotive Approach, Julian Press, New York 1973.
74. Ellis A. Irrational ideas (hand-out), Institute for
Rational Living, New York 1977.
75. Ellis A. The basic clinical theory of rational-
emotive therapy. In A Ellis, R Grieger (Eds).
Handbook of Rational-Emotive Therapy. New
York: Springer 1977.
76. Endicott J, Cohen J, Nee J, et al. Hamilton
Depression Rating Scale: Regular and change
versions of the schedule for affective disorders
and schizophrenia. Arch Gen Psychiatry
1981;38:98-103.
77. Endicott J, Spitzer R, Fleiss J, et al. The global
assessment scale. Arch Gen Psychiatry
1976;33:766-71.
78. Endicott J, Spitzer RL, Fleiss JL, et al. The Global
Assessment Scale: A Procedure for measuring
overall severity of psychiatric disturbance. Arch
Gen Psychiatry 1976;33:766-11.

246 Behavioural Sciences in Medical Practice
79. Endicott J, Spitzer RL. A diagnostic interview: Theschedule for Affective Disorders andSchizophrenia. Arch Gen Psychiatry 1978;35:837-44.
80. Entwistle NJ, Hanley M, Ratcliffe G. Approachesto learning and levels of understanding. Br JEduc Res 1979a;5:99-114.
81. Epstein NB, Bishop DS. Problem-centeredsystems therapy of the family. In AS Gurman, DPKniskern (Eds). Handbook of Family Therapy.New York: Basic Books, 1981.
82. Erikson EH. Identity Youth, and Crises. NewYork: WW Norton 1968.
83. Eron LD. Prescription for reduction of aggression.American Psychologist, 1980;35(3):244-52.
84. Evans BJ, Standley RO, Mestorovic R, Rose L.Effects of communication skills training onstudents diagnostic efficiency. Med Educ1991;25:517-26.
85. Eysenck HJ. Trait theories of personality. In AMColman (Ed) Companion Encyclopedia ofPsychology (Vol. 1) London: Routledge 1990.
86. Feuerstein M, Bush C, Corbisiero T. Stress andchronic headache: A psychophysiologicalanalysis of mechanisms. Journal ofPsychosomatic Research, 1982;26:167-82.
87. Fleming R, Baum A, Gisriel MM, Gatchel RJ.Mediating influences on social support on stressat Three Mile Island. Journal of Human Stress,1982;8:14-22.
88. Fletchner CM. Communication in Medicine.London: Nuffieldi Provincial Hospital Trust 1973.
89. Fordyce WE. Behavioural methods for chronicpain and illness. St. Louis: Mosby 1976.
90. Fordyce WE. Learning processes in pain. In: RASternbach (Ed). The Psychology of Pain. NewYork: Raven Press 1978.
91. Freud S. Morning and Melancholia. StandardEdition, Vol. 14. London: Hogarth Press 1917.
92. Freud S. Three Essays on the Theory of Sexuality.Standard Edition, Vol. 7. London: Hogarth Press1905.
93. Friedman EH. Systems and ceremonies: A familyview of rites of passiage. In: EA Carter, MMcGoldrick (Eds). The Family Life Cycle. GardnerPress, New York 1980.
94. Friedman M, Rosenman RH. Association ofspecific overt behaviour pattern with blood andcardiovascular findings. Journal of the AmericanMedical Association, 1959;169:96-106.
95. Gagne RM. Essentials of Learning for Instruction.Hinsdale, Illinois: Dryden Press 1974.
96. Garb IR, Garb JL, Stunkard AJ. Effectiveness ofa self-help group in obesity control. Arch. Int.Med. 1974;134:716-20.
97. Gardner H. Multiple intelligence: The Theory inPractice. New York: Basic Books 1993.
98. Gillum RF, Barsky AJ. Diagnosis and manage-ment of patient non-compliance. J Am Med Assoc1974;228:1563-67.
99. Goldberg EL, Comstock GW. Epidemiology of lifeevents: Frequency in general populations.American Journal of Epidemiology, 1980;111(6):736-52.
100. Goldberg JO, Shaw BF, Segal ZV. Concurrentvalidity of the Millon Clinical Multiaxial InventoryDepression scales. J Consult Clin Psychol1987;55:785-87.
101. Goldman SR, Hogaboam TW, Bell LC, PerfettiCA. Short-term retention of discourse duringreading. Journal of Educational Psychology1980;68:680-88.
102. Goleman D. Emotional intelligence. New York:Bantam Books 1995.
103. Gorer G. Death, Grief and Mourning. London:Crescent Press 1965.
104. Guilbert JJ. Educational Handbook for HealthPersonnel. WHO offset Publications No.35. WorldHealth Organization. Geneva 1992.
105. Guilford JP. The structure of intellect.Psychological Bulletin 1956;53:267.
106. Haggerty RJ, Bloom SW, Mechanic D, Pardes H.Report of the commission’s subcommittee on theBehavioural Sciences: In Medical Education intransition, Commission on Medical Education:The Sciences of Medical Practice. The RobertWood Johnson Foundation 1993;74-78.
107. Haley J. Problem-Solving Therapy. Jossey-Bass,San Francisco 1976.
108. Hamilton M. Development of a rating scale forprimary depressive illness. Bri J of Social andClinic Psychol 1967;6:278-96.
109. Hamilton M. Rating depressive patients. J ClinPsychiatry 1960;41:21-24.
110. Harris, Louis, Associates. Inc. The public and highblood pressure. Unpublished survey conductedfor the National Heart and Lung Institute, June1973.
111. Hathaway SR, McKinley JC. MinnesotaMultiphasic Personality Inventory (MMPI).

Bibliography 247
Minneapolis, University of Minnesota Press1943.
112. Haynes DL, Sackett RB (Eds). Compliance withtherapeutic regimens. Baltimore: Johns HopkinsUniversity Press 1976.
113. Haynes SG, Feinleib M, Kannel WB. Therelationship of psychosocial factors to coronaryheart disease in the Framingham Study. AmericanJournal of Epidemiology, 1980;lll (l),37-58.
114. Hebb DO. Textbook of Psychology (3rd Ed).Philadelphia: Saunders 1972.
115. Hefler RE. An objective comparison of thepaediatric interviewing skills of freshman andsenior medical students. Paediatrics, 1970;45:623-27.
116. Heider F. The Psychology of InterpersonalRelations. New York: Wiley 1958.
117. Heilman KM, Valenstein E. Clinical Neuro-psychology (IIIrd Ed) UK Oxford University Press1993.
118. Helzer JE, Robins LN, McEvoy LT, et al. Acomparison of clinical and Diagnostic InterviewSchedule diagnoses: Physician reexamination oflay-interviewed cases in the general population.Arch Gen Psychiatry 1985;42:657-66.
119. Helzer JE. The use of a structured interview forroutine psychiatric evaluations. J Nerv Ment Dis1981;169:45-49.
120. Hess JW. A comparison of methods for evaluatingmedical student skills in relation to patients. JMed Educ, 1969;44:934-8.
121. Hill R. Family under stress. New York: Harper &Row 1949.
122. Hinton JM. The physical and mental distress ofthe dying. Quarterly Journal of Medicine1963;32:1.
123. Holm JE, Holroyd KA, Hursey KG, Penzien DB.The role of stress in recurrent tension headache.Headache, 1986;26:160-67.
124. Holmes TH, Masuda M. Life change and illnesssusceptibility. In BP Dohrenwend (Eds). Stressfullife events: Their nature and effects, New York:Wiley 1974.
125. Holmes TH, Rahe RH. The social readjustmentrating scale. Journal of Psychosomatic Research,1967;11:213-18.
126. Horn JL, Wanberg KW, Foster FM. The alcoholUse Inventory. Baltimore, Psych Systems 1983.
127. Hudson L. Contrary Imaginations, Methuen,London 1966.
128. Hughes JR, O’Hara MW, Rehm LP. Measurement
of depression in clinical trials: an overview. J ClinPsychiatry 1982;43:85-88.
129. Hulka BS, Cassel JC, Kupper LL, Burdette JA.
Communication, compliance, and concordancebetween physicians and patients with prescribed
medications. Am J Public Health 1976;66:847-
53.130. Ilfeld FW Jr. Coping styles of Chicago adults.
Description. Journal of Human Stress, 1980;6(2),
2-10.131. Ivey A. Intentional interviewing and counselling.
California: Brooks/Cole Publishing Company
1983.132. Jackson H, Cooper J, Mellinger WJ, et al.
Streptococcal pharyngitis in rural practice:
Rational medical management. J Am Med Assoc1966;197:385-88.
133. James W. What is an emosion? Mind, 1884;9:
188-205.134. Janis IL, Mann L. Decision making: A psycho-
logical analysis of conflict, choice, and
commitment, New York: Free Press 1977.135. Jenkins CD. Recent evidence supporting
psychologic and social risk factors for coronary
disease. New England Journal of Medicine,1976;294(18):987-94.
136. Jensen AR. The nature of the black-white
difference on various psychometric tests:Spearman’s hypothesis. Behavioural and Brain
Sciences 1985;8:193-263.
137. Kagan A, Levi L. Adaptation of the psychosocialenvironment to man’s abilities and needs. In: L
Levi (Ed). Society, stress and disease. London:
Oxford University Press 1971.138. Keefe FJ, Block AR. Development of an
observation method for assessing pain behaviour
in chronic low back pain patients. BehaviourTherapy, 1982;13:363-75.
139. Keefe FJ, Caldwell DS, Williams DA, Gill KM,
Mitchell D, Robertson C, Martinez S, Nunley J,Beckham JC, Crisson JE, Helms M. Pain coping
skills training in the management of osteoarthritic
knee pain: a comparative study. Behav Ther,1990;21:49-62.
140. Khan AU. Clinical Disorders of Memory. New
York: Plenum Publishing Corporation 1986.141. Kohler W. The mentality of apes. New York:
Harcourt, Brace & World 1927.

248 Behavioural Sciences in Medical Practice
142. Kubler-Ross E. On Death and Dying. New York,MacMilan Publishing Co 1969.
143. Lambert MJ, Hatch DR, Kingston MD, et al. Zung,Beck, and Hamilton rating scales as measures oftreatment outcome: A meta- analytic comparison.J Consult Clin Psychol 1986;54:54-59.
144. Lange C. The emotions. Baltimore: Williams &Wilkins. (Ongoing published 1885) 1922.
145. Lazarus RS, Folkman S. Stress, appraisal andcoping. New York: Springer-Verlag 1984.
146. Lazarus RS. Patterns of adjustment. New York:McGraw- Hill 1976.
147. Lazarus RS. Positive denial: The case for notfacing reality. Psychology Today. 1979;13:44-45.
148. Lazarus RS. Psychological stress and coping inadaptation and illness. International Journal ofPsychiatry in Medicine, 1974;5:321-33.
149. Lazarus RS. Psychological stress and the copingprocess. New York: McGraw-Hill 1966.
150. Lazarus RS. Thoughts on the Relations betweenemotions and cognition. American Psychologists1982;37:1019-24.
151. Levy RL. The role of social support in patientcompliance: A review. In RB Haynes, ME Mattson,TO Engebretson (Eds). Patient compliance toprescribed antihypertensive medical regimens: Areport to the National Heart, Lung, and BloodInstitute, Bethesda, MD: National Heart, Lung andBlood Institute 1980.
152. Lewinson PM, Sullivan JM. Distraction andcoping with pain. Psychological applications. InAJ Rush (Ed), Short-term psychotherapies fordepression. New York: Guilford Press 1984.
153. Lewis CE, Resnik BA, Schmidt G, Wazman D.Activities, events and outcomes in ambulatorypatient care. N Engl J Med 1960;280:270-273,291.
154. Lewis CE, Resnik BA. Nurse and progressiveambulatory patient care. N Engl J Med 1967;277:1236-41.
155. Ley P. Giving information to patients. In: Eiser JR(Ed). Social Psychology and BehaviouralMedicine. London: John Wiley 1983;339-74.
156. Lindemann E. The symptomatology andmanagement of acute grief. American Journal ofPsychiatry 1944;101:141.
157. Linton SJ, Melin L. Applied relaxation in themanagement of chronic pain. BehaviouralPsychotherapy, 1983;11:337-50.
158. Luria AR. The frontal lobes and the regulationof behaviour. In KH Pibram, AR Luria (Eds).Psychophysiology of the Frontal Lobes. NewYork: Academic Press 1973.
159. Maguire GP, Rutter DR. History-taking for medicalstudents: Deficiencies in performance. The Lancet1976;556-58.
160. Mahoney M. Cognition and BehaviourModification. Ballinger, Cambridge MA 1974.
161. Malik SL, Manchanda SK, Deepak KK, SunderamKR. The attitudes of medical students to theobjective structured practical examination. MedEduc. 1988;22:40-6.
162. Mannuzza S, Fyer AJ, Jlein DF, et al. Schedulefor Affective Disorders and Schizophrenia-Lifetime Version modified for the study of anxietydisorders (SADS-LA): Rationale and conceptualdevelopment. J. Psychiatr Res 1986;20:317-25.
163. Marcotte DB, Held JP. A conceptual model forattitude assessment in all areas of medicaleducation. J. Med. Educ. 1978;53:310-4.
164. Marlatt GA. The Drinking Profile: A questionnairefor the behavioural assessment of alcoholism. InEJ Mash, LG Terdal. Behaviour TherapyAssessment. New York: Springer 1976.
165. Marlon F. Describing conceptions of the worldabout us, Research Report from the Institute ofEducation, University of Gothenburg 1978.
166. Marlon FS. On qualitative differences in learningoulcome and process. Br J Educ Psychol,1976b;46:4-11.
167. Marsella AJ, Sartorius N, Jablensky A, et al.Depression across cultures, in Culture andDepression. University of California Press 1985.
168. Marsella AJ. An interactional theory ofpsychopathology. In B Lubin, W Connor (Eds).Ecological Models in Clinical and CommunityPsychology. New York: John Wiley 1984.
169. Marsella AJ. Depressive experience and disorderacross cultures. In H Triandis, J Draguns (Eds).Handbook of Crosscultural Psychology:Psychopathology (Vol 6). Boston: Allyn & Bacon,1980.
170. Marsella AJ. The measurement of depressiveexperience and disorders across cultures. In AJMarsella, R Hirschfeld, M Katz, The Measurementof Depression: Biological, Psychological,Behavioural, and Social Aspects. New York:Guilford Press 1987.

Bibliography 249
171. Maruta T, Osborne D, Swanson DW, Hailing JM.Chronic pain patients and spouses: Marital andsexual adjustment Mayo Clin Proc, 1981;56:307-10.
172. Maslow AH. Motivation & Personality. New York:Harper & Row 1970.
173. Mathews AM, Gelder MG, Johnston DW.Programmed Practice for Agoraphobia: Partners’Manual, London: Tavistock Publications 1981.
174. Matson JL, Andrasik M. Treatment Issues andInnovations in Mental Retardation (Ed). NewYork: Phenum Press 1983.
175. McGuire WJ. The nature of attitudes and attitudechange. In G Lindzey, E Aronson (Eds).Handbook of Social Psychology. Vol. 3 (2ndEdition). Addison-Wesley: Reading Mass, 1969.
176. Mckellar P. Imagination and Thinking. London:Cohen and West 1957.
177. Mechanic D. Effects of Psychological distress onperceptions of physical health and use of medicaland psychiatric facilities. Journal of Human Stress,1978b;5:26-32.
178. Mechanic D. Medical Sociology (2nd ed). NewYork: Macmillan 1978a.
179. Mechanic D. The concept of illness behaviour.Journal of Chronic Diseases 1962;15:189.
180. Mehta M, Chawla HM. Behavioural interventionin asthma, a report of acase. Ind Jr Clinic Psych1985;12(2):75-78.
181. Mehta M, Kumar D, Sethi SS. Family charac-teristics of children with Somatoform andAttention Deficit disorders. Abstracted in 13thinternational Association for Child andAdolescent Psychiatry and Allied Professions, SanFrancisco, USA 1994;17, SP-02-005.
182. Mehta M. Behaviour therapy for different type ofphobias in Indian setting, DEI Research Journalof Educational and psychology, Special issue onBehaviour Therapy, 1986;3:l 57-62.
183. Mehta M. Identification of study styles ofundergraduate medical students. Unpublishedresearch report. KL Wig CMET, AIIMS, New Delhi1995.
184. Mehta M. Student Learning Symposium onmedical education, Ind. J. Pediatrics, 1994;61:121-26.
185. Mehta M. Training Mothers of Mentally RetardedChildren. Evaluation of Variables DeterminingSuccess. Indian Council of Medical Research,New Delhi 1987.
186. Meichenbaum D, Turk DC. The behavioural
management of anxiety, anger and pain. In: PODavidson (Ed). The behavioural management of
anxiety, depression and pain. New York: Burner/
Mazel 1976.187. Meichenbaum D. Cognitive Behaviour Modi-
fication: An Integrative Approach. New York:
Plenum Press 1977.188. Meichenbaum DH. Self-instructional methods. In
FH Kanfer, AP Goldstein. Helping people change:
A textbook of methods. New York: Pergamon,1975;357-91.
189. Melzack R, Torgerson WS. On the language of
pain. Anesthesiology, 1971;34:50-59.190. Melzack R, Wall PD. Pain mechanisms: A new
theory. Science, 1965;150:971-79.
191. Melzack R. The McGill Pain Questionnaire. In:Melzack R (Ed): Pain measurement and
assessment. New York: Raven Press 1983.
192. Michaels JW, Blommel JM, Brocato RM, LinkousRA, Rowe JS. Social facilitation and inhibition in
a natural setting, Replications in Social
Psychology, 1982;2:21-4.193. Millon T, Green C, Meagher R. Handbook of
Clinical Health Psychology. New York: Plenum
Press 1982.194. Millon T. Millon Clinical Multiaxial Inventory
Manual, 3rd ed. Minneapolis, National Computer
Systems 1983.195. Milner B. Some effects of prefrontal lobectomy
in man. Behaviour. New York: McGraw-Hill.
196. Minuchin S. Families and family therapy.Cambridge: Harvard University Press 1974.
197. Mischel W. On the future of personality
measurement. American Psychologist, 1977;32:246-54.
198. Monchy DC, Richardson R, Brown RA, Harden
RN. Measuring attitudes of doctors: the doctor-patient rating. Med Educ 1988;22:231-39.
199. Moos RH (Ed). Coping with physical illness. New
York: Plenum Press 1977.1 percent. Morton F. Describing conceptions of
the world about us. Research report from the
Institute of Education University of Gothenburg1978.
200. Moos RH, Tsu VD. The crisis of physical illness:
An overview. In: Moos RH (Ed): Coping withPhysical Illness. New York. Plenum Medical
1977.

250 Behavioural Sciences in Medical Practice
201. Nerenz DR, Leventhal H. Self-regulation theoryin chronic illness. In: Burish T, Bradley L (Eds):Coping with Chronic Disease: Research andApplications. New York: Academic Press 1983.
202. Parkes CM. Bereavement and mental illness. PartIIA classification of bereavement reactions. Br JMed Psychol 1965;38:1.
203. Parsons T. Social structure and personality.London: Collier-Macmillan 1964.
204. Parsons T. The sick role and the role of thephysician reconsidered. Milbank Memorial FundQuarterly, 1975;53:257-58.
205. Pearlin LI, Schooler. The structure of coping.Journal of Health and Social Behaviour,1978;19(1):2-21.
206. Pershad D. The Construction & Standardizationof a Clinical Test of Memory. NationalPsychological Corporation, Agra 1977.
207. Philips C. Headache and personality. JPsychosomatic Research, 1976;20(6):535-42.
208. Piaget J. The Moral Judgment of the Child.London: Routledge and Kegan Paul 1932.
209. Pilowsky I. A general classification of abnormalillness behaviours. British Journal of MedicalPsychology, 1978;51(2):131-37.
210. Platt S, Weyman A, Hirsch S, et al. The SocialBehaviour Assessment Schedule (SBAS):Rationale, contents, scoring and reliability of anew interview schedule. Soc Psychiatry1980;15:43-55.
211. Powell GF, Brasel JA, Blizzard RM. Emotionaldeprivation and growth retardation simulatingidiopathic hypopituitarism. I. Clinical evaluationof the syndrome. New England Journal ofMedicine, 1967;276:1271-78.
212. Ramsden P. Student learning and perception ofthe academic environment. Higher Educ;1979;8:411-28.
213. Reisberg B, Ferris S, de Leon M, et al. The globaldeterioration scale (CDS): An instrument for theassessment of primary degenerative dementia(FDD). Am J Psychiatry; 1982;139:1136-39.
214. Reisberg B, Ferris S, de Leon M, et al. The globaldeterioration scale (CDS): An instrument for theassessment of primary degenerative dementia(PDD). Am J Psychiatry 1982;139:1136-39.
215. Reisberg B, Schneck M, Ferris S, et al. The briefcognitive rating scale (BCRS): Finding in primarydegenerative dementia (PDD). PsychopharmacolBull, 1983;19:47-50.
216. Reynolds W, Cormack D. Psychiatric and MentalHealth Nursning, Theory and Practice Chapmanand Hall, UK 1990.
217. Romano JM, Turner JA. Chronic pain anddepression: Does the evidence support therelationship? Psychol. Bull, 1985;9718-34.
218. Rosen W, Mohs R, Davis K. A new rating scalefor Alzheimer’s disease. Am J Psychiatry,1984;141:1356-64.
219. Rosensteil AK, Keefe FJ. The use of copingstrategies in chronic low back pain patients:Relationships to patient characteristics and currentadjustment. Pain, 1983;17:33-40.
220. Russell EW. A multiple scoring method for theassessment of complex memory functions. JConsult Clin Psychol 1975;43:800-09.
221. Salovey P, Mayer JD. Emotional intelligence.Imagination, cognition and personality1990;9:185.
222. Sarason IG. Life Stress, self-preoccupation andsocial supports. In Sarason IG, Spielberger CD(Eds). Stress and anxiety. New York: HemispherePublishing 1980;73-94.
223. Schachter S, Singer J. Cognitive social andphysiological determinants of emotional state.Psychological review. 1962;69:379-99.
224. Schellenberg JA. An invitation to socialpsychology. USA: Allyn and Bacon 1993.
225. Scott W. Measuring Mental Illness: PsychometricAssessment for Clinicians. American PsychiatricPress, Inc. 1989.
226. Seligman MEP. Helplessness: On depression,development and death. San Francisco: WHFreeman 1975.
227. Selye H. Stress in health and disease. Reading,MA: Butterworth 1976.
228. Selye H. The stress concept today. In IL Kutash,LB Schlesinger, et al (Eds). Handbook on stressand anxiety. San Francisco: Josey-Bass1980;127-29.
229. Selye H. The stress of life. New York: McGRAw-Hill 1956.
230. Selzer ML. The Michigan Alcoholism ScreeningTest: the quest for a new diagnostic instrument.Am J Psychiatry 1971;127:1653-58.
231. Serban G. Social Stress and FunctioningInventory for Psychotic Disorders (SSFIPD):measurement and prediction of schizophrenics’community adjustment. Compr Psychiatry1978;19:337-47.
Bibliography 251
232. Silverman D. Communication and medicalpractice: Social relations in the clinic. India: SagePublication 1987.
233. Skevington SM. Psychological aspects of pain inrheumatoid arthritis: A review, Soc Sci Med,1986;23:(6) 567-75.
234. Skinner BF. The behaviour of Organisms. NewYork: Appleton-Centure-Crofts 1938.
235. Skinner HA, Allen BA. Alcohol dependencesyndrome: Measurement and validation. JAbnorm Psychol 1982;91:199.
236. Skinner HA, Horn JL. Alcohol Dependence ScaleUser’s Guide. Toronto, Canada: AddictionResearch Foundation 1984.
237. Skinner HA. The drug abuse screening test.Addict Behav 1982;7:363-71.
238. Solnit A. Change and the sense of time. InAnthony EJ, Chilands C (Eds): The child and hisfamily: Children and Their Parents in a ChangingWorld. New York: Wiley 1978.
239. Spitzer R, Williams J, Gibbon M, et al. StructuredClinical Interview for DSM-III-R-Patient Version.New York: Biometrics Research Department,New York State Psychiatric Institute 1988.
240. Spurgeon P, Roy D, Chapman T. Elements ofApplied Psychology. Switzerland: HardwoodAcademic Publishers 1994.
241. Stemberg RJ. Metaphors of Mind: Conceptionsof the Nature of Intelligence. New York:Cambridge University Press 1984.
242. Sternberg RJ. Beyond IQ New York: CambridgeUniversity Press 1985.
243. Stewart M, Roter D (Eds). Communicating withMedical Patients. Sage Publication 1989.
244. Thompson WD, Orvaschel H, Prusoff BA, et al.An evaluation of the family history method forascertaining psychiatric disorders, Arch GenPsychiatry 1982;39:53-58.
245. Thurstone LL. Primary Mental Abilities. Chicago:University of Chicago Press 1938.
246. Turk DC, Meichenbaum D, Genest M. Pain andbehavioural medicine: A cognitive behaviouralperspective. New York: Guilford Press 1983.
247. Turner JA, Chapman CR. Psychologicalinterventions for chronic pain: A critical review.I. Relaxation training and biofeedback. Pain,1981;12(1):1-21.
248. Turner JA, Chapman CR. Psychological inter-ventions for chronic pain. A critical review-II.
Operant conditioning, hypnosis, and cognitive-behaviour therapy. Pain, 1982;12(1):23-46.
249. Turner JA, Clancy S, Vitaliano PP. Relationshipsof stress, appraisal and coping, to chronic low-
back pain. Behav Res Ther, 1987;25:281-88.
250. Vaughn C, Leff J. The measurement of expressedemotion in the families of psychiatric patients.
British Journal of Social and Clinical Psychology
1976;15:157-65.251. Verma K, IX Monte B, Adkoli BV, Nayar U, Kacker
SK. Inquiry Driven Strategies for Innovation in
Medical Education: Experiences in India. IndianJ Pediatr 1993;60:739-49.
252. Wasir HS. Traditional Wisdom for Heart Care.
New Delhi: Vikas Publishing House 1995.253. Weakland J. O.K. - You have been a bad mother.
In: Papp P (Ed): Family Therapy: Full Length Case
Studies. New York: Gardner Press 1977.254. Wechsler D. A standardized memory scale for
clinical use. J Psychol 1945;19:87-95.
255. Wechsler D. The measurement of adultintelligence (3rd ed). Baltimore: Williams &
Wilkins 1944.
256. Weissman M, Sholomskas M, John K. The
assessment of social adjustment: an update. Arch
Gen Psychiatry 1981;38:1250-58.
257. Wetzler S. Measuring Mental Illness: Psychometric
Assessment for Clinicians (1982). Washington:
American Psychiatric Press Inc 1989.
258. Wetzler S. Measuring Mental Illness: Psychometric
Assessment for Clinicians. Washington: American
Psychiatric Press, Inc. 1989.
259. Wooley SC, Blackwell B, Winget C. A learning
theory model of chronic illness behaviour:
Theory, treatment and research. Psychosomatic
Medicine, 1978;40:379-401.
260. Wooley SC, Blackwell B, Winget C. A learning
theory model of chronic illness A: Theory,
treatment and research. Psychosomatic Medicine,
1978;40:379-401.
261. Wooley SC, Blackwell B. A Behavioural probe
into social contingencies on a psychosomatic
ward. Journal of Applied Behaviour Analysis,
1975;8:337-39.
262. World Health Organization. Doctor-patient
interaction and communication. Geneva 1983.
263. Zung W. A self-rating depression scale. Arch Gen
Psychiatry 1965;12:63-70.


Index
A
Adolescence 116clinical applications 120ego and identity 119emotions 117
adolescent love 117anger 117anxiety 117relationship with peers 118sexuality 117
personality and social deve-lopment 120
Adulthood 124stages in adult development
124age 30 transition 125early adult transition 124entering the adult world
125midlife transition 125setting down 125
Alcohol dependence scale 172Assessment in behavioural
sciences 161assessment interviews 163clinical observation 163goals 161personality tests 170psychological assessment 165
attention and concen-tration 165
memory assessment 165neuropsychological
assessment165
perception 165
psychological tests 163objectives 164
questionnaires 171
rating scales 170self-assessment 163
semiprojective test 171
sources 162physical evaluation 162
psychosocial assessment
162Attention 19
attention deficit 23
clinical applications 22factors facilitating attention 20
external factors 20
internal factors 20types 20
automatic and conscious
processing 21divided attention 21
selective attention 20
sustained attention 21Attitudes 138
assessment 143
indirect methods 144observational rating scales
144
rating scales 143developments 140
family 140
peers 140methods to change attitudes
142
nature 138role of attitudes in nursing
139
B
Beck’s cognitive model 196Behaviour medicine 206
applications 208chronic pain 208headache 208
biopsychosocial contexts ofproblems 206
aetiology 206compliance 207disease mechanism 206host-resistance 206intervention 207patient-decision making
206health promotion 209
AIDS prevention 210diabetes 211exercise adherence 209management of stress
210medication adherence
210smoking cessation 209
techniques 207self-monitoring 207stimulus control 207
Behaviour therapy 185applications 192
behavioural training 193behavioural training for
mentallysubnormalchildren 192
assessment 187characteristics 186

254 Behavioural Sciences in Medical Practice
foundation 185process 187treatment methods 188
aversion therapy 191biofeedback training 188contingency contracting
192exposure 189hypnosis 189operant conditioning 191procedure 190relaxation training 188social skills training 191
Behavioural sciences 1scope 3
doctor-patient relationship3
health and illnessbehaviour 4
hole of self-attention onsymptomamplication 5
human development 4illness-disability
perception 5impact of social support
5importance of self-efficacy
5psychophysical relations
4social class and health
behaviour 4subject content 2
Bereavement 134characteristics 137clinical applications 135stages 134
C
Cognitive behaviour therapy196
behavioural analysis 199clinical applications 203cognitive approaches 197cognitive learning therapies
198methods of assessment 199process 198
self-monitoring 200strategies for treatment of
depression203
techniques 200activity schedules 201distraction 201modelling 203problem solving 201rehearsal 202role-playing 202self-statements 201thought stopping 200
theoretical basis 196treatment of anxiety 204
Coloured progressive matrices 174Communication skills 212
assessment 220components 213
closing the interview 214empathy, and warmth
213greeting patients 213language 213listening 213
specific situations 214breaking bad news 217information gathering
214strategies to communicate bad
news 218allow patient time to
integrateinformation219
never tell the patient afalsehood 219
patient control over thequantity 219
plan in mind beforestarting 218
soften bad news withgood news219
Compliance 155assessment 159clinical application 159
accommodation 160change in therapeutic
regimen 160
education 159enhancement of doctor-
patientrelationship160
modification ofenvironmentaland socialfactors 160
factors related to compliance158
patient characteristics 158provider characteristics
159types 156
contact with healthprovider 157
lifestyle changes 157medication compliance
157Coping with stress 93
assessment of stress andcoping 95
clinical applications 95disease-related problem 97effect of stress on health
95sickness-related problems
97family coping 94stress-inoculation training 94vulnerability 97
Coronary heart disease 107Counselling 177
characteristics 181communication 181empathy 182warmth 181
counselling in health care 183goals 179process 182
change of utililsation 183closing phase 183counselling structure 183emphasis on strength
183necessary support 183
respect 182client expectations 182genuineness 182

Index 255
skills 179attending 180initiating 180passive listening 179perceiving 180responding 180summarising 180
D
Dartmouth pain questionnaire235
Drug abuse screening test 172
E
Ellis based on rational emotivebehaviourtherapy 196
Emotion 77adrenal glands 79autonomic nervous system
78parasympathetic nervous
system 79sympathetic nervous
system 78clinical applicational 85cognitive factors 82emotional expression 84
innate emotionsexpression 84
general adaptation syndrome80
homeostatic balance 79intrapsychic aspects 81physiology 78role of learning in emotional
arousal 83theoretical explanation 80
Cannon-Bard theory ofcentral neuralprocesses 81
James-Lange theory ofbodily reactions80
Lasarus-Schachter theory81
types 83
F
Family 146
affective involvement 149
clinical application 153
communication in families 150
control styles 149
family counselling 153
family temperament 150
family therapy 153
pathology 150
role of family in health and
illness 147
structure 146
systems theory 151
equifinality 151
feedback 151
homeostasis 151
wholeness 151
values and norms 149
Forgetting 28
amnesia 30
alcohol and drug abuse 30
biological amnesias 30
childhood amnesia 30
defensive amnesia 31
normal aging 31
psychological amnesia 30
senile dementia 30
transient global amnesia
30
clinical applications 33
encoding 33
retrieval 34
storage 34
clinical assessment 33
interference 28
methods to improve memory
31
chunking 32
making a story 32
method of loci 31
mnemonics 31
pegword method 31
remembering names and
faces 32
rhyming 32
motivated forgetting 29
I
Illness behaviour 222abnormal illness behaviour
223causes of maladaptive illness
behaviour 224disposition 224psychodynamic 225social learning 225sociocultural influences
224clinical applications 227management 226psychosocial adaptation to
illness 225sick role 223
absence pf responsibility223
being sick is undesirable223
seeking adequate help223
Infancy and childhood 111cognitive development 112
concrete operational stage112
preoperational stage 112sensory motor stage 112stage of formal operations
113psychosexual development
113anal stage 113latency period 114oral stage 113phallic stage 114
psychosocial development 114autonomy vs shame,
doubt 115generativity vs stagnation
115identity vs identity
confusion 115industry vs inferiority 115initiative vs guilt 115integrity vs despair 116intimacy vs isolation 115trust vs mistrust 115

256 Behavioural Sciences in Medical Practice
Intelligence 48clinical applications 56determinants of intelligence 53
environment 54heredity 53
emotional intelligence 51extremes of intelligence 54
mental subnormality 54growth of intelligence 52intelligence quotient 51nature 48
information processingtheories 50
multifactor theories 49primary mental abilities 49process oriented theories
49two factor theory 49
normal distribution ofintelligence 56
stability of intelligence 53
L
Learning 35avoid undue anxiety 43biological learning 41
contraprepared 41prepared 41unprepared 41
classical conditioning 36acquisition 36discrimination 36stimulus generalization 36stimulus substitution 36
cognitive learning 39insight learning 40sign learning 40
distribution of practiceperiods 43
knowledge of results 43latent learning 41logical learning 43observational learning 40operant conditioning 37
nature of reinforcers 37reinforcement 37schedule of reinforcement
38
principles of learning 41contextual 42feedback 43individuality of learner 42role of motivation 42
rational use of media 44social learning 40
Learning styles 44clinical applications 46role of teachers in facilitating
learning 46student autonomy 45
steps 45
M
McGill pain questionnaire (MPQ)235
Memory 24memory process 24memory systems 25
episodic memory 27long-term memory 27rehearsal 27semantic memory 27sensory memory 26short-term memory 26working memory 26
types 28Memory questionnaires 167Methods to deal with dying
patients 133Michigan alcoholism screening
test 172Middle adulthood 126
physical changes 126intelligence and memory
126parenthood and deve-
lopment 127personality 127
Motivation 67arousal and curiosity 72classification 70
achievement motive 71aggression motive 71hunger motive 71
clinical applications 73indications 67
models 67drive model 67homeostatic model 68humanistic model 69social cognitive model 70
motivational basis of addictivebehaviour 74
eating disorders 74motives and conflict 72
OOld age or the senescence 128
clinical applications 130developmental tasks 128health changes 128personality changes 129psychological changes 128
intelligence 128learning and memory 128
social changes 130stressful life events 130
PPerception 8
clinical applications 16hallucinations 17pain perception 16perceptual function 16sensory defects 16sensory deprivation 17
extrasensory perception 14perception as developmental
process 13perceptual processes 8
depth perception 9form perception 8movement perception 10visual pattern perception 9
social perception 15attribution 15
Personality 100behaviour patterns and
coronary heartdisease 108
clinical applications 109determinants 100
environment 101heredity 101
Index 257
personality related to illness107
theories 102humanistic approach 106psychodynamic theories
102social learning theories
106trait and type theories
104type A and physiological
reactivity 108PGI memory scale 167Psychological assessment of
children 173Psychology of pain 229
coping with chronic pain 232gate control theory 230methods to assess pain
profile 232behavioural analysis 235history of pain 233quantification of pain 233questionnaires 234
pain in elderly 240physiological and
psychosocialmodels of pain230
psychological approaches topain control238
biofeedback training 239cognitive-behavioural
approach 239hypnosis 239operant therapy 238relaxation training 239
psychological evaluation 236depression 237life stress 237psychological dysfunction
237somatisation disorders 237
S
Sensation 7Stress 88
components 88executive stress 92family stress 91personality and stress 93stress-esteem 92test anxiety 92types 89
daily hassles 90stressful life events 90
T
Thinking 58blocks in cognitive process 64clinical applications 65decision making 63different theories 62
gestalt theory 62information processing
theory 62learning theory 62
functions 61problem solving 61reasoning 61
judging 64neurological basis 60types 61
convergent and divergentthinking 61
purposive and fantasythinking 61
WWechsler intelligence scale for
children 174
ZZeigarnik effect 30