managing diabetes and hyperglycemia how to improve inpatient care diabetes special interest group...
TRANSCRIPT

Managing Diabetes and Hyperglycemia
How To Improve Inpatient Care
Diabetes Special Interest Group Georgia Hospital Association

Objectives for Modules 1 - 7
• Increase awareness of the importance of controlling inpatient hyperglycemia
• Provide guidelines for recognizing and triaging patients with hyperglycemia
• Describe hyperglycemia management techniques
Learning Modules
Module Topic
1 Hyperglycemia and hospital outcomes
2 Challenges and opportunities for care improvement
3 Initial recognition, triaging, and management
4 Pharmacologic management: Insulin 1
5 Pharmacologic management: Insulin 2
6 Review of policies and procedures
7 Getting patients ready for discharge
This course consists of 7 on-line modules. You will also be asked to complete a pre-course survey and module post-tests.
Module One Objectives
1.Describe the prevalence of diabetes and hyperglycemia in the inpatient population
2.Understand the relationship between hospital hyperglycemia and patient outcomes
3.Review the mechanisms of glucose damage in hospitalized patients

Pre-Course SurveyGlycemic Control: A Survey of
Current Practices
1. Does your facility assess glucose on admission for all patients?
2. Is it a policy at your facility to obtain an A1C on all patients with elevated glucose levels if one is not available from the past 60 days?
3. Does your facility have established glucose targets for various departments?

Pre-Course Survey Continued
4. Does your facility track the prevalence of hyperglycemia?
5. Does your facility track length of stay and infection rates related to the incidence of hyperglycemia?
6. Does your facility track the prevalence of hypoglycemia?
Pre-Course Survey Continued
7. Does your facility investigate the cause of hypoglycemia when it occurs?
8. Does your facility have guidelines for managing hyperglycemia?
9. Does your facility have guidelines for treating hypoglycemia?
Pre-Course Survey Continued
10. Is hyperglycemia a patient safety concern at your facility?11. Does your facility use clinical information systems to monitor glucose control?12.Does your facility have a standardized
curriculum for teaching patients about diabetes self-care?

Section 1
Prevalence of Diabetes and Hyperglycemia
in the Hospital
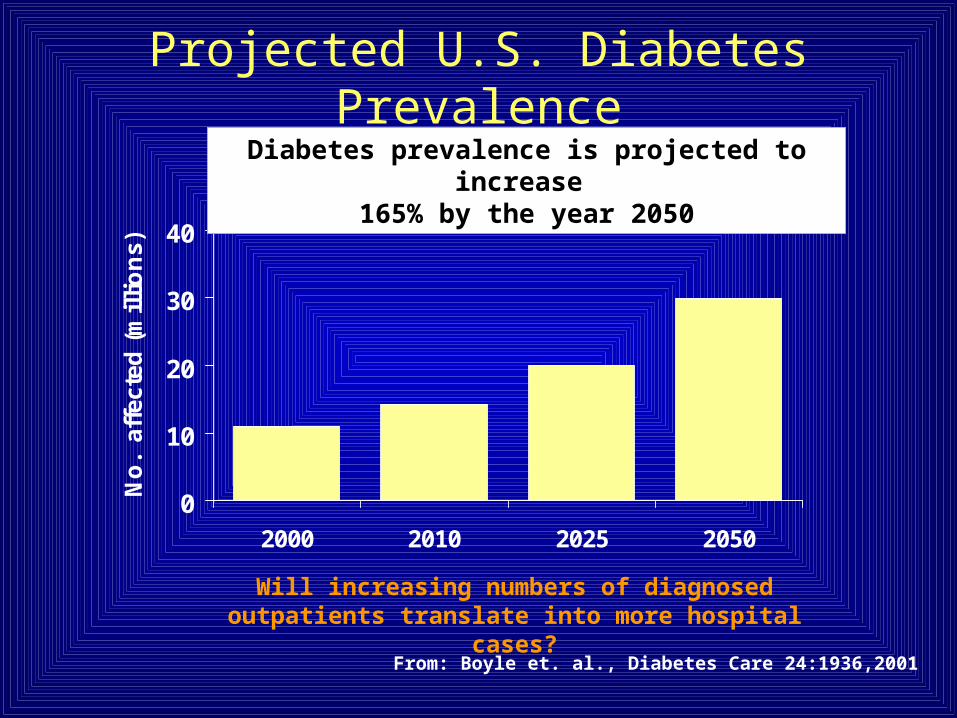
Projected U.S. Diabetes Prevalence
0
10
20
30
40
2000 2010 2025 2050
No
. a
ffec
ted
(m
illi
on
s)
From: Boyle et. al., Diabetes Care 24:1936,2001
Diabetes prevalence is projected to increase 165% by the year 2050
Will increasing numbers of diagnosed outpatients translate into more hospital cases?

Changes in US Diabetes-Related Hospitalizations
Data from Centers for Disease Control and Prevention, available at http://www.cdc.gov/diabetes/statistics/dmany/index.htm
Hospitalizations with diabetes
have been rising

National Hospital StatisticsDiabetes is the fourth most common co-morbidity encountered in the inpatient setting.
– 562,000 discharges as primary diagnosis– 4 million discharges listed with diabetes overall
Hospitalization represents the highest expense of diabetes care, with one third of patients requiring more than 2 hospitalizations per year.
Background: Cost of Poor Quality
• Projected total direct and indirect costs of diabetes:– In 2007 $174 billion– In 2025, up to $351 billion
• “Honeycutt, et al, projects an increase in diagnosed diabetes from 12 million in 2000 to 39 million in 2050.”
Source: Diabetes Care 31:596-615, 2008
Diabetes Forecasts to 2025 and Beyond: The Looming Crisis Demands Change

Joint Commission, ADA collaborate on Inpatient Diabetes Care Certification
Two of the nation's leaders in improving health care for Americans are collaborating to recognize hospital inpatient diabetes programs that meet national quality standards and raise the quality of care provided to patients with diabetes.
Regulatory Response

Regulatory Response Continued
Organizations seeking inpatient diabetes care certification undergo an on-site review of their compliance with national standards and the management of diabetes patients through clinical guidelines.
The review also includes an assessment of performance measurement and
improvement activities..
Regulatory Response Continued
In addition, organizations are assessed regarding the qualifications and competencies of practitioners; processes established to encourage patient self-management; demonstrated leadership support for the program; and use of clinical information systems to monitor patient care management.
News release, 20 July 2006
Section 2
The Relationship Between Hyperglycemia and
Hospital Outcomes

Hyperglycemia in Hospitalized Patients
• Hyperglycemia (>200 mg/dL x 2) occurred in 38% of hospitalized patients
- 26% had known history of diabetes- 12% had no history of diabetes
• Newly discovered hyperglycemia was associated with:- Longer hospital stays- Higher admission rates to intensive care units- Less chance to be discharged to home (required more
transitional or nursing home care)
Umpierrez GE, et al. J Clin Endocrinol Metab. 2002;87:978–982.
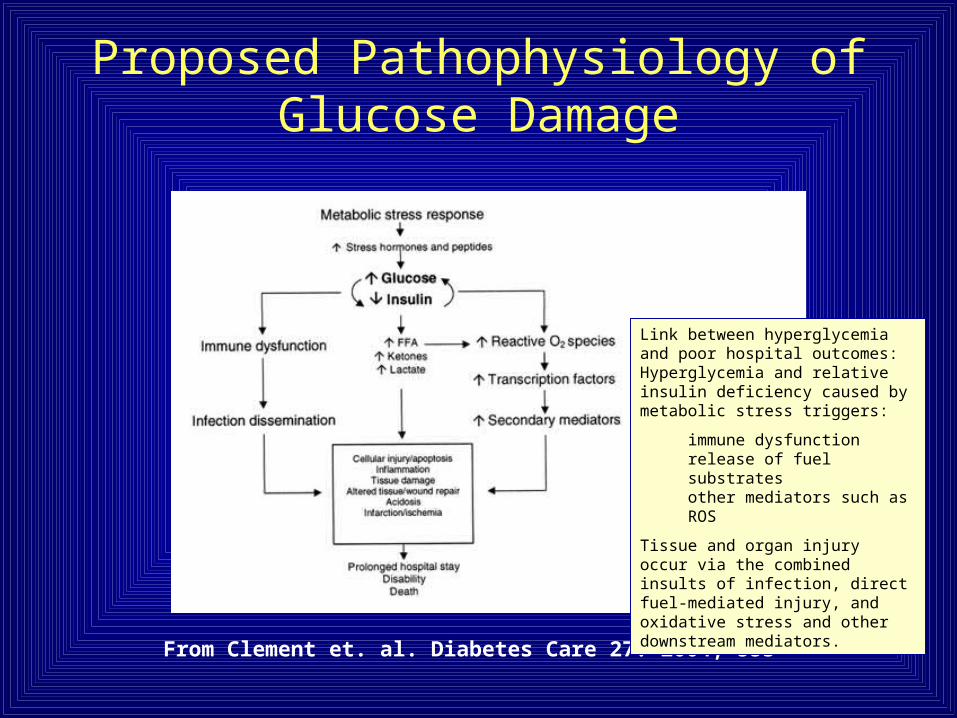
From Clement et. al. Diabetes Care 27: 2004, 553
Link between hyperglycemia and poor hospital outcomes: Hyperglycemia and relative insulin deficiency caused by metabolic stress triggers:
immune dysfunctionrelease of fuel substratesother mediators such as ROS
Tissue and organ injury occur via the combined insults of infection, direct fuel-mediated injury, and oxidative stress and other downstream mediators.
Proposed Pathophysiology of Glucose Damage
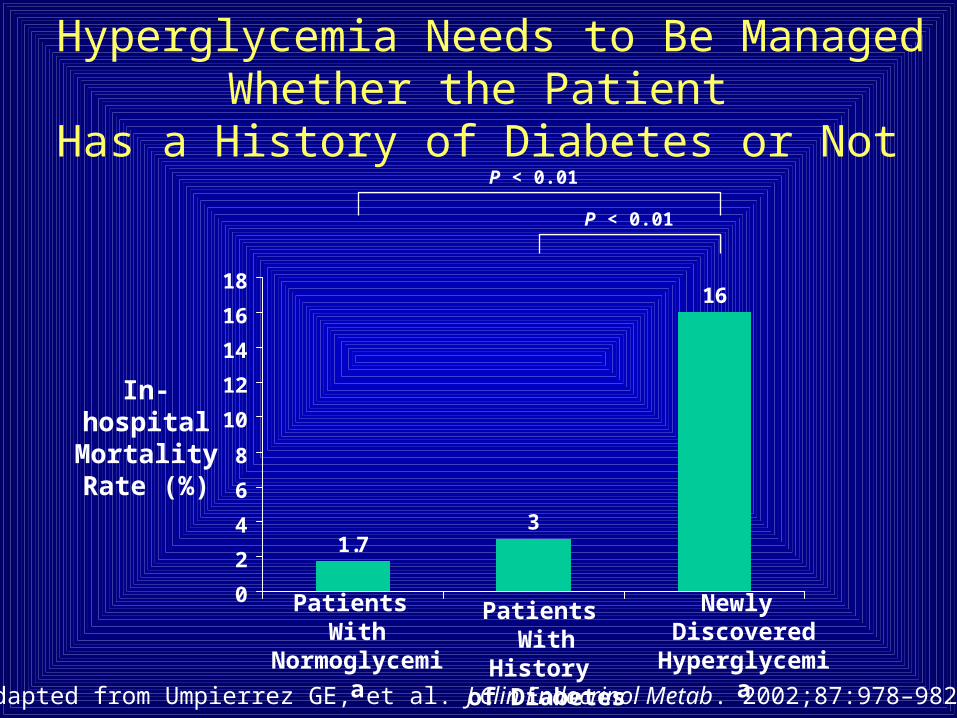
Hyperglycemia Needs to Be Managed Whether the Patient
Has a History of Diabetes or Not
Adapted from Umpierrez GE, et al. J Clin Endocrinol Metab. 2002;87:978–982.
1.73
16
0
2
4
6
8
10
12
14
16
18
In-hospital Mortality Rate (%)
Newly Discovered
Hyperglycemia
Patients With History of Diabetes
Patients With
Normoglycemia
P < 0.01
P < 0.01

05
1015202530354045
80-99 100-119
120-139
140-159
160-179
180-199
200-249
250-299
>300
Average ICU glucose (mg/dL)
Mor
talit
y %
Hyperglycemia and Hospital Mortality1826 consecutive ICU patients 10/99 thru 4/02, Stamford CT
Krinsley JS: Mayo Clin Proc 78: 1471-1478, 2003

Tight Glycemic Control in Critically Ill Patients
Decreases Morbidity and Mortality
van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.
-60
-50
-40
-30
-20
-10
0
Percent Reduction
Mortality Sepsis Dialysis PolyneuropathyBlood
Transfusion
34%
46%41%
44%50%
1548 patients: 153 vs 103 mg/dL1548 patients: 153 vs 103 mg/dL
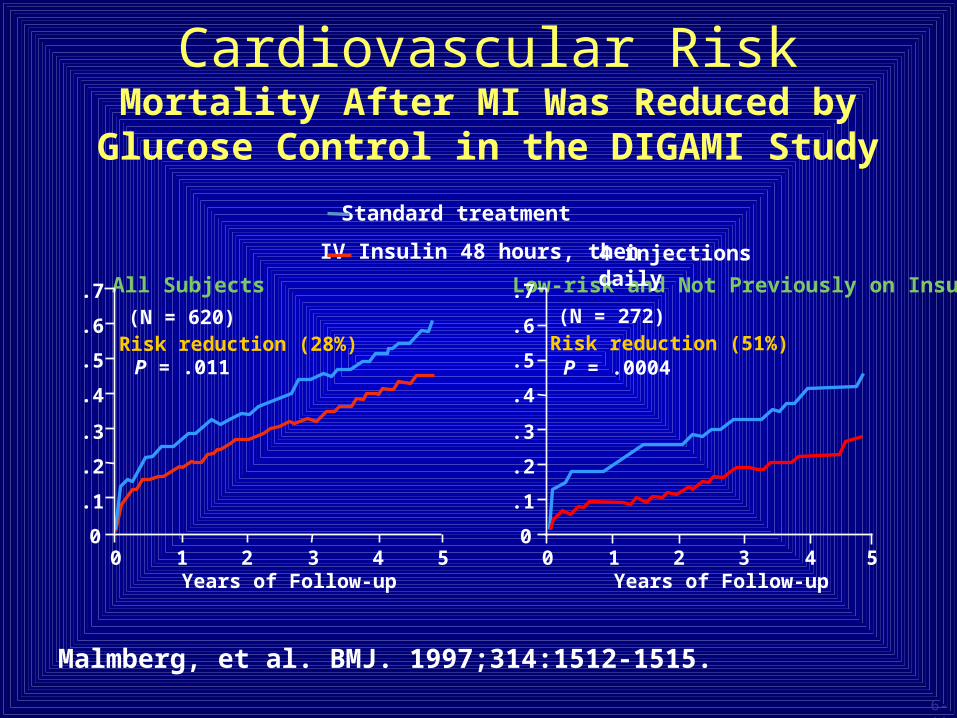
Cardiovascular RiskMortality After MI Was Reduced by Glucose
Control in the DIGAMI Study
Malmberg, et al. BMJ. 1997;314:1512-1515.
All Subjects
(N = 620)Risk reduction (28%)
P = .011
Standard treatment
0
.3
.2
.4
.7
.1
.5
.6
0 1Years of Follow-up
2 3 4 5
Low-risk and Not Previously on Insulin
(N = 272)Risk reduction (51%)
P = .0004
IV Insulin 48 hours, then 4 injections daily
0
.3
.2
.4
.7
.1
.5
.6
0 1Years of Follow-up
2 3 4 5
6-11

Acute MI Data
• Elevated glucose levels predict mortality in acute MI patients with and without diabetes
• Elevated glucose levels in STEMI is associated with larger infarct size in patients without history of diabetes
• Meta-analysis of 15 studies of patients with acute MI reports higher mortality and more frequent CHF when glucose >110 mg/dL
Sala J, et al. J Epidemiol Community Health. 2002;56:707-712.
Kosiborod M, et al. Circulation. 2005;111:3078-3086.
Timmer J, et al. Am Heart J. 2004;148:399-404.
Capes S, et al. Lancet. 2000;355:773-778.
General Surgery
When blood glucose exceeds 200
• Renal threshold is exceeded leading to increased urine output
• Dehydration
• Electrolyte swings
• Impaired WBC function
RABBIT 2 Trial(Randomized Study of Basal-Bolus
Insulin Therapy in the Inpatient Management of Patients
With Type 2 Diabetes)
• Multicenter non-ICU hospital setting• 130 Type 2, insulin naive patients • Started insulin for BGs > 140• Randomized to Multiple Daily Injections (MDI)
or Sliding Scale Insulin (SSI) Therapy

RABBIT continued• MDI with glargine and glulisine insulin dosage for BG 140-200 was 0.4 U/Kg/day dosage for BG 201-400 was 0.5 U/Kg/day• SSI with Regular insulin• MDI: BG<140, 66% of the time• SSI: BG<140, only 38%• Despite increasing insulin doses, 14% in the SSI
group maintained BGs > 240 • There was NO DIFFERENCE IN RATE OF
HYPOGLYCEMIA
Source: Diabetes Care 30:2181-2186, 2007

Serum Glucose > 220 on POD 1 (Study of 100 elective surgery patients excluding “minor” post-op
infections UTI) • BG > 220 mg/dL on post-op day #1 increased
risk of serious infections 5.8 TIMES !• Consider the brief doubling time of many
bacteria (E.Coli as little as 20 minutes), a few hours of impaired host resistance can allow growth of bacterial pathogen/clinically significant infection
• Two hours hyperglycemia results in impaired WBC function for weeks
• Pomposelli JJ, Jour Parenteral and Enteral Nutrition 22: 77-81., 1998
Section 3
Treating Hyperglycemia
in the Hospital
Improves Outcomes
Was It Van den Berghe?“Diabetic patients requiring major operations, such as appendectomy, cholecystectomy, and tonsillectomy, or removal of teeth, are first rendered sugar- and acetone-free, unless the severity of symptoms demand immediate attention. Patients formerly considered bad surgical risks, if given proper dietetic treatment with insulin may be protected from the acidosis, hyperglycaemia, and glycosuria which otherwise usually result from the anaesthetic. In the diabetic, infections such as boils and carbuncles, and also intercurrent infections such as bronchitis, influenza, and fevers are favorably influenced by the normal blood sugar and increased metabolism which the administration of insulin permits. In the diabetic with tuberculosis, insulin allows the administration of proper nourishment to combat the tubercle infection.”
Source: F. G. Banting, Nobel Lecture, Sept. 15, 1925

Frederick Grant BantingNobel Lecture, September 15, 1925
• Healing may be achieved by the use of insulin
• Due to the infection, there is a marked variation in the insulin production
• Patients remain on insulin for varying periods after the procedure
• Mild hypoglycemia suggesting an overdose of insulin occurs by 3 to 4 weeks

84+ Years LaterSummary and Recommendation
• Diabetes is epidemic and increasing• Hospitalizations are common among diabetes patients• Studies concur that in the hospital:
– Hyperglycemia is bad– Euglycemia (normal glucose) is good
• Recommended upper limits for inpatient glycemic targets Non-critical care units
Intensive care units Preprandial Maximal glucose
110 mg/dl 110 mg/dl 180 mg/dl
American College of Endocrinology Position Statement on Inpatient Diabetes and Metabolic Control. Endocrine Practice 10:77, 2004

The Goals of Insulin Therapy…..
• are to maintain the blood glucose in the target range and
• to achieve early identification and treatment of hyperglycemia
• thereby reducing infections, length of stay, and costs,
• and improving outcomes. ICU < 110 mg/dL Med/Surg < 180
References• American Diabetes Association. “Economic Costs of Diabetes in the U.S. In 2007.”
Diabetes Care 31: 596-615, 2008.
• Banting, F. G. Nobel Lecture 09-15-1925.
• Boyle, J. P., A. A. Honeycutt, et al. (2001). "Projection of diabetes burden through 2050: impact of changing demography and disease prevalence in the U.S." Diabetes Care 24(11): 1936-40.
• Clement, S., S. S. Braithwaite, et al. (2004). "Management of diabetes and hyperglycemia in hospitals. [erratum appears in Diabetes Care. 2004 Mar;27(3):856 Note: Hirsh, Irl B [corrected to Hirsch, Irl B]; dosage error in text]." Diabetes Care 27(2): 553-91.
• Gandhi, G. Y., G. A. Nuttall, et al. (2005). "Intraoperative hyperglycemia and perioperative outcomes in cardiac surgery patients." Mayo Clinic Proceedings 80(7): 862-6.
• Krinsley, J. S. (2004). "Effect of an intensive glucose management protocol on the mortality of critically ill adult patients. [see comment] [erratum appears in Mayo Clin Proc. 2005 Aug;80(8):1101]." Mayo Clinic Proceedings 79(8): 992-1000.
• Krinsley, J. S. and R. L. Jones (2006). "Cost analysis of intensive glycemic control in critically ill adult patients." Chest 129(3): 644-50.
References
• Providence Health System: The Portland Protocol Retrieved September 7, 2007 http://www.providence.org/Oregon/Programs_and_Services/Heart/portlandprotocol/default.htm
• Umpierrez, G. E. , et al. (2007). “Randomized Study of Basal-Bolus Insulin Therapy in the Inpatient Management of Patients With Type 2 Diabetes.” Diabetes Care 30:2181-2186.
• Umpierrez, G. E., S. D. Isaacs, et al. (2002). "Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. [see comment]." Journal of Clinical Endocrinology & Metabolism 87(3): 978-82.
• Van den Berghe, G., A. Wilmer, et al. (2006). "Intensive insulin therapy in the medical ICU. [see comment]." New England Journal of Medicine 354(5): 449-61.
• van den Berghe, G., P. Wouters, et al. (2001). "Intensive insulin therapy in the critically ill patients. [see comment]." New England Journal of Medicine 345(19): 1359-67.
• Yendamuri, S., G. J. Fulda, et al. (2003). "Admission hyperglycemia as a prognostic indicator in trauma." Journal of Trauma-Injury Infection & Critical Care 55(1): 33-8.