management of hyperglycemia in type 2 diabetes, 2018. a ... · management of hyperglycemia in type...
TRANSCRIPT

Management of Hyperglycemiain Type 2 Diabetes, 2018.A Consensus Report by theAmerican Diabetes Association(ADA) andtheEuropeanAssociationfor the Study of Diabetes (EASD)https://doi.org/10.2337/dci18-0033
The American Diabetes Association and the European Association for the Study ofDiabetes convened a panel to update the prior position statements, published in2012 and 2015, on the management of type 2 diabetes in adults. A systematicevaluation of the literature since 2014 informed new recommendations. Theseinclude additional focus on lifestyle management and diabetes self-managementeducation and support. For those with obesity, efforts targeting weight loss,including lifestyle, medication, and surgical interventions, are recommended.Withregards to medication management, for patients with clinical cardiovasculardisease, a sodium–glucose cotransporter 2 (SGLT2) inhibitor or a glucagon-likepeptide 1 (GLP-1) receptor agonist with proven cardiovascular benefit is recom-mended. For patients with chronic kidney disease or clinical heart failure andatherosclerotic cardiovascular disease, an SGLT2 inhibitor with proven benefit isrecommended. GLP-1 receptor agonists are generally recommended as the firstinjectable medication.
The goals of treatment for type 2 diabetes are to prevent or delay complications andmaintainquality of life (Fig. 1). This requires control ofglycemiaandcardiovascular riskfactormanagement, regular follow-up, and, importantly, apatient-centeredapproachto enhance patient engagement in self-care activities (1). Careful consideration ofpatient factors and preferences must inform the process of individualizing treatmentgoals and strategies (2,3).This consensus report addresses the approaches to management of glycemia in
adults with type 2 diabetes, with the goal of reducing complications and maintainingquality of life in the context of comprehensive cardiovascular risk management andpatient-centered care. The principles of how this can be achieved are summarized inFig. 1 and underpin the approach to management and care. These recommendationsarenot generally applicable topatientswithmonogenic diabetes, secondarydiabetes,or type 1 diabetes, or to children.
Data Sources, Searches, and Study SelectionThe writing group accepted the 2012 (4) and 2015 (5) editions of this positionstatement as a starting point. To identify newer evidence, a search was conducted onPubMed for randomized clinical trials (RCTs), systematic reviews, and meta-analyses
1Diabetes Research Centre, University of Leices-ter, Leicester, U.K.2Leicester Diabetes Centre, Leicester GeneralHospital, Leicester, U.K.3DepartmentofMedicine,DukeUniversitySchoolof Medicine, Durham, NC4National Institute of Diabetes and Digestiveand Kidney Diseases, National Institutes ofHealth, Bethesda, MD5Department of Medicine, Yale School of Med-icine, New Haven, CT6Clinical and Experimental Endocrinology, UZGasthuisberg, KU Leuven, Leuven, Belgium7Department of Internal Medicine, Catholic Uni-versity, Rome, Italy8DiabetesandNutritional Sciences,King’sCollegeLondon, London, U.K.9Steno Diabetes Center Copenhagen, Gentofte,Denmark10University of Copenhagen, Copenhagen, Den-mark11Second Medical Department, Aristotle Univer-sity Thessaloniki, Thessaloniki, Greece12Department of Medicine and Diabetes Unit,Massachusetts General Hospital, Boston, MA13Harvard Medical School, Boston, MA14Department of Medicine, University of NorthCarolina School of Medicine, Chapel Hill, NC
Corresponding author: John B. Buse, [email protected].
M.J.D.andJ.B.B.wereco-chairs for theConsensusStatement Writing Group. D.A.D’A., J.F., W.N.K.,and D.J.W. were the writing group members forthe American Diabetes Association. C.M., G.M.,P.R., andA.T.werewritinggroupmembers for theEuropean Association for the Study of Diabetes.
This article is being simultaneously published inDiabetes Care and Diabetologia by the AmericanDiabetes Association and the European Associ-ation for the Study of Diabetes.
© 2018 American Diabetes Association andEuropean Association for the Study of Diabetes.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
Melanie J. Davies,1,2 David A. D’Alessio,3
Judith Fradkin,4 Walter N. Kernan,5
Chantal Mathieu,6 Geltrude Mingrone,7,8
Peter Rossing,9,10 Apostolos Tsapas,11
Deborah J. Wexler,12,13 and John B. Buse14
Diabetes Care 1
CONSEN
SUSREP
ORT
Diabetes Care Publish Ahead of Print, published online October 4, 2018

Figure
1—Decisioncycleforpatient-centeredglycem
icmanagem
entin
type
2diabetes.
2 Consensus Report Diabetes Care

published in English between 1 January2014 and 28 February 2018; eligiblepublications examined the effectivenessor safety of pharmacological or nonphar-macological interventions in adults withtype 2 diabetes mellitus. Reference listswere scanned in eligible reports to iden-tify additional articles relevant to the sub-ject. Details on the keywords and thesearch strategy are available at https://doi.org/10.17632/h5rcnxpk8w.1. Paperswere grouped according to subject, andthe authors reviewed this new evidence toinform the consensus recommendations.The draft consensus recommendationswere peer reviewed (see “Acknowledg-ments”), and suggestions incorporatedas deemed appropriate by the authors.Nevertheless, though evidence-based,the recommendations presented hereinare the opinions of the authors.
The Rationale, Importance, andContext of Glucose-LoweringTreatmentLifestylemanagement, includingmedicalnutrition therapy (MNT), physical activ-ity, weight loss, counseling for smokingcessation, and psychological support,oftendelivered in the context of diabetesself-management education and support(DSMES), are fundamental aspects ofdiabetes care. The expanding numberof glucose-lowering treatmentsdfrombehavioral interventions to medica-tions and surgerydand growing infor-mation about their benefits and risksprovides more options for people withdiabetes and providers, but can compli-cate decision making. In this consen-sus statement, we attempt to providean approach that summarizes a largebody of recent evidence for practi-tioners in the U.S. and Europe.Marked hyperglycemia is associated
with symptoms including frequent uri-nation, thirst, blurred vision, fatigue, andrecurring infections. Beyond alleviat-ing symptoms, the aim of blood glu-cose lowering (hereafter, referred toas glycemic management) is to reducelong-term complications of diabetes.Good glycemic management yields sub-stantial and enduring reductions in on-set and progression of microvascularcomplications. This benefit has beendemonstrated most clearly early in thenatural history of the disease in studiesusing metformin, sulfonylureas, and in-sulin but is supported by more recent
studies with other medication classes.The greatest absolute risk reduction(ARR) comes from improving poor gly-cemic control, and a more modest re-duction results from near normalizationof glycemia (6). The impact of glucosecontrol on macrovascular complica-tions is less certain. Because the bene-fits of intensive glucose control emergeslowly, while the harms can be immedi-ate, people with longer life expectancyhave more to gain from intensive glu-cose control. A reasonable HbA1c targetfor most nonpregnant adults with suffi-cient life expectancy to see microvascu-lar benefits (generally ;10 years) isaround 53 mmol/mol (7%) or less (6).Glycemic treatment targets should beindividualized based on patient prefer-ences and goals, risk of adverse effectsof therapy (e.g., hypoglycemia andweight gain), and patient characteris-tics, including frailty and comorbidconditions (2).
Atherosclerotic cardiovascular dis-ease (ASCVD) is the leading cause ofdeath in people with type 2 diabetes(7). Diabetes confers substantial inde-pendent ASCVD risk, and most peoplewith type 2 diabetes have additional riskfactors such as hypertension, dyslipide-mia, obesity, physical inactivity, chronickidney disease (CKD), and smoking. Nu-merous studies have demonstratedthe benefits of controlling modifiableASCVD risk factors in people with di-abetes. Substantial reductions in ASCVDevents and death are seen when multi-ple ASCVD risk factors are addressedsimultaneously, with long-standing ben-efits (8,9). Comprehensive implementa-tion of evidence-based interventions haslikely contributed to the significant re-ductions in ASCVD events and mortalityseen in people with diabetes in recentdecades (10). ASCVD risk managementin its many forms is an essential partof diabetes management that is beyondthe scope of this statement, but physi-cians should be aware of the impor-tance of multifactorial treatment intype 2 diabetes (7).
Glucose Management: MonitoringGlycemic management is primarily as-sessedwith the HbA1c test, whichwas themeasure studied in trials demonstratingthe benefits of glucose lowering (2). Theperformance of the test is generallyexcellent for NGSP-certified assays and
laboratories (www.ngsp.org) (11). Aswith any laboratory test, HbA1c has lim-itations (2). Because there is variabilityin the measurement of HbA1c, cliniciansshould exercise judgment, particularlywhen the result is close to the thresholdthat might prompt a change in therapy.HbA1c results may be discrepant from thepatient’s true mean glycemia in certainracial and ethnic groups, and in condi-tions that alter red blood cell turnover,such as anemia, end-stage renal disease(ESRD) (especially with erythropoietintherapy), and pregnancy, or if an HbA1cassay sensitive to hemoglobin variantsis used in someone with sickle cell traitor other hemoglobinopathy. Discrep-ancies between measured HbA1c andmeasured or reported glucose levelsshould prompt consideration that oneof these may not be reliable (12).
Regular self-monitoringofbloodglucose(SMBG) may help with self-managementand medication adjustment, particularlyin individuals taking insulin. SMBG plansshould be individualized. People withdiabetes and thehealth care teamshoulduse the data in an effective and timelymanner. In people with type 2 diabetesnot using insulin, routine glucose mon-itoring is of limited additional clinicalbenefit while adding burden and cost(13,14). However, for some individuals,glucose monitoring can provide insightinto the impact of lifestyle and medica-tion management on blood glucose andsymptoms, particularly when combinedwith education and support. Novel tech-nologies, such as continuous or flashglucose monitoring, provide more infor-mation. However, in type 2 diabetes,they have been associated with onlymodest benefits (15).
Principles of Care
Consensus recommendation
c Providers and health care systemsshould prioritize the delivery ofpatient-centered care.
Providing patient-centered care thatacknowledges multimorbidity, and isrespectful of and responsive to individ-ual patient preferences and barriers,including the differential costs of thera-pies, is essential to effective diabetesmanagement (16). Shared decision mak-ing, facilitated by decision aids thatshow the absolute benefit and risk ofalternative treatment options, is a useful
care.diabetesjournals.org Davies and Associates 3

strategy to arrive at the best treatmentcourse for an individual (17–20). Pro-viders should evaluate the impact ofany suggested intervention, includingself-care regimens, in the context ofcognitive impairment, limited literacy,distinct cultural beliefs, and individualfears or health concerns given theirimpact on treatment efficacy.
DSMES
Consensus recommendation
c All people with type 2 diabetesshould be offered access to ongo-ing DSMES programs.
DSMES is a key intervention to en-able people with diabetes to makeinformed decisions and to assume re-sponsibility for day-to-day diabetesmanagement. DSMES is central to es-tablishing and implementing the princi-ples of care (Fig. 1). DSMES programsusually involve face-to-face contact ingroup or individual sessions with trainededucators, and key components areshown in Table 1 (21–25). While DSMESshould be available on an ongoing basis,critical junctures when DSMES shouldoccur include at diagnosis, annually,when complications arise, and duringtransitions in life and care (22).DSMES programs delivered from
diagnosis can promote medicationadherence, healthy eating, and physi-cal activity, and increase self-efficacy.
In type 2 diabetes, high-quality evi-dence has consistently shown thatDSMES is a cost-effective interventionin the health care systems studied.DSMES significantly improves clinicaland psychological outcomes, improvesglycemic control, reduces hospital ad-missions, improves patient knowledge,and reduces the risk of all-cause mor-tality (22,26–31). The best outcomesare achieved in those programs with atheory-based and structured curricu-lum and with contact time of over10 h. While online programs may re-inforce learning, there is little evi-dence they are effective when usedalone (27).
Consensus recommendation
c Facilitating medication adherenceshould be specifically consideredwhen selecting glucose-loweringmedications.
Suboptimal adherence, including poorpersistence, to therapy affects almosthalf of people with diabetes, leadingto suboptimal glycemic and cardiovas-cular disease (CVD) risk factor control aswell as increased risk of diabetes com-plications, mortality, hospital admis-sions, and health care costs (32–36).Though this consensus recommenda-tion focuses on medication adherence(including persistence), the principlesare pertinent to all aspects of diabetes
care. Multiple factors contribute toinconsistent medication use and treat-ment discontinuation, including patient-perceived lack of medication efficacy,fear of hypoglycemia, lack of accessto medication, and adverse effects ofmedication (37). Medication adherence(including persistence) varies acrossmedication classes and careful consider-ation of these differences may help im-prove outcomes (38). Ultimately, patientpreference is a major factor driving thechoice of medication. Even in caseswhere clinical characteristics suggestthe use of a particular medication basedon the available evidence from clinicaltrials, patient preferences regardingroute of administration, injection de-vices, side effects, or cost may preventtheir use by some individuals (39).
Therapeutic inertia, sometimes re-ferred to as clinical inertia, refers tofailure to intensify therapy when treat-ment targets are not met. The causesof therapeutic inertia are multifacto-rial, occurring at the level of the prac-titioner, patient, and/or health caresystem (40). Interventions targetingtherapeutic inertia have facilitatedimproved glycemic control and timelyinsulin intensification (41,42). Forexample, multidisciplinary teams thatinclude nurse practitioners or pharma-cists may help reduce therapeutic iner-tia (43,44). A fragmented health caresystem may contribute to therapeuticinertia and impair delivery of patient-centered care. A coordinated chroniccare model, including self-managementsupport, decision support, delivery sys-tem design, clinical information sys-tems, and community resources andpolicies, promotes interaction betweenmore empowered patients and betterprepared and proactive health careteams (45).
RECOMMENDED PROCESS FORGLUCOSE-LOWERINGMEDICATION SELECTION: WHEREDOES NEW EVIDENCE FROMCARDIOVASCULAR OUTCOMESTRIALS FIT IN?
In prior consensus statements, efficacyin reducing hyperglycemia, along withtolerability and safety were primaryfactors in glucose-lowering medicationselection. Patient preferences, glycemictargets, comorbidities, polypharmacy,side effects, and cost were additional
Table 1—Key components of DSMES (21,23–25)c Evidence-based
c Individualized to the needs of the person, including language and culture
c Has a structured theory-driven written curriculum with supporting materials
c Delivered by trained and competent individuals (educators) who are quality assured
c Delivered in group or individual settings
c Aligns with the local population needs
c Supports the person and their family in developing attitudes, beliefs, knowledge, and skills toself-manage diabetes
c Includes core content; i.e., diabetes pathophysiology and treatment options; medicationusage; monitoring, preventing, detecting, and treating acute and chronic complications;healthy coping with psychological issues and concerns; problem solving and dealing withspecial situations (i.e., travel, fasting)
c Available to patients at critical times (i.e., at diagnosis, annually,when complications arise, andwhen transitions in care occur)
c Includes monitoring of patient progress, including health status, quality of life
c Quality audited regularly
DSMES is a critical element of care for all people with diabetes and is the ongoing processof facilitating the knowledge, skills, and ability necessary for diabetes self-care as well as activitiesthat assist a person implementing and sustaining behaviors needed to manage theirdiabetes on an ongoing basis. National organizations in the U.S. and Europe have publishedstandards to underpin DSMES. In the U.S., these are defined as DSMES “services,” whereas inEurope they are often referred to as “programs.”Nevertheless, the broad components are similar.
4 Consensus Report Diabetes Care

important considerations. For every in-dividual, the choice of glucose-loweringmedication should be underpinned bylifestyle management, DSMES, and thepatient-centered care principles outlinedin Fig. 1.Figure 2 describes our new consensus
approach to glucose lowering with med-ications in type 2 diabetes. Because of thenew evidence for the benefit of specificmedications to reduce mortality, heartfailure (HF), and progression of renaldisease in the setting of establishedCVD, their use was considered compel-ling in this patient group. Thus, we rec-ommend that providers consider ahistory of CVD very early in the processof treatment selection. Other factorsaffect the choice of glucose-loweringmedications, particularly in the settingof patient-centered care. In addition toCVD, we recommend early considerationof weight, hypoglycemic risk, treatmentcost, and other patient-related factorsthat may influence treatment selection(Figs. 2–6).
Implications of New Evidence FromCardiovascular Outcomes TrialsThe major change from prior consensusreports is based on new evidence thatspecific sodium–glucose cotransporter2 (SGLT2) inhibitors or glucagon-likepeptide 1 (GLP-1) receptor agonists im-prove cardiovascular outcomes, as wellas secondary outcomes such as HF andprogression of renal disease, in patientswith established CVD or CKD. Therefore,an important early step in this newapproach (Fig. 3) is to consider the pres-ence or absence of ASCVD, HF, and CKD,conditions inaggregate affecting15–25%of the population with type 2 diabetes.While the new evidence supporting theuse of particular medications in patientswho also have established CVD or are athigh risk of CVD is derived from largecardiovascular outcomes trials (CVOTs)demonstrating substantial benefits over2–5 years, it is important to rememberthat each trial constitutes a single ex-periment. Within each drug class, resultshave been heterogeneous. It is not clearwhether there are true drug-class ef-fects with different findings for individ-ual medications due to differences intrial design and conduct, or whetherthere are real differences betweenmedications within a drug class due toproperties of the individual compounds.
Where the current evidence is strongestfor a specific medication within a class, itis noted. The American Diabetes Asso-ciation’s (ADA) Standards of MedicalCare in Diabetes will align with thisdocument and will be updated to reflectnewevidenceas it emerges fromongoingclinical trials.
Consensus recommendation
c Among patients with type 2 diabe-tes who have established ASCVD,SGLT2 inhibitors or GLP-1 recep-tor agonists with proven cardiovas-cular benefit are recommendedas part of glycemic management(Figs. 2 and 3).
ASCVD is defined somewhat differ-ently across trials, but all trials enrolledindividuals with established CVD (e.g.,myocardial infarction [MI], stroke,any revascularization procedure) whilevariably including related conditionscompatible with clinically significantatherosclerosis (e.g., transient ischemicattack, hospitalized unstable angina,amputation, congestive heart failureNew York Heart Association [NYHA] classII–III,.50% stenosis of any artery, symp-tomatic or asymptomatic coronary arterydisease documented by imaging, CKDwith estimated glomerular filtration rate[eGFR],60mL min21[1.73]22).Most trialsalso included a “risk factor only” groupwith entry criteria basedon age and usuallythe presence of two or more cardiac riskfactors (46). Trials were designed to eval-uate cardiovascular safety (i.e., statisticalnoninferiority comparedwith placebo), butseveral showed ASCVD outcome benefit(i.e., statistical superiority compared withplacebo), including, in somecases,mortality.
Among GLP-1 receptor agonists, lira-glutide, studied in the LiraglutideEffect and Action in Diabetes: Evalua-tion of Cardiovascular Outcome Results(LEADER) trial (n59,340), demonstratedan ARR of 1.9% with a hazard ratio (HR)of 0.87 (95% CI 0.78, 0.97; P 5 0.01 forsuperiority) for the primary compositeoutcome of cardiovascular death, non-fatal MI, and nonfatal stroke (major ad-verse cardiac events [MACE]) comparedwith placebo over 3.8 years. Each com-ponent of the composite contributed tothe benefit, and the HR for cardiovasculardeath was 0.78 (95% CI 0.66, 0.93; P 50.007; ARR 1.7%). The LEADER trial alsodemonstrated an HR of 0.85 (95% CI,
0.74, 0.97; P 5 0.02; ARR 1.4%) forall-cause mortality (47). In the Trial toEvaluate Cardiovascular and Other Long-term Outcomes with Semaglutide inSubjects with Type 2 Diabetes (SUSTAIN6) (n 5 3,297), semaglutide comparedwith placebo demonstrated an ARR of2.3% with HR 0.74 for MACE (95% CI 0.58,0.95; P 5 0.02 for superiority) over 2.1years, but the reduction in events ap-peared to be driven by the rate of strokerather than CVD death (48). The Exena-tide Study of Cardiovascular Event Low-ering (EXSCEL) compared exenatideextended-release with placebo over3.2 years in 14,752 participants withtype 2 diabetes. While the medicationwas safe (noninferior), the HR for MACEin the entire trial was 0.91 (95% CI 0.83,1.0; P5 0.06) not reaching the thresholdfor demonstrated superiority versus pla-cebo; ARRwas 0.8% (49). All-cause deathwas lower in the exenatide arm (ARR 1%,HR 0.86 [95% CI 0.77, 0.97]), but it wasnot considered to be statistically signif-icant in the hierarchical testing proce-dure applied. Lixisenatide, a short-actingGLP-1 receptor agonist, did not demon-strate CVD benefit or harm in a trial ofpatients recruited within 180 days of anacute coronary syndrome admission (50).Taken together, it appears that amongpatientswith established CVD, some GLP-1 receptor agonists may provide cardio-vascular benefit, with the evidence ofbenefit strongest for liraglutide, favorablefor semaglutide, and less certain for ex-enatide. There is no evidence of cardio-vascular benefitwith lixisenatide. Adverseeffects for the class are discussed in thesection “The Full Range of TherapeuticOptions: Lifestyle Management, Medica-tion, and Obesity Management.”
Among the SGLT2 inhibitors, em-pagliflozin compared with placebo wasstudied in the Empagliflozin, Cardiovas-cular Outcome Event Trial in Type 2Diabetes Mellitus Patients (EMPA-REGOUTCOME) in 7,020 participants withtype 2 diabetes and CVD. With a medianfollow-up of 3.1 years, the ARR was 1.6%and the HR was 0.86 (95% CI 0.74, 0.99;P5 0.04 for superiority) for the primarycomposite end point of nonfatal MI,nonfatal stroke, and cardiovasculardeath. The ARR was 2.2% and the HRwas 0.62 (95% CI 0.49, 0.77; P , 0.001)for cardiovascular death (51). The ARRwas 2.6% and the HR was 0.68 (95% CI0.57, 0.82; P , 0.001) for death from
care.diabetesjournals.org Davies and Associates 5

Figure
2—Glucose-loweringmed
icationintype
2diabetes:overallapproach.CV,cardiovascular;DPP
-4i,dipep
tidylpep
tidase4inhibitor;GLP-1RA,glucagon-likepep
tide1receptoragonist;SG
LT2i,SGLT2inhibitor;
SU,sulfonylurea.
6 Consensus Report Diabetes Care

Figure 3—Choosing glucose-lowering medication in those with established ASCVD, HF, and CKD. CV, cardiovascular; DPP-4i, dipeptidyl peptidase4 inhibitor; GLP-1 RA, glucagon-like peptide 1 receptor agonist; SGLT2i, SGLT2 inhibitor; SU, sulfonylurea.
care.diabetesjournals.org Davies and Associates 7

Figure 4—Choosing glucose-lowering medication if compelling need to minimize weight gain or promote weight loss. GLP-1 RA, glucagon-like peptide1 receptor agonist; T2DM, type 2 diabetes; SGLT2i, SGLT2 inhibitor; SU, sulfonylurea.
8 Consensus Report Diabetes Care

Figure 5—Choosing glucose-lowering medication if compelling need to minimize hypoglycemia. DPP-4i, dipeptidyl peptidase 4 inhibitor; GLP-1 RA,glucagon-like peptide 1 receptor agonist; SGLT2i, SGLT2 inhibitor.
care.diabetesjournals.org Davies and Associates 9
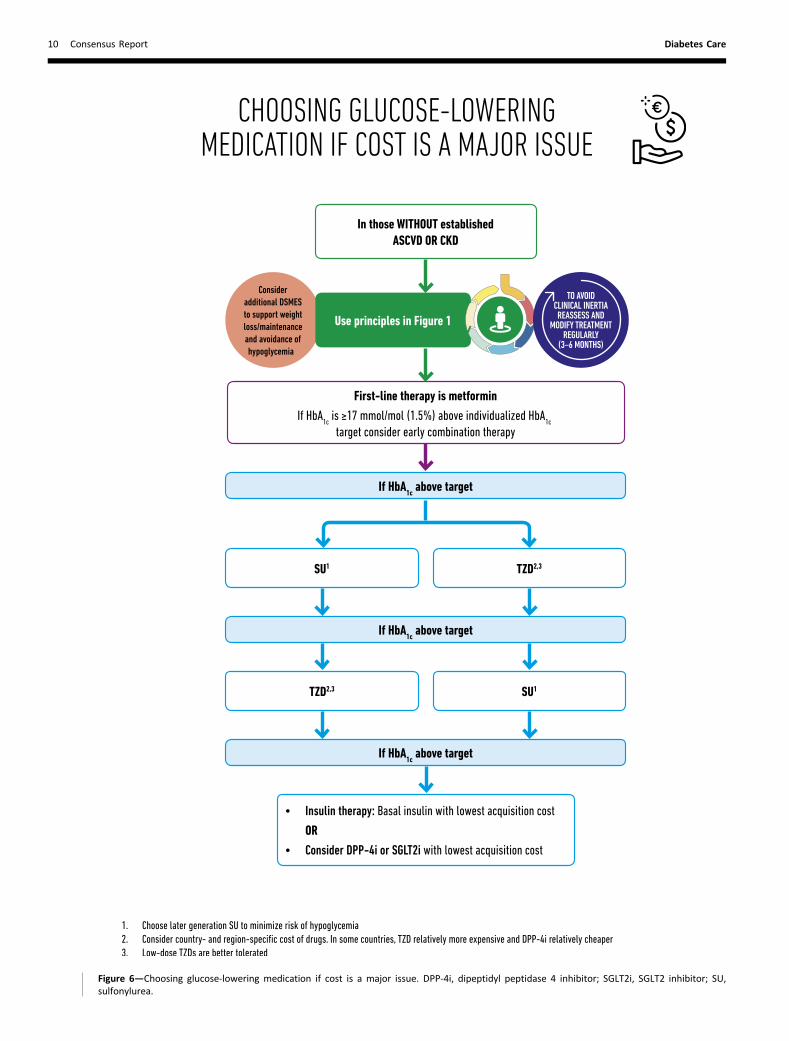
Figure 6—Choosing glucose-lowering medication if cost is a major issue. DPP-4i, dipeptidyl peptidase 4 inhibitor; SGLT2i, SGLT2 inhibitor; SU,sulfonylurea.
10 Consensus Report Diabetes Care

any cause. Canagliflozin compared withplacebo was studied in the CanagliflozinCardiovascular Assessment Study(CANVAS) Program (comprised of twosimilar trials, CANVAS and CANVAS-Renal; n 5 10,142) in participants withtype 2 diabetes, 66% of whom hada history of CVD. Participants werefollowed for a median of 3.6 years. Inthe combined analysis of the two trials,the primary composite end point ofMI, stroke, or cardiovascular death wasreduced with canagliflozin (26.9 vs.31.5 participants per patient-year withplacebo; HR 0.86 [95% CI 0.75, 0.97];P 5 0.02) for superiority in the pooledanalysis, with consistent findings inthe component studies. Though therewas a trend toward benefit for cardio-vascular death, the difference fromplacebo was not statistically significantin the CANVAS Program (52). For theSGLT2 inhibitors studied to date, it ap-pears that among patientswith establishedCVD, there is likely cardiovascular benefit,with the evidence of benefit modestlystronger for empagliflozin than canagli-flozin. Adverse effects for the classare discussed in the section “The FullRange of Therapeutic Options: LifestyleManagement, Medication, and ObesityManagement.”While the evidence of an ASCVD out-
comes benefit for GLP-1 receptor ago-nists and SGLT2 inhibitors has beendemonstrated for people with estab-lished ASCVD, the evidence of benefitbeyond glucose lowering has not beendemonstrated in those without ASCVD.Indeed, in subgroup analyses of thesetrials, lower-risk individuals have notbeenobserved tohave anASCVDbenefit.While this may be due to the short timeframe of the studies and the low eventrate in those without ASCVD, the findingis consistent across the reported trials.Overall, CVOTs of dipeptidyl peptidase4 (DPP-4) inhibitors have demonstratedsafety, i.e., noninferiority relative to pla-cebo, for the primary MACE end point,but not cardiovascular benefit.The available evidence for cardiovas-
cular event reduction in patients withtype 2 diabetes and clinical CVD is derivedfrom trials in which the participants werenot meeting glycemic targets (HbA1c$53 mmol/mol [$7%] at baseline). Fur-thermore, most (;70% across trials)participants were treated with metfor-min at baseline. Thus, we recommend
that patients with clinical CVD not meet-ing individualized glycemic targets whiletreated with metformin (or in whommetformin is contraindicated or not tol-erated) should have an SGLT2 inhibitoror GLP-1 receptor agonist with provenbenefit for cardiovascular risk reductionadded to their treatment program. Thereare no clinical trial data that supportprescribing an SGLT2 inhibitor or GLP-1 receptor agonist with the intent ofreducing cardiovascular risk in patientswith an HbA1c ,53 mmol/mol (,7%).Limited data suggest that there is noheterogeneity in the cardiovascular ben-efits of SGLT2 inhibitors or GLP-1 recep-tor agonists as a function of backgroundglucose-lowering therapy. Thus, back-ground glucose-lowering therapy in pa-tients with clinical CVD arguably is notpertinent in clinical decision making.However, dose adjustment or discontin-uation of background medications maybe required to avoid hypoglycemiawhen adding a new agent to a regi-men containing insulin, sulfonylurea, orglinide therapy, particularly in patients ator near glycemic goals. Full efforts toachieve glycemic and blood pressuretargets and to adhere to lipid, antiplate-let, antithrombotic, and tobacco ces-sation guidelines (7) should continueafter an SGLT2 inhibitor or GLP-1 re-ceptor agonist is added, as such effortswere integral to all studies that havedemonstrated cardiovascular benefitof these agents.
Consensus recommendation
c Among patients with ASCVD inwhom HF coexists or is of specialconcern, SGLT2 inhibitors are rec-ommended (Figs. 2 and 3).
Patients with type 2 diabetes are atincreased risk of HF (53). In the EMPA-REG OUTCOME and CANVAS CVOT stud-ies testing SGLT2 inhibitors, whichenrolled participants with ASCVD,.85%of participants did not have symptomaticHF at baseline. Yet, in both trials therewasa clinically and statistically significantreduction in hospitalization for HF forthe SGLT2 inhibitor as compared withplacebo. In the EMPA-REG OUTCOMEstudy with empagliflozin (54), the ARRwas 1.4%, and the HR 0.65 (95% CI0.50, 0.85), and in the CANVAS Pro-gram with canagliflozin, the HR was0.67 (95% CI 0.52, 0.87), with a rate of
hospitalized HF of 5.5 vs. 8.7 events per1,000 patient-years (55). Because HF wasneitherwell characterized at baselinenoras carefully adjudicated as it would havebeen in a trial specifically designed toevaluate HF outcomes, and because HFwas a secondary end point in the trials,further ongoing studies are required toconclusively address the issue. That said,the significant reduction in hospitaliza-tion for HF demonstrated in the twostudy populations and the consistencyacross two independent trial programssuggest to us that treatment with SGLT2inhibitors in the setting of clinical HF mayprovide substantial benefit and shouldbe specifically considered in people withtype 2 diabetes and ASCVD and HF.
In the GLP-1 receptor agonist studiesLEADER, SUSTAIN 6, and EXSCEL, therewas no significant effect on hospitaliza-tion for HF with HR 0.86 (95% CI 0.71,1.06), 1.11 (95% CI 0.77, 1.61), and 0.94(95% CI 0.78, 1.13), respectively (47–49).Two short-term studies of liraglutide inpatients with reduced ejection fractionsuggested a lack of benefit in this setting(56,57).
Among the recent cardiovascularsafety outcomes trials testing DPP-4 in-hibitors, the Saxagliptin Assessment ofVascular Outcomes Recorded in Patientswith Diabetes Mellitus–Thrombolysisin Myocardial Infarction 53 (SAVOR-TIMI 53) study evaluating saxagliptindemonstrated a significant increased riskof HF, with 3.5% risk of hospitalizationfor HF versus 2.8% for placebo (HR 1.27;95% CI 1.07, 1.51; P5 0.007) (58). In thesubsequent Examination of Cardiovascu-lar Outcomes with Alogliptin versus Stan-dard of Care (EXAMINE) study of alogliptinthere was no statistically significant dif-ference in HF hospitalization (3.9% vs. 3.3%with placebo) (59), and in the Trial Eval-uating Cardiovascular Outcomes withSitagliptin (TECOS), the rate of hospital-ization for HF was 3.1% in both sitagliptin-and placebo-treated patients (60).
Consensus recommendation
c For patients with type 2 diabetesand CKD, with or without CVD,consider the use of an SGLT2 in-hibitor shown to reduce CKD pro-gression or, if contraindicated ornot preferred, a GLP-1 receptoragonist shown to reduce CKD pro-gression (Figs. 2 and 3).
care.diabetesjournals.org Davies and Associates 11

Patients with type 2 diabetes and kidneydisease are at an increased risk for car-diovascular events. A substantial numberof participants with an eGFR of 30–60 mLmin–1 [1.73m]–2 were included in EMPA-REG OUTCOME, CANVAS, LEADER, andSUSTAIN 6. An important finding in thestudies was reduction of the primaryASCVDoutcomeevenamongparticipantswith stage 3 CKD (eGFR 30–60 mL min–1
[1.73m]–2). For SGLT2 inhibitors, this con-trasts with the glucose-lowering effect,which diminishes with declining eGFR.In addition to the primary cardiovas-
cular end points, most of the SGLT2inhibitor and GLP-1 receptor agonistCVOTs reported benefit in renal endpoints, albeit as secondary outcomes.The renal outcome benefit has beenmost pronounced and consistent forSGLT2 inhibitors. EMPA-REG OUTCOME(empagliflozin) demonstrated an ARR6.1%, HR of 0.61 (95% CI 0.53, 0.70)for the composite outcome of new orworsening nephropathy (progression tourine albumin/creatinine ratio .33.9mg/mmol [.300 mg/g], doubling of se-rum creatinine and ESRD, or death byESRD). The most prevalent outcome com-ponent was the development of sustainedalbuminuria, but the other componentswere each significantly reduced relativeto placebo (61). CANVAS (canagliflozin)reported an HR of 1.7 (95% CI 1.51, 1.91)for regression of albuminuria and a 40%reduction in risk in the composite out-come of eGFR, ESRD, or renal death (5.5vs. 9.0 participants per 1,000 patient-years; HR 0.60; 95% CI 0.47, 0.77) (52).Additional trials with primary renal endpoints are ongoing in high-risk renalpopulations. The Evaluation of the Ef-fects of Canagliflozin on Renal and Car-diovascular Outcomes in Participantswith Diabetic Nephropathy (CREDENCE)trial examining canagliflozin in CKD withproteinuria has been stopped at a plannedinterim analysis for achieving the primaryefficacy end point (62).In LEADER and SUSTAIN 6, the GLP-1
receptor agonist liraglutide was associ-ated with an ARR of 1.5% and an HR of0.78 (95% CI 0.67, 0.92) for new or wors-ening nephropathy (63), and semaglu-tide demonstrated an ARR of 2.3%and an HR of 0.64 (95% CI 0.46, 0.88)for new or worsening nephropathy (48).Progression of albuminuria was themost prevalent component of the com-posite renal end point, whereas the other
components (doubling of serum creati-nine, ESRD, or renal death) did not con-tribute substantially to the benefit. Inthe DPP-4 inhibitor CVOTs, the DPP-4 in-hibitors have been shown to be safefrom a renal perspective, with modestreduction in albuminuria (64).
THE FULL RANGEOFTHERAPEUTICOPTIONS: LIFESTYLEMANAGEMENT, MEDICATION,AND OBESITY MANAGEMENT
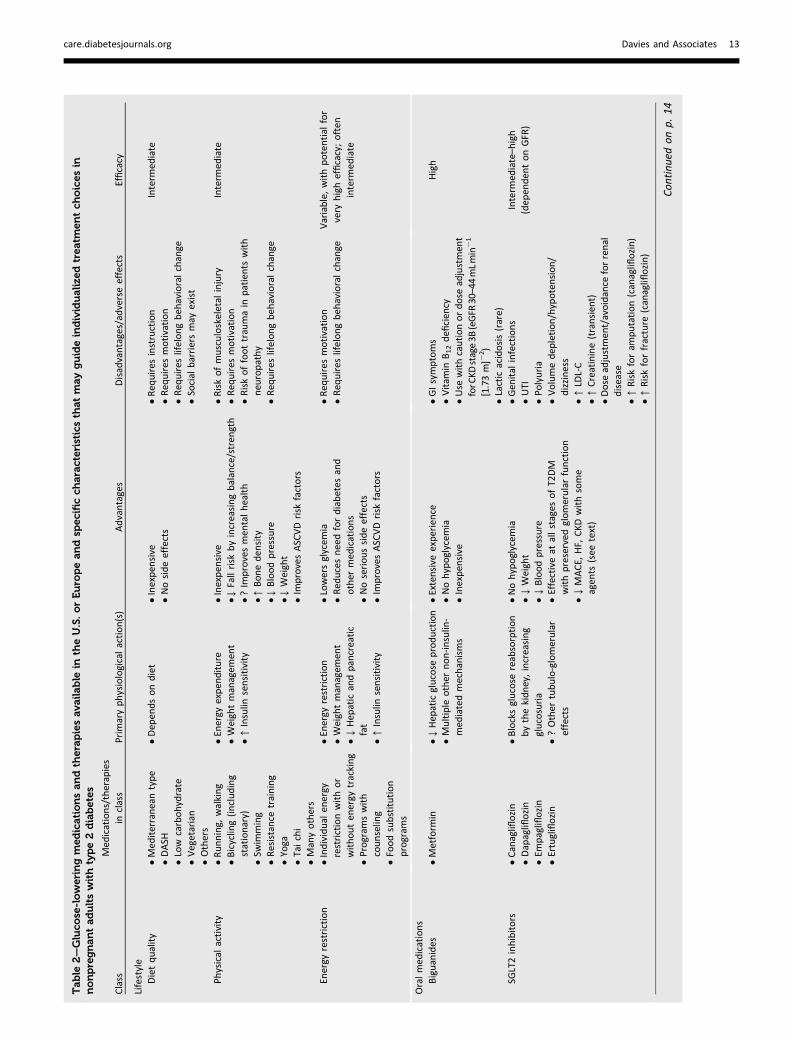
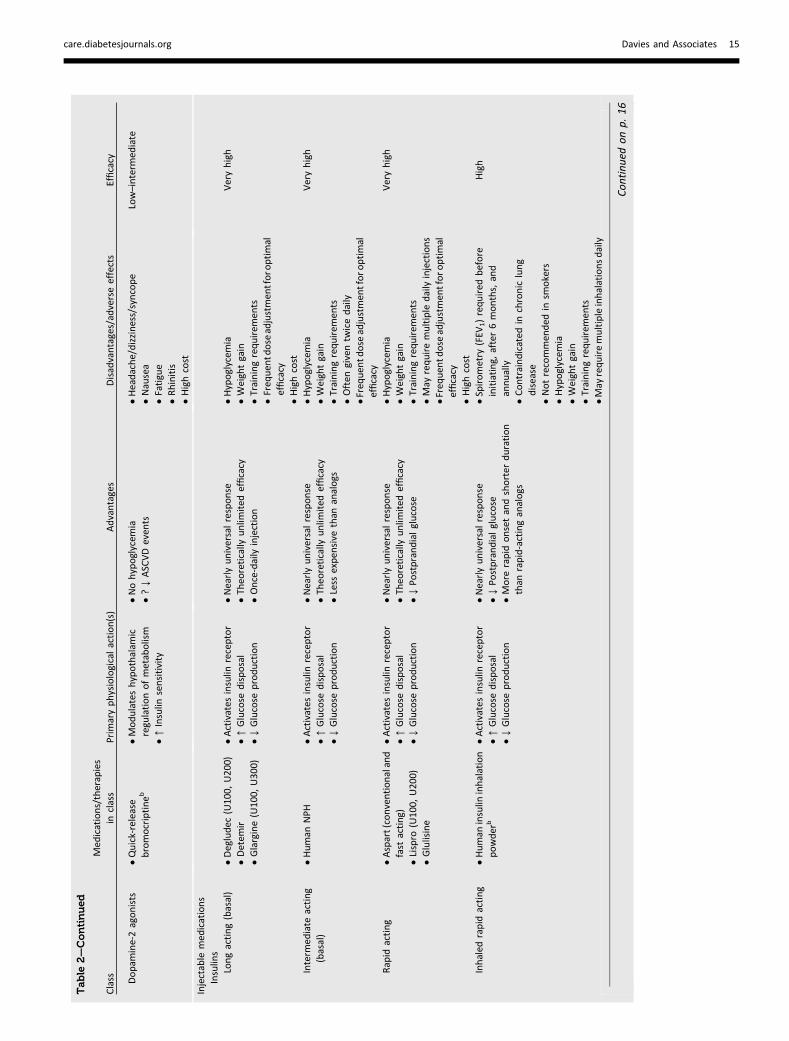
This section summarizes the lifestyle,medication, and obesity managementtherapies that lower glucose or improveother outcomes in patients with type 2diabetes. A more comprehensive discus-sion of these issues is available elsewhere(3,21,65). Formore details onweight lossmedications and metabolic surgery, seethe section “Obesity Management BeyondLifestyle Intervention.” Basic informationabout specific options in each category oftherapy is summarized in Table 2.
Lifestyle interventions, including MNTand physical activity, are effective andsafe for improving glucose control in type2 diabetes. For these reasons, they arerecommended as first-line therapies fromthe time of diagnosis and as cotherapyfor patients who also require glucose-lowering medications or metabolic sur-gery. Lifestyle management should be partof the ongoing discussion with individ-uals with type 2 diabetes at each visit.
Lifestyle Management
Consensus recommendation
c An individualized program of MNTshould be offered to all patients.
Medical Nutrition Therapy
MNTcompriseseducationandsupport tohelp patients adopt healthy eating pat-terns. The goal of MNT is to manageblood glucose and cardiovascular riskfactors to reduce risk fordiabetes-relatedcomplications while preserving the plea-sure of eating (21). Two basic dimensionsofMNT includedietary quality and energyrestriction. Strategies directed at eachdimension can improve glycemic control.
DietaryQuality andEatingPatterns.There isno single ratio of carbohydrate, proteins,and fat intake that is optimal for everyperson with type 2 diabetes. Instead,there are many good options and pro-fessional guidelines usually recommendindividually selected eating patterns that
emphasize foods of demonstrated healthbenefit, that minimize foods of demon-strated harm, and that accommodatepatient preference andmetabolic needs,with the goal of identifying healthy di-etary habits that are feasible and sustain-able. Three trials of a Mediterraneaneating pattern reported modest weightloss and improved glycemic control(66–68). In one of these, people withnew-onset diabetes assigned to a low-carbohydrate Mediterranean eating pat-tern were 37% less likely to requireglucose-lowering medications over 4years compared with patients assignedto a low-fat diet (HR 0.63 [95% CI 0.51,0.86]). A meta-analysis of RCTs in pa-tients with type 2 diabetes showed thatthe Mediterranean eating pattern re-duced HbA1c more than control diets(mean difference 23.3 mmol/mol, 95%CI25.1,21.5mmol/mol [20.30%, 95% CI20.46%,20.14%]) (69). Low-carbohydrate,low glycemic index, and high-protein diets,and the Dietary Approaches to Stop Hyper-tension (DASH) diet all improve glycemiccontrol, but the effect of the Mediterra-nean eating pattern appears to be thegreatest (70–72). Low-carbohydrate diets(,26%of total energy) produce substan-tial reductions in HbA1c at 3months (25.2mmol/mol, 95% CI 27.8, 22.5 mmol/mol[20.47%, 95% CI 20.71%, 20.23%]) and6months (4.0 mmol/mol, 95% CI 26.8,21.0 mmol/mol [20.36%, 95% CI 20.62%,20.09%]), with diminishing effects at 12and 24 months; no benefit of moderatecarbohydrate restriction (26–45%) wasobserved (73). Vegetarian eating pat-terns have been shown to lower HbA1c,but not fasting glucose, compared withnonvegetarian ones (74). Very recent tri-als of different eating patterns in type 2diabetes have typically also includedweight reduction, hindering firm con-clusions regarding the distinct contribu-tion of dietary quality.
Consensus recommendation
c All overweight and obese patientswith diabetes should be advised ofthe health benefits of weight lossand encouraged to engage in aprogram of intensive lifestyle man-agement, which may include foodsubstitution.
Nonsurgical Energy Restriction for Weight
Loss. If a patient wishes to aim for re-mission of type 2 diabetes, particularly
12 Consensus Report Diabetes Care
Table
2—Gluco
se-loweringmed
icationsandtherapiesava
ilable
intheU.S.orEuro
peandsp
ecificch
aracteristicsthat
mayguideindividualize
dtreatm
entch
oicesin
nonpregnantadultswithtype2diabetes
Class
Med
ications/therapies
inclass
Prim
aryphysiologicalaction(s)
Advantages
Disadvantages/adverseeffects
Efficacy
Lifestyle
Dietquality
cMed
iterraneantype
cDASH
cLow
carbohydrate
cVegetarian
cOthers
cDep
endsondiet
cInexpen
sive
cNosideeffects
cReq
uires
instruction
cReq
uires
motivation
cReq
uires
lifelongbeh
avioralchange
cSocial
barriersmay
exist
Interm
ediate
Physical
activity
cRunning,
walking
cBicycling(including
stationary)
cSw
imming
cResistance
training
cYoga
cTaichi
cManyothers
cEnergy
expen
diture
cWeightmanagem
ent
c↑Insulin
sensitivity
cInexpen
sive
c↓Fallrisk
byincreasingbalance/stren
gth
c?Im
provesmen
talhealth
c↑Boneden
sity
c↓Bloodpressure
c↓Weight
cIm
provesASCVDrisk
factors
cRiskofmusculoskeletal
injury
cReq
uires
motivation
cRiskoffoottraumain
patients
with
neu
ropathy
cReq
uires
lifelongbeh
avioralchange
Interm
ediate
Energy
restriction
cIndividual
energy
restrictionwithor
withou
ten
ergy
tracking
cProgram
swith
counseling
cFoodsubstitution
program
s
cEnergy
restriction
cWeightmanagem
ent
c↓Hep
aticandpancreatic
fat
c↑Insulin
sensitivity
cLowersglycem
iacRed
ucesneedfordiabetes
and
other
med
ications
cNoserioussideeffects
cIm
provesASCVDrisk
factors
cReq
uires
motivation
cReq
uires
lifelongbeh
avioralchange
Variable,withpotential
for
very
highefficacy;often
interm
ediate
Oralmed
ications
Biguanides
cMetform
inc↓Hep
aticglucose
production
cMultiple
other
non-insulin-
med
iatedmechanisms
cExtensive
expe
rien
cecNohypoglycem
iacInexpen
sive
cGIsymptoms
cVitam
inB12defi
cien
cycUse
withcautionordose
adjustmen
tforCKD
stage3B
(eGFR
30–44mLmin21
[1.73m]2
2)
cLacticacidosis(rare)
High
SGLT2inhibitors
cCanagliflozin
cDapagliflozin
cEm
pagliflozin
cErtugliflozin
cBlocksglucose
reabsorption
bythekidney,increasing
glucosuria
c?Other
tubulo-glomerular
effects
cNohypoglycem
iac↓Weight
c↓Bloodpressure
cEffectiveat
allstages
ofT2DM
withpreserved
glomerularfunction
c↓MACE,
HF,
CKD
withsome
agen
ts(see
text)
cGen
ital
infections
cUTI
cPo
lyuria
cVolumedep
letion/hypotension/
dizziness
c↑LD
L-C
c↑Creatinine(transien
t)cDose
adjustmen
t/avoidance
forrenal
disease
c↑Riskforam
putation(canagliflozin)
c↑Riskforfracture
(canagliflozin)
Interm
ediate–high
(dep
enden
tonGFR)
Con
tinu
edon
p.14
care.diabetesjournals.org Davies and Associates 13

Table
2—Continued
Class
Med
ications/therapies
inclass
Prim
aryphysiologicalaction(s)
Advantages
Disadvantages/adverseeffects
Efficacy
c↑RiskforDKA
(rare)
cFournier’sgangren
e(rare)
cExpen
sive
DPP
-4inhibitors
cSitagliptin
cVildagliptina
cSaxagliptin
cLinagliptin
cAlogliptin
cGlucose
dep
enden
t:↑Insulin
secretion
↓Glucagonsecretion
cNohypoglycem
iacWeightneu
tral
cWelltolerated
cRareurticaria/angioed
ema
c↑HFhospitalization(saxagliptin)
cDose
adjustmen
t/avoidance
forrenal
disease
dep
endingonagen
tc?Pancreatitis
c?Arthralgia
c?Bullouspem
phigoid
cExpen
sive
(U.S.);variable
inEurope
Interm
ediate
Sulfonylureas
cGliben
clam
ide/glyburide
cGlipizide
cGliclazidea
cGlim
epiride
c↑Insulin
secretion
cExtensive
expe
rien
cec↓Microvascularrisk
(UKP
DS)
cInexpen
sive
cHypoglycem
iac↑Weight
cUncertaincardiovascularsafety
cDose
adjustmen
t/avoidance
forrenal
disease
cHighrate
ofsecondaryfailure
High
TZDs
cPioglitazone
cRosiglitazoneb
c↑Insulin
sensitivity
cLow
risk
forhypoglycem
iacDurability
c↑HDL-C
c↓Triacylglycerols(pioglitazone)
c↓ASCVDeven
ts(pioglitazone:
ina
poststroke
insulin-resistantpopulationand
assecondaryen
dpointin
ahigh-risk-of-
CVDdiabetes
population
)cLower
cost
c↑Weight
cEdem
a/heart
failure
cBoneloss
c↑Bonefractures
c↑LD
L-C(rosiglitazone)
c?Bladder
cancer
c?Maculared
ema
High
Meglitinides
(Glinides)
cRep
aglinide
cNateglinide
c↑Insulin
secretion
c↓Po
stprandialglucose
excursions
cDosingflexibility
cSafe
inadvancedrenal
disease
with
cautiousdosing(especially
repaglinide)
cLower
cost
cHypoglycem
iac↑Weight
cUncertaincardiovascularsafety
cFreq
uen
tdosingsched
ule
Interm
ediate–high
a-Glucosidaseinhibitors
cAcarbose
cMiglitol
cSlowscarbohydrate
digestion/absorption
cLow
risk
forhypoglycem
iac↓Po
stprandialglucose
excursions
cNonsystem
icmechanism
ofaction
cCardiovascularsafety
cLower
cost
cFreq
uen
tGIsideeffects
cFreq
uen
tdosingsched
ule
cDose
adjustmen
t/avoidance
forrenal
disease
Low–interm
ediate
Bile
acid
sequestrants
cColesevelam
bc?↓Hep
aticglucose
production
c?↑Incretin
levels
cNohypoglycem
iac↓LD
L-C
cConstipation
c↑Triacylglycerols
cMay
↓absorptionofother
med
ications
cInterm
ediate
expen
se
Low–interm
ediate
Con
tinu
edon
p.15
14 Consensus Report Diabetes Care
Table
2—Continued
Class
Med
ications/therapies
inclass
Prim
aryphysiologicalaction(s)
Advantages
Disadvantages/adverseeffects
Efficacy
Dopam
ine-2agonists
cQuick-release
bromocriptineb
cModulateshypothalam
icregulationofmetabolism
c↑Insulin
sensitivity
cNohypoglycem
iac?↓ASCVDeven
tscHeadache/dizzine
ss/syncope
cNausea
cFatigue
cRhinitis
cHighcost
Low–interm
ediate
Injectable
med
ications
Insulins
Longacting(basal)
cDegludec
(U100,
U20
0)cDetem
ircGlargine(U10
0,U30
0)
cActivates
insulin
receptor
c↑Glucose
disposal
c↓Glucose
production
cNearlyuniversalresponse
cTheo
retically
unlim
ited
efficacy
cOnce-daily
injection
cHypoglycem
iacWeightgain
cTrainingrequirem
ents
cFreq
uen
tdoseadjustmen
tforoptimal
efficacy
cHighcost
Veryhigh
Interm
ediate
acting
(basal)
cHuman
NPH
cActivates
insulin
receptor
c↑Glucose
disposal
c↓Glucose
production
cNearlyuniversalresponse
cTheo
retically
unlim
ited
efficacy
cLess
expe
nsive
than
analogs
cHypoglycem
iacWeightgain
cTrainingrequirem
ents
cOften
giventw
icedaily
cFreq
uen
tdose
adjustmen
tforoptimal
efficacy
Veryhigh
Rapid
acting
cAspart(conventionaland
fast
acting)
cLispro
(U100,
U20
0)cGlulisine
cActivates
insulin
receptor
c↑Glucose
disposal
c↓Glucose
production
cNearlyuniversalresponse
cTheo
retically
unlim
ited
efficacy
c↓Po
stprandialglucose
cHypoglycem
iacWeightgain
cTrainingrequirem
ents
cMay
requiremultiple
dailyinjections
cFreq
uen
tdose
adjustmen
tforoptimal
efficacy
cHighcost
Veryhigh
Inhaled
rapid
acting
cHuman
insulin
inhalation
powder
bcActivates
insulin
receptor
c↑Glucose
disposal
c↓Glucose
production
cNearlyuniversalresponse
c↓Po
stprandialglucose
cMore
rapid
onsetandshorter
duration
than
rapid-actinganalogs
cSpirometry
(FEV
1)required
before
initiating,
after6months,and
annually
cContraindicated
inchroniclung
disease
cNotrecommen
ded
insm
okers
cHypoglycem
iacWeightgain
cTrainingrequirem
ents
cMay
requiremultipleinhalationsdaily
High
Con
tinu
edon
p.16
care.diabetesjournals.org Davies and Associates 15

Table
2—Continued
Class
Med
ications/therapies
inclass
Prim
aryphysiologicalaction(s)
Advantages
Disadvantages/adverseeffects
Efficacy
cFreq
uen
tdose
adjustmen
tforoptimal
efficacy;lim
ited
optionsin
dosing
interval
cHighcost
cRespiratory
sideeffects(e.g.,
bronchospasm,cough,declinein
FEV1)
Short
acting
cHuman
regular(U10
0,U50
0)cActivates
insulin
receptor
c↑Glucose
disposal
c↓Glucose
production
cNearlyuniversalresponse
cTheo
retically
unlim
ited
efficacy
c↓Po
stprandialglucose
cLess
expe
nsive
than
analogs
cHypoglycem
iacWeightgain
cTrainingrequirem
ents
cFreq
uen
tdose
adjustmen
tforoptimal
efficacy
cMay
requiremultiple
dailyinjections
Veryhigh
Prem
ixed
cMany
cActivates
insulin
receptor
c↑Glucose
disposal
c↓Glucose
production
cNearlyuniversalresponse
cTheo
retically
unlim
ited
efficacy
cFewer
injectionsthan
basal/bolus
before
everymeal
cRecombinanthuman
analogs
areless
expe
nsive
cHypoglycem
iacWeightgain
cTrainingrequirem
ents
cFreq
uen
tdose
adjustmen
tforoptimal
efficacy
cHighcost
(excep
thuman
insulin
premix)
cCan
lead
toobligateeating
Veryhigh
GLP-1
RA
Shorter
acting
cExen
atide
cLixisenatide
cGlucose
dep
enden
t:↑Insulin
secretion
↓Glucagonsecretion
cSlowsgastricem
ptying
c↑Satiety
cNohypoglycem
iaas
monotherapy
c↓Weight
cExcellentpostprandialglucose
efficacy
formealsafterinjections
cIm
provescardiovascularrisk
factors
cFreq
uen
tGIsideeffectsthat
may
be
transien
tcModestly↑heart
rate
cTrainingrequirem
ents
cDose
adjustmen
t/avoidance
inrenal
disease
cAcute
pancreatitis(rare/uncertain)
cVeryhighcost
Interm
ediate–high
Longeracting
cDulaglutide
cExen
atideextended
-release
cLiraglutide
cSemaglutide
cGlucose
dep
enden
t:↑Insulin
secretion
↓Glucagonsecretion
c↑Satiety
cNohypoglycem
iaas
monotherapy
c↓Weight
c↓Po
stprandialglucose
excursions
cIm
provescardiovascularrisk
factors
c↓MACEwithsomeagen
ts(see
text)
c↓Albuminuriawithsomeagen
ts(see
text)
cGIsideeffects,includinggallbladder
disease
cGreater
↑heart
rate
cTrainingrequirem
ents
cDose
adjustmen
t/avoidance
forsome
agen
tsin
renal
disease
cAcute
pancreatitis(rare/uncertain)
High–very
high
Con
tinu
edon
p.17
16 Consensus Report Diabetes Care

Table
2—Continued
Class
Med
ications/therapies
inclass
Prim
aryphysiologicalaction(s)
Advantages
Disadvantages/adverseeffects
Efficacy
cGreater
loweringoffasting
glucose
vs.short-actingpreparations
cOnce-w
eeklydosing(excep
tliraglutide,
whichisdaily)
cC-cellhyperplasia/med
ullary
thyroid
tumors
(rare/uncertain;observed
inanim
alsonly)
cVeryhighcost
Other
injectables
Amylin
mim
etics
cPram
lintideb
c↓Glucagonsecretion
cSlowsgastricem
ptying
c↑Satiety
c↓Po
stprandialglucose
excursions
c↓Weight
cHypoglycem
iacFreq
uen
tdosingsched
ule
cTrainingrequirem
ents
cFreq
uen
tGIsideeffects
cVeryhighcost
Interm
ediate
Fixed-dose
combinationofG
LP-1
RAandbasal
insulin
analogs
cLiraglutide/degludec
cLixisenatide/glargine
cCombined
activities
of
componen
tscEnhancedglycem
icefficacy
vs.componen
tscRed
ucedadverseeffects(e.g.,GI,
hypoglycem
ia)
vs.componen
ts
cLess
weightloss
than
GLP-1
receptor
agonistalone
cVeryhighcost
Veryhigh
Weightloss
med
ications
cLorcaserinb
cNaltrexone/bupropion
cOrlistat
cPh
enterm
ine/
topiram
ateb
cLiraglutide3mg
cRed
ucedappetite
cFatmalabsorption(orlistat)
cMean3–9kg
weightloss
vs.placebo
cHighdiscontinuationratesfrom
side
effects
c,50
%achieve
$5%
weightloss
cDrug-specificsideeffects
cLimited
durability
cHighcost
Interm
ediate
Metabolic
surgery
cVSG
cRYG
BcAdjustable
gastricband
cBPD
cRestrictionoffoodintake
(all)
cMalabsorption(RYG
B,BPD
)cChangesin
horm
onal
and
possibly
neu
ronal
signaling
(VSG
,RYG
B,BPD
)
cSustained
weightreduction
c↑Rateofremissionofdiabetes
c↓Number
ofdiabetes
drugs
c↓Bloodpressure
cIm
provedlipid
metabolism
cHighinitialcost
c↑Riskforearlyandlate
surgical
complications
c↑Riskforreoperation
c↑Riskfordumpingsyndrome
c↑Nutrientandvitaminmalabsorption
c↑Riskfornew
-onsetdep
ression
c↑Riskfornew
-onsetopioid
use
c↑Riskforgastroduoden
alulcer
c↑Riskforhypoglycem
iac↑Riskforalcoholuse
disorder
Veryhigh
More
detailsavailable
inADA’sStan
dardsof
Medical
Carein
Diabetesd
2018
(3).Glucose-loweringefficacy
ofdrugs
bychange
inHbA1c:.22
mmol/mol(2%)very
high,11–22
mmol/mol(1–2%
)high,6–11
mmol/mol(0.5–1.5%
)interm
ediate,,6mmol/mol(0.5%)low.aNotlicen
sedin
theU.S.fortype
2diabetes.bNotlicen
sedin
Europefortype
2diabetes.BPD
,biliop
ancreaticdiversion;
DKA
,diabeticketoacidosis;FEV1,forced
expiratory
volumein
1sonpulm
onaryfunctiontesting;
GI,gastrointestinal;GLP-1
RA,glucagon-likepep
tide1receptoragonist;HDL-C,HDL-cholesterol;LD
L-C,
LDL-cholesterol;RYG
B,Roux-en
-Ygastricbypass;VSG
,vertical
sleeve
gastroplasty;
T2DM,type2diabetes
mellitus;UTI,urinarytractinfection.
care.diabetesjournals.org Davies and Associates 17

within 6 years of diagnosis, evidence-basedweightmanagement programs areoften successful.The most effective nonsurgical strat-
egies for weight reduction involve foodsubstitution and intensive, sustainedcounseling (e.g., 12–26 individual coun-seling sessions over 6–12 months).Among adults with type 2 diabetes,meal replacement (825–853 kcal/day[3,450–3,570 kJ/day] formula diet for3–5 months) followed by gradual rein-troduction of food and intensive coun-seling resulted in 9-kg placebo-adjustedweight loss at 1 year and high rates ofdiabetes remission (46% vs. 4%; oddsratio [OR] 19.7 [95% CI 7.8, 49.8]) com-pared with best usual practice (75). Interms of intensive behavioral interven-tions, the Action for Health in Diabetes(Look AHEAD) trial (76) randomized5,145 overweight or obese patientswith type 2 diabetes to an intensivelifestyle program that promoted energyrestriction, incorporating meal replace-ments to induce and sustain weight loss,along with increased physical activitycompared with standard diabetes edu-cation and support in the control group.After 9.6 years, weight loss was greaterin the intervention group (8.6% vs. 0.7%at 1 year; 6.0% vs. 3.5% at study end;both P , 0.05). HbA1c also fell in theintervention group despite less use ofglucose-lowering medications. Cardio-vascular event rates were not reduced,but there were numerous other bene-fits. In a 12-month trial, 563 adults withtype 2 diabetes who were randomizedto Weight Watchers compared with stan-dard care had a 2.1% net weight loss(24.0% vs. 21.9%; P , 0.001), a 5.3mmol/mol (23.5 vs. 11.8 mmol/mol;P5 0.020) net absolute improvement inHbA1c (0.48% [20.32%vs.10.16%]), anda greater reduction in use of glucose-lowering medications (226% vs. 112%;P , 0.001) (77). Similar programs haveresulted in a net 3-kg weight loss over12–18 months (78–80).
Physical Activity
Consensus recommendation
c Increasing physical activity improvesglycemic control and should be en-couraged in all people with type 2diabetes.
Aerobic exercise, resistance training, andthe combination of the two are effective
in reducing HbA1c by about 6.6 mmol/mol(0.6%) (81–84). Of these modalities, someevidence suggests that aerobic exer-cise and the combination of aerobic ex-ercise and resistance training may bemore effective than resistance trainingalone (85), but this remains controver-sial. When considering exercise interven-tions, special considerations are requiredfor individuals with CVD, uncontrolledretinopathy or nephropathy, and severeneuropathy. A wide range of physicalactivity, including leisure time activities(e.g., walking, swimming, gardening, jog-ging, tai chi, and yoga) can significantlyreduce HbA1c (86–90). In general, super-vision of exercise and motivational strat-egies, such as monitoring using a stepcounter, can improve the effect of exer-cise on HbA1c compared with advicealone (84,91). The combinationofdietarychange forweight reduction and physicalexercise improves hyperglycemia andreduces cardiovascular risk factors morethan dietary interventions or physicalactivity alone (92).
Medications for Lowering Glucose
Metformin
Metformin is an oral medication thatreduces plasma glucose via multiple mech-anisms. It is available as an immediate-release formulation that is typicallyadministered twice a day and as ex-tended-release formulations for once-daily or twice-daily administration. Theformulations are equally effective withno consistent differences in side effectprofile (93). Dosages of immediate-release metformin start at 500 mg onceor twice a day with meals and should beincreased as tolerated to a target dosageof 1,000 mg twice a day. The maximumdaily dose is 2,550 mg in the U.S. and3,000 mg in the European Union, thoughdoses above 2,000 mg are generallyassociated with little additional efficacyand poorer tolerability (94). Gastroin-testinal symptoms are common anddose dependent, and may improve overtime or with dose reduction. Metforminshould not be used in patients with aneGFR,30 mL min–1 [1.73 m]–2 and dosereduction should be considered whenthe eGFR is ,45 mL min–1 [1.73 m]–2
(95–97). Caution should be taken whenconditions are present that may re-duce eGFR. Advantages of metformininclude its high efficacy, low cost, min-imal hypoglycemia risk when used as
monotherapy, and the potential forsome weight loss. Some studies havesuggested a benefit for preventingCVD (98), but this has not been supportedby the results of a recent meta-analysis(99). However,metforminmay lower riskfor cardiovascular mortality comparedwith sulfonylurea therapy (100). Rarecases of lactic acidosis have been re-ported, usually in the setting of severeillness or acute kidney injury. Therefore,metformin should be omitted in the set-ting of severe illness, vomiting, or de-hydration. Metforminmay result in lowerserum vitamin B12 concentration; there-fore, periodic monitoring and supple-mentation is generally recommendedif levels are deficient, particularly inthose with anemia or neuropathy (101).Because of its high efficacy in loweringHbA1c, good safety profile, and low cost,metformin remains the first-line medica-tion for management of type 2 diabetes.
SGLT2 Inhibitors
SGLT2 inhibitors are oral medicationsthat reduce plasma glucose by enhancingurinary excretion of glucose (102). Theglucose-lowering efficacy of these med-ications is dependent on renal function.Initiation and continuation of SGLT2 in-hibitors are restricted by eGFR and re-quire intermittent monitoring of renalfunction (refer to European MedicinesAgency and U.S. Food and Drug Ad-ministration prescribing informationfor current recommendations). Thesemedications are of high efficacy in low-ering glucose in the setting of normalrenal function (51,52,103). All SGLT2 in-hibitors are associated with a reductionin weight and blood pressure. Alone orwithmetformin, they do not increase therisk for hypoglycemia. Empagliflozin andcanagliflozin have cardiac and renal ben-efits in patients with established or athigh risk of ASCVD. Cardiac and renalbenefits have been demonstrated downto an eGFR of 30 mL min–1 [1.73 m]–2,though currently none of the SGLT2inhibitors have been approved foruse by regulators at an eGFR below45 mL min–1 [1.73 m]–2 (see the section“Recommended Process for Glucose-Lowering Medication Selection: WhereDoes New Evidence From CardiovascularOutcomes Trials Fit In?”) (51,52,61). Theclass is associated with increased risk formycotic genital infections (mostly vagi-nitis in women, balanitis in men) (51,
18 Consensus Report Diabetes Care

52,104,105). Case reports of diabeticketoacidosis with SGLT2 inhibitors intype 2 diabetes continue to raise con-cern, though increased rates have notbeen confirmed in large trials (102,106).Therefore, the SGLT2 inhibitors shouldbe used with caution and appropriatepatient education should be provided forthose with insulin deficiency. SGLT2 in-hibitors have been associated with anincreased risk of acute kidney injury,dehydration, and orthostatic hypoten-sion; caution should be taken whenSGLT2 inhibitors are used in combina-tion with diuretics and/or ACE inhibi-tors and angiotensin receptor blockers.Canagliflozin has been associated withincreased risk for lower-limb amputa-tion (6.3 canagliflozin vs. 3.4 per 1,000patient-years with placebo after 3.1years; HR 1.97 [95% CI 1.41, 2.75]) (52).Similarly, fracture risk has been reportedwith canagliflozin (15.4 vs. 11.9 partici-pants with fracture per 1,000 patient-years; HR 1.26 [95% CI 1.04, 1.52]) (52). Itis uncertain whether amputation andfractures are class effects.
GLP-1 Receptor Agonists
GLP-1 receptor agonists are currentlydelivered by subcutaneous injection.These medications stimulate insulin se-cretion and reduce glucagon secretionin a glucose-dependent manner, im-prove satiety, and promote weight loss(107,108). Structural differences amongGLP-1 receptor agonists affect dura-tion of action, and their formulationand dosing may affect efficacy for glu-cose-lowering and weight reduction aswell as side effect profile and cardio-vascular effects (109). Dulaglutide,exenatide extended-release, and sema-glutide are administered once weekly(108,109). Liraglutide and lixisenatideare administered once daily, and exena-tide is available in a twice-daily formu-lation. GLP-1 receptor agonists have highglucose-lowering efficacy, but with var-iation within the drug class (110,111).Evidence suggests that the effect maybe greatest for semaglutide once weekly,followed by dulaglutide and liraglutide,closely followed by exenatide onceweekly, and then exenatide twice dailyand lixisenatide (110,112–116). The short-acting medications exenatide twice dailyand lixisenatide have greater postpran-dial effects, at least after the meals withwhich they are administered. All GLP-1
receptor agonists reduce weight (110);the reduction ranges from about 1.5 kgto 6.0 kg over about 30 weeks of ther-apy (110,117). Liraglutide and semaglutidehave been shown to improve cardiovas-cular outcomes (47,48) (see the section“Recommended Process for Glucose-Lowering Medication Selection: WhereDoes New Evidence From Cardiovascu-lar Outcomes Trials Fit In?”). The mostcommon side effects of GLP-1 receptoragonists are nausea, vomiting, and di-arrhea, though these tend to diminishover time. GLP-1 receptor agonists haveminimal risk for hypoglycemia, but mayincrease the hypoglycemic potentialof insulin and sulfonylureas when com-bined with those medications (118).Contrary to early signals, GLP-1 receptoragonists do not seem to substan-tially increase risk for pancreatitis, pan-creatic cancer, or bone disease (119).They are associated with increased riskof gallbladder events (120). Semaglu-tide was associated with increased ret-inopathy complications in the SUSTAIN6 trial (HR1.76, 95%CI 1.11, 2.78), largelyamong those with baseline retinopa-thy who had rapid improvement ofglycemic control (48). While this ob-servation remains unexplained, this isalso a recognized effect of intensifica-tion of glycemic control with insulin.
DPP-4 Inhibitors
DPP-4 inhibitors are oral medications thatincrease insulin secretion and reduce glu-cagon secretion in a glucose-dependentmanner. They have moderate glucose-lowering efficacy (121,122). DPP-4 inhib-itors are well tolerated, have a neutraleffect on weight, and have minimal risk ofhypoglycemiawhen usedasmonotherapy(123). When added to sulfonylurea ther-apy, however, the risk for hypoglycemia isincreased 50% compared with sulfonyl-urea therapy alone (124). The recom-mended dose for each DPP-4 inhibitoris determined and needs to be adjustedbased on renal function; linagliptin is theexception as it hasminimal renal excretion.Rare but increased rates of pancreatitis(125) and musculoskeletal side effectshave been reported (126). CVOTs dem-onstrated the cardiovascular safety butno cardiovascular benefit of three DPP-4inhibitors (saxagliptin, alogliptin, andsitagliptin) as well as imbalances regard-ing HF for saxagliptin and alogliptin(127,128) (see the section “Recommended
Process for Glucose-Lowering Medica-tion Selection: Where Does New Evi-dence From Cardiovascular OutcomesTrials Fit In?”).
Thiazolidinediones
Thiazolidinediones (TZDs) (pioglitazoneand rosiglitazone) are oral medicationsthat increase insulin sensitivity and areof high glucose-lowering efficacy (129–131). TZDs increase HDL-cholesterol(132,133), and pioglitazone has beenshown to reduce cardiovascular endpoints (132,134–138) and hepatic steato-hepatitis (139), but without conclusiveevidence for benefit. TZDs are associatedwith the best evidence among glucose-lowering medications for glycemic du-rability (140). However, these notablebenefits must be balanced with safetyconcerns regarding fluid retention andcongestive heart failure (136,140,141),weight gain (132,136,140–142), bonefracture (143,144), and, possibly, bladdercancer (145). Lower-dose therapy (e.g.,pioglitazone 15–30mg) mitigates weightgain and edema, but the broader ben-efits and harms of low-dose TZD therapyhave not been evaluated.
Sulfonylureas
Sulfonylureas are oral medications thatlower glucose by stimulating insulin se-cretion from pancreatic b-cells. They areinexpensive, widely available, and havehigh glucose-lowering efficacy (146).Sulfonylureas were used as part of theglucose-lowering regimen in the UK Pro-spective Diabetes Study (UKPDS) (147)and Action in Diabetes and VascularDisease: Preterax and Diamicron MRControlled Evaluation (ADVANCE) (148)trials, which both demonstrated reduc-tions in microvascular complications. Sul-fonylureas are associated with weightgain and risk for hypoglycemia and downtitration of dose to reduce the risk ofhypoglycemia results in higher HbA1c(146,149,150). Sulfonylureas are knownto be associated with a lack of durableeffect on glucose lowering (144,151). Theweight gain associated with sulfonyl-ureas is relatively modest in large cohortstudies and the incidence of severe hy-poglycemia is lower than with insulin(152). Important differences among sul-fonylureas affect both safety and effi-cacy. Glibenclamide (known as glyburidein the U.S. and Canada) has a higher risk
care.diabetesjournals.org Davies and Associates 19

of hypoglycemia compared with othersulfonylureas (153).Glipizide, glimepiride,and gliclazide may have a lower risk forhypoglycemia compared with other sul-fonylureas (152,154). Adverse cardio-vascular outcomes with sulfonylureas insome observational studies have raisedconcerns, although findings from recentsystematic reviews have found no in-crease in all-cause mortality comparedwith other active treatments (152). Asnewer-generation sulfonylureas appearto confer a lower risk of hypoglycemiaand have favorable cost, efficacy, andsafety profiles, sulfonylureas remain a rea-sonable choice among glucose-loweringmedications, particularly when cost is animportant consideration. Patient educa-tion anduse of lowor variable dosingwithlater generation sulfonylureas may beused to mitigate the risk of hypoglyce-mia. Greatest caution in this regard iswarranted for people at high risk ofhypoglycemia, such as older patientsand those with CKD.
Insulin
Numerous formulations of insulin areavailable with differing durations of ac-tion. Human insulins (NPH, regular [R],and premixed combinations of NPH andR) are recombinant DNA-derived humaninsulin, while insulin analogs have beendesigned to change the onset or durationof action. The main advantage of insulinover other glucose-loweringmedicationsis that insulin lowers glucose in a dose-dependent manner over a wide range, toalmost any glycemic target as limited byhypoglycemia. Older formulations of in-sulin have also demonstrated reductionin microvascular complications and withlong-term follow-up, all-cause mortality,and diabetes-related death (147,155).Beyond hypoglycemia, the disadvan-tages of insulin include weight gain andthe need for injection, frequent titrationfor optimal efficacy, and glucose moni-toring (156).The effectiveness of insulin is highly
dependent on its appropriate use; pa-tient selection and training; adjustmentof dose for changes in diet, activity, orweight; and titration to acceptable,safe glucose targets. Formulations ofintermediate- and long-acting insulinhave different timings of onset, durationsof action, and risks of hypoglycemia.However, the way in which insulin is ad-ministered, including the dose, timing
of injection, and glycemic targets, has agreater impact on the adverse effects ofinsulin than differences among insulinformulations.
Basal Insulin. Basal insulin refers tolonger-acting insulin that is meant tocover the body’s basal metabolic insulinrequirement (regulating hepatic glucoseproduction), in contrast to bolus or pran-dial insulin, which is meant to reduceglycemic excursions after meals. Basalinsulin is the preferred initial insulinformulation in patients with type 2diabetes. Options include once- or twice-daily administration of intermediate-acting NPH or detemir insulin and theonce-daily administration of glargine(U100 or U300) or degludec (U100 orU200). Long-acting insulin analogs (de-gludec [U100 or U200], glargine [U100and U300], detemir) have a modestlylower absolute risk for hypoglycemia com-pared with NPH insulin, but cost more(157–160). However, in real-world set-tings where patients are treated to con-ventional treatment targets, initiation ofNPH compared with determir or glargineU100 did not increase hypoglycemia-related emergency department visits orhospital admissions (161). When com-paring human and analog insulins, costdifferences can be large while differ-ences in hypoglycemia risk are mod-est and differences in glycemic efficacyminimal.
Degludec is associated with a lowerrisk of severe hypoglycemia comparedwith glargine U100 insulin when target-ing intensive glycemic control in patientswith long-standing type 2 diabetes athigh risk of CVD; absolute incidencedifference of 1.7% over 2 years (rateratio 0.60; P , 0.001 for superiority;OR 0.73; P , 0.001 for superiority)(162). Biosimilar formulations are nowavailable for glarginewith similar efficacyprofile and lower cost (163). No insulinhas been shown to reduce risk for CVD(156), but data suggest that glargineU100 and degludec do not increaserisk for MACE (162,164).
Concentrated formulations of de-gludec (U200) and glargine (U300) areavailable that allow injection of a re-duced volume, a convenience for patientson higher doses. Glargine U300 is asso-ciated with a lower risk of nocturnalhypoglycemia compared with glargineU100 but requires a 10–14% higher
dose of glargine for equivalent efficacy(165–167).
Not all patients have their blood glu-cose adequately controlled with basalinsulin. In particular, patientswith higherpretreatment HbA1c, higher BMI, longerduration of disease, and a greater num-ber of oral glucose-loweringmedicationsare more likely to require intensifiedtherapy (168).
Other Insulin Formulations. Short- andrapid-acting insulin formulations admin-istered at mealtime are generally usedto intensify basal insulin therapy inpatients not meeting glycemic targets.Options include human regular insulin,various analogs (aspart, glulisine, andlispro), formulations (faster insulin as-part, lispro U200), biosimilars (lispro),and insulins with different routes ofadministration (inhaled). Rapid-actinginsulin analogs have a modestly lowerrisk for hypoglycemia compared withhuman regular insulin but at a highercost. Various premixed formulations ofhuman and analog insulins are availableand continue to be widely used in someregions, though they tend to have anincreased risk of hypoglycemia as com-pared with basal insulin alone (Table 2and Fig. 7).
Other Glucose-Lowering Medications
Other oral glucose-lowering medications(i.e., meglitinides, a-glucosidase inhibitors,colesevelam, quick-release bromocriptine,pramlintide) are not used commonly intheU.S. and some are not licensed at all inEurope. No major new scientific informa-tion on these medications has emergedin recent years. Their basic characteristicsare listed in Table 2.
Obesity Management Beyond LifestyleIntervention
Medications for Weight Loss
Several clinical practice guidelines rec-ommend weight-loss medications asan optional adjunct to intensive lifestylemanagement for patients with obesity,particularly if they have diabetes(169–171). Others do not (172). Severalmedications and medication combina-tions approved in the U.S. or Europefor weight loss have been found toimprove glucose control in people withdiabetes (173,174). One glucose-loweringmedication, liraglutide, is also ap-proved for the treatment of obesity
20 Consensus Report Diabetes Care

Figure 7—Intensifying to injectable therapies. FRC, fixed-ratio combination; GLP-1 RA, glucagon-like peptide 1 receptor agonist; FBG, fasting bloodglucose; FPG, fasting plasma glucose; max, maximum; PPG, postprandial glucose.
care.diabetesjournals.org Davies and Associates 21

at a higher dose (175). Cost, side effects,and modest efficacy limit the role ofpharmacotherapy in long-term weightmanagement.
Metabolic Surgery
Consensus recommendation
c Metabolic surgery is a recommendedtreatment option for adults withtype 2 diabetes and 1) a BMI$40.0 kg/m2 (BMI $37.5 kg/m2
in people of Asian ancestry) or 2)a BMI of 35.0–39.9 kg/m2 (32.5–37.4 kg/m2 in people of Asian an-cestry) who do not achieve durableweight loss and improvement incomorbidities with reasonable non-surgical methods.
Metabolic surgery is highly effective inimproving glucose control (176–178)and often produces disease remission(179–182). The effects can be sustainedfor at least 5 years (177,182). Benefitsinclude a reduction in the number ofglucose-lowering medications needed toachieve glycemic targets (178,179).Several clinical practice guidelines
and position statements recommendconsideration of metabolic surgeryas a treatment option for adults withtype 2 diabetes and 1) a BMI $40.0kg/m2 (BMI $37.5 kg/m2 in people ofAsian ancestry) or 2) a BMI of 35.0–39.9 kg/m2 (32.5–37.4 kg/m2 in peopleof Asian ancestry) who do not achievedurable weight loss and improvement incomorbidities with reasonable nonsurgi-cal methods (65,183). Because baselineBMI does not predict surgical benefits onglycemia or hard outcomes and the im-provement inglycemic controloccursearlythrough weight-independent mechanisms(183), metabolic surgerymay be consideredfor those with a BMI of 30.0–34.9 kg/m2
(27.5–32.4 in people of Asian ancestry)who do not achieve durable weight lossand improvement in comorbidities withreasonable nonsurgical methods.Adverse effects of bariatric surgery,
which vary by procedure, include surgicalcomplications (e.g., anastomotic or sta-ple line leaks, gastrointestinal bleeding,intestinal obstruction, the need for re-operation), late metabolic complications(e.g., protein malnutrition, mineral defi-ciency, vitamin deficiency, anemia, hypo-glycemia), and gastroesophageal reflux(184,185). Patients who undergo meta-bolic surgerymay be at risk for substance
use, including drug and alcohol use andcigarette smoking (186). People withdiabetes presenting for metabolic sur-gery also have increased rates of depres-sion and other major psychiatric disorders(187). These factors should be assessedpreoperatively and during follow-up. Met-abolic surgery should be performed inhigh-volume centers with multidisciplin-ary teams that are experienced in themanagement of diabetes and gastrointes-tinal surgery. Long-term lifestyle supportand routine monitoring of micronutrientand nutritional status must be providedto patients after surgery (188,189).
PUTTING IT ALL TOGETHER:STRATEGIES FORIMPLEMENTATION
For an increasing number of patients,presence of specific comorbidities (e.g.,ASCVD, HF, CKD, obesity), safety con-cerns (e.g., risk of hypoglycemia), or healthcare environment (e.g., cost of medica-tions) mandate a specific approach tothe choice of glucose-lowering medica-tion. These are considered in Figs. 2–6.For patients not reaching their targetHbA1c, it is important to re-emphasizelifestyle measures, assess adherence, andarrange timely follow-up (e.g., within3–6 months) (Fig. 1).
Initial Monotherapy
Consensus recommendation
c Metformin is the preferred initialglucose-lowering medication formost people with type 2 diabetes.
Metformin remains the preferred optionfor initiating glucose-lowering medica-tion in type 2 diabetes and should beadded to lifestyle measures in newlydiagnosed patients. This recommenda-tion is based on the efficacy, safety,tolerability, low cost, and extensiveclinical experience with this medication.Results from a substudy of UKPDS (n 5342) showed benefits of initial treatmentwith metformin on clinical outcomesrelated to diabetes, with less hypoglyce-mia and weight gain than with insulin orsulfonylureas (98).
Initial Combination TherapyCompared With Stepwise Addition ofGlucose-Lowering Medication
Consensus recommendation
c The stepwise addition of glucose-lowering medication is generally
preferred to initial combinationtherapy.
In most patients, type 2 diabetes is aprogressive disease, a consequence gen-erally attributed to a steady decline ofinsulin secretory capacity. The practicalimpact of gradual loss ofb-cell function isthat achieving a glycemic target withmonotherapy is typically limited to sev-eral years. Stepwise therapy (i.e., addingmedications to metformin to maintainHbA1c at target) is supported by clinicaltrials (3).While there is some support forinitial combination therapy due to thegreater initial reduction of HbA1c thancan be provided by metformin alone(190,191), there is little evidence thatthis approach is superior to sequentialaddition of medications for maintainingglycemic control or slowing the progres-sion of diabetes. However, since theabsolute effectiveness of most oral med-ications rarely exceeds an 11 mmol/mol(1%) reduction in HbA1c, initial combi-nation therapy may be considered inpatients presenting with HbA1c levelsmore than 17 mmol/mol (1.5%) abovetheir target. Fixed-dose formulations canimprove medication adherence whencombination therapy is used (192), andmay help achieve glycemic targets morerapidly (100). Potential benefits of com-bination therapy need to be weighedagainst the exposure of patients to mul-tiple medications and potential side ef-fects, increased cost, and, in the case offixed combination medications, less flex-ibility in dosing.
Choice of Glucose-LoweringMedication After Metformin
Consensus recommendation
c The selection of medication addedto metformin is based on patientpreference and clinical character-istics. Important clinical charac-teristics include the presence ofestablished ASCVD and other co-morbidities such as HF or CKD; therisk for specific adversemedicationeffects, particularly hypoglycemiaand weight gain; as well as safety,tolerability, and cost (Figs. 2–6).
As detailed in the “Medications for Low-ering Glucose” section, the glucose-lowering medications that can be addedto metformin have distinct profiles of
22 Consensus Report Diabetes Care

action, efficacy, and adverse effects(100,193). The early introduction of basalinsulin is well established, in particu-lar when HbA1c levels are very high(.97 mmol/mol [.11%]), symptomsof hyperglycemia are present, or thereis evidence of ongoing catabolism (e.g.,weight loss). This constellation of symp-toms can occur in type 2 diabetes butsuggest insulin deficiency and raise thepossibility of autoimmune (type 1) orpancreatogenic diabetes in which insu-lin would be the preferred therapy.While this remains the usual strategyfor patients when HbA1c levels are veryhigh, SGLT2 inhibitors (194) and GLP-1receptor agonists (195) have demon-strated efficacy in patients with HbA1clevels exceeding 75 mmol/mol (9%), withthe additional benefits of weight reduc-tion and reduced risk of hypoglycemia.Evidence from clinical trials supports
the use of several of the SGLT2 inhibitorsand GLP-1 receptor agonists as add-ontherapy for people with type 2 diabeteswithanHbA1c.53mmol/mol (.7%)andestablished CVD (48,51,52). However,since only 15–20% of patients withtype 2 diabetes conform to the charac-teristics of patients in these trials, otherclinical features need to be consideredin the majority when selecting secondmedications to add to metformin (Figs.2–6) (149,196–204).Sulfonylureas and insulin are associ-
ated with an increased risk for causinghypoglycemia and would not be pre-ferred for patients in whom this is aconcern. Furthermore, hypoglycemia isdistressing and somay reduce treatmentadherence (Fig. 5). For patients prioritiz-ing weight loss or weight maintenance(Fig. 4), important considerations includethe weight reduction associated withSGLT2 inhibitors and GLP-1 receptoragonists, the weight neutrality of DPP-4inhibitors, and the weight gain associ-ated with sulfonylureas, basal insulin,and TZDs. An important considerationfor society in general and for manypatients in particular is the cost ofmedications; sulfonylureas, pioglita-zone, and recombinant human insulinsare relatively inexpensive, althoughtheir cost may vary across regions.Short-term acquisition costs, longer-term treatment cost, and cost-effective-ness should be considered in clinicaldecision making when data are available(Fig. 6).
Intensification Beyond TwoMedications
Consensus recommendation
c Intensification of treatment be-yond dual therapy to maintainglycemic targets requires consider-ation of the impact of medicationside effects on comorbidities, aswell as the burden of treatmentand cost.
The lack of a substantial response to oneor more noninsulin therapies shouldraise the issue of adherence and, in thosewith weight loss, the possibility that thepatient has autoimmune (type 1) orpancreatogenic diabetes. However, itis common in people with long-standingdiabetes to require more than twoglucose-lowering agents, often includinginsulin. Compared with the knowledgebase guiding dual therapy of type 2 di-abetes, there is less evidence guidingthese choices (205). In general, inten-sification of treatment beyond twomedications follows the same generalprinciples as the addition of a secondmedication, with the assumption that theefficacy of third and fourth medicationswill be generally less than expected.No specific combination has demon-strated superiority except for thosethat include insulin and GLP-1 receptoragonists that have broad ranges of gly-cemic efficacy. As more medicationsare added, there is an increased riskof adverse effects. It is important toconsider medication interactions andwhether regimen complexity may be-come an obstacle to adherence. Finally,with each additional medication comesincreased costs, which can affect patientburden,medication-taking behavior, andmedication effectiveness (193,205–211).
While most patients require intensi-fication of glucose-lowering medica-tions, some require medication reductionor discontinuation of medication, partic-ularly if the therapy is ineffective or isexposing patients to a higher risk of sideeffects such as hypoglycemia or whenglycemic goals have changed due to achange in clinical circumstances (e.g.,development of comorbidities or evenhealthy aging). A guiding principle is thatfor all therapies the response should bereviewed at regular intervals, includingthe impact on efficacy (HbA1c, weight)and safety; the therapy should bestopped or the dose reduced if there are
minimal benefits or if harm outweighsany benefit. In particular, ceasing or reduc-ing the dose of medications that havean increased risk of hypoglycemia is im-portant when any new glucose-loweringtreatment (lifestyle or medication) isstarted (Fig. 7) (40). HbA1c levels below48 mmol/mol (6.5%) or substantially be-low the individualized glycemic targetshould prompt consideration of stoppingor reducing the dose of medications withrisk of hypoglycemia or weight gain.
Addition of Injectable Medications
Consensus recommendation
c In patients who need the greaterglucose-lowering effect of an in-jectable medication, GLP-1 recep-tor agonists are the preferredchoice to insulin. For patientswith extreme and symptomatic hy-perglycemia, insulin is recom-mended (Fig. 7).
See the “Insulin” and “Basal Insulin”sections in “Medications for LoweringGlucose” for more medication details.
Patients often prefer combinations oforal medications to injectable medications.The range of combinations available withcurrent oral medications allows many peo-ple to reach glycemic targets safely. How-ever, there is currently no evidence thatany single medication or combination hasdurable effects and, for many patients, in-jectable medications become necessarywithin 5–10 years of diabetes diagnosis.
Evidence from trials comparing GLP-1receptor agonists and insulin (basal, pre-mixed, or basal-bolus) shows similar oreven better efficacy in HbA1c reduction(212,213). GLP-1 receptor agonistshave a lower risk of hypoglycemia andare associated with reductions in bodyweight compared with weight gain withinsulin (212,214). Some GLP-1 receptoragonists allow for once-weekly injec-tions, as opposed to daily or more oftenfor insulin. Based on these consider-ations, a GLP-1 receptor agonist is thepreferred option in a patient with a def-inite diagnosis of type 2 diabetes whoneeds injectable therapy. However, thetolerability and high cost of GLP-1 re-ceptor agonists are important limita-tions to their use. If additional glucoselowering is needed despite therapy witha long-acting GLP-1 receptor agonist, theaddition of basal insulin is a reason-able option (215,216).
care.diabetesjournals.org Davies and Associates 23

Alternatively, the addition of insulin tooral medication regimens is well estab-lished. In particular, using basal insulinin combination with oral medications iseffective, and has less hypoglycemia andweight gain than combinations usingpremixed insulin formulations or pran-dial insulin (217). A standard approachfor optimizing basal insulin regimens isto titrate the dose based on a target fast-ing glucose concentration, which is a sim-ple index of effectiveness. Either NPHinsulin or long-acting insulin analogs areefficacious for controlling fasting glu-cose, although basal analog formulationsshow reduced risks of hypoglycemia,particularly overnight, when titrated tothe same fasting glucose target as NPHinsulin (157,218).
Beyond Basal Insulin
Consensus recommendation
c Patients who are unable to main-tain glycemic targets on basal in-sulin in combination with oralmedications can have treatmentintensified with GLP-1 receptor ag-onists, SGLT2 inhibitors, or prandialinsulin (Figs. 7 and 8).
It has become common practice to ap-proach insulin use in people with type 2diabetes by following the establishedparadigms developed for those withtype 1 diabetes. This includes multipledaily injections with doses of insulinanalogs before meals that are adjustedbased on ambient blood glucose andmeal constituents. While this is reason-able for people with type 2 diabeteswho are lean, insulinopenic, and sensi-tive to exogenous insulin, it ignores thesubstantial differences in pathophysiol-ogy between most people with type 2diabetes and type 1 diabetes. Most peo-ple with type 2 diabetes are obese andinsulin resistant, requiring much largerdoses of insulin and experiencing lowerrates of hypoglycemia than those withtype 1 diabetes. In patients with type 2diabetes, weight gain is a particularlyproblematic side effect of insulin use.Recent evidence supports the effective-ness of combinations of insulin withglucose-lowering medications that donot increase body weight. For example,SGLT2 inhibitors can be added to insulinregimens to lower blood glucose levelswithout increasing insulin doses, weightgain, or hypoglycemia (219–221). In a
meta-analysis that studied the combi-nation of either SGLT2 inhibitors or DPP-4 inhibitors with insulin, the SGLT2inhibitor–insulin combination was associ-ated with a greater reduction in HbA1c,an advantage in terms of body weightand no increase in the rates of hypo-glycemia (222,223). Depending onbaseline HbA1c, glycemic profile, andindividual response, the insulin dosemay need to be reduced to preventhypoglycemia when adding an SGLT2inhibitor.
The combination of basal insulin anda GLP-1 receptor agonist has high effi-cacy, with recent evidence from clinicaltrials demonstrating the benefits ofthis combination to lower HbA1c andlimit weight gain and hypoglycemiacompared with intensified insulin reg-imens (224,225). Most data come fromstudies in which a GLP-1 receptor ago-nist is added to basal insulin. However,there is evidence that insulin added to aGLP-1 receptor agonist can also effectivelylower HbA1c, although some weight gainresults (215). Fixed-ratio combinationsof insulin and GLP-1 receptor agonistsare available and can decrease thenumber of injections compared withadministering the medications sepa-rately (226–228).
A final approach to glycemic manage-ment when basal insulin plus oral med-ications is insufficient to achieve HbA1ctargets is intensified insulin regimens(Figs. 7 and 8). DSMES focused on insulintherapy is particularly helpful when in-tensified insulin therapy is considered.Referral to a diabetes specialist teamshould be considered in cases wherethe provider is uncomfortable or unfa-miliar with intensification, poor out-comes continue despite intensification,or patients have other issues that com-plicate intensification. Intensified insulinregimens include 1) one or more dailyinjections of rapid- or short-acting insulinbefore meals (prandial insulin) or 2)switching to one to three daily admin-istrations of afixed combination of short-and long-acting insulin (premixed orbiphasic insulins) (229,230). When addingprandial insulin, giving one injection withthe largest meal of the day is a simple andsafe approach (231). Over time, if glyce-mic targets are not met with one dose ofprandial insulin daily, additional prandialinjections can be added to other meals(232). Results of meta-analyses suggest
a modestly greater reduction in HbA1cwith basal-prandial regimens com-pared with biphasic insulin regimens,but at the expense of greater weightgain (233–235). While still commonlyused, we do not generally advocatepremixed insulin regimens, particularlythose administered three times daily,for routine use when intensifying insulinregimens (Fig. 7).
Continuous insulin infusion using in-sulin pumps may have a role in a smallminority of people with type 2 diabetes(236).
Access and Cost
Consensus recommendation
c Access, treatment cost, and in-surance coverage should all beconsidered when selecting glucose-lowering medications.
The availability of glucose-loweringmedications, patient support systems,and blood glucose-monitoring devicescan differ worldwide, depending on aregion’s economy, culture, and healthcare system. Cost of and access to newermedications and insulin remain impor-tant issues throughout the world. Al-though the economics of diabetes careis complex and broadly includes the coststo society of diabetic complications andlong-term outcomes, the cost of drugsand the affordability of treatment areoften the primary basis for decisionmaking. Within health care systems, var-iance in medication coverage is based ondifferent assessments of cost-effectiveness.This results in huge disparities in thecost of new and old glucose-loweringmedications in some countries, limitingaccess to the full range of diabe-tes therapies in large segments of thepopulation, and creating a two-tieredsystem of treatment. Since glycemicmanagement remains a cornerstone ofthe prevention of diabetes complica-tions, these disparities raise questionsof fairness, equity, and overall publichealth. Nonetheless, the use of lessexpensive agents, such as metformin,sulfonylureas, andhuman insulin, remaineffective options (Figs. 2 and 6). Redou-bling lifestyle management efforts canalso have great impact, but behavioralintervention and support can also becostly, and socioeconomic barriers toimproving lifestyle are well described(237).
24 Consensus Report Diabetes Care

Emerging TechnologyThere is an increasing call for the use oftechnology and telemedicine to improvepatients’ health (238). Many types ofinputs can be digitalized, such as bloodglucose levels, time spent exercising,steps walked, energy ingested, medica-tion doses administered, blood pressure,and weight. Patterns in these variablescan be identified by software, leading
to specific treatment recommendationssupported by real-time algorithms.Telemedicine incorporates multiple typesof communication services, such as two-way video, e-mail, texting, smartphones,tablets, wireless monitors, decision sup-port tools, and other forms of telecom-munication technologies. Results overallsuggest a modest improvement in glyce-mic control (239,240).
KEY KNOWLEDGE GAPS
Despite over 200 years of research onlifestyle management of diabetes andmore than 50 years of comparative-effectiveness research in diabetes,innumerable unanswerecd questionsregarding the management of type 2diabetes remain. In the context ofour current consensus recommenda-tions, the following is an incomplete
Figure 8—Considering oral therapy in combinationwith injectable therapies. DKA, diabetic ketoacidosis; DPP-4i, dipeptidyl peptidase 4 inhibitor; GLP-1RA, glucagon-like peptide 1 receptor agonist; SGLT2i, SGLT2 inhibitor; SU, sulfonylurea.
care.diabetesjournals.org Davies and Associates 25

discussion of vexing issues that must beaddressed.Evolving areas of current investiga-
tion will provide improvements in dia-betes care and hold great hope for newtreatments.
c Implementation science. The toolsavailable to prevent and treat diabetesare vastly improved. However, imple-mentation of effective innovation haslagged behind.
c Basic science. Our understanding ofthe basic mechanisms of diabetes, thedevelopment of complications, andthe treatment of both, though contin-uously advancing, has highlighted howmuch we do not know.
c Personalized/precision medicine.Though promising, these –omics andbig data approaches addressing bothpersonal and environmental factorsand their interaction are largely un-realized in diabetes care and willrequire large investments and coordi-nation to have impact.
c Informatics. The benefits and roleof enhanced monitoring of glucoseand other variables leveraged withreal-time informatics-based approachesto adapt treatment on an individualbasis has great potential but has notbeen elucidated.
c Overweight/obesity. Current therapyis clearly inadequate. Innovation inmethods and implementation wouldtransform diabetes prevention andcare. Understanding the biology, psy-chology, and sociology of obesity toidentify pharmacological, behavioral,and political approaches to preventingand treating this principal cause oftype 2 diabetes is essential.
c Lifestyle management and DSMES.Though the benefits of these ap-proaches are clear, better paradigmson how to target, individualize, andsustain the effects are needed.
c b-Cell function. Preserving and en-hancing b-cell function is perceivedas the holy grail of diabetes and yeteffective techniques are inadequatelydeveloped.
c Translational research. There is a hugegap between the knowledge gainedfrom clinical trials and application ofthat information in clinical practice.This gap should be filled with prag-matic studies and other designs thatinclude costs, measures of patient
preference, and other patient-recordedoutcome measures. Patients and otherstakeholders should have more inputinto trial designs and outcomes. Prag-matic designs will enhance generaliz-ability of results and reduce cost.Better application of “real-world ev-idence”will complement randomizedtrial evidence.
c Drug development. New medicationswill require demonstration of broadefficacy for glucose, comorbiditiesand/or complications, aswell as safetyand tolerability to compete in themarketplace.
c Complications. Steatohepatitis, HF,nonalbuminuric CKD, chronic mentalillness, and other emerging issues arecomplications in diabetes that maysupplant classical microvascular andmacrovascular disease in importanceand impact. Understanding optimaldiagnostic, screening, and treatmentstrategies is urgently needed.
Other areas of importance include bet-ter segmentation of “type 2 diabetes,” aswell as appropriate diagnosis of second-ary diabetes, which should allow moreinformed individualization of care. Betterdata on optimal approaches to diabetesmanagement in frail and older adultpatients is urgently required consideringthe controversy around glycemic targetsand the benefits and harms of specifictreatments from lifestyle managementto medications. Current approaches to themanagement of type 2 diabetes in ado-lescents and young adults do not seem toalter the loss ofb-cell function andmostindividuals in this age-group quicklytransition to insulin therapy. Studiesto guide optimal therapy in this emergingpopulation with a terrifyingly high risk ofearly disability is an immediate need.
There are enduring questions thatcontinue to challenge guideline develop-ment. For example, does metformin pro-vide cardiovascular benefit in patientswith type 2 diabetes early in the naturalhistory of diabetes, as suggested by theUKPDS? Is metformin’s role as first-linemedication management truly evidence-based or a quirk of history? Though therationale for early combination therapytargeting normal levels of glycemia inearly diabetes is seductive, clinical trialevidence to support specific combina-tions and targets is essentially nonexis-tent. As the cost implications for these
approaches is enormous, evidence is des-perately needed. Different models ofcare are being implemented globally.Defining optimal cost-effective approachesto care, particularly in the managementof patients (multimorbidity), is essential.
New questions arise from the recentcardiovascular outcomes studies. Dothe cardiovascular and renal benefits ofSGLT2 inhibitors and GLP-1 receptor ag-onists demonstrated in patients withestablished CVD extend to lower-riskpatients? Is there additive benefit ofuse of GLP-1 receptor agonists andSGLT2 inhibitors for prevention of car-diovascular and renal events? If so, inwhat populations?
Addressing these and other vital clin-ical questions will require additional in-vestment in basic, translational, clinical,and implementation research. Moretime- and cost-efficient research para-digms to address patient-centered endpoints will need to be developed throughregulatory reform and leveraging infor-matics and coordinated learning healthcare systems. The increasing burden ofcardiorenal metabolic disease in termsof incidence, prevalence, and cost isan existential threat to society. Urgentattention to improve prevention andtreatment is of the essence.
The management of hyperglycemia intype 2 diabetes has become extraor-dinarily complex with the number ofglucose-lowering medications now avail-able. Patient-centered decision makingand support and consistent efforts toimprove diet and exercise remain thefoundation of all glycemic management.Initial use of metformin, followed byaddition of glucose-lowering medicationsbased on patient comorbidities and con-cerns is recommended as we await an-swers to themany questions that remain.
Acknowledgments. The authors would like toacknowledge Mindy Saraco (Associate Director,Scientific & Medical Communication), GedeonTopacio (Finance& ProjectManager, Research&Scientific Programs), and Erika Berg (Director,Scientific & Medical Affairs) from the AmericanDiabetes Association as well as Mary Hata (Ex-ecutive Assistant) and Petra Niemann (ExecutiveAssistant) from EASD for their help with thedevelopment of the consensus report and re-lated meetings/presentations. The authorswould like to also acknowledge Mike Bonar(Creative Director) and Charlie Franklin (De-sign Assistant) from the Leicester Diabetes Cen-tre, Leicester, U.K., who provided considerable
26 Consensus Report Diabetes Care

support indraftingandamending thefigures.Theauthors also acknowledge Francesco Zaccardi(PhD, Clinical Research Fellow, University ofLeicester, Leicester, U.K.) and David Kloecker(Medical Student, University of Leicester) whoassisted with extracting PubMed articles andidentifying relevant records by title and abstract;Francesco Zaccardi helped to define the initialsearch strategy and prepare the Excel file. Theauthors acknowledge the invited peer reviewerswho provided comments on an earlier draft ofthis report: Amanda Adler (Addenbroke’s Hospital,Cambridge, U.K.), Kare I. Birkeland (University ofOslo, Oslo, Norway), James J. Chamberlain (St.Mark’s Hospital, Salt Lake City, UT), Jill P. Crandall(Albert Einstein College of Medicine, New YorkCity, NY), Ian H. de Boer (University of Washington,Seattle, WA), Stefano Del Prato (University ofPisa, Pisa, Italy), George Dimitriadis (Athens Uni-versity, Athens, Greece), Sean Dinneen (NationalUniversity of Ireland, Galway, Ireland), Vivian A.Fonseca (Tulane University, New Orleans, LA),SimonR.Heller (University of Sheffield, Sheffield,U.K.), Richard I.G.Holt (UniversityofSouthampton,Southampton, U.K.), Silvio E. Inzucchi (Yale Uni-versity, NewHaven, CT), Eric L. Johnson (Universityof North Dakota, Grand Forks, ND), JoshuaJ. Neumiller (Washington State University, Spo-kane,WA), KamleshKhunti (University of Leicester,Leicester, U.K.), Harald H. Klein (Ruhr University ofBochum, Bochum, U.K.), Line Kleinebreil (Hopitalnational de Saint Maurice, Saint-Maurice, France),Jose Manuel Fernandez-Real (Universitat de Gi-rona, Girona, Spain), Sally M. Marshall (NewcastleUniversity, Newcastle upon Tyne, U.K.), ManelMata-Cases (Institut Universitari d’Investigacio enAtencio Primaria Jordi Gol [IDIAP Jordi Gol], Bar-celona, Spain), David R. Matthews (University ofOxford, Oxford, U.K.), David M. Nathan (Mas-sachusetts General Hospital, Boston,MA),MichaelA. Nauck (Diabetes Center Bochum-Hattingen,St. Josef-Hospital, Ruhr-University, Bochum,Germany), Frank Nobels (OLV-Hospital, Aalst,Belgium), Richard E. Pratley (Florida HospitalDiabetes Institute, Orlando, FL), Maria JoseRedondo (Baylor College of Medicine, Houston,TX), Michael R. Rickels (University of Pennsylvania,Philadelphia, PA), Matthew C. Riddle (OregonHealth & Science University, Portland, OR), JulioRosenstock (Diabetes and Endocrine Center, Dallas,TX), Giorgio Sesti (Magna Graecia University ofCatanzaro, Catanzaro, Italy), Neil Skolnik (AbingtonFamily Medicine, Jenkintown, PA), Krzysztof Strojek(SilesianMedicalUniversity, Zabrze, Poland), JenniferTrujillo (University of Colorado, Denver, CO),Guillermo E. Umpierrez (Emory University,Atlanta, GA), and Jennifer Wyckoff (Universityof Michigan, Ann Arbor, MI).Funding. This activity was funded by the Amer-ican Diabetes Association and the EuropeanAssociation for the Study of Diabetes.Dualityof Interest.M.J.D. reports personal feesand grants from Boehringer Ingelheim, Janssen,Novo Nordisk, and Sanofi and personal fees fromAstraZeneca,Eli Lilly,GileadSciencesLtd., Intarcia/Servier, Merck Sharp & Dohme, MitsubishiTanabe Pharma Corporation, and Takeda Phar-maceuticals International Inc. D.A.D’A. reportspersonal fees from Eli Lilly, Merck, Novo Nordisk,and Intarcia and grants from Merck and Ligandduring the conduct of the study; personal feesfrom Eli Lilly, Merck, Novo Nordisk, and Intarcia
and grants from Merck and Ligand outside thesubmitted work. J.F. has nothing to disclose. J.F.’sinput into this consensus report is from her ownperspective and the report does not reflect theview of the National Institutes of Health, De-partment of Health and Human Services, or theU.S. Government. W.N.K. has nothing to disclose.C.M. reports grants and personal fees fromNovoNordisk, grants and personal fees from Sanofi,grants and personal fees from Merck Sharp &Dohme, grants and personal fees from Eli Lillyand Company, grants and personal fees fromNovartis, personal fees from Bristol-Myers Squibb,personal fees from AstraZeneca, grants andpersonal fees from Boehringer Ingelheim, per-sonal fees from Hanmi Pharmaceuticals, grantsandpersonal fees fromRocheDiagnostics, grantsand personal fees from Medtronic, grants andpersonal fees from Intrexon, grants and personalfees from Abbott, and personal fees from UCB,outside the submitted work. G.M. reports grantsand personal fees from Novo Nordisk, personalfees from Johnson & Johnson, and personal feesfromFractyl Inc., during the conduct of the study.P.R. reports grants and nonfinancial and othersupport from Novo Nordisk, grants and othersupport from AstraZeneca, other support fromBayer, other support fromBoehringer Ingelheim,other support from Merck Sharp & Dohme, andother support from Eli Lilly, during the conduct ofthe study. A.T. reports nonfinancial support fromthe European Association for the Study of Di-abetes during the conduct of the study; grantsand other support from Boehringer Ingelheim,grants and other support from Novo Nordisk,other support from Novartis, grants and othersupport from Sanofi, grants and other supportfrom AstraZeneca, grants from GSK, and grantsandother support fromEuropeanFoundation forthe Study of Diabetes, outside the submittedwork. D.J.W. has nothing to disclose. J.B.B. hasprovided consultation to Adocia, AstraZeneca,Eli Lilly, GI Dynamics, Intarcia, MannKind,NovaTarg, Novo Nordisk, Senseonics, and vTvTherapeutics with fees paid to the Universityof North Carolina. He has received grant supportfrom AstraZeneca, Johnson & Johnson, NovoNordisk, Sanofi, and vTv Therapeutics. He is aconsultant to Neurimmune AG. He holds stockoptions in Mellitus Health, PhaseBio, and Stabil-ity Health. He is supported by a grant from theNational Institutes of Health (UL1TR002489). Noother potential conflicts of interest relevant tothis article were reported.Author Contributions. All authors were re-sponsible for drafting the article and revising itcritically for important intellectual content. Allauthors approved the version to be published.Data Availability. The details of the searchstrategy, the results, and the classificationfor the included articles are available athttps://dx.doi.org/10.17632/h5rcnxpk8w.1.
References1. Rodriguez-Gutierrez R, Gionfriddo MR,Ospina NS, et al. Shared decision making inendocrinology: present and future directions.Lancet Diabetes Endocrinol 2016;4:706–7162. American Diabetes Association. 6. Glyce-mic targets: Standards of Medical Care in Dia-betesd2018. Diabetes Care 2018;41(Suppl. 1):S55–S64
3. American Diabetes Association. 8. Pharma-cologic approaches to glycemic treatment: Stan-dards of Medical Care in Diabetesd2018.Diabetes Care 2018;41(Suppl. 1):S73–S854. Inzucchi SE, Bergenstal RM, Buse JB, et al.;Position Statement of the American DiabetesAssociation (ADA) and the European Associ-ation for the Study of Diabetes (EASD). Man-agement of hyperglycaemia in type 2 diabetesa patient-centered approach. Position state-ment of the American Diabetes Association(ADA) and the European Association for theStudy of Diabetes (EASD). Diabetologia 2012;55:1577–15965. Inzucchi SE, Bergenstal RM, Buse JB, et al.Management of hyperglycaemia in type 2 di-abetes, 2015: a patient-centred approach. Up-date to a position statement of the AmericanDiabetes Association and the European Associ-ation for the Study of Diabetes. Diabetologia2015;58:429–4426. Riddle MC, Gerstein HC, Holman RR, et al.A1C targets should be personalized to maxi-mize benefits while limiting risks. Diabetes Care2018;41:1121–11247. American Diabetes Association. 9. Cardiovas-cular disease and risk management: Standardsof Medical Care in Diabetesd2018. DiabetesCare 2018;41(Suppl. 1):S86–S1048. Gæde P, Oellgaard J, CarstensenB, et al. Yearsof life gained by multifactorial intervention inpatientswith type 2 diabetesmellitus andmicro-albuminuria: 21 years follow-up on the Steno-2randomised trial. Diabetologia 2016;59:2298–23079. Khunti K, Kosiborod M, Ray KK. Legacy ben-efits of blood glucose, blood pressure and lipidcontrol in individuals with diabetes and cardio-vascular disease: time to overcome multifactorialtherapeutic inertia? Diabetes Obes Metab 2018;20:1337–134110. Gregg EW, Sattar N, Ali MK. The changingface of diabetes complications. Lancet DiabetesEndocrinol 2016;4:537–54711. Little RR, Rohlfing CL, Sacks DB. Status ofHbA1cmeasurement and goals for improvement:from chaos to order for improving diabetes care.Clin Chem 2011;57:204–21412. American Diabetes Association. 2. Classifi-cation and diagnosis of diabetes: Standards ofMedical Care in Diabetesd2018. Diabetes Care2018;41(Suppl. 1):S13–S2713. Mannucci E, Antenore A, Giorgino F, ScaviniM. Effects of structured versus unstructuredself-monitoring of blood glucose on glucosecontrol in patients with non-insulin-treatedtype 2 diabetes: a meta-analysis of randomizedcontrolled trials. J Diabetes Sci Technol 2018;12:183–18914. Young LA, Buse JB, Weaver MA, et al.;Monitor Trial Group. Glucose self-monitoringin non–insulin-treated patients with type 2 di-abetes in primary care settings: a randomizedtrial. JAMA Intern Med 2017;177:920–92915. Anjana RM, Kesavadev J, Neeta D, et al. Amulticenter real-life study on the effect of flashglucose monitoring on glycemic control in pa-tients with type 1 and type 2 diabetes. DiabetesTechnol Ther 2017;19:533–54016. American Diabetes Association. 3. Compre-hensive medical evaluation and assessment ofcomorbidities: Standards of Medical Care in
care.diabetesjournals.org Davies and Associates 27

Diabetesd2018. Diabetes Care 2018;41(Suppl.1):S28–S3717. Kunneman M, Montori VM, Castaneda-Guarderas A, Hess EP. What is shared decisionmaking? (and what it is not). Acad Emerg Med2016;23:1320–132418. Breslin M, Mullan RJ, Montori VM. Thedesign of a decision aid about diabetesmedicationsfor use during the consultation with patientswith type 2 diabetes. Patient Educ Couns 2008;73:465–47219. Mullan RJ, Montori VM, Shah ND, et al. Thediabetes mellitus medication choice decisionaid: a randomized trial. Arch Intern Med 2009;169:1560–156820. Stacey D, Legare F, Lewis K, et al. Decisionaids for people facing health treatment or screen-ing decisions. Cochrane Database Syst Rev 2017;4:CD00143121. American Diabetes Association. 4. Lifestylemanagement: Standards of Medical Care inDiabetesd2018. Diabetes Care 2018;41(Suppl.1):S38–S5022. Powers MA, Bardsley J, Cypress M, et al.Diabetes self-management education and sup-port in type2diabetes: a joint position statementof the American Diabetes Association, the Amer-ican Association of Diabetes Educators, and theAcademy of Nutrition and Dietetics. DiabetesCare 2015;38:1372–138223. Department of Health. Diabetes UK. Struc-tured patient education in diabetes: reportfrom the Patient Education Working Group.Structured patient education in diabetes: reportfromthePatientEducationWorkingGroup,2005.Available from http://webarchive.nationalarchives.gov.uk/20130105204013/http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4113195.Accessed 29 August 201824. National Institute for Health and ClinicalExcellence. (2011) Quality Standard for Diabetesin Adults, Statements 2 and 3, 2011. Availablefrom https://www.nice.org.uk/guidance/qs6.Accessed 29 August 201825. Beck J,GreenwoodDA,BlantonL, et al.; 2017Standards Revision Task Force. 2017 Nationalstandards for diabetes self-management educa-tion and support. Diabetes Educ 2017;43:449–46426. Chrvala CA, Sherr D, Lipman RD. Diabetesself-management education for adults withtype 2 diabetes mellitus: a systematic reviewof the effect on glycemic control. Patient EducCouns 2016;99:926–94327. Pillay J, Armstrong MJ, Butalia S, et al. Be-havioral programs for type 2 diabetes mellitus: asystematic review and network meta-analysis.Ann Intern Med 2015;163:848–86028. ZhaoF-F,SuhonenR,KoskinenS, Leino-KilpiH.Theory-based self-management educationalinterventions on patients with type 2 diabetes: asystematic review and meta-analysis of random-ized controlled trials. J Adv Nurs 2017;73:812–83329. Odgers-Jewell K, Ball LE, Kelly JT, Isenring EA,Reidlinger DP, Thomas R. Effectiveness of group-based self-management education for individu-als with type 2 diabetes: a systematic reviewwithmeta-analyses andmeta-regression. DiabetMed 2017;34:1027–103930. He X, Li J, Wang B, et al. Diabetes self-management education reduces risk of all-cause
mortality in type 2 diabetes patients: a system-atic review and meta-analysis. Endocrine 2017;55:712–73131. Chatterjee S, Davies MJ, Heller S, Speight J,Snoek FJ, Khunti K. Diabetes structured self-management education programmes: a narrativereview and current innovations. Lancet DiabetesEndocrinol 2018;6:130–14232. Egede LE, Gebregziabher M, Echols C, LynchCP. Longitudinal effects of medication nonad-herence on glycemic control. Ann Pharmacother2014;48:562–57033. Huber CA, Reich O.Medication adherence inpatients with diabetes mellitus: does physiciandrug dispensing enhance quality of care? Evi-dence from a large health claims database inSwitzerland. Patient Prefer Adherence 2016;10:1803–180934. Iglay K, Cartier SE, Rosen VM, et al. Meta-analysis of studies examining medication adher-ence, persistence, and discontinuation of oralantihyperglycemic agents in type2diabetes.CurrMed Res Opin 2015;31:1283–129635. McGovern A, Tippu Z, Hinton W, Munro N,Whyte M, de Lusignan S. Systematic review ofadherence rates by medication class in type 2diabetes: a study protocol. BMJ Open 2016;6:e01046936. Khunti K, Seidu S, Kunutsor S, Davies M.Association between adherence to pharma-cotherapy and outcomes in type 2 diabetes: ameta-analysis. Diabetes Care 2017;40:1588–159637. Polonsky WH, Henry RR. Poor medicationadherence in type 2 diabetes: recognizing thescope of the problem and its key contributors.Patient Prefer Adherence 2016;10:1299–130738. McGovern A, Tippu Z, Hinton W, Munro N,Whyte M, de Lusignan S. Comparison of med-ication adherence and persistence in type 2diabetes: a systematic review andmeta-analysis.Diabetes Obes Metab 2018;20:1040–104339. Lasalvia P, Barahona-Correa JE, Romero-Alvernia DM, et al. Pen devices for insulinself-administration compared with needle andvial: systematic review of the literature andmeta-analysis. J Diabetes Sci Technol 2016;10:959–96640. Khunti K, Davies MJ. Clinical inertia-time toreappraise the terminology? Prim Care Diabetes2017;11:105–10641. Furler J, O’Neal D, Speight J, et al. Supportinginsulin initiation in type 2 diabetes in primarycare: results of the Stepping Up pragmatic clusterrandomised controlled clinical trial. BMJ 2017;356:j78342. Manski-Nankervis J-A, Furler J, O’Neal D,Ginnivan L, Thuraisingam S, Blackberry I. Over-coming clinical inertia in insulin initiation inprimary care for patients with type 2 diabetes:24-month follow-up of the Stepping Up clusterrandomised controlled trial. Prim Care Diabetes2017;11:474–48143. TabeshM,Magliano DJ, Koye DN, Shaw JE.The effect of nurse prescribers on glycaemiccontrol in type 2 diabetes: a systematic reviewandmeta-analysis. Int J Nurs Stud 2018;78:37–4344. Murphy ME, Byrne M, Galvin R, Boland F,Fahey T, Smith SM. Improving risk factor man-agement for patients with poorly controlled type2 diabetes: a systematic review of healthcare
interventions in primary care and communitysettings. BMJ Open 2017;7:e01513545. American Diabetes Association. 1. Improv-ing care and promoting health in populations:Standards of Medical Care in Diabetesd2018.Diabetes Care 2018;41(Suppl. 1):S7–S1246. Cefalu WT, Kaul S, Gerstein HC, et al. Car-diovascular outcomes trials in type 2 diabetes:where do we go from here? Reflections from aDiabetes Care Editors’ Expert Forum. DiabetesCare 2018;41:14–3147. Marso SP, Daniels GH, Brown-Frandsen K,et al.; LEADER Steering Committee; LEADER TrialInvestigators. Liraglutide and cardiovascular out-comes in type 2 diabetes. N Engl JMed2016;375:311–32248. Marso SP, Bain SC, Consoli A, et al.; SUSTAIN-6 Investigators. Semaglutide and cardiovascularoutcomes in patientswith type2diabetes.N EnglJ Med 2016;375:1834–184449. Holman RR, Bethel MA, Mentz RJ, et al.;EXSCEL Study Group. Effects of once-weekly ex-enatide on cardiovascular outcomes in type 2diabetes. N Engl J Med 2017;377:1228–123950. Pfeffer MA, Claggett B, Diaz R, et al.; ELIXAInvestigators. Lixisenatide in patients with type 2diabetes and acute coronary syndrome. N EnglJ Med 2015;373:2247–225751. Zinman B, Wanner C, Lachin JM, et al.;EMPA-REG OUTCOME Investigators. Empagli-flozin, cardiovascular outcomes, and mortalityin type 2 diabetes. N Engl J Med 2015;373:2117–212852. Neal B, Perkovic V, Mahaffey KW, et al.;CANVAS Program Collaborative Group. Cana-gliflozin and cardiovascular and renal eventsin type 2 diabetes. N Engl J Med 2017;377:644–65753. Lehrke M, Marx N. Diabetes mellitus andheart failure. Am J Med 2017;130(6S):S40–S5054. Fitchett D, Zinman B, Wanner C, et al.;EMPA-REG OUTCOME� trial investigators. Heartfailure outcomes with empagliflozin in patientswith type 2 diabetes at high cardiovascular risk:results of the EMPA-REG OUTCOME� trial. EurHeart J 2016;37:1526–153455. Radholm K, Figtree G, Perkovic V, et al.Canagliflozin and heart failure in type 2 diabetesmellitus: results from the CANVAS Program.Circulation 2018;138:458–46956. Margulies KB, Hernandez AF, Redfield MM,et al.; NHLBI Heart Failure Clinical ResearchNetwork. Effects of liraglutide on clinical stabilityamong patients with advanced heart failure andreduced ejection fraction: a randomized clinicaltrial. JAMA 2016;316:500–50857. Jorsal A, KistorpC,HolmagerP, et al. Effect ofliraglutide, a glucagon-like peptide-1 analogue,on left ventricular function in stable chronic heartfailure patients with and without diabetes(LIVE)-a multicentre, double-blind, randomised,placebo-controlled trial. Eur J Heart Fail 2017;19:69–7758. Scirica BM, Bhatt DL, Braunwald E, et al.;SAVOR-TIMI 53 Steering Committee and Inves-tigators. Saxagliptin and cardiovascular outcomesin patients with type 2 diabetes mellitus. N EnglJ Med 2013;369:1317–132659. White WB, Cannon CP, Heller SR, et al.;EXAMINE Investigators. Alogliptin after acutecoronary syndrome in patients with type 2 di-abetes. N Engl J Med 2013;369:1327–1335
28 Consensus Report Diabetes Care

60. Green JB, Bethel MA, Armstrong PW, et al.;TECOS Study Group. Effect of sitagliptin oncardiovascular outcomes in type 2 diabetes. NEngl J Med 2015;373:232–24261. Wanner C, Inzucchi SE, Lachin JM, et al.;EMPA-REG OUTCOME Investigators. Empagliflo-zin and progression of kidney disease in type 2diabetes. N Engl J Med 2016;375:323–33462. Jardine MJ, Mahaffey KW, Neal B, et al.;CREDENCE study investigators. The Canagliflozinand Renal Endpoints in Diabetes with EstablishedNephropathy Clinical Evaluation (CREDENCE)study rationale, design, and baseline character-istics. Am J Nephrol 2017;46:462–47263. Mann JFE, Ørsted DD, Brown-Frandsen K,et al.; LEADER Steering Committee and Investi-gators. Liraglutide and renal outcomes in type 2diabetes. N Engl J Med 2017;377:839–84864. DeaconCF. A reviewofdipeptidyl peptidase-4 inhibitors. Hot topics from randomized con-trolled trials. Diabetes Obes Metab 2018;20(Suppl. 1):34–4665. American Diabetes Association. 7. Obesitymanagement for the treatment of type 2 diabe-tes: Standards of Medical Care in Diabetesd2018. Diabetes Care 2018;41(Suppl. 1):S65–S7266. Shai I, Schwarzfuchs D, Henkin Y, et al.;Dietary Intervention Randomized ControlledTrial (DIRECT) Group. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet.N Engl J Med 2008;359:229–24167. Esposito K, Maiorino MI, Ciotola M, et al.Effects of aMediterranean-style diet on theneedfor antihyperglycemic drug therapy in patientswith newly diagnosed type 2 diabetes: a ran-domized trial. Ann Intern Med 2009;151:306–31468. Esposito K, Maiorino MI, Petrizzo M,Bellastella G, Giugliano D. The effects of a Med-iterranean diet on the need for diabetes drugsand remission of newly diagnosed type 2 di-abetes: follow-up of a randomized trial. DiabetesCare 2014;37:1824–183069. Huo R, Du T, Xu Y, et al. Effects of Medi-terranean-style diet on glycemic control, weightloss and cardiovascular risk factors among type 2diabetes individuals: a meta-analysis. Eur J ClinNutr 2015;69:1200–120870. Snorgaard O, Poulsen GM, Andersen HK,Astrup A. Systematic review and meta-analysisof dietary carbohydrate restriction in patientswith type 2 diabetes. BMJ Open Diabetes ResCare 2017;5:e00035471. Ajala O, English P, Pinkney J. Systematicreview and meta-analysis of different dietaryapproaches to the management of type 2 di-abetes. Am J Clin Nutr 2013;97:505–51672. Azadbakht L, Fard NRP, Karimi M, et al.Effects of the Dietary Approaches to Stop Hy-pertension (DASH) eating plan on cardiovascularrisks among type 2 diabetic patients: a random-ized crossover clinical trial. Diabetes Care 2011;34:55–5773. Sainsbury E, Kizirian NV, Partridge SR, Gill T,Colagiuri S, Gibson AA. Effect of dietary carbo-hydrate restriction on glycemic control in adultswith diabetes: a systematic review and meta-analysis. Diabetes Res Clin Pract 2018;139:239–25274. Yokoyama Y, Barnard ND, Levin SM,Watanabe M. Vegetarian diets and glycemiccontrol in diabetes: a systematic review and
meta-analysis. Cardiovasc Diagn Ther 2014;4:373–38275. LeanME, LeslieWS, BarnesAC, et al. Primarycare-led weight management for remission oftype 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet 2018;391:541–55176. Wing RR, Bolin P, Brancati FL, et al.; LookAHEAD Research Group. Cardiovascular effectsof intensive lifestyle intervention in type 2 di-abetes. N Engl J Med 2013;369:145–15477. O’Neil PM, Miller-Kovach K, Tuerk PW, et al.Randomized controlled trial of a nationally avail-able weight control program tailored for adultswith type2diabetes.Obesity (SilverSpring)2016;24:2269–227778. Jebb SA, Ahern AL, Olson AD, et al. Primarycare referral to a commercial provider for weightloss treatment versus standard care: a rando-mised controlled trial. Lancet 2011;378:1485–149279. Leblanc ES, O’Connor E, Whitlock EP,Patnode CD, Kapka T. Effectiveness of primarycare-relevant treatments for obesity in adults:a systematic evidence review for the U.S. Pre-ventive Services Task Force. Ann Intern Med2011;155:434–44780. Delahanty LM, Dalton KM, Porneala B, et al.Improving diabetes outcomes through lifestylechange – a randomized controlled trial. Obesity(Silver Spring) 2015;23:1792–179981. Boule NG, Haddad E, Kenny GP, Wells GA,Sigal RJ. Effects of exercise on glycemic controland body mass in type 2 diabetes mellitus: ameta-analysis of controlled clinical trials. JAMA2001;286:1218–122782. Chudyk A, Petrella RJ. Effects of exerciseon cardiovascular risk factors in type 2 diabetes:a meta-analysis. Diabetes Care 2011;34:1228–123783. Yang Z, Scott CA, Mao C, Tang J, Farmer AJ.Resistance exercise versus aerobic exercise fortype 2 diabetes: a systematic review and meta-analysis. Sports Med 2014;44:487–49984. Balducci S, Zanuso S, Nicolucci A, et al.;Italian Diabetes Exercise Study (IDES) Investiga-tors. Effect of an intensive exercise interventionstrategy on modifiable cardiovascular risk fac-tors in subjects with type 2 diabetes mellitus: arandomized controlled trial: the Italian Diabetesand Exercise Study (IDES). Arch Intern Med2010;170:1794–180385. Schwingshackl L, Missbach B, Dias S, Konig J,Hoffmann G. Impact of different training mo-dalities on glycaemic control and blood lipids inpatients with type 2 diabetes: a systematic re-view and network meta-analysis. Diabetologia2014;57:1789–179786. Qiu S, Cai X, Schumann U, Velders M, Sun Z,Steinacker JM. Impact of walking on glycemiccontrol and other cardiovascular risk factors intype 2 diabetes: a meta-analysis. PLoS One 2014;9:e10976787. Rees JL, Johnson ST, Boule NG. Aquaticexercise for adults with type 2 diabetes: ameta-analysis. Acta Diabetol 2017;54:895–90488. Pai L-W, Li T-C, Hwu Y-J, Chang SC, Chen LL,Chang PY. The effectiveness of regular leisure-time physical activities on long-term glycemiccontrol in people with type 2 diabetes: a sys-tematic review and meta-analysis. Diabetes ResClin Pract 2016;113:77–85
89. Lee MS, Jun JH, Lim H-J, Lim H-S. A sys-tematic review and meta-analysis of tai chi fortreating type 2 diabetes. Maturitas 2015;80:14–2390. Cui J, Yan J-H, Yan L-M, Pan L, Le JJ, Guo YZ.Effects of yoga in adults with type 2 diabetesmellitus: a meta-analysis. J Diabetes Investig2017;8:201–20991. Qiu S, Cai X, Chen X, Yang B, Sun Z. Stepcounter use in type 2 diabetes: a meta-analysisof randomized controlled trials. BMCMed 2014;12:3692. Franz MJ, Boucher JL, Rutten-Ramos S,VanWormer JJ. Lifestyleweight-loss interventionoutcomes in overweight and obese adults withtype 2 diabetes: a systematic review and meta-analysis of randomized clinical trials. J Acad NutrDiet 2015;115:1447–146393. Aggarwal N, Singla A, Mathieu C, et al.Metformin extended-release versus immediate-release: an international, randomized, double-blind, head-to-head trial inpharmacotherapy-naıvepatients with type 2 diabetes. Diabetes ObesMetab 2018;20:463–46794. Garber AJ, Duncan TG, Goodman AM, MillsDJ, Rohlf JL. Efficacy of metformin in type IIdiabetes: results of a double-blind, placebo-controlled, dose-response trial. Am J Med1997;103:491–49795. Inzucchi SE, Lipska KJ, Mayo H, Bailey CJ,McGuire DK. Metformin in patients with type2 diabetes and kidney disease: a systematicreview. JAMA 2014;312:2668–267596. Lalau J-D, Kajbaf F, Bennis Y, Hurtel-LemaireAS,BelpaireF,DeBroeME.Metformin treatmentin patients with type 2 diabetes and chronickidney disease stages 3A, 3B, or 4. Diabetes Care2018;41:547–55397. Imam TH. Changes in metformin use inchronic kidney disease. Clin Kidney J 2017;10:301–30498. UK Prospective Diabetes Study (UKPDS)Group. Effect of intensive blood-glucose controlwith metformin on complications in overweightpatients with type 2 diabetes (UKPDS 34). Lancet1998;352:854–86599. Griffin SJ, Leaver JK, Irving GJ. Impact ofmetformin on cardiovascular disease: a meta-analysis of randomised trials among peoplewith type 2 diabetes. Diabetologia 2017;60:1620–1629100. Maruthur NM, Tseng E, Hutfless S, et al.Diabetes medications as monotherapy ormetformin-based combination therapy for type 2diabetes: a systematic review and meta-analysis.Ann Intern Med 2016;164:740–751101. Aroda VR, Edelstein SL, Goldberg RB, et al.;Diabetes Prevention Program Research Group.Long-term metformin use and vitamin B12 de-ficiency in the Diabetes Prevention ProgramOutcomes Study. J Clin Endocrinol Metab 2016;101:1754–1761102. Zhang X-L, Zhu Q-Q, Chen Y-H, et al. Car-diovascular safety, long-term noncardiovascularsafety, and efficacy of sodium-glucose cotrans-porter 2 inhibitors in patients with type 2diabetes mellitus: a systemic review and meta-analysis with trial sequential analysis. J Am HeartAssoc 2018;7:e007165103. Storgaard H, Gluud LL, Bennett C, et al.Benefits and harms of sodium-glucose co-transporter 2 inhibitors in patients with type 2
care.diabetesjournals.org Davies and Associates 29

diabetes: a systematic review and meta-analysis.PLoS One 2016;11:e0166125104. LiD,WangT, ShenS, Fang Z,DongY, TangH.Urinary tract and genital infections in patientswith type 2 diabetes treated with sodium-glucoseco-transporter 2 inhibitors: a meta-analysis ofrandomized controlled trials. Diabetes ObesMetab 2017;19:348–355105. Jabbour S, Seufert J, Scheen A, Bailey CJ,Karup C, Langkilde AM. Dapagliflozin in patientswith type 2 diabetes mellitus: a pooled analysisof safety data from phase IIb/III clinical trials.Diabetes Obes Metab 2018;20:620–628106. TangH, LiD,WangT, Zhai S, SongY. Effectofsodium-glucose cotransporter 2 inhibitors on di-abetic ketoacidosis among patients with type 2diabetes: a meta-analysis of randomized con-trolled trials. Diabetes Care 2016;39:e123–e124107. Thrasher J. Pharmacologic managementof type 2 diabetes mellitus: available therapies.Am J Med 2017;130(6S):S4–S17108. Karagiannis T, Liakos A, Bekiari E, et al.Efficacy and safety of once-weekly glucagon-likepeptide 1 receptor agonists for themanagementof type2diabetes: a systematic reviewandmeta-analysis of randomized controlled trials. Diabe-tes Obes Metab 2015;17:1065–1074109. Zaccardi F, Htike ZZ, Webb DR, Khunti K,Davies MJ. Benefits and harms of once-weeklyglucagon-like peptide-1 receptor agonist treat-ments: a systematic review and network meta-analysis. Ann Intern Med 2016;164:102–113110. Htike ZZ, Zaccardi F, Papamargaritis D,Webb DR, Khunti K, Davies MJ. Efficacy andsafety of glucagon-like peptide-1 receptor ago-nists in type 2 diabetes: a systematic review andmixed-treatment comparison analysis. DiabetesObes Metab 2017;19:524–536111. Sorli C, Harashima S-I, Tsoukas GM, et al.Efficacy and safety of once-weekly semaglutidemonotherapy versus placebo in patients withtype 2 diabetes (SUSTAIN 1): a double-blind,randomised, placebo-controlled, parallel-group,multinational, multicentre phase 3a trial. LancetDiabetes Endocrinol 2017;5:251–260112. Pratley RE, Aroda VR, Lingvay I, et al.;SUSTAIN 7 investigators. Semaglutide versusdulaglutide once weekly in patients with type 2diabetes (SUSTAIN 7): a randomised, open-label,phase 3b trial. LancetDiabetes Endocrinol 2018;6:275–286113. Dungan KM, Povedano ST, Forst T, et al.Once-weekly dulaglutide versus once-daily lira-glutide inmetformin-treatedpatientswith type2diabetes (AWARD-6): a randomised, open-label,phase 3, non-inferiority trial. Lancet 2014;384:1349–1357114. Buse JB, Nauck M, Forst T, et al. Exenatideonce weekly versus liraglutide once daily inpatients with type 2 diabetes (DURATION-6):a randomised, open-label study. Lancet 2013;381:117–124115. Buse JB, Rosenstock J, Sesti G, et al.; LEAD-6Study Group. Liraglutide once a day versusexenatide twice a day for type 2 diabetes: a26-week randomised, parallel-group, multina-tional, open-label trial (LEAD-6). Lancet 2009;374:39–47116. Drucker DJ, Buse JB, Taylor K, et al.;DURATION-1 Study Group. Exenatide onceweekly versus twice daily for the treatment of
type 2 diabetes: a randomised, open-label, non-inferiority study. Lancet 2008;372:1240–1250117. Andreadis P, Karagiannis T, Malandris K,et al. Semaglutide for type 2 diabetes mellitus: asystematic review and meta-analysis. DiabetesObes Metab 2018;20:2255–2263118. Li Z, Zhang Y, Quan X, et al. Efficacy andacceptability of glycemic control of glucagon-likepeptide-1 receptor agonists among type 2 di-abetes: a systematic review and network meta-analysis. PLoS One 2016;11:e0154206119. Storgaard H, Cold F, Gluud LL, Vilsbøll T,Knop FK. Glucagon-like peptide-1 receptor ago-nists and risk of acute pancreatitis in patientswith type2diabetes. DiabetesObesMetab2017;19:906–908120. MonamiM, Nreu B, Scatena A, et al. Safetyissues with glucagon-like peptide-1 receptoragonists (pancreatitis, pancreatic cancer andcholelithiasis): data from randomized controlledtrials. Diabetes Obes Metab 2017;19:1233–1241121. Esposito K, Chiodini P, Maiorino MI,Bellastella G, Capuano A, Giugliano D. Glycaemicdurability with dipeptidyl peptidase-4 inhibi-tors in type 2 diabetes: a systematic review andmeta-analysis of long-term randomised controlledtrials. BMJ Open 2014;4:e005442122. Aroda VR, Henry RR, Han J, et al. Efficacy ofGLP-1 receptor agonists and DPP-4 inhibitors:meta-analysis and systematic review. Clin Ther2012;34:1247–1258.e22123. Wu S, Chai S, Yang J, et al. Gastrointestinaladverse events of dipeptidyl peptidase 4 inhib-itors in type 2 diabetes: a systematic review andnetwork meta-analysis. Clin Ther 2017;39:1780–1789.e33124. Salvo F,MooreN, ArnaudM, et al. Additionof dipeptidyl peptidase-4 inhibitors to sulpho-nylureas and risk of hypoglycaemia: systematicreview and meta-analysis. BMJ 2016;353:i2231125. Tkac I, Raz I. Combined analysis of threelarge interventional trials with gliptins indicatesincreased incidence of acute pancreatitis inpatients with type 2 diabetes. Diabetes Care2017;40:284–286126. Mascolo A, Rafaniello C, Sportiello L, et al.Dipeptidyl peptidase (DPP)-4 inhibitor-inducedarthritis/arthralgia: a review of clinical cases.Drug Saf 2016;39:401–407127. Nauck MA, Meier JJ, Cavender MA, Abd ElAziz M, Drucker DJ. Cardiovascular actions andclinical outcomes with glucagon-like peptide-1receptor agonists and dipeptidyl peptidase-4inhibitors. Circulation 2017;136:849–870128. Li L, Li S, Deng K, et al. Dipeptidyl peptidase-4 inhibitors and risk of heart failure in type 2diabetes: systematic review and meta-analysisof randomised and observational studies. BMJ2016;352:i610129. Aronoff S, Rosenblatt S, Braithwaite S, EganJW, Mathisen AL, Schneider RL. Pioglitazonehydrochloride monotherapy improves glycemiccontrol in the treatment of patients with type 2diabetes: a 6-month randomized placebo-controlled dose-response study. The Pioglita-zone 001 Study Group. Diabetes Care 2000;23:1605–1611130. Einhorn D, Rendell M, Rosenzweig J, EganJW, Mathisen AL, Schneider RL. Pioglitazonehydrochloride in combination with metforminin the treatment of type 2 diabetes mellitus:a randomized, placebo-controlled study. The
Pioglitazone 027 Study Group. Clin Ther 2000;22:1395–1409131. Yki-Jarvinen H. Thiazolidinediones. N Engl JMed 2004;351:1106–1118132. KernanWN, Viscoli CM, Furie KL, et al.; IRISTrial Investigators. Pioglitazone after ischemicstroke or transient ischemic attack. N Engl J Med2016;374:1321–1331133. HanefeldM,Marx N, Pfutzner A, et al. Anti-inflammatory effects of pioglitazone and/or sim-vastatin in high cardiovascular risk patients withelevated high sensitivity C-reactive protein: thePIOSTAT Study. J Am Coll Cardiol 2007;49:290–297134. SaremiA, SchwenkeDC,BuchananTA, et al.Pioglitazone slows progression of atherosclero-sis in prediabetes independent of changes incardiovascular risk factors. Arterioscler ThrombVasc Biol 2013;33:393–399135. Nissen SE, Nicholls SJ, Wolski K, et al.;PERISCOPE Investigators. Comparison of pioglita-zone vs glimepiride on progression of coronaryatherosclerosis in patients with type 2 diabetes:the PERISCOPE randomized controlled trial. JAMA2008;299:1561–1573136. Dormandy JA, Charbonnel B, Eckland DJA,et al.; PROactive Investigators. Secondary pre-vention of macrovascular events in patientswith type 2 diabetes in the PROactive Study(PROspective pioglitAzoneClinical Trial Inmacro-Vascular Events): a randomised controlled trial.Lancet 2005;366:1279–1289137. BachRG,BrooksMM,LombarderoM,et al.;BARI 2D Investigators. Rosiglitazone and out-comes for patients with diabetes mellitus andcoronaryarterydisease in theBypassAngioplastyRevascularization Investigation 2 Diabetes (BARI2D) trial. Circulation 2013;128:785–794138. Mahaffey KW, Hafley G, Dickerson S, et al.Results of a reevaluation of cardiovascular out-comes in the RECORD trial. AmHeart J 2013;166:240–249.e1139. Cusi K, Orsak B, Bril F, et al. Long-termpioglitazone treatment for patients with non-alcoholic steatohepatitis and prediabetes ortype 2 diabetes mellitus: a randomized trial.Ann Intern Med 2016;165:305–315140. Kahn SE, Haffner SM, Heise MA, et al.;ADOPT Study Group. Glycemic durability ofrosiglitazone, metformin, or glyburide mono-therapy. N Engl J Med 2006;355:2427–2443141. Home PD, Pocock SJ, Beck-Nielsen H, et al.;RECORD Study Team. Rosiglitazone evaluatedfor cardiovascular outcomes in oral agent com-bination therapy for type 2 diabetes (RECORD):a multicentre, randomised, open-label trial. Lan-cet 2009;373:2125–2135 [Lond Engl]142. Hanefeld M, Brunetti P, Schernthaner GH,Matthews DR, Charbonnel BH; QUARTET StudyGroup. One-year glycemic control with a sulfo-nylurea plus pioglitazone versus a sulfonylureaplus metformin in patients with type 2 diabetes.Diabetes Care 2004;27:141–147143. Viscoli CM, Inzucchi SE, Young LH, et al.; IRISTrial Investigators. Pioglitazone and risk forbone fracture: safety data from a randomizedclinical trial. J Clin Endocrinol Metab 2017;102:914–922144. Kahn SE, Zinman B, Lachin JM, et al.;Diabetes Outcome Progression Trial (ADOPT)Study Group. Rosiglitazone-associated fracturesin type 2 diabetes: an analysis from A Diabetes
30 Consensus Report Diabetes Care

Outcome Progression Trial (ADOPT). DiabetesCare 2008;31:845–851145. Lewis JD, Habel LA, Quesenberry CP, et al.Pioglitazone use and risk of bladder cancer andother common cancers in persons with diabetes.JAMA 2015;314:265–277146. Hirst JA, Farmer AJ, Dyar A, Lung TW,Stevens RJ. Estimating the effect of sulfonylureaon HbA1c in diabetes: a systematic review andmeta-analysis. Diabetologia 2013;56:973–984147. UK Prospective Diabetes Study (UKPDS)Group. Intensive blood-glucose control withsulphonylureas or insulin compared with con-ventional treatment and risk of complications inpatients with type 2 diabetes (UKPDS 33). Lancet1998;352:837–853148. Patel A, MacMahon S, Chalmers J, et al.;ADVANCE Collaborative Group. Intensive bloodglucose control and vascular outcomes in pa-tients with type 2 diabetes. N Engl J Med 2008;358:2560–2572149. Monami M, Dicembrini I, Kundisova L,Zannoni S, Nreu B, Mannucci E. A meta-analysisof the hypoglycaemic risk in randomized con-trolled trials with sulphonylureas in patients withtype 2 diabetes. Diabetes Obes Metab 2014;16:833–840150. Del Prato S, Camisasca R, Wilson C, Fleck P.Durability of the efficacy and safety of alogliptincompared with glipizide in type 2 diabetesmellitus: a 2-year study. Diabetes Obes Metab2014;16:1239–1246151. Mishriky BM, Cummings DM, TanenbergRJ. The efficacy and safety of DPP4 inhibitorscompared to sulfonylureas as add-on therapy tometformin in patients with type 2 diabetes: asystematic review and meta-analysis. DiabetesRes Clin Pract 2015;109:378–388152. Khunti K,ChatterjeeS,GersteinHC,et al.Dosulphonylureas still have a place in clinical prac-tice? Lancet Diabetes Endocrinol 2018;Feb 28:pii:S2213-8587(18)30025-1153. Gangji AS, Cukierman T, Gerstein HC,Goldsmith CH, Clase CM. A systematic reviewand meta-analysis of hypoglycemia and cardio-vascular events: a comparison of glyburide withother secretagogues and with insulin. DiabetesCare 2007;30:389–394154. Chan SP, Colagiuri S. Systematic review andmeta-analysis of the efficacy and hypoglycemicsafety of gliclazide versus other insulinotropicagents. Diabetes Res Clin Pract 2015;110:75–81155. Holman RR, Paul SK, Bethel MA, MatthewsDR, Neil HA. 10-year follow-up of intensiveglucose control in type 2 diabetes. N Engl JMed 2008;359:1577–1589156. Erpeldinger S, Rehman MB, Berkhout C,et al. Efficacy and safety of insulin in type 2diabetes: meta-analysis of randomised con-trolled trials. BMC Endocr Disord 2016;16:39157. OwensDR, Traylor L,Mullins P, LandgrafW.Patient-level meta-analysis of efficacy and hy-poglycaemia in people with type 2 diabetesinitiating insulin glargine 100U/mL or neutralprotamine Hagedorn insulin analysed accordingto concomitant oral antidiabetes therapy. Di-abetes Res Clin Pract 2017;124:57–65158. Goldman J, Kapitza C, Pettus J, Heise T.Understanding how pharmacokinetic and phar-macodynamic differences of basal analog insulinsinfluence clinical practice. Curr Med Res Opin2017;33:1821–1831
159. Freemantle N, Chou E, Frois C, et al. Safetyand efficacy of insulin glargine 300 u/mL com-pared with other basal insulin therapies in pa-tients with type 2 diabetes mellitus: a networkmeta-analysis. BMJ Open 2016;6:e009421160. Russell-Jones D, Gall M-A, Niemeyer M,Diamant M, Del Prato S. Insulin degludec resultsin lower rates of nocturnal hypoglycaemia andfasting plasma glucose vs. insulin glargine: ameta-analysis of seven clinical trials. Nutr MetabCardiovasc Dis 2015;25:898–905161. LipskaKJ, ParkerMM,MoffetHH,HuangES,Karter AJ. Association of initiation of basal insulinanalogs vs neutral protamine hagedorn insulinwith hypoglycemia-related emergency depart-ment visits or hospital admissions and withglycemic control in patientswith type 2 diabetes.JAMA 2018;320:53–62162. Marso SP, McGuire DK, Zinman B, et al.;DEVOTE Study Group. Efficacy and safety ofdegludec versus glargine in type 2 diabetes. NEngl J Med 2017;377:723–732163. Rosenstock J,HollanderP,BhargavaA, et al.Similar efficacy and safety of LY2963016 insulinglargine and insulin glargine (Lantus�) in pa-tients with type 2 diabetes who were insulin-naıve or previously treated with insulin glargine:a randomized, double-blind controlled trial (theELEMENT 2 study). Diabetes Obes Metab 2015;17:734–741164. Gerstein HC, Bosch J, Dagenais GR, et al.;ORIGIN Trial Investigators. Basal insulin andcardiovascular and other outcomes in dysglyce-mia. N Engl J Med 2012;367:319–328165. Riddle MC, Yki-Jarvinen H, Bolli GB, et al.One-year sustained glycaemic control and lesshypoglycaemia with new insulin glargine 300 U/mlcompared with 100 U/ml in people with type 2diabetes using basal plus meal-time insulin: theEDITION 1 12-month randomized trial, including6-month extension. Diabetes Obes Metab 2015;17:835–842166. Yki-Jarvinen H, Bergenstal R, Ziemen M,et al.; EDITION 2 Study Investigators. New insulinglargine 300 units/mL versus glargine 100 units/mLin people with type 2 diabetes using oralagents and basal insulin: glucose control andhypoglycemia in a 6-month randomized con-trolled trial (EDITION 2). Diabetes Care 2014;37:3235–3243167. Riddle MC, Bolli GB, Ziemen M, Muehlen-Bartmer I, Bizet F, Home PD; EDITION 1 StudyInvestigators. New insulin glargine 300 units/mLversus glargine 100 units/mL in people withtype 2 diabetes using basal andmealtime insulin:glucose control and hypoglycemia in a 6-monthrandomized controlled trial (EDITION 1). Diabe-tes Care 2014;37:2755–2762168. Khunti K, Damci T, Husemoen LL, Babu V,Liebl A. Exploring the characteristics of subopti-mally controlled patients after 24 weeks of basalinsulin treatment: an individualized approach tointensification. Diabetes Res Clin Pract 2017;123:209–217169. Jensen MD, Ryan DH, Apovian CM, et al.;American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines;Obesity Society. 2013 AHA/ACC/TOS guidelinefor the management of overweight and obesityin adults: a report of the American College ofCardiology/American Heart Association TaskForce on Practice Guidelines and The Obesity
Society. J AmColl Cardiol 2014;63(25Pt B):2985–3023170. Garvey WT, Mechanick JI, Brett EM, et al.;Reviewers of the AACE/ACE Obesity ClinicalPractice Guidelines. American Association ofClinical Endocrinologists and American Collegeof Endocrinology Comprehensive Clinical Prac-tice Guidelines for Medical Care of Patients withObesity. Endocr Pract 2016;22(Suppl. 3):1–203171. Apovian CM, Aronne LJ, Bessesen DH,et al.; Endocrine Society. Pharmacological man-agement of obesity: an Endocrine Society clinicalpractice guideline. J Clin EndocrinolMetab 2015;100:342–362172. Moyer VA; U.S. Preventive Services TaskForce. Screening for andmanagement of obesityin adults: U.S. Preventive Services Task Forcerecommendation statement. Ann Intern Med2012;157:373–378173. Van Gaal L, Dirinck E. Pharmacologicalapproaches in the treatment and maintenanceof weight loss. Diabetes Care 2016;39(Suppl. 2):S260–S267174. KheraR,PandeyA,ChandarAK,etal. Effectsof weight-loss medications on cardiometabolicrisk profiles: a systematic review and networkmeta-analysis. Gastroenterology 2018;154:1309–1319.e7175. Davies MJ, Bergenstal R, Bode B, et al.;NN8022-1922StudyGroup. Efficacy of liraglutidefor weight loss among patients with type 2diabetes: the SCALE diabetes randomized clinicaltrial. JAMA 2015;314:687–699176. Schauer PR, Bhatt DL, Kirwan JP, et al.;STAMPEDE Investigators. Bariatric surgery versusintensive medical therapy for diabetesd3-yearoutcomes. N Engl J Med 2014;370:2002–2013177. Schauer PR, Bhatt DL, Kirwan JP, et al.;STAMPEDE Investigators. Bariatric surgery ver-sus intensive medical therapy for diabetesd5-year outcomes. N Engl J Med 2017;376:641–651178. Ikramuddin S, Korner J, Lee W-J, et al.Lifestyle intervention and medical managementwith vs without Roux-en-Y gastric bypass andcontrol of hemoglobin A1c, LDL cholesterol, andsystolic blood pressure at 5 years in the diabetessurgery study. JAMA 2018;319:266–278179. Dixon JB,O’Brien PE, Playfair J, et al. Adjust-able gastric banding and conventional therapyfor type2diabetes: a randomizedcontrolled trial.JAMA 2008;299:316–323180. MingroneG, Panunzi S, DeGaetanoA, et al.Bariatric surgery versus conventional medicaltherapy for type 2 diabetes. N Engl J Med2012;366:1577–1585181. Sjostrom L, Peltonen M, Jacobson P, et al.Association of bariatric surgery with long-termremission of type 2 diabetes and with microvas-cular and macrovascular complications. JAMA2014;311:2297–2304182. MingroneG, Panunzi S, DeGaetanoA, et al.Bariatric-metabolic surgery versus conventionalmedical treatment in obese patients with type 2diabetes: 5 year follow-up of an open-label,single-centre, randomised controlled trial. Lan-cet 2015;386:964–973183. Rubino F, Nathan DM, Eckel RH, et al.;Delegates of the 2nd Diabetes Surgery Summit.Metabolic surgery in the treatment algorithmfor type 2 diabetes: a joint statement by inter-national diabetes organizations. Diabetes Care2016;39:861–877
care.diabetesjournals.org Davies and Associates 31

184. Maggard-Gibbons M, Maglione M, LivhitsM, et al. Bariatric surgery for weight loss andglycemic control in nonmorbidly obese adultswith diabetes: a systematic review. JAMA 2013;309:2250–2261185. Mingrone G, Bornstein S, Le Roux CW.Optimisation of follow-up after metabolic sur-gery. Lancet Diabetes Endocrinol 2018;6:487–499186. Conason A, Teixeira J, Hsu C-H, Puma L,Knafo D, Geliebter A. Substance use followingbariatric weight loss surgery. JAMA Surg 2013;148:145–150187. Dawes AJ, Maggard-GibbonsM,Maher AR,et al. Mental health conditions among patientsseeking and undergoing bariatric surgery: ameta-analysis. JAMA 2016;315:150–163188. Mechanick JI, Kushner RF, Sugerman HJ,et al. (2009) American Association of ClinicalEndocrinologists, TheObesity Society, andAmer-ican Society for Metabolic & Bariatric Surgerymedical guidelines for clinical practice for theperioperative nutritional, metabolic, and non-surgical support of the bariatric surgery patient.Obesity (Silver Spring) 2009;17(Suppl. 1):S1–S70,v189. Mechanick JI, Youdim A, Jones DB, et al.(2013) Clinical practice guidelines for the peri-operativenutritional,metabolic, andnonsurgicalsupport of the bariatric surgery patient–2013update: cosponsored by AmericanAssociation ofClinical Endocrinologists, The Obesity Society,and American Society for Metabolic & BariatricSurgery. Obesity (Silver Spring) 2013;21(Suppl.1):S1–S27190. PhungOJ, Sobieraj DM, Engel SS, RajpathakSN. Early combination therapy for the treatmentof type 2 diabetes mellitus: systematic reviewand meta-analysis. Diabetes Obes Metab 2014;16:410–417191. Abdul-Ghani MA, Puckett C, Triplitt C, et al.Initial combination therapy with metformin,pioglitazone and exenatide is more effectivethan sequential add-on therapy in subjects withnew-onset diabetes. Results from the Efficacy andDurability of Initial CombinationTherapy for Type2Diabetes (EDICT): a randomized trial. DiabetesObes Metab 2015;17:268–275192. Vijayakumar TM, Jayram J, MeghanaCheekireddy V, Himaja D, Dharma Teja Y,Narayanasamy D. Safety, efficacy, and bioavail-ability of fixed-dose combinations in type 2 di-abetes mellitus: a systematic updated review.Curr Ther Res Clin Exp 2017;84:4–9193. Mearns ES, SaulsberryWJ,White CM, et al.Efficacy and safety of antihyperglycaemic drugregimensadded tometforminandsulphonylureatherapy in type 2 diabetes: a network meta-analysis. Diabet Med 2015;32:1530–1540194. Henry RR, Murray AV, Marmolejo MH,Hennicken D, Ptaszynska A, List JF. Dapagliflozin,metformin XR, or both: initial pharmacother-apy for type 2 diabetes, a randomised controlledtrial. Int J Clin Pract 2012;66:446–456195. Buse JB, Peters A, Russell-Jones D, et al. Isinsulin the most effective injectable antihyper-glycaemic therapy? Diabetes Obes Metab 2015;17:145–151196. Vaccaro O, Masulli M, Nicolucci A, et al.;Thiazolidinediones Or Sulfonylureas Cardiovas-cular Accidents Intervention Trial (TOSCA.IT)study group; Italian Diabetes Society. Effects
on the incidence of cardiovascular events ofthe addition of pioglitazone versus sulfonylureasin patients with type 2 diabetes inadequatelycontrolled with metformin (TOSCA.IT): a rando-mised, multicentre trial. Lancet Diabetes Endo-crinol 2017;5:887–897197. Wang Z, Sun J, Han R, et al. Efficacy andsafety of sodium-glucose cotransporter-2 inhib-itors versus dipeptidyl peptidase-4 inhibitors asmonotherapy or add-on tometformin in patientswith type 2 diabetes mellitus: a systematic re-view and meta-analysis. Diabetes Obes Metab2018;20:113–120198. Kawalec P, Mikrut A, Łopuch S. The safetyof dipeptidyl peptidase-4 (DPP-4) inhibitors orsodium-glucose cotransporter 2 (SGLT-2) inhib-itors added to metformin background therapyin patients with type 2 diabetes mellitus: a sys-tematic reviewandmeta-analysis. DiabetesMetabRes Rev 2014;30:269–283199. Leiter LA, Yoon K-H, Arias P, et al. Canagli-flozin provides durable glycemic improvementsand body weight reduction over 104 weeksversus glimepiride in patients with type 2 di-abetes on metformin: a randomized, double-blind, phase 3 study. Diabetes Care 2015;38:355–364200. Del Prato S, NauckM, Duran-Garcia S, et al.Long-term glycaemic response and tolerabilityof dapagliflozin versus a sulphonylurea as add-on therapy to metformin in patients with type 2diabetes: 4-year data. Diabetes Obes Metab2015;17:581–590201. Ridderstrale M, Andersen KR, Zeller C, KimG,Woerle HJ, Broedl UC; EMPA-REGH2H-SU trialinvestigators. Comparison of empagliflozin andglimepiride as add-on to metformin in patientswith type 2 diabetes: a 104-week andomized,active-controlled, double-blind, phase 3 trial.Lancet Diabetes Endocrinol 2014;2:691–700202. Zhang Y, Hong J, Chi J, GuW, Ning G, WangW. Head-to-head comparison of dipeptidylpeptidase-IV inhibitors and sulfonylureas – ameta-analysis from randomized clinical trials.Diabetes Metab Res Rev 2014;30:241–256203. Foroutan N, Muratov S, Levine M. Safetyand efficacy of dipeptidyl peptidase-4 inhibitorsvs sulfonylurea inmetformin-based combinationtherapy for type 2 diabetes mellitus: systematicreview and meta-analysis. Clin Invest Med 2016;39:E48–E62204. Chen K, Kang D, Yu M, et al. Direct head-to-head comparison of glycaemic durability ofdipeptidyl peptidase-4 inhibitors and sulphonyl-ureas in patients with type 2 diabetes mellitus: ameta-analysis of long-term randomized controlledtrials. Diabetes Obes Metab 2018;20:1029–1033205. Zaccardi F, Dhalwani NN, Dales J, et al.Comparison of glucose-lowering agents afterdual therapy failure in type 2 diabetes: a sys-tematic review and network meta-analysis ofrandomized controlled trials. Diabetes ObesMetab 2018;20:985–997206. Downes MJ, Bettington EK, Gunton JE,Turkstra E. Triple therapy in type 2 diabetes;a systematic review and network meta-analysis.PeerJ 2015;3:e1461207. Lee CMY, Woodward M, Colagiuri S. Tripletherapy combinations for the treatment of type2 diabetes – a network meta-analysis. DiabetesRes Clin Pract 2016;116:149–158
208. LukashevichV,DelPratoS,AragaM,KothnyW. Efficacy and safety of vildagliptin in patientswith type 2 diabetes mellitus inadequately con-trolled with dual combination of metformin andsulphonylurea. Diabetes Obes Metab 2014;16:403–409209. Hong AR, Lee J, Ku EJ, et al. Comparison ofvildagliptin as an add-on therapy and sulfonyl-urea dose-increasing therapy in patients withinadequately controlled type 2 diabetes usingmetformin and sulfonylurea (VISUAL study): arandomized trial. Diabetes Res Clin Pract 2015;109:141–148210. Moses RG, Kalra S, Brook D, et al. Arandomized controlled trial of the efficacy andsafety of saxagliptin as add-on therapy in patientswith type 2 diabetes and inadequate glycaemiccontrol on metformin plus a sulphonylurea. Di-abetes Obes Metab 2014;16:443–450211. Moses RG, Round E, Shentu Y, et al. Arandomized clinical trial evaluating the safetyand efficacy of sitagliptin added to the combi-nation of sulfonylurea andmetformin in patientswith type 2 diabetes mellitus and inadequateglycemic control. J Diabetes 2016;8:701–711212. Singh S, Wright EE Jr, Kwan AYM, et al.Glucagon-like peptide-1 receptor agonists com-pared with basal insulins for the treatment oftype 2 diabetesmellitus: a systematic review andmeta-analysis. Diabetes Obes Metab 2017;19:228–238213. Levin PA, Nguyen H, Wittbrodt ET, Kim SC.Glucagon-like peptide-1 receptor agonists: asystematic review of comparative effectivenessresearch. Diabetes Metab Syndr Obes 2017;10:123–139214. Abd El Aziz MS, Kahle M, Meier JJ, NauckMA. A meta-analysis comparing clinical effectsof short- or long-acting GLP-1 receptor agonistsversus insulin treatment from head-to-headstudies in type 2 diabetic patients. DiabetesObes Metab 2017;19:216–227215. Eng C, Kramer CK, Zinman B, Retnakaran R.Glucagon-like peptide-1 receptor agonist andbasal insulin combination treatment for themanagement of type 2 diabetes: a systematicreview and meta-analysis. Lancet 2014;384:2228–2234216. ArodaVR, Bailey TS, CariouB, et al. Effect ofadding insulin degludec to treatment in patientswith type 2 diabetes inadequately controlledwith metformin and liraglutide: a double-blindrandomized controlled trial (BEGIN: ADD TO GLP-1Study). Diabetes Obes Metab 2016;18:663–670217. Aschner P, Sethi B, Gomez-Peralta F, et al.Insulin glargine compared with premixed insulinfor management of insulin-naıve type 2 diabetespatients uncontrolled on oral antidiabetic drugs:the open-label, randomized GALAPAGOS study.J Diabetes Complications 2015;29:838–845218. Rosenstock J, Fonseca V, Schinzel S, DainMP, Mullins P, Riddle M. Reduced risk of hypo-glycemia with once-daily glargine versus twice-daily NPH and number needed to harmwith NPHto demonstrate the risk of one additional hypo-glycemic event in type 2 diabetes: evidencefrom a long-term controlled trial. J DiabetesComplications 2014;28:742–749219. Tang H, Cui W, Li D, et al. Sodium-glucose co-transporter 2 inhibitors in addi-tion to insulin therapy for management oftype 2 diabetes mellitus: a meta-analysis of
32 Consensus Report Diabetes Care

randomized controlled trials. Diabetes ObesMetab 2017;19:142–147220. Rosenstock J, Jelaska A, Zeller C, Kim G,Broedl UC, Woerle HJ; EMPA-REG BASALTM trialinvestigators. Impact of empagliflozin added onto basal insulin in type 2 diabetes inadequatelycontrolled on basal insulin: a 78-week random-ized, double-blind, placebo-controlled trial. Di-abetes Obes Metab 2015;17:936–948221. Rosenstock J, Jelaska A, Frappin G, et al.;EMPA-REG MDI Trial Investigators. Improvedglucose control with weight loss, lower insulindoses, and no increased hypoglycemia withempagliflozin added to titrated multiple dailyinjections of insulin in obese inadequately con-trolled type 2 diabetes. Diabetes Care 2014;37:1815–1823222. Yang W, Cai X, Gao X, Chen Y, Chen L, Ji L.Addition of dipeptidyl peptidase-4 inhibitors toinsulin treatment in type 2 diabetes patients: ameta-analysis. J Diabetes Investig 2018;9:813–821223. Min SH, Yoon J-H, Hahn S, Cho YM. Com-parison between SGLT2 inhibitors and DPP4inhibitors added to insulin therapy in type 2diabetes: a systematic review with indirect com-parison meta-analysis: SGLT2 or DPP4 inhibitorwith insulin. Diabetes Metab Res Rev 2017;33:e2818224. Wysham CH, Lin J, Kuritzky L. Safety andefficacy of a glucagon-like peptide-1 receptoragonist added to basal insulin therapy versusbasal insulin with or without a rapid-acting in-sulin in patients with type 2 diabetes: resultsof a meta-analysis. Postgrad Med 2017;129:436–445225. Maiorino MI, Chiodini P, Bellastella G,Capuano A, Esposito K, Giugliano D. Insulinand glucagon-like peptide 1 receptor agonistcombination therapy in type 2 diabetes: a sys-tematic review andmeta-analysis of randomizedcontrolled trials.DiabetesCare2017;40:614–624
226. Gough SCL, Bode BW, Woo VC, et al. One-year efficacy and safety of a fixed combination ofinsulin degludec and liraglutide in patients withtype 2 diabetes: results of a 26-week extensionto a 26-week main trial. Diabetes Obes Metab2015;17:965–973227. Rosenstock J, Aronson R, Grunberger G,et al.; LixiLan-O Trial Investigators. Benefits ofLixiLan, a titratable fixed-ratio combination ofinsulin glargine plus lixisenatide, versus insulinglargine and lixisenatide monocomponents intype 2 diabetes inadequately controlled on oralagents: the LixiLan-O randomized trial. DiabetesCare 2016;39:2026–2035228. Aroda VR, Rosenstock J, Wysham C, et al.;LixiLan-L Trial Investigators. Efficacy and safety ofLixiLan, a titratable fixed-ratio combination ofinsulin glargine plus lixisenatide in type 2 di-abetes inadequately controlled on basal insulinand metformin: the LixiLan-L randomized trial.Diabetes Care 2016;39:1972–1980229. Garber AJ, Wahlen J, Wahl T, et al. Attain-ment of glycaemic goals in type 2 diabetes withonce-, twice-, or thrice-daily dosingwith biphasicinsulin aspart 70/30 (the 1-2-3 study). DiabetesObes Metab 2006;8:58–66230. Linjawi S, Lee B-W, Tabak O, Lovdahl S,Werther S, Abusnana S. A 32-week randomizedcomparison of stepwise insulin intensification ofbiphasic insulin aspart (BIAsp30) versus basal-bolustherapy in insulin-naıve patients with type 2 di-abetes. Diabetes Ther 2018;9:1–11231. Raccah D, Huet D, Dib A, et al. Review ofbasal-plus insulin regimen options for simplerinsulin intensification in people with type 2 di-abetesmellitus. DiabetMed2017;34:1193–1204232. Rodbard HW, Visco VE, Andersen H, HiortLC, Shu DH. Treatment intensification with step-wise addition of prandial insulin aspart bolusescomparedwith full basal-bolus therapy (FullSTEPStudy): a randomised, treat-to-target clinicaltrial. Lancet Diabetes Endocrinol 2014;2:30–37
233. Giugliano D, Chiodini P, Maiorino MI,Bellastella G, Esposito K. Intensification of insulintherapy with basal-bolus or premixed insulinregimens in type 2 diabetes: a systematic reviewand meta-analysis of randomized controlledtrials. Endocrine 2016;51:417–428234. Wang C, Mamza J, Idris I. Biphasic vs basalbolus insulin regimen in type 2 diabetes: asystematic review and meta-analysis of random-ized controlled trials. Diabet Med 2015;32:585–594235. AnyanwaguU,Mamza J,Gordon J,DonnellyR, Idris I. Premixed vs basal-bolus insulin regimenin type 2 diabetes: comparison of clinical out-comes from randomized controlled trials andreal-world data.DiabetMed2017;34:1728–1736236. Aronson R, Reznik Y, Conget I, et al.; OpT2-mise Study Group. Sustained efficacy of insulinpump therapy compared with multiple dailyinjections in type 2 diabetes: 12-month datafrom the OpT2mise randomized trial. DiabetesObes Metab 2016;18:500–507237. Kelly S,Martin S, Kuhn I, CowanA, BrayneC,Lafortune L. Barriers and facilitators to theuptake and maintenance of healthy behavioursby people at mid-life: a rapid systematic review.PLoS One 2016;11:e0145074238. Gee PM, Greenwood DA, Paterniti DA,Ward D, Miller LM. The eHealth EnhancedChronic Care Model: a theory derivation ap-proach. J Med Internet Res 2015;17:e86239. Faruque LI, Wiebe N, Ehteshami-Afshar A,et al.; Alberta Kidney Disease Network. Effect oftelemedicine on glycated hemoglobin in di-abetes: a systematic review and meta-analysisof randomized trials. CMAJ 2017;189:E341–E364240. Lee SWH,ChanCKY, Chua SS, ChaiyakunaprukN. Comparative effectiveness of telemedicinestrategies on type 2 diabetes management: asystematic review and network meta-analysis.Sci Rep 2017;7:12680
care.diabetesjournals.org Davies and Associates 33