management of post-mortem examinations
TRANSCRIPT

Tayside Acute Services Division
Local Report ~ February 2005
Management of Post-mortem Examinations
Local Report ~ February 2005
Management of Post-mortem Examinations
The purpose of a post-mortem examination is to determine the cause of death. Post-mortem examination also serves the public by providing information leading to further medical advances. Developing patient care depends on learning as much as we can from the health of others by comparing the findings from the various tests carried out in life with the actual findings after death. This information is important in: assessing and improving the quality of medical care; research into the nature, causes and prevention of disease; and medical education. It is also important for public health planning, by providing facts and figures as to why and how people have died, and what they have died from.
The Management of Post-mortem Examinations Project Group has developed five standards covering the key elements of care after death in terms of the hospital post-mortem examination process. This report presents the findings from the peer review of performance against the standards.
© NHS Quality Improvement Scotland 2005
ISBN 1-84404-231-6
First published February 2005
NHS Quality Improvement Scotland (NHS QIS) consents to the photocopying, electronic reproduction by ‘uploading’ or ‘downloading’ from the website, retransmission, or other copying of the findings contained in this report, for the purpose of implementation in NHSScotland and educational and ‘not-for-profit’ purposes. No reproduction by or for commercial organisations is permitted without the express written permission of NHS QIS.
Copies of this report, the Standards for Management of Post-mortem Examinations, and other documents produced by NHS QIS, are available in print format and on the website.
www.nhshealthquality.org

3 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
3Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Contents
1 Setting the Scene 5
1.1 How the Standards were Developed 6
1.2 How the Review Process Works 6
1.3 Reports 9
2 Summary of Findings 11
2.1 Overview of Local Service Provision 11
2.2 Summary of Findings Against the Standards 13
3 Detailed Findings Against the Standards 17
Appendix 1 Glossary of Abbreviations 47
Appendix 2 Details of Review Visit 48
Appendix 3 Management of Post-mortem Examinations
Project Group Members 49
Appendix 4 Timetable of Review Visits 51
Contents
5 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
5Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
NHS Quality Improvement Scotland (NHS QIS) was set up by the Scottish Parliament in 2003 to take the lead in improving the quality of care and treatment delivered by NHSScotland. NHS QIS does this by setting standards and monitoring performance, and by providing NHSScotland with advice, guidance and support on effective clinical practice and service improvements.
About this Report
The Standards for Management of Post-mortem Examinations were published in March 2003. These standards are being used to assess the quality of services provided by NHSScotland nationwide.
This report presents the fi ndings from the peer review of Tayside Acute Services Division. This review visit took place on 21 April 2004, and details of the visit, including membership of the review team, can be found in Appendix 2.
1 Setting the Scene1 Setting the Scene

6 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
1.1 How the Standards were Developed
In August 2001, a Management of Post-mortem Examinations Project Group was established under the chairmanship of Professor Sally Macintyre, Director, Medical Research Council, Social and Public Health Sciences Unit, University of Glasgow. Membership of the Group includes both healthcare professionals and members of the public (see Appendix 3).
The Group oversees the quality assurance process of:
• developing standards
• reviewing performance against the standards throughout Scotland, using self-assessment and external peer review
• reporting the fi ndings from the review. When developing standards for the management of post-mortem examinations, a Scotland-wide consultation process was undertaken. The views of health service staff were sought, and all the relevant evidence available at the time was taken into account. In May 2002, draft standards were piloted at two sites: Crosshouse Hospital, Ayrshire & Arran Acute Hospitals NHS Trust1; and Monklands Hospital, Lanarkshire Acute Hospitals NHS Trust.
1.2 How the Review Process Works
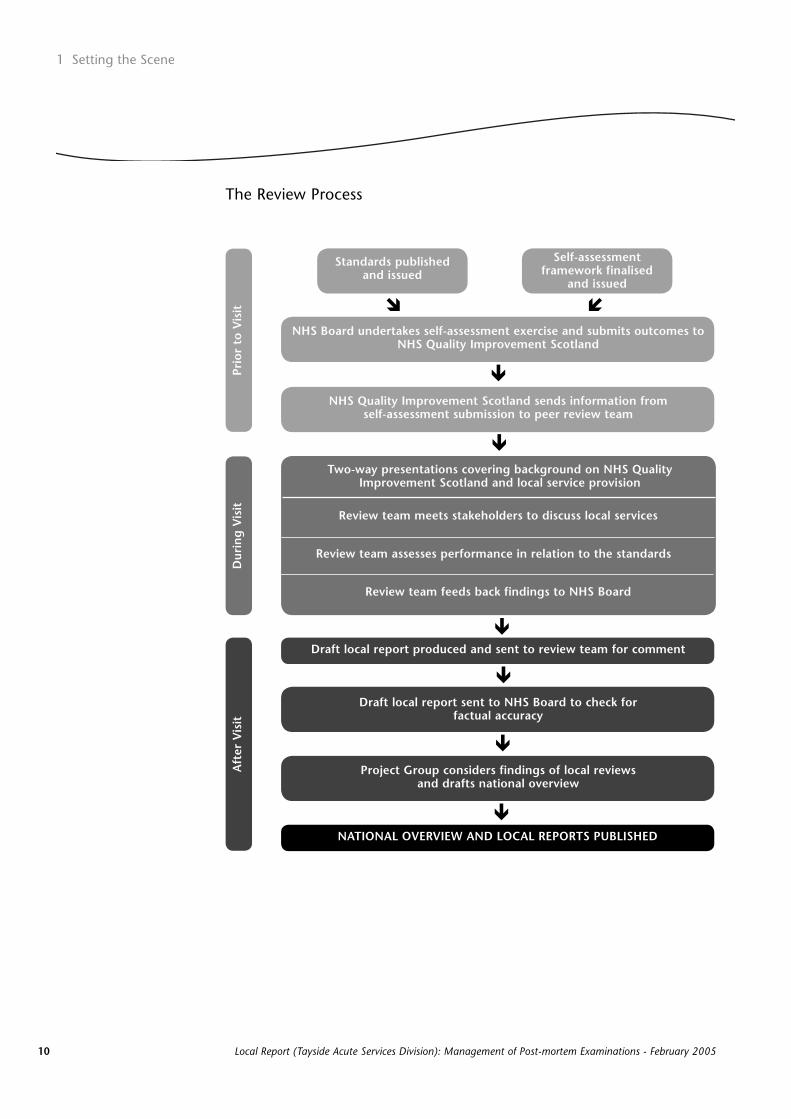
The review process has two key parts: local self-assessment followed by external peer review. First, each NHS Board assesses its own performance against the standards. An external peer review team then further assesses performance, both by considering the self-assessment data and visiting the NHS Board to validate this information and discuss related issues. The review process is described in more detail below (see also the fl ow chart on page 10).
Self-Assessment by NHS Boards
On receiving the standards, each NHS Board assesses its own performance using a framework produced by NHS QIS. This framework includes guidance about the type of evidence (eg guidelines, audit reports) required to allow a proper assessment of performance against the standards to be made.
1 Setting the Scene
1 Please note that NHS Trusts were abolished on 1 April 2004. Single-system working is now being introduced across NHSScotland.
7Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
The NHS Board submits the data it has collected for this self-assessment exercise to NHS QIS before the on-site visit, and it is this information that constitutes the main source of written evidence considered by the external peer review team.
External Peer Review
An external peer review team then visits and speaks with local stakeholders (eg staff, patients, carers) about the services provided. Review teams are multidisciplinary, and include both healthcare professionals and members of the public. All reviewers are trained. Each review team is led by an experienced reviewer, who is responsible for guiding the team in their work and ensuring that team members are in agreement about the assessment reached.
The composition of each team varies, and members have no connection with the NHS Board they are reviewing. Both of these factors facilitate the sharing of good practice across NHSScotland, and ensure that each review team assesses performance against the standards rather than make comparisons between one NHS Board and another.
At the start of the on-site visit, the review team meets key personnel responsible for the service under review. Reviewers then speak with local stakeholders about the services provided. After these meetings, the team assesses performance against the standards, based on the information gathered during both the self-assessment exercise and the on-site visit.
The visit concludes with the team providing feedback on its fi ndings to the NHS Board. This includes specifi c examples of local initiatives drawn to the attention of the review team (recognising that other such examples may exist), together with an indication of any particular challenges.

8 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Assessment Categories
Each review team assesses performance using the categories ‘met’, ‘not met’ and ‘not met (insuffi cient evidence)’, as detailed below.
• ‘Met’ applies where the evidence demonstrates the standard and/or criterion is being attained.
• ‘Not met’ applies where the evidence demonstrates the standard and/or criterion is not being attained.
• ‘Not met (insuffi cient evidence)’ applies where no evidence is available for the review team, or where the evidence available is insuffi cient to allow an assessment to be made.
A fi nal category ‘not applicable’ is used where a standard and/or criterion does not apply to the NHS Board under review.
1 Setting the Scene
9Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
1.3 Reports
After each review visit, NHS QIS staff, with clinical input as appropriate, draft a local report detailing the fi ndings of the review team. This draft report is sent to the review team for comment, and then to the NHS Board to check for factual accuracy. The local report is published only after all the visits for that topic have been undertaken nationwide.
Once a national review cycle is completed, the relevant project group reconvenes to examine review fi ndings and make recommendations. The project group then oversees the production of a national overview of service provision across Scotland in relation to the standards. This document includes both a summary of the fi ndings (highlighting examples of local initiatives and challenges for the service) and recommendations for improvement.
Part of the remit of NHS QIS is to report whether the services provided by NHSScotland, both nationally and locally, meet the agreed standards. This does not include reviewing the work of individual healthcare professionals. In achieving this aim, variations in practice (and potential quality) within a service will be encountered, and subsequently reported.
Please note – all reports published are available in print format and on the NHS QIS website.
10 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
1 Setting the Scene
NHS Quality Improvement Scotland sends information from self-assessment submission to peer review team
Self-assessment framework finalised
and issued
Standards published and issued
Draft local report produced and sent to review team for comment
Draft local report sent to NHS Board to check for factual ac cu ra cy
Project Group considers findings of local reviewsand drafts na tion al overview
NATIONAL OVERVIEW AND LOCAL REPORTS PUBLISHED
NHS Board undertakes self-assessment exercise and submits outcomes to NHS Quality Improvement Scotland
Dur
ing
Vis
itA
fter
Vis
itPr
ior
to V
isit � �
�
�
�
�
�
�
Two-way presentations covering background on NHS QualityImprovement Scotland and local service provision
Review team meets stakeholders to discuss local services
Review team assesses performance in relation to the standards
Review team feeds back findings to NHS Board
The Review Process

11 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
11Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
2 Summary of Findings
2.1 Overview of Local Service Provision
Tayside is situated in the east of Scotland and has a population of around 386,550. Many of the population live in urban areas, of which Dundee and Perth are the largest in the region, although a signifi cant proportion live in rural areas. The proportion of older people in the population is higher than the national average, whereas levels of illness and deprivation are close to the national average.
Local NHS System and Services
The Board of NHS Tayside is responsible for improving the health of the local population and for the delivery of the healthcare required. It provides strategic leadership and has responsibility for the effi cient, effective and accountable performance of the NHS in Tayside.
At the time of the review visit, the NHS Board area contained two NHS operating divisions: Tayside Acute Services Division (acute care services); and Tayside Primary Care Division (primary care services).
The NHS Board is accountable for both continuously improving the quality of their services, and safeguarding high standards of care, by creating an environment in which excellence in clinical care will fl ourish (framework of clinical governance).
Further information about the local NHS system can be accessed via the website of NHS Tayside (www.nhstayside.scot.nhs.uk/).
2 Summary of Findings

12 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Service Organisation
Information obtained from a scoping study exercise undertaken in 2003 indicated that there are 15 NHS organisations within Scotland that perform hospital post-mortem examinations. These examinations include general, neuropathology, paediatric and perinatal cases.
In Tayside Acute Services Division, general and paediatric post-mortem examinations are carried out at Ninewells Hospital, Dundee, and Perth Royal Infi rmary. Neuropathology examinations are carried out at the Western General Hospital, Edinburgh. All these examinations are performed either at the request of a relative or on the recommendation of the hospital, and require authorisation from the next of kin.
Post-mortem examinations are normally undertaken within 2 working days of receiving authorisation. Following completion of the examination, the post-mortem examination report is sent directly from the pathology department to the requesting clinician and passed on to the deceased’s GP.
Within Tayside Acute Services Division, data are collected to allow the various stages of the post-mortem examination process to be monitored.
2 Summary of Findings
13Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
2.2 Summary of Findings Against the Standards
A summary of the fi ndings from the review, including examples of local initiatives drawn to the attention of the review team, is presented in this section. A detailed description of performance against the standards/criteria is included in Section 3.
Pathology Practice
Tayside Acute Services Division provides a general and paediatric post-mortem examination service at Ninewells Hospital and Perth Royal Infi rmary. Fourteen consultant pathologists (two have a specialist interest in paediatric pathology) deliver this service. The Division has currently been unable to recruit a neuropathologist to the post in Dundee, and at present a service-level agreement for neuropathology exists with NHS Lothian.
Post-mortem examination reports compiled at the Division are based on and audited according to the Royal College of Pathologists’ (RCPath) Guidelines on autopsy practice (September 2002). There are comprehensive protocols in place to ensure correct identifi cation of the deceased. The Central Health Index (CHI) of unique identifi cation numbers for each individual is used throughout NHS Tayside which the review team noted as a strength of the service.
Staff reported that post-mortem examinations are undertaken within 2 working days of receipt of authorisation, but the Division was unable to provide audit data to validate this. Producing the initial and fi nal reports from these examinations within the recommended timescale was noted to be a challenge for the Division, but more recent data indicated that this is improving following active steps to fi ll vacant posts within the pathology department.
The review team noted that the oncology, obstetric and paediatric services take a proactive approach regarding care of the deceased and liaison with relatives, in some instances offering to speak with relatives up to several years after a post-mortem examination has occurred, if requested.
The Division plans to create a bereavement offi ce and have designated staff support the co-ordination of all administration work following the death of an in-patient, and the communication between clinical staff and relatives. While Division staff acknowledged that this initiative will be challenging, the review team supported the decision to take this forward.
14 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
2 Summary of Findings
Example of a local initiative
Clinical staff requesting a post-mortem examination use a checklist
with key prompting questions about the process. The checklist ensures
that all aspects of the authorisation process are adequately covered.
One of the questions on the checklist prompts the invitation for the
requesting clinician to attend the examination.
Authorisation and Information
The review team identifi ed that, while the authorisation forms and addenda in use within the Division did incorporate all the major headings as recommended in Appendix 5 of the preliminary report of the Independent Review Group on Retention of the Organs at Post-Mortem, these forms did not clearly record relatives’ wishes in relation to the use of organs for education and research. However, it was noted that this issue will be addressed with the implementation of the new national standard authorisation forms when they become available.
The Division uses a variety of information leafl ets to inform relatives about the post-mortem examination process. However, while the information used includes most of the recommendations found in Appendix 6 of the Independent Review Group on Retention of the Organs at Post-Mortem, there was limited information on education and research, and no information about the timing and release of results of the examinations.
Example of a local initiative
The Division has developed a comprehensive guidance document for
staff obtaining authorisation. NHS Tayside’s clinical informed consent
policy details the standards and procedures that apply to healthcare
professionals obtaining informed consent across all clinical services in
NHS Tayside to ensure compliance with national guidance.
Close supervision of junior medical staff by consultants for end of life procedures is in place in oncology, obstetric and paediatric services, and consultant involvement in the authorisation process is evident throughout other areas across the Division.

15Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
No audit of the authorisation process, and relatives’ experience of this, has yet been undertaken. However, there is a mechanism to receive feedback from relatives via the Pregnancy Loss Support Group and the Neonatal Bereavement Group.
Storage, Handling and Disposal
The review team noted that detailed policies are in place for the storage, handling and disposal of post-mortem examination material. Relatives’ wishes regarding disposal of organs to be retained for diagnostic purposes are documented. This information is recorded on the authorisation form and on one of the three additional forms for post-mortem examinations of adults, children or babies/fetuses, and also on the mortuary database. Disposal arrangements are undertaken according to relatives’ wishes and details regarding organs are also recorded electronically on a database.
Record-keeping
Post-mortem examination carried out within the Division is fully documented, and the pathology department retains the authorisation form, a copy of the clinical summary and the fi nal post-mortem examination report. It was noted that while the original authorisation form is retained as part of the pathology department record, no copy of this form is fi led as part of the deceased’s medical record.
Education
There are good areas of training provided within the Division, including a structured induction programme for junior medical staff which covers a range of end of life issues and instruction in completing the documentation required following death. However, a challenge for the Division is to ensure that this training is provided to all medical staff. The Division is currently updating the medical training curriculum, and work is under way to develop an induction course for all new staff.
The review team commended the Division on its provision of a wide range of communication skills courses offered to all grades of staff.

16 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
2 Summary of Findings
Example of a local initiative
Training seminars were held in conjunction with local funeral directors
and crematoria in Dundee and Perth. These seminars aimed to help
nursing staff gain a better understanding of the funeral director’s role
and of the cremation process. Seminars ran for several weeks to allow
all interested staff to attend; Division staff reported that the sessions
were informative and useful.
All staff involved in handling the deceased before and after a post-mortem examination are aware of current Health and Safety regulations, including control of infection notifi cation procedures. There are good instruction policies in place for infection control, and nursing staff receive this information as part of their induction. Rolling programmes of training in procedures for safe handling of potential sources of infection are in place for other members of healthcare staff. The review team particularly commended the training programme for porters.

17 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
17Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 1(a): Pathology Practice – Hospital Post-mortem Examinations
Standard StatementPathology Examination and Reporting: Where a post-mortem examination takes place, both the examination
and report follow the guidelines set by the Royal College of Pathologists (RCPath). The post-mortem
examination is carried out as soon as appropriate after authorisation is received and the initial and final
reports are sent to the clinician in charge of the case within a reasonable timescale.
Tayside Acute Services Division
Essential Criteria
1a.1: Post-mortem examinations are audited according to the most recent RCPath guidelines.
STATUS: Met
The Division reported that post-mortem examination reports are compiled based on the Royal College of Pathologists’ (RCPath) Guidelines on autopsy practice (September 2002). Anonymised copies of these reports were provided to the review team confi rming compliance with the guidelines.
An audit into the trends of pathology practice conducted recently at Ninewells Hospital, Dundee, comprised a retrospective, comparative analysis of hospital post-mortem examinations in the years 1997 and 2002. The audit considered: information regarding the pathologist carrying out the examination; details of retained organs; specialist investigations; dates of completion of preliminary and fi nal reports; causes of death; and seniority of staff requesting authorisation. The review team found the detail of the audit to be informative and in line with current guidelines.
1a.2: Protocols and procedures are in place to ensure accurate identification of the deceased.
STATUS: Met
The Division has a variety of protocols in place to ensure accurate identifi cation of the deceased. For adult deaths, nursing staff follow the ‘Last Offi ces’ procedure detailed in the caring for an in-patient after death policy. Identifi cation of the body is by means of an identity bracelet, a name tag, and a completed mortuary card secured to the outside covering of the body at chest level. Before transferring the body from the ward to the mortuary, porters ensure that details on the mortuary card match those on a ‘Notice to Death’ card. On arrival at the mortuary, staff enter the deceased’s details in the mortuary register and computer database.
18 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
A ‘Bereavement Guideline’ booklet is in place for staff working in the neonatal unit and contains information on: last offi ces; transport of baby to the mortuary; guidelines for staff when parents wish to take their baby home following death; the bereaved parents; viewing; book of remembrance; remembrance box; follow-up; funeral costs; request for post-mortem; and details of Division staff available to provide support. The review team commended the content of this document.
Pathology staff reported that they use the Community Health Index (CHI) for patient identifi cation, and fi nd that these unique numbers are robust and in use throughout NHS Tayside. The review team recognised the use of this system across the NHS Board area as a strength.
1a.3: Information for relatives, where requested, is available in non-medical language.
STATUS: Met
The leafl et entitled ‘Practical Help and Information for the Bereaved’, produced by the Trust’s Bereavement Group in consultation with bereaved families and funeral directors, uses non-medical language to give relatives some useful advice when making arrangements following the death of a relative in hospital. The leafl et contains details of professional and voluntary support organisations and local counselling services. Division staff reported that this document has been under review, and has recently been fi nalised for consultation before being implemented across NHS Tayside.
A separate leafl et, produced by the Women & Reproductive Health Bereavement Group in consultation with the Stillbirth and Neonatal Death Society (SANDS) Tayside, gives practical information for parents making funeral arrangements following the loss of a baby in pregnancy or in infancy. This leafl et includes contact details of local professionals and support services as well as suggested reading material, and is also written in plain language.
A ‘Guide to the Postmortem Examination’ leafl et is also available, and provides brief notes for parents and families following the loss of a baby in pregnancy or in infancy.
1a.4: The post-mortem examination is supervised, or carried out, by a pathologist on the specialist register
of the General Medical Council (GMC).
STATUS: Met
The Division submitted evidence confi rming that post-mortem examinations are supervised, or carried out, by pathologists on the specialist register of the General Medical Council (GMC).
19Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
1a.5: Paediatric and perinatal post-mortem examinations are supervised or carried out by a pathologist
trained in this specific field.
STATUS: Met
The review team noted that paediatric and perinatal post-mortem examinations are normally carried out at Ninewells Hospital and Perth Royal Infi rmary by pathologists trained in paediatric and perinatal pathology. However, on occasions where further specialist examination is required, these cases would be referred to a specialist regional service at the Royal Hospital for Sick Children, Yorkhill, Glasgow, and the Royal Infi rmary of Edinburgh.
At the time of the visit, it was reported that the pathologists undertaking paediatric and perinatal post-mortem examinations are not full-time, and have limited opportunity for personal development in this specialty. The review team recommended that the pathologists specialising in these specifi c fi elds be offered protected work sessions, and be supported in participating in relevant external quality assurance (EQA) schemes for paediatric and perinatal pathology.
1a.6: The post-mortem examination is carried out by the department performing the examination within 2
working days of receipt of authorisation.
STATUS: Not met (insuffi cient evidence)
The Division provided the review team with a copy of its post mortem administration, histology and reporting - procedure for pathologists document, which states that post-mortem examinations are to be carried out within 2 working days of receipt of authorisation. Staff verbally reported that if a request for a post-mortem examination and completed documentation is received before midday, the examination will be performed on the day of request, or on the following day if the request is received later in the afternoon.
As the Division was unable to provide audit data to confi rm that post-mortem examinations are performed within 2 working days of receipt of authorisation, the review team considered this criterion to be not met due to insuffi cient evidence.
1a.7: 90% of initial reports are sent to requesting clinicians within 2 working days of completion of the
post-mortem examination.
STATUS: Not met
Audit data provided to the review team indicated that the Division is currently meeting the essential criterion for producing initial reports within 2 working days of completion of post-mortem
20 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
examinations at one hospital site. The other site is outwith the essential criterion. However, staff reported that more recent data indicated that the timescale for producing these reports was improving, and that this was partly due to the introduction of a single-page preliminary report.
1a.8: 90% of final reports are sent to requesting clinicians within 21 working days. Where reports are
delayed, eg due to toxicology or histology investigations, information about the delay is available.
STATUS: Not met
Audit data provided to the review team indicated that the Division does not meet the essential criterion for sending fi nal reports to the requesting clinician within 21 working days of completion of the post-mortem examination. The review team acknowledged that this criterion is only applicable for adult general cases as results from tests for specialised paediatric and neuropathology cases take longer to process.
It was noted that the Division is working to increase the number of fi nal reports issued within this timescale, which has been assisted by the recently appointed quality manager who follows up delayed reports. However, it was also noted that there is limited clerical support within the pathology department.
The Division has a standard operating procedure (SOP) in place for managing all enquiries relating to post-mortem examination reports and recording delays in reporting.
1a.9: Information from the post-mortem examination is communicated by the clinical team to the
deceased’s GP.
STATUS: Met
The Division submitted evidence of its procedure for communicating information from the post-mortem examination to the deceased’s GP. This states that a copy of the examination report is routinely sent to the consultant in charge of the deceased in life and to the deceased’s GP. In addition, for paediatric cases, a letter is sent to the deceased’s GP after the 6-week follow-up meeting with parents to report the fi ndings from the examination.
21Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Desirable Criteria
1a.10: Other consultants who cared for the deceased in life are identified to the pathology department and
also receive copies of the final report.
STATUS: Met
A copy of the fi nal report is sent to the consultant who cared for the deceased in life and to other requesting clinicians involved in their care. The review team was provided with a copy of the pathology department policy for issuing and mailing post mortem reports which supports this process.
22 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 1(b): Pathology Practice – Hospital Post-mortem Examinations
Standard StatementCommunication: There is effective communication between all those involved before and after the post-
mortem examination and there is an identified member of staff to facilitate this.
Tayside Acute Services Division
Essential Criteria
1b.1: The pathologist carrying out the post-mortem examination is provided with a clinical summary and
a copy of the authorisation form which details the relatives’ wishes. The pathologist has access to the
deceased’s medical records, where these are available.
STATUS: Met
The Division reported that the pathologist carrying out the post-mortem examination receives the original authorisation form, which contains a record of relatives’ wishes and a clinical summary. Division staff stated that an examination will not be carried out unless all the relevant documentation is in place.
1b.2: There is a procedure to encourage the requesting clinician to attend the post-mortem examination.
STATUS: Met
There are informal and formal procedures in place to encourage requesting clinicians to attend post-mortem examinations. Clinical staff requesting an examination use a checklist with key prompting questions about the process. This checklist contains a question that prompts the invitation for the requesting clinician to attend the examination.
1b.3: Relatives are offered: the opportunity to speak to clinical staff involved in the care of the deceased
and key information is provided in non-medical terms if possible; and a copy of the post-mortem
examination report if they wish it.
STATUS: Met
Staff reported that, although relatives are not routinely verbally offered the opportunity to discuss the key information from the post-mortem examination report with clinical staff, this would be arranged if requested and the information would be given in non-medical language. ‘The Post-Mortem
23Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Examination Information for Relatives’ leafl et notes that relatives should contact either the clinician who cared for the patient in life, or the deceased’s GP, to discuss the fi ndings of the examination if they wish.
The review team observed that in services such as oncology, paediatrics and obstetrics, relatives are proactively offered the opportunity for discussion with clinical staff. In cases of paediatric deaths, relatives are invited to meet with the consultant involved in the care of their baby up to 6-weeks after the post-mortem examination to discuss the fi ndings.
The review team encouraged the Division to verbally offer relatives the opportunity to meet with clinical staff in addition to providing this information in written leafl et format.
Desirable Criteria
1b.4: There is a designated administrator whose primary function is to be a point of contact for relatives, to
ensure completion of all appropriate forms and co-ordinate communication between the clinical staff
and relatives.
STATUS: Not met
There is no designated administrator with responsibility to act as a point of contact for relatives within the Division, although this post is being formally considered by the Division’s Care of Patient After Death Group.
Staff reported that the Division has identifi ed the need for a bereavement offi ce to undertake all administration work following the death of a patient. Aspects of this are currently under consideration and include the need for permanent staffi ng in order to facilitate this process, and the potential for the bereavement offi ce to formalise the varying staff training programmes that exist within NHS Tayside. The review team supported this initiative.
1b.5: A summary of the post-mortem examination report is available to relatives in non-medical language,
if requested.
STATUS: Met
The Division submitted evidence that a summary of the post-mortem examination report in non-medical language can be provided to relatives if required, although staff reported that this is not normally requested. Division staff also stated that they would prefer to offer face-to-face meetings between staff and relatives, and that more than one meeting can take place if relatives wish.
24 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 1(c): Pathology Practice – Hospital Post-mortem Examinations
Standard StatementCommunication: Personal, religious and cultural values and beliefs of the deceased and their relatives are
respected.
Tayside Acute Services Division
Essential Criteria
1c.1: Information on bereavement, and religious and cultural support is available.
STATUS: Met
The Division submitted evidence of a wide variety of information leafl ets available to parents and families who have experienced a bereavement, and stated that there are a number of initiatives in place to ensure bereavement, and religious and cultural support is provided throughout the Division. A religions and culture guide to beliefs and customs for health staff and social care services is provided at ward level. The guide contains general guidance on diet, language and names of different faith groups, and gives information on matters such as birth and death, and associated practices and assumptions concerning illness itself. Relatives are provided with the information at the time of death, which includes details of local support groups.
The review team noted the maternity unit’s book of remembrance, which is available at each hospital site and can be easily viewed. A memorial service is held annually to remember all the babies and children who have died. Parents who have experienced the loss of a baby can also be referred to the bereavement support nurse at Ninewells Hospital or the hospital chaplain for bereavement support.
1c.2: A translation service is available.
STATUS: Met
The National Interpreting Service (NIS) is available throughout NHS Tayside which offers 24-hour access to translation by telephone. A face-to-face translation service can also be arranged through Dundee City Council, and sign language services can be obtained via the Tayside Association for the Deaf. Staff reported that this service can also be used for the translation of letters and documents. Notices on how to contact NIS are displayed in clinical areas.
Division staff reported that NHS Tayside is currently discussing the possibility of maintaining stocks of the most popular leafl ets used in languages other than English.

25Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Standard 2(a): Authorisation and Information
Standard StatementAuthorisation is given for all hospital post-mortem examinations, using the national authorisation forms when
these become available. Forms should take into account the wishes of the deceased and where appropriate,
the wishes of the relatives.
Tayside Acute Services Division
Essential Criteria
2a.1: Authorisation forms in use incorporate the major headings of the template in Appendix 5 of the
preliminary report of the Independent Review Group on Retention of Organs at Post-Mortem, only
until the national standard paediatric and adult authorisation forms are available.
STATUS: Met
The authorisation form and associated addenda used incorporate the major headings recommended in Appendix 5 of the preliminary report of the Independent Review Group on Retention of the Organs at Post-Mortem.
The review team was also provided with a copy of a fi nal draft of NHS Tayside’s clinical informed consent policy, which details the standards and procedures applying to healthcare professionals obtaining informed consent across all clinical services in NHS Tayside to ensure compliance with national guidance. The review team commended this initiative.
26 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 2(b): Authorisation and Information
Standard StatementConsultant clinical staff take overall responsibility for end of life procedures on the ward and maintain close
contact with relatives, the pathology department and those involved in support of the deceased’s family.
Tayside Acute Services Division
Essential Criteria
2b.1: There is evidence of close supervision of junior medical staff by consultants.
STATUS: Not met
Evidence submitted to the review team indicated that there is a policy for consultant supervision of junior medical staff. However, this is not practised in all areas throughout the Division. It was reported that close supervision of junior medical staff by consultants is in place in services such as oncology, paediatrics and obstetrics. The review team noted that there is less supervision of junior medical staff by consultants in other areas, in particular junior house offi cers (JHOs)requesting authorisation for adult post-mortem examinations.
The Division submitted evidence that consultant involvement in the authorisation process is slowly improving and a cultural change appears to be gradually occurring. Pathology staff continue to emphasise the importance of consultant involvement in the authorisation for post-mortem examinations.
27Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Standard 2(c): Authorisation and Information
Standard StatementInformation about both the post-mortem examination and the authorisation process is available and
is provided to relatives if they request this. Trusts undertake ongoing audit of the processes involved in
authorisation of post-mortem examinations.
Tayside Acute Services Division
Essential Criteria
2c.1: Information leaflets in use follow the template found in Appendix 6 of the preliminary report of
the Independent Review Group on Retention of Organs at Post-Mortem. The national standard
information leaflet is used when it becomes available.
STATUS: Not met
At the time of the review process (November 2003 to June 2004), the national standard information leafl ets for both adult and paediatric post-mortem examinations had yet to be introduced. The Division has developed and uses a variety of information leafl ets to inform relatives about the post-mortem examination process. For adult cases, the information for relatives leafl et is used during discussion with medical staff at the time of authorisation, and ‘A Guide to the Postmortem Examination’ leafl et is given to parents who have lost a baby to help them to decide whether or not to agree to a post-mortem examination.
However, the information used within the Division includes most, but not all, of the recommendations found in Appendix 6 of the preliminary report of the Independent Review Group on Retention of Organs at Post-Mortem.
2c.2: Audit is facilitated by the Trust audit department, and local protocols are in place to demonstrate:
audit of the authorisation process and relatives’ experience; and mechanisms to provide feedback to
all staff involved.
STATUS: Not met
Division staff reported that, in view of its sensitive nature, no formal audit has yet been undertaken of relatives’ experience of the authorisation process, although the issue has been discussed.
The review team noted, however, that the Division undertakes other audit projects, and an example of a service change, made in response to parents’ views, is in regard to the method of transporting deceased infants from wards to the mortuary. Parents, the Pregnancy Loss Support Group and the Neonatal Bereavement Group expressed a desire that individually decorated boxes or baskets be used for this purpose. In view of this, the casket for transport of the deceased baby is now dependent on the mother’s wishes.

28 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 2(d): Authorisation and Information
Standard StatementEducation: Where hospitals teach medical students on post-mortem examinations, this is explained during the
authorisation process.
Tayside Acute Services Division
Essential Criteria
2d.1: Authorisation forms and leaflets include information on teaching where appropriate.
STATUS: Not met
At the time of the visit, neither the authorisation form, its associated addenda, nor leafl ets about the post-mortem examination process contained suffi cient information on medical teaching.
The review team suggested that it could be benefi cial for the forms and leafl ets to contain more information on teaching and research; to distinguish between teaching and research processes; and to specify how and by whom post-mortem material would be used as part of each process. However, it was recognised that these issues will be addressed with the implementation of the national standard authorisation forms and leafl ets.

29Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Standard 2(e): Authorisation and Information
Standard StatementEducation: Where organs are retained for use in teaching, authorisation is obtained. It is made clear to
relatives at that time that their authorisation may be withdrawn at any time.
Tayside Acute Services Division
Essential Criteria
2e.1: Relatives’ wishes in relation to the use of organs for teaching are clearly indicated on the authorisation
form.
STATUS: Met
Relatives’ wishes in relation to the use of tissue samples for teaching are indicated on the authorisation form.

30 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 2(f): Authorisation and Information
Standard StatementResearch: Organs which have been taken for diagnostic purposes can only be further retained for research if
appropriate authorisation is provided. Information about the purpose of any research will be made available to
the relatives if requested.
Tayside Acute Services Division
Essential Criteria
2f.1: Information on research is provided for relatives as part of the authorisation process.
STATUS: Met
The adult authorisation form contains an option for relatives to choose if they wish tissue to be taken solely for medical education or research. Division staff reported a detailed discussion would take place with relatives as part of the authorisation process.
The review team acknowledged that it is not Division policy to carry out research on post-mortem examination material. However, the review team considered it appropriate for relatives to be provided with information on research for cases which require to be sent to NHS Lothian - University Hospitals Division for specialist neuropathology examination. The review team noted that for paediatric cases, all details regarding research are clearly indicated on the post-mortem examination authorisation form.
2f.2: Relatives’ wishes in relation to the use of organs for research are clearly indicated on the authorisation
form.
STATUS: Met
Relatives’ wishes in relation to the use of tissue and organs for research and clinical examination are indicated on the authorisation form for post-mortem examination.
31Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Standard 2(g): Authorisation and Information
Standard StatementAdditional Material for Research and Education: Authorisation is required if additional tissue slides, blocks or
organs are considered valuable for education and research. Authorisation can be withdrawn at any time.
Tayside Acute Services Division
Essential Criteria
2g.1: There is a protocol for obtaining authorisation for research, which includes information about how
this material is to be used and stored.
STATUS: Not applicable
Research on post-mortem examination material is not currently undertaken at the Division. However, the review team was informed that, should any specifi c research project be undertaken, approval would be required from the Local Research Ethics Committee (LREC) and authorisation obtained from relatives before any research could be carried out. An additional information sheet would be used as part of the authorisation process, and withdrawing authorisation would be discussed with relatives at this time.
2g.2: There is evidence that authorisation has been obtained.
STATUS: Not applicable
Research on post-mortem examination material is not currently undertaken by the Division.
2g.3: There are local arrangements in place to provide feedback on the type of research undertaken.
STATUS: Not applicable
Division staff reported that no research projects using post-mortem examination material are undertaken.

32 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
2g.4: There is evidence of regular review of teaching stock to avoid excess retention.
STATUS: Met
The Division reported that a database of teaching stock is maintained and reviewed annually in conjunction with the University of Dundee. When tissue/organs are no longer required they are disposed of in accordance with relatives’ wishes, and this information is recorded on the mortuary database. The is an SOP in place for disposal arrangements.
33Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Standard 3(a): Storage, Handling and Disposal
Standard StatementGlass Slides and Tissue Blocks: Tissue samples are taken for diagnostic purposes. All glass slides and tissue
blocks taken at post-mortem examination for diagnostic purposes are retained as part of the medical record of
the deceased and are stored securely.
Tayside Acute Services Division
Essential Criteria
3a.1: Glass slides are held for a minimum of 10 years.
STATUS: Met
There is a pathology department policy for the control of clinical material and process records. This detailed document, last updated in February 2004, outlines the identifi cation, collection, indexing, accessing, fi ling, storage and disposal of various material and records used by the pathology department. The policy indicates that glass slides are retained for a minimum of 30 years.
3a.2: Tissue blocks are held for a minimum of 30 years.
STATUS: Met
The pathology department policy for the control of clinical material and process records indicates that tissue blocks are retained for a minimum of 30 years.
3a.3: There is a written policy to ensure secure storage.
STATUS: Met
The pathology department policy for the control of clinical material and process records details storage, security and controlled access to clinical material held by the pathology department. Specifi cally, it states that all storage areas are kept locked, and only authorised personnel can remove material after completing the appropriate documentation.
3a.4: There is a written policy covering disposal where a decision is taken not to retain tissue samples.
STATUS: Met
There is a policy in place for the disposal of glass slides and tissue blocks.
34 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 3(b): Storage, Handling and Disposal
Standard StatementOrgans: Organs which require to be retained for diagnostic purposes are disposed of following diagnosis, with
the knowledge and instruction of the relatives of the deceased.
Tayside Acute Services Division
Essential Criteria
3b.1: There is documentation of the relatives’ wishes.
STATUS: Met
Relatives’ wishes regarding the disposal of organs to be retained for diagnostic purposes are documented on the ‘Post-mortem Consent and Authorisation Form’, and on one of three addenda (for post-mortem examinations of adults, children, or babies/fetuses).
The review team noted that the authorisation form contains only one option for organ disposal (by hospital), however, the addenda each offer three options which include hospital disposal, arranging for organs to be returned to the deceased’s body, or arranging for organs to be returned to the relatives via their funeral director for burial or cremation. The relatives’ wishes for organ disposal are also recorded on the mortuary database.
3b.2: Every hospital carrying out post-mortem examinations has a written protocol for the storage,
handling and disposal of organs.
STATUS: Met
The pathology department’s SOP contains written guidance for this. The storage, handling and disposal of organs is tracked via the tissue retention database on the mortuary computer system.
The review team recognised the tissue retention database as a strength for the Division in terms of record-keeping.
35Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3b.3: For diagnostic cases, organs are retained for a maximum of 3 months after the microscopic report is
completed. Any delays are documented.
STATUS: Met
Staff reported that Division policy states that post-mortem examination tissue/organs must not be kept for more than 3 months after the microscopic report has been issued. Retention times are monitored using the tissue retention database on the mortuary computer system.
3b.4: The arrangements for disposal of an organ are the responsibility of the department carrying out the
post-mortem examination, in line with local protocols. Information on these arrangements is recorded
in the departmental database. This information is also recorded in the database of the pathology
department carrying out the analysis when this differs from the department carrying out the post-
mortem examination.
STATUS: Met
There are local protocols in place for the disposal of an organ. Staff reported that organs are disposed of in respect of relatives’ wishes, as noted on the post-mortem examination authorisation form. Any transfer and disposal of organs are recorded in the transfer log book, the tissue retention database on the mortuary computer system, and on a laboratory computer system. Where it is necessary to transfer organs to other centres for specialist examination (eg neuropathology cases), the transfer is recorded and disposal arrangements are respected.
Funeral directors collecting an organ on behalf of relatives are asked to sign to confi rm receipt. Details are also recorded electronically.

36 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 3(c): Storage, Handling and Disposal
Standard StatementResidual Tissues: Small pieces of residual tissue which are not processed or stored as part of the deceased’s
medical record are disposed of lawfully.
Tayside Acute Services Division
Essential Criteria
3c.1: There is a written policy for the disposal of small pieces of residual tissue which includes recording
how, where and when they are disposed of. Relatives are informed of these arrangements, upon
request.
STATUS: Met
The pathology department policies for surgical and post-morten tissue disposal, and tissue storage/disposal both detail the procedures to be undertaken for the disposal of tissue samples.
Staff reported that relatives’ wishes regarding disposal arrangements are recorded on the mortuary database and that, if relatives request, tissue can be returned to their funeral directors for private burial/cremation, or disposed of by the hospital in accordance with Division policy.

37Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Standard 3(d): Storage, Handling and Disposal
Standard StatementFetuses: Any fetus or embryo having pathological examination is disposed of lawfully and in accordance with
parents’ wishes.
Tayside Acute Services Division
Essential Criteria
3d.1: There is a protocol in place which sets out local arrangements for disposal of fetuses and fetal tissue.
Parents may make alternative arrangements if they wish, and these are documented.
STATUS: Met
The Division has a range of documents in place which sets out local arrangements for disposal of fetuses and fetal tissue.
Parents can choose for the hospital to arrange disposal, or alternatively they can make their own disposal arrangements for burial or cremation via their funeral directors. The preferred choice of arrangement is discussed with clinical staff and recorded on the ‘Women’s & Reproductive Health Notifi cation of Non-Viable Fetus’ Birth Form’, and in the nursing notes. The review team recommended that this notifi cation form be amended to include a relative’s signature in addition to the signature of a midwife.
38 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 3(e): Storage, Handling and Disposal
Standard StatementTransport: Relatives and funeral directors are informed if the deceased, or organs taken for diagnosis, need to
be moved to another hospital for post-mortem examination. Transport arrangements for the deceased and/or
organs are fully documented.
Tayside Acute Services Division
Essential Criteria
3e.1: There is a written protocol for the movement of the deceased and organs between sites. This details
how these will be moved and by whom. The protocol covers informing relatives and funeral directors.
STATUS: Not met
There is a range of pathology department protocols in place for the movement of the deceased and organs between sites.
These protocols cover how the deceased and/or organs will be moved and by whom. However, the protocols do not detail the need to inform relatives and funeral directors when the deceased/organs are being transferred between sites. Division staff reported that there are informal arrangements in place with the funeral directors to inform relatives about any movement of the deceased or organs.
Brains are the only organs which are currently transferred to NHS Lothian for specialist neurological examination, and details of movement are recorded on the mortuary database. The review team was informed that the company contracted to transport specimens on behalf of NHS Tayside operates sensitively and professionally using protocol guidance.
3e.2: There is a system for recording: the organs transported and the reason why; the sending and
receiving centres; who sent and received the organs and the dates; and dates when the organs are
returned to the referring department.
STATUS: Met
The review team noted that the Division uses a comprehensive mortuary database to record: the organs transported and the reason why; the sending and receiving centres; who sent and received the organs and the dates; and dates when the organs are returned to the referring department. The mortuary database also facilitates a clear audit trail of all organs transported from hospital wards to funeral directors.
The review team was informed that transport arrangements between hospitals are timely and satisfactory.
39Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Standard 4(a): Record-keeping
Standard StatementEvery post-mortem examination is fully documented and the records retained in accordance with the most
recent Royal College of Pathologists Guidelines (NB tissue blocks and slides are a part of the medical record).
It is the responsibility of the head of the pathology department carrying out the post-mortem examination to
ensure that the above information is recorded.
Tayside Acute Services Division
Essential Criteria
4a.1: Documentation from each post-mortem examination includes a copy of the following: authorisation
form; clinical summary; and post-mortem examination report.
STATUS: Met
Documentation from each post-mortem examination is fi led in the pathology department and includes the authorisation form, a copy of the clinical summary and the post-mortem examination report. A copy of the clinical summary is included as part of the deceased’s medical record.
4a.2: A copy of the following documents are filed in the department carrying out the post-mortem
examination: authorisation form; clinical summary; and post-mortem examination report.
STATUS: Met
A copy of the authorisation form, clinical summary and fi nal examination report are fi led in the department carrying out the post-mortem examination.
4a.3: The medical records of the deceased contain a copy of the authorisation form and a copy of the post-
mortem examination report.
STATUS: Not met
Staff reported that only the original copy of the post-mortem examination authorisation form is fi led within the pathology department. A copy of the clinical summary and fi nal examination report is fi led in the deceased’s medical records.
40 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
4a.4: All samples taken for cytology, histology and all other investigations are detailed in the post-mortem
examination report.
STATUS: Met
Evidence submitted by the Division confi rmed that post-mortem examination reports detail samples taken for investigations.
41Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Standard 4(b): Record-keeping
Standard StatementClinical Audit: Clinical audit is only carried out on named samples which were initially taken for diagnosis. This
practice is subject to the rules of medical confidentiality. These samples can also be used to validate diagnostic
tests and improve clinical care.
Tayside Acute Services Division
Essential Criteria
4b.1: There is evidence that material used for clinical audit and quality control has been subject to diagnosis
and subsequent report.
STATUS: Not applicable
The Division reported that post-mortem examination material is no longer used for quality control or clinical audit, therefore, this criterion is not applicable.

42 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 5(a): Education
Standard StatementAll medical staff in training in Trusts are instructed in completing the documentation required following death,
the reasons for post-mortem examination, and the ethical and medico-legal framework in which death occur.
Tayside Acute Services Division
Essential Criteria
5a.1: There is an induction programme, with input from pathologists, for all clinical staff dealing with
death, which covers: reasons for a post-mortem examination; the authorisation process; religious and
cultural issues; issuing death certificates; cremation regulations; and deaths that need to be reported
to the procurator fiscal.
STATUS: Not met
There is an induction programme, with input from pathologists, for JHOs which is mandatory and covers a variety of aspects on managing end of life issues. This is supplemented with twice-yearly teaching sessions organised by the Postgraduate Offi ce at Ninewells Hospital, and information on post-mortem examinations which is available in the pathology users handbook. However, only senior house offi cers (SHOs) and specialist registrars (SpRs) receive induction for obstetrics and paediatric pathology.
Division staff reported that the medical training curriculum was currently being updated and awaiting approval. Work was also under way to develop induction processes for all new staff, with the possible provision of a CD-ROM. It is envisaged that the CD-ROM will include information for all Division staff groups and will focus on managing the death process, including authorisation of a post-mortem examination, and religious and cultural issues.
The review team acknowledged the Division’s comprehensive spiritual care policy, which outlines the principles that underpin the delivery of spiritual and religious care within NHS Tayside, and is available to all staff via the intranet. Staff also use the ‘Lothian Race Equality Booklet’ for guidance on religious and cultural issues, and aim to produce their own version of this useful guide with local contact numbers of various faith groups.
The review team concluded that, while there are good areas of induction provided within the Division, there is no formal programme to ensure that all clinical staff receive training in managing end of life issues.
43Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
5a.2: Further training is available in communication skills and the bereavement process.
STATUS: Met
The review team commended the Division on its provision of a wide range of further training available for all groups of staff in communication skills and the bereavement process, beyond the induction level.
A half-day session on communication skills is available and can be tailored to meet individual needs. Education/training sessions on spiritual care are provided for staff in contact with terminally ill patients by the chaplaincy service within Ninewells Hospital. A one-day course on loss and bereavement is delivered 4–5 times per year, for all groups of staff. Training seminars have been held in conjunction with local funeral directors and crematoria in Dundee and Perth, to help nursing staff gain a clearer understanding of the funeral director’s role and the cremation process. The neonatal unit bereavement counsellor also participates in delivering a number of courses, study days and teaching sessions for various staff groups, including medical and nursing students, on issues related to the grieving process and breaking bad news.
The Division has a variety of working groups who meet regularly to discuss issues associated with the bereavement process and to ascertain staff training requirements in bereavement and loss issues. These groups include both staff and patient representatives. It was also acknowledged that a course entitled ‘Good Grief ’ is about to be offered to staff whose work brings them into contact with terminally ill patients or with the relatives of patients who have died.
44 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 5(b): Education
Standard StatementAll staff are aware that, after death, a body can still be a potential source of infection, and observe current
Advisory Committee for Dangerous Pathogens (ACDP) and Health and Safety Executive (HSE) guidelines.
Tayside Acute Services Division
Essential Criteria
5b.1: All staff involved in handling the deceased before and after a post-mortem examination are aware of
current Health and Safety regulations, including control of infection notification procedures.
STATUS: Met
The review team noted that NHS Tayside’s clinical caring for an in-patient after death policy was comprehensive, especially in terms of instruction regarding procedures for infection control. This policy, together with the policy for caring for a patient after death, provides information to staff on handling the deceased before and after a post-mortem examination, current Health and Safety regulations, and control of infection notifi cation procedures.
The Division indicated that nursing staff are aware of universal precautions for control of infection, and handling the deceased before and after the post-mortem examination as part of their induction programme. Staff reported that there are also rolling training programmes on procedures for infection control for all other members of healthcare staff. The review team particularly commended the training programme for porters - this training is compulsory, and its content updated annually. The training includes issues such as safe and lawful handling of the deceased, and procedures for transferring bodies to and from the mortuary.
5b.2: Control of infection notification procedures are in place for the deceased (if required).
STATUS: Met
Guidelines for care of the deceased with notifi able/non-notifi able infections are provided in NHS Tayside’s clinical caring for an in-patient after death policy. This policy states that infection risks are identifi ed on the deceased’s mortuary card. Any known risk of infection is communicated by telephone to the pathology department staff and funeral directors are also informed of this risk.
45Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
At the time of the visit, a confi dentiality agreement between NHS Tayside and local funeral directors was being negotiated to allow necessary information, including any potential infection risk, to be passed on to appropriate parties. A copy of the ‘Guidelines on Confi dentiality of Patient Identifi able Information: Funeral Directors’ document and ‘Confi dentiality Statement Form’ to be signed by the funeral director/representative was provided to the review team for information.
Division staff informed the review team that infection notifi cation signs are also on display in the mortuary to remind staff of the safeguarding procedures for infection control.

46 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
Standard 5(c): Education
Standard StatementAnatomical Pathology Technicians (APTs) receive training in all aspects of mortuary practice, which includes
the educational and research value of a post-mortem examination as well as its diagnostic function and the
risk of infection.
Tayside Acute Services Division
Essential Criteria
5c.1: Anatomical Pathology Technicians (APTs) are qualified and hold a certificate in anatomical pathology
or equivalent, or work under supervision.
STATUS: Met
The Division provided evidence confi rming that anatomical pathology technicians (APTs) hold a diploma from the Royal Institute of Public Health. In-service training programmes for mortuary and medical staff are also carried out according to RCPath guidelines.
47 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
47Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Appendix 1 — Glossary of Abbreviations
APT anatomical pathology technician
BMS biomedical scientist
CPA Clinical Pathology Accreditation
GMC General Medical Council
GP General Practitioner
LREC Local Research Ethics Committee
MLSO medical laboratory scientific officer
MRC Medical Research Council
MREC Multicentre Research Ethics Committee
NHS QIS NHS Quality Improvement Scotland
RCPath Royal College of Pathologists
SOP standard operating procedure
Abbreviation
48 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Appendix 2 — Details of Review Visit
The review visit to Tayside Acute Services Division was conducted on 21 April 2004.
Review Team Members
Dr Charles Swainson (Team Leader)
Medical Director, NHS Lothian - University Hospitals Division
Ms Diane Anderson
Senior Midwife, Yorkhill Division
Mr Larry Bryant
Lay Representative, Greater Glasgow
Mrs Helen Cadden
Lay Representative, Greater Glasgow
Mr Andrew Glancy
Senior Technician, NHS Lothian - University Hospitals Division
Sister Julie Graham
Specialist Palliative Care Nurse, Lanarkshire Acute Hospitals Division
Dr Elizabeth Gray
Consultant Paediatric Pathologist, NHS Grampian
Reverend Sandy Young
Lead Chaplain, NHS Lothian - University Hospitals Division
Mrs Fiona Warner (Observer)
Scottish Executive Health Department
NHS Quality Improvement Scotland Personnel
Ms Brin Jardine
Project Officer
Mr Steven Wilson
Team Manager
During the visit, members of the review team met with local health service personnel, including specialist and general pathology and laboratory staff, service managers, specialist members, midwives, nurses and chaplains.
49 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
49Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
Appendix 3 — Management of Post-mortem Examinations Project Group Members
Chair
Professor Sally Macintyre
Director, Medical Research Council, Social and Public Health Sciences Unit,
University of Glasgow
Project Group Members
Sister Marjorie Andres
Senior Midwife, NHS Ayrshire & Arran
Mr Robert Auld
Senior Anatomical Pathology Technician, NHS Ayrshire & Arran
Professor Jeanne E Bell
Professor of Neuropathology, NHS Lothian - University Hospitals Division
Dr Marjorie Black
Consultant Forensic Pathologist, University of Glasgow
Ms Hazel Brooke
Executive Director, Scottish Cot Death Trust, NHS Greater Glasgow - Yorkhill
Division
Ms Elaine Currie
National Chair, Stillbirth and Neonatal Death Society (SANDS)
Mr John Fegan
Member, Association for Children with Heart Disorders
The Very Reverend Graham J T Forbes
Board Member, NHS Quality Improvement Scotland
Professor Charles Gillis
Chairman, Multicentre Research Ethics Committee (MREC) for Scotland,
North Glasgow University Hospitals Division
Professor Barry Gusterson
Chairman of Joint NHS & University Department of Pathology,
University of Glasgow
Dr Alan Houston
Consultant Paediatric Cardiologist, Yorkhill Division
50 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the StandardsAppendix 3 – Management of Post-mortem Examinations Project Group Members
Dr Allan Howatson
Consultant Paediatric Pathologist, Yorkhill Division
Ms Rhona Jack
Portfolio Manager, Audit Scotland
Dr Aileen Keel
Deputy Chief Medical Officer, Scottish Executive Health Department
Dr Ian Laing
Consultant Neonatologist, NHS Lothian - University Hospitals Division
Ms Geraldine MacDonald
Chairperson, Scottish Organisation Relating to the Retention of Organs
Professor Alison MacLeod
Director of Research & Development, NHS Grampian
Mr Douglas McKay
Team Leader, Co-op Funeral Services
Dr Malcolm McWhirter
Director of Public Health, NHS Forth Valley
Dr Robert Nairn
Consultant Pathologist, NHS Ayrshire & Arran
Mr Will S Scott
Head of Branch, Scottish Executive Health Department
Mr John Service
District Procurator Fiscal, Dumfries & Galloway District
Support from NHS QIS was provided by Ms Jan Warner (Director of
Performance Assessment and Practice Development), Mr Steven Wilson
(Team Manager), Ms Morag Swankie (Senior Project Officer), Ms Sharon
Keane (Project Officer) and Mrs Lorraine Inglis (Project Administrator).
51 Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
3 Detailed Findings Against the Standards
51Local Report (Tayside Acute Services Division): Management of Post-mortem Examinations - February 2005
NHS Argyll & ClydeArgyll & Clyde Acute Hospitals NHS Trust 9 March 2004
NHS Ayrshire & ArranAyrshire & Arran Acute Hospitals NHS Trust 18 November 2003
NHS Borders 19 May 2004
NHS Dumfries & Galloway 23 March 2004
NHS FifeFife Acute Hospitals Division 5 May 2004
NHS Forth ValleyForth Valley Acute Hospitals NHS Trust 26 February 2004
NHS GrampianGrampian University Hospitals NHS Trust 12 November 2003
NHS Greater GlasgowNorth Glasgow University Hospitals NHS Trust 11 February 2004South Glasgow University Hospitals NHS Trust 28 January 2004 Yorkhill NHS Trust 2 December 2003
NHS HighlandHighland Acute Hospitals NHS Trust 18 December 2003
NHS Lanarkshire Lanarkshire Acute Hospitals NHS Trust 13 January 2004
NHS Lothian University Hospitals Division 7 April 2004West Lothian Healthcare Division 3 June 2004
NHS TaysideTayside Acute Services Division 21 April 2004
Appendix 4 — Timetable of Review Visits

NHS Quality Improvement Scotland
Edinburgh Office
Elliott House, 8-10 Hillside Crescent, Edinburgh, EH7 5EA
Phone 0131 623 4300
Glasgow Office
Delta House, 50 West Nile Street, Glasgow G1 2NP
Phone 0141 225 6999
[email protected] www.nhshealthquality.org
Copies of all NHS QIS publications can also be downloaded from the website
This document is produced from elemental chlorine-free material and is sourced from sustainable forests
You can read and download this document from our website. It can also be made available in:
• electronic format
• audio format
• large print
• Braille
• community languages