management of hbv in challenging populationshasld.org › images › gianhang › document ›...
TRANSCRIPT
Management of HBV in Challenging Populations
K. Rajender Reddy, M.D. Ruimy Family President’s Distinguished Professor in Medicine
Professor of Medicine in Surgery Director of Hepatology
Director, Viral Hepatitis Center Medical Director, Liver Transplantation
University of Pennsylvania
Chronic Hepatitis B in Special Populations
• Pregnancy
• HBV Reactivation

1. WHO. Hepatitis B. 2002. 2. Custer B, et al. J Clin Gastroenterol. 2004, 3. WHO/WPRO data.
HBsAg Prevalence (%)1
8: High
2–8: Intermediate <2: Low
Country HBsAg+ (%)
China 5.3-122
South Korea 2.6-5.12
Pakistan/
India 2.4-4.72
Taiwan 10-13.82
Vietnam 5.7-102
Japan 4.4-133
Africa 5-192
Russia 1.4-82
US/Europe 0.3-122
Geographic Distribution of Chronic HBV Infection

Chronic HBV Potential Mechanisms of MTCT
• Antenatal transmission (rare) – Trans placental
– Placental leakage/threatened abortion
– Amniocentesis
• Natal (predominant) – Vaginal exposure during delivery
• Postnatal – Breastfeeding: not a risk
YI S, J Hepatol 2014; 60: 523-9 Deng M, Virol J 2012;9:185
Rac MW, Obstet Gynecol Clin North Am 2014;41:573-92

Management of Mothers with HBV
• Many patients with CHB are immune tolerant when pregnant
• Mandatory testing of mothers for HBsAg
• HBIG for infants born to HBsAg positive mothers within 12-24 hours of birth
• HBV vaccine for all infants first dose, with subsequent vaccination at 1 and 3-6 months of age
– >95% of children then immune to HBV

Managing HBV in Pregnancy Differing Clinical Scenarios
• Pregnant and already on antiviral treatment
• Pregnant and not on treatment
– Potential risk of mother-to-child transmission
Unique clinical setting of balancing risks:
Mother Baby

Case
• 28 yr F who is pregnant, 12 weeks
• On treatment with entecavir 0.5 mg daily for 2 years for chronic HBV
• HBsAg +ve, HBeAg +ve, ALT 18
• HBV DNA undetectable
1. Stop HBV treatment because of risk to the baby?
2. Continue entecavir with no changes ?
3. Switch to tenofovir?
Options in Women on Treatment Who Become Pregnant
• Stop treatment and resume post-partum
– Risk of flare with treatment withdrawal
• Continue treatment but with full discussion of benefits and potential risks
– Change to drug with safety profile suitable for pregnancy

Safety of NA in Pregnancy and Breastfeeding
Drugs Pregnancy category
APR data* (Defects / live births)
Breast feeding
Lamivudine C 344 / 11,678 (2.9%) Biologically significant conc. in breast milk
Telbivudine B 0 / 20 No data
Tenofovir B 77 / 3,442 (2.2%) Significant conc. in breast milk (but poor oral bioavailability in infants)
Adefovir C 0 / 48 No data
Entecavir C 2 / 60 (3.3%) No data
CAT-C: Animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks CAT-B: Animal reproduction studies have failed to demonstrate a risk to the fetus and there are no adequate and well-controlled studies in pregnant women *Antiretroviral Registry: accessed April 2015

Safety of NA in Pregnancy and Breastfeeding
Drugs Pregnancy category
APR data* (Defects / live births)
Breast feeding
Lamivudine C 322 / 11,982 (2.7%) Biologically significant conc. in breast milk
Telbivudine B 0 / 18 No data
Tenofovir B 95 / 4,419 (2.2%) Significant conc. in breast milk (but poor oral bioavailability in infants)
Adefovir C 0 / 48 No data
Entecavir C 2 / 60 (3.3%) No data
CAT-C: Animal reproduction studies have shown an adverse effect on the fetus and there are no adequate and well-controlled studies in humans, but potential benefits may warrant use of the drug in pregnant women despite potential risks CAT-B: Animal reproduction studies have failed to demonstrate a risk to the fetus and there are no adequate and well-controlled studies in pregnant women *Antiretroviral Registry (exposure in the 1st-2nd trimester): Up to July 2016

Risk of Birth Defects Among Women Exposed to Antivirals During Pregnancy
1st Trimester 2nd/3rd Trimester
Registry Drugs # Live Births
Prevalence % (95% CI)
# Live Births
Prevalence (%) 95% CI
APR* (US)
All antivirals 5555 3.0 (2.5-3.4)
7483 2.7 (2.4-3.1)
Lamivudine 3864 3.1 (2.5-3.7)
6230 2.7 (2.3-3.1)
Tenofovir 1092 2.4 (1.6-3.5)
639 2.0 (1.1-3.5)
MACDP (European)
All antivirals
880 2.0 (1.2-3.2)
1765 1.2 (0.7-1.8)
UK/Ireland All antivirals
3190 3.0 (2.4-3.6)
7323 2.8 (2.4-3.2)
Brown R, J Hepatol 2012;57:953-9
*Antiretroviral Pregnancy Registry (www.APRegistry.com) Not significantly different for exposed women from unexposed
women: CDC population-based data: 2.72%, (2.68–2.76%)

Case
• 20 yr F who is pregnant with first child, 20 weeks
• HBsAg +ve, HBeAg +ve, ALT 12
• HBV DNA >108 log or 100 million copies/mL
1. Start HBV treatment now to prevent MTCT?
2. No need to treat during pregnancy as ALT normal?
3. Consider treatment 28-32 weeks if HBV DNA still elevated?
Treatment of Women in the Last Trimester of Pregnancy
• Rationale:
– Higher risk of prophylaxis failure in mothers with high levels of HBV DNA at delivery
– Prophylactic therapy of infants reduces risk of transmission
• Significant variability in delivery of immunoprophylaxis
• Issues: – Risks to infant – Risks to mother post-partum with drug withdrawal – Breastfeeding concerns

HBV: Mother-to-Child Transmission
• Risk Factors – HBeAg positive
– High HBV-DNA
– Aminocentesis
– Prolonged uterine contractions
– Threatened abortion
– Preterm Labor
HBV-DNA log copies/ml
8-10%
5
10
0
< 6 log
< 1%
3%
6-6.99 log 7-7.99 log ≥ 8 log
7-8%
Imm
un
op
rop
hyl
axis
fa
ilure
rat
e (
%)
Piratvisuth T. Liver Int 2013;33(S1):188-94 Zou H, et al. J Viral Hepatol 2012;19:e18-e25
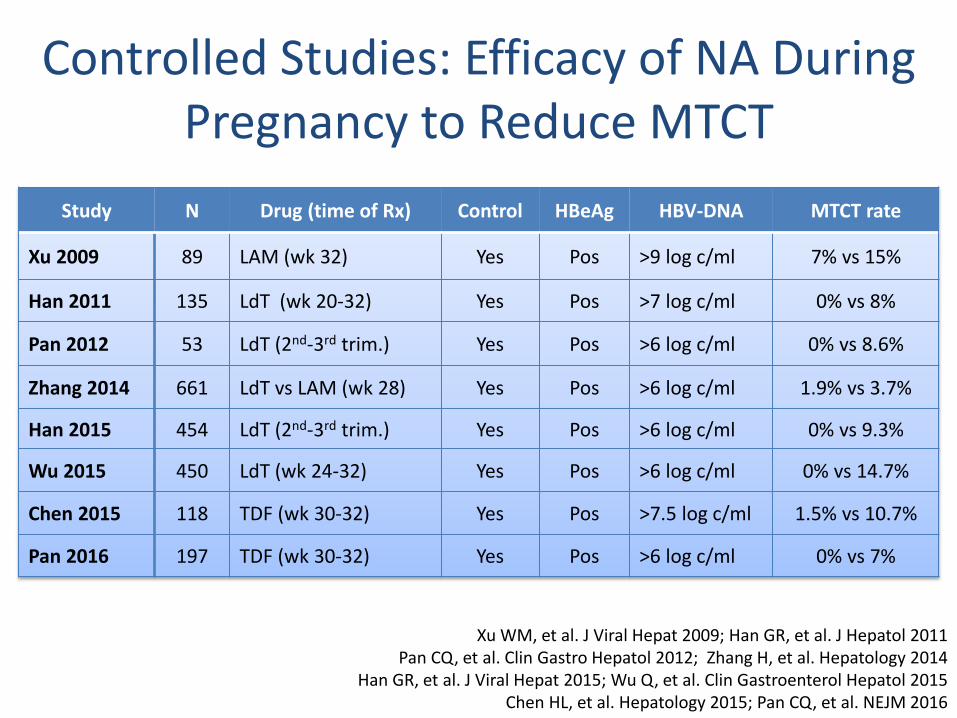
Controlled Studies: Efficacy of NA During Pregnancy to Reduce MTCT
Study N Drug (time of Rx) Control HBeAg HBV-DNA MTCT rate
Xu 2009 89 LAM (wk 32) Yes Pos >9 log c/ml 7% vs 15%
Han 2011 135 LdT (wk 20-32) Yes Pos >7 log c/ml 0% vs 8%
Pan 2012 53 LdT (2nd-3rd trim.) Yes Pos >6 log c/ml 0% vs 8.6%
Zhang 2014 661 LdT vs LAM (wk 28) Yes Pos >6 log c/ml 1.9% vs 3.7%
Han 2015 454 LdT (2nd-3rd trim.) Yes Pos >6 log c/ml 0% vs 9.3%
Wu 2015 450 LdT (wk 24-32) Yes Pos >6 log c/ml 0% vs 14.7%
Chen 2015 118 TDF (wk 30-32) Yes Pos >7.5 log c/ml 1.5% vs 10.7%
Pan 2016 197 TDF (wk 30-32) Yes Pos >6 log c/ml 0% vs 7%
Xu WM, et al. J Viral Hepat 2009; Han GR, et al. J Hepatol 2011 Pan CQ, et al. Clin Gastro Hepatol 2012; Zhang H, et al. Hepatology 2014
Han GR, et al. J Viral Hepat 2015; Wu Q, et al. Clin Gastroenterol Hepatol 2015 Chen HL, et al. Hepatology 2015; Pan CQ, et al. NEJM 2016

Systematic Review of Antiviral Therapy for Prevention of Perinatal Transmission
Outcome N RR 95% CI P Value
Infant HBsAg seropositivity at 6-12 months post-partum
737 (8 RCTs)
0.26 0.16-0.44 (P<0.05)
Infant HBsAg seropositivity at 6-12 months post-partum
1190 (5 observational
studies)
0.21 0.12-0.38 (P<0.05)
~75-80% reduction in risk of perinatal transmission with use of antiviral therapy
Brown R, Hepatology 2016;63(1):319-3
26 studies with a total of 3622 pregnant women were included in the analysis: 10 studies were RCTs and 16 studies were nonrandomized studies
Most of the studies (92%) were conducted in China, and none were conducted in the United States

Rationale:
– Higher risk of failure of prophylaxis in mothers with high levels of HBV
DNA at delivery – ~10% on average
– Risk of prophylaxis failures is related to HBV DNA level in mother at the
time of delivery
– Antiviral therapy could reduce HBV DNA levels to reduce risk of
prophylaxis failure
Treatment of Women in the Last Trimester of Pregnancy
AASLD HBV Treatment Guideline 2016 Hepatology 2016;63;261-83

Tenofovir for Prevention of MTCT of HBV
• RCT of N=200 women HBeAg and HBV DNA level >200,000 IU/mL
• 1:1 randomization to SOC (not antivirals) or TDF
• TDF 300 mg/day started 30-32 wks gestation postpartum wk 4
• Mean duration of TDF before delivery = 8.57±0.53 weeks
• All infants received vaccination and HBIG
Pan C, N Engl J Med 2016.

Timing of Antiviral Therapy to Prevent HBV Transmission
Treatment started Week 20-32 weeks
Han, GR. J Hepatol. 2011;55:1215-21
Treatment started Week 30-32 weeks
8.19
4.67 4.66
3.52
7.73
8.18 8.01
Pan C, N Engl J Med 2016;374:2324-34.
36%of women had HBV DNA >200,000 IU/mL Average 8.6 weeks therapy
6% of women had HBV DNA >1,000,000 IU/mL Average 11.4 weeks therapy
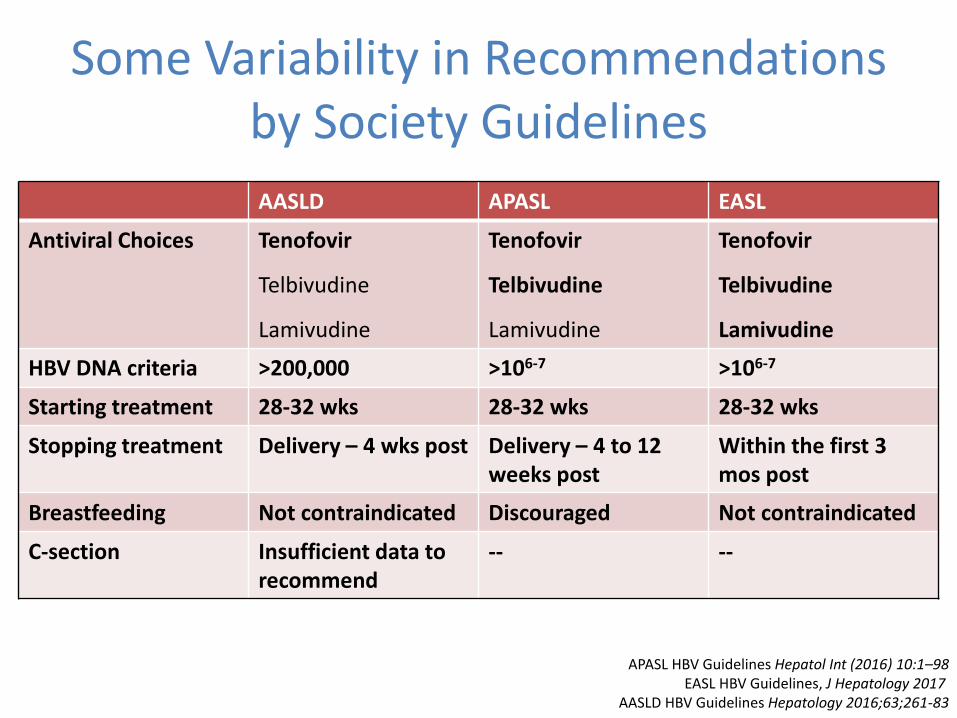
Some Variability in Recommendations by Society Guidelines
AASLD APASL EASL
Antiviral Choices Tenofovir
Telbivudine
Lamivudine
Tenofovir
Telbivudine
Lamivudine
Tenofovir
Telbivudine
Lamivudine
HBV DNA criteria >200,000 >106-7 >106-7
Starting treatment 28-32 wks 28-32 wks 28-32 wks
Stopping treatment Delivery – 4 wks post Delivery – 4 to 12 weeks post
Within the first 3 mos post
Breastfeeding Not contraindicated Discouraged Not contraindicated
C-section Insufficient data to recommend
-- --
APASL HBV Guidelines Hepatol Int (2016) 10:1–98 EASL HBV Guidelines, J Hepatology 2017
AASLD HBV Guidelines Hepatology 2016;63;261-83

C-Section vs Vaginal Delivery?
Chang M, Can J Gastroenterol Hepatol, 2014
N= 10 studies: n=2352 C-section compared with n=2739 vaginal delivery
But …. minimal benefit if use infant HBIG prophylaxis plus treatment of high viremia mothers
Insufficient evidence to recommend
What is the Risk to the Mother with Stopping Antivirals Post-Partum?
• ALT “flares” frequent post-partum
– Up to 45% of women
– Not predicted by HBV DNA level or HBeAg status
• ALT flares may be more frequent in women receiving 3rd trimester antivirals, but ALT >10 times ULN rare
– Most women are in immune tolerant phase low fibrosis
Tagawa et al, Nippon Sanka Fujinka Gakkar Zasshi, 1987 Soderstrom et al, Scand J Inf Dis, 2003
Ter Borg et al, J Viral Hepatitis 2008 Zhang H et al, Hepatology, 2014
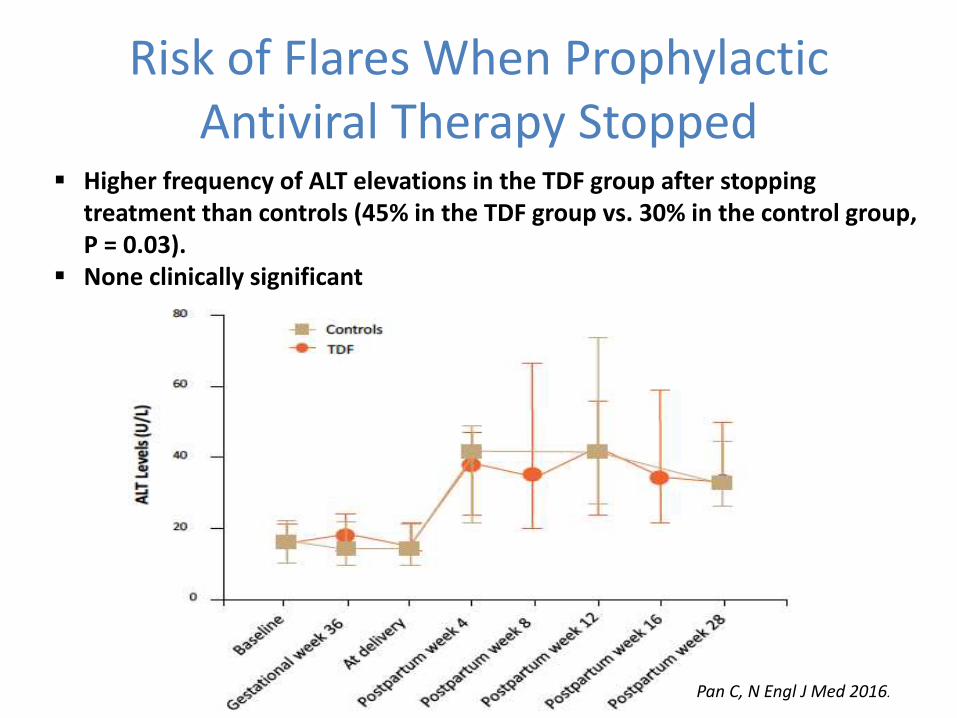
Risk of Flares When Prophylactic Antiviral Therapy Stopped
Higher frequency of ALT elevations in the TDF group after stopping treatment than controls (45% in the TDF group vs. 30% in the control group, P = 0.03).
None clinically significant
Pan C, N Engl J Med 2016.

Suggested Management of HBsAg-Positive Women During Pregnancy
- Continue antiviral therapy post partum
- Breastfeeding not contraindicated
- Discontinue antivirals at delivery or up to 3 months post-partum
- Breastfeeding not contraindicated
* TDF is preferred drug. Initiate therapy ≤28 wks if HBV VL very high to allow time for viral load reduction to <200,000 IU/mL

Treatment of HBV in Pregnancy Summary
HBIG plus vaccination remains the mainstay of prevention of perinatal transmission High maternal viremia increases risk of transmission despite
immunoprophylaxis
Treatment in the 3rd trimester (starting 28-32 weeks of gestation) reduces the risk of perinatal transmission
Tenofovir, telbivudine and lamivudine are options Tenofovir preferred due to minimal risk of resistance
Breastfeeding is not contraindicated on therapy
C-section in those with HBV diagnosis is not indicated

Chronic Hepatitis B in Special Populations
• Pregnancy
• HBV Reactivation

HBV Reactivation (HBVr): Overview • Clinical syndrome characterized by an increase in HBV DNA and
ALT/AST with or without symptoms or jaundice
• Occurs in pts with active (HBsAg+) and resolved/occult (HBsAg-, anti-HBc+) HBV infection
• Wide clinical spectrum for HBVr
– Ranges from silent to liver failure
• Can occur during treatment with many immunosuppressive agents, DAA, HIV, organ transplant
– May also occur up to 12 months after event or treatment
• Preventable by antiviral prophylaxis
Di Bisceglie AM, et al. Hepatology. 2015;61:703-711.
Perrillo RP, et al. Gastroenterology. 2015;148:221-244.

Definitions
• Virologic increase of 1 log IU/ml or de novo appearance of HBV DNA when previously non detectable
Proposed: 2 log increase or de novo or reappearance of HBV DNA to a level of at least 100 IU/mL (AASLD Emerging Trends Conference on HBV Reactivation, March, 2013)
In absence of HBV DNA measurements, reappearance of
HBeAg or HBsAg is reasonable evidence • Increase of 3 fold or greater in ALT levels if BSL levels
normal or 2 fold or greater increase over BSL if initially abnormal.

Case
• 60 yr Asian male with diagnosis of NHL • Plan is to start R-CHOP • HBsAg -ve, HBcAb +ve, HBsAb -ve
1. Start HBV prophylaxis before starting
chemotherapy? 2. No need to treat during chemotherapy as risk is
low ? 3. Consider treatment 28-32 weeks if HBV DNA still
elevated?

Weeks after Exposure
0 4 8 12 16 20 24 28 32 36 52 100
ChemoRx and/or
Steroids Or HCV DAAs
Or Liver SOT
HBV DNA
IMMUNE change or
SUPPRESSION RECOVER
Acute hepatitis
ALT
IMMUNE REBOUND
Recovery of neutropenia or
steroid withdrawal
Natural History of HBV Reactivation During Chemotherapy
Acute liver failure
Death
Chronic hepatitis
Cirrhosis
Liver Transplant
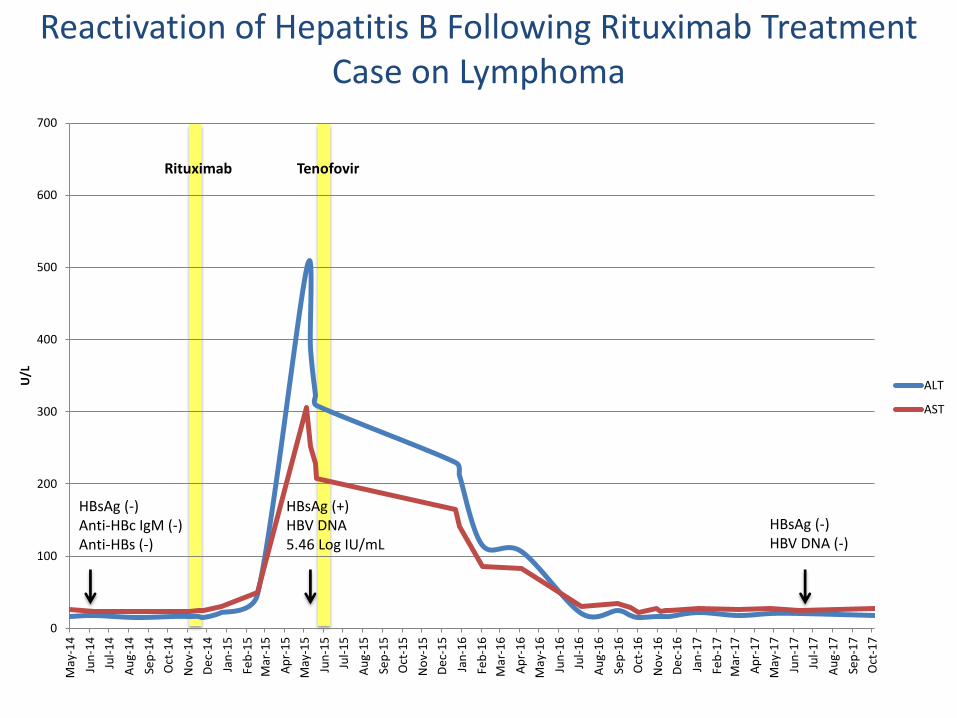
Reactivation of Hepatitis B Following Rituximab Treatment Case on Lymphoma
Rituximab Tenofovir
HBsAg (-) Anti-HBc IgM (-) Anti-HBs (-)
HBsAg (-) HBV DNA (-)
HBsAg (+) HBV DNA 5.46 Log IU/mL
0
100
200
300
400
500
600
700
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
De
c-1
4
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
Jun
-15
Jul-
15
Au
g-1
5
Sep
-15
Oct
-15
No
v-1
5
De
c-1
5
Jan
-16
Feb
-16
Mar
-16
Ap
r-1
6
May
-16
Jun
-16
Jul-
16
Au
g-1
6
Sep
-16
Oct
-16
No
v-1
6
De
c-1
6
Jan
-17
Feb
-17
Mar
-17
Ap
r-1
7
May
-17
Jun
-17
Jul-
17
Au
g-1
7
Sep
-17
Oct
-17
U/L
ALT
AST

Case: 55-Yr-Old Chinese Woman With Stage II Breast Cancer
• Treated with doxorubicin, paclitaxel, dexamethasone, and cyclophosphamide
ALT
Total bilirubin
20
15
10
5
0
4000
3000
2000
1000
0 0 20 40 60 80
Days Following Initiation of Chemotherapy
Tota
l Biliru
bin
(mg/d
L)
Seru
m A
LT
(IU
/L)
Pt dies
Entecavir
initiated
Chemotherapy
discontinued
First abnormal ALT
Courtesy of Dr. Perrillo

HBV may reactivate in anyone who is Anti-HBc+
HBsAg Anti-HBc total
Anti-HBs Anti-HBc IgM
What it means
_ _ _ _ Never exposed
_ _ + _ Vaccinated
_ + + _
Chronic HBV + + _ _
Exposure, Occult, Cleared disease “Isolated core”
_ _ _ _
_ + _ _
+ + _ + Acute HBV
(rare during active/chronic disease)
A
B
C
D
E
F
Exposure, Occult, Cleared disease

Immunosuppressive Therapy (IST) Reported to Cause HBV Reactivation
Immunoodulatory Therapy
Anti-TNF
(Infliximab, adalimumab, etanercept)
Anti-Metabolite (Methotrexate)
Purine Analogues (Azathioprine/6MP)
Steroids (Prednisone, budesonide)
Other
(Rituximab, cyclosporine)

Loomba R, Liang JT Gastroenterology 2017:152;1297-09
HBV lifecycle and targets for Immunosuppressive therapy

High risk for HBVr (>10%)
B-cell depleting agents (rituximab, ofatumumab)
HBsAg + core +
30 – 60%
HBsAg - core +
17%
Anthracycline derivatives (e.g.,doxorubin / epirubicin)
15 – 30%
Categories of confidence in the estimate: (A) High confidence that the estimate lies within group risk boundaries (B) Moderate confidence that the estimate lies within group risk boundaries (C) Little or no confidence that the estimate lies within group risk boundaries
Corticosteroids for > 4 wks (> 10 mg prednisone)
> 10%
Confidence in estimate
A
A
B

Moderate risk (1% - 10%)
TNF-alpha inhibitors (etanercept, adalimumab, certolizimab, infliximab)
HBsAg + core +
1 – 10% (B)
Other cytokine & integrin inhib. (abatacept, ustekinimab, natalizumab, vedolizumab)
1 – 10% (C)
Corticosteroids for > 4 weeks 1 – 10% (B) (low dose: <10 mg)
Tyrosine kinase inhibitors (imatinib, nilotinib)
1 – 10% (B)
HBsAg - core +
1% (C)
1% (C)
1% (C)
1 – 10% (C) (>10 mg)
Anthracycline derivatives (e.g.,doxorubin / epirubicin)
1% (C)

Low risk group (<1%)
Traditional immunsupp. agents (azathioprine, 6-mercaptopurin, methotrexate alone)
HBsAg + core +
<1% (A)
Intra-articular corticosteroid <1% (A)
Corticosteroids for > 4 weeks
Corticosteroids for ≤ 1 week <1% (B)
HBsAg - core +
<<1% (A)
<<1% (A)
<<1% (A)
<1% (B) (low dose: <10 mg)
Categories of confidence in the estimate: (A) High confidence that the estimate lies within group risk boundaries (B) Moderate confidence that the estimate lies within group risk boundaries (C) Little or no confidence that the estimate lies within group risk boundaries

High Risk of Reactivation
with Hematologic Malignancy
48
22
4 4
0
20
40
60
80
100
% o
f H
BsA
g P
ati
en
ts
HBV Reactivation
Jaundice Non-Fatal Liver Failure
Death
100 patients with NHL undergoing CHOP 27 HBsAg +ve
Lok et al, 1991

HBV Reactivation With Rituximab in Pts With Hematologic
Malignancies
• Single-center study of HBsAg-
negative anti-HBc–positive pts
receiving rituximab-containing
chemotherapy (N = 62)
– Baseline HBV DNA
undetectable (< 10 IU/mL)
– No previous HBV treatment
– No chronic liver disease
• 24.2% of patients experienced
HBV reactivation within 9 months
– Reactivation occurred early
(86.7% within 6 months)
• Lower baseline anti-HBs levels associated with subsequent HBV reactivation (P = .015)
Seto WK, et al. 2014.
HBV Reactivation
No HBV Reactivation
100
75
50
25
0
Pa
tie
nts
(%
)
P = .015 Anti-HBs Levels, mIU/mL
≥ 300
100 - < 300
10 - < 100
< 10

Rituximab-Associated HBV Reactivation
in Lymphoproliferative Disorders
• Meta-analysis and review of FDA
safety profiles
– Case reports (n=27)
– Case series reports (n=156)
• Onset post last rituximab dose
– Median: 3 months (range: 0-12
months)
– >6 months: 29%
• Reactivation in anti-HBc positive
patients receiving rituximab
versus no rituximab
– Odds ratio: 5.73 (P=0.0009)
Evens AM, et al. Ann Oncol. 22:1170-1180, 2011
Hui (n=233)
Tsutsumi
(n=47)
Targhetta (n=319)
Yeo
(n=50)
Fukushima (n=48)
Overall (n=697)
HBV Reactivation Risk:
Rituximab-Treated Lymphoma Patients
0.32 1.0 3.16 31.62
Odds Ratio
12.44
5.24
3.38
9.39
1.60
5.64
(2.18-14.54)

Anti-TNF Agents and HBV Reactivation
Disease Studied
No. Patients
HBsAg + HBcAb +
HBsAg – Anti-HBc +
Multiple 257 39% 5%
IBD 88 9/25 (36%) 0%
Rheumatologic 122 12% N/A
Rheumatologic 468 N/A 2%
• TNF-a: proinflammatory cytokine that inhibits HBV replication • Anti-TNF agents associated with HBV reactivation
• Utilized in IBD, psoriasis, rheumatoid arthritis
Perez-Alvarez et al, 2011; Loras et al, 2010; Lee et al, 2013; Lee et al, 2013;
• Antiviral prophylaxis warranted for all HBsAg+ on TNFi • Low risk of HBVr in anti-HBc + only
• Consider monitoring for HBVr • Higher risk may be associated with addition of other IST

Bone Marrow Transplantation: Increased Risk of Reactivation
• Markedly increased rate of reactivation (HBsAg +ve)
– Up to 75%1
– Long-term complications: cirrhosis 10%2
• Reverse seroconversion common if anti-HBc +ve
– Up to 50% become HBsAg +ve3
– May occur very late
1 Lau BMT 1997, 2 Hui Blood 2005, 3 Onozawa Transplantation 2005

Value of Pre-Emptive Antivirals
48
8
36
0
20
0 08
0
20
40
60
80
100
% o
f H
BsA
g P
ati
en
ts
On-Demand Pre-emptive
• Pre-emptive group - start LAM 1 day prior to CHOP
• On-demand - start LAM if ALT>1.5 x ULN
Hepatitis Flare Jaundice
ALT >10xULN
Death (after chemoTx)
Pre-emptive antivirals decrease HBV reactivation
HBsAg +ve pts with NHL treated with CHOP
Randomized ‘Pre-emptive’ vs ‘On-Demand’ Lamivudine
Meta-analysis shows survival benefit to this approach - Loomba Ann Int Med 2008
Hsu et al Hepatology 2008; Lau et al Gastroenterology 2003

Randomized, Controlled Trials of HBV Prophylaxis
P = .001
70
60
40
20
0
50
30
10
HB
V R
eactivation (
%)
Lymphoma,
HBsAg+
(N = 30)
HCC,
HBV DNA+
(N = 76)
Lymphoma,
HBsAg+
(N = 52)
Breast
Cancer,
HBsAg+
(N = 42)
Lymphoma,
HBsAg-
Anti-HBc+
(N = 80)
Lymphoma,
HBsAg-
Anti-HBc+
(N = 30)
Lymphoma,
HBsAg+
(N = 121)
Control
Lamivudine
Control
Entecavir
Control
Tenofovir
Lamivudine
Entecavir
53
P = .002
0 0 0
P < .001 P = .001
P = .02
P = .03 P = NS
41
3
12
56
29
18
2
17
30
7
Perrillo RP, et al. Gastroenterology. 2015;148:221-244.

Choosing an Antiviral for HBV Prophylaxis
• Drugs with high genetic barrier to resistance (tenofovir, entecavir) preferred[1]
• Lamivudine associated with resistance[1]
– Entecavir prophylaxis associated with a significantly lower incidence of HBV reactivation vs lamivudine in randomized controlled trial[2]
• Adefovir less potent than tenofovir for treating HBV[3]
• Lamivudine plus adefovir may be an option[4]
1. Reddy KR, et al. Gastroenterology. 2015;148:215-219. 2. Huang H, et al. JAMA. 2014;312:2521-2530.
3. Marcellin P, et al. N Engl J Med. 2008;359:2442-2455. 4. Vassiliadis TG, et al. J Gastroenterol Hepatol.
2010;25:54-60.

AGA Institute Guidelines on Hepatitis B Reactivation ( HBVr) Clinical Decision Support Tool
High Risk (reactivation risk > 10%)
HBsAg-positive/anti-HBc-positive or HBsAg-negative/anti-HBc-
positive
Patients taking B cell depleting agents (e.g.,
rituximab, ofatumumab)
Patients taking anthracycline derivatives (e.g., doxorubicin,
epirubicin)
GRADE – Strong Recommendation, moderate quality of evidence.
Antiviral prophylaxis for at least 12 months after
discontinuation of immunosuppressive therapy
Antiviral prophylaxis for at least 6 months after discontinuation of immunosuppressive therapy
HBsAg-positive/anti-HBc-positive
Patients taking moderate dose ( 10-20 mg prednisone daily or
equivalent ) or high dose ( > 20 mg prednisone daily or equivalent)
corticosteroids daily for ≥4 weeks
Reddy KR et al Gastroenterology 2015 ;148(1):215-9

Moderate Risk (reactivation risk 1-10%)
Patients taking TNF alpha inhibitors
(e.g., etanercept, adalimumab, certolizumab,
infliximab)
Patients taking moderate dose ( 10-20 mg prednisone daily or equivalent ) or high
dose ( > 20 mg prednisone daily or equivalent) corticosteroids daily for ≥4
weeks. Patients taking anthracycline derivatives (e.g., doxorubicin, epirubicin)
Patients taking other cytokine or integrin
inhibitors (e.g., abatacept,
ustekinumab, natalizumab, vedolizumab)
GRADE – Weak Recommendation, moderate quality of evidence
Suggest antiviral prophylaxis for at least 6 months after discontinuation of immunosuppressive therapy*
AGA Institute Guidelines on Hepatitis B Reactivation ( HBVr) Clinical Decision Support Tool
* Patients who place a higher value on avoiding the long-term use of antiviral therapy and cost associated with its use and a lower value on avoiding the small risk of reactivation (particularly in those who are HBsAg-negative), may reasonably select no prophylaxis over antiviral prophylaxis
HBsAg-positive/anti-HBc-positive or HBsAg-negative/anti-HBc-positive
HBsAg-negative/anti-HBc-positive
Patients taking tyrosine kinase inhibitors (e.g.,
imatinib, nilotinib )
HBsAg-positive/ anti-HBc-positive
Patient taking low-dose ( < 10 mg prednisone daily
or equivalent) corticosteroids daily for
duration of ≥4 weeks
Reddy KR et al Gastroenterology 2015 ;148(1):215-9

Low Risk (reactivation risk <1%)
HBsAg-positive/anti-HBc-positive or HBsAg-negative/anti-HBc-positive
Patients taking traditional immunosuppressive agents
(e.g., azathioprine, 6-mercaptopurine, methotrexate)
Patients taking low dose ( < 10 mg prednisone or equivalent) corticosteroids for ≥ 4 weeks
Patients taking intra-articular corticosteroids.
Patients taking any dose oral corticosteroids daily for duration of
≤ 1 week
GRADE – Weak Recommendation Moderate quality of evidence
Suggest not to use routine antiviral prophylaxis in patients undergoing immunosuppressive drug therapy and are at low risk for HBVr
AGA Institute Guidelines on Hepatitis B Reactivation ( HBVr) Clinical Decision Support Tool
HBsAg-negative/anti-HBc-positive
Reddy KR et al Gastroenterology 2015 ;148(1):215-9

HBV Reactivation Associated with DAA Therapy for HCV
• Case reports of 2 patients:
• Flare of HBV temporally related to initiation of SOF/SMV
• 2 additional cases of ALF in anti-HBc-positive patient on antiviral therapy
Ende et al, 2015; Collins et al, 2015; DeMonte et al, 2016
HBsAg+ HBcAb + only

Safety WARNING: HBV Reactivation and DAAs October, 2016
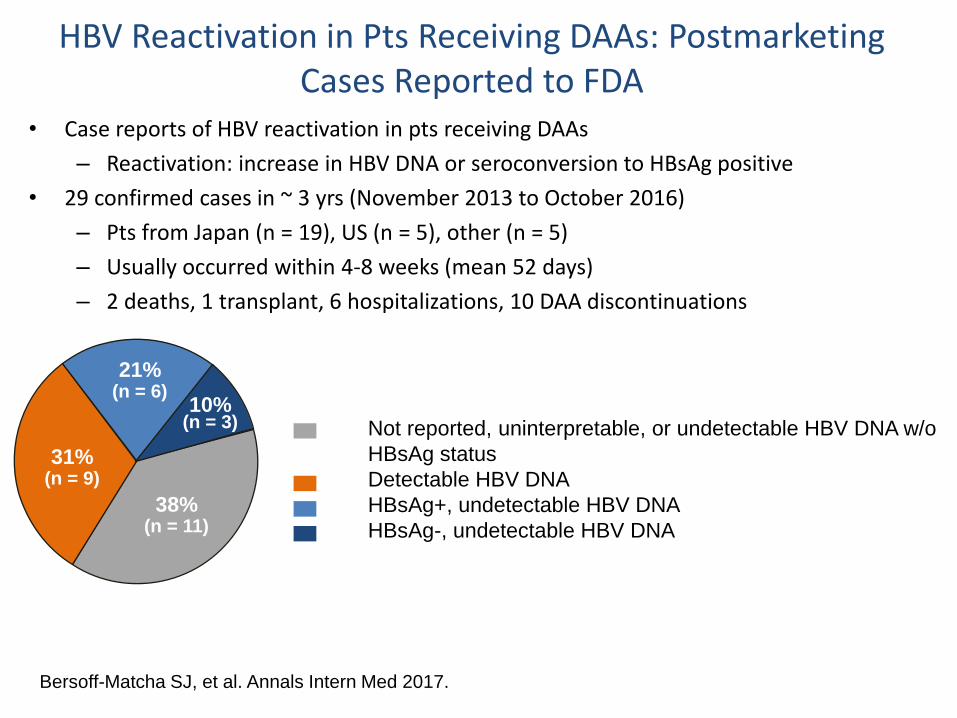
HBV Reactivation in Pts Receiving DAAs: Postmarketing Cases Reported to FDA
• Case reports of HBV reactivation in pts receiving DAAs
– Reactivation: increase in HBV DNA or seroconversion to HBsAg positive
• 29 confirmed cases in ~ 3 yrs (November 2013 to October 2016)
– Pts from Japan (n = 19), US (n = 5), other (n = 5)
– Usually occurred within 4-8 weeks (mean 52 days)
– 2 deaths, 1 transplant, 6 hospitalizations, 10 DAA discontinuations
Bersoff-Matcha SJ, et al. Annals Intern Med 2017.
HBV Reactivation (N = 29)
Not reported, uninterpretable, or undetectable HBV DNA w/o
HBsAg status
Detectable HBV DNA
HBsAg+, undetectable HBV DNA
HBsAg-, undetectable HBV DNA
31% (n = 9)
38% (n = 11)
21% (n = 6)
10% (n = 3)

FDA Recommendations for Monitoring During DAA Therapy
• To decrease the risk of HBV reactivation in patients co-infected with HBV and HCV, health care professionals should:
• • Screen all patients for evidence of current or prior HBV infection before initiating treatment with DAAs by measuring HBsAg and anti-HBc. In patients with serologic evidence of HBV infection, measure baseline HBV DNA prior to DAA treatment.
• Monitor patients who show evidence of current or prior HBV infection for clinical and laboratory signs (i.e., HBsAg, HBV DNA, serum aminotransferase levels, bilirubin) of hepatitis flare or HBV reactivation during DAA treatment and post- treatment follow-up.
• Consult a physician with expertise in managing hepatitis B regarding the monitoring and consideration for HBV antiviral treatment in HCV/HBV co- infected patients.

Jan 2014-Sept 2016 62,290 Veterans completed DAA
HCV therapy
85.5% (53,784/62,920) had HBsAg Test
0.70% (377/53,784)
were HBsAg (+)
84.6% (53,237/62,920) had anti-HBs test
42.2% (22,479/53,237)
were anti-HBs (+)
64.2% (40,383/62,920)
had anti-HBc test
45.7% (18,462/40,383)
were anti-HBc (+)
39.5% (7,295/18,462)
were isolated anti-HBc (+)
Reactivation in 9 cases
8 in HBsAg (+)
1 in anti-HBc alone (+)
Defined reactivation as >1000 IU/ml increase in HBV DNA or HBsAg detection in previously (-)ve case
Evaluation of Hep B Reactivation Among Veterans Treated with Oral Hep C Antivirals
Belperio, P. et al. Hepatology 2017;66:27-36

AASLD Guidance on HBV Reactivation in Pts Receiving HCV DAA Therapy
• HBV vaccination recommended for all susceptible individuals (eg, no previous immunization, no evidence of immunization response, anti-HBc (-)
• All pts starting HCV DAA therapy should be assessed for HBV infection (HBsAg, anti-HBs, and anti-HBc testing)
– If HBsAg+, assess HBV DNA prior to, during, and immediately after HCV DAA therapy
• For active HBV infection, initiate HBV therapy before or simultaneously with HCV DAA therapy
• For low or undetectable HBV DNA, monitor for HBV reactivation during HCV DAA therapy
– Insufficient data to provide recommendations for pts who are HBsAg- and anti-HBc+ or anti-HBs+/anti-HBc+
AASLD/IDSA HCV Guidelines. September 2016.
Summary-HBVr
• ALL patients undergoing chemotherapy should be tested for HBsAg, HBsAb and HBcAb
• All patients who are HBsAg+ should receive prophylaxis prior to chemotherapy – in select cases anti-HBc alone is an indication for
prophylaxis
• Rituximab use and in those with Stem cell transplant: all patients with current or past HBV should receive prophylaxis.
• HBV reactivation on DAA therapy is rare - reactivation in anti-HBc alone cases is even rarer and controversial