management of fever in a paediatric oncology patient · 2018-11-17 · fever in children with...
TRANSCRIPT
Management of Fever in a Paediatric Oncology Patient
Febrile Neutropaenia and Febrile Non-neutropaenia
Document ID CHQ-GDL-01249 Version no. 1.0 Approval date 08/02/2018
Executive sponsor Executive Director Medical Services Effective date 08/02/2018
Author/custodian Director Paediatric Oncology Review date 08/02/2020
Supercedes QPHON Management of Fever in the Neutropenic Paediatric Oncology patient QPHON Management of Paediatric Non-Neutropenic Oncology patient with Fever
Applicable to All CHQ staff
Authorisation Executive Director Clinical Services LCCH
Purpose
This guideline provides a framework for the treatment of children with cancer and fever from presentation to resolution. Pathways are provided for those with suspected neutropaenia and those with known non- neutropaenia at presentation.
Scope
This guideline applies to staff caring for children with cancer in CHQ HHS and can be used by the Queensland Paediatric Palliative care Haematology Oncology Network and other State-wide services.
Contents
Febrile Neutropaenia Definition. Page 1
Initial Management of Suspected Febrile Neutropaenia. Page 1
Antibiotic allergy alternatives. Page 5
Ongoing Management of Febrile Neutropaenia. Page 6
Febrile Neutropaenia Antibiotic Algorithm. Page 9
Febrile Non Neutropaenia Antibiotic Algorithm. Page 10
Exclusion criteria for outpatient management. Page 11
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 2 -
Febrile Neutropaenia follow on management algorithm. Page 12
Risk of serious bacterial infection. Appendix 1. Page 15
High Risk Disease. Appendix 2. Page 15
Normal Range for age specific signs. Table 1. Page 16
Related documents
Policy and standard(s)
• CHQ Nursing standard 03453 IVAD - Central Venous Catheters Nursing Care and Management of Tunnelled (cuffed and non-cuffed) CVC in Paediatric Patients (QH staff only)
• CHQ Nursing standard 03454 IVAD - Venous Port Device: Nursing Care and Management of Totally Implanted Venous Port Device (Port) in Paediatric Patients (QH staff only)
Procedures, Guidelines, Protocols
• CHQ Procedure 03450 Intravascular Access Device Management of (Peripheral and Central Venous Access Devices) (QH staff only)
• CHQ Procedure 01036 Antimicrobial: Prescribing and Management (QH staff only)
• CHQ Procedure 01000 Medication (QH staff only)
• CHQ Procedure 01001 CHQ Procedure 01001: Medication - Prescribing (QH staff only)
• CHQ Guideline Antifungal Prophylaxis and Treatment in Paediatric Oncology and Immunocompromised (QH staff only)
• CHQ Guideline 01202 CHQ Paediatric Antibiocard: Empirical Antibiotic Guidelines (QH staff only)
• CHQ Guideline 07449 Sepsis: Recognition and Early Management in Children (QH staff only)
Forms and templates
• CHQ Clinical Pathway Clinical Pathway: Initial Management of Suspected Neutropaenic Sepsis (QH staff only)
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 3 -
Guideline
Febrile Neutropaenia (FN) Definition
Fever: > 38.50 C on one occasion or
> 38.00 C on two occasions – at least one hour apart WITH EITHER
o Neutropaenia: a neutrophil count of <1 x 109/L ORo Recent Intensive Chemotherapy (within last 14 days) where neutropaenia is expected
Fever in children with cancer is a medical emergency as they are at increased risk of developing severe sepsis and septic shock, and may progress from fever to severe sepsis rapidly. Fever may be the only sign of underlying infection and children presenting with fever should be rapidly triaged (minimum Cat 2). Fever in a child with cancer or chemotherapy/treatment induced neutropaenia is known as Febrile Neutropaenia (FN). Neutropaenia must be suspected in any oncology patient that has received chemotherapy within the last 10 - 14 days. Neutropaenia in CHQ is defined as a neutrophil count of <1 x 109/L.
Antibiotics given within 60 minutes of presentation improve outcomes and decrease the need for admission to PICU (1, 2). These children can deteriorate rapidly and progress to septic shock if not managed appropriately.
ALERT DO NOT wait for blood results before initiating treatment.
Antibiotics should be given within 60 minutes of presentation (or fever spike if inpatient) Antibiotics MUST be commenced after blood cultures but before undertaking other investigations (e.g. CXR, NPA)
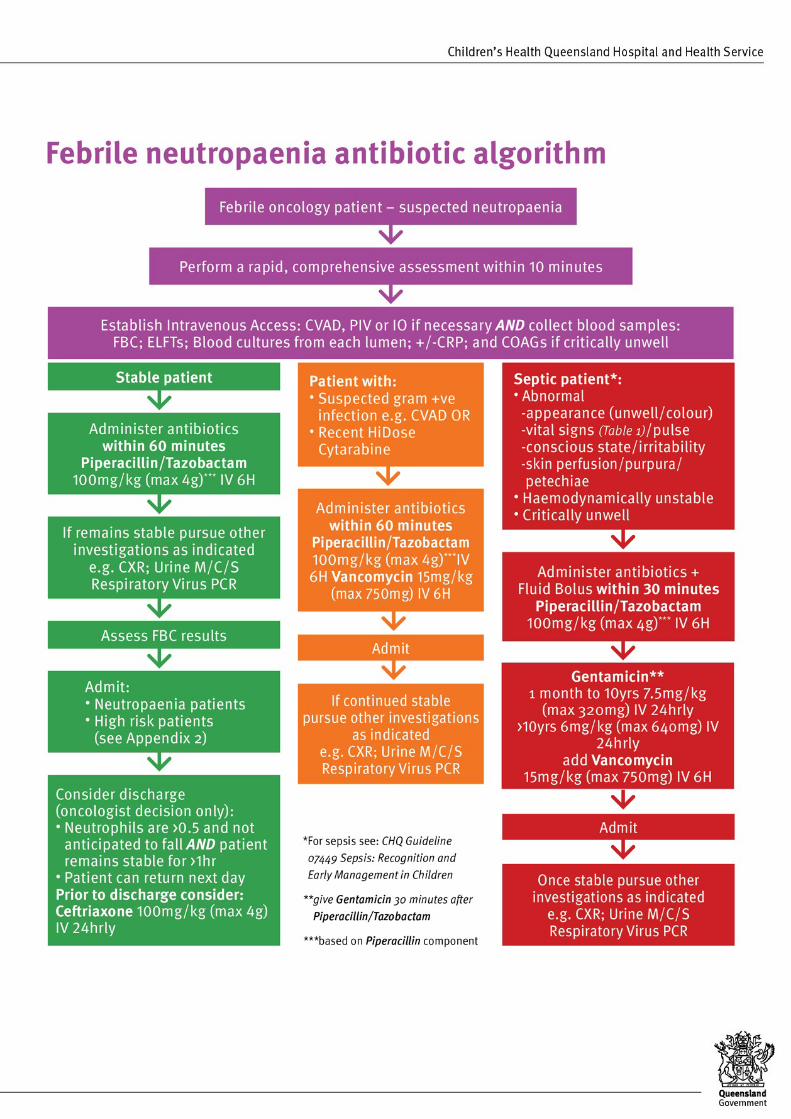
Initial Management of Suspected Febrile Neutropaenia Follow the Febrile Neutropaenia antibiotic algorithm (Page 9) unless neutrophil count is known to be > 1.0, then follow the Non Neutropaenic Flow chart (Page 10).Complete the Clinical Pathway: Initial Management of Suspected Neutropaenic Sepsis (QH staff only) if available.
Triage (if presentation through Emergency Department):
• Triage as minimum Australasian Triage Scale (ATS) 2
Initial Management:
• Comprehensive patient assessment should be performed within 10 minutes of presentation
• Haemodynamically unstable or critically unwell
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 4 -
ABCD management, including fluid bolus (20ml/kg) and oxygen therapy as required.
Refer to CHQ Guideline 07449 Sepsis: Recognition and Early Management in Children (QH staff only) Intravenous Access:
• Immediately establish intravenous (IV) access - use central venous access device (CVAD) as firstoption,
Insert peripheral line (PIV) if CVAD competent staff unavailable
Do not wait for topical anaesthetic
Intraosseous access may be required if there are no other options.
Primary Investigations:
• Collect blood samples - Full Blood Count, Blood Cultures from each lumen of CVAD (peripheral bloodcultures NOT required), and ELFTs (Collect COAG’s only if critically unwell)
Antibiotic Management:
ALERT
Do not delay antibiotic administration whilst waiting for blood results If CVAD in-situ and patent, give IV antibiotics through CVAD, not peripherally
• Commence antibiotics as below and commence intravenous (IV) fluids if clinically indicated
• Piperacillin/tazobactam has both gram negative and gram positive cover and is an effective empirictreatment for most common gram positive infections including S.aureus (MSSA). Exceptions includeenterococcus, coagulase negative staphylococcus, penicillin resistant S.mitis
Dose = 100mg/kg (of piperacillin component) IV 6H (maximum 4000mg Piperacillincomponent per dose)
Administer undiluted (200mg/mL of piperacillin component) as an IV bolus over 3-5minutes via CVAD (can be diluted to 20mg/mL of piperacillin component for infusion over20 minutes via peripheral IV)
If septic, critically unwell or haemodynamically unstable (see Febrile Neutropaenia Antibiotic Algorithm, Page 9) add Gentamicin and Vancomycin as below.
• Gentamicin provides additional gram negative cover including pseudomonas
Dose = 1mth to <10years: 7.5mg/kg every 24 hrs (max 320mg); >10years: 6mg/kg every 24 hrs (max 640mg) (Note: PICU sepsis dosing for gentamicin >10years is 7mg/kg every 24 hrs (max initial dose 640mg) and this dose may be used if septic shock requiring PICU)
Wait 30 minutes after Piperacillin/Tazobactam dose prior to administering the Gentamicin
Infuse IV Gentamicin dose in total volume of 30mL (in sodium chloride 0.9%) over 30 minutes
Document time of administration – may need levels taken at 2 hours and 6 hours after the dose (timed from start of infusion). Please refer to the Tobramycin/Gentamicin Therapeutic Drug Monitoring Guideline (QH staff only)
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 5 -
• Vancomycin provides additional gram positive cover, including MRSA, penicillin resistant S.mitis andcoagulase negative staphylococcus. Add for patients treated with high dose cytarabine (HD ARA C)who have high risk of S.mitis, suspected CVAD infection or MRSA.
Dose = 15mg/kg (max dose 750mg) every 6 hrs (perform therapeutic drug monitoring –Vancomycin trough level 30 minutes before 4th or 5th dose)
Administer once flush following Gentamicin is complete
Dilute to 5mg/mL or less and infuse over 120 minutes (2 hours)
Patients with documented previous Red Man syndrome will require prolonged infusion
Routine addition of vancomycin to the initial empiric regimen within 72 hours does not reduce mortality or time to defervescence and is associated with increased nephrotoxicity
ALERT
All changes to antibiotics need to be discussed with the on-call LCCH Paediatric Oncologist
Special considerations:
• Beta lactam delayed hypersensitivity – Use Ceftazidime (50mg/kg/dose IV every 8 hours (max 2 grams/dose)) and single dose of Gentamicin (as above)
• Beta lactam anaphylaxis – Use Meropenem (40mg/kg/dose IV every 8 hours (max 2 gram/dose))(see ALERT below)
• Antibiotic approvals are required for restricted antibiotic use outside stated protocol. Please refer to the Medication approval process (QH staff only) and the Individual Patient Request form (QH staff only).
ALERT
Restricted antibiotics eg Meropenem, require AMS approval for use > 48 hours
Supplemental Investigations:
• Request other investigations as clinically indicated i.e. ± CXR, urine/stool M/C/S, Respiratory virusPCR, CRP. N.B. Antibiotics MUST be commenced before undertaking other investigations
• Abnormal CXRs should be discussed with the Paediatric Oncologist at the Oncology Services, LCCH
Communication:
ALERT
Discuss all patients with the Regional Paediatrician and on-call Paediatric Oncologist at Oncology Services Group via Lady Cilento Children’s Hospital (LCCH) switch:
(07) 3068 1111.
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 6 -
• Prescribe blood products if required and other relevant medications e.g. paracetamol; antiemetics;prophylactic antibiotics, antivirals, and antifungals
• Discuss with the Paediatric Oncologist whether children receiving oral chemotherapy should continueto receive this treatment
Ongoing Management of Febrile Neutropaenia (Appendix 3, Page 9) Evaluate at 48 hours:
• All culture results should be reviewed and antibiotics adjusted according to isolates and antibioticsensitivities (Discuss with Paediatric Oncologist and Infection Management Fellow/Consultant)
Initially stable with suspected Febrile Neutropaenia:
Afebrile
• Evidence of marrow recovery:
If afebrile for at least 24 hours with all negative cultures - stop empiric antibiotics.
If afebrile for at least 24 hours with negative blood cultures but evidence of resolving localinfection (e.g. UTI, skin, soft tissue, chest) and evidence of marrow recovery - consider ivto oral switch to complete 5-7 days antibiotics
• No evidence of marrow recovery:
Continue and review at 72 hours.
Febrile
• Continue Piperacillin/Tazobactam. Reassess and re-culture. Repeat blood cultures from all lumens ofCVAD no more than once within a 24 hour period.
Initially Unwell or Septic (received Piperacillin/Tazobactam, gentamicin and vancomycin):
• Continue Piperacillin/tazobactam; stop Gentamicin and Vancomycin at 48 hrs if negative cultures andpatient is stable.
• Complete a 5 - 7 day course of appropriate intravenous antibiotics, unless specific viral causeidentified
• If afebrile for at least 24 hours at completion of 5 days of appropriate antibiotics stop antibiotics anddischarge home
• If remains febrile at 4 - 5 days follow as below.
ALERT
Routine addition of vancomycin to the initial empiric regimen within 72 hours does not reduce mortality or time to defervescence

CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 7 -
Evaluate at 72 hours:
Afebrile:
• Evidence of marrow recovery:
If afebrile for at least 24 hours with all negative cultures - stop empiric antibiotics.
If afebrile for at least 24 hours with negative blood cultures but evidence of resolving localinfection (e.g. UTI, skin, soft tissue, chest) and evidence of marrow recovery - consider ivto oral switch to complete 5-7 days antibiotics
• No evidence of marrow recovery:
If afebrile for at least 24 hours, all negative cultures and neutropaenia expected to be lessthan 7 days consider stopping antibiotics and scheduling careful follow up.
If afebrile for at least 24 hours, all negative cultures and neutropaenia expected to beprolonged consider completing a 5-7 day course of antibiotics. If stable, these do not needto be intravenous, consider intravenous to oral switch e.g. oral amoxycillin/clavulanate,cephalexin
Febrile:
• Continue Piperacillin/tazobactam. Reassess and repeat blood cultures from all lumens of CVAD nomore than once within a 24 hour period.
• If there is clinical deterioration, consider change to meropenem or add vancomycin if concern forgram positive infection.
• In children at high risk for invasive fungal disease (IFD) with clinical deterioration consider LiposomalAmphotericin (AmBisome ®) IV 1mg/kg once daily and investigate as below.
ALERT Do not switch initial empiric antibiotics in patients with unresponsive fever unless there is clinical deterioration or a microbiological indication.
Febrile at 4-5 days:
• Reassess and in consultation with the treating team consider:
more invasive investigative procedures and imaging
transfer to LCCH if patient is in a shared-care service
• In high risk children with persistent fever beyond 96 hours perform evaluation for invasive fungaldisease (IFD) e.g. CT scan lung, plus abdominal ultrasound (if LFTs deranged) and other clinicallysuspected areas of infection.
• Add Liposomal Amphotericin (AmBisome ®) IV 1mg/kg once daily (increase to 3mg/kg/day if highclinical or radiological suspicion of IFD) Antifungal Prophylaxis and Treatment in Paediatric Oncologyand Immunocompromised Children
Close monitoring of electrolytes and renal function is essential every 24 hours

CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 8 -
If renal impairment or previous adverse reaction to AmBisome® consider Voriconazole orCaspofungin/Micafungin on Paediatric Infectious Disease (ID) team advice.
• If there is clinical deterioration, consider change to meropenem or add vancomycin if concern forgram positive infection
• Remember the possibility of viral infection HSV, VZV, CMV, EBV, Adenovirus etc. When indicated,request appropriate viral blood PCRs, swabs, urine, stool or respiratory secretions.
• Daily blood culture’s at this stage only when clinically indicated/ requested by senior medical staff.
ALERT
Antifungals require AMS approval for use for more than 72 hours for treatment of presumed Invasive Fungal Disease
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 9 -
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 10 -
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 11 -
Note
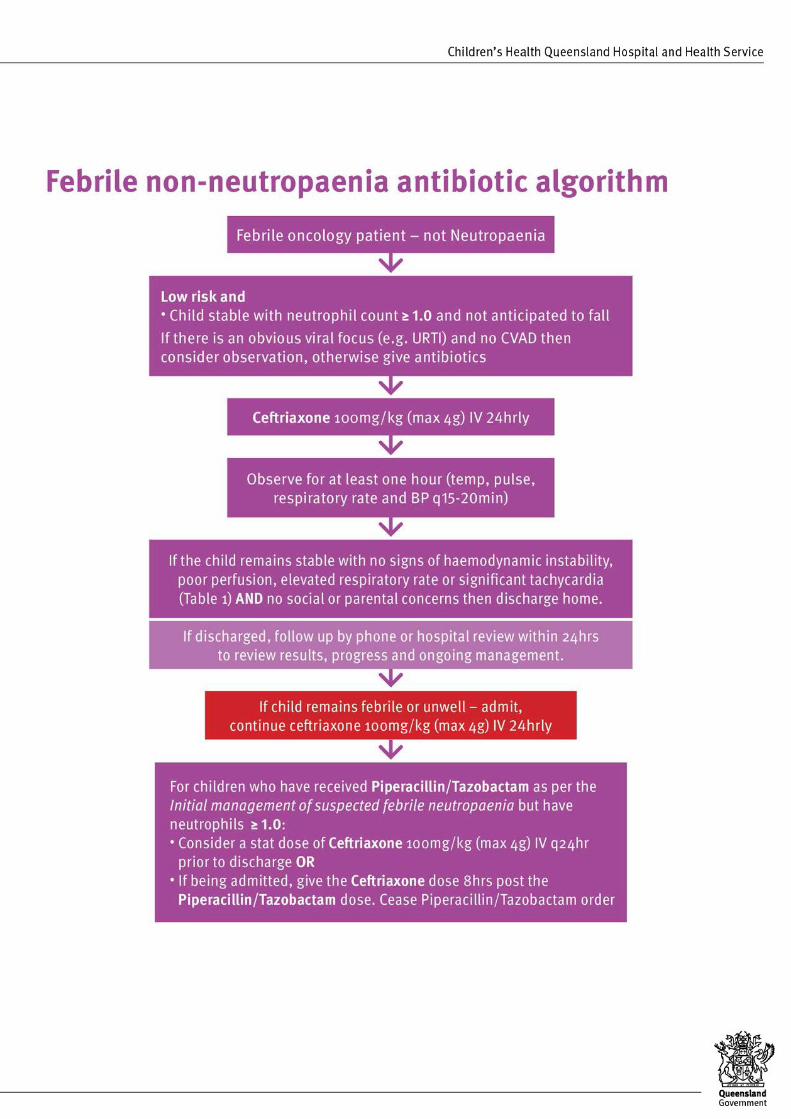
Neuroblastoma and recent IL2; additional gram positive cover is not routinely required as ceftriaxone provides good gram positive cover.
ALERT
Exclusion criteria for Febrile non-neutropaenia antibiotic algorithm outpatient management: Clinical suspicion of bacteraemia: hypotension, poor perfusion, rigors,
significant tachycardia, tachypnoea, dehydration
Impending neutropaenia: IV chemotherapy (other than single agent,Vincristine) within the last 10-14 days
High risk patients: AML, ALL undergoing intensification or relapsetherapy, High risk solid tumours, Down’s Syndrome, infants, Childrenpost HSCT (see Appendix 2)
Admit and follow the Febrile Neutropaenia antibiotic algorithm

CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 12 -
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 13 -
Term Definition
CHQHHS CVAD CVL IMPS IFD AML ALL HSCT HSV VZV CMV EBV GVHD UTI CXR
Children’s Health Queensland Hospital and Health Service Central venous access device Central venous line Infection Management and Prevention Service Invasive fungal disease Acute Myeloid Leukaemia Acute Lymphoblastic Leukaemia Haemapoetic stem cell transplant Herpes Simplex virus Varicella Zoster Virus Cytomegalovirus Epstein barr virus Graft versus host disease Urinary tract infection Chest Xray
Consultation: Key stakeholders who reviewed this version:
• Medical Fellow, Oncology Services Group, CHQHHS
• Director Infection Management
• Statewide Educator, QPPHON
• Clinical Nurse, Oncology Services Group, CHQHHS
• Nurse Educator, Oncology Services Group, CHQHHS
• Antimicrobial Stewardship Pharmacist, Lady Cilento Children’s hospital
• Director Paed BMT, Oncology
• SMO Oncology
• Oncology Director and Oncology SMOs
Definition of terms
Source
References and suggested reading 1. Salstrom J et al. Pediatric Patients who receive antibiotics for fever and neutropenia in less than 60 min have
decreased intensive care needs. Pediatr Blood Cancer 2015;62:807-815
2. Fletcher M et al. Prompt administration of antibiotics is associated with improved outcomes in febrile neutropenia inchildren with cancer. Pediatr Blood Cancer. 2013 Aug;60(8):1299-306

CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 14 -
Version No. Modified by Amendments authorised by
1.0 SGD IMPS Div. Dir. Medicine
3. Cometta A et al. Vancomycin versus Placebo for Treating Persistent Fever in Patients with Neutropenic CancerReceiving Piperacillin-Tazobactam Monotherapy. CID 2003;37:382-9
Guideline revision and approval history
Approved by
EDCS
Keywords Oncology; Fever; Febrile; Neutropaenia; Neutropenic; Non-Neutropenic; Antibiotics; antimicrobial stewardship; sepsis; antifungals, 01249
Accreditation references
NSQHS Standards (1-10): 3; 4; 5; 6; 9
CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 15 -
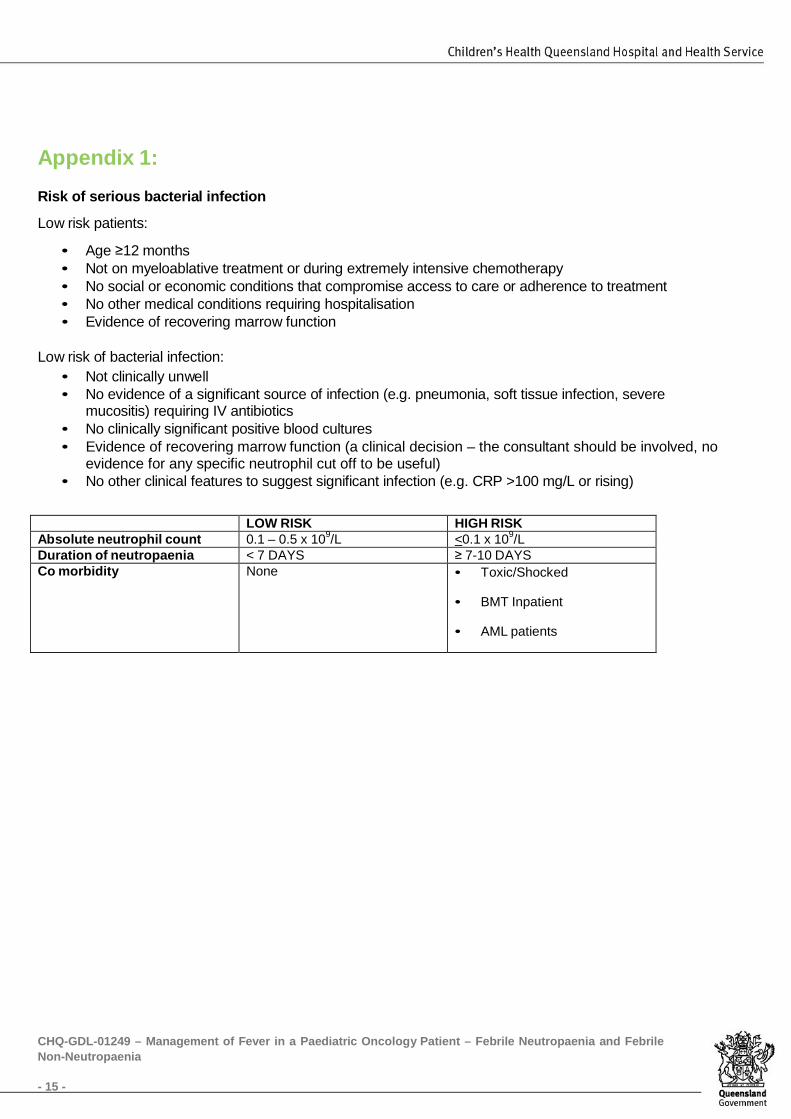
Appendix 1: Risk of serious bacterial infection
Low risk patients:
• Age ≥12 months• Not on myeloablative treatment or during extremely intensive chemotherapy• No social or economic conditions that compromise access to care or adherence to treatment• No other medical conditions requiring hospitalisation• Evidence of recovering marrow function
Low risk of bacterial infection: • Not clinically unwell• No evidence of a significant source of infection (e.g. pneumonia, soft tissue infection, severe
mucositis) requiring IV antibiotics• No clinically significant positive blood cultures• Evidence of recovering marrow function (a clinical decision – the consultant should be involved, no
evidence for any specific neutrophil cut off to be useful)• No other clinical features to suggest significant infection (e.g. CRP >100 mg/L or rising)
LOW RISK HIGH RISK Absolute neutrophil count 0.1 – 0.5 x 109/L <0.1 x 109/LDuration of neutropaenia < 7 DAYS ≥ 7-10 DAYS Co morbidity None • Toxic/Shocked
• BMT Inpatient
• AML patients

CHQ-GDL-01249 – Management of Fever in a Paediatric Oncology Patient – Febrile Neutropaenia and Febrile Non-Neutropaenia
- 16 -
Appendix 2: High risk disease
AML
ALL: Infant ALL (<1y); Induction; Delayed intensification
Downs syndrome Lymphoma: Induction therapy
Neuroblastoma stage IV
Allogeneic transplant: Day -14 to Day +180
Autologous transplant: Day -7 to Day +60
Reinduction therapy for any relapse
Table 1 If in doubt discuss with Oncology Consultant on call or treat as high risk
As per CHQ Guideline 07449 Sepsis: Recognition and Early Management in Children (QH staff only)