management of advanced prostate cancer in senior … · advanced prostate cancer in senior adults:...
TRANSCRIPT
July 2014 version
Management of
advanced prostate
cancer in senior adults:
a booming area
Matti Aapro
Multidisciplinary Oncology Institute
Genolier, Switzerland
July 2014 version
Management of
advanced prostate
cancer in senior adults:
a booming area
Matti Aapro
Multidisciplinary Oncology Institute
Genolier, Switzerland
• Invited speaker / advisory boards
• Sanofi
• Amgen
• GlaxoSmithKline
• Hoffmann-Laroche
• Ferring
• Ipsen
• Janssen
• Novartis
• Pfizer
• Sandoz
3
Disclosures

Treatment options for advanced Prostate Ca
in senior adults
• Castration-sensitive metastatic prostate cancer (mCSPC):
• hot from ASCO and Lancet. NOT AN APPROVED INDICATION….
• Castration-resistant metastatic prostate cancer (mCRPC)
• Palliative therapy for bone metastases
• SIOG guidelines
4

E3805 (CHAARTED) - Chemo-Hormonal vs Androgen
Ablation Randomized Trial in Extensive Disease
N = 780
ADT + Docetaxel (75mg/m2)
for 6 cycles without prednisone
R
A
N
D
O
M
I
Z
E
Stratify:
Extent of metsHigh vs Low
Age≥70 vs <70
ECOG PS0-1 vs 2
CAB >30 daysYes vs No
Prior adjuvant hormonal Tt
> 12 vs ≤12 mo
SRE preventionYes vs No
• Follow-up to
time to
progression
and OS
• Chemotherapy
at investigator’s
discretion at
progression
ADT alone
• ADT allowed up to 120 days prior to
randomization
• Intermittent ADT dosing not allowed
Sweeney C et al. ASCO 2014 – LBA2
ADT: Androgen Deprivation Therapy; OS: overall survival; CAB: ;complete androgen blockade SRE:
skeletal related events; PS: performance status

E3805 (CHAARTED) - Chemo-Hormonal vs Androgen
Ablation Randomized Trial in Extensive Disease
• ADT allowed up to 120 days prior to
randomization
• Intermittent ADT dosing not allowed
Sweeney C et al. ASCO 2014 – LBA2
ADT: Androgen Deprivation Therapy; D: docetaxel (75mg/m2 without prednisone for 6 cycles)

E3805 (CHAARTED) - Chemo-Hormonal vs Androgen
Ablation Randomized Trial in Extensive Disease
Sweeney C et al. ASCO 2014 – LBA2
ADT: Androgen Deprivation Therapy; D: docetaxel (75mg/m2 without prednisone for 6 cycles)

E3805 (CHAARTED) - Chemo-Hormonal vs Androgen
Ablation Randomized Trial in Extensive Disease
Sweeney C et al. ASCO 2014 – LBA2
ADT: Androgen Deprivation Therapy; D: docetaxel (75mg/m2 without prednisone for 6 cycles)

GETUG-15
Presented By Michael Morris at 2014 ASCO Annual Meeting
NO PATIENT ABOVE AGE 68….study from 2004 to 2008
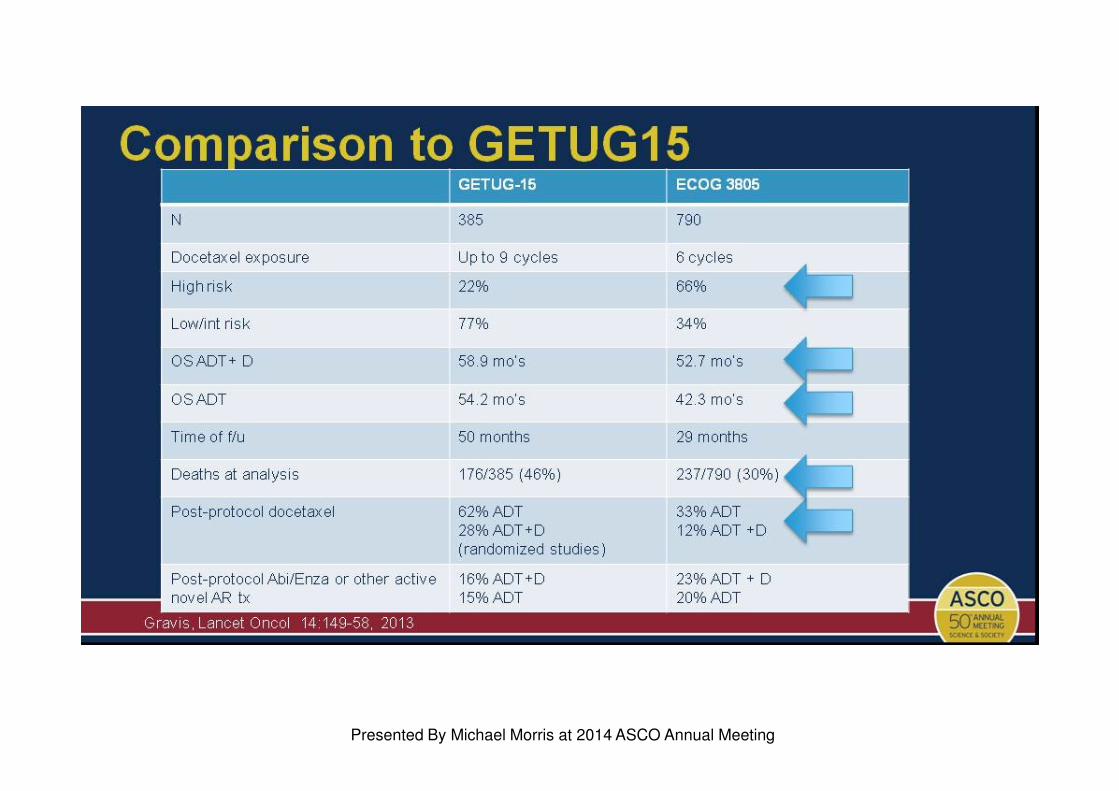
Comparison to GETUG15
Presented By Michael Morris at 2014 ASCO Annual Meeting
Treatment options for advanced Prostate Ca
in senior adults
• Castration-sensitive metastatic prostate cancer (mCSPC)
• Castration-resistant metastatic prostate cancer (mCRPC)
• Palliative therapy for bone metastases
• SIOG guidelines
11

Androgen deprivation therapy in advanced PCa:
Specific considerations for senior adults
• Maximum androgen blockade
results in a small advantage in
OS, which is not clinically
relevant
• Maximum androgen blockade
increases side effects and has
significant effects on QoL
Prostate Cancer Trialists Collaborative Group. Lancet 2000;355:1491–8
ADT: Androgen Deprivation Therapy; OS: overall survival; QoL: quality of life12
First-line ADT in monotherapy is the standard of care

Androgen deprivation therapy: adverse events
• Bone loss with increased risk of
fracture1,2
• Increased risk of diabetes3
• Increased risk of fatal cardiac
events4–6
1. Daniell et al. J Urol 1997;157:439–44
2. Shahinian VB et al. N Engl J Med 2005;352:154–64
3. Keating NL et al. J Clin Oncol 2006;27:4448–56
4. D‘Amico et al. J Clin Oncol 2007;25:2420–25
5. Hayes et al. BJU Int 2010;106:979–85
6. Nguyen et al. Int J Radiat Oncol Biol Phys 2012;82:1411-
6
Years
0
10
20
30
40
50
Cu
mu
lati
ve
fra
ctu
re
inci
de
nce
(%
)
0 1 2 3 4 5 6 7 8 9
Orchiectomy
No orchiectomy
LESS IS BETTER!
Caution in patients with:
� History of stroke
� Chronic heart failure
� Myocardial infarction
� Baseline bone density
� Prevent risk of osteoporosis

Management of advanced PCa:
Specific considerations for senior adults (2/4)
• Castration-sensitive metastatic prostate cancer (mCSPC)
• Castration-resistant metastatic prostate cancer (mCRPC)
� Docetaxel
� 3-weekly schedule is the standard of care1*
� Weekly or bi-weekly schedule for frail patients?2-3
� Cabazitaxel
� Abiraterone acetate
� Enzalutamide
� Sipuleucel-T
• Palliative therapy for bone metastases
• SIOG guidelines
14
1. Berthold D et al. J Clin Oncol 2008;26:242-5
2. Droz JP et al. BJU Int 2010;106:462-9
3. Kellokumpu-Lehtinen P et al. Lancet Oncol 2013;14:117–124
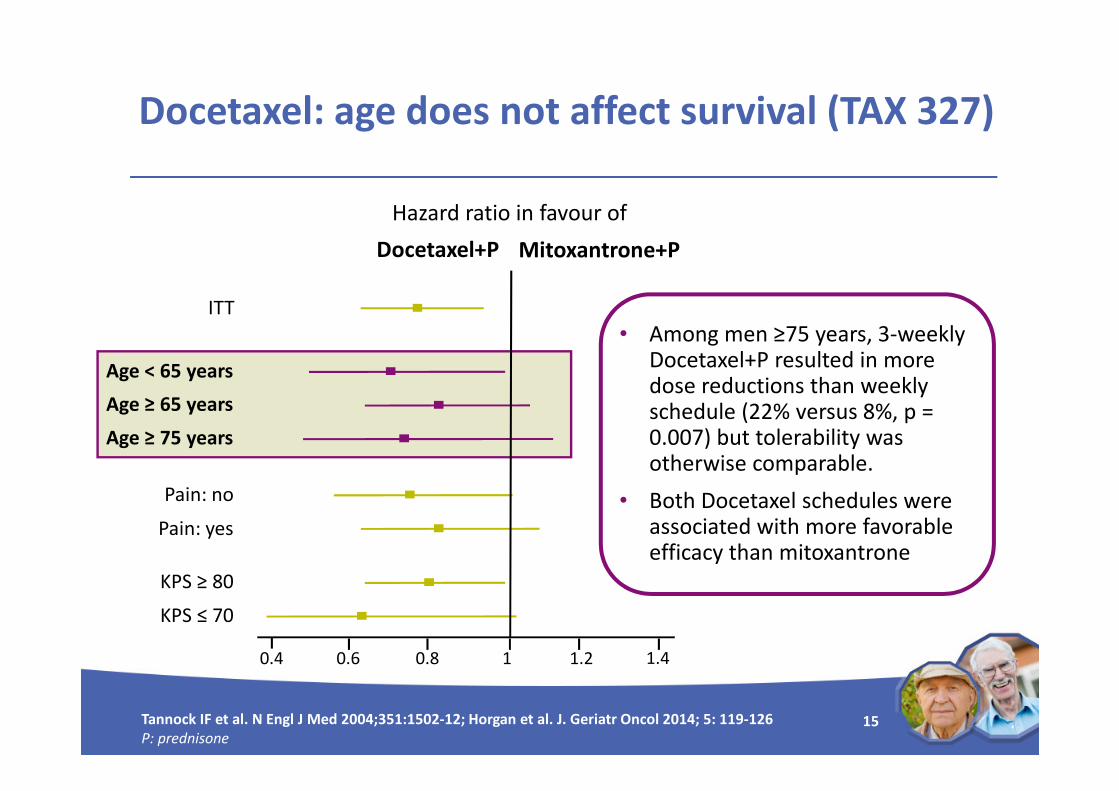
Docetaxel: age does not affect survival (TAX 327)
0.2 0.4 0.6 0.8 1 1.2 1.4
ITT
Age < 65 years
Age ≥ 65 years
Age ≥ 75 years
Pain: no
Pain: yes
KPS ≥ 80
KPS ≤ 70
Hazard ratio in favour of
Docetaxel+P Mitoxantrone+P
15Tannock IF et al. N Engl J Med 2004;351:1502-12; Horgan et al. J. Geriatr Oncol 2014; 5: 119-126
P: prednisone
• Among men ≥75 years, 3-weekly Docetaxel+P resulted in more dose reductions than weekly schedule (22% versus 8%, p = 0.007) but tolerability was otherwise comparable.
• Both Docetaxel schedules were associated with more favorable efficacy than mitoxantrone

Phase 2 study of weekly docetaxel + prednisolone
vs prednisolone alone in mCRPC
Docetaxel weekly+ Prednisolone
Prednisolone
PFS (median)[95% CI]
11 months[5.8–16.2]
4 months[2.4–5.6]
OS (median) [95% CI]
27 months[19.8–34.2]
18 months[15.2–20.8]
Survival rate (%)– 1-year– 2-year
82%61%
67%29%
12-week PSA response rate
69% 36%
QoL improvement– Physical function– Pain– Fatigue– Nausea/vomiting– Global QoL
27%52%38%17%27%
3%16%29%8%
16%
Toxic outcomes N
Gastrointestinal: grade ≥2
Nausea
Vomiting
Diarrhoea
4
1
5
Other/Constitutional: grade ≥2
Nail changes
Alopecia
Conjunctivitis/tearing
Fatigue/Anorexia
Peripheral neuropathy
Atrial flutter
Fluid retention
27
9
8
6
5
4
4
• Median age 70 years
• No cross-over
16
Fossa SD et al. Eur Urol 2007;52:1691–9
mCRPC: metastatic castrate-resistant prostate cancer; OS: overall survival; PFS: progression-free survival;
QoL: quality of life

Phase 3 study of bi-weekly versus 3-weekly
docetaxel plus prednisone in mCRPC
Docetaxelbi-weekly + P
(n=170)
Docetaxel3-weekly + P
(n=169)p
TTTF (median)
[95% CI]
5.6 mo
[5.0–6.2]
4.9 mo
[4.5–5.4]0.014
OS (median)
[95% CI]
19.5 mo
[15.9–23.1]
17 mo
[15.0–19.1]0.021
PSA response 49% 42% 0.49
Best clinical response- CR or PR
- Stable
- Progression
23%
46%
8%
22%
46%
11%
0.95
17
Kellokumpu-Lehtinen P et al. Lancet Oncol 2013;14:117–124
mCRPC: metastatic castrate-resistant prostate cancer; TTTF: Time to Treatment Failure: OS: overall survival
ALP: Alkaline phosphatase
Docetaxelbi-weekly + P
(n=170)
Docetaxel3-weekly + P
(n=169)
Hematological
- Neutropenia
- Leucopenia
- Anemia
- Thrombocytopenia
- Febrile neutropenia
36%
13%
1%
1%
4%
53%
29%
1%
0
14%
Non-hematological
- Fatigue
- Infection without
neutropenia
- Neutropenic
infection
- �ALP
- Diarrhea
- Nausea
15%
11%
6%
9%
1%
1%
15%
12%
24%
6%
2%
1%
Efficacy Grade ≥ 3 toxicities

MATuRITY: Prospective registry in men aged
70+ with mCRPC
At 6 monthsTaxane†
(N=140)
Non-taxane‡
(N=193)P
OS rate 91% 81% 0.027
PFS 66% 50% <0.001
Best clinical benefit 60% 36% <0.001
PSA ↘ ≥ 50% 52.5% 37.4% 0.018
Docetaxel
Grade ≥3 toxicity%
Fatigue 17.1%
Nausea/vomiting 14%
Neutropenia
Febrile neutropenia
9.8%
2.6%
Sensory neuropathy 9.3%
Diarrhea 8.8%
Anemia 7.8%
Loss of appetite 7.3%
Nail change 6.7%
Droz JP et al. ESMO 2012;Poster 934P 18
†75mg/m2 q3w in 83.9% of cases
‡Hormonal manipulations or non-taxane chemotherapy

Bahl A Annals of Oncol 2013; 24: 2402-2408P: prednisone 19
100
90
80
70
60
50
40
30
20
10
00 6 12 18 30
Mitoxantrone+P
% s
urv
ivin
g
Time (months)
Cabazitaxel+P
HR 0.72
(95% CI: 0.61-0.84)
P<0.0001
24
Cabazitaxel significantly improves survival vs
mitoxantrone (TROPIC, post-docetaxel)
755 patients with mCRPC who progressed during or after docetaxel

N HR (95% CI)
All randomized patients 755 0.70 (0.59–0.83)
ECOG status: 0,1 694 0.68 (0.57–0.82)
ECOG status: 2 61 0.81 (0.48–1.38)
Measurable disease: no 350 0.72 (0.55–0.93)
Measurable disease: yes 405 0.68 (0.54–0.85)
Number of previous chemotherapies: 1 528 0.67 (0.55–0.83)
Number of previous chemotherapies: ≥2 227 0.75 (0.55–1.02)
Age<65 years 295 0.81 (0.61–1.08)
Age≥65 years 460 0.62 (0.50–0.78)
Pain at baseline: no 314 0.57 (0.43–0.77)
Pain at baseline: yes 310 0.76 (0.59–0.98)
Rising PSA at baseline: no 159 0.88 (0.61–1.26)
Rising PSA at baseline: yes 583 0.65 (0.53–0.80)
Progression during docetaxel treatment 219 0.65 (0.47–0.90)
Progression <3 months after docetaxel 339 0.70 (0.55–0.91)
Progression ≥3 months after docetaxel 192 0.75 (0.51–1.11)
Cabazitaxel (TROPIC):
Survival not influenced by age
Favors CABA+P Favors MITO+P
20
de Bono et al. Lancet 2010;376:1147–54
ECOG: Eastern Cooperative Oncology Group; CABA+P: cabazitaxel+prednisone;
MITO+P: mitoxantrone+prednisone

Cabazitaxel (European compassionate use
program) - Safety in senior adults
<70 years(n=238)
70-74 years(n=100)
75+ years(n=88)
Treatment exposure
- N cycles, median (range)
- Dose delay for drug-related AE
Dose reduction for any cause
- G-CSF primary prophylaxis (C1)
4 (1-16)
4.3%
18.5%
39.2%
4 (1-12)
13.0%
16.0%
46.1%
4 (1-11)
5.7%
15.9%
50.3%
Hematological, grade ≥3
- Neutropenia
- Leucopenia
- Anemia
- Febrile neutropenia
- Neutropenic sepsis
15.0%
6.2%
5.0%
5.2%
1.0%
16.7%
8.3%
4.4%
5.6%
1.6%
23.4%
9.7%
4.1%
5.5%1.4%
Non-hematological, grade ≥3
- Fatigue
- Asthenia
- Diarrhea
- Nausea
- Vomiting
- Hematuria
- Peripheral neuropathy
- Nail disorders
4.0%
1.4%
3.3%
0%
1.0%
0.5%
0
0
3.3%
4.4%
1.7%
0.6%
1.1%
2.8%
0
0
5.5%5.5%2.8%
3.4%
2.1%
1.4%
0.7%
0
Heidenreich A et al. Eur J Cancer 2014; 50; 1090-99

Abiraterone in post-docetaxel setting significantly
improves survival vs placebo (COU-AA-301)
Fizazi K et al. Lancet Oncol 2012;13(10);983-92
P: prednisone; HR: hazard ratio; CI: confidence interval
22
1195 patients with mCRPC who were previously treated with docetaxel
HR 0.74
(95% CI: 0.64-0.86)
P<0.0001
Ov
era
ll s
urv
iva
l (%
)
Time to death (months)
Placebo+P
11.2 months
Abiraterone acetate+P
15.8 months
100
60
40
20
80
0 6 12 18 24 30
Median age: 69 years
≥75 years: 28%
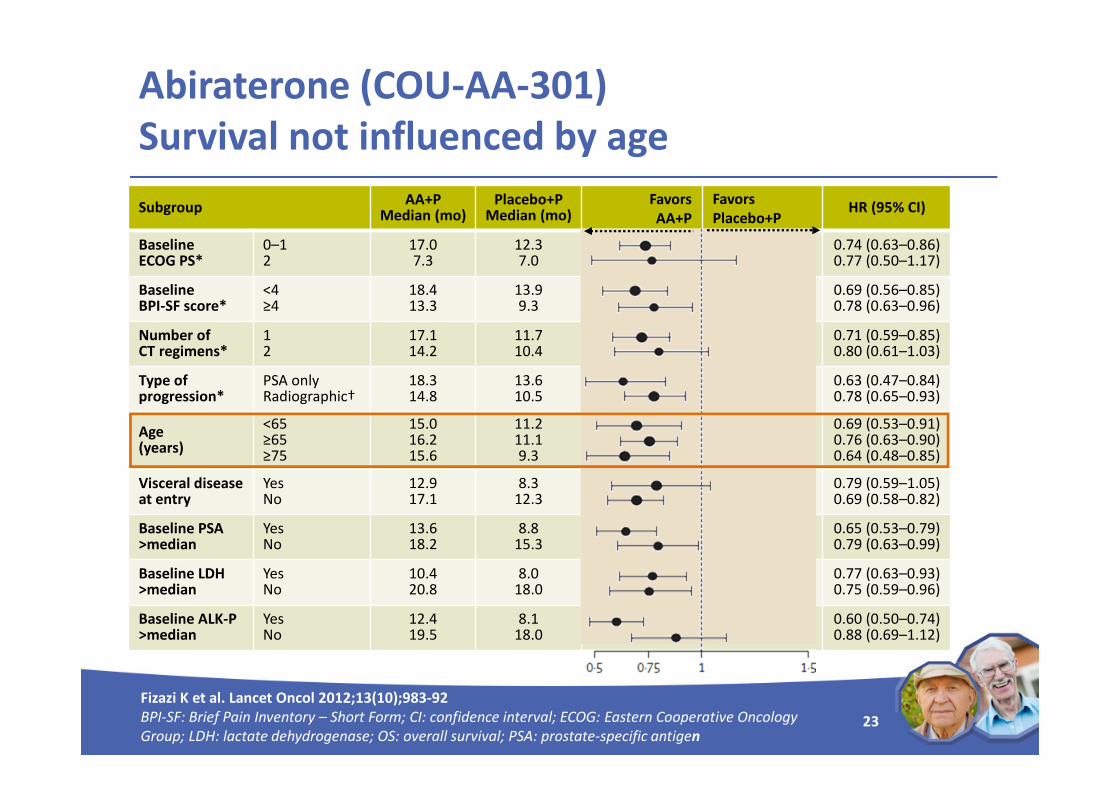
Abiraterone (COU-AA-301)
Survival not influenced by age
SubgroupAA+P
Median (mo)Placebo+P
Median (mo)HR (95% CI)
Baseline ECOG PS*
0–12
17.07.3
12.37.0
0.74 (0.63–0.86)0.77 (0.50–1.17)
Baseline BPI-SF score*
<4≥4
18.413.3
13.99.3
0.69 (0.56–0.85)0.78 (0.63–0.96)
Number of CT regimens*
12
17.114.2
11.710.4
0.71 (0.59–0.85)0.80 (0.61–1.03)
Type of progression*
PSA onlyRadiographic†
18.314.8
13.610.5
0.63 (0.47–0.84)0.78 (0.65–0.93)
Age (years)
<65≥65≥75
15.016.215.6
11.211.19.3
0.69 (0.53–0.91)0.76 (0.63–0.90)0.64 (0.48–0.85)
Visceral disease at entry
YesNo
12.917.1
8.312.3
0.79 (0.59–1.05)0.69 (0.58–0.82)
Baseline PSA >median
YesNo
13.618.2
8.815.3
0.65 (0.53–0.79)0.79 (0.63–0.99)
Baseline LDH >median
YesNo
10.420.8
8.018.0
0.77 (0.63–0.93)0.75 (0.59–0.96)
Baseline ALK-P >median
YesNo
12.419.5
8.118.0
0.60 (0.50–0.74)0.88 (0.69–1.12)
Fizazi K et al. Lancet Oncol 2012;13(10);983-92
BPI-SF: Brief Pain Inventory – Short Form; CI: confidence interval; ECOG: Eastern Cooperative Oncology
Group; LDH: lactate dehydrogenase; OS: overall survival; PSA: prostate-specific antigen23
Favors
AA+P
Favors
Placebo+P

Abiraterone in chemo-naïve patients significantly
improves rPFS but only trend for OS
Overall survivalRadiological PFS
24Ryan C et al. N Engl J Med 2013; 368:138-148
PFS: progression-free survival; P: prednisone
Asymptomatic or mildly symptomatic
chemo-naïve patients without visceral metastases
PF
S (
%)
100
80
60
40
20
00 6 12 18 24 27 303 9 15 21
Months
Abiraterone + P
16.5 mths
OS
(%
)
100
80
60
40
20
00 6 12 18 24 27 30 333 9 15 21
Months
Abiraterone + P
Not reachedPrednisone
27.2 mths
Prednisone
8.3 mths
HR 0.53
(95% CI 0.45–0.62)
P<0.001
HR 0.75
(95% CI 0.61–0.93)
P=0.01
Prespecified P for
significance 0.0035
1088 chemonaive mCRPC patients

Enzalutamide in post-docetaxel setting significantly
improves survival vs placebo (AFFIRM)S
urv
iva
l (%
)
Duration of overall survival (months)
Enzalutamide
OS 18.4 months
Placebo
OS 13.6 months
]
100
90
80
70
60
50
40
30
20
10
0
246 9 12 15 18 2130
HR 0.631
(95% CI: 0.529-0.752)
P<0.0001
Scher HI et al. N Engl J Med 2012;367:1187-97
NYR: not yet reached;OS: overall survival
Median age: 69 years
≥75 years: 25%
1199 patients with mCRPC previously treated with docetaxel
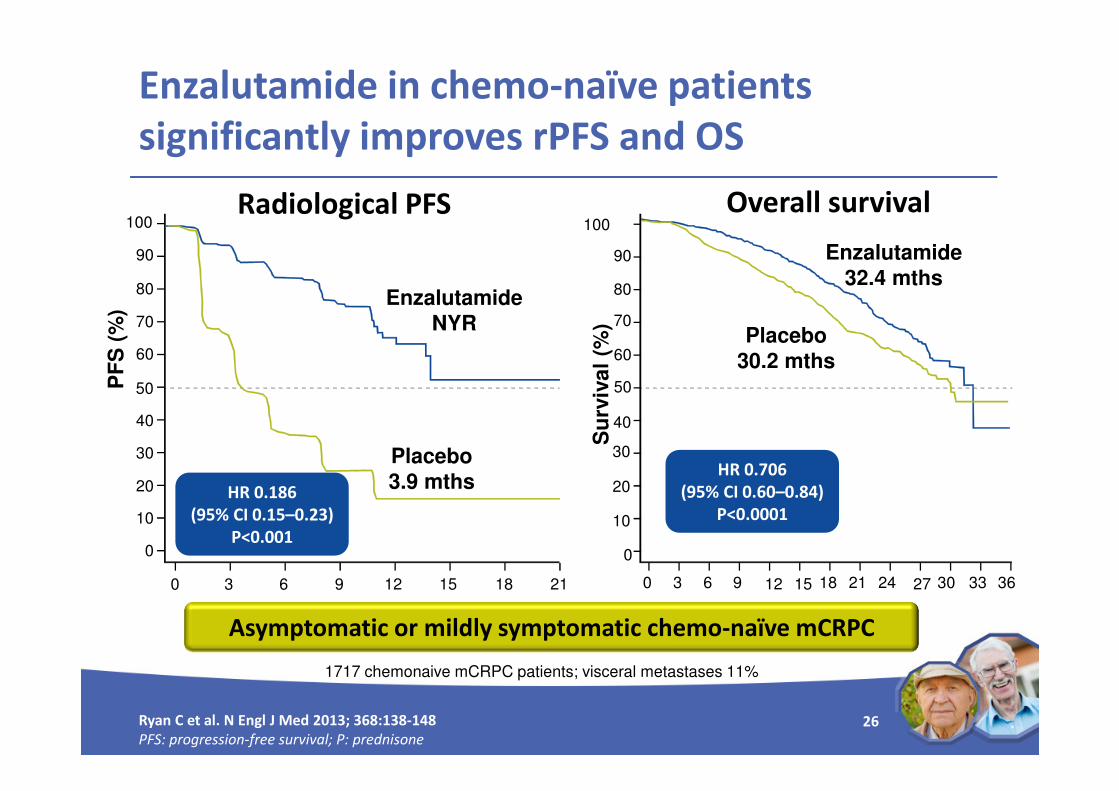
Enzalutamide in chemo-naïve patients
significantly improves rPFS and OS
Overall survivalRadiological PFS
26Ryan C et al. N Engl J Med 2013; 368:138-148
PFS: progression-free survival; P: prednisone
Asymptomatic or mildly symptomatic chemo-naïve mCRPC
0 3 6 9 12 15 18 21
60
50
40
30
20
10
0
90
80
70
100
PF
S (
%)
Enzalutamide
NYR
HR 0.186
(95% CI 0.15–0.23)
P<0.001
Placebo
3.9 mths
Su
rviv
al
(%)
60
50
40
30
20
10
0
90
80
70
100
0 3 6 9 12 15 18 21 24 27 30 33 36
Enzalutamide
32.4 mths
HR 0.706
(95% CI 0.60–0.84)
P<0.0001
Placebo
30.2 mths
1717 chemonaive mCRPC patients; visceral metastases 11%

Enzalutamide (AFFIRM)
Survival not influenced by age
SubgroupHR for death
(95% CI)
Median OS (months)
Enzalutamide/Placebo
All subjects0.63 (0.53–0.75) 18.4/13.6
Age (years) <65
>65
0.63 (0.46–0.87)
0.63 (0.51–0.78)
–/12.6
18.4/13.9
Baseline ECOG PS score 0–1
2
0.62 (0.52–0.75)
0.65 (0.51–0.78)
–/14.2
10.5/7.2
Baseline mean
pain score on BPI-SF
<4
≥4
0.59 (0.47–0.74)
0.71 (0.54–0.94)
–/16.2
12.4/9.1
Geographic region North America
Other
0.63 (0.47–0.83)
0.64 (0.51–0.80)
17.4/12/3
–/14.4
Number of prior
chemotherapy regimens
1
≥2
0.59 (0.48–0.73)
0.74 (0.54–1.03)
–/14.2
15.9/12.3
Type of progression
at study entry
PSA only
PSA ±Radiographic
0.62 (0.46–0.83)
0.64 (0.52–0.80)
–/19.5
17.3/13.0
Baseline value
>median value
PSA
LDH
0.62 (0.50–0.78)
0.61 (0.50–0.76)
15.3/10.3
12.4/8.5
Favors
Enzalutamide
Favors
Placebo
Scher HI et al. N Engl J Med 2012; 367: 1187-97
BPI-SF: Brief Pain Inventory – Short Form; CI: confidence interval; ECOG: Eastern Cooperative Oncology
Group; LDH: lactate dehydrogenase; OS: overall survival; PSA: prostate-specific antigen

28
Caution if history of
seizure, brain injury,
cerebral vascular accident,
brain metastases
Cabazitaxel*1
�Higher risk of febrile
neutropenia (7.5 vs 1.3%)
�Higher risk of diarrhea
(6.5 vs 0.3% grade ≥3)
Abiraterone*2
�Hypokalemia, hypertension
& fluid retention due to
mineralocorticoid excess
�Risk of adrenocortical
insufficiency
�Risk of hepatotoxicity
Enzalutamide3
�Higher risk of fatigue
(34% vs 29%)
�Risk of seizures (0.9%)
�Higher risk of hot flushes
(20 vs 10%)
�Higher risk of falls
(4.6 vs 1.3%)
Specific considerations for senior adults
with VERY advanced disease
Product information: 1. cabazitaxel, 2. abiraterone, 3. enzalutamide; Guidelines: 4. EORTC guidelines Aapro M et al. EJC 2011; 47: 8-32 and ASCOCV: cardiovascular; G-CSF: granulocyte colony-stimulating factor; * administered with prednisone
Consider primary
prophylaxis with G-CSF
in high risk patients4
Rehydration with
antiemetics and
antidiarrheals as needed
Use with caution in
patients with CV diseases
Monitor liver function
Caution if interruption of
daily steroids and/or
infection or stress
Evaluate functional
status & program
exercise support

29
Sipuleucel-T significantly improves survival
vs placebo (IMPACT trial, pre-docetaxel)
Main AEs: chills, fever, headache
Ove
rall
su
rviv
al
(%)
Time (months)
Sipuleucel-T
Placebo
Overall survival
12 24 36 48 60 72
0
20
40
60
80
100
0
Median age: 72 years Median age: 72 years
n=512
Hazard Ratio 0.78
(95% CI, 0.62-0.98)
P=0.03
Hazard Ratio 0.78
(95% CI, 0.62-0.98)
P=0.03
Kantoff PW et al. N Engl J Med 2010;363:411-22mCRPC: metastatic castration-resistant prostate cancer; mths: months
Asymptomatic or mildly symptomatic chemo-naïve mCRPC
Without visceral metastases

July 2014 version
Which drug
for which patient?

1 Loriot Y & Fizazi K. Eur Urol 2013; 63: 983-85 ; 2 van Soest R et al. ASCO 2014 (abstract 5043)
TTP: time to progression; mths: months; D: docetaxel plus prednisone; M: mitoxantrone plus prednisone
Docetaxel2AR targeted agents1
Short response to first ADT may predict poor
response to AR-targeted therapies
• Retrospective analysis in 108
patients with metastatic PCa
• Poor response to subsequent
hormone therapies (including
abiraterone, enzalutamide)
if duration of response to
first ADT < 16 months
• Post-hoc analysis of TAX327
randomized phase III trial
• 335 mCRPC patients treated
with docetaxel+P (D) and 336
with mitoxantrone+P (M)
• Good response to docetaxel
irrespective of duration of 1st ADT
Duration of
response
< 16
mths
≥ 16
mths
↓ PSA ≥50% 18% 58%
Median OS - -
Duration of
response
< 15
mths
≥ 15
mths
↓ PSA ≥50% 62% 60%
Median OS
benefit (D vs M)
3.5 mths 2.5 mths

Extended metastatic spread and high NLR may
predict poor response to abiraterone
Leibowitz-Amit et al., Annals Oncol 2014 (epub ahead of print)
NLR: neutrophil/lymphocyte ratio; *Bone mets only or lymph node mets only; **visceral mets alone or combined with bone or lymph nodes
0
10
20
30
40
50
60
0
5
10
15
20
25
30
35PSA response Overall survival
Pe
rce
nta
ge
with
PS
A d
ecre
ase≥5
0%
Media
novera
llsurv
ival(m
onth
s)
Restricted*
mets & NLR≤5
Extended**
mets & NLR >5Other
casesRestricted*
mets & NLR ≤5
Extended**
mets & NLR >5Other
cases
Princess Margaret (test cohort, n=116)
Royal Marsden (validation cohort, n=250)
58
36
6
50
37
20
23
18
14
30
16
11

1. 1. Loriot Y et al. Ann Oncol 2013; 24: 1907-12; 2. 2. Noonan Kl et al. Ann Oncol 2013; 24: 1802-04; 3. 3. Fizazi K et al. Lancet Oncol 2012; 13: 983-92 33
Loriot1 Noonan2 COU-AA-3013
Prior Enzalutamide Yes No Yes No
Median PFS (months) 2.7 6.5 3.6 5.6
Median OS (months) 7.2 11.4 11.8 14.8
↓PSA ≥50%* 8% 29% 3% 29%
Poor response to abiraterone in patients
progressing on enzalutamide (post-docetaxel)
Loriot [1] and Noonan [2] are retrospective studies conducted in 38 and 30 patients,respectively
OS: overall survival; PFS: progression-free survival
*Confirmed by a second value;

34
Poor response to enzalutamide in patients
progressing on abiraterone (post-docetaxel)
*Confirmed by a second value;
Schrader1 Bianchini2 Thomsen3 Badrising4 AFFIRM5
Prior ABI Yes Yes Yes Yes No
Partial response 2.9% 4.3% - 29%
Median PFS,
months
- 2.8 - 3.0 8.3
Median OS,
months
7.1** - 4.8 7.9 18.4
↓PSA ≥50% 29% 13%* 17% 21% 54%*
*Confirmed by a second value; **mean value
1. Schrader A et al. Eur Urol 2014;65:e22-3; 2. Bianchini D et al. Eur J Cancer 2013 (epub ahead of print) 3. Thomsen FB Scand J Urol Nephro 2013 (epub ahead) ; 4. Badrising S. et al. Cancer 2014;120:968-75); 5. Scher HI et al. Lancet Oncol 2012; 13: 983-92

Management of advanced PCa:
specific considerations for senior adults (3/4)
• Castration-sensitive metastatic prostate cancer (mCSPC)
• Castration-resistant metastatic prostate cancer (mCRPC)
• Palliative therapy for bone metastases
� Zoledronic acid
� Denosumab
� Interventionnal radiology ( vertebroplasty, kyphoplasty )
� Radiation therapy
� Radium-223
• SIOG guidelines
35

0 3 6 9 12 15 18 21 24 27 30 33 36 39
Radium-223 improves survival vs placebo
(ALSYMPCA, post-docetaxel)
Parker C et al. N Engl J Med 2013;369:213-23
%
Placebo (N=307)
Median OS: 11.3 months
Radium-223 (N=614)
Median OS: 14.9 months
100
90
80
70
60
50
40
30
20
10
0
Time to death (months)
Hazard Ratio 0.695
(95% CI, 0.581-0.832)
P=0.00007
Mean age: 70 years
921 patients with symptomatic mCRPC post-docetaxel (or unfit for chemotherapy), ≥2 bone mets, no visceral mets


Matti Aapro
Multidisciplinary Oncology Institute
Genolier, Switzerland
SIOG 2014
prostate guidelines

1. Droz JP et al. Crit Rev Oncol Hematol 2010;73:61-912. Droz JP et al. BJU Int 2010;106:462-9
39
SIOG recommendations for senior adults
1. Droz JP et al. Crit Rev Oncol Hematol 2010;73:61-912. Droz JP et al. BJU Int 2010;106:462-9
40
SIOG recommendations for senior adults
Health status (mainly driven by co-morbidities)
Patient preferences
NOT Chronological age
AND
Treatment recommendations for older men
with prostate cancer should be based on:

Bellara CA et al. Annals Oncol 2012; 23: 2166
G-8 geriatric screening tool
41
0 = severe decrease1 = moderate decrease2 = no decrease
0 = >3kg1 = does not know2 = between 1 &3 kg3 = none
0 = bed or chair bound1 = able to get out of bed/chair but does not go out2 = goes out
0 = severe dementia or depression1 = mild dementia2 = no psychological problems
0 = BMI<191=BMI 19to <212= BMI 21 to <233 = BMI ≥ 23
0 = yes1 = no
0.0 = not as good0.5 = does not know1.0 = as good2.0 = better
0 = >85 yr1= 80-85 yr2 = <80 yr
0-17
A. Has food intake declined over the past 3 months due to loss of appetite, digestive problems, chewing or swallowing difficulties?
B. Weight loss during the last 3 months?
C. Mobility?
D. Neuropsychological problems?
E. BMI (weight in kg/height in m²)
F. Takes more than three prescription drugsper day?
G. In comparison with other people of the same age, how does the patients consider his/her health status?
H. Age
Total score
A fast test• Median 4·4 (± 2.8) minutes
for completion
• 98·7% completion rate in
less than 10 min
A fast test• Median 4·4 (± 2.8) minutes
for completion
• 98·7% completion rate in
less than 10 min
Cut-off value = 14• 14: favourable
• ≤ 14: impairment which
requires comprehensive
geriatric evaluation
Cut-off value = 14• 14: favourable
• ≤ 14: impairment which
requires comprehensive
geriatric evaluation

42
>14
No geriatric
assessment
requested
≤14
Geriatric
assessment
requested
Not reversible:• Abnormal IADL
• Abnormal ADL ≥3
• Severe malnutrition
• Cognitive impairment
• Comorbidities CISR-G
grades 3-4
Reversible:• Abnormal ADL: 1 or 2
• Malnutrition
• Depression
• Comorbidities CISR-G
grades 1-2
G8 screening
VULNERABLEFIT FRAIL
GERIATRIC INTERVENTIONSGERIATRIC INTERVENTIONS

1. Droz JP et al. Crit Rev Oncol Hematol 2010;73:61-912. Droz JP et al. BJU Int 2010;106:462-9
43
Principles of the guideline for PCa
Health status evaluation
Readaptation
Standard treatment
as for younger
patients
Standard treatment
as for younger patients
Symptomatic
management including
adapted specific
treatments
Only palliative
treatment
Group 1
(Healthy)
Group 2
(Vulnerable, i.e.
reversible problem
Group 3
(Frail, i.e. non
reversible problem)
Group 4
(Terminal illness)
Geriatric Screening with G-8 tool

18
14.2
10.8
7.9
5.8
4.3
12.4
9.3
6.7
4.7
3.22.3
6.7
4.9
3.32.2
1.5 1
0
2
4
6
8
10
12
14
16
18
20
70 years 75 years 80 years 85 years 90 years 95 years
Me
dia
n l
ife
exp
ect
an
cy (
yea
rs)
Top 25th percentile 50th percentile Lowest 25th percentile
Walter LC et al. JAMA 2001;285:2750-6
EAU and NCCN recommend therapy of early asymptomatic
disease in all patients with life expectancy > 10 years
44
Should be considered for
therapy:• ‘Fit’ and ‘vulnerable’
aged 70-80 years
• Only ‘fit’ aged 80-85 years

EAU / SIOG 2014 guidelines Individualized treatment
and life expectancy evaluation is mandatory
Mottet N et al. EAU guidelines 2014 (www.uroweb.org)Droz JP, et al. Lancet Oncol 2014 (In press)
Overall conclusions
• Docetaxel (without prednisone) provides benefitversus ADT alone in metastatic hormone-naive PCa(unapproved indication )
• Many new drugs to manage metastatic CRPCin senior adults, representing a significant increase in healthcare expenditure
• Optimal timing, sequencing and potential combinationsof these new agents remain to be determined
• Need to rely on currently available predictorsof response to each drug to optimize patient management


DECEMBER 5: A JOINT MASCC SIOG SESSION
Chairs: D. Keefe (AUS) ; G. Zulian (CH)
…Bone health: a key factor in elderly and not so elderly patients with cancer M. Aapro
(CH)
…Mucositis and new drugs: to prevent or to treat? D. Keefe (AUS)
…Depression: an issue in survivorship for elderly cancer patients. L. Balducci (USA)
…Ovarian cancer: issues in the long term for elderly patients C. Steer (AUS)

49
Matti Aapro
IMO Genolier (Switzerland)
THANK YOU MERCI

Any questions?
50