management model in the healthcare setting: a case …
TRANSCRIPT



MANAGEMENT MODEL IN THE HEALTHCARE SETTING: A CASE STUDY
___________________________________
By
PATRICK OWEN CHADD
___________________________________
A DISSERTATION IN PRACTICE
Submitted to the faculty of the Graduate School of Creighton University in Partial
Fulfillment of the Requirements for the degree of Doctor of Education in
Interdisciplinary Leadership
_________________________________
Omaha, NE
November 9, 2015


iii
Abstract
The US healthcare system has been heavily criticized for its disintegrated nature; more
so, it is very much alarming to have reports show that numbers are increasing on the
restorable errors of medical professionals that have led to death or injury. With the
situation in 2015 of the emergency healthcare field, the researcher felt the urgency and
call for finding ways to correct the system protocols and recommend a model that would
promote patient care and quality to a higher degree. Since there have been a growth on
the use of interdisciplinary or dyad management models in the healthcare systems in the
recent years, it was decided to construct the models as the focal points of the current
study. By employing a qualitative thematic analysis on the interviews with eight
physicians and professional managers, the researcher established six major themes and
formed Chadd's Model of Dyad Management that can be utilized to improve the current
practices and protocols in dyad management. It was then found that the key factor in
creating and implementing dyads or triads is the aim of producing the best solutions for
patient care. Participants also strongly believed that the purpose of dyads or triads was to
form better collaboration and to work together as teams. Participants also suggested that
for dyads and triads to be effective, members should have skills to support arguments
with evidence. They also followed protocols such as formal meetings and discussions
before making decisions on their courses of actions requiring a clear communication
between members. Finally, the physicians and managers contended that dyads and triads
may be modified to be more compelling through removal of message noises and thus
solve issues better.

iv

v
Acknowledgements
Over this doctoral journey I have received support and encouragement from a great
number of individuals.
Dr. Isabelle Cherney has been a mentor, advisor, champion and a source of constant
inspiration and motivation. Her guidance has made this a thoughtful and rewarding
journey.
Dr. Cherney - vous avez changé ma vie et de la perspective et je vous remercie de tout
mon cœur.
Dr. Peggy Hawkins, my fantastic advisor has also been integral to my success in this
endeavor and my research would not have been what it is without her invaluable advice
and efforts to help me focus my ideas and thoughts.
Dr. John Hudson, my dissertation chair for his expertise, time, direction and patience as I
worked through my ideas and research to get to where I am today.
I would like to thank my dissertation committee of Dr. John Hudson and Dr. Peggy
Hawkins for their support and counsel over the past year as I moved from several ideas
and topics to a completed study.
My amazing peers in cohorts 13 and 14 who have been on this journey with me from the
beginning; always encouraging, motivating, supporting and pushing when needed to keep
me on track. The writing workshops, cohort dinners and intra-cohort communication via
phone, text, email and facebook have made this experience wholly immersive and
connected for me.
Many thanks to my amazing spouse, Dr. Edward Hamaty who was always encouraging,
understanding and supportive of me through all the years in this program; as I tried to

vi
juggle work, time away from family and completing my dissertation. But for his
influence, I would not be who and where I am today
Finally, to my parents, Donald J. Chadd and Shizuko Komiya Chadd Matsuzawa who
always believed in me and my abilities; this is for you.

vii
Table of Contents
Abstract .............................................................................................................................. iii
Acknowledgements ............................................................................................................. v
List of Tables ..................................................................................................................... ix
List of Figures ..................................................................................................................... x
CHAPTER ONE: INTRODUCTION ................................................................................. 1
Background of the Problem ............................................................................................. 1
Purpose of the Study ....................................................................................................... 3
Research Questions ......................................................................................................... 3
Significance of the Study ................................................................................................ 4
Aim of the Study ............................................................................................................. 5
Methodology Overview................................................................................................... 5
Delimitations and Limitations ......................................................................................... 5
Leader’s Role and Responsibility in Relation to the Problem ........................................ 7
Summary ......................................................................................................................... 7
CHAPTER TWO: LITERATURE REVIEW ..................................................................... 9
Introduction ..................................................................................................................... 9
Interdisciplinary Decision making .................................................................................. 9
Interdisciplinary Teamwork in the Healthcare Setting .............................................. 10
Benefits and Drawbacks of the Dyadic Model .......................................................... 12
Competencies for Interdisciplinary Teamwork and Leadership ................................ 13
The Healthcare Setting .................................................................................................. 15
Interdisciplinary Leadership .......................................................................................... 16
Reflections of the Researcher ........................................................................................ 19
Summary ....................................................................................................................... 19
CHAPTER THREE: METHODOLOGY ......................................................................... 21
Purpose of the Study ..................................................................................................... 21
Aim of the Study ........................................................................................................... 21
Research Questions ....................................................................................................... 21
Methodology ................................................................................................................. 22
Participants .................................................................................................................... 23

viii
Instrumentation.............................................................................................................. 24
Overview of Data Collection ......................................................................................... 25
Procedures ..................................................................................................................... 26
Data Analysis Plan ........................................................................................................ 27
Reliability and Validity ................................................................................................. 28
Ethical Considerations ................................................................................................... 29
Reflective Practices ....................................................................................................... 29
Summary ....................................................................................................................... 30
CHAPTER FOUR: RESULTS ......................................................................................... 31
Introduction ................................................................................................................... 31
Purpose of the Study ..................................................................................................... 32
Aim of the Study ........................................................................................................... 32
Data Analysis ................................................................................................................ 34
Summary ....................................................................................................................... 69
CHAPTER FIVE: CONCLUSION................................................................................... 71
Introduction ................................................................................................................... 71
Purpose of the Study ..................................................................................................... 72
Aim of the Study ........................................................................................................... 72
Summary of Findings .................................................................................................... 72
Interpretation of Data .................................................................................................... 75
Limitations .................................................................................................................... 79
Recommendations for Further Research ....................................................................... 80
Implications for Action ................................................................................................. 81
Summary ....................................................................................................................... 83
References ......................................................................................................................... 84
APPENDIX A: Interview Prompts or Questions .............................................................. 87

ix
List of Tables
Table 1. Backgrounds of Study Participants ..................................................................... 34
Table 2. Factors Considered in Creating and Implementing Dyads/Triads ...................... 35
Table 3. Objectives/Purposes of Dyads/Triads ................................................................. 39
Table 4. Competencies Perceived as Necessary for Members of Dyads/Triads ............... 44
Table 5. Protocols/Procedures for Decision Making Within Dyads/Triads ..................... 52
Table 6. Perceived Advantages/Disadvantages of Dyads/Triads vs. Non-Interdisciplinary Teams ..................................................................................... 58
Table 7. Suggested Areas of Improvement for Dyad/Triad Effectiveness and Efficiency ............................................................................................................ 65

x
List of Figures
Figure 1. Chadd’s Model of Dyad Management……...…………………………………92

MANAGEMENT MODEL IN HEALTHCARE SETTING 1
CHAPTER ONE: INTRODUCTION
Background of the Problem
In a seminal report, the Institute of Medicine described the U.S. healthcare system
as at least ten years behind other high-risk industries with regards to protocols and
practices that ensure safety, which is defined as freedom from accidental injury (Kohn,
Corrigan, & Donaldson, 2000). The report provided examples of patients who died or lost
important limbs and abilities because of medical errors, including drug overdose, drug
mix-up, misdiagnosis, and errors in patient reports and paperwork. The authors also
indicated that the fragmented nature of the U.S. healthcare system increased the
likelihood of incorrect diagnoses due to incomplete or incorrect medical histories
provided by patients. In order to address the issue of significant errors in the U.S.
healthcare system, the authors recommended a comprehensive approach to improving
patient safety. At the core of these recommendations is an emphasis on the roles of
professionals and organizations in collaborating towards improving safety in the U.S.
healthcare system.
Since the release of this report and its recommendations, significant changes have
occurred in the management and protocols of hospitals and health-related institutions.
One such change is the increased use of the dyad or triad model in healthcare
management and decision making (Zismer & Brueggemann, 2010). Simply put, a dyad is
an interdisciplinary team consisting of two individuals of different professions who share
the same goal or mission but have distinct responsibilities and roles that complement one
another, such that efforts are maximized towards achieving objectives (Zismer &
Brueggemann, 2010). For example, in the management of healthcare systems, a doctor of

MANAGEMENT MODEL IN HEALTHCARE SETTING 2
medicine and a professional manager would take the role of co-managers with distinct
and separate responsibilities that complement each other, such that optimal health care is
provided in their facility. Professional managers in such cases are often nurse managers,
who are nurses who are responsible not only for the conduct and quality of care provided
by nurses within a unit or department, but also for personnel and resource management
within the unit (George & Haag-Heitman, 2011). Another example of a dyad would be a
patient-doctor relationship wherein the patients are provided all necessary information
about their health and the possible courses of action. Then their doctor discusses these
alternatives, and they together make an informed decision on the choice they perceive to
be the best alternative among all others. Consequently, a triadic relationship in such
contexts would be one wherein three individuals with different roles and areas of
expertise collaborate on making better-informed decisions about specific patients,
hospital protocols, and the overall healthcare system.
Numerous forms of dyads and triads have been established and are currently
practiced in healthcare systems for different purposes. This Dissertation in Practice study
focuses on the use of dyads and triads in the management of integrated health systems in
order to minimize preventable adverse errors, to provide more coordinated care, and to
optimize processes while minimizing the cost of procedures. Specifically, the research
was a case study of physicians and professional managers from a selected hospital in
New Jersey who have participated in an interdisciplinary team. Participants were asked to
provide their personal and professional opinions on the use of dyads and triads, especially
on its mechanisms, planning, development, and implementation, necessary competencies
of members, outcomes, its effects on the decision-making process, perceived flaws, and

MANAGEMENT MODEL IN HEALTHCARE SETTING 3
areas for improvement. The aim of this Dissertation in Practice study is to use the
findings on dyads and triads in the healthcare setting to design a decision-making model
for interdisciplinary teams that can be adapted in different settings.
Purpose of the Study
The purpose of this case study was to explore the experiences and perceptions of
physicians and professional managers on interdisciplinary decision-making teams in a
large healthcare organization. Analysis of their perceptions could be used to develop a
decision-making model that can be adapted in different settings, such as businesses, non-
profit organizations, and academic institutions.
Research Questions
In order to identify optimal ways of using interdisciplinary teams in the healthcare
setting, the design and conduct of this study were guided by the following research
question: What are the perceptions of physicians and professional managers on the use of
interdisciplinary teams or dyads/triads in healthcare management and decision making?
Specifically, data collection focused on answering the following sub-questions:
1. What factors are considered in creating and implementing dyads or triads?
2. What objectives, or for what purposes, are dyads or triads usually created?
3. What competencies are perceived as necessary to effectively and efficiently
function in dyads or triads?
4. What protocols and procedures are followed in decision making within dyads
or triads?
5. What are the perceived advantages and disadvantages of dyads and triads
against non-interdisciplinary teams?

MANAGEMENT MODEL IN HEALTHCARE SETTING 4
6. What are the perceived areas or facets of dyads or triads that may be modified
to improve effectiveness and efficiency?
Significance of the Study
The management of healthcare provision systems is a complex task primarily
because of long-range services provided and complex relationships among groups of
professionals involved in systems. The U.S. healthcare system has been greatly criticized
for its fragmented nature and significant numbers of preventable errors that have led to
death or injury (Kohn et al., 2000; Maxson et al., 2011). There is a great and urgent need
to modify the current system and develop one that is more robust, integrated, and safe. In
recent years, there has been an increase in the use of interdisciplinary or dyad
management models in healthcare systems. The dyad model allows physicians and
professional managers to share accountability and responsibilities towards improving
quality of care and services and optimizing financial performance without overburdening
patients or incurring large costs for the country (Zismer & Brueggemann, 2010).
However, as each healthcare organization is unique with respect to its size,
organizational members or employees, patients, protocols, and resources, the use of the
dyad management model would also vary accordingly. This Dissertation in Practice study
adds to current literature on dyad management models by providing case-based
information on the perceived advantages of the model, competencies perceived as
necessary for using the model, and the possible applications of the model. Consequently,
the results of the study may help to improve practice by providing empirically-tested,
effective, interdisciplinary decision-making protocols and suggesting areas of
improvement in the design and implementation of dyads. By exploring the use of

MANAGEMENT MODEL IN HEALTHCARE SETTING 5
interdisciplinary management models in a healthcare system from the perspective of
physicians and professional managers, the study provided more balanced perceptions on
the design and implementation of such models.
Aim of the Study
The purpose of this case study was to explore the experiences and perceptions of
physicians and professional managers on interdisciplinary decision-making teams in a
large healthcare organization. Findings on dyads and triads in the healthcare setting are
expected to aid in developing a decision-making model for interdisciplinary teams that
can be adapted to different settings, such as businesses, non-profit organizations, and
academic institutions.
Methodology Overview
The Dissertation in Practice study used the qualitative case study approach. Data
was collected by conducting individual semi-structured interviews with physicians and
professional managers from a chosen healthcare organization in New Jersey who have
experienced the use of a dyad management model. Additionally, the researcher conducted
a review and analysis of available documents on the organization’s policies and protocols
on the design and implementation of the dyad management model. These documents
provided insight on the procedures followed by dyad teams in setting standards, making
decisions, and managing staff.
Delimitations and Limitations
Limitations are potential weaknesses or problems with the design of the study as
identified by the researcher (Leedy & Ormrod, 2013). As in any instrumental case study,
this study is limited in its generalizability (Creswell, 2013). Additionally, because
MANAGEMENT MODEL IN HEALTHCARE SETTING 6
participation in the study was voluntary and no compensation was provided to the
participants, they were given the right to withdraw from the study at any time. As such,
the results of the study may not be truly or equally representative of the population of
physicians and professional managers in the hospital.
The delimitations of a study succinctly provide the boundaries and specify the
scope of the study (Leedy & Ormrod, 2013). This study was limited to physicians and
professional managers who were experienced in the dyad management model and were
currently employed in a single chosen healthcare organization in New Jersey. As the
participants were limited to physicians and professional managers, the perceptions of
other healthcare system employees, such as nurses who were not managers, aides, and
laboratory workers, were not represented in this report.
Last, as the researcher has significant experience in the healthcare setting and has
also participated in a number of dyad teams, he has already developed his own
perceptions about the model, its advantages and limitations, and its applications. In other
words, the researcher may have personal bias toward the use of such dyadic teams. In
order to control this bias, the researcher used bracketing, which involved setting aside his
own experiences and perceptions as much as possible in order to gather data and view the
case or phenomenon being studied with a blank or fresh perspective (Creswell, 2013). In
particular, the researcher ensured that questions asked to participants were free of
suggestive words and that the analysis and the final report only represented the responses
of the participants and not the researcher’s own perceptions.

MANAGEMENT MODEL IN HEALTHCARE SETTING 7
Leader’s Role and Responsibility in Relation to the Problem
This Dissertation in Practice study was designed to explore the experiences and
perceptions of physicians and professional managers on interdisciplinary decision-
making teams in a large healthcare organization. A large part of managing a healthcare
organization is leading subordinates and coordinating with co-managers or co-leaders in
order to provide best services at optimum costs while avoiding errors. As such, part of the
data collection and analysis was to determine the competencies and responsibilities of
both physician and non-physician leaders with interdisciplinary teams, and compare these
outcomes against known theories or models of leadership styles. Such knowledge on
leadership, based on literature and personal experience, allowed the researcher to analyze
and understand the perspectives of the participants better and to explain such rationales
and perceptions against established theories and models in the literature.
Summary
This Dissertation in Practice study was a case study that explored the experiences
and perceptions of physicians and professional managers on interdisciplinary decision-
making teams in a large healthcare organization. Interdisciplinary teams or dyadic
management teams are composed of individuals from different professions or sectors
who have different yet complementary responsibilities and tasks towards reaching a
single list of identified goals. In this study, such dyads were composed of a physician co-
manager and a professional co-manager. The use of such interdisciplinary teams in the
healthcare setting has increased in recent years as a means to improve services, optimize
resources, and minimize preventable errors by improving management and decision
making through the collaboration of co-managers.

MANAGEMENT MODEL IN HEALTHCARE SETTING 8
The case study was limited to physicians and professional managers with
experience in dyadic management teams and who belonged to a chosen healthcare
organization in New Jersey. Data on the experiences and perceptions of the participants
were collected through individual semistructured interviews and document analyses. The
results of the data analysis were used to develop a general decision-making model for
interdisciplinary teams that can be adapted in different settings, such as businesses, non-
profit organizations, and academic institutions.

MANAGEMENT MODEL IN HEALTHCARE SETTING 9
CHAPTER TWO: LITERATURE REVIEW
Introduction
This section provides a clear picture of the current use of interdisciplinary
leadership teams at various levels in healthcare settings. The first subsection provides a
brief review of recent research on the use of interdisciplinary teams in the healthcare
setting in the U.S. and globally. The second subsection presents a comprehensive
understanding of the professional setting of the study, the U.S. healthcare system, in
order for the reader to understand the context of the study. The third subsection provides
a brief description of a leadership theory that is most applicable in the study. The final
subsections provides the researcher’s reflections on the outcomes of the review of
literature, as well as a summary of these outcomes.
Interdisciplinary Decision making
Safety and effectiveness have been prominent issues in the U.S. healthcare setting
in recent years, especially with the release of reports and statistics on the number of
preventable errors that have led to death or injury (Kohn et al., 2000; Maxson et al.,
2011). Numerous strategies and interventions have been put in place in individual
hospitals, as well as the U.S. healthcare industry as a whole, in order to improve
procedures and protocols that ensure the provision of optimum care to patients and the
safety of patients, visitors, and hospital workers (Allen et al., 2015; Maxson et al., 2011).
These strategies often include the use of modified approaches that have been proven to be
effective in ensuring safety and efficiency in other hospitals, healthcare settings, and
industries (Allen et al., 2015; Carayon et al., 2014).

MANAGEMENT MODEL IN HEALTHCARE SETTING 10
As the provision of efficient and timely healthcare is a task shared among various
professionals, such as doctors of different specializations, nurses, aides, and laboratory
technicians, difficulties often arise when making decisions about the patients’ health and
safety. It follows, then, that the interdisciplinary nature of the hospital setting should be
considered in designing and implementing interventions to improve processes and
protocols in healthcare delivery. For this reason, many of the interventions established in
response to Kohn et al.’s (2000) report on the number of preventable adverse events in
the U.S. involved collaborative planning, design, and execution among the different
professionals in the healthcare setting.
Interdisciplinary Teamwork in the Healthcare Setting
Research and experience has shown that effective collaborative work among
healthcare professionals, most commonly between registered nurses and physicians,
results in lower morbidity and mortality rates, reduced cost of care, and fewer medical
errors (Maxson et al., 2011). Consequently, such effective collaboration can improve job
satisfaction and the retention of nursing staff (Maxson et al., 2011). Collaborative work
between registered nurses, physicians, and other healthcare staff vary in their objectives,
context, scope, and application, and can have their own advantages and weaknesses.
One example of interdisciplinary collaborative work within the healthcare setting
is the surgical team, which typically is comprised of a surgeon, an anesthesiologist, and
an operating room nurse (Walker, Reshamwalla, & Wilson, 2012). In order to improve
safety during surgery, the World Health Organization (WHO) published the surgical
safety checklist, which itemizes all tasks within the three phases of surgical work. The
checklist ideally serves as a tool for effective collaborative work among the members of
MANAGEMENT MODEL IN HEALTHCARE SETTING 11
the surgical team towards improving surgical outcomes (Walker et al., 2012). However,
studies showed that introducing modifications to established procedures, especially
changes to the safety culture in the operating room, presented significant challenges
(Walker et al., 2012). In general, the greatest challenge in shifting to the use of the
checklist was encouraging all teams and team members to adapt to the checklist culture,
i.e., its procedures and standards (Walker et al., 2012). Research indicated that effective
leadership and open communication among members of the interdisciplinary team were
critical to the successful and effective use of the checklist (Walker et al., 2012).
In a separate study, researchers asked registered nurses and physicians to describe
their perceived barriers to working in interdisciplinary teams wherein the work was
labeled as rapid-response, i.e., urgent critical care expertise provided to the patients’
bedside or wherever needed in the hospital setting (Allen et al., 2015). While nurses
indicated that difficulties arose when they activated the rapid-response team, none of the
physicians surveyed indicated any instances when they believed the nurses had activated
the rapid-response team inappropriately (Allen et al., 2015). This result implied that
nurses may feel certain insecurities about being in a team with doctors, despite their
capacity to do their jobs properly; thus rapid-response team leaders should ensure that all
members of the staff have adequate confidence about their capabilities and decision-
making skills. Both nurses and doctors also indicated that open communication lines
were highly important in ensuring that the proper response was provided in a timely and
efficient manner (Allen et al., 2015).
While interdisciplinary teams between registered nurses and physicians can be
within the context of the operating room or as a rapid-response team that provides urgent
MANAGEMENT MODEL IN HEALTHCARE SETTING 12
critical care to the patients’ bedside, such interdisciplinary teams may also be present at
management levels. For example, the Fairview Red Wing Health Services in Minnesota
implements the dyad model in management to improve physician and manager
coordination while enhancing clinical and operational outcomes (Baldwin, Dimunation,
& Alexander, 2011). In this dyadic system, a physician department head in each clinical
and medical department within the services coordinated with a nursing lead who was in
charge of operations (Baldwin et al., 2011). Unlike the traditional structure of hospital
services, wherein a medical practice committee oversees the assignment and practice of
physicians and other healthcare providers while also taking charge of administrative
processes, the dyadic system separates such responsibilities to the physician lead and the
nursing lead. Such coordinated division of tasks and responsibilities allows each of the
two leads to focus on their leadership responsibilities without overburdening them, thus
allowing them to perform their clinical tasks adequately. In other words, the dyadic
structure encourages quality, effective care and service, and appropriate behavior
(Baldwin et al., 2011).
Benefits and Drawbacks of the Dyadic Model
Perhaps the most obvious benefit of the dyad model is that it reduces the
traditional “us-them” perspective commonly present in healthcare organizations, wherein
physicians distance themselves from managerial roles and responsibilities and focus only
on their clinical practices. Such a perspective often leads to misunderstandings between
physicians and managers regarding policies, behaviors, and procedures. The dyadic
model addresses this divide in the traditional structure by involving the physicians

MANAGEMENT MODEL IN HEALTHCARE SETTING 13
throughout the managerial processes while also allowing managers to understand the
circumstances and perspectives of the physicians (Baldwin et al., 2011).
Additionally, the dyad model allows managers and physicians to make more
informed decisions as they bring in different perspectives to viewing a specific problem
or issue to be addressed (Baldwin et al., 2011; Reid Ponte, 2012). This increased
involvement in the decision-making process allows physicians, nurses, and other
members of the healthcare team to better consider alternative courses of action, arrive at a
consensus, and carry out plans with more knowledge, ease, and willingness.
However, dyads or interdisciplinary teams are not without disadvantages. One
obvious drawback of the dyad model is that it creates additional cost for the organization
(Baldwin et al., 2011). Specifically, time and money are needed to educate and train
physicians on managerial techniques and processes, which not only incurs expenses but
also takes them from their practices, i.e., their earning activities. Additionally, the success
of the dyad model is highly contingent on the capabilities of the manager, usually
someone with an MBA, to educate, train, and work with the physicians in the use of the
model. While the managers may be highly knowledgeable and experienced in decision
making and managerial strategies, they may have difficulty working in the unique context
of the hospital setting, as responsibilities, tasks, and authorities are shared between
various individuals in a non-pyramidal structure.
Competencies for Interdisciplinary Teamwork and Leadership
Studies have shown that interdisciplinary teamwork and leadership have led to
improvements in decision making, safety culture, and job satisfaction, both in the
healthcare setting and outside of it (Allen et al., 2015; Tremblay et al., 2014). However,

MANAGEMENT MODEL IN HEALTHCARE SETTING 14
physicians and nurses cannot simply be recruited to take part in interdisciplinary teams
and be expected to perform managerial tasks and exhibit leadership skills without any
background or training (Walker et al., 2012). Certain skills and competencies, aside from
technical skills required in the profession, are necessary for effective collaborative work,
even more so in effective interdisciplinary collaborative work (Walker et al., 2012). As
members of interdisciplinary teams are often trained differently and may follow
contrasting protocols, difficulties may arise during meetings, planning sessions, and in
decision making. Hence, interdisciplinary team leaders will need to be trained in
interpersonal relations and effective professional communication.
The effective sharing of leadership responsibilities with individuals from other
disciplines and professions requires much work, patience, discipline, trust, and effective
and honest communication (Reid Ponte, 2012; Walker et al., 2012). Continuing
professional education teaches and instills these skills and competencies n
interdisciplinary team leaders (Légaré et al., 2013). While there is already a widespread
use of interdisciplinary leadership teams for shared decision making in healthcare
settings, healthcare organizations and associations have yet to arrive at a unitary,
generally agreed-upon definition of shared decision making (Légaré et al., 2013). This
lack of consensus on definitions has also resulted in a lack of consensus on conceptual
frameworks for training in interdisciplinary leadership and teamwork and in identifying
core competencies needed for shared decision making (Légaré et al., 2013). While no
specific competencies have been identified as necessary precursors for successful
collaborative work, research and experience have shown that there are two broad
categories of competencies that physicians, nurses, and professional managers need for

MANAGEMENT MODEL IN HEALTHCARE SETTING 15
effective interdisciplinary teamwork (Légaré et al., 2013). These two competencies are
relational competencies and risk communication competencies (Légaré et al., 2013).
Relational competencies refer to the skills and abilities necessary for creating an
environment that is conducive to communication and interaction (Légaré et al., 2013).
These competencies may be used in the professional relationship between the healthcare
providers and patients, as well as among healthcare professionals. Risk communication
competencies refer to the ability to communicate information about health conditions, the
risks of interventions, and prescribed courses of action (Légaré et al., 2013). Clear and
detailed communication about such information is necessary for a team of physicians and
healthcare providers to arrive at a consensus on the best course of action to take in
specific circumstances.
The Healthcare Setting
The healthcare setting is a complex system because of the different professions
involved in the provision of healthcare, the various departments or disciplines within the
medical profession, and the different levels of organizational management. For example,
a typical healthcare organization includes nurses, doctors, laboratory technicians, aides,
and support staff. There are also typically several departments, such as oncology, internal
medicine, ophthalmology, and dermatology, among others. Additionally, a group of
professional managers are responsible for making decisions regarding management, staff
retention, finances, and organizational growth.
In recent years, especially with the publication of the Institute of Medicine’s
report on preventable adverse errors in both private and public hospitals, the U.S.
healthcare system has received significant criticism for its fragmented nature and its lack

MANAGEMENT MODEL IN HEALTHCARE SETTING 16
of safety (Kohn et al., 2000; Maxson et al., 2011). In response, healthcare organizational
managers and medical organizations have been developing and implementing programs
and modifying organizational operations and management to improve communication,
documentation, and safety (Allen et al., 2105; Baldwin et al., 2011; Maxson et al., 2011;
Walker et al., 2012). One of the most widely-applied interventions is the use of
interdisciplinary leadership at various levels of an organization to improve decision
making regarding the organization, policies, protocols, and procedures.
Interdisciplinary Leadership
Leadership has long been a topic of great interest in academe and in practice
(Lawrence, 2015; Margolis, Rosenberg, Umble, & Chewning, 2013; Reid Ponte, 2012).
Research in this area has mainly focused on leadership theories, best practices, and the
qualities of good leaders. Such work has led to the development of several leadership
theories that describe how leaders lead, how they influence their subordinates, and how
tasks are completed through the use of such methods (Reid Ponte, 2012). These
leadership theories can be applied in various fields and contexts, including politics,
sociology, businesses, and in ethnic groups. Leaders in business organizations are often
educated and trained to become leaders, especially those with Master’s degrees in
business or management. In contrast, doctors or physicians who hold leadership positions
often are not knowledgeable or well-trained in business and management concepts
(Baldwin et al., 2011). Physicians therefore need to increase their organizational
knowledge and managerial skills and use these in combination with their clinical
knowledge when taking leadership roles in healthcare organizations. Additionally, as

MANAGEMENT MODEL IN HEALTHCARE SETTING 17
physician leaders collaborate regularly with professional managers and other healthcare
professionals, they need to be trained in interdisciplinary leadership.
While there are numerous relevant leadership theories and best practices that may
be related and applied in this study, such as transformational leadership and charismatic
leadership, the most relevant theory is interdisciplinary leadership because of the context
of this study. Interdisciplinary leadership fosters collaborative work through open
communication lines through which leaders or managers in various departments or
professions can share their inputs or ideas regarding an issue, plan, or project (Reid
Ponte, 2012). In the healthcare setting, using the dyad model, triad model, or
interdisciplinary approach also increases the chances that the concerns and opinions of all
departments or professions (e.g., nurses, aides, doctors, and laboratory technicians) are
represented by their group leaders at the management level (Reid Ponte, 2012). Such
equal consideration of all perspectives involved in healthcare provision strengthens and
rationalizes decisions regarding objectives, priorities, resource allocation, and policies.
Typical interdisciplinary teamwork or leadership in healthcare organizations takes
the form of the triad. At the executive level are three co-managers: the chief nursing
officer, chief medical officer, and chief operating officer, i.e., a nurse leader, a physician
leader, and a professional manager (Reid Ponte, 2012). In such a structure, each of these
three members of the triad report to the president or chief executive officer and have
different but complementary tasks and responsibilities (Baldwin et al., 2011; Reid Ponte,
2012). Triads at the executive level brainstorm and collaborate to make decisions
regarding policies, program development, and staffing.

MANAGEMENT MODEL IN HEALTHCARE SETTING 18
At the service or frontline level, interdisciplinary leadership teams collaborate on
decisions regarding protocols, procedures, and standards (Reid Ponte, 2012). While
interdisciplinary leadership teams at the executive level focus on macro-level planning,
decision making, and implementation, interdisciplinary leadership teams at the service
level make decisions regarding the department and specific patients. For example, dyads
and triads at this level may collaborate on developing new programs and modifying
existing programs, maintaining and monitoring the quality of service, improving quality
of care, and managing finances and other resources.
Although the specific objectives and missions of each interdisciplinary leadership
team vary, there are general principles that guide such collaborative work. First,
interdisciplinary leaders should adhere to a philosophy of inclusion so that all team
members are involved in the planning and decision-making processes and all disciplines
are represented in the final plan (Reid Ponte, 2012). In addition to ensuring the
involvement of all leaders who represent the various disciplines, leaders must also
commit to representing their constituents by considering their opinions and ideas and by
ensuring transparency (Reid Ponte, 2012). However, as differing perspectives can be
expected, leaders should present unbiased opinions and consider the best options
regardless of the discipline of the team member who suggests the most plausible course
of action (Reid Ponte, 2012). Last, to ensure no redundancy in tasks and responsibilities,
interdisciplinary leaders should ensure that each member’s responsibilities are stated
properly and clearly and that each leader understands fully his or her responsibilities and
tasks (Reid Ponte, 2012).

MANAGEMENT MODEL IN HEALTHCARE SETTING 19
Reflections of the Researcher
The number of preventable adverse events in the country is alarming and warrants
effective and timely intervention. Adverse medical events include ttransfusion errors,
adverse drug events, wrong-site surgery, surgical injuries, avoidable suicides, treatment-
related infections, burns and falls, and even mistaken identity. This review of current
literature on the use of interdisciplinary leadership teams in the healthcare setting to
improve safety and outcomes in the hospital has provided evidence, and along with it
some hope, that preventable adverse events can be minimized. However, the review of
literature has also shown that much research still needs to be done. First, there is a need
to arrive at a concise and generally agreed-upon definition of interdisciplinary decision
making and leadership. This will allow for further work on establishing the necessary
competencies to perform effectively in such positions. When the competencies are
established, it will then be easier to develop continuing education curricula on
interdisciplinary teamwork, interdisciplinary leadership, and interdisciplinary decision
making.
Summary
Chapter 2 provided a review of current literature on the topic or problem
addressed in this study. The review showed that there has been a rise in the use of
interdisciplinary leadership teams at various levels in the healthcare setting to improve
safety and patient outcomes, as well as outcomes for the healthcare providers. Practice
has shown that the use of interdisciplinary teams has its benefits as well as its drawbacks.
Healthcare organizations thus need to design interdisciplinary teams such that they
perform at an optimum level. The review also showed that, while there is no established

MANAGEMENT MODEL IN HEALTHCARE SETTING 20
list of competencies needed by physicians and other healthcare providers to participate in
interdisciplinary leadership teams, there are general principles (e.g., inclusion,
involvement, and respect for differences) and skills (e.g., communication and group
dynamics) that practitioners have generally agreed upon as contingent to the success of
interdisciplinary leadership teams. Last, the review of literature provided a brief
description of the context of this study, the healthcare setting, and a discussion of
interdisciplinary leadership principles in practice.

MANAGEMENT MODEL IN HEALTHCARE SETTING 21
CHAPTER THREE: METHODOLOGY
Purpose of the Study
The purpose of this case study was to explore the experiences and perceptions of
physicians and professional managers on interdisciplinary decision-making teams in a
large healthcare organization.
Aim of the Study
The aim of this Dissertation in Practice study was to use the findings on dyads
and triads in the healthcare setting to design a decision-making model for
interdisciplinary teams that can be adapted in different settings, such as businesses, non-
profit organizations, and academic institutions.
Research Questions
In order to identify optimal ways of using interdisciplinary teams in the healthcare
setting, the design and conduct of this study were guided by the following research
question: What are the perceptions of physicians and professional managers on the use of
interdisciplinary teams or dyads/triads in healthcare management and decision making?
Specifically, data collection focused on answering the following sub-questions:
1. What factors are considered in creating and implementing dyads or triads?
2. What objectives, or for what purposes, are dyads or triads usually created?
3. What competencies are perceived as necessary to effectively and efficiently
function in dyads or triads?
4. What protocols and procedures are followed in decision making within dyads
or triads?

MANAGEMENT MODEL IN HEALTHCARE SETTING 22
5. What are the perceived advantages and disadvantages of dyads and triads
against non-interdisciplinary teams?
6. What are the perceived areas or facets of dyads or triads that may be modified
to improve effectiveness and efficiency?
Methodology
In this Dissertation in Practice study, the researcher used qualitative methods to
explore the use of interdisciplinary leadership teams in the healthcare setting. The use of
qualitative methodologies involved the use of an interpretive and naturalistic approach,
which allows the researcher to locate himself or herself in the world in order to study,
interpret, and represent a certain facet, event, or phenomenon (Denzin & Lincoln, 2005).
In other words, qualitative research allows the researcher to study things in their natural
settings and to attempt to describe and interpret events or phenomena based on the
meanings people assign to them (Denzin & Lincoln, 2005).
In this study, the researcher has chosen to use the case study methodology or
approach to qualitative research, which is appropriate when the objective of the study is
to understand an issue or problem by exploring and understanding a specific case as an
illustration or representation of the issue (Creswell, 2013). Case study research is
concerned with the exploration of one or more cases within a bounded system as a means
to study or understand a specific issue (Creswell, 2013). For this Dissertation in Practice
study, the issue being studied was the use of interdisciplinary leadership teams, and the
healthcare setting was the bounded system.
The case study methodology was appropriate for exploring the use of
interdisciplinary leadership teams within the chosen system of the healthcare setting

MANAGEMENT MODEL IN HEALTHCARE SETTING 23
because the aim of this study was to develop a model and to provide a deep
understanding of the issue, and there are clearly identifiable cases within the bounded
system, i.e., specific hospitals or healthcare facilities within the larger healthcare system.
The qualitative data collected were the perceptions and narratives of experiences of
doctors and professional managers who experienced participating in an interdisciplinary
team.
Measures of quality used included member checking, triangulation, and audit
trail. Member checking and triangulation enhanced the study’s credibility while creating
and providing an audit trail to increase the study’s dependability. These measures are
described in later sections of this dissertation.
Participants
In order to conduct this case study, the researcher chose a healthcare organization
in New Jersey that was both appropriate for the study and had dyads in place. First, the
researcher approached the president of the healthcare facility or the director for affairs to
explain the study and to ask for assistance in recruiting participants. Specifically, the
researcher asked the president or the director for referrals to doctors and professional
managers who held leadership positions on interdisciplinary teams in their facility. The
researcher then sent a letter to the suggested individuals. This letter explained the purpose
of the study, the methodology, and the specific details about the participants’ roles,
rights, and expectations. The researcher also indicated his contact information in the letter
so that the prospective participants were able to contact him for inquiries and to confirm
or decline the request to participate in the study.

MANAGEMENT MODEL IN HEALTHCARE SETTING 24
The prospective participants were given one week to respond to the invitation
letter. After such time, the researcher contacted by phone all prospective participants who
had yet to respond to the letter. Once all prospective participants were contacted, and the
researcher had already recruited at least eight participants from the different professions
(e.g., physicians and professional managers), the researcher scheduled an initial meeting
to debrief all of the study participants. In this initial meeting, the researcher briefly but
concisely explained the roles of the participants, answered any questions they had, and
scheduled the individual interviews. The researcher also asked the participants to provide
him a copy of relevant documents pertinent to the study.
Instrumentation
In order to gather the perspectives and narratives of the experiences of healthcare
professionals and professional managers on the use of interdisciplinary teams in the
healthcare setting, the researcher conducted semi-structured interviews with these
individuals. In order to understand the mechanisms and outcomes of interdisciplinary
leadership teams, the researcher also reviewed and analyzed documents and records on
the use of such teams. The researcher analyzed data gathered from the interviews, along
with the documents and records, in order to see which events or circumstances may have
caused or influenced the professionals’ perspectives and experiences. Triangulation, or
the use of multiple sources of data in a single study, is critical in case study research, as it
confirms and completes the collected data (Houghton, Casey, Shaw, & Murphy, 2013).
This process subsequently enhances the credibility of the study (Houghton et al., 2013).

MANAGEMENT MODEL IN HEALTHCARE SETTING 25
Overview of Data Collection
The issue explored in this Dissertation in Practice study was the use of
interdisciplinary leadership teams in the healthcare setting. In order to explore this issue,
the researcher gathered data from doctors and professional managers who had
experienced participating in an interdisciplinary team. As interdisciplinary leadership
teams were composed of professionals and individuals from different fields or
professions, it was important to gather the perspectives of these different groups of
individuals to better understand the issue. In healthcare settings, interdisciplinary teams
are usually dyads of a doctor and a professional manager or triads consisting of a doctor,
a registered nurse, and a professional manager. Hence, it was important to gather the
perspectives of healthcare professionals and professional managers in order to create a
deeper and more complete understanding of the use of interdisciplinary leadership teams.
The researcher inquired about these individuals’ personal opinions and
professional perspectives on the use of interdisciplinary leadership teams, as well as
reviewed and analyzed documents and records related to, and which emerged out of, such
teamwork. Throughout the data collection and analysis, the researcher maintained a
research journal wherein specific steps taken and procedures followed were noted for
documentation. This process allowed the researcher subsequently to reflect on decisions
that informed the procedures of the study. The journal also helped the researcher to create
an audit trail when writing the final study report. An audit trail is a comprehensive and
chronologically arranged set of notes on the context of the study, the provenance of the
data gathered, and the rationale for methodological decisions, especially data analysis
(Houghton et al., 2013). Including an audit trail in the final report of the study allows

MANAGEMENT MODEL IN HEALTHCARE SETTING 26
readers to better understand or discern the researcher’s interpretations and
methodological decisions, thereby increasing the study’s dependability (Houghton et al.,
2013).
Procedures
There were a total of three meetings with the study participants. The first meeting
was between the researcher and the participants as a group. This meeting served as a
debriefing meeting wherein the researcher introduced the study and explained the
participants’ roles, responsibilities, rights, and expectations. The researcher discussed
with the participants their preferred schedules for the semi-structured interviews.
The second meeting consisted of the individual, semi-structured interviews. As it
was expected that the participants had very rigid schedules, they indicated their preferred
dates and times for the individual interviews. These interviews took place in the
participants’ offices within the healthcare facility, where privacy and a professional
atmosphere was expected. The interviews typically lasted for about an hour and a half to
two hours. It was at this point that it was very critical for the researcher to uphold
bracketing, or epoche, wherein the researcher or analyst sets aside his own experiences
and perceptions as much as possible in order to gather data and view the case or
phenomenon being studied with a blank or fresh perspective (Creswell, 2013).
As the interviews were semi-structured, the researcher followed the interview
guide (see Appendix A); however, the participants were allowed some leeway to discuss
other matters as they deemed them relevant to the study. The participants also brought to
the interview copies of any documents they may have possessed regarding their
experience working in interdisciplinary leadership teams. Such documents included

MANAGEMENT MODEL IN HEALTHCARE SETTING 27
minutes of meetings, project and program documentation, memos and letters, and final
reports.
The third meeting was also one-on-one between the researcher and the participant.
The purpose of this meeting was for member checking, which is the process wherein
participants verify the transcriptions of their own interviews (Koelsch, 2013). In this
meeting, the participants were allowed to modify or delete certain parts of their responses
during their interviews. This step ensured that the researcher had indeed gathered data
and understood the participants’ perceptions and experiences based on their own
accounts.
Data Analysis Plan
In line with typical case study research, it was important to analyze the data from
both data gathering procedures (interviews and document analysis) together and in
chronological order, such that the individual perceptions were related to events within the
case (Creswell, 2013). Hence, the first step in data analysis was to lay out the timeline of
events from the creation of the interdisciplinary team until the time of data collection.
Then, the researcher identified and described the members of the known teams, the
objectives of the teams, the programs and projects of each team, and the tasks and
responsibilities of each of the members. Much of this information was extracted from the
review of the documents provided by the participants.
Next, the researcher incorporated the responses of the participants during the
interviews into the timeline. Specifically, narrated experiences and shared perceptions
and opinions were related to the specific team and specific event to which they refer. This
allowed the researcher to better understand the circumstances that led to such responses

MANAGEMENT MODEL IN HEALTHCARE SETTING 28
from the participants. The researcher then analyzed the timeline by identifying events that
led to positive opinions and successful outcomes, as well as events that led to negative
opinions and unsuccessful outcomes.
Throughout the data collection and analysis, the researcher identified and noted
instances wherein the participants exhibited leadership qualities and managerial skills.
Physicians in leadership roles are often untrained for such positions; hence, it was
expected that the professional managers were more adept at using managerial skills and
applying leadership theories. During the interviews, the participants were asked to reflect
upon or analyze their own participation and the participation of others and describe
whether they thought leadership qualities were applied in certain circumstances.
Reliability and Trustworthiness
Through the development of the methodology and specific procedures for this
Dissertation in Practice study, the researcher has realized the difficulties of conducting a
qualitative study, especially one conducted in a setting that was already very familiar to
the researcher. This difficulty arose when, no matter how hard the researcher tried, there
was some level of bias in the conduct of the study as a result of the researcher’s own
experiences in the same facility and knowledge about the professions and about
leadership skills, qualities, and theories. Having realized this, the researcher decided to
exert even more effort and be more conscious about specific instances wherein personal
bias may have hindered his professionalism, and he subsequently took measures to
address this problem. Additionally, the researcher took the time to reflect after each
interview and throughout the data analysis process in order to recognize instances of bias
and prejudice and to resolve them.

MANAGEMENT MODEL IN HEALTHCARE SETTING 29
Ethical Considerations
Because the personal opinions, perceptions, and professional experiences of
individuals were involved in the conduct of this study, it was important to protect the
identity of the participants throughout data collection and analysis, as well as in the final
product. In order to ensure the personal comfort of the participants, they were allowed to
refrain from responding to questions they did not feel comfortable answering, and they
were provided the right to withdraw from the study at any time. In order to protect the
participants’ identities, the researcher took measures to ensure that no one was able to
identify specific participants’ contribution or participation in the study. The participants
were referred to by a code in the audio recordings of their interviews, the transcriptions of
their interviews, and in the documents that they provided. The participants were also
referred to by code in the final, written dissertation. Last, the audio recordings and
transcriptions were kept in a safe and secure location known only to the researcher and
his adviser, where they will be stored for up to five years from the conduct of the study,
after which such data will be destroyed. Additionally, the researcher went through the
IRB at Creighton University and had permission from the institution as well.
Reflective Practices
In order to document the entire experience of writing and conducting this study,
the researcher kept a journal wherein all interview transcripts, interview analysis, notes,
ideas, and reflections were written down for documentation and future reflection. The
researcher also noted his reflections and perceptions about each of the interviews after
each concluded. The researcher also noted contextual descriptions in this notebook to
provide background and circumstantial information that may have influenced the

MANAGEMENT MODEL IN HEALTHCARE SETTING 30
researcher’s opinions, thoughts, and perceptions at the time of writing. Such contextual
descriptions included the weather, current events, and the researcher’s other
commitments and personal events and experiences.
Summary
The purpose of the Dissertation in Practice study was to explore the experiences
and perceptions of physicians and professional managers on interdisciplinary decision-
making teams in a large healthcare organization. This was conducted through a single
case study. The researcher gathered data from physicians and professional managers who
had experience with participating in an interdisciplinary leadership team. Data were
gathered through individual, semi-structured interviews and document analysis. The data
were analyzed and presented as a chronology of events that included specific information
about the interdisciplinary teams, their objectives, programs, and projects, the individuals
involved and their specific tasks and responsibilities, the outcomes of the teams and their
projects, and the perceptions of the participants regarding the entire endeavor.
Subsequently, the researcher identified events that led to positive opinions and successful
outcomes, as well as events that led to negative opinions and unsuccessful outcomes.

MANAGEMENT MODEL IN HEALTHCARE SETTING 31
CHAPTER FOUR: RESULTS
Introduction
Chapter 4 presents the results from the thematic analysis of the interviews with
healthcare professionals from a healthcare organization. The purpose of the study was to
explore the experiences and perceptions of physicians and professional managers on
interdisciplinary decision-making teams in a large healthcare organization. The
researcher also wanted to extract meanings and themes directly from the perceptions and
experiences of the healthcare professionals about the dyad management model and its
effectiveness in the healthcare setting. The computer software program NVivo10 by QSR
was also employed to aid in the organization and systematic coding of the responses of
the participants. The researcher addressed the main research question of the study, which
was: What are the perceptions of physicians and professional managers on the use of
interdisciplinary teams or dyads/triads in healthcare management and decision making?
The following research sub-questions were the focus of the study:
Research Sub-question 1. What factors are considered in creating and
implementing dyads or triads?
Research Sub-question 2. What objectives, or for what purposes, are dyads or
triads usually created?
Research Sub-question 3. What competencies are perceived as necessary to
effectively and efficiently function in dyads or triads?
Research Sub-question 4. What protocols and procedures are followed in
decision making within dyads or triads?

MANAGEMENT MODEL IN HEALTHCARE SETTING 32
Research Sub-question 5. What are the perceived advantages and disadvantages
of dyads and triads against non-interdisciplinary teams?
Research Sub-question 6. What are the perceived areas or facets of dyads or
triads that may be modified to improve effectiveness and efficiency?
Purpose of the Study
The purpose of this case study was to explore the experiences and perceptions of
physicians and professional managers on interdisciplinary decision-making teams in a
large healthcare organization.
Aim of the Study
The aim of this Dissertation in Practice study was to use the findings on dyads
and triads in the healthcare setting to design a decision-making model for
interdisciplinary teams that can be adapted in different settings, such as businesses, non-
profit organizations, and academic institutions.
Servant Leadership
The healthcare organization used for the study was a major healthcare provider in
New Jersey. It is a $750 million business enterprise and one of the largest employers in
its geographical area, with more than 5,200 employees and 600 physicians on its payroll.
As the region’s provider of health and wellness services, this organization’s goal is to be
the best in five business areas – Best People in the Workplace, Best Customer
Experience, Best Quality, Best Growth, and Best Financial Performance.
The organization understood that, to achieve those goals, it had to build an
engaged and committed internal culture. Creating an engaged workforce plays a large
part in that effort, and the organization ensures that its employees understand how their

MANAGEMENT MODEL IN HEALTHCARE SETTING 33
individual efforts contribute to the achievement of organizational goals. A second
important factor in this organization’s success is its leadership team’s commitment to the
principles of Servant Leadership. All of the organization’s managers go through a 33-
week experiential course on Servant Leadership, which involves classroom activities and
training in 360-degree feedback.
Dyad Decision Making Model
The dyad decision-making model is based on an interprofessional approach to
shared decision making (SDM), and this SDM model assumes that at least two healthcare
professionals from different professions collaborate to achieve SDM with the patients,
either concurrently or sequentially (Légaré et al., 2011). The organization where the
study was conducted takes this model and adjusts it into one where two leaders, one
clinical and one from the administrative position, make the decisions.
The dyads are all composed of one male member and one female member. One of
the members of the dyad is a physician with clinical expertise and experience. The other
member of the dyad is generally an associate vice president and has both an MBA and
training in Servant Leadership. All of the dyad members are experienced leaders and
subject matter experts in their respective areas of expertise.
Description of the Sample
Eight participants were recruited for the study from different departments in the
healthcare organization. Interviews with eight physicians and professional managers on
the use of interdisciplinary teams or dyads/triads in healthcare management and decision
making were conducted to gather their perceptions and experiences. Table 1 describes the
backgrounds of the eight participants.

MANAGEMENT MODEL IN HEALTHCARE SETTING 34
Table 1 Backgrounds of the Study Participants Participant Background Participant 1 Chairman of Emergency Services Participant 2 Service and Satellite Emergency Department Participant 3 Clinical Nurse (Private and Public Practice) Participant 4 Neurosciences, Administration, and Quality Manager Participant 5 Chairman of Critical Care Participant 6 Assistant Vice President of Nursing Participant 7 Medical Director for Hospital Medicine and Chief of the
Medicine Service Line Participant 8 Assistant Vice President for Medicine and Pharmacy Service
Lines
Data Analysis
The researcher performed a qualitative thematic analysis on the participant
interviews. The thematic analysis of the interviews allowed for the discovery of the major
findings and themes that address the main research question, as well as the six research
sub-questions of this study. Creswell (2003) explained that the qualitative thematic
analysis approach provides the foundation for meaningful “descriptions of the
phenomenon” to be established using the clustered codes and themes from the data (as
cited in Wolhuter & de Wet, 2014, p. 64). The researcher then followed the steps reported
by Attride (2001), where the responses of the physicians and professional managers were
analyzed by: (1) “familiarizing with the data; (2) conducting the initial coding; (3)
searching for themes; (4) reviewing of themes; (5) defining and labelling of themes; and
(6) developing of thematic networks” or relationships from the clustered responses (as
cited in Issa, Isaias, & Kommers, 2013, p. 219). In the presentation of findings, the
clustered themes that received the most number of occurrences are considered as the
major findings, and those that followed are the themes of the study or the other

MANAGEMENT MODEL IN HEALTHCARE SETTING 35
significant perceptions and experiences. In the next section, the verbatim texts from the
interviews are also included for better understanding of the findings.
Presentation of Findings
Major Finding 1: To Produce the Best Solutions for Patient Care
The first major finding that emerged was the factor for producing the best
solutions for patient care. This was based on the first research question, which was the
factor in creating and implementing dyads or triads. The first major finding received five
occurrences from the responses of the eight participants, or 63% of the total sample
population. Table 2 contains the major finding and other themes discovered from the data
analysis that addressed the first research question of this study.
Table 2 Factors Considered in Creating and Implementing Dyads/Triads
Major Finding and Theme Number of
Occurrences Percentage of Occurrences
Major finding 1: To produce the best solutions for patient care
5 63%
Theme 1: Aligning the overall vision of the hospital or campus
4 50%
Overall, the first major finding was the factor of wanting to produce the best
solutions for patient care. The researcher considered this finding as one of the six most
significant findings of the study. Participant 1 stated that one factor in creating and
implementing dyads is coming up with the best ideas and solutions for the patient:
There is no hierarchy at all. We are, you know, considered equivalent to each
other when we’re trying to discuss or, you know, come up with an idea or a
solution to a problem, and any protocols that we would develop to put into place
MANAGEMENT MODEL IN HEALTHCARE SETTING 36
for our team to use would also include input from the key stakeholders in those.
So it would be the physician leadership and the nursing leadership all coming
together, identifying what the problem or issue is, and then coming up with all the
potential solutions and then sorting through those solutions and then picking what
the group believes is the best solution to start with.
Participant 2 echoed how another factor is a focus on improving the patient care:
You know, it is a hard question when you’re describing yourself and you think
about it. Um, I, I truly want to be a partner with, um, whoever I’m working with.
I’m truly there trying to advance emergency nursing and, and improving the care.
So I, I do want to be a partner and, um, I’m flexible. I would say I’m very
flexible, 98% of the time.
Participant 4 shared how the main factor considered in establishing the dyad care
is improving the services and developing the best quality care for patients:
In today’s healthcare system, you cannot successfully run as an organization
without having a dyad approach. You 100% need physician engagement
paralleled with your administrators in order to have, you know, an optimal
organization running because o- one can't function without the other. You need
that clinical expertise, you need that engagement for, I mean I could go on and on
and on but for m- almost every single reason from the cost standpoint, you know,
from billing, from quality of care, from strategic planning and, you know, adding
in new services. If you, you're going to fail if you don’t have physician
engagement. It’s that’s the new strategy that you’re going to see everywhere
today, you have to have that buy-in position so I, I know there are some hospitals

MANAGEMENT MODEL IN HEALTHCARE SETTING 37
out there that are very corporate heavy, C-suite heavy as we say where it’s very,
very, you know, y- you’re being, and I have nothing against, you know, there’s a
lot of MBAers, a lot of MBAers out there...
Participant 6 shared that dyads were formed to develop the best and safest patient
care that they could provide:
Well in, in healthcare we’re fortunate enough that we do go to the evidence. We
go to the evidence, and then if we wonder… take time as a factor. We’ll look for
further evidence around success even in time, to set reasonable goals to not be
you know, not approach it out of emotion, not approach it out of any, you know,
different perspective other than for safe patient care and the evidence that governs
that. I think that helps us keep our decisions very uh… I don’t know, we’ve made
some really good ones.
Participant 7 stated how the United States has the most expensive healthcare, and
thus it is right to provide the patients with the best care that they could give:
What you see is this line right here is the United States. We have the most
expensive healthcare in the world, period. Okay. So that should equate to we get
the best bang for the buck. This is a subsequent piece of information. It talks
about life expectancy at first. So even though we are the most expensive
healthcare in the world, we don’t live nearly as long as some of those on average
that are a lot cheaper.
The first and only theme that followed the major finding was the factor of
aligning the overall vision of the hospital or campus. The theme received four
occurrences, or 50% of the total sample population. Participant 3 shared that the model

MANAGEMENT MODEL IN HEALTHCARE SETTING 38
has been beneficial, since it helps the hospital align its vision:
I think overall if I... If you put me on the spot right now, I think it is a beneficial
model. I’m actually glad that AtlantiCare is moving towards that model. It helps
to balance and align the vision, if there’s vision. I think to help lay out, you know,
the strategy and again, if it’s working, if everything is working and kicking all of
the cylinders together, alignment, strategy, vision and the balance of clinical and
admin, it’s a slam dunk model. It’s a great model.
Participant 5 shared how they create dyads to agree and align the vision of the
organization in the end:
I think since most of us go into the dyad knowing that we need to agree to agree,
we work together to work out the process. And sometimes as in with my first
dyad partner, that’s sitting down and having some very frank and… and honest
conversations about this makes me uncomfortable or I think you’re being too
much of a… a heavy person here or me saying I think you’re not dealing directly
with the issue and you’re being too kind and not holding people responsible
enough until we… sort of an iteration process where in the beginning there were
lots of those conversations and an honest attempt by both of us to move closer to
the middle.
Participant 6 echoed the importance of leaders coming together to reach the vision
and mission of the organization:
And so for me, I do believe we are reaping the benefits of seeing the two partners,
the two leaders come together, have the shared vision, mission, the goal, the
purpose and stay the course. We may be redirected, the time, the climate, the
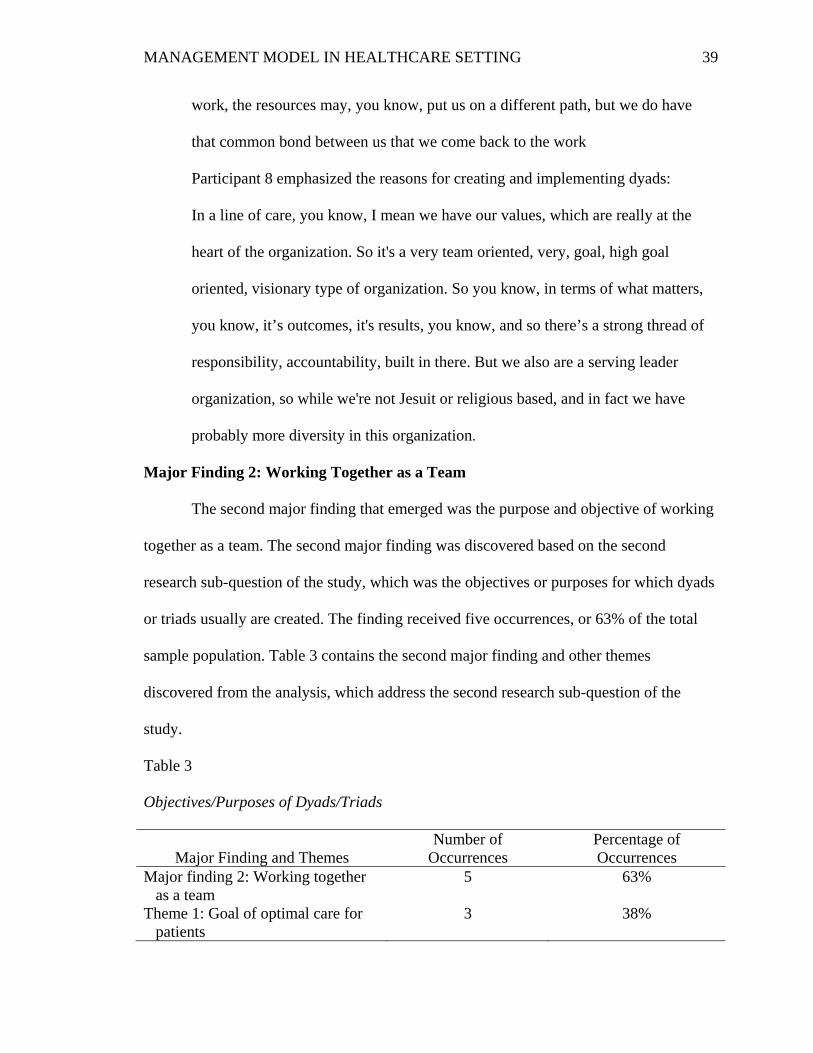
MANAGEMENT MODEL IN HEALTHCARE SETTING 39
work, the resources may, you know, put us on a different path, but we do have
that common bond between us that we come back to the work
Participant 8 emphasized the reasons for creating and implementing dyads:
In a line of care, you know, I mean we have our values, which are really at the
heart of the organization. So it's a very team oriented, very, goal, high goal
oriented, visionary type of organization. So you know, in terms of what matters,
you know, it’s outcomes, it's results, you know, and so there’s a strong thread of
responsibility, accountability, built in there. But we also are a serving leader
organization, so while we're not Jesuit or religious based, and in fact we have
probably more diversity in this organization.
Major Finding 2: Working Together as a Team
The second major finding that emerged was the purpose and objective of working
together as a team. The second major finding was discovered based on the second
research sub-question of the study, which was the objectives or purposes for which dyads
or triads usually are created. The finding received five occurrences, or 63% of the total
sample population. Table 3 contains the second major finding and other themes
discovered from the analysis, which address the second research sub-question of the
study.
Table 3
Objectives/Purposes of Dyads/Triads
Major Finding and Themes Number of
Occurrences Percentage of Occurrences
Major finding 2: Working together as a team
5 63%
Theme 1: Goal of optimal care for patients
3 38%

MANAGEMENT MODEL IN HEALTHCARE SETTING 40
The researcher considers the second major finding, which was the goal of
working together as a team, as one of the six most vital findings of the study. Participant
2 stated that one important objective upon creation of the dyad is that everybody has to
work together as a team to produce the best outcomes and results: “Everybody has got to
get on board.” Participant 3 stated how one objective upon the creating of dyads is to
work together equally, as a team:
Yeah. Exactly. There was no, um, one upping of each other. One would, you
know, back off on if a clinical question came up, the administrative person would
defer to the clinical person, the clinical person would defer on the administrative
question to the administrator. So, there was respect of each other’s, you know,
um, expertise. And they had buy-in from the seniors so they got it done. Um, so
that’s where I’ve seen that work extremely well, and they both had mutual support
for their goal.
Just like a bad marriage, you know, and then you’re like trying to figure
out, you know, relationship dynamics.
Participant 5 shared the different goals and procedures that her dyad teams practice:
It is. In the first dyad with the AVP that resides in the other facility, decisions are
2 thumbs up decision. There is… we don’t leave the meeting until we both agree
on a course of action. In the more informal one, what will often happen is a
decision is made by one or the other of the dyad leaders bounce off of the
respective partner and it’s a yay or a nay. Generally speaking it’s a yay without a
whole of discussion because it’s somewhat of a logical process. In the third one
MANAGEMENT MODEL IN HEALTHCARE SETTING 41
decision are made generally by me and this is one… the sepsis work but then
assessed for efficiency, practicality, doability by the other dyad partners so it’s
more of a veto vote than a governing vote.
Participant 6 compared working in dyads as a marriage in which the teams should
agree to reach and achieve the best care for their patients:
I have remembered reading the article where, again, it’s this marriage, it’s this
partnership and I thought what’s in between us so that it’s never the blame. You
don’t, you never blame each other. You don’t get to walk away because the bond
you have is the patient, first and foremost, and the organization. So the dyad in
my opinion truly is that marriage and it is about co-submission. It is about no
matter what, at the end of the day getting along because there is a patient and
there is the organization. So that’s how I see it.
Participant 8 also emphasized the importance of having an effective model for
teams:
I think the dyad model is effective. I think that it, it asses some structure that
previously you had to connect, you know what I mean? So if I on my own, as the
pharmacy executive, needed to impact something relative to the hospital doctors, I
can’t even think about the steps I’d have to take. But now it’s assed.
The first and only theme that followed the second major finding was the goal of
optimal care for patients. The theme received three occurrences, or 38% of the total
sample population. Participant 1 shared the importance of having the goal of optimal care
for patients or quality service that the patients deserve:

MANAGEMENT MODEL IN HEALTHCARE SETTING 42
We discuss what, and make sure that the, the nursing and the physician, goals and
objectives are, you know, aligned, so that, you know, again, that’s, that’s the basis
and, and the ultimate, sort of what’s the word I wanna use? The ultimate goal is,
you know, for optimal patient care. So that’s sort of the great equalizer of while
the influences and the, you know, the, the ability to a chain, attain those goals
maybe, you know, coming from different directions, at the end of the day, the,
you know, the question that, you know, is the thing that levels the playing field is,
well, what is, what is it that's gonna best serve the patient? [The patient care is
always the core.]
Participant 4 stated that the main goal of the dyad approach is to provide the
lowest cost with the best optimal care and outcome:
So, pretty much everything and anything we do, we take the dyad approach to…
and that combined, you know, both administrator and physician because that’s the
only way you can effectively run the service line. With, you know, our goal is,
obviously, you know, lowest cost with optimal patient care and outcome, so the
only way to succeed as best we can with that is, is doing the dyad approach. So,
we meet on a daily basis. We check in. We have a neurosciences steering
committee meeting, which is ran by myself and the physician lead as my support
for that. We also are on clinical effectiveness teams together as well and those
meet monthly. Again, same thing as far as reducing costs and continuing to
provide optimal patient care. So you have to have that really, really strong
personality, not confrontational but to speak up.
MANAGEMENT MODEL IN HEALTHCARE SETTING 43
Participant 7 explained the goal of the dyads as delivery of quality healthcare to
the patients:
That’s why you have a dyad relationship in this type of a setting and a service line
setting because if I just operated on cost, I take every patient to the operating
room necessarily or unnecessarily. We know how that turned out just recently
with the oncologist in Michigan. I mean, that was his model. He got paid for it
and he’s in jail now but the reality is that isn’t what healthcare is about. So it’s…
it’s balancing the scope of the industry to accomplish that Triple Aim. You have
to deliver quality. It has to be done efficiently. I can’t bring people into the
hospital anymore for… for, you know 10 days to run tests and run more tests. It’s
probably focused and then keeping the customer at the center.
Major Finding 3: Ability to Support Arguments with Evidence
The third major finding that emerged was the ability to support arguments with
evidence. The third major theme was gathered from the third research sub-question,
which was the competencies perceived as necessary to effectively and efficiently function
in dyads or triads. The third chief finding received five occurrences, or 63% of the total
sample population. Table 4 contains the third major finding and other themes discovered
from the analysis, addressing the third research sub-question of the study.

MANAGEMENT MODEL IN HEALTHCARE SETTING 44
Table 4
Competencies Perceived as Necessary for Members of Dyads/Triads
Major Finding and Themes Number of
Occurrences Percentage of Occurrences
Major finding 3: Ability to support arguments with evidence
5 63%
Theme 1: Good communicators 4 50% Theme 2: Flexibility in working with
others 3 38%
Theme 3: Formal education and experience
2 25%
Theme 4: Strong personalities to convince buy-in
2 25%
Theme 5: Positive mentality 1 13% Theme 6: Credible reputation 1 13%
Overall, the researcher considers the third major finding, which was having the
ability to support arguments with evidence, as one of the six most important findings of
the study. Participant 2 also suggested how the members should be able to present and
back up their arguments with concrete data:
You always have to have data to back up your argument. I mean nobody will
listen to you without the data.
You have to have it, or else you’re just spinning your wheels. What’s very
helpful is the individual report cards. So every physician has a report card. Um,
we haven’t gotten to that point with nursing. But every physician has a report
card, and so we know how many patients they see. We know how many studies
they ordered, the over-utilizers, the under-utilizers.

MANAGEMENT MODEL IN HEALTHCARE SETTING 45
Participant 4 explained the importance of dyad members being able to support
their arguments or having evidence-based claims:
I’ll give you an example, we were you know, questioned on our neurotransfer
process and we were told that, you know, it was not working. Our team, our dyad,
protocol that our dyad, we had put together was not working. And it’s very
simple, we always ask people why, give us facts not emotions. I always say I
don't want me e-mails to ever be emotions... Everything is factual. Everything is
fact-based.
Participant 5 also described the importance of having the skill set for data analysis:
My personal leadership quality is in skills. I think of… revolve around the fact
that I’m very good at data analysis. I can pick out patterns from the noise very
easily and very rapidly. I can assess whether or not data is sound pretty quickly
and one of our problems has been the inability to get good pure data. Across all
my dyads that has been a challenge and I have had to work with different software
systems, different report writers and different purveyors of the data to finally get
information that we can rely on. And that’s probably one of the best things that I
brought to my team is the assurance that when we’re looking at numbers, they re-
reflect the reality of the situation.
Participant 6 again highlighted the importance of having concrete evidence to
support their proposals:
You know, fortunately in healthcare you always go to your evidence. So you find
out quickly who else is doing what, what the evidence shows we should be doing.
Now let’s look at the data, what are we doing and where are the gaps and let’s go

MANAGEMENT MODEL IN HEALTHCARE SETTING 46
correct. That, which was really pretty much our approach to it. So we kind of…
there were times where just our relationship could be strained due to the others on
the team straining, but certainly it was always united we stand. We never outright
had that dialogue. I think we just perceived it from each other, just knowing
leadership. I think we both have a strong background in understanding effective
leadership. And so we would go in the room and we would be united, but the team
really had to do a lot of relationship building and learning and communicating.
The first theme that followed the third major finding was the competency of being
good communicators. The finding received four occurrences, or 50% of the total sample
population. Participant 1 stated the importance of the members being good
communicators, where they can communicate about the best care that they can provide to
their patients:
And, and that, the best form or the best success that I found in negotiation is good
communication. So, you know, having, again, the, the patient care as the, you
know, as the, you know, the core focus, that helps to re-orient, you know,
conversations and meetings. When they start to get a little bit down into the weeds
of opinion and maybe prior experience, or projected, you know, outcomes, and we
can say, “Well, let's deal with the here and now” and let’s deal with the
equipment, the resources that we have available to try and achieve this goal with
what we have or if we need to attain something, how do we work together and get
some economy of scale and the latter voice to be able to attain what that resource
is by saying it’s not just one of the two entities, but it’s both entities that feel that
this is really important to try and get done.
MANAGEMENT MODEL IN HEALTHCARE SETTING 47
Participant 3 shared how vital it is to have members of the dyad who know how to
communicate and respect the opinions of one another:
Here’s the con of the dyad model is when you have two, you know, when you
have two leaders who are both excellent leaders but have two different ways of
thinking about the outcome or ways to get to the outcome or don’t agree or, you
know, are not aligned about even the outcome itself. “Why are we doing what
we're doing? I don't think we should do A. We should do B.” It’s I think the
communication then... If you don’t have alignment, the communication is either
good communication but they’re not communicating key things or there’s poor
communication because now we’re not getting along because so we, we’re not
aligned.
Participant 7 stated that one important competency is being able to communicate
the objectives of the task clearly:
Communicating objectives. The first part is to … What are the objectives? What
are you trying to accomplish by the decision that you’re making, is the decision
you’re making going to work to stabilize the program and everything that we
work on is a model that I kind of put forward that our job in this dyad relationship
is to keep the ship afloat and moving forward. We’re trying to get our team from
point A to point B and we’re trying to keep that ship afloat despite the fact that
every day somebody is drilling a hole into the bottom of the ship and they ship is
sinking. And we have to, you know… We have to keep that ship afloat and what’s
what we talked about with our leadership team too.

MANAGEMENT MODEL IN HEALTHCARE SETTING 48
Participant 8 also shared an experience of how she communicates with her dyad
partner:
So the site directors, I meet with Tony constantly. Like we’re in constant
communication. In fact, he calls me his work wife. And I’m like, “Really? That’s
a bad thing.” But like, there’s nothing for me to be riding home for, from work at.
I’m thinking I’m done, phone will ring, “Hi, it’s me just checking in.” It’s like,
who do you need to check in with?
The second theme that followed the third major finding was the competency of
flexibility in working with others. The finding received three occurrences, or 38% of the
total sample population. Participant 2 shared how another competency is the flexibility to
work with others:
You know, it is a hard question when you’re describing yourself and you think
about it. I truly want to be a partner with whoever I’m working with. I’m truly
there trying to advance emergency nursing and, and improving the care. So I, I do
want to be a partner and, um, I’m flexible. I, I would say I’m very flexible, um,
98% of the time.
Participant 3 added that members of the dyads should also know how to balance
their work among each other:
Yeah. I agree with that. I, and I think there are still sharing. I think everyone is
trying to get along and say... They’re trying to play to their strengths, you know,
Hey, “Do you feel passionate about that? Or you go to that, you wanna take that
one?” Okay. Well, then next time something circles back, I’ll take it or ... I, I

MANAGEMENT MODEL IN HEALTHCARE SETTING 49
think between all the dyads I have worked with, there is a sense of fairness that
they do try to equally balance themselves.
Participant 4 shared that one competency of her team is being able to balance their
work effectively:
No, we balance each other because Ed is very particular on especially when it
comes to data and information, as he was just saying. So I complement that by,
you know, maybe taking it a step further in, in terms of, you know, God, I don’t
know how to say this politically correct, this is hard.
The third theme that followed the third major finding was the competency of
having formal education and experience. The finding received two occurrences, or 25%
of the total sample population. Participant 1 stated the equal importance of educational
and experience competencies:
I think they’re very similarly aligned. You know, I think that she comes with,
some, both formal education and some, you know, years of experience. So the
combination of those two, I think, really, you know, they complement each other.
And that’s what I found in myself as well. So then you can take those, you know,
complementary attributes and say, “Here’s the commonalities from what we’ve
learned experientially and here's the commonalities from what we’ve learned from
formal education and this is the way that we can sort of enhance each other's
experience and education to achieve a higher goal.”
Participant 7 simply shared that: “Experience is probably the number 1 thing. I’m
a more senior physician. I’ve been doing this for 20 years as a physician but I was an
army officer before that.”

MANAGEMENT MODEL IN HEALTHCARE SETTING 50
The fourth theme that followed the third major finding was the competency of
having and developing strong personalities to encourage buy-in. The finding received two
occurrences, or 25% of the total sample population. Participant 4 highlighted that another
competency would be having strong personalities to encourage buy-in from stakeholders:
With just our overall decision making when we roll something out. I think we’re
very successful because, personalities. You have to be thick-skinned in -
especially when you don’t have jurisdiction and you have to mandate something
over people who you don't have jurisdiction. You have to be almost like a car
salesman with the neuroscience’s service line, truly. Because you have to, you
have to have the strong personality for the mandated p- parts, like I said, with the
joint commission and the state, and then with the things that technically aren’t
mandated but you want to put, implement in place because it’s the best for the
growth of the service line, that’s where you kind of have to be that car salesman.
Participant 5 echoed how one of her competencies is being able to convince other
stakeholders to support their decisions and potential approaches:
My other skill is that I have the ability to get other people to rally around the
cause by first being a role model and modelling the actions that I’m asking them
to do, but also to be able to assist them in overcoming whatever barriers they
have. So my role is to remove barrier… systemic barriers in the healthcare
system.
The fifth theme that followed the third major finding was the competency of
having a positive mentality. The finding received just one occurrence, or 13% of the total
sample population. Participant 1 highlighted the importance of having a “win-win

MANAGEMENT MODEL IN HEALTHCARE SETTING 51
mentality,” where both members of the dyad have positive outlooks of their end-goal:
I think the ultimate, the one key thing is, is always having a win-win, you know,
mentality. So how can, you know, what I need to happen on my side be a win and
how can the other side of the dyad have a win so that at the end of the day, we’re
gonna be able to trickle all of these down to those that we lead and the mantra will
be, “Well, this is a win for us and this is a win for you.” Therefore, you know, the
buy-in is gonna be a lot, you know, a lot more positive, I think it’s a really… and
in order to get there, it has to be the art of negotiation, you know.
Finally, the sixth theme that followed the third major finding was the competency
of having a credible reputation. The finding again received just one occurrence, or 13%
of the total sample population. Participant 4 stated that they have established their
credibility in the industry, making it easier to implement their approaches as a dyad:
And in 2014, in last year, we actually won an award, the presidential award for
one of our protocols, which was announced, you know, from the president of the
hospital in front of every person that may have bought in… Well it was a huge,
huge presidential award for a large protocol that we initiated as a dyad. Which at
that point, everybody was like, all right, they know what they’re doing. They’re,
they’ve got credibility.
Major Finding 4: Formal Meetings and Discussions
The fourth major finding that emerged was based on the fourth research sub-
question, which was that the protocols and procedures are followed in decision making
within dyads or triads. The researcher discovered that formal meetings and discussions
were the most-employed protocol by the interviewed participants when participating in

MANAGEMENT MODEL IN HEALTHCARE SETTING 52
dyads or triads. The major finding received seven occurrences, or 88% of the total sample
population. Table 5 contains the fourth major finding and other themes discovered from
the analysis, addressing the fourth research sub-question of the study.
Table 5 Protocols/Procedures for Decision Making Within Dyads/Triads
Major Finding and Themes Number of
Occurrences Percentage of Occurrences
Major finding 4: Formal meetings and discussions
7 88%
Theme 1: Professional decision making from members
3 38%
Theme 2: Openness to accept the general consent
1 13%
Theme 3: Following a top-down structure
1 13%
Overall, the fourth major finding was performing formal meetings and discussions
as part of the organization’s protocols and procedures. The researcher considers this to be
one of the six most significant findings of the study. Participant 1 stated that there are
also formal meetings and discussions conducted to discuss the patient’s condition and
status: “Usually there’s minutes that are taken and then the minutes get distributed after
the meeting. It’s all written as opposed to any type of recorded, you know, rehash of what
happened at the meeting.” Participant 2 shared that another formal protocol is having the
meetings and discussions with the committee:
Yes, so on a, on a formal basis, uh, minutes are taken and then minutes are shared
with the committee… uh, the group, the group. And I’m, I’m using the sepsis one
because that’s probably the best one. It’s that, um, he reports. He takes the
information and he shares it with the different physician groups, the critical care

MANAGEMENT MODEL IN HEALTHCARE SETTING 53
group, the med-surg group. He will go to department meetings. He will go to, uh,
the residents’ grand rounds so he takes at that side.
Then I take the information and we, we’re constantly sharing, you know,
presentations so that it’s always the same message, uh, because you’ve got to
have consistency. And so then I take it to the AVPs then I take it to, uh, my
departments. It’s taken, it’s taken to the manager forum. So it’s a, it’s a whole
cascade. It goes down. Issues come up.
Participant 3 echoed that they also conduct regular meetings with the organizational and
structural committees:
If it’s a formal committee, there are... There are organizational committees and
structure committees that are requirements to- for the state. Those will have, um,
committee chairs or co-chairs, meet- meeting minutes and agendas will be taken.
Meaning participants, follow up an action item. So, those things that have to be
documented or documented. Um, there might be other project work and other,
um, committees or, um, initiatives that are going on internally that are also, you
know, requiring that level of structure.
Participant 4 described that the dyad approach has the protocol of conducting
formal meetings and discussions:
So, pretty much everything and anything we do, we take the dyad approach to and
that combined, you know, both administrator and physician because that’s the
only way you can effectively run the service line. With, you know, our goal is,
obviously, you know, lowest cost with optimal patient care and outcome, so the
only way to succeed as best we can with that is, is doing the dyad approach. So,

MANAGEMENT MODEL IN HEALTHCARE SETTING 54
we meet, on a daily basis. We check in. we have a neurosciences steering
committee meeting, which is ran by myself and the physician lead as my support
for that. We also are on clinical effectiveness teams together as well and those
meet monthly. Again, same thing as far as reducing costs and continuing to
provide optimal patient care. Having to space practice and guidelines and things
like that, and we meet in preparation for those bi-weekly as well, so we have
check-ins bi-weekly for those meetings. Protocol, so every single policy and
protocol for the neuroscience's service line we developed as a dyad, it comes from
the administrative team, myself and the physician, all clinical operations.
Participant 5 added that having formal meetings allow the dyads to create and
plan their course of actions:
My second dyad partner is one of the AVPs of nursing at the other facility from
the one in which I do my main clinical work. She and I meet on a formal basis
every 2 weeks in her office setting. And generally one of us will produce an
agenda. Sometimes it’s her, sometimes it’s me because that work is very
prescribed and we… it is also the oldest of the bodies of work and therefore it is
developed or coalesced into a couple of phases or the phases that we started with,
that we’ve accomplished the phases that are ongoing maintenance work and then
there’s the… the phase of continued improvement where different initiatives
coming up that we are trying to move forward.
That’s the most formal of the arrangements. And our protocol for working
and that arrangement is generally that we will vet the ideas to each other first,
anticipate what possible reactions we could have and then plan a combined

MANAGEMENT MODEL IN HEALTHCARE SETTING 55
strategy to overcome those reactions. It’s actually very tactical, very formal and
very deliberate.
Participant 7 also stated that they have both formal and informal protocols, but
lean more on the formal side with regular presentations and reports:
Formal structure, we have a report out that we do, with our senior leadership team
on a periodic basis, myself and Sandy Garrett will actually report out on those
things whether… Like this past June, we reported out to the board, on the
medicine service line and, I put together a PowerPoint presentation and we talked
about our mission, our vision. We talked about, how we’ve operationalized
things. We talked about staffing and then we’ve talked about some of the
outcomes.
The first theme that followed the fourth major finding was the important protocol
of following a professional decision making from members. The theme received three
occurrences, or 38% of the total sample population. Participant 1 stated that members of
the dyad should be professional, especially in making their decisions with regard to the
quality of care of patients:
I think it tends to be, overall, it’s always very professional. I mean that’s one of
the… We have sort of a, a set of rules of engagement that I, you know, that I put
into place with the meetings. So it’s usually we follow Robert’s rules. You know,
everyone has to be treated with respect and only one person talks at a time as
opposed to, you know, over them.
So there’s always that professional level that we start with, and then,
certainly, we don’t want to have, you know, the group think model where

MANAGEMENT MODEL IN HEALTHCARE SETTING 56
everybody just says yes. So we encourage cordial and professional dialogue and
then at the end of, you know, that dialogue, then we’ll call for, you know, a
motion, and then that motion will be seconded and then ultimately, you know,
will be voted upon and that there’ll be a tally of votes. And then the expectation is
regardless of what your position was on the given topic, once it’s decided upon,
then the… all of the leadership team will back whatever the decision was of the
group.
Participant 5 shared that building professional relationships helps in creating valid
decisions:
So with the one partner, the VP partner where we have this… the standard set
every 2 week meeting, that meeting is generally in her office at the other campus
pretty much like clockwork. For the dyad partner, with him I’ve had the ongoing
professional relationship for the last couple of years. Those meetings it… it’s sort
of a running meeting or on a daily basis in communication and in email. No set
formal times for the meetings.
Participant 8 added that the outcomes depend on the professionalism aspect of the
business:
The outcomes, you know. Re-admission, length of stay, mortality, all the DRGs.
You know, we of course have an ACO, so we want to keep business here. So the
amount of referrals, a line of care first, transitions of care is so important. So you
get credit for that, demonstrating you did a hand off with the primary care, we
drive everything through evidence.

MANAGEMENT MODEL IN HEALTHCARE SETTING 57
The second theme that followed the fourth major finding was the openness to
accept the general consent. The theme received just one occurrence, or 13% of the total
sample population. Participant 2 shared that another protocol is being open to the
opinions and general consent of the members: “There’s a common ground of where this
is where we’re going to make it happen and work. So I’m giving, you're giving, and it,
it’s effective for everyone.”
The third theme that followed the fourth major finding was following a top-down
structure. The theme received just one occurrence, or 13% of the total sample population.
Participant 3 stated that in their hospital or organization, they follow or employ a top-
down structure for the dyads:
We have some of our team’s service lines are starting to form more dyad models.
Not all areas have true dyads in the sense that there’s an admin and a clinical dyad
team, um, as a equal. There are, um... There are, uh, clinical leaders who report to
the next level, up, who are admins. Still that structure exist but if your definition
of a dyad is two, two people who are in parallel or equal standing with each other,
not all of the services are like that.
So, I’m still working with people that are, you know, still kind of a top-up,
top-down structure, as well as some of our service lines that are in a dyad type of
form- format. And since we know, with our upcoming merger with Geisinger, that
they are in a dyad. I think some of that transition here started to occur where
we’re starting to put ourselves into more of a dyad model.
Major Finding 5: Good Communication Between Members
The fifth major finding was based on the fifth research sub-question of the study,

MANAGEMENT MODEL IN HEALTHCARE SETTING 58
which was the perceived advantages and disadvantages of dyads and triads against non-
interdisciplinary teams. The researcher found that the main advantage of the dyads or
triads is the good communication between members. The finding received four
occurrences, or 50% of the total sample population. Table 6 contains the fifth major
finding and other themes discovered from the analysis, addressing the fifth research sub-
question of the study.
Table 6 Perceived Advantages/Disadvantages of Dyads/Triads vs. Non-Interdisciplinary Teams
Major Finding and Themes Number of
Occurrences Percentage of Occurrences
Major finding 5: Good communication between members
4 50%
Theme 1: Opportunity to work with professionals with diverse experiences
3 38%
Theme 2: Transparency when making decisions
2 25%
Theme 3: Presence of respect and trust between members
1 13%
Theme 4: Working with physicians who dislike cookbook medicine
1 13%
Theme 5: Weak data collection skills 1 13% Theme 6: Weakness in implementing
fast-paced protocol 1 13%
Overall, the fifth major theme was the good communication between members.
The researcher considers this to be one of the six most vital findings of the study. The
fifth major finding can also be related to one of the most significant competencies
according to 50% of the participants, which was the need for the members of dyads and
triads to be good communicators. Participant 1 stated that one advantage of the use of
dyads and triads is the good communication that members practice:

MANAGEMENT MODEL IN HEALTHCARE SETTING 59
Yes. So it’s probably all of those. So we do always communicate beforehand prior
to a meeting. So it’s always good to have a meeting before the meeting so that
you know what you're gonna say during the meeting. And then sometimes things
are communicated in a combined meeting, and sometimes, probably more often,
they’re communicated in separate meetings, but the message, it’s always agreed
upon, has to be the same in both meetings, because we’re familiar enough that
even though there are separate meetings, at the end of that meeting, there’s gonna
be the post-meeting where the two participant meet, the participants at the
different meetings are gonna get together and, and compare notes as well, so.
Participant 3 contended the importance of having good working communication
processes with the members:
So, here’s the con of the dyad model is when you have two you know, when you
have two leaders who are both excellent leaders but have two different ways of
thinking about the outcome or ways to get to the outcome or don’t agree or, you
know, are not aligned about even the outcome itself. “Why are we doing what
we’re doing? I don’t think we should do A. We should do B.” It’s, I think the
communication then... If you don’t have alignment, the communication is either
good communication but they’re not communicating key things or there’s poor
communication because now we're not getting along because so we, we’re not
aligned.
Participant 6 emphasized the significance of communication between the dyad
members and teams:

MANAGEMENT MODEL IN HEALTHCARE SETTING 60
So we were dysfunctional in the beginning and it came down to just basic good
business sense, communication, communication, communication. We needed to
assess basically everyone on our team, even from the different disciplines. Their
attitude towards the team, towards the work, towards each other and then just
really, communicate a lot and have a lot of face time. So, and transparency. You
know, open, honest and very structured. Very strategic touch points to continually
be together and have the work discussed and seek feedback and input, etc.
Communication, communication.
Participant 8 shared the system of communication that they employ:
Well for him and I, I’m usually the note taker, but it’s more around continuing to
evolve the strategy. It’s not for purpose of communicating out unless it’s
something like what I just described. Now that four buckets of work, we have to
communicate that out. Part of the plan is how are we going to regroup and when?
Is there pre-work that we need to do before that, and then you know, get Cynthia
to make a calendar, invite all these people, and then when we get in the meeting
we usually do a, a little song and dance thing. That’s interesting. We kind of
haven’t figured that out. Like some time, you know, maybe we should talk that
over, but we work really well together and we get these little, “Eh,” awkwardness,
it’s like, eh, so what, you know? But like, for example, we’ll get in the meeting,
and God forbid a senior leader is there.
The first theme that followed the fifth major finding was the advantage of having
the opportunity to work with professionals with diverse experiences. The theme received
three occurrences, or 38% of the total sample population. Participant 2 stated that one

MANAGEMENT MODEL IN HEALTHCARE SETTING 61
advantage is having the opportunity to work with other physicians:
I think that we’re probably going to be doing a lot more projects, definitely using
that dyad approach. I’m thrilled with that because that gives me the opportunity to
work with, other physicians on the inpatient side or even maybe even potentially
outpatient, to improve care. Where it doesn’t work, the only thing I could think of
where it might not work is if you get two personalities that just can’t find a
common ground. And, if you’ve got that then you’ve got some leadership issues.
Participant 5 shared how one advantage is being able to work with professionals
who have diverse skills and experiences:
I know my tools and I know to solve my problems. The other person has their
tools and how to solve their problems but the problem is generally a hybrid
problem and therefore it requires a hybrid skill set to solve. Being paired with an
administrator as a clinician there’s the… the delivery of healthcare side of it
which we both share but from different perspectives. My dyad partners are all
nurses. As a physician I bring my physician perspective to it. They bring their
nursing perspective to it which is valuable. They’re also all MBA administrators
so they bring their MBA training and their administrative expertise to the problem
which is a great.
Participant 7 provided how the dyads allow professionals to work with another,
who can complement and harmonize the strengths and weaknesses of one another:
Everyone has weaknesses and, you know, every dyad is gonna have weaknesses. I
think the strength of the dyad is to recognize what those weaknesses are and then
to compliment what the needs are to keep the ship afloat moving forward. So if I

MANAGEMENT MODEL IN HEALTHCARE SETTING 62
had weaknesses, yes, absolutely I have weaknesses. You know, at times, I could
be too nice and I could be a dangerous fault. Now, you would think that would be
just the opposite from a West Pointer or retired army is but it’s I’m not in the
army anymore.
The second theme that followed the fifth major finding was the advantage of
transparency when making decisions. The theme received two occurrences, or 25% of the
total sample population. Participant 2 shared that another advantage is the transparency
upon making a decision:
It makes it successful in the fact that it, that all levels that are agreeing upon a
decision and that is being shared so that, you know… And, and there’s not this
backdoor, issues going on where somebody is trying to change it, so. We’re
transparent, very transparent. That’s why it also is successful, why it doesn’t fail
and why it is successful.
Participant 6 shared that transparency is achieved when consensus in decision is
gathered:
We do consensus, so you um… We will put something out for feedback, we’ll
solicit responses via email or in face to face meetings. We’ll circle back, we’ll
discuss those, we’ll vet them and there are times where it can be supported or
there’s times where you have to make an executive decision and just say that’s,
that’s not something we can do. It really does need to be this. But then we do have
the responsibility. We are also practicing serving leadership. So you do want to,
you know, that’s about meeting needs versus wants and respect is one of our core
values. So to circle back to your group and at minimum provide the rationale as to

MANAGEMENT MODEL IN HEALTHCARE SETTING 63
why the decision, even if it was executive, why it needed to be made, you know,
an executive decision had to be made. That’s pretty much how we do it.
The third theme that followed the fifth major finding was the advantage of having
the presence of respect and trust between members. The theme received just one
occurrence, or 13% of the total sample population. Participant 2 shared that an advantage
is the transparency upon making a decision:
It makes it successful in the fact that it, that all levels that are agreeing upon a
decision and that is being shared so that, you know… And, and there’s not this
backdoor, issues going on where somebody is trying to change it, so. We’re
transparent, very transparent. That’s why it also is successful, why it doesn’t fail
and why it is successful.
Participant 6 shared that transparency is achieved when consensus in decision is
gathered:
We do consensus… We will put something out for feedback, we’ll solicit
responses via email or in face to face meetings. We’ll circle back, we’ll discuss
those, we’ll vet them and there are times where it can be supported or there’s
times where you have to make an executive decision and just say that’s, that’s not
something we can do. It really does need to be this. But then we do have the
responsibility. We are also practicing serving leadership. So you do want to, you
know, that’s about meeting needs versus wants and respect is one of our core
values. So to circle back to your group and at minimum provide the rationale as to
why the decision, even if it was executive, why it needed to be made, you know,
an executive decision had to be made. That’s pretty much how we do it.
MANAGEMENT MODEL IN HEALTHCARE SETTING 64
The fourth theme that followed the fifth major finding was the disadvantage of
working with physicians who dislike “cookbook medicine.” The theme received just one
occurrence, or 13% of the total sample population. Participant 2 admitted that it is
difficult to work with physicians who claimed to dislike following strict guidelines: “You
know, when you're working with physicians, they really don’t like to function and do the
cookbook medicine.”
The fifth theme that followed the fifth major finding was the disadvantage of
having weak data collection skills. The theme received just one occurrence, or 13% of the
total sample population. Participant 2 stated that data collection by the members is a
weakness, and their skills need to be improved for better outcomes: “It’s data collection.
It is a huge weakness. You have to have the ability to get accurate reports, and it has to
behave. The same information…”
Finally, the sixth theme that followed the fifth major finding was the disadvantage
of the weakness in implementing fast-paced protocol. The theme received just one
occurrence, or 13% of the total sample population. Participant 4 admitted that they have a
disadvantage in implementing a fast-paced protocol:
So that was very challenging because we were instituting kind of, or
implementing a really fast-paced protocol. And initially it was, you know, the, it
was challenging because they, not gave push back, r- good resistance.
Making sure that, you know, we were considering everything and we
recently just rolled out another fast-paced protocol in the ED that involves in the
field with EMS and it was the same thing. We worked with the EMS dyad, their
administrators, their medical director and again it was just the same thing of

MANAGEMENT MODEL IN HEALTHCARE SETTING 65
coming to the table and identifying, you know, safety concerns and things like
that.
Major Finding 6: Removal of Message Noises to Solve the Issues Better
The sixth and last major finding that was established was the perceived areas or
facets of dyads or triads that may be modified to improve effectiveness and efficiency.
The researcher discovered that the teams should learn how to remove message noises to
solve the issues better and with better efficiency. The last major finding received three
occurrences, or 38% of the total sample population. Table 7 contains the sixth major
finding and other themes discovered from the analysis, addressing the sixth research sub-
question of the study.
Table 7 Suggested Areas of Improvement for Dyad/Triad Effectiveness and Efficiency
Major Finding and Themes Number of
Occurrences Percentage of Occurrences
Major finding 6: Removal of message noises to solve the issues better
3 38%
Theme 1: Pushing down of leadership distribution
2 25%
Theme 2: Development of data collection skills
1 13%
Theme 3: Development of servant leadership
1 13%
Theme 4: Instituting a fast-paced protocol
1 13%
Theme 5: Developing new methods for innovation
1 13%
Overall, the last major finding was the removal of message noises to better solve
the issues. The researcher considers this to be one of the six most significant findings of
MANAGEMENT MODEL IN HEALTHCARE SETTING 66
the study. Participant 1 stated how the members could improve in fighting the “message
noise,” or the external factors that affect the communication of the solutions for the
patients:
To be able to say, “All right, you know, I’m getting the message and, and, you
know, all the noise, you know, which both sides would hear.” Not the physical
noise, obviously, but in that whole communication paradigm is, you know, the, all
the confounding variables, all of the naysayers, all of you know, the outside
influences and antagonists to a given situation, are all part of the processing, you
know, of discussing the issue. But at the end of the day, it’s when we agree to
agree or, you know, we have to ultimately agree to agree that to affect the change,
but up until that point, we can agree to disagree on certain elements. But at the
end of the day, we agree on what the overall final concept is gonna be.
Participant 6 echoed how teams could work better if they know how to fight
against factors that hinder their plans:
Very challenging and lo and behold, you know, it did prove, the physicians
proved right. The data was inaccurate, but that’s where you go over to your
serving leader and you be transparent and you mumble and you accept full
responsibility. So all of these things kind of… you know, that’s where the
leadership piece is so, so important to the dyad and because they, the team knew,
okay, okay. And they, they moved on and beyond it much easier than we ever
would have anticipated because you were honest and no one’s going to fault for
being honest. They’re going to fault you for insisting something’s right when it’s
not.

MANAGEMENT MODEL IN HEALTHCARE SETTING 67
Participant 7 also shared how approaching the problem more efficiently should be
followed and improved going forward:
How we approach those problems is what is the most important thing and, you
know, having the skill set to get around those problems and, you know, move
beyond those problems, it’s really what’s important and that’s what the dyad
relationship does. The other thing is sometimes when I’m talking, I’m not
listening. My dyad might be listening and vice versa.
The first theme that emerged was the improvement through pushing down of
leadership distribution. The theme received two occurrences, or 25% of the total sample
population. Participant 2 also advised that the hospital should consider pushing down the
leadership training to the managers and directors so that they can be groomed as future
leaders for the benefit of the patients:
Personally, I, I think that we need to push it down. That the directors are not as
involved, they could be as well as the managers. It would be very beneficial, uh,
not only for the patients but for the organization but also for leadership
development and this is where you see, who are those people, managers and
directors that we need to groom to make that next step? And, um, keep pushing it
down.
Participant 8 echoed that the organization should start developing new leaders who can
lead the company in the future:
Now the formal ones I think, and I talked about the site directors and I didn’t say
anything I wanted to say, that we recently recruited them. They've been in place
maybe a month at the most, and now we want to develop them. Really identify,

MANAGEMENT MODEL IN HEALTHCARE SETTING 68
and I was just thinking... Let me just show you this. This is the kind of stuff I do.
Now we're having this meeting, right? Here's everything I need to talk about.
The second theme that emerged was improvement through the development of
data collection skills. The theme received just one occurrence, or 13% of the total sample
population. Participant 2 again suggested another method of effectiveness, which was the
development of skills of the members in data collection or gathering accurate data: “It’s
data collection. You have to have the ability to get accurate reports, and it has to behave.”
The third theme that emerged was the improvement through the development of
servant leadership. The theme received just one occurrence, or 13% of the total sample
population. Participant 3 stated that they have started to train their leaders to acquire
knowledge and skills on servant leadership: “Yeah. So, interestingly, we just got a new
kinda set of tools. Our organization is sending their leaders to... We’ve, we’ve been on a
servant leadership...”
The fourth theme that emerged was the improvement by instituting a fast-paced
protocol. This theme received just one occurrence, or 13% of the total sample population.
Participant 4 determined that one challenge for them is instituting a fast-paced protocol
which can be developed along the way: “So that was very challenging because we were
instituting kind of, or implementing a really fast-paced protocol. And initially it was, you
know, the, it was challenging because they, not gave push back, good resistance.”
The fifth theme that emerged was the improvement by developing new methods
for innovation. This theme received just one occurrence, or 13% of the total sample
population. Participant 5 admitted that the tenured leaders should be open to innovation
and develop new and better ways to reach their goals:

MANAGEMENT MODEL IN HEALTHCARE SETTING 69
My weakness in that relationship is that I’m sometimes too sure that I know what
to do because we… I’ve been doing it for 32 years and I’m not as open to her
innovative ways of handling the problem as I should be. Likewise sometimes her
wanting to make everything perfect out of the gate on the first go around delays
implementation and she needs to learn that get it up and running and make the
course corrections as necessary because you’ll get to the end faster than trying to
put out the perfect finished product of the gate.
Summary
Chapter 4 presented the findings from the thematic analysis of the interviews.
Through the analysis, the researcher was able to address the main research question,
which was: What are the perceptions of physicians and professional managers on the use
of interdisciplinary teams or dyads/triads in healthcare management and decision
making? The researcher discovered six major themes, which addressed the main research
question and research sub-questions of the study. It was then found that the key factor in
creating and implementing dyads or triads is the goal of producing the best solutions for
patient care. Meanwhile, participants also believed that the main purpose for which dyads
or triads are usually created was to develop collaboration and to work together as a team.
Participants found that, for dyads and triads to be effective, members should have the
ability to support arguments with evidence. They also followed protocols and practices,
such as formal meetings and discussions, before making final decisions on their courses
of action, which implies good communication and understanding between members,
another important aspect of the implementation of dyads and triads. Finally, the
physicians and managers strongly believed that the dyads and triads may be modified to

MANAGEMENT MODEL IN HEALTHCARE SETTING 70
be more effective through the removal of message noises to solve the issues better.
Chapter 5 will discuss further the effectiveness of dyads or triads in relation to the
literature, as well as the recommendations, implications, and conclusions of the study.

MANAGEMENT MODEL IN HEALTHCARE SETTING 71
CHAPTER FIVE: CONCLUSION
Introduction
Chapter 5 presents an in-depth discussion of the findings from the previous
chapter, based on the results of the analysis of the interviews with the healthcare
managers and professionals. The purpose of this study was to explore the experiences and
perceptions of physicians and professional managers on interdisciplinary decision-
making teams in a large healthcare organization. Through the thematic analysis of the
participant interviews, six main findings were established, as well as several other themes
that pertain to the main research question and the sub-questions of the study. The main
research question was: What are the perceptions of physicians and professional managers
on the use of interdisciplinary teams or dyads/triads in healthcare management and
decision making? The following research sub-questions were the focus of the study:
Research Sub-question 1. What factors are considered in creating and
implementing dyads or triads?
Research Sub-question 2. What objectives, or for what purposes, are dyads or
triads usually created?
Research Sub-question 3. What competencies are perceived as necessary to
effectively and efficiently function in dyads or triads?
Research Sub-question 4. What protocols and procedures are followed in
decision making within dyads or triads?
Research Sub-question 5. What are the perceived advantages and disadvantages
of dyads and triads against non-interdisciplinary teams?

MANAGEMENT MODEL IN HEALTHCARE SETTING 72
Research Sub-question 6. What are the perceived areas or facets of dyads or
triads that may be modified to improve effectiveness and efficiency?
This chapter includes the following sections: (a) summary of findings; (b)
interpretation of data; (c) limitations; (d) recommendations; (e) implications; and the (f)
conclusion of the study.
Purpose of the Study
The purpose of this case study was to explore the experiences and perceptions of
physicians and professional managers on interdisciplinary decision-making teams in a
large healthcare organization.
Aim of the Study
The aim of this Dissertation in Practice study was to use the findings on dyads
and triads in the healthcare setting to design a decision-making model for
interdisciplinary teams that can be adapted in different settings, such as businesses, non-
profit organizations, and academic institutions.
Summary of Findings
Through the qualitative thematic analysis on the interviews with the participants,
the researcher discovered six major findings, which all pertain to the main research
question. In addition, themes were formed to support the major findings, as well as
provide a broader and more extensive perspective on the research questions of the study.
Research Sub-question 1
From the analysis, it was discovered that the most important factor in creating and
implementing the dyads or triads was to produce the best solutions for patient care. The
major finding received five occurrences from the eight interviewed participants. Another
MANAGEMENT MODEL IN HEALTHCARE SETTING 73
vital perception on creating or implementing dyads or triads was alignment of the overall
vision of the hospital or campus. The theme received relatively less occurrences than the
first major finding of the research study.
Research Sub-question 2
For the second research sub-question, the researcher discovered that the purpose
of creating dyads revolved around the idea of working together as a team in order to
reach the goal of optimal care for the patients. The participants of the study shared how
teamwork became integral to reaching their goal of providing the best quality of
healthcare to the patients they served. The majority of the interviewed participants shared
these purposes when creating dyads.
Research Sub-question 3
For the third research sub-question, the participants shared the different
competencies that they perceived as necessary to function effectively in a dyad/triad. The
researcher found that a majority of the healthcare professionals believed that the most
important competency was the ability to support arguments with evidence. This major
finding received the highest number of occurrences, with five occurrences or 63% of the
total sample population. The major finding was followed by several other needed abilities
and skills for dyads and triads. The participants shared that members should also be good
communicators and that members should have flexibility when working with others.
Participants also suggested that formal education and experience are still required. Strong
member personalities to encourage buy-in from the stakeholders was also vital, and a
positive mentality of achieving better outcomes was seen as effective. Finally, a credible

MANAGEMENT MODEL IN HEALTHCARE SETTING 74
reputation was also perceived as necessary for members to be efficient while working in
dyads and triads.
Research Sub-question 4
There were also various protocols and procedures followed by the participants in
their organization in terms of their decision making within dyads and triads. The
members primarily had regular formal meetings to discuss the goals and outcomes that
they wanted to achieve for the benefit of their departments and organization. Several
other protocols and procedures also emerged. Participants shared that professional
decision making by members was one example of protocols that they followed and saw
as important. Another crucial procedure was being open to accepting the general
consensus of the group to create a more harmonious working environment. Finally,
another shared protocol was to follow a top-down structure in the organization.
Research Sub-question 5
The researcher discovered that the main advantage perceived by the participants
upon the employment of dyads and triads was the good communication between
members. Other significant advantages were: (a) having the opportunity to work with
professionals with diverse experiences; (b) the presence of transparency when making
decisions; and (c) the presence of respect and trust between members. Meanwhile, the
disadvantages that the participants observed with the model included: (a) working with
physicians who dislike “cookbook medicine;” (b) members having weak data collection
skills; and (c) an apparent weakness in implementing fast-paced protocol.

MANAGEMENT MODEL IN HEALTHCARE SETTING 75
Research Sub-question 6
Finally, the participants shared suggestions for how the model can be improved or
developed. It was mainly found that the model could be advanced through the removal of
message noises to solve the issues better. Participants also suggested that pushing down
of leadership distribution could help to train and discover the future leaders of the
organization. The organization should also invest in the development of data collection
skills and development of servant leadership in order to have better outcomes from the
model in the future. Instituting a fast-paced protocol was also another aspect that could be
developed. Finally, participants also suggested that new methods for innovation were
required.
Interpretation of Data
Research Sub-question 1
The researcher found that different strategies have been shown to be effective in
ensuring safety and efficiency in hospitals, healthcare settings, and industries (Allen et
al., 2015; Carayon et al., 2014). One strategy explored in the current research is the
model of dyads and triads in the healthcare setting. The researcher in this study found that
the healthcare managers believed that the model was formed in order to produce the best
solutions for patient care, which aligns with the mission and vision of the healthcare
organization. Indeed, the findings of the current study coincided with the report in
Chapter 2, which claimed that the dyad model allowed physicians and professional
managers to share accountability and responsibilities for improving the quality of care
and services and optimizing financial performance without overburdening patients or
incurring large costs for the country (Zismer & Brueggemann, 2010). Zismer and

MANAGEMENT MODEL IN HEALTHCARE SETTING 76
Brueggemann’s (2010) statement was validated in this study by the responses shared by
the participants in Chapter 4 and is discussed further below.
Research Sub-question 2
The researcher found how collaboration and teamwork has always been the focus
and objective of the model. Chapter 2 explained that research and experience have shown
that effective collaborative work among healthcare professionals, most commonly
between registered nurses and physicians, results in lower morbidity and mortality rates,
reduced cost of care, and fewer medical errors (Maxson et al., 2011). Subsequently, such
effective collaboration can improve job satisfaction and retention of nursing staff
(Maxson et al., 2011). Indeed, teamwork and collaborative decision making by the
members and stakeholders of the healthcare organization has always been of special
importance to the model. Together with the collaborative team efforts of the members,
the study participants also emphasized the best possible care that they could provide to
the patients. As reported, numerous strategies and interventions have been put in place in
individual hospitals, as well as the U.S. healthcare industry as a whole, in order to
advance procedures and protocols that ensure the provision of optimum care to patients
and the safety of patients, visitors, and hospital workers (Allen et al., 2015; Maxson et al.,
2011). The statements by Allen et al. (2015) and Maxson et al. (2011) strengthen the goal
of the model, which is to provide the most favorable care and quality of health for the
patients seeking their services.
Research Sub-question 3
The researcher discovered several competencies needed for effective functioning
in dyads’ or triads’ management model. However, several competencies were highlighted

MANAGEMENT MODEL IN HEALTHCARE SETTING 77
as crucial to the study, as reported in the earlier chapters. Previous studies have shown
that interdisciplinary teamwork and leadership have led to improvements in decision
making, safety culture, and job satisfaction, both in the healthcare setting and in other
settings (Allen et al., 2015; Tremblay et al., 2014). The current study highlighted and
emphasized the importance of having the education and skills to be able to support and
back up data with concrete evidence to ensure the buy-in of stakeholders. Other effective
qualities as stated by Reid Ponte (2012) and Walker, Reshamwalla, and Wilson (2012)
are patience, discipline, trust, and effective, honest communication. These coincided with
the competencies emphasized by the study participants—especially the abilities to
communicate properly and work effectively with different sets and levels of healthcare
professionals.
Research Sub-question 4
The participants in the study shared both the formal and informal protocols
followed by the members of the dyads or triads in the study. Chapter 2 reported how
members of interdisciplinary teams are often trained differently and may follow
contrasting protocols and that difficulties may arise during meetings, planning sessions,
and in decision making. For this reason, interdisciplinary team leaders need to be trained
in interpersonal relations and effective professional communication. Indeed, as
discovered, the participants focused on formal meetings and discussions as part of their
most-practiced protocols upon the creation of the model. These protocols ensure that they
have one common goal and practice constant communication within their teams.

MANAGEMENT MODEL IN HEALTHCARE SETTING 78
Research Sub-question 5
The fifth research sub-question discussed the different advantages and
disadvantages observed by the participants of the study, based on their experiences. As
reported in Chapter 2, according to Baldwin et al. (2011):
Perhaps the most obvious benefit of the dyad model is that it reduces the
traditional “us-them” perspective commonly present in healthcare organizations,
wherein physicians distance themselves from managerial roles and
responsibilities, and focus only on their clinical practice. Such a perspective often
leads to misunderstandings between physicians and managers about policies,
behaviors, and procedures. The dyadic model addresses this divide in the
traditional structure by involving the physicians throughout the managerial
processes while also allowing managers to understand the circumstances and
perspectives of the physicians.
Baldwin et al.’s (2011) finding was also highlighted in the current research study,
wherein the use of the model has allowed good communication, transparent decision
making, and professionalism to emerge.
The dyad model also permits managers and physicians to make more informed
decisions, as they bring in different perspectives of a specific problem or issue to be
addressed (Baldwin et al., 2011; Reid Ponte, 2012). Having experienced and well-trained
professionals come together to create models and decisions that would serve the
healthcare organization and its members best has opened greater opportunities for both
the organization and its stakeholders. Having a diverse group of professionals who can
create informed decisions has increased the involvement of the members in the decision-

MANAGEMENT MODEL IN HEALTHCARE SETTING 79
making process and has allowed the members of the healthcare team to better consider
alternative courses of action, reach a consensus, and then carry out the plan with more
knowledge, ease, and willingness; these all bring positive results to the organization and
the patients they are serving.
Research Sub-question 6
Finally, the sixth research sub-question discussed the ways in which the
development of the dyads and triads can be improved. These mainly focused on the
removal of noises or hindrances in the courses of action of the leaders, as well as the
continuous training and development of the members, as discussed above. In conclusion,
the study participants all agreed that the future of the model lies in the willingness and
ability of the leaders to innovate and use their knowledge to provide the best solutions
and care to the patients they serve.
Limitations
Although the researcher maximized all resources available to complete this
research study, several nuances and inadequacies were still observed. The researcher
found that the lack of data support and the possibility that the participants controlled their
responses were the major limitations of the study. These limitations were:
1. Lack of formal data to support the claims and perceptions shared by the
healthcare managers and professionals; the findings could have included data
from the organization. Concrete statistics and reports could have been added
to strengthen the findings and support the responses of the interviewed
participants.

MANAGEMENT MODEL IN HEALTHCARE SETTING 80
2. The study participants, as members of a well-respected healthcare
organization, could have controlled their responses, as they may not have
wanted to damage the reputation of the organization. In addition, participants
may not have been comfortable divulging full details of their answers and real
perceptions, as they may have been afraid of being identified through their
responses and were worried about sanctions and consequences that they might
face as a result of the interviews. To address this limitation, the researcher
constantly ensured the participants that their identities were secured and
protected, and that their names would not in any way be divulged in the study.
The researcher used numbers to identify the participants rather than names.
Subsequently, all data gathered both recorded and in print will be kept inside a
vault for a minimum of three years as required by most universities in the
United States, to secure the identities of the participants of the study.
Recommendations for Further Research
Based on the limitations of the study, the researcher recommends the following be
performed by future scholars who plan to conduct a study on the same research topic.
Future studies should:
1. Consider employing a mixed-methodology study, combining both quantitative
and qualitative findings to provide a data-driven study with well-supported
facts and evidence to back up the claims reported in the research findings of
this study. In addition, future studies may also consider incorporating facts
and statistical data provided by the target healthcare organization to reinforce

MANAGEMENT MODEL IN HEALTHCARE SETTING 81
the statements, perceptions, and experiences shared by interviewed healthcare
professionals and managers.
2. Consider interviewing other groups considered to be stakeholders of the dyads
or triads in order to see different viewpoints on the topic. Interviews with
other stakeholders may allow for the discovery of other important elements
and aspects of the model, coming not just from the tenured healthcare
professionals but also from those who have enough knowledge and experience
with the model. This may be useful, given that the main goal of the model is
the inclusion of each stakeholder in decision making, whether at the
healthcare or the administrative level.
Implications for Action
The researcher believes that this study provides a significant contribution to the
healthcare industry, specifically regarding the dyad management model. Given the lack
of available literature on the dyad management model, the current study provides future
scholars with a perception- and experience-based study in which the findings were
gathered directly from those who had knowledge and experience with the subject. The
current research can also be employed by other healthcare organizations who want to
utilize the dyad model to improve management in their institutions.
This study provides suggestions and ideas for six aspects of dyads/triads: (a) the
factors considered when creating and implementing dyads or triads: (b) the objectives, or
purposes, for which dyads or triads are usually created; (c) the competencies necessary
for members to function effectively and efficiently in dyads or triads; (d) the protocols
and procedures for decision making within dyads or triads; (e) the perceived advantages

MANAGEMENT MODEL IN HEALTHCARE SETTING 82
and disadvantages of dyads and triads versus non-interdisciplinary teams; and (f) the
perceived areas or facets of dyads or triads that may be modified to improve effectiveness
and efficiency. These aspects shall allow the other healthcare organizations to decide if
the model is suitable for their environments and to prepare themselves for what to expect
upon employment and implementation of the model, given that the current study has laid
out direct experiences and perceptions from healthcare professionals themselves. Figure 1
is the model or framework developed from the researcher’s analysis of the findings,
which the researcher proposes as Chadd’s Model of Dyad Management.
Figure 1. Chadd’s model of dyad management.

MANAGEMENT MODEL IN HEALTHCARE SETTING 83
Summary
In conclusion, the researcher successfully addressed the main research question
and six sub-questions of the study pertaining to the effectiveness and structure of the
dyad model. Through thematic analysis of the interviews with the participants, the
researcher found that the core reason for creating and implementing the dyad model is to
produce the best solutions for patient care while working together as a team. Healthcare
organizations should note that the core competency that they should require from their
professionals is the ability to support arguments with evidence. In addition, one of the
most important protocols that they should adopt is the use of formal meetings and
discussions to ensure the similarity of the goals and visions of the different teams
involved in the dyad/triad. One advantage of the model is the practice of good
communication between members, which makes it more effective and beneficial to the
organization compared to the other models available. Finally, the removal of message
noises shall allow the model to become fully functional and effective for healthcare
organizations. Therefore, it can be concluded that the employment of the dyad
management model is effective in a healthcare setting due to the ability of the healthcare
professionals and managers to collaborate to achieve the common goal of providing their
patients with optimal care.

MANAGEMENT MODEL IN HEALTHCARE SETTING 84
References
Allen, D., Weinhold, M., Miller, J., Joswiak, M. E., Bursiek, A., Rubin, A., & ... Grubbs,
P. (2015). Nurses as champions for patient safety and interdisciplinary problem
solving (CNE SERIES). MEDSURG Nursing, 24(2), 107-110.
Attride, J. S. (2001). Thematic networks: An analytic tool for qualitative research.
Qualitative Research, 1, 385-405.
Baldwin, K. S., Dimunation, N., & Alexander, J. (2011). Health care leadership and the
dyad model. Physician Executive Journal, 37(4), 66-70.
Carayon, P., Wetterneck, T. B., Rivera-Rodriguez, A. J., Hundt, A. S., Hoonakker, P.,
Holden, R., & Gurses, A. P. (2014). Human factors systems approach to
healthcare quality and patient safety. Applied Ergonomics, 45(1), 14-25.
doi:10.1016/j.apergo.2013.04.023
Creswell, J. W. (2003). Qualitative, quantitative, and mixed methods approaches (2nd
ed.). Thousand Oaks, CA: Sage.
Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five
approaches (3rd ed.). Thousand Oaks, CA: Sage.
Denzin, N. K., & Lincoln, Y. S. (2005). The Sage handbook of qualitative research (2nd
ed.). Thousand Oaks, CA: Sage.
George, V., & Haag-Heitman, B. (2011). Nursing peer review: The manager’s role.
Journal of Nursing Management, 19(2), 254-259. doi:10.1111/j.1365-
2834.2011.01225.x

MANAGEMENT MODEL IN HEALTHCARE SETTING 85
Houghton, C., Casey, D., Shaw, D., & Murphy, K. (2013). Rigour in qualities case-study
research. Nurse Researcher: The International Journal of Research Methodology
in Nursing and Health Care, 20(4), 12-17. doi:10.7748/nr2013.03.20.4.12.e326
Issa, T., Isaias, P., & Kommers, P. (2013). Information systems and technology for
organizations in a networked society. Hershey, PA: IGI Global.
Koelsch, L. E. (2013). Reconceptualizing the member check interview. International
Journal of Qualitative Methods, 12, 168-179. Retrieved from
http://www.ualberta.ca/
Kohn, L. T., Corrigan, J. M., & Donaldson, M. S. (2000). To err is human: Building a
safer health system. Washington, DC: National Academy Press.
Lawrence, T. (2015). Global leadership communication: A strategic proposal. Creighton
Journal of Interdisciplinary Leadership, 1(1), 51-59.
Leedy P. D., & Ormrod, J. E. (2013). Practical research: Planning and design. Upper
Saddle River, NJ: Prentice-Hall.
Légaré, F., Moumjid-Ferdjaoui, N., Drolet, R., Stacey, D., Harter, M., Bastian, H., …, &
Thomson, R. (2013). Core competencies for shared decision making training
programs: Insights from an international, interdisciplinary working group. The
Journal of Continuing Education in the Health Professions, 33(4), 267-273.
doi:10.1002/chp.21197
Légaré, F., Stacey, D., Pouliot, S., Gauvin, F., Desroches, S., Kryworuchko, J., & ...
Graham, I. D. (2011). Interprofessionalism and shared decision-making in
primary care: a stepwise approach towards a new model. Journal of
Interprofessional Care, 25(1), 18-25. doi:10.3109/13561820.2010.490502
MANAGEMENT MODEL IN HEALTHCARE SETTING 86
Margolis, L. H., Rosenberg, A., Umble, K., & Chewning, L. (2013). Effects of
interdisciplinary training on MCH professionals, organizations and systems.
Maternal and Child Health Journal, 17, 949-958.
doi:10.1007/s10995-012-1078-8
Maxson, P. M., Dozois, E. J., Holubar, S. D., Wrobleski, D. M., Overman Dube, J. A.,
Klipfel, J. M., & Arnold, J. J. (2011). Enhancing nurse and physician
collaboration in clinical decision making through high-fidelity interdisciplinary
simulation training. Mayo Clinic Proceedings, 86(1), 31-36.
doi:10.4065/mcp.2010.0282
Reid Ponte, P. (2012). Interdisciplinary leadership in the oncology service line. In M.
Hickey & P. B. Kritek (Eds.), Change leadership in nursing: How change occurs
in a complex hospital system (pp. 215-222). New York, NY: Springer.
Tremblay, D., Touati, N., Roberge, D., Denis, J., Turcotte, A., & Samson, B. (2014).
Conditions for production of interdisciplinary teamwork outcomes in oncology
teams: Protocol for a realist evaluation. Implementation Science, 9(1), 1-22.
doi:10.1186/1748-5908-9-76
Walker, I. A., Reshamwalla, S., & Wilson, I. H. (2012). Surgical safety checklists: Do
they improve outcomes? British Journal of Anaesthesia, 109(1), 47-54.
doi:10.1093/bja/aes175
Wolhuter, C., & de Wet, C. (2014). International comparative perspectives on religion
and education. JNB: African Sun Media.
Zismer, D. K., & Brueggemann, J. (2010). Examining the “dyad” as a management
model in integrated health systems. Physician Executive Journal, 36(1), 14-19.

MANAGEMENT MODEL IN HEALTHCARE SETTING 87
Appendix A
Interview Prompts or Questions
Kindly describe the interdisciplinary team you were part of. (Who were the
participants? What were the objectives?)
Describe you team dynamics and protocols. (How often and where did you meet?
Who took minutes? Etc.)
How would you describe these meetings? Were you comfortable? Did you feel
that there was a general atmosphere of respect and professionalism?
Kindly describe a program or project of your team that presented a challenge for
you.
How did you go about making decisions as a team? Was this a particularly
difficult task?
What are your perceptions regarding the leadership qualities and skills that you
and your teammates exhibited?
What did you perceive that allowed your team to be effective and efficient in its
objectives and processes?
In general, do you think interdisciplinary teams are beneficial in the healthcare
setting? Kindly explain.