malaria parasites dr. gamal allam. learning outcomes by the end of the lecture, you should be able...
TRANSCRIPT

Malaria ParasitesMalaria Parasites
Dr. Gamal Allam

Learning outcomes• By the end of the lecture, you should be able to:1- Define and classify malaria parasites.
2- Mention the geographical distribution of malaria (especially in KSA).
3- Mention Intermediate and definitive hosts of malaria.
4- Explain life cycle of human malaria parasites.
5- Mention routes of disease Transmission.
6- Mention pathology and clinical features of malaria
7- Differentiate between erythrocytic forms of 4 plasmodium species.
8- Diagnose malaria parasites.
Dr. Gamal Allam

Suggested Reading
• http://www.dpd.cdc.gov/dpdx/HTML/Malaria.htm
• http://www.tulane.edu/~wiser/protozoology/notes/malaria.html
• Chiodini, P.L.; Moody, A.H. and Manser, D.W. (2001): Atlas of Medical Helminthology and Protozoology. 4th ed. Churchill Livingstone, P. 62.
Dr. Gamal Allam

Malaria• Malaria is one of the most common vector-
borne infectious disease.• 300-500 million clinical cases per year.• Malaria causes 1.5-2.7 million deaths per year
(90% in Africa).
• The disease is caused by protozoan parasites of the genus Plasmodium .
Dr. Gamal Allam

Human malaria parasites• 4 species of the Plasmodium (P.) parasite are the most
common species that infect humans:1- Plasmodium falciparum:
- the cause of malignant malaria.- the most dangerous species.
2- Plasmodium vivax:- the most frequent, cause benign tertian malaria.
3- Plasmodium ovale:- less frequent, cause of mild benign tertian malaria.
4-Plasmodium malariae:- the cause of benign quartan malaria.
Dr. Gamal Allam

Classification of malaria parasites
• Phylum: Apicomplexa
• Class: Haematozoea
• Genus: Plasmodium
Four species are the most common.
Dr. Gamal Allam

Geographical distribution of malaria
• Malaria widespread in tropical and subtropical regions, including parts of the Americas, Asia, and Africa.
• 40% of the world’s population lives in endemic areas.
Dr. Gamal Allam

Geographical distribution…..cont
Dr. Gamal Allam

Prevalence of malaria in KSA
Dr. Gamal Allam

Vector of malaria
Female Anopheles mosquitoes
Dr. Gamal Allam

Life cycle of human malaria parasites
• Malaria parasites have 2 cycles during their development.
1- Asexual cycle in human (Intermediate host):– Schizogony• Erythrocytic cycle
• Exo-erythrocytic cycle
– Gametogony.
2- Sexual cycle in female Anopheles (Definitive host):– Sporogony.
Dr. Gamal Allam

Life cycle of human malaria parasites• The malaria parasite life cycle involves two hosts. During a
blood meal, a malaria-infected female Anopheles mosquito inoculates sporozoites into the human host (1). Sporozoites infect liver cells (2) and mature into schizonts (3), which rupture and release merozoites (4). (Of note, in P. vivax and P. ovale a dormant stage [hypnozoites] can persist in the liver and cause relapses by invading the bloodstream weeks, or even years later.) After this initial replication in the liver (exo-erythrocytic schizogony (A)), the parasites undergo asexual multiplication in the erythrocytes (erythrocytic schizogony (B)). Merozoites infect red blood cells (5). The ring stage trophozoites mature into schizonts, which rupture releasing merozoites(6). Some parasites differentiate into sexual erythrocytic stages (gametocytes) (7). Blood stage parasites are responsible for the clinical manifestations of the disease.

Life cycle of malaria parasites … cont• The gametocytes, male (microgametocytes) and female
(macrogametocytes), are ingested by an Anopheles mosquito during a blood meal(8). The parasites’ multiplication in the mosquito is known as the sporogonic cycle(C). While in the mosquito's stomach, the microgametes penetrate the macrogametes generating zygotes(9). The zygotes in turn become motile and elongated (ookinetes)(10) which invade the midgut wall of the mosquito where they develop into oocysts(11). The oocysts grow, rupture, and release sporozoites(12) , which make their way to the mosquito's salivary glands. Inoculation of the sporozoites into a new human host perpetuates the malaria life cycle(1).

Life cycle of human malaria parasites

Anopheles
Transmission• sporozoites injected with saliva
• enter circulation• invade liver cells (within 30-60 min.)

Exo-erythrocytic Schizogony
• hepatocyte invasion• asexual replication• Duration, 5-15 days• Number of merozoites
differ in different species
Dr. Gamal Allam

Hypnozoite Forms• some of the sporozoites do not immediately
undergo schizogony (ie, dormant)• merozoites produced months (3-45 wk) after initial
infection• only found in P. vivax and P. ovale
relapse = hypnozoite
Dr. Gamal Allam

gametocytes
Erythrocytic schizogony• 24-48 hr in Pf.• 48 hr in Pv, Po• 72 hr in Pm
Segmenter
Ring form Trophozoite
Schizont
Merozoite
Old trophozoite
Dr. Gamal Allam

Sporogony• occurs in mosquito (9-25 d)• fusion of micro- and macrogametes • zygote ookinete (~24 hr)• ookinete transverses gut epithelium.• ookinete oocyst• asexual replication sporozoites• sporozoites released and invade salivary glands

Invasive Stages
Merozoite• erythrocytesSporozoite• salivary glands• hepatocytesOokinete• epithelium

Routes of disease Transmission
1- Through infected female Anopheles bites.
2- By blood transfusion from infected person.
Dr. Gamal Allam
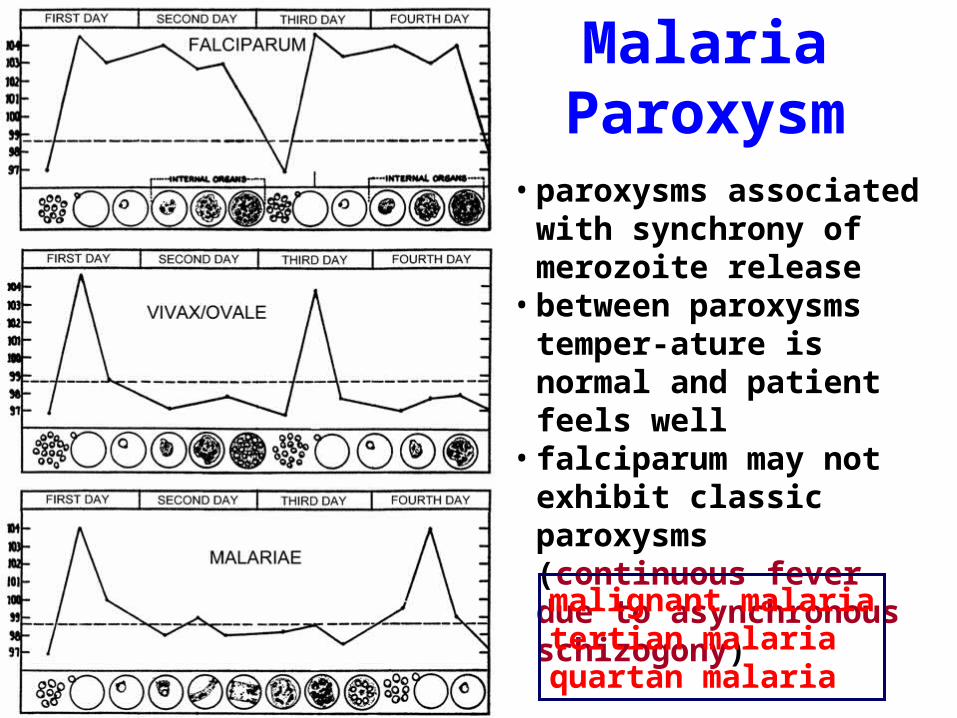
• paroxysms associated with synchrony of merozoite release
• between paroxysms temper-ature is normal and patient feels well
• falciparum may not exhibit classic paroxysms (continuous fever due to asynchronous schizogony)
Malaria Paroxysm
malignant malariatertian malariaquartan malaria

Clinical features of malaria• Characteristic fever:– Shivering & cold stage (30-60 minutes).– Hot stage (1-4 hours, fever with hot dry skin)– Sweating stage (1-2 hours, profuse sweating & temp.
falls.• The attack is repeated at 3rd days (tertian malaria) or
at 4th day ( quartan malaria).• Enlarged spleen.• Anemia due to destruction of RBCs:– Microcytic.– Hypochromic.
Dr. Gamal Allam

Diagnosis of malaria parasites
• Malaria parasites can be diagnosed by:1- Clinical Diagnosis.2- Parasitological Diagnosis.3- Serological Diagnosis.4- Molecular Diagnosis.
Dr. Gamal Allam

1- Clinical Diagnosis of malaria
• Characteristic fever:• The attack is repeated at 3rd days (tertian malaria)
or at 4th day (quartan malaria).
• Enlarged spleen.• Anemia due to destruction of RBCs.
Dr. Gamal Allam
2- Parasitological Diagnosis of malaria
• The definitive diagnosis of malaria infection is still based on finding malaria parasites in blood films.
• Thick blood smears are generally superior for the detection of parasites.
• Whereas thin smears are preferable for species identification.
• If parasites are not found on the first blood smear it is recommended to make additional smears every 6-12 hours for as long as 48 hours.
Dr. Gamal Allam

Morphological Differences Between Human Plasmodium Species in Blood Smears
Dr. Gamal Allam

Key Morphological Differences Between Human Plasmodium Species in Blood Smears
P. vivax P. ovale P. malariae P. falcipar.1- enlarged erythrocyte .2- Schüffner's dots. 3- ameboid trophozoite.
1-elongated oval erythrocyte.2- Schüffner's dots. 3- compact trophozoite .4- usually fewer merozoites in schizont .
1- compact trophozoite. 2- merozoites in rosette.3- Band shape schizont.
1- numerous rings. 2- smaller rings. 3- no trophozoites or schizonts .4- crescent-shaped gametocytes.
Dr. Gamal Allam

3- Serological Diagnosis
• In areas where microscopy is not available, or where laboratory staff are not experienced at malaria diagnosis, there are Rapid Diagnostic test for either:– antibody detection by:• Indirect fluorescent antibody test. • Enzyme linked immunosorbent assay(ELISA).
– malaria antigens.
Dr. Gamal Allam

4- Molecular Diagnosis
• Parasite nucleic acids are detected using polymerase chain reaction (PCR).
• This technique is more accurate and sensetive than microscopy.
• However, it is expensive, and requires a specialized laboratory.
Dr. Gamal Allam