making services safer dr j. secker-walker bsc mbbs frca emeritus consultant university college...
TRANSCRIPT

Making Services Safer
Dr J. Secker-WalkerBSc MBBS FRCA
Emeritus Consultant
University College London Hospitals

Strategic Objectives of Clinical Risk Management
Reduce injuries to patients and staff Identify organisational, system and
environmental problems which may promote human error
Establish early position on liability Learn from accidents by systematic analysis
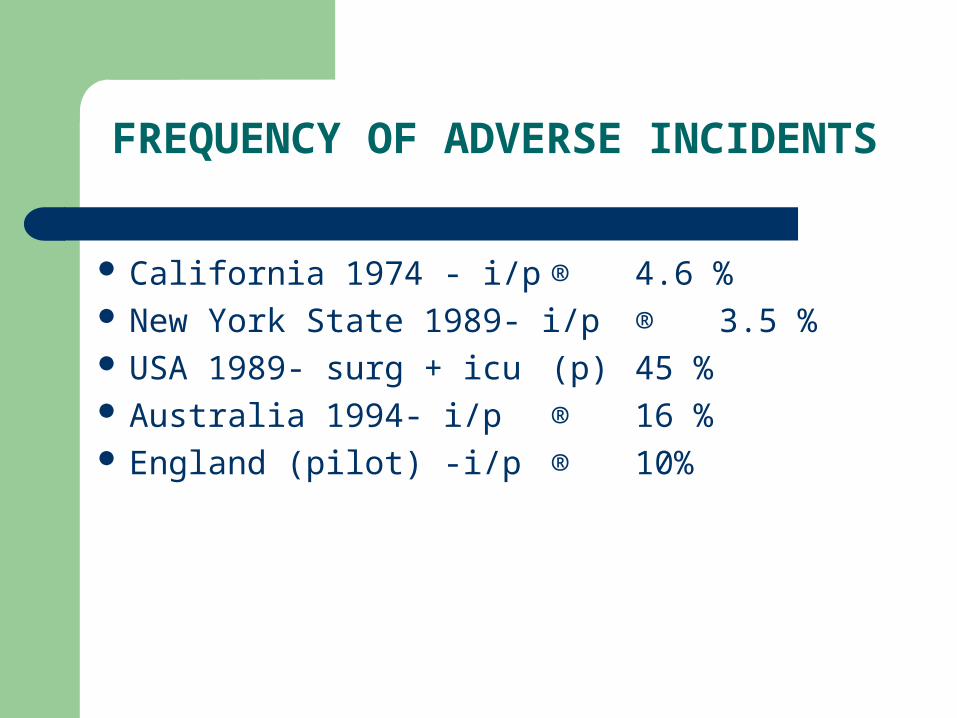
FREQUENCY OF ADVERSE INCIDENTS
California 1974 - i/p ® 4.6 % New York State 1989- i/p ® 3.5 % USA 1989- surg + icu (p) 45 % Australia 1994- i/p ® 16
% England (pilot) -i/p ® 10%

ANALYSIS OF SURGICAL ADVERSE EVENTS
37.5% Individual error - poor judgement or poor technical performance
15.6% Interactive communication problems between teams or
individuals 9.8% Administrative decisions - staffing
levels, inadequate equipment, etc...

CAUSES OF ACCIDENTS
75% Human error 15% Equipment failure 10-30% Human - Equipment
interface

CAUSES OF ACCIDENTS
Usually multi-factorial; very seldom simple Active Human Failures = Unsafe acts by
individuals at the sharp end Latent Human Failures = Inappropriate
organisational policies or decisions - or lack of them
Concept of Resident organisational or environmental “Pathogens” waiting their time

The Development of an Incident
Corporate Culture
Local climate SituationTask
Defence Barriers
Management decisions and organisational processes
Error-producing conditions
Violation-producingconditions
Errors
Violations AccidentsIncidents
Latent failures in defences
J. Reason 1994

ACTIVE HUMAN FAILURES
UNINTENDED ACTION;
Attention failure, memory lapse, interruption INTENDED ACTION; Rule based mistakes Knowledge based mistakes Violations - breaking rules
Human Factors – Attitudes Associated with Critical Incidents
Anti-authority …don’t tell me what to do Impulsivity…..do something quickly Invulnerability….it won’t happen to me Macho….I’ll show you I can do it Resignation…what’s the use, it’s up to the
surgeon

ERRORS
It is the circumstances of their occurrence that determine outcome
Errors that are inconsequential in one situation can be catastrophic in another
Kettle and toaster switches Freezer switch Kegworth - engine switches

ERROR PRODUCING CONDITIONS
High workload Inadequate knowledge, ability, experience Poor interface design Inadequate supervision / instruction Stressful environment Mental state; fatigue, boredom Change

Violations – Breaking Rules or not following Policy
Routine - 79mph on motorway Occupational - required just to do the job Exceptional - breaking the rule saves the day Optimising - bored or something? Sabotage

DEFENCES
Clinical staff - the human condition Pathways of care Preoperative check-lists / swab counts Up-to-date Policies Training in new procedures/equipment Monitoring in anaesthesia and ICU EQA in histopathology Post-take ward rounds

The Human Condition
Error prone slips lapses mistakes violations
Acting as a defence adjustments compensations recoveries improvisations

Teamwork
Stable teams improve the quality of care Team members act as a ‘defence’ for colleagues Inadequate staffing, medical shift systems and
patients on outlying wards make maintenance of consistent teams very difficult to achieve
Pathways of care provide a clear, timed route-map for each patient’s care needs and reduce the risk of communication failures leading to adverse patient incidents

Contributions from Senior Doctors
Junior staff teaching Equipment training for junior staff Appropriate staffing levels Clearly set responsibilities – when to call Emergency room safety procedures: discharge
of children, x-ray review times Mechanism for decisions on delegation
(is X ready to do a hernia unsupervised?)

Organisational Approaches to Accidents
Person (pathological) approach. Focuses on errors and violations of the individual. Remedial effort directed at people at the sharp end
Bureaucratic approach – safety ‘by the book’ with local fixes not global reforms
System (generative, high-reliability) approach. Traces causation to the system as a whole. Remedial effort directed at the environment and organisation. Individuals encouraged to bring concerns to higher management
James Reason 2005

System Approach
Who knows best where the system fails? Staff at the coal-face How do you get them to tell you? Make Incident Reporting constructive and
free of the fear of blame

Disciplinary PolicyA “JUST” POLICY
Should motivate all staff to report Incidents Staff should be free of the fear of disciplinary
action if they report or own up to errors, mistakes or some violations
Exceptions: Criminal behaviour; malicious reporting, gross misconduct, serious breaking of known rules, repeated errors, covering up.

NPSA Incident Definition
“ A patient safety incident is any unintended or unexpected incident which could have or did lead to harm for one or more patients receiving NHS funded healthcare.”
This is also referred to as an adverse event/incident or clinical error, and includes near misses.

HSC Toronto Incident Definition
An Incident is any Occurrence which is not consistent with the routine care of the Patient or the routine operation of the Institution
A near-miss is an Occurrence which but for luck or skilful management would in all probability have become an Incident

0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
5.5
6
6.5
7
7.5
8
98-98 99-00 00-01 01-02 02-03
Women & Children Surgical Medicine Linear (Medicine) Linear (Women & Children) Linear (Surgical)

Obstetric Incident Activity
28
39
28
21
51
32
84
56
67
91
66
37
45 45
61
53
3942
63
40
0
3
6
9
12
15
18
21
24
27
30
33
36
39
42
J an-02 Feb-02 Mar-02 Apr-02 May-02 J un-02 J ul-02 Aug-02 Sep-02 Oct-02 Nov-02 Dec-02 J an-03 Feb-03 Mar-03 Apr-03 May-03 J un-03 J ul-03 Aug-03
Date
No o
f Sho
rtage
s, C
Losu
res
or
Unav
aila
ble
0
5
10
15
20
25
30
35
40
45
50
55
60
65
70
75
80
85
90
95
100
Tota
l Oth
er A
&B In
cide
nts
and
Tota
l In
cide
nts
Staff Shortages / Unit Closure Unavailability of appropriate staff Total all other A&B Total incidents

Total Patient Care Incidents for between October 2000 and September 2003
60
65
70
75
80
85
90
95
100
105
110
115
120
125
130
135
140
145
150
155
160
165
170
175
180
185
190
195
200
205
210
OCT00
NOV00
DEC00
J AN01
FEB01
MAR01
APR01
MAY01
J UN01
J UL01
AUG01
SEP01
OCT01
NOV01
DEC01
J AN02
FEB02
MAR02
APR02
MAY02
J UN02
J UL02
AUG02
SEP02
OCT02
NOV02
DEC02
J AN03
FEB03
MAR03
APR03
MAY03
J UN03
J UL03
AUG03
SEP03
Month & Year
No o
f Inc
ident
s
Total Linear (Total)

Patient Care Incidents for August & September 2002 to 2004
010
20304050
60708090
100110120
130140150160
170180190200
210220
Aug 2002 Aug 2003 Aug 2004 Sep 2002 Sep 2003 Sep 2004
Month & Year
No of
Incid
ents
*A Sentinel
A Very Serious
B Serious
C Moderate
D Slight
E Minor

Swab and Instrument Count Oct 2000 - Sep 2003
43
4
1
34
1 12 2 2
101
4
9
10 6
12
4
8 6 6 6
0
2
4
6
8
10
12
14
16
18
Qtr 3 00/01 Qtr 4 00/01 Qtr 1 01/02 Qtr 2 01/02 Qtr 3 01/02 Qtr 4 01/02 Qtr 1 02/03 Qtr 2 02/03 Qtr 3 02/03 Qtr 4 02/03 Qtr 1 03/04 Qtr 2 03/04
Financial Year / Quarterly
No o
f Inc
iden
ts
Surgical foreign body left in situ Sw ab/instrument count discrepancy


INQUIRY 1
INVESTIGATION29
WALL PAPER
300
WHEN DO YOU HOLD AN INQUIRY?Heinrich ratio
Example : Patient death from medication misadministration / wrong limb / poor performance - incident analysis
Example : Significant medication error, but patient survives
Example : Missed dosage causes no harm. Majority of medication errors / staffing problems - risk trend analysis

The Incident Decision Tree
NPSA procedure to assist managers determine a fair and consistent course of action towards staff involved in a patient incident.
The Deliberate Harm Test – harm intended The Incapacity Test – ill or substance abuse The Foresight Test – adhered to protocols? The Substitution Test – likely peer performance
The sad tale of Mr B aged 18
Sunday 11/11: at gym, hits head on bar Tuesday 13/11: left eye puffs up Wednesday 14/11: off college, eye nearly closed Thursday 15/11: eye completely closed – to GP -
given eye ointment. Sunday 18/11: less eye swelling, reduced appetite,
some vomiting, disliked sister’s music Friday 23/11: to (different) GP – put on antibiotics
and recommended to go to hospital ER

The sad tale of Mr B aged 18
Friday 23/11: seen in ER. Fit shortly after arrival. Pyrexia 37.7. Skull x-ray. Blood count + chem path. Report same day: wbc and neutrophils raised.
Saturday 24/11: seen by neurosurgical registrar: “no fever”. GCS 15/15. Skull x-ray reported as NAD by radiologist. No mention in the notes of the raised wbc. For brain scan
Saturday 24/11: brain scan read by neurosurgical registrar. “no intracranial haematoma, no skull # noted”

The sad tale of Mr B aged 18
Sunday 25/11: scan and patient reviewed by consultant neurosurgeon. Not made aware by (different) registrar that accident had occurred 14 days previously. No mention of wbc or pyrexia on admission. Asked about rhinorrhœa – none, discharged home –”no further seizures, for home today. Not for follow-up”.
The sad tale of Mr B aged 18
Monday 26/11: Neuroradiologist reports on CT scan. Suspicious of orbital #. Suggests urgent discussion with neurosurgeon. Report sent to ward where patient had been.
Tuesday 27/11: mother rings (3rd) GP to say son is still not himself. GP says that he will be ok because hospital had just discharged him! No communication had been received from the hospital.

The sad tale of Mr B aged 18
Friday 30/11: patient found dead in bed by mother. Not able to resuscitate
Friday 30/11: Surgeon sees CT report and wbc result for the first time. Discharge letter to GP not filled in and still in the back of the notes.
Saturday 1/12: Post-mortem shows a brain empyema. Coroner’s inquest found cause of death to be accidental.

NPSA Root Cause Analysis
What happened Why did it happen? What were the most proximate factors -
human, equipment, controllable/ uncontrollable environment?
Why did that happen -what systems and processes underlie those proximate factors - human resources, information management?
Framework for an action plan

Unpicking an Incident
PROBLEM
COMMUNICATIONORGANISATIONAL
FACTORSTASK FACTORS INDIVIDUALS PATIENTS
WORKING CONDITIONS
EDUCATION &TRAINING
DEFENCES
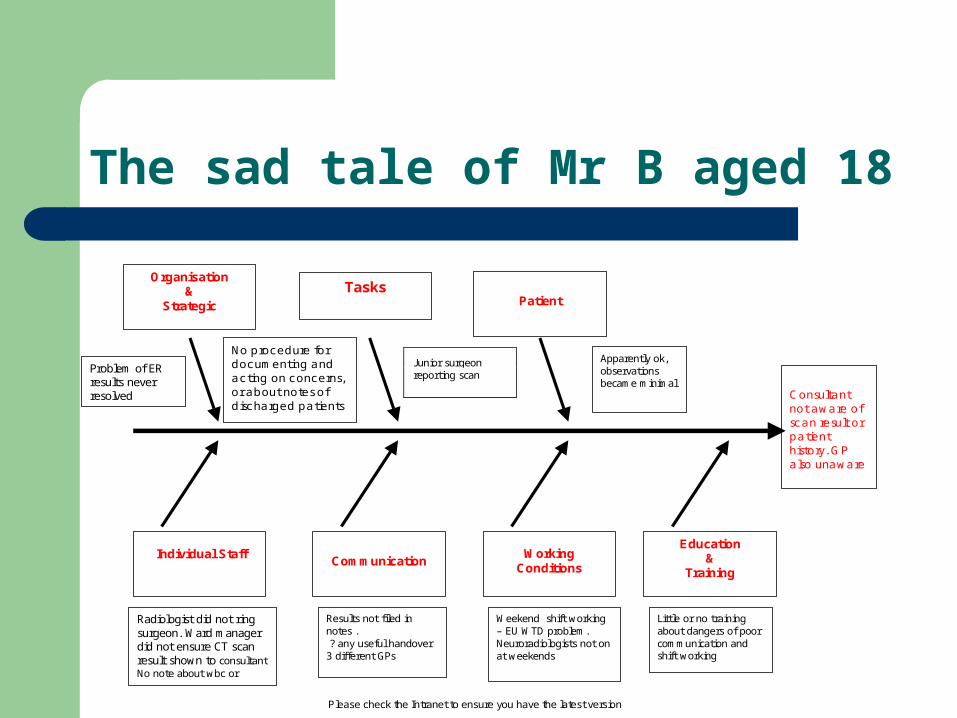
The sad tale of Mr B aged 18
Please check the Intranet to ensure you have the latest version
Junior surgeon reporting scan
Organisation &
Strategic
Tasks
Patient
Consultant not aware of scan result or patient history. GP also unaware
Individual Staff
Communication
Working Conditions
Education &
Training
No procedure for documenting and acting on concerns, or about notes of discharged patients
Radiologist did not ring surgeon. Ward manager did not ensure CT scan result shown to consultant No note about wbc or pyrexia
Problem of ER results never resolved
Results not filed in notes . ? any useful handover 3 different GPs
Weekend shift working – EU WTD problem. Neuroradiologists not on at weekends
Little or no training about dangers of poor communication and shift working
Apparently ok, observations became minimal

CACA ET DECLINOS MEDICOS
INSCRIPTION ON A TOMB IN OSTIA ANTIQUA
Circa AD 57

Relentless Striving For Targets –a cautionary tale
HMS Camperdown – mid 19thC Transition from sail to steam Surplus sailors Competitive culture of ‘brightwork’ – shiniest
surfaces and glossiest paintwork Watertight doors…………..

Reflections
Key points of interest for you How does it compare to local situation Identify areas for action in your own setting
