maimonides medical center makes a quantum leap with ... · 2 maimonides medical center makes a...
TRANSCRIPT

Maimonides Medical CenterMakes a Quantum Leap with Advanced
Computerized Patient Record Technology
Health Information Management Systems Society
San Diego Convention CenterFebruary 12, 2003

2
Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology
Fredrick Cassera, RPh, MBADirector Pharmacy
Steven J. Davidson, MD, MBAChairman Emergency Medicine
Shoshana Haberman, MD, PhDDirector Perinatal Unit
Allan Strongwater, MDChairman Orthopaedic Surgery &
Musculoskeletal ServicesAnn C. Sullivan, MBA
Sr. VP/Chief Information Officer

3
CPR System PlanningThe Medical Center
Brooklyn
Staten Island
Ambulatory sites
Voluntary physician practices with office MACS
Hospitals:Coney Island Medical CenterLutheran Medical Center
Manhattan
Mt. Sinai School of Medicine
Note: Community physician offices toonumerous to indicate on map
36,861 Inpatients5.05 Length of Stay1.87 CMI253,316 Outpatients77,118 Emergency Visits
$564.5 Million Revenue4,612 Employees277 Employed Physicians401 Residents978 Community Physicians
Top 100 Cardiovascular Hospitals (Solucient)Top 100 Most Wired Hospitals (H&HN) 2000, 2001, 20021998 Computerworld Smithsonian Award - Medicine
4
CPR System Planning
Vision…
To improve the quality and effectiveness of patient care by providing real time access to comprehensive clinical information wherever and whenever needed.

5
CPR System PlanningStrategic Priorities
Clinical excellence & patient safetyHumane, patient focused, patient centered careStrengthen physician collaboration & effective communicationSupportive environment for physiciansFiscal viability. . .
6
CPR System Planning Leadership and Governance
CEO firmly committed to project & necessary organizational change
Leadership, financial, medical staffCommunicate process & project statusFinancial commitment includes all ongoing support
7
CPR System PlanningNeeds Assessment
“Stuck in key punch era”New York State’s deregulationStrategic priorities necessitatestate-of-the-art ITDepartmental-specific CPRs
8
CPR System PlanningSystem Acquisition
Inpatient CPR was purchased in 1992 deployed in 1996Patient safety and outcome initiatives required CPRs with knowledge-based decision supportTargeted an integrated single vendor CPR solution

9
CPR System PlanningSystem Acquisition (continued)
No supplier could deliverClinical Department’s diverse requirements were best addressed by CPRs from different vendorsModified “Best of Breed” approach with vendors who conformed with our technology standards
10
CPR System PlanningBusiness Case for CPR
Complexity and expense of implementationUser, workflow committees, task forces, HIS executive committee identify capital initiatives that meet hospital-wide, departmental and individual needsGained buy-in throughout organization

11
CPR System PlanningBusiness Case for CPR (continued)
Strategic priorities yielded investment of $43.909 millionContinuing annual request for $30 millionMetrics tie to business returnRequired technology supports strategic priorities
12
Capital Allocation and Prioritization
Systems (example)Ambulatory, Eclipsys enhancements, ED, document imaging, medication administration, etc.
User wantsClinical success factorsSystem prioritiesEconomic priorities
13
Project Risk ManagementTimeliness, Budget, Completion
Risk reduction strategiesImplementation credibilityResistance to workflow changesManaging vendor relationshipsLack of technology infrastructureUncertainty of success with CPOE with community physicians

14
ImplementationPlanning and Process
InfrastructureATM enterprise networkLeonia, NJ, data centerOS 390/2.5 mainframeOC48 Sonet ring2300+ desktops and wireless devices113 serversNew MIS site

15
ImplementationPlanning and Process (continued)
Simultaneous applications and upgrades 1996–1998
Radiology Information SystemPACSVoice RecognitionDocument Imaging
TranscriptionBlood Bank LaboratoryAnatomical PathologyPatient RegistrationMaster Person IndexPatient AccountingFinancial/HR/PayrollDecision Support

16
ImplementationPlanning and Process (continued)
Physicians sought knowledge-based decision support (1999)Eclipsys SCM to replace E7000Purchased A4HealthSystemsHMED CPR; NextGen CPR –Ambulatory and FacultyPractices; E&C IntelligentPatient Record for Obstetrics

17
ImplementationPlanning and Process (continued)
Data collection, workflow modifications, application screen designIntegrated testing of applications and interfacesDowntime procedures, workflow and useraccess policiesRoll forward approaches“Just-in-Time” Training System “Go Live” support

18
Implementation—Project Governance“Right” Planning Environment
HIS Executive CommitteePhysician Task ForceNursing CouncilProject sponsors break down barriersProject Teams -> user committeesTechnology Infrastructure—command center, training, etc.
19
ImplementationProject Staffing
Maimonides physicians, nurses, pharmacists, lab and radiology technicians
Knowledge of hospital culture, formal and informal organization, institutional memory and medical staff relationshipsIT skill mix broadened by adding cliniciansIT technologists broadened skill mix

20
Impact on OperationsSuccessful System Implementation
Minimize adverse impact on hospital operationsThree to six weeks of go-live supportClosely managed phased approach based on user tolerance
“Big Bang” not possiblePatients come first!

21
Evaluation of Management of CPR Effort Lessons Learned—the Don’ts
Two or more CPRs at the same time“Go Lives” in peak census periods“Go Live” without full volume loadintegrated testing
22
Evaluation of Management of CPR EffortLessons Learned (continued)
Backload data from paper chartsCustomized order sets require physician consensusTrain around the clock with clinicians who understand the specialty and workflow

23
Evaluation of Management of CPR EffortLessons Learned (continued)
Standardize alert levels among CPRsMonitor interfaces 24x7Evaluate and adjust downtime procedures post implementation—Do they really work?Double testing timeQuadruple support for full CPR’s

24
FunctionalityManaging Paper—Ongoing for Years
Scanning forms & documents; signature padsBalance computerized and paper-based dataChart Content Committee:
CPR contentPrinting for internal chart reviewStandardized paper chart for external review
25
FunctionalityKnowledge-Based Prompting
Drug-Drug Interaction CheckingPerinatal- FDB Version “S”Ambulatory- FDB Version “T”ED – FDB Version “U”Inpatient – FDB Version “V”Eclipsys SCM - Multum
26
FunctionalityKnowledge-Based Prompting (continued)
Treatment/Monitoring RecommendationsPerinatal – YesAmbulatory – YesED – NoInpatient – NoEclipsys SCM – Yes

27
MACS guides caregivers, speeding order entry and clinical documentationMACS Perinatal includes:
Order sets and note templatesClinical pathwaysCare plans based on risk or population groupClinicians common choices and preferences (individual and departmental)
FunctionalityOrder / Clinical Practice Standardization

28
Patient Decision SupportRecognizing when patient education is needed
RefusalDate
29
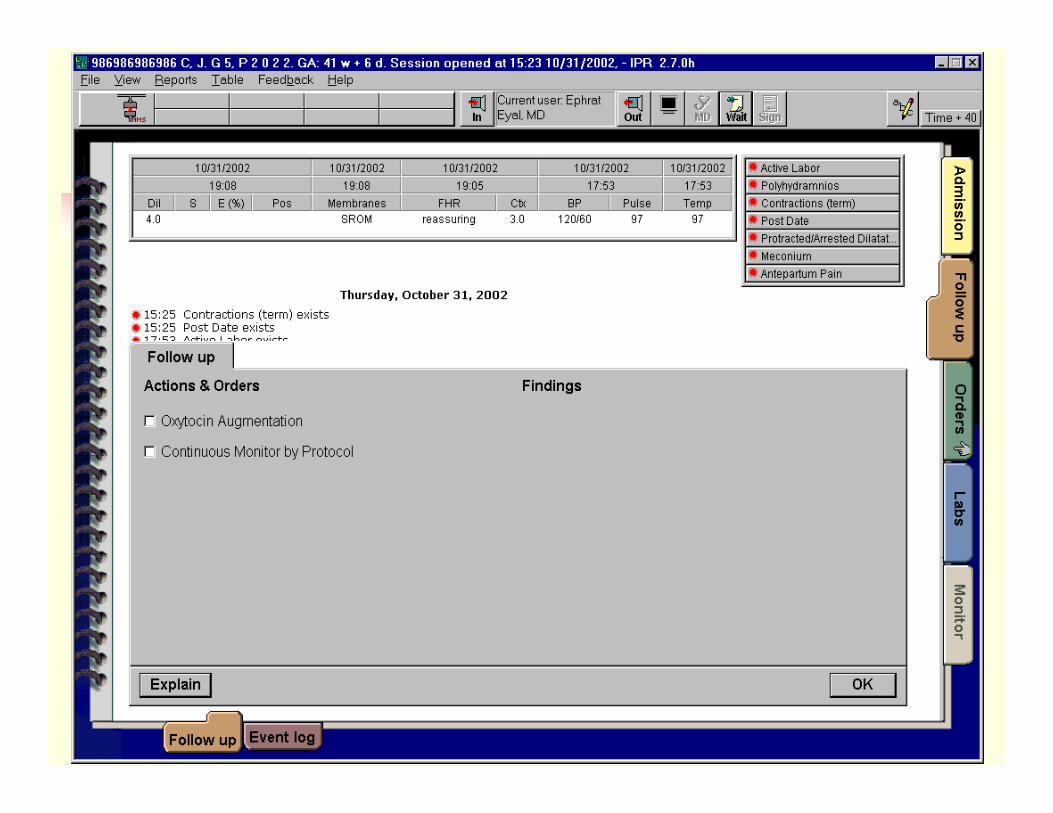
Workflow and Communication
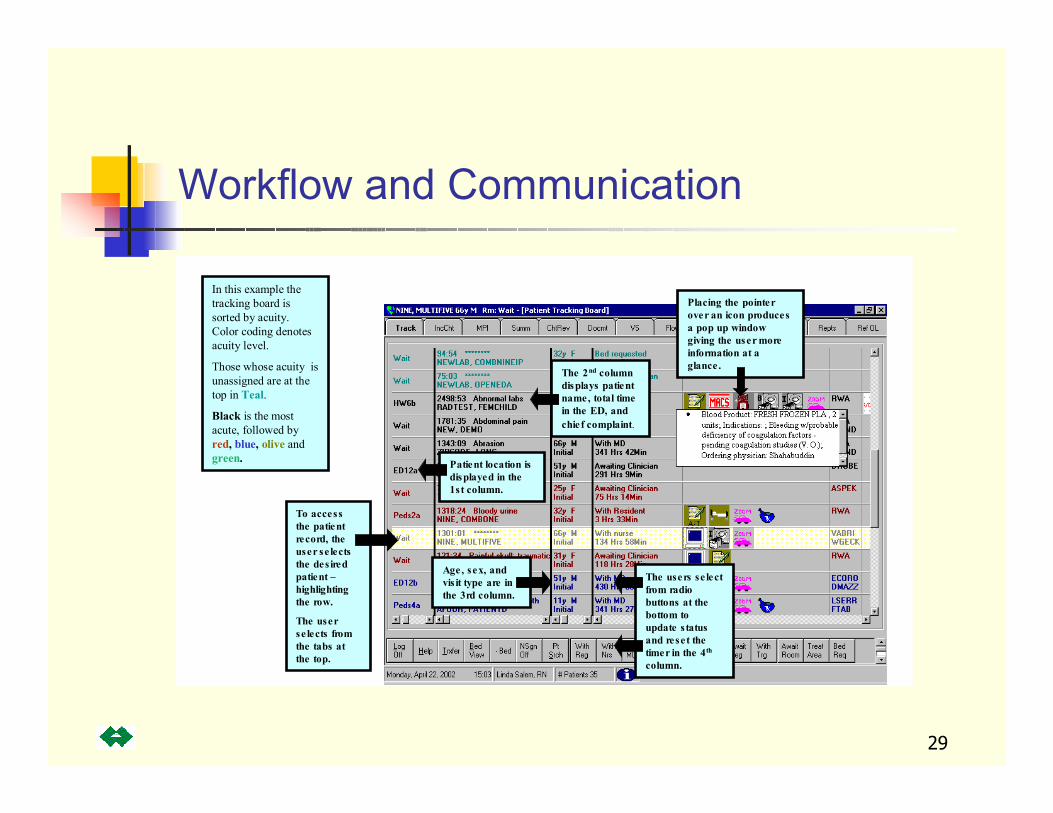
The users se lect from radio buttons at the bottom to update the status in the forth column. This also resets the timer.
To access the patient record, the user se lects the des ired patient –highlighting the row.
The user se lects from the tabs at the top.
Placing the pointer over an icon produces a pop up window giving the user more information at a glance .
In this example the tracking board is sorted by acuity. Color coding denotes acuity level.
Those whose acuity is unassigned are at the top in Teal.
Black is the most acute, followed by red, blue, olive and green. Patient location is
displayed in the 1st column.
The 2nd column displays patient name, total time in the ED, and chief complaint.
Age, sex, and vis it type are in the 3rd column.
The users se lect from radio buttons at the bottom to update s tatus and reset the timer in the 4th
column.

30
Communication Tools

31
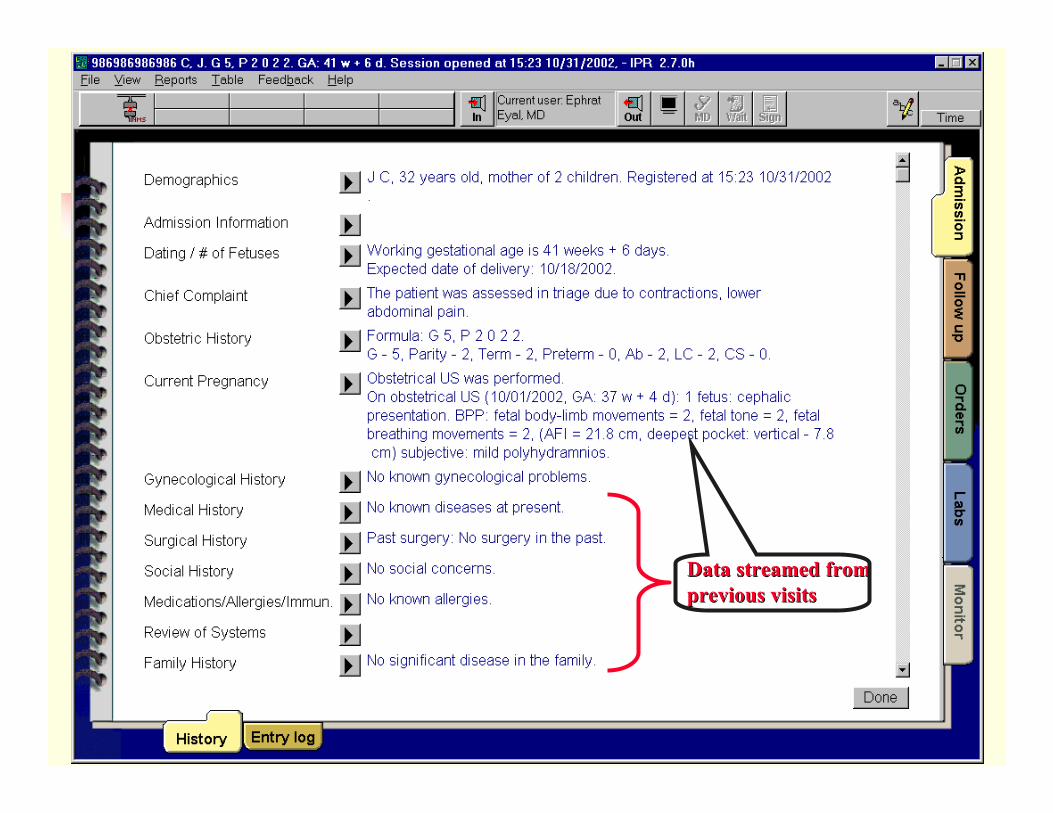
Pregnant patient arrives at triage and is registered.H&P reveals a 32y patient, GA 41w+6d, G5 P2022, whose chief complaint included contractions and lower abdominal pain. Streamed-in data from previous visits included OB US with BPP data suggesting Polyhydramnios.
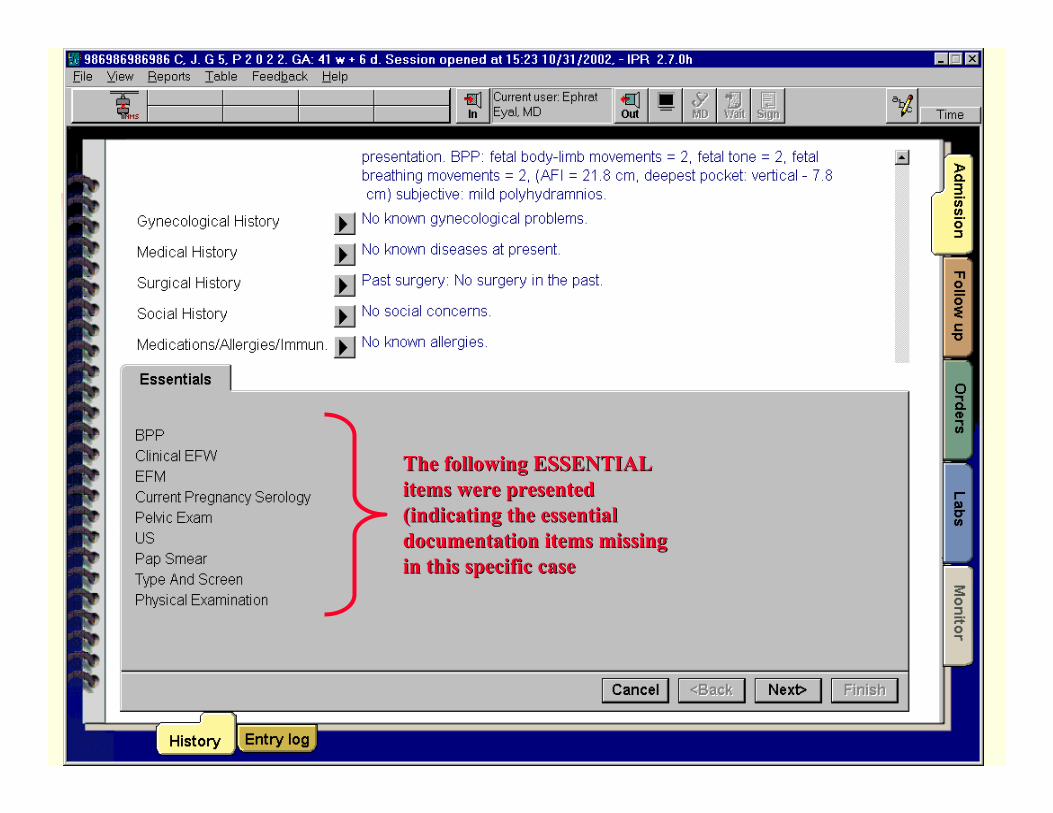
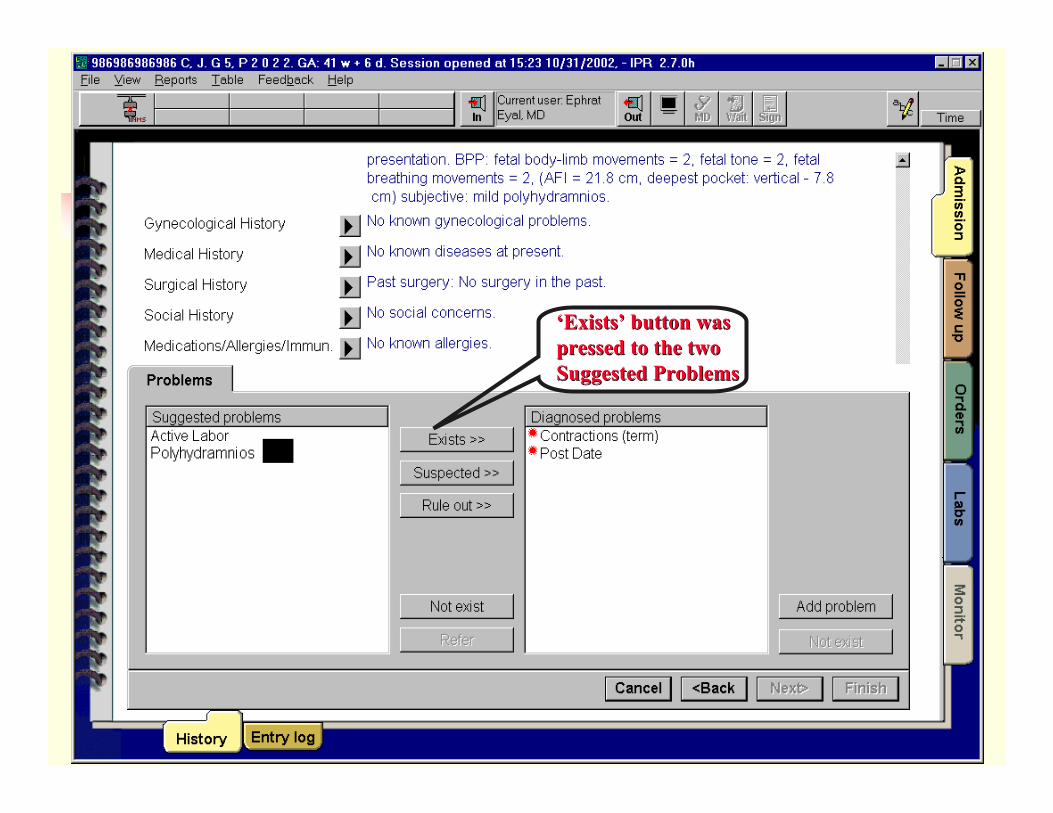
Decision SupportJ. C. - Case Study
32
Data streamed from Data streamed from previous visitsprevious visits
33
The following ESSENTIAL The following ESSENTIAL items were presented items were presented (indicating the essential (indicating the essential documentation items missing documentation items missing in this specific casein this specific case
34
‘Exists’ button was ‘Exists’ button was pressed to the two pressed to the two Suggested ProblemsSuggested Problems

35
Prompted after Done Prompted after Done Sequence in completedSequence in completed
36
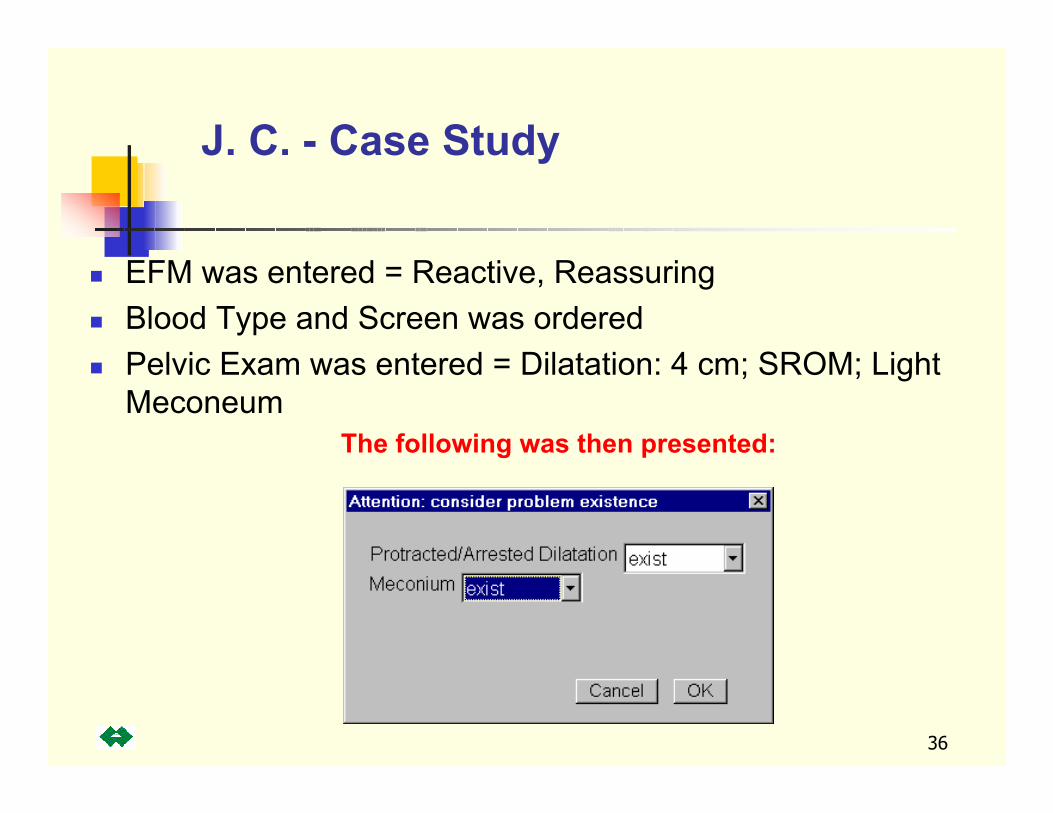
EFM was entered = Reactive, ReassuringBlood Type and Screen was orderedPelvic Exam was entered = Dilatation: 4 cm; SROM; Light Meconeum
The following was then presented:
J. C. - Case Study
37

38
Flexibility (Modified “Best of Breed”)
Applications chosen by users, with MIS guidanceIntegration, Communication, and Security are back-end standard deliverables
AccountabilityTechnical Personnel assigned to applications, not technologiesTechnical Managers responsible for insuring application support coverage
Technology
Philosophy:
39
ScalabilityRolling 3 year capacity planning for all systemsExperience shows almost impossible to over spec storage, memory, or CPU
Transferability“No Fault” Post implementation analysisNo single success, all projects part of evolutionary process improvementInvolvement from all disciplines at all phases
Technology
Philosophy:

40
Technology
Interface EngineSAN (Storage Area Network)Enterprise Network
LANWANWireless
Intrusion Detection Systems
ClusteringInter-System Communication Large storageCommunicationsSecurityRedundancy
De-Mystifying: The driver is healthcare solutions, not technology

41
How to deliver orders, results, & clinical information to all departments quickly and securelyHow to provide 99.999% information availabilityData SecuritySystem Integrity
Interface EngineEnterprise Network
LANWANWireless
SAN (Storage Area Network)Intrusion Detection SystemsClustering
Technology
42
Constantly evaluating flexibility vs. supportabilityIt cannot be achieved 100%
The process of asking the question does yield improvement in efficiency of technology support
It’s touch can be seen in all MMC systemsStandardization creates an inverse relationship between complexity and Total Cost of Ownership
Technology
Standardization: a means to an end
43
Technology
OC-3 OC-3 OC-3 OC-3
1 2 3 4
OC-3 OC-3 OC-3 OC-3
BDF 1
O U TP U TF AI L
A CO K
F A NO K
OU TP U TF A IL
A CO K
F ANO K
OU TP U TF AI L
A CO K
F A NO K
O UTP UTF A IL
ACOK
F ANOK
5500 5500
O UTP U TF A IL
ACOK
F ANOK
O U TP U TF AI L
A CO K
F A NO K
5500
O U TP UTF A I L
A CO K
F A NO K
OU TP U TF AI L
A CO K
F A NO K
5500
O UTP UTF AIL
ACOK
F ANOK
O UTP U TF A IL
ACOK
F ANO K
5500
O U TP UTF A I L
A CO K
F A NOK
OU TP U TF AI L
A CO K
F A NO K
5500
BDF 7
7 BDF's
5000 5000 5000 5000
Typical Floor Closets
5000 5000 5000 5000Typical Floor Closets
OUTP UTF AI L
ACOK
F ANOK
OU TP U TF AI L
A CO K
F A NO K
5500
O U TP U TF AI L
A CO K
F A NO K
OU TP U TF A IL
A CO K
F ANO K
5500
Administration Building
6 875
Maimonides Medical CenterEnterprise Network
O UTP UTF A IL
ACOK
F ANOK
O UTP UTF A IL
ACOK
F ANOK
5500
O U TP U TF A I L
A CO K
F A NO K
OU TP U TF A IL
A CO K
F ANO K
5500
7513
Cisco AS5300A
Cisco AS5300B
PSN
56K Modem
56K Modem
56K Modem
Catalyst 2820
10BT
Cisco 2610
18 Remote Sites (Typical)
PSNISDN
Dial Backup
Data Center
HMED
Server
Command Center
100BT
To Alicomp -Eclipsys E7000
64th StreetDS-3
OC-3
OC-3
OC-12
OC-3
Switched 10/100
To Alicomp(Backup)
64th Street(Backup)
DS-3
T1
T1's
OC-12
OC-12
OC-12
OC-12
OC-12
100BT
100BT
OC-3
OC-3
OC-12
OC-12
OC-12
1stDiagram=Displ2002
Maimonides Medical Center
Network Dwg by : Server Farm
OC3100BT 100BT
DataCenter A DataCenter B
ADMIN A ADMIN BA B
A B
CompOps A CompOps B
Aron BldgCMHC BldgGellman BldgKronish BldgOPD BldgProfessional BldgResearch Bldg
LECSBackup#3
LECS-PrimaryLES/BUS-VLAN1
LECS-Backup#1LES/BUS VLAN2
(Backup)
LES/BUS-VLAN2
LECS-Backup#2LES/BUS-VLAN1 (backup)
OC3
KentroxCSU/DSU
Rack
O UT P UTF AI LACOK FA NOK O U TP UTF A ILACOK FA NOK
5500
O UT P UTF AI LACOK FA NOK O U TP UTF A ILACOK FA NOK
5500OC-3
OC12
DataCenter_MIS
DataCenter_5500C
DS-3
Unisys NCCNetwork
MgmtStation
100BT
IPRobE&C
NextGenServer Farm
Server
100BT
Server Farm
Internet
T1
Cisco 7200CheckPoint
FirewallEmailServer
WEBServer
DMZ
OC3
OC12 OC12
7513
100BT10BT
LS1010
Displ
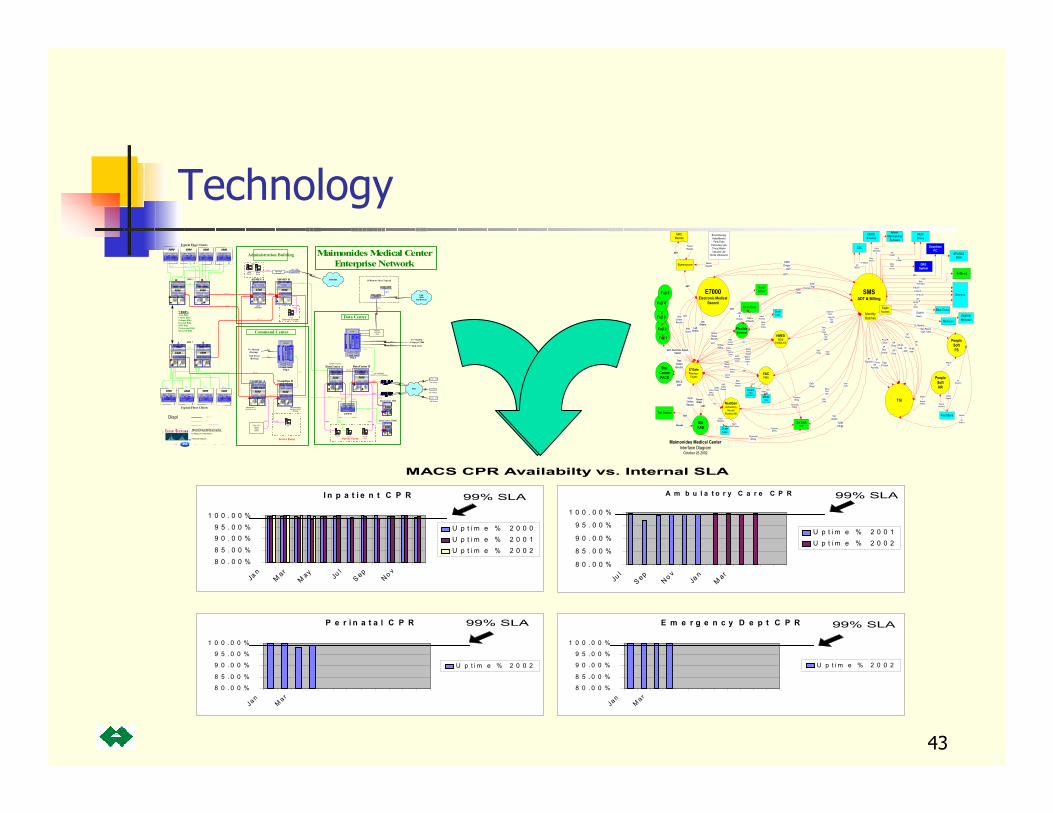
I n p a t i e n t C P R
8 0 . 0 0 %
8 5 . 0 0 %
9 0 . 0 0 %9 5 . 0 0 %
1 0 0 . 0 0 %
Ja n
Mar
May Ju
l
S ep
No v
U p t i m e % 2 0 0 0U p t i m e % 2 0 0 1U p t i m e % 2 0 0 2
A m b u l a t o r y C a r e C P R
8 0 . 0 0 %
8 5 . 0 0 %
9 0 . 0 0 %
9 5 . 0 0 %
1 0 0 . 0 0 %
Jul
S ep
No v
Jan
Mar
U p t i m e % 2 0 0 1U p t i m e % 2 0 0 2
P e r i n a t a l C P R
8 0 . 0 0 %
8 5 . 0 0 %
9 0 . 0 0 %
9 5 . 0 0 %
1 0 0 . 0 0 %
Jan
Ma r
U p t i m e % 2 0 0 2
E m e r g e n c y D e p t C P R
8 0 . 0 0 %
8 5 . 0 0 %
9 0 . 0 0 %
9 5 . 0 0 %
1 0 0 . 0 0 %
Jan
Ma r
U p t i m e % 2 0 0 2
99% SLA 99% SLA
99% SLA 99% SLA
MACS CPR Availabilty vs. Internal SLA
E7000Electronic Medical
Record
SMSADT & Billing
TSI
PeopleSoftFS
FlexilabSunquest
IDXRAD
Fuji 1
StorCommPACS
Talk StationADT
E*GateInterfaceEngine
ADT
Non-PatientCash; Daily
GL Monthly
DRGSystem
Softmed
Admin.Membership
Software
Omnipro
CSC
IDX BAREPS
SurgiServer
EagleAccess
NEICEnvoy
SPARKSDOH
Synersource
MRCMedrite
Fleet Bank
Blue Cross
EMEVSMedicaid
ClaimSubmissio
n
BronchoscopyHolterMonitorPeds Echo
Pulmonary LabTrace MasterVascular Lab
Clicks Ultrasound
FaxedResults
OrdersStatusResults
ADT
IPCOMM
OPCOMM
DowntimePC
MPI
DailyDischarges
OPMDCR
OP BLCR
IP MDCR
IP BLCR
IP MDCDOP
MDCD
Proc IPDisch
IPBed
Census
DiagIP Disch
IPChrgs
OP 90Visits
IPPaymnts
OPVisits
OPChrgs
IP 90Adm
OPPaymnts
IPAdm
CDMChrges
CDMChrgs
CDMChrgs
DailyED
Chrgs
Daily EDVisitsDaily ED
VisitUpdt
DailyVisits
MEDEAmerica
DailyAdmits
MDCRBC
Remit
APReconcil
PeopleSoftHR
PayrollReconcil
PayrollGL
DirectDeposit
Visits
CDMChrgs
VisitUpdate
ADT
ADT
RADOrders
RADOrdersResults
RADOrdersResults
RadOrdersResults
MACSADT
Fuji 2
Monthly
GL(batch)
OrdersStatus
Results
Fuji 3
CancleOrder
ADT
LabOrders
LabOrders
ADT
ADT
ADT
Maimonides Medical CenterInterface Diagram
October 25 2002
Fuji 4
ADT, Rad Ords, Sched,Cancel
FaxedResults
HemoCare
ADT&
Orders Orders& Results
Charges
OPProc
OPDx
MonthlyBatches
Monthly
Payroll(batch)
DailyDRG
Pt Info
Medicare
EligibilityQuery
PhysicianBilling
HMEDEDIS
EWEB-AIE
NextGenAmbulatory
RecordRosetta-AIE
E&CPMIS
ADT
ADT
ADT
OrdersStatusResults
OrdersStatusResults
OrdersStatusResults
OrdersStatus
OrdersStatus
OrdersStatus
Med/IVOrdersChartin
g
RADOrdersResultsRAD
OrdersResults
CancleOrder
CancleOrder
All E7InitiatedOrders
QuestLabs
QuestLabs
BatchADT/
Orders
BatchResultss
BatchResultss
BatchADT/Orders
RADOrdersResults
ClicksUS
AgilentFetal
Monitoring
ADT
ADTResultrs
Orders
PhysicianBilling
PhysicianBilling
PhysicianBilling
DailyChrgs
DailyChrgs
DailyVisitUpdt
DailyVisitUpdt
DailyVisits
DailyVisits
Fuji 5

44
CPR Value
Organizational objectives:Patient safety – clinical excellenceHumane, patient-focused, patient-centered careStrengthen physician collaboration through effective communicationSupportive environment for physiciansStrengthen teaching and researchFiscal viability
Prove return on investment:Demonstrate value of the applicationProvide qualitative and quantitative benefit statementsPromote awareness of process redesign, cultural and organizational issuesIntegrate people, process and technologyInitiate a smarter implementation

45
CPR Return on Investment
9.4%ROI3.84Payback (years)75,876Savings and Efficiencies58,086Ongoing Expenses$31.697Net Cost(4.962)Grants(7.250)Capital Reimbursement
$43.909CPR’s Ancillary; Enterprise Network Interface Engine
(000’s)
46
Warns clinicians of safety checksrequired for High Alert medicationsEnsures safe selection of confusinglook-a-like, sound-a-like drugnamesVerifies the selection of the correct patientReduces the number of adverse drug reactionsImprove medication turnaround timeReduces pharmacy’s drug expenditure; drug spending for 1999-2002 has remained below National Average
CPR Return on Investment
Patient Safety

47
The prescriber is required to check the patient’s serum creatinine and age
After review of the serum creatinine and age, the prescriber may safely proceed to order Metformin
CPR Return on Investment
Patient Safety – High alert medication
48
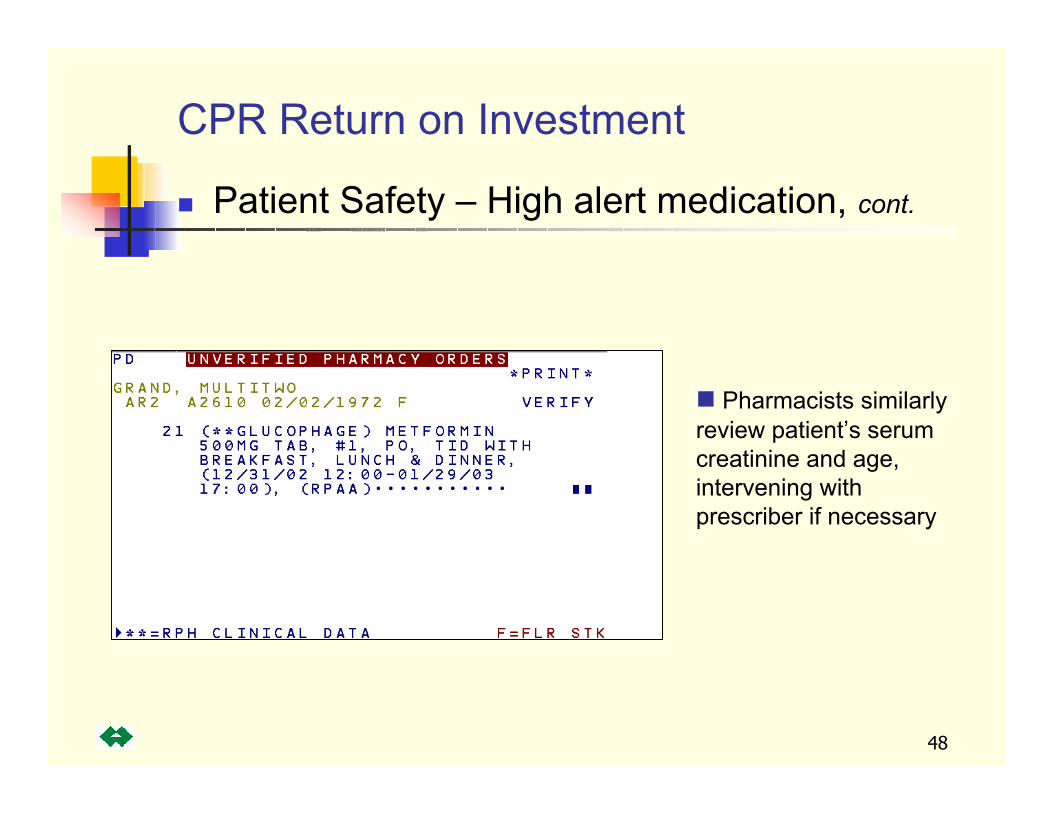
CPR Return on Investment
Patient Safety – High alert medication, cont.
Pharmacists similarly review patient’s serum creatinine and age, intervening with prescriber if necessary
49
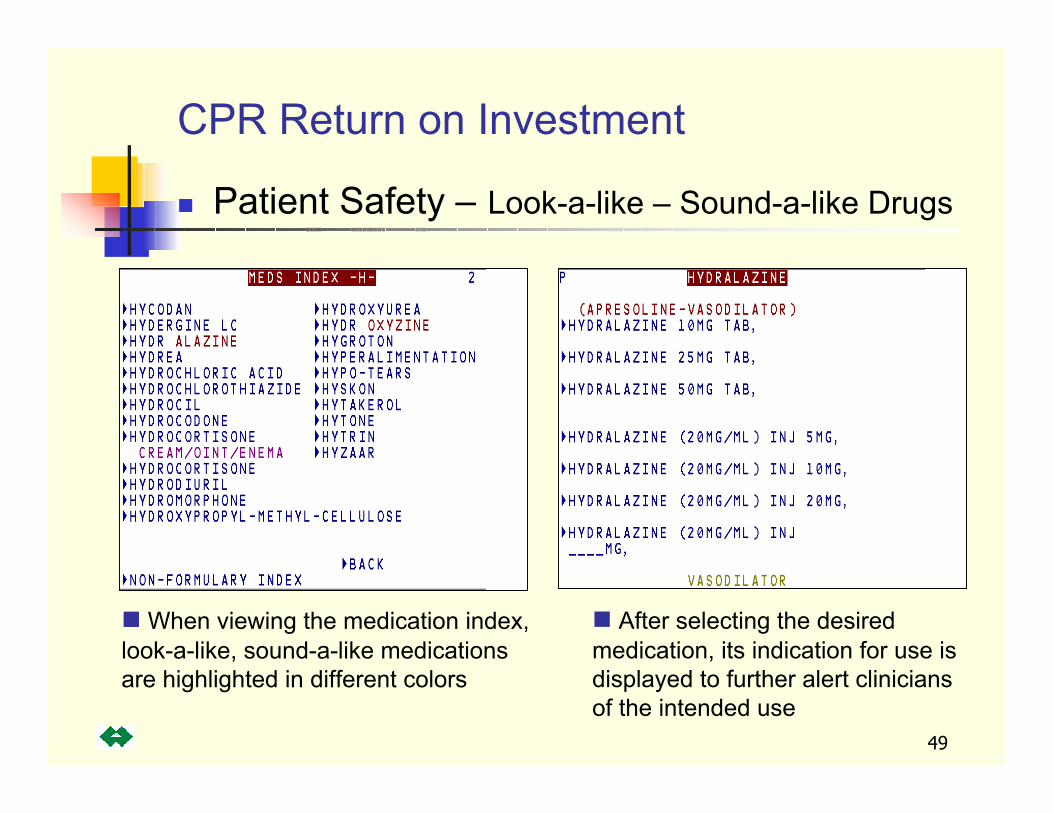
CPR Return on Investment
When viewing the medication index, look-a-like, sound-a-like medications are highlighted in different colors
After selecting the desired medication, its indication for use is displayed to further alert clinicians of the intended use
Patient Safety – Look-a-like – Sound-a-like Drugs
50
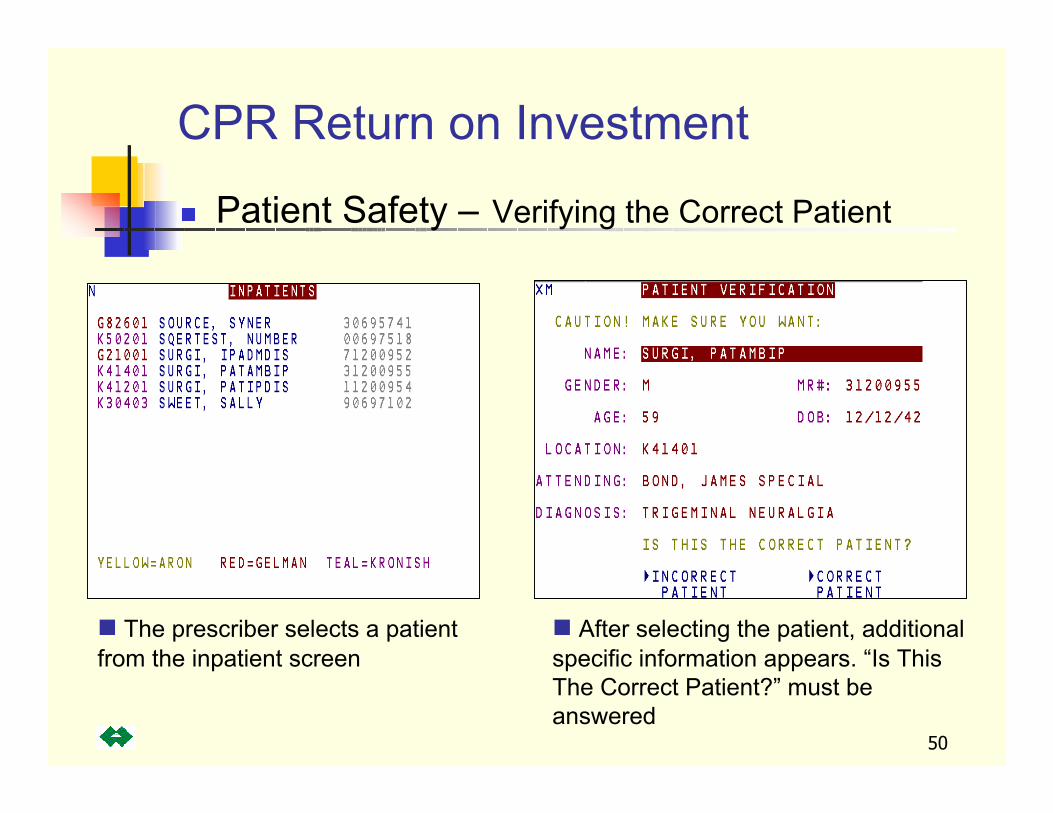
The prescriber selects a patient from the inpatient screen
After selecting the patient, additional specific information appears. “Is This The Correct Patient?” must be answered
Patient Safety – Verifying the Correct Patient
CPR Return on Investment
51
435
1046
619
1450
436
1603
325
1873
0
200
400
600
800
1000
1200
1400
1600
1800
2000
1998 1999 2000 2001
# Adverse Drug Reactions (ADR's)
# Pharmacy's Clinical Interventions
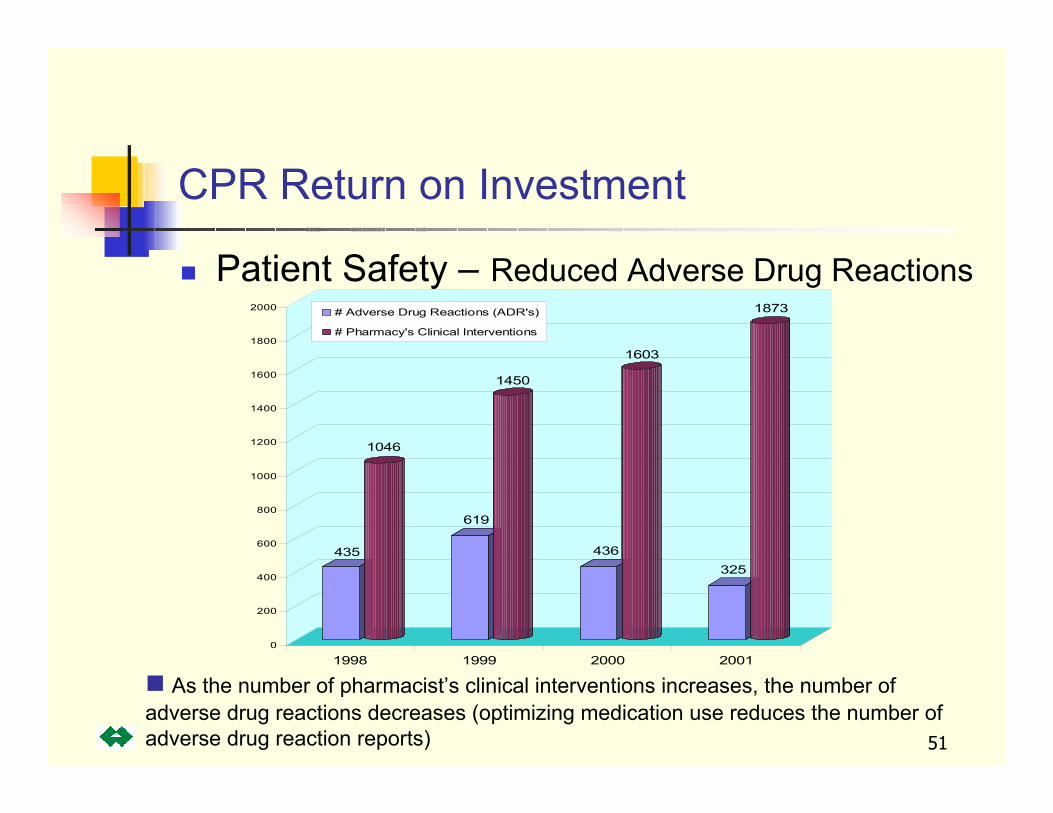
As the number of pharmacist’s clinical interventions increases, the number of adverse drug reactions decreases (optimizing medication use reduces the number of adverse drug reaction reports)
CPR Return on Investment
Patient Safety – Reduced Adverse Drug Reactions
52
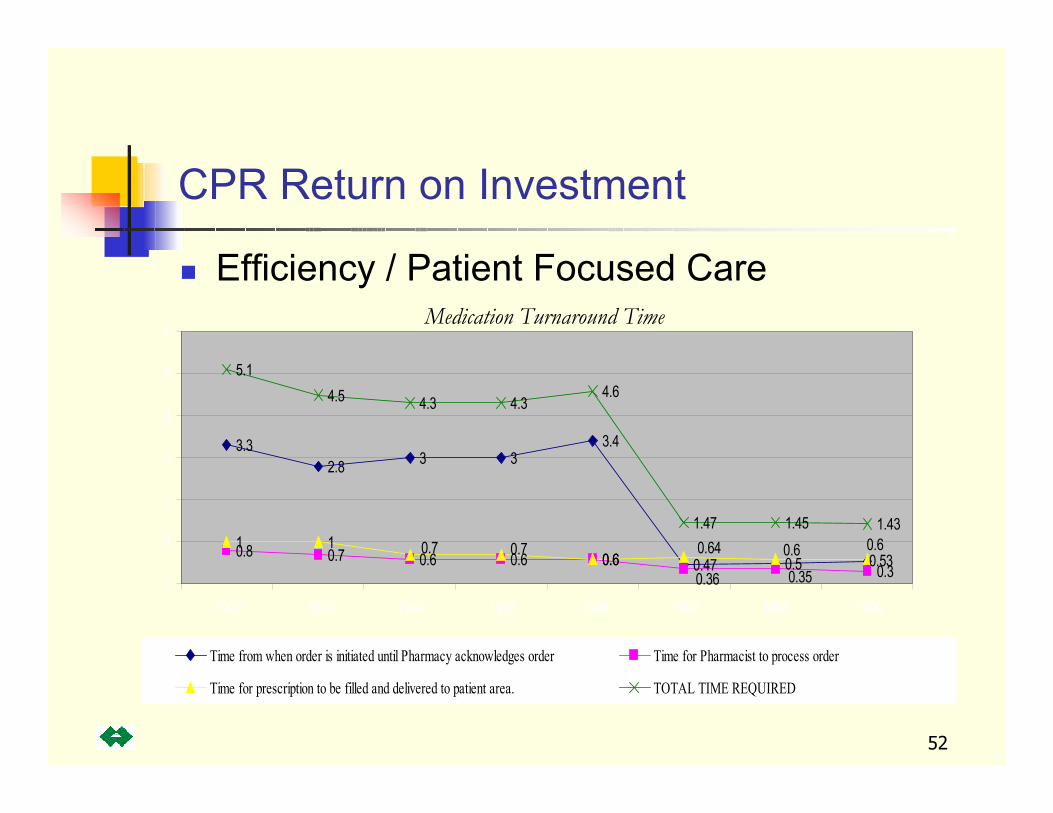
CPR Return on Investment
Efficiency / Patient Focused Care
3.32.8 3 3
3.4
0.47 0.50.8 0.7 0.6 0.6 0.6
0.3
1 10.6
5.14.5 4.3 4.3
4.6
1.47 1.45 1.43
0.530.36 0.35
0.60.60.640.70.7
0
1
2
3
4
5
6
1992 1993 1994 1995 1996 1997 1998 1999
Time from when order is initiated until Pharmacy acknowledges order Time for Pharmacist to process order
Time for prescription to be filled and delivered to patient area. TOTAL TIME REQUIRED
Medication Turnaround Time
53
$10,516,953
$9,692,496
$10,802,384$11,158,487
$11,562,929*
$12,296,652**
$14,202,633*
$8,000,000
$9,000,000
$10,000,000
$11,000,000
$12,000,000
$13,000,000
$14,000,000
$15,000,000
1999 2000 2001 2002
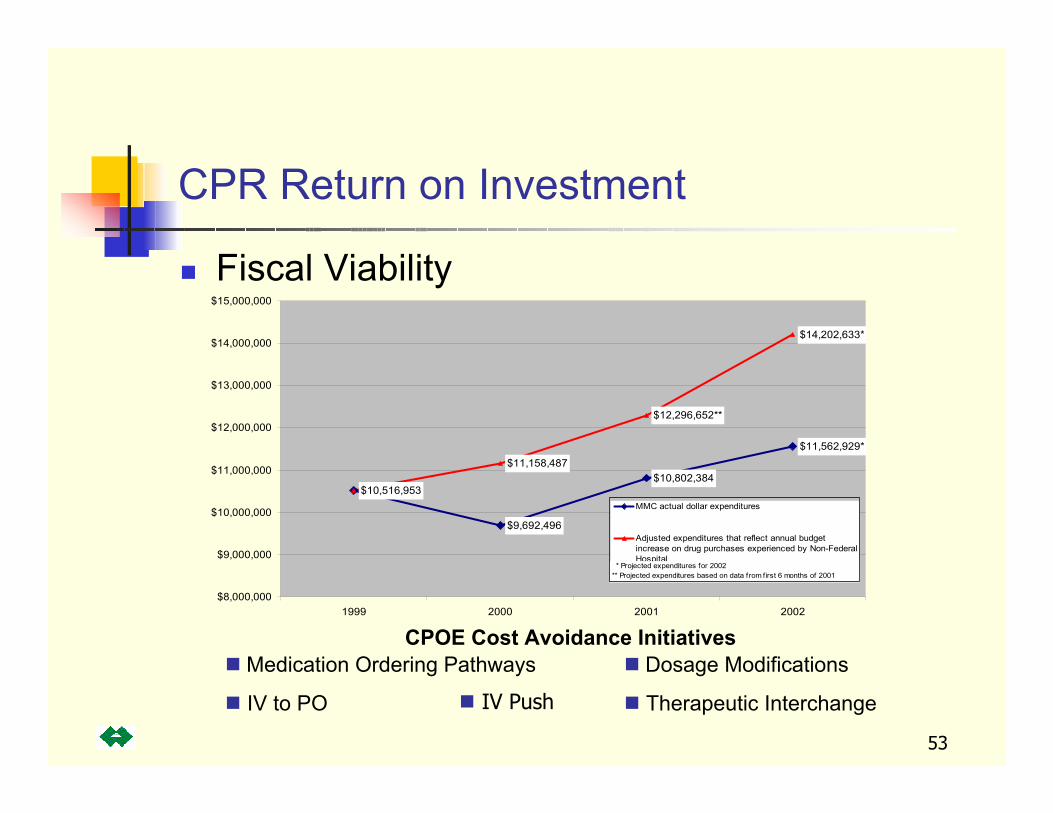
MMC actual dollar expenditures
Adjusted expenditures that reflect annual budget increase on drug purchases experienced by Non-FederalHospital
* Projected expenditures for 2002** Projected expenditures based on data from first 6 months of 2001
CPOE Cost Avoidance InitiativesMedication Ordering Pathways
IV to PO
Dosage Modifications
Therapeutic Interchange
CPR Return on Investment
Fiscal Viability
IV Push

54
CPR Return on Investment
Efficiency / Patient Focused Care
Serology
11640
10460
11433
10884
11900
11515
9500
10000
10500
11000
11500
12000
12500
19 96 19 97 19 98 19 99 20 00 200 1
Tot
al N
umbe
r of T
est
Chemistry
780000
443662 475458 490265 505174
990000
0
20000 0
40000 0
60000 0
80000 0
100000 0
120000 0
1996 1997 1998 1999 2000 2001
Year
Tota
l Num
ber o
f Te
st
Microbiology
60000
4889 9 4 8623
8 0000
474 9149422
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
1996 1997 1998 1999 2000 2001
Tota
l Num
ber
of T
est
Urinalysis
20000
15551 16018
27 000
1576616288
0
50 00
100 00
150 00
200 00
250 00
300 00
19 96 19 97 19 98 19 99 20 00 20 01
Tota
l Num
ber
of T
es
Hematology/Coagulation
231807258466280000
246000262999262936
0
5000 0
10000 0
15000 0
20000 0
25000 0
30000 0
1996 1997 1998 19 99 2000 2001
Year
Tota
l Num
ber
of T
es
Laboratory Tests 1996 - 2001

55
CPR Return on Investment
Patient Focused Care
0
20
40
60
80
100
120
140
160
180
200
Jan-9
9Feb
-99Mar-
99Apr-
99May
-99Ju
n-99
Jul-9
9Aug
-99Sep
-99Oct-
99Nov-9
9Dec-9
9Ja
n-00
Feb-00
Mar-00
Apr-00
May-00
Jun-0
0Ju
l-00
Aug-00
Sep-00
Oct-00
Nov-00
Dec-00
Jan-0
1Feb
-01Mar-
01Apr-
01May
-01Ju
n-01
Jul-0
1Aug
-01Sep
-01Oct-
01Nov-0
1Dec-0
1Ja
n-02
Feb-02
Mar-02A
vera
ge T
ime
Com
plet
ed E
xam
to F
inal
Rep
ort
(hou
rs)
Radiology Turnaround Time to Final Report

56
CPR Return on Investment
Fiscal Viability
Radiology Department Monthly Comparison of Procedures 1999; 2000; 2001; 2002
15249
14489 14493
13702
10500
11500
12500
13500
14500
15500
Jan Feb Mar Apr May Jun Jly Aug Sept OctNov Dec
1999
2000
2001
2002
57
70%
85%
69%
84%
63%
80%
67%72% 73%
84%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1997 2001 1997 2001 1997 2001 1997 2001 1997 2001
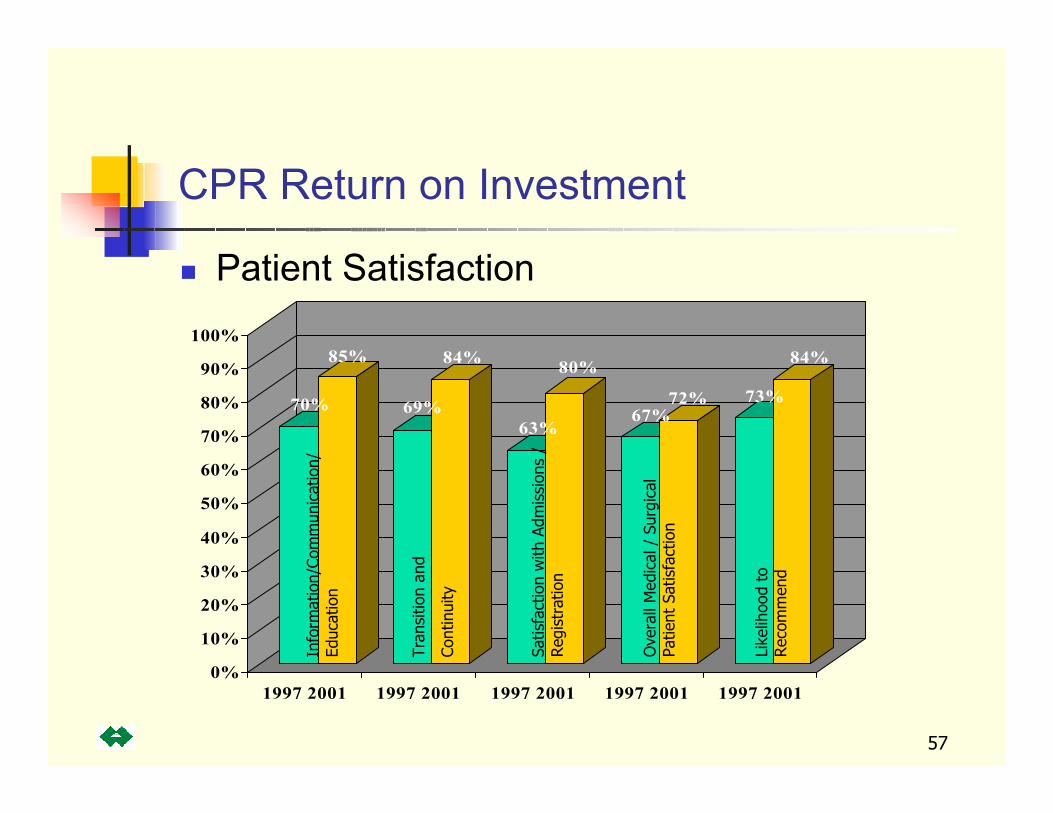
CPR Return on Investment
Patient SatisfactionIn
form
atio
n/Co
mm
unic
atio
n/
Educ
atio
n
Tran
sitio
n an
d
Cont
inui
ty
Satis
fact
ion
with
Adm
issi
ons
/ Reg
istr
atio
n
Ove
rall
Med
ical
/ S
urgi
cal
Patie
nt S
atis
fact
ion
Like
lihoo
d to
Rec
omm
end
58
The Ambulatory CPR:Improved compliance withproblem lists from 67% to 97%Improved allergydocumentation from 88% to 100%Improved pain assessment documentation to 95%Improved medication list documentation from 67% to 100%
CPR Return on Investment
Patient Safety / Regulatory Compliance

59
CPR Return on Investment
Patient Access
804332,168230,6602.21Total
1818727035,626.172001
1833733135,687.232000
1784713735,493.261999
1198479233,148.051998
949379432,150.911997
461184430,200.561996
0028,3561995
Discharges Attributed to MACS
Incremental Discharges vs. Base
YearDischargesLength of Stay
ReductionYear
60
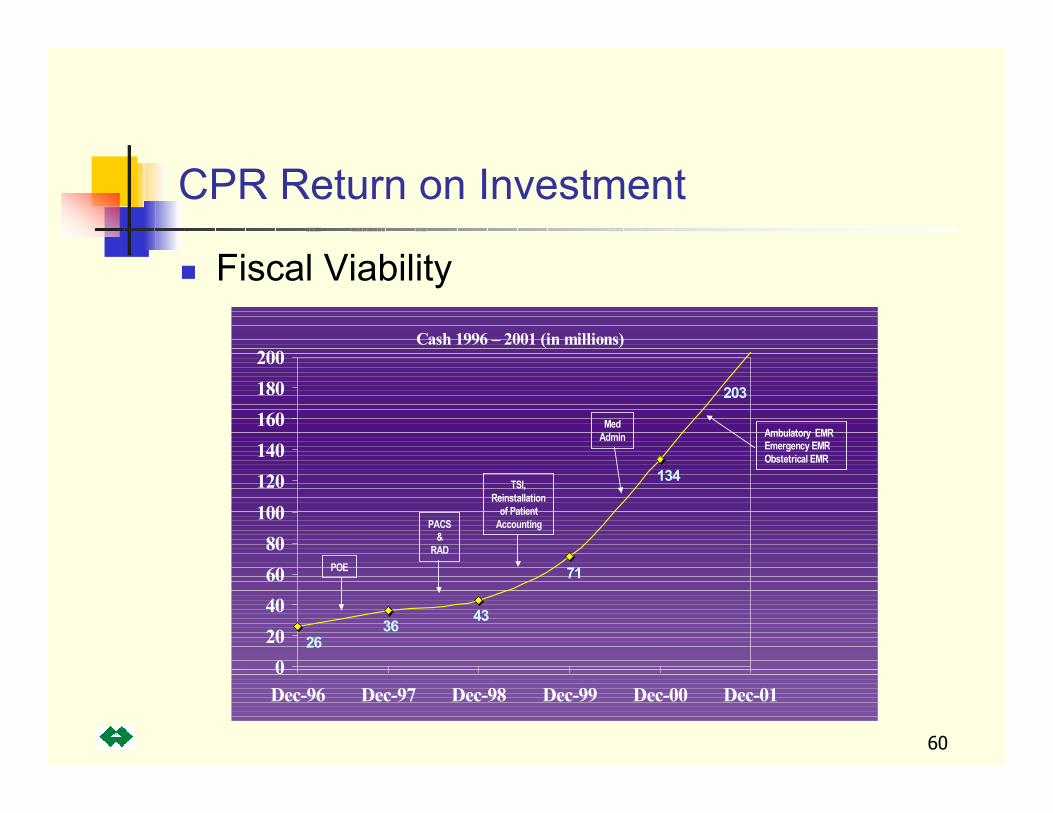
Cash 1996 – 2001 (in millions)
203
134
71
43
2636
020406080
100120140160180200
Dec-96 Dec-97 Dec-98 Dec-99 Dec-00 Dec-01
POE
PACS&
RAD
TSI,Reinstallation
of PatientAccounting
MedAdmin Ambulatory EMR
Emergency EMRObstetrical EMR
CPR Return on Investment
Fiscal Viability

61
Vision For Future
Expand patient safety initiativesExpand decision support and knowledge documentation CPRsBreak Ground New Hospital – planning to become a Digital Hospital
OR/Anesthesia RecordsVirtual Imaging RadiologyClinical Equipment Integration CPR, physiological, images, audioPhysical plant computers