m 1 form - imcp3.orgimcp3.org/images/pdf/m1_formats_new.pdf · m 1 form. chv name: year: village...
TRANSCRIPT

GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
M 1FORM

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
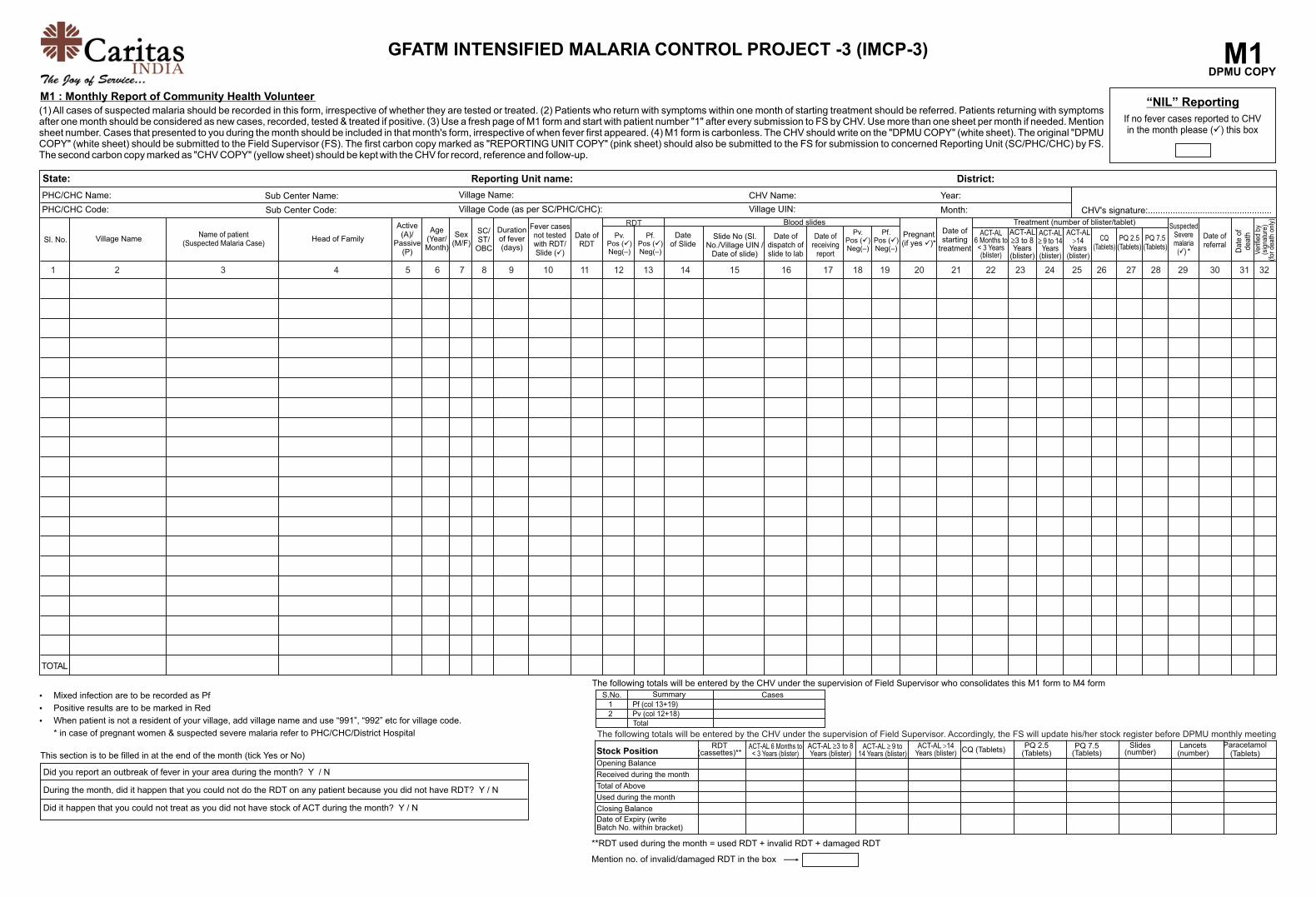
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
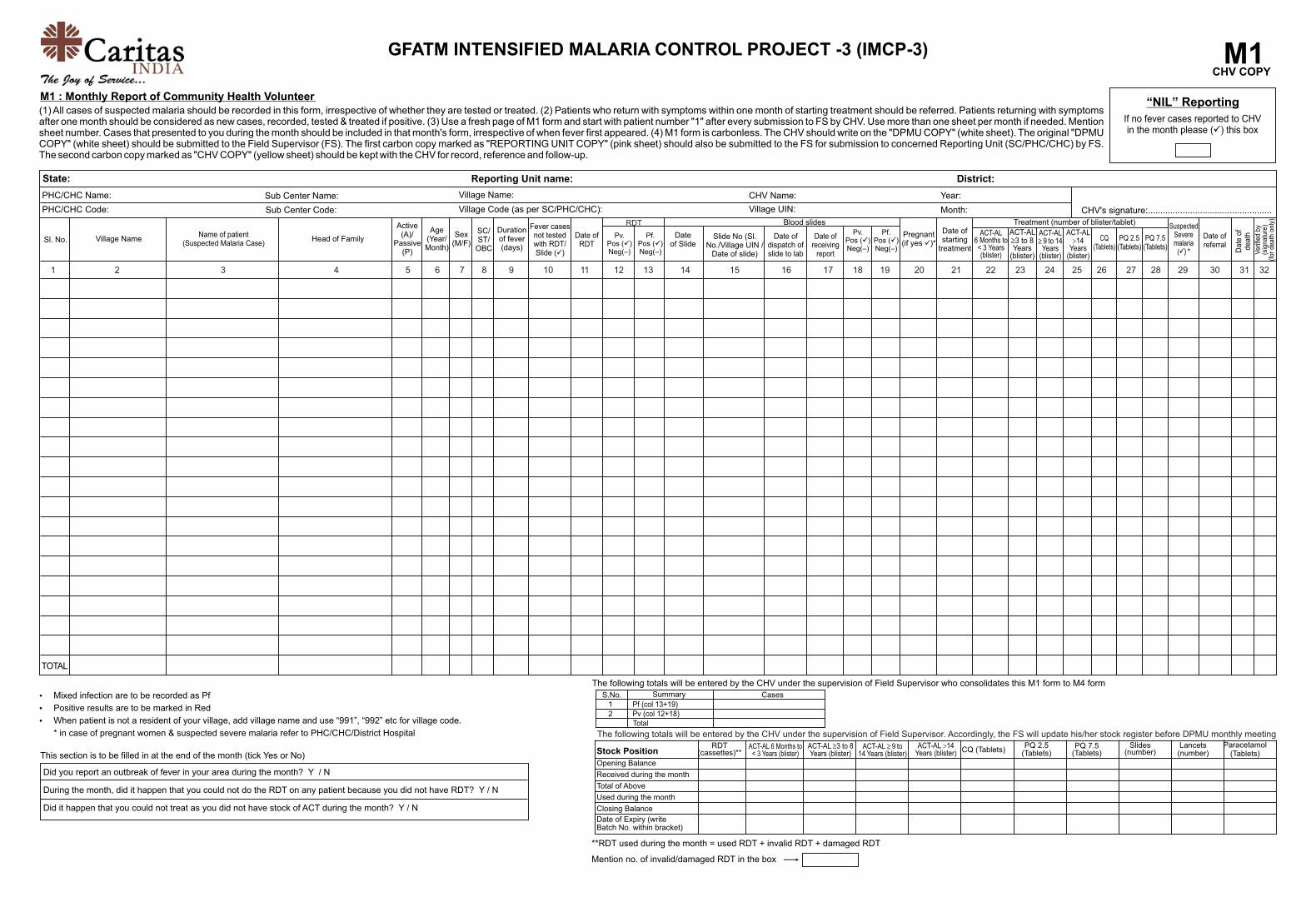
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
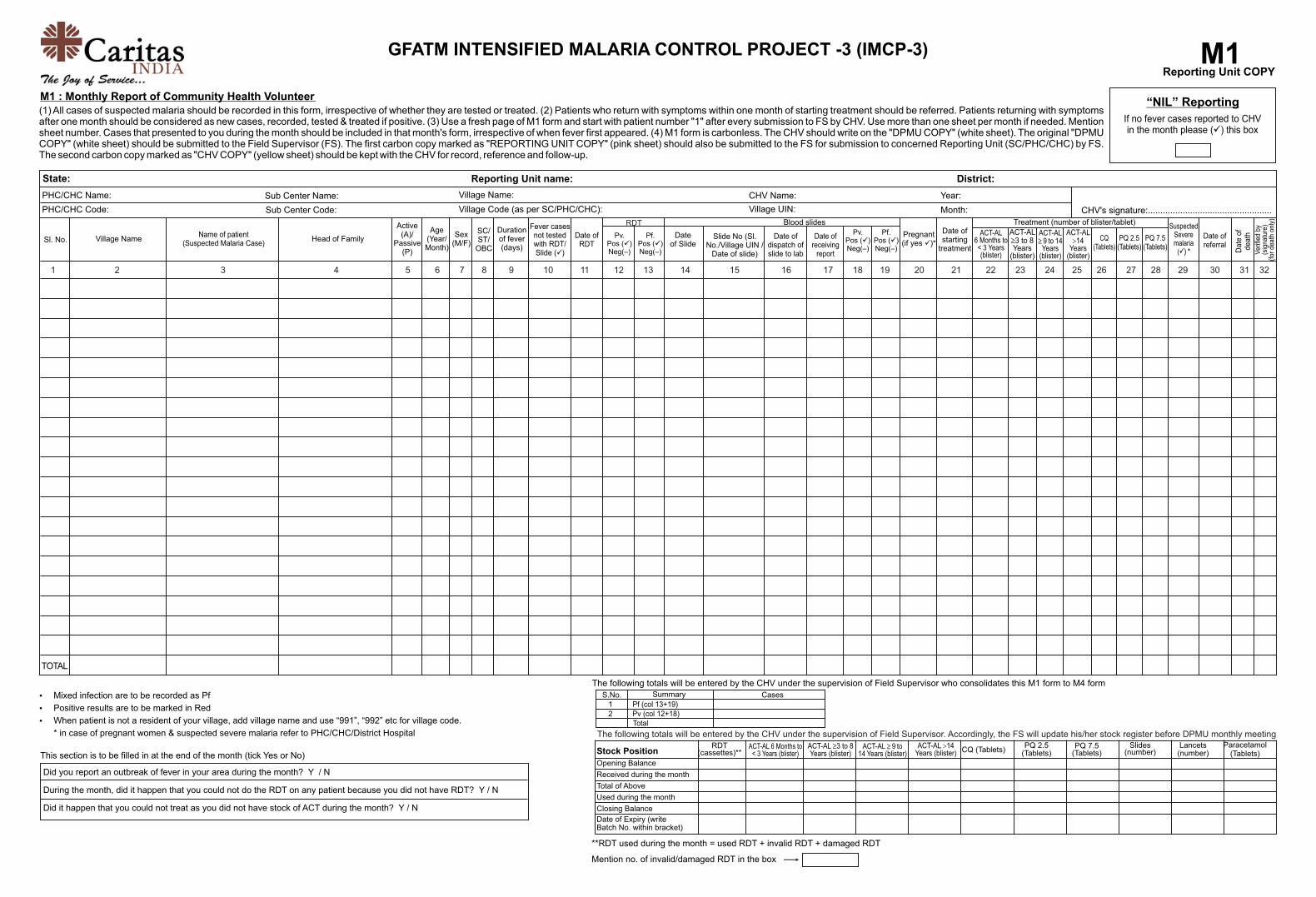
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
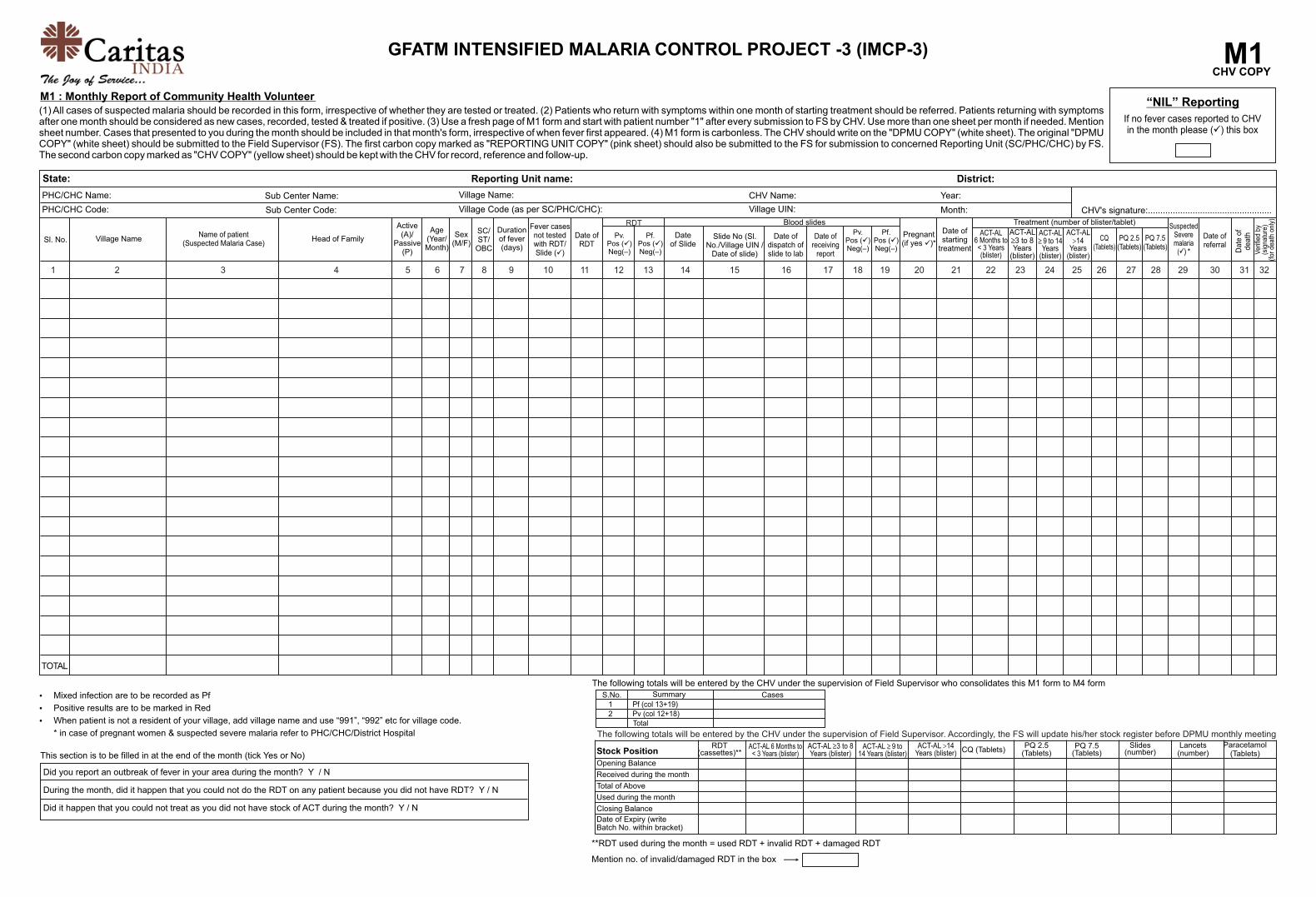
CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

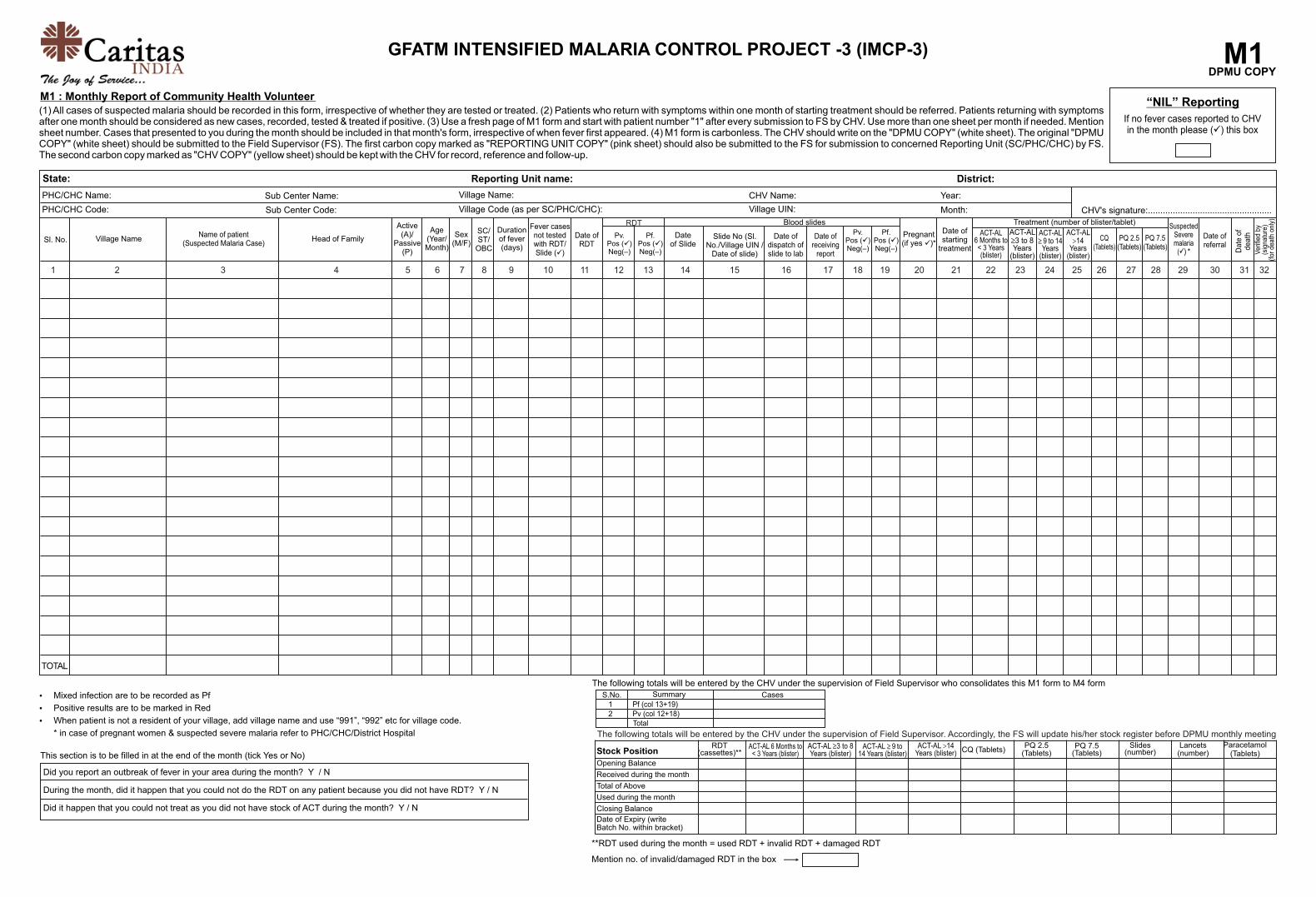
CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

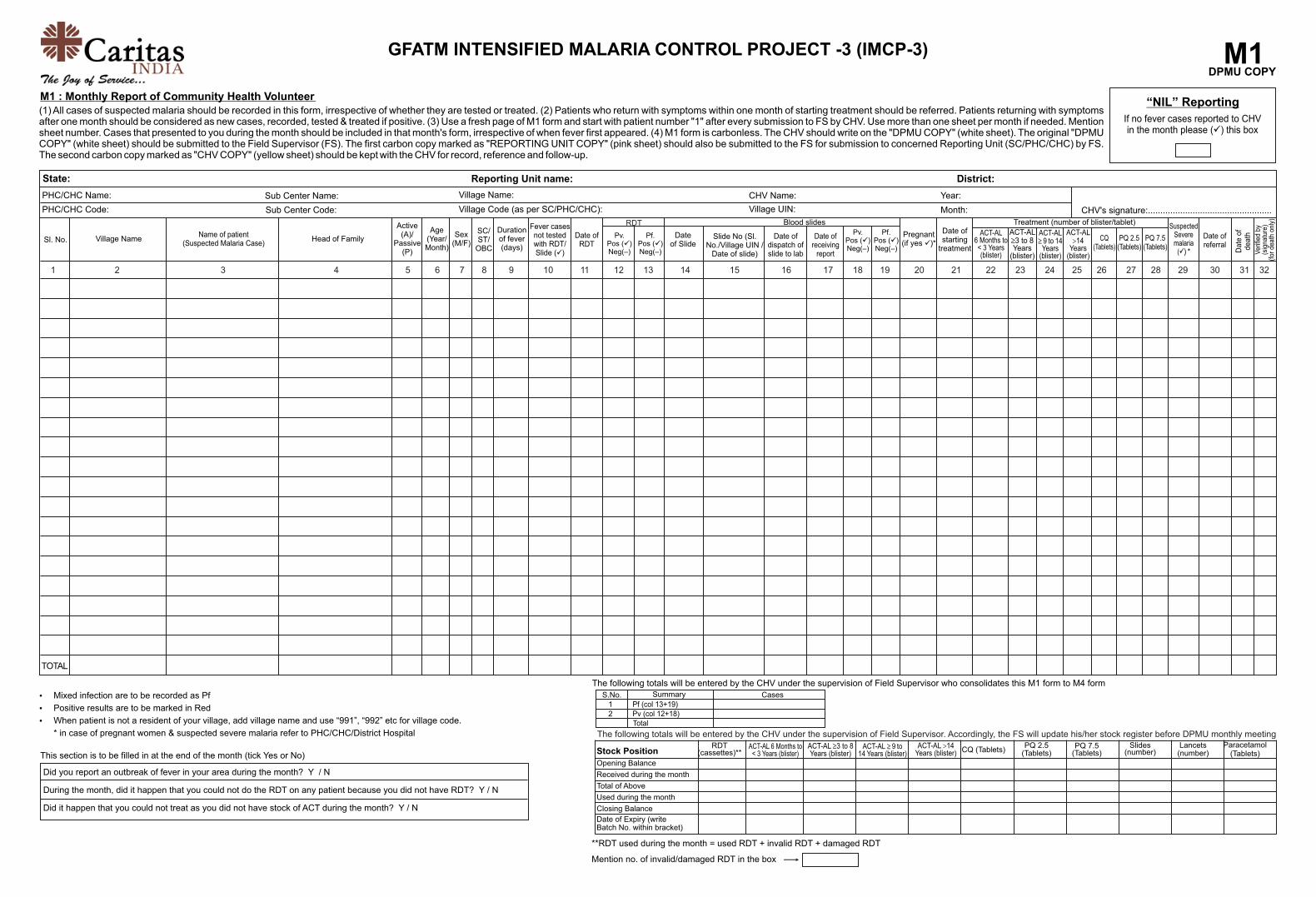
CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

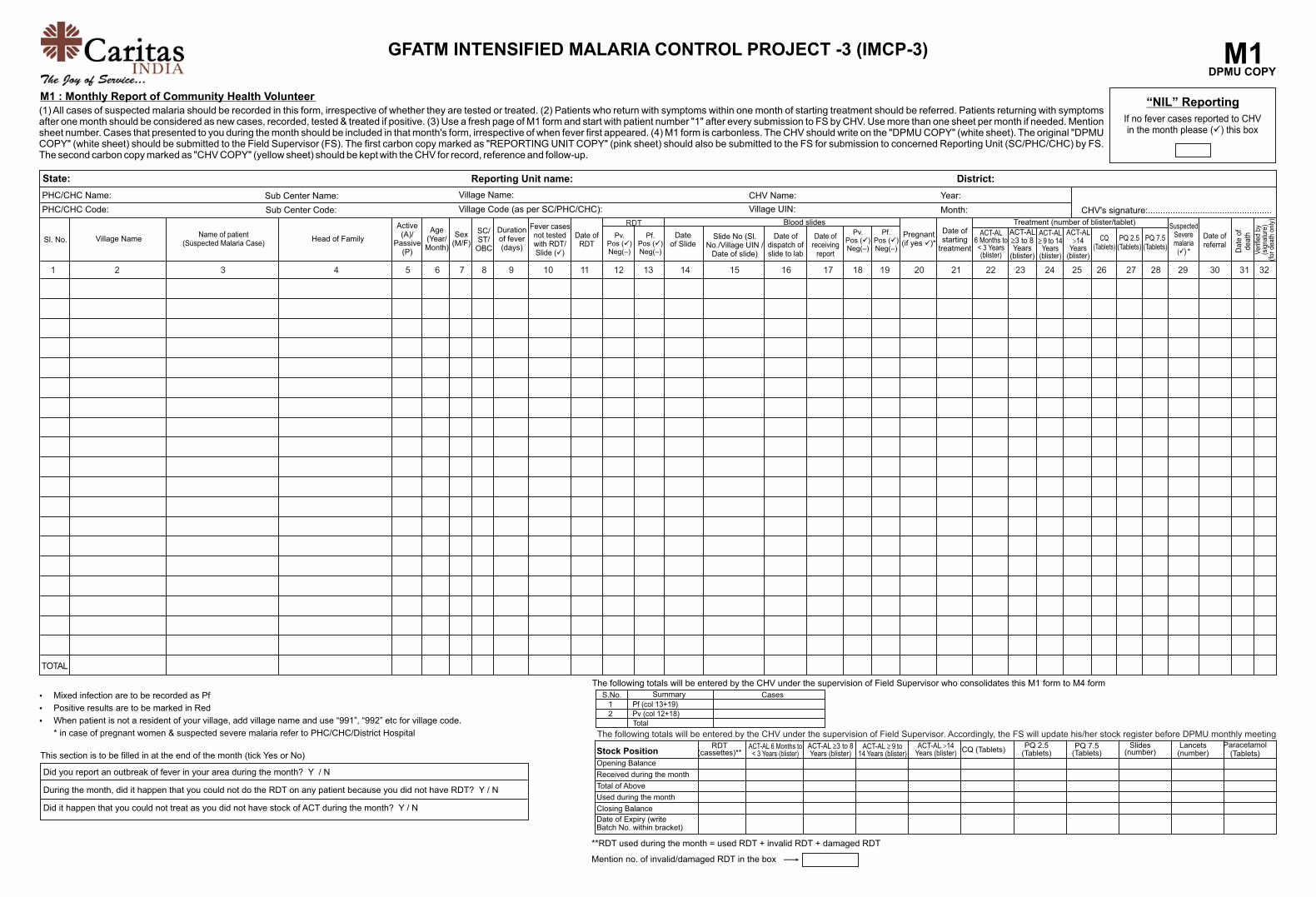
CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

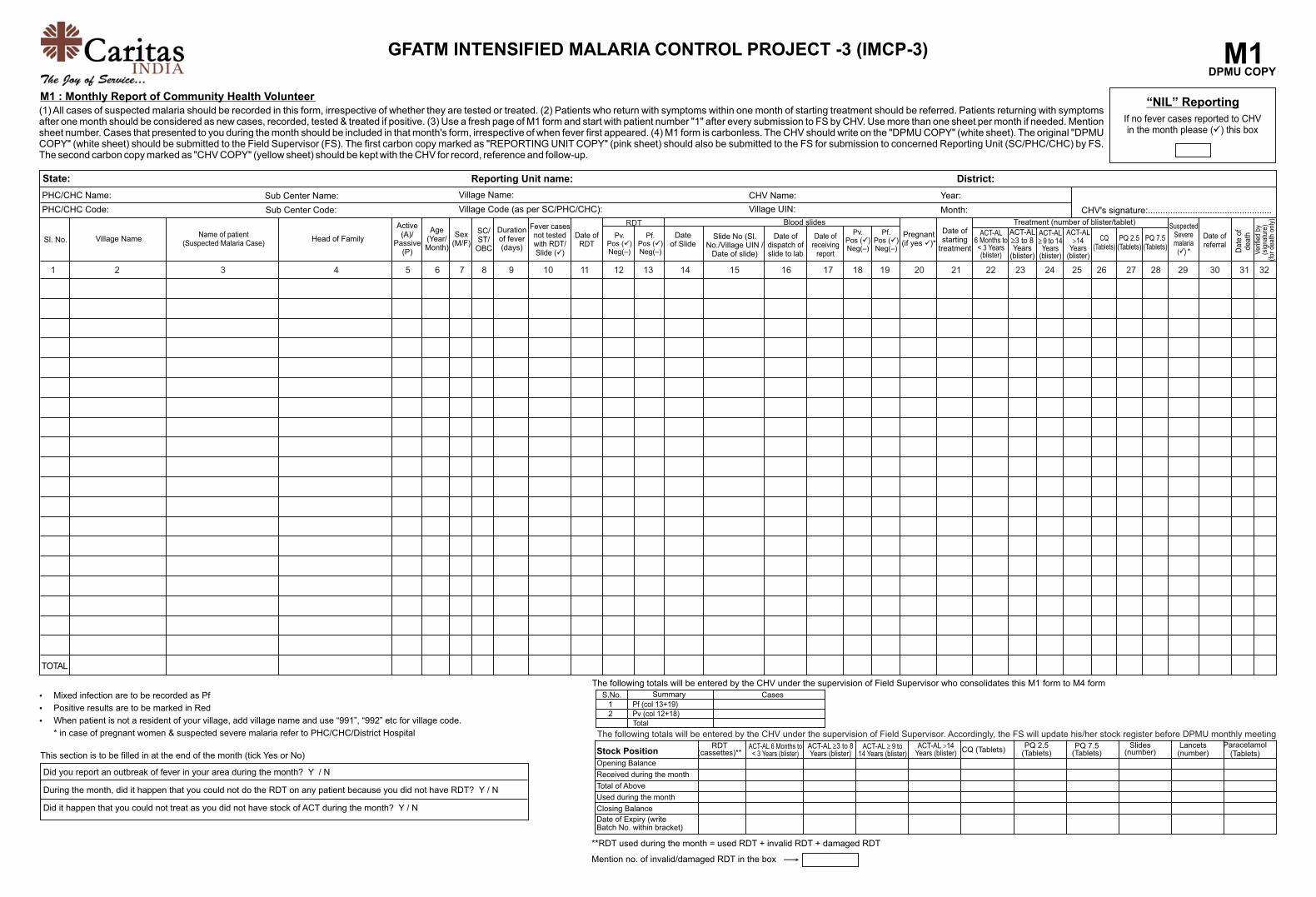
CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N


CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
This section is to be filled in at the end of the month (tick Yes or No)
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
M1DPMU COPY
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1Reporting Unit COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N

CHV Name: Year:
Village UIN: Month:
Pv.Pos ( )üNeg(–)
Date of Slide
Slide No (Sl.No./Village UIN /
Date of slide)
Date of dispatch ofslide to lab
Date ofreceiving
report
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³
Years (blister)
ACT-AL �9�to�14�³Years
(blister)
ACT-AL >14
Years (blister)
CQ (Tablets)
PQ 2.5 (Tablets)
TOTAL
Ÿ Mixed infection are to be recorded as Pf
Ÿ Positive results are to be marked in Red
Ÿ When patient is not a resident of your village, add village name and use “991”, “992” etc for village code.
* in case of pregnant women & suspected severe malaria refer to PHC/CHC/District Hospital
“NIL” Reporting
If no fever cases reported to CHV in the month please ( ) this boxü
GFATM INTENSIFIED MALARIA CONTROL PROJECT -3 (IMCP-3)
District:
PHC/CHC Name:
PHC/CHC Code:
M1 : Monthly Report of Community Health Volunteer
Date of RDT
Village Code (as per SC/PHC/CHC):
Village Name:
CHV's signature:..................................................
(1) All cases of suspected malaria should be recorded in this form, irrespective of whether they are tested or treated. (2) Patients who return with symptoms within one month of starting treatment should be referred. Patients returning with symptoms after one month should be considered as new cases, recorded, tested & treated if positive. (3) Use a fresh page of M1 form and start with patient number "1" after every submission to FS by CHV. Use more than one sheet per month if needed. Mention sheet number. Cases that presented to you during the month should be included in that month's form, irrespective of when fever first appeared. (4) M1 form is carbonless. The CHV should write on the "DPMU COPY" (white sheet). The original "DPMU COPY" (white sheet) should be submitted to the Field Supervisor (FS). The first carbon copy marked as "REPORTING UNIT COPY" (pink sheet) should also be submitted to the FS for submission to concerned Reporting Unit (SC/PHC/CHC) by FS. The second carbon copy marked as "CHV COPY" (yellow sheet) should be kept with the CHV for record, reference and follow-up.
State: Reporting Unit name:
Sub Center Name:
Sl. No. Village NameName of patient
(Suspected Malaria Case) Head of Family
Durationof fever(days)
Age(Year/Month)
Active(A)/
Passive(P)
Sex(M/F)
SC/ST/
OBC
Pregnant(if yes )*ü
Date
of
death
Ver
ified
by
(sig
natu
re)
(for
dea
th o
nly)
Date of starting
treatment
Suspected Severemalaria
(ü) *
Date ofreferral
Sub Center Code:
The following totals will be entered by the CHV under the supervision of Field Supervisor who consolidates this M1 form to M4 form
Fever casesnot testedwith RDT/Slide ( )ü
Pf.Pos ( )üNeg(–)
RDTPv.
Pos ( )üNeg(–)
Pf.Pos ( )üNeg(–)
Blood slides
PQ 7.5 (Tablets)
Treatment (number of blister/tablet)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32
S.No.12
Summary
Total
Pf (col 13+19)Pv (col 12+18)
Cases
The following totals will be entered by the CHV under the supervision of Field Supervisor. Accordingly, the FS will update his/her stock register before DPMU monthly meeting
RDT(cassettes)**
ACT-AL 6 Months to < 3 Years (blister)
ACT-AL 3 to 8 ³Years (blister)
ACT-AL �9�to�³14�Years (blister)
ACT-AL >14Years (blister) CQ (Tablets)
PQ 2.5(Tablets)
PQ 7.5(Tablets)
Slides(number)
Lancets(number)
Paracetamol(Tablets)
**RDT used during the month = used RDT + invalid RDT + damaged RDT
Mention no. of invalid/damaged RDT in the box
Stock Position
Opening Balance
Received during the month
Total of Above
Used during the month
Closing Balance
Date of Expiry (write Batch No. within bracket)
M1CHV COPY
This section is to be filled in at the end of the month (tick Yes or No)
Did you report an outbreak of fever in your area during the month? Y / N
During the month, did it happen that you could not do the RDT on any patient because you did not have RDT? Y / N
Did it happen that you could not treat as you did not have stock of ACT during the month? Y / N
