lpn 8 hour didactic iv education - nehca.org · lpn 8 hour didactic iv education peripheral...
TRANSCRIPT
LPN 8 Hour Didactic IV EducationPeripheral Intravenous Therapy
By Pamela Truscott, MSN, Nurse Educator, RN
• Health assessment and physical examination• Adequacy of blood flow• Integrity of the venous system• Factors impacting circulatory functioning
Peripheral Vascular System
Peripheral Veins• Inspect for varicosities, peripheral edema and phlebitis• Varicosities – superficial veins that become dilated• Dependent edema – sign of venous insufficiency or right-sided heart
failure• Phlebitis – inflammation of vein due to trauma, infection,
immobilization, or prolonged IV catheter insertion
Peripheral Replacement of Fluids and Electrolytes• Peripheral IV – catheter tip lies in a vein in the extremity• Central Venous IV – catheter tip lies in the central circulatory system
• e.g., vena cava close to right atrium of the heart
• Maintain standard precautions to minimize your risk of exposure to bloodborne pathogens
• IV administration of highly concentrated solution containing nutrients and electrolytes
• May be administered, depending on osmolality, through peripheral IV or central IV
• Osmolality – concentration or osmotic pressure of a solution
Parenteral Nutrition
Intravenous Therapy (Crystalloids)• Goal of IV fluid administration – correct or prevent fluid/electrolyte
disturbances• Allows direct access to vascular system• Must have provider’s order for type, amount, speed of administration• Must have knowledge of correct ordered solution, reason ordered,
equipment needed, procedures required to initiation infusion, regulate infusion rate and maintain system, how to identify/correct problems, and how to discontinue infusion
• Isotonic – same effective osmolality as body fluids• e.g., normal saline indicated for extracellular fluid volume replacement
• Hypotonic – effective osmolality less than body fluids• Decreasing osmolality by diluting body fluids and moving water into cells
• Hypertonic – effective osmolality greater than body fluids• Increase osmolality rapidly and pull water out of cells, causing them to shrivel
Types of Solutions
Intravenous SolutionsSolution Comments
Dextrose in Water Solutions Dextrose is another name for glucose
Saline Solutions Saline is sodium chloride in water
Dextrose in Saline Solutions
Balanced Electrolyte Solutions
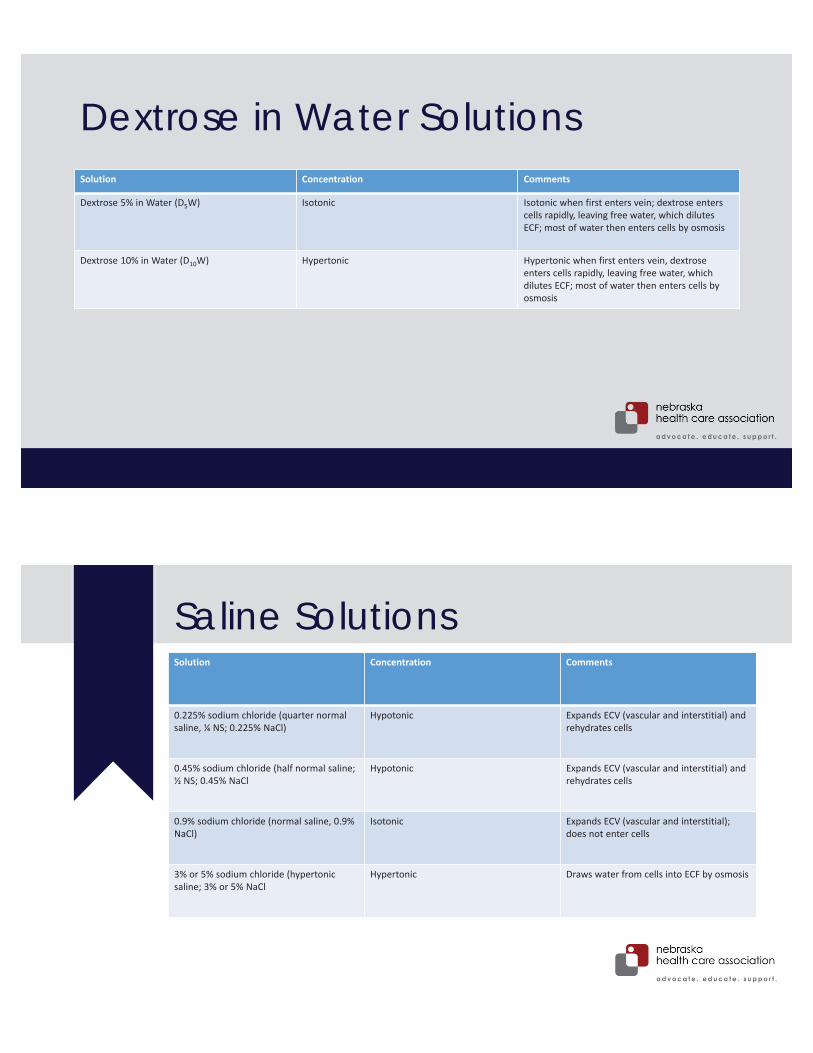
Dextrose in Water SolutionsSolution Concentration Comments
Dextrose 5% in Water (D5W) Isotonic Isotonic when first enters vein; dextrose enters cells rapidly, leaving free water, which dilutes ECF; most of water then enters cells by osmosis
Dextrose 10% in Water (D10W) Hypertonic Hypertonic when first enters vein, dextrose enters cells rapidly, leaving free water, which dilutes ECF; most of water then enters cells by osmosis
Saline SolutionsSolution Concentration Comments
0.225% sodium chloride (quarter normal saline, ¼ NS; 0.225% NaCl)
Hypotonic Expands ECV (vascular and interstitial) and rehydrates cells
0.45% sodium chloride (half normal saline; ½ NS; 0.45% NaCl
Hypotonic Expands ECV (vascular and interstitial) and rehydrates cells
0.9% sodium chloride (normal saline, 0.9% NaCl)
Isotonic Expands ECV (vascular and interstitial); does not enter cells
3% or 5% sodium chloride (hypertonic saline; 3% or 5% NaCl
Hypertonic Draws water from cells into ECF by osmosis
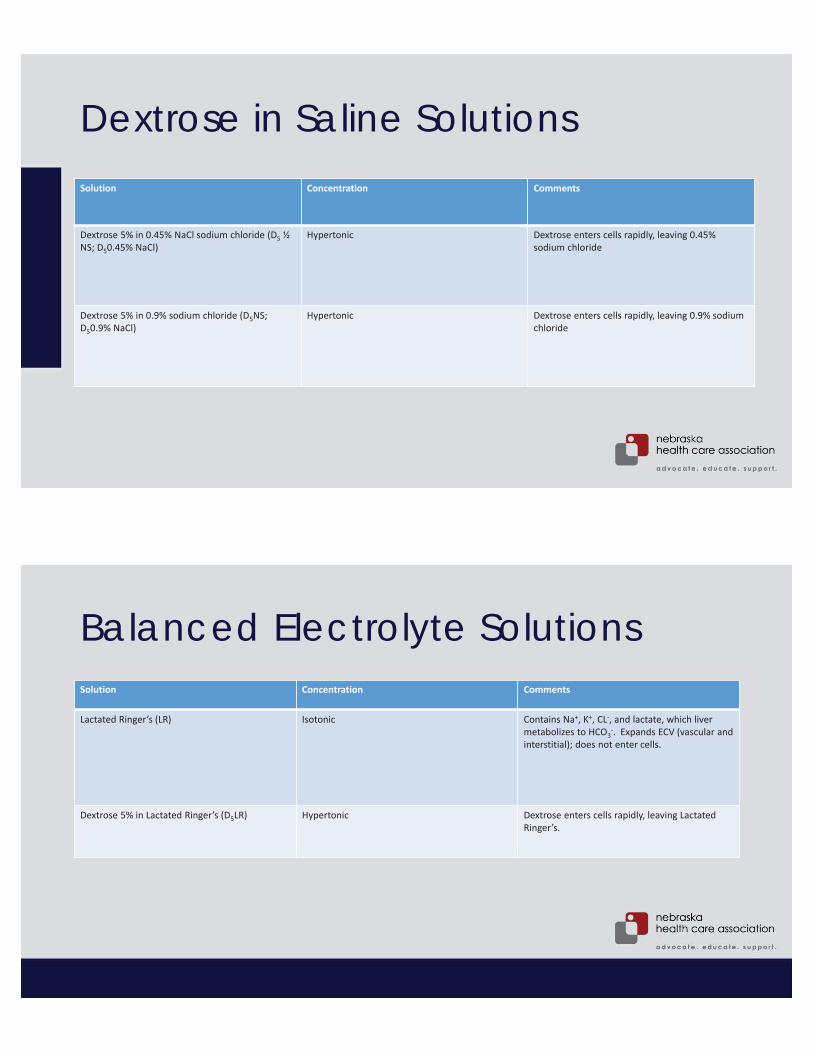
Dextrose in Saline SolutionsSolution Concentration Comments
Dextrose 5% in 0.45% NaCl sodium chloride (D5 ½ NS; D50.45% NaCl)
Hypertonic Dextrose enters cells rapidly, leaving 0.45% sodium chloride
Dextrose 5% in 0.9% sodium chloride (D5NS; D50.9% NaCl)
Hypertonic Dextrose enters cells rapidly, leaving 0.9% sodium chloride
Balanced Electrolyte SolutionsSolution Concentration Comments
Lactated Ringer’s (LR) Isotonic Contains Na+, K+, CL-, and lactate, which liver metabolizes to HCO3
-. Expands ECV (vascular and interstitial); does not enter cells.
Dextrose 5% in Lactated Ringer’s (D5LR) Hypertonic Dextrose enters cells rapidly, leaving Lactated Ringer’s.
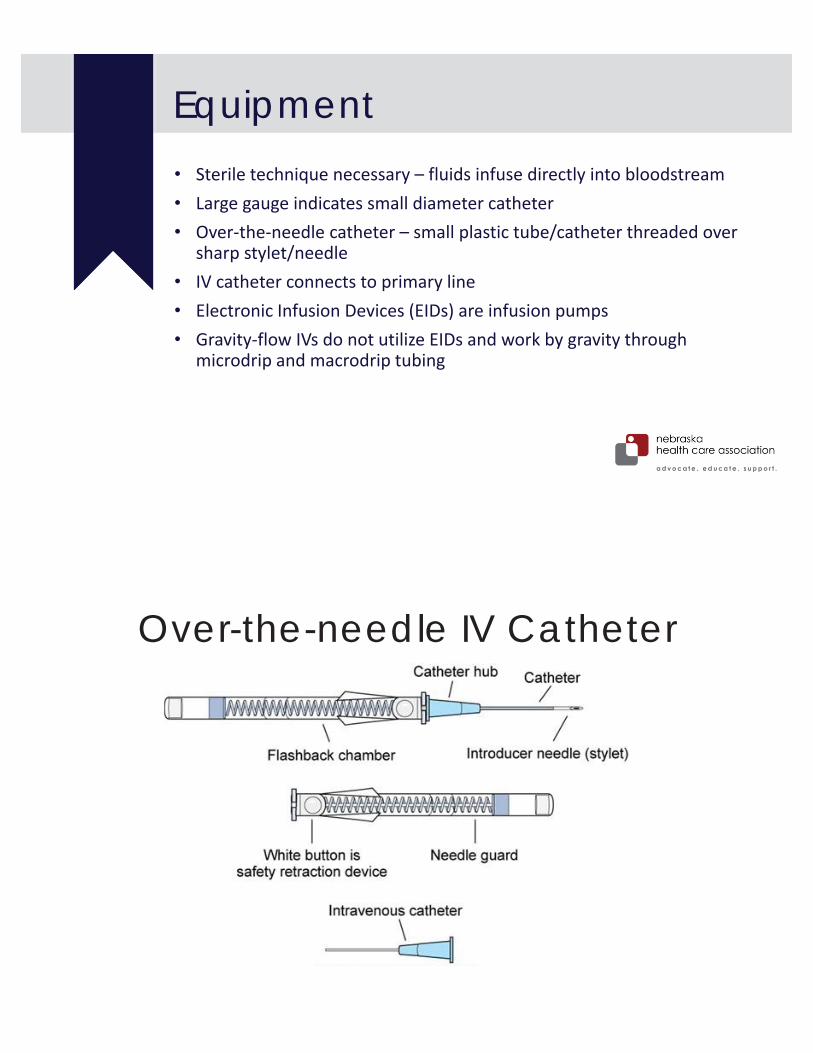
• Sterile technique necessary – fluids infuse directly into bloodstream• Large gauge indicates small diameter catheter• Over-the-needle catheter – small plastic tube/catheter threaded over
sharp stylet/needle• IV catheter connects to primary line• Electronic Infusion Devices (EIDs) are infusion pumps• Gravity-flow IVs do not utilize EIDs and work by gravity through
microdrip and macrodrip tubing
Equipment
Over-the-needle IV Catheter
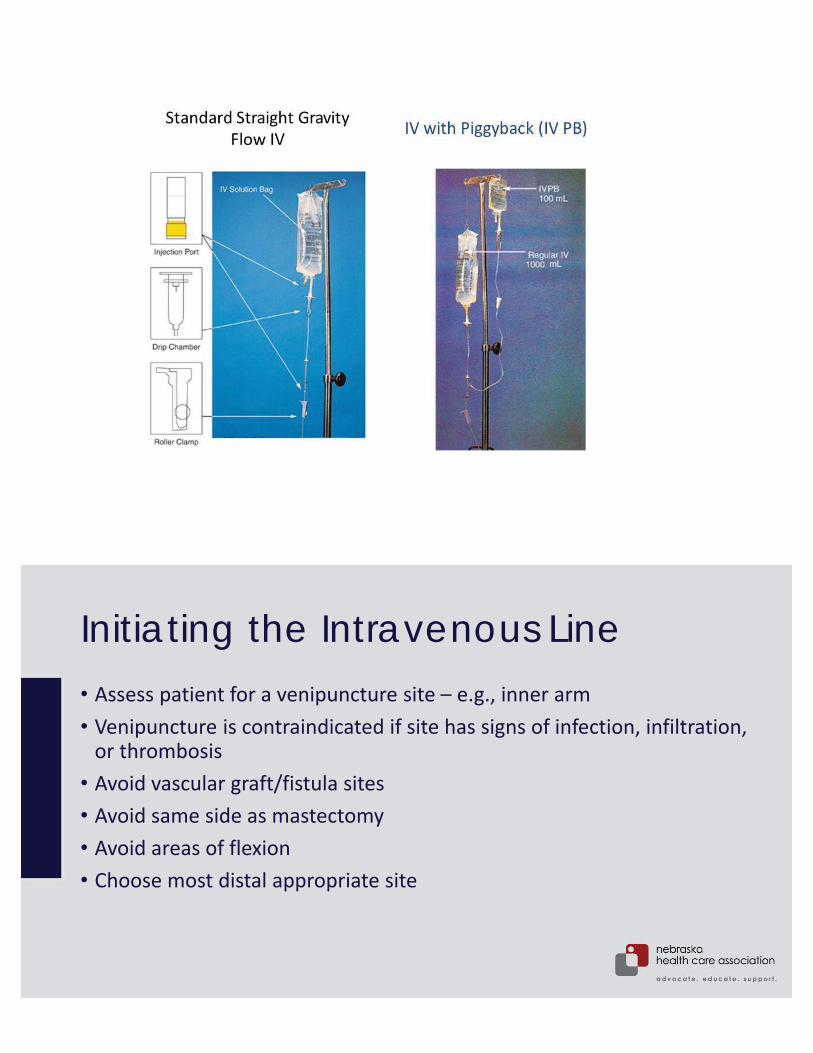
Initiating the Intravenous Line• Assess patient for a venipuncture site – e.g., inner arm• Venipuncture is contraindicated if site has signs of infection, infiltration,
or thrombosis• Avoid vascular graft/fistula sites• Avoid same side as mastectomy• Avoid areas of flexion• Choose most distal appropriate site
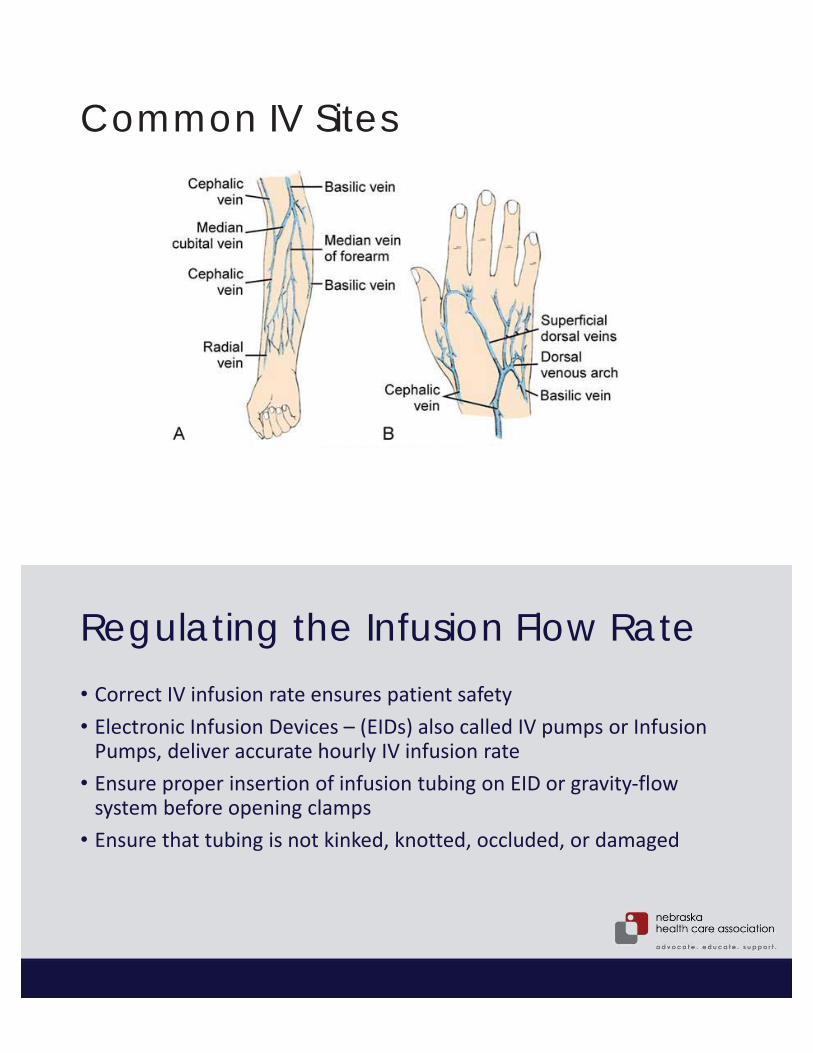
Common IV Sites
Regulating the Infusion Flow Rate• Correct IV infusion rate ensures patient safety• Electronic Infusion Devices – (EIDs) also called IV pumps or Infusion
Pumps, deliver accurate hourly IV infusion rate• Ensure proper insertion of infusion tubing on EID or gravity-flow
system before opening clamps• Ensure that tubing is not kinked, knotted, occluded, or damaged
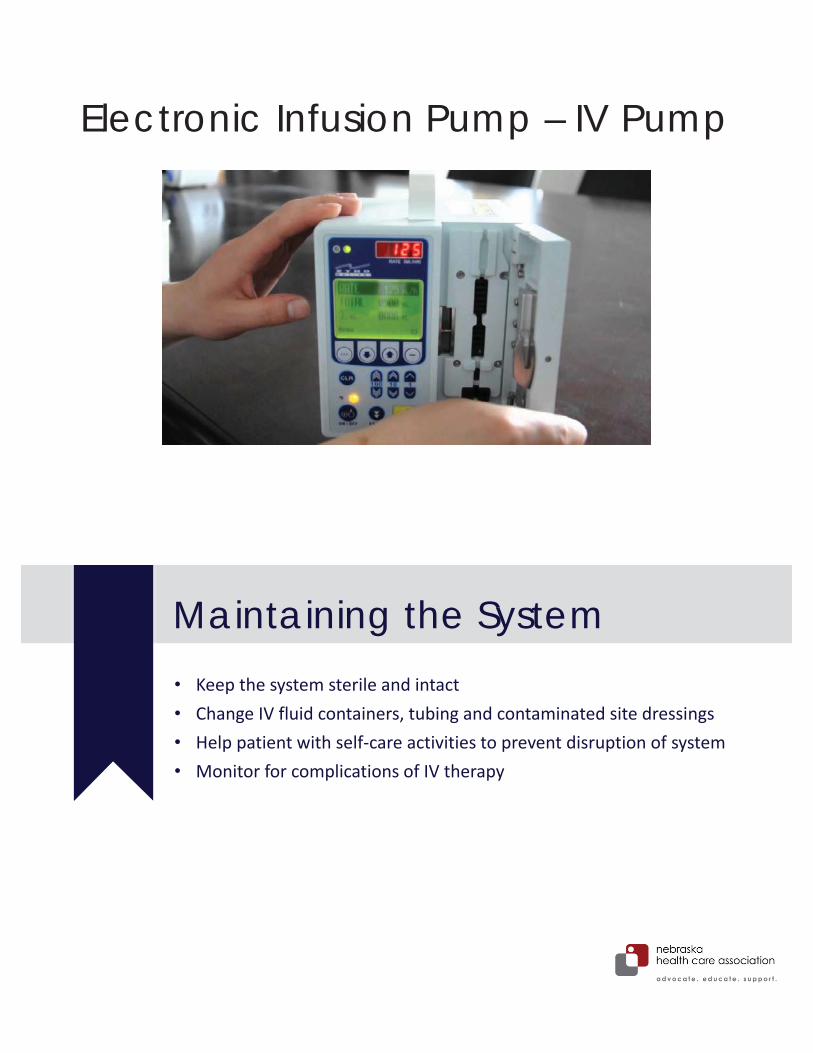
Electronic Infusion Pump – IV Pump
• Keep the system sterile and intact• Change IV fluid containers, tubing and contaminated site dressings• Help patient with self-care activities to prevent disruption of system• Monitor for complications of IV therapy
Maintaining the System
Helping Patients to Protect Intravenous Integrity• Help patient with hygiene, comfort measures, meals, and ambulation• Teach nursing assistants and patients that they must not break the
integrity of the IV line• Arm or hand infusion patients are able to walk unless contraindicated• Check to ensure IV container is at proper height on IV pole, no tension
on tubing, and correct flow rate • Instruct patient to report blood in tubbing, stoppage of flow, or
increased discomfort
• Potentially dangerous complication – circulatory overload• s/s often arise rapidly• Frequent assessment of patients receiving IV therapy is important
Complications of Intravenous Therapy
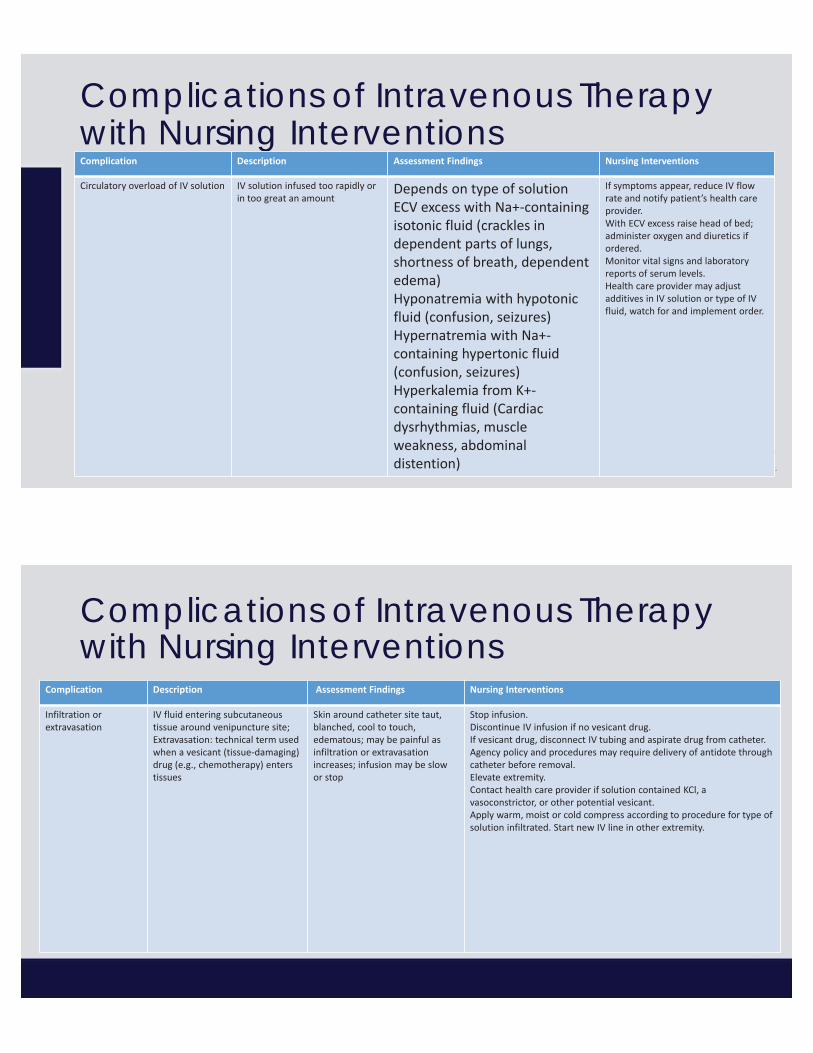
Complications of Intravenous Therapy with Nursing InterventionsComplication Description Assessment Findings Nursing Interventions
Circulatory overload of IV solution IV solution infused too rapidly or in too great an amount
Depends on type of solutionECV excess with Na+-containing isotonic fluid (crackles in dependent parts of lungs, shortness of breath, dependent edema)Hyponatremia with hypotonic fluid (confusion, seizures)Hypernatremia with Na+-containing hypertonic fluid (confusion, seizures)Hyperkalemia from K+-containing fluid (Cardiac dysrhythmias, muscle weakness, abdominal distention)
If symptoms appear, reduce IV flow rate and notify patient’s health care provider.With ECV excess raise head of bed; administer oxygen and diuretics if ordered.Monitor vital signs and laboratory reports of serum levels.Health care provider may adjust additives in IV solution or type of IV fluid, watch for and implement order.
Complications of Intravenous Therapy with Nursing Interventions
Complication Description Assessment Findings Nursing Interventions
Infiltration or extravasation
IV fluid entering subcutaneous tissue around venipuncture site;Extravasation: technical term used when a vesicant (tissue-damaging) drug (e.g., chemotherapy) enters tissues
Skin around catheter site taut,blanched, cool to touch, edematous; may be painful as infiltration or extravasation increases; infusion may be slow or stop
Stop infusion.Discontinue IV infusion if no vesicant drug.If vesicant drug, disconnect IV tubing and aspirate drug from catheter. Agency policy and procedures may require delivery of antidote through catheter before removal.Elevate extremity.Contact health care provider if solution contained KCl, a vasoconstrictor, or other potential vesicant.Apply warm, moist or cold compress according to procedure for type of solution infiltrated. Start new IV line in other extremity.

Complications of Intravenous Therapy with Nursing Interventions
Complication Description Assessment Findings Nursing Interventions
Phlebitis Inflammation of inner layer of a vein
Redness, tenderness, pain, warmth along course of vein starting at access site; possible red streak and/or palpable cord along vein
Stop infusion and discontinue IV line.Start new IV line in other extremity or proximal to previous insertion site if continued IV therapy is necessary. Apply warm, moist compress or contact IV therapy team or health care provider if area needs additional treatment.
Complications of Intravenous Therapy with Nursing InterventionsComplication Description Assessment Findings Nursing Interventions
Local Infection Infection at catheter-skinentry point during infusion or after removal of IV catheter
Redness, heat, swelling at catheter-skin entry point; possible purulent drainage
Culture any draining (if ordered).Clean skin with alcohol; remove catheter and savefor culture; apply sterile dressing.Notify health care provider.Start new IV line in other extremity.Initiate appropriate wound care if needed.
Complications of Intravenous Therapy with Nursing InterventionsComplication Description Assessment Findings Nursing Interventions
Bleeding at venipuncture site
Oozing or slow, continuous seepage of blood from venipuncture site
Fresh blood evident at venipuncture site, sometimes pooling under extremity
Assess if IV system is intact.If catheter is within vein, apply pressure dressing over site or change dressing.Start new IV line in other extremity or proximal to previous insertion site if VAD is dislodged, IV is disconnected, or bleeding from site does not stop.
• Occurs when IV catheter becomes dislodged or vein ruptures• IV fluids inadvertently enter subcutaneous tissue surrounding
venipuncture site• Extravasation occurs when IV fluid contains additives that damage
tissue• Causes coolness, paleness, and swelling of area
Infiltration

Infiltration ScaleGrade Clinical Criteria
0 No symptoms
1 Skin blanched, Edema <2.54 cm (1 inch) in any direction, cool to touch, with or without pain
2 Skin blanched, edema 2.54-15.2 cm (1-6 inches) in any direction, cool to touch, with or without pain
3 Skin blanched, translucent, gross edema >15.2 cm (6 inches) in any direction, cool to touch, mild-moderate pain, possible numbness
4 Skin blanched, translucent, skin tight, leaking, skin discolored, bruised, swollen, gross edema 15.2 cm (6 inches) in any direction, deep pitting tissue edema, circulatory impairment, moderate-to-severe pain, infiltration of any amount of blood product, irritant, or vesicant
Infiltration
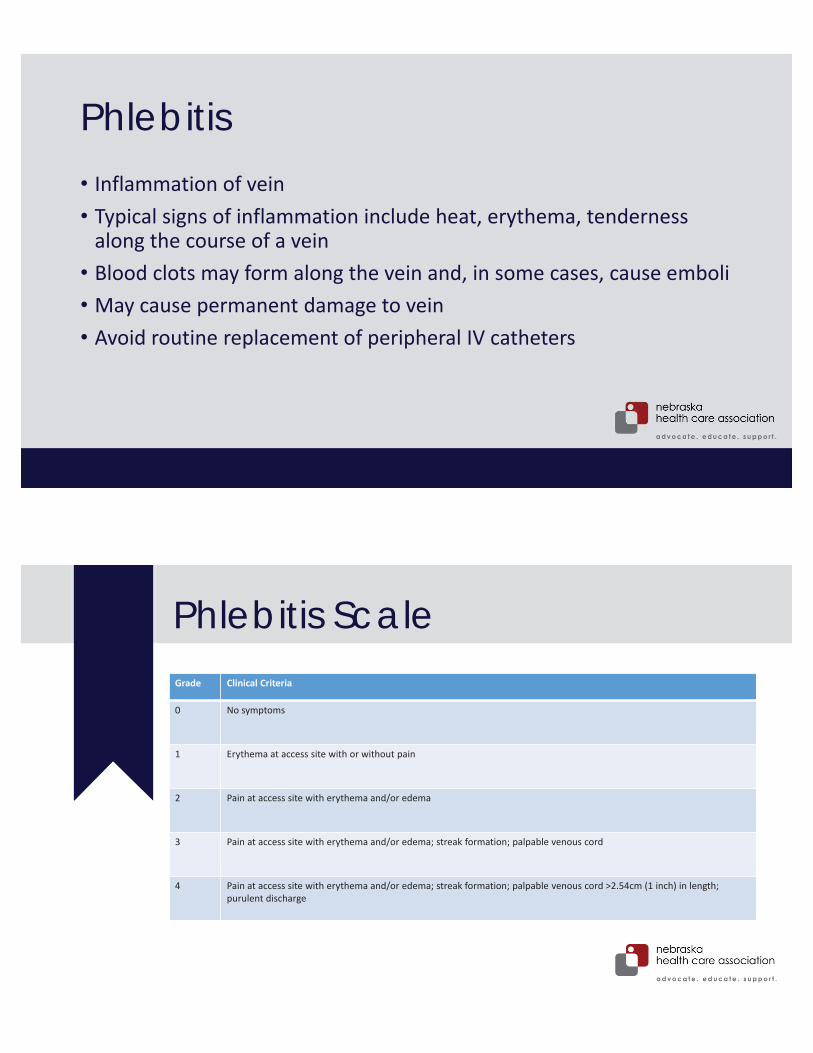
Phlebitis• Inflammation of vein• Typical signs of inflammation include heat, erythema, tenderness
along the course of a vein• Blood clots may form along the vein and, in some cases, cause emboli• May cause permanent damage to vein• Avoid routine replacement of peripheral IV catheters
Phlebitis ScaleGrade Clinical Criteria
0 No symptoms
1 Erythema at access site with or without pain
2 Pain at access site with erythema and/or edema
3 Pain at access site with erythema and/or edema; streak formation; palpable venous cord
4 Pain at access site with erythema and/or edema; streak formation; palpable venous cord >2.54cm (1 inch) in length; purulent discharge
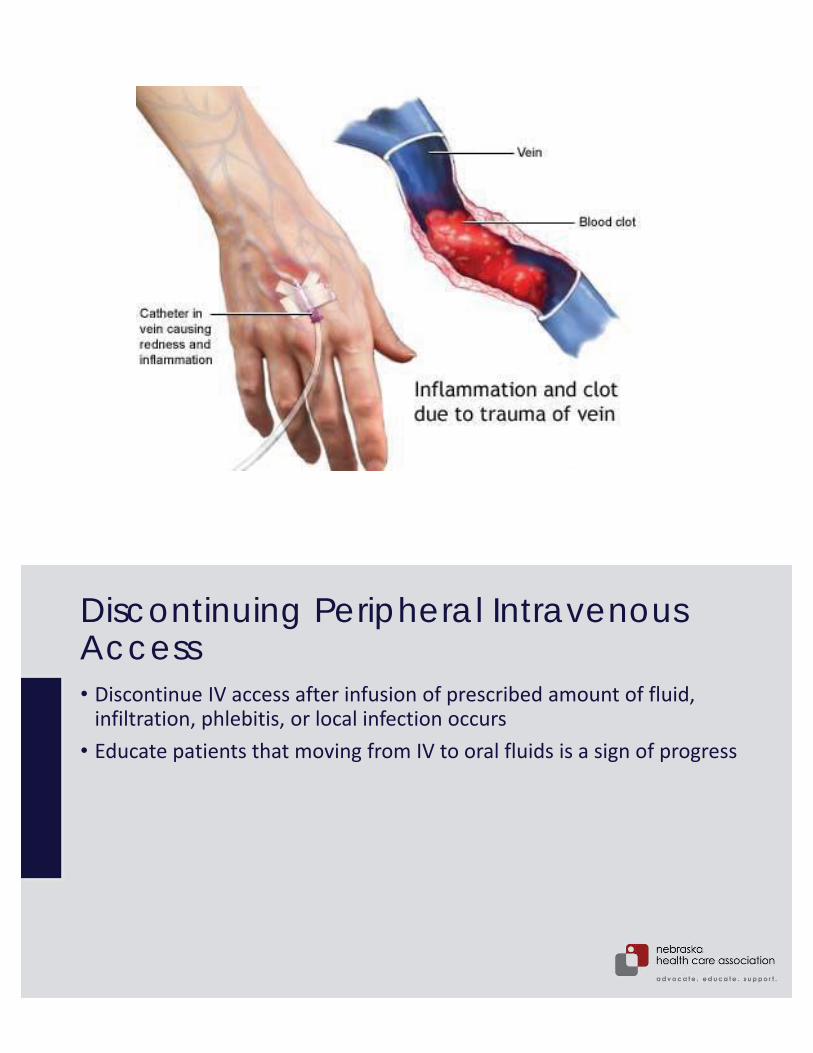
Discontinuing Peripheral Intravenous Access• Discontinue IV access after infusion of prescribed amount of fluid,
infiltration, phlebitis, or local infection occurs• Educate patients that moving from IV to oral fluids is a sign of progress

Protection of Skin and Veins During Intravenous Therapy – Older Adults• Use smallest-gauge catheter or needle• Avoid the back of the hand• Avoid vigorous friction while cleaning• Fragile skin limit tourniquet or place over sleeve – utilize blood pressure cuff• Lower the insertion angle• Veins roll away from needle – use traction • Secure IV site with a catheter stabilization device• Medications and supplements increase likelihood of bruising/bleeding
• Administer medications IV by the following methods:• As mixtures within large volumes of IV fluids• By injection of a bolus or small volume of medication through an existing IV
infusion line or intermittent venous access• By “piggyback” infusion of a solution containing a prescribed medication and a
small volume of IV fluid through an existing IV line
• Because IV medications are immediately available to bloodstream, verify rate of admission with drug reference book or pharmacist
Intravenous Administration
Large-Volume Infusions• Mixing medications in large volumes of fluids is the safest and easiest• With continuous infusion – if IV fluid is infused too rapidly the patient is
at risk for medication overdose and circulatory fluid overload• Current best practices include use of IV medication that come in
standardized concentration and dosages; standardized procedures for ordering, preparing and administering; and ready-to-administer doses
• Do not add medications to IV bags that are already hanging – no way to tell the exact concentration of medication – only add to new IV bags
Intravenous Bolus
• Involves introducing concentrated medication dose directly into the systemic circulation
• IV Bolus/push is the most dangerous method for administration• Bolus may cause direct irritation to the lining of blood vessels• Determine rate of administration for IV bolus/push• Consider the purpose of the IV medication• Consider potential adverse effects related to rate or route

• Administers IV medications through small amounts (50-100mL) of compatible fluids
• Advantages of volume-controlled infusions include:• Reduces risk of rapid-dose infusion by IV push• Allows for administration of medications that are stable for a limited time• Allows for control of IV fluid intake
Volume-Controlled Infusions
Piggyback
• Small (25-250 mL) IV bag/bottle connected to short tubing
• Connects via upper Y-port of primary infusion line or intermittent venous access
• Piggyback tubing is either microdrip or macrodrip system
• Called piggyback because it is placed higher than the primary infusion bag/bottle
Primary infusion bag Piggyback infusion bag
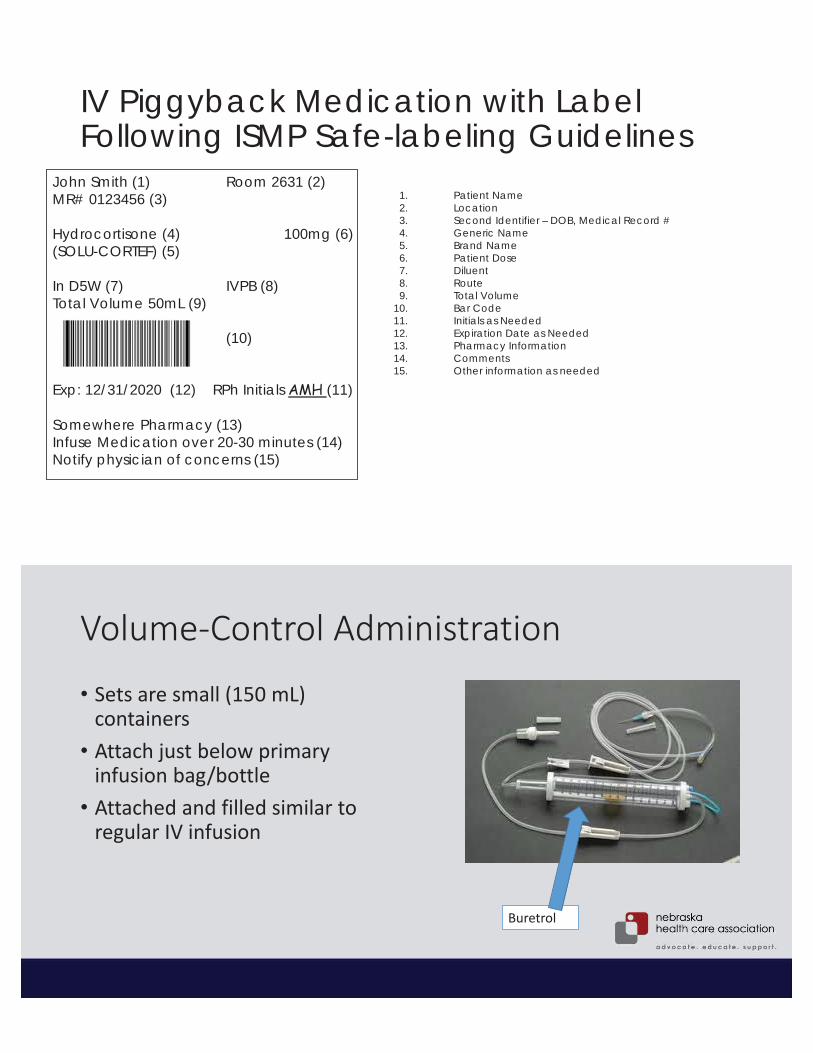
IV Piggyback Medication with Label Following ISMP Safe-labeling Guidelines
1.2.3.4.5.6.7.8.9.
10.11.12.13.14.15.
Patient NameLocationSecond Identifier – DOB, Medical Record #Generic NameBrand NamePatient DoseDiluentRouteTotal VolumeBar CodeInitials as NeededExpiration Date as NeededPharmacy Information CommentsOther information as needed
John Smith (1) Room 2631 (2)MR# 0123456 (3)
Hydrocortisone (4) 100mg (6)(SOLU-CORTEF) (5)
In D5W (7) IVPB (8)Total Volume 50mL (9)
(10)
Exp: 12/31/2020 (12) RPh Initials AMH (11)
Somewhere Pharmacy (13)Infuse Medication over 20-30 minutes (14)Notify physician of concerns (15)
Volume-Control Administration
• Sets are small (150 mL) containers
• Attach just below primary infusion bag/bottle
• Attached and filled similar to regular IV infusion
Buretrol
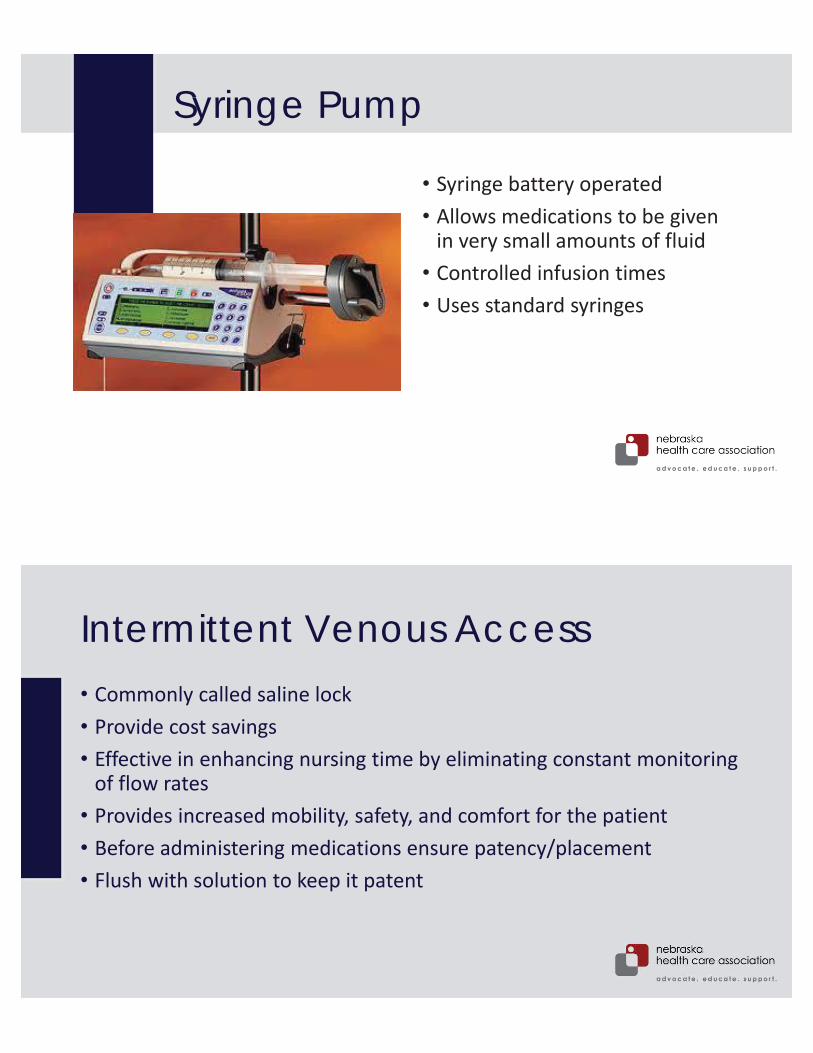
Syringe Pump
• Syringe battery operated• Allows medications to be given
in very small amounts of fluid• Controlled infusion times• Uses standard syringes
Intermittent Venous Access• Commonly called saline lock• Provide cost savings • Effective in enhancing nursing time by eliminating constant monitoring
of flow rates• Provides increased mobility, safety, and comfort for the patient• Before administering medications ensure patency/placement• Flush with solution to keep it patent
• Body fluids contain water, Na+ and other electrolytes are distributed between ECF and ICF compartments
• Osmolality imbalances are abnormal concentrations of body fluids, manifested at altered serum Na+ levels and decreased level of consciousness
• Initiation and maintenance of IV therapy require clinical decision making, skill and organized procedures to maintain sterility and patency of the system
• Nurses monitor vigilantly for complications of IV therapy
Key Points
Safety Guidelines for Nursing Skills• Be vigilant during entire medication administration process• Do not get distracted during medication set up• Verify expiration date• Identify patient correctly• Clarify all unclear orders• Do not use “work-arounds”• Educate patients• Follow Nurse Practice Act and employer policies/procedures

ReferencePotter, P.A., Perry, A.G., Hall, A., & Stockert, P.A. (2017). Fundamentals of Nursing. St Louis, MO: Mosby Elsevier.
Nebraska Health Care AssociationLicensed Practical Nurse Association of Nebraska1200 Libra Drive, Suite 100Lincoln, NE [email protected]
Contact Information