lower birth weight of dutch neonates who were in utero at the time of the 9/11 attacks
TRANSCRIPT

Journal of Psychosomatic Res
Lower birth weight of Dutch neonates who were in utero at the
time of the 9/11 attacks
Luc Smitsa,4, Lydia Krabbendamb, Rob de Biea, Gerard Essedc, Jim van Osb
aDepartment of Epidemiology, Care and Public Health Research Institute, Maastricht University, Maastricht, The NetherlandsbDepartment of Psychiatry and Neuropsychology, South Limburg Mental Health Research and Teaching Network,
European Graduate School of Neuroscience Maastricht, Maastricht University, Maastricht, The NetherlandscDepartment of Obstetrics and Gynaecology, Maastricht University, University Hospital, Maastricht, The Netherlands
Received 25 August 2005; received in revised form 24 April 2006; accepted 27 April 2006
Abstract
Objective: Maternal stress during pregnancy has been reported
to have an adverse influence on fetal growth. The terrorist attacks
of September 11, 2001, on the United States have provoked
feelings of insecurity and stress worldwide. Our aim was to test
the hypothesis that maternal exposure to these acts of terrorism via
the media had an unfavorable influence on mean birth weight in the
Netherlands. Methods: We compared birth weights of 1885 Dutch
neonates who were in utero during the attacks with those of 1258
neonates who were in utero exactly 1 year later. Results: In the
0022-3999/06/$ – see front matter D 2006 Elsevier Inc. All rights reserved.
doi:10.1016/j.jpsychores.2006.04.020
4 Corresponding author. Department of Epidemiology, P.O. Box 616,
6200 MD, Maastricht University, Maastricht, The Netherlands. Tel.: +31 43
3882821.
E-mail address: [email protected] (L. Smits).
exposed group, birth weight was lower than in the nonexposed
group (difference, 48 g; 95% confidence interval=13.6, 82.9;
P=.006). The difference in birth weight could not be explained by
tobacco use, maternal age, parity, or other potential confounders or
by shorter pregnancy durations. Conclusion: These results provide
evidence supporting the hypothesis that exposure of Dutch
pregnant women to the 9/11 events via the media has had an
adverse effect on the birth weight of their offspring.
D 2006 Elsevier Inc. All rights reserved.
Keywords: Birth weight; Netherlands; Pregnancy; September 11 Terrorist Attacks; Stress; Psychological
Introduction
The terrorist attacks against the United States on
September 11, 2001, had a profound psychological impact,
both on those directly involved and on those that were
exposed to them via the media. Seventeen percent of the
U.S. population outside of New York reported symptoms of
9/11-related posttraumatic stress 2 months after the attacks
[1]. Women were found to be more liable to posttraumatic
stress after these events than men (odds ratio, 1.64), and so
were individuals who suffered from anxiety or depression
before the events (odds ratio, 1.84). Since pregnant women
exhibit higher rates of depression and anxiety, exposure to
the 9/11 attacks via the media may have had relatively high
psychological impact within this group.
Experimental animal studies and human studies have
shown associations between maternal stress and pregnancy
outcome [2,3]. Increased risks have been found for, among
others, low birth weight and preterm delivery. We hypothe-
sized that women who were pregnant at the time of the 9/11
attacks on the United States gave birth to smaller babies and
had shorter pregnancy lengths than a comparable group of
women who were pregnant exactly 1 year later.
Methods
We used data from a prospective cohort study of
pregnancy-related pelvic girdle pain, conducted in 2001,
2002, and 2003 in the southeastern part of the Netherlands
[4]. For this study, women were recruited by midwives and
earch 61 (2006) 715–717
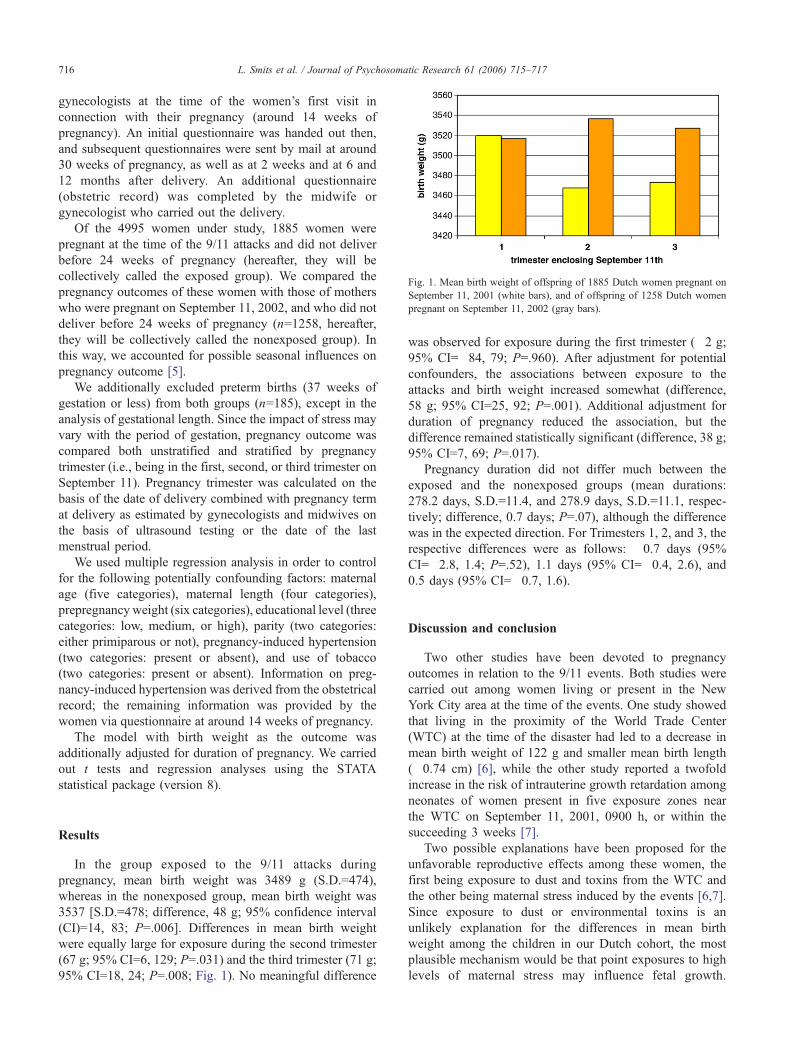
Fig. 1. Mean birth weight of offspring of 1885 Dutch women pregnant on
September 11, 2001 (white bars), and of offspring of 1258 Dutch women
pregnant on September 11, 2002 (gray bars).
L. Smits et al. / Journal of Psychosomatic Research 61 (2006) 715–717716
gynecologists at the time of the women’s first visit in
connection with their pregnancy (around 14 weeks of
pregnancy). An initial questionnaire was handed out then,
and subsequent questionnaires were sent by mail at around
30 weeks of pregnancy, as well as at 2 weeks and at 6 and
12 months after delivery. An additional questionnaire
(obstetric record) was completed by the midwife or
gynecologist who carried out the delivery.
Of the 4995 women under study, 1885 women were
pregnant at the time of the 9/11 attacks and did not deliver
before 24 weeks of pregnancy (hereafter, they will be
collectively called the exposed group). We compared the
pregnancy outcomes of these women with those of mothers
who were pregnant on September 11, 2002, and who did not
deliver before 24 weeks of pregnancy (n=1258, hereafter,
they will be collectively called the nonexposed group). In
this way, we accounted for possible seasonal influences on
pregnancy outcome [5].
We additionally excluded preterm births (37 weeks of
gestation or less) from both groups (n=185), except in the
analysis of gestational length. Since the impact of stress may
vary with the period of gestation, pregnancy outcome was
compared both unstratified and stratified by pregnancy
trimester (i.e., being in the first, second, or third trimester on
September 11). Pregnancy trimester was calculated on the
basis of the date of delivery combined with pregnancy term
at delivery as estimated by gynecologists and midwives on
the basis of ultrasound testing or the date of the last
menstrual period.
We used multiple regression analysis in order to control
for the following potentially confounding factors: maternal
age (five categories), maternal length (four categories),
prepregnancyweight (six categories), educational level (three
categories: low, medium, or high), parity (two categories:
either primiparous or not), pregnancy-induced hypertension
(two categories: present or absent), and use of tobacco
(two categories: present or absent). Information on preg-
nancy-induced hypertension was derived from the obstetrical
record; the remaining information was provided by the
women via questionnaire at around 14 weeks of pregnancy.
The model with birth weight as the outcome was
additionally adjusted for duration of pregnancy. We carried
out t tests and regression analyses using the STATA
statistical package (version 8).
Results
In the group exposed to the 9/11 attacks during
pregnancy, mean birth weight was 3489 g (S.D.=474),
whereas in the nonexposed group, mean birth weight was
3537 [S.D.=478; difference, 48 g; 95% confidence interval
(CI)=14, 83; P=.006]. Differences in mean birth weight
were equally large for exposure during the second trimester
(67 g; 95% CI=6, 129; P=.031) and the third trimester (71 g;
95% CI=18, 24; P=.008; Fig. 1). No meaningful difference
was observed for exposure during the first trimester (�2 g;
95% CI=�84, 79; P=.960). After adjustment for potential
confounders, the associations between exposure to the
attacks and birth weight increased somewhat (difference,
58 g; 95% CI=25, 92; P=.001). Additional adjustment for
duration of pregnancy reduced the association, but the
difference remained statistically significant (difference, 38 g;
95% CI=7, 69; P=.017).
Pregnancy duration did not differ much between the
exposed and the nonexposed groups (mean durations:
278.2 days, S.D.=11.4, and 278.9 days, S.D.=11.1, respec-
tively; difference, 0.7 days; P=.07), although the difference
was in the expected direction. For Trimesters 1, 2, and 3, the
respective differences were as follows: �0.7 days (95%
CI=�2.8, 1.4; P=.52), 1.1 days (95% CI=�0.4, 2.6), and0.5 days (95% CI=�0.7, 1.6).
Discussion and conclusion
Two other studies have been devoted to pregnancy
outcomes in relation to the 9/11 events. Both studies were
carried out among women living or present in the New
York City area at the time of the events. One study showed
that living in the proximity of the World Trade Center
(WTC) at the time of the disaster had led to a decrease in
mean birth weight of 122 g and smaller mean birth length
(�0.74 cm) [6], while the other study reported a twofold
increase in the risk of intrauterine growth retardation among
neonates of women present in five exposure zones near
the WTC on September 11, 2001, 0900 h, or within the
succeeding 3 weeks [7].
Two possible explanations have been proposed for the
unfavorable reproductive effects among these women, the
first being exposure to dust and toxins from the WTC and
the other being maternal stress induced by the events [6,7].
Since exposure to dust or environmental toxins is an
unlikely explanation for the differences in mean birth
weight among the children in our Dutch cohort, the most
plausible mechanism would be that point exposures to high
levels of maternal stress may influence fetal growth.

L. Smits et al. / Journal of Psychosomatic Research 61 (2006) 715–717 717
Although we were not able to adequately measure levels of
stress and anxiety in our population during the first months
after September 11, 2001, and September 11, 2002, other
authors have observed a rise in PTSD symptoms and a rise
in suicidal behavior in the Dutch population in the aftermath
of the terrorist attacks [8,9].
Mulder et al. [2] have proposed several mechanisms by
which maternal stress may reach the fetus and exert
unfavorable effects on fetal growth and gestational length.
First, although a large part of maternal cortisol is converted
in the placenta to the biologically inactive cortisone, rises in
maternal cortisol have been shown to lead to higher cortisol
levels in the fetus. Second, activation of the maternal
sympathetic nervous system by stress may lead to reduced
blood flow to the uterus and fetus, which may contribute to
fetal growth restriction. Third, maternal stress provokes
increased secretions of maternal and placental corticotropin-
releasing hormone, which in turn may initiate a cascade of
events that eventually lead to (early) delivery.
An alternative explanation of our findings could be that
there is a trend of increasing birth weight over the years. We
evaluated this possibility by carrying out regression analyses
of birth weight and gestational duration as a function of time
(days) for children not included in the analysis. These
children were conceived during the following periods: July
2000 to January 2001, September 2001 to January 2002, and
September 2002 to October 2002. The results of the
regression analyses indicate that there were no time trends
in birth weight (b=.03057; P=.55) or gestational duration(b=�.00113; P=.36).
The finding that the effects on birth weight were
confined to the second and third trimesters of pregnancy
is at odds with the observation of some authors that
maternal stress is more harmful during the first trimester, as
opposed to the second and third trimesters of pregnancy
[10]. Notably, the two aforementioned studies of repro-
ductive outcomes after the 9/11 events also did not observe
any statistically significantly larger effect on birth weight,
after controlling for gestational duration, and exposure
during the first trimester as opposed to later exposure [6,7].
Without adjustment for gestational duration, one study
found larger effects for women whose first trimester
encompassed the 9/11 events (�104 g, P=.057) [6]. In
that study, there was also a statistically significant effect of
first-trimester exposure, as opposed to later exposure, on
gestational length (�3.55 days, P=.001).
The external validity of these findings is not easy to
judge. The magnitude of the carnage is unmatched, and the
events brought about immediate and sweeping changes on
the levels of politics, society, and individual psychology.
We surmise that more recent terrorist acts, like the
bombings in Bali, as well as in Madrid and London, did
not have as large an impact on levels of stress, unsafety,
and anxiety worldwide as did the 9/11 events. However,
surviving victims, relatives of affected individuals, or
people living or working close to the afflicted areas may
have experienced more serious psychological effects from
these bombings than from the attacks in New York City
and Washington, DC.
In conclusion, our data provide evidence supporting the
hypothesis that exposure of Dutch pregnant women to the
9/11 terrorist attacks via the media has had a small
unfavorable effect on mean birth weight of their offspring.
References
[1] Silver RC, Holman EA, McIntosh DN, Poulin M, Gil-Rivas V.
Nationwide longitudinal study of psychological responses to
September 11. JAMA 2002;288:1235–44.
[2] Mulder E, Robles de Medina PG, Huizink AC, Van den Berg BRH,
Buitelaar JK, Visser GHA. Prenatal maternal stress: effects on
pregnancy and the (unborn) child. Early Hum Dev 2002;70:3–14.
[3] Orr ST, James SA, Miller CA, et al. Psychosocial stressors and low
birthweight in an urban population. Am J Prev Med 1996;12:459–66.
[4] Bastiaanssen JM, De Bie RA, Bastiaenen CHG, Heuts A, Kroese
GGM, Essed GGM, Van den Brandt PA. Etiology and prognosis of
pregnancy-related pelvic girdle pain: design of a longitudinal study.
BMC Public Health 2003;5:1–8.
[5] Matsuda S, Sone T, Doi T, Kahyo H. Seasonality of mean birth weight
and mean gestational period in Japan. Hum Biol 1993;65:481–501.
[6] Lederman SA, Rauh V, Weiss L, et al. The effects of the World
Trade Center event on birth outcomes among term deliveries at
three lower Manhattan hospitals. Environ Health Perspect 2004;
112:1772–8.
[7] Berkowitz GS, Wolff MS, Janevic TM, Holzaman IR, Yehuda R,
Landrigan PJ. The World Trade Center disaster and intrauterine
growth restriction. JAMA 2003;290:595–6.
[8] Van Zelst W, De Beurs E, Smit JH. Effects of the September 11th
attacks on symptoms of PTSD on community-dwelling older persons
in the Netherlands. Int J Geriatr Psychiatry 2003;18:187–90.
[9] De Lange AW, Neeleman J. The effect of the September 11 terrorist
attacks on suicide and deliberate self harm: a time trend study. Suicide
Life Threat Behav 2004;34:439–47.
[10] Paarlberg KM, Vingerhoets AJJM, Passchier J, Dekker GA, Heinen
HP, Van Geijn HP. Psychosocial predictors of low birth weight: a
prospective study. Br J Obstet Gynaecol 1999;106:834–41.