low grade infection after shoulder surgery
TRANSCRIPT

@thearmclinic
Low Grade Infectionsfollowing
Non-Arthroplasty SurgeryOf the Shoulder
Lennard Funk Umair Khan
Emma TorranceRob TownsendSteve Davies
Tanya Mackenzie
@thearmclinic
Low Grade Infection
• Subacute or chronic infection with no fever and no pus production [Mosby’s Medical Dictionary]
• Persistent pain & stiffness resistant to usual treatments (with positive cultures in most cases) [Schneeberger et al. Chir Organi. 2009]
@thearmclinic
Background
• P acnes commonest organism identified and studied
(Saltzman et al., 2011; Achermann et al., 2014; Aubin et al., 2014; Levy et al., 2013)
• P acnes commonly found on anterolateral aspect of shoulder (Patel et al., 2009; Saltzman et al., 2011)
• P acnes also found in deep tissues of shoulder
(Hudeck et al. JSES. 2014)
• Well documented in shoulder arthroplasty (Singh et al., 2012; Richards et al., 2014; Singh et al., 2012; Cheung et al., 2008
• P acnes incidence at revision shoulder arthroscopy = 29% (vs. 3% primary) (Horneff et al. JSES. 2015)
@thearmclinic
Aims
1. Report a non-arthroplasty cases of clinically suspected low-grade infection
2. Investigate risk factors
3. Describe the cultured organisms
@thearmclinic
Inclusions
• Previous non-arthroplasty elective surgery• Constant & Night Pain and Stiffness
• > 6months • Unresponsive to rehab & injections /
distension• Imaging = repairs intact• Normal inflammatory markers
@thearmclinic
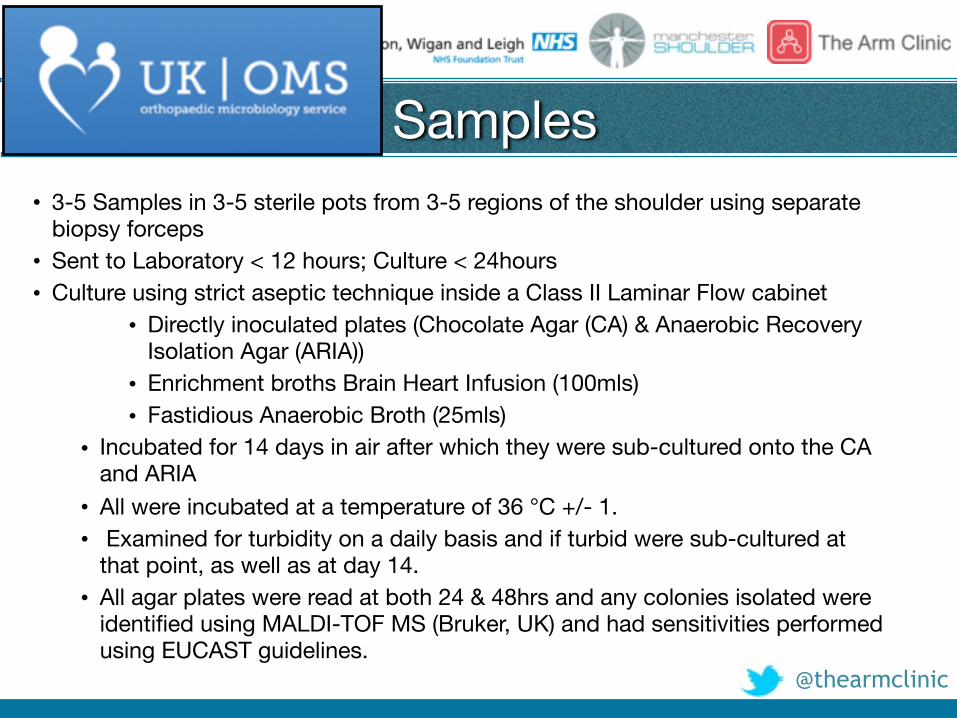
Samples• 3-5 Samples in 3-5 sterile pots from 3-5 regions of the shoulder using separate
biopsy forceps• Sent to Laboratory < 12 hours; Culture < 24hours• Culture using strict aseptic technique inside a Class II Laminar Flow cabinet
• Directly inoculated plates (Chocolate Agar (CA) & Anaerobic Recovery Isolation Agar (ARIA))
• Enrichment broths Brain Heart Infusion (100mls) • Fastidious Anaerobic Broth (25mls)
• Incubated for 14 days in air after which they were sub-cultured onto the CA and ARIA
• All were incubated at a temperature of 36 °C +/- 1. • Examined for turbidity on a daily basis and if turbid were sub-cultured at
that point, as well as at day 14. • All agar plates were read at both 24 & 48hrs and any colonies isolated were
identified using MALDI-TOF MS (Bruker, UK) and had sensitivities performed using EUCAST guidelines.
@thearmclinic
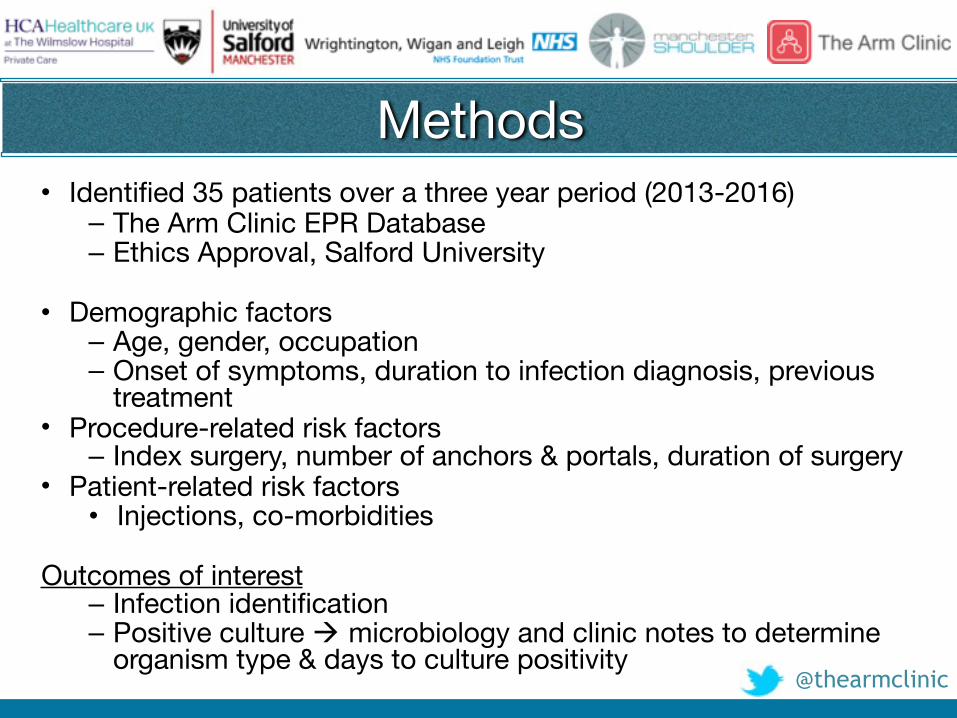
Methods• Identified 35 patients over a three year period (2013-2016)
– The Arm Clinic EPR Database– Ethics Approval, Salford University
• Demographic factors– Age, gender, occupation– Onset of symptoms, duration to infection diagnosis, previous
treatment• Procedure-related risk factors
– Index surgery, number of anchors & portals, duration of surgery• Patient-related risk factors
• Injections, co-morbidities
Outcomes of interest– Infection identification– Positive culture ! microbiology and clinic notes to determine
organism type & days to culture positivity
@thearmclinic
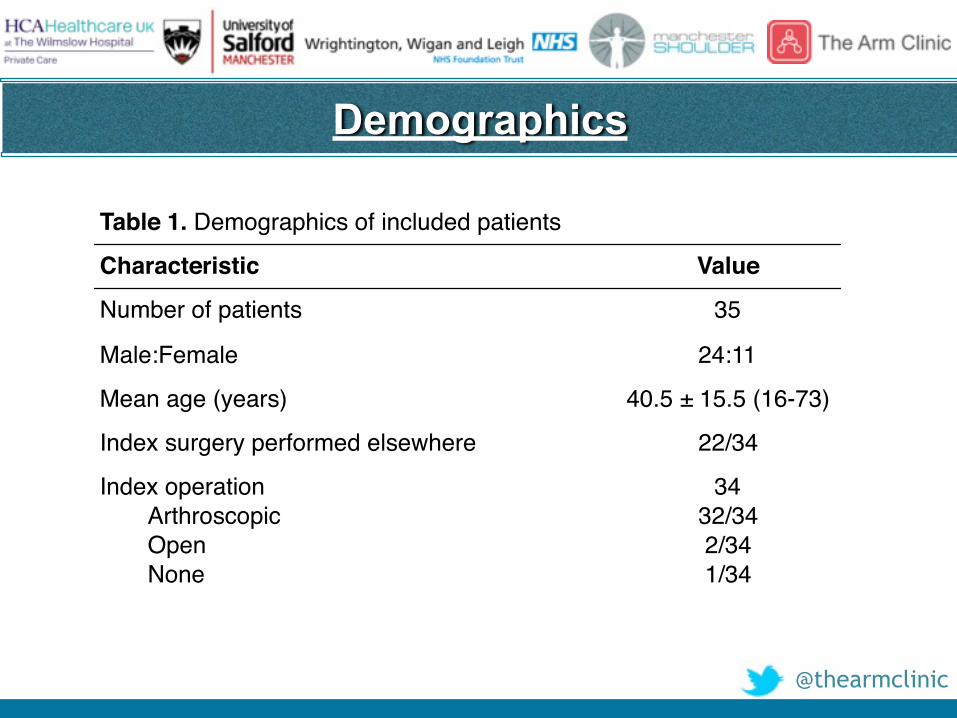
Table 1. Demographics of included patients
Characteristic Value
Number of patients 35
Male:Female 24:11
Mean age (years) 40.5 ± 15.5 (16-73)
Index surgery performed elsewhere 22/34
Index operationArthroscopicOpenNone
3432/342/341/34
Demographics
@thearmclinic
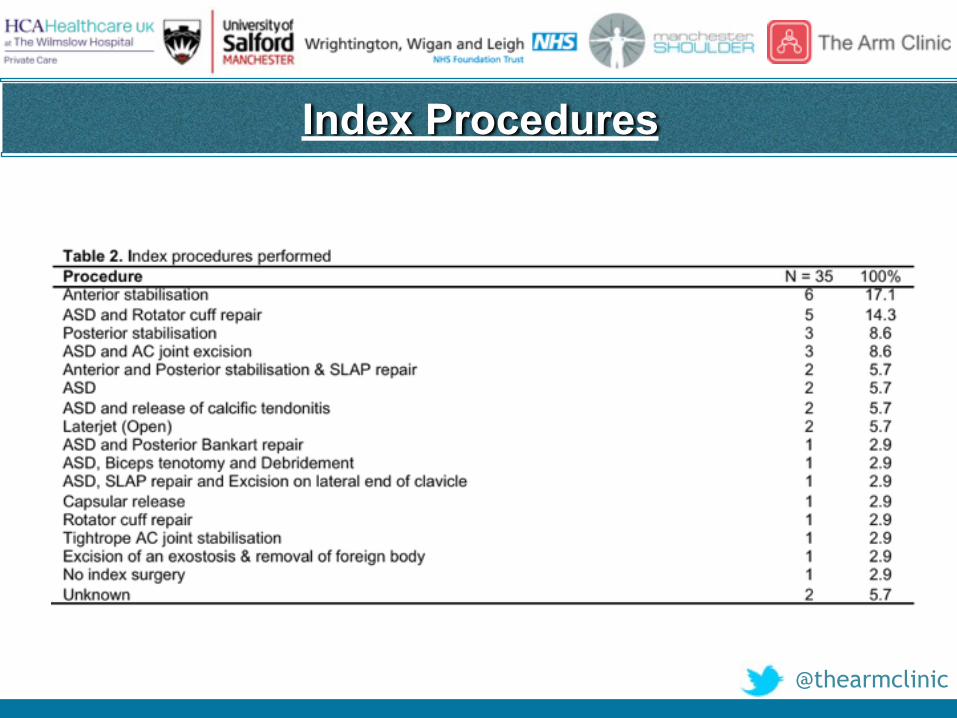
Index Procedures
@thearmclinic
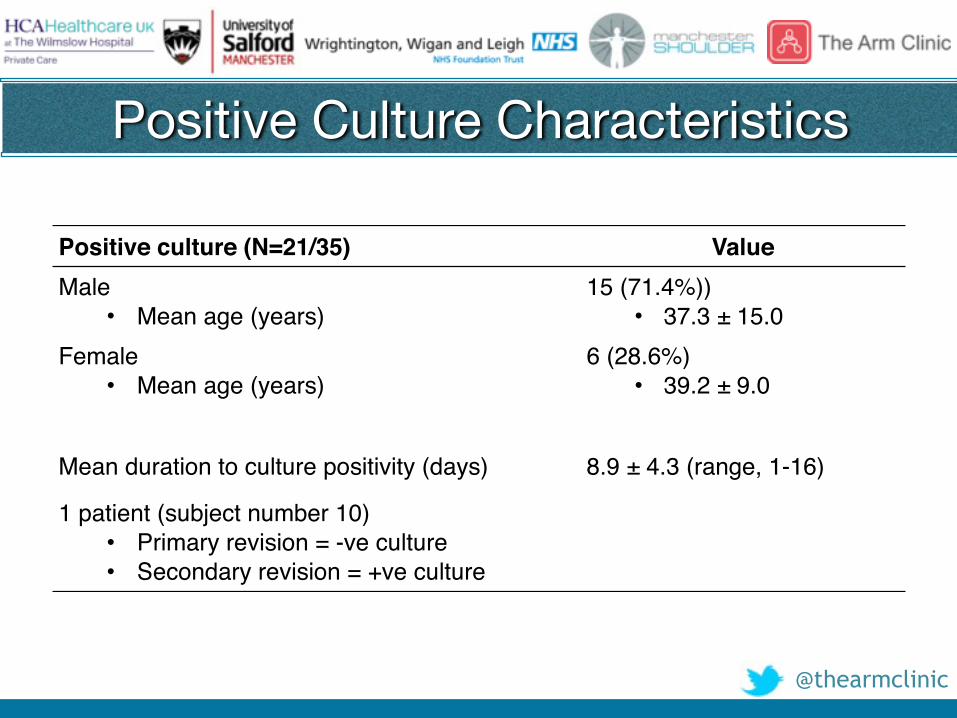
Positive Culture Characteristics
Positive culture (N=21/35) ValueMale
• Mean age (years)15 (71.4%))
• 37.3 ± 15.0Female
• Mean age (years)6 (28.6%)
• 39.2 ± 9.0
Mean duration to culture positivity (days) 8.9 ± 4.3 (range, 1-16)
1 patient (subject number 10)• Primary revision = -ve culture• Secondary revision = +ve culture
@thearmclinic
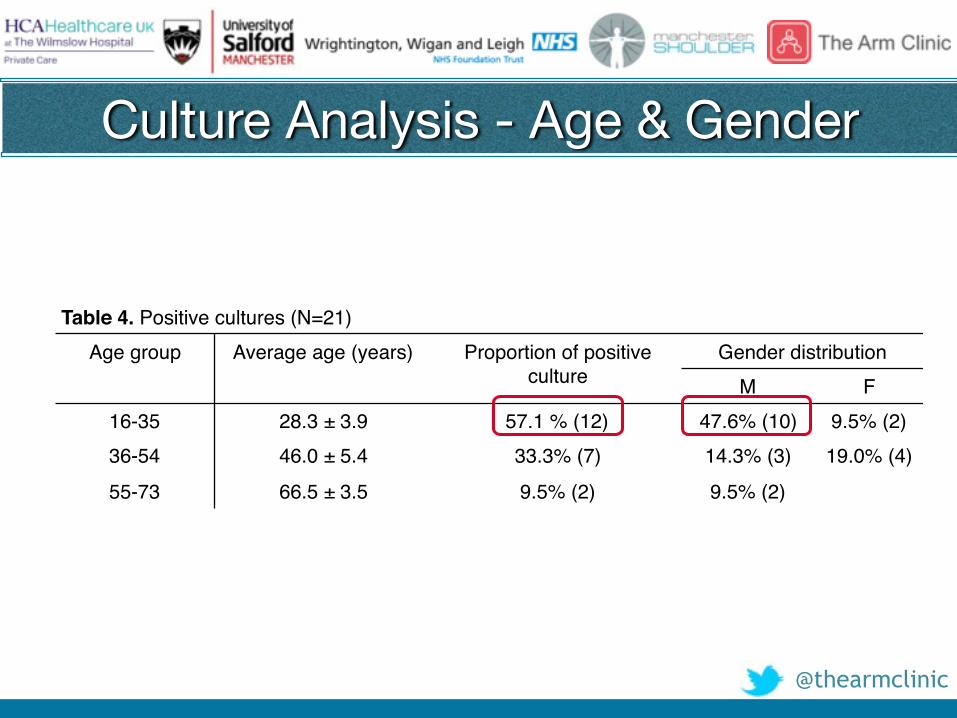
Culture Analysis - Age & Gender
Table 4. Positive cultures (N=21)Age group Average age (years) Proportion of positive
cultureGender distribution
M F16-35 28.3 ± 3.9 57.1 % (12) 47.6% (10) 9.5% (2)36-54 46.0 ± 5.4 33.3% (7) 14.3% (3) 19.0% (4)
55-73 66.5 ± 3.5 9.5% (2) 9.5% (2)
@thearmclinic
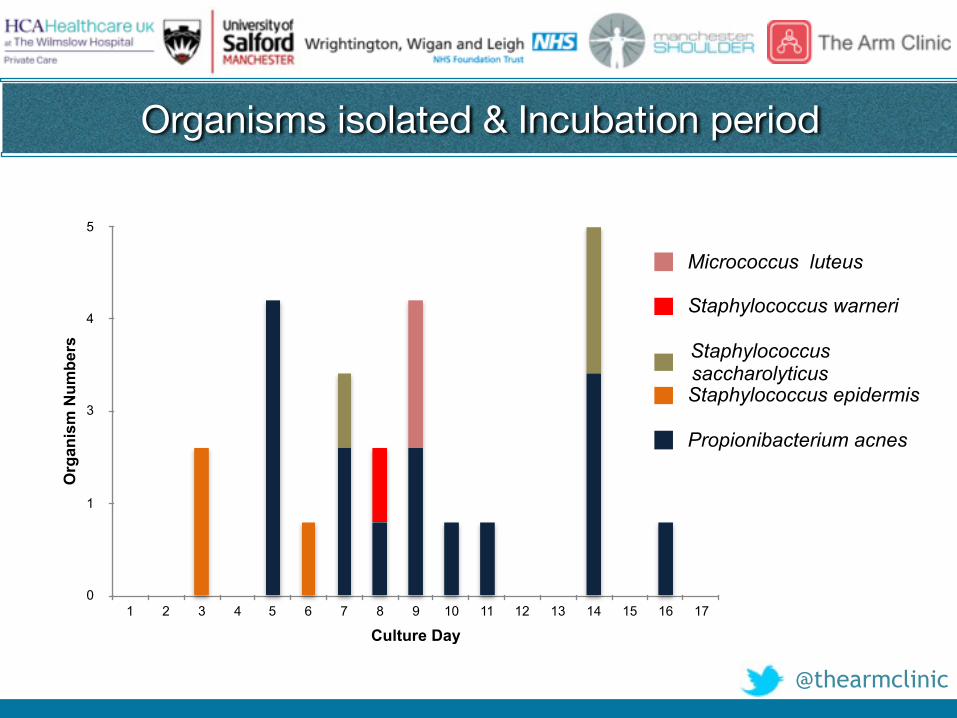
Organisms isolated & Incubation period O
rgan
ism
Num
bers
0
1
3
4
5
Culture Day1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Propionibacterium acnes
Staphylococcus epidermis
Staphylococcus saccharolyticus
Staphylococcus warneri
Micrococcus luteus
@thearmclinic
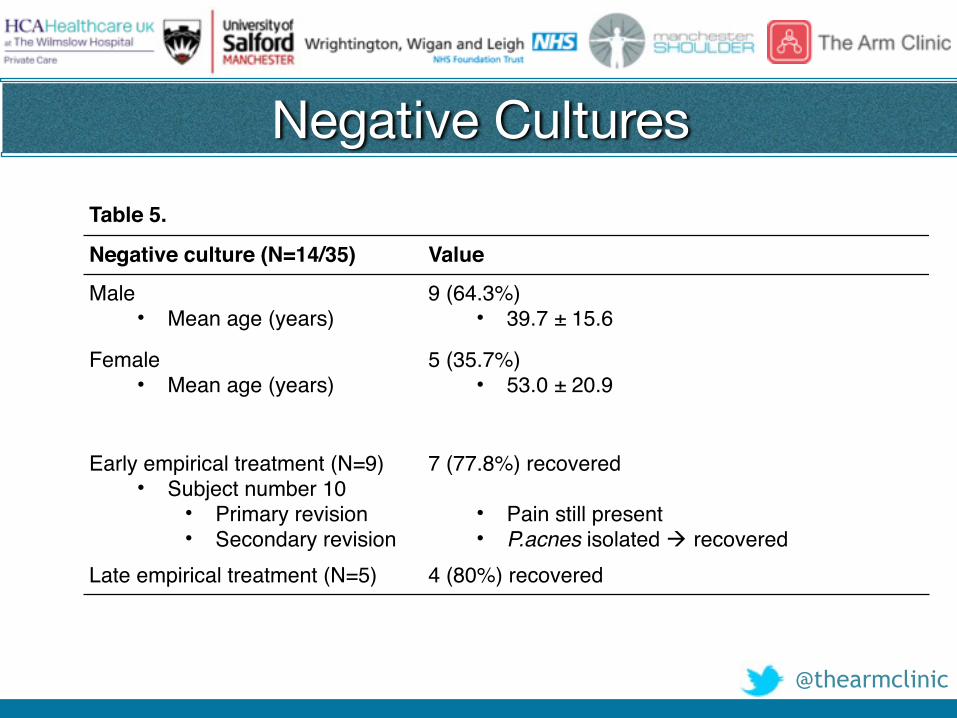
Negative CulturesTable 5.
Negative culture (N=14/35) Value
Male• Mean age (years)
9 (64.3%)• 39.7 ± 15.6
Female• Mean age (years)
5 (35.7%)• 53.0 ± 20.9
Early empirical treatment (N=9)• Subject number 10
• Primary revision• Secondary revision
7 (77.8%) recovered
• Pain still present• P.acnes isolated ! recovered
Late empirical treatment (N=5) 4 (80%) recovered
@thearmclinic
Conclusions
• Young males highest risk
• Propionibacterium acnes most common organism – 76.5% (13/17) P.acnes +ve culture
• Not all patients +ve cultures– 77.8% (7/9) pts reported improvement following early
empirical treatment– 80% (4/5): symptomatic improvement following late
empirical treatment
@thearmclinic
Clinical Relevance
• Consider Low Grade Infection in:• Post-op Frozen Shoulder not improving
with usual treatments• Younger Males
• Extended Cultures with specialised Lab.• But still difficult to detect (?)• If Negative consider Empirical Treatment
@thearmclinic
With thanks to…
1. Umair Khan, Medical Student Manchester Uni.2. Emma Torrance, Research Manager, The Arm Clinic3. Rob Townsend, Microbiologist, UKOMS4. Steve Davies, Scientific Director, UKOMS5.Tanya Mackenzie, Shoulder Therapist
@thearmclinic
References 1. Patel A, Calfee RP, Plante M, Fischer SA, Green A. Propionibacterium acnes colonization of the human shoulder.
J Shoulder Elbow Surg. 2009;18(6):897- 9022. Saltzman MD, Marecek GS, Edwards SL, Kalainov DM. Infection after shoulder surgery. J Am Acad Orthop Surg.
2011;19:208-2183. 2. Achermann Y, Goldstein EJ, Coenye T, Shirtliff ME. Propionibacterium acnes: From commensal to
opportunistic biofilm-associated implant pathogen. Clin Microbiol Rev. 2014;27:419-404. Aubin GG, Portillo ME, Trampuz A, Corvec S. Propionibacterium acnes, an emerging pathogen: From acne to
implant-infections, from phylotype to resistance. Med Mal Infect. 2014;44:241-50 5. Levy O, Iyer S, Atoun E, Peter N, Hous N, Cash D, et al. Propionibacterium acnes: An underestimated etiology in
the pathogenesis of osteoarthritis? J Shoulder Elbow Surg. 2013;22:505-11 6. Singh JA, Sperling JW, Schleck C, Harmsen WS, Cofield RH. Periprosthetic infections after total shoulder
arthroplasty: a 33-year perspective. J Shoulder Elbow Surg. 2012;21:1534–1541 7. Richards J, Inacio MC, Beckett M, Navarro RA, Singh A, Dillon MT, et al. Patient and procedure-specific risk
factors for deep infection after primary arthroplasty. Clin Orthop Relat Res. 2014;472:2809–28158. Singh JA, Sperling JW, Schleck C, Harmsen W, Cofield RH Periprosthetic infections after shoulder
hemiarthroplasty. J Shoulder Elbow Surg. 2012;21:1304–13099. Cheung EV, Sperling JW, Cofield RH. Infection associated with hematoma formation after shoulder arthroplasty.
Clin Orthop Relat Res. 2008;466:1363–1367