low back disability & waddell’s inappropriate symptoms questionnaire
DESCRIPTION
Low Back Disability & Waddell’s Inappropriate Symptoms Questionnaire . Aaron Baker, Curtis Cox, Neil Esarte, Toby Mattson, Steve Meagher. History of Low Back Disability. - PowerPoint PPT PresentationTRANSCRIPT
Low Back Disability & Waddell’s Inappropriate Symptoms
Questionnaire
Aaron Baker, Curtis Cox, Neil Esarte, Toby Mattson, Steve Meagher
History of Low Back Disability• Historically, low back pain was not considered a
disabling condition. In fact the first recorded case of compensation for a work injury was a railroad worker related to the beginning of the industrial revolution.
• By 1920, the problem of low back disability began to increase significantly.
• In the last 45 years an interesting change has occurred regarding our social attitudes towards pain. It has shifted from being a symptom and warning sign of disease, to a disease in itself that demands a treatment and a cure.
Prevalence• 60-80% of people will have LBP sometime in their
lives. • 30% are referred to Ortho; 3% admitted; 0.5%
operated. • 90% LBP resolves in 6 weeks, 75% may experience
symptoms & disability one year after initial consultation.
• The prevalence of LBP has changed little over the years, but the associated disability has increased four fold.
• In the US certified incapacity for LBP was 120 million days in 2004.
• 14 million consultations annually. Overall cost of LBP was approximately 10 billion dollars.
Why Take it Seriously?• Acute low back pain is often recurrent.• Predisposes to chronic pain and disability. • A warning of potential future trouble.• Impacts on the quality of life.• Lost days of productivity.• Huge cost of incapacity payouts.• Enormous burden on healthcare costs when
chronic.
Types of Back Pain• Discogenic Back Pain
– Annulus fibrosus when it is stretched with a bulging disc.
– Outer 1/3 has sensory innervations. – Radial fissuring is associated with painful
discs.
• Radicular back pain – pain extending to the buttock and/or leg – disc herniation , spinal stenosis or intraspinal
pathology
Types of Back Pain Con’t
• Iatrogenic back pain – Dural adhesions. – Post surgical scarring.
• Psychogenic back pain – Must exclude organic pathology. – Waddell's inappropriate signs often present.

Related Terms• Pain- an unpleasant sensory and emotional
experience associated with actual or potential tissue damage, or described in terms of such damage.
• Chronic pain- long standing intractable pain of longer than 6 month duration.
• Chronic pain syndrome- pain which lasts longer than 3 months without underlying cause and interferes with major life activities such as work.
Related Terms Con’t• Symptom Magnification Syndrome- a conscious
or unconscious, self-destructive, socially reinforced behavioral response pattern consistent of reports or displays of symptoms which function to control the life circumstances of the sufferer (other similar terms are malingering, Abnormal Illness Behavior, symptom exaggeration).
• Medical impairment- physically measurable restriction determined by diagnostic measures.
• Functional impairment- movement dysfunction with respect to ROM, quality of motion, velocity of motion, consistency of movement pattern, strength, behavior, verbalization of pain and disability, and distraction of evaluation.
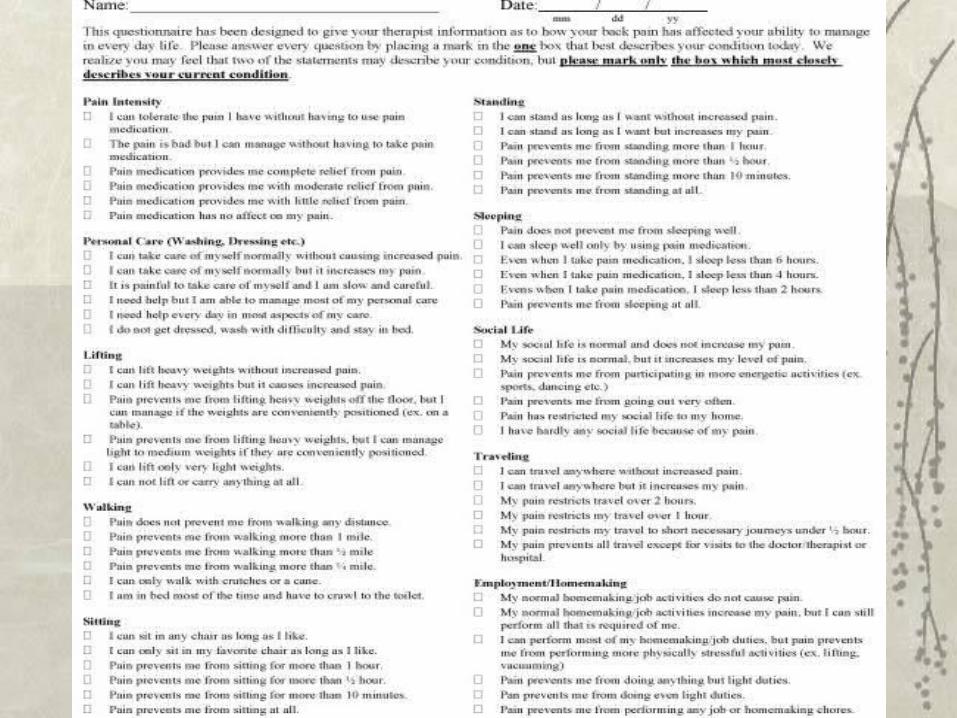
Oswestry Low Back Disability Questionnaire
• An extremely important tool that researchers and disability evaluators use to measure a patient's permanent functional disability.
• The test has been around for 25 years and is considered the "gold standard" of low back functional outcome tools.
Purpose
• 10 item, self report checklist. • Has been shown to be valid in assessing
perceived disability.• Easy to complete for the client and easy for the
evaluator to score.
Administration
• Provide client with the standard 10-item checklist.
• Have them answer the questions by choosing the 'best answer' that describes their 'typical' pain and/or limitations within the last week or two.
• They can only choose ONE answer. • If their limitations fall in-between two questions,
pick the higher point value question.
Scoring
• Each section is scored from 0 to 5 points depending on which statement they check.
• If a section is not checked, potential score is dropped by 5.
• First statement in each sections score is 0.• Second scores 1, third scores 2, etc.• Scores for all answered sections are added
together and divided by the total potential score, then multiplied by 100 to obtain a percentage.
Interpretation
• Minimal Disability (0-20%)– The patient can cope with most living
activities. – Usually no treatment is indicated apart from
advice on lifting, sitting and exercise. – Ex: a secretary or truck driver.
Interpretation Con’t
• Moderate Disability (20-40%)– The patient experiences more pain and
difficulty with sitting, lifting and standing. – Travel and social life are more difficult and
they may be disabled from work. – Personal care, sexual activity and sleeping
are not grossly affected and the patient can usually be managed by conservative means.
Interpretation Con’t
• Severe Disability (40-60%)– Pain remains the main problem in this group
but activities of daily living are affected. – These patients require a detailed
investigation.
Interpretation Con’t
• Crippled (60-80%)– Back pain impinges on all aspects of the
patient's life. – Positive intervention is required.
• Extreme Cases (80-100%)– Either bed-bound or exaggerating symptoms.

Interpretation Con’t
• Simply add up your points for each section and plug it in to the following formula in order to calculate your level of disability: Point total / 50 X 100 = % Disability
Clinical Applications
• Workplace Safety and Insurance Board (WSIB)
• Ergonomics assessment for insurance companies
Waddell’s Inappropriate Symptoms Questionnaire
• In 1980 Dr. Waddell and his colleagues wanted to distinguish and standardize "non-organic" physical signs that sometimes accompany low back pain.
• Pain descriptions usually approximate anatomical and pathological patterns of disease, however, sometimes these descriptions do not follow general clinical experience.
• Inappropriate symptoms are usually attributed to psychological features and are vague, not well localized and lack the normal relationships to time, activity and anatomy.
Purpose
• This is a test to determine whether the clients symptoms are appropriate or inappropriate with respect to low back pain.
• Should be noted that these symptoms may in fact occur in other pathologies such as hip pathology and therefore, the pathology should be confirmed as emanating from the low back before utilizing the test.
Administration
• Provide the client with the questionnaire asking 5 simple questions requiring either a “yes” or a “no” answer.
• There are two additional questions which may be utilized, they are gathered in the routine history which doesn’t appear on the patients questionnaire.
• A “yes” answer to either of these additional questions constitutes an inappropriate response.
Instructions
• Answer the 5 questions by circling either “Yes” or “No” to each question.– 1. Do you get pain at the tip of your tail bone?– 2. Does your whole leg ever become painful?– 3. Does your whole leg ever go numb?– 4. Does your whole leg ever give way?– 5. In the past year, have you had any spells
with very little pain?
Instructions Con’t
• Additional questions:– 6. Do you have an intolerance of or reactions
to treatment?– 7. Have you ever had emergency admission
to hospital with low back pain?– These are the added questions that can be
utilized in the routine history and they do not appear on the clients questionnaire.
Scoring
• A “yes” answer to questions 1 to 4 are inappropriate.
• A “no” answer to question 5 is inappropriate.• A total of 2 or more inappropriate scores is
indicative of inappropriate illness behavior.• Most symptom magnifiers usually score more
than 2 inappropriate answers in the first 5 questions and it is therefore unnecessary to score questions 6 and 7.
Clinical Applications
• Ergonomics assessment for insurance companies.
• Workers Compensations claims.• WSIB
Placebo Tests• Waddell’s Light Pinch
– Non-anatomical tenderness to light pinch.• Waddell’s Axial Vertical Loading
– Vertical loading on a standing patients skull produces low back pain.
• Waddell’s Simulated Rotation– Passive rotation of shoulders and pelvis in the same
plane causes low back pain.• Distraction
– Discrepancy between findings on sitting and supine straight leg raising tests.
• Overreaction– Disproportionate facial expression, verbalization or
tremor during examination.