living with covid-19 operational unit mobilisation plan
TRANSCRIPT

1
Living with Covid-19
Operational Unit Mobilisation Plan and Timeline
1. Introduction & Background
On 17 March 2020 the Cabinet Secretary for Health and Sport placed NHS Scotland in emergency footing for a three month period under Section 1 and Section 78 of the National Health Service Scotland Act 1978 as a consequence of substantial and sustained transmission of Covid-19.
Within the NHS, non-urgent elective operations and routine care was suspended however a commitment was made that vital cancer treatment, emergency care, maternity services and urgent medical procedures would continue as usual. The Cabinet Secretary committed that patients whose operations were cancelled, would stay on a waiting list until it is “clinically appropriate” for scheduled operations to commence again.
It is recognised that Covid-19 will be endemic in society to varying levels for a significant period of time. It is anticipated that normal society will not return and levels of social distancing and lockdown measures will prevail for the foreseeable future. For health care systems the constraints of physical distancing, enhanced cleaning, PPE use, shielding staff and patients all have an impact on the ability to deliver the levels of activity prior to the coronavirus pandemic.
The challenge is how NHS Tayside continues to deliver emergency, urgent and cancer care whilst maintaining Covid-19 capacity, and safely and incrementally restoring routine and elective services that have been paused due to Covid-19. A very important element to delivering services is the retention of the good practice and innovation that has emerged.
This paper sets out NHS Tayside’s approach and mobilisation plan for firstly, the immediate period to the end of July and secondly the next phase of sustaining semi-routine activity in the community and re-introducing routine elective activity. The paper sets out a phased and structured approach that will deliver safe, clinically prioritised and risk-assessed patient pathways of care within the constraints of ‘Living with Covid’. It provides an initial timeline/roadmap aligned to a planning methodology and framework that will support sustainable change and innovation.
The operational unit plan is supported by the three Health and Social Care Partnerships (HSCPs) including Primary and Community Care, Scottish Ambulance Service and the other key stakeholders in recognition that a whole system approach is required.

2
2. Roadmap
The roadmap outlined below provides the key milestones for the next phase of our mobilisation plan.
Approach
The approach is that any changes being proposed are safe for patients and staff, clinically prioritised and risk assessed. Underpinned by staff governance and partnership working.
Underpinning our approach are the following principles:
Plans will be developed in line with local HSCP, regional and national strategic plans
Plans will be developed in partnership with our staff
Patients will only attend hospital if there is no other alternative
Plans will maximise the use of available resources to deliver clinically prioritised care to as much of the population as possible
Plans will be developed in partnership with our primary care and health and social care partners
Plans will align with principles of realistic medicine

3
a) Understanding the impact and constraints of Covid-19 on service delivery models
As a first step in re-mobilising, speciality level templates detail the individual clinical team plans and requirements to support a phased approach to reinstatement of routine elective outpatient, diagnostic and inpatient / day case pathways.
All service plans are based on the following factors:
Optimising capacity for remote care delivery
Need to separate patient pathways into low, indeterminate and high risk
PPE requirements
Sustainable workforce availability
Need to have a scalable and sustainable plan for further potential surges in Covid-19 cases and peaks of admission
Pathway development and innovation
Desire to retain novel ways of working that benefit long term transformation goals
b) Clinical Prioritisation Framework
NHS Tayside is a clinically led, managerially facilitated organisation, and clinical prioritisation has been at the heart of our Covid-19 response. New pathways which prioritise remote working and use of new technologies will be clinically led, with clinical prioritisation embedded throughout. NHS Tayside will follow and aim to exceed national guidelines in this area, with local and regional priority groups optimising clinical capacities.
c) Demand and Capacity Modelling Framework – Predicting Future Performance
The Health & Business Intelligence and Quality Improvement Leads are developing a scenario planning methodology that can be used by individual specialities to develop a revised Demand, Capacity, Activity and Queue plan (DCAQ) for the phases of re-instatement of outpatient and inpatient activity based on the new Living with Covid-19 service delivery models.
DCAQ methods will be tested and worked through with first three specialties by 12 June with a rolling programme of three specialties per week. Therefore, the first three specialties will be modelled by 11 August in line with the lockdown phasing. The programme will continue thereafter with all remaining specialities.
Modelling will be completed for all specialities for both outpatient and inpatient / day case demand, supporting an overarching NHS Tayside performance position for 2020/21 based on scenarios of anticipated referral rates in the coming months as we move out of the lockdown period.
The modelling toolkit can then be used on a sustainable basis by capacity managers and Clinical Care Group teams as part of business as usual service planning and management.

4
d) Outcome Measures
There is an existing set of national measures however, in light of the current situation, consideration needs to be given to developing and agreeing a range of high level engagement, improvement, quality and performance measures that reflect the new service delivery models.
e) Partnership Working
Through NHS Tayside current Command and Control Structure staffside continue to be engaged with and provide support to many groups who have contributed to the plans. Staffside colleagues are members of bronze, silver and gold commands.
There is a continued commitment to work together with staffside colleagues as we work through this next phase to ensure that staff feel involved, valued, supported and safe through any sustained/ongoing changes.
3. Planning for the next Phase – Maintaining Business Critical Services and Covid-19 Capacity
3.1 Acute Hospital Configuration - appendix 1.
There is strong clinical opinion based on evidence from other health care systems that it is necessary to maintain separate patient pathways depending on Covid-19 status to mitigate the risks for patients. NHS Tayside remodelled its acute hospital estate to create a ‘hospital within a hospital’ to provide capacity for additional Covid-19 HDU and ITU, Covid-19 assessment unit and Covid-19 inpatient ward capacity while continuing non Covid-19 emergency, urgent and cancer care.
It is not possible to return to the same pre Covid-19 inpatient model as the service will need to retain the ability to respond due to the requirement to a possible upsurge in Covid-19. As there is uncertainty regarding the progression of Covid-19, we aim to plan our resources with this in mind and establish planned care in a safe manner across our acute hospitals.
To safely and sustainably deliver the priority 1 urgent and cancer surgical procedures the acute hospital has been divided into three zones supporting three separate patient pathways. The aim of these pathways is to minimise the risk of cross infection between patients and staff.
This approach will be different from traditional hospital layouts. Patient care will not be organised into surgical specialities as before, patients will be aligned to care pathways that reflect Covid pre-test probability and risk stratification for both scheduled and unscheduled care.
5
The three pathways are:
Known Covid-19 +ve or displaying symptoms
Covid-19 POSITIVE
Indeterminate Covid-19 / no Pre-Surgery Isolation (PSI)
Indeterminate (Planned or unplanned admissions where patient has not undertaken PSI) (Yellow).
Patients admitted via unscheduled/emergency pathways and who are non-symptomatic and COVID-19 negative
Pre-Surgery Isolation Patient Elective Surgical Pathway
Perioperative Surgical Isolation (Green)
The new ‘Green Zone’ has been set up in Ninewells to protect vulnerable patients coming to hospital for their planned urgent surgery.
The Green Zone consists of wards and surgical theatres and ensures patients are kept apart from the areas in the hospital caring for Covid-19 patients.
All three pathways will be processed through Ninewells Hospital. Only two of the pathways (Yellow and Green) will be processed through Perth Royal Infirmary.
3.2 Covid-19 Adult Pathway
Our plans are based on converting unplanned attendance or assessment to one that is planned and delivered in the community where possible.
Community Assessment Hubs (CAH):
Reducing Covid-19 activity, but with the likelihood of further peaks in Covid-19 cases leads us to a position of maintaining the telephone triage hub and contracting the face-to-face assessment hubs. A CAH will be maintained in Dundee and Perth. Angus is working up a plan which will see Covid-19 cases being returned to the local clusters but maintaining one Covid-19 hub until practices are organised to do this. The rationale behind continuing to run the Covid-19 hubs is not only to comply with Scottish guidance but also to afford practices across Tayside time to adapt their own surgeries and ways of working in clusters to be able to look after Covid-19 patients in their own areas in the very foreseeable future – 3-6 months.
The number of doctors required on the face-to-face shifts is reducing and therefore the facilities required are being relocated to a smaller footprint to release space for more routine activities.
A revised service delivery model will be progressed and included in phase two of the plans. Collaborative discussions with Perth & Kinross Health and Social Care Partnership regarding CAH will enable release of acute hospital footprint at PRI. This future potential may enable potential re-establishment of intermediate and/or minor surgery on the PRI site as part of future phases of Board mobilisation planning.
6
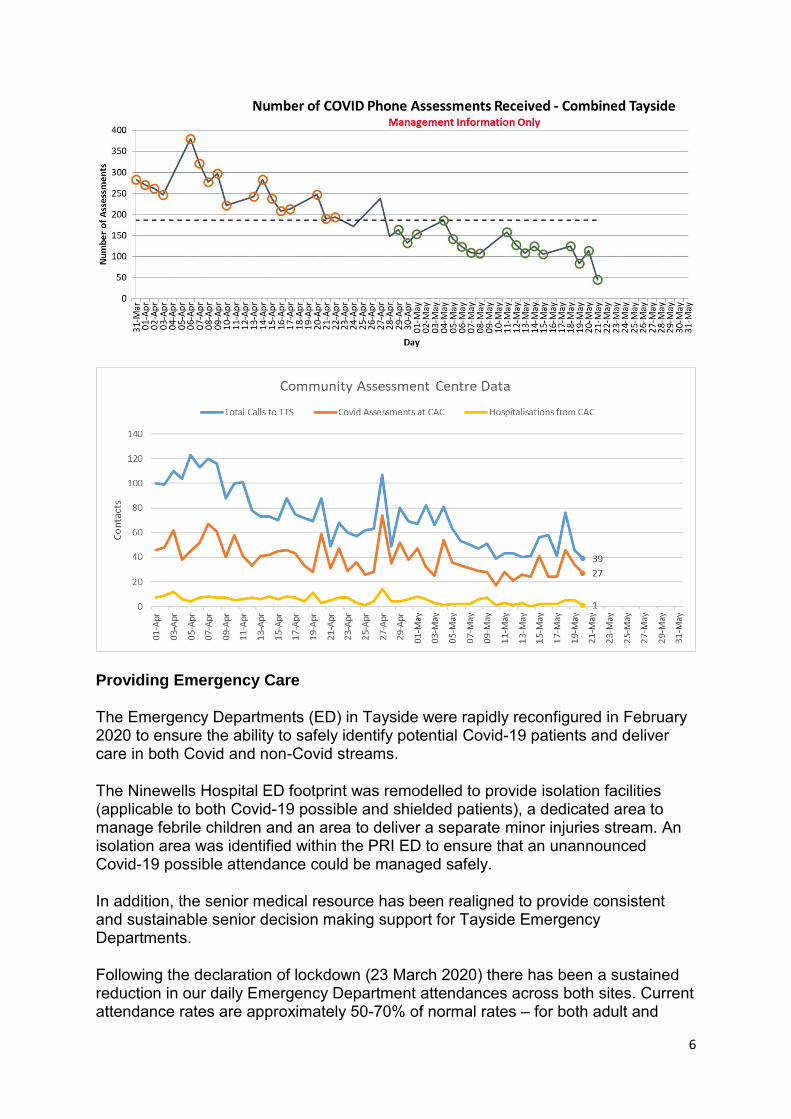
Providing Emergency Care
The Emergency Departments (ED) in Tayside were rapidly reconfigured in February 2020 to ensure the ability to safely identify potential Covid-19 patients and deliver care in both Covid and non-Covid streams.
The Ninewells Hospital ED footprint was remodelled to provide isolation facilities (applicable to both Covid-19 possible and shielded patients), a dedicated area to manage febrile children and an area to deliver a separate minor injuries stream. An isolation area was identified within the PRI ED to ensure that an unannounced Covid-19 possible attendance could be managed safely.
In addition, the senior medical resource has been realigned to provide consistent and sustainable senior decision making support for Tayside Emergency Departments.
Following the declaration of lockdown (23 March 2020) there has been a sustained reduction in our daily Emergency Department attendances across both sites. Current attendance rates are approximately 50-70% of normal rates – for both adult and

7
paediatric populations. This is in line with attendance rates for other Emergency Departments in Scotland.
NHS Tayside has ensured appropriate pathways are in place for patients attending our Emergency Departments. Throughout this period, NHS Tayside has continued to maintain our performance in respect of the four hour wait standard and maintenance of this level of performance will remain a key priority.
The maintenance of performance during the immediate period of lockdown has been underpinned by existing pathways and practice with the NHS Tayside Emergency Departments which ensure effective unscheduled care flow. These include:
Early and mandated senior decision maker involvement for identified presentations
Consistent applications of the NHS Tayside Redirection Guidance to ensure people are directed towards the most appropriate care location
Consultant Connect professional-to-professional telephone support contributing to clinical safety at the PRI Emergency Department and promoting Right Person, Right Place, Right Time interactions with regional ambulance crews and GPs.
Whilst ED presentations have been low during the initial ‘lockdown’ phase of social distancing, there is a reasonable expectation that these will increase as lockdown measures are relaxed over the coming weeks. Further actions will be required to maintain safe and effective clinical care and performance against national standards. These are to be achieved while recognising the limitations of social distancing requirements, increased process and time required for staff to deploy effective PPE.
Actions already undertaken to address this include:
Installation of negative pressure capability in the Ninewells ED isolation corridor to increase safety and also efficiency in decreasing required ‘downtime’ between clinical use
8
Further rationalisation of Senior Doctor Rota with potential inclusion of a remote consultation shift
Clinical survey of the Emergency Departments with recommendations to enable social distancing measures including:
o additional signage, including flooring o modification of waiting room seating o use of alternative exit routes to enable an effective one-way system
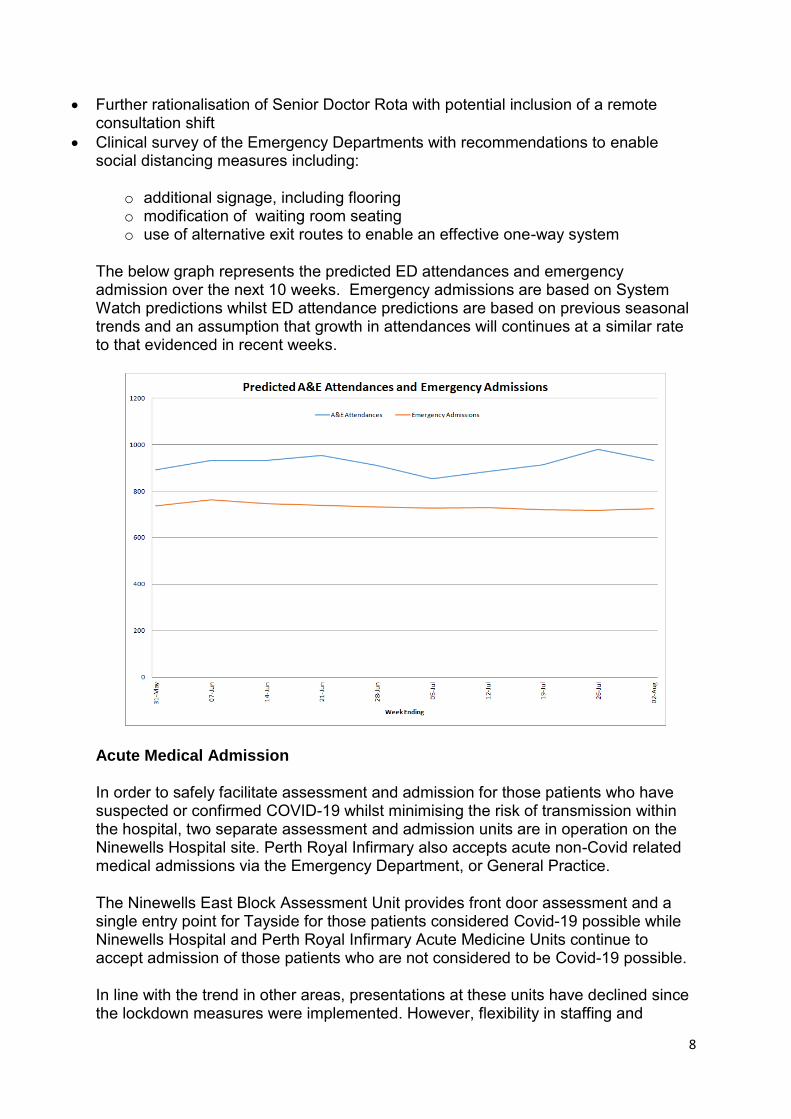
The below graph represents the predicted ED attendances and emergency admission over the next 10 weeks. Emergency admissions are based on System Watch predictions whilst ED attendance predictions are based on previous seasonal trends and an assumption that growth in attendances will continues at a similar rate to that evidenced in recent weeks.
Acute Medical Admission
In order to safely facilitate assessment and admission for those patients who have suspected or confirmed COVID-19 whilst minimising the risk of transmission within the hospital, two separate assessment and admission units are in operation on the Ninewells Hospital site. Perth Royal Infirmary also accepts acute non-Covid related medical admissions via the Emergency Department, or General Practice.
The Ninewells East Block Assessment Unit provides front door assessment and a single entry point for Tayside for those patients considered Covid-19 possible while Ninewells Hospital and Perth Royal Infirmary Acute Medicine Units continue to accept admission of those patients who are not considered to be Covid-19 possible.
In line with the trend in other areas, presentations at these units have declined since the lockdown measures were implemented. However, flexibility in staffing and

9
accommodation is required to enable a rapid response to the anticipated future increase in demand as restrictions are lifted.
In contrast, the activity through the non Covid-19 acute medical admission unit is expected to increase to pre Covid-19 levels. The clinical teams are actively reviewing pathways of care to maintain flow, prevent corridor waits and optimise physical distancing within the existing footprint. With the introduction of over 70s age group Covid-19 testing in non Covid-19 services, there is a potential impact on safe patient placement and flow.
Acute Surgical Receiving Unit (ASRU)
The ASRU now receives all non Covid-19 unscheduled surgical and orthopaedic care referrals to provide a single point of entry for these specialist services.
Considering the impact of Covid-19 infection in addition to a surgical presentation, all patients are tested for Covid-19 on admission to support safe patient placement, mitigating risk of infection spread.
Covid-19 positive and Covid possible admission and assessment
The East Block Assessment Unit provides front door assessment and admission for Covid-19 positive or possible patients in Tayside. Senior medical staff are present 24 hours a day to ensure appropriate clinical decision making. Patients are admitted into isolation rooms pending confirmation of their Covid-19 status and movement to a downstream ward.
The above pathways will be maintained for the duration of the Covid-19 response.
The NHS Tayside Adult Pathway outlines an incremental and dynamic response in ward purpose to address demand for either Covid-19 positive or non-Covid inpatient bed capacity. As has been the case in recent weeks, it will be necessary to ensure that clinical and leadership teams can respond quickly to ensure that capacity is available, on demand.
Pre Hospital Triage
Whilst a general downward trend in attendances has been noted across emergency and urgent care in both Covid-19 and non-Covid streams, it is possible to evidence that proactive out of hospital triage has resulted in ensuring that only those patients requiring medical care and treatment are directed to hospital.
The Emergency Department, Covid-19 Assessment Unit and the Acute Medical Unit in Ninewells provide 24 hour senior medical advice to the Scottish Ambulance Service, General Practice (in and out-of-hours) and other medical specialties. Data demonstrates in April 2020, there were 2206 calls placed to the Emergency Department, Acute Medicine and the Covid-19 Assessment Unit. Comprehensive clinical assessment and advice resulted in 48% of these patients being managed out with hospital.

10
Building on this success, and in an effort to continue to manage patients in the most appropriate setting, the Medicine Division intend to enhance access to specialty clinical advice by the further roll out of Consultant Connect and the evaluation of the impact of this.
NHS24 and Integrated Care
As described above, work has commenced to develop integrated models of care and new pathways in partnership with Primary Care, Out-Of-Hours Services and Paediatric services.
There is also agreement with NHS24 to commence a trial of a ‘Virtual Waiting Room’ to enable remote emergency medicine senior clinical decision maker consultations and decrease need for ED attendance to further manage unscheduled attendances and minimise unnecessary attendances at hospital.
3.3 Women’s Pathways
Maternity care has been adapted following the Royal College of Midwives and Royal College of Obstetrics and Gynaecologists guidance with antenatal and postnatal care appointments through telehealth and face-to-face where required.
The intrapartum service was centralised to Ninewells Hospital with provision for a Covid-19 positive labour suite and ward created in another area. This will require to be maintained for the foreseeable future. Intermediate step up plans are in place to focus on reinstating the home birth provision from 1 June 2020 with Community Midwifery Unit provision for labour and birth to be agreed.
Infant feeding support and antenatal education will continue to be provided virtually following positive feedback. Home blood pressure monitoring is also currently being rolled out.
There has been a necessary pause in the implementation of The Best Start; A Five Year Forward Plan of Care for Maternity and Neonatal Services. This is planned to resume at the end of July with the project staff returning to post.
NHS Tayside planned Badger net implementation was paused and is planned to resume in June 2020.
Visiting will continue to be restricted with no current plans to reinstate partners staying overnight and /or visitors in the inpatient areas.
Positive aspects of Covid-19 response aim to be maintained, such as outpatient induction and labour and the use of Near Me.
Gynaecology
Early pregnancy assessment pathway for Covid-19 and non Covid-19 women and the use of virtual appointments will continue.

11
Termination of pregnancy (TOP) services, in line with Scottish Government direction, and the Early Medical Abortion at Home was extended to include those women up to 11+6 weeks gestation will continue. In addition the gestation for mid trimester TOPs has been increased up to 23+6 weeks. There is no current plan to change either adaption in the intermediate term.
All planned surgery apart from P1 procedures was paused following the directive received from Scottish Government.
Plans for post-menopausal bleeding include adapting the current pathway to enable a one stop service. Community nurse led clinics are being planned and for pessary patients.
All out patient referrals will have a telephone vetting process prior to being offered an appointment.
Assisted Conception Unit
The Scottish Government has an expectation that infertility services will be restarted as soon as possible (by end of May 2020), as per letter to NHS Board Chief Executives.
The anticipated plan for mobilisation is as follows:
May 18 Submit HFEA application for restart approval
Identify priority patients
Once restart approval from HFEA received
May 25 onwards Post natural cycle and HRT frozen embryo transfer (FET) packs
Contact DI patients
AMH screening
June 1 onwards Natural cycle FET Natural cycle FET attend for scan monitoring
Unstimulated DI attend for scan monitoring
June 6 onwards Natural cycle FET / unstimulated DI treatment start: max 4 per day
June 15 onwards HRT-FET baseline scans
June 29 onwards HRT-FET action scans
July 6 onwards Natural cycle FET cycles complete
HRT- FET start
IVF/ICSI baseline
July 13 onwards Egg collection start
12
Initially six frozen embryo transfers will be undertaken per day, taking into account all of the additional precautions required. It is estimated it will be 6-8 weeks before introduction of fresh cycles. We can safely provide 30 frozen transfers per week when the unit reopens.
3.4 Children’s Pathways
School Nursing Services / Looked After Children and Young People Nursing Services / Health Visiting
The immediate focus for the services remains on safeguarding children and those with high vulnerability. Plans will progress in line with the Scottish Government Covid-19 framework for decision making and route map.
Allied Health Profession Services
The Allied Health Profession Advice Line was established to provide families with the opportunity to speak directly to a Speech and Language Therapist, Occupational Therapist or Physiotherapist directly. Tele-health and virtual consultations will continue.
Childhood Immunisation service
Childhood immunisation services will continue to prioritise delivery of all pre-school immunisation programmes. The re-commencement of school aged immunisation programmes will be considered and agreed nationally, and associated recommendations will be implemented by the NHS Tayside Immunisation Steering Group (TISG). The impact of pausing existing School Aged Immunisation Programmes, and of not commencing the HPV programme will also be reviewed and acted on in due course via the Children’s Vaccine Group (CVG) and subsequently report into the TISG.
Additional community clinic sessions for the small number of children who were not vaccinated due to the school closures will be delivered to support completion of the annual Td/IPV, MenACWY and MMR campaign.
Paediatric Complex Disability Service
Glenlaw House and the Armitstead Child Development Centre closed at the end of March. However support for families was maintained through telephone advice. Glenlaw House will now re-commence to provide overnight and/or day respite as an early step in the service recovery plan.
Neonatal Services
Pathways to manage newborn infants who have potentially or proven Covid-19 positive mothers have been implemented and will remain in place. Such pathways will be transferred when the service moves from its current location to a newly refurbished unit.

13
Paediatric Inpatient Services
Plans are being progressed to establish how planned care can be recommenced safely given the ward configuration. Plans are progressing with Primary Care and ED around new ways of working.
The diagram below will remain in place as the interim service model to manage the risks of Covid-19.
Ward 29 a whole hospital in one ward
*Covid positive
**Infectious presentations (resp/fever), swab negative Covid unlikely, can be cohorted
Non infectious presentation swab negative
Non infectious presentation swab awaited
* shielded
*Other communicable disease eg E Coli, varicella, pertussis, measles, gastro
PAU
Ward 29
HDU
elective
emergency
* patients require a side room at all times
** require a side room until swab result known (currently may be 6pm until 2pm next day)
4. Elective Care
a. Outpatient Services
NHS Tayside has seen a c60% reduction in outpatient referrals to acute specialities since the lockdown was introduced. NHS Tayside has prioritised the delivery of new and return outpatient appointments for clinically urgent and cancer patients, and where possible has embraced digital means to support remote consultations as outlined in the table below. This reflects c1000 new and c3000 return (including nurse-led) digital outpatient appointments per week since 23 March.

14
Chart 1. Remote Consultations up to 17th May (Acute, Mental Health, GP and Community)
Our mobilisation plan will maintain our outpatient activity at the current level over the next six weeks and, based on clinical prioritisation, we anticipate an incremental increase in the volumes delivered per week.
To support clinically necessary face-to-face consultations, NHS Tayside has implemented a test of change for outpatient appointments at Ninewells which involves screening for Covid-19 symptoms using a thermal scanner and a web-based app. The purpose of this test is to protect patients, our staff and the public from the transmission of Covid-19. Evaluation is currently under way of this approach.
Please see appendix 2 for a breakdown of activity since 22 March by speciality.

15
The below graph represents the predicted outpatient activity over the next 10 weeks, with incremental growth predicted week-on-week.
b. Diagnostics
Endoscopy
NHS Tayside’s endoscopy activity reflects a c82% reduction in outpatient activity due to Covid-19. Service delivery has recommenced 4 May at c42 procedures per week for patients with an urgent suspicion of cancer. Enhanced vetting and triage is in place, using remote consultation and advice where appropriate.

16
Endoscopy capacity will remain limited due to time inefficiencies resulting from PPE and decontamination between patients. It is anticipated that the weekly activity levels will remain around c60 procedures per week (excluding cystoscopy) through to the end of July. In addition, urgent and urgent suspicion of cancer cystoscopies are being delivered, approximately 20 per week.
17
Colon Capsule Endoscopy (CCE)
An efficient endoscopy service is vital to the diagnosis and management of cancer and other conditions. Endoscopic procedures are considered to be Aerosol Generating Procedures (AGP). Infection control Covid-19 restrictions will reduce capacity to perform upper and lower GI endoscopy by 50% until the risk of transmission from patients to staff is clarified through reliable virus tests.
The clinical service team are preparing a business case exploring the potential use of colon capsule endoscopy, following qFIT stratification of patients, in the intermediate risk category. High risk patients would have colonoscopy as normal as there would be a high likelihood of need for biopsy/polypectomy. The intermediate risk patients who are still thought to have a good indication for colonoscopy would undergo CCE. There are a number of other elements of current endoscopy pathways that could use such non-invasive technology, reducing the demand for endoscopy procedures by up to 20%.
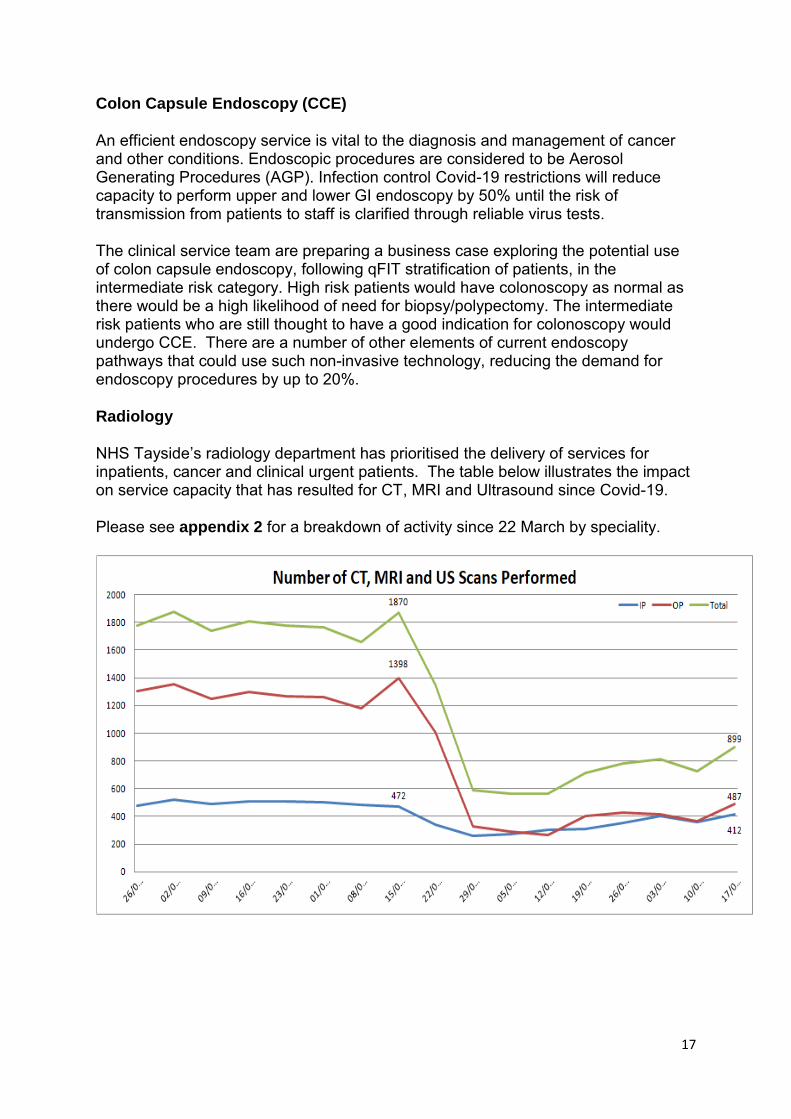
Radiology
NHS Tayside’s radiology department has prioritised the delivery of services for inpatients, cancer and clinical urgent patients. The table below illustrates the impact on service capacity that has resulted for CT, MRI and Ultrasound since Covid-19.
Please see appendix 2 for a breakdown of activity since 22 March by speciality.

18
Current Capacity Vs Pre Covid-19 Capacity
Modality Type Current capacity Pre COVID-19 Capacity Difference
CT IP 155 92
OP 242 435
Total 397 527 25%
MRI IP 53 53
OP 135 317
Total 188 370 49%
US IP 82 172
OP 155 631
Total 237 683 65%
Mobilisation of radiology services will focus on ensuring continued capacity for inpatients, clinically urgent and cancer patients prior to moving to increased capacity for planned and routine patients.
The service team are maximising available NHS and University resource to manage emergency, urgent and inpatient demand whilst appropriately managing appointment times and social distancing measures. Additional lists will be progressed through extended day working.
The safe re-introduction of routine outpatient work will progress across the main hospital sites throughout June. Review and consideration of introduction of activity on peripheral sites and through external capacity will also progress. The Head of Service is leading the national discussion with other Boards and the Department of Health regarding the option to increase capacity to manage required capacity through the introduction of CT pods in Scotland (CT in a box/ not a van).
Cardiology
Cardiology services have continued to provide emergency and urgent care during the Covid-19 response, totalling 183 procedures and necessitating 160 admissions to the Coronary Care Unit.
There are currently 70 patients awaiting cardiac procedures or 30 with cardiac device requirements. Pathways are now in place to allow this activity to be delivered safely, whilst maintaining the capacity to provide emergency care. It is anticipated that those patients awaiting urgent intervention will receive this within the next six weeks.
Clinical Investigation Unit (CIU)
As part of the initial Covid-19 response, the CIUs in both Ninewells and Perth Royal Infirmary stood down the majority of activity and vacated their footprint to allow additional inpatient capacity to be created. The critical role of CIU in avoiding unscheduled admissions has led to a plan being developed for the incremental increase of activity over June.

19
For the duration of the initial Covid-19 response, CIU services have been reconfigured to deliver infusions on the PRI site. Initial feedback indicated this has worked well and it would be the intention to continue this at least for the next two months.
c. Dental Services
Three Urgent Dental Care Centres have been established to provide appropriate triage for acute dental emergencies. In addition a Covid-19 Urgent Dental Care Centre has been established and to date demand for this has been minimal. Urgent services for Oral Surgery, Oral Medicine, Paediatric Dentistry and Orthodontics are also available should they be required. The Head and Neck Cancer pathway is also supported within the dental service.
Advice from the Chief Dental Officer was received on 21 May which outlines the guidance for Remobilisation of NHS Dental Services. This guidance contains three phases which predominantly focuses on increasing capacity in the Urgent Dental Care Centres, restarting Dental Practices and introducing AGPs to Dental Practices.
The guidance does not at this juncture address secondary care dentistry, therefore further clarity has been requested about the plans and guidance for the mobilisation of specialist dentistry in the Dental Hospital setting for both adults and children. Thorough the existing dental collaboration frameworks, Tayside will complete due diligence against the guidance as part of their plan. Locally, work has commenced to identify patients where delay in specialised dental therapies will result in clinical risk for the patient and safe pathways will be designed to accommodate these special cases.
Phase 1 – Increase in Capacity of Urgent Dental Care Centres
Activity through the NHS Tayside Urgent Dental Care Centres is outlined below:
w/c Angus Dundee Perth Tayside Total
30/03/2020 48 205 125 378
06/04/2020 62 202 117 381
13/04/2020 36 158 89 283
20/04/2020 75 159 86 320
27/04/2029 63 158 126 347
04/05/2020 60 172 122 354
11/05/2020 72 219 168 459
During Phase 1, Dental Practices will remain closed to face-to-face dental patient consultations and the dental throughput will be increased in the Urgent Dental Care Centres.

20
Phase 2 – Restarting Dental Practices
NHS Tayside, in line with the expectation from the Chief Dental Officer, will work towards supporting Dental Practices to open for face-to-face consultations for patients in need of urgent care that can be provided using non-Aerosol Generating Procedures by 31 July 2020.
Phase 3 – Introducing AGPs to Dental Practices
Phase 3 outlines a limited introduction of AGPs to Dental Practices. This is specifically dependent on evidence of risk and possible mitigation.
Screening Programmes
NHS Tayside hosts a number of screening services and will develop local plans to support the national screening mobilisation plans as they are progressed. As a key principle, NHS Tayside will assess local capacity and the clinical interdependencies required to support the outcome of screening programmes and work collaboratively with NSS to inform them about restarting screening programmes in Scotland.
d. TTG position
NHS Tayside has seen a c90% reduction in addition to our inpatient and daycase waiting list since the lockdown was introduced. In line with government advice, NHS Tayside has prioritised the delivery of elective procedures for cancer and clinically urgent patients.
Across acute specialities NHS Tayside has delivered 72 TTG elective admissions per week since 23 March. This represents c84% reduction in our elective admissions. NHS Tayside is planning to deliver an incremental increase, based on clinical prioritisation and subject to constraints, for example workforce, equipment, medicines, etc, at Perth Royal Infirmary in the coming weeks. At present the number of cases per week is anticipated to remain at around 72, however as the specific specialities to be introduced at Perth Royal Infirmary are agreed, clarity of the additional numbers to be treated each week will be provided.

21
Please see appendix 3 for a breakdown of activity since 22 March by speciality.
It is anticipated that of the planned 72 weekly cases, approximately 20 cases will be major priority 1 cancer or clinically urgent patients who will be managed via the Pre-Surgery Isolation Elective Surgical Pathway.
The below graph represents the predicted TTG activity over the next 10 weeks, with incremental growth from mid-June when our pathways at Perth Royal Infirmary should be established.
e. Cancer
There has been a marked reduction in urgent suspicion of cancer (USC) referrals received from the middle of March 2020 to the middle of April 2020 with a reduction of c69% over that period. However, the net reduction in referrals to the end of April is c60% following an increase in referrals in the last week of the month.
This is likely to be in response to national and local media messages highlighting that the NHS remains open for business for urgent clinical activity. It is anticipated that referral activity will be back to baseline following reintroduction of national screening programmes.

22
USC Referrals Received
Cancer Type
w/e 19/01/2020 to w/e 15/03/2020
w/e 22/03/2020 to w/e 17/05/2020
% Difference
Breast (Screened Excluded) 113 97 -14.2%
Breast (Screened Only) 0 0 0.0%
Breast Total 113 97 -14.2%
Cervical (Screened Excluded) 43 30 -30.2%
Cervical (Screened Only) 32 10 -68.8%
Cervical Total 75 40 -46.7%
Colorectal (Screened Excluded) 169 113 -33.1%
Colorectal Demand (Screened Only) 280 67 -76.1%
Colorectal Total 449 180 -59.9%
Head and Neck 91 60 -34.1%
Lung 105 29 -72.4%
Lymphoma 9 1 -88.9%
Melanoma 161 94 -41.6%
Ovarian 36 25 -30.6%
UGI 91 58 -36.3%
Urology 123 73 -40.7%
Total Referrals Received 1,253 657 -47.6%
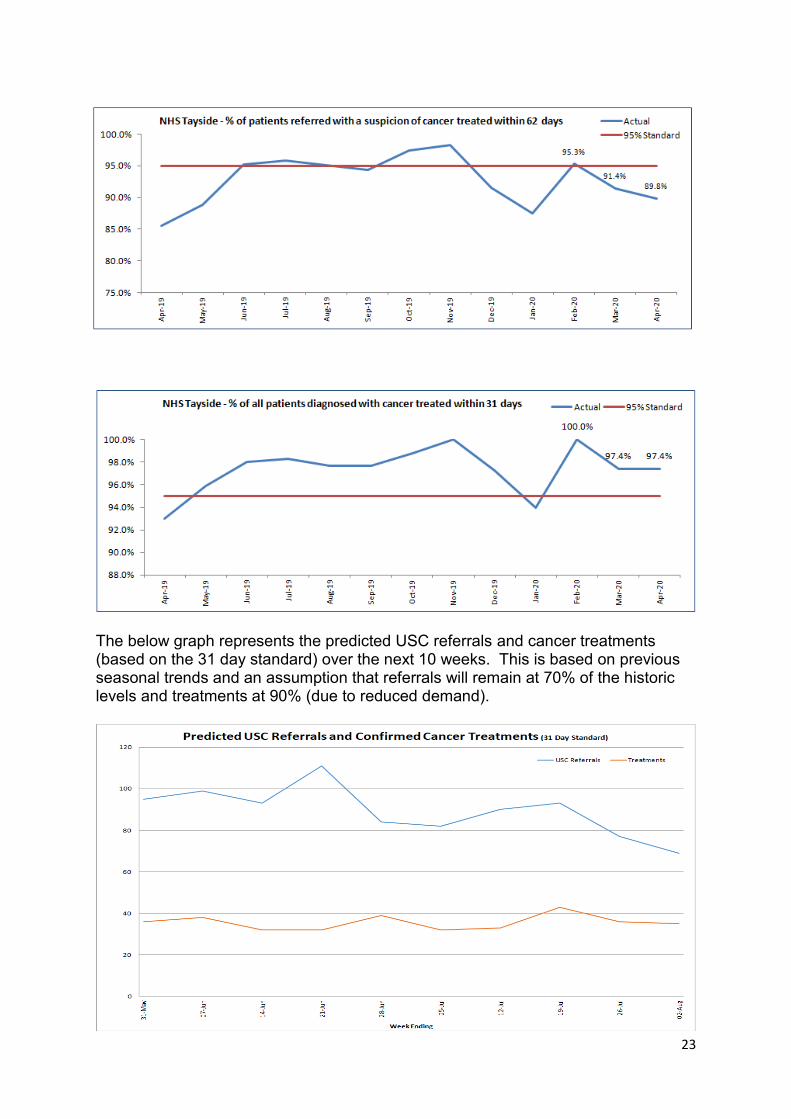
NHS Tayside has successfully maintained outpatient, surgical and oncology services for cancer patients, and whilst reinstatement of diagnostic services has now been achieved, capacity, particularly for endoscopy has been significantly impacted as a consequence of room cleaning times and PPE requirements. The next graph demonstrates weekly referral, diagnostic and treatment numbers. This shows treatments have remained consistent whilst referrals and diagnostics activity have reduced.
NHS Tayside is therefore anticipating that cancer waiting times performance over May and June will be impacted adversely by a reduction in capacity as a consequence of PPE/cleaning guidelines associated with Covid-19.
23
The below graph represents the predicted USC referrals and cancer treatments (based on the 31 day standard) over the next 10 weeks. This is based on previous seasonal trends and an assumption that referrals will remain at 70% of the historic levels and treatments at 90% (due to reduced demand).

24
5. Digital Infrastructure & Innovation
Connectivity
NHS Tayside’s Digital Directorate has conducted a comprehensive assessment of its infrastructure and capacity to accommodate remote working. Prior to Covid-19, eHealth could support a total of 766 remote connections, spread over two different connection methods (254 AnyConnect NHS Tayside laptops and 512 personal devices on Citrix). This was deemed sufficient to support business as usual activities.
In response to Covid-19, this was increased to a total of 1524 total connections split across 750 NHS Tayside laptop connections and 774 Citrix. To help accommodate as many remote connections as possible, a third remote service offering, which would allow access from a user’s personal device to StaffNet, key clinical and business systems, including Trakcare, Clinical Portal, EDD and ICE is being investigated. Plans to further increase capacity to accommodate remote and flexible working will be implemented over the coming months.
Furthermore, the NHS Tayside Digital Directorate have identified a solution to allow remote StaffNet access, which would accommodate around an additional 1800 remote connections at any one time, bringing the total remote capability to 3250 spread over three different service offerings.
Phone System Resilience & Capacity
The Digital Directorate recognised that several services would extend their reliance on the use of phone and data services during the short and medium term. Activities such as remote consultation, pre-attendance checks with patients prior to hospital visit, suspension of hospital visits, patient contact tracing etc., were identified as potentially having an impact on the phone capacity.
The capacity of the phone system was increased by more than 40% to 500 with options to further extend this if required.
Microsoft (MS) Teams
Following the mandate from Scottish Government and the re-alignment of the technical design with our existing MS programme, wide scale adoption is being phased in. With all NHS Tayside PCs having the TEAMS client installed, the enablement of users is currently at 50% of all NHS Tayside employees with direct access and all other users are able to access through the “Guest” route. The current deployment will be complete by 8 June 2020, with all named users being able to access via their authenticated accounts.
In addition, significant support activities are being carried out across the service to build local capability to run and operate the functions of MS TEAMS at a service level and devise and share learning around the tools ability to support collaboration and sharing within and across services.

25
Patient Management Systems
Work is progressing to develop and update digital solutions to support flexible and remote working across clinical services. Clinical builds and templates in TRAK, the referral management system and clinical portal are all being reviewed and updated to facilitate digital ways of working, ensuring robust referral management, patient consultation and advice, as well as waiting list and outcome management.
Rapid and significant progress within the outpatient remote consultation area has now been achieved. A new Remote Consultation Board has been established, and Tayside is now one of the highest achieving Boards in terms of delivering remote consultations as default mechanism of communicating with our patients.
Our ambition is to ensure that post Covid-19, our clinicians and patients readily accept this new way of working as the norm and that the processes established to facilitate these appointments are robust, safe and endure. We will now focus on routine appointments to ensure that, in the long term, we significantly reduce the number of patients visiting our acute centres.
The Near Me (Video Consultation) Project has been re-scoped to support the wide scale adoption of Remote Consultations - Telephone and Near Me (Video) across NHS Tayside.
The areas of adoption include Primary Care and the TrakCare Users across Acute, Mental Health and AHPs. Other areas have direct dealings with patients but which do not record this activity in our Patient Administration systems have also been included.
Since the beginning of March 2020, there has been a significant rise in this consultation method with over 15,000 remote consultations taking place. Additionally, NHS Tayside will work closely with Digital Health and Care Institute and the Scottish Government over the next eight weeks to implement a wide range of digital protocols to support digital home health monitoring in order to embed this where possible in our remote consultation clinical pathways. Remote monitoring of patients will be explored in a wide range of settings with the aim of ensuring the right clinical information is available at the right time in the right setting.
Patient Management Systems
Work is progressing between the Digital Directorate and clinical teams to develop and update digital solutions to support flexible and remote working across clinical services. Clinical builds and templates in TRAK, the referral management system and clinical portal are being reviewed and updated to facilitate digital ways of working, ensuring robust referral management, patient consultation and advice as well as waiting list and outcome management.
6. Financial Framework
It is critical that appropriate consideration is given to financial aspects in terms of both affordability and sustainability as plans are taken forward. We continue to work closely with finance colleagues to ensure our Living with Covid-19 financial plan

26
aligns directly with how our services are operating on the frontline and reflect the revised pathways outlined in this paper.
Costs associated with mobilisation will be returned to Scottish Government in accordance with nationally agreed timeframes. A full review of the Board’s financial plan is also proposed following quarter one results.
7. Testing
Covid-19 testing continues to play a critical role supporting NHS Tayside’s mobilisation plans through a number of its core functions. The Covid-19 testing service extends beyond the requirements to support mobilisation, however the testing functions relevant to mobilisation specifically include:
Staff Testing & Workforce
Covid-19 testing for health and social care staff and their household contacts remains a priority to enable staff to return to work in the event of a negative result. This minimises the requirement for self-isolation and staff absence. To date (effective 20.05.20) the Community Testing Team has undertaken 5011 test for staff or their household contacts; 3006 NHS staff, 1854 social care staff and 150 identified as others. The average positivity rate over the complete testing period is 20% for staff and household contacts, indicating 4009 tests resulted in a staff member returning to work. In terms of return on investment, each negative test will prevent either 5-6 days of self-isolation for a staff member, or 12-13 days of self-isolation where a household contact has been symptomatic, but tested negative.
Pre-admission testing for patients in acute hospital
To minimise risk to patients and staff, patient testing for patients being admitted through the green, or self-isolated elective pathway or the yellow indeterminate pathway for those unable to follow the self-isolation pathways is undertaken at pre-assessment (where applicable) then 48 hours prior to admission. This will ensure as much as possible that patients admitted electively to hospital have been screened and are managed accordingly. The impact is reduced harm to patients, considering the increased mortality risk of Covid-19 in this patient group, reduction in use of PPE and to support appropriate patient placement, and as appropriate prioritising side rooms for admissions with no previous testing.
Testing for patients in hospital and community prior to transfer / admission to care home
Testing for patients prior to admission to a care home is mandated by Scottish Government. Therefore, to maintain effective flow of patients and ensure patients have access to an appropriate safe home care setting testing prior to admission or transfer, is critical.
Outbreak Management
Where a Covid-19 outbreak is suspected early testing to assist with the effective management of an outbreak situation is essential.

27
On admission screening for unscheduled surgical and orthopaedic patients
This is undertaken in the non Covid-19 unscheduled surgery and orthopaedic setting to ensure patients are managed appropriately through the correct pathways, appropriate use of theatre provision, PPE use and patient placement to mitigate risk to self, staff and other patients.
On admission testing of over 70s and ongoing surveillance is undertaken in the non Covid-19 pathway to enhance surveillance of Covid-19 in a low risk but vulnerable patient group to prevent spread, and protect staff and patients.
NHS Tayside capacity for testing from 25 May 2020 will be:
Model Number of Tests Weekly Total
Mon Tues Wed Thurs Fri Sat Sun
ABI 280 280 280 280 280 ------- ------
SeeGene 300 300 300 300 300 200 200
Daily Total 580 580 580 580 580 200 200 3300
Test, Trace, Isolate, Support (TTIS)
Scottish Government (SG) published its ‘Test, Trace, Isolate, Support’ (TTIS) strategy on 4 May 2020 as part of the next stages of COVID-19 management. Central to this is comprehensive contact tracing – a highly effective evidence based means of halting the chain of infectious disease transmission, which will be critical as lockdown measures are eased in order to prevent a second peak in COVID-19 cases, COVID-19 related hospital and intensive care admissions, and fatalities. The nature of the epidemic means this is a rapidly developing and evolving area, much of which is dependent on national decision making and approaches, meaning that practice, guidance and therefore the response needed will evolve over time. This has made the planning for Contact Tracing at scale and pace extremely complex and demanding, and therefore there has been a greater than expected reliance on local modelling, design and decision-making. Local NHS boards are required to have arrangements in place by the end of May 2020. Contract Tracing will recommence the week beginning Monday 25 May 2020 and will enable contact tracing of all positive cases currently diagnosed through NHS Tayside testing facilities (Community Testing Team, Community Hubs including enhanced surveillance and hospitals). The exception is with care home residents who are subject to enhanced care home management arrangements by the specialist Health Protection Team. Inclusion of cases identified through UK Government Testing Centres is expected in the coming weeks as these results become timeously available to Health Boards. Contact Tracing is in the process of being piloted in three NHS Boards from 18 May 2020. This will test the digital platform as well as refine and adapt processes. Interim national guidance has been developed for the pilot sites and

28
accompanying training materials are in development. A Digital Platform is being rolled out across Scotland from 25 May 2020 and full technical support will be provided to NHS Tayside from 28 May 2020 by NSS. Guidance and operational considerations may change in light of the evaluation of the pilot sites.
Gold Command approved a paper on 6 May 2020 setting out the key actions required. Gold Command recognised the importance of a whole organisational effort if Contact Tracing is to be effective and the wider aims of the TTIS are to be met. Additional senior level support was identified to provide the essential connections across the scope of TTIS, including in respect of the additional support that many individuals in isolation may require. The Director of Workforce also identified dedicated senior level support for recruitment to enable the rapid scale up of human resources required for contact tracing and for training and development needed to complement national materials.
NHS Tayside has been widely commended for its distinctive and ambitious local approach to all aspects of its response to COVID-19, and in particular it’s highly successful testing programme. The arrangements that are being put in place in Tayside for Contact Tracing aim to be equally ambitious. Public Health Scotland (PHS) has produced interim guidance to support the scale up for management of uncomplicated contact tracing with an expectation that complex cases are managed by local Health Protection Teams. However, for an effective and sustainable response – even in the short term – we have taken the decision to adopt a bold, comprehensive plan from the outset of its reintroduction. This will be vitally important for the control of the epidemic. It is important to note that close contacts of confirmed COVID-19 will be asked to isolate for 14 days since their last exposure. Testing of asymptomatic contacts of a confirmed case of COVID-19 cannot be used to shorten the self-isolation period. National guidance is awaited on how contact tracing should be conducted in a healthcare setting and local plans are being discussed between the IPCT, Occupational health and Public Health. However, it should be noted that staff risked assessed as being significantly exposed to a confirmed case (e.g. without PPE, PPE breach) may be asked to self-isolate for up to 14 days.
8. Medicine Management
Prior to the onset of the current pandemic, clinical teams developed a critical medicines list, along with the systems to ensure daily oversight of the available stocks of these medicines for Tayside. This work, led by pharmacy teams, is now embedded as a routine business function. The daily monitoring of these critical medicines allows early system alerts to be issued to support timely clinical decision making to agree and implement any remedial actions.
In order to support the appropriate planning of clinical activity, new systems have been implemented to ensure the clinical leads planning theatre activity are sighted on the current stock holding of all critical care medicines allowing an assessment of any implications upon clinical practice. Weekly information is shared and discussed which incorporates full UK level intelligence related to the medicines supply chain.

29
9. Access and Patient Transport
NHS Tayside established a Patient Transport Team (PTT) on 22 April 2020 in response to the Covid-19 pandemic. The initial plan outlined a 24/7 transport service that would support members of the public displaying Covid-19 symptoms, and who had been triaged by General Practitioners, to access the newly established Community Assessment Hub, (CAH) and, subsequently, to transport them either home or to ongoing treatment destinations. This service is for individuals who have no access to their own transport, that of family or carers vehicles or, because of the nature of their illness, to public transport. The transport model would also support the increased demand and pressures on general practitioner capacity in primary care for home visits due to Covid-19 disease.
The service inception was supported in partnership with Transport Scotland and Scottish Government Out-of-Hours Primary Care Division who provided NHS Tayside access to specialist vehicles supplied by Arnold Clark. The development of the service has benefited from input from the British Army Officers deployed to Tayside.
The PTT supports the following services:
CAHs
Emergency community dental and eye services
Mental health services
GP OOH
Routine renal dialysis
Outpatient/diagnostic testing and inpatient admission for those who require urgent/cancer treatment who are in the shielding category
Other shielded patient cohorts
Patients recovering from Covid-19 requiring discharge from hospital
The delivery of hospital chemotherapy regimens to shielded patients at home
01
/03
/20
20
04
/03
/20
20
07
/03
/20
20
10
/03
/20
20
13
/03
/20
20
16
/03
/20
20
19
/03
/20
20
22
/03
/20
20
25
/03
/20
20
28
/03
/20
20
31
/03
/20
20
03
/04
/20
20
06
/04
/20
20
09
/04
/20
20
12
/04
/20
20
15
/04
/20
20
18
/04
/20
20
21
/04
/20
20
24
/04
/20
20
27
/04
/20
20
30
/04
/20
20
03
/05
/20
20
06
/05
/20
20
09
/05
/20
20
0
10
20
30
40
50
60
70
80
90
Number of patient journeys across Tayside OOH service
Angus
Perth
Dundee

30
In total, to date, 435 patients have accessed the transport service many of these transported on more than one journey.
Week 4 data indicates that the highest service demand was within the shielding patient category accounting for 66% of total activity; concomitantly there has been a slight drop in the Covid-19 status category of patient transport requests.
NHS Tayside will require to retain the ability to respond promptly to any future peaks in incidence of Covid-19 and ensure safe clinical pathways for patients presenting with potential Covid-19 symptoms into the foreseeable future, including their transportation.
Although it is anticipated the demand for CAHs will decrease, the current designated Covid-19 clinical care areas will remain operational until a further review is conducted at the end July 2020 to establish need, both at that point and prospectively.
Covid-19 positive, suspected Covid-19 patients and shielded patients fall into a category that would not normally be transported under Scottish Ambulance Service (SAS) criteria but for whom public transport is not feasible. The future of all transport services will need to take into account prescribed public health social distancing measures which will impact significantly on the capacity available for deployment of both vehicles and crew.
Lack of a means to access care by the population will result in potential clinical detriment and widen the health equity gap. It is not clear which organisation retains responsibility to support these patients from a transport perspective however it would be beneficial to work on a ‘once for Scotland’ basis and to promote collaboration between NHS Boards and the SAS to support these patient cohorts.
Financial Costs
NHS Tayside Patient Transport Team incurred no capital cost at commissioning as Arnold Clark provided 17 specialist vehicles free of change on long-term loan and

31
vehicle fuel costs are being met by BP. Vehicle access steps and child seats were donated by Lidl. The service is resourced primarily by existing staff who have been redeployed and a small number of volunteers.
Total costs for the first month of services including for decontamination and PPE provision, are currently being collated.
From week commencing 18 May 2020 the deployed staff cohort have been augmented by Team Rubicon, a group of retired army and ‘blue light’ personnel who provide volunteer support to front line services in times of national crisis. They will provide resilience as deployed staff resume normal duties and support an ambition to sustain an out-of-hours service.
Team Rubicon’s commencement will support the current delivery and ambition to deliver the service 24/7. Team Rubbicon will undertake to test the out-of-hours service in conjunction with the out-of-hours GP service allowing an evaluation of service provision and a determination of whether there is unmet demand. This test will be undertaken at no cost.
Team Rubicon will support NHS Tayside’s Patient Transport Team until the end of July 2020.
Service Redesign
Future service delivery will be determined by Scottish Government Guidance, the development of new clinical pathways and the adoption of innovative ways of delivering clinical services. Advancements in technology implemented during the Covid situation will determine the level of need to physically transport patients to health care facilities.
NHS Tayside will work in conjunction with SAS colleagues to progress a number of initiatives including the introduction of advanced paramedics and develop patient pathways that will reduce the number of acute admissions thus freeing capacity to meet the challenges of shielding, social distancing and isolating before admission to hospital for procedures.
However NHS Tayside will need to consider the sustainability of providing transportation to patients as part of the clinical pathways. In the short-term there will remain a need to develop a business case to maintain the PTT model which would include associated costs if voluntary support, both manpower and infrastructure, is withdrawn. In the long-term options will include collaborative initiatives between health service and the SAS.
10. Staff Deployment Centre
The Staff Deployment Centre (SDC) was established in April 2020 to support the safe and efficient deployment of all existing, new and bank staff across Tayside during the Covid-19 pandemic.
Two internal teams of staff have been supporting the Centre, a Deployment team and a Bank team which pull together all four staff banks (Medical, Nursing &

32
Midwifery, Allied Health Professions and all Non-clinical staff) established for Covid-19 and beyond.
To support the meeting of future workforce capacity requirements and the continued supported deployment of staff into services as they start to mobilise again, the SDC must remain in operation to provide a consistent and prioritised approach for the most effective use of available staffing and their skills.
The main function of the SDC is to match staff and skills available to priority areas that require staffing, either through use of available existing staff or the use of bank staff. The aim of the SDC is to keep people as close to their current base and current role as possible and to endeavour to move staff in groups to allow for internal team support. This has worked well to date.
In total since the opening of the SDC there have been 1915 staff successfully matched to roles and bank shifts. Staff have mainly been deployed to Soft FM services (Porters and Domestics), Workforce and Corporate & Board services (administration and clerical roles) and to support Covid-19 specific activities i.e. Transport Hub, Assessment Hubs and the set up and running of the SDC itself (drivers, administration, etc). Recruitment to the bank has come from a number of sources such as social media advert, NES Accelerated Recruitment Portal (ARP), pre-registration student nurses and contacting retirees/returners.
As the mobilisation of services commences, current staff deployed will be required to return to their normal working areas which may leave gaps within other critical services where they have been working. These returning staff and any potential backfill created and recruitment to new services such as Test and Protect will require the support of the SDC function to ensure a consistent and supported approach is taken for all staff. This will also ensure an overview is maintained across Tayside to highlight any risks and shortfalls in a timely manner.
11. Risk Assessment
As Covid-19 continues to pose a threat over the coming weeks and months the NHS remains in an emergency situation and therefore there are a number of risks that will require to be managed:
Workforce – availability and impact from the first phase
System-wide pressures – there is a risk that switching on and off certain parts of the system will have a negative impact on other parts of the system e.g. critical care dependent elective procedures or the impact on community discharge teams and the third sector
Capacity and productivity – current Covid capacity is being retained and planning for winter is commencing which could further impact on the remobilisation of elective care. The ability to maintain separate red and green facilities may be difficult over time and further compromised by undertaking more complex low volume work which, by its nature, involves larger teams of specialist staff

33
Supply chains – An ongoing assessment and monitoring of availability of supplies including PPE, drugs and equipment is required, recognising that some Boards may increase elective activity while others may have ongoing Covid-19 related requirements. In addition, decisions locally, regionally and nationally (Scotland) must been seen in the context of a wider UK position. These could be rate limiting factors
Ability and willingness to travel – in the event that patients will be required to travel for treatment we will need to consider ways to support this, taking account of physical distancing. This will be important to avoid issues of inequality
Infrastructure implementation of current and further phases of our elective care mo-bilisation plan require a significant investment of time and resource in risk assess-ment of suitability of current facilities and space. A number of environmental changes require to be progressed to ensure that areas are fit for purpose to support safe ways of delivering services.
12. Conclusion
The current Covid-19 pandemic has created the conditions to transform some services within an accelerated timeframe. Some examples of service transformation and innovation are outlined in appendix 5.
The leadership, commitment and efforts by staff, partners and local communities to respond to the pandemic has been exceptional. This has supported NHS Tayside and its partners to respond to the challenges of Covid-19 in an agile and co-ordinated way. All efforts have been undertaken in partnership to ensure efficiency across the system as a whole.
The essential approach of NHS Tayside in developing its Remobilisation Plan has involved the following key principles:
Services which are safe for patients and safe for staff
Services which are developed in clinically-led models with appropriate Standard Operating Procedures and governance arrangements at their heart
Engagement with all those principal actors, but additionally other agencies which may be impacted by, or contribute to, the remobilisation services delivery
The key priority is shifting the balance of care to deliver high value clinical outcomes within a sustainable financial model. The elective mobilisation plan will outline key phases in the short and medium term and will align to the longer term elective aspirations of NHS Tayside and wider capital programmes such as Tayside Elective Care Centre, Critical Care and Cancer Care Centre.
To enact at pace this will require an agreed financial framework to shift resource, and a strategically coordinated but clinically devolved leadership and decision making structure.
34
Appendix 1 – Tayside Acute Hospital Service Plan – Living with COVID19
20200514 Tayside
Acute Hospital Service Plan – Living with COVID 19 Sche....pptx

35
Appendix 2 – Outpatient Activity by Speciality (22/03/20 – 17/05/20)
Specialty New Return
Acute Medicine 178 51
Anaesthetics 15 1,241
Cardiology 307 524
Cardiovascular Risk 0 36
Clinical Genetics 65 21
Clinical Neurophysiology 82 2
Clinical Oncology 395 4,252
Community Dental Practice 0 0
Dermatology 1,172 2,294
Diabetes 82 608
Ear, Nose and Throat (ENT) 225 418
Endocrinology 58 200
Endoscopy 355 229
Gastroenterology 82 250
Breast Clinic 498 303
General Surgery (excl Vascular) 1,350 959
Gynaecology 985 700
Gynaecology - Infertility 4 0
Haematology 25 1,451
Medical Warfarin 12 4,832
Immunology 14 25
Infectious Diseases 149 89
Neurology 525 1,173
Neurosurgery 68 172
Ophthalmology 326 1,457
Oral and Maxillofacial Surgery 115 296
Oral Medicine 22 73
Oral Surgery 87 68
Orthodontics 9 117
Paediatric Dentistry 7 14
Paediatric Surgery 68 111
Paediatric Community 30 254
Paediatrics 337 1,406
Pain Management 10 81
Plastic Surgery 244 776
Renal Medicine 21 692
Respiratory Medicine 163 447
Restorative Dentistry 18 25
Rheumatology 105 608
Trauma and Orthopaedic Surgery 1,256 1,749
Urology 383 1,015
Vascular Surgery 41 100
Total 9,888 29,119

36
Appendix 3 - TTG Admissions by Speciality (22/03/20 – 17/05/20)
Speciality TTG Admis-sions
Anaesthetics 1
Cardiology 49
Clinical Oncology 55
Community Dental Prac-tice
23
Dermatology 2
Ear, Nose and Throat ENT
35
Endocrinology 2
Gastroenterology 6
General Medicine 4
General Psychiatry (Mental Illness)
4
General Surgery (excl Vascular)
126
Gynaecology 78
Haematology 3
Neurology 6
Neurosurgery 9
Ophthalmology 104
Oral and Maxillofacial Surgery
29
Oral Surgery 1
Paediatric Surgery 4
Paediatrics 1
Plastic Surgery 80
Renal Medicine 3
Respiratory Medicine 2
Trauma and Orthopae-dic Surgery
24
Urology 155
Vascular Surgery 19
Total 825

37
Appendix 4 - Activity
w/e w/e w/e w/e w/e w/e w/e w/e w/e w/e Comments
31-May
07-Jun 14-Jun 21-Jun 28-Jun 05-Jul 12-Jul 19-Jul 26-Jul 02-Aug
TTG Inpatient Activity (Definitions as per waiting times data mart)
urgent 72 72 72 82 94 107 107 122 122 139 To remain at current median levels until mid-June when we anticipate gradual in-troduction of activity at PRI
routine 0 0 0 0 0 0 0 0 0 0
TTG Day case Actvity (Definitions as per waiting times data mart)
urgent IP/DC combined above See above
routine
Elective colonoscopy activ-ity (Definitions as per Monthly Management Information)
urgent 36 30 36 30 36 30 36 30 36 30
Based on activity de-livered over recent weeks and capacity for next 2 weeks. Fo-cusing on delivery of all USC and urgent scopes
routine 0 0 0 0 0 0 0 0 0 0
Elective lower endoscopy activity (Definitions as per Monthly Management Information)
urgent 14 10 14 10 14 10 14 10 14 10
routine 0 0 0 0 0 0 0 0 0 0
Elective upper endoscopy activity (Definitions as per Monthly Management Information)
urgent 16 23 16 23 16 23 16 23 16 23
routine 0 0 0 0 0 0 0 0 0 0
Elective cystoscopy activity (Definitions as per Monthly Management Information)
urgent 20 20 20 20 20 20 20 20 20 20
routine 0 0 0 0 0 0 0 0 0 0
urgent 514 570 570 633 633 780 780 780 780 780

38
OP Referrals Received (Definitions as per waiting times data mart)
routine 604 694 694 798 798 950 1131 1131 1346 1346
Assumes incremental increase in both ur-gent and routine re-ferrals based on growth rates seen in recent weeks
OP Activity - (including Vir-tual - telephone, NHS Near Me,...) (Definitions as per waiting times data mart)
urgent 572 600 600 628 628 659 659 690 690 723 Assumes incremental increase in both ur-gent (in response to projected increase in urgent referrals) and routine appts based on growth rates seen in recent weeks
routine 709 734 734 761 761 788 788 816 816 846
A&E Attendance (system watch - core sites)
892 932 933 953 910 854 885 913 979 931
Based on 2019 trends and %age re-duction in attend-ances evident in past 4 weeks
Emergency Admissions (Systemwatch - RAPID)
736 763 747 738 731 728 730 721 717 725 Based on predictions on System Watch
Urgent Suspicion of Cancer - Referrals Received (SG Management Infor-mation)
95 99 93 111 84 82 90 93 77 69
Based on 2019 trends and %age re-duction in referrals as evident over recent weeks (i.e. 70% pf usual rates)
31 Day Cancer - First Treat-ment (Definitions as per pub-lished statistics)
36 38 32 32 39 32 33 43 36 35 Based on 2019 trends and %age re-duction in treatments,

39
based on reduced de-mand, as evident over recent weeks (i.e. 90% of usual rates)
CAMHS - First Treatment (Definitions as per pub-lished statistics)
22 13 22 20 17 18 12 16 7 14
Based on 2019 trends and %age re-duction in attend-ances evident in past 8 weeks
Minor Ailment Scheme
PC OOH – Home Visits
PC OOH – Centre attend-ances & telephone advice calls

40
Appendix 5 - Examples of innovation NHS Tayside March/May 2020
Collaboration
First use of primary/secondary whole system Zoom
First functioning Covid hubs
Palliative care framework, palliative care drug procurement in place from 1 week of response
Whole system approach. ‘One disease, one system, one response’ philosophy from week one
Covid transmission Modelling of Covid-19 transmission throughout Europe by Mike Lonergan has suggested that significant restrictions will need to remain in place to prevent a catastrophic second peak of transmission in the UK (link to press release). This study was discussed in questions with the FM Nicola Sturgeon.
Testing
Early awareness of clinical importance of testing led to NHS Tayside testing system widely regarded as best in UK, based on round the clock virology laboratory working.
Open access publication. Early testing of Health care workers in Tayside has saved over 8000 working weeks of absence over only a three week period (link to press release).
Equipment
PPE 3D printing of shields and face masks, home sewn scrubs
Early testing of thermal imaging for front door screening
Quality Improvement
NHS Tayside is undertaking a real time evaluation of how it has innovated in response to the Covid crisis. Insights gained from the review are informing the design of the structures and approaches which will be needed for the next stage of the recovery.
NHS Tayside is developed new QI tools that will help map and plan the innovations needed to deliver its healthcare services in the new Covid-19, with a focus on the needs of patients and service-users.
Patient experience
Patient Journey App to facilitate perioperative journey in the green zone Remote visiting using NYE app and vcreate
Digital technology
Rapid uptake of remote working systems
Early use of iPads in Covid areas for patient communication

41
Basic research
1. STOP-COVID: £806,767.20 - this is currently the only COVID-19 drug trial to have received urgent public health designation from the NIHR and led from Scotland (UoD press release) 2. PREDICT-COVID: Microbiome £287,000 CSO have funded a genomics study using real-time PCR and nanopore sequencing to detect viruses and bacteria in the lungs of individuals with COVIDin order to improve treatment of severe COVID-19. 3. PREDICT-COVID: Biomarkers- £293,892 School of Medicine and Life Sciences have been funded by the CSO to study the immune systems reaction during severe COVID-19 using proteomics and gene expression. 4. Outcomes from COVID-19 £193,818 David Connell and colleagues at the Medical School have been funded by the CSO to study the longer term damage to lungs and other organs in patients who have recovered from Covid-19. As covered by BBC News 5. Life Arc-funded novel anti-inflammatory trial £639,000, a trial to test a novel anti-inflammatory medication to prevent ARDS in patients with Severe Covid-19. 6. Selective drivers of antimicrobial resistance development in human infections £1,687,054.00 The Wellcome trust has funded a consortium of lung researchers from Dundee, London and Sheffield to examine how repeated courses related to respiratory infections impacts on the development of antibiotic resistance and whether this can be predicted and prevented.
7. To develop evidence-based interventions to support doctors’ well-being and promote resilience during Covid-19 related transitions (and beyond). Scottish Medical Education Research Collaboration (CSO funded, £225,000). A Scottish wide study to determine how doctors are experiencing the transitions associated with the current Covid-19 pandemic? And to explore which interventions will best support doctors’ well-being and resilience during transitions associated with the current Covid-19 pandemic and towards long-term future practice?
8. Development of a Covid-19 vaccine in collaboration with an International Covid-19 taskforce. Using a Dundee established Virus-like-particle vaccine technology we are creating anti-Covid19 vaccines which differ in their expected immune response from the ones presently undergoing early clinical testing.
9. Optimising the use of drugs in clinical trial for the treatment of Covid-19: The humanised mouse model of drug metabolism is being used in collaboration with the DDU to evaluate the pharmacokinetics of novel candidate Covid-19 drugs.

NINEWELLS LAYOUT – Living With CoVid-19 Planning
EAST & MAIN BLOCK SOUTH BLOCK WEST BLOCK GYNAE & MATY BLOCK
Level 8 Ward 34 Ward 33
Level 7 Ward 6 Ward 5 Ward 4 Ward 3 Ward 2 Ward 1 Ward 36 Ward 35
Level 6 Ward 12 Ward 11 Ward 10 Ward 9 & SHDU
Ward 8ASRU
Ward 7ASRU
Ward 23A
Ward 23B & NHDU
Ward 38 Ward 37
Theatre 6 Theatre 5 Theatre 4 Theatre 3 Theatre 2 Theatre 1 ICU2 (TAS) Theatre 7 Theatre 8
Ward 30/ Children’s Theatre
GynaeAssessment Unit
Level 5 Ward 42 Ward 19 Ward 18Ward 17
Ward 16 Ward 15& MHDU Ward 14
Burn
sUni
t
Ward 27 Ward 26 Ward 25 Ward 24 Labour Suite Maty Theatre
MTU
CIUTh 9 Th 10 Th 11 Th 12 Th 14 Th 15
Level 4COVID
ASSESSMENT UNIT
Ward 22 Ward 21 Ward 20 ICU 1 ED Ward 31
NICUWard 29
Paeds
Level 3 Ward 32
Known COVID +ve or displaying symptoms
> 8 days post COVID
Indeterminate COVID / no Pre-Surgery Isolation
Pre-Surgery Isolation Patient Elective Surgical Pathway

Level 7
Ward 6 Ward 5 Ward 4 Ward 3 Ward 2 Ward 1
MfE Surgical & Ortho Frailty General Medicine Respiratory Gastroenterology Cardiology
Level 6
Ward 12 Ward 11 Ward 10 Ward 9 Ward 8 Ward 7
Vascular General Surgery & Urology Orthopaedics Orthopaedics Acute Surgical
Receiving UnitAcute Surgical Receiving Unit
Level 5
Ward 42 Ward 19 Ward 18 Ward 17 Ward 16 Ward 15 Ward 14
COVID Assessment Ward COVID +ve Ward COVID +ve Ward
COVID +ve Surgical Assessment Unit
COVID +ve MHDU (MTU)
AMEAMU
COVID-ve MHDU
Short Stay Medicine
Level 4 COVID Assessment Unit
Ward 21 Ward 20
CCU COVID -ve ICU
Known COVID +ve or displaying symptoms
> 8 days post COVID
Indeterminate COVID / no Pre-Surgery Isolation
Pre-Surgery Isolation Patient Elective Surgical Pathway
COVID-19 Elective Surgical PathwaysNinewells HospitalEAST BLOCK / MAIN BLOCK
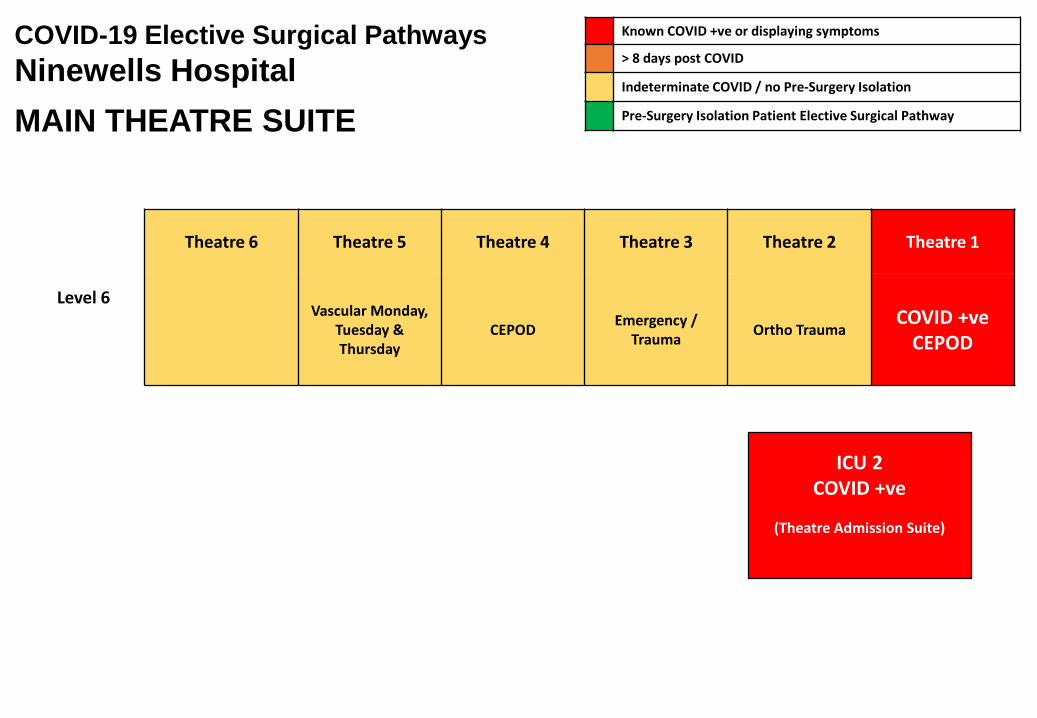
Level 6
Theatre 6 Theatre 5 Theatre 4 Theatre 3 Theatre 2 Theatre 1
Vascular Monday, Tuesday & Thursday
CEPOD Emergency / Trauma Ortho Trauma
COVID +ve CEPOD
ICU 2COVID +ve
(Theatre Admission Suite)
Known COVID +ve or displaying symptoms
> 8 days post COVID
Indeterminate COVID / no Pre-Surgery Isolation
Pre-Surgery Isolation Patient Elective Surgical Pathway
COVID-19 Elective Surgical PathwaysNinewells HospitalMAIN THEATRE SUITE

Known COVID +ve or displaying symptoms
> 8 days post COVID
Indeterminate COVID / no Pre-Surgery Isolation
Pre-Surgery Isolation Patient Elective Surgical Pathway
COVID-19 Elective Surgical PathwaysNinewells HospitalSOUTH BLOCK
Level 6
Ward 23a Ward 23b
NeurologyPlastic Surgery
Neurosurgery & Neuro HDUENT
OMFSOphthalmology
Level 6
Theatre 7 Theatre 8
NeurosurgeryPlastics Trauma
OncologyCardiology

Level 6
Ward 30 / Paediatric Theatre Gynae Assessment
UnitMaternity Emergencies & Electives
Level 5
COVI
D In
dete
rmin
ate
HDU
(B
urns
Uni
t)
Plastic Surgery Day Case Area Ward 27 Ward 26 Ward 25 Ward 24
PSI Pathway Patients
ReceptionPSI Pathway Patients PSI Pathway Patients PSI Pathway Patients PSI Pathway Patients
Level 4Ward 31 Ward 29
NICU Paediatrics Paediatrics
Level 3
Ward 32
Oncology
Level 5
Theatre 9 Theatre 10 Theatre 11 Theatre 12 Theatre 14 Theatre 15
Urology, Vascular & Plastic Surgery
General Surgery, OMFS, Gynae & ENT
General Surgery & Gynae
Known COVID +ve or displaying symptoms
> 8 days post COVID
Indeterminate COVID / no Pre-Surgery Isolation
Pre-Surgery Isolation Patient Elective Surgical Pathway
COVID-19 Elective Surgical PathwaysNinewells HospitalWEST BLOCK WARDS & THEATRES
PSI Patients Meet and Greet
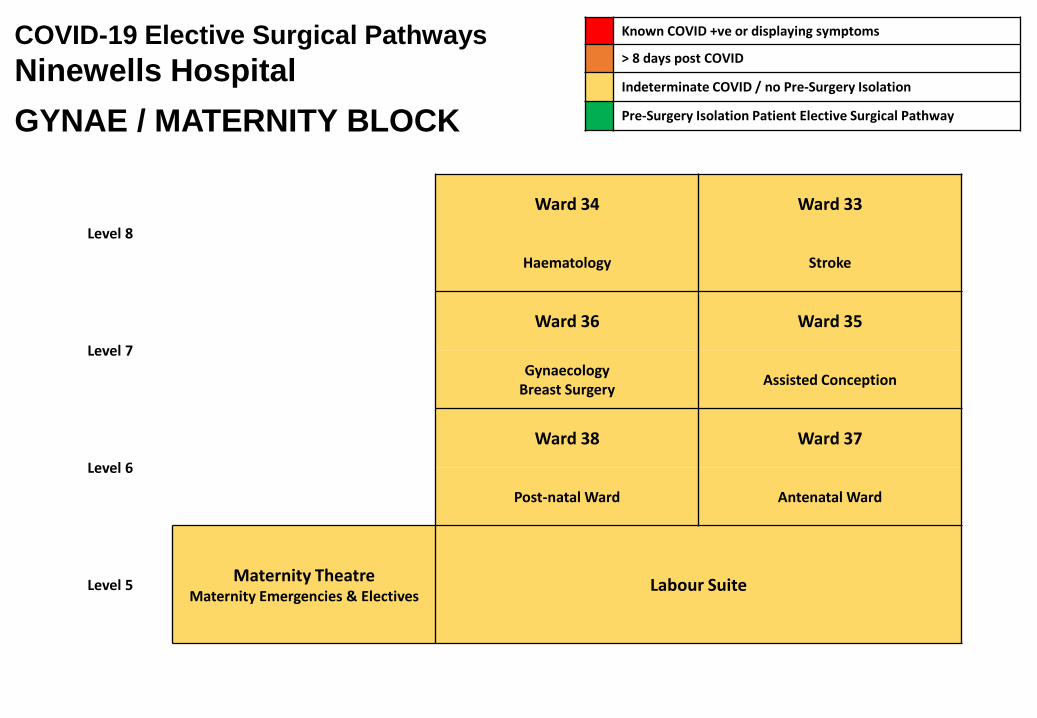
Known COVID +ve or displaying symptoms
> 8 days post COVID
Indeterminate COVID / no Pre-Surgery Isolation
Pre-Surgery Isolation Patient Elective Surgical Pathway
COVID-19 Elective Surgical PathwaysNinewells HospitalGYNAE / MATERNITY BLOCK
Level 8
Ward 34 Ward 33
Haematology Stroke
Level 7
Ward 36 Ward 35
GynaecologyBreast Surgery Assisted Conception
Level 6
Ward 38 Ward 37
Post-natal Ward Antenatal Ward
Level 5 Maternity TheatreMaternity Emergencies & Electives
Labour Suite

COVID Assessment Unit
Ward 7 Ward 8
Ward 2Ward 5
CCU / HDU
Ward 1 Ward 6 Ward 3 Ward 4
Theatre 1 Theatre 2 Theatre 3 Theatre 4 Theatre 5
Trauma Urology
BreastPlastics
GynaePlastics
ECTOrthopaedics
Gynae Block
Ward 10Urology
Diagnostics
Tay WardMfE
Stroke Ward MfE
Acute Medical Admissions
PSI Surgical Admissions
PSI P
atie
nt L
ift
PSI Patients Meet and Greet –via Level 3 Entrance
Known COVID +ve or displaying symptoms
> 8 days post COVID
Indeterminate COVID / no Pre-Surgery Isolation
Pre-Surgery Isolation Patient Elective Surgical Pathway
COVID-19 Elective Surgical PathwaysPerth Royal Infirmary
Day Surgery Admissions
DSU 1Specialty Dependent
CriticalDSU 2
Angus Health & Social Care Partnership
COVID 19 Mobilisation Plans – The Next Phase
22nd May 2020

Executive Lead Gail Smith Chief Officer (Interim) 07740937659
Operational Leads George Bowie Head of Health and Community Care (South Angus) 07554110036
Jillian Galloway Head of Health and Community Care (North Angus)
(Interim)
07775220442
Bill Troup Head of Adult Mental Health 07990920958
Financial Lead Sandy Berry Chief Finance Officer 07896045738
Clinical Lead Dr Alison Clement AHSCP Clinical Director
Nursing Lead Karen Fletcher AHSCP Lead Nurse 07966367674
Staff Side Barbara Tucker AHSCP Staff Side Rep
Nicola Owen Unison
Kenny Forbes Unison

Generic Pandemic Actions
Status
Recovery
Phase
Action Owner Live Ongoing Complete
Agree prioritisation of return of normal services Chief Officer √
Prepare for any possible future wave of influenza pandemic Chief Officer √
Continue pandemic specific vaccine vaccination campaign Chief Officer √
Review previously identified vulnerable groups Chief Officer √
Ensure physical rest/emotional support for staff Chief Officer √
Identify lessons to be learned Chief Officer √
Maintain communications to partners, staff, patients and public Chief Officer √

Angus Health and Social Care Partnership – COVID-19 Mobilisation Plan – The Next Phase
This document describes Organisational and Service Plans that support the overarching plan.
Categories – Partnership / Health / Social Care / Independent Providers / Third Sector
ORGANISATIONAL MOBILISATION – THE NEXT PHASE - PARTNERSHIP
Service Action Status / Target Dates
Lead Officer Update Financial Impact (per month)
Theme
Management Local Silver / Bronze groups in place Ongoing Chief Officer and local leads
N/A
Data Continue to capture Services and redeployment update info as required
Ongoing All N/A
Meetings Continuation of business critical meetings including Executive Management Meeting, Strategic Planning Group, IJB etc
Ongoing Executive Management Team
N/A
Premises Support agile working where possible and use of digital platforms for meetings as required
July 20 Heads of Service
TBC - more detailed plans to be developed
Work with clinical services and estates to identify footprint requirements as a result of COVID 19 new ways of working
July 20 Service Leads TBC - more detailed plans to be developed
Learning Capture the learning from COVID-19 to help inform new ways of working and
May 20 Heads of Service
N/A
Workforce Resilience Ensure staff have access to health and well being support
Ongoing Heads of Service
TBC - more detailed plans to be developed
Ensure plans in place for the partnership to increase respond to
Ongoing Heads of Service
TBC - more detailed plans to

any further peaks of COVID over the next 12-18 months
be developed
Financial Planning/Monitoring
Continue to log all relevant costs and developing financial plans
Ongoing Chief Finance Officer
N/A
Financial Planning (non COVID-19)
Accept slippage on Improvement and Change Actions
Ongoing Chief Finance Officer
Bespoke profile now agreed. C£44k/month
Primary/Secondary Care Interface
Ensure representation at Primary/Secondary Care relevant interface groups
July 20 Clinical Director
N/A
Establish local oversight group for supporting care homes
May 20 Chief Officer/Chief Social Work Officer
N/A
Ensure clinical priorities as identified are included in service planning priorities
July 20 Heads of Service, Lead Nurse and Clinical Director
N/A
Public Health Flu Vaccination Planning Ongoing Primary Care Manager
N/A
Communications Continue to send out briefings to ensure all staff are kept up to date
Ongoing Sally Wilson £1k/month
Ensure regular updates on AHSP website and Facebook as required
Ongoing Sally Wilson N/A
Responding to press enquiries when required working closely with NHS Tayside and Angus Council to ensure continuity of messaging
Ongoing Sally Wilson N/A
Digital Working Support the expansion of remote consulting across primary and secondary care using Near Me
Ongoing Sally Wilson TBC - more detailed plans to be developed
Support expansion of TEC for remote/home monitoring etc
Ongoing Sally Wilson £5k for 6 months
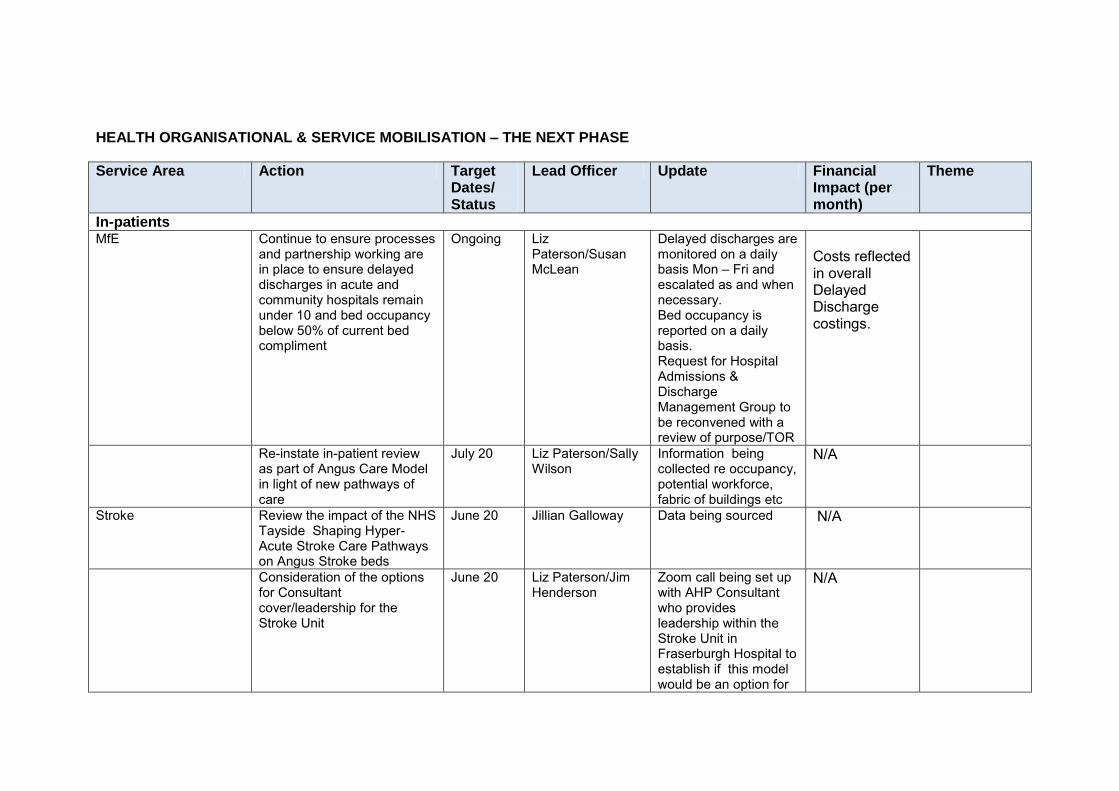
HEALTH ORGANISATIONAL & SERVICE MOBILISATION – THE NEXT PHASE
Service Area Action Target Dates/ Status
Lead Officer Update Financial Impact (per month)
Theme
In-patients MfE Continue to ensure processes
and partnership working are in place to ensure delayed discharges in acute and community hospitals remain under 10 and bed occupancy below 50% of current bed compliment
Ongoing Liz Paterson/Susan McLean
Delayed discharges are monitored on a daily basis Mon – Fri and escalated as and when necessary. Bed occupancy is reported on a daily basis. Request for Hospital Admissions & Discharge Management Group to be reconvened with a review of purpose/TOR
Costs reflected in overall Delayed Discharge costings.
Re-instate in-patient review as part of Angus Care Model in light of new pathways of care
July 20 Liz Paterson/Sally Wilson
Information being collected re occupancy, potential workforce, fabric of buildings etc
N/A
Stroke Review the impact of the NHS Tayside Shaping Hyper- Acute Stroke Care Pathways on Angus Stroke beds
June 20 Jillian Galloway Data being sourced N/A
Consideration of the options for Consultant cover/leadership for the Stroke Unit
June 20 Liz Paterson/Jim Henderson
Zoom call being set up with AHP Consultant who provides leadership within the Stroke Unit in Fraserburgh Hospital to establish if this model would be an option for
N/A

Stracathro
POA Continue to work across POA Tayside to manage admissions particularly in relation to covid to minimise risk of spread.
Ongoing Mandy Warden N/A
Continue to manage beds across Tayside to manage admissions safely due to increased demand
Ongoing Mandy Warden
Continue work where possible on improving the discharge pathway to help capacity and flow
Ongoing Mandy Warden
Continue to work towards minimal delayed discharges
Ongoing Mandy Warden
Supporting staff with resilience and mental health issues as the pandemic continues over a longer period – adapting to change and acknowledging the stressors that are attached to this
Ongoing Mandy Warden
Work to develop new ways of using technology to support patients and families – ie decision making/visiting/keeping in touch
Ongoing Mandy Warden
Continue with improvements Ongoing Mandy Warden
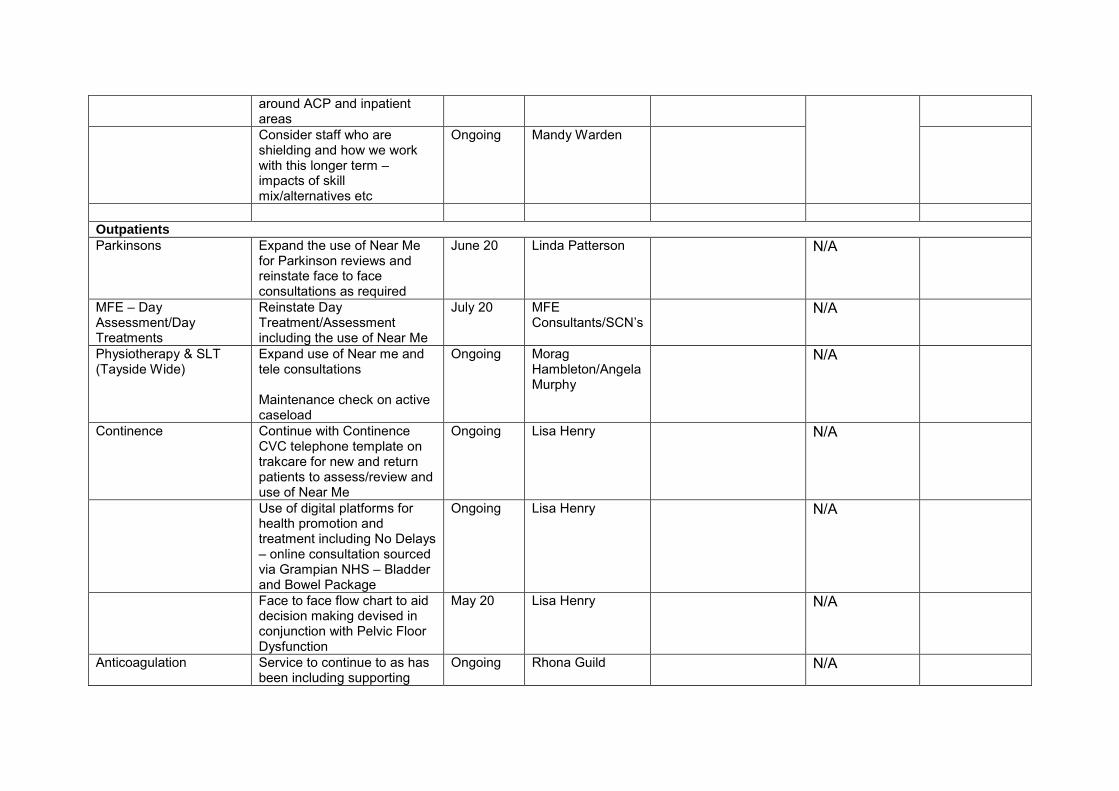
around ACP and inpatient areas
Consider staff who are shielding and how we work with this longer term – impacts of skill mix/alternatives etc
Ongoing Mandy Warden
Outpatients
Parkinsons Expand the use of Near Me for Parkinson reviews and reinstate face to face consultations as required
June 20 Linda Patterson N/A
MFE – Day Assessment/Day Treatments
Reinstate Day Treatment/Assessment including the use of Near Me
July 20 MFE Consultants/SCN’s
N/A
Physiotherapy & SLT (Tayside Wide)
Expand use of Near me and tele consultations Maintenance check on active caseload
Ongoing Morag Hambleton/Angela Murphy
N/A
Continence Continue with Continence CVC telephone template on trakcare for new and return patients to assess/review and use of Near Me
Ongoing Lisa Henry N/A
Use of digital platforms for health promotion and treatment including No Delays – online consultation sourced via Grampian NHS – Bladder and Bowel Package
Ongoing Lisa Henry N/A
Face to face flow chart to aid decision making devised in conjunction with Pelvic Floor Dysfunction
May 20 Lisa Henry N/A
Anticoagulation Service to continue to as has been including supporting
Ongoing Rhona Guild N/A

those who are shielded.
POA Community Services (Out patients/CMHT/PDS/DLT
Redeploy staff back into their own teams and areas
June – August 20
Mandy Warden/Susan McLean
N/A
Review buildings and layouts to promote safe working and social distancing
June 20 Mandy Warden/Susan McLean
Implement Near Me Produce a plan/risk assessed/triage based for determining which type of contact and when i.e. telephone/near me/face to face
July 20 Mandy Warden/Susan McLean
Collaborate with colleagues Tayside wide to agree a model for cognitive/neuro testing for Near Me Work with partners to ensure services including respite and carer support are re-established/enhanced
July 20 Mandy Warden/Susan McLean
Map out potential increases in referrals due to impact of covid 19 on our population and new/increased mental health needs
June 20 Mandy Warden/Susan McLean
Re visit small tests of change re diagnosis in primary care – different now due to covid – but appetite still there.
June 20 Mandy Warden/Susan McLean
Community and Primary Care
Community Nursing Restart LTC reviews for Ongoing Liz Murray N/A

patients on caseloads. Continue to support Care Homes as required
PCIP Continue to progress plan and ensure alignment with developing opportunities as a result of COVID
Ongoing Rhona Guild N/A
First Contact Physiotherapy - Tel/Near Me and face to face only if necessary Increased capacity from mainstream physio outpatients to now cover all Angus practices.
Mid June-August 20
Rhona Guild N/A
Year Three Plan to be presented to LMC/IJB in June for approval, taking into account national guidance and impact of Covid covering:
Vaccine Transformation
Pharmacotherapy
Community Treatment and Care
Urgent Care
Additional Services- MSK
Additional Services- Mental Health
Social Prescribing/Links Workers
June 20 Rhona Guild Vaccine Transformation- programmes prioritised for delivery with exception of school age children programme which is currently suspended Pharmacotherapy- plans in place to test a hub model in NE Angus and final round of recruitment proposed
Community Treatment and Care- Ear Care suspended due to Covid with only urgent cases managed. Leg ulcer service continued in SE/SW but > in home based service
N/A
due to Covid. Planning meeting to conclude roll-out plans planned Urgent Care- SAS service suspended due to Covid. Discussions planned to conclude roll-out plans. Additional Services- MSK- interviews held to recruit last 3 wte posts 19/5. Service expanded SE/SW with roll out to NW/NE planned over next 4 weeks. Additional Services- Mental Health- contracting process concluding. Providers issued contracts this week. Following recruitment of staff services will be rolled out. Social Prescribing/Links Workers- full recruitment of team. Induction ongoing. Planning underway to implement services in each area.
Long Term Condition Management
Generic Self-Management Support
Rhona Guild
N/A

Resource collation of resources available to support people living with LTCs in their own home during pandemic Respiratory Service: Reintroduce services using digital support where appropriate. Reintroduce 1:1 face to face reviews where required. Testing of options for modified delivery of pulmonary rehabilitation, in collaboration with colleagues across Tayside. Fatigue Management: Testing of 1:1 Fatigue Management support (OT service) using group session manual, with telephone and Near Me support/review. Generic Self-Management Support Resource collation of resources available to support people living with LTCs in their own home during pandemic
June 20 May 20 June 20 Ongoing Ongoing May 20

Diabetes Test of remote access to an education and behaviour change programme regionally for newly diagnosed Type 2 Diabetics
May 20
General Practice (Angus)
Continue to support increased use of digital solutions within practice in line with agreed regional strategy
Ongoing Rhona Guild TBC - more detailed plans to be developed
Support ACP Ongoing Rhona Guild/Alison Clement
N/A
Ensure capacity and capability in workforce to respond to the needs of the practice population including supporting Community Assessment Centres/COVID pathways in practice
Ongoing Rhona Guild/Alison Clement
TBC - more detailed plans to be developed. May be part of a national response.
NHS Tayside Primary Care
Support whole system working with care centred around patients according to agreed national and local priorities through strong representation at existing interface groups including silver zoom, OLT, elective care board (includes outpatients) and unscheduled care board (includes care home improvement)
Ongoing Jane Bruce/Alison Clement/Jillian Galloway
N/A

Clinical Pathway development for COVID with comprehensive pathways for COVID including palliative care in the community and community assessment centres. These allow clear guidance for primary care on provision of services within their own practices as appropriate with less reliance on community care and treatment services. Plans are in place to continue clinical pathway work across non-COVID work now.
Ongoing Jane Bruce/Alison Clement
N/A
Development of escalation and de-escalation plans which take into consideration of whole system and agreed clinical pathways for patients.
July 20 Jane Bruce/Alison Clement
N/A
Support for review of patients on waiting lists according to priorities as needed e.g. radiology waiting list to ensure patients are prioritised according to clinical need including for suspected cancer.
July 20 Jane Bruce/Alison Clement
N/A
Workforce is supported through daily METs reporting within partnerships for issues and staff testing as needed.
July 20 Rhona Guild/Alison Clement
N/A
Development of healthcare premises to support safe ingress based on best evidence.
June 20 Alison Clement TBC - more detailed plans to be developed. May be part of a national

response.
Community Optometry – Independent Contractors
Increase capacity of the Emergency Eye Treatment Centres
July 20 Ross Henderson TBC - more detailed plans to be developed.
Expand use of remote triage and consultations using either Near Me or telephone consultations
July 20 Ross Henderson TBC - more detailed plans to be developed.
Independent Dental Practitioners
Continue to contribute and increase capacity in Urgent Dental Centres across Tayside
June 20 Morag Curnow TBC - more detailed plans to be developed.
Participate in planning re re-establishing face to face contacts within Dental surgeries for routine examinations and non AGP procedures
July 20 Morag Curnow TBC - more detailed plans to be developed.
Community Pharmacy – Independent Contractors
Work with contractors to increase the numbers and management of repeat prescriptions
July 20 David Coulson N/A
Support the roll out of the NHS Pharmacy First Scotland service across Tayside
July 20 David Coulson N/A
Unscheduled Primary Care (OOH & MIIUs)
Establish working group with ED/OOH/Peadiatrics/NHS 24 to review pathways and calls to OOH and ED attendances
July 20 Lisa Prudom/ OOH Clinical Leads
N/A
Redesign operational and rotas to support continuation of triaging calls
July 20 Lisa Prudom/ OOH Clinical Leads
N/A
Implementation of Near Me June 20 Lisa Prudom/Pauline Kelly
N/A
Review MIIU provision in Angus along with GP OOH based at Arbroath as part of
On going Lisa Prudom/Catherine Carrie/Clinical
N/A

second phase of Angus Care Model
Leads
Additional Support to IONA service which will also provide additional support to care homes
July 20 Lisa Prudom/Catherine Carrie
N/A
Community Assessment Centres
Review demand of CACs (both telephone and face to face assessment) and consider model of delivery for the next 3-6 months
May 20 Sandy Berry/Jane Bruce/ Alison Clement/Hamish Dougall/Jillian Galloway/ Jaime Lyon/David Shaw
Paper being drafted for NHS T Silver Zoom
TBC - more detailed plans to be developed
Work with HSCPs and Secondary Care to review footprint required to support returning of other services/elective work
June 20 Jane Bruce N/A
Palliative Care Continue to deliver Palliative &End of Life Care across Angus Community Hospitals.
June 20 Elaine Colville Senior Nurse for Palliative Care is delivering training from the NHS Tayside COVID 19 website in collaboration with Tayside Specialist Palliative Care Services. Care experience interviews are ongoing Plans in place to resume Palliative End of Life Care Action Plan & Implementation Group in a virtual format
N/A
Community AHPs Physiotherapy/OT Community rehab team (including ECS, comm.
Support increased access to assessment and rehabilitation to support prevention of admission and step
Ongoing Morag Hambilton/Angela Murphy
N/A

Hosp, GP referral) And Speech and Language Therapy Tayside.
down/discharge from hospital
Forensic Medical Services and Custody Healthcare
Continue with business as usual with provisions made for people coming into custody displaying or reporting covid symptoms. Staff wearing appropriate PPE when seeing patients
Ongoing Dawn Wigley/Angela Cunningham
N/A
Review workforce planning to ensure appropriate staffing levels to meet the needs of the services
June 2020 Dawn Wigley/Angela Cunningham
N/A

MENTAL HEALTH – ORGANISATIONAL & SERVICE MOBILISATION – THE NEXT PHASE
Service Area Action Target Dates/ Status
Lead Officer
Update Financial Impact (per month)
Theme
Community Mental Health Services (CMHS)
Tayside SBAR categories of care to be utilised to support planning.
NA Bill Troup Only limited services were stopped – face to face groups and routine medical appointments.
N/A
Resuming scheduled Services
Community Mental Health Services (CMHS)
Communicating with patients on waiting lists
NA Operational managers
Letters sent to patients to
advise them of changes to
service, contact numbers
etc.
Patients on waiting list
contacted and reviewed
regularly based on need/
risk.
Clear flowchart used if
patients uncontactable .
N/A
Community Mental Health Services (CMHS) Angus Integrated Drug and Alcohol Recovery Service (AIDARS)
Supporting early discharges when
this is safe.
Collaboration with 3rd
sector and care
home providers for service provision
and planning.
Implementation of Mental Health and
Wellbeing Peer Worker service in GP
Practices expedited
Increase in demand for
commissioned and statutory services
likely. Monitoring this with Third
July 2020
Terry Irvine.
Capacity and flow

sector
Community Mental Health Services (CMHS) Angus Integrated Drug and Alcohol Recovery Service (AIDARS)
Further testing and evaluation of technology. Consider ‘champions’ to support staff buy in and service delivery. A National review and evaluation of the effectiveness of NearMe technology would be appreciated
Review July 2020
Bill Troup N/A NearMe and use of technology
Community Mental Health Services (CMHS)
Promote Online Mental health and Wellbeing information
Review Psychological Therapies Lead.
Mental health and wellbeing pages on AHSCP website - advice & signposting to local & national organisations. NHS Tayside COVI19 mental health and wellbeing microsite. NHS 24 staff MH&W info See psychological therapies
N/A
COVID19/ Non COVID19 pathways of care
Review July 2020
Bill Troup AHSCP flowcharts used for pathways of care.
N/A
Community Mental Health Services (CMHS) Angus Integrated Drug and Alcohol Recovery Service (AIDARS)
Social distancing. Analysis of buildings, processes and social distancing control measures is being undertaken. NHS Tayside guidelines in draft form.
Review 2020
Bill Troup N/A
Community Mental Health Services (CMHS)
Staff wellbeing
Implement rest, relax, recharge.
July 2020 Bill Troup TBC - more detailed plans to
Angus Integrated Drug and Alcohol Recovery Service (AIDARS)
Staff wellbeing supports publicised
and promoted.
Coaching availability increased.
Weekly staff bulletins.
Provision of staff Break Out rooms in
Whitehills and Gownlea
be developed

ADULT SOCIAL CARE – ORGANISATIONAL & SERVICE MOBILISATION – THE NEXT PHASE
Service Area Action Target Dates/ Status
Lead Officer
Update Financial Impact (per month)
Theme
Resolve Delayed Discharge
Courts are not convening to consider Guardianship applications; consequently, nearly all delays are related to AWI work. NB numbers remain very small.
George Bowie
It is not possible to resolve this issue until the Scottish Court Service resumes business. It has not yet been necessary to use 13 ZA powers under CV legislation but that is a possibility (any use must be agreed by SG and MWC).
c£16k/month
Care Management A review of care management functioning in light of CV 19 was conducted 5-5-20 covering preceding two weeks. This covered all adult social work services. It also included Adult Protection. This was satisfactory, and will be repeated at 6 weekly intervals.
Ongoing George Bowie
Accessing peoples’ homes during lockdown is presenting challenges but care managers are showing flexibility and adaptability in managing this.
N/A
Adult Protection Ensure continued effective functioning of AP systems. (See above)
Ongoing George Bowie
Statutory duties remain as pre-CV 19 outbreak and these will continue to be implemented, including use of LSIs in care homes where required.
N/A
Older People – Residential Care Home
Considering options to expand
capacity Developing options
though not required to date and
N/A

Now assuming not required based
on current trajectories.
Can be revisited if mass testing in
care homes reduces staffing
availability. Redeployment bronze
group is monitoring.
Ongoing.
George Bowie
Physical and Learning Disability
Considering whether some LD day provision can be restarted with social distancing and PPE.
Timescale will depend on SG decisions about lifting lockdown and restrictions on vulnerable groups.
George Bowie
Enactment is not yet feasible but planning for reintroduction is proceeding. Note; staff from ADCs have been redeployed to residential care and mass testing may reduce available staff in residential setting. It will be necessary to make decisions about where we allocate these staff (i.e. prioritisation.)
TBC - more detailed plans to be developed

INDEPENDENT SECTOR – ORGANISATIONAL & SERVICE MOBILISATION – THE NEXT PHASE
Service Area Action Target Dates/ Status
Lead Officer
Update Financial Impact (per month)
Theme
Residential sector-general
Sustain joint approach to problem solving in terms of staff availability, PPE, admissions, visiting, AWI, and testing.
New procedures for quality monitoring in care homes being implemented w/b 18-5-20
George Bowie
N/A
Executive Oversight Group will be supported by multi-agency Angus operational group providing data per care home and analysis thereof, as well as recommendations for action. RAG status information re infection control will continue. Joint visits between social work and DPH will take place to failing care homes for assessment and action.
George Bowie
N/A
Older People – Residential IIC
Normal arrangement applies in South but commissioned service in North could be enhanced for step down if provider willing/able. Priority may be given to DD. Work to review IIC contracts underway.
Ongoing George Bowie
AC Procurement team with operational managers have produced options for consideration. NB this is not a CV 19 response but indicates the end phase of existing contracted provision. CV 19 may delay procurement process but extensions are permitted.
N/A
THIRD SECTOR – ORGANISATIONAL & SERVICE MOBILISATION – THE NEXT PHASE
Service Area Action Target Dates/ Status
Lead Officer
Update Financial Impact (per month)
Theme

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 1 of 13
Dundee Health and Social Care Partnership 2.2
Overview of COVID19 Mobilisation Plan May 2020 to Support NHS Tayside’s Response
Dundee HSCP have not yet experienced the same plateauing of demand that has been apparent in the acute sector and, in some areas, such as care home provision, we are continuing to experience the need to further enhance COVID-19 related supports and responses. Expert advice and modelling has not yet extended to provide a full system perspective, including likely future progression of the pandemic and related demands within community settings. For these reasons our work to develop recovery plans is necessarily at a different stage to that of NHS Boards. The Partnership is committed to progressing recovery planning that focuses on protecting our capacity to respond to the virus, alongside a commitment to recovery of non-COVID related supports and services and, over the medium to long-term, implementation of strategic and commissioning priorities. Our recovery planning process has begun with delegated services considering learning from the first phase of COVID response and identifying priorities for phased recovery moving forward. We anticipate having our first draft recovery plan available for discussion with partners by w/b 8th June 2020. We note that John Connaghan’s letter advises the establishment of interface groups with primary/secondary care to support whole system recovery and look forward to receiving details of the intended approach to this in Tayside. We will welcome the opportunity to share and discuss our emerging recovery plan with this group to enhance discussions that are already taking place at the interface between acute / primary / secondary care at a service specific level. John Connaghan’s letter references a small number of specific priority areas that fall within the services delegated to HSCPs: 1 Mental Health Services Mental Health Services is the broad term used to describe the Dundee Community Integrated Mental Health and Learning Disability Services and the hosted Tayside wide services of Psychological Therapies Service, Multidisciplinary Adult Psychotherapy Service, Veterans First Point, Tayside Adult Autism Consultancy Team and Tayside Eating Disorder Service. Emergency, urgent and routine mental health services have continued with the exception of those aspects of care and treatment which involved people congregating together (for example, Day Hospitals, respite care or group treatments). Individuals so affected have instead been offered individual support. The following document outlines the principles that have been employed to ensure that services have been as safe as possible for service users and staff.
Guidance 16th April
Version 5.docx

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 2 of 13
The following document details the further risk-based scaling back of services that would have happened should the level of staff absence and/or deployment to other areas having been required. This will continue to be the principles used in the face of further waves of COVID-19.
COVID 19
categories.docx 1.1 General approach to people already in treatment Two main contextual factors are important in understanding the service delivery during COVID-19. Firstly, existing staff shortages (particularly Consultant Psychiatrists) meant that a very significant number of service users were already waiting further out-patient review or allocation to CMHT based staff. Secondly, a number of staff were considered to be in shielding category for their own health and wellbeing (or that of their families) and could fulfil only limited roles. Service users already in treatment were assessed by the clinical staff providing their care and treatment and categorised as “suitable for telephone care and treatment / support” or “requires face-to-face care and treatment/support.” It is reasonable to say that we have endeavoured to provide a continuation of care and treatment; the changes being in the ways this has been delivered. The use of Near Me consultations has been modest, consequent to lack of availability of suitable devices such as cameras and/or functioning laptops. A very small number of service users indicated that they preferred treatment to be placed on hold until after they could more safely attend face-to-face appointments. A Dundee Discharge Hub was established to provide additional support for people around the transition from in-patient and Intensive Home Treatment to ‘ordinary’ levels of community care. Group treatment approaches such as Survive and Thrive and STEPPS and the use of Behaviour Family Therapy have stopped but where this has happened, people have moved to telephone support. A much lower level of support has been afforded to those awaiting appointments or intervention. However, an enhanced level of Duty Worker support was put in place such that people calling in could be afforded an equivalent telephone appointment. Communication was given/sent to all active patients explaining the arrangements for service delivery and signposting to resources. This has been enhanced by the development of resource pages within the respective Council websites and the NHS Tayside internet site.

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 3 of 13
1.2 General approach to people awaiting first appointment All mental health services have continued to accept referrals with unchanged eligibility criteria. Following some initial increases in referrals rates, there has been a small reduction in referrals. Referrals have been subject to the same processes as in pre-COVID times where waiting times meant that routine waits might be substantial. The total number of people waiting for services is considerable. The process of writing out to people has therefore been approached in a ‘batched’ way. Communication explaining the arrangements for service delivery during COVID-19 and signposting to resources was dealt with in this way. This has been enhanced by the development of resource pages within the respective Council websites and the NHS Tayside internet site. MHO services have continued to deliver all Mental Health Act functions with a reduction in Adults with Incapacity function as determined by the decisions to reduce work at Court level. Face-to-face Detention of service-users in community settings with MHO and Section 22 Approved Psychiatrists have taken place where necessary. Supports available at a primary care level have been enhanced with the implementation of Social Prescribing across all GP practices (previously limited to practices in a more limited number of deprived areas). 1.3 Implementation of Virtual Team Working & Clinical Service Delivery During the Next Phase Mental health staff largely have access to desktop computer equipment without camera and/or soundcard in shared office space. Whilst the use of Zoom has proved very successful for meeting purposes (although often reliant on people using mobile phones), the use of Near Me has been much more limited. There are only a limited number of camera devices in clinical areas although the local implementation team have been very efficient in registering all staff who ask for access.
• Capacity of IT equipment will require to be increased significantly to support future arrangements. Both DCC and NHS Tayside are working to provide against the Services initial needs assessment, this will be ongoing.
The nature of treatment within mental health means that there will always be a significant number of people for whom face-to-face treatment represents the safest and most effective approach. 1.4 Making Online Mental Health and Wellbeing Information and Support Available for Staff
and the Local Population Both local Council and NHS Tayside websites have clear mental health and wellbeing advice; for staff and service users. Staff in a range of disciplines within the mental health family have written and produces online videos to support wellbeing and direct people to trusted resources.

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 4 of 13
1.5 Modelling Likely Future Demand for Mental Health Services There are three component parts to this work.
• Firstly, strategic planning and commissioning of services to cope with increased population demands for mild-moderate anxiety and disorders and mood disorders.
• Secondly, work to address an increase in waiting times as those currently in treatment are likely to require longer-than-expected treatment episodes causing reduced throughput.
• Thirdly, work to address the provision of mental health treatments to those staff across acute, community and care home settings who have been adversely affected by dealing with COVID-19 patients and patient death.
It is likely that all three will require additional resources if increases in waiting times are to be avoided, further detailed modelling is in process. It is unlikely that Distress Brief Interventions (DBI) will impact on this core cluster of work but will provide an excellent source of help and support for people presenting with high levels of distress. 1.6 Modelling Future Service Delivery The Scottish Government have outlined a four phased approach to the lessening of restrictions. Mental health services are outlined as being with Phases 1 and 2. However, the services that require people to congregate together for care and treatment will require to wait until at least Phase 3. Given the outline above that we have attempted to continue to deliver our key functions, the main changes to be implemented are the balance between remote and face-to-face contact with service users and carers. This will be critically influenced by:
• The availability of space for staff where they can be socially distanced • The availability of waiting area space for service users where they can be socially
distanced • The availability of public transport • The end point of shielding arrangements for staff
It is likely that all services will be required to consider changed patterns of working (for example, evenings and weekends) to be able to accommodate any significant increase in face-to-face appointments. The framework that will be used with regard to the above will be:
• All staff will review existing caseloads and categorise these on the basis of clinical need to transition back to face-to-face care. This will be bases of the 4 Categories of care as outlined in the document embedded above. An additional step to this will be making a judgement as to whether clinic or domiciliary visits are appropriate AND which of these represents the lowest level of COVID-19 risk to service users, carers and staff
• Each clinical area will be reviewed to determine the safe capacity for face-to-face appointments
• There will then be a gradual transition over of those with greatest clinical need, even where that means different services working across clinic settings ‘belonging’ to other service components.

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 5 of 13
• There will be continued support for the use of NearMe where clinically appropriate and acceptable for service users. It must be noted that Dundee City has high levels of deprivation and NearMe is not free (there being ‘hidden costs’ to this in WiFi availability).
1.7 Social Models of Support The provision of day type supports for people with learning disabilities and mental health challenges will require a careful and small stepped approach.
• A risk based approach will continue to identify those people who are potentially most vulnerable in order that support can be provided in a more personalised way.
• It is envisaged the use of buildings for group support will, in most areas, reintroduce at a stage beyond the end of July.
• For people with profound and multiple disabilities current planning would suggest that the commencement on a phased reintroduction may be possible at an earlier stage.
• Staffing capacity to support more flexible and potentially extended hours, will require to be created. Continued ability to use overall resources creatively with voluntary sector partners will be necessary, systems are in place to support process
• Respite provision will continue to be available albeit with revised standard operating procedures and contingency arrangements. A detailed draft plan is already in place.
• Resource requirements to support people who face barriers to employment over the next 18-24 months is currently being assessed to ensure there is capacity to increase tailored approaches, particularly for those furthest away from employment.
• Use of housing stock / void properties will continue to be used creatively to reduce unnecessary delays in hospital and support vulnerable people within the community.
• MHO capacity has continued to meet demand to date, however planning is underway to ensure no undue delays in responding to a backlog of Adults with Incapacity activity arising from current restraints.
1.8 Staff Wellbeing In addition to the COVID-19 response to staff support described above, for ‘front-line’ staff, there will be a continued focus on provision of accurate and clear information to guide day-to-day practice. There is Staff Partnership involvement on twice weekly leadership team teleconference calls and on Mental Health Bronze and Silver Command Structures. This includes:
• Staff supervision has continued – although moved to virtual meetings where necessary, with this viewed as a key component of staff support.
• There is a wealth of on-line resources for staff wellbeing and counselling available through OHSAS.
• Psychological Therapies Services had delivered resilience training to very large numbers of acute care staff with this now moving across to mental health settings.
• Staff RRR rooms will be implemented although most service team bases are already overcapacity and the small size of shared offices will create a need for meeting rooms and clinic space to be used to house staff.
• All managers will be required to complete the TURAS based learning about staff well-being and all staff encouraged to complete the appropriate psychological first aid learning.
• There is an established supply chain and adequate supplies of PPE in all areas and a nominated Service lead for co-ordination and governance purposes. This extends to
NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 6 of 13
support/escalation process for partners within voluntary/independent sector mental health and learning disability services locally.
2 Primary Care We are providing information that specifically relates to aspects of primary care provision delegated and managed by DHSCP, we anticipate that this will supplement / support content related to primary care submitted to you through other routes. 2.1 Treatment Room Services Treatment room services are normally delivered in practice in Dundee and we do not have a centralised treatment room service. The evolving care and treatment services team has been developing over the last 18 months to look at shifting that work and some aspects has rolled out to some clusters. With Covid 19 further support was offered for key areas, where the clinical need was urgent, or practice staffing was impacted in a way that meant they could not deliver time critical care. This included DMARDS, other urgent bloods and injections such as B12. Next steps
• Work with clusters and GP sub to review key areas which can be resumed in practices as their staffing base stabilise.
• In tandem work as part of Primary care improvement planning to continue to develop the care and treatment services team to increase capacity to allow more of this work to move from practices.
• Progress TUPE discussions to assess if some practice staff can be employed via Dundee HSCP to expand the team.
• Continue to support practices when staffing destabilises, recognising there may be further peaks of Covid activity which will impact on this.
• There is an ongoing need for appropriate space. 2.2 MSK Care A significant amount of initial MSK care has moved to be a core part of First Contact Physiotherapy Services (FCP), closely integrated with and based in general practice. During the Covid phase the team have expanded to clusters 2 & 4 which were not previously supported. Utilisation of the service was initially low, due to reduced numbers of patients presenting via their GP practice. The service operates a Virtual First approach, contacting patients by telephone, via NearMe and only face to face as required. The MSK team have developed support for staff at this time point, recognising the impact of working in a Covid environment. This will continue to be delivered at present but will be reviewed across Tayside in due course. Next steps: Development over next 2 months Increase FCP sessions in June and July to continue to support all practices in Dundee on an ongoing basis. 25 sessions per week from 25th May, 33 in July.
NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 7 of 13
- Review of service delivery model planned – develop the flexibility in the team to include option of telephone / NearMe appointment as well as face-face appointments, in line with practice policy. This may encourage the hard to reach groups to utilise the service.
- Identify space to do this as the physio team were displaced by the Community/covid assessment centre in Dundee.
Resume normal services Long Term Conditions support and management
• Agree with clusters leads a plan to prioritise long term conditions reviews restarting so there is consistent support to patients across the city, while recognising the variation in practice populations
• Recognise the limited capacity of care and treatment services to support the monitoring element of this. Work with practices to look at available capacity, and develop longer term plans over the coming months.
• Continue to use technology to support care where feasible, while having appropriate environments for face to face contact where possible. Continue to ensure that ACP’s and self -management plans and care are a core part of care for those who are prioritised at this stage.
2.3 Adult Screening Programmes Once there is clarity from a national perspective on screening programmes this area will be progressed. This will include the need to prioritise certain groups of people, particularly for programmes in practice like cervical screening. Practices will work with PH and national colleagues to progress this. 2.4 General Practice Consultations As a response to the pandemic practices have reduced their footfall and embraced the use of technology to support patient care in a timely way. Contacts initially reduced significantly but this is now steadily increasing. National and local communications are key to ensure that people are aware that general practices services, particularly for acute issues, are in place as normal just being seen slightly differently. There has been an increasing use of Near Me technology in most Dundee practices over the past month in particular. • We will work with practices to support patient pathways of care to ensure that people can be
assessed and supported. This will continue to use phone both for initial triage and assessment, Near Me consultation, and as professional and public confidence increases with changes to lockdown face to face consultations will increase, but where they are required.
• There is a new system in place to support practices in Tayside to access PPE which will give confidence in face to face contact.
• We will start to scope over next 2 months how covid assessment can take place in clusters/practices and plan the premises work that will be required to deliver that model on an ongoing basis which is sustainable for some time.

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 8 of 13
2.5 Referrals to Secondary Care We will work with colleagues to review pathways that require referral to other parts of the system in both secondary and primary care, recognising the waiting lists which will be in place already. Work has taken place with radiology to prioritise those who are urgent on the waiting list. This is not appropriate for other specialties. 2.6 Anticipatory Care Plans Practice teams and the wider primary care team, have continued to develop and update ACCP’s, many of which were in place. Ongoing support has been provided for those by phone for those who were perceived to be more unstable clinically. This will continue, although as more routine reviews for LTC’s start then this will be integrated back into that process. 2.7 Shielded Patients Minimising contact while ensuring appropriate care for those in the shielding and high risk groups is a balance. Where possible those in these groups will be supported remotely, along with their carers. • For those in the shielded group our care and treatment services team are providing clinical
nursing care at home. We will review this with the team and practices to assess if we can move to a model of a “clean” and protected area in a cluster model which might be suitable for this.
• Where GP review is required face to face this will be done in the most appropriate setting for that individual. Again if “clean” areas are developed this may be the best environment longer term.
2.8 Infrastructure (including digital) Practices are actively reviewing how they best use their premises to work safely in a covid era. We will work with practices and wider teams who use the buildings to prioritise which services can safely be delivered in the next few weeks and months. From this we will be able to identify pressures and gaps. This is reliant on teams having the digital infrastructure and appropriate space to use it. We have worked with our colleagues in the digital team to roll out Near Me. Additional hardware is awaited which will allow a further expansion of this in the next 2 months. There will be work which will need to be carried out to maximise the use of the space we have, especially where we have open plan offices for teams. 2.9 Flow to Secondary Care Primary care teams, including GP’s, will take cognisance of the current pressures created by Covid when making referrals to specialist and secondary care services. Pathways have an ability to highlight higher priority patients. Thresholds for referral will be based on clinical assessment of relative risk, where a diagnosis is perhaps unclear. 2.10 Community Assessment Centre Dundee CAC will continue for the next 3 – 6 months while we develop a suitable model and premises to deliver within a cluster/local basis. A model which allows for safe staffing and ability to cope with
NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 9 of 13
the wide variation in numbers of people presenting will be finalised. This will allow a move with the reconfiguration of the current site to a smaller footprint, supporting the resumption of other services which have been displaced. We will work with colleagues in Angus and P&K as components of the Dundee service are Tayside wide. 2.11 Management of Prescriptions The pharmacy team will work with practices and patients to continue to implement more efficient and effective systems for prescription management. This will include increasing the number of people who have a registered/preferred pharmacy and an increase in serial prescriptions. The increase in this over the period to July will be limited given other pressures on the system with Covid. As part of practice development to triage and signpost to the most appropriate clinician to meet clinical need for an individual we will continue planning to develop the signposting materials we have available locally to ensure that we use all our clinicians and teams appropriately. This will include a range of materials which highlights the role of Pharmacy First. By July we will have scoped what these options are. 2.12 Care Homes General practice teams work closely with care home teams to provide support to those resident in the home. GP’s will continue to support residents care when required. Where possible this will be remotely, and will increasingly look to use Near Me to support this. This minimises footfall into care homes and the risks of introducing covid (given that GP’s will also be seeing patients who are likely to have Covid.) The development in Dundee of the care home team has supported a different approach to (urgent) care which fits well in the current climate. That model will continue where in place. It will not be able to expand to support other practices or care homes in the short term, but modelling going forward will take cognisance of this and we will review plans and trajectories in June/July. 2.13 Urgent Care Urgent care is critical and significant part of general practice work. This covers both on the day demand in practice and home visits. The development of the care home team as part of PCI development has been positive. This team are core to support care homes at the current time. The element of home visiting which was being developed was currently based on SAS advanced practice paramedics. These staff have been redeployed back to full time SAS work in the current pandemic. We will review with SAS over the next 2 months the likely progress of the current crisis and how some of this work can be reinstated. 2.14 Transport Transport solutions have been developed as part of the covid response. This has been really effective to transport patients to the CAC centre. Data clearly demonstrates that the number of people with suspected covid who had to be seen in practice because they could not get safely to

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 10 of 13
Kings Cross dropped when the transport service was introduced. We have previously discussed transport solutions, including as part of flu planning, as this could reduce demand for home visits which are time consuming. We will liaise with those who have developed the transport solutions to explore if this could be a realistic long term option to support practice workload. 2.15 Community Testing DHSCP has been engaged with ongoing discussions regarding arrangements for the maintenance of this function. It is our understanding that comprehensive planning information has already been provided by Kathryn Brechin and therefore we are making no separate return to you on this aspect of recovery planning. 3 Other Delegated Areas of Responsibilities Beyond these specific areas, other emerging recovery priorities relevant for the period to end of July 2020 are: 3.1 Community Based Health and Social Care • Work to support additional staffing capacity within Community Nursing Adult Services (15 WTE
registered nurses and 4 WTE HCSW) to sustain three COVID-19 positive / suspected pathways, alongside maintenance of essential nursing care for patients unaffected by COVID-19. This includes community based palliative care for both COVID and non-COVID patients.
• Continued implementation of Independent Living Review Team to review the number of packages of care in the community, to work with community care staff and contribute positively to support and enable earlier discharge for individuals from hospital, and to enable their independence in the home environment.
• Consider approaches to support the continued provision of social care services to those who are COVID positive and are shielding, including provision of PPE.
• Respond to increasing demand from people recovering from COVID who have experienced significant broader impacts on their physical and mental health, for example exacerbation of pre-existing long-term conditions.
• Move towards reinstatement of full assessment for all service users by care management teams. • Develop models to support reintroduction of day support taking into account social distancing
requirements. • Continued implementation of integrated community teams, building on progress made during
initial COVID-19 period. • Continue to implement enhanced support model for care homes. 3.2 Community Rehabilitation / AHPs • Rehabilitation is critical to ensuring our population’s recovery from the impacts of the pandemic
and the long-term sustainability of the health and social care system. AHPs are at the centre of shaping the rehabilitation agenda while working as part of the wider multidisciplinary and multiagency teams across all sectors. This collective approach is necessary as we anticipate an increase in the need for rehabilitation across four main population groups:

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 11 of 13
1. people recovering from COVID-19, both those who remained in the community and those who have been discharged following extended critical care/hospital stays 2. people whose health and function are now at risk due to pauses in planned care 3. people who avoided accessing health services during the pandemic and are now at greater risk of ill-health because of delayed diagnosis and treatment 4. people dealing with the physical and mental health effects of lockdown
• The rehabilitation needs of these at-risk groups are vitally important and need to be met as we collectively support people to recover, regain health and wellbeing, and reach their potential, and ultimately ensure we flourish as a nation.
• Continued development of Community Rehab model (anticipated timescale for implementation is September 2020) to enhance preventative approaches, reduce falls and POCS.
• Develop models to support reintroduction of elective surgery within discharge management and AHP functions.
• Implement single point of access for AHP services. • Implement post COVID rehab model. 3.3 Inpatient Services Medicine for the Elderly/Psychiatry of Old Age • Develop COVID BAU model within in-patients. • Develop COVID model in POA. 3.4 Centre for Brain Injury Rehabilitation • Develop transition from COVID-Rehab model currently in CBIR to a specialist rehab facility • Develop of inpatient management pathways to support further specialist community
rehabilitation 3.5 Palliative Care Services • Develop models of care that continue to link into Covid pathways across community and acute
care settings • Re-establish model for in-patient end of life care and management of condition support for
those with non-Covid conditions • Maintain a number of Covid+ beds for those with Covid 19 and for those who have non Covid
end of life conditions, but showing symptoms of positive for Covid 19 • Identify process to establish future provision of ongoing day care models 3.6 Drug and Alcohol Services • Review access pathways, including options for re-opening of direct access, taking account of
social distancing requirements. • Plan for long-term continuation MAT delivery to individual homes. • Enhance capacity to provide outreach services and respond to increasing demand from those
people whose drug use has started / escalated during lockdown. • Implement robust risk management approaches to support prioritised contact with service
users whilst lockdown / social distancing restrictions remain in place.

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 12 of 13
• Plan for the reinstatement of work to implement the Action Plan for Change, including whole system redesign activities.
3.7 Sexual Health • Move towards reinstatement of a number of sexual health clinics. This to include provision of
LARC which requires direct clinical intervention. This to be triaged non symptomatic patients within in-patient facilities.
• Identify further clinics which may continue to utilise virtual methodology • Identify and/or create clinical accommodation which can be used for clinical interventions with
Covid+ or symptomatic patients. • Identify staff requirements to support reintroduction of clinics whilst staff being re-deployed to
priority areas requesting specialist skills such as Test and Tracing. • Move towards reinstatement of partial sexual health contribution to service delivery models at
The Corner taking into account those that can utilise virtual methodology
3.8 Protecting People • Work with carer’s organisation to better understand the impacts of lockdown on their needs /
priorities and develop enhanced responses, including to carer stress. • Further develop our understanding of and response to hidden harm whilst lockdown restrictions
and social distancing remain in place across a range of vulnerable groups (including adults at risk, women experiencing domestic abuse and carers).
• Contribute to the development and implementation of TTIS approach, including planning for the potential impact on the health and social care workforce.
• Plan for continuation of support to people who are shielding (including those people who use drugs), in partnership DCC / Third Sector.
3.9 All settings • Continued expansion of use of NearMe in clinical settings. • Move towards reinstatement of a number of sexual health clinics. This to include provision of
LARC which requires direct clinical intervention. This to be triaged non symptomatic patients within in-patient facilities.
• Identify further clinics which may continue to utilise virtual methodology • Identify and/or create clinical accommodation which can be used for clinical interventions with
Covid+ or symptomatic patients. • Identify staff requirements to support reintroduction of clinics whilst staff being re-deployed to
priority areas requesting specialist skills such as Test and Tracing. • Move towards reinstatement of partial sexual health contribution to service delivery models at
The Corner taking into account those that can utilise virtual methodology • Maintain access to PPE and support the management of the local PPE Hub

NHS Tayside Mobilisation Plans: Next Phase: Dundee HSCP Page 13 of 13
4 Financial Framework The delivery of the next stages of the mobilisation plan will be funded through a combination of reconfiguration of existing HSCP budgets and additional funding from the Scottish Government to support the response to COVID19. This additional expenditure will continue to be reported back to the Scottish Government through the fortnightly financial returns including refining financial estimates of the future costs of service provision in partnership with the NHS Finance team. Version 3 Updated 22/05/2020

THERE ARE CHANGES TO THIS DOCUMENT FROM ISSUE 4
16th April 2020 (Issue 5)
Community Mental Health, Psychological Therapies & Learning Disability Services
Guidance for Service Provision During COVID-19
This guidance is intended to provide advice to staff of all disciplines with regard to how we will continue to provide safe and effective care, treatment and support to our service users and carers. This includes measures intended to protect staff and the wider responsibilities they may have out-with the workplace setting.
This guidance will be updated and reissued regularly. As you will be aware, the guidance being issued by the Scottish Government, Chief Medical Officer, NHS Tayside, Dundee City Council and the Dundee Health & Social Care Partnership has been – and will likely continue to be – changed on a regular basis. This does not mean that previous guidance was ‘incorrect’; simply that certain measures are being staggered and changes made on the basis of emergent trends and new information about COVID-19.
The duty of care we have as health and social care professionals means that the guidance issued to the general public will not always directly apply. However, that does not mean that the safety and welfare of staff is not of paramount importance.
Please take the time to read this document in its entirety before thinking through how the principles and recommended procedures apply to your work. Where you are unable to use this guidance to make decisions about your everyday work, please discuss this with your line manager who will be participating in regular briefings about responding to COVID-19.
Service users with a Learning Disability may not always be able to reliably report when they are experiencing symptoms indicative of COVID-19. Where corroborative information is not available from a carer or care staff, staff should work on the assumption that the service user is at high risk of having COVID-19.
The Scottish Government and other three Nations have agreed new guidance on the use of PPE. This guidance is extensive and covers a variety of clinical environments and situations.
The complete guidance can be accessed here and all staff should read this:
https://www.gov.uk/government/publications/wuhan-novel-coronavirus-infection-prevention-and-control/covid-19-personal-protective-equipment-ppe
This information will be summarised for our main clinical scenarios, within the main text of this document.
Please note that the guidance around the categories of people previously referred to as “at risk” and “at high risk” consequent to physical health conditions and recommended to exercise “stringent social distancing” as a result, has been updated. The “at high risk” group are now being referred to as “shielded patients.” These individuals will have received a letter from the Chief Medical Officer in the last week. This states that the safest course of action is to stat at home at all time and avoid all
face-to-face contact for at least twelve weeks, except from carers and healthcare workers who you must see as part of your medical care. For those living with other people, the other household members should minimise the time spent with the person in shared spaces (which should be well ventilated), keep 2m away, sleep in separate beds and use a separate bathroom if possible. Kitchenware and towels should be kept exclusively for use by the shielded person and cleaned/laundered at high temperatures.
The letter states that essential carers or visitors should continue to visit as long as they don’t have symptoms of COVID-19 and should exercise hand hygiene on arriving and during the visit.
The further PPE guidance issued since that letter advised more stringent measures than this and these are given below.
Section One – Services and Treatments Where A Number of Service Users or Carers Are Brought Together in Close Contact With Each Other and Staff
Examples of this include people attending Day Hospital settings and delivery of therapeutic group interventions in community mental health service and psychological therapy service settings.
The guiding principle here is that we will STOP bringing servicer users into these settings. Instead, each service must review the needs of each person attending the service/group and plan how else effective support will be delivered.
Wherever possible, that support will be delivered by telephone. However, we must recognise that a significant number of people we support may require face-to-face contact. Where this is required, please consider this person as falling under Section Three below.
Section Two – Community Patients Where Care, Support and Treatment Can Be Safely Delivered by Telephone
Examples of this include CMHT and psychological therapies service users who ordinarily attend our out-patient clinic settings for one-to-one appointments where service users are not considered to be at significant risk of harm to self or others and where mental state can be reasonably assessed over the telephone (that is, face-to-face observation will not add critical information to the assessment process).
The guiding principle here is that we will move to conducting appointments by telephone or, where available, using Near Me. Whether this level of support is sufficient for people should be kept under regular review and all service-users reminded of additional available supports such as Duty Worker systems for CMHT. Appointments should be pre-booked in order to align as closely as possible to the level of treatment and support normally afforded to people.
This approach can be used both with people who are asymptomatic and those experiencing symptoms raising suspicion of COVID-19 should they be well enough to participate.

Section Three - Community Patients With Low Risk of COVID-19 Where Care, Support and Treatment Can Only Be Safely Delivered by Face-to-Face Appointments in an Out-Patient Setting (but not those falling within the category of Stringest Social Distancing)
Examples of this include service users where there are significant concerns about assessing and mitigating risk of harm to self or others, where accurate mental state assessment requires direct observation or where service users are having their finances managed by the Local Authority.
Step One: telephone the service user in advance of the appointment (preferably the day before) and determine whether they have any of the following:
a) a persistent new cough and/or a fever
b) are living with anyone with a persistent new cough and/or fever or who is thought to be infected with COVID-19
c) are experiencing a loss of sense of smell
d) have been in close proximity with anyone within the last seven days where there is suspicion of that they have been symptomatic with COVID-19
Where the answer to all of the above is “no”, then ask the service user to attend their clinic appointment as scheduled. However, advise the service user that if they become unwell over-night or are exposed to category d) above, they MUST NOT ATTEND their appointment and must phone for further advice. Should this be the case, please begin to manage the patient using Section Four below.
Step Two: Conducting the out-patient appointment. Please ensure that you can collect your service-user from Reception as soon as they arrive. Reception staff will advise service-users to maintain a distance of 2m from any other waiting patient. The move to telephone contact for the majority of service users, should make this possible (that is, waiting areas should be less busy than usual). Hand sanitiser will be placed in Reception/waiting areas and people asked to use this on arrival.
During the appointment, please maximise the distance between the service user and yourself. The guidance for the use of Personal Protection Equipment (PPE) for out-patient appointments with service users without symptoms has been updated. This states that staff should don appropriate PPE equipment when seeing people unless there is good and specific risk assessed reasons not to. Staff should use hand washing or sanitiser before and after each appointment. Please see the end of this guidance for further information on PPE.
Section Four - Community Patients With Active Symptoms of COVID-19 or High Risk of COVID-19 or Falling Under the Category of Stringent Social Distancing Where Care, Support and Treatment Can Only Be Safely Delivered by Face-to-Face Appointments
Examples of this include service users where there are significant concerns about assessing and mitigating risk of harm to self or others, where accurate mental state assessment requires direct observation or where service users are having their finances managed by the Local Authority.

Step One: telephone the service user in advance of the appointment (preferably the day before) and confirm using questions a) – d) above that the service user is indeed at high risk.
Use this telephone call to determine whether there is an immediacy to see the service user or whether this can be delayed until the recommended isolation period is over (at time of writing 14 days from likely exposure or 7 days from development of symptoms). Where at all possible, delay the appointment but provide assurance that telephone support will be provided.
Where an appointment needs to take place, proceed to Step 2 below.
Where the potential risk to health and social care workers cannot be established prior to face-to-face assessment, the situation should be consider as High Risk for COVID-19.
Step Two: Service users falling into this category should NOT routinely be brought to a clinic setting. Instead, service users will be visited in their home environment. Staff undertaking these visits must wear appropriate PPE equipment and should maximise the distance between themselves and the service user. At the end of the visit, the PPE equipment must be bagged and left in the service-user’s own home environment. This must be left for at least 72 hours before being placed in the ordinary household waste. Staff should NOT remove this waste from the household.
Staff should use hand sanitiser both before and after the appointment.
Please also see the section at the end of this document relating to information from Health Protection Scotland.
Section Five – Community Patients Requiring a Depot Who Ordinarily Attend the Depot Clinic and Have Low Risk of COVID-19 and Do Not Fall Under the Category of Stringent Social Distancing
Step one: in advance of the appointment. Service-users scheduled to attend a Depot clinic should be contacted the day before they are scheduled to attend in order to determine whether they have any of the following:
a) a persistent new cough and/or a fever
b) are living with anyone with a persistent new cough and/or fever or who is thought to be infected with COVID-19
c) are experiencing a loss of sense of smell
d) have been in close proximity with anyone within the last seven days where there is suspicion of that they have been symptomatic with COVID-19
Where the answer to all of the above is “no”, then ask the service user to attend their depot clinic appointment as scheduled. However, advise the service user that if they become unwell over-night or are exposed to category d) above, they MUST NOT ATTEND their appointment and must phone for further advice. Should this be the case, please begin to manage the patient using Section Six below.

Step Two: Administering the depot. Please ensure that you can collect your service-user from Reception as soon as they arrive. Reception staff will advise service-users to maintain a distance of 2m from any other waiting patient. Hand sanitiser will be placed in Reception/waiting areas and people asked to use this on arrival.
During the appointment, please maximise the distance between the service user and yourself until the point of having to physically administer the injection. The guidance on PPE use for people presenting with low risk of COVID-19 has been updated. This states that staff should don PPE at a level additional to the PPE normally used for depot administration and use hand washing or sanitiser before and after each appointment. Please see the additional guidance on PPE later in this document.
Section Six – Community Patients Requiring a Depot Who Ordinarily Attend the Depot Clinic and Have Been Identified as Actively Having COVID-19 or at High Risk of COVID-19 or Fall Under the Category of Stringent Social Distancing
Step One: telephone the service user in advance of the appointment (preferably the day before) and confirm using questions a) – d) above that the service user is indeed at high risk.
There should be a presumption towards administering depots on the day that they are due. Administration of a depot to a service user actively unwell with symptoms of COVID-19 should be discussed with medical staff before administration. In this case, there should be a risk based analysis undertaken to determine whether the administration of the depot should be delayed. A delay of a longer than 48 hours will require medical staff to re-write the Kardex. If it is considered that there is not immediacy to administer the depot, this should be delayed until the recommended isolation period is over (at time of writing 14 days from likely exposure or 7 days from development of symptoms). Provide assurance that telephone support will be provided over the time.
Where an appointment needs to take place to administer the depot, proceed to Step 2 below.
Where the potential risk to health and social care workers cannot be established prior to face-to-face assessment, the service user should be treated as being at High Risk of COVID-19.
Step Two: Service users falling into this category should NOT routinely be brought to a clinic setting. Instead, service users will be visited in their home environment. Staff undertaking these visits must wear appropriate PPE equipment and should maximise the distance between themselves and the service user. At the end of the visit, the PPE equipment must be bagged and left in the service-user’s own home environment. This must be left for at least 72 hours before being placed in the ordinary household waste. Staff should NOT remove this waste from the household.
Staff should use hand sanitiser both before and after the appointment.
Please also see the section at the end of this document relating to PPE information and the more comprehensive information from Health Protection Scotland.

Section Seven – Community Patient Requiring a Depot Who Ordinarily Receive This In Their Home Environment at Low Risk of COVID-19 and Do Not Fall Under the Category of Stringent Social Distancing
Where service-users are in receipt of depot medication where this is ordinarily administered in their home environment, this arrangement should continue.
Step one: in advance of the appointment. Service-users scheduled to receive a Depot should be contacted the day before they are scheduled to be seen in order to determine whether they have any of the following:
a) a persistent new cough and/or a fever
b) are living with anyone with a persistent new cough and/or fever or who is thought to be infected with COVID-19
c) have experienced a loss of sense of smell
d) have been in close proximity with anyone within the last seven days where there is suspicion of that they have been symptomatic with COVID-19
Where the answer to all of the above is “no”, then inform the service user their depot will be administered as normal. However, advise the service user that if they become unwell over-night or are exposed to category d) above, they MUST NOT ALLOW their appointment to go ahead without first phoning for further advice. Should this be the case, please begin to manage the patient using Section Six below.
Step Two: Administering the depot. During the appointment, please maximise the distance between the service user and yourself until the point of having to physically administer the injection. The guidance on PPE use for people presenting with low risk of COVID-19 has been updated. This states that staff should don PPE at a level additional to the PPE normally used for depot administration. Hand washing or sanitiser must be used before and after each appointment. Please see the additional guidance on PPE later in this document.
Section Eight – Community Patient Requiring a Depot Who Ordinarily Receive This In Their Home Environment with Active Symptoms of COVID-19 or High Risk of COVID-19 or Fall Under the Category of Stringent Social Distancing
Step One: telephone the service user in advance of the appointment (preferably the day before) and confirm using questions a) – d) above that the service user is indeed at high risk.
Whilst there should be a presumption towards administering depots on the day that they are due, administration of a depot to a service user actively unwell with symptoms of COVID-19 should be discussed with medical staff before administration. In this case, there should be a risk based analysis undertaken to determine whether the administration of the depot should be delayed. A delay of a longer than 48 hours will require medical staff to re-write the Kardex. If it is considered that there is not immediacy to administer the depot, this should be delayed until the recommended isolation period is over (at time of writing 14 days from likely exposure or 7 days from development of symptoms). Provide assurance that telephone support will be provided over the time.
Where an appointment needs to take place to administer the depot, proceed to Step 2 below.
Where the potential risk to health and social care workers cannot be established prior to face-to-face assessment the service user should be consider to be at High Risk of COVID-19.
Step Two: Service users falling into this category should NOT routinely be brought to a clinic setting. Instead, service users will be visited in their home environment. Staff undertaking these visits must wear appropriate PPE equipment and should maximise the distance between themselves and the service user. At the end of the visit, the PPE equipment must be bagged and left in the service-user’s own home environment. This must be left for at least 72 hours before being placed in the ordinary household waste. Staff should NOT remove this waste from the household.
Staff should use hand sanitiser both before and after the appointment.
Please also see the section at the end of this document relating to information from Health Protection Scotland.
Section Nine – Service Users on Clozapine Medication
Service users on Clozapine must be considered a priority group and management of Clozapine is a core function that must be preserved given the potential risk to life with adverse effects. There are two issues to be considered: physical monitoring and dispensing of medication.
Those in charge of Clozapine clinics should identify patients with comorbid physical conditions that mean they fall with the health categories requiring stringent social distancing. These patients should not be brought into clinic settings and Physical Monitoring undertaken as if the service user is at High Risk of COVID-19 in being symptomatic or having contact with a suspected case.
Physical monitoring Step One: telephone the service user in advance of the appointment (preferably the day before) and determine whether they have any of the following:
a) a persistent new cough and/or a fever
b) are living with anyone with a persistent new cough and/or fever or who is thought to be infected with COVID-19
c) have experienced a loss of sense of smell
d) have been in close proximity with anyone within the last seven days where there is suspicion of that they have been symptomatic with COVID-19
Where the answer to all of the above is “no”, then ask the service user to attend their clinic appointment as scheduled. However, advise the service user that if they become unwell over-night or are exposed to category d) above, they MUST NOT ATTEND their appointment and must phone for further advice. Should this be the case, please begin to manage the patient using the Section directly below.

Step Two: Conducting the Clozapine appointment. Please ensure that you can collect your service-user from Reception as soon as they arrive. Reception staff will advise service-users to maintain a distance of 2m from any other waiting patient. The move to telephone contact for the majority of service users, should make this possible (that is, waiting areas should be less busy than usual). Hand sanitiser will be placed in Reception/waiting areas and people asked to use this on arrival.
During the appointment, please maximise the distance between the service user and yourself. The guidance on PPE use for people presenting with low risk of COVID-19 has been updated. This states that staff should don PPE for the duration of the appointment unless there is a good and risk based clinical reason not to wear PPE. and use hand washing or sanitiser before and after each appointment. Please see the additional guidance on PPE later in this document.
Sufficient time should be built in between appointments to minimise the crossover contact with patients and allow staff to sanitise the clinic setting. As part of the interaction, extra instruction given as to the actions the service user should take if developing symptoms suggestive of COVID-19. In addition to adhering to general NHS advice, the service user should be told to telephone the Duty Worker in order that a preliminary assessment can be made as to whether the apparent symptoms may actually be consequent of Clozapine. This may lead to a discussion with medical staff and/or the person’s GP. Where a service user is identified as being at high risk of COVID-19 or has active symptoms or falls into the category of stringent social distancing, they should be instructed NOT to attend the Clozapine clinic. Instead, a home visit will be arranged where the assessment/procedures undertaken within the clinic will still take place. These visits MUST take place given the possibility that a high temperature may be due to Clozapine complications. That is, they should not be deferred, regardless of the person being high risk. Staff undertaking these visits must wear additional appropriate PPE equipment for a high risk case and should maximise the distance between themselves and the service user until physical contact needs to take place. At the end of the visit, the PPE equipment must be bagged and left in the service-user’s own home environment. This must be left for at least 72 hours before being placed in the ordinary household waste. Staff should NOT remove this waste from the household.
Staff should use hand sanitiser both before and after the appointment.
Please also see the section at the end of this document relating to information from Health Protection Scotland.
Dispensing of Clozapine Medication Clozapine medication will be delivered to all service users in their home setting. Two members of staff will undertake this function with both signing (but not the service user) a pre-prepared document to testify that the medication was handed over. This will be provided by Team Leaders. Medication must only be given to the service user themselves unless that person is known to be actively symptomatic with COVID-19 where it would be acceptable to give the medication to a known relative who is present at the service user’s own address. The identity of the person should be cross-checked with the medication being delivered. Staff delivering medicine should not enter

the home environment . That is, the medication should be handed to the service without skin contact or prolonged conversation. Where an individual is known to be at high risk of COVID-19 or falls into the category of a “shielded person” with high risk comorbid conditions, staff should wear PPE but be sensitive to the effects of this on the service user. Staff should use hand sanitiser before and after each visit. Where people have a low risk of COVID-19, staff should don PPE unless there is a good and risk assessed reason why this should not be worn. Please see the additional guidance on PPE later in this document.
Where a service user is not present at the home address at time of delivery, a note should be left asking them to contact the Duty Worker as soon as possible. A further delivery drop can then be arranged. Section Ten – Community Based Patient Attending the Lithium Clinic Step One: telephone the service user in advance of the appointment (preferably the day before) and determine whether they have any of the following:
a) a persistent new cough and/or a fever
b) are living with anyone with a persistent new cough and/or fever or who is thought to be infected with COVID-19
c) have experienced a loss of sense of smell
d) have been in close proximity with anyone within the last seven days where there is suspicion of that they have been symptomatic with COVID-19
Where the answer to all of the above is “no”, then ask the service user to attend their clinic appointment as scheduled. However, advise the service user that if they become unwell over-night or are exposed to category d) above, they MUST NOT ATTEND their appointment and must phone for further advice. Should this be the case, please begin to manage the patient using instructions for high risk cases below.
Time should be factored in between appointments to minimise crossover contact with other service users and staff. Service users should use hand sanitiser before and after their appointment. Where service users indicate that they do not wish to attend the Lithium clinic, the safety of this will be discussed with medical staff. It is likely that for most people monitoring can be safely delayed where a Lithium level has been taken at some point within the previous six month period. Where service users are identified as being at high risk of COVID-19, they should be instructed NOT to attend their appointment and this situation highlighted to medical staff. It is likely that for most people monitoring can be safely delayed where a Lithium level has been taken at some point within the previous six month period. Where it is consider not safe to delay monitoring and this can not wait until the risk of infection has subsided, then the person will be seen at home. The procedures outlined in Section Nine for conducting Clozapine monitoring at home with high risk COVID-19 cases or those subject to stringent social distancing should be adopted.

It is likely that given the low risks associated with delays to Lithium clinic checks, a number of appointments each week will be rearranged to allow for minimised contact between service users. Clinic lists will be reviewed by experienced medical staff and schedules of monitoring implemented using this expert advice.
Special Considerations Transporting Patients By Car
It is not unusual in mental health and learning disability services for staff to use their own vehicle to transport patients. This practice should STOP unless there is specific clinical and/or risk management reasons to do so. Where there is a need for staff to transport patients in cars, due consideration should already have been given as to whether such journeys are absolutely necessary. Where this is the case, as much distance as possible should be maintained between staff and the service user. Only one service user must be transported at a time and the vehicle wiped down with appropriate cleanser between uses. Staff should don appropriate PPE equipment during these journeys unless there is a good and risk assessed reason to not wear PPE. On the very rare occasion where a service user who is at high risk of COVID-19 or has been confirmed as such needs to be transported, this should be discussed with your Team Leader/line manager. Where alternatives cannot be arranged, it is likely that distancing measures and PPE should be adopted and the vehicle interior cleaned after use. Consideration should be given to the use of a Crown vehicle.
Resuscitation
There are occasional times when community based staff encounter situations (generally following over-dose or other self-harm) when a service user requires resuscitation. At this time, all such cases should be considered as High Risk of COVID-19 and only chest compressions should be used. Current guidance from the Resuscitation Council UK states:
Recognise cardiac arrest by looking for the absence of signs of life and the absence of normal breathing. Do not listen or feel for breathing by placing your ear and cheek close to the patient’s mouth. If you are in any doubt about confirming cardiac arrest, the default position is to start chest compressions until help arrives
Make sure an ambulance is on its way. If COVID 19 is suspected, tell them when you call 999 If there is a perceived risk of infection, rescuers should place a cloth/towel over the victims mouth
and nose and attempt compression only CPR and early defibrillation until the ambulance (or advanced care team) arrives. Put hands together in the middle of the chest and push hard and fast
Early use of a defibrillator significantly increases the person’s chances of survival and does not increase risk of infection
If the rescuer has access to personal protective equipment (PPE) (e.g. FFP3 face mask, disposable gloves, eye protection), these should be worn
After performing compression-only CPR, all rescuers should wash their hands thoroughly with soap and water; alcohol-based hand gel is a convenient alternative. They should also seek advice from the NHS 111 coronavirus advice service or medical adviser
Other Relevant Information Health Protection Scotland have provided Guidance entitled “COVID-19: Information and Guidance for Guidance for Social or Community Care & Residential Settings” (Version 1.6 2 April 2020) which can be found here:
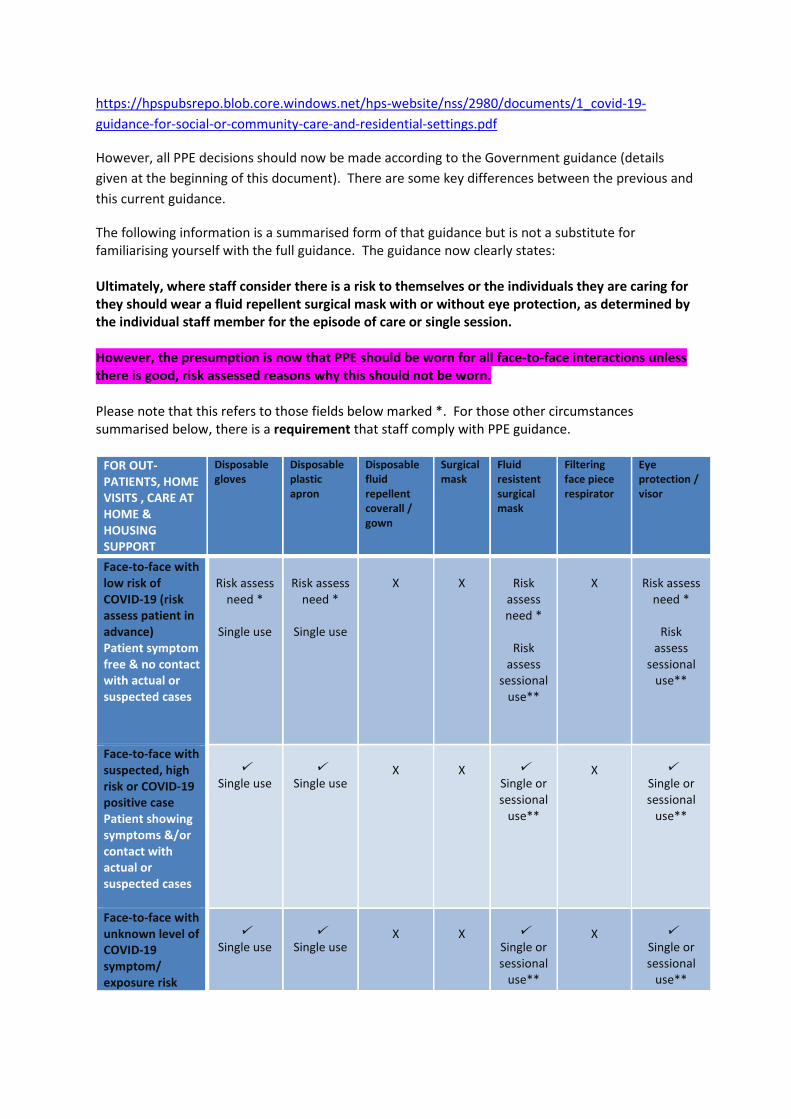
https://hpspubsrepo.blob.core.windows.net/hps-website/nss/2980/documents/1_covid-19-guidance-for-social-or-community-care-and-residential-settings.pdf
However, all PPE decisions should now be made according to the Government guidance (details given at the beginning of this document). There are some key differences between the previous and this current guidance.
The following information is a summarised form of that guidance but is not a substitute for familiarising yourself with the full guidance. The guidance now clearly states: Ultimately, where staff consider there is a risk to themselves or the individuals they are caring for they should wear a fluid repellent surgical mask with or without eye protection, as determined by the individual staff member for the episode of care or single session. However, the presumption is now that PPE should be worn for all face-to-face interactions unless there is good, risk assessed reasons why this should not be worn. Please note that this refers to those fields below marked *. For those other circumstances summarised below, there is a requirement that staff comply with PPE guidance.
FOR OUT-PATIENTS, HOME VISITS , CARE AT HOME & HOUSING SUPPORT
Disposable gloves
Disposable plastic apron
Disposable fluid repellent coverall / gown
Surgical mask
Fluid resistent surgical mask
Filtering face piece respirator
Eye protection / visor
Face-to-face with low risk of COVID-19 (risk assess patient in advance) Patient symptom free & no contact with actual or suspected cases
Risk assess
need *
Single use
Risk assess
need *
Single use
X
X
Risk
assess need *
Risk
assess sessional
use**
X
Risk assess
need *
Risk assess
sessional use**
Face-to-face with suspected, high risk or COVID-19 positive case Patient showing symptoms &/or contact with actual or suspected cases
Single use
Single use
X
X
Single or sessional
use**
X
Single or sessional
use**
Face-to-face with unknown level of COVID-19 symptom/ exposure risk
Single use
Single use
X
X
Single or sessional
use**
X
Single or sessional
use**

That is, risk assessment could not be undertaken in advance Face-to-face with a shielded person or where another shielded person in same household
Single use
Single use
X
Single use
X
X
X
*The risk assessment here refers to utilising PPE when there is an anticipated / likely risk of contamination with splashes, droplets or body fluids. Where staff consider there is a risk to themselves or the individuals they are caring for they should wear fluid repellent surgical mask with or without eye protection as determined by the individual staff member for the care episode / single session. The presumption, however, is now towards wearing this unless there is a valid clinic reason as to why not. **A single session refers to a period of time where a health care worker is undertaking duties in a specific care setting / exposure environment (e.g. on a ward round). A session ends when the health care worker leaves the care setting / exposure environment.
The guidance clearly states that staff must comply with all infection control procedures as set out in the above guidance and the National Infection Prevention and Control Manual. http://www.nipcm.hps.scot.nhs.uk/ There are two particularly important elements to this: 1) Staff who are pregnant of otherwise immunosuppressed should not provide direct care to a person with possible or confirmed COVID-19 2) Staff attending to care for someone who is a possible or confirmed case of COVID-19 should not , where possible, attend to care for further people who are not self-isolating due to COVID-19. If this cannot be avoided, consider caring for these individuals at the end of caseloads.
Linda Graham (Clinical Lead for Mental Arlene Mitchell (Locality Manager)
Health & Learning Disability)
Dundee Health & Social Care Partnership
Appendix 3 – Health Protection Scotland (amended to include disposal)
Putting on PPE: PPE should be put on before entering the clinical situation/house

Removal of PPE: PPE should be removed in the order that minimises the potential for cross contamination (i.e. as outlined below even where not all components of PPE have been used)
Gloves: grasp the outside of the glove with the opposite hand; peel off
Hold the removed glove in the gloved hand
Slide the fingers of the un-gloved hand under the remaining glove at the wrist
Peel the glove off and discard appropriately
Apron: Unfasten or break ties
Pull apron away from the neck and shoulders, touching the inside of the apron only
Turn the apron inside out, fold or roll into a bundle and discard appropriately
Eye Protection (only if advised): to remove handle by headband or earpieces and discard appropriately
Facemask (only if advised): Remove after leaving the care area
Untie or break bottom ties, followed by top ties or elastic and remove by handling the ties only and discard as per below
Untie and allow to fall away from the face and discard appropriately
Perform hand hygiene immediately after removing all PPE
Disposal of PPE: PPE and personal waste (e.g. tissues) should be placed with a bin bag. When full, bags should be placed in a second bag and tied. These bags should be stored for 72 hours before being put out for collection.

MENTAL HEALTH SERVICES COVID-19 CATEGORIES TO ASSIST WITH PRIOITISATION OF CARE
This document is intended to assist those working within our mental health service in prioritising patients according to their needs and the functions we provide to meet those needs. The involved services are Community Mental Health Services, Integrated Substance Misuse Services, Learning Disability Services, CAMHS, Psychological Therapies Services and the Multidisciplinary Adult Psychotherapy Service. Forensic services are out-with the scope of this document. Older People’s Services are already working to an equivalent document and are also out with scope.
Mental health need is a complex, dynamic concept. The interaction between, for example, diagnosis, emotional dysregulation and distress and risk issues means that people can present with a frequently changing clinical picture and services need to be able to respond in a dynamic way. There must therefore be recognition that a person may move between the categorisations given below.
Please note that the examples are intended to be illustrative; not exhaustive.
CATGEORY 1
Failure to maintain this function may result in risk to life, major permanent incapacity or extensive injury to self or others
Carers highly unlikely to cope with additional demands
Adverse event arising from service reduction/withdrawal will cause serious reputational risk & high likelihood of external body scrutiny, criticism, prosecution or Fatal Accident Inquiry
National press interest expected
Examples include (but not exclusively) : maintenance of physical monitoring of people prescribed medications that can cause extremely serious physical complication (for example, Clozapine or cholinesterase Inhibitor death); full and assertive treatment of mood or other disorders giving rise to increased suicide risk ; treatment of psychosis where emergence of symptoms may lead to increase risk to self and others; management of mental health/substance misuse in pregnant and post-natal women; provision of the Duty Worker system; management of Anorexia Nervosa and other eating disorders where physical wellbeing can deteriorate and become life-threatening; young people with eating disorders; provision of enteral feeding and maintenance/changing of tube site ; support to vulnerable person exposed to harm ; Speech & Language dysphagia assessments; post in-patient discharge support (high associated higher risk of suicide); management and support of people subject to community based Detention; management of people subject to Local Authority Guardianship or Adult/Child Support & Protection measures ; management of non fatal overdose within Opiate Substitution Therapy; assessment for OST where there are significant risks including physical co morbidities; management of substance misuse in people discharged hospital and liberated from prison; people with significant psychological and behavioural symptoms of dementia (PBSD) causing high levels of distress or high risk to self and/or others

CATEGORY 2
Failure to maintain this function will result in treatment deviating from recognised best practice and contribute to poorer patient outcome in the longer term
Carers likely to experience difficulties coping and be at increased risk of developing own mental health problems
Adverse event arising from service reduction/withdrawal will cause moderate reputational risk & external body interest but with less risk of prosecution or FAI
Local press interest which may be picked up nationally
Examples include: administration of depot injections and other antipsychotic medications; inadequate treatment of severe depressive and other mood disorders; lack of timely response to people at risk of self-harm and suicidal behaviour; assertive rehabilitation; treatment of Complex-PTSD where treatment has already commenced; individual treatment of adults and young people with Emotionally Unstable Personality Disorder; management of people with co-morbid substance misuse issues (who are not psychotic); assessments and initiation of detoxification for alcohol and opiate dependence ; people with moderate PBSD causing moderate levels of distress, carer stress or risk of harm to self/others
CATEGORY 3
Failure to maintain this function will result in likely delays in recovery but no evidence that this will contribute to poorer longer-term outcome once treatment recommences (albeit that distress may be prolonged)
Carers likely to experience some additional request for support but at manageable level in the short-term
Adverse event from service reduction/withdrawl will cause moderate reputational risk (low risk unlikely given context of Trust & Respect) but no external body interest.
Local press interest only
Examples include: changes in medication for chronic disorders (where response is adequate but not maximised); treatment of moderate & mild depressive disorders (both psychological treatment and pharmacological treatment); treatments for adult single event PTSD; Personality disorder (excluding Emotionally Unstable); treatment of gender dysphoria; treatment of health anxiety; treatment of Obsessive Compulsive Disorder; provision of expert consultation to agencies supporting looked after children; advice and support to families with children with neuro-developmental disorders ; initiation of treatment and support for adults with ADHD and Autistic Spectrum Conditions; people receiving recognised drug treatments not recognised in Tayside drug formulary; routine review of Opiate Substitution Therapy and associated recovery care plan and risk assessment; psychosocial interventions for addictions; routine dementia diagnosis when patients

are stable and managing at home without difficulty; routine post-diagnostic support where distress and carer stress are minimal.
CATEGORY 4
Failure to maintain this function will have no direct impact on service users. Care, treatment and support can be stopped or suspended in the short-term with no worsening of mental health or impact on longer-term outcome
Carers unlikely to experience change in level of input required from them
Adverse event is unlikely to have root cause located in suspension of this service/care and treatment. Reputational risk is moderate (low risk unlikely given context of Trust and Respect) but no external body interest.
Local press interest likely to have minimal impact
Examples include: treatment of simple anxiety disorders; young people with neuro-developmental disorders where school was asking for management advice; assessment of suitability for Exceptional Aesthetic Referrals and bariatric surgery (procedures not possible at the moment); treatment of self-esteem issues; people asking to wait until social distancing has ended; Acetylcholinesterase Inhibitor review/monitoring other than 3 weeks after initiation/dose escalation
.
Produced by short-life working group led by Linda Graham, Clinical Lead for Mental Health & Learning Disability, DHSCP (10th April 2020)
Perth & Kinross Health & Social Care Partnership 2.3Stage 2 Mobilisation Plan: Respond, Recover, Renew VERSION 25TH MAY 2020
Executive Lead Gordon Paterson, Chief Officer Mobile - 07816 855097
Operational Leads Diane Fraser, Head of Adult Social Work and Social Care Mobile - 07785 570020
Evelyn Devine, Head of HealthMobile - 07590 924622
Strategic Lead Jane Smith, Chief Financial OfficerMobile - 07966 875713
Review Operational Review Silver Command/ IMT
Reporting PKHSCP Gold Command/Executive Management Team Scottish Government Via NHS Tayside

PKHSCP Stage 2 Mobilisation Plan
Introduction
It is now recognised that Covid-19 will be an ongoing challenge to varying levels for the forseeable future with levels of social distancing and lockdown measures in place for 12 months or more. For health and social care services across Perth & Kinross the ongoing constraints of PPE use, isolation and shielding of both staff and service users has a signficant impact on the ability to deliver services in the same way. The challenge is how PKHSCP rebuilds health and social care services whilst maintaining service capacity to respond to a potential further surge in Covid-19 activity.
The Covid-19 Pandemic response by PKHSCP has resulted in a dramatic and unprecedented level of change in how day to day services are delivered with new access channels , new ways of working implimented including signficant use of digital and telephone services, as well as signficant efforts to free up hospital bed capacity. Going forward into the recovery phase we are identifying how these changes were delivered and which chages should now be embedded in service models and practice moving forward, seizing the good practice and innovation that has emerged.
The PKHSCP Stage 2 mobilisation plan sets out the steps that will deliver safe, prioritised and risk-assessed care within the constraints of ‘Living with COVID’. However, it also sets out initial plans to harness the transformative service change that has emerged in the initial response period. The PKJHSCP Stage 3 Renewal Programme will further set out our longer term plans with work already progressing in a number of areas which will be accelerated over June/July. The overall thrust of the recovery and renewal process will be to support services to return to the 'new normal' learning from the experience of the pandemic situtaion and retaining as much as possible of the transfomation that has occurred. Key programmes of work will be 'People, Learning and Culture' and 'Public Engagement and Communication'. It is proposed that the initial planning timeframe for Phase 3 should be Winter 2020/21.
This Phase 2 Mobilisation Plan supercedes the Phase 1 Plan previously submittted. The financial implications are set out and include initial estimates of the further service change required to support recovery. Business Cases will be brought forward for this proposed investment. Potential offsets are still to be determined based on actual expenditure patterns in the first quarter.
The Covid-19 response is currently being delivered through the PKHSCP Gold Command structure. This structure will continue to provide the oversight of ongoing response with the Executive Management Team meeting as a Renewal Group to oversee longer term service change. Reporting to the IJB Strategic Planning Group and the IJB itself will be essential as we begin to consider alignment of the previously agreed Strategic Commissioning Plan and 3 Year Financial Recovery Plan with Covid-19 Response Recovery and Renewal Plans.
The Phase 2 Plan has been developed in full discussion with NHS Tayside to ensure a connected full-system response.

Nature of Provision RefActions Planned
SRO Lead OfficerStatus
RAG2020/21
Cost*Hospital Bed capacity and effective flow and discharge 1.1 Increase capacity within Tay Ward from 14 to 22 beds to provide care for Post-COVID 19 patients requiring
complex rehabilitation and patients from current NHST elective pathway (Orthopaedics and General Surgery) be transferred to Tay Ward for rehabilitation.
Evelyn Devine Caitlin Charlton Amber £579k
1.2 Ensure adequate spacing in all inpatient areas in line with guidance. Evelyn Devine Caitlin Charlton / Lindsey Bailie / Amanda Taylor
Amber
1.3 Integrated Discharge Hub: increase capacity to ensure a whole-system Integrated Discharge Hub in line with Ninewells, including 7-day working across PRI, Murray Royal Hospital and Community Hospitals to support discharge pathways, transitional and complex care.
Evelyn Devine Caitlin Charlton / Karyn Sharp /
Lindsey Bailie / Amanda Taylor
Amber £135k
1.4 Enhanced rehabilitation staff on the PRI site for Unscheduled Medicine and MFE which will support 7-day working, to ensure effective rehabilitation and reduce length of stay.
Evelyn Devine Caitlin Charlton Amber TBC
1.5 Enhanced Specialist POA Liaison Service in PRI to provide transitional care for people in acute wards. Evelyn Devine
Caitlin Charlton / Lindsey Bailie
Green £40k
1.6 Provide OT and PT inpatient support to "Green Elective Zone" in PRI Evelyn Devine
Caitlin Charlton / Morag Otley
Red
1.7 As part of redesign of Medicine for the Elderly Medical Model, recruit to Clinical Fellow posts to support flow in Community Hospitals and Tay Ward.
Evelyn Devine Caitlin Charlton / Dirk Habicht
Amber TBC
1.8 For POA wards agree admission criteria and COVID/NON COVID admission pathway. Ensure preadmission testing where possible and provide self isolation for patients admitted in a crisis until testing can be completed. Continue to support with increased staffing levels to ensure safety.
Evelyn Devine Lindsey Bailie Amber £103k
1.9 For POA Wards increase Social Work support to support discharge and reduce readmissions to hospital. Develop rehabilitation framework for complex discharges including step-down and discharge to assess.
Diane Fraser Karyn sharp / Lindsey Bailie
Green £25k
1.10 Contracts and compliance to ensure maximum use of bed capacity in care homes for example review of interim placements, self funding beds.
Diane Fraser Zoe Robertson Green £224k
1.11 RVS to facilitate Home-from-Hospital Service, providing practical and social support for people returning home from hospital.
Diane Fraser Zoe Robertson/ Karyn Sharp
Green £56k
Intermediate Care Capacity 2.1 Additional Interim Step Down capacity in Beechgrove and Parkdale remain prepared and will be staffed as required.
Diane Fraser Brian Kinnear Green £28k
2.2 Increase staffing within PKC Care Homes to safety and wellbeing of care home residents and staff and to minimise cross-infection across care home wings.
Diane Fraser Brian Kinnear Amber TBC
2.3 Additional Step Down capacity in Ptlochry Community Hospital ( Atholl Unit 7 Beds) and Crieff Community Hospital ( 10 beds wiith abaility t to surge to 15) remain prepared to receive patients and will be staffed if
Evelyn Devine Amanda Taylor / Lindsey Bailie
Green £206k
Supporting the Care Home Sector 3.1 Infection Protection and Control - maintain close contact/weekly calls with the Health Protection Team, Care Inspectorate, Scottish Care and Commissioning and Team and Nursing/ Health Leads. Ensure effective communication with visiting health professionals (District Nursing, ANPs, Care Home Liaison, and GPs) to and from Commissioning Team, other relevant stakeholders regards Infection Prevention and Control.Ensure consistency of approach and standards across multiple teams. Ensure Homes are informed and operating to the most recent guidance. Ensure effective training and instruction are in place for Care Homes and relevant others. Introduce visits for Care Homes with significant outbreaks or to those observed as not following guidance, and therefore require further specialist support/intervention.Ensure continuation of weekly reporting to Scottish Government and daily reporting to Care Homes Clinical and Care Professional Oversight Team.
Sandra Gourlay/ Diane Fraser
Brian Kinnear/ Carolyn Wilson
Amber

3.2 Testing - ensure testing is maintained as a priority, with clear routes and responsibilities set out to ensure staff and patients and service users are tested in accordance with the guidance in relation particularly to admissions to care homes.Contact tracing is undertaken where required. Linked home testing will be delivered.Care Homes will continue to refer their symptomatic staff through the existing systems in place. Amber
3.3 Staffing Support - jointly PKHSCP, PKC and NHST will ensure clinical and care resource is provided to care homes to ensure staff rotas are maintained to deliver safe and effective care. A Care Home Rapid response team will be indentified and deployed as necessary.NHS Tayside will provide clinical staff through a variety of mechanisms including bank staff, volunteers and from community teams (this may be in the form of enhanced existing activity or by way of provision of clinical support and supervision).
Diane Fraser Alison FairlieSandra GourlayZoe Robertson
Amber £130k
3.4 Health and Wellbeing measures - staff within care homes will be supported both by their own internal mechanisms but will continue to access resources made available i.e. Tayside Counselling service. We will intervene early and ensure support is offered when and where available.
Diane Fraser Zoe Robertson Amber
3.5 Care quality - Additional staffing required to ensure daily reporting to Care homes, reporting to Clinical and Care Professional Oversight Team, maintain close links and clear lines of communication from visiting health professionals (District Nursing, ANPs, Care Home Liaison, and GPs) to and from commissioning team, other relevant stakeholdersincluding Health Protection Team, Care Inspectorate, Scottish Care, nursing/ health representative and Commissioning and Policy team.
Sandra Gourlay/ Diane Fraser
Careen Mullen-Mckay/ Carolyn
Wilson
Amber TBC
3.6 Ongoing proactive approach around the safety and wellbeing of care home residents and staff through strong leadership jointly with GP's ANP's, LINCS, AHPs, and Public Health. Diane
Fraser/Evelyn Devine
Brian Kinnear/Amamda
TaylorAmber
Ensure Care Providers remain operationally and financially viable
4.1 For Care at Home/Supported Living pay providers for planned hours and reasonable costs including PPE, staffing costs due to sick pay, staff self isolating and agency costs.
Diane Fraser/Jane Smith
Zoe Robertson /Donna Mitchell
Ongoing Green £3,107k
4.2 Make every effort to pay providers as quickly as possible including uplifts for living wage and National Care Home Contract
Jane Smith Zoe Robertson /Donna Mitchell
Ongoing Green £185k
5.1 Ensure adequate IT equipment and training to support maximum use of 'Near Me' by multiple users. Explore digital and IT requirements to implement mobile working in communities.
Evelyn Devine Caitlin Charlton Amber
5.2 Enable staff to gain knowledge, skills and insight into the opportunities presented via investment in Digital Technology to improve future service delivery across localities. Complete Digital Service Baseline Profile information gathering, to inform and drive service needs.
Evelyn Devine Chris Lamont Green
5.3 Installation of new GSM Community Alarm units which do not require installation to a phone line, can be accessed remotely and have improved virtual links to digital devices such as mobile phones, "Alexa".
Diane Fraser Brian Kinnear Amber
5.4 Care Home visits and contacts with family / relatives via digital options such as Face Time and Zoom. Diane Fraser Brian Kinnear Green
5.5 Further promote the Respiratory Self Management App. across all communities. Evelyn Devine Audrey Ryman GreenCare and Treatment Services 6.1 Maintain redeployment of MIIU and Anticoag staff to support CCAT, inpatient services and District Nursing to
continue to provide more complex and palliative care at home.Evelyn Devine Amanda Taylor Green
6.2 Explore opportunities for MSK services and other AHP Services to support Care and Treatment approaches, e.g., Podiatric interventions, Nutrition and Dietetic services.
Angie McManus N/A Red
Outpatients 7.1 Simpson Day Clinic Rapid Access Clinic to be tested within localities utilising the LINCS model, ANPs and Clinical Fellows / Speciality
Evelyn Devine Caitlin Charlton Amber
7.2 Improve the use of technology solutions such as Near Me, telephone triage and virtual contacts to reduce the MSK and AHP waiting times provide multi-agency assessment clinics, MFTE Clinics, Parkinsons Disease Clinics. Evelyn Devine/
Diane FraserCaitlin Charlton/
Kenny Ogilvie Green
Digital First : Changing Service Provision

8.1 Implement and embed fully the Integrated Pathways across Perth & Kinross Localities supported by the Locality Integrated Care Service, Advanced Nurse Practitioners, Rapid Response, Specialist Respiratory Service, plus continue to test the 24/7 community nursing.
Evelyn Devine Amanda Taylor Amber TBC
8.2 Continue to esnure enhanced SCOs cover to LINCS on 24/7 basis for urgent/crisis requests. Diane Fraser Shona MacLean Green TBC
8.3 Enhance provision for unpaid carers at home supporting those with urgent care needs. Diane Fraser Karyn sharp / Lindsey Bailie
Green
Primary Care: Re-establishment, Redesign and Increased Need
9.1 Utilise AHP opportunities to support Primary Care Services ( First Contact Physiotherapy scale, Podiatric Vascular Surgery, Occupational Therapy First Contact, Nutrition and Dietetic First Contact)
Angie McManus N/A Amber
9.2 Develop understanding of role and impact on unpaid carer in Primary Care. Diane Fraser Karyn Sharp Amber
9.3 Ensure Primary / Secondary / Social Care Interface Group in place to co-ordinate current demand and the growing backlog of care.
Hamish Dougall Lorna Jackson-Hall Green
9.4 Resume of review and management of all long-term conditions (LTC). Hamish Dougall Lorna Jackson-Hall Ongoing Green
9.5 Ensure Anticipatory Care Planning (ACP) is in place Hamish Dougall Lorna Jackson-Hall Ongoing Green
9.6 Home visits are taking place for those patients in the shielding group and the over-70s non-shielding at risk group Hamish Dougall Lorna Jackson-Hall Ongoing Green
9.7 Work with NHS Tayside (who hold this responsibility) to ensure that practices have the appropriate hardware, software and connectivity infrastructure to maximise the use of digital technology.
Hamish Dougall Lorna Jackson-Hall Ongoing Green
9.8 Ensure preparedness for administrating the next round of flu vaccinations. Hamish Dougall Lorna Jackson-Hall Ongoing Green
9.9 Review the current and anticipated demand/resource needs of COVID-19 hubs and assessment centres. Hamish Dougall Lorna Jackson-Hall Ongoing Green
9.10 Explore with NHST, GP direct call access to relevant consultant specialists for advice and guidance, where required.
Hamish Dougall Dirk Habicht Red
Community Care : Re-establishment, Redesign and Increased Need
10.1 Support the reduction in waiting times within Older Peoples Community Mental Health Service. Explore remote opportunities to provide memory assessment in a timely manner to reduce the increasing waiting times. Evelyn Devine Lindsey Bailie Amber
10.2 Review Care Home Liaison Team ways of working across localities to support Urgent Care and LiNCs models to deliver enhanced support to Care Homes
Evelyn Devine Lindsey Bailie Amber
10.3 Support the reduction in waiting times within Older Peoples Community Mental Health Explore remote opportunities to provide memory assessment in a timely manner to reduce the increasing waiting times. Evelyn Devine Lindsey Bailie Amber
10.4 Provide increased support to unpaid carers including respite care. Support ethnic minority group carers with culturally-specific needs.
Diane Fraser Karyn Sharp Amber
10.5 Increase social care management capacity for 6 months to improve capacity and flow across hospital, community development and crisis response.
Diane Fraser Karyn Sharp Green £24k
Social Care : Re-establishment, Redesign and Increased Need
11.1 Increase capacity of Care at Home through COVID retasking team. This will create further capacity within HART to allow focus on reablement, rehabilitation and intensive post discharge support.
Diane Fraser Karyn Sharp Green
11.2 Review potential long term Care at Home team options for rural localities to be employed by the partnership. Diane Fraser Karyn Sharp Amber £985k
11.3 Continue to review current packages with regards to the suitability of single-handed care Diane Fraser Ongoing Green £20k
11.4 Provide increased support to Carers Voice as representatives of unpaid carers to ensure capacity and resources. Re-tasked staff or recruited staff. Welfare Rights & Citizen's Advice may require support, as Carers may also have lost employment as a result of lockdown/recession.
Diane Fraser Karyn Sharp Amber TBC
11.5 Review of the "Risk Stratification Document" (red amber green screening programme) which was introduced to offer the appropriate care to the individual. Client categorisation to be reviewed and updated for Day Care and Day Opportunity service users.
Diane Fraser Brian Kinnear Amber
11.6 Ongoing delivery of "Outreach Day Care" which was newly implemented at start of Covid 19 contingencies. Providing support to service users and carers who are most vulnerable and/or who are suffering from carer stress. Outreach support has increased as the weeks have gone on.
Diane Fraser Brian Kinnear Green
Urgent Care

11.7 OP Day Care and LD Day Opportunity "Impact Assessment" with regards to stepped down registered services, Outreach Day Care, and Virtual Day Opportunities as part of plans for our next phase. Diane Fraser Brian Kinnear Red
Tayside Public Dentistry 12.1 Repatriate redeployed Dentistry Workforce in order to plan for increased activity in PDS areas across Tayside as directed by the Chief Dental Officer, immediately. Within a timescale to be advised by CDO, retain workforce for PDS patients and to support GDPs provide AGPs for their own patients.'
Evelyn Devine Morag Curnow Amber
Tayside Podiatry 13.1 Gradual return of deployed staff will increase service capacity. Treatment will be on demand for those with long term conditions which put their lower limb at significant risk and those whose condition is now creating a loss of either physical or social function Service will liaise closely with primary care partners to ensure safety at all clinical sites.
Evelyn Devine Lee Sievwright Amber
14.1 Develop business case for Distress Brief Intervention as part of wider Tayside plan. Evelyn Devine Chris Lamont Amber TBC
14.2 Increase Primary Care Mental Health Nursing Cohort to improve access for those in mild to moderate psychological distress including carer breakdown, anxiety disorders etc. Ennsure easy access staff support service.
Evelyn Devine Chris Lamont Amber Amber £203k
14.3 Embed Mental Health Advanced Nurse posts in Access Team (SPOC) to support early intervention and prevention based on the learning from redeploying mental health staff during Phase 1.
Evelyn Devine Chris Lamont Amber Amber TBC*
14.4 Increased support through commissioned services for Mental Health Carers including extension of befriending support, support for local rural community groups to respond to isolation, sense of powerlessness, stress of caring responsibilities, loss of employment, impact on self-esteem, loss of income and working life. Signposting
Diane Fraser Karyn Sharp Amber
14.5 Next steps to be identified for Learning Disabilitiy and Mental Health Clients who were being supported into work by Employment Support Team prior to crisis. Improved access to digital platforms and equipmen will be required.
Diane Fraser Brian Kinnear Red
14.6 Implementation of "Virtual Day Opportunities" across Learning Disability Services daily, using digital platforms such as Zoom Teams, and Duo. To reduce isolation, create structure and opportunity for socialising and engagement in activities.
Diane Fraser Brian Kinnear Amber
14.7 Wellbeing Support Team to move to face to face contact (in line with governmental policy and safe social distancing) along with use of tele and video conferencing. Improved access to equipment will be required.
Diane Fraser Ian Wilkie Amber
Effective Drug and Alcohol Services 15.1 Specific support for carers/young carers of people with drug and alcohol issues, to minimise crisis due to misuse or withdrawal as a result of lockdown. Work with Education & Children's Services and PKAVS Young Carers.
Diane Fraser Karyn Sharp Amber TBC
15.2 Assessments and reviews to be completed using information from clients, carers, professionals gathered by phone or other virtual means such as Nearme wherever possible. Home visits carried out when necessary due to level of risk.
Diane Fraser Kenny Ogilvy Green
15.3 Joint working with Third Sector organisations to continue eg home delivery of ORT prescriptions Diane Fraser Kenny Ogilvy Green
Forward thinking on PPE 16.1 Ensure ongoing supply of PPE through Hubs across health and whole social care sector; with extended provision to include unpaid/family carers and personal assistants. Identify capacity to continue to support FFP3 face masks.
Diane Fraser/Sandra
Gourlay
Brian Kinnear Green £27k
16.2 Pathways to PPE Hubs implemented for all registered services, Personal Assistants, Self Employed and Unpaid Carers. Pathways support the "business as usual" processes where providers source their own stock of PPE. Diane Fraser
Brian Kinnear / Carolyn Wilson
Green
Transport solutions 17.1Increasing physical activity and community resilience 18.1 Enhance Care About Physical Activity ( CAPA) model across Perth & Kinross through appointment of additonal
staff to support community resilience, mental health and wellbeing, physical activity and reduction in social isolation. within care homes, communities, care at home, with carers and third sector. Promote the Live Active Wellbeing Leaflet
Evelyn Devine Carolyn Wilson Amber TBC
Effective Communication 19.1 Further enhance communications with staff, service users and other stakeholders though further development of staff newsletter, regular bulletins, awareness campaigns (including role of unpaid carers) , proactive social media and website development. Identify additional expert capacity for 6 months.
Jane Smith/ Evelyn Devine/ Diane
Fraser
TBC Ongoing Amber £16k
Workforce Resilience 20.1 Daily workforce review and accelerated redeployment of staff within HSCP to ensure services operate effectively.
Diane Fraser/ Evelyn Devine/
Chris Jolly
N/A Ongoing Green £867k
Mental Health : Responding to Increased Need
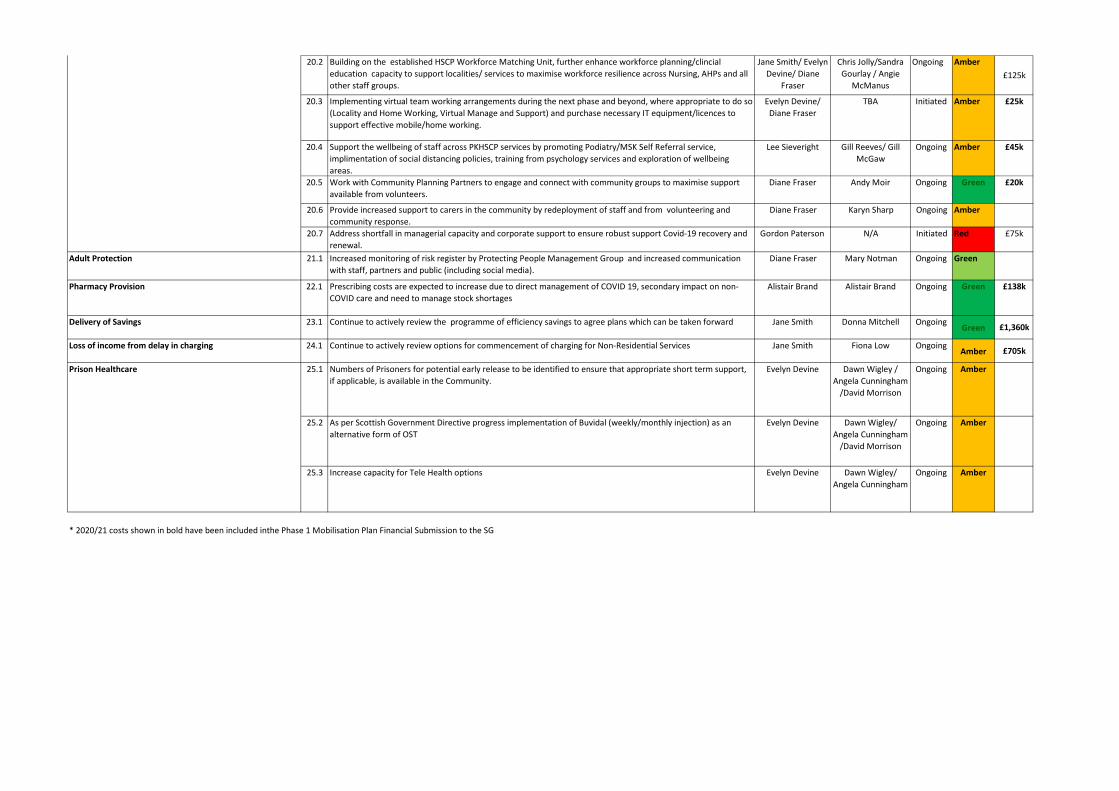
20.2 Building on the established HSCP Workforce Matching Unit, further enhance workforce planning/clincial education capacity to support localities/ services to maximise workforce resilience across Nursing, AHPs and all other staff groups.
Jane Smith/ Evelyn Devine/ Diane
Fraser
Chris Jolly/Sandra Gourlay / Angie
McManus
Ongoing Amber£125k
20.3 Implementing virtual team working arrangements during the next phase and beyond, where appropriate to do so (Locality and Home Working, Virtual Manage and Support) and purchase necessary IT equipment/licences to support effective mobile/home working.
Evelyn Devine/ Diane Fraser
TBA Initiated Amber £25k
20.4 Support the wellbeing of staff across PKHSCP services by promoting Podiatry/MSK Self Referral service, implimentation of social distancing policies, training from psychology services and exploration of wellbeing areas.
Lee Sieveright Gill Reeves/ Gill McGaw
Ongoing Amber £45k
20.5 Work with Community Planning Partners to engage and connect with community groups to maximise support available from volunteers.
Diane Fraser Andy Moir Ongoing Green £20k
20.6 Provide increased support to carers in the community by redeployment of staff and from volunteering and community response.
Diane Fraser Karyn Sharp Ongoing Amber
20.7 Address shortfall in managerial capacity and corporate support to ensure robust support Covid-19 recovery and renewal.
Gordon Paterson N/A Initiated Red £75k
Adult Protection 21.1 Increased monitoring of risk register by Protecting People Management Group and increased communication with staff, partners and public (including social media).
Diane Fraser Mary Notman Ongoing Green
Pharmacy Provision 22.1 Prescribing costs are expected to increase due to direct management of COVID 19, secondary impact on non-COVID care and need to manage stock shortages
Alistair Brand Alistair Brand Ongoing Green £138k
Delivery of Savings 23.1 Continue to actively review the programme of efficiency savings to agree plans which can be taken forward Jane Smith Donna Mitchell OngoingGreen £1,360k
Loss of income from delay in charging 24.1 Continue to actively review options for commencement of charging for Non-Residential Services Jane Smith Fiona Low OngoingAmber £705k
Prison Healthcare 25.1 Numbers of Prisoners for potential early release to be identified to ensure that appropriate short term support, if applicable, is available in the Community.
Evelyn Devine Dawn Wigley / Angela Cunningham
/David Morrison
Ongoing Amber
25. Prison Healthcare 25.2 As per Scottish Government Directive progress implementation of Buvidal (weekly/monthly injection) as an alternative form of OST
Evelyn Devine Dawn Wigley/ Angela Cunningham
/David Morrison
Ongoing Amber
25. Prison Healthcare 25.3 Increase capacity for Tele Health options Evelyn Devine Dawn Wigley/ Angela Cunningham
Ongoing Amber
* 2020/21 costs shown in bold have been included inthe Phase 1 Mobilisation Plan Financial Submission to the SG

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
3
Living with COVID-19 –Health and Learning Disability Mobilisation Plan
1. Introduction & Background
On the 17th March the Cabinet Secretary for health placed NHS Scotland in emergency footing for a 3 month period under Section 1 and Section 78 of the National Health Service Scotland Act 1978 as a consequence of substantial and sustained transmission of COVID-19. Within the NHS, non-urgent elective operations and routine care was suspended however a commitment that vital cancer treatment, emergency care, maternity services and urgent medical procedures would continue as usual. It is recognised that COVID-19 will be endemic in society to varying levels for a significant period of time. It is anticipated that normal society will not return and levels of social distancing and lockdown measures will be in place for 12 months or more. For health care systems the constraints of enhanced cleaning, PPE use, social distancing and shielding staff and patients will all have an impact on the ability to deliver the levels of activity prior to the COVID-19 pandemic. The challenge now is NHS Tayside along with Health and Social Care Partners continue to deliver Mental Health and Learning Disability Services whilst safely restoring services to pre COVID levels, learning and retaining the good practice and innovation that has emerged. This paper sets out NHS Tayside, Dundee, Angus and Perth and Kinross Health and Social Care Partnerships (HSCPs) approach and mobilisation plan for firstly, the immediate period to the end of July .The paper sets out a phased and structured approach that will deliver safe, clinically prioritised and risk-assessed patient pathways of care within the constraints of ‘Living with COVID-19’. The plan has been developed in partnership with NHS Tayside, Primary Care, Dundee, Angus and Perth and Kinross HSCPs to ensure a collective whole system response to the delivery of Mental Health and Learning Disability Services across Tayside. Partners have worked collectively to ensure that Mental Health and Learning Disability Services remain accessible and available to people and Table 1 sets out the currents status of Mental Health and Learning Disability Health Services within Tayside. Table 1
Community Mental Health Services (GAP) Changes to Core Function(s) Yes IdentifiedCommunity Learning Disabilities Services Changes to Core Function(s) Yes IdentifiedOlder Peoples Community Mental Health Services Changes to Core Function(s) Yes IdentifiedInpatient GAP Services Changes to Core Function(s) No In DiscussionInpatient LD Services Changes to Core Function(s) No In DiscussionOlder Peoples Inpatient Services Business as Usual Not Applicable Not ApplicableInpatient Substance Misuse Services Stopped Yes In Process of ImplementationYoung Persons Unit Business as Usual Not Applicable Not ApplicableChild and Adolescent Mental Health Outpatient Servic Changes to Core Function(s) No In Process of ImplementationSecure Inpatient Services Changes to Core Function(s) No In Process of ImplementationForensic Community Services Changes to Core Function(s) No In Process of ImplementationIntegrated Substance Misuse Services Changes to Core Function(s) Yes IdentifiedPsychological Therapies Services Changes to Core Function(s) Yes IdentifiedCrisis Resolution and Home Treatment Services Changes to Core Function(s) Yes Identified
COVID19 Changes to Service Delivery
Reinstatement of pre-COVID19 service delivery by end of July
Priority ActionsArea

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
2. Unscheduled Care Following the declaration of lockdown (23 March 2020) there has been a noticeable and sustained decline in daily Emergency Department attendances across Ninewells Hospital and Perth Royal Infirmary. Current attendance rates are approximately 50-70% of normal rates – for both adult and paediatric populations. This is in line with attendance rates for other Emergency Departments in Scotland. Mental Health presentations have been an element of this decrease and Mental Health Services have ensured that appropriate Psychiatric Liaison Services are available at the Emergency Departments on both Ninewells and Perth Royal Infirmary sites. For Ninewells Hospital the total number of Mental Health attendances at Emergency Departments month on month; February – 224, March – 268 and April – 138. Perth Royal Infirmary experienced a trend with attendances dropping month on month; February – 115, March – 87 and April – 60. In addition, there has been a decline in new Emergency and Short Term Detentions under the Mental Health Care and Treatment (Scotland) Act as set out in Table 2 below. Further analysis of emergency and short term detention data is underway to establish patterns and variation. Table 2
3. Living with COVID 19 Mobilisation Plans Crisis Resolution and Home Treatment Services NHS Tayside with Health and Social Care Partners have maintained 7 day a week 24 hour a day Crisis Resolution Services. The Service has developed COVID and non –COVID pathways and has implemented Near Me consultations as part of new ways of working to support patients. Near –me is one of a range of interventions which includes telephone and in person support when needed. The team have experienced a reduction in referral activity in line with other unscheduled care services however retains the capacity to flex to the anticipated increase in demand for mental health support as the psychological and emotional impact of living with COVID. The Service will maintain its COVID and non COVID pathways and offer the same range of support through the use of technology and in-person assessment until the end of July. Further evaluation of the learning from the service changes and in particular remote consultation is underway to consider new opportunities for future service model. Community Police Triage Community Police Triage remains a function of the Crisis Resolution Team and will continue to be provided.
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)AngusEmergency Detention 2 1 -1 7 5 -2Short Term Detention 4 1 -3 2 4 2
DundeeEmergency Detention 11 10 -1 15 18 3Short Term Detention 18 17 -1 18 13 -5
Perth & KinrossEmergency Detention 9 4 -5 13 6 -7Short Term Detention 8 5 -3 13 7 -6
Emergency and Short Term Detention

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
Home Treatment Home Treatment continues to be available to Patients within Dundee and Perth and Kinross. The Home Treatment Teams have implemented Near Me consultations as part of new ways of working to support patients. Near – me video consultation is one of a range of interventions which includes telephone and in person support when needed. General Adult Psychiatry (GAP) In-Patients There has been no change to the overall bed availability within GAP In-Patient Services. However the service moved quickly to establish COVID and non COVID care pathways and developed a deteriorating patient referral pathway with the Acute COVID Hospital Services. The requirement for the COVID pathway has been limited however the plan is to maintain it in place until the end of July in the first instance. There will be a review undertaken of maintaining a COVID pathway beyond July and the advantage and disadvantages of this on capacity and flow will be assessed. Table 3 sets out the admissions and discharges to General Adult Psychiatry In-Patient Services Table 3
Further data analysis is underway to understand admission and discharge trends and patterns. Learning Disability In-Patients Learning Disability In-Patient Service continue to be provided at pre-COVID level. The nature of the Learning Disability Hospital estate is such that it is difficult to identify specific COVID and non COVID pathways however each ward has a contingency plan in place. The impact of social distancing, the requirement for PPE, the cessation of visiting and the disruption of established routines has been particularly challenging for the patient group and staff have worked as flexibly as possible within the restrictions required to minimise this impact. Table 4 Sets out the admissions and discharges to Learning Disability In-Patient Services Table 4
Older Peoples Mental Health In-Patients Older Peoples Mental Health In-Patient Services continue to provide specialist care for older people. There has been no change to overall bed provision however there has been requirement to temporarily close wards to admissions in response to outbreaks of COVID – 19 amongst the patient group.
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)Admissions 95 78 -17 98 77 -21Discharges 111 130 +19 95 62 -33
General Adult Psychiatry Inpatients
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)Admissions 1 0 -1 4 1 -3Discharges 1 2 +1 3 1 -2
Learning Disability Inpatients

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
Older Peoples Service across Tayside have worked collaboratively to ensure that people who require admission can be admitted albeit to a bed outside of their Local Authority Area. Older People In-Patient Services will continue to provide the same level of service. Table 5 Sets out the admissions and discharges to Older People In-Patient Services. Table 5
4. Elective Care
Kinclaven Ward In March the inpatient substance and misuse service at Kinclaven Ward was stepped down. All patients who had planned admission were communicated with and were made aware of the reason for the delay. Planning has commenced for the reinstatement of the service from the 15th June. Initial pa-tient numbers will be restricted to 4 due to social distancing requirements and will prioritise patients requiring alcohol detoxification. Community Substance Misuse Teams have been advised of the recommencement date and are identifying patients for admission. Table 6 Sets out the admissions and discharges to Kinclaven Ward. Table 6
5. Community Mental Health and Outpatient Services NHS Tayside has seen a c60% reduction in outpatient referrals to acute specialities since the lockdown was introduced. In line with government advice, NHS Tayside has prioritised the delivery of new and return outpatient appointments for clinically urgent and cancer patients, and where possible has embraced digital means to support remote consultations. This has led to an expansion in capacity and activity in remote consultation through Near Me and telephone consultation in Mental Health and Learning Disability Services. This is being supported and enabled through a remote consultation programme board. Chart 1. Remote Consultations up to 17th May (Mental Health)
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)Admissions 32 34 +2 30 12 -18Discharges 43 34 -9 34 22 -12
Older People's Mental Health Inpatients
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)Admissions 22 15 -7 26 0 -26Discharges 23 21 -2 26 0 -26
Substance Misuse (Murray Royal Hospital - Kinclaven)

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
Community Mental Health Teams Community Mental Health Teams(CMHT) across Tayside have continued to accept referrals. Two main contextual factors are important in understanding the service delivery during COVID-19. Firstly, existing staff shortages (particularly Consultant Psychiatrists) has meant that within some teams there is already service users who are waiting further out-patient review or allocation to CMHT based staff. Secondly, a number of staff were considered to be in shielding category for their own health and wellbeing (or that of their families) and could fulfil only limited roles. Service users already in treatment have been assessed by the clinical staff providing their care and treatment and consideration given to the most appropriate means of maintaining contact. A very small number of service users indicated that they preferred treatment to be placed on hold until after they could more safely attend face-to-face appointments. Group treatment approaches such as Survive and Thrive and STEPPS and the use of Behaviour Family Therapy have stopped but where this has happened, people have moved to telephone support. Communication was given/sent to all active patients explaining the arrangements for service delivery and signposting to resources. This has been enhanced by the development of resource pages within the respective Council websites and the NHS Tayside internet site. General approach to people awaiting first appointment All mental health services have continued to accept referrals with unchanged eligibility criteria. Following some initial increases in referrals rates, there has been a small reduction in referrals. Referrals have been subject to the same processes as in pre-COVID times where waiting times meant that routine waits might be substantial. Communication explaining the arrangements for service delivery during COVID-19 and signposting to resources has been coordinated and enhanced by the development of resource pages within the respective Council websites and the NHS Tayside internet site. MHO services have continued to deliver all Mental Health Act functions with a reduction in Adults with Incapacity function as determined by the decisions to reduce work at Court level. Face-to-face Detention of service-users in community settings with MHO and Section 22 Approved Psychiatrists has taken place where necessary.

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
Table 7 sets out the referrals Community Mental Health Teams across Tayside. Table 7
A short life working group is developing or has developed (is the group set up) developed guidance for community mental health services in Tayside to help prioritise patients according to their needs and the functions provided to meet those needs. This involved services from Community Mental Health Services, Integrated Substance Misuse Services, Learning Disability Services, CAMHS, Psychological Therapies Services and the Multidisciplinary Adult Psychotherapy Service. This risk based approach has been developed to enable Community Staff to prioritise patients in the event of staff shortages. Primary Care Supports available at a primary care level have been a clear focus with opportunities for enhanced support being identified through Social Prescribing and Primary Care Liaison roles. It is anticipated that the same level of service will be provided until the end of July. Feedback from an out of hours General Practice perspective has been positive with opportunity to continue to improve upon the General Practice/Crisis Care interface.
Craigmill Centre The Craigmill Centre provides therapeutic support and interventions to individuals with a Learning Disability Diagnosis who have a forensic history with challenging behaviour on an out-patient and day patient basis. The Centre stepped down it service provision from the 1st April and individual community risk assessed support is being provided through a range of contacts along with regular review and support for care providers. The service will continue this model of care delivery until July.
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)Child and Adolescent Mental Health Services (CAMHS) 102 111 +9 60 31 -29
Paediatric Neurodevelopmental 58 40 -18 47 14 -33Forensic Psychiatry 3 7 +4 13 4 -9Community Psychiatry 1 0 -1 6 0 -6Dundee Community Mental Health East Team 37 41 +4 47 21 -26
Dundee Community Mental Health West Team 52 46 -6 45 22 -23General Psychiatry - Arbroath/Carnoustie CMHT 33 39 +6 47 20 -27General Psychiatry - Dundee Crisis Team 189 161 -28 191 110 -81General Psychiatry - Forfar/Kirriemuir CMHT 18 25 +7 25 12 -13
General Psychiatry - Montrose/Brechin CMHT 37 35 -2 25 20 -5General Psychiatry - North Perth CMHT 18 11 -7 21 11 -10General Psychiatry - Perth City CMHT 53 97 +44 76 70 -6General Psychiatry - South Perth CMHT 20 18 -2 17 11 -6Liaison Psychiatry 91 96 +5 79 43 -36Tayside Adult Autism Consultancy Team 19 14 -5 15 7 -8Tayside Eating Disorder Service 5 1 -4 8 1 -7Tayside Substance Misuse - Alcohol 45 22 -23 26 5 -21Tayside Substance Misuse - Dundee 45 43 -2 39 34 -5Tayside Substance Misuse Service 98 90 -8 112 81 -31Learning Disability 44 34 -10 65 23 -42Psychiatry of Old Age 228 193 -35 234 108 -126Psychotherapy 22 6 -16 6 4 -2
Outpatient Referrals(Total Routine,Urgent and Emergency Referrals Received)
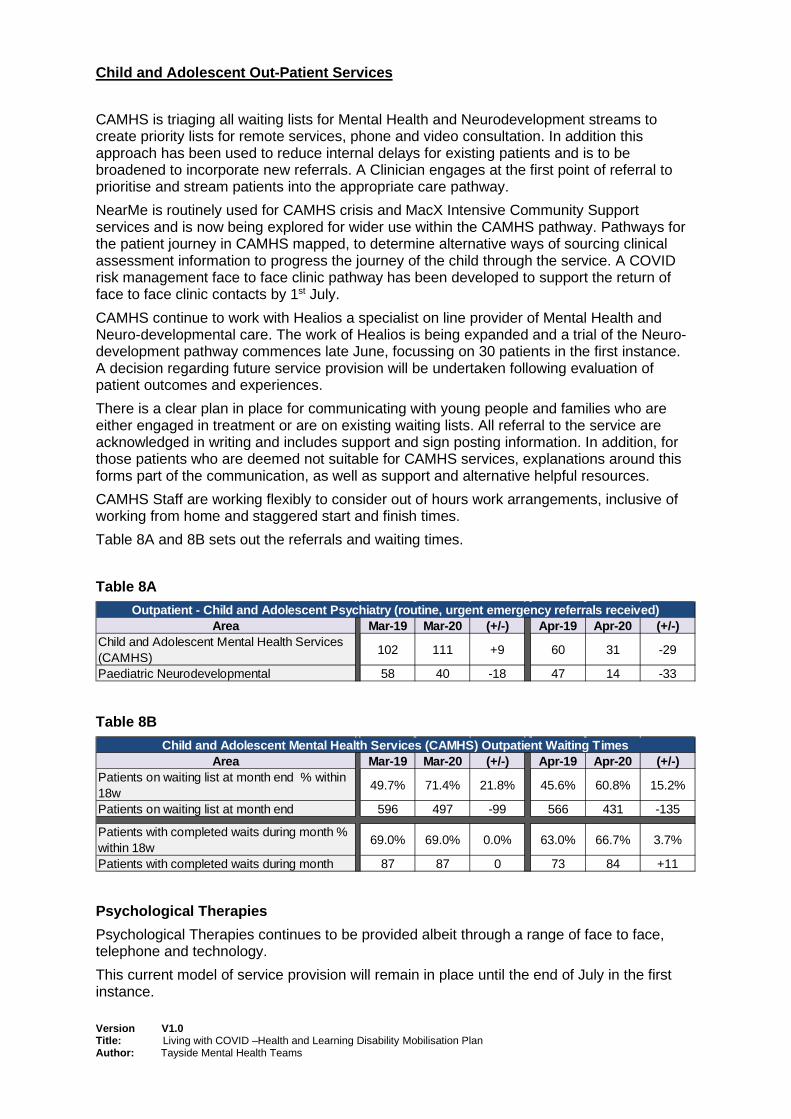
Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
Child and Adolescent Out-Patient Services CAMHS is triaging all waiting lists for Mental Health and Neurodevelopment streams to create priority lists for remote services, phone and video consultation. In addition this approach has been used to reduce internal delays for existing patients and is to be broadened to incorporate new referrals. A Clinician engages at the first point of referral to prioritise and stream patients into the appropriate care pathway. NearMe is routinely used for CAMHS crisis and MacX Intensive Community Support services and is now being explored for wider use within the CAMHS pathway. Pathways for the patient journey in CAMHS mapped, to determine alternative ways of sourcing clinical assessment information to progress the journey of the child through the service. A COVID risk management face to face clinic pathway has been developed to support the return of face to face clinic contacts by 1st July. CAMHS continue to work with Healios a specialist on line provider of Mental Health and Neuro-developmental care. The work of Healios is being expanded and a trial of the Neuro-development pathway commences late June, focussing on 30 patients in the first instance. A decision regarding future service provision will be undertaken following evaluation of patient outcomes and experiences. There is a clear plan in place for communicating with young people and families who are either engaged in treatment or are on existing waiting lists. All referral to the service are acknowledged in writing and includes support and sign posting information. In addition, for those patients who are deemed not suitable for CAMHS services, explanations around this forms part of the communication, as well as support and alternative helpful resources. CAMHS Staff are working flexibly to consider out of hours work arrangements, inclusive of working from home and staggered start and finish times. Table 8A and 8B sets out the referrals and waiting times. Table 8A
Table 8B
Psychological Therapies
Psychological Therapies continues to be provided albeit through a range of face to face, telephone and technology. This current model of service provision will remain in place until the end of July in the first instance.
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)Child and Adolescent Mental Health Services (CAMHS) 102 111 +9 60 31 -29
Paediatric Neurodevelopmental 58 40 -18 47 14 -33
Outpatient - Child and Adolescent Psychiatry (routine, urgent emergency referrals received)
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)Patients on waiting list at month end % within 18w 49.7% 71.4% 21.8% 45.6% 60.8% 15.2%
Patients on waiting list at month end 596 497 -99 566 431 -135
Patients with completed waits during month % within 18w 69.0% 69.0% 0.0% 63.0% 66.7% 3.7%
Patients with completed waits during month 87 87 0 73 84 +11
Child and Adolescent Mental Health Services (CAMHS) Outpatient Waiting Times

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
Table 9 sets out the referrals and waiting times Table 9
6. Regional Services Secure Care Services Secure Care Services have been reporting to the Restricted Patient Team in Scottish Government initially on a weekly and now a fortnightly basis. The focus has been on the management of restricted patients and the continuation of Regional and National Secure Services during Covid-19 The Service initially stepped down planned admissions, transfers and discharges from the 23rd March 2020. The planning for admissions and transfers resumed on the 4th May and there have been subsequent admission to the Low Secure Service. The planning for discharge to the community has become more challenging and some discharges had to be delayed at the end of March, due to the lack of support packages in the community compounded by the impact of Covid-19. The Service have introduced Near-Me consultation to support Community Patients and has maintained regular contact both verbally and in writing, with patients on the waiting list for admission or transfer and their local teams and carers. We have no other waiting list for patients in our service. The Service will continue with this planned level of service until the end of July. Young Persons Unit The Regional In-Patient Service has been maintained at the Young Persons Unit and there has been no change to inpatient capacity. There have been some changes to the delivery of therapeutic services and new ways of supporting family and carer visiting for the young people using ‘virtual’ approaches. Communication has been maintained across the Regional Network to review and respond to new ways of working.
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)Patients on waiting list at month end % within 18w 65.3% 60.6% -4.7% 65.1% 57.4% -7.7%
Patients on waiting list at month end 2436 2605 169 2322 2188 -134
Patients with completed waits during month % within 18w 72.3% 66.2% -6.1% 70.5% 62.5% -8.0%
Patients with completed waits during month 647 616 -31 610 496 -114
Psychological Therapies Outpatient Waiting Times
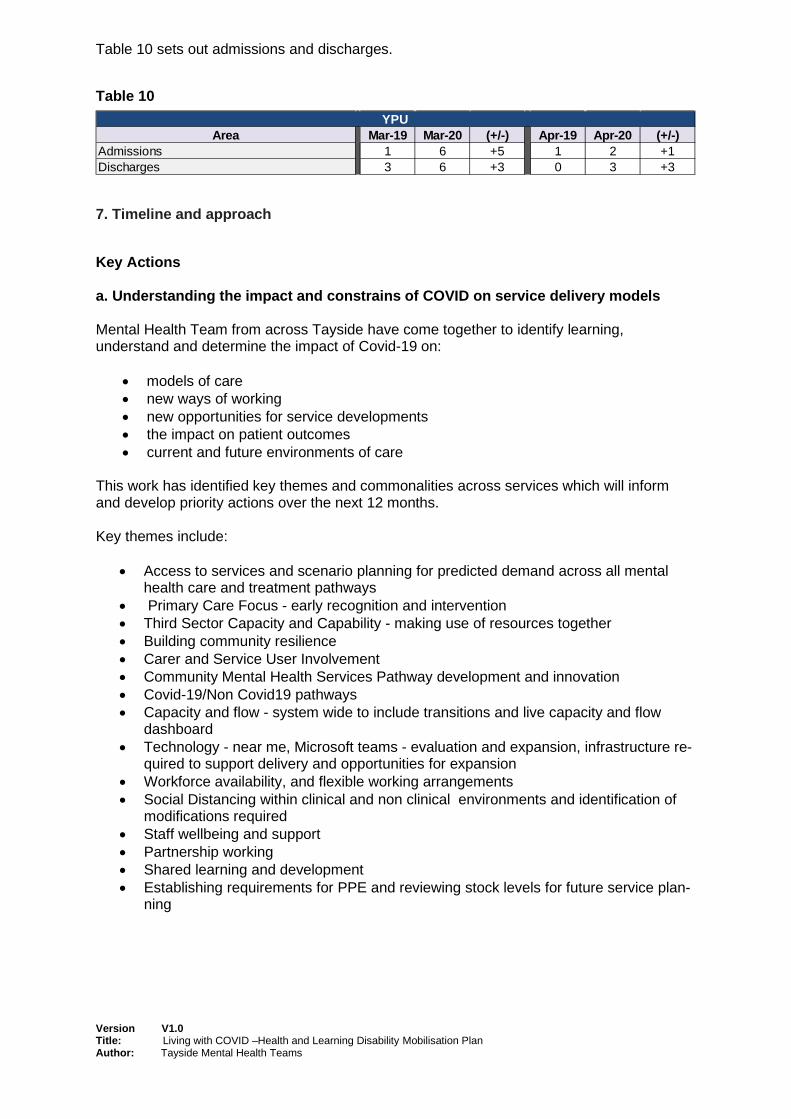
Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
Table 10 sets out admissions and discharges. Table 10
7. Timeline and approach
Key Actions a. Understanding the impact and constrains of COVID on service delivery models Mental Health Team from across Tayside have come together to identify learning, understand and determine the impact of Covid-19 on:
• models of care • new ways of working • new opportunities for service developments • the impact on patient outcomes • current and future environments of care
This work has identified key themes and commonalities across services which will inform and develop priority actions over the next 12 months. Key themes include:
• Access to services and scenario planning for predicted demand across all mental health care and treatment pathways
• Primary Care Focus - early recognition and intervention • Third Sector Capacity and Capability - making use of resources together • Building community resilience • Carer and Service User Involvement • Community Mental Health Services Pathway development and innovation • Covid-19/Non Covid19 pathways • Capacity and flow - system wide to include transitions and live capacity and flow
dashboard • Technology - near me, Microsoft teams - evaluation and expansion, infrastructure re-
quired to support delivery and opportunities for expansion • Workforce availability, and flexible working arrangements • Social Distancing within clinical and non clinical environments and identification of
modifications required • Staff wellbeing and support • Partnership working • Shared learning and development • Establishing requirements for PPE and reviewing stock levels for future service plan-
ning
Area Mar-19 Mar-20 (+/-) Apr-19 Apr-20 (+/-)Admissions 1 6 +5 1 2 +1Discharges 3 6 +3 0 3 +3
YPU

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
The Services have started to develop detailed plans that will consider:
• How much work can be delivered remotely/technology • The Need to have a scalable and sustainable plan for further potential surges in
COVID cases and peaks of admission
The key elements of which will be:
• Developing different models of care utilising more care in the community • Establishing and maintaining Patient Advice Lines • Enhanced vetting • Remote working and consultation - telephone and near me • Face to face where necessary - reduced numbers per clinic • Flexible and extended day working – evening and weekends – patient centre
Given the outline above that we have attempted to continue to deliver our key functions, the main changes to be implemented are the balance between remote and face-to-face contact with service users and carers. This will be critically influenced by:
o The availability of space for staff where they can be socially distanced
o The availability of waiting area space for service users where they can be socially distanced
o The availability of public transport
o The end point of shielding arrangements for staff and overall availability of the work-force
8.Staff Wellbeing
Staff wellbeing has been a key consideration for NHS Tayside and the Local Authorities and significant work has been undertaken to develop resources, information and services that staff can access and engage with. In order to maintain individual’s mental health and Wellbe-ing and also to notice and appreciate the impact that Covid -19 is having on people. Invest-ment in the development of Rest, Relaxation and Recuperation (triple R) rooms is underway.
9. Communication Both local Council and NHS Tayside websites have clear mental health and wellbeing advice; for staff and service users. Staff in a range of disciplines within the mental health family have written and produced online videos to support wellbeing and direct people to trusted resources.
10. Infrastructure & Innovation Mental Health and Learning Disability Services are linking with the wider NHS Tayside Digital Directorate in relation to the technological infrastructure required to support and develop services. 11. Patient Management Systems Work is progressing between the Digital Directorate and our clinical teams to develop and update digital solutions to support flexible and remote working across clinical services. Clinical builds and templates in TRAK, the referral management system and clinical portal are all being reviewed and updated to facilitate digital ways of working, ensuring robust referral management, patient consultation and advice, as well as waiting list and outcome management.

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams
12. Financial Framework It is critical that appropriate consideration is given to financial aspects in terms of both affordability and sustainability as plans are taken forward. We continue to work closely with Finance colleagues to ensure our Living with Covid-19 financial plan aligns directly with how our services are operating on the front-line and reflects the revised pathways outlined earlier in this paper. It’s important that we continue to work with our HSCP partners and harness the impact of changes within Primary Care as these develop over time, particularly where that leads to a shift in the balance of care. To support this work we have developed a “Whole System Financial Framework” as a tool to support the implementation of future service change plans involving shifting services from acute hospital setting into the community and primary care setting. The framework articulates a process for resources to be moved across organisational boundaries. 13. Conclusion Mental Health and Learning Disability Services have responded effectively to the many challenges associated with COVID. The Services response has been characterised by joint working, collective planning and the willingness to share and learning from others experiences. There is a recognition that there is work still to be done in preparation for living with COVID and responding effectively to any future peaks of infection. However there is a collective focus and determination to continue to provide person centred mental health care and treatment.

Version V1.0 Title: Living with COVID –Health and Learning Disability Mobilisation Plan Author: Tayside Mental Health Teams

NHS Tayside Mobilisation Plans: Next Phase: Workforce Page 1 of 3
4 Mobilisation Plans: Next Phase WORKFORCE Introduction In our immediate response to Covid-19, many changes have been implemented to ensure the safety of staff and patients, particularly in those areas dedicated to caring for those who are Covid-19 positive and in the continued our delivery of emergency, urgent and cancer services. The challenges of remobilisation of elective care delivery whilst continuing to meet Covid-19 clinical priorities will mean that managers and staff will require to further adjust to different working arrangements in all areas including hospital, mental health and community-based services. Its delivery in our Operational Unit and through our three Health and Social Care Partnerships must be built on strong partnership working trade unions, and full engagement with our workforce, discussing together how we best respond to protect both themselves and those we serve. Staffing Our Services: Promoting Workforce Agility Key to our successful remobilisation will be adopting alternative ways of working which promote a safe working environment. The impact of a new societal ‘normal’ as we learn to live with Covid-19 - including, for example, changes to carer responsibilities arising from the Scottish Government’s approach to blended learning, and emerging changes around how and when staff commute to and from the workplace - will directly influence workforce availability, and therefore the way in which we deliver our services in the future. Given the wide range of clinical and non-clinical environments across the NHS, it is not possible to identify a single common approach. Each specialty will require to identify what is appropriate for its area in order to deliver effective services and produce a revised workforce model accordingly. Building on existing NHS Scotland’s ‘Once for Scotland’ approach within PIN Guidelines, and other existing employment policies, services are being asked to plan against the range of options for alternative working arrangements. Work is already underway, with service areas being asked to determine what measures will be appropriate, with specialist advice available to them from HR, Health and Safety, Occupational Health, and Infection Control. These include consideration of compressed hours, staggered hours, and alternating days. This is alongside further developing technologically-enabled solutions that facilitate, where appropriate, enhanced remote working or working at home, occasionally or part of a week. This may be required in order to maintain social distancing within a work area where, through use of PPE or workspace redesign, where there is no safe alternative. Work is ongoing to increase the Board’s digital capacity and facilitate critical developments such as remote consultation, diagnostic reporting, and enable agile working by key clinical staff and other service-critical teams. This should be viewed as a primary enabler to new and different working arrangements. Partnership working will continue to underpin the approach to staff engagement in NHS Tayside. Such an approach will clarify the pros and cons of different working arrangements, promote staff understanding and involvement in decisions which affect staff, and provide an opportunity to generate ideas for improvement.
NHS Tayside Mobilisation Plans: Next Phase: Workforce Page 2 of 3
At the outset of the Coronavirus pandemic, NHS Tayside took early steps to establish a Staff Deployment Centre which aimed to ensure staff, those from outside our organisation who reached out to be part of the NHS, and volunteers, were deployed in the places we needed them most, when we needed them most. From this, we are now establishing an all-Staff Bank that aims to maximise workforce flexibility and ensure we have a wider pool of skilled and experienced staff available for rapid deployment in circumstances of any second Covid-19 infection wave. Health and Safety Our primary focus must be to ensure that work areas are safe for patients and staff alike, and compliant with national and local guidance. This will require our organisation to make practical changes to ensure maintenance of physical distancing and enhanced infection control within the workplace, as part of the ‘new normal’ as we adjust to living with Covid-19. While continued observation of advice designed to control the virus - through regular hand washing, provision and use of appropriate PPE, and basic cough hygiene - will remain essential, we have a duty to reduce workplace risk to the lowest reasonably practicable level by taking preventative measures. To help meet that duty, NHS Tayside has led development of detailed guidance on applying physical distancing for staff within the workplace. This is built upon UK-wide advice published by the Health and Safety Executive (HSE). Services, working in partnership, will need to translate this guidance in to any specific actions it believes it will need to take in our workplaces, including within our patient facing areas. These plans will then be subject to separate risk assessment with input from Health and Safety and Infection Control specialists. Where agreed, services will be expected to act to assess and take action to implement any appropriate adjustments, whether physical or by changing how work is organised, operated and managed, and in partnership monitor ongoing compliance. While taking these steps to ensure staff safety, we must ensure that as a healthcare organisation we take similar steps to enable the safe provision of services to those who look to us for their care. Many of the potential adjustments that will be identified using the guidance referenced above will be of mutual benefit to those who use our services; separate work is however also taking place to further review our hospital environments to ensure the wellbeing of our patients. In particular, how we manage access to and movement in our common public areas, how we facilitate safe patient transport and travel, and through the benefits of existing Scottish Government intervention promote best use of our currently-free car parking facilities. Mental Health, Wellbeing and Staff Support In response to the COVID-19 pandemic, the Scottish Minister for Mental Health contacted all Health Board Chief Executives dated 27 March 2020, requesting that that current staff health and wellbeing support structures are maintained and enhanced during COVID-19. This was further echoed in correspondence to all Boards from the Minister dated 26 March 2020, including a nationally-developed ‘Health and Wellbeing Communications Toolkit’ adopted by NHS Tayside in full. The Coronavirus pandemic has already placed huge pressure on staff across NHS Tayside. Change continues to run at a very fast pace, with many staff being asked to take on new roles, work in different ways, and work in completely different areas. Each employee also carries the strain of their own domestic concerns, with restricted travel, school closures, food access issues and the risk these may pose to their family. NHS Tayside made an early determination in partnership to ensure a coordinated approach to promote staff wellbeing and support both practical measures and staff mental health during this period.

NHS Tayside Mobilisation Plans: Next Phase: Workforce Page 3 of 3
Building on the excellent toolkit produced nationally to support NHS Scotland staff, NHS Tayside has put in place a wide range of resources that support individual resilience. This sits alongside ensuring basic practical provision of essentials such as ensuring easy access to water in workplaces, to guidance helping team leaders offer the right support at the right time to those they manage. Working together with our trades unions, there is now a package of online tools on our dedicated wellbeing web pages, access for all staff to 24:7 counselling services, and staff side colleagues have co-led the roll out of the Rest, Relax and Refresh rooms across our clinical sites. These health and wellbeing resources sit alongside and complement our existing Occupational Health, Healthy Working Lives, and Wellbeing specialty support services. These actions, and more, are led by the Board’s Wellbeing Group, which reports through our Health & Safety Committee into the Staff Governance Committee. This focus on extended support for staff mental health and wellbeing remains a key Area Partnership Forum priority, and ensures we retain the strategic oversight and organisational commitment required to support staff in implementing changes in these challenging and stressful times.